
Submitted:
18 April 2025
Posted:
19 April 2025
You are already at the latest version
Abstract
A process evaluation was embedded in the multinational Music Interventions for Dementia and Depression in ELderly care (MIDDEL) trial to better understand barriers and facilitators for implementation of music-based interventions. Stakeholders from 66 care home units across 5 countries completed a survey at baseline (n = 229) and after the six-month intervention period (n = 101), comparing expectations and experiences between countries, intervention groups, and stakeholders. MBIs were evaluated as relevant and feasible. Main implementation barriers include lack of support, changes in employees, lack of motivation. Facilitators include: people involved facilitate and stimulate implementation, stable well-functioning teams, clear communication, and maintaining project planning. Presence of barriers related to care staff workload and time investment needed for implementing new MBIs in care homes were less than expected. Involving stakeholders in key positions is essential: care home managers are pivotal for policy making and sustainable adoption of MBIs, whereas commitment and involvement of care staff is needed for day-to-day implementation. MBIs can be beneficial for people with dementia, yet implementation of in care homes can be challenging due to contextual factors. Insight into influential barriers and facilitators of implementation can contribute to the interpretation of effect study results.
Keywords:
long-term care
; dementia
; music-based intervention
; music therapy
; singing
; program evaluation
; process evaluation
; implementation
1. Introduction
Over 55 million people live with a type of dementia worldwide, a degenerative syndrome that affects cognitive and behavioral functioning, and this number is only expected to increase in the coming decades (Dementia, 2023). Depression is a common manifestation of neuropsychiatric symptoms in dementia, although the nature of the relationship between dementia and depression remains unclear (Leung et al., 2021; Matovic et al., 2023; Wiels et al., 2020). Music-based interventions (MBIs) have been found effective in improving symptoms of depression and quality of life in people with dementia (Baker et al., 2022; Kishita et al., 2020; van der Steen et al., 2025), but the quality of evidence of these non-pharmacological interventions varies (Meyer & O’Keefe, 2020; Vink & Hanser, 2018). Studies that assess effectiveness of MBIs to date often have a small sample size, weak research design, or insufficiently reliable results (van der Steen et al., 2025). Often, a description of basic elements and the rationale for the intervention is lacking (Sousa et al., 2021). Detailed intervention description and research reporting are essential components to be able to replicate, interpret, and translate research findings to practice (Sousa et al., 2021). MBIs are complex and are delivered and evaluated at multiple levels (Skivington et al., 2021). There can be interacting components, various stakeholders with different characteristics and needs, and differences in contexts in which the intervention is implemented. The implementation and uptake of an MBI can vary between care home organizations due to a range of organizational, staff-related, and environmental factors.
Common implementation strategies of MBI for people with dementia in care homes include education, quality management, planning, restructuring, and costs. Outcomes include appropriateness, fidelity, adoption, sustainability, and acceptability, differentiating between studies focusing on music therapy provided by a trained music therapist and individualized music provided by care staff or researchers (Amano et al., 2021). Recommendations for implementing an individualized music listening intervention included contextual factors, such as the presence and influence of care staff in sessions and placement in and interaction with the environment (Töpfer et al., 2024). Main implementation barriers include limited staff time, low staff engagement, lack of training, high costs, and technical issues. Facilitators include stakeholder support, observed positive effects, training, family involvement, accessible equipment, and financial resources (Kwak et al., 2020; Sung et al., 2008). However, evidence on barriers and facilitators for group BMIs in this context remains limited.
To address this gap, a process evaluation of the multinational trial Music Interventions for Dementia and Depression in ELderly care (MIDDEL) was conducted to gain insight into implementation in various different country contexts, to assess whether MBIs were implemented as intended, and to identify factors which appear to determine successful implementation. In other words, the overall aim of this study was to assess barriers and facilitators for MBI implementation across countries, care homes, and residents. Evaluation of these contextual aspects of implementation informs the overall assessment of acceptability and feasibility of MBIs. In accordance with Leontjevas' framework, first- and second-order process data were examined (Leontjevas et al., 2012). The first-order process evaluation includes assessment of intervention quality, internal and external validity, after which intervention effects and cost effectiveness can be examined. A second-order process evaluation combines implementation knowledge such as insights into hindering and facilitating factors for future interventions and studies.
The primary objective of the process evaluation was to gain insight into intervention quality, measured by satisfaction, relevance and feasibility (first-order process data), and presence and influence of anticipated and experienced potential barriers and facilitators for implementation (second-order process data) of MBIs for people with dementia and depression in care homes of different stakeholders. To this end, differences between expected and perceived barriers and facilitators between allocated intervention groups (GMT, RCS, GMT+RCS combined, control) at baseline (T0) and post-intervention (T6) were described in the current study. Differences between stakeholders and countries were described beforehand, to get a thorough picture of potential barriers and facilitators that occur in day-to-day practice.
2. Materials and Methods
2.1. About the MIDDEL Trial
Music Interventions for Dementia and Depression in ELderly care (MIDDEL) was a multinational cluster-randomized controlled trial, conducted in Australia, Norway, Germany, the UK, Türkiye, and the Netherlands. A total of 86 care home units (CHUs, an organizational cluster of residents that live together and are cared for by care staff) with 1021 residents were included in the main study. Each CHU with its consenting residents with dementia and (at least mild) depressive symptoms was randomly allocated to one of four intervention groups: 1) group music therapy (GMT), 2) recreational choir singing (RCS), 3) the combination of both (combi), 4) care as usual (control group receiving no MBIs) (Figure 1). GMT and RCS are two widely used group MBIs (Gold et al., 2019). GMT was offered by a trained music therapist to groups of approximately five to seven care home residents. GMT sessions consisted of an introduction with a welcome song, singing familiar songs and reminiscence, optional improvisation on instruments, optional movement to music, singing familiar songs again, and ending with a closing song. Core principles of GMT were affect regulation through reciprocal musicking, attunement, meeting psychosocial needs of individual residents, working in the here and now, and relationship building. RCS was offered by a skilled musician in groups of ten or more residents. RCS sessions consisted of an introduction with welcome song, singing familiar songs, learning new songs, and ending with a closing song. Core principles of RCS were to sing familiar songs, provide a familiar musical environment, foster connectedness, emotional well-being and enjoyment. After completing baseline assessment (T0), MBIs were offered twice a week for 45 minutes per session in month 1-3, and once a week for 45 minutes in month 4-6. Follow-up assessments in the main study were carried out by blinded assessors at 3 (T3), 6 (T6) and 12 (T12) months after randomization. The aim of MIDDEL was to assess and compare the effectiveness of GMT and RCS, primarily on depressive symptoms in care home residents with dementia (clinical trial registration nr NCT03496675, Gold et al., 2019). The primary outcome was the severity of depressive symptoms at six months (T6) measured with the Montgomery-Åsberg Depression Rating Scale (MADRS) (Montgomery & Åsberg, 1979). Secondary outcomes included cognitive functioning, neuropsychological symptoms of dementia, quality of life, well-being, stress levels, care staff sick leave days and caregiver burden.
2.2. Study Design
A survey was developed to assess first- and second-order process data related to the MIDDEL trial, which is described in detail elsewhere (Gold et al., 2019). The framework of Leontjevas (Leontjevas et al., 2012) has been used by previous studies to perform first- and second-order process evaluations of interventions for care home residents with dementia (Appelhof et al., 2018; Dam et al., 2019; Kormelinck et al., 2019; Zwijsen et al., 2014). This framework argues that once the validity of the study or intervention has been confirmed (step 1), effects and cost-effectiveness can be examined (step 2), which together with knowledge about implementation (step 3) can be decisive for further implementation or improvement of the intervention (Figure 2) (Leontjevas et al., 2012). The focus of the current study was on intervention quality (relevance, feasibility, satisfaction) and on barriers and facilitators for implementation. The process evaluation was embedded in the main MIDDEL trial (Figure 1), and included the five European countries involved in the project (excluding Australia due to differences in time of recruitment). The optional survey at timepoint T12 was excluded in the current study, due to the primary outcome being at T6, and risk of recall bias amongst participants six months post-intervention period.
2.3. Participants
Care home managers, care staff, and interventionists associated with CHUs and residents involved in the MIDDEL trial were eligible for participation; they were asked for their views about implementation of the MIDDEL trial. We defined care home managers as persons acting as location managers, policy and development functions, staff officers and supervisors. Care staff was defined as registered nurses, enrolled nurses, personal care attendants, allied health professionals, leisure staff or others. Interventionists were music therapists and choir leaders who provided MBIs (GMT and/or RCS) at one or more participating care homes.
2.4. Survey Development
The survey was initially developed in English by NR, MS, SJ, AV and SZ. To enable comparisons between countries and reduce language barriers, only closed binary questions (such as yes-no questions) and five-point Likert scale questions were used. The first version of the survey was shared with all researchers involved in the MIDDEL trial for feedback. In the adapted second version of the survey, each country marked questions that did not apply to their national situation and sent the remarks to the survey to the Dutch researchers, who adapted the survey accordingly. Next, researchers from each country translated the survey to their national language (Dutch, German, Norwegian, and Turkish). The Dutch MIDDEL Team developed a REDCap database for the process evaluation, including the Multi-Language Management module that enabled each respondent to fill out the survey in their national language (Harris et al., 2019). The survey was available in paper format and online via the REDCap electronic data capture web application (Harris et al., 2019), hosted at the independent research institute NORCE (NORCE, n.d.). The survey was distributed 1) at baseline (T0, prior to allocation to one of the four intervention groups), 2) six months after randomization, at the end of the intervention period (T6, post-intervention), and 3) an optional long-term follow-up twelve months after randomization (T12, follow-up). The T0 survey focused on expectations of participants about the trial, whereas the T6 and T12 survey focused on experiences. The survey was adapted to be appropriate for the targeted stakeholder, meaning the survey had minor differences for each stakeholder: management, care staff, and interventionists. To illustrate, the baseline (T0) survey questions and statements were formulated in simple future tense (e.g., “Recreational choir singing will be relevant for the care home residents with dementia and depressive symptoms.” and “Please indicate below for each factor (regardless of whether it is hindering or facilitating) to what extent you expect its presence may influence the implementation of the intervention.”). Items of the post-intervention survey T6 were formulated in the past tense (e.g., “To what extent were you satisfied with the implementation of the MIDDEL-project?” and “Please indicate below for each factor or statement whether this was applicable within your organization during the MIDDEL-project”). A single statement, for which stakeholders indicated to what extent a factor was present, was worded differently per stakeholder. The statement for managers was “Lack of support from board of directors to implement the MIDDEL-project”, whereas the statement for care staff was “Lack of support from care home management to implement the MIDDEL project”.
Common barriers and facilitators for implementation of complex psychosocial interventions in care homes were identified in previous RCTs and formed the basis of the survey. The survey consisted of multiple sections that were similar across stakeholders and timepoints: (1) informed consent; (2) demographics; (3a) relevance and feasibility; (3b) effect; (3c) satisfaction; (3d) implementation and sustainability; (4) barriers and facilitators related to care home organization and staff; (5) barriers and facilitators related to MBIs. The surveys of the stakeholder “Care staff” can be found in Supplemental file 1 (English version), as most surveys were filled out by care staff.
2.5. Procedure
The research team of each country distributed information and surveys in paper format and/or electronically via email. The aim and procedures of the process evaluation were explained in the national language, and all participants provided informed consent before answering the survey. Initially, a response rate of 30% was targeted, to be able to make reliable statements about barriers and facilitators to implementation of the MBIs, and to ensure collection of a full range of perspectives of different stakeholders from different countries. The research team of each country decided for themselves how many surveys to send out, depending on burden and time investment. Each country distributed the survey to different stakeholders (management, interventionists, and care staff) at 2 or 3 timepoints (T0, T6, optional T12). In practice, this meant – estimating 4 CHUs participate in 1 care home organization – in each care home organization in each country at timepoints T0, T6 (and optional T12), surveys were filled out by at least: 1 care home manager; 2 interventionists (1 music therapist, 1 choir leader); 4 care staff. Surveys were distributed from the start of the European MIDDEL trial in 2020 until the last assessments in summer 2023.
2.6. Data analysis
Data were analyzed using SPSS version 28. Demographics, views related to relevance and feasibility, effect and satisfaction, implementation and sustainability, and barriers and facilitators for implementation from care home managers, care staff and interventionists of the participating countries were analyzed using descriptive statistics. The authors decided not to include a statistical test to assess whether differences between allocated groups were significant, as this surpasses the descriptive purpose of this study. First, data were stratified by stakeholder to describe differences between stakeholders at baseline (T0) and post-intervention (T6). Second, data were stratified by country to describe baseline (T0) differences. Third, data were stratified by allocated intervention group. Sample size varied across countries, stakeholders and timepoints. Median and interquartile ranges were provided for all Likert-scale questions. For yes/no questions, the percentages were provided. Differences between stakeholders, countries, and intervention groups were visualized using heatmaps. For pragmatic reasons, due to the amount of data, differences in percentage of respondents that answered ‘Yes’ to whether a statement would be/was applicable are described in text only if the differences within/between groups are larger than 20%. Similarly, differences in the median of the extent to which a factor influenced implementation are described only for those factors illustrating a difference of 2 points or more within/between groups.
3. Results
The survey was completed by 229 respondents at baseline and by 101 respondents at T6. A total of 453 surveys were started, of which 11 were excluded (6 respondents only filled out the informed consent form, 5 respondents from the UK filled out a survey not corresponding to their stakeholder role). In the results section of this paper, the largest observed differences between stakeholders, countries and intervention groups are highlighted and discussed. Figure 3 provides an overview of the total number of completed surveys (n = 442 surveys) during the MIDDEL trial, of which 330 (T0 plus T6) were included in the current study.
3.1. Comparison at stakeholder-level
Baseline and post-intervention surveys were filled out by care home managers (n = 36 at baseline, n = 19 post-intervention), interventionists (n = 32 at baseline, n = 19 post-intervention) and care staff (n = 161 at baseline, n = 65 post-intervention). Descriptive characteristics of the sample at baseline (T0) and post-intervention (T6) are presented per stakeholder group (Table 1). Majority of respondents were care staff and in each stakeholder group, majority of respondents were female (72.7% - 88.9%). Majority of interventionists were aged 18 – 29 years (38.5% - 50.0%). Over 50% of care staff had over a decade of work experience, while around one-third of interventionists had less than two years, and over half of them less than five years of work experience. Less than one third (n = 7, 28.0%) of interventionists worked at the care home organization before the start of the MIDDEL trial. Twenty percent of care home management and care staff indicated that no MBI such as GMT or RCS was being provided in their care home. In each stakeholder group, the majority of respondents were involved throughout the entire duration of the MIDDEL trial. Stakeholders were not blinded for intervention group allocation. Nevertheless, at post-intervention (T6), half of the stakeholders did not know the exact intervention group (GMT, RCS, COMBI, or CONTROL) their CHU(s) and its residents were allocated to.
Expectations (T0) and experiences (T6) regarding relevance and feasibility were comparable across stakeholder groups, except for the statement ‘I know which tasks I have to fulfill for the MIDDEL-project’ at baseline, interventionists strongly agreed (median 5.0), most care staff neither agreed nor disagreed (median 3.0) (Table 2). Across stakeholders, effect of MBIs was noticed most in care home residents. Interventionists reported the highest percentage of observed effects, followed by care home management.
Heatmaps are used to shows differences within and between stakeholders before (T0) and after (T6) the intervention period of six months from the stakeholder (Figure 4), country (Figure 5) and intervention group (Figure 6) perspective. Grey columns represent applicability of barriers and facilitators, with darker grey indicating more respondents expected/experienced that factor to be present. Blue columns represent influence of those barriers and facilitators, with darker blue indicating higher expected/experienced influence of a factor.
Within interventionists, the barrier of ‘lack of support’ was more applicable than expected. In contrast, the barriers ‘high workload of care staff’ and ‘keeping a music intervention running’ were less present than expected. The facilitator ‘people involved facilitate and stimulate implementation’ was less applicable than expected by interventionists. The barrier ‘lack of care staff’ was less than expected both within care staff and within interventionists. Within care staff, the barriers ‘reorganizations’, ‘participating in other projects’, and ‘general resistance to change’ were less present than expected. The barrier ‘in general, implementing an intervention on the CHU takes a lot of time’ was less applicable than expected within each stakeholder group.
Differences between stakeholders’ expectations at baseline show most care home managers expected presence of the facilitator 'open communication and flat hierarchy' to be high and of barriers 'lack of care staff' and ‘reorganizations’ to be low, in contrast to expectations of care staff and interventionists. Managers expected the facilitator ‘integration of music interventions in the care program’ to be present, compared to interventionists. Compared to care staff, more managers expected ‘difficulties due to COVID’. Interventionists expected presence of barriers ‘participating in other projects’ and ‘changes in employees’, more than care staff and management. Compared to care staff they expected less presence of ‘lack of support’ and ‘general resistance to change’. Compared to managers, more interventionists expected presence of the barrier ‘high workload for care staff’.
Differences between stakeholder experiences indicate presence of the facilitator ‘stable, well-functioning teams’ was lower and barriers ‘changes in employees’ and ‘lack of motivation among those involved’ was higher for interventionists. Compared to care home management, interventionists experienced more presence of barriers ‘lack of support’, ‘people involved facilitate and stimulate implementation’, but less presence of ‘participating in other projects.’
The influence of barriers and facilitators differed within stakeholder groups (2.0 points difference in median) for three factors: influence of the facilitator ‘stable and well-functioning teams’ was larger than expected according to interventionists (median 2.0 to 4.0), whereas influence of the barrier ‘lack of motivation amongst those involved’ was lower than expected (median 4.0 to 2.0). For care home managers, influence of the barrier ‘in general, implementing an intervention on the CHU takes a lot of time’ was lower than expected (median 4.0 to 2.0).
Differences between stakeholders in expected influence of factor indicated interventionists expected less influence of the facilitator ‘stable, well-functioning teams’ (median 2.0 vs. 4.0) and the barrier ‘participating in other projects’ (median 1.0 vs. 3.0) than care home managers.
Differences between stakeholders in experienced influence indicate care home managers experienced higher influence of the facilitator ‘open communication and flat hierarchy’ compared to interventionists (median 5.0 vs. 3.0), and less influence of the barrier ‘reorganizations’ compared to care staff (median 1.0 vs. 3.0).
3.2. Comparison at country-level
For the comparison between countries, baseline (T0) surveys from the Netherlands (n = 93), Norway (n = 49), Türkiye (n = 61), and Germany (n = 24) were included. Surveys from the United Kingdom (n = 2) were excluded. Expectations (T0) about relevance and feasibility were comparable countries, except for the statement ‘I know which tasks I have to fulfill for the MIDDEL-project’, where German respondents strongly agreed (median 5.0) and most Dutch respondents neither agreed nor disagreed (median 3.0) (Table 3).
Expectations about presence of barriers and facilitators varied largely between countries, with percentages differing up to 100% (Figure 5). Across countries, expected presence of factors was highest for organizational barriers ‘high workload’ and ‘lack of care staff’, whereas expected presence of the barrier ‘lack of support’ was low. Expected presence of factors for related to MBI implementation was highest for facilitators ‘clear communication’, ‘people involved facilitate implementation’, and ‘project planning is maintained’ (Figure 5). In 8 out of 9 organizational factors, the percentage in Germany is highest for facilitators and lowest for the expected presence of hindering factors. For Türkiye expected presence was highest in 3 organizational barriers and lowest for the barrier ‘implementing an intervention on the CHU takes a lot of time’, compared to the other countries. Of 8 factors related to MBI implementation, expected presence of the barrier ‘keeping a music intervention running is a lot of work’ was much lower for Türkiye, whereas the barriers ‘lack of motivation’ and ‘scarce resources’ were higher than in other countries. Expected presence of the barrier ‘changes in employees’ was lower in Norway compared to the other countries.
Across all countries, expected influence of factors on implementation of the MIDDEL trial and its MBIs was largest for the organizational barriers ‘high workload’, ‘lack of care staff’, and the facilitators ‘open communication and flat hierarchy’ and ‘well-functioning teams’. In each country, the same three facilitators related to implementation of MBI had the largest expected influence: ‘clear communication’, ‘people involved facilitate implementation’, and ‘planning is maintained’. (Figure 5).
Between countries, differences in median expected influence were larger for organizational factors than for factors related to MBI implementation. For 5 out of 9 organizational factors, Türkiye had a higher median expected influence compared to (some of) the other countries (a difference of ≥ 2.0 points on the median). This applied to the facilitator ‘open communication and flat hierarchy’, and the barriers ‘lack of support’, ‘reorganizations’, ‘participating in other projects’, and ‘general resistance to change’.
3.3. Comparison at intervention group-level
For analysis of differences between intervention groups, twenty-five surveys were excluded: 22 surveys were from respondents involved in multiple intervention groups, and for 3 surveys the allocated intervention group was unknown. Number of respondents varies per survey item, as no items were obligated to fill out. Most respondents were in the COMBI group (n = 39 at baseline, n = 32 post-intervention), followed by CONTROL (n = 30 at baseline, n = 25 post-intervention), GMT (n = 26 at baseline, n = 23 post-intervention), and RCS (n = 24 at baseline, n = 17 post-intervention).
Between all four intervention groups (GMT, RCS, COMBI, and CONTROL), expectations (T0) regarding relevance and feasibility was comparable, except for a median difference of 1.5 points for the statement ‘participating in the project will be relevant for this care home organization’: care home managers in the RCS arm did not agree nor disagree (median 3.0), in the COMBI arm they agreed (median 4.0), and in the CONTROL and GMT arm they agreed – strongly agreed (median 4.5) (Table 5). At post-intervention, care home managers from the GMT group strongly agreed that ‘participating in the project was relevant’, whereas managers from the CONTROL group did not agree nor agree.
Respondents were asked whether they noticed any effect of the MBIs (in residents, care staff, or on the CHU). In the RCS arm, almost all respondents noticed an effect in residents (93.3%). In the GMT and in the COMBI arm, more than half of the respondents noticed an effect in residents (60.0% and 57.1%, respectively). Notably, almost half of the respondents in the CONTROL arm also reported they noticed an effect of the MBI on care home residents (28.0%), care staff (8.0%) or on the CHU (12.0%), even though they received no MBI as part of the MIDDEL trial.
For each intervention group, presence of the barriers ‘lack of care staff’ and ‘in general, implementing an intervention on the CHU takes a lot of time’ was less (difference ≥20%) than expected (Figure 6). Within GMT, organizational barriers ‘lack of support’, ‘reorganizations’, ‘participating in other projects’, ‘resistance to change’ were less present than expected. Related to MBI implementation, the presence of the barriers ‘keeping a music intervention running is a lot of work’ and ‘difficulties due to COVID’ was less than expected. Within RCS, the organizational barriers ‘resistance to change’, ‘high workload for care staff’ and barriers related to MBI implementation ‘keeping a music intervention running is a lot of work’ and ‘difficulties due to COVID’ were less present than expected. Within COMBI, the organizational facilitator ‘stable and well-functioning teams’ was more present than expected, whereas the facilitator ‘clear communication’ was less present than expected. Within CONTROL group, presence of the organizational facilitator ‘stable and well-functioning teams’ was more than expected. Organizational barriers ‘reorganizations’ and ‘high workload of care staff’ was less present than expected. Related to MBI implementation, the barrier ‘lack of motivation’ was less present than expected.
At baseline between groups, in 4 out of 9 organizational factors, expected presence was highest in RCS for the facilitators ‘open communication and flat hierarchy’ and ‘high workload for care staff’, and lowest for the barriers ‘participating in other projects’ and ‘lack of care staff’. For 7 out of 10 factors related to MBI implementation, expected presence was highest in GMT for the barriers ‘keeping an intervention running is a lot of work’, ‘changes in employees’, ‘difficulties due to COVID’, and ‘in general, implementing an intervention on the CHU takes a lot of time’, and lower for the facilitators ‘project planning is maintained’, ‘clear communication’, and ‘there are musical activities in the care home’ compared to the other groups. In 6 out of 10 factors, COMBI had the lowest score for expected presence of barriers ‘keeping a music intervention running is a lot of work’, the highest score for the barrier ‘in general, implementing an intervention on the CHU takes a lot of time’ and for the facilitators ‘project planning maintained’, clear communication’, ‘there are musical activities in the care home’, and ‘music-based interventions are well-integrated’.
Differences within intervention groups regarding the influence of factors, occurred for COMBI for the facilitator ‘stable and well-functioning team’, with a median of 2.5 at baseline to 5.0 post-intervention. Within RCS the median influence of four barriers decreased, indicating its influence was less than expected: ‘lack of support’ (median 3.0 to 1.0), ‘lack of motivation’, ‘scarce resources’, and ‘in general, implementing an intervention on the CHU takes a lot of time’ (medians from 4.0 to 2.0). For this last item median changed similarly for CONTROL.
Between intervention groups median differences ≥2.0 occurred for the facilitator ‘there are music activities in the care home’ at baseline, with a median of 4.0 in COMBI and 2.0 in CONTROL. Post-intervention differences in influence of a factor were found for the barrier ‘participating in other projects’ with a median of 3.0 for GMT and 1.0 for COMBI; and the facilitator ‘project planning maintained’ with a median of 5.0 in COMBI and 3.0 in RCS. Respondents in COMBI experienced the largest influence of ‘keeping an intervention running is a lot of work’ (median 3.5), compared to the other groups.
4. Discussion
This process evaluation of a large multinational trial of group MBIs, investigated expectations and experiences related to barriers and facilitators for implementation of MBI for people with dementia living in care homes. Care home managers, care staff, and interventionists from Germany, the Netherlands, Norway, Türkiye, and the United Kingdom filled out a survey at baseline and after the six-month intervention period. Allocated intervention groups were group music therapy (GMT), recreational choir singing (RCS), the combination of both interventions (COMBI), or a control group receiving no structural MBIs (CONTROL). Key findings were organized and presented across three levels: the stakeholder perspective, the country perspective, and the intervention group perspective.
4.1. Interpretation of main findings
Group MBIs can successfully be implemented for people with dementia and depression in care home settings. Overall, respondents deemed the MBIs relevant and feasible, although not all stakeholders were certain what was expected of them during the project. Majority of respondents noticed an effect of the MBI on participants, although part of them was uncertain about the exact allocated intervention group. Main barriers for implementation of group MBIs in care homes for people with dementia include lack of support, changes in employees, lack of motivation in those involved. Important facilitators to reinforce are: people involved facilitate and stimulate implementation, stable and well-functioning teams, clear communication, and project planning is maintained. Despite a high influence, the presence of barriers keeping an MBI running is a lot of work, time needed to implement an intervention in general and an MBI specifically, high workload of care staff, lack of care staff and discontinuity due to COVID were all less than respondents expected beforehand. Majority of respondents were unaware of any plans for sustainable adoption of the MBI after the trial. Engaging key stakeholders is essential: care home managers are pivotal for policy making and sustainable adoption of music interventions, whereas commitment and involvement of care staff is needed for day-to-day implementation. Even though this study did not specifically focus on policy context and related financial and systemic barriers for implementation of music interventions for people with dementia living in care homes, the approach of differentiating perspectives of care home management, care staff and interventionists shed light on showed differences within the system depending on someone's role in it.
4.1.1. Country-perspective
The contexts in which complex interventions such as these are implemented can have a large influence on intervention outcomes (Skivington et al., 2021), although contextual factors and their interaction with interventions are often not taken into full consideration (Wyman et al., 2022). However, the question is not only whether an intervention is effective, but also under what circumstances it can reach its full potential in daily practice. Possible contextual factors that may influence external validity include amongst others, differences between cultures, countries, healthcare systems, selection of care homes and care home residents, intervention protocols, clinically relevant outcome measures (Rothwell, 2005). Several findings indeed may be due to cultural and healthcare system differences. To illustrate, German and Turkish respondents anticipated high presence and influence of a ‘flat hierarchy’, whereas Dutch and Norwegian respondents anticipated high presence and influence of implementation of the MBI taking a lot of time. One difference in healthcare systems is for example, that in Germany no elderly care physicians and psychologists are employed by the care home, implying less hierarchic structure (Fassmer et al., 2024). Also, in the Netherlands interventionists were contracted by the care home organization, in Norway by the municipalities, whereas in Germany and Türkiye interventionists were contracted by the research institute conducting the MIDDEL trial. Those interventionists went to various CHUs to offer the assigned interventions to the participating residents. Another difference between countries was the level of education and certification of interventionists and experience in applying music therapy in a clinical setting such as elderly care. To elaborate, in Türkiye music therapy in general is not (yet) a recognized profession, whereas in the other countries it is. Rather, music therapy is recognized as a technique only trained medical doctors or dentists can apply, indicating it is actually music in medicine that is practiced (Uçaner & Heiderscheit, 2016). The high anticipated influence of ‘participating in other studies or projects’ in Turkish respondents, could be explained by a difference in previous experiences with trials in care homes.
4.1.2. Stakeholder-perspective
Differences between stakeholders’ evaluation of presence and influence of factors indicate each stakeholder group looked from a different perspective, was involved in the trial in a different way, and therefore experienced different barriers and facilitators. Previous studies identified factors related to staff, communication, stimulation of implementation, and expectations to have a large influence on implementation (Gerritsen et al., 2021; Groot Kormelinck et al., 2021). An ambassador or key contact person for MIDDEL was present at the CHU to facilitate implementation and maintained the project planning, which has previously demonstrated to be a valuable strategy to facilitate implementation (Gerritsen et al., 2021). Implementation strategies between countries also differed, which could explain why Dutch respondents knew to a lesser extent which tasks they had to fulfill for the MIDDEL trial. To elaborate, in the Netherlands all care staff and managers – also when involved to a lesser extent – were asked to fill out the survey, whereas in the other countries, a selection of stakeholders was specifically asked to fill out the survey.
During the trial, care home managers had a key position enhancing facilitators and minimizing barriers to the implementation of group MBIs at care staff-level. They are in the position to offer organizational support in the form of allocating time, education and resources for care staff to facilitate and maintain implementation and maintenance of the MBIs (Sung et al,, 2008). In terms of sustainability, intention and efforts of care home management for continuation and adoption of MBIs are pivotal. Sung et al. (2008) also emphasized that involving care staff in protocol adaptations fostered greater sense of ownership and responsibility for implementation. Similarly, stakeholders of the MIDDEL trial were unsure about their role and tasks during the trial. This may have hindered their involvement and sense of shared responsibility to maintain the MBIs.
4.1.3. Intervention group-perspective
Differences observed in the anticipated presence of factors provide insight into the preconditions that differed between intervention groups prior to randomization to the allocated intervention group (GMT, RCS, COMBI or CONTROL). In each group, baseline percentage of respondents that expected factors to be present during the trial was much higher than the percentage of respondents that experienced a factor to have been present. The effects that respondents noticed in care home residents were highest in RCS, followed by GMT and COMBI. An interesting next step would be to compare these findings with the results found in the MIDDEL effect study. Respondents in the CONTROL group also noticed an effect in residents.
The findings of this study highlight that the type and dose of MBI affects implementation. Stakeholders involved in the COMBI group encountered greater organizational challenges, as sessions had to be organized not twice but four times a week. Perceived barriers and facilitators varied depending on an individual’s role in the project. For care home managers initiating a new intervention, clear communication across organizational levels was particularly important, whereas for care staff, key facilitators included sufficient time, role clarity, and effective collaboration.
4.2. Strengths and limitations
This study knows several strengths. The design of this study and the survey was based on previous studies into barriers and facilitators for implementation in nursing homes (Appelhof et al., 2018; Leontjevas et al., 2012; Zwijsen et al., 2011). We opted for a repeated survey with closed questions from different stakeholders involved in the MIDDEL trial, to obtain insight into expectations and experiences related to implementation of the MIDDEL trial and its MBIS. A descriptive approach was chosen to analyze the large quantity of data. The survey was completed by four different groups of stakeholders, each with their own area of expertise, (work) experiences and opinions, which in turn influenced their evaluation of the implementation. Each stakeholder group was involved in the project in a different way and could therefore experience factors (potential barriers and facilitators) differently. The survey was completed at several timepoints, allowing us to gain insight into changes over time. The survey consists solely of quantitative statements, enabling us to conduct the survey in multiple languages. This allowed us to make comparisons between countries with minimal language barriers.
This study also knows several limitations. First, strategies to interweave the survey in the MIDDEL trial differed per country. Before the start of the trial, it was decided that each country would try to approach 30% of the stakeholders for the process evaluation. Due to the size of the trial, it was not feasible for all participating countries to embed the process evaluation survey in the MIDDEL trial to the same extent. As a result, the sample size differs between countries and stakeholders. Each country could also decide for itself how to achieve this target number, with the result that in some countries only stakeholders from certain units have been asked and other units not at all. In addition, selection bias was suspected: specific people were asked by MIDDEL researchers to share their perspective by completing the survey. Furthermore, the moment that the process evaluation was rolled out and completed differed across countries and participating homes, so that in one care home the presence and impact of COVID (restrictions) may have been much more prominent than in homes that started the process evaluation at a later time. No information is available about those who did not fill in the survey. Respondents who completed the survey at baseline may differ from those who completed the survey post-intervention. These limitations may create an incomplete, biased picture of the overall implementation; therefor findings should be interpreted with caution. One item in the survey that may have been ambiguous was the question about ‘any’ observed effect of the MBIS. Firstly, a third of respondents from the control group indicated they noticed an effect in care home residents. The cause remains unknown: perhaps socially desired answers were given, a placebo-effect occurred due to positive expectations related to participating in the trial, or respondents filled out the survey with other musical activities – that were part of standard care in their care home – in mind when completing the survey. In addition, it is unknown whether the observed effects are valued in a positive or negative way.
4.3. Recommendations for future studies and practice
Thorough documentation of process evaluation for complex interventions, like group MBIS, is essential to assess not only the intervention’s effectiveness, but also the effectiveness of the implementation strategies employed. A descriptive, theory driven approach was chosen for data analysis of this study (Skivington et al., 2021), although future studies focusing on process evaluation embedded in an RCT for psychosocial interventions might consider using a standardized questionnaire, where significance testing is also possible. Several survey items can be formulated differently in future trials. Specifically, in a future study, it could be valuable to differentiate between positive effect (such as joy) and negative effect (such as participant burden), when asking stakeholders whether they observed ‘any effect’. In future trials, a deliberate decision can be made whether or not to remind respondents at the start of the survey which arm their CHU was allocated to. On the one hand, this ensures that respondents complete the survey with the right intervention in mind. On the other hand, it is also valuable to know that respondents do not know exactly whether and which MBI the residents were offered. This study focused on expectations and experiences of stakeholders. For a more complete picture of the implementation of the trial and the MBIS, it is recommended to assess multiple aspects of the process evaluation, such as intervention dose, session attendance, and reliability and validity of the MBIS by assessing treatment fidelity.
Differences between countries were large, warranting further exploration of local/national barriers and facilitators for implementation. Evaluation of implementation could be explored in-depth for each participating country separately, as was done in the UK arm of the MIDDEL trial (Schneider et al. 2024). The anecdotes described herein provide a vivid picture of the universal challenges that arise when implementing a group MBI in a care home setting.
5. Conclusions
Findings of this process evaluation illustrate how implementing a complex intervention in care homes can be challenging, based on how potential barriers and facilitators, that is, organizational factors and factors related to the MBI (i.e., the type and dose) affect implementation and adoption of the MBI in the care home. Different MBIS come with different organizational and practical challenges for the organization, care home management, interventionists and care staff. When starting a randomized trial and implementing MBIS, consideration should be given to factors related to support from board/management, well-functioning teams, workload and availability of care staff, clear communication, that people involved facilitate implementation, and that project planning is maintained. Findings of this process evaluation can help to interpret the results of the primary outcomes of the MIDDEL trial.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org. Supplemental file ‘Care staff process evaluation survey’.
Author Contributions
Conceptualization: NR, SZ, AV and SJ. Funding acquisition: CG, SZ, BU, GK, JS. Methodology: NR, SZ, AV, CG, MG, SJ. Project administration: NR, VS, BU, and UF. Resources: NR, VS, JN, and BU. Software: NR, MS, and JW. Investigation: NR, MS, VS, JN, MG, BU, YS, JA, and HN. Formal analysis: NR. Writing – original draft: NR. Writing – review & editing: All authors.
Funding
Funding was supported by the EU Joint Programme – Neurogenerative Disease Research (JPND) project (JPND2019-466-067), through the following national funding organizations: Germany: Federal Ministry of Education and Research (BMBF, project number 01ED2011); the Netherlands: The Netherlands Organization for Health Research and Development (ZonMw, project number 733051108); Norway: The Research Council of Norway (RCN, project number 311628); Turkey, Scientific and Technological Research Council of Türkiye (TUBITAK, project number 119N125); The United Kingdom: United Kingdom Research and Innovation Medical Research Council (UKRI MRC project number MR/T046740/1).
Institutional Review Board Statement
The research was carried out in accordance with the WMA Declaration of Helsinki. Ethical approval was obtained prior to data collection in Germany: Medical Ethics Committee at the Carl von Ossietzky University Oldenburg (approval date: September 9, 2020); in the Netherlands: Medical Ethical Committee (METc) of the University Medical Center Groningen (approval date: January 12, 2021); in Norway: Regional Committees for Medical and Health Research Ethics (REC), Norway (approval date: June 29, 2020); in Türkiye: Ethics commission at the Ankara Haci Bayram Veli University (approval date: January 30, 2020); the United Kingdom: Wales Research Ethics Committee, United Kingdom (approval date: October 16, 2020). Study- and patient-related documentation was adapted where needed to meet national ethical requirements. Clinical trial registration nr NCT03496675.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data can be obtained from the corresponding author upon request.
Acknowledgments
The authors are grateful to all the participants and stakeholders who made it possible to carry out this process evaluation embedded within the main MIDDEL trial.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| MIDDEL | Music Interventions for Dementia and Depression in ELderly care |
| MBI | Music-Based Intervention |
| CHU | Care Home Unit |
| GMT | Group Music Therapy |
| RCS | Recreational Choir Singing |
| COMBI | Combination group receiving both GMT and RCS |
| CONTROL | Control group receiving no structural music interventions |
| MADRS | Montgomery-Åsberg Depression Rating Scale |
| RCT | Randomized Controlled Trial |
References
- Amano, T., Hooley, C., Strong, J., Inoue, M. (2021). Strategies for implementing music-based interventions for people with dementia in long-term care facilities: a systematic review. International Journal of Geriatrics, 37(1). [CrossRef]
- Appelhof, B., Bakker, C., van Duinen-van den IJssel, J. C. L., Zwijsen, S. A., Smalbrugge, M., Verhey, F. R. J., de Vugt, M. E., Zuidema, S. U., & Koopmans, R. T. C. M. (2018). Process Evaluation of an Intervention for the Management of Neuropsychiatric Symptoms in Young-Onset Dementia. Journal of the American Medical Directors Association, 19(8), 663–671. [CrossRef]
- Baker, F. A., Lee, Y. E. C., Sousa, T. V., Stretton-Smith, P. A., Tamplin, J., Sveinsdottir, V., Geretsegger, M., Wake, J. D., Assmus, J., & Gold, C. (2022). Clinical effectiveness of music interventions for dementia and depression in elderly care (MIDDEL): Australian cohort of an international pragmatic cluster-randomised controlled trial. The Lancet Healthy Longevity, 3(3), e153–e165. [CrossRef]
- Dam, A. E. H., Christie, H. L., Smeets, C. M. J., van Boxtel, M. P. J., Verhey, F. R. J., & de Vugt, M. E. (2019). Process evaluation of a social support platform ‘Inlife’ for caregivers of people with dementia. Internet Interventions, 15(November 2018), 18–27. [CrossRef]
- Dementia. (2023). World Health Organization. https://www.who.int/news-room/fact-sheets/detail/dementia.
- Fassmer, A. M., Zuidema, S. U., Janus, S. I. M., & Hoffmann, F. (2024). Comparison of medical care needs and actual care in German and Dutch nursing home residents: A cross-sectional study conducted in neighboring European countries. Archives of Gerontology and Geriatrics, 117. [CrossRef]
- Gerritsen, D. L., De Vries, E., Smalbrugge, M., Smeets, C. H. W., Van Der Spek, K., Zuidema, S. U., & Koopmans, R. T. C. M. (2021). Implementing a multidisciplinary psychotropic medication review among nursing home residents with dementia: A process evaluation. International Psychogeriatrics, 33(9), 933–945. [CrossRef]
- Gold, C., Eickholt, J., Assmus, J., Stige, B., Wake, J. D., Baker, F. A., Tamplin, J., Clark, I., Lee, Y. E. C., Jacobsen, S. L., Ridder, H. M. O., Kreutz, G., Muthesius, D., Wosch, T., Ceccato, E., Raglio, A., Ruggeri, M., Vink, A., Zuidema, S., … Geretsegger, M. (2019). Music Interventions for Dementia and Depression in ELderly care (MIDDEL): Protocol and statistical analysis plan for a multinational cluster-randomised trial. BMJ Open, 9(3). [CrossRef]
- Groot Kormelinck, C. M., van Teunenbroek, C. F., Zuidema, S. U., Smalbrugge, M., & Gerritsen, D. L. (2021). Process evaluation of a tailored intervention to Reduce Inappropriate psychotropic Drug use in nursing home residents with dementia. BMC Geriatrics, 21(414). [CrossRef]
- Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O’Neal, L., McLeod, L., Delacqua, G., Delacqua, F., Kirby, J., & Duda, S. N. (2019). The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics, 95(103208). [CrossRef]
- Kishita, N., Backhouse, T., & Mioshi, E. (2020). Nonpharmacological Interventions to Improve Depression, Anxiety, and Quality of Life (QoL) in People With Dementia: An Overview of Systematic Reviews. Journal of Geriatric Psychiatry and Neurology, 33(1), 28–41. [CrossRef]
- Kormelinck, C. G., Van Teunenbroek, C., Zuidema, S., Gerritsen, D., & Smalbrugge, M. (2019). Process evaluation of a participatory action research-RCT aimed at reducing inappropriate psychotropic drug use in nursing home residents with dementia by tailored intervention-and implementation plans. International Psychogeriatrics, 31, 115–116.
- Kwak, J., Ha, J-H., & O’Connell Valuch, K. (2020). Lessons learned from the statewide implementation of the Music & Memory program in nursing homes in Wisconsin in the USA. Dementia, 20(5). 1617-1630. [CrossRef]
- Leontjevas, R., Gerritsen, D. L., Koopmans, R. T. C. M., Smalbrugge, M., & Vernooij-Dassen, M. J. F. J. (2012). Process Evaluation to Explore Internal and External Validity of the “ Act in Case of Depression” Care Program in Nursing Homes. Journal of the American Medical Directors Association, 13(5), 488.e1-488.e8. [CrossRef]
- Leung, D. K. Y., Chan, W. C., Spector, A., & Wong, G. H. Y. (2021). Prevalence of depression, anxiety, and apathy symptoms across dementia stages: A systematic review and meta-analysis. International Journal of Geriatric Psychiatry, 36(9), 1330–1344. [CrossRef]
- Matovic, D., Ahern, M., & Wuthrich, V. M. (2023). The Next Steps in Reducing Risk for Dementia. Advances in Psychiatry and Behavioral Health, 3(1), 159–175. [CrossRef]
- Meyer, C., & O’Keefe, F. (2020). Non-pharmacological interventions for people with dementia: A review of reviews. Dementia, 19(6), 1927–1954. [CrossRef]
- Montgomery, S. A., & Asberg, M. (1979). A new depression scale designed to be sensitive to change. The British journal of psychiatry : the journal of mental science, 134, 382–389. (n.d.). NORCE. Retrieved April 11, 2024, from https://www.norceresearch.no/en/. [CrossRef]
- Rothwell., P. M. (2005). External validity of randomised controlled trials: “To whom do the results of this trial apply?” The Lancet, 365, 82–93. [CrossRef]
- Schneider, J., Ablewhite, J., Bloska, J., Gold, C., Orrell, M., Dowson, B., McArdle, C., Tooth, H., Trevers, S., Narippatta, S.M., Fan, Y., Wake, J.D., Peach, A., Duckworth, B. and Sveinsdottir, V. (2024) ‘Music in Care Home Settings: Guidelines for Implementation and Evaluation Based on the Music Interventions for Depression and Dementia in ELderly Care (MIDDEL) Study in the UK’, Journal of Long Term Care, 252–262. [CrossRef]
- Skivington, K., Matthews, L., Simpson, S. A., Craig, P., Baird, J., Blazeby, J. M., Boyd, K. A., Craig, N., French, D. P., McIntosh, E., Petticrew, M., Rycroft-Malone, J., White, M., & Moore, L. (2021). A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. The BMJ, 374(n2061). [CrossRef]
- Sousa, L., Neves, M. J., Moura, B., Schneider, J., & Fernandes, L. (2021). Music-based interventions for people living with dementia, targeting behavioral and psychological symptoms: A scoping review. International Journal of Geriatric Psychiatry, 36(11), 1664–1690. [CrossRef]
- Sung, H.-C., Chang, A.M. & Abbey, J. (2008), An implementation programme to improve nursing home staff's knowledge of and adherence to an individualized music protocol. Journal of Clinical Nursing, 17: 2573-2579. [CrossRef]
- Töpfer, N.F., Schön, L., Jakob, E., Hillebrand, M.C., Reichertz, J., Rother, D., Weise, L., Wilz, G. (2024). Sounds of Difference: A Typology of Reactions of People With Dementia to Individualized Music in the Presence of a Monitoring Person. The Gerontologist, 64(6). [CrossRef]
- Uçaner, B., & Heiderscheit, A. (2016). Music Therapy in Turkey: Curriculum and Resource Development Through Professional Collaboration. Music Therapy Today, 12(1), 8–20.
- van der Steen, J.T., van der Wouden, J.C., Methley, A.M., Smaling, H.J.A, Vink, A.C., Bruinsma, M.S. (2025) Music-based therapeutic interventions for people with dementia. Cochrane Database of Systematic Reviews 3. [CrossRef]
- Vink, A., & Hanser, S. (2018). Music-Based Therapeutic Interventions for People with Dementia: A Mini-Review. Medicines, 5(4). [CrossRef]
- Wiels, W., Baeken, C., & Engelborghs, S. (2020). Depressive symptoms in the elderly—an early symptom of dementia? A systematic review. Frontiers in Pharmacology, 11(February), 1–13. [CrossRef]
- Wyman, D. L., Butler, L., Bright, P., Morgan-Trimmer, S., Budgett, J., & Cooper, C. (2022). A systematic review of process evaluations for psychosocial interventions designed to improve the wellbeing and quality of life of community-dwelling people with dementia and their carers. International Journal of Geriatric Psychiatry, 37(12). [CrossRef]
- Zwijsen, S. A., Smalbrugge, M., Eefsting, J. A., Gerritsen, D. L., Hertogh, C. M. P. M., & Pot, A. M. (2014). Grip on challenging behavior: Process evaluation of the implementation of a care program. Trials, 15(1), 1–11. [CrossRef]
- Zwijsen, S. A., Smalbrugge, M., Zuidema, S. U., Koopmans, R. T., Bosmans, J. E., Van Tulder, M. W., Eefsting, J. A., Gerritsen, D. L., & Pot, A. M. (2011). Grip on challenging behaviour: A multidisciplinary care programme for managing behavioural problems in nursing home residents with dementia. Study protocol. BMC Health Services Research, 11(1), 41. [CrossRef]
Figure 1.
Flowchart illustrating the design of the process evaluation embedded in the main MIDDEL trial.
Figure 1.
Flowchart illustrating the design of the process evaluation embedded in the main MIDDEL trial.
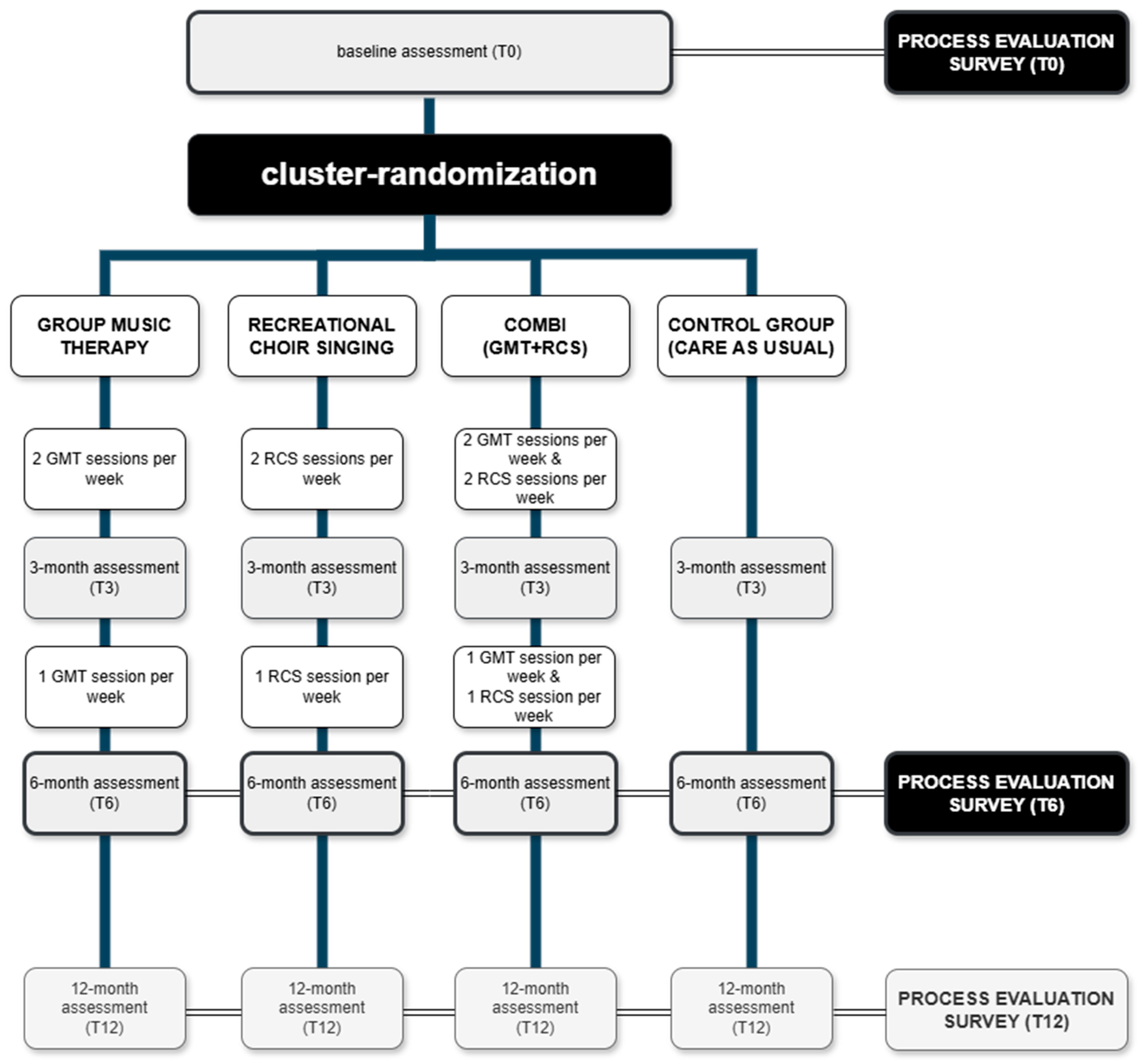
Figure 2.
Path diagram illustrating the operationalization of elements derived from Leontjevas’ framework (Leontjvas et al., 2012) for process evaluation within the MIDDEL trial. Elements presented in gray fall outside the scope of the current study.
Figure 2.
Path diagram illustrating the operationalization of elements derived from Leontjevas’ framework (Leontjvas et al., 2012) for process evaluation within the MIDDEL trial. Elements presented in gray fall outside the scope of the current study.
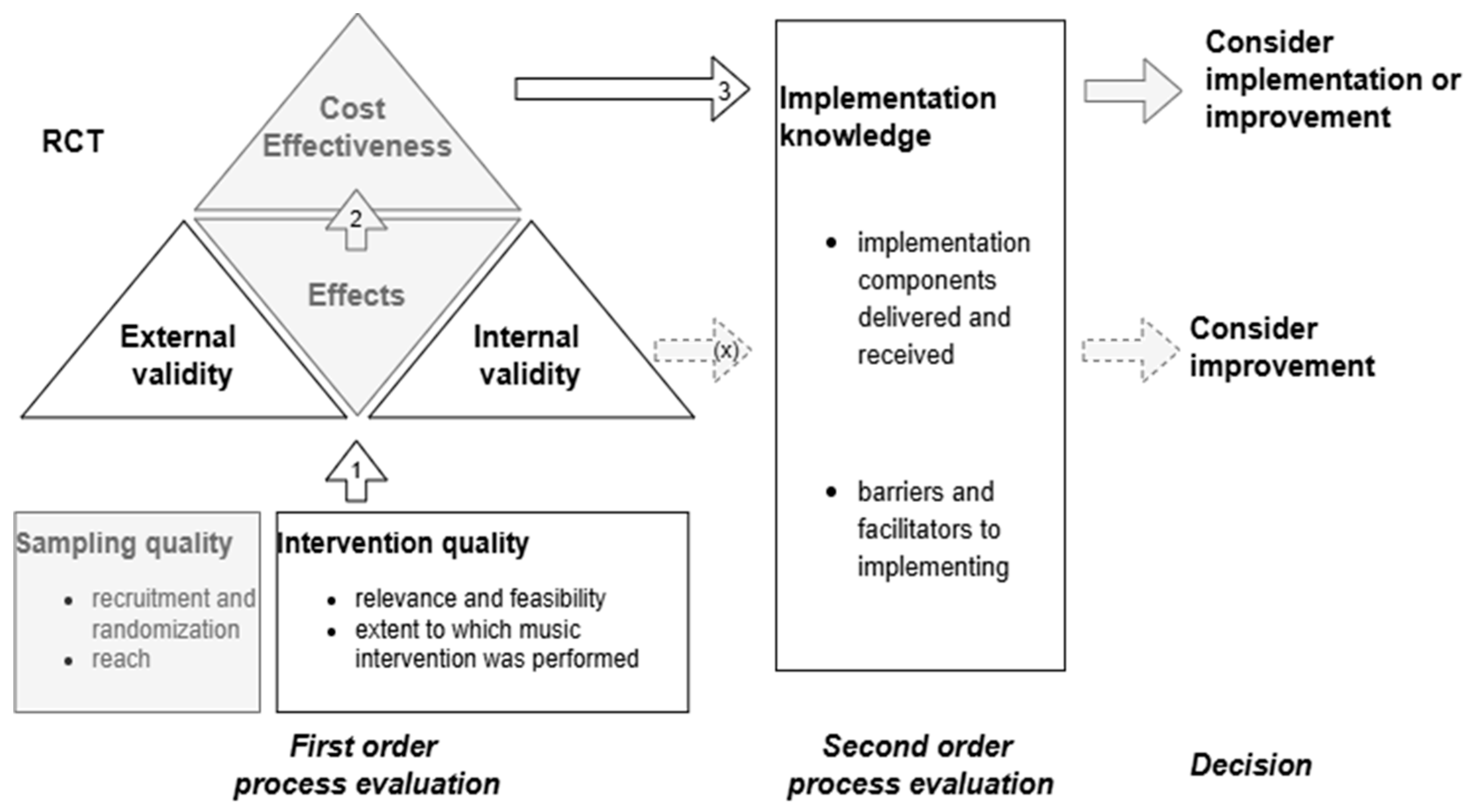
Figure 3.
Overview of MIDDEL process evaluation surveys collected per country, presented per timepoint and stakeholder group.
Figure 3.
Overview of MIDDEL process evaluation surveys collected per country, presented per timepoint and stakeholder group.
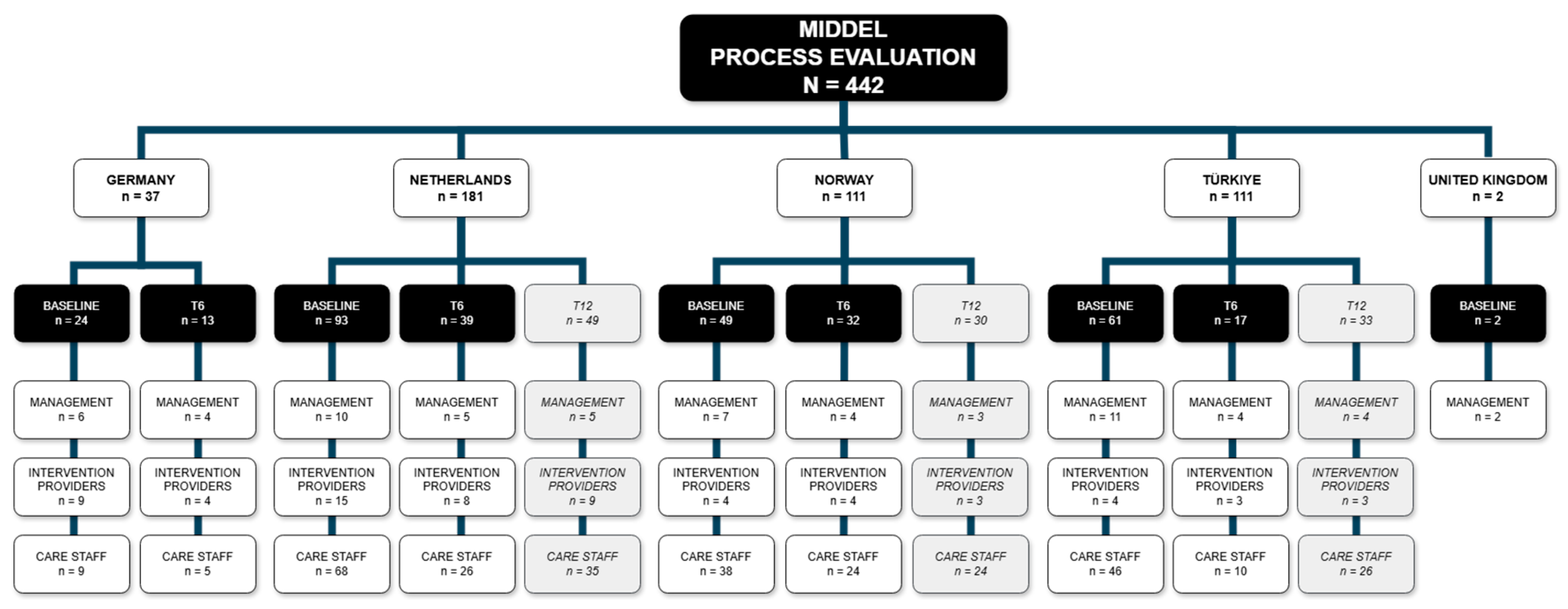
Figure 4.
Heatmap visualizing the percentage of stakeholders that expected (T0) and experienced (T6) barriers and facilitators to be present during the MIDDEL trial and median scores of expected and experienced influence of those factors on the implementation of the MIDDEL trial and music interventions. Bold numbers indicate between-group differences, underscored numbers indicate within-group differences ≥ 20%/≥ 2.0 points on the median.
Figure 4.
Heatmap visualizing the percentage of stakeholders that expected (T0) and experienced (T6) barriers and facilitators to be present during the MIDDEL trial and median scores of expected and experienced influence of those factors on the implementation of the MIDDEL trial and music interventions. Bold numbers indicate between-group differences, underscored numbers indicate within-group differences ≥ 20%/≥ 2.0 points on the median.
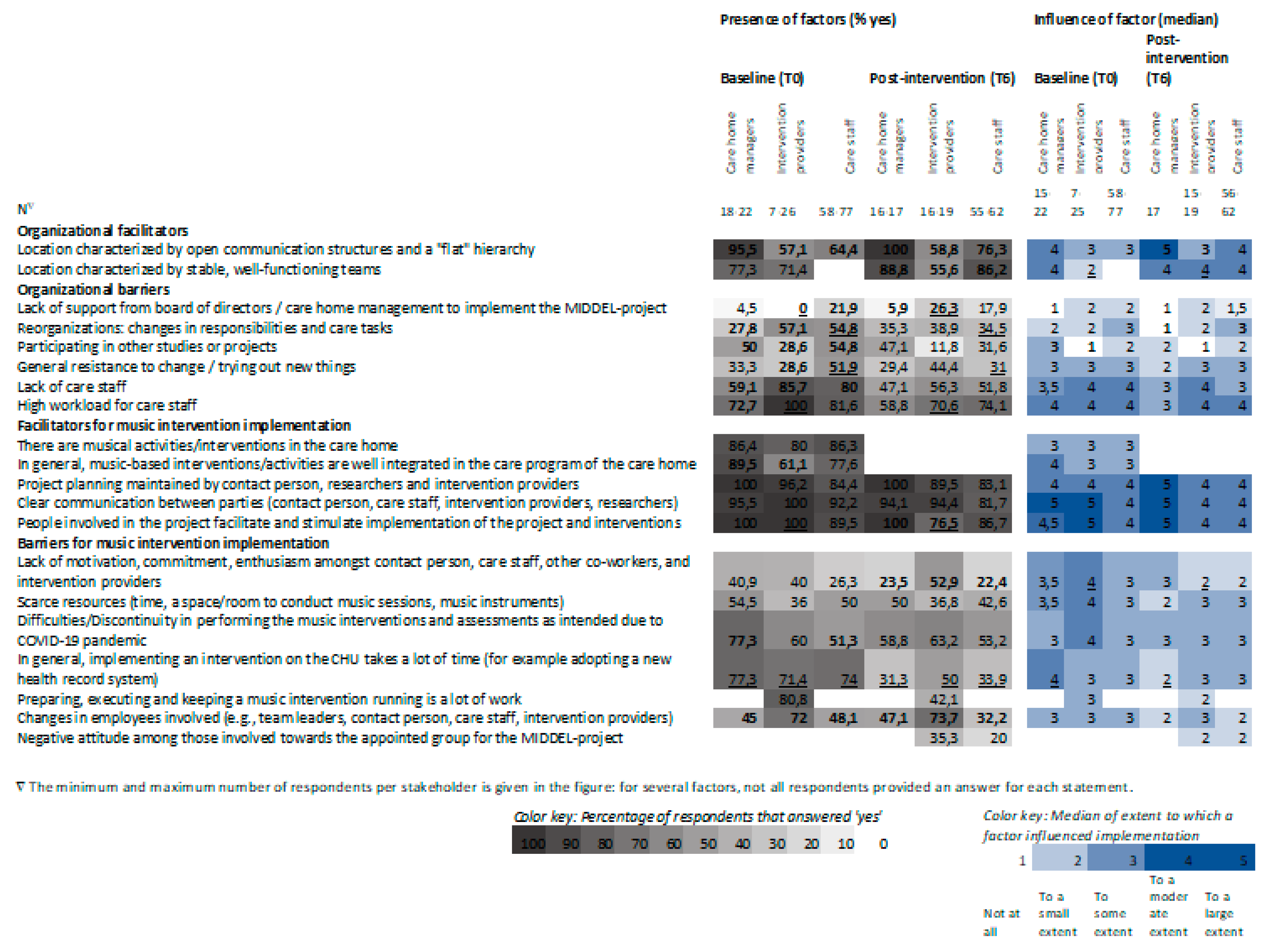
Figure 5.
Heatmap visualizing the percentage of respondents per country that expected barriers and facilitators to be present during the MIDDEL trial and median scores of expected influence of those factors on the implementation of the MIDDEL trial and music interventions. Bold numbers indicate between-country differences ≥ 20%/≥ 2.0 points on the median.
Figure 5.
Heatmap visualizing the percentage of respondents per country that expected barriers and facilitators to be present during the MIDDEL trial and median scores of expected influence of those factors on the implementation of the MIDDEL trial and music interventions. Bold numbers indicate between-country differences ≥ 20%/≥ 2.0 points on the median.

Figure 6.
Heatmap visualizing the percentage of respondents in each intervention group that expected and experienced a hindering or facilitating factor to be present during the MIDDEL trial and median scores of expected and experienced influence of those factors on the implementation of the MIDDEL trial and music interventions. Bold numbers indicate between-group differences, underscored numbers indicate within-group differences ≥ 20%/≥ 2.0 points on the median.
Figure 6.
Heatmap visualizing the percentage of respondents in each intervention group that expected and experienced a hindering or facilitating factor to be present during the MIDDEL trial and median scores of expected and experienced influence of those factors on the implementation of the MIDDEL trial and music interventions. Bold numbers indicate between-group differences, underscored numbers indicate within-group differences ≥ 20%/≥ 2.0 points on the median.
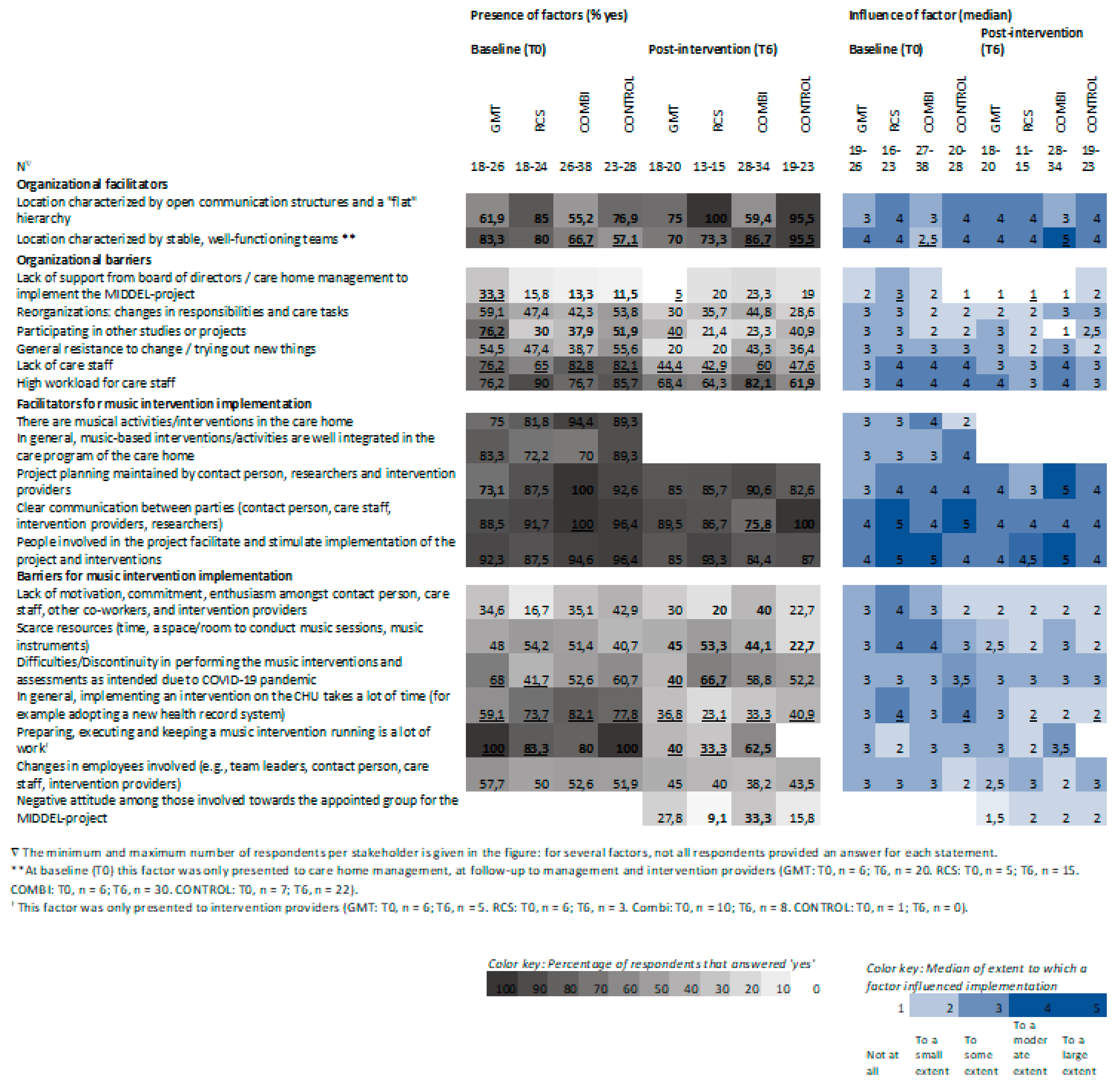

Table 1.
Descriptive characteristics of stakeholder groups at baseline (T0) and post-intervention (T6).
Table 1.
Descriptive characteristics of stakeholder groups at baseline (T0) and post-intervention (T6).
| Stakeholder demographics per timepoint | T0 | T6 |
| Care home management (n) | 22 | 17 |
| Age, n | 18 | 16 |
| 18 -29 years, n (%) | 4 (22.2%) | 3 (18.8%) |
| 30 – 39 years, n (%) | 5 (27.8%) | 4 (25.0%) |
| 40 – 49 years, n (%) | 2 (11.1%) | 4 (25.0%) |
| 50 – 59 years, n (%) | 5 (27.8%) | 3 (18.8%) |
| over 60 years, n (%) | 2 (11.1%) | 2 (12.5%) |
| Sex, n | 22 | 17 |
| Female, n (%) | 16 (72.7%) | 15 (88.2%) |
| Work experience n | 22 | 16 |
| Less than 2 years, n (%) | 6 (27.3%) | 7 (43.8% |
| 2 to 5 years, n (%) | 6 (27.3%) | 2 (12.5%) |
| 5 to 10 years, n (%) | 3 (13.6%) | 2 (12.5%) |
| More than 10 years, n (%) | 7 (31.8%) | 5 (31.3%) |
| Function, n | 19 | 14 |
| Location manager (department leader), n (%) | 7 (36.8%) | 4 (28.6%) |
| Staff officer, n (%) | 1 (5.3%) | - |
| Supervisor (organization leader) , n (%) | 6 (31.6%) | 6 (42.9%) |
| Other | 5 (26.3%) | 4 (28.6%) |
| Familiar with music interventions, n | 20 | |
| GMT, n (%) | 2 (10.0%) | |
| RCS, n (%) | 7 (35.0%) | |
| Both, n (%) | 7 (35.0%) | |
| No, n (%) | 4 (20.0%) | |
| Involved during full trial length, n | 15 | |
| Yes, n (%) | 14 (93.3%) | |
| Group allocation, n | 14 | |
| Correct, n (%) | 9 (64.3%) | |
| Partially correct, n (%) | 1 (7.1%) | |
| Incorrect, n (%) | 4 (28.6%) | |
| Duration to start after baseline assessment, n | 14 | |
| 2 weeks or less, n (%) | 2 (14.3%) | |
| 2 – 4 weeks, n (%) | 4 (28.6% | |
| I don’t know, n (%) | 7 (50.0% | |
| Not applicable, n (%) | 1 (7.1%) | |
| Familiar with Ambassador/contact person, n | 19 | 16 |
| Yes, n (%) | 17 (89.5%) | 12 (75.0%) |
| I don’t know, n (%) | 2 (10.5% | 4 (25.0%) |
| Intervention providers (n) | 26 | 19 |
| Age, n | 26 | 17 |
| 18 -29 years, n (%) | 10 (38.5%) | 7 (41.2%) |
| 30 – 39 years, n (%) | 4 (15.4%) | 2 (11.8%) |
| 40 – 49 years, n (%) | 3 (11.5%) | 2 (11.8%) |
| 50 – 59 years, n (%) | 7 (26.9%) | 4 (23.5%) |
| over 60 years, n (%) | 2 (7.7%) | 2 (11.8%) |
| Sex, n | 26 | 19 |
| female n (%) | 21 (80.8%) | 15 (78.9%) |
| Work experience, n | 25 | 15 |
| Less than 2 years, n (%) | 8 (32.0%) | 5 (33.3%) |
| 2 to 5 years, n (%) | 11 (44.0%) | 8 (53.3%) |
| 5 to 10 years, n (%) | 3 (12.0%) | 2 (13.3%) |
| More than 10 years, n (%) | 3 (12.0%) | - |
| Working at CHU before this trial, n | 25 | |
| Yes, n (%) | 7 (28.0%) | |
| Involved during full trial length, n | 18 | |
| Yes, n (%) | 16 (88.9%) | |
| Group allocation, n | 16 | |
| Correct, n (%) | 12 (75.0%) | |
| Partially correct, n(%) | 1 (6.3%) | |
| Incorrect, n (%) | 3 (18.8%) | |
| Duration to start after baseline assessment, n | 19 | |
| 2 weeks or les, n (%) | 7 (36.8%) | |
| 2 – 4 weeks, n (%) | 4 (21.1%) | |
| 6 – 8 weeks, n (%) | 1 (5.3%) | |
| I don’t know, n (%) | 7 (36.8%) | |
| Familiar with Ambassador/contact person, yes n (%) | 19 (100.0%) | |
| Care staff (n) | 81 | 71 |
| Age, n | 67 | 71 |
| 18 -29 years, n (%) | 13 (19.4%) | 11 (20.8%) |
| 30 – 39 years, n (%) | 17 (25.4%) | 10 (18.9%) |
| 40 – 49 years, n (%) | 9 (13.4%) | 12 (22.6%) |
| 50 – 59 years, n (%) | 17 (25.4%) | 15 (28.3%) |
| over 60 years, n (%) | 11 (16.4%) | 5 (9.4%) |
| Sex, n | 81 | 63 |
| Female, n (%) | 71 (87.7%) | 56 (88.9%) |
| Work experience, n | 71 | 43 |
| Less than 2 years, n (%) | 2 (2.8%) | - |
| 2 to 5 years, n (%) | 9 (12.7%) | 3 (7.0%) |
| 5 to 10 years, n (%) | 16 (22.5%) | 10 (23.3%) |
| More than 10 years, n (%) | 44 (62.0%) | 30 (69.8%) |
| Function, n | 65 | 52 |
| Registered nurse, n(%) | 15 (23.1%) | 12 (23.1% |
| Enrolled nurse, n(%) | 34 (52.3%) | 33 (63.5%) |
| Personal care attendant, n(%) | 6 (9.2%) | 5 (9.6%) |
| Allied health professional, n(%) | 5 (7.7%) | - |
| Leisure staff, n(%) | 1 (1.5%) | 2 (3.8%) |
| Other, n(%) | 4 (6.2%) | - |
| Familiar with music interventions, n | 81 | |
| GMT, n (%) | 16 (19,8%) | |
| RCS, n (%) | 22 (27.2%) | |
| Both, n (%) | 27 (33.3%) | |
| No , n (%) | 16 (19.8%) | |
| Involved during full trial length, n | 58 | |
| Yes, n (%) | 50 (86.2%) | |
| Group allocation, n | 65 | |
| Correct, n (%) | 32 (49.2%) | |
| Partially correct, n(%) | 4 (6.2%) | |
| Incorrect, n (%) | 29 (44.6%) | |
| Duration to start after baseline assessment, n | 59 | |
| 2 weeks or les, n (%) | 5 (8.5%) | |
| 2 – 4 weeks, n (%) | 5 (8.5%) | |
| 4 – 6 weeks, n (%) | 2 (3.4%) | |
| 6 – 8 weeks, n (%) | 5 (8.5%) | |
| I don’t know, n (%) | 41 (69.5%) | |
| Not applicable, n (%) | 1 (1.7%) | |
| Familiar with Ambassador/contact person, n | 78 | 59 |
| Yes, n (%) | 49 (62.8%) | 45 (76.3%) |
| No, n (%) | 5 (6.4%) | 2 (3.4%) |
| I don’t know, n (%) | 24 (30.8%) | 12 (20.3%) |
| Group allocation across stakeholders, n | 95 | |
| Correct, n (%) | 53 (55.8%) | |
| Partially correct, n (%) | 6 (6.3%) | |
| Incorrect, n (%) | 36 (37.9%) |
Table 2.
Stakeholders’ expectations (T0) and experiences (T6) related to relevance, feasibility and implementation of the trial and music interventions.
Table 2.
Stakeholders’ expectations (T0) and experiences (T6) related to relevance, feasibility and implementation of the trial and music interventions.
| Expectations at baseline (T0) |
Care home management (n = 23) |
Intervention providers (n = 25) |
Care staff (n = 80) |
|
| Relevance and feasibility of the organization (level of agreement*) | ||||
| Participating in the project will be relevant (meaningful, fitting, important) for this care home organization | n | 23 | ||
| Median [IQR] | 4.0 [4.0 – 5.0] | |||
| Recreational choir singing will be relevant for the care home residents with dementia and depressive symptoms | n | 23 | 25 | 80 |
| Median [IQR] | 5.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | |
| Group music therapy will be relevant for the care home residents with dementia and depressive symptoms | n | 23 | 25 | 78 |
| Median [IQR] | 5.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 4.0 [4.0 – 5.0] | |
| Recreational choir singing will fit well into the day-to-day practice of the participating CHU(s) | n | 23 | 25 | 78 |
| Median [IQR] | 4.0 [4.0 – 5.0] | 4.0 [3.0 – 5.0] | 4.0 [4.0 – 5.0] | |
| Group music therapy will fit well into the day-to-day practice of the participating CHU(s) | n | 23 | 25 | 79 |
| Median [IQR] | 4.0 [4.0 – 5.0] | 4.0 [3.5 – 5.0] | 4.0 [3.0 – 5.0] | |
| I know which tasks I have to fulfill for the MIDDEL project | n | 22 | 26 | 76 |
| Median [IQR] | 4.0 [3.0 – 5.0] | 5.0 [4.0 – 5.0] | 3.0 [2.0 – 4.0] | |
| Implementation expectations at baseline (T0) (to what extent✴) | ||||
| Anticipated facilitators will be reinforced | n | 20 | 21 | 77 |
| Median [IQR] | 3.0 [3.0 – 4.0] | 4.0 [3.5 – 4.5] | 3.0 [3.0 – 4.0] | |
| Anticipated barriers will be resolved | n | 20 | 17 | 77 |
| Median [IQR] | 4.0 [3.3 – 4.0] | 4.0 [3.5 – 5.0] | 4.0 [3.0 – 4.0] | |
| Experiences post-intervention (T6) |
Care home management (n = 17) |
Intervention providers (n = 19) |
Care staff (n = 65) |
|
| Relevance and feasibility of the organization (level of agreement*) | ||||
| Participating in the project was relevant (meaningful, fitting, important) for this care home organization | n | 16 | ||
| Median [IQR] | 4.5 [4.0 – 5.0] | |||
| The music intervention was relevant for care home residents with dementia and depressive symptoms | n | 13 | 17 | 54 |
| Median [IQR] | 5.0 [4.0 -5.0] | 5.0 [4.0 -5.0] | 4.0 [3.0 -5.0] | |
| The music intervention was relevant to reduce depressive symptoms | n | 13 | 17 | 52 |
| Median [IQR] | 4.0 [3.5 – 5.0] | 4.0 [4.0 -5.0] | 3.0 [3.0 -4.0] | |
| The music intervention fit well into the day-to-day practice of the participating CHU(s) | n | 14 | 17 | 56 |
| Median [IQR] | 4.5 [4.0 – 5.0] | 4.0 [3.0 -5.0] | 3.0 [2.0 – 3.0] | |
| The music intervention turned out to be too complex to use | n | 15 | 19 | 50 |
| Median [IQR] | 2.0 [2.0 – 3.0] | 3.0 [1.0 – 4.0] | 3.0 [2.0 -3.0] | |
| The music intervention was in line with how we are used to working | n | 13 | 18 | 54 |
| Median [IQR] | 4.0 [2.5 – 4.5] | 4.0 [3.0 -5.0] | 3.5 [3.0 – 4.0] | |
| I would recommend the music intervention to other care homes | n | 14 | 17 | 57 |
| Median [IQR] | 5.0 [3.8 – 5.0] | 5.0 [4.5 – 5.0] | 4.0 [4.0 -5.0] | |
| Effect | ||||
| Did you notice any effect of the music intervention(s)? | n | 17 | 19 | 65 |
| Yes, on the CHU, n (%) | 5 (29.4%) | 7 (36.8%) | 8 (12.3%) | |
| Yes in care staff, n (%) | 6 (35.3%) | 9 (47.4%) | 7 (10.8%) | |
| Yes, in residents, n (%) | 11 (64.7%) | 18 (94.7%) | 28 (43.1%) | |
| No, n (%) | 0 (0.0%) | 0 (0.0%) | 16 (24.6%) | |
| I don’t know, n (%) | 2 (11.8%) | 2 (10.5%) | 10 (15.4%) | |
| Not applicable, n (%) | 3 (17.6%) | 0 (0.0%) | 8 (12.3%) | |
| Satisfaction (level of satisfaction≥) | ||||
| To what extent were you satisfied with the implementation of the MIDDEL-project? | n | 17 | 17 | 59 |
| Median [IQR] | 5.0 [3.5 – 5.0] | 4.0 [3.0 -4.5] | 4.0 [3.0 -4.0] | |
| Implementation (to what extent✴) | ||||
| To what degree was the music intervention implemented on the CHU? | n | 17 | 18 | 57 |
| Median [IQR] | 4.0 [4.0 -5.0] | 4.0 [3.8 – 5.0] | 4.0 [3.0 – 5.0] | |
| Anticipated facilitators will be reinforced | n | 17 | 19 | 58 |
| Median [IQR] | 3.0 [2.5 – 4.0] | 3.0 [3.0 – 4.0] | 3.0 [2.0 -4.0] | |
| Anticipated barriers will be resolved | n | 17 | 17 | 59 |
| Median [IQR] | 4.0 [3.0 – 4.0] | 4.0 [3.0 -4.0] | 3.0 [2.0 -4.0] | |
| Sustainability | ||||
| Will the music intervention continue on the participating CHU(s) after the 6-month intervention period? | n | 16 | 19 | 62 |
| Yes, n (%) | 3 (18.8%) | 1 (5.3%) | 6 (9.7%) | |
| I don’t know, n (%) | 11 (68.8%) | 11 (57.9%) | 50 (80.6%) | |
*Answer options: 1 = Strongly disagree, 2 = Disagree, 3 = Neither agree nor disagree, 4 = Agree, 5 = Strongly agree. ✴Answer options: 1 = Not at all, 2 = To a small extent, 3 = To some extent, 4 = To a moderate extent, 5 = To a large extent. ≥ Answer options: 1 = Not satisfied, 2 = Hardly satisfied, 3 = Somewhat satisfied, 4 = Satisfied, 5 = Completely satisfied.
Table 3.
Countries’ median (IQR) baseline expectations (T0) related to relevance, feasibility and implementation of the trial and music interventions.
Table 3.
Countries’ median (IQR) baseline expectations (T0) related to relevance, feasibility and implementation of the trial and music interventions.
| Germany (n = 24) |
The Netherlands (n = 93) | Norway (n = 49) |
Türkiye (n = 61) |
Total** (n = 297) |
||
| Relevance and feasibility of the organization (level of agreement*), median [IQR] | ||||||
| Participating in the project will be relevant (meaningful, fitting, important) for this care home organization∇ | n | 6 | 5 | 4 | 6 | 21 |
| Median [IQR] | 4.0 [3.0 – 5.0] | 4.0 [4.0 – 4.5] | 4.5 [3.3 – 5.0] | 4.0 [3.8 – 5.0] | 4.0 [4.0 – 5.0] | |
| Recreational choir singing will be relevant for the care home residents with dementia and depressive symptoms | n | 21 | 43 | 36 | 26 | 126 |
| Median [IQR] | 5.0 [4.0 – 5.0] | 4.0 [4.0 – 5.0] | 5.0 [4.3 – 5.0] | 4.0 [3.8 – 5.0] | 5.0 [4.0 – 5.0] | |
| Group music therapy will be relevant for the care home residents with dementia and depressive symptoms | n | 21 | 43 | 35 | 25 | 124 |
| Median [IQR] | 4.0 [4.0 – 5.0] | 4.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 4.0 [4.0 – 5.0] | 4.5 [4.0 – 5.0] | |
| Recreational choir singing will fit well into the day-to-day practice of the participating CHU(s) | n | 21 | 43 | 34 | 26 | 124 |
| Median [IQR] | 4.0 [3.0 – 4.5] | 4.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 4.0 [3.8 – 5.0] | 4.0 [4.0 -5.0] | |
| Group music therapy will fit well into the day-to-day practice of the participating CHU(s) | n | 21 | 43 | 35 | 26 | 125 |
| Median [IQR] | 4.0 [3.0 – 4.0] | 4.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 4.0 [3.0 – 5.0] | 4.0 [4.0 – 5.0] | |
| I know which tasks I have to fulfill for the MIDDEL project | n | 21 | 43 | 32 | 26 | 122 |
| Median [IQR] | 5.0 [4.0 – 5.0] | 3.0 [2.0 – 4.0] | 4.0 [1.3 – 5.0] | 4.0 [3.0 – 4.0] | 4.0 [3.0 -5.0] | |
| Implementation, median [IQR] | ||||||
| Anticipated facilitators will be reinforced | n | 19 | 40 | 34 | 25 | 118 |
| Median [IQR] | 4.0 [3.0 – 4.0] | 3.0 [3.0 – 4.0] | 4.0 [3.0 – 4.0] | 4.0 [1.5 – 4.5] | 4.0 [3.0 – 4.0] | |
| Anticipated barriers will be resolved | n | 16 | 39 | 34 | 25 | 114 |
| Median [IQR] | 4.0 [3.0 – 4.0] | 4.0 [3.0 – 4.0] | 4.0 [3.0 – 4.0] | 4.0 [2.5 – 4.5] | 4.0 [3.0 – 4.0] | |
*Answer options: 1 = Strongly disagree, 2 = Disagree, 3 = Neither agree nor disagree, 4 = Agree, 5 = Strongly agree. **As there were only 2 surveys from the United Kingdom, these surveys are excluded from this analysis. ∇ This statement was only applicable for care home management.
Table 4.
Expectations (T0) and experiences (T6) across intervention groupsrelated to relevance, feasibility and implementation of the trial and music interventions.
Table 4.
Expectations (T0) and experiences (T6) across intervention groupsrelated to relevance, feasibility and implementation of the trial and music interventions.
| Expectations at baseline (T0) |
GMT (n = 26) |
RCS (n = 24) |
COMBI (n = 39) |
CONTROL (n = 30) |
|
| Relevance and feasibility (level of agreement*) | |||||
| Participating in the project will be relevant (meaningful, fitting, important) for this care home organization | n | 4 | 3 | 4 | 6 |
| Median [IQR] | 4.5 [4.0 – 5.0] | 3.0 [3.0] | 4.0 [ 4.0 – 4.8] | 4.5 [3.0 – 5.0] | |
| Recreational choir singing will be relevant for the care home residents with dementia and depressive symptoms | n | 25 | 24 | 39 | 30 |
| Median [IQR] | 4.0 [3.5 – 5.0] | 5.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 4.0 [4.0 – 5.0] | |
| Group music therapy will be relevant for the care home residents with dementia and depressive symptoms | n | 26 | 22 | 39 | 29 |
| Median [IQR] | 4.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 4.0 [4.0 – 5.0] | |
| Recreational choir singing will fit well into the day-to-day practice of the participating CHU(s) | n | 24 | 24 | 39 | 29 |
| Median [IQR] | 4.0 [3.0 – 5.0] | 4.0 [4.0 – 5.0] | 4.0 [4.0 – 5.0] | 4.0 [3.0 – 5.0] | |
| Group music therapy will fit well into the day-to-day practice of the participating CHU(s) | n | 26 | 23 | 39 | 29 |
| Median [IQR] | 4.0 [3.0 – 5.0] | 4.0 [3.0 – 5.0] | 4.0 [3.0 – 5.0] | 4.0 [4.0 – 5.0] | |
| I know which tasks I have to fulfill for the MIDDEL project | n | 25 | 23 | 37 | 29 |
| Median [IQR] | 3.0 [1.5 – 5.0] | 4.0 [3.0 – 4.0] | 4.0 [3.0 – 5.0] | 3.0 [2.0 – 4.0] | |
| Implementation | |||||
| Anticipated facilitators will be reinforced | n | 25 | 22 | 37 | 27 |
| Median [IQR] | 3.0 [3.0 – 4.0] | 4.0 [3.8 – 4.3] | 4.0 [3.0 – 5.0] | 3.0 [3.0 – 4.0] | |
| Anticipated barriers will be resolved | n | 23 | 22 | 36 | 26 |
| Median [IQR] | 4.0 [3.0 – 4.0] | 4.0 [4.0 – 4.0] | 4.0 [3.0 – 4.0] | 4.0 [3.0 – 4.0] | |
| Experiences at post-intervention (T6) |
GMT (n = 23) |
RCS (n = 17) |
COMBI (n = 35) |
CONTROL (n = 25) |
|
| General | |||||
| There was an Ambassador/contact person for the MIDDEL-project. | n | 19 | 15 | 31 | 23 |
| Yes, n (%) | 13 (68.4%) | 12 (80.0%) | 28 (90.3%) | 17 (73.9%) | |
| I don’t know, n (%) | 5 (26.3%) | 3 (20.0%) | 3 (9.7%) | 5 (21.7%) | |
| Supervision | |||||
| The supervision and guidance for the MIDDEL-project was sufficient | n | 4 | 3 | 7 | |
| Median [IQR] | 4.5 [4.0 – 5.0] | 5.0 [5.0 – 5.0] | 5.0 [4.0 – 5.0] | ||
| The supervision sessions throughout the MIDDEL-project were useful | n | 4 | 2 | 6 | |
| Median [IQR] | 4.5 [4.0 – 5.0] | 5.0 [5.0 – 5.0] | 5.0 [4.0 – 5.0] | ||
| Instruction | |||||
| Did you receive information explaining the MIDDEL-project? | n | 11 | 7 | 19 | 18 |
| Yes, n (%) | 6 (54.5%) | 6 (85.7%) | 14 (73.7%) | 14 (77.8%) | |
| I don’t know, n (%) | 1 (9.1%) | 1 (14.3%) | 1 (5.3%) | 2 (11.1%) | |
| I knew which tasks I had to fulfill for the MIDDEL-project |
n | 10 | 7 | 20 | 14 |
| Median [IQR] | 3.0 [1.0 – 4.3] | 4.0 [2.0 – 5.0] | 4.0 [4.0 – 5.0] | 4.0 [3.8 – 5.0] | |
| I was satisfied with the information offered prior to the start of the project | n | 12 | 8 | 20 | 16 |
| Median [IQR] | 4.0 [1.3 – 5.0] | 4.0 [3.0 – 4.8] | 4.0 [3.0 – 5.0] | 4.0 [3.0 – 5.0] | |
| The information, instruction, and guidance for the MIDDEL-project was sufficient | n | 10 | 8 | 21 | 15 |
| Median [IQR] | 3.5 [1.0 – 4.3] | 4.0 [3.0 – 4.0] | 4.0 [2.5 – 5.0] | 4.0 [4.0 – 5.0] | |
| It was relevant to receive information prior to the start of the MIDDEL-project | n | 11 | 7 | 23 | 15 |
| Median [IQR] | 4.0 [3.0 – 5.0] | 4.0 [3.0 – 4.0] | 5.0 [3.0 – 5.0] | 4.0 [4.0 – 5.0] | |
| Relevance and feasibility (level of agreement*) | |||||
| Participating in the project was relevant (meaningful, fitting, important) for this care home organization | n | 2 | 3 | 3 | 3 |
| Median [IQR] | 5.0 [5.0] | 4.0 [4.0] | 4.0 [3.0] | 3.0 [3.0] | |
| The music intervention was relevant for care home residents with dementia and depressive symptoms* | n | 23 | 17 | 32 | 15 |
| Median [IQR] | 4.0 [3.0 – 5.0] | 4.0 [3.5 – 5.0] | 4.0 [3.0 – 5.0] | 4.0 [4.0 – 5.0] | |
| The music intervention was relevant to reduce depressive symptoms | n | 22 | 17 | 32 | 14 |
| Median [IQR] | 3.0 [3.0 – 5.0] | 4.0 [3.0 – 5.0] | 3.0 [3.0 – 4.0] | 4.0 [3.0 – 5.0] | |
| The music intervention fit well into the day-to-day practice of the participating CHU(s) | n | 18 | 15 | 32 | 17 |
| Median [IQR] | 5.0 [4.0 – 5.0] | 4.0 [4.0 – 5.0] | 4.0 [3.0 – 4.0] | 5.0 [3.5 – 5.0] | |
| The music intervention turned out to be too complex to use | n | 17 | 15 | 32 | 14 |
| Median [IQR] | 3.0 [1.5 – 3.0] | 2.0 [1.0 – 2.0] | 3.0 [2.0 – 4.0] | 2.0 [1.0 – 3.0] | |
| The music intervention was in line with how we are used to working | n | 19 | 13 | 31 | 16 |
| Median [IQR] | 3.0 [2.0 – 4.0] | 4.0 [3.0 – 5.0] | 3.0 [2.0 – 4.0] | 4.5 [3.0 – 5.0] | |
| I would recommend the music intervention to other care homes | n | 19 | 15 | 31 | 17 |
| Median [IQR] | 5.0 [4.0 – 5.0] | 5.0 [4.0 – 5.0] | 4.0 [3.0 – 5.0] | 5.0 [4.0 – 5.0] | |
| Effect | |||||
| Did you notice any effect of the music intervention(s)? | n | 20 | 15 | 35 | 25 |
| Yes, on the CHU, n (%) | 6 (30.0%) | 3 (20.0%) | 6 (17.1%) | 3 (12.0%) | |
| Yes in care staff, n (%) | 4 (20.0%) | 5 (33.3%) | 9 (25.7%) | 2 (8.0%) | |
| Yes, in residents, n (%) | 12 (60.0%) | 14 (93.3%) | 20 (57.1%) | 7 (28.0%) | |
| No, n (%) | 2 (10.0%) | 11 (31.4%) | 3 (12.0%) | ||
| I don’t know, n (%) | 5 (25.0%) | 1 (6.7%) | 2 (5.7%) | 5 (20.0%) | |
| Not applicable, n (%) | 3 (15.0%) | 7 (8.0%) | |||
| Satisfaction (level of satisfaction≥) | |||||
| To what extent were you satisfied with the implementation of the MIDDEL-project? | n | 19 | 15 | 32 | 21 |
| Median [IQR] | 4.0 [3.0 – 4.0] | 4.0 [4.0 – 5.0] | 4.0 [3.0 – 4.8] | 4.0 [3.0 – 4.5] | |
| Implementation (to what extent✴) | |||||
| To what degree was the music intervention implemented on the CHU? | n | 19 | 15 | 31 | 22 |
| Median [IQR] | 4.0 [3.0 – 4.0] | 4.0 [3.0 – 4.0] | 3.0 [2.0 – 4.0] | 3.0 [2.0 – 4.0] | |
| Anticipated facilitators were reinforced | n | 20 | 15 | 32 | 22 |
| Median [IQR] | 3.0 [3.0 – 4.0] | 4.0 [3.0 – 4.0] | 3.0 [2.0 – 4.0] | 4.0 [3.0 – 4.0] | |
| Anticipated barriers were resolved | n | 20 | 15 | 32 | 22 |
| Median [IQR] | 4.0 [3.0 – 4.0] | 4.0 [4.0 – 5.0] | 4.0 [3.0 – 5.0] | 4.0 [2.3 – 5.0] | |
| Sustainability | |||||
| Will the music intervention continue on the participating CHU(s) after the 6-month intervention period? | n | 20 | 15 | 34 | 23 |
| Yes, n (%) | 2 (10.0%) | 2 (13.3%) | 2 (5.9%) | 4 (17.4%) | |
| I don’t know, n (%) | 15 (75.0%) | 11 (73.3%) | 27 (79.4%) | 15 (65.2%) | |
*Answer options: 1 = Strongly disagree, 2 = Disagree, 3 = Neither agree nor disagree, 4 = Agree, 5 = Strongly agree. ✴Answer options: 1 = Not at all, 2 = To a small extent, 3 = To some extent, 4 = To a moderate extent, 5 = To a large extent. ≥ Answer options: 1 = Not satisfied, 2 = Hardly satisfied, 3 = Somewhat satisfied, 4 = Satisfied, 5 = Completely satisfied.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



