Submitted:
15 April 2025
Posted:
16 April 2025
You are already at the latest version
Abstract
The main source of microorganisms in the blood is the intestinal and oral microflora through the route of atopobiosis. It is clear that the blood microbiome undergoes signifi-cant changes in response to various pathological conditions within the human body. In this review, we summarized data from studies of the human blood microbiome in diseas-es of the nervous system, cardiovascular, respiratory, liver, kidney, and metabolite disor-ders. Links between blood microbiome and the above mentioned diseases were demon-strated. In support of this understanding, it is evident that analogous alterations in microbiome composition occur across various disease categories; however, the microbial signatures associated with the blood microbiome exhibit specificity. For instance, elevated abundancy of Proteobacteria have been identified in cardiovascular, renal, and metabolic disorders. Conversely, while Firmicutes are found to be abundant in renal and metabolic conditions, their levels are diminished in cardiovascular diseases. Additionally, patients suffering from respiratory and liver ailments typically show a heightened presence of Bacteroidetes; notably, Flavobacterium is prevalent in respiratory diseases, whereas Enterobacteriaceae is associated with liver diseases. Hence, human blood microbiome could be considered as potentiаl biomarker in certain diseases.
Keywords:
blood
; microbiome
; nervous system
; cardiovascular diseases
; metabolite disorders
; microorganisms
; erythrocytes
1. Introduction
A well-regulated microbiome, consisting of viruses, bacteria, and fungi, is present in the bloodstream. Increasing evidence indicates that these entities represent living microbiota whose specific roles within the macroorganism remain largely undefined. It is believed that they gain entry into the circulatory system via the intestinal mucosal barrier [1] and the oral cavity [2]. Kalfin (1997), who reported the existence of non-pathogenic microbiota within erythrocytes [3], conducted one of the pioneering studies in this field. Following this, research has explored the microbial content in erythrocytes among both healthy individuals [4,5] and those suffering from chronic illnesses [6,7]. Recently, there has been a surge in scientific inquiry into this subject, yielding a wealth of new information. The review by Castillo et al. (2019) supports the contemporary understanding that microorganisms are normally present in the blood of healthy individuals, challenging the earlier belief that blood is sterile or that detected microbiota are merely “imported” from the intestinal and skin microbiomes [8]. An experiment by Lucchinetti et al. (2022) involving experimental mice on total parenteral nutrition further substantiates the notion that the intestinal and blood microbiomes represent distinct compartments [9]. In this context, Velmurugan et al. (2020) concluded that, in contrast to the intestinal microflora, which is predominantly composed of Firmicutes and Bacteroidetes, the blood microbiome is primarily characterized by a high abundance of Proteobacteria (85-90%) [10]. Sciarra et al. (2023) provide a comprehensive overview of the current understanding regarding the composition of the blood microbiome in healthy individuals, including its origins and localization within and outside the formed elements [11]. Numerous investigations have focused on the composition and variations of the human blood microbiome in response to various factors and in pathological conditions. Furthermore, a pilot study from 2024 investigated the possibility of considering the microbiome signature as a method for identification of different body fluids (including blood) in forensic medicine [12].
Research indicates variations in the composition of the blood microbiome based on factors such as age, race, and specific conditions like smoking and pregnancy. A study conducted in 2022 examined the blood microbiome of healthy individuals, revealing age-related differences [13]. The analysis involved 37 blood samples from five families in South Korea, which demonstrated that over 95% of the blood microbiota consisted of Proteobacteria. Each age cohort exhibited distinct characteristics in their blood microbiome. Notably, individuals over 60 years showed a predominance of Gammaproteobacteria, while the classes Alphaproteobacteria, Deltaproteobacteria, and Clostridia were significantly less prevalent compared to younger age groups. The authors suggest that this pattern may be linked to chronic diseases commonly associated with aging, which are influenced by a microbiota that contributes to metabolic endotoxemia and chronic inflammation.
Further research by Gupta et al. (2017) identified geographical differences in the blood microbiome composition among healthy individuals based on latitude [14]. The findings indicated that populations in Germany and Poland exhibited a higher concentration of microorganisms in the central compartment, while Italy and Finland showed average levels, and Belgium and Austria had lower concentrations.
The inaugural study examining the distinct composition of the blood microbiome as a potential contributor to persistently elevated levels of interleukin-6 (IL-6) in healthy African Americans compared to Caucasian Americans was published in 2024 [15]. This investigation focused exclusively on female participants from both demographic groups, revealing the presence of eight bacterial genera/phyla. IL-6 is a critical mediator in chronic inflammatory processes, which are observed with greater frequency in the African American population. The research team identified five bacterial genera that exhibited a significant association with IL-6 levels, notably finding that the abundance of Actinomyces was directly correlated with elevated plasma concentrations of this pro-inflammatory cytokine in healthy African Americans. While this research marks a promising advancement in the realm of personalized medicine, the authors did not provide epidemiological data regarding the incidence of chronic inflammatory diseases among the study participants. Additionally, a limitation of the study is its exclusive focus on female subjects.
The blood microbiome investigation conducted by You et al. (2019) spans the years 2008 to 2010 and involved 45 pregnant women who were tested two or three times throughout their pregnancy and identified Firmicutes, Proteobacteria, Bacteroidetes, and Actinobacteria as the predominant phyla [16]. Notably, the microbiome composition differed in women who experienced premature births, with an increase in Firmicutes and Bacteroidetes, while Proteobacteria exhibited a decrease. In instances of premature birth, a microbiome rich in Bacteroides, Lactobacillus, Sphingomonas, Fastidiosipila, Weissella, and Butyriciococcus was documented, leading researchers to propose that these specific taxonomic groups may be linked to the complications associated with premature delivery.
A 2021 study conducted a comparative analysis of the blood microbiome profiles of former and current smokers, marking a significant advancement in this field of research [17]. The authors assert that this comprehensive investigation will elucidate the connections between the microbiome and various pathological processes in humans, thereby enhancing the potential for personalized therapeutic approaches.
In a pioneering investigation, the hypothesis of a "dormant" blood microbiome in healthy individuals had been explored, leading to the isolation of specific microbial members [18]. The study identified similarities in operational taxonomic units (OTUs) across cultured and uncultured samples, revealing 47 bacterial orders from 15 species and 39 fungal orders from 2 phyla. This research also marked the first instance of isolating and sequencing a fungal blood microbiota in healthy subjects, while further examining variations associated with different blood types. The findings bolster the hypothesis that a dormant blood microbiome is an inherent characteristic of healthy individuals. In 2021, our research investigated the differences in microbial biodiversity between whole blood and blood subjected to stress conditions [19]. The findings indicated that certain microbial species exhibited an increase in abundance, indicating proliferation, while others showed a decline. Additionally, in two other studies conducted by our team, we performed microscopic characterization of blood microbiota cultivated in a cell-free environment [18,20]. A significant diversity of OTUs was identified in both cultured and uncultured blood samples, encompassing six phyla and fifteen bacterial orders, with a predominance of genera from the Proteobacteria phylum. Among the fungi identified, the Ascomycota and Basidiomycota phyla were the most prevalent [19].
The etiology of cancer remains a persistent area of scientific inquiry [21,22]. Recent advancements in microbiome analysis and bioinformatics have revealed that microbial component also contributes to cancer etiology [23]. Two recent studies have been published that outline bioinformatics models for analyzing the blood microbiome in rare diseases, including sarcoidosis [24,25]. These studies assessed the severity of the disease and identified specific microbial species associated with it.
Latent infections, such as tuberculosis, are known to be triggered by microbial species that remain uncultured during the latent phase. This latent state can persist for many years, sometimes even decades. Research has demonstrated that various viruses can exist in either a lytic or latent form within the blood and tissues throughout an individual's lifetime [26,27]. It is reasonable to propose that for numerous microbial species, this represents a strategy to inhabit the blood or tissues of the host organism without inducing disease. Under conditions of stress, these latent infections may become active, leading to the proliferation of the persistent microbial species.
A comprehensive investigation of the blood microbiome has the potential to yield significant scientific insights that could enhance the management of human health. Currently, our understanding of dysbiosis within this central compartment is markedly limited. Such dysbiotic conditions are frequently linked to a suspected infectious origin that remains unexplained. Notably, diseases like schizophrenia, amyotrophic lateral sclerosis, and cancer may be correlated with the pathological state of the blood microbiome [28].
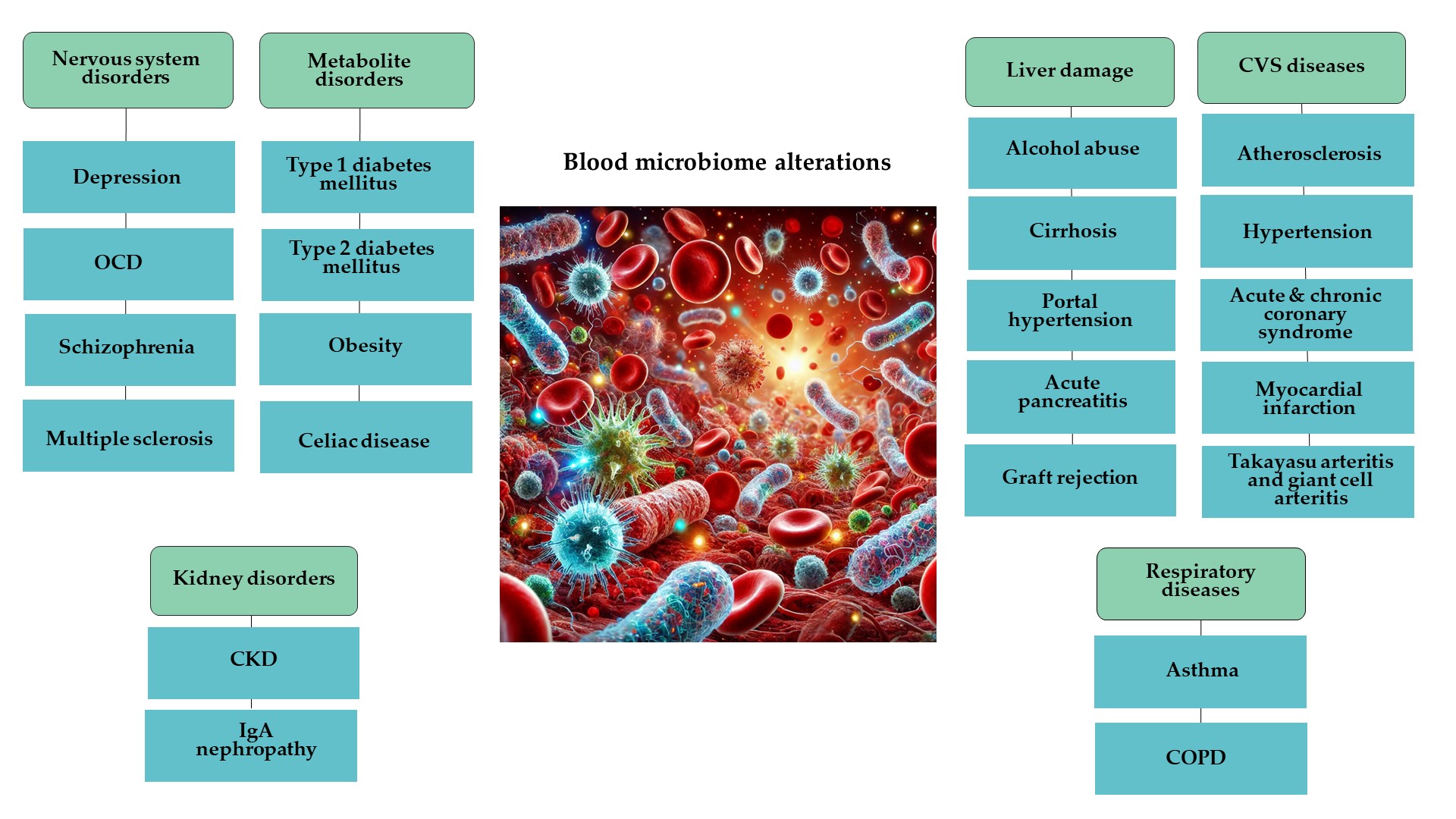
Numerous studies have emerged over the past decade that investigate various dimensions of this hypothesis. These studies highlight certain inconsistencies and address the limitations of the proposed concepts. It is clear that the blood microbiome undergoes significant changes in response to various pathological conditions within the human body as illustrated in Figure 1.
These alterations have been observed across multiple systems, including the gastrointestinal [29,30,31,32], cardiovascular [33,34,35], respiratory [17], excretory [36,37,38], and reproductive systems [39,40]. Additionally, changes in the blood microbiome have been linked to type 2 diabetes [41] and various malignancies [42,43].
There is a compilation of data regarding the composition of the circulating microbiome, particularly concerning the presence of dysbiosis in patients with non-infectious conditions such as diabetes and cardiovascular diseases, aimed at enhancing understanding of early detection and the pathogenetic mechanisms involved [44]. Additionally, another review article explores the association between dysbiotic blood microbiota (specifically L-type or cell wall-deficient microbes) and various diseases, including multiple sclerosis, Parkinson's disease, psoriasis, diabetes, and thyroid cancer, considering its potential to trigger disease and serve as a prognostic model [45].
Pilot studies have been undertaken to explore the potential mechanisms underlying the interactions between microbiota and macroorganisms. Microorganisms engage with the cells of a healthy host through various compounds produced during circulation, including metabolites, lipoglycans, peptides, proteins, and bacterial extracellular vesicles [46]. In their comprehensive review, Jensen and Benson (2019) discuss the hypothesis that the composition of the circulating microbiome differs in patients with chronic diseases compared to that of healthy individuals [47]. Supporting this notion, Luo et al. (2021) conducted a study aimed at identifying an appropriate method for detecting alterations in the plasma microbiome of immunocompromised patients, thereby enhancing the qualitative application of this approach in clinical settings [48]. Recent advancements have enabled the monitoring of changes in the blood microbiome composition, which may serve as diagnostic and prognostic indicators in clinical practice [49]. Accumulated clinical evidence from various conditions, including early-stage cardiovascular diseases [34,50], type 2 diabetes [33], and non-alcoholic fatty liver disease in obese individuals [29], suggests that alterations in the blood microbiome could function as biomarkers.
An increasing body of research is focused on the alterations in the blood microbiome, specifically dysbiosis, associated with particular diseases or disease categories. Variety of reviews have been released that explore different aspects of this topic, including the application of dysbiosis in the blood microbiome as a potential biomarker for certain diseases [11]. Additionally, these reviews address the difficulties associated with microbiota detection and the need for standardized methodologies [40]. Furthermore, they provide insights into the characterization of both eubiotic and dysbiotic conditions of the microbiome found in the bloodstream [51]. The current approach to conducting blood microbiome composition is presented in Figure 2.
Enhancing the expertise of professionals in this area could prove beneficial not only for the prediction and monitoring of pathological conditions but also for evaluating the risks associated with blood transfusions. This review aims to consolidate recent findings to enhance the comprehension of pathological mechanisms in relation to circulating microbiotas. The necessity for a comprehensive summary of current knowledge is evident, particularly following a mini-review published in 2020 [52] and an editorial from 2023 [53], both of which referenced only a limited number of sources.
2. Results
2.1. Changes in Blood Microbiome in Nervous System Disorders
Central nervous system is of extreme importance for appropriate function of the whole body. Brain is well protected through blood-brain barrier which excludes most microbes. Nevertheless, bacteria can pass through the gut barrier and be found in the blood. In this regard, recently it was demonstrated that extracellular vesicles, produced by gut microbiota, can enter systemic circulation and be delivered to body sites, including the brain [54]. Hence, it is not surprising that blood microbiome was shown to be involved in some nervous system disorders. It is interesting to note that an oral bacterium, Porphyromonas gingivalis, was detеcted to translocate to the brain and to play a role in Alzheimer’s disease [55].
Serum microbiome composition may be an useful tool in distinguishing between major depressive disorder and bipolar disorder [56]. In particular, Rhee and coworkers (2020) demonstrated that Ruminococcaceae UCG-002 and Prevotella 2 genera might be used for distinguishing the upper mentioned depressive disorders. Inspired by the results, the team continued research on this topic, and found out that аnxiety symptoms were associated positively with Dеsulfovibrionacеaе fаmily DNA composition in the serum of pаtients [57]. On the other hand, Dеsulfovibrionacеa family was shown to be composed of gram-negative anaerobes which produce hydrogen sulfide [58]. In such regard, pro-inflammatory property of hydrogen sulfide could mediate the association between inflammation and anxiety severity [59]. Patients with depression were also shown to possess a distinct blood microbiome that changes after antidepressant treatment [60]. Using shallow-shotgun metagenomic sequencing to characterize the plasma microbiome of people with human immunodeficiency viruses and healthy controls, all of whom underwent a comprehensive neuropsychiatric assessment, Taylor and coworkers demonstrated that the risk of major depressive disorder might be increased by circulating plasma microbiome in people with human immunodeficiency viruses [61].
Recently, transcriptome analysis in whole blood was shown to reveal increased microbial diversity in schizophrenia [62]. In this interesting study by using high-quality RNA sequencing reads, authors investigated blood microbiome in patients with bipolar disorder, amyotrophic lateral sclerosis, schizophrenia as well as in healthy controls. As a result wide range of bacterial and archaeal phyla were detected in the blood. Increased microbial diversity was demonstrated in patients with schizophrenia as compared to those with amyotrophic lateral sclerosis, bipolar disorder or healthy individuals [62].
Obsessive–compulsive disorder (OCD) is often considered as a highly disabling neuropsychiatric disorder which could impair general functions of an individual. Kang and coworkers (2023) examined bacterial DNA in serum samples taken from OCD patients and healthy controls [63]. They found that Pseudomonas, Caulobacteraceae (f), Streptococcus, Novosphingobium, and Enhydrobacter at the genus level were significantly less prevalent in patients with OCD than in healthy controls. In addition, among patients with OCD, the microbial composition in the early-onset versиs late-onset types was significantly different with respect to the genera Corynebacterium and Pelomonas.
Links between multiple sclerosis and human blood microbiome were studied by the change in the representation of microbiota phylotypes, the proportion of coccal flora, the proportion of anaerobic, gram-negative, proteolytically active microflora, as well as the concentration of markers of bacterial plasmalogen and endotoxin in the blood [64]. It was shown that the proportion of coccal, gram-negative, anaerobic microflora with a proteolytic type of metabolic activity increases in multiple sclerosis. These elevation in blood concentrations of microbial markers of bacterial plasmalogen and endotoxin may be associated with an increase in the permeability of the intestinal wall. Нence, multiple sclerosis could be associated with pathological changes in the structurе of microbiome, which might be among important factors in the pathogenesis of this disease.
2.2. Changes in Blood Microbiome in Cardiovascular Diseases
Cardiovascular diseases (CVD) represent a significant public health concern, impacting a substantial segment of the global population. This category encompasses conditions such as hypertension, hyperlipidemia, atherosclerosis, and heart failure, along with associated complications. These diseases not only pose risks of severe health complications and mortality but are also frequently linked with co-morbidities involving metabolic, renal, and other disorders. The expression and prognosis of these conditions are influenced by a variety of factors. Recently, there has been growing interest within the scientific community regarding the microbiome's influence on the pathological mechanisms that affect cardiovascular health. A study conducted by Guo et al. (2021), which synthesizes findings from 17 studies with over 9,000 participants, explores the connection between hypertension and the intestinal microbiome [65]. The proliferation of certain Proteobacteria and Bacteroidetes has been associated with the enhanced production of lipopolysaccharides, the activation of specific transporters, and the inhibition of the metabolism of various amino acids. This phenomenon is indicative of dysbiosis within the intestinal microbiota, characterized by diminished diversity, alterations in microbial composition and functionality, changes in microbial interactions, and other contributing factors.
Over a decade ago, Amar et al. (2013) explored the potential implications of the blood microbiome in the context of cardiovascular diseases [33]. Their research, which encompassed nearly 4,000 patients over a nine-year follow-up period, identified dysbiosis of the blood microbiota as an independent risk factor for the onset of heart disease. Among those who experienced cardiovascular complications during the study, a notable reduction in the normally present microbiota alongside an increase in Proteobacteria levels was observed. Rajendhran et al. (2013) elucidated the distinct composition of the blood microbiome in healthy individuals versus those suffering from cardiovascular diseases in India [66]. In healthy subjects, the predominant bacterial phyla are Firmicutes and Proteobacteria. Conversely, patients exhibit a notable dysbiosis, characterized by a significant increase in Proteobacteria, particularly from the family Pseudomonadaceae and class Gammaproteobacteria, alongside a reduction in Firmicutes, specifically from the family Staphylococcaceae. Supporting this observation, Koren et al. (2011) reported a similar microbiota composition within atherosclerotic plaques [67]. Additionally, Sharifullina et al. (2023) investigated the circulating microbiome in individuals with atherosclerotic vascular damage, involving a cohort of 35 patients (23 men and 12 women) diagnosed with carotid artery atherosclerosis [68]. The bacterial cultures derived from both blood samples and atherosclerotic plaques exhibited slow growth on nutrient media, with the growth rate correlating with leukocyte counts and high-density lipoprotein levels in the participants' blood. According to the findings of Dinakaran et al. (2014), patients with CVD exhibited elevated levels of circulating bacterial DNA and greater bacterial diversity compared to healthy individuals. Specifically, in the cohort of CVD patients (n = 80), Actinobacteria were the most prevalent phylum, followed by Proteobacteria [34]. In contrast, healthy controls (n = 40) showed a predominance of Proteobacteria, with Actinobacteria following. Furthermore, while healthy individuals demonstrated a higher prevalence of eukaryotic viruses, particularly Lymphocystis virus and Torque Teno viruses, the virome in CVD patients was notably enriched with bacteriophages, primarily those associated with Propionibacterium, Pseudomonas, and Rhizobium.
In their studies conducted in 2020 and 2022, Velmurugan et al. highlighted the significant role of the human microbiome in the development and progression of various cardiovascular and metabolic disorders [10,69]. They substantiated the hypothesis that dysbiosis and a reduction in the diversity of blood microbiota are prevalent in conditions that impact the cardiovascular system and metabolic health. The authors suggest that these findings may facilitate the integration of microbiome-focused strategies into therapeutic interventions. Additionally, Jing et al. (2021) examined the correlation between the composition of the peripheral microbiome and the likelihood of developing hypertension [70]. Their research involved 150 individuals diagnosed with hypertension and 150 healthy participants, carefully matched for sex and age. The results indicated a higher prevalence of Proteobacteria and a lower prevalence of Firmicutes and Bacteroidetes in the hypertensive group compared to the control group without hypertension.
Khan's research team published a series of studies in 2022 that provided an in-depth analysis of the alterations in the blood microbiome associated with various nosological conditions impacting the cardiovascular system. One notable study focused on the influence of circulating microbiota on atherosclerotic damage [71]. This investigation involved 70 patients diagnosed with acute coronary syndrome, 70 with chronic coronary syndrome, and 70 healthy control subjects from China. The findings revealed an increase in microbiota diversity among patients with acute coronary syndrome, whereas a decrease was observed in those with chronic conditions. The blood microbiome exhibited distinct compositions across the three participant groups, with the microbial profiles of both acute and chronic coronary syndrome patients differing significantly from that of the healthy cohort. This supports the hypothesis that the microbial ecology within the blood undergoes alterations in pathological states. At the phylum level, the blood microbiota of patients with acute coronary syndrome, chronic coronary syndrome, and healthy individuals was predominantly composed of Firmicutes (39%, 45%, 43%, respectively), Bacteroidetes (31%, 32%, 29%, respectively), and Proteobacteria (19%, 15%, 15%, respectively). Comparative analysis between the heart disease groups indicated that Proteobacteria were overrepresented in acute coronary syndrome patients (19% vs. 9%), while Firmicutes (44% vs. 38%) and Bacteroidota (32% vs. 31%) were found to be underrepresented in this group relative to those with chronic disease. In blood of patients with acute coronary syndrome, a notable increase in the phylum Acidobacteriota was observed, followed by Actinobacteriota, Cloacimonadota, Fibrobacterota, Fusobacteriota, Latescibacterota, Myxococcota, Nitrospirota, Proteobacteria, Synergistota, and Thermotogota. Conversely, there was a marked reduction in the levels of Cyanobacteria, Deferribacterota, Desulfobacterota, Firmicutes, Gemmatimonadota, Patescibacteria, and Verrucomicrobiota when compared to individuals with chronic coronary syndrome. A comparative analysis of the blood microbiome composition between affected patients and healthy controls further substantiates the hypothesis that such evaluations may yield potential biomarkers for the identification of coronary diseases. In the cohort with acute coronary syndrome, Bacteroidota and Proteobacteria emerged as the most prevalent phyla, whereas Firmicutes predominated in the healthy control group. In contrast, the chronic coronary syndrome group exhibited a slight increase in Firmicutes and Bacteroidota, alongside a decrease in Proteobacteria relative to healthy volunteers. The researchers later broadened their investigation to include patients diagnosed with myocardial infarction (n = 29) [72]. Their findings revealed a notable reduction in microbial diversity within the myocardial infarction cohort when compared to healthy controls (n = 29). Additionally, there were significant differences in both the composition and richness of the microbiota between the infarction patients and the healthy subjects. Notably, members of the Actinobacteria phylum (class Actinobacteria, order Bifidobacteriales, family Bifidobacteriaceae, genus Bifidobacterium) were found to be significantly more prevalent among the myocardial infarction patients, whereas the Bacteroidetes phylum (class Bacteroidia, order Bacteroidales) was more dominant in the healthy control group. A subsequent study conducted in 2024 further substantiated the notion that alterations in the blood microbiome could serve as an independent biomarker for acute myocardial infarction [73]. This investigation involved 55 patients with acute myocardial infarction and 62 patients with unstable angina. The results indicated a significantly higher diversity of the serum microbiome in the infarction group compared to those with unstable angina. Conversely, the unstable angina patients exhibited a greater abundance of Gammaproteobacteria, Proteobacteria, Ralstonia pickettli, Ralstonia, Burkholderiaceae, and Burkholderiales, while the infarction group showed higher levels of Bacteroidales, Bacteroidia, Bacteroidota, Clostridia, and Firmicutes.
In addition, other diseases within this category impact the vascular wall. In 2021, Desbois et al. identified a distinct microbiome signature in patients suffering from inflammatory diseases affecting large vessels, specifically Takayasu arteritis and giant cell arteritis [74]. This investigation included 13 patients with Takayasu arteritis, 9 with giant cell arteritis, and 15 healthy controls. The findings revealed elevated levels of Clostridia, Cytophagia, and Deltaproteobacteria, along with a reduction in Bacilli among patients with Takayasu arteritis. Conversely, those diagnosed with giant cell arteritis exhibited an increased presence of Rhodococcus and an unidentified member of the Cytophagaceae family. Notably, the microbiota in Takayasu arteritis patients displayed higher levels of Candidatus Aquiluna and Cloacibacterium compared to those with giant cell arteritis.
Lawrence et al. (2022) established a connection between the composition of the circulating microbiome and the risk of mortality due to cardiovascular disease [35]. Their case-cohort study spanned nine years and involved age-matched participants (n = 227) who succumbed to cardiovascular disease, alongside controls who were randomly selected from the same cohort (n = 178). A limitation of this research is that it exclusively included male participants. The study identified three bacterial genera that were significantly correlated with mortality as independent factors: elevated levels of Kocuria and Enhydrobacter were associated with increased cardiovascular mortality, whereas Paracoccus exhibited an inverse relationship.
Table 1 provides a schematic representation of the characteristics of the microbiome in individuals diagnosed with CVD.
2.3. Changes in Blood Microbiome in Respiratory Diseases
Research concerning the influence of the microbiome on lung disease has predominantly concentrated on the specific characteristics of the gut microbiome [75,76,77,78]. The investigation of the local microbiome within the respiratory tract, particularly in relation to pathological processes that impact the respiratory system, represents a relatively novel area of research [79,80,81,82].
At present, there is a scarcity of literature examining the changes in the microbiome plasma signature linked to diseases of the respiratory system. The beforementioned study conducted by Morrow et al. (2021) involved a sample of 2,590 participants, which included both individuals who had previously smoked and those who were current smokers, as well as individuals with and without chronic obstructive pulmonary disease (COPD) [17]. The predominant bacterial phyla identified in the blood samples included Proteobacteria, Actinobacteria, Firmicutes, and Bacteroides. Notable correlations were observed between the severity of dyspnea and the presence of Acinetobacter, Serratia, Streptococcus, and Bacillus in the bloodstream. In active smokers, the blood microbiome was primarily characterized by the dominance of Acinetobacter, Serratia, and Cutibacterium. In the preceding year, Morrow et al. released findings concerning alterations in the blood microbiome that correlate with the clinical manifestations of chronic obstructive pulmonary disease [83]. The occurrence of Flavobacterium has been linked to both the onset and advancement of emphysema. Additionally, a correlation was identified between the exacerbation of COPD and the relative prevalence of Staphylococcus, Acidovorax, and Cupriavidus.
A research investigation conducted in the same year revealed variations in the blood microbiome and suggested these differences as a possible diagnostic indicator for asthma [84]. A total of 260 healthy participants and 190 individuals diagnosed with asthma were recruited for this study. Notable differences were observed in the blood microbiome between asthma patients and healthy controls. Specifically, at the phylum level, Bacteroidetes exhibited a higher prevalence in individuals with asthma, whereas Actinobacter, Verrucomicrobia, and Cyanobacteria were found to be more abundant in the healthy control group.
A separate investigation examined the microbiome signature present in the blood, gastrointestinal tract, and lungs of individuals suffering from acute respiratory distress syndrome [85]. Blood samples from a cohort of 16 patients, collected over the course of one year, were analyzed. The study revealed a 20% overlap in the microbiota composition across the three examined compartments. Notably, the presence of the Proteobacteria phylum was observed in the blood of healthy individuals, correlating with reduced inflammation levels in the clinical cases assessed. Conversely, Bacteroidetes emerged as the predominant phylum within the blood microbiome of patients suffering from acute respiratory distress syndrome. It is important to note that the pilot study is constrained by a limited sample size, as well as other methodological considerations, rendering the findings more suggestive than statistically robust.
2.4. Changes in Blood Microbiome in Liver Damage
The liver plays a crucial role in the survival of the organism. Its strategic position and diverse functions render it susceptible to various diseases, which can arise from different causes, including infectious, toxicological, and parasitological factors. These conditions are frequently associated with immune responses, inflammatory reactions, or metabolic alterations.
The hypothesis linking microbiome composition to overall health has been recognized in scientific discourse for some time. However, it was not until 2016 that two separate studies were published examining the relationship between the blood microbiome and individuals suffering from liver cirrhosis and obesity by Lelouvier et al. (2016) [29], as well as those with liver cirrhosis and ascites by Santiago et al., (2016) [86]. The research conducted by Lelouvier et al., which involved 50 patients from Spain and 71 from Italy, identified an increased presence of microorganisms in patients with liver fibrosis, yet it did not succeed in pinpointing a distinct microbiome signature. Santiago et al. (2016) conducted a study examining the microbiome composition of intestinal, blood, ascitic, and fecal microflora in patients with liver cirrhosis accompanied by ascites (n = 13), in comparison to those with cirrhosis without ascites (n = 14). Their findings revealed that the serum microbiome of individuals with ascites exhibited elevated levels of lipopolysaccharide-binding protein, a known indicator of microbial translocation. This phenomenon accounts for the increased diversity and relative abundance of Clostridiales and an unidentified genus within the phylum Cyanobacteria, alongside a diminished presence of Moraxellaceae in patients with ascites relative to those without. The authors suggest that alterations in the blood and fecal microbiome composition may serve as biomarkers for assessing the progression of cirrhosis. Building on the work of Santiago et al. (2016), a subsequent study conducted in the following year by Traykova et al. (2017) focused on the blood microbiome of patients with decompensated cirrhosis (n = 9) compared to healthy controls (n = 9) [30]. This investigation revealed a significant increase in the number of bacterial species present in the blood of cirrhotic patients compared to the control group. Specifically, 9 out of 12 bacterial orders were identified in individuals with liver disease, whereas only 2 were detected in healthy subjects. The microbiota in cirrhotic patients included the following types: Firmicutes (9 species), Proteobacteria (6 species), Bacteroidetes (3 species), and Verrucomicrobia (1 species). However, the study's limitations include the small sample size and the exclusive inclusion of male participants. Conversely, the research was enhanced by exploring the correlations between the identified microbiota and various hemodynamic parameters and inflammatory markers. A study conducted in 2019 analyzed the blood microbiome composition of 66 patients suffering from liver cirrhosis alongside 14 healthy individuals [31]. The investigation revealed that patients exhibited 183 distinct taxonomic units at the genus level, in contrast to the 123 units identified in the healthy cohort. Notably, the blood microbiome of individuals with the liver disease showed a marked increase in Enterobacteriaceae, whereas the levels of Akkermansia (phylum Verrucomicrobiota), Rikenellaceae (Phylum: Bacteroidota), and Erysipelotrichales (phylum Bacillota) were significantly diminished when compared to the healthy controls.
A study conducted in 2024 established a correlation between the progression from compensated to decompensated liver cirrhosis in hepatitis C patients and alterations in blood microbiome composition [87]. This investigation included a total of 88 subjects. The findings revealed that individuals with decompensated cirrhosis exhibited a significant reduction in microbial diversity, characterized by an increased prevalence of Proteobacteria, Alphaproteobacteria, Sphingomonadales, and Sphingomonadaceae when compared to those with compensated cirrhosis.
Further research in this domain has been conducted, including studies from 2018 that explored the blood microbiome in various liver diseases, specifically in patients suffering from severe acute pancreatitis and alcoholic hepatitis. One particular study involved 50 patients diagnosed with severe acute pancreatitis—comprising groups with no infection (n = 17), with infection (n = 16), and septic cases (n = 17)—alongside 12 healthy controls [88]. The objective was to monitor changes in microbial composition and to establish correlations with disease severity and the likelihood of complications. The microbiomes associated with blood and neutrophils in pancreatitis cases were found to be enriched in Bacteroidetes and Firmicutes, while a decline in Actinobacteria was noted. These microbial alterations were associated with elevated serum cytokine levels and various immunological markers. The authors concluded that the observed changes in the blood microbiome during acute pancreatitis do not serve as reliable predictors for the risk of infectious complications. A study conducted by Puri et al. in 2018 examined patients with moderate (n = 18) and severe (n = 19) alcoholic hepatitis, comparing their results with those of alcoholics without liver disease (n = 19) and non-alcoholic controls (n = 20) [89]. The findings revealed a significant reduction in the presence of Bacteroidetes among all individuals who consumed alcohol when compared to the non-alcoholic controls. Conversely, all alcohol-consuming groups exhibited an increased presence of Fusobacteria, with the highest levels found in alcoholics without liver damage, which subsequently decreased in the groups with alcoholic hepatitis. Notably, the analysis indicated that both alcoholics without hepatitis and those with severe alcoholic hepatitis harbored gram-negative bacterial flora, suggesting that excessive alcohol consumption is a contributing factor to the alterations observed in the circulating microbiome.
Additionally, a study by Gedgaudas et al. (2022) focused on the blood microbiome variations in patients suffering from portal hypertension, analyzing its composition across two distinct vascular compartments: the peripheral and hepatic veins [90]. This investigation included 58 cirrhotic patients and 46 healthy controls, while also monitoring pH levels, liver function, inflammatory markers, and gut permeability. The findings revealed that the blood microbiome of individuals with liver damage exhibited elevated levels of Comamonas (Class: Betaproteobacteria), Cnuella (phylum Bacteroidota), Dialister (phylum Bacillota), Escherichia/Shigella (class Gammaproteobacteria), and Prevotella (phylum Bacteroidota), alongside reduced levels of Bradyrhizobium (class Alphaproteobacteria), Curvibacter (class Betaproteobacteria), Diaphorobacter (class Betaproteobacteria), Pseudarcicella, and Pseudomonas (class Gammaproteobacteria). The presence of genera such as Bacteroides, Escherichia/Shigella, and Prevotella was linked to severe clinical manifestations, with Escherichia/Shigella and Prevotella correlating with heightened interleukin-8 levels. Nevertheless, the authors concluded that the profiles of circulating microbiota do not serve as reliable predictors of disease severity.
In 2023, Vasudevan et al. examined alterations in the blood microbiome associated with various liver diseases, such as liver cirrhosis, fibrosis, hepatocellular carcinoma, chronic viral liver failure, and alcoholic hepatitis, among others [91]. The authors explored the potential of these microbiome changes as independent biomarkers for liver-related pathologies.
An intriguing area of research involves the examination of microbiome dynamics in patients undergoing liver transplantation. A study conducted in 2021 monitored 51 liver transplant recipients for a duration of up to 8 weeks post-surgery [92]. The analysis revealed significant fluctuations in the blood microbiome composition, particularly concerning the levels of Anelloviridae, Nocardiaceae, Microbacteriaceae, and Enterobacteriaceae at various postoperative intervals. Notably, in patients experiencing acute cellular graft rejection, there was a marked increase in Enterobacteriaceae levels and a reduction in microbiome diversity, in contrast to those who did not face rejection. Additionally, a recent study from 2024 explored the potential correlation between alterations in the plasma microbiome and the onset of liver failure following partial hepatectomy [93]. Samples were obtained from 158 participants at three critical time points: preoperatively, during surgery from the portal vein prior to occlusion, and one day post-intervention. The findings indicated that patients who subsequently developed liver failure exhibited a higher bacterial load in the central compartment, along with a more diverse mycobiome prior to the surgical procedure.
The observed changes in the blood microbiome in various liver injuries are summarized in Table 2.
2.5. Changes in Blood Microbiome in Kidney Diseases
A significant body of literature investigates the connection between renal disease and the human microbiome, with the majority of these studies emphasizing the importance of the gut microbiome [94,95,96,97,98,99,100,101,102,103,104]. In contrast to current understanding, Bossola and associates published findings in 2009 indicating that healthy volunteers exhibited no detectable blood microbiota. Conversely, their investigation involving 58 hemodialysis patients revealed the presence of several bacterial species, including E. coli, S. aureus, P. aeruginosa, S. epidermidis, E. faecalis, P. mirabilis, and S. haemolyticus [105].
Liu et al. (2020) conducted a review highlighting the significance of urinary microbiome composition within the pelvic region of individuals suffering from nephrolithiasis [106]. Furthermore, another investigation indicated that similar alterations occur in cases of acute kidney injury [107]. Additionally, various studies have tracked modifications in the urogenital [108] and oral [109,110] microbiomes associated with chronic kidney disease (CKD).
The existing knowledge regarding the connection between the blood microbiome and kidney diseases remains limited. A pioneering investigation in this area was conducted by Simoes-Silva et al. in 2018 [111]. The research team investigated the effects of hemodialysis and peritoneal dialysis on various microbiomes, including those of the skin, oral cavity, intestines, and peritoneum, as well as the blood microbiome, in patients suffering from chronic kidney disease. Subsequently, a pilot study detailing alterations in the blood microbiome among these patients was published the following year [36]. The research involved 20 individuals diagnosed with moderate non-diabetic chronic renal failure and 20 healthy participants. The limited sample size and the variability within the renal impairment cohort were identified as limitations of the study. Nevertheless, the findings revealed a notable reduction in α diversity, indicating a decrease in the richness of bacterial taxa within the chronic kidney disease group when compared to the healthy controls. Furthermore, there was a significant increase in the proportion of Proteobacteria, specifically the class Gammaproteobacteria, in the renal impairment group relative to the control group. Additionally, patients with CKD exhibited greater diversity within the Enterobacteriaceae and Pseudomonadaceae families, which was found to correlate with a diminished glomerular filtration rate.
The analysis conducted by Wehedy et al. (2022) explores the significance of dysbiosis within the intestinal, urinary, and blood microbiomes concerning the initiation and advancement of chronic kidney disease [112]. According to the authors, endotoxins produced by intestinal microorganisms, entering the circulation, have the potential to alter the blood microbiome, causing dysbiosis in the central compartment.
A pilot study conducted in 2022 established a connection between alterations in the gut and blood microbiomes of patients with chronic kidney failure who were receiving peritoneal dialysis. The study comprised 44 participants from Portugal, with 11 individuals exhibiting no vascular complications, while the remaining patients had experienced vascular calcification [38]. Variations in the blood microbiome composition have been observed among patients with CKD, particularly distinguishing those with vascular complications from those without. Notably, the taxa Cutibacterium (Class Actinomycetia), Pajaroellobacter, Devosia (Class Alphaproteobacteria), and Hyphomicrobium (Class Alphaproteobacteria) are prevalent in individuals experiencing vascular calcification. In contrast, Pelomonas is more frequently found in patients who do not exhibit this complication. Furthermore, an elevated presence of the Devosia genus is associated with a higher mortality risk among these patients. Recently, a preclinical study involving experimental rats with adenine-induced CKD and vascular calcification investigated alterations in both the gut and blood microbiomes. Additionally, it explored the correlation between the characteristics of CKD-associated microbiota and variations in kidney function [113]. The findings indicate the presence of Acinetobacter in the circulating microbiome a potential risk factor for chronic kidney disease and its associated vascular complications.
IgA nephropathy, also known as Berger's disease, represents the most prevalent type of glomerulonephritis when compared to other variants of this condition [114]. A study conducted in 2021 examined alterations in the blood microbiome among 20 individuals diagnosed with progressive IgA nephropathy, in contrast to a control group of 20 healthy volunteers [115]. In instances of Berger's disease, an elevated presence of the class Coriobacteriia and species from the genera Legionella (Class Gammaproteobacteria), Enhydrobacter (Class Gammaproteobacteria), and Parabacteroides was observed in the bloodstream. A significant limitation of the study is the relatively small sample size. Conversely, a notable strength lies in its consideration of alterations in the intestinal microbiome, leading to the conclusion that the blood microbiome does not exert a direct influence on the intestinal microbiome. This finding stands in contrast to the earlier conclusions drawn by Wehedy et al. (2022) [112], which assert a direct correlation between the compositions of the intestinal and blood microbiomes, thereby highlighting the necessity for additional research into other potential mechanisms that may regulate the blood microbiome.

Table 2.
Microbiome alterations in patients with liver damage.
| Condition | Increased compared to healthy controls | Decreased compared to healthy controls | Reff. |
| Alcohol abuse | Fusobacteria | Bacteroidetes | [89] |
| Cirrhosis | Enterobacteriaceae |
Akkermansia (Phylum: Verrucomicrobiota) Rikenellaceae (Phylum: Bacteroidota) Erysipelotrichales (Phylum: Bacillota) |
[31] |
| Cirrhosis with ascites |
Clostridiales Cyanobacteria |
Moraxellaceae | [29] |
| Decompensated cirrhosis |
Firmicutes Protobacteria Bacteroidetes Verrucomicrobia |
- | [30] |
| Portal hypertension (cirrhosis) |
Comamonas (Class: Betaproteobacteria) Cnuella (Phylum: Bacteroidota) Dialister (Phylum: Bacillota) Escherichia/Shigella (Class: Gammaproteobacteria) Prevotella (Phylum: Bacteroidota) |
Bradyrhizobium (Class: Alphaproteobacteria) Curvibacter (Class: Betaproteobacteria) Diaphorobacter (Class: Betaproteobacteria) Pseudarcicella Pseudomonas (Class: Gammaproteobacteria) |
[90] |
| Portal hypertension (cirrhosis) - severe symptoms |
Bacteroides Escherichia/Shigella Prevotella |
- | [90] |
| Acute pancreatitis |
Bacteroidetes Firmicutes |
Actinobacteria | [116] |
| Graft rejection after liver transplantation | Enterobacteriaceae | - | [92] |
| Patients who develop liver failure after partial hepatectomy | Diversity | [93] |
A recent investigation analyzed the microbiome composition in the oral cavity, intestines, and bloodstream following kidney transplantation [116]. This study involved a limited cohort of six patients, who were evaluated three months post-transplantation. Preliminary findings indicate that the blood of transplant recipients exhibits a diminished diversity of microbiota, primarily consisting of Proteobacteria and Firmicutes.
Currently, research on blood dysbiosis in different kidney disorders remains scarce, and there is a notable absence of data regarding the blood microbiome in cases of acute kidney disease.
2.6. Changes in Blood Microbiome in Metabolite Disorders
It is known that metabolite levels in fecal and serum samples are altered in individuals with metabolic diseases due to intestinal dysbiosis [117]. Disorders such as obesity, diabetes, and celiac disease (CD) are among the most prevalent and challenging health issues for public health. Beyond lifestyle and genetics, the blood microbiome has emerged as a critical factor influencing these conditions that are usually associated with metabolic dysregulation, inflammation, autoimmune response. As mentioned in the previous chapters, alterations in blood microbial composition can disrupt immune function, inflammation, and metabolic pathways, linking them closely to disease development and progression. There is an intricate interplay between the microbiota, nutrition, and host genetic and metabolic composition [118].
As a worldwide epidemic, obesity has been defined by metabolic disorders, energy imbalance, an excessive buildup of fat, and persistent low-grade inflammation [119]. The gut microbiota is thought to be one of the possibly causative human-environment interactions for the significant rise in obesity and related mortality and morbidity over the past few decades. [120]. It is believed that one of the foundations through which the blood microbiome forms is the gut microbiome. Therefore, alteration in the gut microbiota linked to obesity may potentially have an impact on the blood microbiome [121].
In their study, Chakaroun et al. (2021) found a "circulating bacterial signature" that was connected to inflammation and metabolic disorders, indicating that certain bacterial DNA in the blood could be connected to metabolic health. This discovery suggests a possible link between blood microbiota and conditions such as obesity, type 2 diabetes (T2D), and CVD [122]. Most of the current research focuses on the relationship between the gut microbiota and obesity, underscoring the need for more research on the blood microbiota's function in metabolic health.
Asnicar et al. (2021) described relationships between microbiome and host metabolism and dietary habits in 1,098 people with detailed phenotypes [120]. Their study suggests that the blood microbiome is a significant predictor of fasting and postprandial cardiometabolic markers, such as triglycerides and glucose. These findings emphasize the potential of microbiome-based interventions for improving metabolic health. A research project that examined how the blood microbiome of obese patients (n=101) and healthy donors (n=116) was affected by metabolic obesity characteristics, performed metagenomic analysis of the blood microbiome, focusing on sequencing the variable V3-V4 region of the 16S rRNA gene. As a result, it was observed that the blood microbial diversity was higher in patients with metabolically unhealthy obesity (MUHO) than in healthy donors or those with metabolically healthy obesity. Therefore, Bacteroidetes, Firmicutes, Proteobacteria, and Actinobacteria were the dominant phyla found in MUHO. The greater frequency of less common phyla such as Acidobacteria, TM7, and Verrucomicrobia was specifically connected to MUHO, indicating distinctive microbiota changes associated with metabolic health status [121].
In contrast, heightened energy extraction from compounds that would typically be diminished by fecal matter and fat accumulation in individuals with obesity has been associated with elevated concentrations of Firmicutes within the gut microbiome. Research indicates that the rise in Firmicutes is positively correlated with both the storage of fat and the consumption of digestible energy [119]. Similarly, a shift in the gut microbiota favoring Firmicutes, particularly with a high-fat/carb diet, improves energy extraction and causes weight gain, according to Amabebe et al. (2020) [123]. Since this phyla was found abundantly in the blood microbiome of MUHO, it can be stipulated that it may encourage increased fat deposition and calorie absorption, which might lead to obesity.
While the role of gut microbiota in obesity has been extensively studied, there is a paucity of data that explicitly links blood microbial diversity to obesity. The concept of increased microbial diversity, along with the presence of pro-inflammatory taxa such as Proteobacteria, is well documented in research concerning the intestinal microbiome and its association with obesity-related inflammation [124,125]. However, evidence supporting this phenomenon within the blood microbiome remains scarce, despite it being a burgeoning field of investigation.
Diabetes, especially type 2 diabetes, and obesity are closely related due to metabolic and inflammatory processes (especially persistent low-grade inflammation) that are regulated by both the blood and gut microbiomes. Obesity-related excess adipose tissue releases pro-inflammatory cytokines, such as IL-6 and tumor necrosis factor-alpha (TNF-α). A major contributing factor to the development of T2D is insulin resistance, which is caused by these cytokines interfering with insulin signaling pathways. Due to increased intestinal permeability brought on by obesity-associated dysbiosis, pro-inflammatory taxa such as Proteobacteria cause microbial translocation and endotoxemia, which in turn cause systemic inflammation [126,127,128]. Insulin signaling is interfered with by this inflammation, which makes glucose intolerance worse. Obesity and weight increase are significant risk factors for insulin resistance and T2D, and both disorders are exacerbated by chronic inflammation brought on by an excess of lipid buildup. Furthermore, obesity-related changes in microbiota profiles limit the production of healthy short-chain fatty acids (SCFAs), which affects the metabolism of fats and carbohydrates (e.g. increased energy extraction) [129,130,131]. Moreover, one of the most researched and prevalent metabolites of gut microbiota are SCFAs, which typically include butyrate, propionate, and acetate [132].
Qiu et al. (2019), in their case-control study, using pre-diagnostic blood samples taken from T2D patients and controls, directly evaluated the blood microbiome by high-throughput sequencing of the 16S rRNA gene [41]. They then compared the two groups for baseline general blood microbiome composition and relative abundance of particular bacterial taxa. The results show that when compared to non-diabetic controls (non-T2D), the blood microbiome in people with T2D has a greater diversity and distinct microbial patterns. For instance, individuals with the genus Sediminibacterium (which is a member of the phylum Proteobacteria) are more likely to develop T2D. On the other hand, the genus Bacteroides is inversely related to the development of T2D. At the same time, T2D patients have greater abundances of Actinotalea, Alishewanella, Sediminibacterium, and Pseudoclavibacter than non-T2D controls, whereas Aquabacterium, Xanthomonas, and Pseudonocardia had lower abundances. Therefore, it can be suggested that the blood microbiome has the potential to be a diagnostic and prognostic tool, and it may also be an etiology factor for developing T2D [41].
Goraya et al. (2023) observed that blood dysbiosis in T2D patients is typified by a loss of families (Bacillaceae and Bukholderiaceae), a decline in orders (Rhodospirillales and Myxococcales), and genus (Lactobacillus, Acinetobacter, and Lactococcus) in comparison to the healthy population [133]. In a longitudinal investigation conducted by Amar et al. (2011), which included 3,280 participants free from diabetes and obesity at the outset and followed over a period of nine years, the findings indicated that elevated levels of 16S rDNA were associated with the onset of T2D, independent of other risk factors. Notably, the Ralstonia genus emerged as the predominant member of the Proteobacteria phylum in the bloodstream of individuals who subsequently developed diabetes [134]. In another study, Sato et al. (2014) found a high rate of gut bacteria in the blood circulation, pointing out that the translocation of bacteria from the gut to the bloodstream is plausible [50]. They found high 16S bacterial rRNA levels in T2D patients, and Clostridium coccoides and the Atopobidum cluster were especially frequent. Massier et al. (2020) reported that higher levels of Thahibacter are associated with T2D [135].
Previous studies have largely overlooked the potential influence of the blood microbiome in type 1 diabetes (T1D), gestational diabetes, and various other forms of diabetes. The predominant emphasis has been on type 2 diabetes (T2D) [10,133]. In a recent cross-sectional study, Yuan et al. (2024) examined microbial diversity and its potential relevance to the pathophysiological mechanisms underlying T1D [136]. This study compared the blood microbiomes of 64 children recently diagnosed with T1D to those of 77 healthy controls, utilizing 16S rRNA gene amplification and sequencing techniques. The T1D group showed a large rise in the abundance of most phyla, including Firmicutes, Actinobacteriota, and Bacteroidota. Similar to T2D, Proteobacteria was the most abundant phylum in the blood. Sphingomonas, Caulobacter, and Stenotrophomonas were among the potentially harmful species that were significantly more prevalent in the blood microbiome of T1D patients, and these microorganisms could be involved in systemic inflammation. The blood, gut, and oral microbiomes were shown to be similar, which may indicate the transfer of bacteria carried on by T1D patients' impaired oral barrier or increased gut permeability. The authors also emphasized that additional research utilizing transcriptomics, metabolomics, and metagenomics is required to investigate the possible processes underpinning the link between T1D and the blood microbiome [136]. The connection between T1D and the dysregulation of circulating microbiota remains to be fully elucidated and explored.
Celiac disease as an immune-mediated enteropathy is triggered by the ingestion of gluten and the associated prolamins (from wheat, barley, and rye) in genetically predisposed individuals [137,138]. This challenging public-health condition is marked by chronic inflammation and malabsorption, small intestinal villous atrophy and crypt hyperplasia in the small bowel [139]. Microbiome changes in the digestive tract have been linked to several autoimmune conditions, and CD is no exception. This is due to the interaction between the immune system and gut microbiota. In individuals with CD, the gut microbiome undergoes significant alterations, reflecting changes in microbial diversity, composition, and functionality. Patients with CD typically display variations in microbial metabolic processes, a reduction in microbial diversity and an imbalance in the relative abundance of different bacterial taxa. These modifications can lead to immunological dysregulation, inflammation, and compromised intestinal barrier integrity, which are key features in the pathogenesis of the disease [140].
The significance of the gut microbiota in CD has been thoroughly studied; however, there are not many studies that particularly address the blood microbiome in this condition. Valitutti et al. (2019) thoroughly examined the connection between CD and alterations in gut microbiota in their review, highlighting the necessity for further research to fully understand these associations, as no distinct microbiological signature has yet been recognized [141]. Scher (2016) highlights the intricacy of microbial participation in CD in another study, which examines the microbiome's function in this condition beyond diet-genetic connections [142].
Since damaged, inflamed, and hence permeable epithelium is the primary pathway via which commensal microorganisms enter the circulation, it would make sense that specific changes should appear in CD bloodstream. Therefore, when analyzing the adult population with CD, Serena et al. (2019) in their research described patients by alterations in the blood microbiome and how these changes may relate to the intestinal microbiome composition and, ultimately, to the loss of tolerance to gluten [143]. They saw that CD patients showed decreased levels of Clostridiales (Firmicutes phylum) and Bifidobacterium and a higher prevalence of Bacillales (Firmicutes phylum). These modifications align with the alterations in CD-related inflammation and immunological modulation. Moreover, their analysis also revealed that the general microbiome taxonomy of fecal and blood samples differs, with Firmicutes and Bacteroidetes defining the fecal samples and Proteobacteria being abundant in the hematic specimens. Furthermore, the CD blood samples were less phylogenetically diverse compared with controls, with lower alpha diversity. On the other hand, the CD pediatric population was the main subject for Mehrotra et al. (2021) in their case control study [144]. Here, Bacteroidetes were the most prevalent phylum, closely followed by Firmicutes and Proteobacteria. Taxa including Campylobacterales (namely Campylobacter jejuni, Campylobacter coli, Helicobacteraceae), Odoribacteraceae, and Bacteroides acidifaciens, which have been connected to inflammation and the immune response, were less common in active CD patients. At the same time, it was noted that when compared to controls, those with active CD had higher beta diversity, suggesting notable species compositional changes. Future study is crucial to clarify the blood microbiome possible significance in the etiology and development of CD, given there are currently few investigations on this matter. Future treatments that target these microbial changes may be able to supplement the gluten-free diet and provide more effective disease management techniques.
In the context of metabolic disorders, the blood microbiome represents a significant yet underexplored element. The microbial imbalances identified in the bloodstream, as outlined in Table 3, influence various physiological processes, including immunity, metabolism, and inflammation. Advances in microbiome research and technology have the potential to revolutionize the prevention, diagnosis, and treatment of these disorders, offering hope for improved health outcomes and enhanced quality of life.
3. Discussion
The term “microbiome” can be described as the community of phages, viruses, bacteria, archaea, fungi and protozoa that occupy a specific ecological niche, including their products and extracellular DNA/RNA [145], i.e. the totality of all microorganisms, genes and their products in the surrounding environment. In the course of evolution, many microbial species have successfully adapted to the macroorganism. In this regard, it was reported that human body has 10 times more bacteria than the number of human cells [146].
Blood is a special type of connective tissue, made up of cellular elements and liquid plasma, circulating in a common bloodstream circulatory system. The blood microbiome was until recently unknown and still poorly studied [147]. It is known that microorganisms do not enter the bloodstream directly. Initially, they are found in the intercellular (interstitial) space of the macroorganism, and then through the lymphatic capillaries they pass into the blood. The membrane of the lymphatic capillaries is permeable to large molecules and microorganisms, and the lymph nodes after the afferent vessels have the task of retaining and destroying the entered pathogens. Experiments on rats have shown that when injecting the afferent lymphatic vessel of a lymph node with different concentrations of S. aureus and subsequent analysis of the efferent lymph, up to 90 % clearance of S. aureus with the efferent lymph was found [148].
Although the blood microbiome is still a mystery, its existence has been conclusively proven over the past 50 years. The assumption of the presence of normal microflora in the blood was made in the last century [149,150,151]. Bulgarian scientists have made an outstanding contribution in this field. In 1993, the Bulgarian scientist Emil Kalfin, who at that time headed the microbiology laboratory of the “Pulmonary Diseases” Hospital at the Scientific Institute of Pulmonary Diseases at the Medical Academy in Sofia, expressed the opinion and experimentally proved that normal microflora exists in the blood of healthy people [3]. He initially examined the blood of a patient with sarcoidosis. Subsequently, he found that the liquid cultures of healthy control subjects were also positive. Kalfin suggested that the blood microbiome, which he called “normal blood flora”, could be activated by stress factors and be cultured.
Bacteremia has been demonstrated by culture after tooth brushing or oral douching [152,153]. It is assumed that the presence of transient microorganisms in the bloodstream is well tolerated by healthy individuals. The main source of microorganisms in the blood is the intestinal and oral microflora through the route of atopobiosis, i.e. the translocation of microbial cells into the blood or other tissues [154]. Numerous studies have provided evidence of multiplying microorganisms in the blood of clinically healthy individuals [3,18,45,155,156,157] or have demonstrated circulating microbial DNA or RNA [5,158,159].
A significantly larger number of studies discuss results from analysis of blood samples from patients with various diseases. In this review, we summarized data from studies of the human blood microbiome in disorders of the nervous system, cardiovascular, respiratory, liver, kidney diseases, and metabolite disorders. Links between blood microbiome and the above mentioned diseases were demonstrated. Hence, human blood microbiome could be considered as potentiаl biomarker in certain disorders. In support of this understanding, it is evident that analogous alterations in microbiome composition occur across various disease categories; however, the microbial signatures associated with the blood microbiome exhibit specificity. For instance, elevated levels of Proteobacteria have been identified in cardiovascular, renal, and metabolic disorders. Conversely, while Firmicutes are found to be abundant in renal and metabolic conditions, their levels are diminished in cardiovascular diseases. Additionally, patients suffering from respiratory and liver ailments typically show a heightened presence of Bacteroidetes; notably, Flavobacterium is prevalent in respiratory diseases, whereas Enterobacteriaceae is associated with liver diseases.
It could be assumed that in the next few years, research teams would focus on accumulating new knowledge about the blood microbiome and its relationship to numerous diseases with a suspected infectious etiology, such as some forms of arthritis, sarcoidosis, blood anemia, etc., which are still insufficiently investigated.
Author Contributions
Conceptualization, S.D., S.P. and R.K.; literature overview and literature resources, S.P., S.D., and R.K.; methodology, L.T. and S.M; writing—original draft preparation, S.D., D.S. and R.K; writing—review and editing, S.D. and R.K.; project administration, R.K.; funding acquisition, S.P. and R.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Grant KΠ-06-H73/5-05.12.2023 from the National Science
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TNF-α | Tumor necrosis factor-alpha |
| IL-6 | Interleukin-6 |
| OTUs | Operational taxonomic units |
| OCD | Obsessive–compulsive disorder |
| CVD | Cardiovascular diseases |
| COPD | Chronic obstructive pulmonary disease |
| CD | Celiac disease |
| T1D | Type 1 diabetes |
| T2D | Type 2 diabetes |
| MUHO | Metabolically unhealthy obesity |
| SCFAs | Short-chain fatty acids |
| CKD | Chronic kidney disease |
References
- Berg, R.D. Bacterial translocation from the gastrointestinal tract. Adv Exp Med Biol 1999, 473, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Fardini, Y.; Wang, X.; Témoin, S.; Nithianantham, S.; Lee, D.; Shoham, M.; Han, Y.W. Fusobacterium nucleatum adhesin FadA binds vascular endothelial cadherin and alters endothelial integrity. Mol Microbiol 2011, 82, 1468–1480. [Google Scholar] [CrossRef] [PubMed]
- Kalfin, E. Resident microbial flora in human erythrocytes. J Cult Collect 1998, 2, 77–82. [Google Scholar]
- Nikkari, S.; McLaughlin, I.J.; Bi, W.; Dodge, D.E.; Relman, D.A. Does blood of healthy subjects contain bacterial ribosomal DNA? J Clin Microbiol 2001, 39, 1956–1959. [Google Scholar] [CrossRef]
- McLaughlin, R.W.; Vali, H.; Lau, P.C.; Palfree, R.G.; De Ciccio, A.; Sirois, M.; Ahmad, D.; Villemur, R.; Desrosiers, M.; Chan, E.C. Are there naturally occurring pleomorphic bacteria in the blood of healthy humans? J Clin Microbiol 2002, 40, 4771–4775. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.S. Pleomorphic microbes in health and disease: proceedings of the first annual symposium. Montreal, Quebec, Canada; 1999.
- Jensen, G.S. Pleomorphic microbes in health and disease: proceedings of the second annual symposium. Montreal, Quebec, Canada; 2000.
- Castillo, D.J.; Rifkin, R.F.; Cowan, D.A.; Potgieter, M. The healthy human blood microbiome: fact or fiction? Front Cell Infect Microbiol 2019, 9, 148. [Google Scholar] [CrossRef]
- Lucchinetti, E.; Lou, P.H.; Lemal, P.; Bestmann, L.; Hersberger, M.; Rogler, G.; Zaugg, M. Gut microbiome and circulating bacterial DNA (“blood microbiome”) in a mouse model of total parenteral nutrition: Evidence of two distinct separate microbiotic compartments. Clin Nutr ESPEN 2022, 49, 278–288. [Google Scholar] [CrossRef]
- Velmurugan, G.; Dinakaran, V.; Rajendhran, J.; Swaminathan, K. Blood Microbiota and Circulating Microbial Metabolites in Diabetes and Cardiovascular Disease. Trends Endocrinol Metab 2020, 31, 835–847. [Google Scholar] [CrossRef]
- Sciarra, F.; Franceschini, E.; Campolo, F.; Venneri, M.A. The diagnostic potential of the human blood microbiome: are we dreaming or awake? Int J Mol Sci 2023, 24, 10422. [Google Scholar] [CrossRef]
- Gouello, A.; Henry, L.; Chadli, D.; Salipante, F.; Gibert, J.; Boutet-Dubois, A.; Lavigne, J.P. Evaluation of the Microbiome Identification of Forensically Relevant Biological Fluids: A Pilot Study. Diagnostics 2024, 14, 187. [Google Scholar] [CrossRef]
- Lee, E.J.; Sung, J.; Kim, H.L.; Kim, H.N. Whole-genome sequencing reveals age-specific changes in the human blood microbiota. J Pers Med 2022, 12, 939. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Paul, S.; Dutta, C. Geography, Ethnicity or Subsistence-Specific Variations in Human Microbiome Composition and Diversity. Front Microbiol 2017, 8, 1162. [Google Scholar] [CrossRef]
- Fan, K.D.; Ogunrinde, E.; Wan, Z.; Li, C.; Jiang, W. Racial Disparities in Plasma Cytokine and Microbiome Profiles. Microorganisms 2024, 12, 1453. [Google Scholar] [CrossRef]
- You, Y.A.; Yoo, J.Y.; Kwon, E.J.; Kim, Y.J. Blood microbial communities during pregnancy are associated with preterm birth. Front Microbiol 2019, 10, 1122. [Google Scholar] [CrossRef]
- Morrow, J.D.; Castaldi, P.J.; Chase, R.P.; Yun, J.H.; Lee, S.; Liu, Y.Y.; Hersh, C.P. Peripheral blood microbial signatures in current and former smokers. Sci Rep 2021, 11, 19875. [Google Scholar] [CrossRef] [PubMed]
- Panaiotov, S.; Filevski, G.; Equestre, M.; Nikolova, E.; Kalfin, R. Cultural Isolation and Characteristics of the Blood Microbiome of Healthy Individuals. Adv Microbiol 2018, 406–421. [Google Scholar] [CrossRef]
- Panaiotov, S.; Hodzhev, Y.; Tsafarova, B.; Tolchkov, V.; Kalfin, R. Culturable and Non-Culturable Blood Microbiota of Healthy Individuals. Microorganisms 2021, 9, 1464. [Google Scholar] [CrossRef]
- Tsafarova, B.; Hodzhev, Y.; Yordanov, G.; Tolchkov, V.; Kalfin, R.; Panaiotov, S. Morphology of blood microbiota in healthy individuals assessed by light and electron microscopy. Front Cell Infect Microbiol 2023, 12, 1091341. [Google Scholar] [CrossRef]
- Pease, P. Discussion: microorganisms associated with malignancy. Ann N Y Acad Sci 1970, 174, 782–785. [Google Scholar] [CrossRef]
- Narunsky-Haziza, et al. Pan-cancer analyses reveal cancer-type-specific fungal ecologies and bacteriome interactions. Cell 2022, 185, 3789–3806. [Google Scholar] [CrossRef]
- Nejman, D.; Livyatan, I.; Fuks, G.; Gavert, N.; Zwang, Y.; Geller, L.T.; Rotter-Maskowitz, A.; Weiser, R.; Mallel, G.; Gigi, E.; Meltser, A.; Douglas, G.M.; Kamer, I.; Gopalakrishnan, V.; Dadosh, T.; Levin-Zaidman, S.; Avnet, S.; Atlan, T.; Cooper, Z.A.; Arora, R.; Cogdill, A.P.; Khan, M.A.W.; Ologun, G.; Bussi, Y.; Weinberger, A.; Lotan-Pompan, M.; Golani, O.; Perry, G.; Rokah, M.; Bahar-Shany, K.; Rozeman, E.A.; Blank, C.U.; Ronai, A.; Shaoul, R.; Amit, A.; Dorfman, T.; Kremer, R.; Cohen, Z.R.; Harnof, S.; Siegal, T.; Yehuda-Shnaidman, E.; Gal-Yam, E.N.; Shapira, H.; Baldini, N.; Langille, M.G.I.; Ben-Nun, A.; Kaufman, B.; Nissan, A.; Golan, T.; Dadiani, M.; Levanon, K.; Bar, J.; Yust-Katz, S.; Barshack, I.; Peeper, D.S.; Raz, D.J.; Segal, E.; Wargo, J.A.; Sandbank, J.; Shental, N.; Straussman, R. The human tumor microbiome is composed of tumor type-specific intracellular bacteria. Sci. 2020, 368, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Hodzhev, Y. Analysis of blood microbiome dysbiosis in pulmonary sarcoidosis by decision tree model. Biotechnol Biotechnol Equip 2023, 37. [Google Scholar] [CrossRef]
- Hodzhev, Y.; Tsafarova, B.; Tolchkov, V.; Youroukova, V.; Ivanova, S.; Kostadinov, D.; Yanev, N.; Zhelyazkova, M.; Tsonev, S.; Kalfin, R.; Panaiotov, S. Visualization of the individual blood microbiome to study the etiology of sarcoidosis. Comput Struct Biotechnol J 2023, 22, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Della Fera, A.N.; Warburton, A.; Coursey, T.L.; Khurana, S.; McBride, A.A. Persistent Human Papillomavirus Infection. Viruses 2021, 13, 321. [Google Scholar] [CrossRef]
- Lin, W.H.; Kouyos, R.D.; Adams, R.J.; Grenfell, B.T.; Griffin, D.E. Prolonged persistence of measles virus RNA is characteristic of primary infection dynamics. Proc Natl Acad Sci USA 2012, 109, 14989–14994. [Google Scholar] [CrossRef]
- Mangul, S.; Olde Loohuis, L.; Ori, A.P.; Jospin, G.; Koslicki, D.; Yang, H.T.; Ophoff, R.A. Total RNA Sequencing reveals microbial communities in human blood and disease specific effects. bioRxiv 2016, 057570. [Google Scholar] [CrossRef]
- Lelouvier, B.; Servant, F.; Païssé, S.; Brunet, A.C.; Benyahya, S.; Serino, M.; Valle, C.; Ortiz, M.R.; Puig, J.; Courtney, M. , et al. Changes in blood microbiota profiles associated with liver fibrosis in obese patients: A pilot analysis. Hepatology 2016, 64, 2015–2027. [Google Scholar] [CrossRef]
- Traykova, D.; Schneider, B.; Chojkier, M.; Buck, M. Blood Microbiome Quantity and the Hyperdynamic Circulation in Decompensated Cirrhotic Patients. PLoS ONE 2017, 12, e0169310. [Google Scholar] [CrossRef]
- Kajihara, M.; Koido, S.; Kanai, T.; Ito, Z.; Matsumoto, Y.; Takakura, K.; Saruta, M.; Kato, K.; Odamaki, T.; Xiao, J.Z. , et al. Characterisation of blood microbiota in patients with liver cirrhosis. Eur J Gastroenterol Hepatol 2019, 31, 1577–1583. [Google Scholar] [CrossRef]
- Schierwagen, R.; Alvarez-Silva, C.; Madsen, M.S.; Kolbe, C.C.; Meyer, C.; Thomas, D.; Uschner, F.E.; Magdaleno, F.; Jansen, C.; Pohlmann, A., Praktiknjo; Hischebeth, G.T.; Molitor, E.; Latz, E.; Lelouvier, B.; Trebicka, J.; Arumugam, M. Circulating microbiome in blood of different circulatory compartments. Gut 2019, 68, 578–580. [Google Scholar] [CrossRef]
- Amar, J.; Lange, C.; Payros, G.; Garret, C.; Chabo, C.; Lantieri, O.; Courtney, M.; Marre, M.; Charles, M.A.; Balkau, B. , et al. Blood microbiota dysbiosis is associated with the onset of cardiovascular events in a large general population: The D.E.S.I.R. study. PLoS ONE 2013, 8, e54461. [Google Scholar] [CrossRef] [PubMed]
- Dinakaran, V.; Rathinavel, A.; Pushpanathan, M.; Sivakumar, R.; Gunasekaran, P.; Rajendhran, J. Elevated levels of circulating DNA in cardiovascular disease patients: Metagenomic profiling of microbiome in the circulation. PLoS ONE 2014, 9, e105221. [Google Scholar] [CrossRef]
- Lawrence, G.; Midtervoll, I.; Samuelsen, S.O.; Kristoffersen, A.K.; Enersen, M.; Håheim, L.L. The blood microbiome and its association to cardiovascular disease mortality: Case-cohort study. BMC Cardiovasc Disord 2022, 22, 344. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.B.; Allegretti, A.S.; Nigwekar, S.U.; Kalim, S.; Zhao, S.; Lelouvier, B.; Servant, F.; Serena, G.; Thadhani, R.I.; Raj, D.S. , et al. Blood Microbiome Profile in CKD: A Pilot Study. Clin J Am Soc Nephrol 2019, 14, 692–701. [Google Scholar] [CrossRef]
- Mair, R.D.; Sirich, T.L. Blood Microbiome in CKD: Should We Care? Clin J Am Soc Nephrol 2019, 14, 648–649. [Google Scholar] [CrossRef] [PubMed]
- Merino-Ribas, A.; Araujo, R.; Pereira, L.; Campos, J.; Barreiros, L.; Segundo, M.A.; Silva, N.; Costa, C.; Quelhas-Santos, J.; Trindade, F. , et al. Vascular Calcification and the Gut and Blood Microbiome in Chronic Kidney Disease Patients on Peritoneal Dialysis: A Pilot Study. Biomolecules 2022, 12, 867. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, Q.; Zhao, L.; Bin, Y.; Wang, L.; Wang, L.; Zhang, K.; Li, Q. Blood Bacterial 16S rRNA Gene Alterations in Women With Polycystic Ovary Syndrome. Front Endocrinol 2022, 13, 814520. [Google Scholar] [CrossRef]
- Cheng, H.S.; Tan, S.P.; Wong, D.M.K.; Koo, W.L.Y.; Wong, S.H.; Tan, N.S. The blood microbiome and health: current evidence, controversies, and challenges. Int J Mol Sci 2023, 24, 5633. [Google Scholar] [CrossRef]
- Qiu, J.; Zhou, H.; Jing, Y.; Dong, C. Association between blood microbiome and type 2 diabetes mellitus: A nested case-control study. J Clin Lab Anal 2019, 33, e22842. [Google Scholar] [CrossRef]
- Poore, G.D.; Kopylova, E.; Zhu, Q.; Carpenter, C.; Fraraccio, S.; Wandro, S.; Kosciolek, T.; Janssen, S.; Metcalf, J.; Song, S.J. , et al. Microbiome analyses of blood and tissues suggest cancer diagnostic approach. Nature 2020, 579, 567–574. [Google Scholar] [CrossRef]
- Yang, D.; Wang, X.; Zhou, X.; Zhao, J.; Yang, H.; Wang, S.; Morse, M.A.; Wu, J.; Yuan, Y.; Li, S. , et al. Blood microbiota diversity determines response of advanced colorectal cancer to chemotherapy combined with adoptive T cell immunotherapy. Oncoimmunology 2021, 10, 1976953. [Google Scholar] [CrossRef] [PubMed]
- Goraya, M.U.; Li, R.; Mannan, A.; Gu, L.; Deng, H.; Wang, G. Human circulating bacteria and dysbiosis in non-infectious diseases. Front Cell Infect Microbiol 2022, 12, 932702. [Google Scholar] [CrossRef] [PubMed]
- Markova, N.D. Eubiotic vs. dysbiotic human blood microbiota: the phenomenon of cell wall deficiency and disease-trigger potential of bacterial and fungal L-forms. Discov Med 2020, 29, 17–26. [Google Scholar] [CrossRef]
- Magrone, T.; Jirillo, E. The impact of bacterial lipopolysaccharides on the endothelial system: pathological consequences and therapeutic countermeasures. Endocr Metab Immune Disord Drug Targets 2011, 11, 310–325. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.S.; Benson, K.F. The blood as a diagnostic tool in chronic illness with obscure microbial involvement: A critical review. Int J Complement Alt Med 2019, 12, 203–212. [Google Scholar] [CrossRef]
- Luo, Z.; Alekseyenko, A.V.; Ogunrinde, E.; Li, M.; Li, Q.Z.; Huang, L.; Jiang, W. Rigorous plasma microbiome analysis method enables disease association discovery in clinic. Front Microbiol 2021, 11, 613268. [Google Scholar] [CrossRef]
- Walsh, P. ImmunoAdept – bringing blood microbiome profiling to the clinical practice. 2018 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Madrid, Spain, 2018, 1577-1581. [CrossRef]
- Sato, J.; Kanazawa, A.; Ikeda, F.; Yoshihara, T.; Goto, H.; Abe, H.; Watada, H. Gut dysbiosis and detection of “live gut bacteria” in blood of Japanese patients with type 2 diabetes. Diabetes Care 2014, 37, 2343–2350. [Google Scholar] [CrossRef]
- Suparan, K.; Sriwichaiin, S.; Chattipakorn, N.; Chattipakorn, S.C. Human blood bacteriome: Eubiotic and dysbiotic states in health and diseases. Cells 2022, 11, 2015. [Google Scholar] [CrossRef]
- Li, X.; He, W.; Wen, Y.; Jiang, W.; Huang, L. The Role of Blood Microbiome and Microbial Product Translocation in Disease Pathogenesis. Adv Case Stud 2020, 2, 5. [Google Scholar] [CrossRef]
- Demirci, M.; Saribas, A.S.; Siadat, S.D.; Kocazeybek, B.S. Blood microbiota in health and disease. Front Cell Infect Microbiol 2023, 13, 1187247. [Google Scholar] [CrossRef]
- Cuesta, C.M.; Guerri, C.; Ureña, J.; Pascual, M. Role of microbiota-derived extracellular vesicles in gut-brain communication. Int. J. Mol. Sci. 2021, 22, 4235. [Google Scholar] [CrossRef] [PubMed]
- Dominy, S.S.; Lynch, C.; Ermini, F.; Benedyk, M.; Marczyk, A.; et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci. Adv. 2019, 5. [Google Scholar] [CrossRef]
- Rhee, S.J.; Kim, H.; Lee, Y.; Lee, H.J.; Park, C.H.K.; Yang, J.; Kim, Y.K.; Kim, S.; Ahn, Y.M. Comparison of serum microbiome composition in bipolar and major depressive disorders. J. Psychiatr. Res. 2020, 123, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.J.; Kim, H.; Lee, Y.; Lee, H.J.; Park, C.H.K.; Yang, J.; Kim, Y.-K.; Ahn, Y.M. The association between serum microbial DNA composition and symptoms of depression and anxiety in mood disorders. Sci. Rep. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Baffert, C.; Kpebe, A.; Avilan, L.; Brugna, M. Hydrogenases and H2 metabolism in sulfate-reducing bacteria of the Desulfovibrio genus. Adv. Microb. Physiol. 2019, 74, 143–189. [Google Scholar] [CrossRef]
- de Baumont, A.; Bortoluzzi, A.; de Aguiar, B.W.; Scotton, E.; Guimarães, L.S.P.; Kapczinski, F.; Cristiano da Silva, T.B.; Manfro, G.G. Anxiety disorders in childhood are associated with youth IL-6 levels: A mediation study including metabolic stress and childhood traumatic events. J. Psychiatr. Res. 2019, 115, 43–50. [Google Scholar] [CrossRef]
- Ciocan, D.; Cassard, A.M.; Becquemont, L.; Verstuyft, C.; Voican, C.S.; El Asmar, K.; Colle, R.; David, D.; Trabado, S.; Feve, B.; Chanson, P.; Perlemuter, G.; Corruble, E. Blood microbiota and metabolomic signature of major depression before and after antidepressant treatment: A prospective case–control study. J. Psychiatry Neurosci. 2021, 46, E358–E368. [Google Scholar] [CrossRef]
- Taylor, B.C.; Sheikh Andalibi, M.; Wandro, S.; Weldon, K.C.; Sepich-Poore, G.D.; Carpenter, C.S.; Fraraccio, S.; Franklin, D.; Ludicello, J.E.; Letendre, S.; Gianella, S.; Grant, I.; Ellis, R.J.; Heaton, R.K.; Knight, R.; Swafford, A.D. Signatures of HIV and major depressive disorder in the plasma microbiome. Microorganisms 2023, 11. [Google Scholar] [CrossRef]
- Olde Loohuis, L.M.; Mangul, S.; Ori, A.P.; Jospin, G.; Koslicki, D.; Yang, H.T.; Wu, T.; Boks, M.P.; Lomen-Hoerth, C.; Wiedau-Pazos, M.; Cantor, R.M.; de Vos, W.M.; Kahn, R.S.; Eskin, E.; Ophoff, R.A. Transcriptome analysis in whole blood reveals increased microbial diversity in schizophrenia. Transl. Psychiatry 2018, 8. [Google Scholar] [CrossRef]
- Kang, J.I.; Seo, J.H.; Park, C.I.; Kim, S.T.; Kim, Y.K.; Jang, J.K.; Kwon, C.O.; Jeon, S.; Kim, H.W.; Kim, S.J. Microbiome analysis of circulating bacterial extracellular vesicles in obsessive-compulsive disorder. Psychiatry Clin. Neurosci. 2023, 77, 646–652. [Google Scholar] [CrossRef]
- Sadekov, T.S.; Boyko, A.N.; Omarova, M.A.; Rogovskii, V.S.; Zhilenkova, O.G.; Zatevalov, A.M.; Mironov, A.Y. Evaluation of the structure of the human microbiome in multiple sclerosis by the concentrations of microbial markers in the blood. Klin. Lab. Diagn. 2022, 67, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, X.; Wang, Z.; Yu, B. Gut microbiota dysbiosis in human hypertension: A systematic review of observational studies. Front. Cardiovasc. Med. 2021, 8, 650227. [Google Scholar] [CrossRef] [PubMed]
- Rajendhran, J.; Shankar, M.; Dinakaran, V.; Rathinavel, A.; Gunasekaran, P. Contrasting circulating microbiome in cardiovascular disease patients and healthy individuals. Int. J. Cardiol. 2013, 168, 5118–5120. [Google Scholar] [CrossRef] [PubMed]
- Koren, O.; Spor, A.; Felin, J.; Fåk, F.; Stombaugh, J.; Tremaroli, V.; Behre, C.J.; Knight, R.; Fagerberg, B.; Ley, R.E.; Bäckhed, F. Human oral, gut, and plaque microbiota in patients with atherosclerosis. Proc. Natl. Acad. Sci. USA 2011, 108, 4592–4598. [Google Scholar] [CrossRef]
- Sharifullina, D.M.; Pozdeev, O.K.; Khayrullin, R.N. Blood microbiome of patients with atherosclerosis. ATERO-SCLEROZ 2023, 57. [Google Scholar] [CrossRef]
- Velmurugan, G.; Ramprasath, T.; Mithieux, G. Human microbiota: A key player in the etiology and pathophysiology of cardiovascular and metabolic diseases. Front. Cardiovasc. Med. 2022, 9, 1081722. [Google Scholar] [CrossRef]
- Jing, Y.; Zhou, H.; Lu, H.; Chen, X.; Zhou, L.; Zhang, J.; Wu, J.; Dong, C. Associations between peripheral blood microbiome and the risk of hypertension. Am. J. Hypertens. 2021, 34, 1064–1070. [Google Scholar] [CrossRef]
- Khan, I.; Khan, I.; Usman, M.; Jianye, Z.; Wei, Z.X.; Ping, X. .; Lizhe, A. Analysis of the blood bacterial composition of patients with acute coronary syndrome and chronic coronary syndrome. Front. Cell. Infect. Microbiol. 12, 943808. [CrossRef]
- Khan, I.; Khan, I.; Kakakhel, M.A.; Xiaowei, Z.; Ting, M.; Ali, I. .; Lizhe, A. Comparison of microbial populations in the blood of patients with myocardial infarction and healthy individuals. Front. Microbiol. 13, 845038. [CrossRef]
- Chen, R.; Ye, Y.; Ding, Y.; Wan, Z.; Ye, X.; Liu, J. Potential biomarkers of acute myocardial infarction based on the composition of the blood microbiome. Clin. Chim. Acta 2024, 556, 117843. [Google Scholar] [CrossRef]
- Desbois, A.C.; Ciocan, D.; Saadoun, D.; Perlemuter, G.; Cacoub, P. Specific microbiome profile in Takayasu’s arteritis and giant cell arteritis. Sci. Rep. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, R.; Barve, K. Gut microbiome: a promising target for management of respiratory diseases. Biochem. J. 2020, 477, 2679–96. [Google Scholar] [CrossRef] [PubMed]
- Chunxi, L.; Haiyue, L.; Yanxia, L.; Jianbing, P.; Jin, S. The gut microbiota and respiratory diseases: new evidence. J. Immunol. Res. 2020, 2020. [Google Scholar] [CrossRef]
- Liu, Y.; Teo, S.M.; Méric, G.; Tang, H.H.; Zhu, Q.; Sanders, J.G.; Vázquez-Baeza, Y.; Verspoor, K.; Vartiainen, V.A.; Jousilahti, P.; Lahti, L. The gut microbiome is a significant risk factor for future chronic lung disease. J. Allergy Clin. Immunol. 2023, 151, 943–52. [Google Scholar] [CrossRef]
- Özçam, M.; Lynch, S.V. The gut–airway microbiome axis in health and respiratory diseases. Nat. Rev. Microbiol. 2024, 22, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Budden, K.F.; Shukla, S.D.; Rehman, S.F.; Bowerman, K.L.; Keely, S.; Hugenholtz, P.; Armstrong-James, D.P.; Adcock, I.M.; Chotirmall, S.H.; Chung, K.F.; Hansbro, P.M. Functional effects of the microbiota in chronic respiratory disease. Lancet Respir. Med. 2019, 7, 907–20. [Google Scholar] [CrossRef]
- Santacroce, L.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Luperto, P.; De Nitto, E.; Topi, S. The human respiratory system and its microbiome at a glimpse. Biology 2020, 9. [Google Scholar] [CrossRef]
- Belizário, J.; Garay-Malpartida, M.; Faintuch, J. Lung microbiome and origins of respiratory diseases. Curr. Res. Immunol. 2023, 4, 100065. [Google Scholar] [CrossRef]
- Li, R.; Li, J.; Zhou, X. Lung microbiome: new insights into the pathogenesis of respiratory diseases. Signal Transduct. Target. Ther. 2024, 9. [Google Scholar] [CrossRef]
- Morrow, J.D.; Castaldi, P.J.; Chase, R.P.; Yun, J.H.; Lee, S.; Liu, Y.Y. . & COPDGene Investigators. Peripheral blood microbial signatures in COPD. bioRxiv 2020, 2020–05. [Google Scholar] [CrossRef]
- Lee, J.H.; Choi, J.P.; Yang, J.; Won, H.K.; Park, C.S.; Song, W.J. . & Cho, Y.S. Metagenome analysis using serum extracellular vesicles identified distinct microbiota in asthmatics. Sci. Rep. 2020, 10. [Google Scholar] [CrossRef]
- Barbeta, E.; López-Aladid, R.; Bueno-Freire, L.; Llonch, B.; Palomeque, A.; Motos, A.; Mellado-Artigas, R.; Zattera, L.; Ferrando, C.; Soler, A.; Fernández-Barat, L.; Torres, A. Biological effects of pulmonary, blood, and gut microbiome alterations in patients with acute respiratory distress syndrome. ERJ Open Res. 2024. [Google Scholar] [CrossRef] [PubMed]
- Santiago, A.; Pozuelo, M.; Poca, M.; Gely, C.; Nieto, J. C.; Torras, X.; Guarner, C. Alteration of the serum microbiome composition in cirrhotic patients with ascites. Sci. Rep. 2016, 6, 25001. [Google Scholar] [CrossRef] [PubMed]
- Brochado-Kith, O.; Rava, M.; Berenguer, J.; González-García, J.; Rojo, D.; Díez, C.; Hontañon, V.; Virseda-Berdices, A.; Ibañez-Samaniego, L.; Llop-Herrera, E.; Olveira, A.; Pérez-Latorre, L.; Barbas, C.; Fernández-Rodríguez, A.; Resino, S.; Jiménez-Sousa, M. A. Altered blood microbiome in patients with HCV-related Child-Pugh class B cirrhosis. J. Infect. Public Health 2024, 17, 102524. [Google Scholar] [CrossRef]
- Li, Q.; Wang, C.; Tang, C.; Zhao, X.; He, Q.; Li, J. Identification and characterization of blood and neutrophil-associated microbiomes in patients with severe acute pancreatitis using next-generation sequencing. Front. Cell. Infect. Microbiol. 2018, 8, 5. [Google Scholar] [CrossRef]
- Puri, P.; Liangpunsakul, S.; Christensen, J. E.; Shah, V. H.; Kamath, P. S.; Gores, G. J.; TREAT Consortium. The circulating microbiome signature and inferred functional metagenomics in alcoholic hepatitis. Hepatology 2018, 67, 1284–1302. [Google Scholar] [CrossRef]
- Gedgaudas, R.; Bajaj, J. S.; Skieceviciene, J.; Varkalaite, G.; Jurkeviciute, G.; Gelman, S.; Kupcinskas, J. Circulating microbiome in patients with portal hypertension. Gut Microbes 2022, 14, 2029674. [Google Scholar] [CrossRef]
- Vasudevan, D.; Ramakrishnan, A.; Velmurugan, G. Exploring the diversity of blood microbiome during liver diseases: Unveiling novel diagnostic and therapeutic avenues. Heliyon 2023, 9. [Google Scholar] [CrossRef]
- Okumura, T.; Horiba, K.; Kamei, H.; Takeuchi, S.; Suzuki, T.; Torii, Y.; Ito, Y. Temporal dynamics of the plasma microbiome in recipients at early post-liver transplantation: A retrospective study. BMC Microbiol. 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Santol, J.; Whittle, E.; Brunnthaler, L.; Laferl, V.; Kern, A.; Ortmayr, G.; Starlinger, P. The blood microbiome and its impact on hepatic failure after liver surgery. HPB 2024, 26, S604. [Google Scholar] [CrossRef]
- Ramezani, A.; Raj, D. S. The gut microbiome, kidney disease, and targeted interventions. J. Am. Soc. Nephrol. 2014, 25, 657–670. [Google Scholar] [CrossRef] [PubMed]
- Sampaio-Maia, B.; Simões-Silva, L.; Pestana, M.; Araujo, R.; Soares-Silva, I. J. The role of the gut microbiome on chronic kidney disease. Adv. Appl. Microbiol. 2016, 96, 65–94. [Google Scholar] [CrossRef]
- Al Khodor, S.; Shatat, I. F. Gut microbiome and kidney disease: A bidirectional relationship. Pediatr. Nephrol. 2017, 32, 921–931. [Google Scholar] [CrossRef] [PubMed]
- Nallu, A.; Sharma, S.; Ramezani, A.; Muralidharan, J.; Raj, D. Gut microbiome in chronic kidney disease: Challenges and opportunities. Transl. Res. 2017, 179, 24–37. [Google Scholar] [CrossRef]
- Armani, R. G.; Ramezani, A.; Yasir, A.; Sharama, S.; Canziani, M. E.; Raj, D. S. Gut microbiome in chronic kidney disease. Curr. Hypertens. Rep. 2017, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hobby, G. P.; Karaduta, O.; Dusio, G. F.; Singh, M.; Zybailov, B. L.; Arthur, J. M. Chronic kidney disease and the gut microbiome. Am. J. Physiol. Renal Physiol. 2019, 316, F1211–F1217. [Google Scholar] [CrossRef]
- Chen, Y. Y.; Chen, D. Q.; Chen, L.; Liu, J. R.; Vaziri, N. D.; Guo, Y.; Zhao, Y. Y. Microbiome–metabolome reveals the contribution of gut–kidney axis on kidney disease. J. Transl. Med. 2019, 17, 1–11. [Google Scholar] [CrossRef]
- Ren, Z.; Fan, Y.; Li, A.; Shen, Q.; Wu, J.; Ren, L.; Lu, H.; Ding, S.; Ren, H.; Liu, C.; Liu, W. Alterations of the human gut microbiome in chronic kidney disease. Adv. Sci. 2020, 7, 2001936. [Google Scholar] [CrossRef]
- Liu, F.; Xu, X.; Chao, L.; Chen, K.; Shao, A.; Sun, D.; Hong, Y.; Hu, R.; Jiang, P.; Zhang, N.; Xiao, Y. Alteration of the gut microbiome in chronic kidney disease patients and its association with serum free immunoglobulin light chains. Front. Immunol. 2021, 12, 609700. [Google Scholar] [CrossRef]
- Sato, N.; Kakuta, M.; Hasegawa, T.; Yamaguchi, R.; Uchino, E.; Murashita, K.; Nakaji, S.; Imoto, S.; Yanagita, M.; Okuno, Y. Metagenomic profiling of gut microbiome in early chronic kidney disease. Nephrol. Dial. Transplant. 2021, 36, 1675–1684. [Google Scholar] [CrossRef]
- Tourountzis, T.; Lioulios, G.; Fylaktou, A.; Moysidou, E.; Papagianni, A.; Stangou, M. Microbiome in chronic kidney disease. Life 2022, 12, 1513. [Google Scholar] [CrossRef] [PubMed]
- Bossola, M.; Sanguinetti, M.; Scribano, D.; Zuppi, C.; Giungi, S.; Luciani, G.; Torelli, R.; Posteraro, B.; Fadda, G.; Tazza, L. Circulating bacterial-derived DNA fragments and markers of inflammation in chronic hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Zhang, N.; Wu, Y.; Jiang, P.; Jiang, T.; Wang, Y.; Zhang, Y.; Zhai, Q.; Zou, Y.; Feng, N. The pelvis urinary microbiome in patients with kidney stones and clinical associations. BMC Microbiol. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Gerges-Knafl, D.; Pichler, P.; Zimprich, A.; Hotzy, C.; Barousch, W.; Lang, R. M.; Lobmeyr, E.; Baumgartner-Parzer, S.; Wagner, L.; Winnicki, W. The urinary microbiome shows different bacterial genera in renal transplant recipients and non-transplant patients at time of acute kidney injury: A pilot study. BMC Nephrol. 2020, 21, 1–10. [Google Scholar] [CrossRef]
- Araujo, R.; Merino-Ribas, A.; Pereira, L.; Campos, J.; Silva, N.; Alencastre, I. S.; Pestana, M.; Sampaio-Maia, B. The urogenital microbiome in chronic kidney disease patients on peritoneal dialysis. Nefrologia 2024, 44, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Sheng, J.; Hu, L.; Zhang, B.; Guo, W.; Wang, Y.; Gu, Y.; Jiang, P.; Lin, H.; Lydia, B.; Sun, Y. Salivary microbiome in chronic kidney disease: What is its connection to diabetes, hypertension, and immunity? J. Transl. Med. 2022, 20, 387. [Google Scholar] [CrossRef]
- Guo, S.; Wu, G.; Liu, W.; Fan, Y.; Song, W.; Wu, J.; Gao, D.; Gu, X.; Jing, S.; Shen, Q.; Ren, L. Characteristics of human oral microbiome and its non-invasive diagnostic value in chronic kidney disease. Biosci. Rep. 2022, 42, BSR20210694. [Google Scholar] [CrossRef]
- Simoes-Silva, L.; Araujo, R.; Pestana, M.; Soares-Silva, I.; Sampaio-Maia, B. The microbiome in chronic kidney disease patients undergoing hemodialysis and peritoneal dialysis. Pharmacol. Res. 2018, 130, 143–151. [Google Scholar] [CrossRef]
- Wehedy, E.; Shatat, I. F.; Al Khodor, S. The human microbiome in chronic kidney disease: A double-edged sword. Front. Med. 2022, 8, 790783. [Google Scholar] [CrossRef]
- Sun, M.; Fang, Y.; Zheng, J.; Shi, G.; Guo, J.; Zhang, X.; Zhang, R. Role of symbiotic microbiota dysbiosis in the progression of chronic kidney disease accompanied with vascular calcification. Front. Pharmacol. 2024, 14, 1306125. [Google Scholar] [CrossRef]
- Kiryluk, K.; Li, Y.; Sanna-Cherchi, S.; Rohanizadegan, M.; Suzuki, H.; et al. Geographic differences in genetic susceptibility to IgA nephropathy: GWAS replication study and geospatial risk analysis. PLOS Genet. 2012, 8, e1002765. [Google Scholar] [CrossRef] [PubMed]
- Shah, N. B.; Nigwekar, S. U.; Kalim, S.; Lelouvier, B.; Servant, F.; Dalal, M.; Krinsky, S.; Fasano, A.; Tolkoff-Rubin, N.; Allegretti, A. S. The gut and blood microbiome in IgA nephropathy and healthy controls. Kidney360 2021, 2, 1261–1274. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, S.; Araujo, R.; Merino-Riba, A.; Lelouvier, B.; Servant, F.; Quelhas-Santos, J.; Pestana, M.; Sampaio-Maia, B. Blood, gut, and oral microbiome in kidney transplant recipients. Indian J. Nephrol. 2023, 33, 366–370. [Google Scholar] [CrossRef]
- Proffitt, C.; Bidkhori, G.; Moyes, D.; Shoaie, S. Disease, drugs and dysbiosis: Understanding microbial signatures in metabolic disease and medical interventions. Microorganisms 2020, 8, 1381. [Google Scholar] [CrossRef]
- Zietek, T.; Rath, E. Inflammation meets metabolic disease: gut feeling mediated by GLP-1. Front. Immunol. 2016, 7, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Zhang, L.; Yang, L.; Chu, H. The critical role of gut microbiota in obesity. Front. Endocrinol. (Lausanne) 2022, 13, 1025706. [Google Scholar] [CrossRef]
- Asnicar, F.; Berry, S.E.; Valdes, A.M.; Nguyen, L.H.; Drew, D.A.; Leeming, E.; Gibson, R.; Roy, C. Le; Khatib, A.; Francis, L.; et al. Microbiome Connections with Host Metabolism and Habitual Diet from 1,098 Deeply Phenotyped Individuals. Nat. Med. 2021, 27, 321–332. [Google Scholar] [CrossRef]
- Shestopalov, A. V.; Kolesnikova, I.M.; Gaponov, A.M.; Grigoryeva, T. V.; Khusnutdinova, D.R.; Kamaldinova, D. R. Rumyantsev, S.A. Effect of Metabolic Type of Obesity on Blood Microbiome. Probl. Biol. Med. Pharm. Chem. 2022, 25, 35–41. [Google Scholar] [CrossRef]
- Chakaroun, R.M.; Massier, L.; Heintz-buschart, A.; Said, N.; Fallmann, J.; Crane, A.; Schütz, T.; Dietrich, A.; Blüher, M.; Stumvoll, M.; et al. Circulating Bacterial Signature Is Linked to Metabolic Disease and Shifts with Metabolic Alleviation after Bariatric Surgery. Genome Med. 2021, 13. [Google Scholar] [CrossRef]
- Amabebe, E.; Robert, F.O.; Agbalalah, T.; Orubu, E.S.F. Microbial Dysbiosis-Induced Obesity: Role of Gut Microbiota in Homoeostasis of Energy Metabolism. Br. J. Nutr. 2020, 123, 1127–1137. [Google Scholar] [CrossRef]
- Shantaram, D.; Hoyd, R.; Blaszczak, A.M.; Antwi, L.; Jalilvand, A.; Wright, V.P.; Liu, J.; Smith, A.J.; Bradley, D.; Lafuse, W.; et al. Obesity-Associated Microbiomes Instigate Visceral Adipose Tissue in Fl Ammation by Recruitment of Distinct Neutrophils. Nat. Commun. 2024, 15, 5434. [Google Scholar] [CrossRef]
- Xu, Z.; Jiang, W.; Huang, W.; Lin, Y.; Chan, F.K.L.; Ng, S.C. Gut Microbiota in Patients with Obesity and Metabolic Disorders — a Systematic Review. Genes Nutr. 2022, 17. [Google Scholar] [CrossRef] [PubMed]
- Shoelson, S.E.; Herrero, L.; Naaz, A. Obesity, Inflammation, and Insulin Resistance. Gastroenterology 2007, 132, 2169–2180. [Google Scholar] [CrossRef] [PubMed]
- Sumida, K.; Han, Z.; Chiu, C.-Y.; Mims, T.S.; Bajwa, A.; Demmer, R.T.; Datta, S.; Kovesdy, C.P.; Pierre, J.F. Circulating Microbiota in Cardiometabolic Disease. Front. Cell. Infect. Microbiol. 2022, 12, 892232. [Google Scholar] [CrossRef] [PubMed]
- Kolesnikova, I.M.; Gaponov, A.M.; Roumiantsev, S.A.; Karbyshev, M.S.; Grigoryeva, T. V.; Makarov, V. V.; Yudin, S.M.; Borisenko, O. V.; Shestopalov, A. V. Relationship between Blood Microbiome and Neurotrophin Levels in Different Metabolic Types of Obesity. J. Evol. Biochem. Physiol. 2022, 58, 1937–1949. [Google Scholar] [CrossRef]
- Ghaemi, F.; Fateh, A.; Sepahy, A.A.; Zangeneh, M.; Ghanei, M.; Siadat, S.D. Blood Microbiota Composition in Iranian Pre-Diabetic and Type 2 Diabetic Patients. Hum. Antibodies 2021, 29, 243–248. [Google Scholar] [CrossRef]
- Murugesan, S.; Nirmalkar, K.; Hoyo-Vadillo, C.; García-Espitia, M.; Ramírez-Sánchez, D.; García-Mena, J. Gut Microbiome Production of Short-Chain Fatty Acids and Obesity in Children. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 621–625. [Google Scholar] [CrossRef]
- Scheithauer, T.P.M.; Rampanelli, E.; Nieuwdorp, M.; Vallance, B.A.; Verchere, C.B.; van Raalte, D.H.; Herrema, H. Gut Microbiota as a Trigger for Metabolic Inflammation in Obesity and Type 2 Diabetes. Front. Immunol. 2020, 11, 1–29. [Google Scholar] [CrossRef]
- Lin, K.; Zhu, L.; Yang, L. Gut and Obesity/Metabolic Disease: Focus on Microbiota Metabolites. MedComm 2022, 3, e171. [Google Scholar] [CrossRef]
- Goraya, M. U.; Li, R.; Gu, L.; Deng, H.; Wang, G. Blood Stream Microbiota Dysbiosis Establishing New Research Standards in Cardio-Metabolic Diseases, A Meta-Analysis Study. Microorganisms 2023, 11, 777. [Google Scholar] [CrossRef]
- Amar, J.; Serino, M.; Lange, C.; Chabo, C.; Iacovoni, J.; Mondot, S.; Lepage, P.; Klopp, C.; Mariette, J.; Bouchez, O.; et al. Involvement of Tissue Bacteria in the Onset of Diabetes in Humans: Evidence for a Concept. Diabetologia 2011, 54, 3055–3061. [Google Scholar] [CrossRef] [PubMed]
- Massier, L.; Chakaroun, R.; Tabei, S.; Crane, A.; Didt, K.D.; Fallmann, J.; Von Bergen, M.; Haange, S.B.; Heyne, H.; Stumvoll, M.; et al. Adipose Tissue Derived Bacteria Are Associated with Inflammation in Obesity and Type 2 Diabetes. Gut 2020, 69, 1796–1806. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Yang, X.; Xu, Z.; Li, J.; Sun, C.; Chen, R. ,... & Luo, F. The Profile of Blood Microbiome in New-Onset Type 1 Diabetes Children. ISCIENCE 2024, 27, 110252. [Google Scholar] [CrossRef]
- Jansson-Knodell, C.L.; Rubio-Tapia, A. Gluten-Related Disorders From Bench to Bedside. Clin. Gastroenterol. Hepatol. 2024, 22, 693–704.e1. [Google Scholar] [CrossRef]
- Saviano, A.; Petruzziello, C.; Brigida, M.; Morabito Loprete, M.R.; Savioli, G.; Migneco, A.; Ojetti, V. Gut Microbiota Alteration and Its Modulation with Probiotics in Celiac Disease. Biomedicines 2023, 11, 1–12. [Google Scholar] [CrossRef]
- DeGeorge, K.C.; Frye, J.W.; Stein, K.M.; Rollins, L.K.; McCarter, D.F. Celiac Disease and Gluten Sensitivity. Prim. Care - Clin. Off. Pract. 2017, 44, 693–707. [Google Scholar] [CrossRef] [PubMed]
- Stanciu, D.; Staykov, H.; Dragomanova, S.; Tancheva, L.; Pop, R.S.; Ielciu, I.; Crisan, G. Gluten Unraveled: Latest Insights on Terminology, Diagnosis, Pathophysiology, Dietary Strategies, and Intestinal Microbiota Modulations—A Decade in Review. Nutrients 2024, 16, 3636. [Google Scholar] [CrossRef]
- Valitutti, F.; Cucchiara, S.; Fasano, A. Celiac Disease and the Microbiome. Nutrients 2019, 11, 1–19. [Google Scholar] [CrossRef]
- Scher, J.U. The Microbiome in Celiac Disease: Beyond Diet-Genetic Interactions. Cleve. Clin. J. Med. 2016, 83, 228–230. [Google Scholar] [CrossRef]
- Serena, G.; Davies, C.; Cetinbas, M.; Sadreyev, R.I.; Fasano, A. Analysis of Blood and Fecal Microbiome Profile in Patients with Celiac Disease. Hum. Microbiome J. 2019, 11, 100049. [Google Scholar] [CrossRef]
- Mehrotra, I.; Serena, G.; Cetinbas, M.; Kenyon, V.; Martin, V.M.; Harshman, S.G.; Zomorrodi, A.R.; Sadreyev, R.I.; Fasano, A.; Leonard, M.M. Characterization of the Blood Microbiota in Children with Celiac Disease. Curr. Res. Microb. Sci. 2021, 2, 100069. [Google Scholar] [CrossRef] [PubMed]
- Berg, G.; Rybakova, D.; Fischer, D.; et al. Microbiome definition re-visited: old concepts and new challenges. Microbiome 2020, 8, 103. [Google Scholar] [CrossRef]
- Sender, R.; Fuchs, S.; Milo, R. Revised estimates for the number of human and bacteria cells in the body. PLoS Biology 2016, 14, e1002533. [Google Scholar] [CrossRef] [PubMed]
- Païssé, S.; Valle, C.; Servant, F.; Courtney, M.; Burcelin, R.; Amar, J.; Lelouvier, B. Comprehensive description of blood microbiome from healthy donors assessed by 16S targeted meta- genomic sequencing. Transfusion 2016, 56, 1138–1147. [Google Scholar] [CrossRef]
- Clement, C.; Wang, W.; Dzieciatkowska, M.; Cortese, M.; Hansen, K.C.; Becerra, A.; Thangaswamy, S.; Nizamutdinova, I.; Moon, J.-Y.; Stern, L.J.; Gashev, A.A.; Zawieja, D.; Santambrogio, L. Quantitative Profiling of the Lymph Node Clearance Capacity. Sci Rep 2018, 8, 11253. [Google Scholar] [CrossRef]
- Rife, R.R. Filterable bodies seen with the Rife microscope. Science 1931, 74, 10–10. [Google Scholar] [CrossRef]
- Wuerthele-Caspe, V. The presence of consistently recurring invasive mycobacterial forms in tumor cells. NY Microsc Soc Bull 1948, 2, 5–18. [Google Scholar]
- Carpenter, C.M.; Nelson, E.L.; Lehman, E.L.; Howard, D.H.; Primes, G. The isolation of unidentified pleomorphic bacteria from the blood of patients with chronic illness. J Chronic Dis 1955, 2, 151–161. [Google Scholar] [CrossRef]
- Berger, S.A.; Weitzman, S.; Edberg, S.C.; Casey, J.I. Bacteremia after the use of an oral irrigation device. A controlled study in subjects with normalappearing gingiva: comparison with use of toothbrush. Ann Intern Med 1974, 80, 510–511. [Google Scholar] [CrossRef]
- Maharaj, B.; Coovadia, Y.; Vayej, A.C. An investigation of the frequency of bacteraemia following dental extraction, tooth brushing and chewing. Cardiovasc J Afr 2012, 23, 340–344. [Google Scholar] [CrossRef]
- Potgieter, M.; Bester, J.; Kell, D.B.; Pretorius, E. The dormant blood microbiome in chronic, inflammatory diseases. FEMS Microbiol Rev 2015, 39, 567-591. https://academic.oup.com/femsre/article/39/4/567/2467761.
- Domingue, G.J.; Woody, H.B. Bacterial persistence and expression of disease. Clin Microbiol Rev 1997, 10, 320–334. [Google Scholar] [CrossRef] [PubMed]
- Damgaard, C.; Magnussen, K.; Enevold, C.; Nilsson, M.; Tolker-Nielsen, T.; Holmstrup, P.; Nielsen, C.H. Viable bacteria associated with red blood cells and plasma in freshly drawn blood donations. PloSone. 2015, 10, e0120826. [Google Scholar] [CrossRef] [PubMed]
- Markova, N.; Slavchev, G.; Michailova, L. Presence of mycobacterial L-forms in blood: challenge of BCG vaccination. Hum Vaccin Immunother 2015, 11, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Gosiewski, T.; Ludwig-Galezowska, A.H.; Huminska, K.; Sroka-Oleksiak, A.; Radkowski, P.; Salamon, D.; Wojciechowicz, J.; Kus-Slowinska, M.; Bulanda, M.; Wolkow, P.P. Comprehensive detection and identification of bacterial DNA in the blood of patients with sepsis and healthy volunteers using next-generation sequencing method - the observation of DNAemia. Eur J Clin Microbiol Infect Dis 2017, 36, 329–336. [Google Scholar] [CrossRef]
- Whittle, E.; Leonard, M.O.; Harrison, R.; Gant, T.W.; Tonge, D.P. Multi-Method Characterization of the Human Circulating Microbiome. Front Microbiol 2019, 9, 3266. [Google Scholar] [CrossRef]
Figure 1.
Examples of pathological conditions linked to blood microbiome dysbiosis.
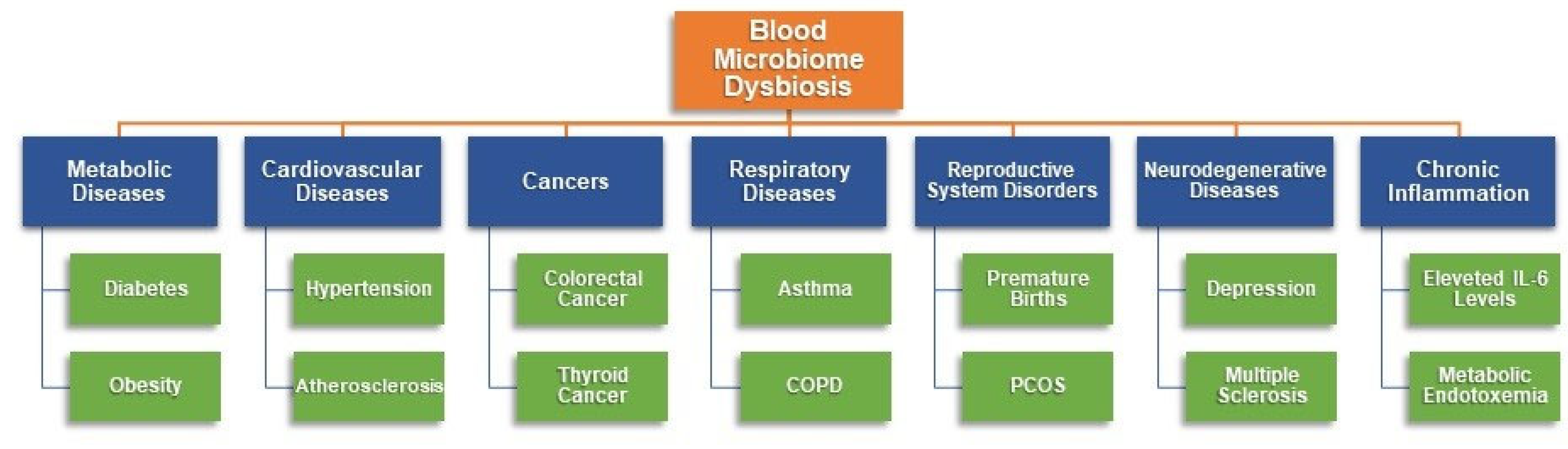
Figure 2.
The Process of Blood Microbiome Analysis.
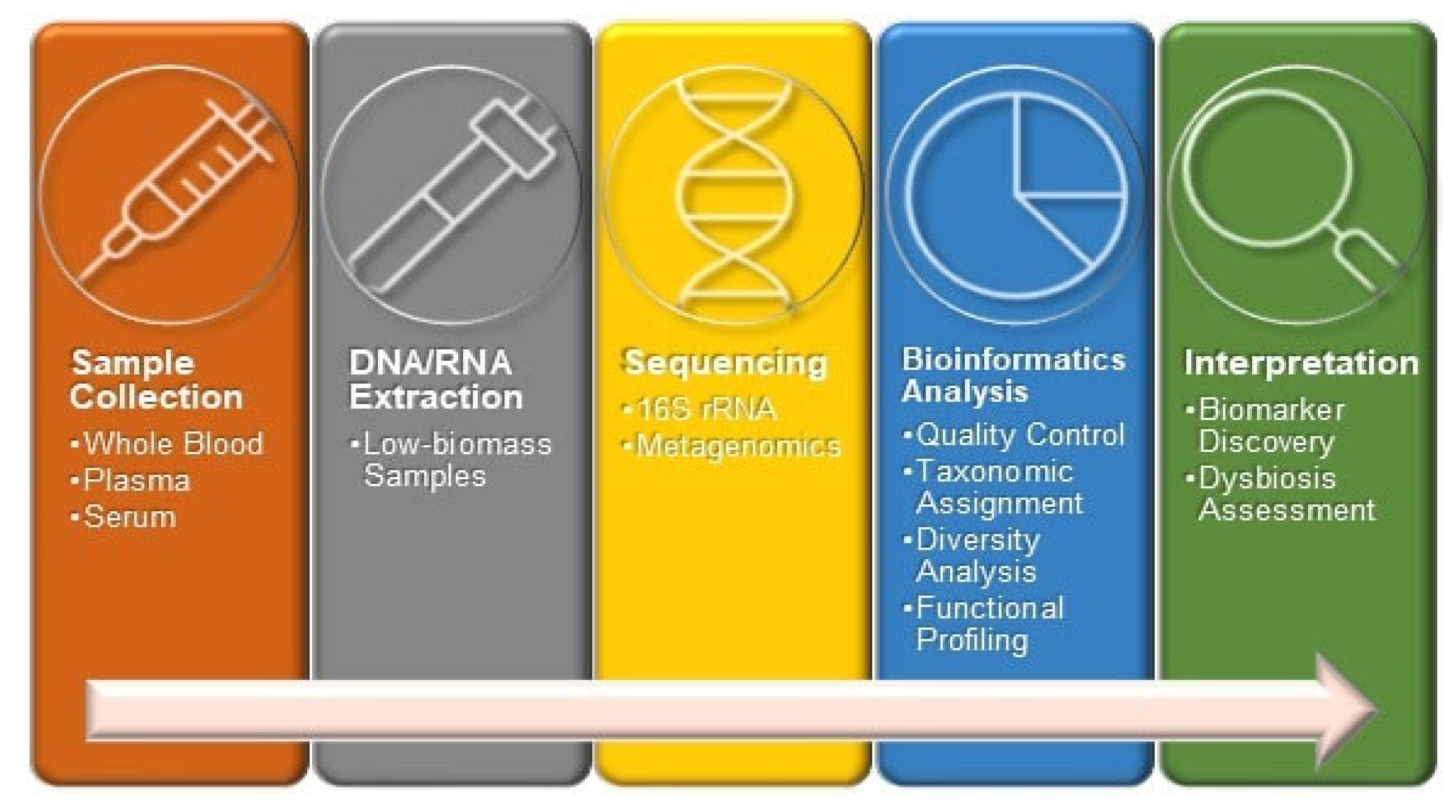
Table 1.
Microbiome alterations in CVD patients.
| Condition | Increased compared to healthy controls | Decreased compared to healthy controls | Reff. |
| Individuals to develop CVD | Proteobacteria | - | [33] |
| CVD | Proteobacteria (F. Pseudomonaceae, Cl. Gammaproteobacteria) | Firmicutes (F. Staphylococcaceae) | [66] |
|
Actinobacteria Bacteriophages |
- | [34] | |
| Hypertension | Proteobacteria | Firmicutes; Bacteroidetes | [70] |
| Acute coronary syndrome |
Proteobacteria Bacteroidota |
- | [71] |
| Chronic coronary syndrome |
Bacteroidota Firmicutes |
Proteobacteria | [71] |
| Myocardial infarction | Actinobacteria | - | [72] |
| Vasculitis (Takayasu's arteritis) |
Clostridia Cytophagia Deltaproteobacteria |
Bacilli | [74] |
| Vasculitis (giant cell arteritis) |
Cytophagaceae Rhodococcus |
[74] | |
| CVD mortality |
Enhydrobacter Kocuria |
Paracoccus | [35] |
Table 3.
Microbiome alterations in metabolic disorders.
| Condition | Increased compared to healthy controls | Decreased compared to healthy controls | Reff. |
| Obesity |
Actinobacteria Acidobacteria Bacteroidetes Firmicutes Proteobacteria Saccharibacteria (TM7) Verrucomicrobia |
- | [121] |
| Type 1 Diabetes |
Actinobacteriota Bacteroidota Firmicutes Proteobacteria (Sphingomonas, Caulobacter, Stenotrophomonas) |
- | [136] |
| Type 2 Dyabetes |
Proteobacteria (Sediminibacterium, Ralstonia, Alishewanella, Thahibacter) Actinobacteriota (Actinotalea, Pseudoclavibacter, Atopobidum cl.) Firmicutes (Clostridium coccoides) |
Bacteroidota (Bacteroides) Proteobacteria (Aquabacterium, Xanthomonas, Bukholderiaceae, Rhodospirillales, Myxococcales, Acinetobacter) Firmicutes (Bacillaceae, Lactobacillus, Lactococcus) Actinobacteriota (Pseudonocardia) |
[41] [133] [134] [50] [135] |
| Celiac Disease |
Firmicutes (Bacillales), Proteobacteria Bacteroidota (Bacteroides) |
Firmicutes (Clostridiales) Actinobacteriota (Bifidobacterium) Proteobacteria (Campylobacterales: Campylobacter jejuni, Campylobacter coli, Helicobacteraceae) Bacteroidota (Odoribacteraceae, Bacteroides acidifaciens) |
[143] [144] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



