
Submitted:
15 April 2025
Posted:
16 April 2025
You are already at the latest version
Abstract
The etiology of blurry vision often remains elusive. In this retrospective study, we assessed objective test findings of 145 patients reporting blurry vision at an outpatient neck clinic in 2022. Patients with previously identified causes were excluded. Viable patients underwent digital motion x-ray (videofluoroscopy) and upright cone beam CT scan of the cervical spine, pupillometry, tonometry, and ultrasound of the carotid sheath and eye. Abnormal ocular test results (bilateral totals) include elevated optic nerve sheath diameter (ONSD >12.2 mm) in 142 (98%), excessive percent light constriction (>60%) in 138 (95%), and increased pupil diameters (>8 mm) in 134 (92%). Abnormal cervical structural findings include forward head posture (C6-atlas interval >10 mm) in 145 (100%), vagus nerve degeneration (< 4.2 mm total) in 138 (95%), decreased internal jugular vein cross-sectional area (IJV CSA) at C1 (total < 180 mm) in 143 (99%), decreased depth of curve (< 7 mm) in 128 (89%), and ligamentous cervical instability (LCI) at C1-C2 (total >4 mm) in 124 (88%). Pupil diameter correlated with intraocular pressure (IOP, r=0.26, p=0.002), and LCI C1-C2 correlated with ONSD (r=0.18, p=0.039). These data indicate that some cases of blurry vision may result from ocular pathology due to LCI and loss of lordosis, causing IJV compression and vagus nerve degeneration.
Keywords:
blurry vision
; jugular vein
; vagus nerve
; visual symptoms
; pupil diameter
; intraocular pressure
; pupillary response
; optic nerve sheath diameter
; cerebrospinal fluid
; ligamentous cervical instability
1. Introduction
Blurry vision is a decrease in visual sharpness or clarity that may appear in one or both eyes. While blurry vision is a common visual symptom associated with conditions with known ocular pathology such as cataracts, macular degeneration, glaucoma, refractive errors, and ocular hypertension, its etiology is less clear with other associated neurological conditions, including dysautonomia, intracranial hypertension, and computer vision syndrome, as well as musculoskeletal conditions such as neck pain, cervical spondylosis (degeneration), headaches, and text neck [1,2,3,4,5]. Blurry vision is becoming a more prevalent complaint in clinical practice, as 90% of people who spend at least 3 hours a day using a computer have computer vision syndrome, with 30-60% experiencing blurry vision as their primary complaint [6,7,8]. A significant association is found between hours of use (screen time) in not only vision-related problems, but also neck disability [9,10]. It is clear that digital devices are significantly contributing to vision-related problems, including text neck syndrome, which is associated with not only visual changes, but also headaches and neck and shoulder pain, although the specific processes leading to these symptoms are yet to be defined [11]. While there are many hypotheses as to what may be causing the blurry vision and other visual symptoms due to electronic device use, such as blue light, glare, quality of the screen, and ergonomics, a clear consensus has not yet been established [12,13,14].
We hypothesize that these computer vision and text neck syndromes involving blurry vision can be further explained by the effects of the modern facedown/forward head lifestyle, which is comprised of looking down at screens for many hours a day and putting excessive forces on the cervical spine. The head is naturally positioned on the most mobile segments of the spine (C1-C2) to allow for optimal function and range of motion, but we are not meant to be looking down or leaning forward for a majority of the day. When looking down, the neck muscles relax, and the vertebrae spread apart while the posterior cervical ligaments stretch. A flexed neck looking down at a cell phone (40-45°) endures triple the force from the weight of the head, averaging 10 kg greater force than in an upright position, and is a known risk factor for neck pain and symptoms [15,16,17]. Extended time in this facedown/forward head posture potentially leads to injury of the posterior ligament complex, contributing to ligamentous cervical instability, a degenerative condition of the ligamentous integrity of the cervical spine which can progress to a breakdown of the normal cervical lordotic curve (cervical dysstructure), with net effects of a forward-shifted atlas in the sagittal plane, causing stretch and compression of carotid sheath, including the internal jugular veins and vagus nerves [16,17,18,19]. (See Figure 1.)
Here we relate clinical characteristics and objective cervical structural and ocular test findings in 145 consecutive patients reporting blurry vision at our outpatient neck center. The significant cervical structural pathologies found included ligamentous cervical instability, especially at the atlantoaxial C1-C2 facet joint, increased C6-atlas interval (C6AI, measurement of forward head), and decreased depth of cervical curve alongside elevated ONSD, excessive pupillary response, and increased pupil diameter. Compression of the carotid sheath was found to occur at the atlas (C1), causing internal jugular vein compression and vagus nerve degeneration, which we believe form the basis for the ocular pathology seen. (See Figure 2.) Significant ocular findings include pupillary dilation, increased pupillary constriction to light, and increased fluid around the optic nerve; the mechanisms by which these symptoms occur and account for the patients’ blurry vision are discussed.
2. Materials and Methods
2.1. Study Population
The population included 145 consecutive patients reporting blurry vision, aged 20-50 years, presenting to an outpatient neck center for care from January 1-June 30, 2022. The retrospective study was approved by the WCG Institutional Review Board (Study #1364545). The inclusion criteria included reporting blurry vision upon initial intake with no previously identified obvious cause. We excluded patients with a known diagnosis of ocular disease issues that necessitated current usage of eye medication or surgery, or a known preceding traumatic event (motor vehicle accident, sporting incident, injury, or surgery). Patients underwent dynamic cervical structural, carotid sheath, and ocular tests, including optic nerve sheath diameter, intraocular pressures, pupillary diameters, and pupillary light constriction.
2.2. Dynamic Cervical Structural Testing
All patients received 2 scans of the cervical spine, performed by a radiology technologist: an upright digital motion x-ray (DMX, videofluoroscopy) and an upright cervical cone beam CT (CBCT) scan. Scanning in the upright position allows for better visualization of how gravity affects the cervical spine and can reveal abnormalities that can be missed during a lying-down position [20]. To evaluate for ligamentous cervical instability, measurements were obtained in the lower cervical spine in flexion and extension, and in the upper cervical spine (C1-C2) in lateral flexion with open mouth views. To evaluate structural forward head and neck posture, C6AI was measured as the horizontal distance between the posterior border of the C6 vertebral body and a line drawn perpendicular from the anterior arch of the atlas in the sagittal view. C6AI objectively identifies forward head and neck posture, as it analyzes the position of the atlas in relation to the lower cervical spine in the sagittal plane. Depth of curve (DOC) was measured as the distance from the posteroinferior aspect of the C4 vertebra to a line drawn from the posteroinferior aspect of the C6 vertebral body to the peak of the dens of C2. DOC is used to objectively identify the state of cervical lordosis. (See Figure 3.)
2.3. Neck Vitals Analysis
A neck vitals analysis was performed on each patient by a medical ultrasonographer, which included cervical and ocular ultrasounds and measurements. Cross-sectional areas of the vagus nerves (mid-neck, approximately C4) and internal jugular veins (supine position at C1 and at C4-C5) were measured using Canon Aplio a550 ultrasound with 7 MHz linear probe, pupil diameter and light reflex were measured using NeurOptics NPi®-200 pupillometer, intraocular pressure was measured using iCare ic200 tonometer, and optic nerve sheath diameter was measured using Canon ultrasound, ocular setting. Measurements are reported and analyzed as bilateral totals. (See Figure 4.)
2.4. Statistical Analysis
Quantitative data were analyzed using RStudio 2024.04.2+764. The data were presented as mean + standard deviation (SD) or percentages (frequencies). A paired t-test was conducted to compare IJV CSA supine at C1 to IJV CSA supine at C4-C5, and a non-parametric Wilcoxon signed-rank test was conducted to verify the findings. A paired t-test was conducted to compare IJV CSA C1 supine to IJV CSA C1 with use of a Denneroll®, an orthotic device which enhances the cervical lordotic curve. Pearson correlation coefficient analysis was used to quantify linear relationships between LCI C1-C2 and ONSD, and between pupil diameter and IOP.
3. Results
3.1. Demographics and Objective Test Results
A total of 145 patients reported blurry vision with no known etiology during their initial intake at an outpatient neck center between January 1, 2022 and June 30, 2022 to be included in this retrospective study. The average age was 37.8 +/- 8.5 years, with 72 (49.7%) female and 73 (50.3%) male. The mean and SD of the dynamic cervical structural tests, as well as the total (bilateral) IJV and vagus nerve CSAs, pupillary diameters, IOPs, ONSDs, and light reflex percentages of the 145 patients with blurry vision are summarized in Table 1.
The percentages of significant abnormal cervical structural and objective eye testing findings are described in Table 2.
3.2. Comparisons and Linear Relationships
To assess whether there is a significant difference between IJV C1 supine and IJV C4-C5 supine, a paired t-test and a Wilcoxon signed-rank test were conducted. Both tests confirmed a statistically significant difference between the 2 variables (p <0.001), the mean difference being -56.84 units with a 95% confidence interval, indicating that on average, IJV C1 supine is significantly lower than IJV C4-C5 supine. A paired t-test was also performed to evaluate the mean difference between IJV CSA C1 supine and IJV CSA C1 while using a cervical orthotic, the Denneroll®. The results revealed a statistically significant difference between IJV C1 supine and IJV with the Denneroll® device (t [119] = -10.719, p <0.001). The mean difference was -37.14 mm, with a 95% confidence interval. These results suggest that, on average, IJV C1 supine is significantly lower than IJV C1 with use of the Denneroll®. (See Figure 5.)
Normal unilateral IJV CSA is >90-100 mm2, easily measured under B-mode ultrasound [22,23,24]. (See Figure 6.) Our study documents that measuring IJV at the level of the atlas (C1) is a more sensitive test when evaluating for IJV compression with ultrasound, compared to the mid-cervical region (C4-C5), which is where IJV CSA is typically measured [25]. Lower IJV C1 supine values are likely due to a forward-shifted atlas causing compression, both from LCI and a breakdown of the cervical curve, which can result in a forward shift of the atlas in 3-D space. In this patient population, the bilateral IJV compression predominantly at C1 (atlas) can likely be attributed to the documented LCI, increased C6AI, and decreased DOC. Restoration of the lordotic cervical curve, as stimulated by the cervical orthotic device the Denneroll®, can lead to improvement of IJV C1 measurements, potentially increasing fluid flow out of the eye and brain.
Pearson correlation analysis was conducted to evaluate whether a positive linear relationship exists between pupil diameter and IOP, as well as LCI at C1-C2 and ONSD. A significant positive relationship was identified between pupil diameter and IOP (r = 0.26, p = 0.002). The findings show that as pupil diameter increases, intraocular pressure increases. (See Figure 7).
The analysis also revealed a weak but significant positive linear relationship between LCI C1-C2 and ONSD (r = 0.18, p = 0.039), indicating that increased LCI C1-C2 was associated with increased ONSD. (See Figure 8.)
These linear relationships provide additional support for our hypothesis that LCI C1-C2 can lead to blurry vision by way of LCI causing IJV compression, interrupting fluid outflow, increasing ONSD, and—by vagus nerve degeneration—triggering ocular dysautonomia such as dilated pupils, a known mechanism that raises intraocular pressure [26,27]. The implications of these correlations and linear relationships found in our patient population are further discussed in Section 3.5 and Section 3.6.
3.3. Analysis of Cervical Sagittal Upright Images
Static cervical structure was evaluated by upright CBCT to assess loss of lordotic cervical curvature. We measured the DOC and C6AI (sagittal x-ray used if C6 vertebra not seen with CBCT). C6AI is the amount of forward displacement of the atlas (C1) compared to the lower cervical vertebra (C6) in the sagittal plane, a measurement that elucidates abnormal cervical structure such as forward head posture [28,29,30]. All 145 (100%) patients had C6AI greater than 10 mm (normal <10 mm) in the sagittal plane, the average being 41.7 mm (1.7 inches). A total of 128 (89%) patients were found to have decreased DOC (<7 mm), with the average cervical lordosis depth being decreased at 2.68 mm. Ideal cervical lordosis depth, evaluated by the Borden method, is between 7-17 mm [31,32].
Forward head posture is the most common cervical postural abnormality in the sagittal plane, but it typically refers to forward placement of the head in relation to the shoulder, when a clinical shift to prioritizing objective cervical radiographic measurements should be considered [33,34]. Forward head posture causes known pathologic changes in both the upper and lower cervical spine, including an increase in upper cervical angle (increased extension) and flexion in the lower cervical spine [35,36]. To better clarify what specifically is going on in the entire cervical region in the sagittal plane, we measured C6AI, which compares the anatomy in the upper cervical (specifically, the atlas) to the lower cervical spine (C6) [37]. In addition to leading to a forward-shifted atlas which may sometimes go unrecognized, forward head posture makes one prone to ligamentous cervical instability [38]. In our patient population, LCI was documented not only in the upper cervical region with lateral flexion in the open mouth view averaging 7.19 mm total, but also with flexion and extension in the lower cervical spine, with average totals of 4.36 mm and 4.27 mm, respectively. Neck pain and muscular tension are often discussed regarding forward head posture, but what may be overlooked is ligament pathology.
3.4. Frequency of Ligamentous Cervical Instability
Many patients, 127 (88%), had ligamentous upper cervical (C1-C2) instability (>4 mm total), with the average being 7.19 mm +/- 2.98 mm. LCI was assessed by DMX (videofluoroscopy), which allows for a detailed and uninterrupted examination of the cervical spine (C0-C7) during various movements and in multiple dimensions, including frontal and sagittal, as well as rotational, planes [39]. LCI is characterized by more than 2 mm of vertebral translation in one direction, examined in various positions, and is defined by the degree of overhang by an adjacent vertebra, but some consider as little as 1 mm to be significant [21,40]. The DMX studies show the functional integrity of the ligaments in the cervical spine with a high degree of accuracy in the upright position, specifically the anterior and posterior longitudinal, supraspinous, interspinous, transverse, alar, facet capsular, and ligamentum flavum ligaments [39]. The capsular ligaments through the cervical spine provide structural support for the 4 major movements of the head and neck: flexion, extension, axial rotation, and lateral flexion [41]. We documented weakened capsular ligaments in the upper cervical spine by the overhang of the inferior articular pillar of the atlas on the superior articular pillar of C2, and in the lower cervical spine the motion is seen in flexion and extension.
The most mobile joint in the cervical spine is the C1-C2 joint, which sits between 2 more stable areas (C0-C1 and C2-C7) and is responsible for a large amount of rotation and flexibility due to the peglike dens structure of C2 around which the arch of C1 rotates. In this study, LCI C1-C2 seen in 127 (88%) patients was identified using DMX. The 2 lateral C1-C2 facet joints are to be differentiated from the atlantodens (median atlantoaxial) joint. Ligamentous atlantoaxial instability primarily involves the transvers ligament and is typically diagnosed using non-motion MRI or CT imaging, with extreme cases warranting surgical intervention [42,43]. (See Figure 9.) Upright and motion scanning allow for structural deviations to be seen during movements and amongst different positions, which can document vertebral translations that could be putting strain on vital structures in the area surrounding the excess motion, such as the IJV and vagus nerve in the area of C1 [44,45].
In this study, 137 (94%) also reported neck pain. While the etiology of chronic neck pain can be multifactorial, it is probable that neck pain in this patient population relates to the chronic neck tension induced by the ligamento-muscular reflex from the upper and lower cervical instability seen, presumably similar to muscle strain felt from the resultant forward head posture and loss of lordosis [46,47]. The ligamento-muscular reflex is a protective mechanism to instill stability in a joint that is unstable to protect not only the joint but adjacent neurovascular structures, in this case the carotid sheath [48,49]. (See Figure 10.) It is the cervical structural changes, LCI, increased C6AI, and decreased DOC that can lead to unfavorable outcomes for the neck (causing pain) and also for the visual system by causing stretch and compression of vital structures such as the IJV and vagus nerves, potentially resulting in blurry vision and other visual disturbances by a variety of potential mechanisms.
3.5. High Prevalence of IJV Compression and Elevated ONSD
IJV compression (total IJV CSA supine <180 mm2) at the level of C1 was documented in 98.6%. Also, in 87%, IJV CSA C1 supine was significantly lower than IJV CSA C4-C5 supine (mean difference -56.84 mm), determined by a paired t-test and a Wilcoxon signed-rank test. The average total IJV C1 supine was 68.94 mm2 compared to 131.79 mm2 at C4-C5 (ideal >180 mm2). IJV measurements are typically taken only mid-neck, at the C4-C5 level, leaving room for error when assessing pathological IJV compression [50]. In the supine position, normal unilateral IJV CSA is >90-100 mm, collapsing to about 25 mm in the upright position due to negative pressure in the thoracic cavity with respiration, to maintain intracranial pressure in the upright position [22,23,24]. IJV CSA C1 while using a cervical orthotic, the Denneroll®, was significantly higher than IJV CSA supine (mean 42.3 mm, t [119]). This finding supports our theory that correcting the cervical curve and restoring cervical structural integrity would lead to increased IJV CSA at C1 supine, relieving compression, improving cerebral drainage, and leading to improved vision.
Consequences of IJV compression include elevated CSF pressure, as well as increased cerebral venous sinus and episcleral venous pressures, potentially causing increased IOP and ICP [51,52,53,54]. Outflow from the orbit of the eyes travels through the episcleral veins into the superior ophthalmic veins, which lead to the cavernous sinus and the petrosal sinus, and exit the head through the IJVs [55,56]. Compression at the IJV will cause upstream effects of built-up pressure, possibly all the way back up to the episcleral veins, hindering the outflow from the eye, which would cause an increase in intraocular pressure. According to the modified Goldman equation, episcleral venous pressure accounts for about 47-60% of IOP in humans [54].
Ocular hypertension, defined as increased IOP >42 mmHg total, was identified in 28 (19%) blurry vision patients. The optic nerve is exposed to IOP from within the eye, and to ICP via CSF within the subarachnoid space. A change in these 2 pressurized zones is known to cause damage to retinal ganglion cell axons, causing diseases such as glaucoma [57].
CSF surrounds the optic nerve through the subarachnoid space, all the way up to the back of the globe, playing a significant role in determining the retrolaminar pressure, as evidenced by Morgan, et al, and cerebral drainage is proven to be hindered by IJV compression [58,59]. If both CSF pressure and IOP are elevated, the eye becomes subject to compressive pressures from the inside and outside, a “double eye squish,” particularly posing a threat to the retina, which is subject to both forces. The result of double pressure on the retina can be detrimental, leading to not only blurry vision but also double vision and focusing issues, and can progress to glaucoma, as well as macular and retinal degeneration. (See Figure 11.)
As 98.6% of patients had compression of the IJV at the atlas, 98.6% likewise had elevation of ONSD (total bilateral >12.2 mm). ONSD is a widely used noninvasive measurement to assess elevated intracranial pressure [60]. Elevation of ONSD is emerging as a reliable indicator of intracranial hypertension (>20 mmHg). While some studies utilize a number as low as 5.0-5.2 mmHg, we chose 6.1 mm as our cut-off of elevated ONSD, which has a high sensitivity and specificity for ICH [61,62,63,64]. We presume that the increase in CSF around the optic nerve head occurs as CSF pressure increases due to cerebral venous outflow obstruction of the IJV as it exits the brain at the level of the atlas. A Pearson correlation coefficient analysis showed a positive relationship between LCI C1-C2 and ONSD (r = 0.18, p = 0.039).
It must be remembered, at any given time, that most of the blood volume in the brain is in the venous system trying to get out [65]. While 32 quarts of fluids flow through the brain each day, 70-80% of them are contained in the brain’s venous system [ibid]. In 94% of healthy people, the IJV is the main venous system through which blood exits the brain, while only 6% of people drain less than one-third of the brain’s fluids through the IJV [66]. As CSF accumulates around the optic nerve, the increase in pressure can cause impaired electric impulse conduction, swelling of the optic nerve (optic neuritis), or even degeneration (optic neuropathy), all of which can lead to blurry vision [67]. (See Figure 12.)
3.6. Vagus Nerve Degeneration and Ocular Dysautonomia
Vagus nerve degeneration (vagus nerve CSA total <4.2 mm) was evident in 138 (95%) patients [68]. The vagus nerve is under the same stretch and compression as the IJV with LCI and CD, as they run together within the carotid sheath and enter/exit the brain via the jugular foramen. These torsion, shear, and traction forces can easily be seen with cervical ultrasound. (See Figure 13.) In addition, 138 (95%) had excessive pupillary light reflex (percent change in pupil diameter >60% total), and 134 (92%) had enlarged pupil diameters (total >8 mm) [69,70,71]. The pupillary light response is commonly used in clinical settings to assess dysautonomia [72,73,74]. Dysautonomia is characterized by dysregulation of the autonomic nervous system (ANS), an imbalance between the sympathetic and parasympathetic nervous systems. As our patient population had both vagus nerve degeneration and excessive pupil dilation, we believe they may be connected through the vagus nerve’s influence on the sympathetic nervous system being a main contributor to parasympathetic balance. The vagus nerve is a sympathetic inhibitor, so if vagus nerve activity is decreased because of degeneration due to LCI, sympathetic dominance or excess sympathetic responses would therefore occur and could have detrimental effects on ocular physiology, including chronic pupillary dilation [75,76,77]. Vagus nerve dysfunction could be the reason why so many patients with text neck and computer vision syndrome have many other symptoms besides visual disturbance and neck pain, including gastrointestinal issues, dizziness, anxiety, tachycardia, and a host of others [78,79].
While the vagus nerve is the main component of the parasympathetic nervous system and makes up about 75-80% of the parasympathetic nerve fibers, many sympathetic ganglia also run alongside the anterior vertebral bodies from the upper neck to the coccyx which can be affected by structural changes in the cervical spine, including instability [80]. The face and head are specifically provided with sympathetic efferent innervation by the superior cervical sympathetic ganglion (SCSG), which sits approximately at the level of the second and third cervical vertebrae (C2 and C3) [81]. The SCSG is the main sympathetic ganglion responsible for innervation to the eye, with neurons projecting to the dilator pupillae muscle of the iris to cause pupillary dilation. The most common symptom of sympathetic dominance is photophobia (light sensitivity) [82]. Light sensitivity comes from dilated pupils allowing more light into the eye, which can cause blurry vision in brightly lit environments.
Both the vagus nerve and the SCSG are not only interconnected with each other, but also with many other structures in the upper cervical region, including the trigeminal, facial, glossopharyngeal, accessory, and hypoglossal nerves (cranial nerves V, VII, IX, XI, and XII), along with the connections to the cervical sympathetic trunks and C1-C3 spinal nerve roots [83,84,85,86]. Decreased vagal tone may cause sympathetic dominance, which can lead to blurry vision by instigating dilated pupils, as seen with photophobia [87]. Pupil dilation is also a known cause of elevated IOP, with ocular hypertension commonly being associated with blurry vision and many ocular diseases [27,88]. Pupil dilation seen in this patient population, then, likely contributes to blurry vision.
While structural neck postures and disorders can impair vagus nerve function, dysfunctional neck issues could also potentially negatively affect the sympathetic ganglia and fibers in the cervical spine, especially the superior cervical sympathetic ganglia, another potential etiology for dysautonomia and chronic symptoms [81,89,90,91]. The anterior locations traversing the neck make both the nodose ganglion of the vagus nerve and the SCSG easily compressed or aggravated by LCI and cervical dysstructure, such as the forward shift of the upper cervical spine seen with increased C6AI, all profoundly documented in our patient population. (See Figure 14.)
4. Discussion
In this retrospective chart review, we analyzed the objective test results and cervical structural findings of 145 patients reporting blurry vision during their initial intake at an outpatient neck center. To our knowledge, this is the first study to analyze objective cervical structural and ocular pathologies in relatively young patients (average age 37.8) with no obvious cause for their blurry vision. Over 87% of the patients were shown to have abnormal cervical structural findings, including ligamentous C1-C2 facet joint instability, ligamentous lower cervical (C2-C7) extension and flexion instability, reduced cervical lordosis (decreased depth of curve), and a forward-shifted atlas (C1) in relation to the lower cervical spine in the sagittal plane (increased C6AI). Ocular objective findings revealed 95% to have increased percent light constriction, 98% to have increased ONSD, and 92% to have dilated pupils. The study population had evidence of vagus nerve degeneration (95%) and narrowing/compression of the IJV at C1 (99%). IJV CSA at C1 (atlas) was found to be statistically significantly (p <0.001) smaller than in the mid-neck. The bilateral IJV CSA at C1 improved by 61% from 68.9 to 111.2 mm2 when measured without the Denneroll® (supine) and then with a Denneroll®, which was also highly statistically significant (p <0.001), signifying on average that IJV CSA at C1 is significantly higher with use of the Denneroll®.
Blurry vision is a possible symptom of almost all ocular diseases, including glaucoma, macular degeneration, dry eye, and retinal detachments, but in this young (age 20-52) patient population, age-related factors are unlikely and patients with previously known disease were excluded. This study involved people in an age group with a high likelihood of their cervical neck structure being affected by many hours and decades of screen time, as the iPhone was introduced in 2007, by 2018 over 95% of adolescents aged 13-16 owned a smartphone, and by 2024 the average American aged 16-34 spent over 7 hours a day on screens [92,93,94]. Now, increased time spent using electronic devices is being associated with visual symptoms and neck pain [95]. This study provides evidence that the cause of some of the visual symptoms that computer and cell phone users experience are coming from their neck. The data could explain why common maladies such as computer vision and text neck syndrome share many eye, visual, and musculoskeletal symptoms with LCI. (See Figure 15.)
Our study documented that the patient population had 3 types of LCI, with the mean amount of total ligamentous lower cervical (C2-C7) instability in flexion being 4.36 mm, in extension 4.27 mm, and in the upper cervical (C1-C2) region in lateral flexion 7.19 mm. Clinical ligamentous cervical instability is an inability of the cervical ligaments to maintain individual, adjacent, or global vertebral alignment, especially at the facet joints, when subjected to increased forces by various postures, positions, and/or motions that alter bony, soft tissue, and/or neurovascular alignment and function such that symptoms result [96,97]. The LCI in the upper and lower cervical spine and resultant breakdown of the patients’ cervical lordotic curves, as documented by the anterior arch of the atlas being an average 41.7 mm in front of the posterior border of C6 in the sagittal plane (C6AI), explains the decreased IJV CSA at the atlas (C1), and the documented vagus nerve degeneration due to stretch compression.
The most significant objective ocular pathology found was the mean bilateral total ONSD of 15.35 mm (normal total <12.2 mm). As the optic nerve acts as the sole pathway for transmitting visual electrical impulses with information from the retina to the optic nerve to the brain so we can see clearly, it is easy to surmise that extra CSF fluid surrounding the optic nerve within the optic nerve sheath might impede or interrupt the proper transmission of visual information, this disruption leading to blurry vision. We found it to be quite significant that only 1 patient in this cohort did not have elevated ONSD in at least one eye. Abnormalities in the optic nerve are a common pathology found in almost all eye conditions, including glaucoma, macular degeneration, hypertension, and eye symptoms such as blurry vision, eye pain, visual field defects, and visual distortions [98,99,100]. The elevation of ONSD in this patient population likely represents intracranial hypertension resulting from IJV compression at the atlas due to ligamentous upper cervical instability. This connection is supported by a Pearson correlation coefficient of r = 0.18, p = 0.039 between ligamentous C1-C2 facet joint instability (LCI C1-C2) and ONSD, showing that as LCI C1-C2 goes up, so does ONSD. Blurry vision and other visual and eye symptoms are common with intracranial hypertension [101,102]. Cerebral and cervical venous outflow disorders are a known cause of increased brain pressure [103,104].
While the gold standard for identifying increased brain pressure remains invasive intracranial devices, ONSD is a preferred method compared to CT and MRI for tracking real-time changes in CSF and intracranial pressures and can be especially helpful as an initial and noninvasive evaluation [105,106,107]. Ultrasound ONSD measurement, utilized in this study, is a valid indicator of increased intracranial pressure, and easily accessible and replicable in an in-office setting for detecting and monitoring intracranial hypertension [108,109,110]. The ONSD should be measured by identifying the hypoechoic linear structure with a hyperechoic border (nerve sheath) that emerges from the posterior part of the globe and should measure 3 mm behind the posterior rim of the globe, including the outer rim. Generally, in healthy adults, ONSD should measure 4.9-5.3 mm [111]. The typical cutoff for diagnosing intracranial hypertension is an ONSD greater than 6 mm, used in emergency rooms and other settings, though some use an even lower cutoff [64,112,113,114,115]. Most recently, a cutoff of 5.7 mm has been revealed to indicate high intracranial pressure [63]. (See Figure 16.)
Furthermore, blurry vision as a result of idiopathic intracranial hypertension is frequently discussed in literature as resulting from CSF accumulating around the optic nerve, but still idiopathic, meaning without a known cause [116]. Nonetheless, blurry vision with intracranial hypertension is known to be associated with elevated CSF pressure, papilledema, increased ONSD measurements, and even visual loss, all of which have been demonstrated to improve immediately following reduction of intracranial pressure, and there is general agreement that abnormal cerebral spinal fluid flow dynamics and increased venous sinus pressure are likely involved [117,118]. Despite CSF removal being a common procedure to reduce intracranial pressure and thereby reduce ONSD, it has not proven to be a long-term solution nor thought to be a particularly useful therapeutic method [119]. Perhaps some cases of intracranial hypertension associated with blurry vision are not actually idiopathic, but rather from cervical structural issues impeding venous fluid outflow from the brain [120]. Additionally, we find it important to consider that blurry vision, along with headaches and neck pain, is frequently reported in patients with restricted cervical movement and is also associated with extensive computer or cell phone use, with which the correlation remains unclear, insinuating there could be a shared etiology amongst many overlapping diagnoses [11,121,122].
As the vagus nerve travels with the internal jugular vein within the carotid sheath, it was not surprising to also find an extremely high rate of vagus nerve degeneration (95%) in this patient population. Since approximately 75-80% of the nerve fibers in the parasympathetic nervous system originate from the vagus nerve, injury to the vagus nerve would cause low vagal tone, an increasing recognized cause of dysautonomia, specifically parasympathetic nervous system dysfunction [123,124,125]. Ocular parasympathetic nervous system dysfunction was evident in our patient population as 92% had baseline mydriasis (total pupil diameter >8 mm), averaging 10.29 mm, and 95% had abnormal pupillary light responses (>60% bilateral total), averaging 75% total [69,70,71].
Autonomic nervous system dysfunction is increasingly recognized as causing or occurring in ocular diseases and is most often related to parasympathetic nervous system dysfunction [126,127]. The ANS is involved with many physiological functions of the eye, including regulation of intraocular pressure, pupil dimensions and function, lens accommodation, and circulation within the eyes. Pupillary metrics including size and dynamic responses to light as seen on a pupillometer are recognized as a reliable indicator of ANS dysfunction, not just for the eye, but systemically for the body [73,128,129]. The chronically dilated pupils seen with nervous system dysfunction can cause blurry vision by hindering the ability to focus (decreased depth of field) and by allowing more light to enter the eye and hit the retina, either directly or peripherally, which can cause ocular aberrations [130].
The pupillary light reflex is under the control of the ANS and is defined as the constriction and subsequent dilation of the pupil in response to light. The pupillary light reflex can be affected by a wide range of disorders and by parasympathetic or sympathetic stimulation or inhibition [71,131]. As our patient population had dilated pupils and excessive percentage constriction to light, a milieu of sympathetic dominance or parasympathetic deficiency was present, a condition we termed ocular dysautonomia. Ocular dysautonomia causing pupil dilation can increase IOP due to accumulation of aqueous humor from fluid outflow obstruction at the trabecular meshwork and Schlemm’s canal, and this pressure can cause blurry vision by putting pressure on the optic nerve from inside the eye, as seen in glaucoma.
The ocular autonomic dysfunction seen in our patient population can be explained from cervical structural effects of the forward-shifted atlas on the vagus nerve, as the 2 vagus nerve ganglia—the nodose ganglion and the jugular ganglion—sit just anterior to the atlas (C1), as well as on the superior cervical sympathetic ganglion, which is located just anterior to the axis (C2). Cervical sympathetic ganglion stimulation has been shown to increase IOP [132]. The vagus nerve is the main inhibitory mechanism to sympathetic stimulation, as it has direct communication with the SCSG [81,133]. (See Figure 17.)
Since almost all of the patients experienced mydriasis, it would be expected that some (19% in our study) would have increased intraocular pressure (>21 mmHg), given that pupil dilation is a well-known cause of raising intraocular pressure [27,87]. A Pearson correlation coefficient analysis supported this conjecture, showing a strong positive relationship between pupil diameter and intraocular pressure (r = 0.26, p = 0.002). Though not tested in our patient population, accommodation dysfunction is a possible etiology of blurry vision, potentially also affected by the ocular dysautonomic state produced by LCI, as pupillary diameter and ocular accommodation are each controlled by eye muscles in the iris and ciliary body, receiving innervation by the ciliary (parasympathetic) and postganglionic fibers in the upper cervical (sympathetic) ganglion [134].
The discussed mechanisms of blurry vision arising from LCI and cervical dysstructure are not exclusive causes of blurry vision but possibly overlooked pathophysiological pathways that can potentially be enhanced with treatment directed at improving cervical structure. Further studies analyzing the association between cervical structural changes and eye symptoms should include cervical structural treatment and follow-up data to compare and document improvement to not only cervical structural tests, but all neck vitals and eye measurements, as well as changes in severity, or resolution, of blurry vision. Should follow-up studies prove resolution or improvement of blurry vision by correcting the cervical structural issues and the pathophysiology it causes, including IJV compression and vagus nerve degeneration, then a large group of patients who have otherwise unknown etiology, and whose quality of life is greatly affected by this visual disturbance, may be presented with new and promising treatment options.
Limitations of this study include the absence of other specific objective ophthalmic and retinal tests, including optic coherence tomography, the absence of a control group with a normal, stable lordotic curve to compare frequencies and objective test results, and the study’s retrospective design, therefore treatment protocols, follow-up testing, and progress were not included.
The data from this particular patient population supports our hypothesis that LCI and cervical dysstructure are a potential etiology of blurry vision, and we recommend that further studies replicate these diagnostics to confirm LCI pathologies and utilize dynamic structural medicine treatment protocols to potentially improve outcomes of patients with blurry vision of otherwise unknown etiology.
The findings in this study led us to consider a structural and overlooked etiology of blurry vision to be ligamentous cervical instability and cervical dysstructure. Due to our excluding patients with previously known traumatic events or diagnosis, the cervical structural changes seen in this patient population are likely caused by the ever-increasing, adopted lifestyle involving prolonged time spent in unnatural postures of cervical spine flexion while using electronic devices, which leads to a slow stretching and thus elongation of the cervical ligaments, allowing for loss of cervical lordosis and eventually a forward-shifted atlas in 3-D space from LCI, causing stretch and compression of vital structures of the neck (nerves and blood vessels) [135]. If blurry vision is related to cervical structural changes, then blurry vision might improve or resolve with relieving carotid sheath compression by following a cervical structural program that restores cervical lordosis and improves stability. This dynamic structural medicine protocol could include recommendations such as postural ergonomic changes (computer setup and prism glasses to view cell phones), physical therapy, therapeutic exercises, gentle chiropractic or osteopathic adjustments, and regenerative therapies to assist in cervical curve stabilization by strengthening the ligaments with Prolotherapy [34,48,136].
5. Conclusions
This study analyzed objective test findings from a cohort of 145 patients, representing a subset of patients who have blurry vision with no previously identified cause. To-date, we believe this to be the only study reporting on objective cervical structural and ocular clinical data in a cohort of patients with blurry vision. Objective dynamic cervical structural tests documented forward head/neck posture (abnormal C6AI measurements), decreased cervical lordosis (decreased depth of curve), ligamentous lower cervical instabilities in flexion and extension, and ligamentous upper cervical (C1-C2) facet joint instability in lateral flexion. The documented cervical spine dysfunction is likely causing compression of the carotid sheath at the atlas, leading to a decreased CSA of the IJVs and vagus nerves. The data suggest that some cases of blurry vision could be explained by ocular pathology due to ligamentous cervical instability and/or a breakdown of the cervical curve, causing internal jugular vein compression with consequent elevation in ONSD, and vagus nerve degeneration with resultant ocular dysautonomia, including pupillary dilation and increased pupillary constriction to light.
Blurry vision with otherwise unknown etiology, such as is associated with text neck syndrome or computer vision syndrome, is likely due to the facedown/forward head lifestyle putting excessive forces on the cervical spine, causing structural changes leading to ligamentous cervical instability and cervical dysstructure. If some cases of blurry vision of unknown etiology are from structural neck disorders, then a dynamic structural program to restore cervical lordosis and structural integrity (including proper ergonomics while viewing electronic devices, physical therapy, low-force atlas adjustments, and Prolotherapy) should be considered as a possible treatment option.
Author Contributions
Conceptualization, Ross Hauser; Data curation, Ross Hauser; Formal analysis, Ashley Watterson; Investigation, Ross Hauser and Danielle Matias; Methodology, Ross Hauser; Project administration, Ross Hauser; Resources, Ross Hauser and Danielle Matias; Supervision, Ross Hauser; Validation, Ross Hauser and Morgan Griffiths; Visualization, Ross Hauser, Morgan Griffiths and Benjamin Rawlings; Writing – original draft, Ross Hauser and Morgan Griffiths; Writing – review & editing, Morgan Griffiths and Benjamin Rawlings.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of WCG (protocol code 1364545 on November 1, 2023).
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results can be provided upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ANS | Autonomic nervous system |
| C6AI | C6-atlas interval |
| CBCT | Cone beam computerized tomography |
| CSA | Cross-sectional area |
| CSF | Cerebral spinal fluid |
| CT | Computerized tomography |
| DOC | Depth of curve |
| IJV | Internal Jugular Vein |
| IOP | Intraocular Pressure |
| LCI | Ligamentous cervical instability |
| MRI | Magnetic resonance imaging |
| ONSD | Optic nerve sheath diameter |
References
- Pavel IA, Bogdanici CM, Donica VC, et al. Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era. Medicina (Kaunas). 2023;59(2):412. Published 2023 Feb 20. [CrossRef]
- Uddin O, Light J, Henderson A. Headaches and Blurry Vision. J Neuroophthalmol. 2024 Dec 1;44(4):e526. [CrossRef]
- Hu CX, Zangalli C, Hsieh M, Gupta L, Williams AL, Richman J, Spaeth GL. What do patients with glaucoma see? Visual symptoms reported by patients with glaucoma. Am J Med Sci. 2014 Nov;348(5):403-9. [CrossRef]
- Sun Y, Muheremu A, Tian W. Atypical symptoms in patients with cervical spondylosis: Comparison of the treatment effect of different surgical approaches. Medicine (Baltimore). 2018 May;97(20):e10731. [CrossRef]
- Leung KKY, Chu EC, Chin WL, Mok STK, Chin EWS. Cervicogenic visual dysfunction: an understanding of its pathomechanism. Med Pharm Rep. 2023 Jan;96(1):16-19. [CrossRef]
- Erdinest N, Berkow D. [COMPUTER VISION SYNDROME]. Harefuah. 2021 Jun;160(6):386-392. Hebrew.
- Adane F, Alamneh YM, Desta M. Computer vision syndrome and predictors among computer users in Ethiopia: a systematic review and meta-analysis. Trop Med Health. 2022 Mar 24;50(1):26. [CrossRef]
- Bogdănici CM, Săndulache DE, Nechita CA. Eyesight quality and Computer Vision Syndrome. Rom J Ophthalmol. 2017 Apr-Jun;61(2):112-116. [CrossRef]
- Teo C, Giffard P, Johnston V, Treleaven J. Computer vision symptoms in people with and without neck pain. Appl Ergon. 2019 Oct;80:50-56. [CrossRef]
- Sen A, Richardson S. A study of computer-related upper limb discomfort and computer vision syndrome. J Hum Ergol (Tokyo). 2007 Dec;36(2):45-50.
- Tsantili AR, Chrysikos D, Troupis T. Text Neck Syndrome: Disentangling a New Epidemic. Acta Med Acad. 2022 Aug;51(2):123-127. [CrossRef]
- Singh S, Keller PR, Busija L, et al. Blue-light filtering spectacle lenses for visual performance, sleep, and macular health in adults. Cochrane Database Syst Rev. 2023 Aug 18;8(8):CD013244. [CrossRef]
- Abudawood GA, Ashi HM, Almarzouki NK. Computer Vision Syndrome among Undergraduate Medical Students in King Abdulaziz University, Jeddah, Saudi Arabia. J Ophthalmol. 2020, Article 2789376. [CrossRef]
- Blehm C, Vishnu S, Khattak A, Mitra S, Yee RW. Computer vision syndrome: a review. Surv Ophthalmol. 2005 May-Jun;50(3):253-62. [CrossRef]
- Anderst W. (2014). In vivo cervical spine kinematics arthrokinematics and disc loading in asymptomatic control subjects and anterior fusion patients. [Dissertation]. [Pittsburgh (PA)]: University of Pittsburgh. http://d-scholarship.pitt.edu/22226/1/anderst_edt2014.pdf. Accessed July 6, 2023.
- Bonney RA, Corlett EN. Head posture and loading of the cervical spine. Appl Ergon. 2002 Sep;33(5):415-7. [CrossRef]
- Lee S, Kang H, Shin G. Head flexion angle while using a smartphone. Ergonomics. 2015;58(2):220-6. [CrossRef]
- Hauser RA, Matias D, Rawlings B. The ligamentous cervical instability etiology of human disease from the forward head-facedown lifestyle: emphasis on obstruction of fluid flow into and out of the brain. Front Neurol. 2024 Nov 27;15:1430390. [CrossRef]
- Guan X, Fan G, Wu X, et al. Photographic measurement of head and cervical posture when viewing mobile phone: a pilot study. Eur Spine J. 2015 Dec;24(12):2892-8. [CrossRef]
- Gupta V, Khandelwal N, Mathuria SN, Singh P, Pathak A, Suri S. Dynamic magnetic resonance imaging evaluation of craniovertebral junction abnormalities. J Comput Assist Tomogr. 2007;31:354–9. [CrossRef]
- Alvarez AP, Anderson A, Farhan SD, et al. The Utility of Flexion-Extension Radiographs in Degenerative Cervical Spondylolisthesis. Clin Spine Surg. 2022 Aug 1;35(7):319-322. [CrossRef]
- Gisolf J, van Lieshout JJ, van Heusden K, Pott F, Stok WJ, Karemaker JM. Human cerebral venous outflow pathway depends on posture and central venous pressure. J Physiol. 2004 Oct 1;560(Pt 1):317-27. [CrossRef]
- Tartière D, Seguin P, Juhel C, Laviolle B, Mallédant Y. Estimation of the diameter and cross-sectional area of the internal jugular veins in adult patients. Crit Care. 2009;13(6):R197. [CrossRef]
- Yoon HK, Lee HK, Jeon YT, Hwang JW, Lim SM, Park HP. Clinical significance of the cross-sectional area of the internal jugular vein. J Cardiothorac Vasc Anesth. 2013 Aug;27(4):685-9. [CrossRef]
- Buch K, Groller R, Nadgir RN, Fujita A, Qureshi MM, Sakai O. Variability in the Cross-Sectional Area and Narrowing of the Internal Jugular Vein in Patients Without Multiple Sclerosis. AJR Am J Roentgenol. 2016 May;206(5):1082-6. [CrossRef]
- Gharieb Ibrahim HM. Effect of Pharmacological Mydriasis on the Intraocular Pressure in Eyes with Filtering Blebs Compared to Normal Eyes: A Pilot Study. Clin Ophthalmol. 2022 Feb 1;16:231-237. [CrossRef]
- Siam GA, de Barros DS, Gheith ME, et al. The amount of intraocular pressure rise during pharmacological pupillary dilatation is an indicator of the likelihood of future progression of glaucoma. Br J Ophthalmol. 2007 Sep;91(9):1170-2. [CrossRef]
- Hauser RA. Hauser’s Laws on the Ligamentous Structural Causes of Chronic Disabling Symptoms of Human Diseases. On J Neur & Br Disord. 2024;7(1):642-689. [CrossRef]
- Teo AQA, Thomas AC, Hey HWD. Sagittal alignment of the cervical spine: do we know enough for successful surgery? J Spine Surg. 2020 Mar;6(1):124-135. [CrossRef]
- Patel PD, Arutyunyan G, Plusch K, Vaccaro A Jr, Vaccaro AR. A review of cervical spine alignment in the normal and degenerative spine. J Spine Surg. 2020 Mar;6(1):106-123. [CrossRef]
- Borden AGB, Rechtman AM, Gershon-Cohen J. The normal cervical lordosis. Radiology; 1960; 74:806-809. [CrossRef]
- Hou SB, Sun XZ, Liu FY, et al. Relationship of Change in Cervical Curvature after Laminectomy with Lateral Mass Screw Fixation to Spinal Cord Shift and Clinical Efficacy. J Neurol Surg A Cent Eur Neurosurg. 2022 Mar;83(2):129-134. [CrossRef]
- Mahmoud NF, Hassan KA, Abdelmajeed SF, Moustafa IM, Silva AG. The Relationship Between Forward Head Posture and Neck Pain: a Systematic Review and Meta-Analysis. Curr Rev Musculoskelet Med. 2019 Dec;12(4):562-577. [CrossRef]
- Oakley PA, Moustafa IM, Haas JW, Betz JW, Harrison DE. Two Methods of Forward Head Posture Assessment: Radiography vs. Posture and Their Clinical Comparison. J Clin Med. 2024 Apr 8;13(7):2149. [CrossRef]
- Poursadegh M, Azghani MR, Chakeri Z, Okhravi SM, Salahzadeh Z. Postures of the head, upper, and lower neck in forward head posture: Static and quasi-static analyses. Middle East J Rehabil Health Stud. 2024;10(4), e136377. [CrossRef]
- Shaghayegh fard B, Ahmadi A, Maroufi N, Sarrafzadeh J. Evaluation of forward head posture in sitting and standing positions. Eur Spine J. 2016;25(11):3577–3582. [CrossRef]
- Deniz Y, Pehlivan E, Cicek E. Biomechanical variances in the development of forward head posture. Phys Ther Korea. 2024;31(2), 104–113. [CrossRef]
- Chu ECP, Lo FS, Bhaumik A. Plausible impact of forward head posture on upper cervical spine stability. J Family Med Prim Care. 2020 May 31;9(5):2517-2520. [CrossRef]
- Freeman MD, Katz EA, Rosa SL, Gatterman BG, Strömmer EMF, Leith WM. Diagnostic Accuracy of Videofluoroscopy for Symptomatic Cervical Spine Injury Following Whiplash Trauma. Int J Environ Res Public Health. 2020 Mar 5;17(5):1693. [CrossRef]
- Daffner R.H. Imaging of Vertebral Trauma. 3rd ed. Cambridge University Press; Cambridge, UK: 2011. p. 163. [Google Scholar] Accessed April 1, 2025.
- Bogduk N. Functional anatomy of the spine. Handb Clin Neurol. 2016;136:675-88. [CrossRef]
- Radcliff K, Kepler C, Reitman C, Harrop J, Vaccaro A. CT and MRI-based diagnosis of craniocervical dislocations: the role of the occipitoatlantal ligament. Clin Orthop Relat Res. 2012 Jun;470(6):1602-13. [CrossRef]
- Dickman CA, Mamourian A, Sonntag VKH, Drayer BP. Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurg. 1991;75(2), 221–227. [CrossRef]
- Liao S, Jung MK, Hörnig L, Grützner PA, Kreinest M. Injuries of the upper cervical spine-how can instability be identified? Int Orthop. 2020;44:1239–53. [CrossRef]
- Freeman MD, Rosa S, Harshfield D, et al. A case-control study of cerebellar tonsillar ectopia (Chiari) and head/neck trauma (whiplash). Brain Inj. (2010) 24:988–94. [CrossRef]
- Azar NR, Kallakuri S, Chen C, Lu Y, Cavanaugh JM. Strain and load thresholds for cervical muscle recruitment in response to quasi-static tensile stretch of the caprine C5-C6 facet joint capsule. J Electromyogr Kinesiol. 2009 Dec;19(6):e387-94. [CrossRef]
- Patwardhan AG, Khayatzadeh S, Havey RM, et al. Cervical sagittal balance: a biomechanical perspective can help clinical practice. Eur Spine J. 2018 Feb;27(Suppl 1):25-38. [CrossRef]
- Steilen D, Hauser R, Woldin B, Sawyer S. Chronic neck pain: making the connection between capsular ligament laxity and cervical instability. Open Orthop J. 2014;8:326–345. [CrossRef]
- Solomonow M. Sensory-motor control of ligaments and associated neuromuscular disorders. J Electromyogr Kinesiol. 2006 Dec;16(6):549-67. [CrossRef]
- Jeon JC, Choi WI, Lee JH, Lee SH. Anatomical Morphology Analysis of Internal Jugular Veins and Factors Affecting Internal Jugular Vein Size. Medicina (Kaunas). 2020 Mar 18;56(3):135. [CrossRef]
- Manfré L, Lagalla R, Mangiameli A, et al. Idiopathic intracranial hypertension: orbital MRI. Neuroradiology. 1995 Aug;37(6):459-61. [CrossRef]
- Simon MJ, Iliff JJ. Regulation of cerebrospinal fluid (CSF) flow in neurodegenerative, neurovascular and neuroinflammatory disease. Biochim Biophys Acta. 2016 Mar;1862(3):442-51. [CrossRef]
- Ghate D, Kedar S, Havens S, et al. The Effects of Acute Intracranial Pressure Changes on the Episcleral Venous Pressure, Retinal Vein Diameter and Intraocular Pressure in a Pig Model. Curr Eye Res. 2021;46(4), 524–531. [CrossRef]
- Lee SS, Robinson MR, Weinreb RN. Episcleral Venous Pressure and the Ocular Hypotensive Effects of Topical and Intracameral Prostaglandin Analogs. J Glaucoma. 2019 Sep;28(9):846-857. [CrossRef]
- Ngnitewe Massa R, Minutello K, Mesfin FB. Neuroanatomy, Cavernous Sinus. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459244/.
- Kiel JW. The Ocular Circulation. San Rafael (CA): Morgan & Claypool Life Sciences; 2010. Chapter 2, Anatomy. Available from: https://www.ncbi.nlm.nih.gov/books/NBK53329/#.
- Siaudvytyte L, Januleviciene I, Daveckaite A, et al. Literature review and meta-analysis of translaminar pressure difference in open-angle glaucoma. Eye (Lond). 2015 Oct;29(10):1242-50. [CrossRef]
- Morgan WH, Yu DY, Cooper RL, Alder VA, Cringle SJ, Constable IJ. The influence of cerebrospinal fluid pressure on the lamina cribrosa tissue pressure gradient. Invest Ophthalmol Vis Sci. 1995 May;36(6):1163-72.
- Mohammed NY, Di Domenico G, Gambaccini M. Cerebral venous drainage through internal jugular vein. Veins Lymphatics. 2019;8(1). [CrossRef]
- Yu ZY, Xing YQ, Li C, et al. Ultrasonic optic disc height combined with the optic nerve sheath diameter as a promising non-invasive marker of elevated intracranial pressure. Front Physiol. 2023 Mar 10;14:957758. [CrossRef]
- Raffiz M, Abdullah JM. Optic nerve sheath diameter measurement: a means of detecting raised ICP in adult traumatic and non-traumatic neurosurgical patients. Am J Emerg Med. 2017 Jan;35(1):150-153. [CrossRef]
- Maissan IM, Dirven PJ, Haitsma IK, Hoeks SE, Gommers D, Stolker RJ. Ultrasonographic measured optic nerve sheath diameter as an accurate and quick monitor for changes in intracranial pressure. J Neurosurg. 2015 Sep;123(3):743-7. [CrossRef]
- Malky IE, Aita WE, Elkordy A, et al. Optic nerve sonographic parameters in idiopathic intracranial hypertension, case-control study. Sci Rep. 2025 Jan 13;15(1):1788. [CrossRef]
- Kishk NA, Ebraheim AM, Ashour AS, Badr NM, Eshra MA. Optic nerve sonographic examination to predict raised intracranial pressure in idiopathic intracranial hypertension: The cut-off points. Neuroradiol J.2018;31(5):490-495. [CrossRef]
- Chen S, Chen Y, Xu L, et al. Venous system in acute brain injury: Mechanisms of pathophysiological change and function. Exp Neurol. 2015 Oct;272:4-10. [CrossRef]
- Doepp F, Schreiber SJ, von Münster T, Rademacher J, Klingebiel R, Valdueza JM. How does the blood leave the brain? A systematic ultrasound analysis of cerebral venous drainage patterns. Neuroradiology. 2004;46:565–70. [CrossRef]
- Margolin E. The swollen optic nerve: an approach to diagnosis and management. Pract Neurol. 2019 Aug;19(4):302-309. [CrossRef]
- Abdelnaby R, Elsayed M, Mohamed KA, et al. Sonographic Reference Values of Vagus Nerve: A Systematic Review and Meta-analysis. J Clin Neurophysiol. 2022 Jan 1;39(1):59-71. [CrossRef]
- Kiel M, Grabitz SD, Hopf S, et al. Distribution of Pupil Size and Associated Factors: Results from the Population-Based Gutenberg Health Study. J Ophthalmol. 2022 Sep 9;2022:9520512. [CrossRef]
- Couret D, Boumaza D, Grisotto C, et al. Reliability of standard pupillometry practice in neurocritical care: an observational, double-blinded study. Crit Care. 2016 Mar 13;20:99. [CrossRef]
- Hall CA, Chilcott RP. Eyeing up the Future of the Pupillary Light Reflex in Neurodiagnostics. Diagnostics (Basel). 2018 Mar 13;8(1):19. [CrossRef]
- Hamrakova A, Ondrejka I, Sekaninova N, et al. Central autonomic regulation assessed by pupillary light reflex is impaired in children with attention deficit hyperactivity disorder. Physiol Res. 2020 Dec 31;69(Suppl 3):S513-S521. [CrossRef]
- Karahan M, Demirtaş AA, Hazar L, et al. Autonomic dysfunction detection by an automatic pupillometer as a non-invasive test in patients recovered from COVID-19. Graefes Arch Clin Exp Ophthalmol. 2021 Sep;259(9):2821-2826. [CrossRef]
- Tsitsi P, Nilsson M, Waldthaler J, et al. Pupil light reflex dynamics in Parkinson's disease. Front Integr Neurosci. 2023 Aug 31;17:1249554. [CrossRef]
- Larsen RS, Waters J. Neuromodulatory Correlates of Pupil Dilation. Front Neural Circuits. 2018 Mar 9;12:21. [CrossRef]
- De Couck M, Mravec B, Gidron Y. You may need the vagus nerve to understand pathophysiology and to treat diseases. Clin Sci (Lond). 2012 Apr;122(7):323-8. [CrossRef]
- Mathôt S. Pupillometry: Psychology, Physiology, and Function. J Cogn. 2018 Feb 21;1(1):16. [CrossRef]
- David D, Giannini C, Chiarelli F, Mohn A. Text Neck Syndrome in Children and Adolescents. Int J Environ Res Public Health. 2021 Feb 7;18(4):1565. [CrossRef]
- Anbesu EW, Lema AK. Prevalence of computer vision syndrome: a systematic review and meta-analysis. Sci Rep. 2023 Jan 31;13(1):1801. [CrossRef]
- Watanuki A. [The effect of the sympathetic nervous system on cervical spondylosis (author's transl)]. Nihon Seikeigeka Gakkai Z. 1981 Apr;55(4):371-85. Japanese.
- Mitsuoka K, Kikutani T, Sato I. Morphological relationship between the superior cervical ganglion and cervical nerves in Japanese cadaver donors. Brain Behav. 2016 Dec 29;7(2):e00619. [CrossRef]
- D L A, Raju TR. Autonomic Nervous System and Control of Visual Function. Ann Neurosci. 2023 Jul;30(3):151-153. [CrossRef]
- Chawla JC, Falconer MA. Glossopharyngeal and vagal neuralgia. Br Med J. 1967 Aug 26;3(5564):529-31. [CrossRef]
- Cardinali DP, Vacas MI, Gejman PV. The sympathetic superior cervical ganglia as peripheral neuroendocrine centers. J Neural Transm.1981;52(1-2):1-21. [CrossRef]
- Mul Fedele ML, Galiana MD, Golombek DA, Muñoz EM, Plano SA. Alterations in Metabolism and Diurnal Rhythms following Bilateral Surgical Removal of the Superior Cervical Ganglia in Rats. Front Endocrinol (Lausanne). 2018 Jan 9;8:370. [CrossRef]
- Anterieu P, Vassal F, Sindou M. Vagoglossopharyngeal neuraligia revealed through predominant digestive vagal manifestations. Case report and literature review. Neurochirugie. 2016 Jun;62(3):174-7. [CrossRef]
- Kim JM, Park KH, Han SY, et al. Changes in intraocular pressure after pharmacologic pupil dilation. BMC Ophthalmol. 2012 Sep 27;12:53. [CrossRef]
- Lewczuk K, Jabłońska J, Konopińska J, Mariak Z, Rękas M. Schlemm's canal: the outflow 'vessel'. Acta Ophthalmol. 2022 Jun;100(4):e881-e890. [CrossRef]
- Tominaga Y, Maak TG, Ivancic PC, Panjabi MM, Cunningham BW. Head-turned rear impact causing dynamic cervical intervertebral foramen narrowing: implications for ganglion and nerve root injury. J Neurosurg Spine. 2006 May;4(5):380-7. [CrossRef]
- Chen HS, van Roon L, Ge Y, et al. The relevance of the superior cervical ganglion for cardiac autonomic innervation in health and disease: a systematic review. Clin Auton Res. 2024 Feb;34(1):45-77. [CrossRef]
- Dieguez HH, Romeo HE, González Fleitas MF, et al. Superior cervical gangliectomy induces non-exudative age-related macular degeneration in mice. Dis Model Mech. 2018 Feb 7;11(2):dmm031641. [CrossRef]
- Betsch M, Kalbhen K, Michalik R, et al. The influence of smartphone use on spinal posture - A laboratory study. Gait Posture. 2021 Mar;85:298-303. [CrossRef]
- Anderson M, Jiang J. (2018, May 31). Teens, social media & technology 2018. Pew Research Center. https://www.pewresearch.org/internet/2018/05/31/teens-social-media-technology-2018/ Accessed April 2. 2025.
- DemandSage. (2024). Screen time statistics: 2024 data and trends. DemandSage. https://www.demandsage.com/screen-time-statistics/ Accessed March 5, 2025.
- Tsang SMH, Cheing GLY, Lam AKC, et al. Excessive use of electronic devices among children and adolescents is associated with musculoskeletal symptoms, visual symptoms, psychosocial health, and quality of life: a cross-sectional study. Front Public Health. 2023 Jun 29;11:1178769. [CrossRef]
- Vij N, Tolson H, Kiernan H, Agusala V, Viswanath O, Urits I. Pathoanatomy, biomechanics, and treatment of upper cervical ligamentous instability: A literature review. Orthop Rev (Pavia). 2022 Aug 5;14(3):37099. [CrossRef]
- Olson KA, Joder D. Diagnosis and treatment of cervical spine clinical instability. J Orthop Sports Phys Ther. 2001 Apr;31(4):194-206. [CrossRef]
- D'Angelo A, Vitiello L, Lixi F, et al. Optic Nerve Neuroprotection in Glaucoma: A Narrative Review. J Clin Med. 2024 Apr 11;13(8):2214. [CrossRef]
- Wilhelm H, Schabet M. The Diagnosis and Treatment of Optic Neuritis. Dtsch Arztebl Int. 2015 Sep 11;112(37):616-25; quiz 626. [CrossRef]
- Bennett JL. Optic Neuritis. Continuum (Minneap Minn). 2019 Oct;25(5):1236-1264. [CrossRef]
- Li M, Sun Y, Chan CC, Fan C, Ji X, Meng R. Internal jugular vein stenosis associated with elongated styloid process: five case reports and literature review. BMC Neurol. 2019 Jun 4;19(1):112. [CrossRef]
- Toshniwal SS, Kinkar J, Chadha Y, et al. Navigating the Enigma: A Comprehensive Review of Idiopathic Intracranial Hypertension. Cureus. 2024 Mar 16;16(3):e56256. [CrossRef]
- Fargen KM, Midtlien JP, Margraf CR, Hui FK. Idiopathic intracranial hypertension pathogenesis: The jugular hypothesis. Interv Neuroradiol. 2024 Aug 8:15910199241270660. [CrossRef]
- Tuță S. Cerebral Venous Outflow Implications in Idiopathic Intracranial Hypertension-From Physiopathology to Treatment. Life (Basel). 2022 Jun 8;12(6):854. [CrossRef]
- Hassen GW, Al-Juboori M, Koppel B, Akfirat G, Kalantari H. Real time optic nerve sheath diameter measurement during lumbar puncture. Am J Emerg Med. 2018 Apr;36(4):736.e1-736.e3. [CrossRef]
- Li Z, Zhang XX, Yang HQ, et al. [Correlation between ultrasonographic optic nerve sheath diameter and intracranial pressure]. Zhonghua Yan Ke Za Zhi. 2018 Sep 11;54(9):683-687. Chinese. [CrossRef]
- Robba C, Santori G, Czosnyka M, et al. Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: a systematic review and meta-analysis. Intensive Care Med. 2018 Aug;44(8):1284-1294. [CrossRef]
- Wang LJ, Chen LM, Chen Y, et al. Ultrasonography Assessments of Optic Nerve Sheath Diameter as a Noninvasive and Dynamic Method of Detecting Changes in Intracranial Pressure. JAMA Ophthalmol. 2018 Mar 1;136(3):250-256. [CrossRef]
- Hylkema C. Optic Nerve Sheath Diameter Ultrasound and the Diagnosis of Increased Intracranial Pressure. Crit Care Nurs Clin North Am. 2016 Mar;28(1):95-9. [CrossRef]
- Mathieu E, Gupta N, Ahari A, Zhou X, Hanna J, Yücel YH. Evidence for Cerebrospinal Fluid Entry Into the Optic Nerve via a Glymphatic Pathway. Invest Ophthalmol Vis Sci. 2017 Sep 1;58(11):4784-4791. [CrossRef]
- Ertl M, Knüppel C, Veitweber M, et al. Normal Age- and Sex-Related Values of the Optic Nerve Sheath Diameter and Its Dependency on Position and Positive End-Expiratory Pressure. Ultrasound Med Biol. 2020 Dec;46(12):3279-3285. [CrossRef]
- Lochner P, Brio F, Zedde ML, et al. Feasibility and usefulness of ultrasonography in idiopathic intracranial hypertension or secondary intracranial hypertension. BMC Neurol. 2016 Jun 2;16:85. [CrossRef]
- Ussahgij W, Toonpirom W, Munkong W, Ienghong K. Optic nerve sheath diameter cutoff point for detection of increased intracranial pressure in the emergency room. Maced J Med Sci. 2020. Feb 25; 8(B): 62-65. [CrossRef]
- Lee SJ, Choi MH, Lee SE, et al. Optic nerve sheath diameter change in prediction of malignant cerebral edema in ischemic stroke: an observational study. BMC Neurol. 2020 Sep 22;20(1):354. [CrossRef]
- Dubourg J, Javouhey E, Geeraerts T, Messerer M, Kassai B. Ultrasonography of optic nerve sheath diameter for detection of raised intracranial pressure: a systematic review and meta-analysis. Intensive Care Med. 2011 Jul;37(7):1059-68. [CrossRef]
- Berberat J, Pircher A, Gruber P, Lovblad KO, Remonda L, Killer HE. Case Report: Cerebrospinal Fluid Dynamics in the Optic Nerve Subarachnoid Space and the Brain Applying Diffusion Weighted MRI in Patients With Idiopathic Intracranial Hypertension-A Pilot Study. Front Neurol. 2022 Apr 15;13:862808. [CrossRef]
- Sarrami AH, Bass DI, Rutman AM, et al. Idiopathic intracranial hypertension imaging approaches and the implications in patient management. Br J Radiol. 2022 Aug 1;95(1136):20220136. [CrossRef]
- Bozdoğan Z, Şenel E, Özmuk Ö, Karataş H, Kurşun O. Comparison of Optic Nerve Sheath Diameters Measured by Optic Ultrasonography Before and After Lumbar Puncture in Idiopathic Intracranial Hypertension Patients. Noro Psikiyatr Ars. 2023 May 5;60(2):117-123. [CrossRef]
- Zaic S, Krajnc N, Macher S, et al. Therapeutic effect of a single lumbar puncture in idiopathic intracranial hypertension. J Headache Pain. 2024 Sep 5;25(1):145. [CrossRef]
- Dinkin M, Oliveira C. Men Are from Mars, Idiopathic Intracranial Hypertension Is from Venous: The Role of Venous Sinus Stenosis and Stenting in Idiopathic Intracranial Hypertension. Semin Neurol. 2019 Dec;39(6):692-703. [CrossRef]
- Singh S, McGuinness MB, Anderson AJ, Downie LE. Interventions for the Management of Computer Vision Syndrome: A Systematic Review and Meta-analysis. Ophthalmology. 2022 Oct;129(10):1192-1215. [CrossRef]
- Zamysłowska-Szmytke E, Adamczewski T, Ziąber J, Majak J, Kujawa J, Śliwińska-Kowalska M. Cervico-ocular reflex upregulation in dizzy patients with asymmetric neck pathology. Int J Occup Med Environ Health. 2019 Oct 16;32(5):723-733. [CrossRef]
- Huckemann S, Mueller K, Averdunk P, et al. Vagal cross-sectional area correlates with parasympathetic dysfunction in Parkinson's disease. Brain Commun. 2023 Jan 18;5(1):fcad006. [CrossRef]
- Goldberger JJ, Arora R, Buckley U, Shivkumar K. Autonomic Nervous System Dysfunction: JACC Focus Seminar. J Am Coll Cardiol. 2019 Mar 19;73(10):1189-1206. [CrossRef]
- Zanin A, Amah G, Chakroun S, et al. Parasympathetic autonomic dysfunction is more often evidenced than sympathetic autonomic dysfunction in fluctuating and polymorphic symptoms of "long-COVID" patients. Sci Rep. 2023 May 22;13(1):8251. [CrossRef]
- Murakami A. Autonomic nervous system dysfunction in ocular diseases. Juntendon Med J. 2016;62:377-380. [CrossRef]
- Kaido M, Arita R, Mitsukura Y, Ishida R, Tsubota K. Variability of autonomic nerve activity in dry eye with decreased tear stability. PLoS One. 2022 Nov 16;17(11):e0276945. [CrossRef]
- Park HL, Jung SH, Park SH, Park CK. Detecting autonomic dysfunction in patients with glaucoma using dynamic pupillometry. Medicine (Baltimore). 2019 Mar;98(11):e14658. [CrossRef]
- Jain D, Arbogast K, McDonald C. Objective eye tracking metrics of vision and autonomic dysfunction distinguish adolescents with acute concussion and those with persistent post-concussion symptoms from uninjured controls. Neurology. 2022;98. [CrossRef]
- Manion GN, Stokkermans TJ. The Effect of Pupil Size on Visual Resolution. [Updated 2024 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK603732/?utm_source=chatgpt.com Accessed April 3, 2025.
- [1] Bittner DM, Wieseler I, Wilhelm H, Riepe MW, Müller NG. Repetitive pupil light reflex: potential marker in Alzheimer's disease? J Alzheimers Dis. 2014;42(4):1469-77. [CrossRef]
- [1] Gallar J, Liu JH. Stimulation of the cervical sympathetic nerves increases intraocular pressure. Invest Ophthalmol Vis Sci. 1993 Mar;34(3):596-605.
- Mitsuoka K, Kikutani T, Sato I. Morphological relationship between the superior cervical ganglion and cervical nerves in Japanese cadaver donors. Brain Behav. 2016 Dec 29;7(2):e00619. [CrossRef]
- Khalid K, Padda J, Pokhriyal S, et al. Pseudomyopia and Its Association With Anxiety. Cureus. 2021 Aug 24;13(8):e17411. [CrossRef]
- Kasumovic M, Gorcevic E, Gorcevic S, Osmanovic J. Cervical syndrome - the effectiveness of physical therapy interventions. Med Arch. 2013 Dec;67(6):414-7. [CrossRef]
- Moustafa IM, Diab AA, Hegazy F, Harrison DE. Demonstration of central conduction time and neuroplastic changes after cervical lordosis rehabilitation in asymptomatic subjects: a randomized, placebo-controlled trial. Sci Rep. 2021 Jul 28;11(1):15379. [CrossRef]
Figure 1.
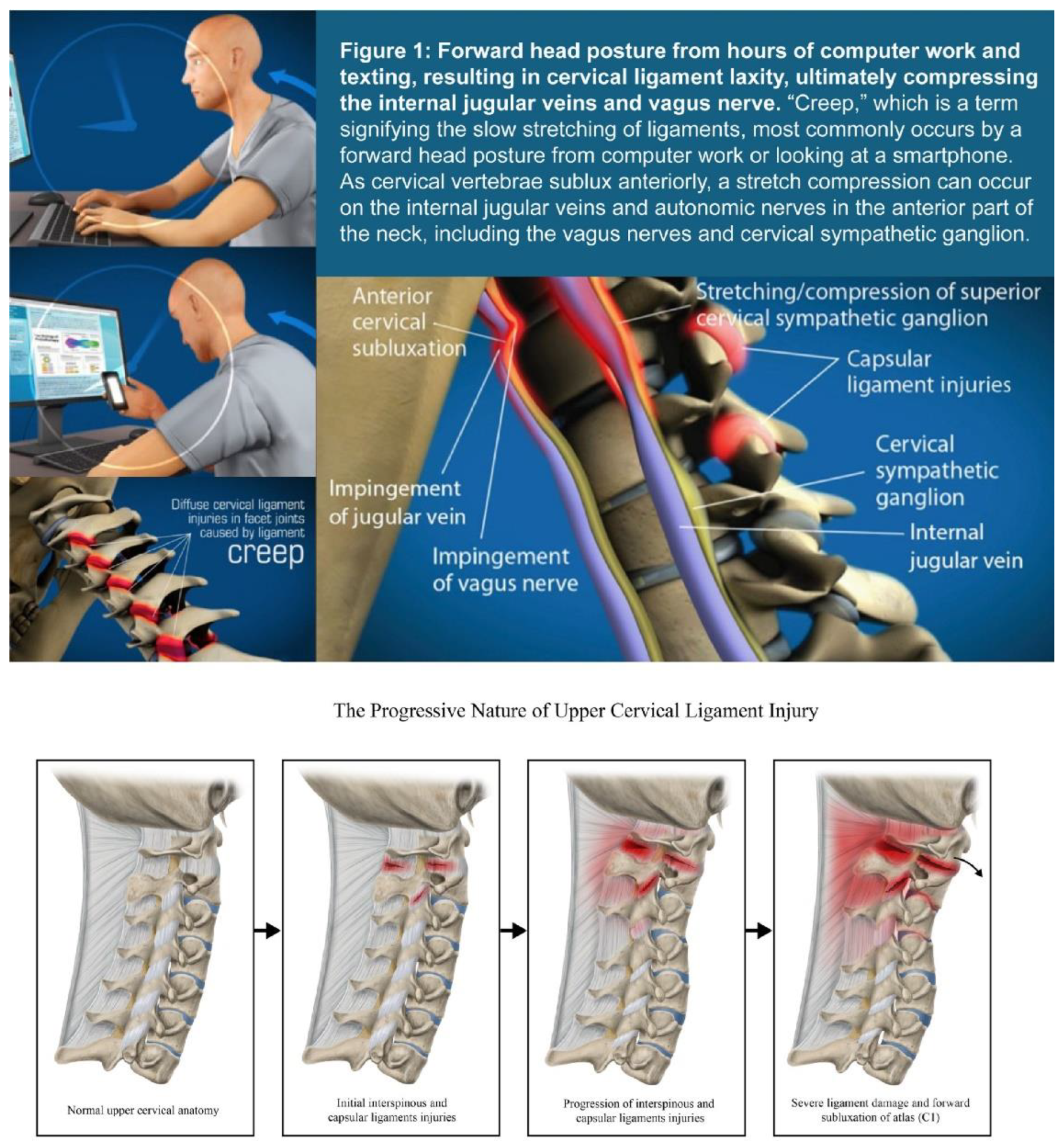
Figure 2.
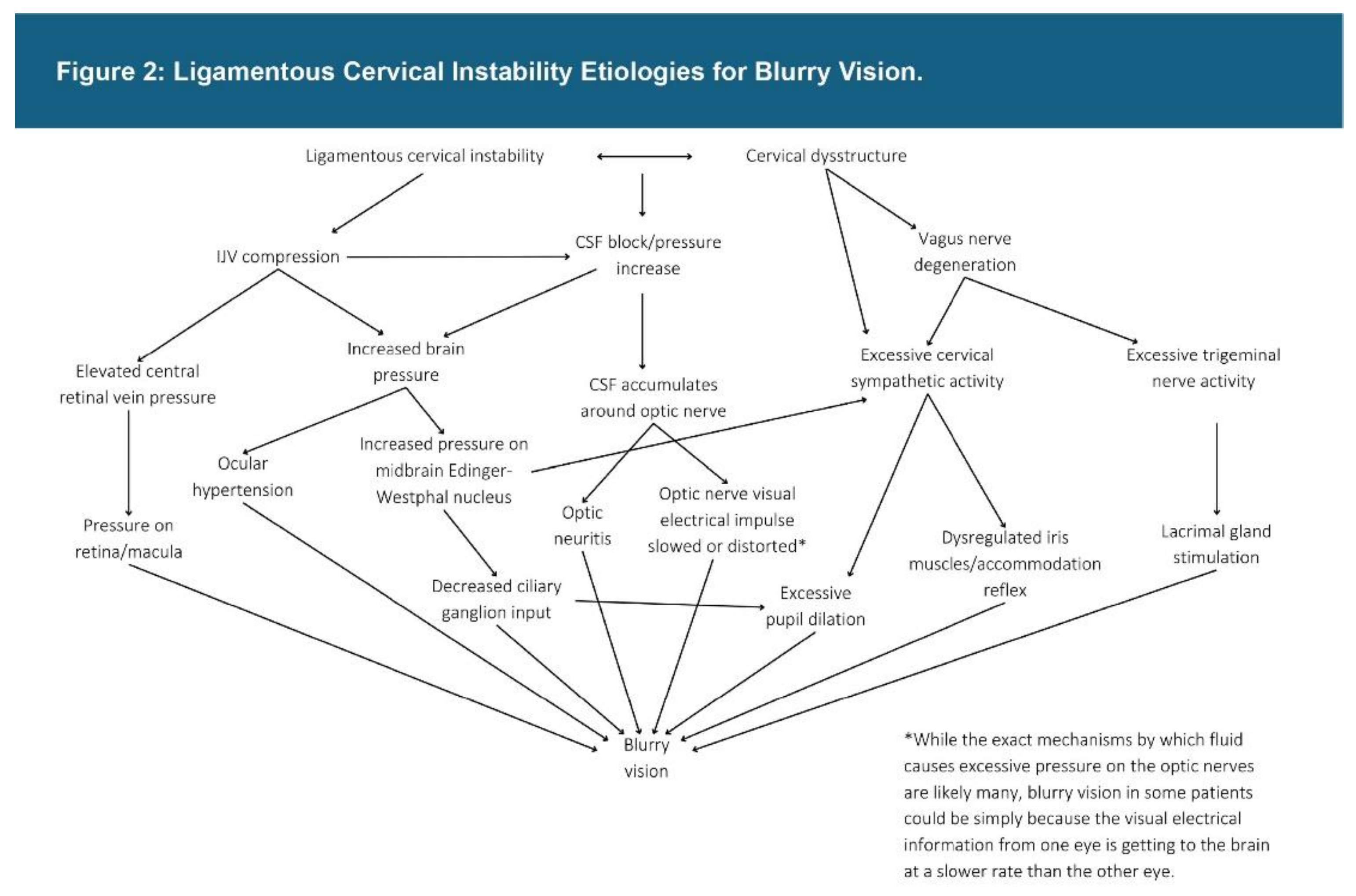
Figure 3.
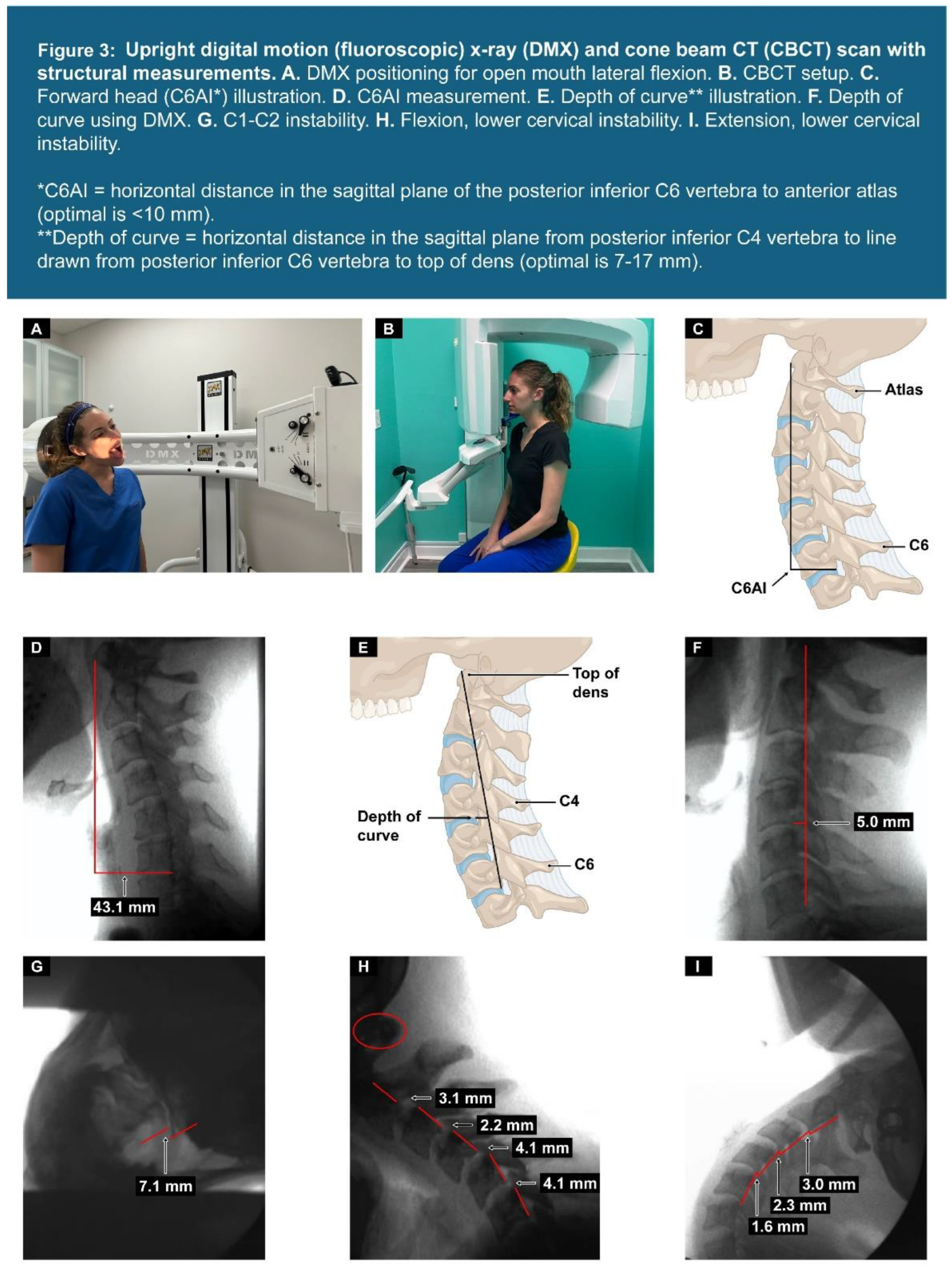
Figure 4.
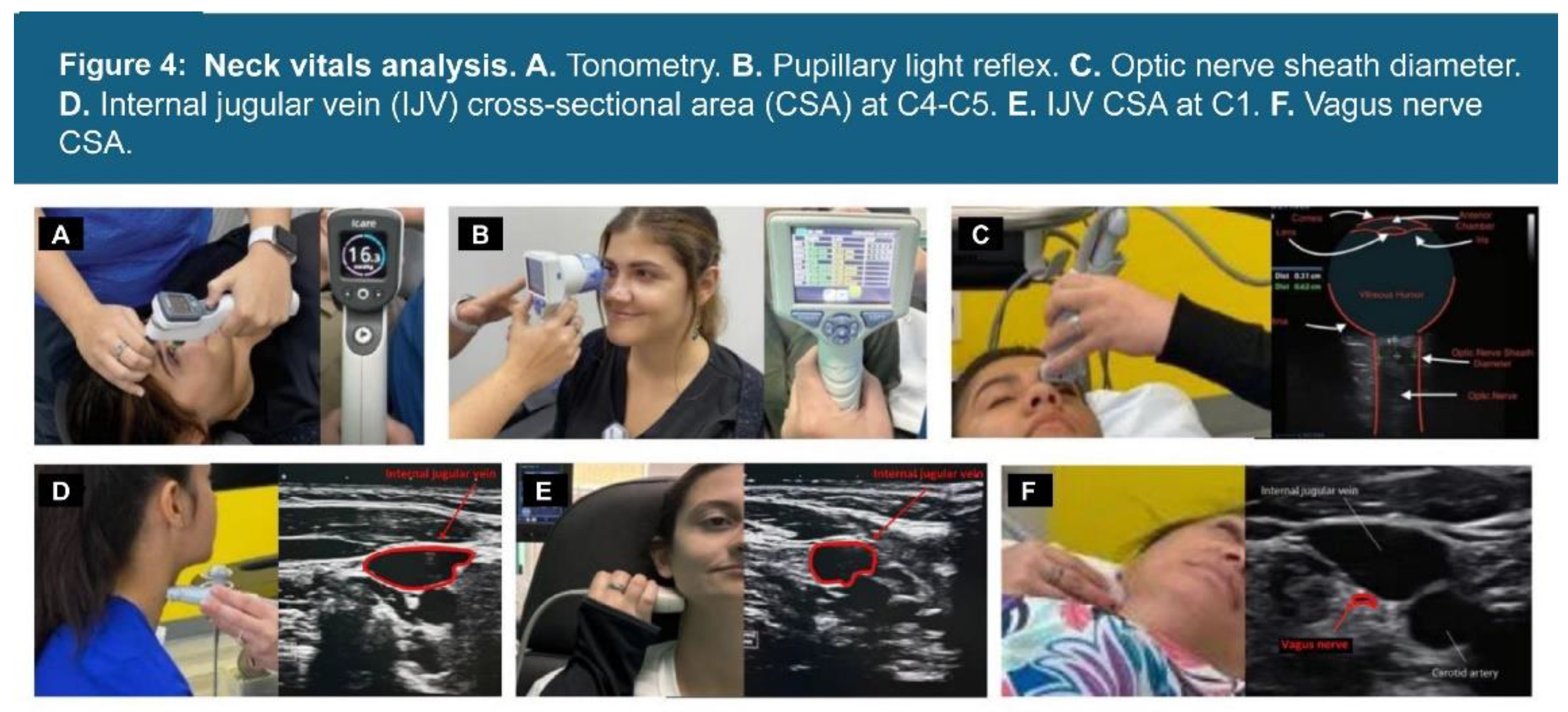
Figure 5.
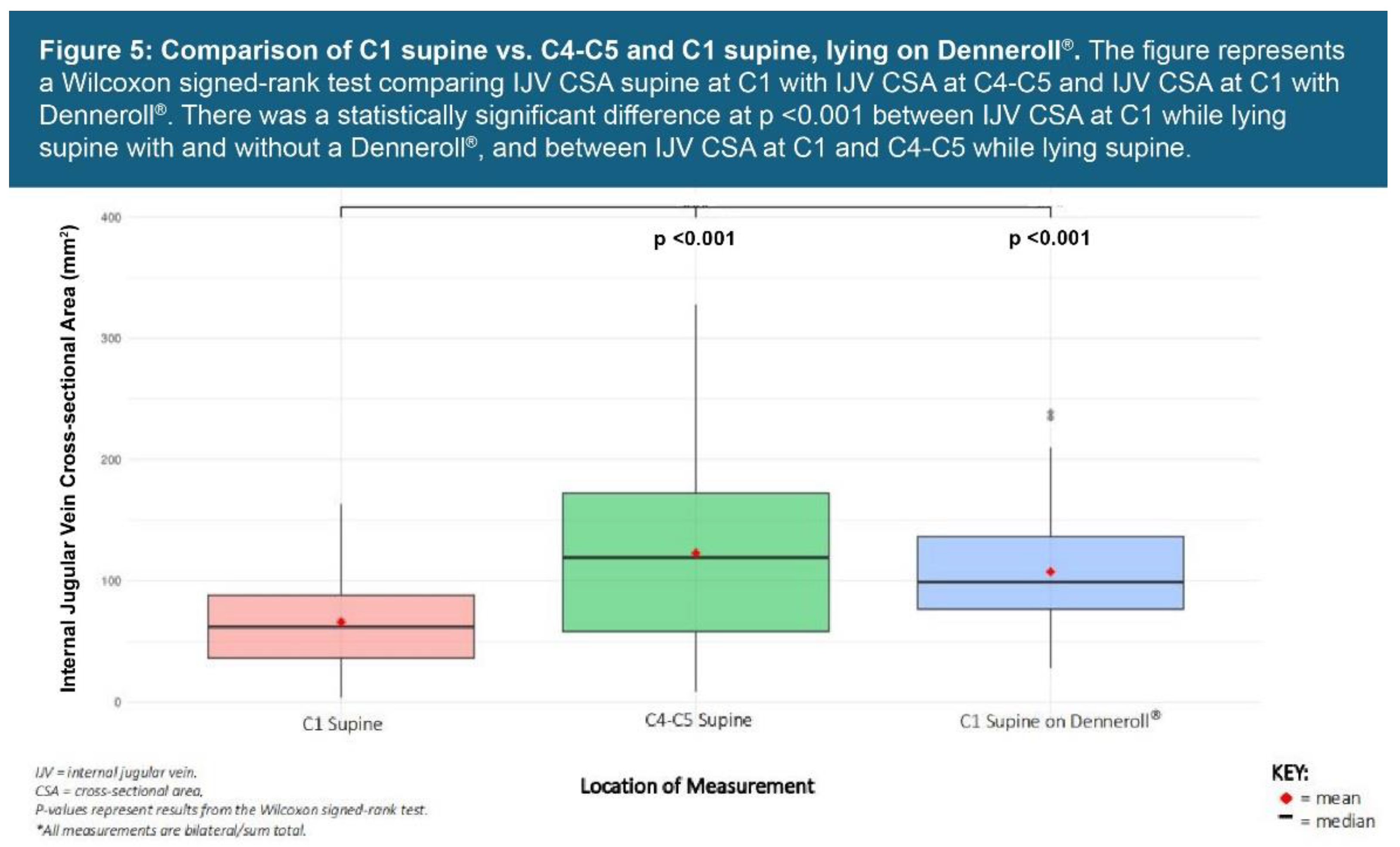
Figure 6.
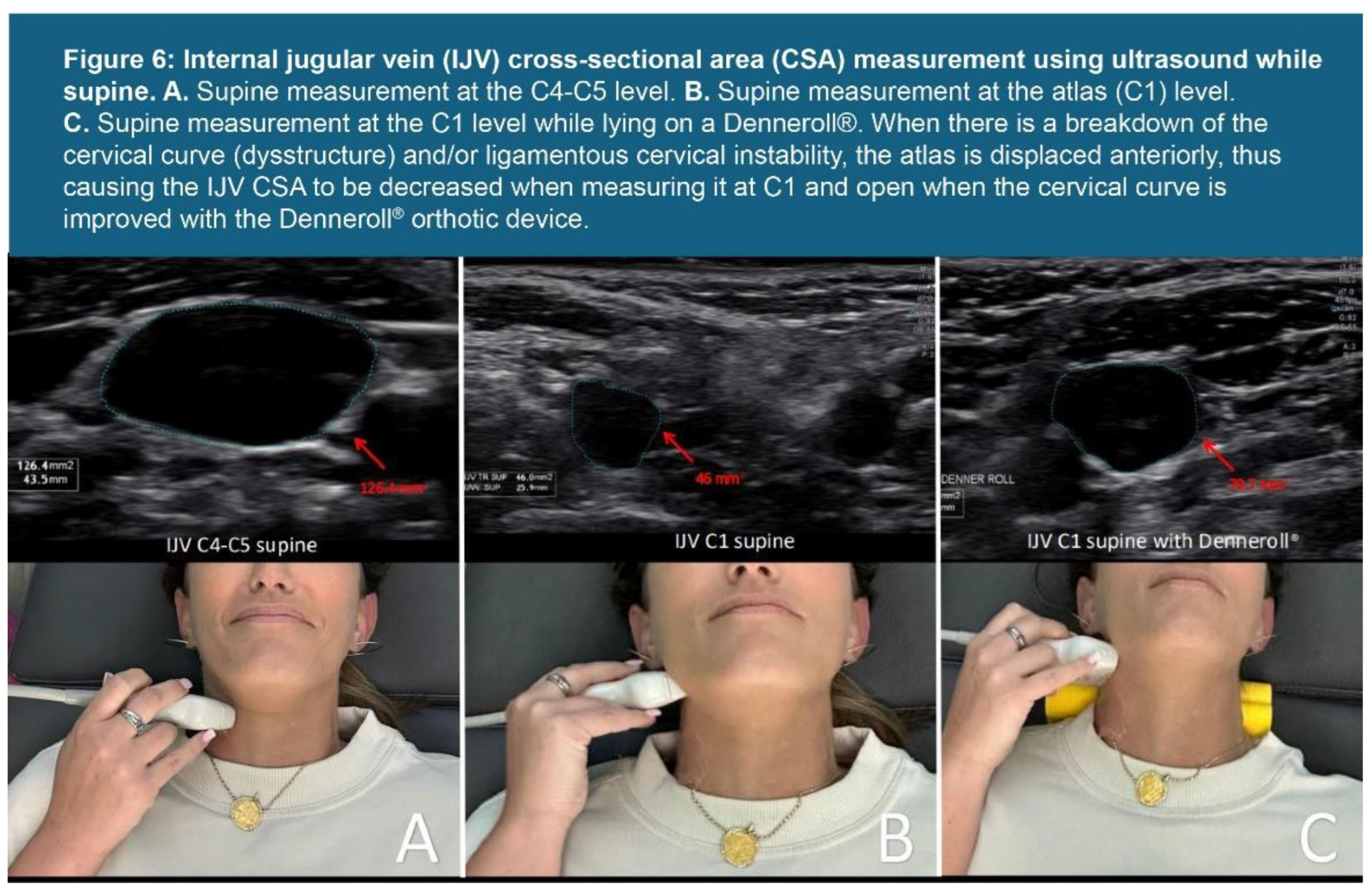
Figure 7.
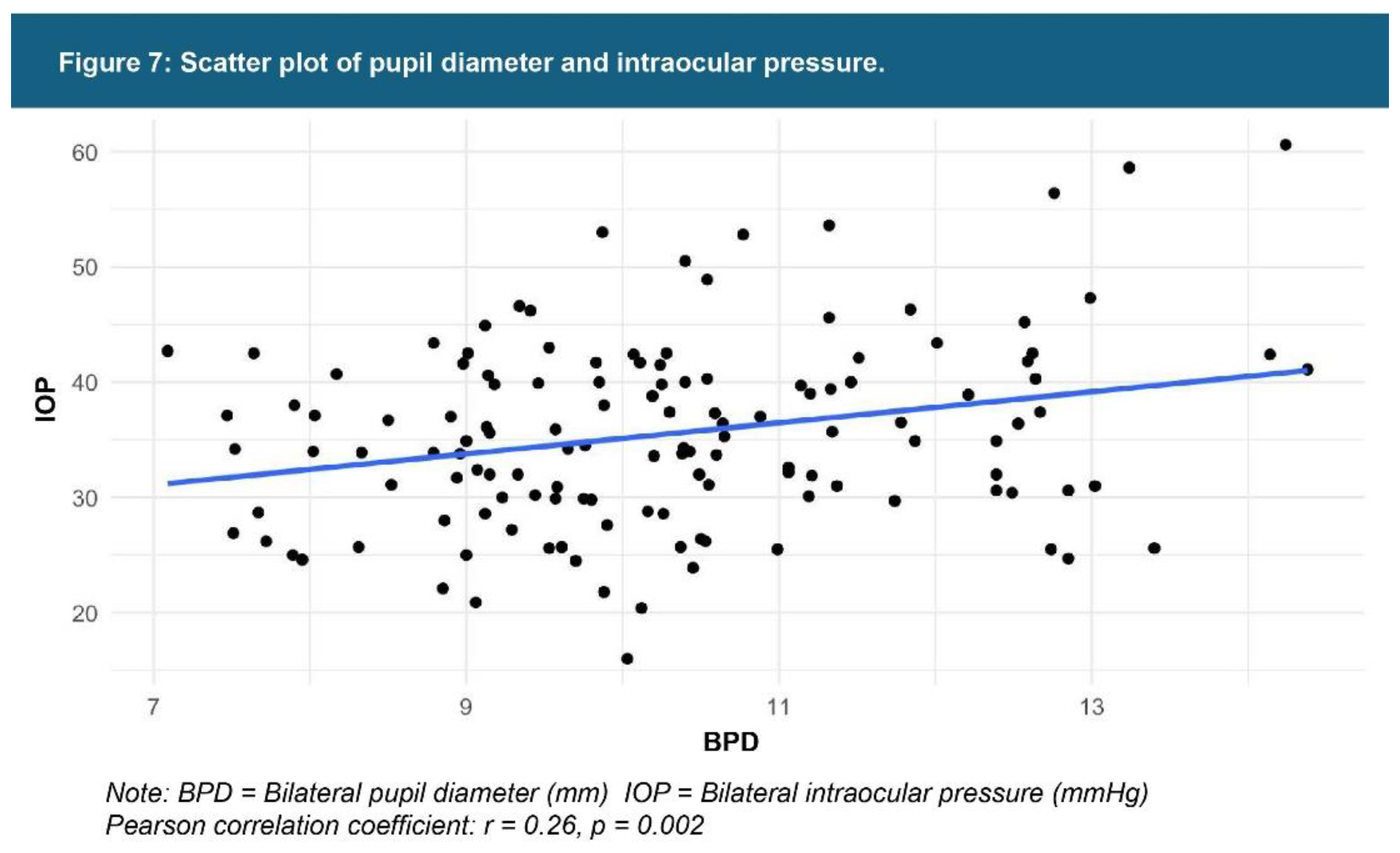
Figure 8.
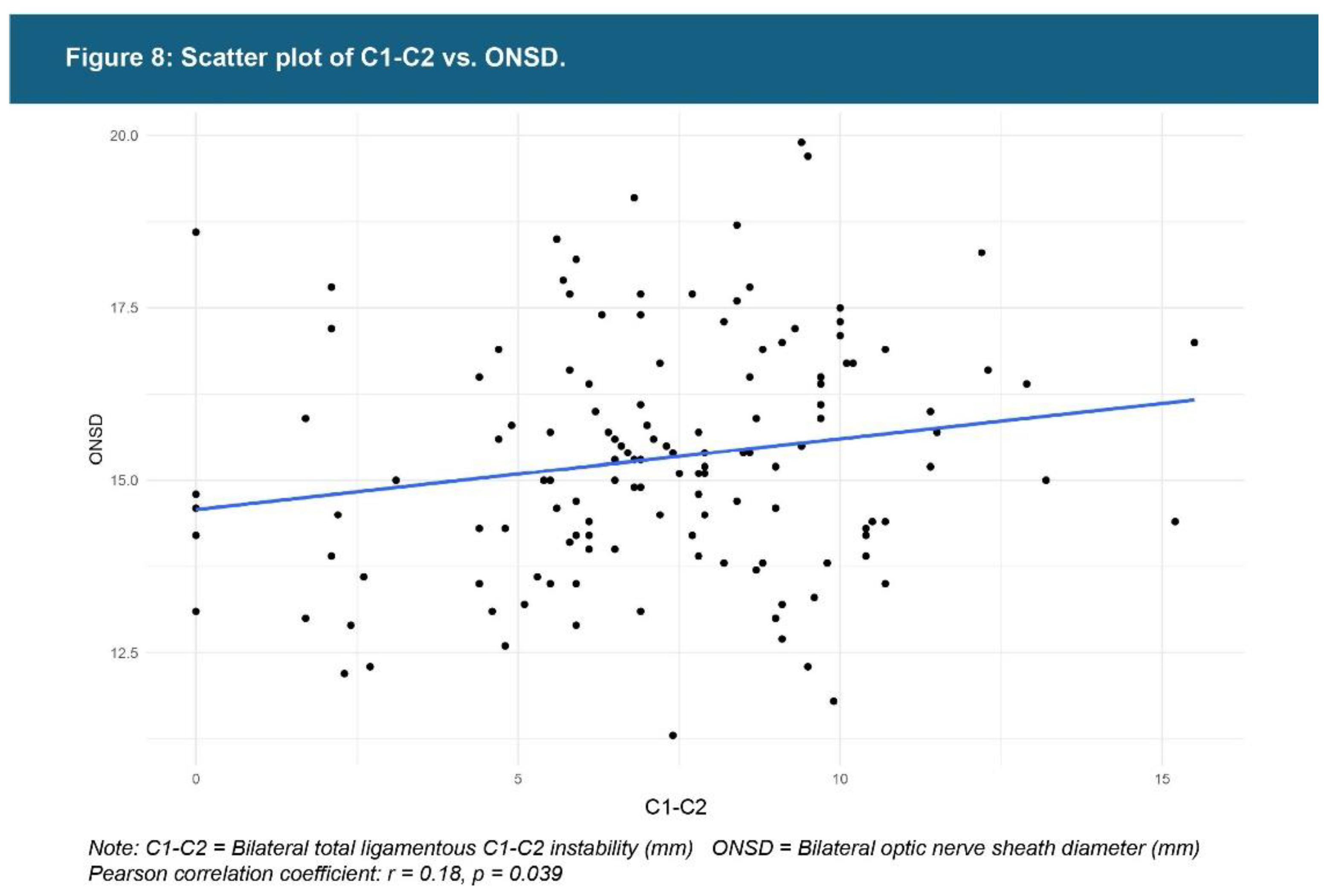
Figure 9.
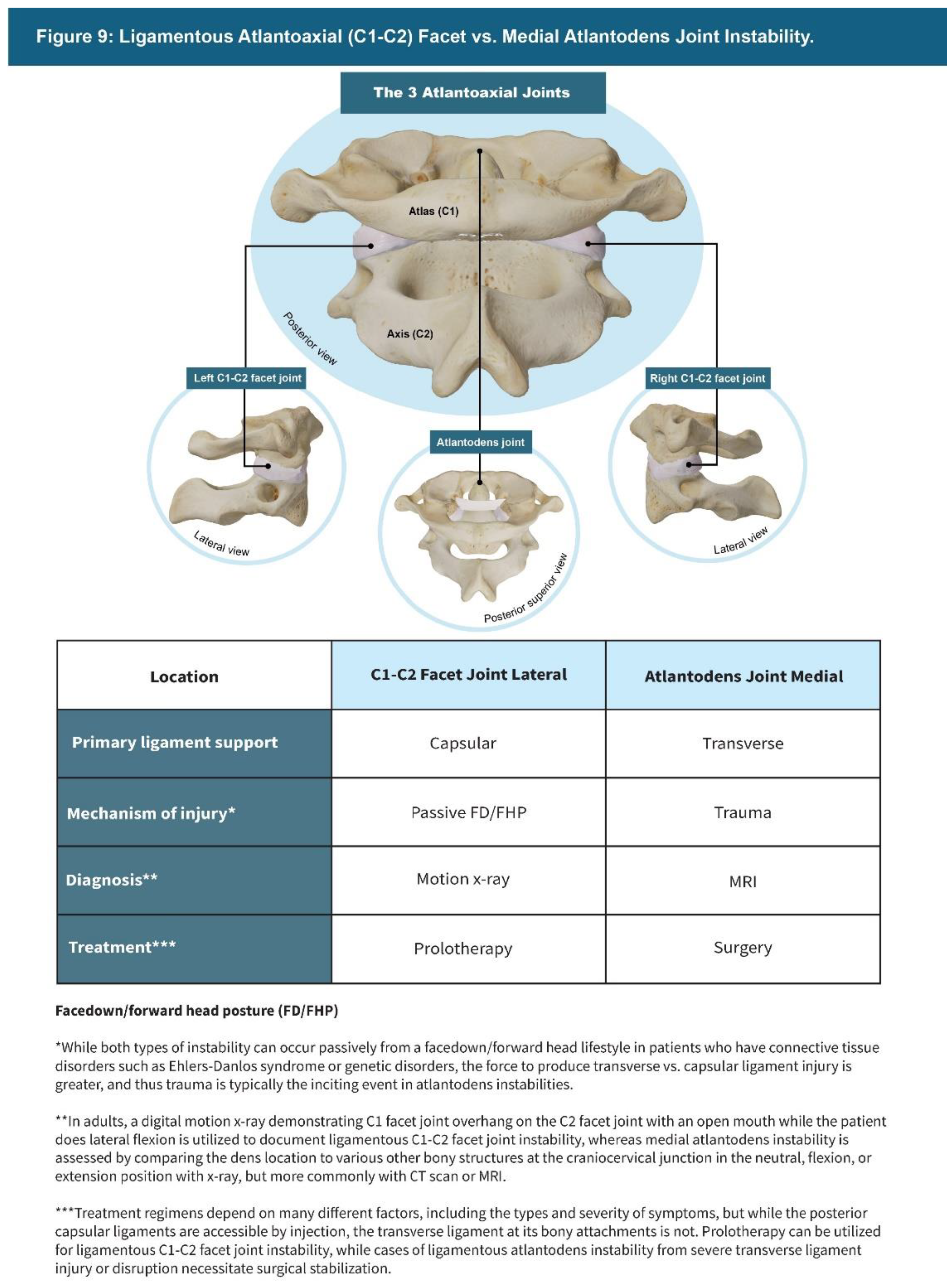
Figure 10.
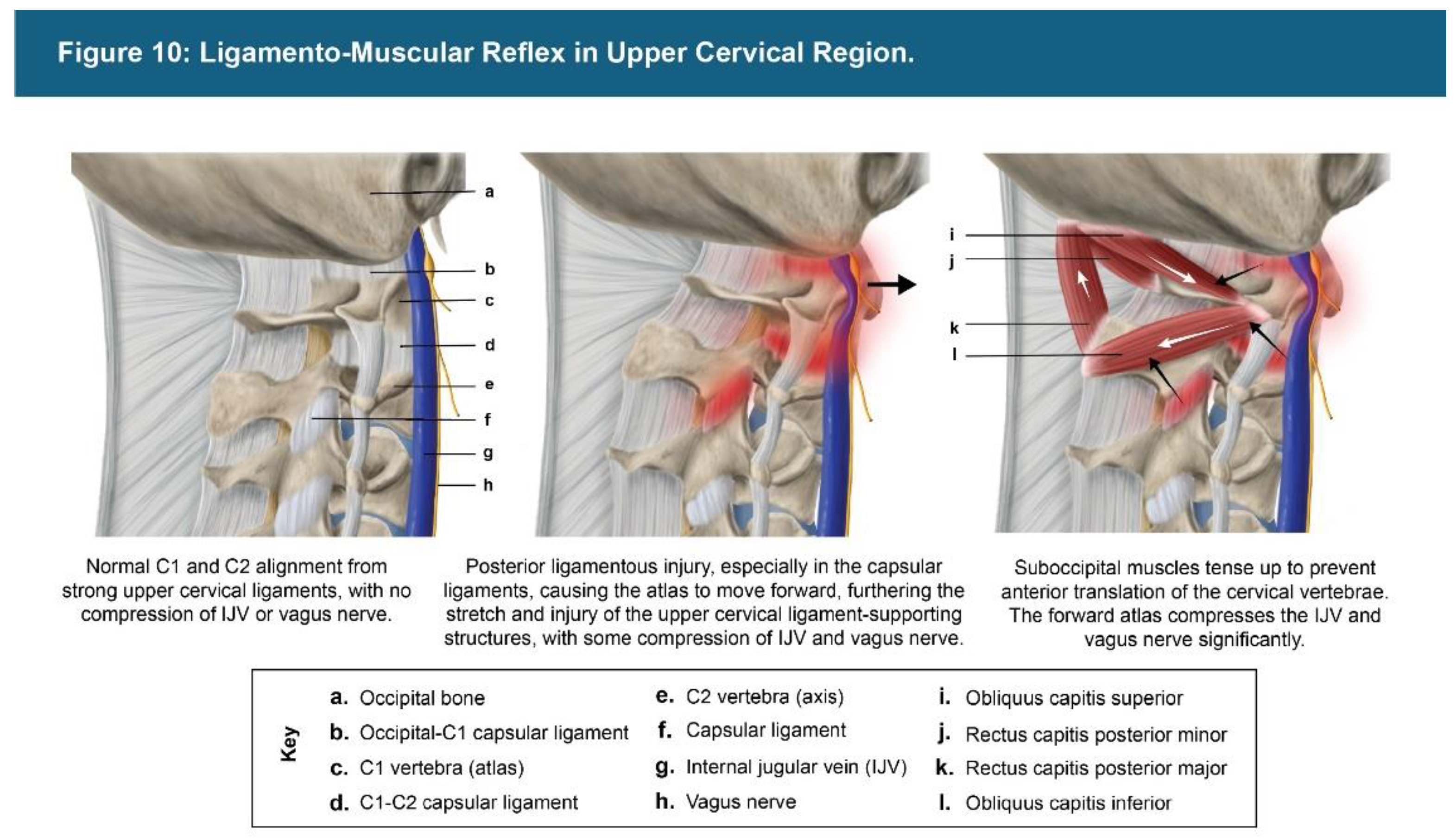
Figure 11.
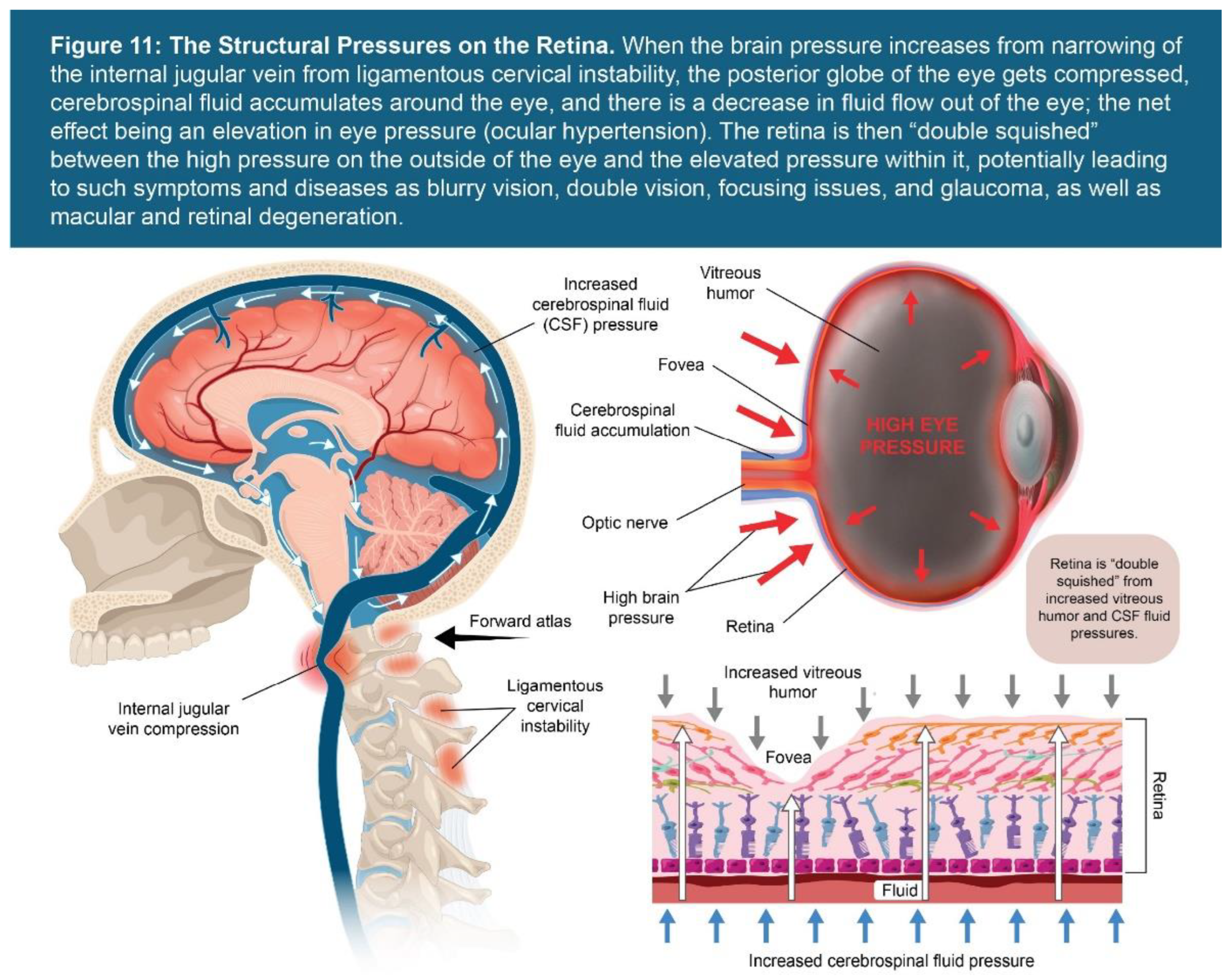
Figure 12.
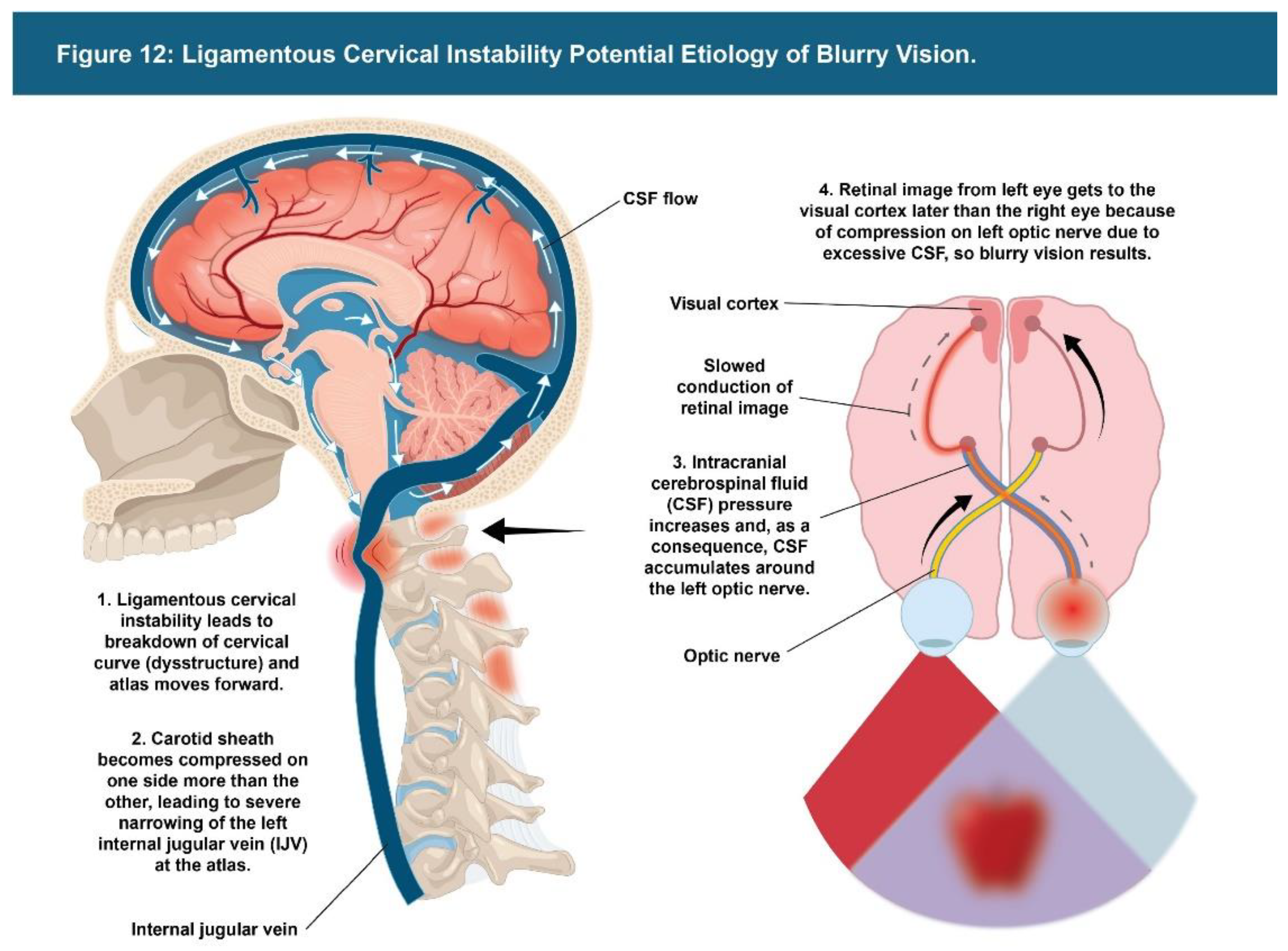
Figure 13.
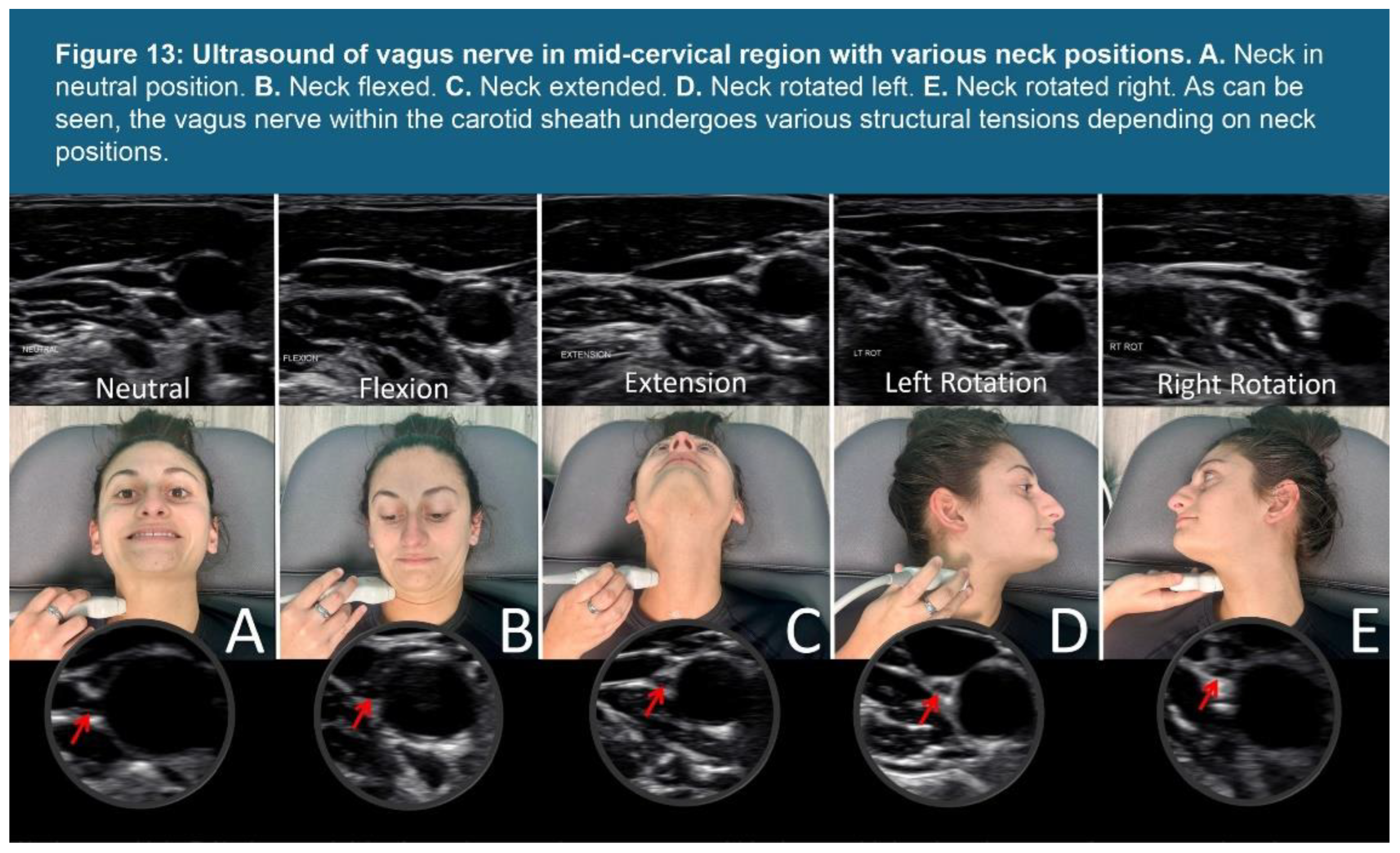
Figure 14.
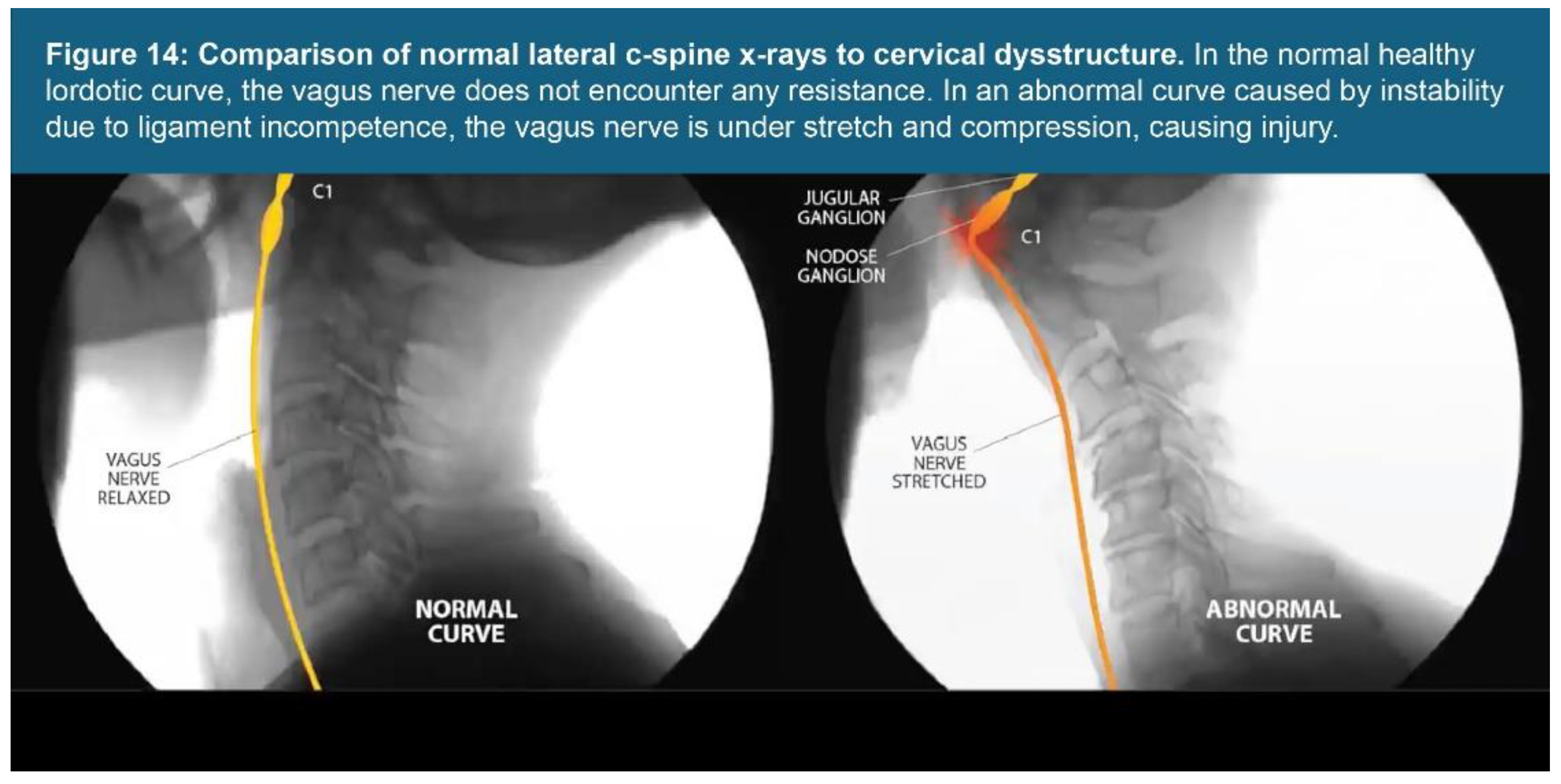
Figure 15.
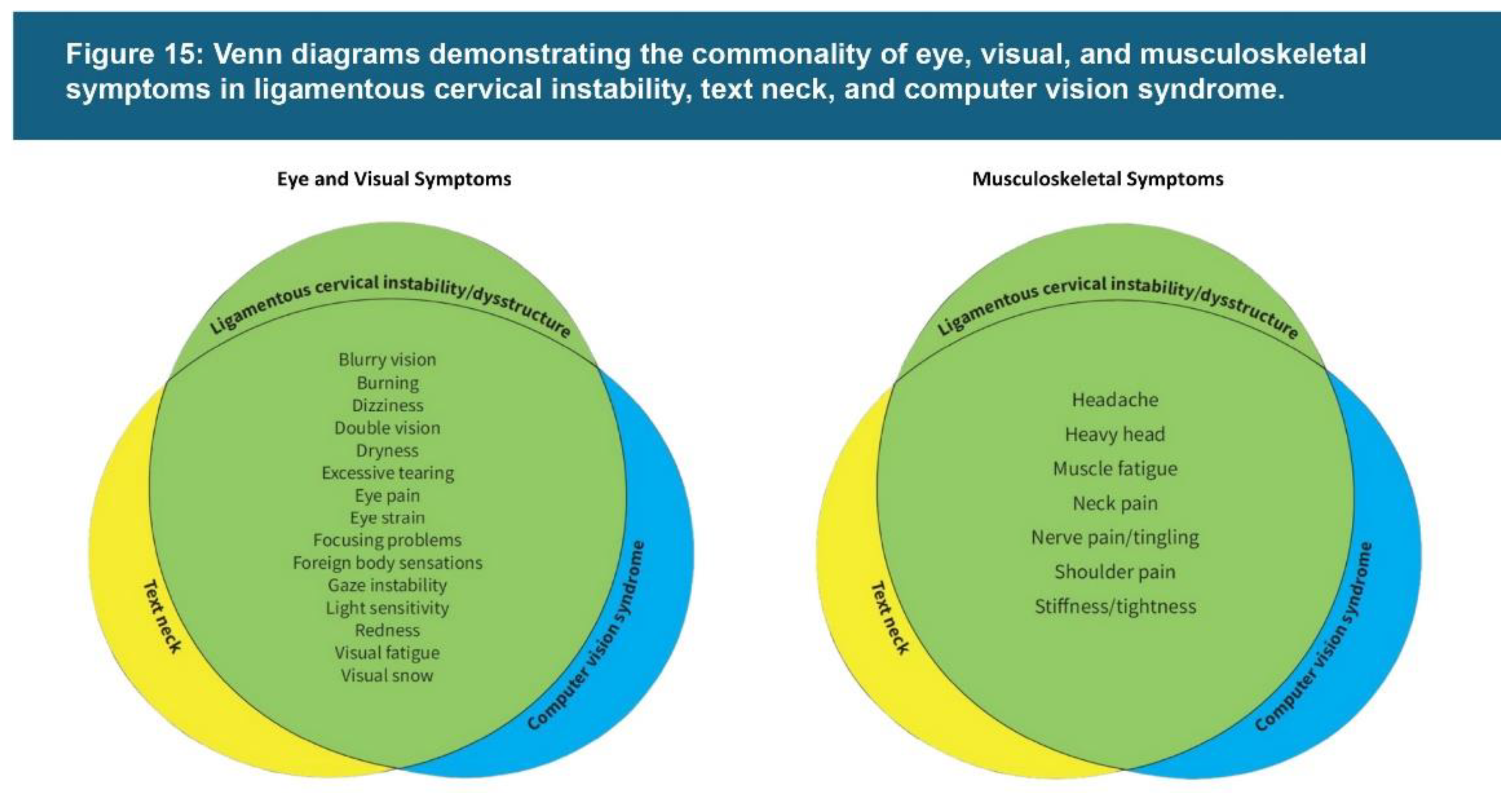
Figure 16.
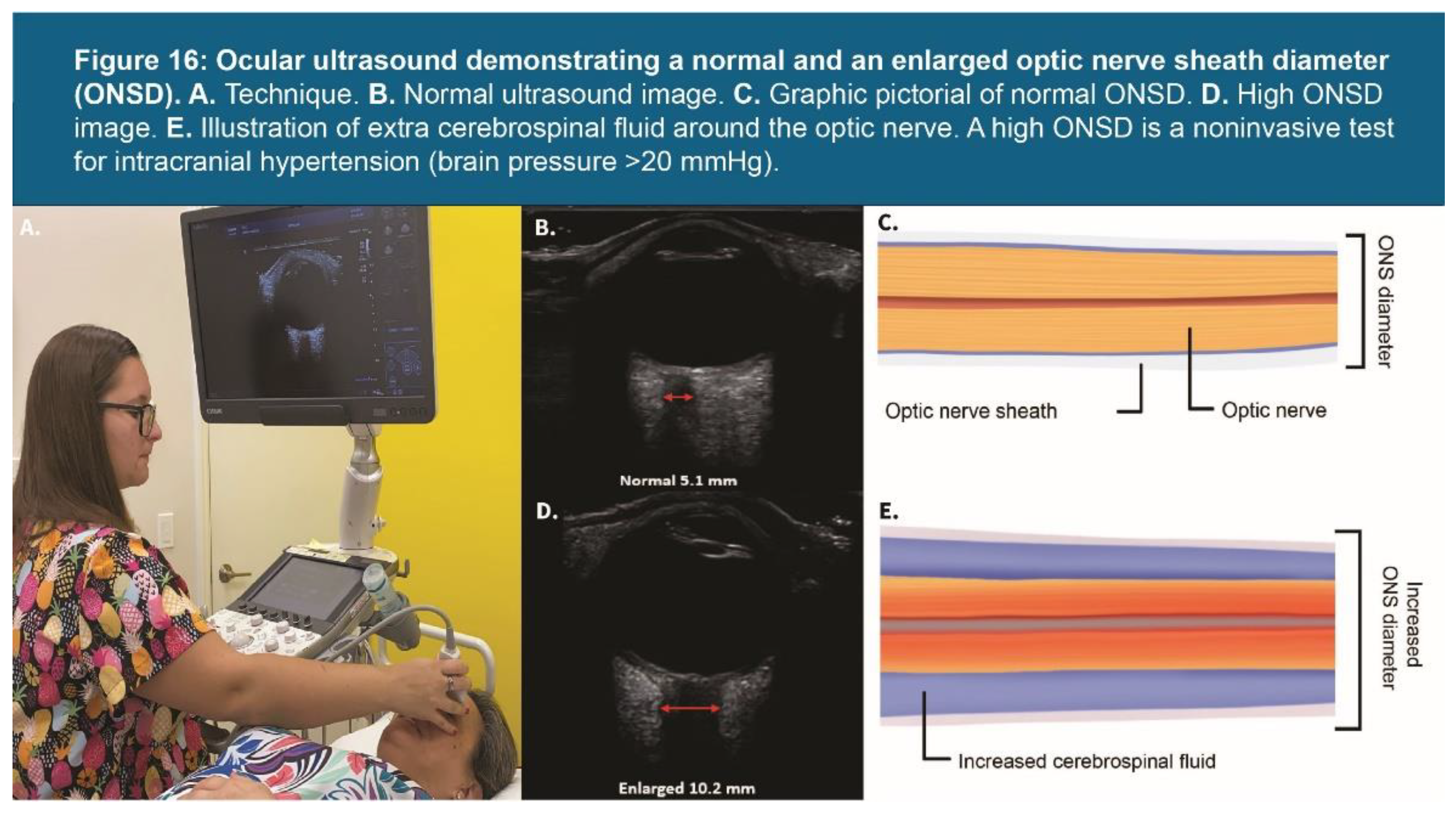
Figure 17.
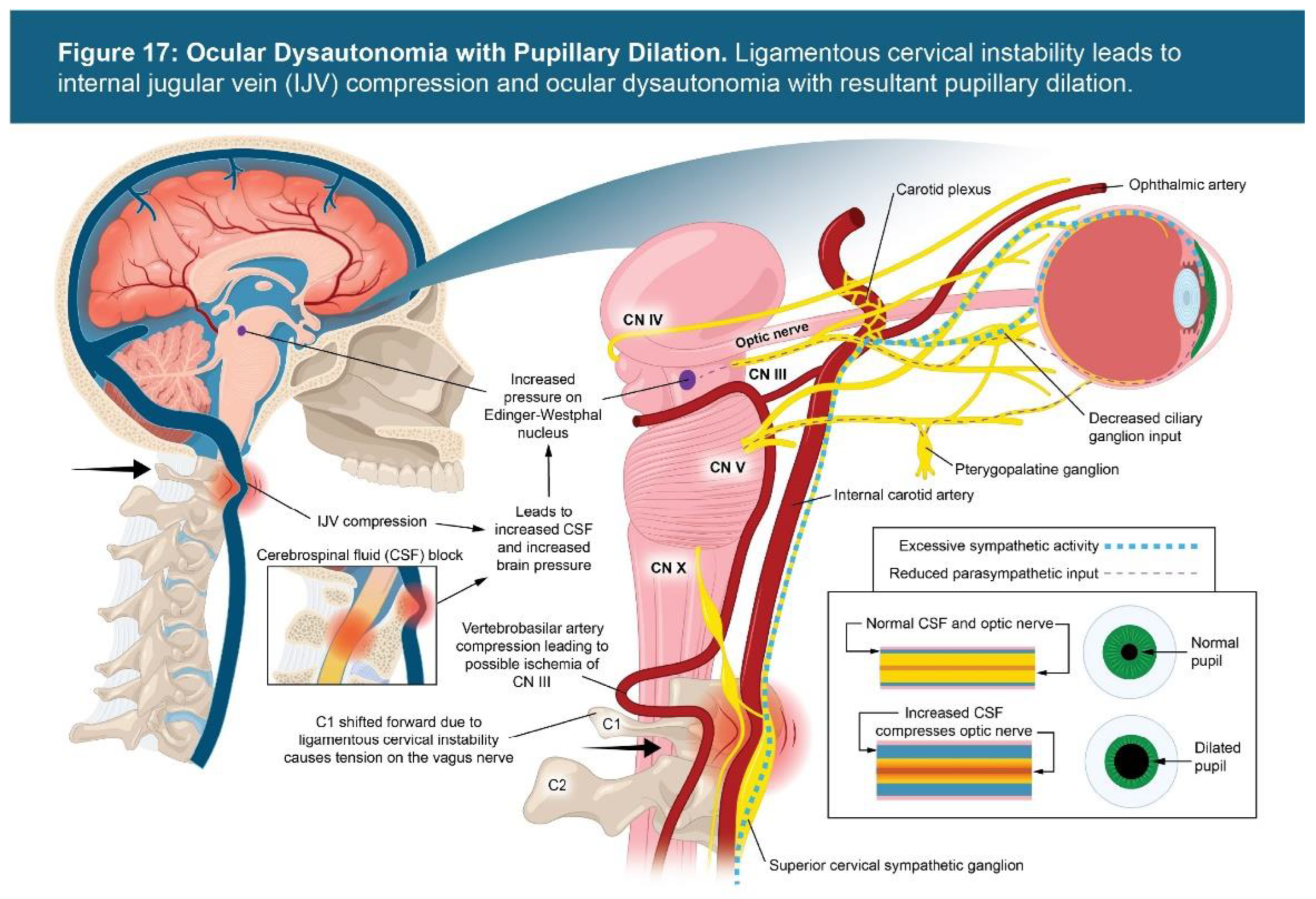

Table 1.
Neck Vitals Analysis Summary (n = 145).
| Testing Parameters | Mean | SD |
|---|---|---|
| C6AI | 41.67 mm | 14.12 |
| Depth of curve | 2.68 mm | 3.86 |
| Flexion instability total* | 4.36 mm | 3.18 |
| Extension instability total* | 4.27 mm | 3.35 |
| C1-C2 facet joint instability** | 7.19 mm | 2.98 |
| IJV C4-C5 supine** | 131.79 mm2 | 83.66 |
| IJV CSA C1 supine** | 68.94 mm2 | 37.95 |
| IJV CSA C1 supine with Denneroll® (n = 131)** |
111.20 mm2 | 48.30 |
| Vagus nerve CSA** | 2.69 mm2 | 0.82 |
| Pupil diameter** | 10.34 mm | 1.55 |
| Intraocular pressure** | 35.71 mmHg | 8.33 |
| ONSD** | 15.35 mm | 1.71 |
| Percent change (light reflex)** | 74.70% | 10.41 |
*Sum totals C2-C6. **Bilateral totals.
Table 2.
Summary of cervical structural and objective testing parameters that were abnormal in cohort of 145 patients with blurry vision.
Table 2.
Summary of cervical structural and objective testing parameters that were abnormal in cohort of 145 patients with blurry vision.
| Testing Parameters | % Abnormal Findings (Number of Patients) | Established Normal Values |
|---|---|---|
| C6AI | 100% (145) | <10 mm |
| Depth of curve (n = 144) | 89% (128) | 7-17 mm |
| C1-C2 facet joint instability* | 88% (127) | <4 mm |
| Flexion/extension instability C2-C6** | 88% (127) | <4 mm |
| Vagus nerve CSA* | 95% (138) | >4.2 mm |
| IJV CSA C1 supine* | 99% (143) | >180 mm |
| IJV C4/C5 supine* | 76% (110) | >180 mm |
| IJV CSA C1 supine with Denneroll® (n = 131)* |
90% (118) | >180 mm |
| Pupil diameter* | 92% (134) | <8 mm |
| ONSD* | 98% (142) | <12.2 mm |
| Percent change (light reflex)* | 95% (138) | <60% |
| Intraocular pressure* | 19% (28) | <42 mmHg |
* Bilateral totals. ** Total flexion and extension instability at each level from C2 through C6 (as C6-C7 was not consistently seen on DMX nor cone beam CT scan). Normal is <4 mm [21].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



