Submitted:
15 April 2025
Posted:
15 April 2025
You are already at the latest version
Abstract
Background and Objectives: Dental anxiety is a common barrier to pediatric oral care. Non-pharmacological relaxation techniques like Jacobson’s Progressive Muscle Relaxation (JPMR) and Breathing Control (BC) may help reduce psychological and physiological stress. This study assessed the utility of JPMR and BC in reducing dental anxiety and physiological arousal in children and adolescents. Materials and Methods: In this observational study, 189 participants aged 8–17 undergoing non-invasive dental procedures were assigned to JPMR (n = 63), BC (n = 63), or control (n = 63) groups. Dental anxiety was measured with the Romanian-validated IDAF-4C⁺, and physiological stress via blood pressure and heart rate. Pre- and post-intervention data were analyzed using paired t-tests, ANOVA, and cluster analysis. Results: JPMR led to the highest reductions in IDAF-4C⁺ scores (Δ = −1.23, p < 0.001, d = 1.12) and systolic blood pressure (Δ = −9.4 mmHg, p < 0.01). BC showed moderate anxiety reduction (Δ = −0.64, p < 0.05, d = 0.61) with minor physiological changes. The control group showed no significant change. Cluster analysis revealed three response patterns: (1) high anxiety–strong responders (n = 58), mainly benefiting from JPMR; (2) moderate anxiety–partial responders (n = 74); and (3) low anxiety–non-responders (n = 57). Younger age and female gender were linked to better JPMR response. Conclusions: JPMR is an effective and practical method for reducing dental anxiety and physiological stress in pediatric dental care.
Keywords:
dental anxiety
; youth
; Jacobson’s Progressive Muscle Relaxation
; Breathing Control
; physiological stress
; IDAF-4C⁺
1. Introduction
Dental anxiety (DA) is an emotion similar to fear but diffuse, anticipatory, and non-specific, manifested in the dental office. It is essential to differentiate between dental fear, dental phobia, and dental anxiety, which are three different ways of perceiving dental treatment and lead to three different types of reactions to this medical intervention [1]. Dental fear is a specific fear reaction toward a particular object or clearly defined situation within the context of dental treatment [2]. The distinction between dental anxiety and dental fear is difficult to make [1,2]. Dental phobia goes beyond fear or anxiety, leading to an avoidance behavior toward treatment, which the patient perceives as a disproportionately large threat compared to the actual situation [3].
A systematic review with meta-analysis [4] found that the overall estimated prevalence of DA was 23.9%, with a 95% confidence interval ranging from 20.4% to 27.3%. When broken down by age group, the pooled prevalence was highest among preschool-aged children at 36.5% (95% CI: 23.8–49.2), followed by school-aged children at 25.8% (95% CI: 19.5–32.1), and adolescents at 13.3% (95% CI: 9.5–17.0). A higher incidence of DA was observed in preschoolers and school-aged children with a history of dental caries and in adolescent girls.
Another systematic review [5] indicated that approximately 30% of children aged 2 to 6 years exhibited dental fear and anxiety, with the confidence interval ranging from 25% to 36%. The likelihood of experiencing DA was significantly greater in children who had never visited a dentist before (odds ratio: 1.37; 95% CI: 1.18–1.59) and in those who had a history of dental caries (odds ratio: 1.18; 95% CI: 1.09–1.27), compared to children who had previous dental visits or were free of caries.
Baier et al. [6] stated that 20% of children suffer from dental anxiety, and 21% display negative behavior during treatments. Children with negative, uncooperative behavior tend to have higher levels of dental anxiety, and those who suffer from dental anxiety exhibit negative behavior. Klingberg and Broberg [7] found that dental anxiety affects 10% of children and adolescents. This negative emotion is prevalent among children, ranging from 5.7% to 19.5%, due to differences in the studied populations and environments. Dental anxiety predominantly affects females and younger children.
Understanding the sources of dental anxiety helps to develop methods or strategies to reduce its intensity. Patients’ phobias are often related to the use of injections and needles (trypanophobia) [8], to pain [9], to the sounds made by dental drills, and to the use of handpieces and instruments [10]. Sometimes, even the smell of dental debris can trigger anxiety [10]. Patients may have a fear of choking (pseudo dysphagia) or swallowing small objects handled by the dentist during treatment [3,10].
Fear of pain causes experiences in the dental office to be perceived more intensely. Previous painful and unpleasant experiences in the dental setting, or traumatic events and feelings shared by others, influence patients. Researchers have shown that even scaling and tooth brushing can be strongly associated with the perception of pain [11]; it is the anticipation of pain during these procedures, rather than the actual pain itself, that increases patients’ anxiety levels [12]. A systematic review found a positive correlation between levels of dental anxiety and fear of dental pain [13].
Dental anxiety is a common issue in pediatric practice, modulated by various psychological and physiological factors. One of the most significant contributors is temperament, a set of stable, inherited characteristics manifesting early in life and influencing individual responses to stress [14]. As a modulator of emotional reactivity, temperament plays a key role in how children adapt to fearful or unfamiliar experiences, such as those encountered in the dental office.
Children with impulsive and highly active temperaments are more prone to treatment refusal. These children may become agitated and exhibit negative emotional responses before the clinical encounter begins. In contrast, dental anxiety is often higher in shy children, who may internalize their fear [14,15]. Consequently, the pediatric dentist or orthodontist must assess each patient’s capacity for cooperation and communication before initiating treatment, as these factors are essential to performing clinical procedures [16].
Establishing doctor-patient communication is often compromised when anxiety interferes with the child's ability to build trust with the practitioner [17]. This interference may result in exaggerated emotional responses, delay or interruption of procedures, and treatment resistance. The anticipation of pain or trauma is typically the root cause of dental anxiety [18], which in turn amplifies the perception of pain during treatment, creating a vicious cycle that has to be interrupted through appropriate intervention [19].
The dentist and patient enter this interaction from inherently different positions within a shared stress-laden context: the doctor bears professional responsibility and faces clinical challenges, and the patient is overwhelmed by uncertainty and fear [20]. A successful therapeutic alliance depends on mutual adjustment, facilitated by communication and an environment designed for minimizing stress [19,20]. For this reason, children should not wait too long before treatment begins, as prolonged anticipation exacerbates anxiety [21]. Psychologically vulnerable cases should ideally be scheduled separately to avoid transmitting distress to other patients [22].
Creating a welcoming environment in pediatric dental offices may influence children's emotional responses. Dental units shaped like animals or cartoon characters, colorful gowns (as opposed to white ones commonly associated with discomfort), and concealing anesthetic injections from the patient are all strategies that reduce anticipatory fear [23,24,25]. Observing the child’s facial expressions and body language enables the dentist to infer their psychological profile and adapt their approach accordingly. Honest communication is crucial—surprise interventions have been reported to erode trust and intensify fear. Empathy may support building rapport and fostering cooperation [26,27].
Anxiety is often a transient emotional state, reflecting a person's perception of their ability to cope with a perceived threat [27]. Its intensity can vary based on individual constitution, health history, fatigue, mood, and even family environment—whether overly permissive or excessively perfectionistic. While anxiety may arise from past negative experiences, it can also be rooted in temperament, presenting a complex interplay of innate and acquired influences.
Children can display a range of coping behaviors in the dental setting. Some are mildly anxious, remain cooperative, and employ emotion-focused strategies to manage their fears [28]. Others exhibit guarded behavior, rely on problem-solving solutions, and may present heightened physical reactivity and exaggerated emotional responses that are difficult to modulate [29].
Physiologically, anxiety activates the autonomic nervous system, particularly the sympathetic branch, resulting in measurable systemic changes. In the respiratory system, this may include hyperventilation, respiratory alkalosis, dyspnea, or sensations of choking or suffocation [30,31,32]. Cardiovascular responses such as elevated systolic and diastolic blood pressure and increased peripheral pulse are commonly associated with states of heightened anxiety [33]. These parameters may serve as objective indicators of physiological arousal and are often used in observational studies to explore associations with emotional states or behavioral strategies, including relaxation techniques [34].
Normal blood pressure (BP) values vary by age, sex, and height percentile. Table 1 shows average systolic and diastolic values, which are reasonable for children and adolescents [35]:
Heart rate (HR) values for children and adolescents, according to Kliegman et al. [35], are illustrated in Table 2:
Individual clinical assessment considers additional factors (e.g., height, physical fitness, stress, medication). These values are meant as reference averages—not strict diagnostic cutoffs.
An exception that still falls within the normal range is in athletic adolescents, who may have resting heart rates as low as 40–50 beats per minute. Heart rate increases in situations of anxiety, elevated catecholamine levels, or increased thyroid hormone levels [35].
The values described are for a state of rest. During physical exertion or stress, heart rate may rise to the upper limit of the normal range for that age.
Over the past decade, non-pharmacological interventions for managing dental anxiety in both children and adults have been getting a significant appraisal. Relaxation techniques have emerged as safe, low-cost alternatives to anxiolytic medications like benzodiazepines, which carry potential side effects [36]. The clinicians have to be responsible and minimize patient anxiety through the least invasive methods available.
In this study, we employed two techniques: the Breathing Control Technique (BC) [37,38,39,40,41,42]and Jacobson’s Progressive Muscle Relaxation (JPM) [37,38]. We selected these methods for their simplicity, utility, and accessibility.
The Breathing Control Technique is particularly beneficial during episodes of panic or acute anxiety [38,39]. Its primary goal is to relax the body and restore physiological parameters to baseline levels by rebalancing autonomic activity [38]. It interrupts the cycle of pulmonary hyperventilation and the resulting drop in blood CO₂ that can trigger panic symptoms [38,39,40].
The patient is comfortably seated with full body support, allowing for optimal relaxation of the muscles. The dentist gently guides the child to inhale slowly through the nose over three to four seconds and then exhale calmly over four seconds, either through the nose, mouth, or both, depending on what feels most natural. Breathing should be diaphragmatic to encourage oxygen-carbon dioxide exchange and reduce sympathetic nervous system activity [40,42]. This practice, typically lasting between five and eight minutes, helps lower physiological markers of anxiety and improves cooperation. Supporting the technique with a calm voice and, optionally, soft background music enhances its soothing effect [39]. The effects of controlled breathing in reducing dental anxiety in children have clinical evidence. A study by Peretz and Gluck [41] demonstrated that structured breathing techniques significantly reduced anxiety levels in pediatric patients during dental treatment, suggesting this method is an accessible and efficient behavior management strategy in clinical practice [42].
Jacobson’s Progressive Muscle Relaxation, developed by Edmund Jacobson in the early 20th century, involves systematically tensing and relaxing different muscle groups to promote deep physical and psychological relaxation [3]. This method requires individuals to intentionally tense specific muscle groups for 6-10 seconds, followed by a gradual conscious release of that tension for 15-20 seconds. The technique is repeated in cycles, helping the patient to be aware of the contrast between muscular tension and relaxation, eventually leading to a full-body calming effect. When learned, JPM takes approximately 15 minutes and can have a profound result because it alleviates muscular tension and reduces anxiety-induced physiological responses (Appendix A) [3].
JPM works through both “top-down” and “bottom-up” neurological mechanisms. The “top-down” aspect involves the brain’s higher processing centers—such as the cerebral cortex—which consciously initiate the muscle contractions and subsequent relaxation [37,38]. In contrast, the “bottom-up” process begins with sensory feedback from the muscles, which travels through the spinal cord and brainstem, stimulating calming responses in the central nervous system [36]. This dual mechanism helps induce rapid and noticeable relief from stress and tension.
Both techniques are non-invasive, practical, and applicable in a pediatric dental setting, contributing to better patient cooperation and easier dental care.
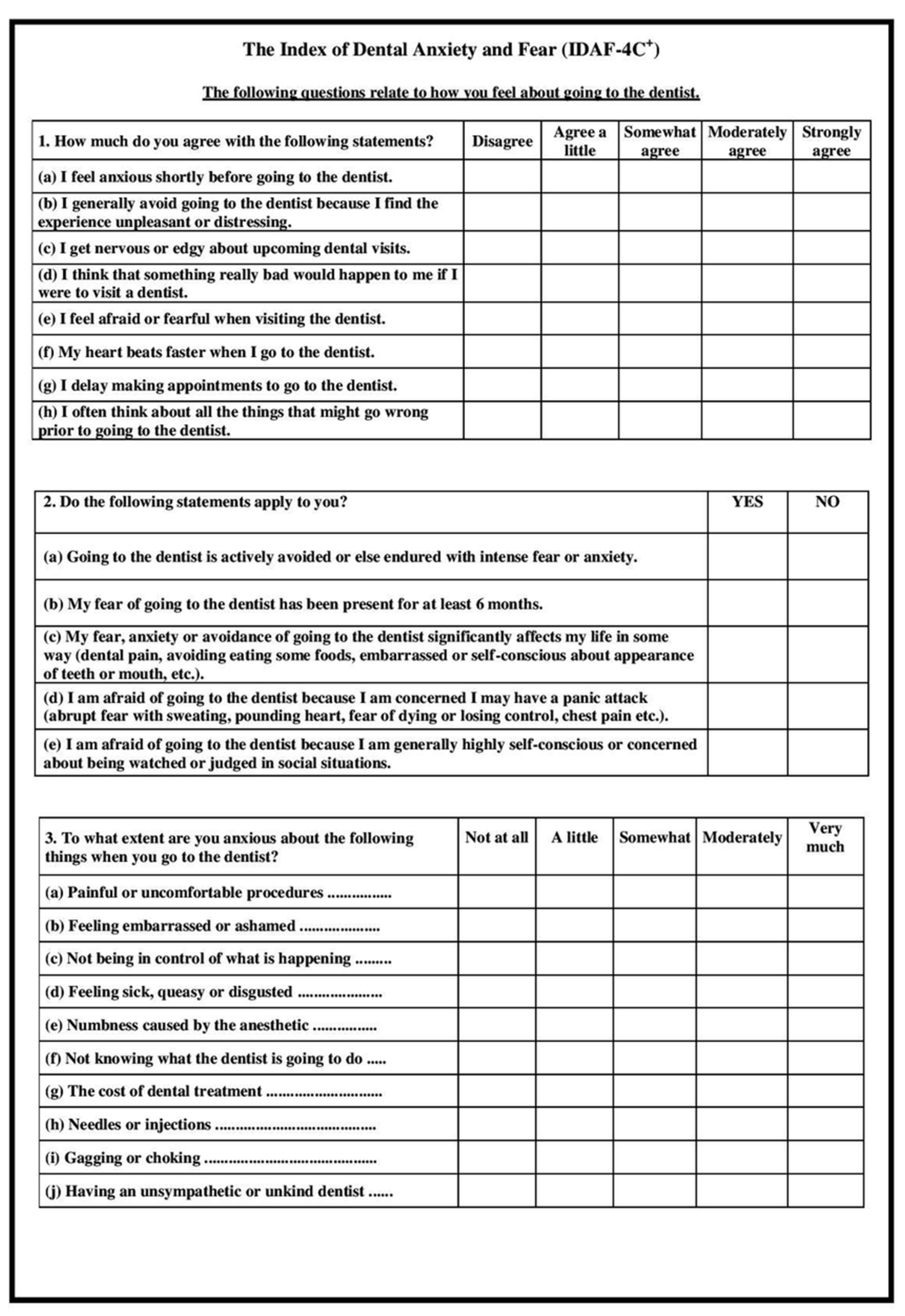
The IDAF-4C+ (Index of Dental Anxiety and Fear) questionnaire, initially formulated by Armfield [43], serves as a standardized tool to assess individuals’ levels of dental-related fear and anxiety. It comprises three distinct components: the core section, a stimuli-based section, and a phobia-focused module. The core component investigates four domains—cognitive, behavioral, emotional, and physiological reactions—through a series of items rated on a five-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree).
The stimuli section gauges the intensity of anxiety triggered by ten specific dental-related situations, also using a five-level scale that spans from "not at all" to "very much" [43]. Meanwhile, the phobia section includes five binary (yes/no) items to identify signs of dental phobia.
Scoring is derived solely from the core section, calculated by averaging the participants' responses. A threshold value of 3 distinguishes between individuals with and without dental anxiety: scores below 3 suggest no significant anxiety, and scores of 3 or above indicate the presence of dental anxiety [43,44].
There is a validated Romanian version of the Index of Dental Anxiety and Fear (IDAF-4C+). A study published in July 2023 assessed its psychometric properties and found that the Romanian version demonstrated good internal validity, with a Cronbach's alpha of 0.945, and strong convergent validity, showing positive correlations with the Dental Anxiety Scale and a single-item measure of dental fear. This suggests that the Romanian IDAF-4C+ is a reliable and valid instrument for assessing dental anxiety and fear in the Romanian population [45].
This study aimed to evaluate the effects of two relaxation techniques, Breathing Control, and Jacobson’s Progressive Muscle Relaxation, on patients’ anxiety in the dental office and compare their utility in reducing anxiety, as indicated by psychological changes investigated by IDAF-4C+ use, and physiological markers such as blood pressure and heart rate.
2. Materials and Methods
Study Design
This observational study investigated the associations between two psychological relaxation techniques—Breathing Control (BC) and Jacobson’s Progressive Muscle Relaxation (JPMR)—and levels of dental anxiety and physiological stress among children and adolescents. The study was conducted at Dimitrie Cantemir University’s Dental Clinic between October 2023 and March 2025.
Participants were observed in three naturally formed groups:
- ▪
- Group A (Breathing Control) practiced guided diaphragmatic breathing before dental treatment.
- ▪
- Group B (JPMR) received a brief structured muscle relaxation session before treatment.
- ▪
- The Control Group received standard dental care with no relaxation intervention.
Participants
Inclusion Criteria
- ▪
- Children and adolescents aged 8–17 years;
- ▪
- Scheduled for non-invasive prophylactic dental procedures;
- ▪
- Fluent in Romanian or able to follow instructions with minimal support;
- ▪
- Provided informed consent (by parent/guardian) and assent (by the child).
Exclusion Criteria
- ▪
- Diagnosed cognitive or developmental disorders;
- ▪
- Ongoing psychiatric treatment or use of anxiolytic medication;
- ▪
- Acute dental pain or emergency treatment needs.
Ethical Considerations
Our observational study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of ”Dunărea de Jos” University (no. 40541/CEU/2024). Participation was voluntary, with signed consent from guardians and assent from minors.
Group Allocation and Data Collection
Participants were allocated to groups based on scheduling availability and clinic flow, ensuring balanced demographic distribution. Due to the nature of the interventions, neither participants nor providers were blinded. However, outcome assessments were conducted by trained, independent evaluators following standardized protocols.
Psychological Measures
Dental Anxiety was measured using the Romanian-validated version of the Index of Dental Anxiety and Fear (IDAF-4C⁺) with :
- ▪
- Core module (8 items) that evaluate emotional, behavioral, cognitive, and physiological anxiety dimensions using a 5-point Likert scale.
- ▪
- Interpretation: a mean score ≥3 indicates clinically significant dental anxiety.
Physiological Measures
Blood Pressure (BP) and Heart Rate (HR) were recorded using a validated pediatric automatic monitor under resting conditions:
- ▪
- Baseline: Measured before intervention or procedure;
- ▪
- Post-intervention: Measured immediately after the dental treatment.
Intervention Protocols
- ▪
- Group A (BC): 5-minute diaphragmatic breathing session guided by trained personnel; participants were instructed to inhale deeply through the nose and exhale slowly through the mouth, with hand-on-abdomen for tactile feedback.
- ▪
- Group B (JPMR): 10-minute JPMR session guided by audio and an assistant; focused on sequential tensing and relaxing muscle groups (hands, arms, shoulders, face, legs), emphasizing the contrast between tension and relaxation.
- ▪
- The Control Group received routine dental care without any relaxation technique.
Procedure Overview
-
Initial Assessment:
- ▪
- IDAF-4C⁺ administered;
- ▪
- Baseline BP and HR recorded.
-
Intervention:
- ▪
- Groups A and B received respective relaxation interventions;
- ▪
- The control group proceeded directly to treatment.
-
Post-Treatment Assessment:
- ▪
- IDAF-4C⁺ re-administered;
- ▪
- Post-treatment BP and HR measured.
All sessions were conducted in a quiet, adjacent room under researcher supervision.
Data Analysis
Software: IBM SPSS Statistics for Windows, Version 29.0 (IBM Corp., Armonk, NY, USA), which includes built-in support for both Python 3.10.4 and R 4.2.0, enhancing its capabilities for advanced statistical modeling and custom analyses.
Descriptive Statistics: frequencies for categorical variables; means ± SD or medians with IQR for continuous data.
Inferential Statistics:
- ▪
- Paired t-tests assessed within-group pre-post changes.
- ▪
- ANOVA with Tukey’s post-hoc tests evaluated between-group differences.
- ▪
- Effect sizes (Cohen’s d) reported where applicable.
Cluster Analysis:
- ▪
- Hierarchical clustering (Ward’s linkage, Euclidean distance) based on IDAF-4C⁺, BP, HR, age, and gender;
- ▪
- Cluster validity was evaluated using silhouette scores and elbow method.
Reliability: Internal consistency of the IDAF-4C⁺ assessed via Cronbach’s alpha (α ≥ 0.70 considered acceptable).
Missing Data:
- ▪
- Exclusion of cases with >10% missing data;
- ▪
- <5% missingness handled via multiple imputation;
- ▪
- Outliers managed using z-scores and Mahalanobis distance.
3. Results
3.1. Participants:
A total of 189 children and adolescents were included, with equal distribution across groups:
- ▪
- Group A (BC): n = 63
- ▪
- Group B (JPMR): n = 63
- ▪
- Control Group: n = 63

Table 3.
Demographic Characteristics and Baseline Anxiety.
| Variable | Group A (BC) | Group B (JPMR) | Control | p-value |
|---|---|---|---|---|
| Age (mean ± SD) | 12.4 ± 2.5 | 12.6 ± 2.4 | 12.5 ± 2.6 | 0.88 |
| Gender (M/F) | 34 / 29 | 32 / 31 | 33 / 30 | 0.94 |
| Baseline IDAF-4C⁺ | 3.32 ± 0.41 | 3.33 ± 0.44 | 3.31 ± 0.40 | 0.92 |
No significant baseline differences were observed.
3.2. Within-Group Comparisons
Table 4.
Pre- vs. Post-Intervention Outcomes (Paired t-tests).
| Measure | Time | BC (Group A) | JPMR (Group B) | Control |
|---|---|---|---|---|
| IDAF-4C⁺ | Pre | 3.32 ± 0.41 | 3.33 ± 0.44 | 3.31 ± 0.40 |
| Post | 3.02 ± 0.43 ✱ | 2.64 ± 0.39 ✱✱ | 3.28 ± 0.38 | |
| Systolic BP (mmHg) | Pre | 108.9 ± 7.8 | 109.1 ± 7.5 | 108.4 ± 8.0 |
| Post | 105.7 ± 7.2 ✱ | 102.2 ± 6.9 ✱✱ | 107.6 ± 7.9 | |
| Heart Rate (bpm) | Pre | 91.0 ± 9.3 | 91.5 ± 8.8 | 90.7 ± 9.1 |
| Post | 87.6 ± 8.6 ✱ | 83.1 ± 8.1 ✱✱ | 90.2 ± 9.3 |
✱ p < 0.05; ✱✱ p < 0.01 (within-group comparison).
Reductions in anxiety and physiological indicators were more pronounced in the JPMR group.
3.3. Between-Group Comparisons
Table 5.
Post-intervention outcomes (ANOVA and Effect Sizes).
| Outcome | ANOVA p | Significant Post-hoc | Effect Size (Cohen’s d) |
|---|---|---|---|
| IDAF-4C⁺ Score | < 0.001 | JPMR < BC < Control | JPMR vs. BC = 0.70 |
| Systolic BP | 0.041 | JPMR < Control | JPMR vs. Control = 0.62 |
| Heart Rate | 0.053 | – (trend only) | – |
JPMR produced the greatest reductions in dental anxiety scores (IDAF-4C⁺: Δ = −1.23, 95% CI: −1.36 to −1.10, p < 0.001; Cohen’s d = 1.12, 95% CI: 0.89–1.34), followed by BC (Δ = −0.64, 95% CI: −0.79 to −0.48, p < 0.05; Cohen’s d = 0.61, 95% CI: 0.39–0.83).
3.4. Cluster Analysis: Individual Response Patterns
Method: Hierarchical clustering using Ward’s method on combined psychological and physiological data. Validation: Silhouette score = 0.64
Table 6.
Cluster Characteristics.
| Cluster | Key Traits | n | Most common group |
|---|---|---|---|
| Cluster 1 | High anxiety; strong reduction post-JPMR; younger, more females | 58 | JPMR |
| Cluster 2 | Moderate anxiety; partial responders | 74 | Mixed |
| Cluster 3 | Low anxiety; non-responsive | 57 | Control & BC |
Table 7.
Cluster Summary.
| Cluster | Baseline IDAF | Post IDAF | Δ Systolic BP | Δ HR | Age Range | Gender Trend |
| Cluster 1 | 3.91 | 2.38 | -9.4 mmHg | -6.5 bpm | 8–12 yrs | More females |
| Cluster 2 | 2.91 | 2.54 | -3.2 mmHg | -2.4 bpm | 10–14 yrs | Balanced |
| Cluster 3 | 2.34 | 2.30 | -0.8 mmHg | -0.5 bpm | 13–17 yrs | Balanced |
Interpretation
:
- ▪
- Cluster 1 showed significant improvement primarily in the JPMR group.
- ▪
- Cluster 2 included mixed responders with moderate improvements.
- ▪
- Cluster 3 comprised minimally responsive participants with low initial anxiety.
A heatmap visualization (Figure 1) further emphasized the differential impact of interventions across clusters.
4. Discussion
This study assessed the efficacy of two non-pharmacological interventions—Jacobson’s Progressive Muscle Relaxation (JPM) and Breathing Control (BC)—in managing dental anxiety and physiological stress markers (blood pressure and heart rate) among children and adolescents aged 8–17. A total of 189 participants were equally allocated into three groups: JPM, BC, and standard care (control). Using a culturally validated Romanian version of the IDAF-4C⁺, alongside physiological indicators, we observed meaningful patterns of anxiety reduction and response variability across both interventions.
JPM emerged as the most effective intervention, producing a mean IDAF-4C⁺ score reduction of 1.23 points (p < 0.001) and a large effect size (Cohen’s d = 1.12). This substantial improvement reflects JPM's holistic impact on both somatic and cognitive-emotional dimensions of anxiety. Moreover, physiological responses confirmed these findings, with systolic blood pressure decreasing by 9.4 mmHg on average (p < 0.01) and moderate reductions in heart rate, suggesting a shift toward parasympathetic nervous system dominance—a hallmark of somatic de-arousal. These outcomes are consistent with prior studies emphasizing JPM’s utility in procedural anxiety settings in children and adolescents [37,46], and they extend this evidence to a Romanian pediatric population using validated psychometric tools.
The BC intervention also led to significant reductions in anxiety (mean Δ = 0.64, p < 0.05), with a moderate effect size (Cohen’s d = 0.61). However, these effects were consistently smaller than those achieved through JPM. While slight declines in heart rate were observed, no statistically significant changes in blood pressure were noted. This profile reflects BC’s narrower therapeutic mechanism, emphasizing autonomic modulation through respiratory control, without the full-spectrum cognitive and somatic engagement characteristic of JPM [37,38]. As such, BC may serve as a valuable intervention for children with mild anxiety profiles or in resource-limited settings where brief interventions are needed.
The control group, which received routine dental care without psychological intervention, showed no significant changes in IDAF-4C⁺ scores or physiological indicators. This result underscores the necessity of incorporating structured anxiety-reduction techniques into pediatric dental care, particularly for patients with pre-existing anxiety.
Heart rate and blood pressure reductions followed a similar pattern. While both interventions contributed to improvements, only JPM achieved statistically significant inter-group differences in BP. The absence of significant HR differences between groups despite within-group improvements, might be explained by inter-individual variability, younger participants' baseline cardiovascular dynamics, or the shorter exposure to interventions.
To explore response heterogeneity, hierarchical agglomerative clustering was applied to standardized pre-to-post changes in IDAF-4C⁺, systolic/diastolic blood pressure, and heart rate across all participants. The three-cluster solution offered nuanced, clinically relevant insights:
Cluster 1 – “high anxiety – strong responders” (n = 58): participants in this group showed the most reduction in IDAF-4C⁺ (mean from 3.91 to 2.38), along with significant physiological improvements. Predominantly composed of JPM participants (62%), this cluster included younger adolescents (8–12 years) and a higher proportion of females—demographic factors often associated with increased dental fear and greater reactivity to relaxation techniques [47,48]. These children likely exhibit heightened baseline anxiety and respond to multi-modal relaxation techniques that engage both cognitive and somatic components, such as JPM.
Cluster 2 – “moderate anxiety – partial responders” (n = 74) across all study groups, these participants presented with moderate anxiety levels and showed minor reductions in anxiety, without statistically significant physiological change. This cluster suggests that for children having moderate distress, even minimal interventions or exposure to a familiar clinical setting may elicit improvement.
Cluster 3 – “low anxiety – non-responsive” (n = 57): present in all groups, including JPM, this cluster comprised children with consistently low IDAF-4C⁺ scores (<2.5) and negligible physiological or psychological change. These children appear to possess intrinsic emotional resilience, indicating that additional psychological interventions may not be necessary or efficient in such cases.
These results increase ecological validity by demonstrating that not all children benefit equally, an important finding for clinical applications.
This cluster-based approach enriched the interpretation of treatment effects and reinforced the principle that anxiety interventions should be personalized, rather than uniformly applied. It adds depth to the interpretation and increases ecological validity, showcasing that psychological techniques must be tailored to individual needs.
Previous studies have underscored the usefulness of JPM in reducing procedural anxiety in pediatric populations, especially in contexts like preoperative settings, school stress, or behavioral therapy [48,49,50]. Our findings are consistent while contributing novel data through the Romanian-validated version of IDAF-4C⁺, addressing the limitations of previous studies that used unvalidated scales like STAI for children [51]. Other strengths include the use of exploratory clustering analysis to enhance the personalization of strategies and a controlled design that enables a clear interpretation of therapeutic effects.
The study’s findings reinforce a multi-dimensional understanding of dental anxiety, implicating physiological arousal and cognitive-emotional processing. JPM’s superiority likely stems from its dual-action mechanism: reducing muscle tension while redirecting attention away from threatening stimuli. In contrast, BC appears to primarily modulate autonomic arousal without significantly influencing cognitive or emotional dimensions of anxiety. A controlled design with a sufficient sample size (n = 189), objective physiological measures alongside self-reported anxiety, and cluster analysis to explore heterogeneity in treatment response are clear strengths of this research.
The clinical implications are substantial. Implementing brief relaxation interventions, especially JPM, before dental procedures may significantly reduce patient distress, increase cooperation, and improve procedural efficiency in pediatric dental practices. These approaches are non-invasive, cost-effective, and easily integrated into routine care. Non-uniform treatment responses support the development of pre-treatment screening tools—potentially supported by decision algorithms—to match interventions to patient profiles based on baseline anxiety, age, sex, or dental history [4,10,22,37,49].
Given its minimal training requirements, non-invasiveness, and low cost, JPM represents a practical and effective strategy for pediatric dental anxiety. Its integration into routine care could improve both patient experience and procedural cooperation.
Despite its strengths—including controlled group allocation, a culturally validated anxiety measure, and objective physiological data—this study has limitations. The short-term design precludes conclusions about long-term anxiety reduction or behavioral changes. The fidelity of intervention delivery was not formally assessed, potentially introducing variability in therapeutic exposure. Additionally, contextual factors such as parental anxiety, previous trauma, or clinician-child rapport were not measured, yet these could substantially influence outcomes. Physiological data (HR and BP) may also be sensitive to external stressors unrelated to dental anxiety. Finally, while the cluster analysis yielded insights, it was exploratory and lacked external validation; replication in larger samples is necessary.
Future research should employ longitudinal follow-up to assess the durability of anxiety reduction and examine its impact on future dental cooperation. Studies should also investigate behavioral predictors—such as temperament, attachment style, or family dynamics to personalize interventions. Furthermore, digital integration of JPM via mobile applications could enable pre-visit training, increase accessibility, and prepare children outside the clinical setting. Expanding this model to multi-center trials would improve generalizability and allow cross-cultural comparisons, especially in underserved populations.
5. Conclusions
This study affirms Jacobson’s Progressive Muscle Relaxation as a superior intervention for reducing dental anxiety in pediatric patients, offering psychological relief and physiological regulation. While Breathing Control shows partial benefits, its effects are less consistent and generally milder. Response variability, captured through cluster analysis, highlights the value of individualized approaches in anxiety management. Incorporating psychological techniques like JPM into standard pediatric dental practice holds promise for improving treatment outcomes, patient experience, and clinical efficiency.
Author Contributions
Conceptualization, S.M.B and I.M.C.; methodology, I.M.C.; software, D.I.C.; validation, S.M.B, I.M.C., and E.S.B.; formal analysis, E.S.B.; investigation, B.S.M., I.M.C. and E.S.B.; resources, D.I.C., E.S.B.; data curation, D.I.C. and C.G.; writing—S.M.B. and C.G,; writing—review and editing, I.M.C.; visualization, C.G; supervision, C.G.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of ”Dunărea de Jos” University. (no. 40541/CEU/2024). Participation was voluntary, with signed consent from guardians and assent from minors.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Participation was voluntary, with signed consent from guardians and assent from minors, in cases of minor patients. Written informed consent has been obtained from the patient(s) or guardians to publish this paper.
Data Availability Statement
Data supporting reported results can be found by e-mailing Dr. Sorana Maria Bucur, at bucursoranamaria@gmail.com.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Jacobson’s Progressive Muscle Relaxation (PMR) Technique in the Dental Setting [3]
Progressive Muscle Relaxation (PMR), developed by Edmund Jacobson, can be effectively adapted for children and adolescents in a dental environment to ease anxiety and enhance cooperation during treatment. This method systematically involves tightening and releasing specific muscle groups, fostering awareness of tension and relaxation. The goal is to induce a state of calm before or during dental care, especially in anxious patients.
The technique is modified for comfort and feasibility when applied in a dental chair. The child is guided step-by-step, in a calm voice, to gently contract and relax various muscle groups, all while remaining seated or reclined. A relaxed position in the dental chair is encouraged: feet flat, arms resting loosely, and head supported. Relaxing background music can further assist the process.
Guided Steps Adapted for the Dental Chair:
- Begin with a few slow, gentle breaths. Ask the patient to inhale softly, pause, and then exhale slowly.
- Feet and legs: The child pulls the toes upward slightly toward the knees—just enough to feel the muscles engage—then holds for a moment and releases. Then press the heels down onto the footrest, hold briefly, and relax.
- Legs and hips: ask the child to press their knees gently together, hold briefly, and allow them to drift apart slightly. Then have them squeeze the gluteal muscles together, hold, and relax.
- Abdomen: guide the child to draw their tummy slightly toward their spine, hold, and then release. Emphasize noticing how their body feels when relaxed.
- Shoulders and arms: ask the child to slowly lift their shoulders toward their ears—just enough to notice tension—hold, and let them drop. Then, have them gently press their elbows into their sides, hold, and relax.
- Hands: instruct them to softly clench their fists, hold for a few seconds, then open their hands and let them rest.
- Neck and face: tilts the head forward, makes a break, and lets it return to a natural, balanced position. Ask to clench their teeth slightly, hold, and then let the jaw relax. Press lips together gently, hold, then let them loosen naturally. Instruct the child to press their tongue against the roof of their palate, hold it, and let it fall into a relaxed position.
- Eyes and forehead: ask the child to squint the eyes gently, then release them. Finally, have them furrow their brow slightly, hold, and then allow the forehead to soften.
Throughout the process, the clinician or assistant can softly prompt the child to notice the difference between tension and relaxation. The technique typically takes 10–15 minutes but can be shortened based on clinical needs or the patient's age and attention span.
This adaptation of JPM has been shown to help reduce dental anxiety in children and enhance cooperation, creating a positive clinical experience for both the patient and the practitioner.
Appendix B
Romanian Index of Dental Anxiety and Fear (IDAF-4C+) [45]
 |
References
- Stein Duker, L.I.; Grager, M.; Giffin, W.; Hikita, N.; Polido, J.C. The Relationship between Dental Fear and Anxiety, General Anxiety/Fear, Sensory Over-Responsivity, and Oral Health Behaviors and Outcomes: A Conceptual Model. Int. J. Environ. Res. Public Health 2022, 19, 2380. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Hamzah, S.H.; Yiu, C.K.; McGrath, C.; King, N.M. Dental fear and anxiety in children and adolescents: Qualitative study using YouTube. J. Med. Internet Res. 2013, 15, e29. [Google Scholar] [CrossRef]
- Appukuttan, D.P. Strategies to manage patients with dental anxiety and dental phobia: Literature review. Clin. Cosmet. Investig. Dent. 2016, 8, 35–50. [Google Scholar] [CrossRef]
- Grisolia, B.M.; Dos Santos, A.P.P.; Dhyppolito, I.M.; Buchanan, H.; Hill, K.; Oliveira, B.H. Prevalence of dental anxiety in children and adolescents globally: A systematic review with meta-analyses. Int. J. Paediatr. Dent. 2021, 31, 168–183. [Google Scholar] [CrossRef]
- Sun, I.G.; Chu, C.H.; Lo, E.C.M.; Duangthip, D. Global prevalence of early childhood dental fear and anxiety: A systematic review and meta-analysis. J. Dent. 2024, 142, 104841. [Google Scholar] [CrossRef]
- Baier, K.; Milgrom, P.; Russell, S.; Mancl, L.; Yoshida, T. Children's fear and behavior in private pediatric dentistry practices. Pediatr. Dent. 2004, 26, 316–321. [Google Scholar] [PubMed]
- Klingberg, G.; Broberg, A.G. Dental fear/anxiety and dental behaviour management problems in children and adolescents: A review of prevalence and concomitant psychological factors. Int. J. Paediatr. Dent. 2007, 17, 391–406. [Google Scholar] [CrossRef] [PubMed]
- Orenius, T.; Säilä, H.; Mikola, K.; Ristolainen, L. Fear of injections and needle phobia among children and adolescents: An overview of psychological, behavioral, and contextual factors. SAGE Open Nurs. 2018, 4, 2377960818759442. [Google Scholar] [CrossRef]
- Shim, Y.S.; Kim, A.H.; Jeon, E.Y.; An, S.Y. Dental fear & anxiety and dental pain in children and adolescents: A systemic review. J. Dent. Anesth. Pain Med. 2015, 15, 53–61. [Google Scholar]
- Rath, S.; Das, D.; Sahoo, S.K.; Raj, A.; Guddala, N.R.; Rathee, G. Childhood dental fear in children aged 7–11 years old by using the Children's Fear Survey Schedule-Dental Subscale. J. Med. Life 2021, 14, 45–49. [Google Scholar] [CrossRef]
- Guzeldemir, E.; Toygar, H.U.; Cilasun, U. Pain perception and anxiety during scaling in periodontally healthy subjects. J. Periodontol. 2008, 79, 2247–2255. [Google Scholar] [CrossRef]
- Santos-Puerta, N.; Peñacoba-Puente, C. The role of dental fear, pain anticipation and self-efficacy in endodontic therapy. Community Dent. Health 2023, 40, 85–91. [Google Scholar]
- Lin, C.S.; Wu, S.Y.; Yi, C.A. Association between anxiety and pain in dental treatment: A systematic review and meta-analysis. J. Dent. Res. 2017, 96, 153–162. [Google Scholar] [CrossRef]
- Mehrabkhani, M.; Khanmohammdi, R.; Nematollahi, H.; Rajabi, N.; Gheidari, A. Influence of temperament on children's cooperation during dental treatment. Dent. Res. J. (Isfahan) 2024, 21, 45. [Google Scholar] [CrossRef] [PubMed]
- Janeshin, A.; Habibi, M. The relationship between temperament and behavior in 3–7-year-old children during dental treatment. Dent. Res. J. (Isfahan) 2021, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.C.-Y.; Chai, H.H.; Lo, E.C.-M.; Huang, M.-Z.; Chu, C.-H. Strategies for effective dentist–patient communication: A literature review. Patient Prefer. Adherence 2024, 18, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Al Homoud, R.A.; Alshellatie, A.K.; Alzumaie, A.S.; Al-Bayati, S.A. Behavior and anxiety levels in pediatric patients: The behavioral changes and anxiety of pediatric patients in dental clinics. Clin. Exp. Dent. Res. 2023, 9, 1223–1231. [Google Scholar] [CrossRef]
- Kvesić, A.J.; Hrelja, M.; Lovrić, Ž.; Šimunović, L.; Špiljak, B.; Supina, N.; Vranić, L.; Vranić, D.N. Possible risk factors for dental fear and anxiety in children who suffered traumatic dental injury. Dent. J. 2023, 11, 190. [Google Scholar] [CrossRef]
- Esian, D.; Bica, C.; Vlasa, A.; Bud, E.; Stepco, E.; Bud, A.; Beresescu, L. Retrospective study regarding the correlation between dental anxiety and color preferences in children with severe early childhood caries. Dent. J. 2024, 12, 155. [Google Scholar] [CrossRef]
- Bagchi, A.; Lahiri, B.; Jalaluddin, M.; Kumar, G.; Das, S.; Dhull, K.S. Quantification and measurement of changes in anxiety levels in preschool children and their mothers through multiple-visit dental treatment. J. Int. Soc. Prev. Community Dent. 2017, 7, 125–130. [Google Scholar] [CrossRef]
- Fux-Noy, A.; Zohar, M.; Herzog, K.; Shmueli, A.; Halperson, E.; Moskovitz, M.; Ram, D. The effect of the waiting room’s environment on the level of anxiety experienced by children prior to dental treatment: A case-control study. BMC Oral Health 2019, 19, 294. [Google Scholar] [CrossRef] [PubMed]
- Kohli, N.; Hugar, S.M.; Soneta, S.P.; Saxena, N.; Kadam, K.S.; Gokhale, N. Psychological behavior management techniques to alleviate dental fear and anxiety in 4–14-year-old children in pediatric dentistry: A systematic review and meta-analysis. Dent. Res. J. (Isfahan) 2022, 19, 47. [Google Scholar] [PubMed]
- Jayakaran, T.G.; Rekha, C.V.; Annamalai, S.; Baghkomeh, P.N.; Sharmin, D.D. Preferences and choices of a child concerning the environment in a pediatric dental operatory. Dent. Res. J. (Isfahan) 2017, 14, 183–187. [Google Scholar] [CrossRef]
- Oliveira, L.B.; Massignan, C.; De Carvalho, R.M.; Savi, M.G.; Bolan, M.; Porporatti, A.L.; Luca Canto, G. Children's perceptions of dentist's attire and environment: A systematic review and meta-analysis. Int. J. Clin. Pediatr. Dent. 2020, 13, 700–716. [Google Scholar] [CrossRef]
- Bani-Hani, T.; Al-Fodeh, R.; Tabnjh, A.; Leith, R. The use of local anesthesia in pediatric dentistry: A survey of specialists' current practices in children and attitudes in relation to articaine. Int. J. Dent. 2024, 2024, 2468502. [Google Scholar] [CrossRef]
- Caleza-Jiménez, C.; López-de Francisco, M.D.M.; Mendoza-Mendoza, A.; Ribas-Pérez, D. Relationship between children's lifestyle and fear during dental visits: A cross-sectional study. Children 2022, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Britton, J.C.; Grillon, C.; Lissek, S.; Norcross, M.A.; Szuhany, K.L.; Chen, G.; Ernst, M.; Nelson, E.E.; Leibenluft, E.; Shechner, T.; Pine, D.S. Response to learned threat: An fMRI study in adolescent and adult anxiety. Am. J. Psychiatry 2013, 170, 1195–1204. [Google Scholar] [CrossRef]
- Gautam, S.; Jain, A.; Chaudhary, J.; Gautam, M.; Gaur, M.; Grover, S. Concept of mental health and mental well-being, its determinants and coping strategies. Indian J. Psychiatry 2024, 66 (Suppl 2), S231–S244. [Google Scholar] [CrossRef]
- Kwarta, P.; Pietrzak, J.; Miśkowiec, D.; Stelmach, I.; Górski, P.; Kuna, P.; Antczak, A.; Pietras, T. Personality traits and styles of coping with stress in physicians. Pol. Merkur. Lekarski 2016, 40, 301–307. [Google Scholar]
- Okuro, R.T.; Freire, R.C.; Zin, W.A.; Quagliato, L.A.; Nardi, A.E. Panic disorder respiratory subtype: psychopathology and challenge tests—an update. Braz. J. Psychiatry 2020, 42, 420–430. [Google Scholar] [CrossRef]
- Banushi, B.; Brendle, M.; Ragnhildstveit, A.; Murphy, T.; Moore, C.; Egberts, J.; Robison, R. Breathwork interventions for adults with clinically diagnosed anxiety disorders: A scoping review. Brain Sci. 2023, 13, 256. [Google Scholar] [CrossRef] [PubMed]
- Pippalapalli, J.; Lumb, A.B. The respiratory system and acid-base disorders. BJA Educ. 2023, 23, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Li, S.; Zhang, R. Effects of dental anxiety and anesthesia on vital signs during tooth extraction. BMC Oral Health 2024, 24, 632. [Google Scholar] [CrossRef]
- Hamdani, S.U.; Zill-E-Huma; Zafar, S.W.; Suleman, N.; Um-Ul-Baneen; Waqas, A.; Rahman, A. Effectiveness of relaxation techniques ‘as an active ingredient of psychological interventions’ to reduce distress, anxiety and depression in adolescents: A systematic review and meta-analysis. Int. J. Ment. Health Syst. 2022, 16, 31. [CrossRef]
- Kliegman, R.M. ; St. Geme, J.W.; Blum, N.J.; Shah, S.S.; Tasker, R.C.; Wilson, K.M. Nelson Textbook of Pediatrics, 21st ed.; Elsevier: Philadelphia, PA, USA, 2020. [Google Scholar]
- Balon, R.; Starcevic, V. Role of benzodiazepines in anxiety disorders. Adv. Exp. Med. Biol. 2020, 1191, 367–388. [Google Scholar] [CrossRef]
- Toussaint, L.; Nguyen, Q.A.; Roettger, C.; Dixon, K.; Offenbächer, M.; Kohls, N.; Hirsch, J.; Sirois, F. Effectiveness of progressive muscle relaxation, deep breathing, and guided imagery in promoting psychological and physiological states of relaxation. Evid. Based Complement. Alternat. Med. 2021, 2021, 5924040. [Google Scholar] [CrossRef]
- Aalami, M.; Jafarnejad, F.; ModarresGharavi, M. The effects of progressive muscular relaxation and breathing control technique on blood pressure during pregnancy. Iran J. Nurs. Midwifery Res. 2016, 21, 331–336. [Google Scholar] [CrossRef]
- Bentley, T.G.K.; D’Andrea-Penna, G.; Rakic, M.; Arce, N.; LaFaille, M.; Berman, R.; Cooley, K.; Sprimont, P. Breathing practices for stress and anxiety reduction: Conceptual framework of implementation guidelines based on a systematic review of the published literature. Brain Sci. 2023, 13, 1612. [Google Scholar] [CrossRef]
- Griffin, J.B. Psychological disturbances of vegetative function. In Clinical Methods: The History, Physical, and Laboratory Examinations; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; 3rd ed.; Butterworths: Boston, MA, USA, 1990; Chapter 205. Available online: https://www.ncbi.nlm.nih.gov/books/NBK318/. [Google Scholar]
- Peretz, B.; Gluck, G.M. Assessing an active distracting technique for local anesthetic injection in pediatric dental patients: Repeated deep breathing and blowing out air. J. Clin. Pediatr. Dent. 1999, 24, 5–8. [Google Scholar] [PubMed]
- Levi, M.; Bossù, M.; Luzzi, V.; Semprini, F.; Salaris, A.; Ottaviani, C.; Violani, C.; Polimeni, A. Breathing out dental fear: A feasibility crossover study on the effectiveness of diaphragmatic breathing in children sitting on the dentist's chair. Int. J. Paediatr. Dent. 2022, 32, 801–811. [Google Scholar] [CrossRef]
- Armfield, J.M. Development and psychometric evaluation of the Index of Dental Anxiety and (IDAF-4C+). Psychol. Assess. 2010, 22, 279–287. [Google Scholar] [CrossRef]
- Ibrahim, H.; Lyons, K.M.; Armfield, J.M.; Thomson, W.M. Performance of the Index of Dental Anxiety and Fear in a population-based sample of adults. Aust. Dent. J. 2017, 62, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Done, A.E.; Preoteasa, E.; Preoteasa, C.T. Psychometric assessment of the Romanian version of the Index of Dental Anxiety and Fear (IDAF-4C+). Healthcare 2023, 11, 2129. [Google Scholar] [CrossRef]
- Nasiri, E.; Mahmodi, M.A. Effectiveness of Jacobson’s relaxation technique on anxiety in children undergoing dental treatment.
- Heft, M.W.; Meng, X.; Bradley, M.M.; Lang, P.J. Gender differences in reported dental fear and fear of dental pain. Community Dent. Oral Epidemiol. 2007, 35, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Sabherwal, P.; Kalra, N.; Tyagi, R.; Khatri, A.; Srivastava, S. Hypnosis and progressive muscle relaxation for anxiolysis and pain control during extraction procedure in 8–12-year-old children: A randomized control trial. Eur. Arch. Paediatr. Dent. 2021, 22, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, M.S.; Shafique, M.A.; Zaidi, S.D.E.Z.; et al. Preoperative anxiety management in pediatric patients: A systemic review and meta-analysis of randomized controlled trials on the efficacy of distraction techniques. Front. Pediatr. 2024, 12, 1353508. [Google Scholar] [CrossRef]
- Uman, L.S.; Birnie, K.A.; Noel, M.; Parker, J.A.; Chambers, C.T.; McGrath, P.J.; Kisely, S.R. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2013, (10), CD005179. [Google Scholar] [CrossRef]
- AlAzmah, A.; Sharanesha, R.B.; Abushanan, A.; Khojah, A.B.; Dhaafi, A.A.; Almakenzi, A.A.; Alqarni, A.S.; Alagla, M.; Al Ghwainem, A.; Alghamdi, S. Comparison of parental and children’s dental anxiety levels using the Modified Dental Anxiety Scale and Modified Short State-Trait Anxiety Inventory (EMOJI) Scale. Children 2024, 11, 1532. [Google Scholar] [CrossRef]
Figure 1.
Mean Changes in Anxiety and Physiological Measures by Cluster.
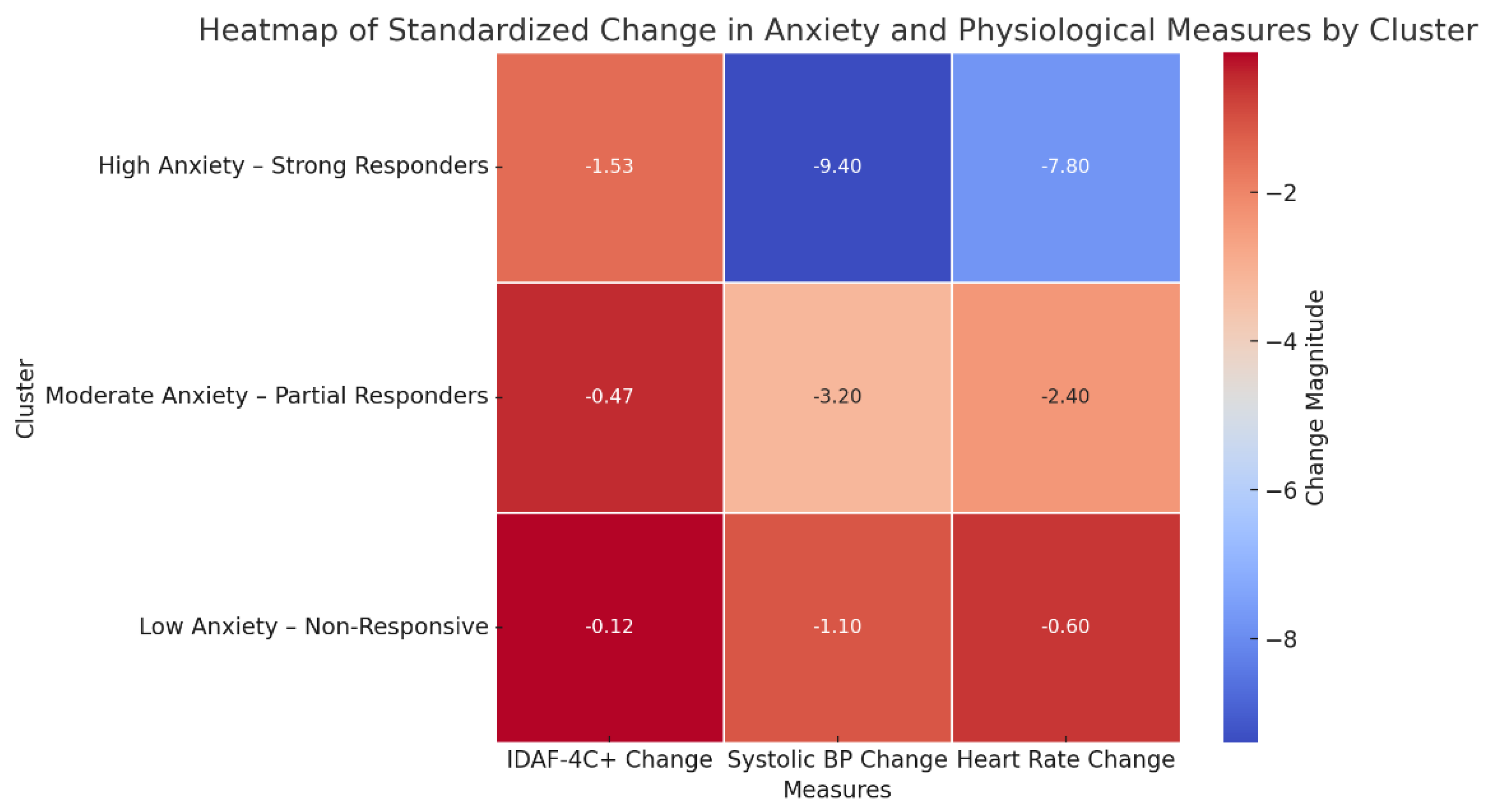
Table 1.
Blood Pressure Average Values.
| Age | Systolic BP (mm Hg) | Diastolic BP (mm Hg) | Status |
|---|---|---|---|
| 10 years | 102 ± 11 | 64 ± 10 | Normal |
| 13 years | 108 ± 13 | 66 ± 11 | Normal |
| 16 years | 115 ± 12 | 67 ± 11 | Normal |
Table 2.
Heart Rate Values in Children and Adolescents by Age and Sex.
| Age (years) | Sex | Mean HR (beats/min) | Normal Range (beats/min) |
|---|---|---|---|
| 10 | Girls & Boys | 90 | 70–110 |
| 12 | Girls | 90 | 70–110 |
| 12 | Boys | 85 | 65–105 |
| 14 | Girls | 85 | 65–105 |
| 14 | Boys | 80 | 60–100 |
| 16 | Girls | 80 | 60–100 |
| 16 | Boys | 75 | 55–95 |
| 18 | Girls | 75 | 55–95 |
| 18 | Boys | 70 | 50–90 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



