
Submitted:
10 April 2025
Posted:
10 April 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic has presented a serious challenge to Nephrologists as it led to severe kidney injury in the form of acute tubular necrosis, many of whom required renal replacement therapy. This was predominantly seen in people who developed severe respiratory manifestations like ARDS from the viral infection, cytokine storm and septic shock with unstable hemodynamics. It has also presented with various Glomerular injuries mainly collapsing glomerulopathy in high risk APOL1 genotype patient's, thrombotic microangiopathy related renal failure due to hyper coagulopathy and occasionally pauci-immune glomerulonephritis due to immune dysregulation. All the glomerular disorders due to COVID 19 infection have been described under an entity named COVAN (covid 19 associated nephropathy). Proteinuria was a predominant presentation in Glomerular disorders. Gross hematuria and AKI without any respiratory symptoms from COVID-19 infection have not been described so far in the literature. We have encountered a rare case of gross hematuria and severe acute renal failure who was found to have infection related crescentic glomerulonephritis due to active COVID-19 infections on kidney biopsy without any respiratory symptoms clinically. He has responded well to treatment with steroid taper and antiviral (Remdesivir). This is a very rare Renal manifestation of COVID-19 infection.
Keywords:
COVID-19
; Tubuloreticular inclusion body
; Crescentic Glomerulonephritis
1. Introduction
Involvement of kidneys in various systemic conditions is well-known. Infections often affect kidneys and most common involvement of kidneys in infections is due to sepsis which leads to acute tubular necrosis/acute kidney injury from unstable hemodynamics. Infection related glomerulonephritis is a well-known entity which is usually seen after severe acute bacterial infections mainly involving Staphylococcus and Streptococcus [1]. Viral infections leading to infection related Glomerulonephritis are relatively less common than bacterial infections. The recent pandemic due to COVID-19 infection has affected kidneys severely and the most common manifestation was acute tubular necrosis due to sepsis from COVID-19 infection [2]. Another commonly described entity was collapsing glomerulopathy in high risk APOL1 genotype patients [2]. Infection related glomerulonephritis due to COVID-19 infection has not been described in detail so far. Here we have described one such rare case and reviewed the literature of the various COVID-19 related kidney manifestations.
2. Case Presentation
A 69-year-old gentleman with obesity, hyperlipidemia, tobacco use, hypertension, psoriasis, irritable bowel syndrome presented to the emergency room with gross hematuria of 1-week duration. He was admitted to the hospital because of AKI and concerns about urinary tract infection. His blood pressure was 200/100 mm hg in the emergency room. He has normal renal function at baseline, with creatinine around 1 mg/dL and EGFR around 75 mL/minute. His urinalysis showed large blood,> 100 RBC per high-power field), 20-30 WBC per high-power field and more than 300 mg/dL protein (Supplementary Table S3). His BMP showed acute kidney injury with creatinine at 2.2 mg/dL, mild hypokalemia with serum potassium at 3.3 millimoles per L. His kidney ultrasound, renal artery doppler study and CT abdomen pelvis without contrast were unremarkable. His urine culture was negative. He received a dose of IV Rocephin initially and was later switched to oral cephalexin. His hemoglobin was 16 grams/deciliter, platelet count was 171 and WBC count was 6.9. (Supplementary Table S1). He was started on IV fluids, home dose of atenolol 50 mg daily and hydrochlorothiazide 25 mg was continued and was started on Amlodipine 5 mg daily. His creatinine improved to 1.8 mg/dL after 24 hours. His hematuria has also improved. Urology recommended outpatient evaluation with cystoscopy and CT urogram for hematuria.
He was discharged and seen in the clinic a week later. During this visit, he reported severe fatigue, poor appetite, bilateral flank discomfort and persistent dark urine. Labs results showed severe acute renal failure with creatinine worsening up to 5.7 mg/dL (Supplementary Figure S2) and urinalysis showed large blood,> 100 RBC per high-power, orange turbidity and 20-30 WBC per high-power field (Supplementary Table S3). We couldn’t test urine for NGAL and Beta-2 Microglobulin as these are not offered at our laboratory. He was oliguric with a urine output less than 500 cc per day and hypertensive with blood pressure around 160/90 mm Hg. He was admitted to the hospital. His renal function continued to worsen, creatinine worsened to 6.4 mg/dL, BUN up to 96 mg/dL, had persistent oliguria and hematuria.
He underwent extensive investigation. His blood and urine cultures were negative. Serologies for Antinuclear antibody, anti PLA2R ab, viral hepatitis panel, ANCA panel, cryoglobulins, complements C3, C4, anti-GBM antibody, serum protein electrophoresis and serum free light chains have all come back negative. He tested negative for influenza and positive for SARS-CoV- 2 virus (Supplementary Table S2). He did not have any respiratory symptoms, and his chest X-ray was clear. Renal vein Doppler studies, bilateral lower extremity Doppler studies and V/Q scan to look for any pulmonary embolus in the setting of active COVID-19 infection have all come back negative. He underwent a kidney biopsy. Biopsy showed Focal necrotizing and crescentic glomerulonephritis with mesangial proliferative changes and C3 deposits (active COVID infection-associated). Other causes of Glomerulonephritis, bacterial infection related Glomerulonephritis and C3GN, were also considered. But his blood cultures, urine cultures and anti-streptolysin O titers have come back negative, and biopsy did not show any significant staining for IgG (bacterial infection related GN usually shows strong staining for C3 and IgG). C3GN was strongly considered. His serum C3 and C4 were within normal range. We tested for complement pathway abnormalities, which have come back negative. But since his biopsy showed tubular injury (usually seen with covid 19 infection),tubuloreticular inclusion bodies (indicating high interferon activity seen with viral infections) several C3 deposits (seen due to complement activation in covid infection) and had active covid 19 infection, it was diagnosed as active covid-19 infection induced glomerulonephritis rather than C3GN. Pathologist determined that the pattern of C3 deposition and overall features of biopsy(light microscopy ,EM and IF)are not suggestive of typical C3GN but are secondary to COVID 19 infection. He started on Remdesivir (5 days), pulse steroids and oral prednisone taper.
His renal function, hematuria and urine output gradually improved. He was in the hospital for 10 days. He was discharged with prolonged prednisone taper, with starting the dose of 60 mg daily. 4 weeks later, creatinine improved to 5 mg/dl. 8 weeks later, his creatinine improved to 2.5 mg/dL and 3 months later improved to 1.8 mg/dL and stabilized around 1.8 mg/dL and eGFR improved to 35 ml/min (Supplementary Figures S2 and S3). He tapered down his prednisone to 5 mg over the next three-months. His follow-up urinalysis showed only 3-10 RBC per high-power field, but no WBC, blood or protein, and clear clarity (Supplementary Table S3). His urine albumin to creatinine ratio improved from 249 mg/g to 17 mg/g (Supplementary Figure S1). His blood pressure eventually improved, and he was maintained on atenolol 50 mg daily, hydrochlorothiazide 25 mg daily and amlodipine 10 mg daily.
3. Comment
The biopsy demonstrates focal necrotizing (1 of 16) and crescentic glomerulonephritis (1 of 16) associated with C3 deposits in the mesangium and capillary walls. The differential diagnosis includes an infection-related versus C3 glomerulonephritis. Given the presence of ongoing COVID infection this is favored to be secondary to the infection.
4. Final Diagnosis
Focal necrotizing and crescentic glomerulonephritis with mesangial proliferative changes and C3 deposits (active COVID infection-associated).
5. Discussion
Covid-19 virus infects Lungs primarily, but several other organ systems are also affected due to it. A study published by Pei et all from China revealed the incidence of Acute kidney injury up to 75% in COVID-19 infected patients [3]. Most common risk factors for COVID 19 related acute renal failure are CKD, Diabetes mellitus type 2, hypertension, male sex, old age and severity of COVID 19 infection [2]. COVID-19 affects the tubular, vascular, and Glomerular compartments of the kidneys [4]. This susceptibility is partly due to the presence of Angiotensin-converting enzyme 2 (ACE2) receptors in the kidneys, particularly in Podocytes and proximal tubule epithelial cells [2]. The spike protein on the virus interacts with these ACE2 receptors, allowing entry into host cells. Due to high concentration of ACE2 receptors in the lungs and kidneys, these organs become primary targets for the virus [2]. The interaction between the virus and ACE2 receptors on endothelial cells and podocytes in the glomerulus can lead to hematuria, proteinuria, and reduction in glomerular filtration rate [5]. These organs are suspected to act as the reservoir of the virus and detection of viral mRNA in urine specimens reported in some studies adds further strength to these clinical findings [2].
Acute kidney injury associated with COVID-19 infection is a multifactorial etiology, cardiovascular effects due to unstable hemodynamics, direct viral impact on the kidneys, immune system dysregulation, cytokine storm, hyper coagulopathy, endothelial injury, collapsing glomerulopathy, and thrombotic microangiopathy play a role [6].The most common cause of AKI in COVID-19 infection is acute tubular necrosis from septic shock [2]. The virus infects proximal tubular cells, leading to vacuolar degeneration and loss of the brush border of tubular epithelial cells leading to the development of ATN [6]. Endothelial cell infection by the virus leads to formation of fibrin thrombi in the glomerular capillaries [6]. This endothelial injury, along with prothrombotic state, leads to small vessel vasculitis and extensive micro thrombosis leading to thrombotic microangiopathy (TMA) and renal injury from it. Interleukin-6 (IL-6) is crucial in the cytokine storm syndrome observed in COVID-19 infections. The cytokine storm contributes to ARDS and impairs hemodynamics, which leads to reduced renal perfusion, renal medullary hypoxia and tubular cell damage leading to acute tubular necrosis [6].
6. Various Glomerular Pathologies Seen After COVID-19
6.1. Infection Across Published Studies
6.1.1. Podocytopathies
● Collapsing glomerulopathy (CG)
● Membranous nephropathy (MN)
● Secondary focal segmental glomerulosclerosis (FSGS)
● Global glomerulosclerosis
● Minimal change disease (MCD)
● Primary FSGS
6.1.2. Immune Complex-Mediated Glomerulonephritis (GN)
● IgA nephropathy
● Lupus nephritis
● Immune complex-mediated GN with polytypic IgG3 and IgM-dominant immune deposits
6.1.3. Pauci-Immune GN
● ANCA associated GN
● Anti-glomerular basement membrane (anti-GBM) GN
6.1.4. Vascular Dominant
● Thrombotic microangiopathy (TMA)
6.1.5. Patients with Multiple Pathologies on Biopsy
● ATN + Collapsing glomerulopathy (CG)
● ATN + Minimal change disease (MCD)
● ATN + Membranous nephropathy (MN)
● ATN + IgA nephropathy
● ATN + Thrombotic microangiopathy
● ATN + CG + MN
● ATN + CG + IgA nephropathy.
● ATN + Henoch-Schönlein purpura nephritis
Glomerular diseases associated with COVID-19 are described under an entity called COVID-19 associated nephropathy (COVAN) [7]. During the COVID-19 pandemic, glomerular diseases have been reported more frequently. This is due to immune dysregulation, autoantibody production, cytokine storm, complement activation and direct viral toxicity associated with COVID-19 infection which led to various forms of glomerular injuries [7]. Treatment of the glomerular diseases in the setting of active or recent COVID-19 infection is challenging as these diseases require immunosuppression [7].
In a review study conducted by Kudose et al on-kidney biopsy findings of patients with COVID 19 related kidney injury, patients with collapsing glomerulopathy and minimal change disease were found to have high risk APOL1 genotypes on genetic studies and electron microscopy showed endothelial tubuloreticular inclusions in 60% samples [8]. The presence of tubuloreticular inclusions indicate the role of interferon mediated injury in genetically susceptible individuals with covid 19 infection [8,9]. These inclusions, referred to as "interferon footprints," indicate a significant role for interferon in the kidney pathology associated with COVID-19 [7]. Despite extensive investigation using multiple distinctive methods, this study did not detect any viral particles within the kidney cells [8]. Even in patients with positive Covid -19 RT-PCR , immunohistochemical staining of the kidney biopsy samples and electron microscopy did not show any viral particles (SARS-CoV-2) in the kidney tissues [4].
PLA2R, expressed in the respiratory tract and the kidney, may trigger PLA2R-mediated Membranous nephropathy if the respiratory tract is infected by SARS-CoV-2. There are case reports describing the association of membranous nephropathy and COVID-19 infection, with elevated PLA2R titters observed in these cases. Biopsies from these patients have shown features of secondary membranous nephropathy and they have responded to immunosuppression [10].
Gobor et.al described a case of crescentic membranoproliferative glomerulonephritis after receiving covid 19 vaccine in a patient with a previous history of chronic membranoproliferative glomerulonephritis. This patient responded well to aggressive immunosuppression which led to normalization of renal function and improvement in proteinuria. This report illustrates possibility of covid 19 vaccination triggering glomerular disease [11].
In a study conducted in South Korea by Kim et.al, the most common glomerular disease diagnosed after infection with covid 19 was podocytopathy with primary focal segmental glomerulosclerosis and minimal change disease. Whereas post vaccination the most common glomerular diseases were IgA nephropathy, Henoch Schönlein purpura nephritis, few cases of Lupus Nephritis and Pauci-immune crescentic glomerulonephritis. Covid 19 infection and vaccination can lead to autoimmune glomerulonephritis through activation of innate and adaptive immune responses. Covid-19 vaccinations, particularly mRNA vaccines are believed to enhance immune reactions which can trigger the development of glomerulonephritis [12].
Winkler et.al reported a case of recurrent Anti glomerular Basement membrane disease in a patient following SARS-CoV-2 infection. This patient had negative serologies, but biopsy has shown fibro cellular crescents, segmental fibrinoid necrosis and linear IgG, IgM and C3 deposits along glomerular basement membrane. This patient was treated with plasma exchange, pulse steroids and Rituximab with a positive outcome. This case illustrates the possibility that COVID infection can reactivate pre-existing auto reactive T lymphocytes, B lymphocytes and activate the complement system leading to inflammation which leads to glomerular endothelial injury resulting in crescentic glomerulonephritis [13].
Ta et.al described a case of ANCA associated vasculitis with mucosal involvement in a patient recovering from COVID-19 pneumonia. This paper suggests that COVID-19 infection triggered autoimmunity through molecular mimicry, viral persistence, epitope spreading and formation of neutrophil extra cellular traps. These neutrophil extra cellular traps are formed by activated neutrophils which lead to endothelial injury, complement activation, production of P-ANCA and C ANCA which led to crescentic glomerulonephritis. They also suggest that the expression of neutrophil extracellular traps expression is increased in COVID-19 patients [14].
Pfister et.al studied kidney biopsies of patients with COVID-19 infection and discovered marked complement activation in the vascular beds and tubules. All 3 pathways of complement activation were observed in COVID-19 infection. Complement activation in kidneys was observed to be indirect rather than direct as viruses were not detected in kidney tissue by in situ hybridization and immunohistochemistry in the study. Complement C3 C and specifically C3d deposition was noted extensively in the tubules of patients with COVID infection and the intensity of staining correlated with the severity of COVID-19 infection. C5b-9 deposits were also detected and showed high intensity staining in COVID-19 infection patients. These findings highlight the role of complement related kidney injury in COVID-19 [15].
C3 glomerulopathy is due to dysregulation of alternate complement pathway mainly related to complement gene abnormalities. It is characterized by persistently low serum C3 and autoantibodies directed against various complement factors that can be detected in serum. It can present clinically with asymptomatic hematuria, proteinuria or severe glomerulonephritis and progress to ESRD. Biopsy shows 3+ staining for C3 either in form of sausage shaped deposits and thickening of basement membrane in dense deposit disease or as electron dense deposits in mesangial and subendothelial regions in C3GN. Biopsy picture is described as MPGN usually. Treatment response is usually poor but might respond to anti complement agents (anti C5a agent-Eculizumab) and MMF [20]. In comparison, covid related glomerulopathy is secondary to covid infection. Clinical presentation is usually variable. Excessive proteinuria is usually seen in cases of collapsing glomerulopathy, which is seen in cases of high risk APOL1 carriers. Biopsy findings are not consistent unlike in C3 glomerulopathy. ATN is the predominant finding in biopsy. Tubuloreticular inclusion bodies are noted in biopsies of Covid -19 associated kidney injury indicating interferon activity which is not seen in C3GN.Complement activation is secondary to infection and serum C3 levels eventually normalize unlike in C3 glomerulopathy. Biopsy shows C3 deposits usually in tubules, vascular beds and all 3 pathways of complement system are activated. Treatment is directed against covid-19 with antivirals.
Yilmaz et.al reported a case of an adolescent with biopsy proven IgA nephropathy and Alport syndrome who developed crescentic glomerulonephritis due to flare up of IgA nephropathy following COVID-19 infection. Despite immunosuppression with pulse steroids, it has progressed to end stage renal disease and became dialysis dependent. This paper describes that COVID-19 infection stimulates IL-6 production, leading to excess production of galactose deficient IgA1 and flares up IgA Nephropathy. Various cytokines released in response to COVID-19 infection stimulate maturation and proliferation of IgA1 producing B cells. Covid -19 vaccination like influenza vaccination stimulates production of IgA1 monomers leading to IgA nephropathy flare up [17].
Duran et al described cases of pauci immune glomerulonephritis (ANCA associated vasculitis) following Covid -19 infection which were successfully treated with pulse steroids, Cyclophosphamide and plasma exchange [19].
Klomjit et al describe managing Collapsing glomerulopathy, Membranous nephropathy, Crescentic IgA Nephropathy, Sero positive crescentic pauci immune glomerulonephritis, Anti GBM glomerulonephritis, Proliferative Glomerulonephritis with Monoclonal Immunoglobulin deposits which have presented in patients following covid-19 infection and were managed with various immunosuppressive regimens which included steroids, cyclophosphamide, Rituximab, Cyclosporine, Tacrolimus along with antivirals and Plex in few cases with varying outcomes [7].
Bell et al describe modifying immunosuppressive regimen in transplant patients to improve the outcomes. These include discontinuing or holding Mycophenolate and switching to a mechanistic target of rapamycin(mTOR) based regimen. Patients on CNI (calcineurin inhibitors), mTOR and prednisone regimen have shown better outcomes according to this paper [18]. Using various antivirals and monoclonal antibodies directed against Covid-19 virus early in the course of infection has been advocated in this paper [18]. Kronbichler et al proposed that in patients with COVID-19 infection with lymphopenia and kidney transplant recipients with severe COVID-19 infection, further suppressing the T-cell immunity with immunosuppressants should be avoided. Controlling the cytokine storm and inflammatory state with anti-IL-6 agents should be considered. Kidney transplant recipients on triple immunosuppression, should hold antiproliferative drugs to allow the immunity to fight the infection. Severe COVID-19 infections associated with severe lymphopenia could slow progression of immune mediated glomerular disease even if immunosuppression is discontinued or not initiated [21].
Management of COVID-19-related acute kidney injury (AKI) involves treating septic shock, adapting lung-protective ventilation strategies, controlling cytokine storms and using antiviral agents targeting SARS-CoV-2. Renal replacement therapy is in cases of hypervolemia causing refractory hypoxemia, acid-base disturbances, and electrolyte abnormalities. Continuous renal replacement therapy (CRRT) helps remove inflammatory molecules from the body and mitigate the cytokine storm [2]. Mortality rates in patients with COVID-19-related AKI correlate with viral load and AKI severity. Patients with pre-existing chronic kidney disease (CKD) required renal replacement therapy more frequently and those with advanced CKD who developed AKI often continued maintenance dialysis after discharge [2].
Ueda et al. published a case series of five patients with biopsy-proven IgA nephropathy who developed gross hematuria within 48 hours of COVID-19 symptom onset, which lasted for one week. Acute kidney injury accompanied hematuria in some cases and notably, some patients had no prior history of gross hematuria despite having IgA nephropathy [16].
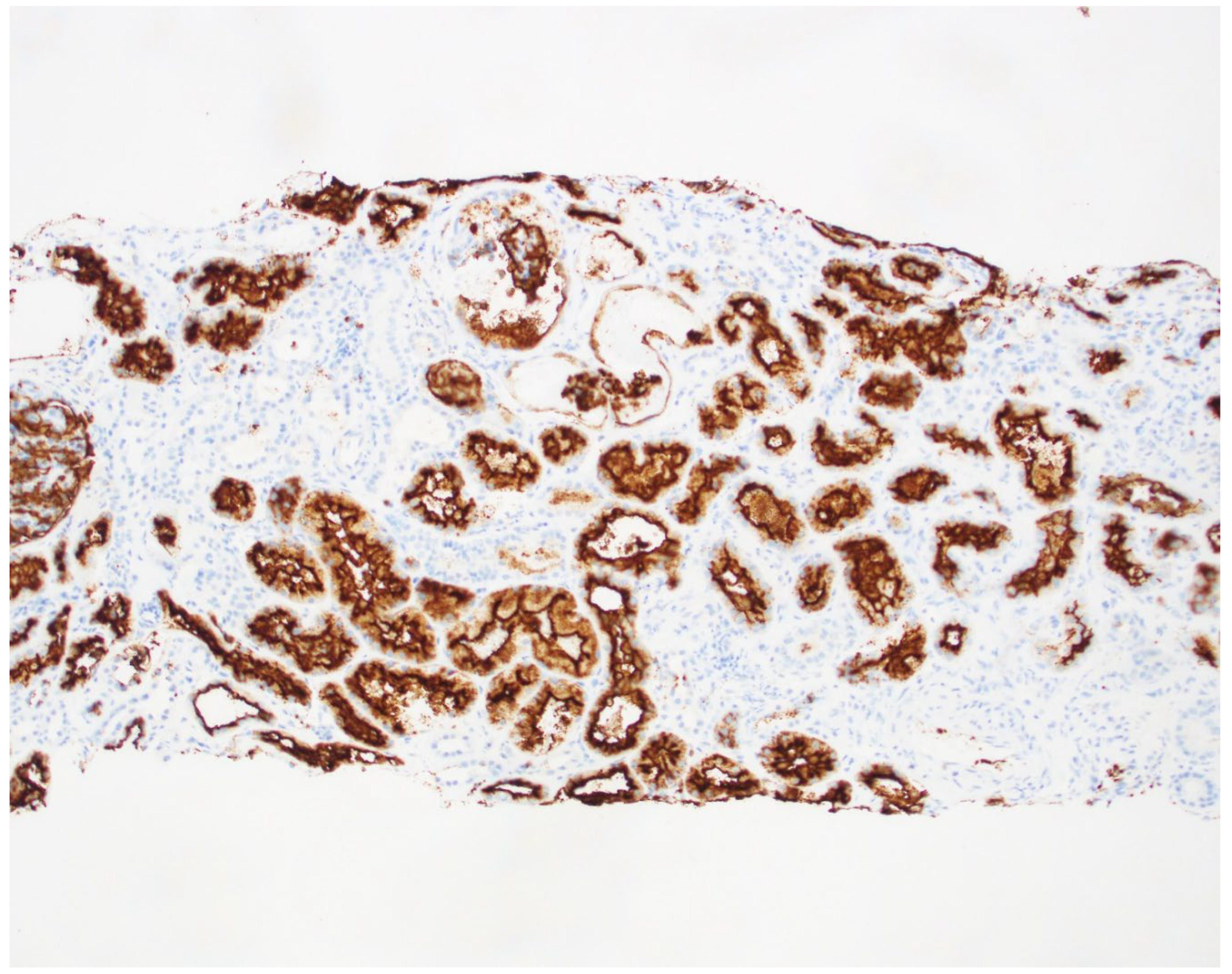
In our case, the patient had no previous history of chronic kidney disease or IgA nephropathy. His hematuria was attributed to infection-mediated crescentic glomerulonephritis secondary to COVID-19 infection. The biopsy revealed fibrinoid necrosis, crescentic glomerulonephritis, several RBC casts (in distal tubules), tubuloreticular inclusions in endothelial cells and C3 deposits supporting the diagnosis of infection-related glomerulonephritis [Figure 1and Figure 2-biopsy images] from active COVID 19 infections. We did the CD10 staining to identify the proximal tubules. Despite the absence of respiratory symptoms, the patient was treated with Remdesivir (an antiviral agent inhibiting SARS-CoV-2 RNA-dependent RNA polymerase), pulse steroids, and a prolonged prednisone taper over three months. The treatment led to the resolution of hematuria and improved renal function. This case is unique as it represents infection-related crescentic glomerulonephritis secondary to COVID-19 presenting initially with gross hematuria, a manifestation not previously described in the literature.
Figure 1.
Light microscopy findings: A. Glomerulus with segmental fibrinoid necrosis (arrow). B. Glomerulus with segmental cellular crescent (arrow). C. Red blood cell casts (arrows) in distal tubules. D. Immunofluorescence histology for C3 shows granular mesangial and capillary loop staining.
Figure 1.
Light microscopy findings: A. Glomerulus with segmental fibrinoid necrosis (arrow). B. Glomerulus with segmental cellular crescent (arrow). C. Red blood cell casts (arrows) in distal tubules. D. Immunofluorescence histology for C3 shows granular mesangial and capillary loop staining.
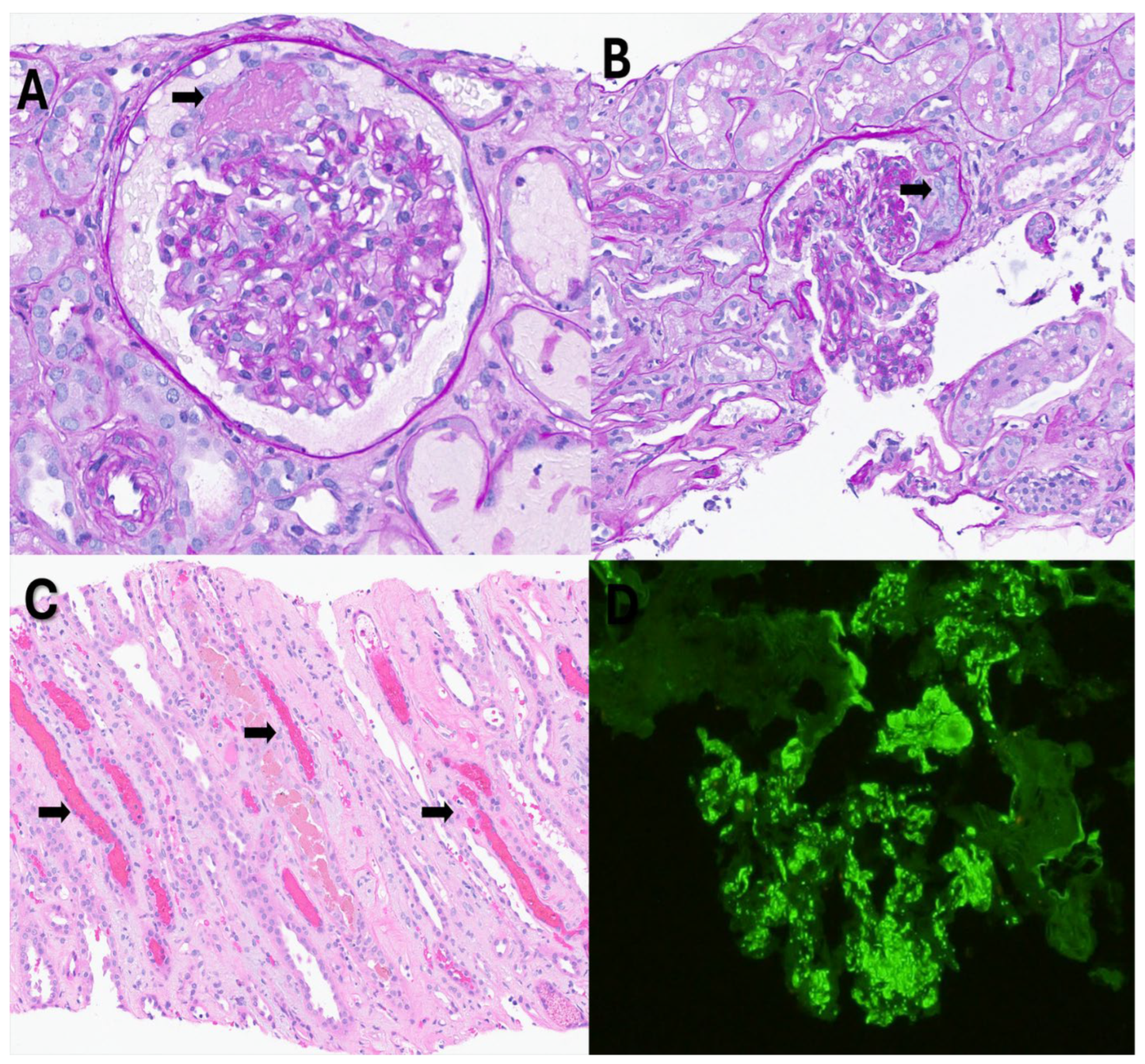
Figure 2.
Electron microscopy findings: A. Electron dense deposits(arrows) in the mesangial region (P: Visceral epithelial cell; M: Mesangial cell). B. Tubuloreticular inclusion body(arrow) (P: Visceral epithelial cell; E: Endothelial cell).
Figure 2.
Electron microscopy findings: A. Electron dense deposits(arrows) in the mesangial region (P: Visceral epithelial cell; M: Mesangial cell). B. Tubuloreticular inclusion body(arrow) (P: Visceral epithelial cell; E: Endothelial cell).
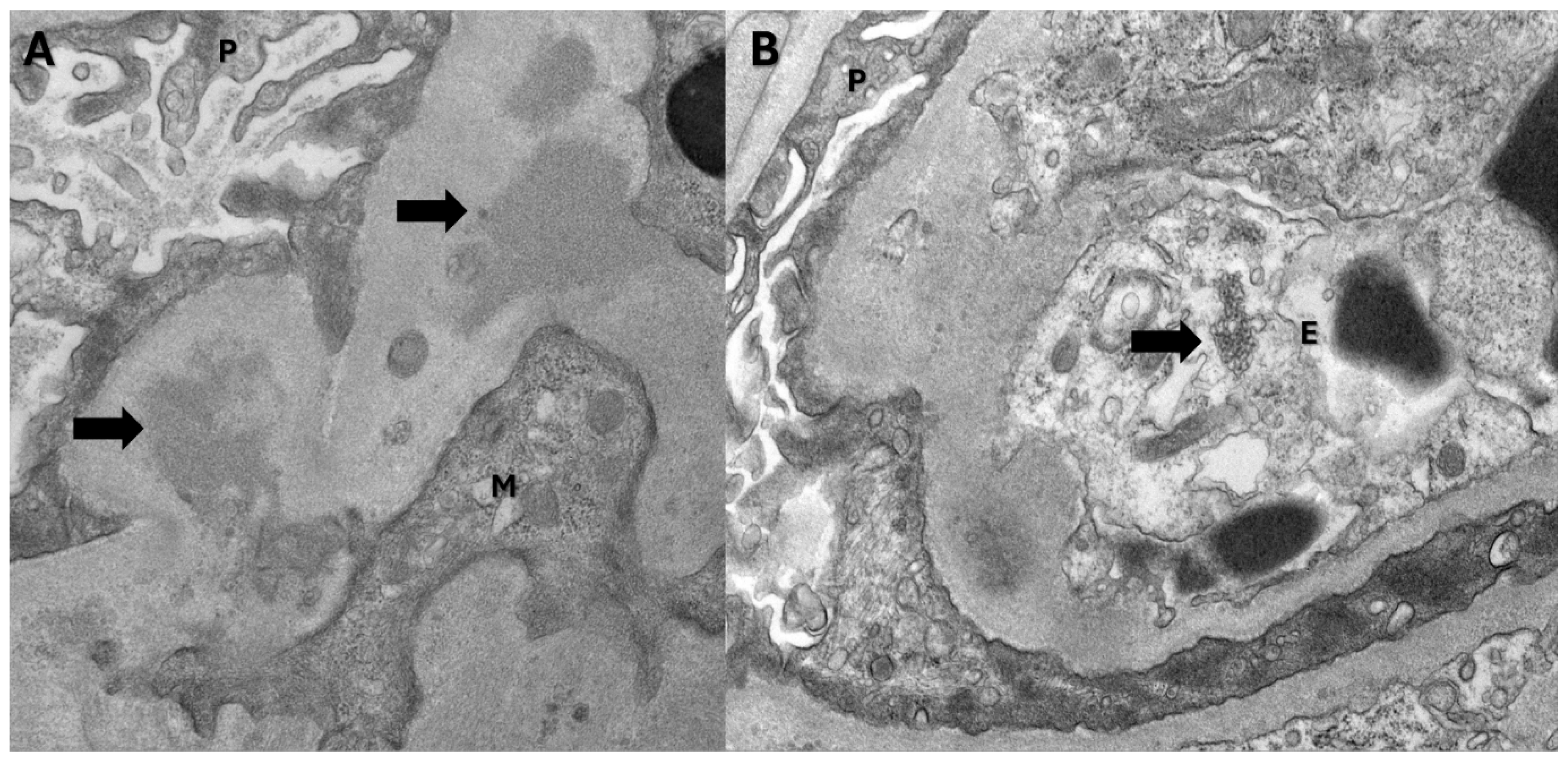
Figure 3.
Biopsy slide with CD 10 staining of the Proximal tubule.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Albumin/creatinine trend over time; Figure S2: creatinine trend over time; Figure S3: eGFR variation over time; Table S1: Complete Blood Count (CBC) Results Summary; Table S2: Infectious and Autoimmune Serology Re-sults Summary; Table S3: Urinalysis Results Summary
Author Contributions
1. Dr.Praveen Errabelli- conceptualization, data curation, original draft preparation, review and editing. 2. Dr.Lathiya Maulik-original draft preparation, Review and editing. 3. Dr.Neeharik Mareedu- review and editing. 4. Dr.Hernandez-Resources, review and editing.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study as it was only a case report.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
All data pertaining to this study is presented in the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wang, S.Y.; Bu, R.; Zhang, Q.; Liang, S.; Wu, J.; Liu, X.Z.S.; Cai, G.Y.; Chen, X.M. Clinical, Pathological, and Prognostic Characteristics of Glomerulonephritis Related to Staphylococcal Infection. Medicine 2016, 95, e3386. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chávez-Valencia, V.; Orizaga-de-la-Cruz, C.; Lagunas-Rangel, F.A. Acute Kidney Injury in COVID-19 Patients: Pathogenesis, Clinical Characteristics, Therapy, and Mortality. Diseases 2022, 10, 53. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pei, G.; Zhang, Z.; Peng, J.; Liu, L.; Zhang, C.; Yu, C.; Ma, Z.; Huang, Y.; Liu, W.; Yao, Y.; Zeng, R.; Xu, G. Renal Involvement and Early Prognosis in Patients with COVID-19 Pneumonia. J. Am. Soc. Nephrol. 2020, 31, 1157–1165. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sharma, P.; Uppal, N.N.; Wanchoo, R.; Shah, H.H.; Yang, Y.; Parikh, R.; Khanin, Y.; Madireddy, V.; Larsen, C.P.; Jhaveri, K.D.; Bijol, V. Northwell Nephrology COVID-19 Research Consortium. COVID-19-Associated Kidney Injury: A Case Series of Kidney Biopsy Findings. J. Am. Soc. Nephrol. 2020, 31, 1948–1958. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ronco, C.; Reis, T. Kidney involvement in COVID-19 and rationale for extracorporeal therapies. Nat. Rev. Nephrol. 2020, 16, 308–310. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wishahi, M.; Kamal, N.M. Multidisciplinary basic and clinical research of acute kidney injury with COVID-19: Pathophysiology, mechanisms, incidence, management and kidney transplantation. World J. Nephrol. 2022, 11, 105–114. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Klomjit, N.; Zand, L.; Cornell, L.D.; Alexander, M.P. COVID-19 and Glomerular Diseases. Kidney Int. Rep. 2023, 8, 1137–1150. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kudose, S.; Batal, I.; Santoriello, D.; Xu, K.; Barasch, J.; Peleg, Y.; Canetta, P.; Ratner, L.E.; Marasa, M.; Gharavi, A.G.; Stokes, M.B.; Markowitz, G.S.; D'Agati, V.D. Kidney Biopsy Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1959–1968. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shetty, A.A.; Tawhari, I.; Safar-Boueri, L.; Seif, N.; Alahmadi, A.; Gargiulo, R.; Aggarwal, V.; Usman, I.; Kisselev, S.; Gharavi, A.G.; Kanwar, Y.; Quaggin, S.E. COVID-19-Associated Glomerular Disease. J. Am. Soc. Nephrol. 2021, 32, 3340. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mateus, C.; Theias Manso, R.; Martins, A.R.; Branco, P.Q. Membranous nephropathy after a recent SARS-CoV-2 infection. BMJ Case Rep. 2023, 16, e252468. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Göndör, G.; Ksiazek, S.H.; Regele, H.; Kronbichler, A.; Knechtelsdorfer, M.; Säemann, M.D. Development of crescentic membranoproliferative glomerulonephritis after COVID-19 vaccination. Clin. Kidney J. 2022, 15, 2340–2342. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Kim, E.H.; Roh, Y.H.; et al. Glomerulonephritis following COVID-19 infection or vaccination: a multicenter study in South Korea. Kidney Res. Clin. Pract. 2024, 43, 165–176. [Google Scholar] [CrossRef]
- Winkler, A.; Zitt, E.; Sprenger-Mähr, H.; Soleiman, A.; Cejna, M.; Lhotta, K. SARS-CoV-2 infection and recurrence of anti-glomerular basement disease: a case report. BMC Nephrol. 2021, 22, 75. [Google Scholar] [CrossRef] [PubMed]
- Ta, H.; Awada, H.; Kang, P.; et al. Antineutrophil Cytoplasmic Autoantibody (ANCA)-Associated Vasculitis with Mucosal Involvement Following COVID-19 Pneumonia. Cureus 2022, 14, e31441. [Google Scholar] [CrossRef]
- Pfister, F.; Vonbrunn, E.; Ries, T.; et al. Complement Activation in Kidneys of Patients With COVID-19. Front. Immunol. 2021, 11, 594849. [Google Scholar] [CrossRef] [PubMed]
- Ueda, H.; Okabe, M.; Shimizu, A.; Yokote, S.; Nakashima, A.; Tsuboi, N.; Ikeda, M.; Miyazaki, Y.; Yokoo, T. Gross Hematuria Following SARS-CoV-2 Infection in IgA Nephropathy: A Report of 5 Cases. Kidney Med. 2023, 5, 100627. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yılmaz, E.K.; Saygılı, S.; Musayeva, G.; Gülmez, R.; Ağbaş, A.; Özlük, Y.; Canpolat, N. A case of crescentic glomerulonephritis with exacerbation of pre-existing IgA nephropathy after COVID-19. Turk J Pediatr. 2024, 66, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Perkins, G.B.; Anandh, U.; Coates, P.T. COVID and the Kidney: An Update. Semin. Nephrol. 2023, 43, 151471. [Google Scholar] [CrossRef]
- Izci Duran, T.; Turkmen, E.; Dilek, M.; Sayarlioglu, H.; Arik, N. ANCA-associated vasculitis after COVID-19. Rheumatol. Int. 2021, 41, 1523–1529. [Google Scholar] [CrossRef]
- Smith, R.J.H.; Appel, G.B.; Blom, A.M.; et al. C3 glomerulopathy - understanding a rare complement-driven renal disease. Nat. Rev. Nephrol. 2019, 15, 129–143. [Google Scholar] [CrossRef]
- Kronbichler, A.; Gauckler, P.; Windpessl, M.; et al. COVID-19: implications for immunosuppression in kidney disease and transplantation. Nat. Rev. Nephrol. 2020, 16, 365–367. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



