Submitted:
26 March 2025
Posted:
27 March 2025
You are already at the latest version
Abstract
Maternal influenza vaccination (MIV) is the most effective measure of preventing severe influenza-related complications in pregnant women. However, there is limited knowledge about MIV uptake in Kuwait. This study aimed to assess pregnant women’s knowledge, attitudes, and perceptions regarding MIV uptake and provision. Methods: A cross-sectional online survey, based on the TIP-FLU framework, was conducted among 272 pregnant and recently delivered women attending government maternity hospitals and antenatal clinics across Kuwait. Results: The influenza vaccination rate was low, with only 8.1% of participants vaccinated. Additionally, 58.8% of participants had a knowledge score on influenza infection and prevention below the median, while 92% had a knowledge score on MIV uptake below the median. Furthermore, 63% reported that their healthcare providers (HCPs) did not recommend MIV. Participants expressed neutral responses regarding social relationships, media, and religion as influences on MIV uptake (median=3.0; IQRs=2.0, 1.0) on a 1–5 scale. Strategies to improve uptake were identified, with participants emphasising the importance of obstetricians recommending MIV during pregnancy (median=5.0; IQR=1.0). They also highlighted the need for accessible educational materials, such as posters, leaflets, or social media content from the Ministry of Health (median=5.0; IQR=1.0). Conclusions: Health promotion campaigns are needed to increase MIV awareness and acceptance among pregnant women. Further research is required to explore MIV provision and uptake from HCPs’ perspectives.
Keywords:
Influenza
; Vaccination
; Pregnant women
; Healthcare providers
; Kuwait
1. Introduction
Influenza infection can be serious, leading to severe respiratory illness and increased morbidity and mortality. H1N1 was responsible for the pandemic in 2009 that led to more than 250,000 deaths globally [1]. Pregnant women are at higher risk for influenza infection due to their modified immune system [2]. Therefore, the World Health Organisation (WHO) [3] recommends annual vaccinations against influenza, especially for high-risk groups, including pregnant women.
Although annual influenza vaccination campaigns are conducted in Kuwait, there is no specific programme designed to target pregnant women. Additionally, there are no published data about current MIV coverage in Kuwait. Two central targets in public health are increasing vaccine uptake rates and improving maternal health. The WHO prioritises maternal health as a human right and links it to the efforts for universal health coverage [4]. In its sustainable development goals, the United Nations [5] called for promoting universal maternal health to prevent infectious diseases; vaccination is the most cost-effective way of doing this.
The risk of infectious diseases is high in Kuwait for two main reasons. The first reason is Hajj [6], when more than 2 million pilgrims from 160 countries meet in Mecca, including approximately 8000 pilgrims from Kuwait [7]. The second reason is the demography of Kuwait, where expats represent more than two-thirds of the population, potentially affecting the transmission of infectious diseases and lowering vaccine coverage rates [7,8]. Therefore, pregnant women in Kuwait are at an increased risk of contracting influenza, and the provision of MIV needs be considered among the vaccination programmes provided in pregnancy to avoid influenza infection complications.
Despite the importance of the influenza vaccine, there is a notable lack of research in Kuwait regarding knowledge and attitudes among pregnant women toward maternal influenza vaccine (MIV). Questions such as what factors can influence pregnant women to ward the uptake of MIV need to be addressed. Therefore, the aim of the study is to explore pregnant women’s knowledge, attitudes and perceptions regarding the uptake of MIV in Kuwait.
2. Materials and Methods
2.1. Study Design, Population and Sampling
A cross-sectional study was carried out in governmental maternity hospitals across six governmental regions of Kuwait. The research used opportunistic sampling of pregnant and recently delivered women who were visiting governmental maternity hospitals and their antenatal clinics. Since the influenza vaccination campaign is conducted annually from November to February, data collection started in March posed a potential risk of selection bias if only pregnant women were included. To mitigate this, recently delivered women were also included in the study. Their recent experience with the vaccination decision-making process ensured more accurate and reliable responses. Data collection took place from March to June 2022.
2.2. Recruitment and Data Collection
To determine the required sample size for the survey, the most recent published hospital statistics on the number of deliveries across Kuwait’s governorates in 2019 were utilised. According to previous published papers [9,10,11,12,13], for 95% confidence level, 5% margin of error, 50% response proportion and population size (N = 53,774) and after applying the formula n= (z 2 × p × q)/d2 , where:
- Z is the Z-score for a 95% confidence level (1.96)
- p is the response proportion (0.5)
- q=1−p=0.5
- E is the margin of error (0.05)
Using this formula, the calculated required sample size was 381 participants, ensuring statistical validity and representativeness of the study population.
A survey was derived from the Tailoring Immunisation Programme (TIP-FLU) (2017) guidance survey questionnaire [14]. The survey consisted of six groups of questions, including demographics, childhood vaccination, influenza and influenza prevention during pregnancy, influenza vaccination during pregnancy, influenza infection experience and information about influenza and influenza vaccination. The six groups of questions contained subsequent questions with different response options.
2.3. Pilot Study
Before the main data collection, a pilot study was conducted to identify any possible difficulties with processing, collecting, and analysing the data and confirm that the respondents correctly understood the questions to determine any necessary modifications. Following the pilot study some changes to the wording were made to increase clarity. Some questions were removed because they were unclear, culturally insensitive or irrelevant to the study’s aim and objectives; some questions were added, following the most recent evidence-based available about MIV provision and uptake (Supplementary 1). No data from the pilot study were used in the final analysis.
2.4. Survey Questionnaire Tool, Locations and Delivery
The web-based software tool, the Joint Information Systems Committee survey in Bristol, UK, was used for the online survey. Posters with QR codes linking to the survey were placed in six hospitals and disseminated at different hospital departments, including antenatal care, emergency rooms, hospitals’ waiting rooms, and prelabour rooms. The average time taken to complete the survey was eight minutes. The survey was available in both Arabic and English to accommodate participants’ preferences. The survey was closed on June 30, 2022. The Arabic dataset was retranslated into English. Then, the two datasets were exported into SPSS software (version 28.0; SPSS Inc., Chicago, USA) and merged. All statistical analyses were undertaken using SPSS.
2.5. Data Analysis
The data were cleaned and checked for missing data; there were two entries with missing responses, and they were discarded. Normality tests were performed using the Kolmogorov–Smirnov and Shapiro–Wilk tests, both showed p-values less than 0.05, indicating a violation of normality. Categorical variables were summarised as frequencies and percentages, and continuous data were summarised using medians and interquartile ranges (IQRs), as the data were not normally distributed.
3. Results
3.1. Characteristics of the Study Population
A total of 272 pregnant and recently delivered women from across Kuwait responded to the survey, constituting 71% of the required sample. Among the participants, 30.5% were aged between 28 and 32 years. The majority (73.2%) were Kuwaiti nationals, and 93.4% identified as Muslim, reflecting the demographic composition of the study population. All participants had received some form of education; the highest level of education for the majority of the participants (86.4%) was higher education, including university graduates and post-graduates. About half of the participants (47.2%) were in their third trimester. In addition, more than two-thirds of the participants (73.7%) had previous pregnancy/pregnancies. 8.1% of the participants received MIV during their current/most recent pregnancy, whereas 91.9% of the participants did not. Moreover, 79.2% of the participants could not remember receiving any vaccines during their past pregnancy/pregnancies, including influenza, tetanus, diphtheria, and pertussis. The sociodemographic and pregnancy characteristics of the sample are presented in Table 1.
3.2. Knowledge About Influenza Infection and Prevention Measures
Participants’ knowledge about influenza infection and prevention varied. Of the participants 43.4% agreed that the influenza vaccine can prevent influenza infection, while 36.4% disagreed. Most of the participants (85.3%) believed that taking vitamin supplements can prevent influenza infection. More than half of the participants (54.0%) believed that natural remedies could prevent influenza infection. However, 73.9% of the participants understood that a healthy lifestyle, including exercise and diet, could prevent influenza infection and 91.5% of the participants indicated that good hand hygiene could prevent influenza infection. Furthermore, the overall knowledge score showed that more than half (58.8%) of the participants had a low level of knowledge about influenza infection and prevention Table 2.
Knowledge score above the median
3.2. Knowledge About MIV Uptake During Pregnancy
Forty-three percent of the participants were unsure whether MIV can prevent complications caused by influenza infection and 50.7% of the participants did not know whether MIV could provide immunity for the first six months of their neonate’s life. About half of the participants (46.7%) disagreed that influenza is considered a serious infection. The created knowledge score showed that 92% of the participants showed a knowledge score below the median (mid-point of data) on knowledge about MIV, Table 3.
3.2. Perceptions and Attitudes of Vaccinated Participants Toward MIV Uptake
Among the vaccinated participants (60%) strongly disagreed that influenza was a serious disease during pregnancy (median= 5.0; IQR= 1.0) while 98% of unvaccinated participants agreed (median=4, IQR= 1.0). 85% of unvaccinated participants were unsure whether getting the MIV had any side effects on them or their unborn children (median= 3.0; IQR= 1.0). Additionally, 76% of unvaccinated participants did not have a definite opinion, neither disagreed nor agreed, on several statements, such as whether the MIV vaccine was effective in protecting against influenza infection complications during pregnancy (median= 3.0; IQR= 1.0), and whether their immunity was strong during pregnancy which could provide prevention against infection (median= 3.0; IQR= 1.0). However, 72% of vaccinated participants disagreed that getting MIV had side effects on them or their unborn children (median=4.0; IQ=1) while 76% of vaccinated participants were unsure whether MIV was effective in protecting them against influenza complications (Figure 1) (Medians and IQRs are presented in Supplementary material 2 and Supplementary material 3).
3.2. HCPs Recommendations and Provision of MIV
68.5% of the participants agreed that their HCPs recommended the uptake of MIV without offering it. Furthermore, 63% of the participants stated that their HCPs did not recommend or offer the MIV and 25.9% of the participants could not remember while 10.1% of the participants disagreed with the statement that their HCPs did not recommend or offer the MIV (Figure 2).
3.2. Influence of Different HCPs Toward MIV
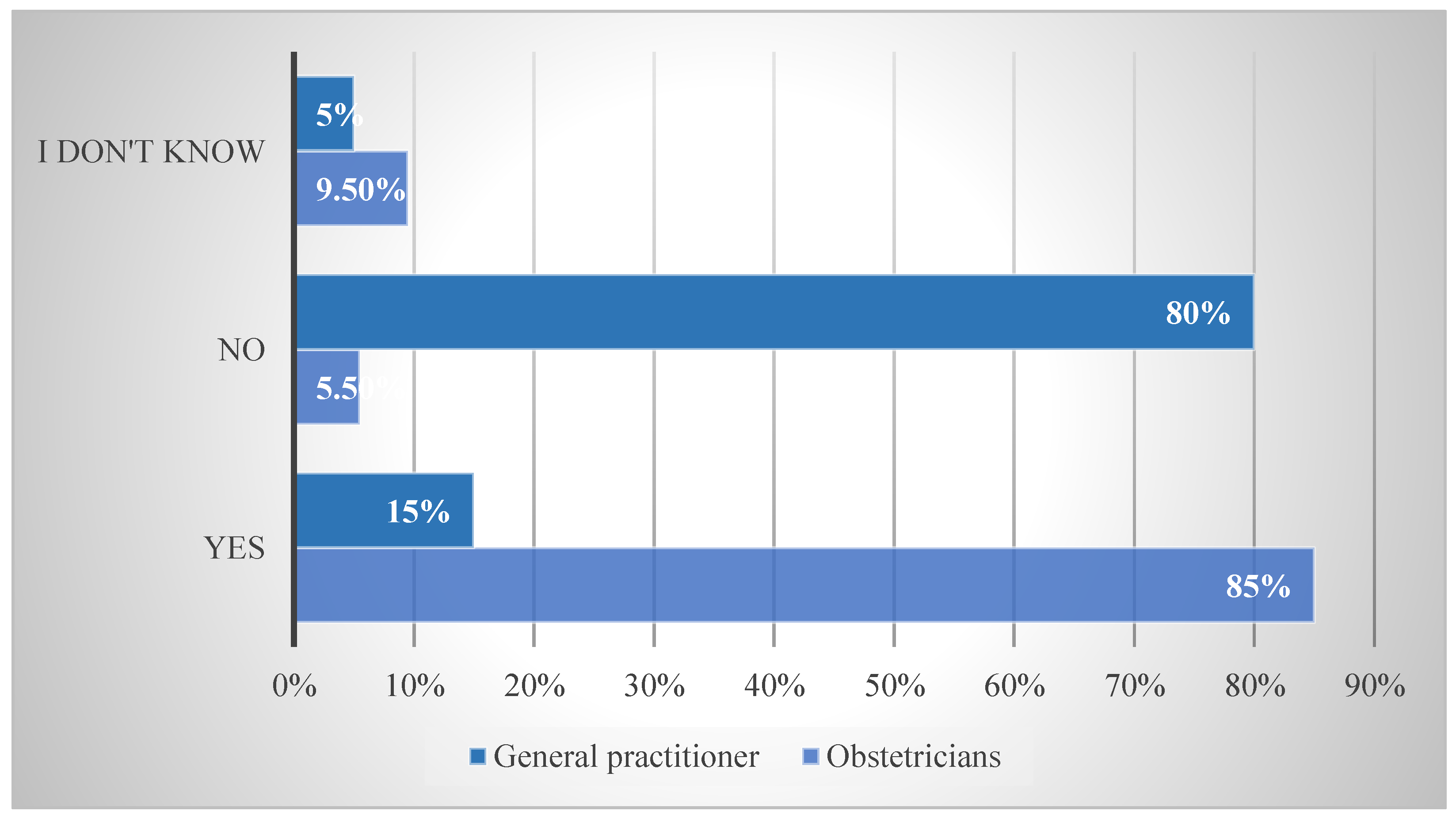
To understand the influence of different HCPs in recommending MIV uptake among pregnant women, participants were asked if it was important to receive recommendations for MIV from their obstetricians and general practitioners. The results showed that participants considered it was extremely important to obtain recommendations from and conversation with their obstetricians regarding the uptake of MIV (median= 5.0; IQR= 1.0). They also indicated that receiving MIV recommendations and discussion of MIV from their family physician was very important (median= 4.0; IQR= 3.0) (Figure 2) (medians and IQRs are presented in Supplementary material 4).
Figure 3.
Pregnant women preferences of HCPs in recommending and discussing MIV uptake.
3.2. Importance of Different Influences on Pregnant Women’s Perceptions Toward MIV Uptake
Participants were asked about the impact of various social relationships on their decision related to uptake of MIV. Participants did not express disagreement or agreement regarding the influence of different social relationships on their decision to receive MIV during pregnancy, including relationships with their husband, parents, other family members, and friends. The median response for all relationships was 3.0, with an IQR of 2.0. In addition, participants neither agreed nor disagreed that social media or religious beliefs were important in influencing their opinion on the uptake of MIV (median=3; IQR= 1, for both) (Figure 4) (Details on medians and IQR are presented in Error! Reference source not found.Error! Reference source not found.).
3.2. Recommendations to Enhance the Uptake of MIV
Participants were asked to rate the importance of various measures to encourage their uptake of MIV. They reported that consulting with their obstetricians about the MIV uptake was extremely important (median= 5.0; IQR=1.0). Additionally, they indicated that receiving information on the safety of MIV during pregnancy through posters, leaflets, and ministry of health social media channels was also very important (median= 4.0; IQR= 2.0). Furthermore, they considered it extremely important to receive information about the seriousness of influenza infection for pregnant women and their newborns, delivered through posters, leaflets, and social media channels from the ministry of health (median= 5.0; IQR= 1.0) (Table 4).
4. Discussion
This study is, to our knowledge, the first to examine pregnant women’s knowledge, attitudes, and perceptions regarding the uptake of the influenza vaccine (MIV) in Kuwait. Our findings indicate that MIV uptake was low among the participants, which may reflect the overall vaccine coverage in the country. Additionally, pregnant women demonstrated a low level of knowledge about influenza infection and vaccination. The study also highlighted the important role HCPs play in recommending MIV, with obstetricians being particularly prioritised by pregnant women for MIV recommendations and discussions over other healthcare providers. Furthermore, despite the potential influence of social relationships, the opinions of husbands, parents, family members, or friends did not appear to affect pregnant women’s decisions regarding MIV. Furthermore, the study showed that providing pregnant women with targeted health information materials could enhance their knowledge and improve vaccine acceptance.
One of the main findings of this study is that pregnant women’s overall knowledge of influenza infection and prevention is low; most participants had a low-risk perception toward influenza infection. Published literature indicated that a lack of knowledge about influenza infection and its preventive measures contributes to a low perception of risk among pregnant women, making them more likely to reject MIV uptake [15,16,17,18,19,20,21,22,23,24,25,26,27,28]. According to Castillo et al. [28] pregnant women do not feel the need to protect their foetuses and perceive pregnancy as a “protected state”. Some pregnant women not only underestimated their risk of contracting influenza infection but also thought that the side effects of MIV were higher compared to the effects of an influenza infection [29]. For other pregnant women, MIV is simply not a priority [30].
Another finding of this study was the vital role of healthcare providers (HCPs) in recommending MIV for pregnant women; our findings showed that pregnant women would prefer to have recommendation about MIV uptake from their HCPs. Several published studies have examined the influence of HCPs recommendation about MIV on pregnant women [31,32,33,34,35,36,37,38,39]. A systematic review and meta-analysis conducted in 2020 aimed to identify factors influencing the decision-making process regarding vaccination among pregnant women [35]. The review concluded that pregnant women who received a recommendation from their HCPs were ten to twelve times more likely to receive MIV. Studies showed that the likelihood of pregnant women receiving the MIV is significantly higher when they receive a recommendation for vaccination from their HCPs [21,31,34,35,36]. Therefore, HCPs are considered significant influencers in the decision-making process of pregnant women regarding MIV and the recommendations of HCPs have a significant impact on pregnant women’s likelihood of accepting MIV.
The findings revealed that obstetricians and general practitioners play a crucial role in influencing pregnant women’s acceptance of MIV uptake. When asked about their preferred healthcare providers for discussing MIV, participants emphasised that receiving a recommendation from their obstetrician was extremely important to their decision-making process. Multiple studies have examined how the trust-based relationship between pregnant women and their HCPs can influence the acceptance of MIV. For instance, a qualitative study highlighted that pregnant women place significant trust in their obstetricians to manage their health due to their expertise [31]. The study emphasised the importance of the HCP-patient relationship, where pregnant women feel comfortable discussing and questioning their obstetricians about MIV, confident in their knowledge. However, a qualitative review by Alhendyani et al. [40]. examining global perspectives of HCPs on MIV concluded that the level of trust between pregnant women and their HCPs can be influenced by the duration of their relationship, the knowledge of the HCPs, and the way MIV discussions are initiated.
In our study, we investigated the influence of various social relationships on pregnant women’s decisions regarding the uptake of MIV. Our findings revealed that, in Kuwait, pregnant women are not swayed by the opinions of their husbands, parents, family members, or friends when it comes to accepting MIV. This finding contradicts several published studies [31,41,42,43]. For instance, a study conducted in Kenya [31] indicated that, in societies where men hold dominance over women, pregnant women often face barriers to receiving antenatal care due to their husbands’ influence. This dynamic could contribute to the low uptake of MIV in such regions. Conversely, in China, HCPs struggle to convince pregnant women to receive MIV. In these cases, influential family members, like mothers-in-law, often prohibit them from getting vaccinated [41]. Additionally, in Pakistan, a study found that 88% of the participants identified their husbands and parents-in-law as the primary decision-makers regarding their healthcare, regardless of their own intentions to accept MIV [42]. However, in England, pregnant women requested advice from their contacts not to acquire information or inform decisions about MIV uptake but rather to engage in personally focused discussions, receive advice, and feel support from their associations [43].
Furthermore, our study showed that providing pregnant women with health information materials could enhance their acceptance toward MIV uptake. Pregnant women often remain uninformed about the general influenza vaccine recommendation during their pregnancy, including MIV, primarily due to insufficient information and inadequate guidance from HCPs [15]. Many reasons have been discussed in published studies for the lack of knowledge and, hence, low uptake of MIV among pregnant women; for example, Prospero et al. [29] found that pregnant women are often unaware of the guidelines for maternal influenza vaccines, including MIV. This lack of awareness is related to the absence of discussion and recommendations from their HCPs and lack of provision of health information materials. Therefore, the availability and the provision of different health education materials in the form of posters in the hospital waiting rooms, leaflets and brochures about the significance of influenza infection and its complications, as well as the importance of the uptake of MIV during pregnancy, are essential to eliminate pregnant women concerns and promote MIV uptake [44,45,46].
This study has several limitations. First, as a cross-sectional study, it is not possible to infer causality because temporal sequence cannot be established. Second, the study sample was not randomly selected; rather, it was an opportunistic sample, which limits generalisability and affects the external validity of the findings. The sample was drawn from individuals attending governmental health services, which predominantly represents the lower- and middle-class population. This may introduce confounding variables, as health-seeking behaviours and perceptions can differ between patients using private and public healthcare facilities. Additionally, not reaching the required sample size is another limitation. This could have impacted the generalizability of the findings, as a smaller sample size may not fully represent the target population, potentially introducing bias and limiting the robustness of the results.
Despite these limitations, we obtained important information giving an overview of pregnant women’s knowledge, attitudes and perceptions about MIV in Kuwait using a validated survey questionnaire by the WHO European region.
5. Conclusions
Despite the recommendations concerning the uptake of MIV during pregnancy, there is a notable gap in pregnant women’s understanding of the complications associated with influenza infection and vaccination in Kuwait. This highlights the need for health education programmes aimed at increasing awareness about MIV and its efficacy and safety among this population.
Furthermore, these findings indicate the necessity for additional studies to identify barriers faced by HCPs regarding influenza vaccination in Kuwait. It is essential to educate and train obstetricians to enhance their roles in recommending and discussing MIV, which could potentially enhance the uptake of MIV among pregnant women in Kuwait.
Appendix A
Appendix A.1

Table A1.
Modified survey questions, sub-questions and responses.
|
Group |
Sub-group | responses |
|---|---|---|
| Demography | Nine questions. | Choose one answer |
| Questions about influenza and influenza prevention during pregnancy | Influenza infection’s preventive measures. | Yes No I do not know |
| Knowledge of MIV provision in Kuwait. | Agree Disagree I do not now |
|
| In the third to sixth questions, about the timing and form in which knowledge about MIV was delivered. | Choose one answer. | |
| Questions about influenza vaccination during pregnancy | Questions about vaccination history, including MIV and COVID-19 vaccines. | Yes No I cannot remember |
| The rule of the different specialists of HCPs in MIV recommendations. | Participants can select all answers that apply (can be more than one). | |
| Vaccinated participants were asked thirteen questions about their perception of MIV. | Likert Scale of five responses for the importance. | |
| Seventeen questions to be answered by non-vaccinated participants about their perception of MIV. | Likert scale of five responses for the agreement with a statement. |
|
| Six questions about how the perception of non-vaccinated participants could be changed for future acceptance of MIV uptake. Vaccinated and non-vaccinated participants answered this category. | Likert scale of six responses for importance, participants can choose a “Not applicable” answer. |
Appendix A.2
Table A2.
Medians and IQR of unvaccinated participants’ attitudes and perceptions toward influenza and MIV uptake during pregnancy.
Table A2.
Medians and IQR of unvaccinated participants’ attitudes and perceptions toward influenza and MIV uptake during pregnancy.
| Influenza Statement | Median | Q1-Q3 | IQR |
|---|---|---|---|
| Influenza is not a serious disease during pregnancy | 4.0 | 3.0-4.0 | 1.0 |
| I am concerned about vaccine side effects for myself | 3.0 | 3.0-4.0 | 1.0 |
| I am concerned about vaccine side effects for my baby | 3.0 | 3.0-4.0 | 1.0 |
| The vaccine isn’t effective in protecting against influenza | 3.0 | 3.0-4.0 | 1.0 |
| My immunity is strong during pregnancy, and this protects me from influenza. | 3.0 | 3.0-4.0 | 1.0 |
Appendix A.3
Table A3.
Medians and IQR of vaccinated participants’ attitudes and perceptions toward influenza and MIV uptake during pregnancy.
Table A3.
Medians and IQR of vaccinated participants’ attitudes and perceptions toward influenza and MIV uptake during pregnancy.
| Influenza Statement | Median | Q1-Q3 | IQR |
|---|---|---|---|
| Influenza is not a serious disease during pregnancy | 5.0 | 4.0-5.0 | 1.0 |
| I am concerned about vaccine side effects for myself | 4.0 | 3.0-4.0 | 1.0 |
| I am concerned about vaccine side effects for my baby | 4.0 | 3.0-4.0 | 1.0 |
| The vaccine isn’t effective in protecting against influenza | 3.0 | 3.0-4.0 | 1.0 |
| My immunity is strong during pregnancy, and this protects me from influenza. | 4.0 | 3.0-4.0 | 1.0 |
Appendix A.4
Table A4.
Medians and IQRs of the importance of HCP’s recommendations about MIV uptake.
| HCP’ recommendations | Median | Q1-Q3 | IQR |
|---|---|---|---|
| It is important to get a recommendation from my family physician about MIV | 4.0 | 1.75-5.0 | 3.0 |
| It is important to get a recommendation from my obstetrician about MIV | 5.0 | 3.75-5.0 | 1.0 |
Appendix A.5
Table A5.
Medians and IQR for different social relationships, social media and religious beliefs influence participants’ perceptions toward MIV uptake.
Table A5.
Medians and IQR for different social relationships, social media and religious beliefs influence participants’ perceptions toward MIV uptake.
| Social Relations’ Influence | Median | Q1-Q3 | IQR | |||
|---|---|---|---|---|---|---|
| Husband | 3.0 | 2.0-4.0 | 2.0 | |||
| Parents | 3.0 | 2.0-4.0 | 2.0 | |||
| Other family members (mother-in-law, sisters, etc.) | 3.0 | 3.0-4.0 | 2.0 | |||
| Friends | 3.0 | 3.0-4.0 | 2.0 | |||
| Social media | 3.0 | 2.0-4.0 | 1.0 | |||
| Religion | 3.0 | 2.0-4.0 | 1.0 | |||
References
- Centers for Disease Control and Prevention. Understanding flu viruses [Internet]. Atlanta: CDC; 2019 [cited 2021 Jan 28]. Available from: https://www.cdc.gov/flu/about/viruses/index.htm.
- Somerville L, Basile K, Dwyer D, Kok J. The impact of influenza virus infection in pregnancy. Future Microbiol. 2018; 13:263–74. [CrossRef]
- World Health Organization. Influenza (seasonal) [Internet]. Geneva: WHO; 2018 [cited 2021 Jan 28]. Available from: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal).
- World Health Organization. Maternal health [Internet]. Geneva: WHO; 2020 [cited 2020 Aug 3]. Available from: https://www.who.int/health-topics/maternal-health#tab=tab_3.
- United Nations. SDG media zone – the importance of vaccines [Internet]. 2020 [cited 2020 Aug 3]. Available from: https://www.un.org/sustainabledevelopment/?p=86081.
- Gautret P, Bauge M, Simon F, Benkouiten S, Parola P, Brouqui P. Pneumococcal vaccination and Hajj. Int J Infect Dis. 2011;15(10): e730.
- Feldman C, Abdulkarim E, Alattar F, Al Lawati F, Al Khatib H, Al Maslamani M, et al. Pneumococcal disease in the Arabian Gulf: recognizing the challenge and moving toward a solution. J Infect Public Health. 2013; 6:401–9. [CrossRef]
- AlEnizi A, AlSaeid K, Alawadhi A, Hasan E, Husain E, AlFadhli A, et al. Kuwait recommendations on vaccine use in people with inflammatory rheumatic diseases. Int J Rheumatol. 2018; 2018:1–12. [CrossRef]
- Mayet A, Al-Shaikh G, Al-Mandeel H, Alsaleh N, Hamad A. Knowledge, attitudes, beliefs, and barriers associated with the uptake of influenza vaccine among pregnant women. Saudi Pharm J. 2017;25(1):76–82. [CrossRef]
- Barry M, Aljammaz K, Alrashed A. Knowledge, attitude, and barriers influencing seasonal influenza vaccination uptake. Can J Infect Dis Med Microbiol. 2020; 2020:1–6. [CrossRef]
- Otieno N, Nyawanda B, Otiato F, Adero M, Wairimu W, Atito R, et al. Knowledge and attitudes towards influenza and influenza vaccination among pregnant women in Kenya. Vaccine. 2020;38(43):6832–8. [CrossRef]
- Bödeker B, Walter D, Reiter S, Wichmann O. Cross-sectional study on factors associated with influenza vaccine uptake and pertussis vaccination status among pregnant women in Germany. Vaccine. 2014;32(33):4131–9. [CrossRef]
- Quattrocchi A, Mereckiene J, Fitzgerald M, Cotter S. Determinants of influenza and pertussis vaccine uptake in pregnant women in Ireland: A cross-sectional survey in 2017/18 influenza season. Vaccine. 2019;37(43):6390–6.
- World Health Organization Regional Office for Europe. Tailoring immunization programmes for seasonal influenza (TIP FLU) - a guide for increasing pregnant women’s uptake of seasonal influenza vaccination (2017) [Internet]. Geneva: WHO; 2021 [cited 2021 May 17]. Available from: https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/publications/2017/tailoring-immunization-programmes-for-seasonal-influenza-tip-flu-a-guide-for-increasing-pregnant-womens-uptake-of-seasonal-influenza-vaccination-2017.
- Adeyanju GC, Engel E, Koch L, et al. Determinants of influenza vaccine hesitancy among pregnant women in Europe: a systematic review. Eur J Med Res. 2021; 26:116. [CrossRef]
- Yuen C, Dodgson J, Tarrant M. Perceptions of Hong Kong Chinese women toward influenza vaccination during pregnancy. Vaccine. 2016;34(1):33–40. [CrossRef]
- Okoli GN, Reddy VK, Al-Yousif Y, Neilson CJ, Mahmud SM, Abou-Setta AM. Sociodemographic and health-related determinants of seasonal influenza vaccination in pregnancy: A systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2021;100(6):997–1009.
- Ahluwalia IB, Jamieson DJ, Rasmussen SA, D’Angelo D, Goodman D, Kim H. Correlates of seasonal influenza vaccine coverage among pregnant women in Georgia and Rhode Island. Obstet Gynecol. 2010; 116:949–55. [CrossRef]
- Payandeh Sh, Nabavi N, Movahedinia S, Poudineh V, Afzoon S, Malakoti N. Pregnant women’s knowledge, attitude, practice, and barriers associated with the uptake of influenza vaccination: a systematic review. Health Provid. 2023;3(1):37–54.
- Smith S, Sim J, Halcomb E. Nurses’ knowledge, attitudes and practices regarding influenza vaccination: An integrative review. Journal of Clinical Nursing. 2016;25(19–20):2730–44. 21. [CrossRef]
- Dhaouadi S, Kharroubi G, Cherif A, Cherif I, Bouguerra H, Bouabid L, et al. Knowledge attitudes and practices toward seasonal influenza vaccine among pregnant women during the 2018/2019 influenza season in Tunisia. PLOS ONE. 2022;17(3): e0265390. 22.
- Morales KF, Menning L, Lambach P. The Faces of Influenza Vaccine Recommendation: A Literature Review of the determinants and barriers to health providers’ recommendation of influenza vaccine in pregnancy. Vaccine. 2020;38(31):4805–15. 23. [CrossRef]
- Bödeker B, Walter D, Reiter S, Wichmann O. Cross-sectional study on factors associated with influenza vaccine uptake and pertussis vaccination status among pregnant women in Germany. Vaccine. 2014; 32(33):4131-9. 24. [CrossRef]
- Bödeker B, Betsch C, Wichmann O. Skewed risk perceptions in pregnant women: the case of influenza vaccination. BMC public health. 2015 Dec;15(1):1-1. [CrossRef]
- Maltezou HC, Koutroumanis PP, Kritikopoulou C, Theodoridou K, Katerelos P, Tsiaousi I, et al. Knowledge about influenza and adherence to the recommendations for influenza vaccination of pregnant women after an educational intervention in Greece. Hum Vaccin Immunother. 2019;15(5):1070-4. [CrossRef]
- Tuells J, Rodríguez-Blanco N, Torrijos JL, Vila-Candel R, Bonmati AN. Vaccination of pregnant women in the Valencian Community during the 2014-15 influenza season: a multicentre study. Rev Esp Quimioter. 2018;31(4):344.
- Vila-Candel R, Navarro-Illana P, Navarro-Illana E, Castro-Sánchez E, Duke K, Soriano-Vidal FJ, et al. Determinants of seasonal influenza vaccination in pregnant women in Valencia, Spain. BMC Public Health. 2016; 16:1-7. [CrossRef]
- Castillo E, Patey A, MacDonald N. Vaccination in pregnancy: Challenges and evidence-based solutions. Best Pract Res Clin Obstet Gynaecol. 2021; 76:83-95. [CrossRef]
- Prospero E, Galmozzi S, Paris V, Felici G, Barbadoro P, D’Alleva A, et al. Factors influencing refusal of flu vaccination among pregnant women in Italy: Healthcare workers’ role. Influenza Other Respir Viruses. 2019;13(2):201-7. [CrossRef]
- Maurici M, Dugo V, Zaratti L, Paulon L, Pellegrini MG, Baiocco E, et al. Knowledge and attitude of pregnant women toward flu vaccination: a cross-sectional survey. J Matern Fetal Neonatal Med. 2016;29(19):3147-50. [CrossRef]
- Bergenfeld I, Nganga S, Andrews C, Fenimore V, Otieno N, Wilson A, et al. Provider perspectives on demand creation for maternal vaccines in Kenya. Gates Open Res. 2018;2(34). [CrossRef]
- Marcus JA. Patient-physician relationships. In: Philosophy and Medicine. Dordrecht: Springer; 2008. p. (Humanizing Modern Medicine, vol 99).
- Barnard J, Dempsey A, Brewer S, Pyrzanowski J, Mazzoni S, O’Leary S. Facilitators and barriers to the use of standing orders for vaccination in obstetrics and gynecology settings. Am J Obstet Gynecol. 2017;216(1):69. e1–7. [CrossRef]
- Kaufman J, Attwell K, Hauck Y, Omer S, Danchin M. Vaccine discussions in pregnancy: interviews with midwives to inform design of an intervention to promote uptake of maternal and childhood vaccines. Hum Vaccin Immunother. 2019;15(11):2534–43. 2. [CrossRef]
- Kilich E, Dada S, Francis MR, Tazare J, Chico RM, et al. Factors that influence vaccination decision-making among pregnant women: A systematic review and meta-analysis. PLOS ONE. 2020;15(7): e0234827. [CrossRef]
- Taksdal SE, Mak DB, Joyce S, Tomlin S, Carcione D, Armstrong PK, Effler PV. Predictors of uptake of influenza vaccination: a survey of pregnant women in Western Australia. Aust Fam Physician. 2013;42(8):582-6. 4.
- Greyson D, Dubé È, Fisher WA, Cook J, Sadarangani M, Bettinger JA. Understanding influenza vaccination during pregnancy in Canada: attitudes, norms, intentions, and vaccine uptake. Health Educ Behav. 2021;48(5). [CrossRef]
- Herzog R, Álvarez-Pasquin MJ, Díaz C, Del Barrio JL, Estrada JM, Gil Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health. 2013; 13:1-7. 2.
- Kaoiean S, Kittikraisak W, Suntarattiwong P, Ditsungnoen D, Phadungkiatwatana P, Srisantiroj N, Asavapiriyanont S, Chotpitayasunondh T, Dawood FS, Lindblade KA. Predictors for influenza vaccination among Thai pregnant women: The role of physicians in increasing vaccine uptake. Influenza Other Respir Viruses. 2019;13(6):582-92. 3. [CrossRef]
- Alhendyani F, Jolly K, Jones LL. Views and experiences of maternal healthcare providers regarding influenza vaccine during pregnancy globally: A systematic review and qualitative evidence synthesis. PLOS ONE. 2022;17(2): e0263234. [CrossRef]
- Li R, Xie R, Yang C, Rainey J, Song Y, Greene C. Identifying ways to increase seasonal influenza vaccine uptake among pregnant women in China: A qualitative investigation of pregnant women and their obstetricians. Vaccine. 2018;36(23):3315–22. 2. [CrossRef]
- Khan AA, Varan AK, Esteves-Jaramillo A, Siddiqui M, Sultana S, Ali AS, Zaidi AK, Omer SB. Influenza vaccine acceptance among pregnant women in urban slum areas, Karachi, Pakistan. Vaccine. 2015;33(39):5103–9. [CrossRef]
- Wilson RJ, Chantler T, Lees S, Paterson P, Larson H. The patient–healthcare worker relationship: how does it affect patient views towards vaccination during pregnancy? In: Health and health care concerns among women and racial and ethnic minorities. Emerald Publishing Limited; 2017. p. 59–77. 4.
- Bruno S, Nachira L, Villani L, Beccia V, Di Pilla A, Pascucci D, Quaranta G, Carducci B, Spadea A, Damiani G, Lanzone A. Knowledge and beliefs about vaccination in pregnant women before and during the COVID-19 pandemic. Front Public Health. 2022; 10:903557. 5. [CrossRef]
- Bessi A, Zollo F, Del Vicario M, Puliga M, Scala A, Caldarelli G, et al. Users polarization on Facebook and YouTube. PLOS ONE. 2016;11(8):1–24. [CrossRef]
- Jones CE, Munoz FM, Spiegel HM, Heininger U, Zuber PL, Edwards KM, Lambach P, Neels P, Kohl KS, Gidudu J, Hirschfeld S. Guideline for collection, analysis and presentation of safety data in clinical trials of vaccines in pregnant women. Vaccine. 2016;34(49):5998–6006. [CrossRef]
Figure 1.
attitudes and perceptions of vaccinated and unvaccinated participants toward MIV uptake.
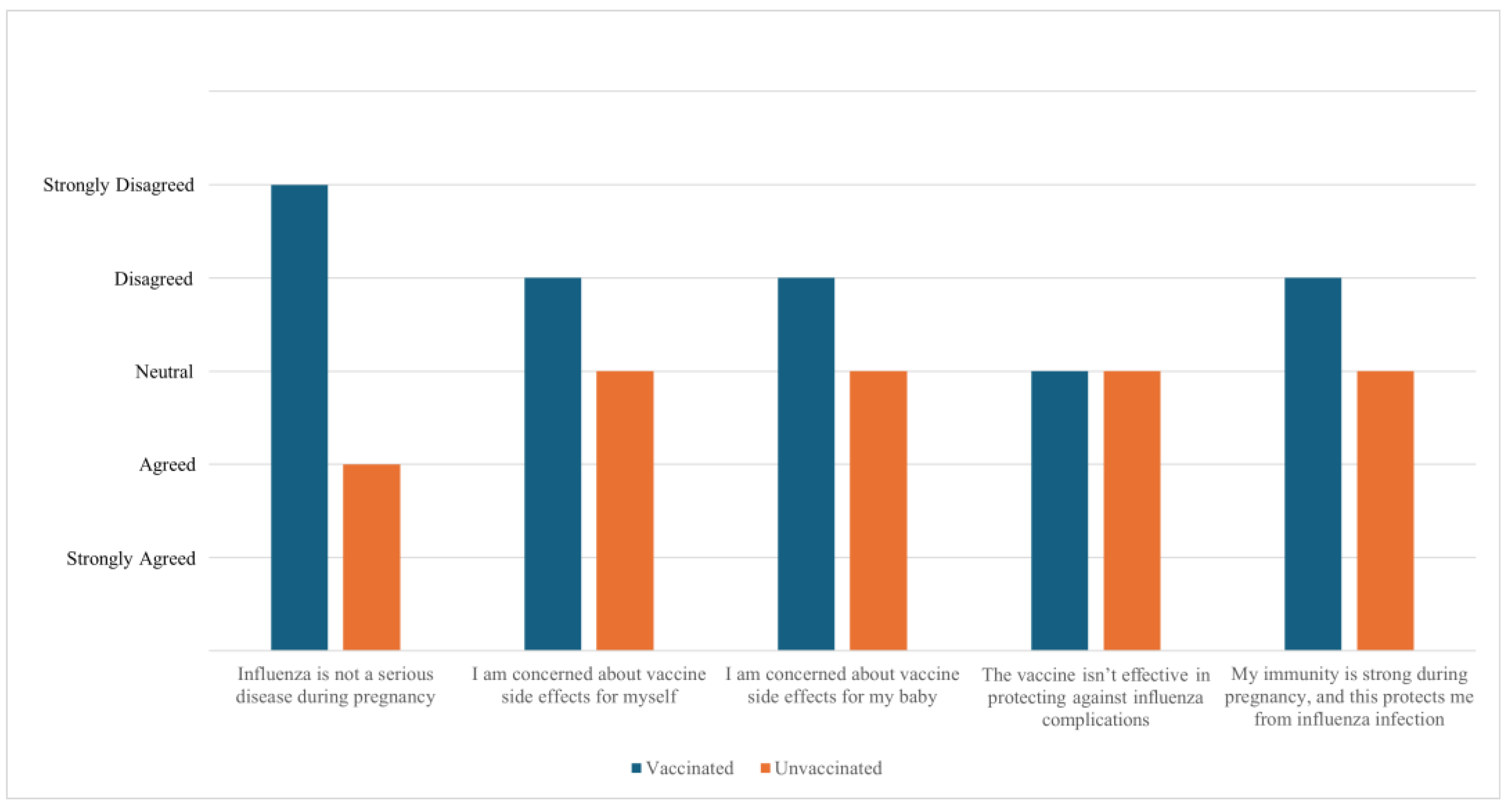
Figure 2.
HCPs recommendations and provision of MIV.
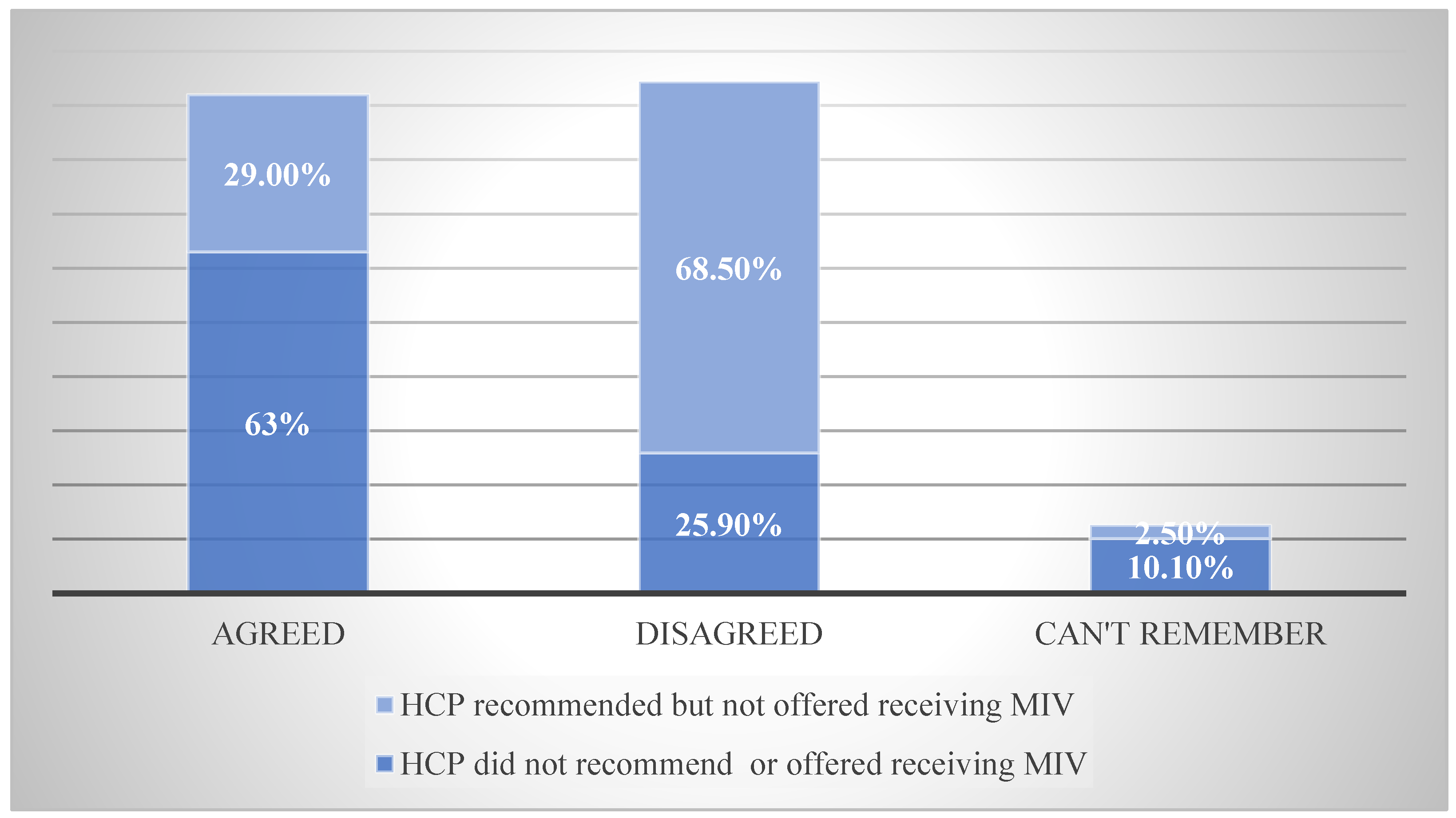
Figure 4.
Importance of different influences toward MIV uptake.
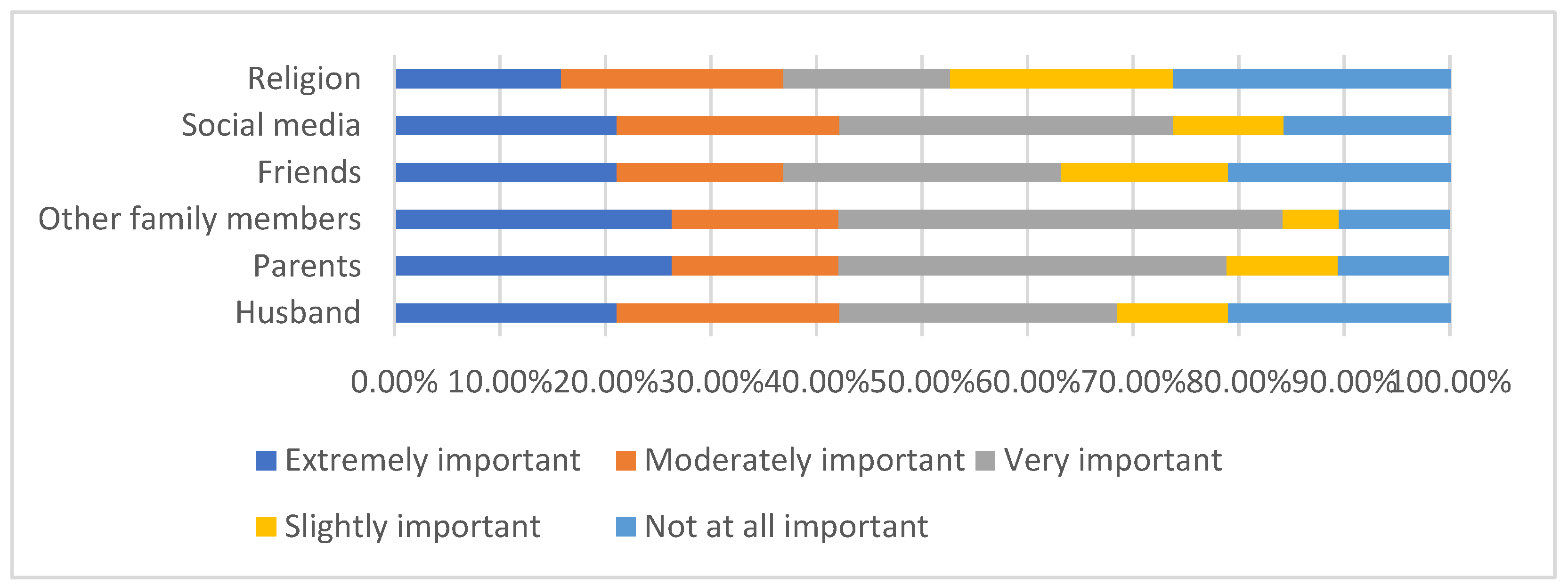
Table 1.
Sociodemographic characteristics, pregnancy and vaccine history.
| Demography | N | % | |
|---|---|---|---|
| Age | 18–22 years | 10 | 3.7 |
| 23–27 years | 50 | 18.4 | |
| 28–32 years | 83 | 30.5 | |
| 33–37 years | 69 | 25.4 | |
| 38–42 years | 45 | 16.5 | |
| > 42 years | 15 | 5.5 | |
| Nationality | Kuwaiti | 199 | 73.2 |
| Non-Kuwaiti | 73 | 26.8 | |
| Religion | Muslim | 254 | 93.4 |
| Christian | 18 | 6.6 | |
| Buddhism | 0 | 0.0 | |
| Other | 0 | 0.0 | |
| Highest level of education | None | 0 | 0.0 |
| Primary school | 4 | 1.5 | |
| Middle school | 13 | 4.8 | |
| High school | 20 | 7.4 | |
| Higher education | 235 | 86.4 | |
| Weeks of pregnancy | 1-13 weeks | 17 | 6.4% |
| 14-26 weeks | 21 | 7.9% | |
| 27-40 weeks | 126 | 47.2% | |
| Recently delivered | 103 | 38.6% | |
| Is this your first pregnancy? | Yes | 70 | 26.3 |
| No | 196 | 73.7 | |
| Received influenza vaccine during current/most recent pregnancy | Yes | 22 | 8.1 |
| No | 250 | 91.9 | |
| Received any vaccines during previous pregnancies (for women with multiple pregnancies) | Yes | 19 | 9.4 |
| No | 93 | 34.19 | |
| Can’t remember | 160 | 79.2 |
Table 2.
Proportions and percentages of participants’ knowledge about influenza infection and prevention and knowledge score.
Table 2.
Proportions and percentages of participants’ knowledge about influenza infection and prevention and knowledge score.
| Influenza Prevention Techniques | N | % | |
|---|---|---|---|
| Getting the influenza vaccine | Yes | 118 | 43.4 |
| No | 99 | 36.4 | |
| I don’t know. | 55 | 20.2 | |
| Taking vitamin supplements | Yes | 232 | 85.3 |
| No | 25 | 9.2 | |
| I don’t know. | 15 | 5.5 | |
| Eating ginger and/or garlic | Yes | 147 | 54.0 |
| No | 72 | 26.5 | |
| I don’t know. | 53 | 19.5 | |
| Having a healthy lifestyle | Yes | 201 | 73.9 |
| No | 49 | 18.0 | |
| I don’t know. | 22 | 8.1 | |
| Hand washing/hand hygiene | Yes | 249 | 91.5 |
| No | 12 | 4.4 | |
| I don’t know. | 11 | 4.0 | |
| Knowledge score equal to median or below | 160 | 58.8 | |
| Knowledge score above the median | 112 | 41.2 | |
Table 3.
Proportions, percentages and score of participants’ knowledge about MIV.
| MIV Knowledge | N | % | |
|---|---|---|---|
| Influenza vaccines during pregnancy can protect me from complications from influenza infection, such as hospital admission. | Agree | 91 | 33.5 |
| Disagree | 64 | 23.5 | |
| I don’t know. | 117 | 43.0 | |
| Influenza vaccination during pregnancy can protect my new-born baby against influenza infection during their first months of life | Agree | 58 | 21.3 |
| Disagree | 76 | 27.9 | |
| I don’t know. | 138 | 50.7 | |
| Influenza infection during pregnancy is a serious disease. | Agree | 62 | 22.8 |
| Disagree | 127 | 46.7 | |
| I don’t know. | 83 | 30.5 | |
| Knowledge score equal to or below median | 230 | 92 | |
| Knowledge score above the median | 20 | 8 | |
Table 4.
Medians and IQR for participants’ opinions toward measures to enhance the uptake of MIV.
| Influence of Measures to Enhance MIV Uptake | Median | Q1-Q3 | IQR |
|---|---|---|---|
| My obstetrician advises me to get vaccinated | 5.0 | 4.0-5.0 | 1.0 |
| I get information on the safety of influenza vaccination during pregnancy in the form of posters, leaflets and ministry of health social media channels | 4.0 | 3.0-5.0 | 2.0 |
| I get information about the seriousness of influenza for pregnant women and neonates in the form of posters, leaflets and ministry of health social media channels | 5.0 | 4.0-5.0 | 1.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



