
Submitted:
26 March 2025
Posted:
27 March 2025
You are already at the latest version
Abstract
Atrial fibrillation (AF) is a leading arrhythmia worldwide, and autonomic nervous system (ANS) dysfunction is pivotal in its pathogenesis. This review synthesizes mechanistic insights into how sympathetic and parasympathetic dysregulation modulates atrial electrophysiology, highlighting emerging therapies targeting neural pathways. We critically appraise pharmacologic, catheter-based, and neuromodulatory approaches, including beta-blockers, low-level vagus nerve stimulation (LL-VNS), renal denervation (RDN), and ganglionated plexi (GP) ablation. Understanding the ANS's role offers a framework for innovative AF management, with implications for personalized, mechanism-driven therapy. Key findings include the identification of specific neural pathways involved in AF pathogenesis and the evaluation of various therapeutic strategies, such as beta-blockers, LL-VNS, RDN, and GP ablation.
Keywords:
atrial fibrillation (AF)
; autonomic nervous system (ANS)
; electrophysiology
; catheter ablation
; sympathetic nervous system
; parasympathetic nervous system
Introduction
Atrial fibrillation (AF) is the most cardiac arrhythmia encountered in clinical practice, affecting millions of individuals worldwide. Atrial fibrillation (AF) affects an estimated 59.7 million individuals globally, making it the most prevalent arrhythmia [1]. It is associated with significant morbidity and mortality, including an increased risk of stroke, heart failure, and all-cause mortality [2]. Despite advances in our understanding of its pathophysiology and the development of various therapeutic strategies, AF remains a major clinical challenge due to its complex and multifactorial nature.
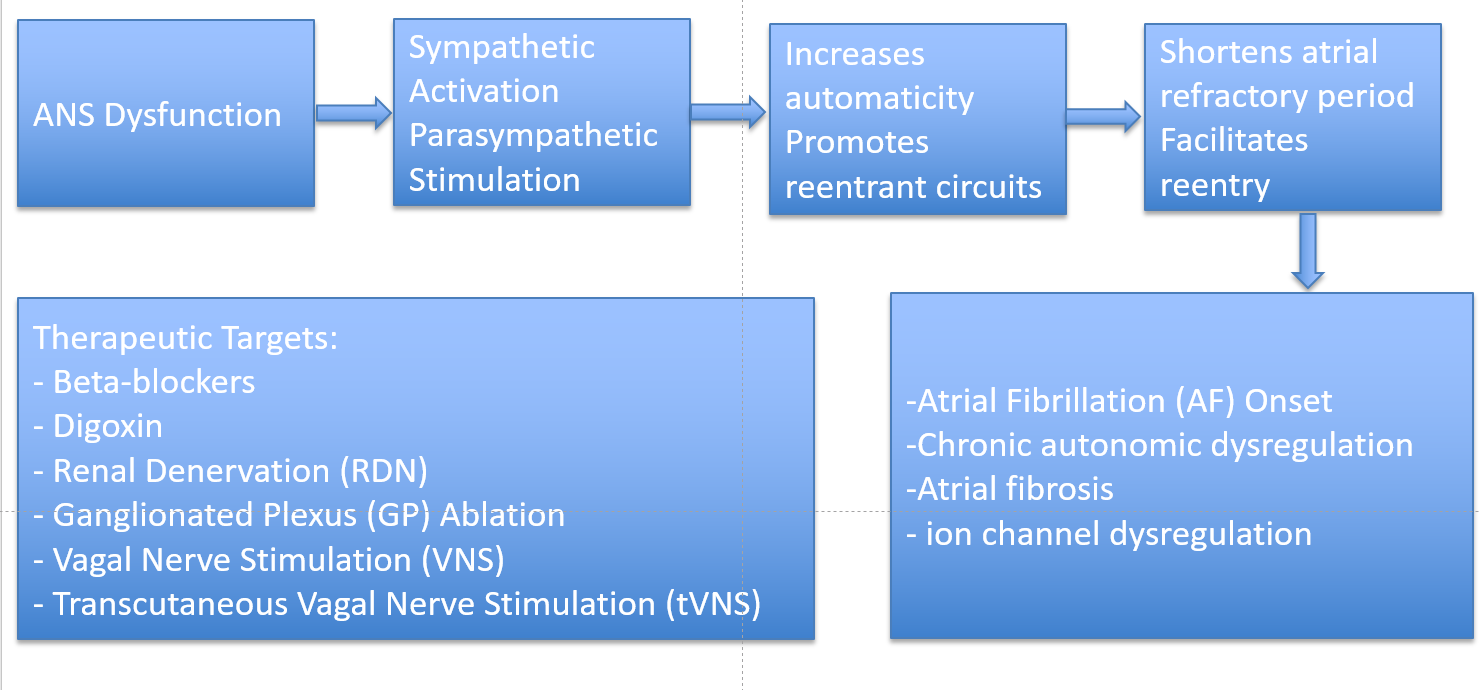
The autonomic nervous system (ANS) plays a crucial role in the initiation, maintenance, and progression of AF [3]. The intricate interplay between the sympathetic and parasympathetic branches of the ANS significantly influences atrial electrophysiology, contributing to the arrhythmogenic substrate that predisposes individuals to AF [3]. Sympathetic activation can indeed lead to increased automaticity, triggered activity, and reentrant circuits, while parasympathetic stimulation can shorten the atrial refractory period and promote reentry [4]. The dynamic balance between these opposing forces is critical in determining the susceptibility to AF [4]. Recent studies have provided valuable mechanistic insights into the role of the ANS in AF. These investigations have elucidated the molecular and cellular pathways through which autonomic modulation affects atrial electrophysiology [3]. For instance, autonomic remodeling, characterized by changes in the density and distribution of autonomic nerves within the atria, has been implicated in the pathogenesis of AF [5]. Additionally, the role of specific neurotransmitters, ion channels, and signaling pathways in mediating the effects of autonomic stimulation on atrial myocytes has been extensively studied [6].
Therapeutic strategies targeting the ANS have shown promise in the management of AF. Neuromodulation techniques, such as ganglionated plexus ablation, renal sympathetic denervation, and vagal nerve stimulation, have demonstrated efficacy in reducing AF burden and improving clinical outcomes [7]. Pharmacological approaches aimed at modulating autonomic tone, including beta-blockers, antiarrhythmic drugs, and novel agents targeting specific autonomic pathways, have also been explored [8]. Furthermore, lifestyle interventions, such as exercise and stress reduction, have been shown to influence autonomic function and may have a role in AF management [8].
This review aims to provide a comprehensive overview of the mechanistic insights into the role of the ANS in AF and to discuss the current and emerging therapeutic targets for autonomic modulation in the management of this arrhythmia. By integrating the latest research findings, we hope to shed light on the complex interplay between the ANS and AF and to highlight potential avenues for future therapeutic development.
Sympathovagal Interactions in AF
The SNS and PNS do not operate in isolation; rather, they interact dynamically to regulate cardiac electrophysiology [2]. This complex interplay, known as sympathovagal interaction, plays a pivotal role in AF initiation and maintenance [2,4]. While both autonomic branches can independently create pro-arrhythmic conditions, their combined influence often results in even greater atrial vulnerability to fibrillatory activity [2]. The dynamic balance or imbalance between sympathetic excitation and parasympathetic inhibition determines the electrophysiological substrate upon which AF develops [2]. One well-characterized mechanism of sympathovagal interaction involves initial sympathetic overdrive, leading to increased intracellular calcium, followed by abrupt vagal activation that shortens the effective refractory period (ERP) [5]. This sequence creates a vulnerable substrate for premature atrial contractions (PACs), particularly from pulmonary veins [2,6]. However, the precise temporal dynamics and patient-specific variability of these autonomic shifts remain incompletely understood, highlighting the need for further investigation through high-resolution autonomic monitoring [4,11]. Elevated sympathetic tone increases intracellular calcium levels and enhances automaticity, making atrial myocytes more excitable [3]. When this sympathetic surge is abruptly followed by strong vagal activation, the resultant shortening of the atrial ERP creates an ideal setting for short-coupled ectopic beats [12]. These PACs, particularly those originating from the pulmonary veins, can initiate reentrant circuits that sustain AF [15]. This phenomenon is frequently observed in paroxysmal AF episodes, where autonomic fluctuations precipitate abrupt atrial arrhythmias [12].
Beyond acute triggers, chronic autonomic remodeling in AF further exacerbates arrhythmogenic susceptibility. Persistent AF leads to structural and functional remodeling of the cardiac ANS, including increased local autonomic nerve density in the atria [8]. This remodeling results in a greater concentration of both sympathetic and parasympathetic nerve fibers, amplifying the potential for autonomic imbalances and abnormal neural discharge patterns [7]. Increased local nerve density enhances regional autonomic heterogeneity, fostering dispersion of repolarization and conduction abnormalities, both of which are critical in sustaining AF [7]. Studies have demonstrated that atrial tissues from patients with long-standing AF exhibit heightened autonomic nerve activity, reinforcing the concept that ANS remodeling perpetuates AF progression [13]. This remodeling contributes to the transition from paroxysmal to persistent AF, as autonomic nerve hyperplasia and altered neurotransmitter release create a self-perpetuating arrhythmogenic cycle [7]. Additionally, autonomic ganglia located near the pulmonary veins and posterior left atrium become hyperactive, further destabilizing atrial electrophysiology and increasing susceptibility to AF recurrence [8].
Sympathetic Nervous System (SNS) and Atrial Fibrillation
The SNS plays a fundamental role in regulating cardiac excitability and conduction, and its overactivation is strongly linked to the development and maintenance of AF [4]. Increased sympathetic activity enhances atrial automaticity, calcium handling, and action potential duration dispersion, all of which contribute to an arrhythmogenic environment [11]. Through multiple interconnected mechanisms, excessive SNS stimulation promotes electrical and structural remodeling in the atria, ultimately increasing susceptibility to AF [12]. One of the primary mechanisms by which the SNS influences AF is β-adrenergic receptor activation, which triggers a cascade of intracellular signaling events that elevate intracellular calcium levels [3]. This increase in calcium can lead to afterdepolarizations, spontaneous electrical discharges that disturb normal atrial rhythm and serve as a critical factor in AF initiation [4]. Heightened adrenergic tone further exacerbates this instability, increasing the likelihood of ectopic activity and atrial reentry circuits, both of which are fundamental to the pathophysiology of AF [4].
Another key contributor to AF development is abnormal calcium homeostasis, driven by excessive sympathetic activation. Disruptions in calcium regulation result in delayed afterdepolarizations (DADs) and triggered activity, both of which promote abnormal automaticity and spontaneous atrial excitability [13]. This dysregulated calcium handling is particularly significant in patients with underlying cardiovascular disease, as it creates a vulnerable substrate for AF persistence. Additionally, sympathetic overactivity shortens the atrial ERP, promoting reentrant circuits that perpetuate AF by creating vulnerable atrial tissue prone to continuous electrical cycling [13]. Reentry occurs when electrical impulses continuously cycle through vulnerable atrial tissue, preventing the heart from maintaining a stable rhythm. This spatiotemporal dispersion of repolarization creates a heterogeneous electrical environment, further predisposing the atria to chaotic and sustained fibrillatory activity [4]. Beyond these electrophysiological effects, excessive SNS activity contributes to atrial structural remodeling, including atrial fibrosis and increased conduction heterogeneity, both of which reinforce the pro-arrhythmic substrate [4]. Studies have demonstrated that direct sympathetic stimulation and heart failure models result in significant atrial remodeling, making the atria more susceptible to AF [14].
Parasympathetic Nervous System (SNS) and Atrial Fibrillation
The PNS also crucial role in modulating atrial electrophysiology, primarily through vagus nerve stimulation, which exerts profound effects on atrial excitability and conduction [5]. While the PNS is generally associated with slowing heart rate and stabilizing cardiac function, excessive vagal tone can paradoxically promote AF by facilitating conditions favorable for reentry and electrical instability [15]. One of the primary mechanisms by which the PNS contributes to AF is a shortening of the ERP [5]. Increased vagal activity leads to enhanced acetylcholine (ACh) release, which activates muscarinic receptors in the atria, resulting in potassium current activation and accelerated repolarization [5,14]. This shortened ERP creates an ideal substrate for reentrant circuits, as electrical impulses can re-excite atrial tissue before it fully recovers from prior activation. Interestingly, vagal-mediated reentry in these regions may also interact with local sympathetic elements, suggesting that targeted interventions should address both limbs of the autonomic system [15]. Another critical factor in vagally induced AF is heterogeneous atrial repolarization, which disrupts the uniform recovery of atrial tissue following each heartbeat [11]. This heterogeneity promotes wavefront fractionation, where electrical impulses break into multiple, unstable wavelets that sustain AF [11]. The spatial and temporal dispersion of repolarization increases conduction heterogeneity, further amplifying the risk of reentry and the persistence of AF episodes [11].
A key molecular mechanism underlying parasympathetic-driven AF is the activation of acetylcholine-mediated potassium currents (IK, ACh) [3]. These currents play a direct role in shortening action potential duration and increasing atrial excitability, both of which contribute to the development of vagally induced AF [3]. In experimental models, IK, ACh activation has been shown to promote spontaneous atrial ectopy and create a highly excitable atrial substrate, facilitating the onset and maintenance of fibrillatory activity [3]. Additionally, direct electrical stimulation of ganglionated plexi (GP) near the pulmonary veins has been shown to decrease heart rate and induce AF [8]. The ganglionated plexi serve as critical autonomic control centers in the heart, integrating both sympathetic and parasympathetic inputs [8]. Stimulation of these structures enhances vagal activity, leading to marked atrial ERP shortening and increased AF susceptibility. This phenomenon highlights the significance of neurally mediated AF, where autonomic imbalances particularly heightened parasympathetic drive act as potent AF triggers [5]. Moreover, high parasympathetic activity has been associated with AF recurrence following catheter ablation procedures, as reflected by deceleration capacity, a marker of vagal modulation of heart rate [15]. Patients exhibiting strong vagal tone before or after ablation may experience a higher likelihood of AF recurrence, suggesting that autonomic influences persist even after pulmonary vein isolation [15]. These findings consolidate the importance of autonomic modulation in AF maintenance and post-ablation outcomes, making it a crucial factor to consider in long-term rhythm management.
Mechanistic Insights (Fibrosis, Ion Channels, Ganglia)
Neural Remodeling and Atrial Fibrosis
One of the most significant consequences of chronic autonomic dysregulation is atrial fibrosis, which disrupts normal conduction pathways and increases conduction heterogeneity, promoting reentrant circuits that sustain AF. Persistent sympathetic and parasympathetic activation drives fibrotic remodeling through increased transforming growth factor-beta (TGF-β) signaling, a key mediator of extracellular matrix deposition [16,17]. Studies have demonstrated that elevated TGF-β levels correlate with increased atrial fibrosis and a higher propensity for AF recurrence [18]. Additionally, hyperactivity of ganglionated plexi (GP) near the pulmonary veins has been identified as a major contributor to electrical instability in AF [8]. The GP serves as an autonomic control hubs within the heart, integrating sympathetic and parasympathetic inputs [8]. When overactivated, these structures enhance local neural discharge, increasing atrial excitability and shortening refractory periods, both of which create conditions favorable for AF induction and maintenance [5].
Ion Channel Dysregulation
Autonomic modulation of ion channel activity plays a pivotal role in AF pathogenesis [14].SNS hyperactivity leads to upregulation of Cav1.2 channels, which are responsible for L-type calcium currents (ICa,L) [14]. Increased Cav1.2 expression enhances intracellular calcium loading, predisposing atrial myocytes to spontaneous depolarizations and ectopic activity, a hallmark of AF [14]. This calcium overload further contributes to triggered activity via DADs, fostering arrhythmic propagation [14]. Conversely, parasympathetic (vagal) stimulation promotes AF triggers via activation of IK, ACh which facilitates repolarization and shortens the ERP, facilitating the formation of reentrant circuits [9].
Role of the Cardiac Autonomic Ganglia
The intrinsic cardiac nervous system (ICNS), particularly the ganglionated plexi (GP), plays a critical role in modulating autonomic influences on atrial electrophysiology. These autonomic ganglia, located predominantly near the pulmonary veins, left atrium, and atrioventricular junction, serve as integration centers for sympathetic and parasympathetic inputs [8]. Hyperactivity within the GP can drive sustained autonomic discharges, leading to atrial electrical instability and increased AF susceptibility. Clinical and experimental studies have shown that GP ablation can significantly reduce AF recurrence, highlighting their pro-arrhythmic role in AF pathogenesis [8]. Ablation of hyperactive GP sites has been associated with improved rhythm control outcomes, particularly in patients with vagally mediated or paroxysmal AF [8]. This suggests that targeting the intrinsic cardiac nervous system may be a promising strategy for AF management, particularly in cases where autonomic triggers play a dominant role.
Therapeutic Targets Modulating the Autonomic Nervous System (ANS) in Atrial Fibrillation (AF)
Given the significant role of the ANSin AF pathogenesis, therapeutic strategies targeting autonomic modulation have emerged as promising approaches for reducing AF burden and improving rhythm control. These interventions range from pharmacological therapies that blunt sympathetic overactivity to neuromodulatory techniques aimed at restoring autonomic balance. The following sections highlight key strategies in ANS-targeted AF therapy, including beta-blockers, vagal modulation, catheter-based autonomic interventions, and emerging neuromodulation techniques.
Established Pharmacological Modulation (Beta-blockers, Digoxin)
Beta-blockers persist as the epicenter of AF management, particularly in sympathetically driven arrhythmias, by antagonizing β-adrenergic receptors and reducing SNS-mediated increases in heart rate, intracellular calcium loading, and adrenergic excitability [9,19]. Their effects include rate control, prevention of calcium overload, and reduction of adrenergic excitability, thereby stabilizing atrial electrophysiology and preventing AF initiation [9]. They also have anti-remodeling effects, mitigating neurohormonal activation and reducing atrial fibrosis [9].Their efficacy, however, varies by AF subtype. In paroxysmal AF (PAF), where sympathetic surges (e.g., stress, caffeine, exercise) often trigger episodes, beta-blockers significantly reduce arrhythmia frequency [9]. In persistent and long-standing AF, where autonomic remodeling is more advanced, beta-blockers alone are less effective but they remain useful for rate control, often requiring combination therapy with antiarrhythmic drugs (AADs) such as amiodarone [14,17]. In AF with heart failure (AF-HF), beta-blockers play a dual role in both rate control and improving survival [20]. In HFrEF, carvedilol and metoprolol succinate are preferred due to their additional ventricular remodeling benefits [20,21,22,23,24,25]. However, in HFpEF, excessive heart rate reduction may worsen diastolic dysfunction, necessitating careful use, with nebivolol being a potential alternative. Nebivolol is a β1-selective beta-blocker with unique vasodilatory properties via nitric oxide (NO) release, making it particularly beneficial in AF patients with HFpEF, hypertension, or vascular dysfunction [26,27]. Unlike traditional beta-blockers, it improves arterial compliance, reduces afterload, and minimizes excessive bradycardia, which is crucial in HFpEF patients who rely on higher heart rates for adequate diastolic filling. Its favorable metabolic profile makes it preferable in diabetic and elderly patients, while its vasodilatory effects enhance peripheral perfusion, reducing symptoms like fatigue and exercise intolerance [27]. Beta-blocker selection should be tailored to individual patient profiles, balancing their antiadrenergic benefits with potential side effects such as bradycardia and hypotension.
Among pharmacologic agents that modulate the autonomic nervous system in AF, digoxin holds a unique position as a vagomimetic agent that exerts parasympathetic enhancement at the AV node [28]. By increasing vagal tone, digoxin prolongs the refractory period and slows conduction through the AV node, thereby contributing to ventricular rate control in AF [28]. This effect makes digoxin mechanistically relevant in discussions of autonomic modulation. However, despite its historical prominence, the contemporary role of digoxin is limited due to several critical factors. First, its rate-slowing effects are attenuated during sympathetic activation, rendering it less effective for rate control during exertion or stress [29]. Second, concerns regarding a narrow therapeutic window and potential proarrhythmic and toxic effects, including associations with increased mortality in some observational studies, have led to a decrease in its routine use [30]. Nevertheless, digoxin remains a consideration in specific clinical scenarios, particularly in patients with heart failure with HFrEF and atrial fibrillation, where beta-blockers or calcium channel blockers are contraindicated or insufficient. Importantly, digoxin does not address the underlying atrial substrate or autonomic remodeling that perpetuate AF, and thus, it is not a rhythm control agent nor a disease-modifying therapy. Its inclusion in the therapeutic discussion underscores the complexity of autonomic interactions in AF and highlights the need for targeted, mechanistically informed therapies beyond rate control alone.
Catheter-Based Autonomic Modulation
Interventional strategies targeting the ANS through catheter-based techniques have gained traction as potential adjuncts to pulmonary vein isolation (PVI) in AF ablation therapy. Two key approaches include: Renal Denervation (RDN) and Ganglionated Plexi (GP) Ablation.
Renal denervation (RDN)
RDN has emerged as a promising interventional strategy for autonomic modulation in AF, particularly among patients with hypertension-associated AF, where SNS overactivity plays a pivotal role in atrial arrhythmogenesis [31,32,33,34]. The renal sympathetic nerves exert systemic autonomic influence through both efferent and afferent pathways: efferent fibers contribute to increased sympathetic vasoconstrictor tone, while afferent sensory fibers provide feedback to central autonomic centers, amplifying global adrenergic activity [34]. This autonomic hyperactivity fosters a pro-arrhythmic atrial substrate by promoting shortening of atrial effective refractory periods ERPs, increasing electrical and structural remodeling, enhancing conduction heterogeneity, and facilitating atrial ectopy and reentry [32,33]. Hypertensive patients, characterized by elevated catecholaminergic drive, are particularly prone to AF due to these maladaptive autonomic influences [33]. By interrupting renal sympathetic signaling, RDN aims to reduce systemic sympathetic outflow, lower blood pressure, and, importantly, attenuate atrial electrophysiological vulnerability to AF. Supporting this mechanistic rationale, the ERADICATE-AF randomized clinical trial demonstrated that the combination of RDN and catheter ablation significantly reduced AF recurrence compared to ablation alone in patients with paroxysmal AF and hypertension [31]. Moreover, meta-analyses have confirmed that RDN as an adjunct to AF ablation improves clinical outcomes, including sustained sinus rhythm maintenance, in hypertensive patients [32,33]. Finally, long-term follow-up data from the SYMPLICITY HTN-3 trial have further validated the efficacy of RDN in achieving sustained sympathetic inhibition and blood pressure reduction, reinforcing its potential as a strategy to modulate autonomic drivers of AF [34]. RDN has demonstrated significant benefits in hypertensive and sympathetic-driven AF, as evidenced by the ERADICATE-AF trial, yet its role in normotensive or non-adrenergic AF remains uncertain. Overall, these findings highlight RDN as a mechanistically targeted and clinically impactful intervention for AF in the setting of autonomic dysregulation.
Ganglionated Plexi (GP) Ablation
GP ablation has emerged as a targeted neuromodulatory strategy aimed at disrupting intrinsic cardiac autonomic inputs that contribute to both the initiation and maintenance of AF [35,36,37,38,39]. The GP are dense clusters of autonomic nerve fibers, located within epicardial fat pads of the atria, predominantly around the pulmonary vein (PV) antra, posterior left atrium, and interatrial septum [35,37]. These autonomic hubs integrate both sympathetic and parasympathetic inputs and play a pivotal role in modulating local atrial electrophysiology, including refractoriness and conduction velocity [36,38]. In the context of hyperactive GP, excessive vagal stimulation can induce abrupt shortening of atrial ERP, increased conduction heterogeneity, and the formation of reentrant circuits, thus creating a substrate for AF initiation and perpetuation [36,38]. As a result, targeting GP through ablation has been proposed to modulate autonomic tone, suppress vagally mediated AF episodes, and enhance the efficacy of pulmonary vein isolation (PVI) as part of a comprehensive rhythm control strategy [35,37,39].
Despite a compelling mechanistic rationale, clinical trials evaluating GP ablation have yielded mixed results, reflecting both its therapeutic potential and limitations. The AFACT trial, a multicenter randomized controlled trial (RCT), demonstrated that although thoracoscopic GP ablation effectively modulated autonomic tone, it did not improve long-term freedom from AF when added to PVI, and was associated with a higher incidence of complications, including sinus node dysfunction [40]. In contrast, the GAP-AF trial showed that selective GP ablation combined with PVI significantly improved arrhythmia-free survival in patients with paroxysmal, vagally mediated AF, highlighting the importance of patient selection [41]. Similarly, the GAPP-AF trial, a multicenter RCT, reported that adjunctive GP ablation reduced early AF recurrence following PVI; however, long-term outcomes were comparable to PVI alone, raising questions about the durability of autonomic remodeling achieved through GP ablation [42]. These findings underscore the need for better identification of target patient populations and refined procedural techniques.
Several limitations continue to hinder the widespread adoption of GP ablation. First, there is no standardized method for identifying and localizing GP, with anatomical variability and functional heterogeneity posing major procedural challenges [37]. Second, excessive autonomic disruption carries a risk of iatrogenic bradyarrhythmias, including sinus node dysfunction and AV block, as reported in AFACT [40]. Third, concerns persist regarding the long-term stability of autonomic modulation, as autonomic nerves exhibit plasticity and may reinnervate over time, potentially leading to AF recurrence [38,42]. Nonetheless, GP ablation remains a mechanistically promising intervention, particularly for vagally mediated AF, and ongoing research is focused on optimizing patient selection, procedural strategies, and durable clinical outcomes [35,41,42].
Despite these mixed results, GP ablation continues to hold potential, particularly in specific AF phenotypes such as vagally mediated AF. However, several limitations must be addressed before its routine clinical application. First, there is a lack of standardization in the identification and localization of GP, as anatomical variability and functional heterogeneity present procedural challenges. Second, there is an ongoing concern regarding excessive autonomic disruption, with risks of iatrogenic bradyarrhythmias, including sinus node dysfunction and atrioventricular block [50]. Third, the long-term stability of autonomic modulation following GP ablation remains uncertain, as autonomic nerves may exhibit plasticity and reinnervate over time, potentially leading to AF recurrence [51]
Neuromodulation Therapies
Stellate Ganglion Modulation
The stellate ganglia represent critical sympathetic outflow centers that play a fundamental role in cardiac autonomic regulation, influencing atrial electrophysiology and arrhythmogenesis [43,44,45,46]. Increased stellate ganglion activity is associated with enhanced norepinephrine release, which leads to atrial ERP shortening, increased atrial excitability, and a heightened propensity for AF initiation and maintenance [43,44,45,46]. Given this pathophysiologic role, stellate ganglion modulation has emerged as a novel therapeutic strategy to target sympathetically driven AF, particularly in patients with adrenergic-mediated or refractory AF [43,44,45,46]. There are two principal approaches to modulating stellate ganglion activity: stellate ganglion block (SGB) and stellate ganglion ablation (SGA).
Stellate Ganglion Block (SGB): SGB involves the percutaneous injection of local anesthetics (e.g., bupivacaine, lidocaine) around the cervical sympathetic chain, aiming to transiently inhibit stellate ganglion function and reduce sympathetic outflow [47]. Clinical reports indicate that SGB can acutely reduce AF burden, particularly in patients with autonomic dysregulation, adrenergic AF triggers, or stress-mediated AF episodes [47]. Notably, SGB has been employed to terminate rapid AF episodes in acute settings, offering a minimally invasive, bedside intervention [47]. However, its effects are transient, and the long-term efficacy of SGB remains uncertain, underscoring the need for larger controlled studies [45,47].
Stellate Ganglion Ablation (SGA): In contrast, stellate ganglion ablation (SGA), through radiofrequency ablation (RFA) or surgical sympathectomy, seeks to achieve permanent modulation of sympathetic outflow [46]. Bilateral stellate ganglion ablation has shown promise in reducing AF recurrence in patients with high sympathetic tone, supporting its role as a potential intervention in refractory cases [45,46]. By disrupting the sympathetic innervation of the atria, SGA may stabilize atrial electrophysiological properties and suppress adrenergically mediated triggers [46]. Nevertheless, SGA carries significant risks, including autonomic imbalance, hypotension, Horner’s syndrome, and phrenic nerve injury, which have limited its widespread adoption [45,46]
Vagal Modulation Strategies
Vagal nerve stimulation (VNS)
VNS has emerged as a promising therapeutic strategy for autonomic modulation in atrial fibrillation (AF); however, its clinical success depends critically on the intensity and dosing of stimulation [48]. While high-intensity VNS (HI-VNS) can paradoxically promote AF by amplifying vagally mediated proarrhythmic mechanisms, low-level VNS (LL-VNS) has demonstrated robust antiarrhythmic potential by restoring autonomic balance and attenuating sympathetic overactivity [48,49]. Thus, understanding the dose-dependent dichotomy of VNS is crucial for integrating this approach into precision-based AF management [44,45].
1. High-Intensity VNS (HI-VNS): Proarrhythmic Effects in AF
Although vagal activation is often considered protective, HI-VNS has been shown to induce AF in preclinical and translational models through several mechanisms. HI-VNS shortens the atrial effective refractory period (ERP) via activation of acetylcholine-sensitive potassium currents (IK,ACh), facilitating atrial repolarization and promoting functional reentry circuits [44,46]. Moreover, HI-VNS generates marked conduction heterogeneity and dispersion of refractoriness, a substrate that fosters wavebreak and fibrillatory conduction [46]. Importantly, HI-VNS not only destabilizes atrial electrophysiology but also induces autonomic imbalance, where excessive vagal drive can paradoxically trigger sympathetic rebound, further exacerbating AF risk [43,44]. This is particularly relevant in patients with vagally mediated AF or baseline high vagal tone, in whom HI-VNS may worsen arrhythmic burden [44,45]. In animal studies, HI-VNS has been associated with up to a 70% reduction in ERP and tripled AF inducibility, underscoring its proarrhythmic potential [46]. Consequently, HI-VNS is not a viable therapeutic strategy for AF suppression and highlights the need for careful modulation of vagal stimulation intensity [44,46].
2. Low-Level VNS (LL-VNS): Antiarrhythmic Mechanisms and Therapeutic Promise
In contrast to HI-VNS, LL-VNS has emerged as a safe and effective modality for AF suppression, particularly in cases where sympathetic overdrive plays a critical role [48,52]. LL-VNS selectively attenuates sympathetic activity while preserving beneficial parasympathetic tone, avoiding excessive vagal stimulation that could otherwise shorten ERP [44,48]. Mechanistically, LL-VNS modestly prolongs ERP without inducing conduction heterogeneity, thereby stabilizing atrial electrophysiology [48]. Moreover, LL-VNS blunts beta-adrenergic stimulation, reducing atrial ectopy, triggered activity, and spontaneous depolarizations, making it especially valuable in adrenergically mediated AF, such as stress-induced or postoperative AF [44,49]. Notably, LL-VNS exerts anti-inflammatory effects, suppressing interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) expression, while reducing oxidative stress, thus preventing atrial structural remodeling and fibrosis, which are central to AF progression [43,48]. LL-VNS may reduce inflammatory pathways that contribute to atrial fibrosis and remodeling, although direct human evidence for structural reversal remains limited and requires further study.These combined autonomic and anti-inflammatory actions position LL-VNS as a comprehensive antiarrhythmic strategy.
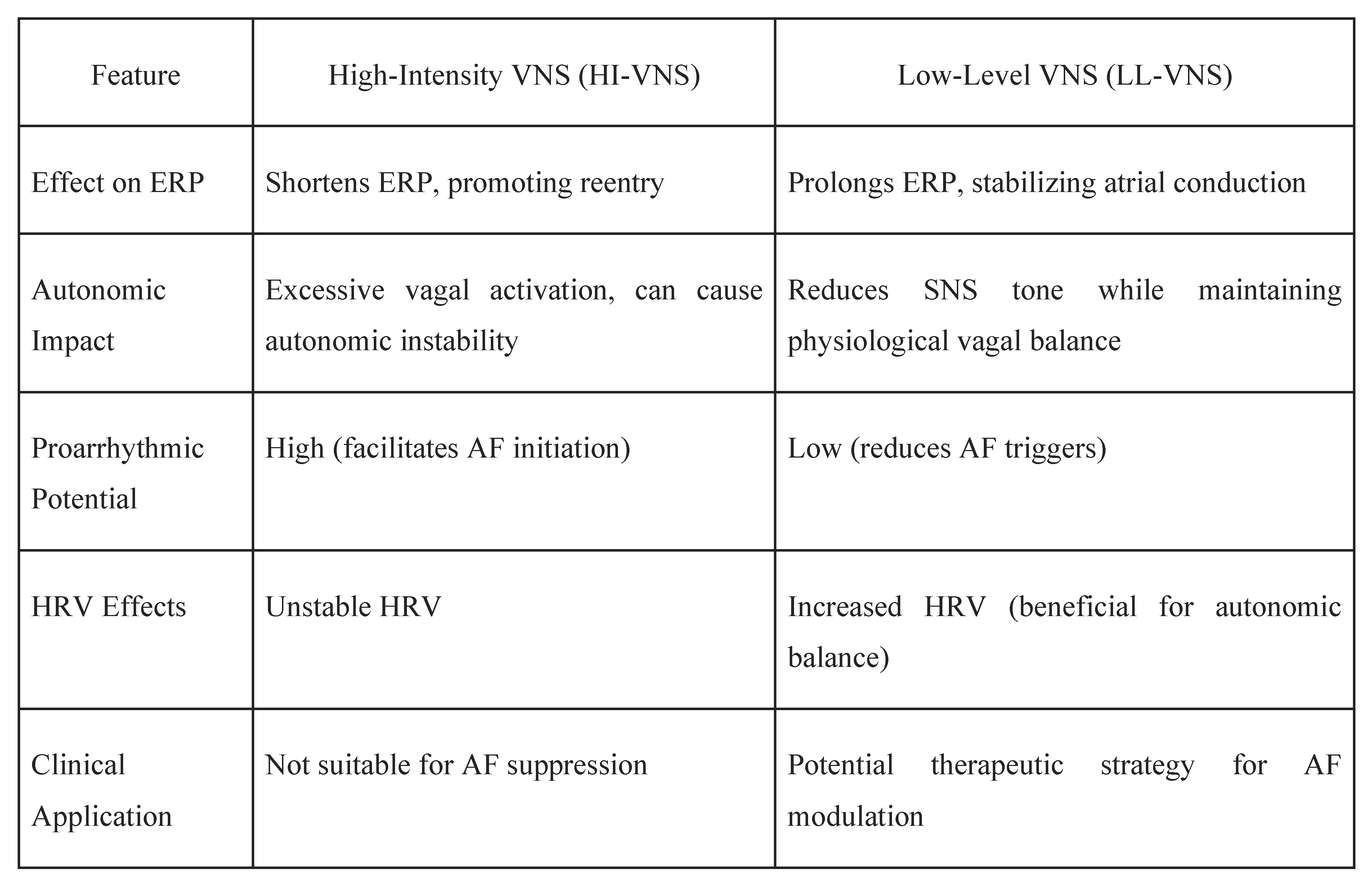
Emerging clinical trials and translational studies have validated the therapeutic promise of LL-VNS in AF. The TREAT-AF trial, a landmark randomized controlled trial, demonstrated that transcutaneous LL-VNS significantly reduced AF burden and improved heart rate variability (HRV), reflecting enhanced autonomic balance in patients with paroxysmal AF [50]. Additionally, LL-VNS led to a 23% reduction in TNF-α levels (ratio of medians: 0.77; 95% CI: 0.63–0.94; p = 0.0093), suggesting a potent anti-inflammatory effect that may attenuate AF progression [50]. Furthermore, while the ANTHEM-HF trial primarily focused on heart failure with reduced ejection fraction (HFrEF), it also provided compelling evidence that chronic LL-VNS improves autonomic function and reduces arrhythmic burden, with significant enhancements in left ventricular ejection fraction (LVEF) [51]. Although ANTHEM-HF was not specifically designed to assess AF outcomes, its findings support the systemic autonomic benefits of VNS, which are highly relevant in AF patients with coexisting heart failure [51]. Table 1 below provides a comparative analysis of HI-VNS and LL-VNS in the management of atrial fibrillation (AF). It highlights the differences in their effects on the ERP, autonomic impact, proarrhythmic potential, heart rate variability (HRV), and clinical applications.
Comparative Analysis of High-Intensity VNS (HI-VNS) and Low-Level VNS (LL-VNS) in Atrial Fibrillation Management.
Figure 1.
Comparative analysis of High-Intensity Vagal Nerve Stimulation (HI-VNS) and Low-Level Vagal Nerve Stimulation (LL-VNS) in atrial fibrillation (AF) management, highlighting differences in their effects on the effective refractory period (ERP), autonomic impact, proarrhythmic potential, heart rate variability (HRV), and clinical applications.
Figure 1.
Comparative analysis of High-Intensity Vagal Nerve Stimulation (HI-VNS) and Low-Level Vagal Nerve Stimulation (LL-VNS) in atrial fibrillation (AF) management, highlighting differences in their effects on the effective refractory period (ERP), autonomic impact, proarrhythmic potential, heart rate variability (HRV), and clinical applications.
3. Non-Invasive Transcutaneous Vagal Nerve Stimulation (tVNS)
Unlike invasive autonomic modulation techniques [ganglionated plexi (GP) ablation or renal denervation (RDN)], Transcutaneous vagal nerve stimulation (tVNS) has emerged as an innovative, non-invasive approach to autonomic modulation in atrial fibrillation (AF), offering a promising alternative to invasive procedures such as ganglionated plexi ablation or renal denervation. By targeting the auricular branch of the vagus nerve (ABVN), accessible at the tragus, tVNS aims to enhance parasympathetic tone and suppress sympathetic overactivity, addressing the autonomic imbalance that contributes to AF initiation and maintenance [52]. Notably, tVNS has demonstrated a favorable safety and tolerability profile, supporting its potential as a home-based therapy for autonomically driven AF [52,53].
Mechanistically, tVNS exerts multifaceted antiarrhythmic effects, including:
- Modulation of systemic inflammation, with evidence suggesting reductions in inflammatory markers that are known to contribute to atrial fibrosis and AF persistence [51].
Clinical Evidence Supporting tVNS in AF
Clinical investigations into tVNS have provided compelling evidence for its therapeutic role in AF management. One of the landmark studies in this field is the TREAT-AF trial, a randomized controlled trial led by Stavrakis et al., which demonstrated that low-level tragus stimulation (a form of tVNS) significantly reduced AF burden in patients with paroxysmal AF [50]. Importantly, patients in the active stimulation group showed enhanced parasympathetic activity and reduced sympathetic tone, reflected in improved heart rate variability (HRV) [50]. In addition to suppressing AF episodes, tVNS significantly reduced PAC burden, supporting its broader antiarrhythmic impact on atrial ectopy [50]. These findings underscore the potential of tVNS not only as a preventive strategy against AF recurrence but also as a means to modulate atrial substrate vulnerability.
Earlier mechanistic studies laid the foundation for these clinical insights. In a pivotal 2015 study by Stavrakis et al., low-level tVNS was shown to reduce AF inducibility and duration during electrophysiological testing in patients undergoing catheter ablation, providing direct evidence that external vagal modulation can suppress atrial arrhythmogenicity in real-time [49]. This proof-of-concept study highlighted the ability of tVNS to stabilize atrial electrophysiology without the risks associated with invasive autonomic interventions.
Furthermore, while the ANTHEM-HF trial primarily focused on vagal nerve stimulation (VNS) in heart failure, it provided important translational insights for AF, demonstrating that chronic VNS improves autonomic balance, reduces sympathetic drive, and favorably impacts cardiac electrophysiology [51]. These systemic autonomic benefits are highly relevant to AF patients, especially those with concomitant heart failure or heightened adrenergic tone [51].
In addition to cardiovascular applications, tVNS is safe and effective in other autonomic disorders, such as postural orthostatic tachycardia syndrome (POTS), further validating its broader clinical feasibility [53]. Systematic evaluations confirm that tVNS is well tolerated, with minimal side effects, positioning it as a practical and patient-friendly option for long-term autonomic modulation [52,53].
Conclusions
Atrial fibrillation (AF) remains a major clinical challenge due to its complex interplay with the autonomic nervous system (ANS). Sympathetic overactivity increases atrial excitability and reentrant circuits, while excessive parasympathetic stimulation shortens the atrial refractory period, facilitating AF onset. Their combined influence, along with chronic autonomic remodeling, perpetuates AF progression.
Targeting the ANS has emerged as a promising therapeutic strategy. Beta-blockers remain foundational. Neuromodulation techniques including LL-VNS, RDN, and GP ablation show potential in restoring autonomic balance and reducing AF burden. Non-invasive strategies like tVNS and BAT offer exciting avenues for future exploration. Personalized autonomic profiling, advanced neuromodulation, and integrative approaches combining catheter ablation, lifestyle interventions, and wearable technology could enhance AF management. Long-term trials are needed to confirm safety and efficacy, while molecular research may unlock novel pharmacologic targets.
Author Contributions
[Author 1 Name] conducted the literature search, data extraction, and drafting of the manuscript. [Author 2 Name] contributed to the critical revision of the manuscript for important intellectual content. [Author 3 Name] provided supervision and final approval of the version to be published. All authors read and approved the final manuscript.
Funding
This literature review did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
Not applicable, as this study is a literature review and does not involve human participants or animal subjects.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable, as this study is a literature review and does not involve the generation of new datasets.
Conflict of Interest
The authors declare that they have no competing interests. Any potential conflicts of interest that could be perceived as influencing the research are disclosed.
References
- Li X, Liu Z, Jiang X, Xia R, Li Y, Pan X, Yao Y, Fan X. Global, regional, and national burdens of atrial fibrillation/flutter from 1990 to 2019: An age-period-cohort analysis using the Global Burden of Disease 2019 study. J Glob Health. 2023 Nov 22;13:04154. [CrossRef] [PubMed]
- Ndakotsu A, Dwumah-Agyen M, Patel M. The bidirectional relationship between obstructive sleep apnea and atrial fibrillation: Pathophysiology, diagnostic challenges, and strategies - A narrative review. Curr Probl Cardiol. 2024 Dec;49(12):102873. [CrossRef] [PubMed]
- Linz D, Elliott AD, Hohl M, Malik V, Schotten U, Dobrev D, Nattel S, Böhm M, Floras J, Lau DH, Sanders P. Role of autonomic nervous system in atrial fibrillation. Int J Cardiol. 2019 Jul 15;287:181-188. [CrossRef] [PubMed]
- Carnagarin R, Kiuchi MG, Ho JK, Matthews VB, Schlaich MP. Sympathetic Nervous System Activation and Its Modulation: Role in Atrial Fibrillation. Front Neurosci. 2019 Jan 23;12:1058. [CrossRef] [PubMed]
- Chen PS, Chen LS, Fishbein MC, Lin SF, Nattel S. Role of the autonomic nervous system in atrial fibrillation: pathophysiology and therapy. Circ Res. 2014 Apr 25;114(9):1500-15. [CrossRef] [PubMed]
- Vandenberk B, Haemers P, Morillo C. The autonomic nervous system in atrial fibrillation-pathophysiology and non-invasive assessment. Front Cardiovasc Med. 2024 Jan 4;10:1327387. [CrossRef] [PubMed]
- Gussak G, Pfenniger A, Wren L, Gilani M, Zhang W, Yoo S, Johnson DA, Burrell A, Benefield B, Knight G, Knight BP, Passman R, Goldberger JJ, Aistrup G, Wasserstrom JA, Shiferaw Y, Arora R. Region-specific parasympathetic nerve remodeling in the left atrium contributes to creation of a vulnerable substrate for atrial fibrillation. JCI Insight. 2019 Oct 17;4(20):e130532. [CrossRef] [PubMed]
- Aksu T, Skeete JR, Huang HH. Ganglionic Plexus Ablation: A Step-by-step Guide for Electrophysiologists and Review of Modalities for Neuromodulation for the Management of Atrial Fibrillation. Arrhythm Electrophysiol Rev. 2023 Jan;12:e02. [CrossRef] [PubMed]
- Zicha S, Tsuji Y, Shiroshita-Takeshita A, Nattel S. Beta-blockers as antiarrhythmic agents. Handb Exp Pharmacol. 2006;(171):235-66. [PubMed]
- Yang Z, Qi X, Li G, Wu N, Qi B, Yuan M, Wang Y, Hu G, Yang Q. The type of exercise most beneficial for quality of life in people with atrial fibrillation: a network meta-analysis. Front Cardiovasc Med. 2025 Jan 9;11:1509304. [CrossRef] [PubMed]
- Scridon, A. Autonomic imbalance and atrial ectopic activity-a pathophysiological and clinical view. Front Physiol. 2022;13:1058427. Published 2022 Dec 2. [CrossRef]
- Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659-666. [CrossRef]
- Rebecchi M, De Ruvo E, Sgueglia M, Lavalle C, Canestrelli S, Politano A, Jacomelli I, Golia P, Crescenzi C, De Luca L, Panuccio M, Fagagnini A, Calò L. Atrial fibrillation and sympatho-vagal imbalance: from the choice of the antiarrhythmic treatment to patients with syncope and ganglionated plexi ablation. Eur Heart J Suppl. 2023 Apr 26;25(Suppl C):C1-C6. [CrossRef] [PubMed]
- Denham NC, Pearman CM, Caldwell JL, et al. Calcium in the Pathophysiology of Atrial Fibrillation and Heart Failure. Front Physiol. 2018;9:1380. Published 2018 Oct 4. [CrossRef]
- Călburean PA, Osório TG, Sieira J, et al. High parasympathetic activity as reflected by deceleration capacity predicts atrial fibrillation recurrence after repeated catheter ablation procedure. J Interv Card Electrophysiol. 2021;60(1):21-29. [CrossRef]
- Nattel S, Burstein B, Dobrev D. Atrial remodeling and atrial fibrillation: mechanisms and implications. Circ Arrhythm Electrophysiol. 2008 Apr;1(1):62-73. [CrossRef] [PubMed]
- Asuka E, Arole O, Ndakotsu A. Extensive Atrial Fibrosis and Recalcitrant Atrial Fibrillation: A Case Report and Brief Literature Review. Cureus. 2025;17(2):e79169. Published 2025 Feb 17. [CrossRef]
- Wu CH, Hu YF, Chou CY, et al. Transforming growth factor-β1 level and outcome after catheter ablation for nonparoxysmal atrial fibrillation. Heart Rhythm. 2013;10(1):10-15. [CrossRef]
- Molenaar P, Christ T, Ravens U, Kaumann A. Carvedilol blocks beta2- more than beta1-adrenoceptors in human heart. Cardiovasc Res. 2006;69(1):128-139. [CrossRef]
- Pasternak B, Svanström H, Melbye M, Hviid A. Association of treatment with carvedilol vs metoprolol succinate and mortality in patients with heart failure [published correction appears in JAMA Intern Med. 2014 Nov;174(11):1875]. JAMA Intern Med. 2014;174(10):1597-1604. [CrossRef]
- Lund LH, Benson L, Dahlström U, Edner M, Friberg L. Association between use of β-blockers and outcomes in patients with heart failure and preserved ejection fraction. JAMA. 2014;312(19):2008-2018. [CrossRef]
- Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM, Deswal A, Eckhardt LL, Goldberger ZD, Gopinathannair R, Gorenek B, Hess PL, Hlatky M, Hogan G, Ibeh C, Indik JH, Kido K, Kusumoto F, Link MS, Linta KT, Marcus GM, McCarthy PM, Patel N, Patton KK, Perez MV, Piccini JP, Russo AM, Sanders P, Streur MM, Thomas KL, Times S, Tisdale JE, Valente AM, Van Wagoner DR; Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jan 2;149(1):e1-e156. [CrossRef] [PubMed]
- Poole-Wilson PA, Swedberg K, Cleland JG, Di Lenarda A, Hanrath P, Komajda M, Lubsen J, Lutiger B, Metra M, Remme WJ, Torp-Pedersen C, Scherhag A, Skene A; Carvedilol Or Metoprolol European Trial Investigators. Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET): randomised controlled trial. Lancet. 2003 Jul 5;362(9377):7-13. [CrossRef] [PubMed]
- Torp-Pedersen C, Poole-Wilson PA, Swedberg K, et al. Effects of metoprolol and carvedilol on cause-specific mortality and morbidity in patients with chronic heart failure--COMET. Am Heart J. 2005;149(2):370-376. [CrossRef]
- Bristow MR, Gilbert EM, Abraham WT, Adams KF, Fowler MB, Hershberger RE, Kubo SH, Narahara KA, Ingersoll H, Krueger S, Young S, Shusterman N. Carvedilol produces dose-related improvements in left ventricular function and survival in subjects with chronic heart failure. MOCHA Investigators. Circulation. 1996 Dec 1;94(11):2807-16. [CrossRef] [PubMed]
- Ferri, C. The role of nebivolol in the management of hypertensive patients: from pharmacological profile to treatment guidelines. Future Cardiol. 2021;17(8):1421-1433. [CrossRef]
- Kitzman DW, Sahadevan J, Higginbotham MB, et al. Effect of Nebivolol on Exercise Capacity in Patients With Heart Failure With Preserved Ejection Fraction: A Randomized Clinical Trial.
- Tieleman RG, Blaauw Y, Van Gelder IC, De Langen CD, de Kam PJ, Grandjean JG, Patberg KW, Bel KJ, Allessie MA, Crijns HJ. Digoxin delays recovery from tachycardia-induced electrical remodeling of the atria. Circulation. 1999 Oct 26;100(17):1836-42. [CrossRef] [PubMed]
- Gheorghiade M, Adams KF Jr, Colucci WS. Digoxin in the management of cardiovascular disorders. Circulation. 2004 Jun 22;109(24):2959-64. [CrossRef] [PubMed]
- Crane AD, Militello M, Faulx MD. Digoxin is still useful, but is still causing toxicity. Cleve Clin J Med. 2024 Aug 1;91(8):489-499. [CrossRef] [PubMed]
- Steinberg JS, Shabanov V, Ponomarev D, Losik D, Ivanickiy E, Kropotkin E, Polyakov K, Ptaszynski P, Keweloh B, Yao CJ, Pokushalov EA, Romanov AB. Effect of Renal Denervation and Catheter Ablation vs Catheter Ablation Alone on Atrial Fibrillation Recurrence Among Patients With Paroxysmal Atrial Fibrillation and Hypertension: The ERADICATE-AF Randomized Clinical Trial. JAMA. 2020 Jan 21;323(3):248-255. [CrossRef] [PubMed]
- Atti V, Turagam MK, Garg J, Lakkireddy D. Renal sympathetic denervation improves clinical outcomes in patients undergoing catheter ablation for atrial fibrillation and history of hypertension: A meta-analysis. J Cardiovasc Electrophysiol. 2019 May;30(5):702-708. [CrossRef] [PubMed]
- Nawar K, Mohammad A, Johns EJ, Abdulla MH. Renal denervation for atrial fibrillation: a comprehensive updated systematic review and meta-analysis. J Hum Hypertens. 2022 Oct;36(10):887-897. [CrossRef] [PubMed]
- Bhatt DL, Vaduganathan M, Kandzari DE, et al. Long-term outcomes after catheter-based renal artery denervation for resistant hypertension: final follow-up of the randomised SYMPLICITY HTN-3 Trial. Lancet. 2022;400(10361):1405-1416. [CrossRef]
- Arora R, Doshi S, Wilber DJ. Mechanisms of atrial fibrillation and targets for catheter ablation. J Interv Card Electrophysiol. 2017;50(1):1-10. [CrossRef]
- Patterson E, Po SS, Scherlag BJ, Lazzara R. Triggered firing in pulmonary veins initiated by in vitro autonomic nerve stimulation. Heart Rhythm. 2005;2(6):624-631. [CrossRef]
- Gordon D, Kim S, Brooks AG, Sugumar H, Lau DH, Sanders P. Autonomic Modulation in Atrial Fibrillation: Where Are We in 2021? Heart Lung Circ. 2021;30(10):1516-1525. [CrossRef]
- Oh S, Zhang Y, Bibevski S, Marrouche NF, Natale A, Mazgalev TN. Vagal denervation and atrial fibrillation inducibility: role of the posterior left atrium. J Am Coll Cardiol. 2011;57(4):366-374. [CrossRef]
- Pokushalov E, Romanov A, Corbucci G, Artyomenko S, Turov A, Shirokova N, Karaskov A, Steinberg JS. Selective ganglionated plexi ablation for paroxysmal atrial fibrillation. Heart Rhythm. 2009;6(9):1257-1264. [CrossRef]
- Driessen AHG, Berger WR, Krul SPJ, et al. Ganglion Plexus Ablation in Advanced Atrial Fibrillation: The AFACT Study. J Am Coll Cardiol. 2016;68(11):1155-1165. [CrossRef]
- Katritsis DG, Pokushalov E, Romanov A, et al. Autonomic denervation added to pulmonary vein isolation for paroxysmal atrial fibrillation: a randomized clinical trial. J Am Coll Cardiol. 2013;62(24):2318-2325. [CrossRef]
- Duytschaever M, Demolder A, El Haddad M, et al. Ganglionated Plexi Ablation Added to Pulmonary Vein Isolation for Paroxysmal Atrial Fibrillation: A Multicenter Randomized Trial (GAPP-AF). Eur Heart J. 2020;41(28):2841-2849. [CrossRef]
- Lei Q, Jiang Z, Shao Y, Liu X, Li X. Stellate ganglion, inflammation, and arrhythmias: a new perspective on neuroimmune regulation. Front Cardiovasc Med. 2024;11:1453127. Published 2024 Sep 12. [CrossRef]
- Shen MJ, Zipes DP. Role of the autonomic nervous system in modulating cardiac arrhythmias. Circ Res. 2014;114(6):1004-1021. [CrossRef]
- Vaseghi M, Shivkumar K. The role of the autonomic nervous system in sudden cardiac death. Prog Cardiovasc Dis. 2008;50(6):404-419. [CrossRef]
- Nakagawa H, Scherlag BJ, Patterson E, Ikeda A, Lockwood D, Jackman WM. Pathophysiologic basis of autonomic ganglionated plexus ablation in patients with atrial fibrillation. Heart Rhythm. 2009;6(12 Suppl):S26-S34. [CrossRef]
- Groenendyk J, Mandler A, Luan D, et al. Management of Rapid Atrial Fibrillation Using Stellate Ganglion Blockade. JACC Case Rep. 2024;29(18):102530. Published 2024 Sep 18. [CrossRef]
- Li S, Scherlag BJ, Yu L, Sheng X, Zhang Y, Ali R, Dong Y, Ghias M, Po SS. Low-level vagosympathetic stimulation: a paradox and potential new modality for the treatment of focal atrial fibrillation. Circ Arrhythm Electrophysiol. 2009 Dec;2(6):645-51. [CrossRef] [PubMed]
- Stavrakis S, Humphrey MB, Scherlag BJ, et al. Low-level transcutaneous electrical vagus nerve stimulation suppresses atrial fibrillation. J Am Coll Cardiol. 2015;65(9):867-875. [CrossRef]
- Stavrakis S, Stoner JA, Humphrey MB, et al. TREAT AF (Transcutaneous Electrical Vagus Nerve Stimulation to Suppress Atrial Fibrillation): A Randomized Clinical Trial. JACC Clin Electrophysiol. 2020;6(3):282-291. [CrossRef]
- Premchand RK, Sharma K, Mittal S, Monteiro R, Dixit S, Libbus I, DiCarlo LA, Ardell JL, Rector TS, Amurthur B, KenKnight BH, Anand IS. Autonomic regulation therapy via left or right cervical vagus nerve stimulation in patients with chronic heart failure: results of the ANTHEM-HF trial. J Card Fail. 2014 Nov;20(11):808-16. [CrossRef] [PubMed]
- Jongkees BJ, Immink MA, Finisguerra A, Colzato LS. Transcutaneous Vagus Nerve Stimulation (tVNS) Enhances Response Selection During Sequential Action. Front Psychol. 2018 Jul 6;9:1159. [CrossRef] [PubMed]
- Stavrakis S, Chakraborty P, Farhat K, et al. Noninvasive Vagus Nerve Stimulation in Postural Tachycardia Syndrome: A Randomized Clinical Trial. JACC Clin Electrophysiol. 2024;10(2):346-355. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



