
Submitted:
19 March 2025
Posted:
20 March 2025
You are already at the latest version
Abstract
Alterations in sympathetic nervous activity are evident in response to changes in body weight. Sympathetic nervous activity and sympathetic responses to weight change are regionalized, with alterations in end organ function dependent on the changes occurring in brain regulatory pathways invoked and in the effector organs engaged. Obesity-induced activation of the sympathetic nervous system likely contributes to the initiation and worsening of cardiometabolic risk factors, including elevated blood pressure, cardiac dysfunction, dyslipidaemia, increased fasting blood glucose, insulin resistance and non-alcoholic steatohepatitis. Unintended weight loss, as occurs in cachexia, is driven, at least in part, by activation of sympathetic nervous-stimulated thermogenesis. The complexity of sympathetic nervous regulation renders the use of global measures of sympathetic activity problematic and the development of targeted therapies difficult, but not without promise or precedent. Knowledge of the central and peripheral pathways involved in sympathetic nervous regulation has opened opportunities for pharmacological, surgical and device-based approaches to mitigate the burden of disease development and progression. In this narrative review, we elaborate on sympathetic activity in response to changes in body weight, the brain pathways involved, and the cardiovascular and metabolic risks associated with perturbations in regional sympathetic activity.
Keywords:
obesity
; body weight
; autonomic nervous system
; brain pathways
; cachexia
; anorexia
; cardiovascular risk
; diabetes
; noradrenaline
1. Introduction
Malnutrition is often viewed through a prism concentrating on either low body weight and unintentional weight loss or weight gain and obesity. Importantly, when viewed as a continuous variable, being at each end of the body weight spectrum confers elevated risk of cardiometabolic disease development. Overweight and obesity are well-recognised as conferring increased risk for hypertension [1], diabetes [2] and cardiovascular disease [3] with the elevated risk of disease development being driven by the accumulation of body fat and fat distribution rather than increased body mass index (BMI) per se [4]. The excess adipose tissue in obese individuals produces adipokines that can act centrally and inflammatory cytokines that promote endothelial dysfunction, vascular inflammation and oxidative stress, further exacerbating cardiometabolic risk. The relationship between adiposity and cardiovascular risk is, however, not linear and better described as U-shaped, given that large population studies have indicated that being underweight is also linked with increased relative risk of stroke, myocardial infarction, and coronary artery disease [5,6,7]. Unintentional weight loss seen in clinical conditions such as anorexia nervosa and cachexia, are associated with cardiovascular and metabolic complications.
The determinants linking energy balance, body weight and disease development are complex, involving interaction between multiple social and environmental factors that influence behavioral and physiological factors that drive food intake and energy disposition. While the pathophysiological mechanisms underlying the development of the metabolic syndrome and the generation of obesity–related illness are complex and extend beyond the important triad of increased sedentary lifestyle, poor diet and genetic predisposition, it is clear from clinical and preclinical observations that the sympathetic nervous system is important in the generation of obesity-related illness. Chronic sympathetic activation in obesity leads to high blood pressure, metabolic dysregulation and contributes to the development of left ventricular hypertrophy, arterial stiffness, and endothelial dysfunction, all of which are independent risk factors for cardiovascular disease. The role of the sympathetic nervous system in underweight-related illness is less clear, largely due to the limited investigations at the stages of disease development and recovery.
2. Assessing Sympathetic Nervous Activity
Following von Euler’s identification of noradrenaline (sympathin) as the sympathetic neurotransmitter [8] and the subsequent demonstration of an association between the frequency of splenic nerve stimulation and noradrenaline release in the spleen [9], a wide range of measures have been used to provide an index of sympathetic nervous activity in clinical, experimental and epidemiological studies. While not extensive, as new and apparently novel markers are regularly proposed, the list includes:
- Direct nerve recording using microneurography [14];
- Isotope dilution during a tracer dose infusion of radiolabeled noradrenaline for estimating the rate of release of neurotransmitter [15];
- Tissue microdialysis [16];
- I123-metaiodobenzylguanidine (MIBG) imaging of the heart [17];
- Visualizing catecholamine containing nerve fibers using glyoxylic acid histofluorescence [20];
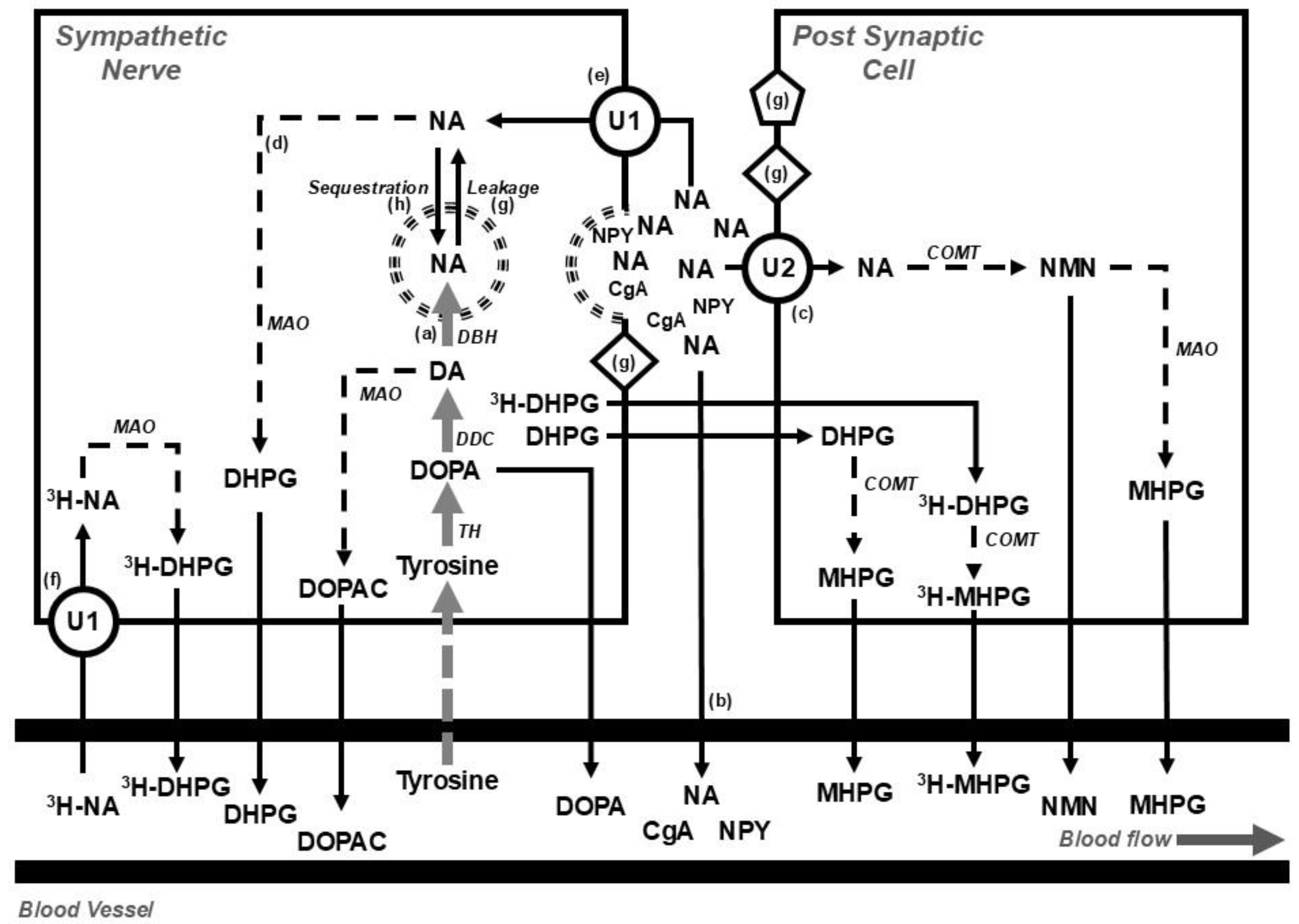
While some of these methods do provide insight into sympathetic nervous processes, whether they provide an accurate indication of sympathetic nervous activity or nerve firing rate, is problematic and interpretation is dependent on context and consideration of other factors, including rates of synthesis, storage, release, and metabolism of noradrenaline [23] (Figure 1). The tissue concentration of noradrenaline, for instance, provides little information on nerve firing rates. Similarly, levels of noradrenaline in plasma are dependent on the rate of entry into and clearance from the circulation, so that elevated plasma levels that occur with head-up tilt or standing may arise because of a reduction in plasma clearance rather than an increase in nerve firing as occurs with head-up tilt in patients with autonomic failure [24]. Similarly, the noradrenaline transporter is responsible for the intraneuronal reuptake of noradrenaline [25] so that changes in noradrenaline transporter expression may also contribute to alterations in plasma noradrenaline spillover to plasma is evident following transporter blockade with desipramine [27] and increased heart rate in response to standing occurs in patients with the postural orthostatic tachycardia syndrome in whom reduced expression of the noradrenaline transporter was documented [28,29]. Expression and trafficking of the noradrenaline transporter to the cell surface is regulated by a raft of intracellular and extracellular compounds, including signaling molecules, acetylcholine, insulin, angiotensin II, and noradrenaline [30]. Additionally, expression of the noradrenaline transporter maybe reduced due to single nucleotide polymorphisms [28,31], and epigenetic mechanisms involving histone modifications on the gene promotor [32].
Figure 1.
Diagram showing (top section) the disposition of noradrenaline in postganglionic sympathetic nerve endings and post synaptic cells (e.g. blood vessel, muscle cell, cardiac myocyte) and (bottom) overflow into the systemic circulation under basal conditions and during a steady state infusion of a tracer dose of tritium labeled noradrenaline (3H-NA). The use of tritium enables the calculation of the rate of noradrenaline clearance from, and spillover to, plasma. At steady state, the rate of noradrenaline synthesis (a) equals the rate of noradrenaline turnover; where noradrenaline turnover is equal to the sum of the rates of spillover of noradrenaline to plasma (b), extraneuronal uptake and metabolism of noradrenaline (c) and, intraneuronal metabolism of noradrenaline (d). The availability of noradrenaline for intraneuronal metabolism is determined on the balance between the entry of noradrenaline into the axoplasm via the processes of reuptake (e) and leakage (g), and removal from the axoplasm by vesicular sequestration. Circulating 3H-NA may be extracted from plasma via the process of neuronal uptake (uptake 1; U1) and metabolized intraneuronally (f) or extraneuronally (U2). Following an influx of calcium, storage vesicles migrate to the nerve ending and release their contents. The contents include noradrenaline and other vesicular constituents including neuropeptide Y (NPY) and chromogranin A (CgA). Compounds released from the storage vesicles can act on pre- or post-neuronal receptors (g) or overflow into the circulation (b). The synthesis of noradrenaline from tyrosine occurs in the neuronal cell body and is indicated in grey, catabolic pathways are indicated by dotted arrows. Figure adapted from Eisenhofer et al [33]. Abbreviations: CgA, chromogranin A; COMT, catechol-O-methyltransferase; DA, dopamine; DBH, dopamine β hydroxylase; DDC, DOPA decarboxylase; DOPA, dihydroxyphenylalanine; NA, noradrenaline; DHPG, 3,4-dihydroxyphenylglycol; DOPAC, dihydroxyphenylacetic acid; MAO, monoaminoxidase; MHPG, 3-methoxy-4-hydroxyphenylglycol; NMN, normetanephrine; NPY, neuropeptide Y; TH, tyrosine hydroxylase; U1, uptake 1; U2, uptake 2; 3H, tritium.
Figure 1.
Diagram showing (top section) the disposition of noradrenaline in postganglionic sympathetic nerve endings and post synaptic cells (e.g. blood vessel, muscle cell, cardiac myocyte) and (bottom) overflow into the systemic circulation under basal conditions and during a steady state infusion of a tracer dose of tritium labeled noradrenaline (3H-NA). The use of tritium enables the calculation of the rate of noradrenaline clearance from, and spillover to, plasma. At steady state, the rate of noradrenaline synthesis (a) equals the rate of noradrenaline turnover; where noradrenaline turnover is equal to the sum of the rates of spillover of noradrenaline to plasma (b), extraneuronal uptake and metabolism of noradrenaline (c) and, intraneuronal metabolism of noradrenaline (d). The availability of noradrenaline for intraneuronal metabolism is determined on the balance between the entry of noradrenaline into the axoplasm via the processes of reuptake (e) and leakage (g), and removal from the axoplasm by vesicular sequestration. Circulating 3H-NA may be extracted from plasma via the process of neuronal uptake (uptake 1; U1) and metabolized intraneuronally (f) or extraneuronally (U2). Following an influx of calcium, storage vesicles migrate to the nerve ending and release their contents. The contents include noradrenaline and other vesicular constituents including neuropeptide Y (NPY) and chromogranin A (CgA). Compounds released from the storage vesicles can act on pre- or post-neuronal receptors (g) or overflow into the circulation (b). The synthesis of noradrenaline from tyrosine occurs in the neuronal cell body and is indicated in grey, catabolic pathways are indicated by dotted arrows. Figure adapted from Eisenhofer et al [33]. Abbreviations: CgA, chromogranin A; COMT, catechol-O-methyltransferase; DA, dopamine; DBH, dopamine β hydroxylase; DDC, DOPA decarboxylase; DOPA, dihydroxyphenylalanine; NA, noradrenaline; DHPG, 3,4-dihydroxyphenylglycol; DOPAC, dihydroxyphenylacetic acid; MAO, monoaminoxidase; MHPG, 3-methoxy-4-hydroxyphenylglycol; NMN, normetanephrine; NPY, neuropeptide Y; TH, tyrosine hydroxylase; U1, uptake 1; U2, uptake 2; 3H, tritium.
The association between changes in body weight, the development of obesity and sympathetic nervous activation are influenced by a number of factors including, but not limited to, ageing [34], resting energy expenditure and the thermic effect of food [35], ethnicity [36] and sex [37,38]. When considering the role of the sympathetic nervous system in the genesis of weight-related physiological complications, it is important to note that sympathetic nervous activity is regionalized and that sympathetic nervous responses are specific to the type and magnitude of the initiating factor or stressor [39]. For instance, the level of change in muscle sympathetic nerve activity (MSNA) during hand grip exercise is dependent on body position and biological sex, with males demonstrating more pronounced increases in MSNA during upright exercise than females [40]. In heart failure there is a marked increase in MSNA [41] and cardiac noradrenaline spillover [41,42] early in disease development, with renal noradrenaline spillover being increased in more prolonged and severe disease [41]. With laboratory mental stress, the sympathetic outflow to the heart is preferentially activated [43] whilst the response of MSNA to mental stress demonstrates substantial variability [44]. Similarly, in response to carbohydrates, elevation of MSNA is evident following glucose but not fructose infusion [45], with the magnitude of response to glucose being dependent on the baseline level of insulin sensitivity [46]. Taken together, while changes in sympathetic nervous activation may drive disease development and impact on outcomes, it is important to consider the measure in question and any changes in relation to end-organ function and the context in which variations occur.
3. Sympathetic Activity and Body Weight
3.1. Obesity and Weight Gain
Numerous preclinical studies have documented the effects of weight gain on sympathetic nervous activity. In high fat-fed rabbits, for instance, the resulting weight gain leads to a rapid increase in renal sympathetic nerve activity [47]. However, in humans, due to the invasive nature of testing, the effects of weight gain on sympathetic drive have been less documented. Nevertheless, work done by Gentile et al demonstrated that even modest diet-induced weight gain was accompanied by increased sympathetic neural activity of ∼15–20% in healthy, non-obese males. The increment in MSNA was correlated with the magnitude of body weight and fat gain and was accompanied by increased blood pressure [48]. Similarly, weight gain during late pregnancy has recently been shown to be associated with increased MSNA and higher blood pressure [49]. Cross-sectional studies examining sympathetic tone in individuals with various levels of adiposity are more common. On balance, studies have demonstrated an association between BMI and MSNA in normal weight and overweight individuals [50]. However, it is important to note that several factors may influence the relationship between adiposity and MSNA. In those with metabolic syndrome, the elevated MSNA is more strongly associated with blood pressure rather than the degree of obesity [51].
The pattern of sympathetic activation in lean and obesity-related hypertension differs with regards to the firing characteristics of individual sympathetic fibers and the sympathetic outflows involved [52,53]. This implies that the central nervous system drivers of sympathetic activation and potential therapeutic targets differ between the hypertensive phenotypes. In normotensive humans, obesity is associated with increased turnover of serotonin in the brain, but the level of serotonin bears no association with the degree of sympathetic outflow [54]. This contrasts to that seen in subjects with hypertension in whom subcortical noradrenaline turnover is elevated and quantitatively linked with measures of sympathetic activation [55].
In young adults, we found an association between MSNA and markers of obesity and the plasma lipidomic profile, with the association being stronger in Asian subjects despite their BMI and other markers of obesity being less [56,57]. Previous studies indicated that obesity is linked with sympathetic activation in males whereas in females, MSNA is more closely associated with blood pressure rather than BMI [37,38]. In women with polycystic ovary syndrome (PCOS), MSNA is elevated but the degree of activation is not related to BMI [58,59]. Circulating androgens were more closely linked to the elevated MSNA [58] and were negatively associated with brown adipose tissue (BAT) thermogenesis [60]. Surprisingly, the elevated MSNA in women with PCOS was not reduced following treatment with moxonidine, indicating that the central driver of sympathetic tone in this group was not the rostral ventrolateral medulla (RVLM) [61]. Lansdown and colleagues provided support for increased MSNA in PCOS and demonstrated an association between functional magnetic resonance imaging (fMRI)-detected activation in the right orbitofrontal cortex and insulin sensitivity [62].
While these observational and experimental studies have demonstrated the detrimental effects of weight gain in adulthood on increasing cardiometabolic risk, it is important to appreciate that obesity and other risk factors in childhood are associated with cardiovascular events later in life [63,64]. Obesity exerts a detrimental effect on cardiovascular structure and function during childhood and adolescence [63] and is a primary correlate of cardiovascular risk factors such as lipids, glucose metabolism and blood pressure [65]. Although these observations parallel what is seen in adults, whether sympathetic nervous activation plays a role in the complications of obesity in children is difficult to determine given that few studies have used direct measures of sympathetic activity in this cohort. Resting heart rate has been proposed as a marker of cardiac sympathetic activity [66,67]. A review and meta-analysis of prospective studies found a positive association between resting heart rate and risk of cardiovascular disease, total cancer and all-cause mortality, with a linear dose–response increase in the relative risk of 15% for cardiovascular disease and 17% for all-cause mortality for each 10 beats per minute increase in resting heart rate [68]. In obese children and adolescents, heart rate has been associated with dyslipidaemia [69] and, across a range of BMI, with blood pressure and waist circumference [70]. Increased heart rate is not uncommon in obese adults [71]. Interestingly, a rise in heart rate has been linked to markers of inflammation [72] and in adults with high blood pressure, heart rate is strongly associated with cardiac noradrenaline spillover [66] but not MSNA [50]. Obesity is an important risk factor for the development of obstructive sleep apnoea and in adults, is characterised by elevated MSNA [73]. Similarly, urinary noradrenaline levels are elevated in children with obstructive sleep apnoea and sleep disordered breathing [74,75,76], although whether these are linked to obesity is uncertain [74].
A growing body of evidence supports the developmental hypothesis of disease whereby in utero growth restriction and low birth weight with subsequent accelerated weight gain lead to the development of metabolic disturbances later in life [77]. Low birth weight and accelerated postnatal growth are associated with higher blood pressure [78]. Bhargava and colleagues demonstrated an association between low weight at two years of age and impaired glucose tolerance or diabetes in young adulthood, despite not being obese [79]. Data from the Bogalusa Heart Study showed an inverse relationship between birth weight and the metabolic profile, with low birth weight being inversely associated with subsequent insulin resistance, and elevated plasma triglycerides and total cholesterol in adulthood [80]. Whether these observations are linked to elevated [81] or reduced [82] sympathetic tone remains unknown. In an experimental model of intrauterine growth restriction, an increased sympathetic activity and impaired glucose tolerance were observed in adult life but only in female animals [83]. Denton and colleagues have similarly described gender-specific differences in sensitivity to changes in the in utero environmental, with female offspring being more susceptible to the development of hypertension [84].
Taken together, available data provides strong evidence of sympathetic nervous activation occurring with weight gain. The degree of activation is, in general, proportional to the excess weight gain and is strongly linked to the distribution of fat, with intraabdominal visceral fat being an important driver of sympathetic activation.
3.2. Weight Loss
3.2.1. Lifestyle - Diet and Exercise
Lifestyle interventions including diet and exercise remain at the fore in managing and preventing obesity and obesity-related disease. Data from the 2001–2006 National Health and Nutrition Examination Survey indicated that around two-thirds of obese adults had reported trying to lose weight in the previous year [85]. Of these, 40% lost ≥5% and 20% lost ≥10% weight. Successful weight loss was associated with reduced intake of dietary fat, greater engaging in exercise, use of prescription weight loss medications, or participation in commercial weight loss programs [85]. Previous studies have demonstrated the effect of diet-induced weight loss on reducing sympathetic tone in normotensive individuals with obesity [86] or in those with the metabolic syndrome [87]. Exercise programs have been shown to reduce MSNA [88] and total and renal, but not cardiac, spillover of noradrenaline to plasma [88,89]. Although exercise programs are associated with improvement in fitness, body composition, blood pressure and metabolic profile, they do not necessarily confer added benefit in reducing sympathetic tone than diet alone [88]. Additionally, while exercise is an unequivocally important driver of health, exercise programs per se provide only a modest benefit to weight loss [90,91]. While there is clear evidence that diet-induced weight loss is associated with sympathetic inhibition, it is important to note that baseline sympathetic activity and sympathetic response to a glucose load, is predictive of successful weight loss following a 12-week diet [92].
3.2.2. Bariatric Surgery
Bariatric–metabolic surgery is an established and effective part of the weight loss management of patients with clinical obesity [4]. Commonly performed operations for the treatment of obesity worldwide include sleeve gastrectomy, adjustable gastric band, Roux-en-Y gastric bypass and biliopancreatic diversion with duodenal switch [93]. Data from the Swedish Obese Subjects study demonstrated that maximal weight loss of between 20–32% was achieved 1-2 years post-surgery [94]. The weight loss achieved with surgery has been shown to confer health benefits, including reduced mortality associated with cardiovascular disease and cancer and improved physical and mental health [95]. Ten percent weight loss after laparoscopic adjustable gastric band surgery was accompanied by reduction in MSNA and improvement in blood pressure, baroreflex sensitivity, metabolic profile, and renal function [96]. Similarly, improvement in metabolic and hemodynamic function and a decrease in MSNA was evident following weight loss after vertical sleeve gastrectomy [97].
3.2.3. Anorexia Nervosa
In women with current anorexia nervosa and BMI around 16 kg/m2, MSNA and sudomotor function as well as systolic blood pressure and heart rate were significantly reduced compared with healthy counterparts [98]. Decreased plasma noradrenaline and reduced urinary 3-methoxy-4-hydroxyphenylglycol, the deaminated and O-methylated metabolite of noradrenaline (Figure 1), have also been described in acutely ill patients [99]. Depressed sympathetic activity in anorexia nervosa may be attributed to abnormal glucose levels and regulation and low leptin [98]. Anorexia nervosa is known to have a high mortality rate with a significant contributor of mortality being cardiovascular complications encompassing structural, conduction and haemodynamic abnormalities occurring both during the state of starvation and after treatment with re-feeding [100]. Previous data by Zamboni and colleagues demonstrated that adults with current anorexia nervosa have a higher proportion of visceral than subcutaneous adipose tissue [101] and at least in the initial period following weight restoration, subjects present with increased abdominal obesity [102,103], normalization of leptin [104] and an increase in MSNA and urinary noradrenaline, albeit to a resting level that remains lower to that seen in healthy BMI-matched control subjects [98,99]. Small increments in abdominal obesity in weight-recovered patients are however associated with decreased insulin sensitivity [105]. Whether changes in glucose metabolism and/or leptin concentrations are responsible for sympathetic activation following re-feeding remains unclear.
3.2.4. Cachexia
Cachexia is a hypermetabolic condition characterised by unintended weight loss, muscle and adipose tissue atrophy, systemic inflammation, fatigue and loss of appetite [106]. It develops in the advanced stages of chronic diseases, primarily in cancer and heart failure, kidney disease and obstructive pulmonary disease and is usually associated with poorer prognosis. In cancer-associated cachexia the browning of white and beige adipocytes accelerates disease progression by increasing sympathetic nervous-stimulated thermogenesis [107,108]. Given the presentation of the disease and the important role of the sympathetic nervous system in energy disposition, therapeutic targets in cachexia include modifying adrenergic signalling, either through agents such as, but not limited to, beta-blockers acting in the periphery [106] or centrally-acting agents.
Recent data from the ROMANA 1 and ROMANA 2 clinical trials showed that treatment with the selective ghrelin receptor agonist, anamorelin, was associated with significant weight gain and improved body composition in patients with inoperable lung cancer and cachexia [109]. In patients with heart failure where high sympathetic tone predicts poor prognosis [110,111] and may be related to a hypermetabolic state, it has been shown that MSNA was higher in those who experienced weight loss and was the best predictor of subsequent weight loss in this population [112]. This suggests that reducing sympathetic tone may be a target to prevent weight loss in patients with heart failure.
3.2.5. Pharmacological Agents
Pharmacological interventions may be needed to augment the management of body weight and improving weight-related co-morbidities such as insulin resistance, glucose tolerance, dyslipidaemia and hypertension. Previous reports have reviewed drug classes associated with weight management and their influence on sympathetic nervous regulation [113]. While some earlier studies using beta adrenergic blocking drugs were shown to promote weight gain and worsen insulin resistance, newer agents, such as carvedilol, may exert a more favourable effect on metabolic parameters. Similarly, centrally acting agents such as imidazoline I1 agonists may improve metabolic control. Here we concentrate on some of the recent developments, with a focus on incretins and glifozins. Pharmacological approaches for weight gain in cachexia and anorexia nervosa have been noted previously.
Incretins
The incretins, glucagon-like peptide-1 (GLP-1, produced by the L cells of the lower gut) and glucose-dependent insulinotropic peptide (GIP, produced by the K cells of the upper gut), are released shortly after eating to stimulate insulin and glucagon secretion. Both incretins are rapidly deactivated by dipeptidyl peptidase 4 (DPP4). Functionally, the L cells in the gut are innervated by sympathetic nerves which, if activated, suppress postprandial GLP-1 secretion and impair glucose utilization [114]. Receptors for GLP-1 are distributed throughout the body and may exert effects beyond glucose control and satiety [115]. For instance, Pauza et al demonstrated GLP-1 receptor expression in the carotid body in rats and humans and found that its decreased expression was linked to sympathetic activation, driving blood pressure elevation in obese rats [116].
An increasing number of GLP-1 agents have been developed and trialed, showing improvement in glucose control and weight reduction [117]. The recent demonstration of the effectiveness of tirzepatide [118] and retatrutide [119] holds promise for combination therapy targeting GLP-1, GIP and glucagon to promote weight loss and reduce obesity-related co-morbidities. These agents exert beneficial effects in addition to weight loss, with data from the LEADER Trial indicating that use of the GLP-1 receptor agonist, liraglutide, reduced death from cardiovascular disease, nonfatal myocardial infarction, and nonfatal stroke among patients with type 2 diabetes [120]. Further, tirzepatide, which is a GIP and GLP-1 receptor agonist, improved blood pressure and physical aspects of quality of life [118], and the triple combination, retatrutide, reduced liver and abdominal fat and improved insulin sensitivity and lipid metabolism in obese individuals [121]. Paradoxically, given the relationship between heart rate and mortality [68], these improvements following therapy contrast with the effect of GLP-1 agonists on heart rate, with short-acting drugs associated with a transient increase of 1-3 beats per minute and longer-acting agents a rise of around 3-10 beats per minute [122]. The increased heart rate following GLP-1 therapy likely does not engage the autonomic nervous system, perhaps explaining this paradox. In a comprehensive series of experiments, Lubberding and colleagues demonstrated that the chronotropic effect of GLP-1 is independent of sympathetic and vagal innervation; but rather, depends on a direct activation of GLP-1 receptors in pacemaker cells of the sinus node [123]. At least acutely, in humans, GLP-1 administration has been shown to exert a differential effect on cardiac and muscle vasoconstrictor sympathetic outflows, increasing MSNA with no change in heart rate or measures of heart rate variability [124].
Glifozins
Sodium glucose cotransporters (SGLTs) occur mainly in the kidneys and play a key role managing hyperglycemia independently of insulin [125]. By inhibiting the SGLT2 receptor, gliflozins prevent the reuptake of glucose by the kidney and lower the glucose level in the blood by promoting the excretion of glucose in the urine. Many trials have demonstrated the benefit of SGLT blockade, with a recent meta-analysis clearly showing that SGLT2 inhibition reduces the risk of major adverse cardiovascular events across patient groups, irrespective of the presence of atherosclerotic cardiovascular disease, diabetes or renal function at baseline [126]. The effect was evident largely due to a reduction in cardiovascular death, particularly heart failure and sudden cardiac death. A further meta-analysis of trials revealed that patients receiving an SGLT2 inhibitor of combined SGLT1/SGLT2 inhibitors had a mean body weight reduction of -1.79 kg (BMI change -0.71) compared with placebo [127].
Indicative of the effect of SGLT receptor blockade on sympathetic innervation, kidney and heart from neurogenic hypertensive Schlager mice treated with dapagliflozin displayed reduced tyrosine hydroxylase staining and a reduced kidney noradrenaline content compared with control mice [128]. In parallel, sympathetic denervation with 6-hydroxydopamine reduced blood pressure, improved glucose metabolism and led to a reduction in SGLT2 expression in the kidney [128]. A role for SGLT receptors in regulating sympathetic outflow is further supported by the demonstration of SGLT1 and SGLT2 receptors in the RVLM in the brainstem [129] and SGLT2 receptors in the hypothalamus, amygdala and periaqueductal gray [130] of the mouse. Treatment with the SGLT2 receptor blocker, empagliflozin, hyperpolarized neurones in the RVLM [129], thereby providing evidence of potential central sympathoinhibition associated with SGLT receptor blockade. Treatment with dapagliflozin was associated with increased c-fos expression in the hypothalamus, amygdala and periaqueductal gray [130]. While these experiments provide some support for interaction between SGLT receptor blockade and sympathetic nervous activity, short-term treatment with empagliflozin in patients with type 2 diabetes had no effect on MSNA [131]. In a more recent study from the same group, Heusser and colleagues observed no difference in MSNA between treatment with an SGLT2 blocker and hydrochlorothiazide in patients with type 2 diabetes [132]. The change in MSNA following therapy was negatively associated with the change in body weight, with empagliflozin treatment showing a greater weight loss [132]. The authors proposed that the changes observed may have been influenced by changes in renal sodium excretion. Whether SGLT blockade influences cardiac or renal sympathetic activity in humans remains unknown.
4. Brain Pathways Associated with Sympathetic Regulation
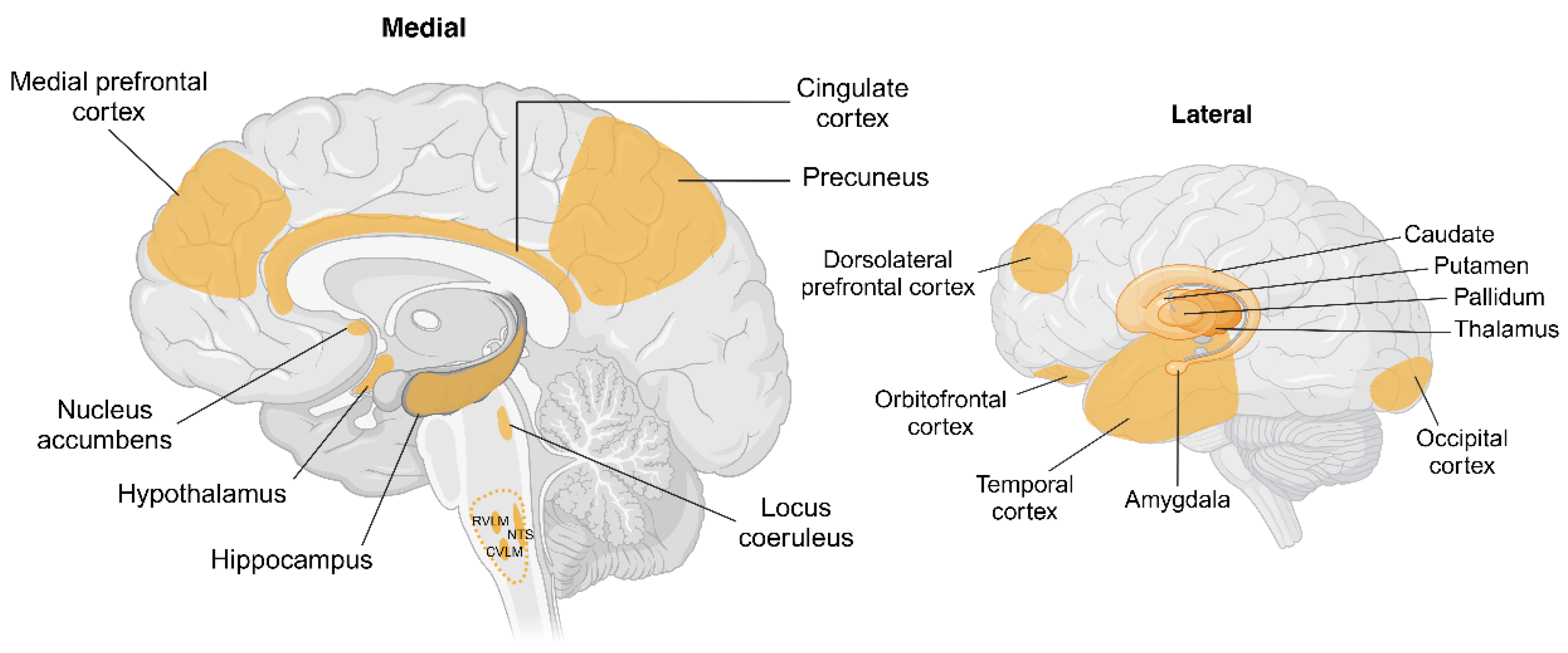
While the sympathetic nervous system is, by definition, part of the peripheral nervous system, it is regulated by a coordinated interplay between peripheral and central processes. Direct monosynaptic inputs from the brain to the sympathetic preganglionic neurones in the intermediolateral column (Figure 2) arise from the RVLM, caudal ventrolateral medulla (CVLM), paraventricular nucleus (PVN) of the hypothalamus, caudal raphe and pontine noradrenergic A5 group [133]. Work in animals has demonstrated the importance of the RVLM along with its connections with brainstem and hypothalamic nuclei as important in regulating sympathetic outflow to the muscle, splanchnic and renal vascular beds [134,135]. Beat-to-beat regulation of sympathetic tone is achieved through the coordinated activity of the nucleus tractus solitarius (NTS) which receives baroreceptor input and projects excitatory signals to the CVLM which in turn leads to inhibitory control of the RVLM [134]. Similarly, pressor noradrenergic neurones in the A5 region, locus coeruleus (A6 region) and hypothalamus have been shown to influence sympathetic outflow [136,137,138]. Studies in humans using internal jugular vein blood sampling provided some evidence for an association between brain noradrenaline turnover, changes in pulmonary wedge pressure and cardiac sympathetic activity [42] whilst internal jugular venous overflow of noradrenaline provides an index of cerebrovascular sympathetic nerve activity [139]. Interestingly, most noradrenaline in the brain is in the locus coeruleus [140] which, recently, has been shown to be pivotal in the regulation of the glymphatic system during sleep [141]. Recent studies in humans utilizing direct recordings of MSNA provides us with a picture of near real-time correlation of sympathetic outflow with activity in the brain. Macefield and Henderson coupled fMRI with MSNA and identified several cortical and subcortical brain regions that contribute to central autonomic control [142,143]. Further, signal intensity within key hypothalamic nuclei including the ventromedial (VMH) and dorsomedial hypothalamus (DMH) have also shown significant positive covariations with MSNA [144]. The arcuate nucleus (ARC) within the hypothalamus is known to have neuronal projections to the VMH and DMH but was not reported to have significant associations with MSNA. Overall, in the cortex, regions including the insula, dorsolateral prefrontal cortex, posterior cingulate and precuneus also showed positive correlations with MSNA. Further, the same study also reported functional connectivity of the RVLM with the VMH and DMH as well as the thalamus, insula, posterior cingulate and precuneus. Similarly, the VMH was shown to be functionally coupled to the RVLM, insula, dorsolateral prefrontal cortex and precuneus, highlighting the complexity of sympathetic regulation and the contribution of these cortical and subcortical regions to the sympathetic connectome.
Figure 2.
Schematic showing brain regions associated with changes in body weight and sympathetic nervous system activity. Key cortical and subcortical regions within the brain undergo structural and functional changes with weight gain or weight loss. Hypothalamic regions including arcuate, paraventricular, ventromedial and dorsomedial nuclei are identified as targets for peripherally or centrally originating afferent and humoral signals involving adipokines, insulin and glucose. Key brainstem regions including the nucleus tractus solitarius (NTS), caudal and rostral ventrolateral medulla (CVLM and RVLM respectively) are recognized to be involved in the generation of sympathetic nerve activity with RVLM being the primary nucleus for outflow to renal, splanchnic and muscle vascular beds. Cortical regions shown are known to be influenced by body weight however the pathways by which these occur are not understood well. Abbreviations: CVLM, caudal ventrolateral medulla; NTS, nucleus tractus solitarius; RVLM, rostral ventrolateral medulla. Created in BioRender. Braun, J. (2025) https://BioRender.com/a80q797.
Figure 2.
Schematic showing brain regions associated with changes in body weight and sympathetic nervous system activity. Key cortical and subcortical regions within the brain undergo structural and functional changes with weight gain or weight loss. Hypothalamic regions including arcuate, paraventricular, ventromedial and dorsomedial nuclei are identified as targets for peripherally or centrally originating afferent and humoral signals involving adipokines, insulin and glucose. Key brainstem regions including the nucleus tractus solitarius (NTS), caudal and rostral ventrolateral medulla (CVLM and RVLM respectively) are recognized to be involved in the generation of sympathetic nerve activity with RVLM being the primary nucleus for outflow to renal, splanchnic and muscle vascular beds. Cortical regions shown are known to be influenced by body weight however the pathways by which these occur are not understood well. Abbreviations: CVLM, caudal ventrolateral medulla; NTS, nucleus tractus solitarius; RVLM, rostral ventrolateral medulla. Created in BioRender. Braun, J. (2025) https://BioRender.com/a80q797.
4.1. Brain Pathways Associated with Weight Gain
Preclinical and clinical investigations using neuroimaging techniques such as magnetic resonance imaging (MRI), fMRI, positron emission tomography (PET), computed tomography (CT) and magnetoencephalography (MEG) have been used to gain insight into the key brain regions that undergo structural and functional changes with weight gain. Although several articles have discussed obesity and weight-loss associated brain changes in the context of reward-circuitry, cognitive function and energy metabolism [145,146,147,148,149], here we summarise obesity-associated changes in brain function with a particular focus on regions linked with sympathetic dysregulation, building on our recent review on this topic [150].
Tadross and colleagues recently published a comprehensive cellular transcriptomic map of the human hypothalamus, highlighting spatially distinct neuronal clusters and noting that six genes (MC4R, PCSK1, POMC, CALCR, BSN and CORO1A) were associated with BMI at the population level [151]. Not surprisingly, some of these genes are prominent in pathways involved in the regulation of satiety and energy balance and may influence sympathetic nervous regulation. For instance, increased adiposity drives hyperleptinemia. The elevated circulating leptin acts on the proopiomelanocortin (POMC) neurones in the ARC and agouti-related peptide (AgRP) neurones leading to an ARC-specific leptin resistance [152]. In the lean state, leptin-induced activation of POMC neurones in the ARC activates melanocortin receptor neurones in the PVN and DMH, thereby increasing sympathetic outflow to BAT [153]. Microinjection of leptin within the VMH has been shown to increase renal sympathetic nerve activity and blood pressure in rats [154]. Additionally, studies by Greenwood and colleagues provided support for melanocortin signalling in the control of human blood pressure through an insulin-independent mechanism [155]. The melanocortin receptor expressing neurones of the VMH have been shown to receive input from the POMC and AgRP neurones of the ARC, and activation of POMC neuronal input to the VMH was demonstrated to increase renal sympathetic nerve activity in obese rabbits [156]. Supporting these observations, studies in humans have shown increased brain production of leptin in obese individuals and that whole body leptin production was associated with renal noradrenaline spillover to plasma [157]. The neuronal populations within the ARC and VMH are also sensitive to circulating glucose [158]. Obesity-associated neuroinflammation, particularly in the hypothalamic neurones and glial cells, may drive glucose intolerance and insulin resistance [159]. Chronic disruption of insulin signalling in obesity is associated with blunted sympathetic response to glucose while maintaining an increased state of sympathetic outflow [160].
Regions within the brainstem and associated hypothalamic nuclei play a role in the beat-to-beat generation of sympathetic outflow [135]. Studies in obese Zucker rats have shown that impaired glutamatergic activation in the NTS is associated with increased sympathetic nervous activity and impaired baroreflex control [161]. Previous studies in animals have shown that a high-fat diet promoted oxidative stress and inflammation within the RVLM which, combined, contributed to obesity-induced sympathoexcitation [162]. In line with this evidence, therapeutic interventions such as calorie restriction which produces an antioxidant effect in the RVLM [163], or treatment with the imidazoline-agonist moxonidine [164] results in weight loss and inhibits sympathetic drive by acting at the level of the RVLM. Activity in subcortical regions including the amygdala and hippocampus have also been shown to be associated with BMI [165]. While cortical regions undergo structural and functional changes in obesity, whether they are associated directly with changes in sympathetic activity remains unknown.
4.2. Brain Pathways Associated with Weight Loss
Approaches to intentional weight loss may include lifestyle changes such as diet and exercise, bariatric surgery and pharmacological interventions. The changes in brain activity and connectivity associated with these interventions have recently been reviewed [149]. With bariatric surgery, the reduction in plasma ghrelin that occurs following sleeve gastrectomy was associated with decreased activation in the brain’s reward-related areas in response to energy-rich foods [166]. In line with this observation, intravenous infusion of ghrelin in lean and overweight individuals, at least acutely, has been shown to increase MSNA and plasma cortisol [167]. Improvements in both grey and white matter volumes and functional connectivity across multiple brain regions following sleeve gastrectomy have also been described [168]. Two years following Roux-en-Y surgery, improvements in cognition, and cardiovascular and mental health were accompanied by increased cortical thickness and maintenance of white matter and hippocampal volume [169]. Changes in brain function following lifestyle or pharmacological interventions depend, at least in part, on the intervention (for review see [149]) and the success in attaining weight loss. For instance, changes in the mesolimbic reward centre were related to reduced ghrelin levels and was only evident in those individuals who achieved successful weight loss [170]. With GLP-1 receptor agonist-induced weight loss, gut-derived signals stimulate the NTS, nucleus accumbens and ventral tegmental area, increasing serotonergic activity to promote satiety [171]. Additionally, activation of GLP-1 receptors in the area postrema in the brainstem modulates dopaminergic activity to reduce food intake and modulate activity the ARC of the hypothalamus [172,173]. With unintentional weight loss as occurs in, for instance, cancer cachexia, alterations in the gut microbiome have been shown to drive hypothalamic inflammation and changes in PVN activity in an animal model [174]. In patients with anorexia nervosa, widespread reduction in cortical thickness and reduced volumes in subcortical structures including the nucleus accumbens, amygdala, caudate, pallidum, hippocampus, putamen and thalamus has been described [175]. Importantly, the degree of change in brain structure was associated with BMI and was improved in those with partial weight recovery.
In summary, the monosynaptic (direct) determinants of sympathetic outflow from the intermediolateral column in the spinal cord are well-described. It is important to note that while these regions are important for the regulation of sympathetic nervous activity, higher brain regions are also engaged and respond to a wide range of humoral, hormonal, neural and psychological stimuli. The diversity of inputs controlling sympathetic outflow ensures that sympathetic responses are regionalized and likely offer precision and gain in regulating efferent responses. The diversity in regulatory sites may provide opportunistic targets and approaches for therapy. The subcortical and cortical brain regions implicated in the context of sympathetic activity and weight change include the ARC, PVN, VMH and DMH within the hypothalamus and RVLM and NTS within the brainstem. These regions receive afferent and humoral input that influence sympathetic outflow to various effector organs. Cortical areas including the frontal, temporal, occipital and insular regions have also been shown to undergo structural and functional changes associated with increased adiposity, however further investigations are required to fully understand the mechanisms driving these changes and their relation to sympathetic activity.
5. Regional Sympathetic Nervous Activity and Cardiometabolic Risk
The global escalation in obesity has led to a pronounced increase in prevalence of the metabolic syndrome, a clustering of metabolic disturbances and cardiovascular risk factors that is characterised by abdominal obesity, hyperglycaemia, impaired insulin sensitivity, high blood pressure, abnormal lipids and a systemic pro-inflammatory state. Obesity contributes to cardiovascular risk factors and, additionally, exerts direct adverse effects on cardiac structure and function [176], contributing to the development of both atherosclerotic and non-atherosclerotic cardiovascular disease independently of other risk factors [177]. While the pattern of cardio-metabolic risk associated with weight gain and obesity has been well described, the role of the sympathetic nervous system in generating or modifying risk is likely dependent on the pattern and strength of the sympathetic outflows engaged (Figure 3). While intentional weight loss exerts positive effects on sympathetic tone, unintentional weight loss as occurs in anorexia nervosa or cachexia is associated with detrimental physiological effects. In this section, we review the influence of weight change on regional sympathetic activity. It is important to note that effects on an organ may influence other vascular beds and so effects should not necessarily be considered in isolation but rather, considered as a network of integrated activities.
Figure 3.
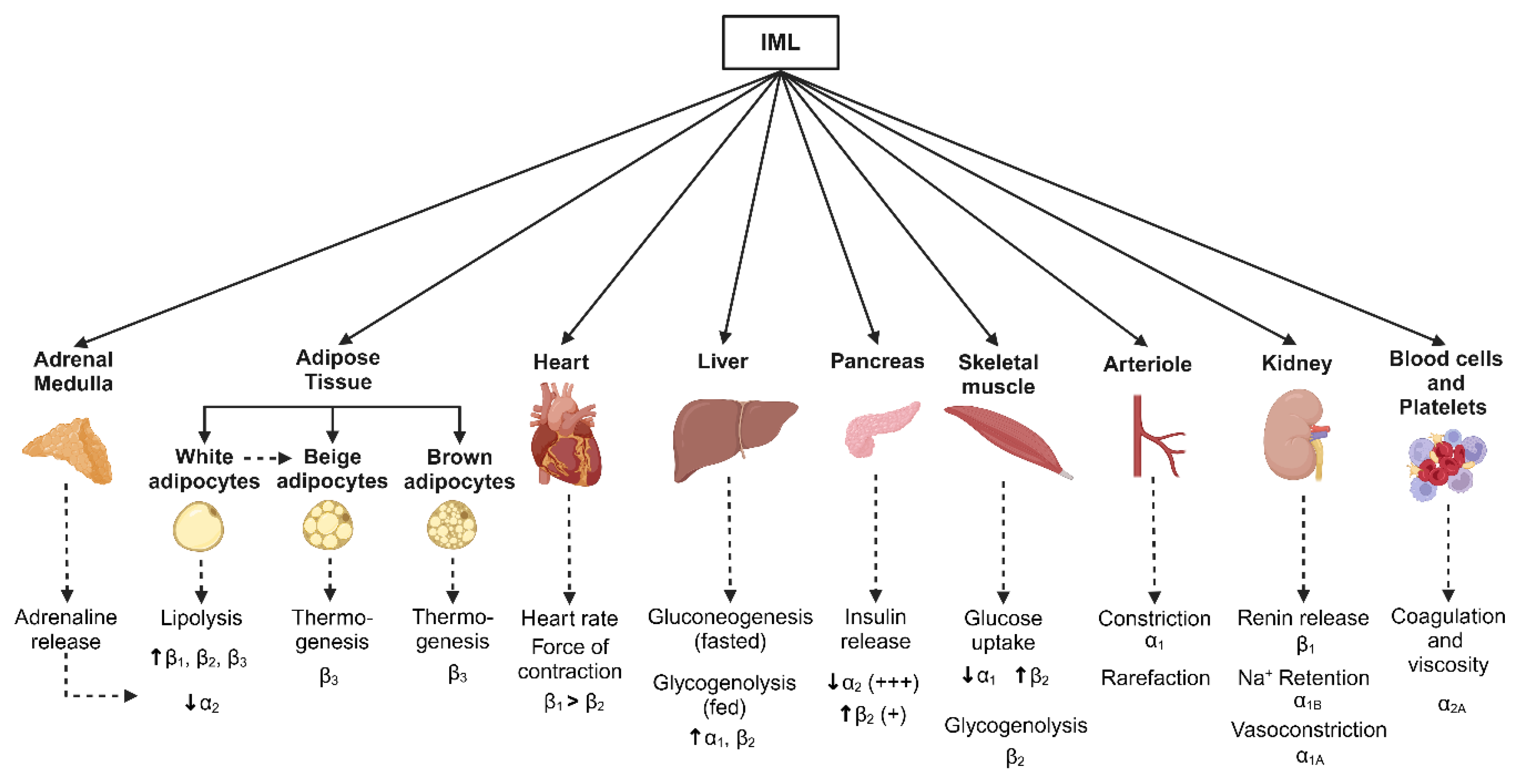
Schematic showing metabolic pathways associated with changes in body weight and sympathetic nervous system activity. Monosynaptic projections arising from brain regions including rostral and caudal ventrolateral medulla, caudal raphe, pontine noradrenergic A5 group as well as paraventricular nucleus of the hypothalamus provide input to the sympathetic preganglionic neurones in the intermediolateral cell (IML) column of the spinal cord. Sympathetic postganglionic neurones then project to target organs. Although sympathetic nervous-associated pathways vary between the weight gain and weight loss states, key effector organs and the corresponding adrenergic receptors in response to sympathetic activation are shown. Created in BioRender. Braun, J. (2025) https://BioRender.com/t56w833.
Figure 3.
Schematic showing metabolic pathways associated with changes in body weight and sympathetic nervous system activity. Monosynaptic projections arising from brain regions including rostral and caudal ventrolateral medulla, caudal raphe, pontine noradrenergic A5 group as well as paraventricular nucleus of the hypothalamus provide input to the sympathetic preganglionic neurones in the intermediolateral cell (IML) column of the spinal cord. Sympathetic postganglionic neurones then project to target organs. Although sympathetic nervous-associated pathways vary between the weight gain and weight loss states, key effector organs and the corresponding adrenergic receptors in response to sympathetic activation are shown. Created in BioRender. Braun, J. (2025) https://BioRender.com/t56w833.
5.1. Adipose Tissue
Obesity and the expansion in fat mass that typically occurs with weight gain is associated with sympathetic nervous activation [50] and increased cardiometabolic disease risk [178]. Data shows that the type and distribution of fat are important determinants of disease development with visceral obesity being the prime driver of sympathetic nervous activation [48,179,180]. Recent data points to a role for intramuscular fat being an important determinant of cardiometabolic disease development and progression [181]. Muscle sympathetic nerve activity is elevated in men with visceral but not subcutaneous obesity [179] and even modest increases in adipose tissue mass is linked with increased MSNA [48,182]. The classification and function of adipose tissue is dependent on the type of adipocytes present. White adipose tissue (WAT) is principally involved in energy storage and BAT in thermogenesis. Beige adipocytes have thermogenic properties and are found within WAT depots [183]. White adipose tissue is distributed throughout the body and forms most subcutaneous, visceral, and perivascular fat depots. The adipocytes in WAT store energy in the form of triglycerides loaded in large lipid droplets [184]. Energy production occurs through the generation of free fatty acids (FFAs) via lipolysis through the actions of insulin, the sympathetic nervous system and catecholamines via action on adrenergic receptors [185]. Conversely, increasing sympathetic drive to BAT facilitates energy expenditure and generation of heat through stimulation of BAT thermogenesis [186].
The detection of BAT in adult humans [187] raised the possibility that dysfunction in the genesis or function of BAT may underpin and predispose to the development of obesity. BAT activity, which is under sympathetic control [188], can be assessed by combining single photon emission CT (SPECT)/CT and 18F-flurodeoxyglucose PET/CT scanning [189]. While observations indicating a negative association between the amount of BAT and BMI [187], central obesity and liver fat [190], and altered function in obesity [191,192] indicates a possibly important role for BAT in metabolism and weight maintenance, the actual mechanisms at play remain to be determined. Carey and colleagues demonstrated that ephedrine could activate BAT in lean but not obese individuals [191] whereas Bahler et al found no difference in BAT activity in response to cold exposure between lean and obese men [193]. Recent studies using the β3 receptor agonist, mirabegron, demonstrated no effect on body weight but an improvement in glucose tolerance, hemoglobin A1c, and insulin sensitivity in obese subjects after 12 weeks of treatment [194].
Leptin is produced predominantly by fat cells [195], with subcutaneous fat being the main site of leptin production [196]. The concentration of leptin in plasma and cerebrospinal fluid is proportional to the degree of adiposity [197]. As noted previously, leptin released into the circulation acts centrally to influence appetite and energy expenditure but, in the obese state the metabolic action of leptin is impaired [198] whilst its sympathetic cardiovascular stimulatory effect remains preserved [199]. Studies in rabbits exposed to a high-fat diet have clearly shown that leptin plays a role in driving obesity-hypertension via a stimulatory effect on renal sympathetic nerve activity [47]. Whether this is the case clinically remains uncertain. In human obesity-related hypertension, there is evidence of sympathetic activation, based on an almost two-fold increase in the rate of spillover to plasma of noradrenaline into the renal veins [200] and increased nerve firing to the skeletal muscle vascular bed [201]. The increase in sympathetic outflow to the kidneys appears to be a necessary but apparently not a sufficient cause for the development of clinical hypertension, commonly being present also in overweight people with blood pressure in the normotensive range.
Adipose tissue plays an important role in energy storage and metabolism. Triacylglycerol stored in adipose tissue can be rapidly metabolized, converted to non-esterified fatty acids and released into the circulation for use as an energy source [202]. While white adipose tissue is innervated by sympathetic nerves and sympathetic activation to white fat is essential for lipolysis [186]. Previous work by our group has noted associations between MSNA and elements of the circulating lipidomic profile, including non-esterified fatty acids and triacylglycerol [57]. Circulating FFAs in plasma are an energy substrate and influence the development of insulin resistance. Free fatty acid availability is determined mainly by the rate of mobilization from adipose tissue triacylglycerol stores via the direct effect of sympathetic activation on lipolysis [186]. Other factors such as insulin, growth hormone, natriuretic peptides and some adipocytokines may also influence lipolysis. Free fatty acids can act throughout the body to disrupt insulin signaling and impair glucose uptake. In obesity, the increase in circulating FFAs that occurs with increased lipolysis contributes to the development of insulin resistance, glucose intolerance, and hypertension through combined effects on skeletal muscle and the renin-angiotensin system [202].
Adipose tissue also is the site of production and release of innate and adaptive immune cells and numerous cytokines, including leptin, adiponectin, resistin, tumor necrosis factor alpha and interleukin-6. Through their various pro- and anti-inflammatory processes, adipokines can exert positive or negative effects on a range of conditions including insulin resistance, diabetes, inflammation, and atherosclerosis [203]. There occurs an increase in expression of pro-inflammatory monocytes in obesity, with their abundance being associated with increasing BMI and waist circumference, and elevated circulating triglycerides, hemoglobin A1c, and decreasing high-density lipoprotein (HDL)-cholesterol [204]. Immune cells express adrenoceptors on their cell surface [205], raising the possibility that sympathetic activation contributes to adipose tissue inflammation [205]. Dietary interventions can exert differential effects on the production of anti-inflammatory adipokines, such as adiponectin, and pro-inflammatory adipokines, including interleukin-6 [206], and positively influence endothelial function [206] and measures of whole-body noradrenaline spillover to plasma and MSNA [182].
5.2. Liver and Pancreas
Noradrenaline containing nerve fibers arise from the celiac and superior mesenteric ganglia and project to hepatocytes in the liver [207]. Stimulation of the hepatic nerve in man causes a rapid increase in circulating glucose [208]. Similarly, the release of catecholamines following adrenal medulla stimulation is associated with hepatic glucose production [209]. The sympathetic nervous system promotes glucose production by activating glycogen breakdown (glycogenolysis) after a meal and increasing gluconeogenesis (glucose production from lactate, pyruvate and fatty acids) during overnight fasting or in between meals. In obese individuals and in patients with type 2 diabetes, however, rates of hepatic gluconeogenesis and glycogenolysis are increased, and rates of glycogen synthesis decreased which, combined, leads to elevated fasting and postprandial glucose levels [210]. Indeed, activation of the sympathetic nervous system is evident along the diabetes continuum, with elevated sympathetic activity occurring in subjects with impaired glucose tolerance [211], being further augmented in patients with type 2 diabetes [211,212]. Kato et al demonstrated that steatosis was linked with raised insulin resistance in muscle in patients with non-alcoholic fatty liver disease [213]. In an animal model, diet-induced steatosis was associated with a two-fold increase in the firing rate of the hepatic sympathetic nerves [214]. Subsequent denervation of the hepatic sympathetic nerves improved steatosis and liver triglyceride accumulation, independent of changes in body weight, caloric intake or body fat [214]. Taken together, these data clearly demonstrate an important role of the hepatic sympathetic nerves in generating at least some of the complications associated with the development of non-alcoholic fatty liver disease.
The pancreas is composed of multiple cell types including alpha (producing glucagon), beta (producing insulin), delta (producing somatostatin) and pancreatic polypeptide producing cells. While the beta and alpha cells in the pancreas respond directly to changes in blood glucose, neural input from the autonomic nervous system also plays an important role in glucose regulation. In general, sympathetic activation to the pancreas increases blood glucose through a combined effect on alpha and beta cells, increasing glucagon and reducing insulin secretion [215]. Additionally, sympathetic nerves have been shown to innervate endothelial cells adjacent to capillaries and reduce capillary diameter and islet blood flow in pancreatic slices [216,217]. Taken together, these observations demonstrate the multiple mechanisms by which the autonomic nervous system can influence glucose disposition through effects directly or indirectly on the pancreas.
In line with clinical observations [46,48,211], a recent experimental study reinforced that diet-induced insulin resistance and metabolic disorder occurs through increased sympathetic nervous system activity [218]. The sympathetic stimulatory effects of insulin are thought to be mediated by a direct increase in centrally driven sympathetic nervous outflow and a baroreflex mediated response to the vasodilatory actions of insulin [219]. Work by Sakamoto and colleagues showed in a mouse model that reduction in catecholamine signaling reduces lipolysis and protects against diet-induced insulin resistance, hyperglucagonemia, adipose tissue dysfunction, and the development of fatty liver disease [218].
5.3. Skeletal Muscle
Previous studies have clearly demonstrated that the sympathetic nervous system has anabolic effects on skeletal muscle [220] and that skeletal muscle is responsible for the majority of glucose uptake following an oral glucose load [221]. The development of insulin resistance is associated with the desensitization of muscle to insulin released by the pancreas to drive glucose uptake, resulting in elevated levels of circulating glucose [221]. Skeletal muscle insulin resistance in fact can appear well before the onset of pancreatic β-cell failure and diagnosis of type 2 diabetes. Sympathetic nerves innervating skeletal muscle can modulate glucose uptake via activation of β-adrenergic receptors. Conversely, stimulation of α-adrenergic receptors in the vasculature can impair glucose uptake in skeletal muscle via an effect on glucose delivery. While the sympathetic nervous innervation of blood vessels supplying skeletal muscle is well recognized [222], recent studies have also demonstrated a clear role for sympathetic nerves at the neuromuscular junction [223], with sympathetic activity playing an important role in maintaining skeletal muscle structure and function [224]. In a mouse model of heart failure sympathetic activation was demonstrated to contribute to the morphological alterations in skeletal muscle myopathy [225]. In patients with heart failure and sarcopenia, MSNA was elevated, compared to patients without sarcopenia, and was negatively correlated with appendicular lean muscle mass [226]. With ageing, a selective loss of sympathetic axons projecting to myofibers and the neuromuscular junction occurs, resulting in a degree of muscle denervation [223,227]. While increased MSNA occurs with healthy ageing (for review see [228]) the elevated cardiac noradrenaline spillover to plasma that occurs in parallel is accompanied by a reduction in noradrenaline uptake [229], beta-adrenergic responsiveness [230] and nerve growth factor expression [231] which, taken together, is consistent with a catecholamine-induced reduction in nerve density.
5.4. Kidney
The global increase in prevalence of obesity has seen a parallel rise in incidence of chronic kidney disease [232,233]. Importantly, damage to the kidney, as indicated from the urinary albumin:creatine ratio, is an independent predictor of mortality risk in the general population [234]. Although the impact of obesity on chronic kidney disease may be influenced and accentuated by comorbidities such as diabetes and hypertension, excess weight and visceral fat are crucial in disease development [235]. Recent data derived from the National Health and Nutrition Examination Survey has demonstrated a substantial rise in the prevalence of obesity-related hypertension over the past two decades [236]. Increased renal sympathetic activity is evident in obesity, with elevated noradrenaline spillover into the renal veins evident in both normotensive and hypertensive obese individuals [200]. At a young age, alterations in kidney function are evident with weight gain. Overweight or obese young adults present with elevated creatinine clearance compared with their lean counterparts, with the increment in creatinine clearance being directly and positively correlated with MSNA [237]. Indeed, sympathetic activation to the kidney may contribute to the development of renal diseases by causing glomerular hyperfiltration and injury to the glomerular and proximal tubules [238]. Additionally, obesity-induced compression of the kidney may lead to increased sodium reabsorption and contribute to renal vasodilation, glomerular hyperfiltration, and increased renin secretion in obese subjects [235]. While the management of cardiovascular and kidney complications associated with weight gain includes diet and exercise, cessation of tobacco smoking, glycemic and dyslipidemia control and lowering blood pressure, additionally, there are four pharmacological pillars of therapy. These include targeting the renin-angiotensin-aldosterone system, SGLT-2 inhibition, blockade of the mineralocorticoid receptor and GLP-1 agonists [239]. Whether the therapeutic benefit of these agents rests solely with their direct pharmacological action or via a secondary beneficial effect on modulating sympathetic tone is not known.
5.5. Heart and Vascular Function
Longitudinal data from the Framingham Heart Study indicated that each 1 kg/m2 increase in BMI over 14 years was associated with a 5-7% increase in risk of heart failure [240]. Importantly, weight-related changes in left ventricular structure and function are evident even in young and middle-aged individuals prior to the onset of clinical signs of disease [237,241]. Indicative of a role of the sympathetic nervous system in the development of cardiac hypertrophy, alterations in left ventricular structure and function have been shown to correlate with MSNA in young overweight subjects [237] and to cardiac noradrenaline spillover in patients with hypertension [242]. Obesity-related activation of the renin-angiotensin system may also play a role in cardiac remodeling. The release of angiotensin II, combined with the parallel increase in sympathetic nervous activity, may lead to vasoconstriction, fluid retention, and increased left ventricular pre- and afterload [243]. The observations of Burns and colleagues [244], who showed that combined treatment targeting the sympathetic and renin-angiotensin-aldosterone system provided a greater reduction in left ventricular mass compared with a thiazide diuretic and calcium channel blocker, despite equal blood pressure reduction, provided further support for engagement of the sympathetic nervous and renin-angiotensin-aldosterone systems in generating left ventricular hypertrophy.
Vascular aging is an important determinant of cardiovascular morbidity and mortality and can be examined using a raft of techniques including measurement of endothelial dysfunction, arterial stiffness and carotid intima-media thickness [245]. Endothelial dysfunction has been shown to precede the development of atherosclerosis and is one of the early factors in the cascade of cardiovascular disease development. Similarly, large artery stiffness is an independent predictor of all-cause and cardiovascular mortality [246]. Although these techniques are widely used to assess “vascular ageing” in general, the measures likely reflect differing underlying physiology [247]. Previous studies have demonstrated an association between MSNA and endothelial dysfunction in lean [248] and overweight or obese adults [237], with only modest gains in visceral fat mass being shown to be linked with endothelial dysfunction [249]. In line with this, recent analysis of data derived from the UK Biobank and Fuqing Cohort indicated an association of arterial stiffness with central obesity but not BMI [250]. Oren and colleagues examined aortic stiffness using pulse wave velocity and carotid intima-media thickness and found an association between BMI and carotid intima-media thickness but not BMI and pulse wave velocity, which was related to male sex and blood pressure [247]. The habitual consumption of a diet high in saturated fat in relation to poly-unsaturated and mono-unsaturated fat was strongly associated with impaired endothelial function in young overweight adults [251].
A large body of literature has contributed to our understanding of the mechanisms of vascular ageing and how perturbations initiate the development and worsening prognosis of cardiovascular disease [252,253]. Mechanisms involved include increased adipokine-induced inflammation, hyperinsulinemia, reciprocal changes in low- and high-density lipoproteins, and activation of the renin-angiotensin-aldosterone systems. While an association between MSNA and endothelial function in young overweight individuals has been described [237,248] and MSNA has been shown to be associated with increased pulse wave velocity in both peripheral and central vessels [254], whether activation of the sympathetic nervous system contributes to vascular ageing independent of changes in blood pressure or lipids remains to be determined.
6. Conclusions
A large body of evidence has demonstrated the importance of the sympathetic nervous system in weight regulation and in the cardiometabolic consequences associated with changes in body weight and body composition. Preclinical studies and the advancement and application of brain mapping techniques in humans have contributed to our understanding of the brain regulatory pathways involved in the regionalization of sympathetic outflow. Recent developments in therapies for weight gain and weight loss have benefited from these findings, with approaches developed to target the pathways and physiology to improve clinical outcomes.
Author Contributions
Conceptualization, G.W.L.; resources, G.W.L. and E.A.L.; writing—original draft preparation, G.W.L. M.P. and E.A.L.; writing—review and editing, G.W.L., M.P. and E.A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The authors are supported through funding from Swinburne Research at Swinburne University of Technology and the National Health and Research Council of Australia
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Brown, C.D.; Higgins, M.; Donato, K.A.; Rohde, F.C.; Garrison, R.; Obarzanek, E.; Ernst, N.D.; Horan, M. Body mass index and the prevalence of hypertension and dyslipidemia. Obes Res 2000, 8, 605–619. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.M.; Rimm, E.B.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care 1994, 17, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Despres, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed]
- Rubino, F.; Cummings, D.E.; Eckel, R.H.; Cohen, R.V.; Wilding, J.P.H.; Brown, W.A.; Stanford, F.C.; Batterham, R.L.; Farooqi, I.S.; Farpour-Lambert, N.J.; et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol 2025, 13, 221–262. [Google Scholar] [CrossRef]
- Folsom, A.R.; Kaye, S.A.; Sellers, T.A.; Hong, C.P.; Cerhan, J.R.; Potter, J.D.; Prineas, R.J. Body fat distribution and 5-year risk of death in older women. JAMA 1993, 269, 483–487. [Google Scholar] [CrossRef]
- Kwon, H.; Yun, J.M.; Park, J.H.; Cho, B.L.; Han, K.; Joh, H.K.; Son, K.Y.; Cho, S.H. Incidence of cardiovascular disease and mortality in underweight individuals. J Cachexia Sarcopenia Muscle 2021, 12, 331–338. [Google Scholar] [CrossRef]
- Park, D.; Lee, J.H.; Han, S. Underweight: another risk factor for cardiovascular disease?: A cross-sectional 2013 Behavioral Risk Factor Surveillance System (BRFSS) study of 491,773 individuals in the USA. Medicine (Baltimore) 2017, 96, e8769. [Google Scholar] [CrossRef]
- von Euler, U.S. A specific sympathetic ergone in adrenergic nerve fibres (sympathin) and its relation to adrenaline and noradrenaline. Acta Physiol Scand 1946, 12, 73–97. [Google Scholar] [CrossRef]
- Brown, G.L.; Gillespie, J.S. The output of sympathetic transmitter from the spleen of the cat. J Physiol 1957, 138, 81–102. [Google Scholar] [CrossRef]
- Von Euler, U.S.; Hellner, S.; Purkhold, A. Excretion of noradrenaline in urine in hypertension. Scand J Clin Lab Invest 1954, 6, 54–59. [Google Scholar] [CrossRef]
- Kramer, R.S.; Mason, D.T.; Braunwald, E. Augmented sympathetic neurotransmitter activity in the peripheral vascular bed of patients with congestive heart failure and cardiac norepinephrine depletion. Circulation 1968, 38, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Engelman, K.; Portnoy, B.; Lovenberg, W. A sensitive and specific double-isotope derivative method for the determination of catecholamines in biological specimens. Am J Med Sci 1968, 255, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Zweifler, A.J.; Julius, S. Increased platelet catecholamine content in pheochromocytoma: a diagnostic test in patients with elevated plasma catecholamines. N Engl J Med 1982, 306, 890–894. [Google Scholar] [CrossRef] [PubMed]
- Hagbarth, K.E.; Vallbo, A.B. Mechanoreceptor activity recorded percutaneously with semi-microelectrodes in human peripheral nerves. Acta Physiol Scand 1967, 69, 121–122. [Google Scholar] [CrossRef]
- Esler, M.; Jackman, G.; Bobik, A.; Kelleher, D.; Jennings, G.; Leonard, P.; Skews, H.; Korner, P. Determination of norepinephrine apparent release rate and clearance in humans. Life Sci 1979, 25, 1461–1470. [Google Scholar] [CrossRef]
- Gronlund, B.; Astrup, A.; Bie, P.; Christensen, N.J. Noradrenaline release in skeletal muscle and in adipose tissue studied by microdialysis. Clin Sci (Lond) 1991, 80, 595–598. [Google Scholar] [CrossRef]
- Wieland, D.M.; Brown, L.E.; Rogers, W.L.; Worthington, K.C.; Wu, J.L.; Clinthorne, N.H.; Otto, C.A.; Swanson, D.P.; Beierwaltes, W.H. Myocardial imaging with a radioiodinated norepinephrine storage analog. J Nucl Med 1981, 22, 22–31. [Google Scholar]
- DeQuattro, V.; Miura, Y.; Lurvey, A.; Cosgrove, M.; Mendez, R. Increased plasma catecholamine concentrations and vas deferens norepinephrine biosynthesis in men with elevated blood pressure. Circ Res 1975, 36, 118–126. [Google Scholar] [CrossRef]
- Guenter, J.; Lenartowski, R. Molecular characteristic and physiological role of DOPA-decarboxylase. Postepy Hig Med Dosw (Online) 2016, 70, 1424–1440. [Google Scholar] [CrossRef]
- Guidry, G. A method for counterstaining tissues in conjunction with the glyoxylic acid condensation reaction for detection of biogenic amines. J Histochem Cytochem 1999, 47, 261–264. [Google Scholar] [CrossRef]
- Morris, M.J.; Cox, H.S.; Lambert, G.W.; Kaye, D.M.; Jennings, G.L.; Meredith, I.T.; Esler, M.D. Region-specific neuropeptide Y overflows at rest and during sympathetic activation in humans. Hypertension 1997, 29, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Vaingankar, S.M.; Li, Y.; Biswas, N.; Gayen, J.; Choksi, S.; Rao, F.; Ziegler, M.G.; Mahata, S.K.; O'Connor, D.T. Effects of chromogranin A deficiency and excess in vivo: biphasic blood pressure and catecholamine responses. J Hypertens 2010, 28, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Esler, M.; Jennings, G.; Lambert, G.; Meredith, I.; Horne, M.; Eisenhofer, G. Overflow of catecholamine neurotransmitters to the circulation: source, fate, and functions. Physiol Rev 1990, 70, 963–985. [Google Scholar] [CrossRef] [PubMed]
- Meredith, I.T.; Eisenhofer, G.; Lambert, G.W.; Jennings, G.L.; Thompson, J.; Esler, M.D. Plasma norepinephrine responses to head-up tilt are misleading in autonomic failure. Hypertension 1992, 19, 628–633. [Google Scholar] [CrossRef]
- Pacholczyk, T.; Blakely, R.D.; Amara, S.G. Expression cloning of a cocaine- and antidepressant-sensitive human noradrenaline transporter. Nature 1991, 350, 350–354. [Google Scholar] [CrossRef]
- Esler, M.; Alvarenga, M.; Pier, C.; Richards, J.; El-Osta, A.; Barton, D.; Haikerwal, D.; Kaye, D.; Schlaich, M.; Guo, L.; et al. The neuronal noradrenaline transporter, anxiety and cardiovascular disease. J Psychopharmacol 2006, 20, 60–66. [Google Scholar] [CrossRef]
- Esler, M.D.; Wallin, G.; Dorward, P.K.; Eisenhofer, G.; Westerman, R.; Meredith, I.; Lambert, G.; Cox, H.S.; Jennings, G. Effects of desipramine on sympathetic nerve firing and norepinephrine spillover to plasma in humans. Am J Physiol 1991, 260, R817–R823. [Google Scholar] [CrossRef]
- Shannon, J.R.; Flattem, N.L.; Jordan, J.; Jacob, G.; Black, B.K.; Biaggioni, I.; Blakely, R.D.; Robertson, D. Orthostatic intolerance and tachycardia associated with norepinephrine-transporter deficiency. N Engl J Med 2000, 342, 541–549. [Google Scholar] [CrossRef]
- Lambert, E.; Eikelis, N.; Esler, M.; Dawood, T.; Schlaich, M.; Bayles, R.; Socratous, F.; Agrotis, A.; Jennings, G.; Lambert, G.; et al. Altered sympathetic nervous reactivity and norepinephrine transporter expression in patients with postural tachycardia syndrome. Circ Arrhythm Electrophysiol 2008, 1, 103–109. [Google Scholar] [CrossRef]
- Mandela, P.; Ordway, G.A. The norepinephrine transporter and its regulation. J Neurochem 2006, 97, 310–333. [Google Scholar] [CrossRef]
- Marques, F.Z.; Eikelis, N.; Bayles, R.G.; Lambert, E.A.; Straznicky, N.E.; Hering, D.; Esler, M.D.; Head, G.A.; Barton, D.A.; Schlaich, M.P.; et al. A polymorphism in the norepinephrine transporter gene is associated with affective and cardiovascular disease through a microRNA mechanism. Mol Psychiatry 2017, 22, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Harikrishnan, K.N.; Bayles, R.; Ciccotosto, G.D.; Maxwell, S.; Cappai, R.; Pelka, G.J.; Tam, P.P.; Christodoulou, J.; El-Osta, A. Alleviating transcriptional inhibition of the norepinephrine slc6a2 transporter gene in depolarized neurons. J Neurosci 2010, 30, 1494–1501. [Google Scholar] [CrossRef] [PubMed]
- Eisenhofer, G.; Esler, M.D.; Meredith, I.T.; Dart, A.; Cannon, R.O., 3rd; Quyyumi, A.A.; Lambert, G.; Chin, J.; Jennings, G.L.; Goldstein, D.S. Sympathetic nervous function in human heart as assessed by cardiac spillovers of dihydroxyphenylglycol and norepinephrine. Circulation 1992, 85, 1775–1785. [Google Scholar] [CrossRef] [PubMed]
- Seals, D.R.; Bell, C. Chronic sympathetic activation: consequence and cause of age-associated obesity? Diabetes 2004, 53, 276–284. [Google Scholar] [CrossRef]
- Limberg, J.K.; Malterer, K.R.; Matzek, L.J.; Levine, J.A.; Charkoudian, N.; Miles, J.M.; Joyner, M.J.; Curry, T.B. Resting sympathetic activity is associated with the sympathetically mediated component of energy expenditure following a meal. Physiol Rep 2017, 5. [Google Scholar] [CrossRef]
- Weyer, C.; Pratley, R.E.; Snitker, S.; Spraul, M.; Ravussin, E.; Tataranni, P.A. Ethnic differences in insulinemia and sympathetic tone as links between obesity and blood pressure. Hypertension 2000, 36, 531–537. [Google Scholar] [CrossRef]
- Lambert, E.; Straznicky, N.; Eikelis, N.; Esler, M.; Dawood, T.; Masuo, K.; Schlaich, M.; Lambert, G. Gender differences in sympathetic nervous activity: influence of body mass and blood pressure. J Hypertens 2007, 25, 1411–1419. [Google Scholar] [CrossRef]
- Tank, J.; Heusser, K.; Diedrich, A.; Hering, D.; Luft, F.C.; Busjahn, A.; Narkiewicz, K.; Jordan, J. Influences of gender on the interaction between sympathetic nerve traffic and central adiposity. J Clin Endocrinol Metab 2008, 93, 4974–4978. [Google Scholar] [CrossRef]
- Esler, M.; Jennings, G.; Korner, P.; Willett, I.; Dudley, F.; Hasking, G.; Anderson, W.; Lambert, G. Assessment of human sympathetic nervous system activity from measurements of norepinephrine turnover. Hypertension 1988, 11, 3–20. [Google Scholar] [CrossRef]
- D'Souza, A.W.; Moore, J.P.; Manabe, K.; Lawley, J.S.; Washio, T.; Hissen, S.L.; Sanchez, B.; Fu, Q. The interactive effects of posture and biological sex on the control of muscle sympathetic nerve activity during rhythmic handgrip exercise. Am J Physiol Regul Integr Comp Physiol 2024, 327, R133–R144. [Google Scholar] [CrossRef]
- Rundqvist, B.; Elam, M.; Bergmann-Sverrisdottir, Y.; Eisenhofer, G.; Friberg, P. Increased cardiac adrenergic drive precedes generalized sympathetic activation in human heart failure. Circulation 1997, 95, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Lambert, G.W.; Kaye, D.M.; Lefkovits, J.; Jennings, G.L.; Turner, A.G.; Cox, H.S.; Esler, M.D. Increased central nervous system monoamine neurotransmitter turnover and its association with sympathetic nervous activity in treated heart failure patients. Circulation 1995, 92, 1813–1818. [Google Scholar] [CrossRef] [PubMed]
- Esler, M.; Jennings, G.; Lambert, G. Measurement of overall and cardiac norepinephrine release into plasma during cognitive challenge. Psychoneuroendocrinology 1989, 14, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.R.; Ray, C.A. Sympathetic neural responses to mental stress: responders, nonresponders and sex differences. Am J Physiol Heart Circ Physiol 2009, 296, H847–H853. [Google Scholar] [CrossRef]
- Vollenweider, P.; Tappy, L.; Randin, D.; Schneiter, P.; Jequier, E.; Nicod, P.; Scherrer, U. Differential effects of hyperinsulinemia and carbohydrate metabolism on sympathetic nerve activity and muscle blood flow in humans. J Clin Invest 1993, 92, 147–154. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Lambert, E.A.; Grima, M.T.; Eikelis, N.; Richards, K.; Nestel, P.J.; Dawood, T.; Masuo, K.; Sari, C.I.; Dixon, J.B.; et al. The effects of dietary weight loss on indices of norepinephrine turnover: modulatory influence of hyperinsulinemia. Obesity 2014, 22, 652–662. [Google Scholar] [CrossRef]
- Prior, L.J.; Eikelis, N.; Armitage, J.A.; Davern, P.J.; Burke, S.L.; Montani, J.P.; Barzel, B.; Head, G.A. Exposure to a high-fat diet alters leptin sensitivity and elevates renal sympathetic nerve activity and arterial pressure in rabbits. Hypertension 2010, 55, 862–868. [Google Scholar] [CrossRef]
- Gentile, C.L.; Orr, J.S.; Davy, B.M.; Davy, K.P. Modest weight gain is associated with sympathetic neural activation in nonobese humans. Am J Physiol Regul Integr Comp Physiol 2007, 292, R1834–R1838. [Google Scholar] [CrossRef]
- Hissen, S.L.; Takeda, R.; Badrov, M.B.; Arias-Franklin, S.; Patel, S.; Nelson, D.B.; Babb, T.G.; Fu, Q. Impact of maternal obesity on resting muscle sympathetic nerve activity during uncomplicated pregnancy: a longitudinal assessment. Am J Physiol Regul Integr Comp Physiol 2024, 326, R10–R18. [Google Scholar] [CrossRef]
- Grassi, G.; Biffi, A.; Seravalle, G.; Trevano, F.Q.; Dell'Oro, R.; Corrao, G.; Mancia, G. Sympathetic neural overdrive in the obese and overweight state. Hypertension 2019, 74, 349–358. [Google Scholar] [CrossRef]
- Quarti Trevano, F.; Dell'Oro, R.; Biffi, A.; Seravalle, G.; Corrao, G.; Mancia, G.; Grassi, G. Sympathetic overdrive in the metabolic syndrome: meta-analysis of published studies. J Hypertens 2020, 38, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Vaz, M.; Jennings, G.; Turner, A.; Cox, H.; Lambert, G.; Esler, M. Regional sympathetic nervous activity and oxygen consumption in obese normotensive human subjects. Circulation 1997, 96, 3423–3429. [Google Scholar] [CrossRef] [PubMed]
- Lambert, E.; Straznicky, N.; Schlaich, M.; Esler, M.; Dawood, T.; Hotchkin, E.; Lambert, G. Differing pattern of sympathoexcitation in normal-weight and obesity-related hypertension. Hypertension 2007, 50, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Lambert, G.W.; Vaz, M.; Cox, H.S.; Turner, A.G.; Kaye, D.M.; Jennings, G.L.; Esler, M.D. Human obesity is associated with a chronic elevation in brain 5- hydroxytryptamine turnover. Clin Sci (Colch) 1999, 96, 191–197. [Google Scholar] [CrossRef]
- Ferrier, C.; Jennings, G.L.; Eisenhofer, G.; Lambert, G.; Cox, H.S.; Kalff, V.; Kelly, M.; Esler, M.D. Evidence for increased noradrenaline release from subcortical brain regions in essential hypertension. J Hypertens 1993, 11, 1217–1227. [Google Scholar] [CrossRef]
- Lambert, E.; Straznicky, N.; Sari, C.I.; Eikelis, N.; Hering, D.; Head, G.; Dixon, J.; Esler, M.; Schlaich, M.; Lambert, G. Dyslipidemia is associated with sympathetic nervous activation and impaired endothelial function in young females. Am J Hypertens 2013, 26, 250–256. [Google Scholar] [CrossRef]
- Eikelis, N.; Lambert, E.A.; Phillips, S.; Sari, C.I.; Mundra, P.A.; Weir, J.M.; Huynh, K.; Grima, M.T.; Straznicky, N.E.; Dixon, J.B.; et al. Muscle sympathetic nerve activity Is associated with elements of the plasma lipidomic profile in young Asian adults. J Clin Endocrinol Metab 2017, 102, 2059–2068. [Google Scholar] [CrossRef]
- Sverrisdottir, Y.B.; Mogren, T.; Kataoka, J.; Janson, P.O.; Stener-Victorin, E. Is polycystic ovary syndrome associated with high sympathetic nerve activity and size at birth? Am J Physiol Endocrinol Metab 2008, 294, E576–E581. [Google Scholar] [CrossRef]
- Lambert, E.A.; Teede, H.; Sari, C.I.; Jona, E.; Shorakae, S.; Woodington, K.; Hemmes, R.; Eikelis, N.; Straznicky, N.E.; De Courten, B.; et al. Sympathetic activation and endothelial dysfunction in polycystic ovary syndrome are not explained by either obesity or insulin resistance. Clinical endocrinology 2015, 83, 812–819. [Google Scholar] [CrossRef]
- Shorakae, S.; Jona, E.; de Courten, B.; Lambert, G.W.; Lambert, E.A.; Phillips, S.E.; Clarke, I.J.; Teede, H.J.; Henry, B.A. Brown adipose tissue thermogenesis in polycystic ovary syndrome. Clinical endocrinology 2019, 90, 425–432. [Google Scholar] [CrossRef]
- Shorakae, S.; Lambert, E.A.; Jona, E.; Ika Sari, C.; de Courten, B.; Dixon, J.B.; Lambert, G.W.; Teede, H.J. Effect of central sympathoinhibition with moxonidine on sympathetic nervous activity in polycystic ovary syndrome-A randomized controlled trial. Front Physiol 2018, 9, 1486. [Google Scholar] [CrossRef] [PubMed]
- Lansdown, A.J.; Warnert, E.A.H.; Sverrisdottir, Y.; Wise, R.G.; Rees, D.A. Regional cerebral activation accompanies sympathoexcitation in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2019, 104, 3614–3623. [Google Scholar] [CrossRef] [PubMed]
- Ayer, J.; Charakida, M.; Deanfield, J.E.; Celermajer, D.S. Lifetime risk: childhood obesity and cardiovascular risk. Eur Heart J 2015, 36, 1371–1376. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.R., Jr.; Woo, J.G.; Sinaiko, A.R.; Daniels, S.R.; Ikonen, J.; Juonala, M.; Kartiosuo, N.; Lehtimaki, T.; Magnussen, C.G.; Viikari, J.S.A.; et al. Childhood cardiovascular risk Factors and adult cardiovascular events. N Engl J Med 2022, 386, 1877–1888. [Google Scholar] [CrossRef]
- Goodman, E.; Dolan, L.M.; Morrison, J.A.; Daniels, S.R. Factor analysis of clustered cardiovascular risks in adolescence: obesity is the predominant correlate of risk among youth. Circulation 2005, 111, 1970–1977. [Google Scholar] [CrossRef]
- Esler, M.; Lambert, G.; Esler, D.; Ika Sari, C.; Guo, L.; Jennings, G. Evaluation of elevated heart rate as a sympathetic nervous system biomarker in essential hypertension. J Hypertens 2020, 38, 1488–1495. [Google Scholar] [CrossRef]
- Grassi, G.; Seravalle, G.; Vanoli, J.; Facchetti, R.; Spaziani, D.; Mancia, G. Relationships between sympathetic markers and heart rate thresholds for cardiovascular risk in chronic heart failure. Clin Res Cardiol 2023, 112, 59–67. [Google Scholar] [CrossRef]
- Aune, D.; Sen, A.; o'Hartaigh, B.; Janszky, I.; Romundstad, P.R.; Tonstad, S.; Vatten, L.J. Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality - A systematic review and dose-response meta-analysis of prospective studies. Nutr Metab Cardiovasc Dis 2017, 27, 504–517. [Google Scholar] [CrossRef]
- Freitas Junior, I.F.; Monteiro, P.A.; Silveira, L.S.; Cayres, S.U.; Antunes, B.M.; Bastos, K.N.; Codogno, J.S.; Sabino, J.P.; Fernandes, R.A. Resting heart rate as a predictor of metabolic dysfunctions in obese children and adolescents. BMC Pediatr 2012, 12, 5. [Google Scholar] [CrossRef]
- Kwok, S.Y.; So, H.K.; Choi, K.C.; Lo, A.F.; Li, A.M.; Sung, R.Y.; Nelson, E.A. Resting heart rate in children and adolescents: association with blood pressure, exercise and obesity. Arch Dis Child 2013, 98, 287–291. [Google Scholar] [CrossRef]
- Rossi, R.C.; Vanderlei, L.C.; Goncalves, A.C.; Vanderlei, F.M.; Bernardo, A.F.; Yamada, K.M.; da Silva, N.T.; de Abreu, L.C. Impact of obesity on autonomic modulation, heart rate and blood pressure in obese young people. Auton Neurosci 2015, 193, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Al-Rashed, F.; Sindhu, S.; Al Madhoun, A.; Ahmad, Z.; AlMekhled, D.; Azim, R.; Al-Kandari, S.; Wahid, M.A.; Al-Mulla, F.; Ahmad, R. Elevated resting heart rate as a predictor of inflammation and cardiovascular risk in healthy obese individuals. Sci Rep 2021, 11, 13883. [Google Scholar] [CrossRef] [PubMed]
- Narkiewicz, K.; Somers, V.K. Sympathetic nerve activity in obstructive sleep apnoea. Acta Physiol Scand 2003, 177, 385–390. [Google Scholar] [CrossRef] [PubMed]
- O'Driscoll, D.M.; Horne, R.S.; Davey, M.J.; Hope, S.A.; Anderson, V.; Trinder, J.; Walker, A.M.; Nixon, G.M. Increased sympathetic activity in children with obstructive sleep apnea: cardiovascular implications. Sleep Med 2011, 12, 483–488. [Google Scholar] [CrossRef]
- Cheng, E.T.W.; Chan, R.N.C.; Chan, K.C.C.; Au, C.T.; Li, A.M. Level of urinary catecholamine in children with sleep disordered breathing: A systematic review and meta-analysis. Sleep Med 2022, 100, 565–572. [Google Scholar] [CrossRef]
- Ji, J.; Wang, Y.; Chen, B.; Xu, X.; Lv, M. Is there an association between cognitive impairment and urinary adrenaline, norepinephrine, gamma-aminobutyric acid, and taurine levels in children with obstructive sleep apnea?: A case control study. BMC Pediatr 2025, 25, 156. [Google Scholar] [CrossRef]
- Barker, D.J. The developmental origins of adult disease. J Am Coll Nutr 2004, 23, 588S–595S. [Google Scholar] [CrossRef]
- Huxley, R.R.; Shiell, A.W.; Law, C.M. The role of size at birth and postnatal catch-up growth in determining systolic blood pressure: a systematic review of the literature. J Hypertens 2000, 18, 815–831. [Google Scholar] [CrossRef]
- Bhargava, S.K.; Sachdev, H.S.; Fall, C.H.; Osmond, C.; Lakshmy, R.; Barker, D.J.; Biswas, S.K.; Ramji, S.; Prabhakaran, D.; Reddy, K.S. Relation of serial changes in childhood body-mass index to impaired glucose tolerance in young adulthood. N Engl J Med 2004, 350, 865–875. [Google Scholar] [CrossRef]
- Mzayek, F.; Cruickshank, J.K.; Amoah, D.; Srinivasan, S.; Chen, W.; Berenson, G.S. Birth weight was longitudinally associated with cardiometabolic risk markers in mid-adulthood. Ann Epidemiol 2016, 26, 643–647. [Google Scholar] [CrossRef]
- Ijzerman, R.G.; Stehouwer, C.D.; de Geus, E.J.; van Weissenbruch, M.M.; Delemarre-van de Waal, H.A.; Boomsma, D.I. Low birth weight is associated with increased sympathetic activity: dependence on genetic factors. Circulation 2003, 108, 566–571. [Google Scholar] [CrossRef]
- Weitz, G.; Deckert, P.; Heindl, S.; Struck, J.; Perras, B.; Dodt, C. Evidence for lower sympathetic nerve activity in young adults with low birth weight. J Hypertens 2003, 21, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Jansson, T.; Lambert, G.W. Effect of intrauterine growth restriction on blood pressure, glucose tolerance and sympathetic nervous system activity in the rat at 3-4 months of age. J Hypertens 1999, 17, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Denton, K.M.; Flower, R.L.; Stevenson, K.M.; Anderson, W.P. Adult rabbit offspring of mothers with secondary hypertension have increased blood pressure. Hypertension 2003, 41, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Nicklas, J.M.; Huskey, K.W.; Davis, R.B.; Wee, C.C. Successful weight loss among obese U.S. adults. Am J Prev Med 2012, 42, 481–485. [Google Scholar] [CrossRef]
- Grassi, G.; Seravalle, G.; Colombo, M.; Bolla, G.; Cattaneo, B.M.; Cavagnini, F.; Mancia, G. Body weight reduction, sympathetic nerve traffic, and arterial baroreflex in obese normotensive humans. Circulation 1998, 97, 2037–2042. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Lambert, E.A.; Lambert, G.W.; Masuo, K.; Esler, M.D.; Nestel, P.J. Effects of dietary weight loss on sympathetic activity and cardiac risk factors associated with the metabolic syndrome. J Clin Endocrinol Metab 2005, 90, 5998–6005. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Lambert, E.A.; Nestel, P.J.; McGrane, M.T.; Dawood, T.; Schlaich, M.P.; Masuo, K.; Eikelis, N.; de Courten, B.; Mariani, J.A.; et al. Sympathetic neural adaptation to hypocaloric diet with or without exercise training in obese metabolic syndrome subjects. Diabetes 2010, 59, 71–79. [Google Scholar] [CrossRef]
- Meredith, I.T.; Friberg, P.; Jennings, G.L.; Dewar, E.M.; Fazio, V.A.; Lambert, G.W.; Esler, M.D. Exercise training lowers resting renal but not cardiac sympathetic activity in humans. Hypertension 1991, 18, 575–582. [Google Scholar] [CrossRef]
- Bellicha, A.; van Baak, M.A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; Carraca, E.V.; Dicker, D.; Encantado, J.; Ermolao, A.; et al. Effect of exercise training on weight loss, body composition changes, and weight maintenance in adults with overweight or obesity: An overview of 12 systematic reviews and 149 studies. Obes Rev 2021, 22 Suppl 4, e13256. [Google Scholar] [CrossRef]
- Jayedi, A.; Soltani, S.; Emadi, A.; Zargar, M.S.; Najafi, A. Aerobic exercise and weight loss in adults: A systematic review and dose-response meta-analysis. JAMA Netw Open 2024, 7, e2452185. [Google Scholar] [CrossRef] [PubMed]
- Straznicky, N.E.; Eikelis, N.; Nestel, P.J.; Dixon, J.B.; Dawood, T.; Grima, M.T.; Sari, C.I.; Schlaich, M.P.; Esler, M.D.; Tilbrook, A.J.; et al. Baseline sympathetic nervous system activity predicts dietary weight loss in obese metabolic syndrome subjects. J Clin Endocrinol Metab 2012, 97, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.B.; Straznicky, N.E.; Lambert, E.A.; Schlaich, M.P.; Lambert, G.W. Surgical approaches to the treatment of obesity. Nat Rev Gastroenterol Hepatol 2011, 8, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Sjostrom, L.; Narbro, K.; Sjostrom, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 2007, 357, 741–752. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Youdim, A.; Jones, D.B.; Garvey, W.T.; Hurley, D.L.; McMahon, M.M.; Heinberg, L.J.; Kushner, R.; Adams, T.D.; Shikora, S.; et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient--2013 update: cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery. Obesity 2013, 21 Suppl 1, S1–27. [Google Scholar] [CrossRef]
- Lambert, E.A.; Rice, T.; Eikelis, N.; Straznicky, N.E.; Lambert, G.W.; Head, G.A.; Hensman, C.; Schlaich, M.P.; Dixon, J.B. Sympathetic activity and markers of cardiovascular risk in nondiabetic severely obese patients: the effect of the initial 10% weight loss. Am J Hypertens 2014, 27, 1308–1315. [Google Scholar] [CrossRef]
- Seravalle, G.; Colombo, M.; Perego, P.; Giardini, V.; Volpe, M.; Dell'Oro, R.; Mancia, G.; Grassi, G. Long-term sympathoinhibitory effects of surgically induced weight loss in severe obese patients. Hypertension 2014, 64, 431–437. [Google Scholar] [CrossRef]
- Jenkins, Z.M.; Castle, D.J.; Eikelis, N.; Phillipou, A.; Lambert, G.W.; Lambert, E.A. Autonomic nervous system function in women with anorexia nervosa. Clin Auton Res 2022, 32, 29–42. [Google Scholar] [CrossRef]
- Gross, H.A.; Lake, C.R.; Ebert, M.H.; Ziegler, M.G.; Kopin, I.J. Catecholamine metabolism in primary anorexia nervosa. J Clin Endocrinol Metab 1979, 49, 805–809. [Google Scholar] [CrossRef]
- Sachs, K.V.; Harnke, B.; Mehler, P.S.; Krantz, M.J. Cardiovascular complications of anorexia nervosa: A systematic review. Int J Eat Disord 2016, 49, 238–248. [Google Scholar] [CrossRef]
- Zamboni, M.; Armellini, F.; Turcato, E.; Todisco, P.; Gallagher, D.; Dalle Grave, R.; Heymsfield, S.; Bosello, O. Body fat distribution before and after weight gain in anorexia nervosa. Int J Obes Relat Metab Disord 1997, 21, 33–36. [Google Scholar] [CrossRef] [PubMed]
- El Ghoch, M.; Calugi, S.; Lamburghini, S.; Dalle Grave, R. Anorexia nervosa and body fat distribution: a systematic review. Nutrients 2014, 6, 3895–3912. [Google Scholar] [CrossRef] [PubMed]
- Mayer, L.; Walsh, B.T.; Pierson, R.N., Jr.; Heymsfield, S.B.; Gallagher, D.; Wang, J.; Parides, M.K.; Leibel, R.L.; Warren, M.P.; Killory, E.; et al. Body fat redistribution after weight gain in women with anorexia nervosa. Am J Clin Nutr 2005, 81, 1286–1291. [Google Scholar] [CrossRef] [PubMed]
- Hebebrand, J.; Muller, T.D.; Holtkamp, K.; Herpertz-Dahlmann, B. The role of leptin in anorexia nervosa: clinical implications. Mol Psychiatry 2007, 12, 23–35. [Google Scholar] [CrossRef]
- Prioletta, A.; Muscogiuri, G.; Sorice, G.P.; Lassandro, A.P.; Mezza, T.; Policola, C.; Salomone, E.; Cipolla, C.; Della Casa, S.; Pontecorvi, A.; et al. In anorexia nervosa, even a small increase in abdominal fat is responsible for the appearance of insulin resistance. Clinical endocrinology 2011, 75, 202–206. [Google Scholar] [CrossRef]
- Diba, P.; Sattler, A.L.; Korzun, T.; Habecker, B.A.; Marks, D.L. Unraveling the lost balance: Adrenergic dysfunction in cancer cachexia. Auton Neurosci 2024, 251, 103136. [Google Scholar] [CrossRef]
- Petruzzelli, M.; Schweiger, M.; Schreiber, R.; Campos-Olivas, R.; Tsoli, M.; Allen, J.; Swarbrick, M.; Rose-John, S.; Rincon, M.; Robertson, G.; et al. A switch from white to brown fat increases energy expenditure in cancer-associated cachexia. Cell Metab 2014, 20, 433–447. [Google Scholar] [CrossRef]
- Xie, H.; Heier, C.; Meng, X.; Bakiri, L.; Pototschnig, I.; Tang, Z.; Schauer, S.; Baumgartner, V.J.; Grabner, G.F.; Schabbauer, G.; et al. An immune-sympathetic neuron communication axis guides adipose tissue browning in cancer-associated cachexia. Proc Natl Acad Sci U S A 2022, 119. [Google Scholar] [CrossRef]
- Laird, B.J.A.; Skipworth, R.; Bonomi, P.D.; Fallon, M.; Kaasa, S.; Giorgino, R.; McMillan, D.C.; Currow, D.C. Anamorelin efficacy in non-small-cell lung cancer patients with cachexia: InsightsfFrom ROMANA 1 and ROMANA 2. J Cachexia Sarcopenia Muscle 2025, 16, e13732. [Google Scholar] [CrossRef]
- Kaye, D.M.; Lefkovits, J.; Jennings, G.L.; Bergin, P.; Broughton, A.; Esler, M.D. Adverse consequences of high sympathetic nervous activity in the failing human heart. J Am Coll Cardiol 1995, 26, 1257–1263. [Google Scholar] [CrossRef]
- Petersson, M.; Friberg, P.; Eisenhofer, G.; Lambert, G.; Rundqvist, B. Long-term outcome in relation to renal sympathetic activity in patients with chronic heart failure. Eur Heart J 2005, 26, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Joho, S.; Ushijima, R.; Nakagaito, M.; Kinugawa, K. Sympathetic overactivation predicts body weight loss in patients with heart failure. Auton Neurosci 2020, 223, 102625. [Google Scholar] [CrossRef] [PubMed]
- Lambert, E.A.; Esler, M.D.; Schlaich, M.P.; Dixon, J.; Eikelis, N.; Lambert, G.W. Obesity-associated organ damage and sympathetic nervous activity. Hypertension 2019, 73, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Ren, W.; Chen, J.; Wang, W.; Li, Q.; Yin, X.; Zhuang, G.; Zhou, H.; Zeng, W. Sympathetic nerve-enteroendocrine L cell communication modulates GLP-1 release, brain glucose utilization, and cognitive function. Neuron 2024, 112, 972–990. [Google Scholar] [CrossRef]
- Drucker, D.J. The biology of incretin hormones. Cell Metab 2006, 3, 153–165. [Google Scholar] [CrossRef]
- Pauza, A.G.; Thakkar, P.; Tasic, T.; Felippe, I.; Bishop, P.; Greenwood, M.P.; Rysevaite-Kyguoliene, K.; Ast, J.; Broichhagen, J.; Hodson, D.J.; et al. GLP1R attenuates sympathetic response to high glucose via carotid body inhibition. Circ Res 2022, 130, 694–707. [Google Scholar] [CrossRef]
- Drucker, D.J. Efficacy and safety of GLP-1 medicines for type 2 diabetes and obesity. Diabetes Care 2024, 47, 1873–1888. [Google Scholar] [CrossRef]
- Jastreboff, A.M.; Aronne, L.J.; Ahmad, N.N.; Wharton, S.; Connery, L.; Alves, B.; Kiyosue, A.; Zhang, S.; Liu, B.; Bunck, M.C.; et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med 2022, 387, 205–216. [Google Scholar] [CrossRef]
- Jastreboff, A.M.; Kaplan, L.M.; Frias, J.P.; Wu, Q.; Du, Y.; Gurbuz, S.; Coskun, T.; Haupt, A.; Milicevic, Z.; Hartman, M.L.; et al. Triple-hormone-receptor agonist retatrutide for obesity - A phase 2 trial. N Engl J Med 2023, 389, 514–526. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016, 375, 311–322. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Kaplan, L.M.; Frias, J.P.; Brouwers, B.; Wu, Q.; Thomas, M.K.; Harris, C.; Schloot, N.C.; Du, Y.; Mather, K.J.; et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nat Med 2024, 30, 2037–2048. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.; Lawson, F.; Owens, D.; Raccah, D.; Roy-Duval, C.; Lehmann, A.; Perfetti, R.; Blonde, L. Differential effects of glucagon-like peptide-1 receptor agonists on heart rate. Cardiovasc Diabetol 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Lubberding, A.F.; Veedfald, S.; Achter, J.S.; Nissen, S.D.; Soattin, L.; Sorrentino, A.; Vega, E.T.; Linz, B.; Eggertsen, C.H.E.; Mulvey, J.; et al. Glucagon-like peptide-1 increases heart rate by a direct action on the sinus node. Cardiovasc Res 2024, 120, 1427–1441. [Google Scholar] [CrossRef] [PubMed]
- Bharucha, A.E.; Charkoudian, N.; Andrews, C.N.; Camilleri, M.; Sletten, D.; Zinsmeister, A.R.; Low, P.A. Effects of glucagon-like peptide-1, yohimbine, and nitrergic modulation on sympathetic and parasympathetic activity in humans. Am J Physiol Regul Integr Comp Physiol 2008, 295, R874–R880. [Google Scholar] [CrossRef]
- Chao, E.C. SGLT-2 Inhibitors: A new mechanism for glycemic control. Clin Diabetes 2014, 32, 4–11. [Google Scholar] [CrossRef]
- Patel, S.M.; Kang, Y.M.; Im, K.; Neuen, B.L.; Anker, S.D.; Bhatt, D.L.; Butler, J.; Cherney, D.Z.I.; Claggett, B.L.; Fletcher, R.A.; et al. Sodium-glucose cotransporter-2 inhibitors and major adverse cardiovascular outcomes: A SMART-C collaborative meta-analysis. Circulation 2024, 149, 1789–1801. [Google Scholar] [CrossRef]
- Cheong, A.J.Y.; Teo, Y.N.; Teo, Y.H.; Syn, N.L.; Ong, H.T.; Ting, A.Z.H.; Chia, A.Z.Q.; Chong, E.Y.; Chan, M.Y.; Lee, C.H.; et al. SGLT inhibitors on weight and body mass: A meta-analysis of 116 randomized-controlled trials. Obesity 2022, 30, 117–128. [Google Scholar] [CrossRef]
- Herat, L.Y.; Magno, A.L.; Rudnicka, C.; Hricova, J.; Carnagarin, R.; Ward, N.C.; Arcambal, A.; Kiuchi, M.G.; Head, G.A.; Schlaich, M.P.; et al. SGLT2 Inhibitor-induced sympathoinhibition: A novel mechanism for cardiorenal protection. JACC Basic Transl Sci 2020, 5, 169–179. [Google Scholar] [CrossRef]
- Oshima, N.; Onimaru, H.; Yamashiro, A.; Goto, H.; Tanoue, K.; Fukunaga, T.; Sato, H.; Uto, A.; Matsubara, H.; Imakiire, T.; et al. SGLT2 and SGLT1 inhibitors suppress the activities of the RVLM neurons in newborn Wistar rats. Hypertens Res 2024, 47, 46–54. [Google Scholar] [CrossRef]
- Nguyen, T.; Wen, S.; Gong, M.; Yuan, X.; Xu, D.; Wang, C.; Jin, J.; Zhou, L. Dapagliflozin activates neurons in the central nervous system and regulates cardiovascular activity by inhibiting SGLT-2 in mice. Diabetes Metab Syndr Obes 2020, 13, 2781–2799. [Google Scholar] [CrossRef]
- Jordan, J.; Tank, J.; Heusser, K.; Heise, T.; Wanner, C.; Heer, M.; Macha, S.; Mattheus, M.; Lund, S.S.; Woerle, H.J.; et al. The effect of empagliflozin on muscle sympathetic nerve activity in patients with type II diabetes mellitus. J Am Soc Hypertens 2017, 11, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Heusser, K.; Tank, J.; Diedrich, A.; Fischer, A.; Heise, T.; Jordan, J. Randomized trial comparing SGLT2 inhibition and hydrochlorothiazide on sympathetic traffic in type 2 diabetes. Kidney Int Rep 2023, 8, 2254–2264. [Google Scholar] [CrossRef] [PubMed]
- Strack, A.M.; Sawyer, W.B.; Platt, K.B.; Loewy, A.D. CNS cell groups regulating the sympathetic outflow to adrenal gland as revealed by transneuronal cell body labeling with pseudorabies virus. Brain Res 1989, 491, 274–296. [Google Scholar] [CrossRef] [PubMed]
- Dampney, R.A.; Polson, J.W.; Potts, P.D.; Hirooka, Y.; Horiuchi, J. Functional organization of brain pathways subserving the baroreceptor reflex: studies in conscious animals using immediate early gene expression. Cell Mol Neurobiol 2003, 23, 597–616. [Google Scholar] [CrossRef]
- Lindberg, D.; Chen, P.; Li, C. Conditional viral tracing reveals that steroidogenic factor 1-positive neurons of the dorsomedial subdivision of the ventromedial hypothalamus project to autonomic centers of the hypothalamus and hindbrain. J Comp Neurol 2013, 521, 3167–3190. [Google Scholar] [CrossRef]
- Van Huysse, J.W.; Bealer, S.L. Central nervous system norepinephrine release during hypotension and hyperosmolality in conscious rats. Am J Physiol 1991, 260, R1071–R1076. [Google Scholar] [CrossRef]
- Huangfu, D.H.; Koshiya, N.; Guyenet, P.G. A5 noradrenergic unit activity and sympathetic nerve discharge in rats. Am J Physiol 1991, 261, R393–R402. [Google Scholar] [CrossRef]
- Singewald, N.; Philippu, A. Catecholamine release in the locus coeruleus is modified by experimentally induced changes in haemodynamics. Naunyn Schmiedebergs Arch Pharmacol 1993, 347, 21–27. [Google Scholar] [CrossRef]
- Mitchell, D.A.; Lambert, G.; Secher, N.H.; Raven, P.B.; van Lieshout, J.; Esler, M.D. Jugular venous overflow of noradrenaline from the brain: a neurochemical indicator of cerebrovascular sympathetic nerve activity in humans. J Physiol 2009, 587, 2589–2597. [Google Scholar] [CrossRef]
- Foote, S.L.; Bloom, F.E.; Aston-Jones, G. Nucleus locus ceruleus: new evidence of anatomical and physiological specificity. Physiol Rev 1983, 63, 844–914. [Google Scholar] [CrossRef]
- Hauglund, N.L.; Andersen, M.; Tokarska, K.; Radovanovic, T.; Kjaerby, C.; Sorensen, F.L.; Bojarowska, Z.; Untiet, V.; Ballestero, S.B.; Kolmos, M.G.; et al. Norepinephrine-mediated slow vasomotion drives glymphatic clearance during sleep. Cell 2025, 188, 606–622. [Google Scholar] [CrossRef] [PubMed]
- Macefield, V.G.; Henderson, L.A. Real-time imaging of the medullary circuitry involved in the generation of spontaneous muscle sympathetic nerve activity in awake subjects. Hum Brain Mapp 2010, 31, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Macefield, V.G.; Henderson, L.A. Identification of the human sympathetic connectome involved in blood pressure regulation. Neuroimage 2019, 202, 116119. [Google Scholar] [CrossRef] [PubMed]
- James, C.; Macefield, V.G.; Henderson, L.A. Real-time imaging of cortical and subcortical control of muscle sympathetic nerve activity in awake human subjects. Neuroimage 2013, 70, 59–65. [Google Scholar] [CrossRef]
- Wang, G.-J.; Volkow, N.D.; Logan, J.; Pappas, N.R.; Wong, C.T.; Zhu, W.; Netusll, N.; Fowler, J.S. Brain dopamine and obesity. The Lancet 2001, 357, 354–357. [Google Scholar] [CrossRef]
- Carnell, S.; Gibson, C.; Benson, L.; Ochner, C.N.; Geliebter, A. Neuroimaging and obesity: current knowledge and future directions. 2012, 13, 43–56. [CrossRef]
- Zhang, P.; Wu, G.W.; Yu, F.X.; Liu, Y.; Li, M.Y.; Wang, Z.; Ding, H.Y.; Li, X.S.; Wang, H.; Jin, M.; et al. Abnormal regional neural activity and reorganized neural network in obesity: Evidence from resting-state fMRI. Obesity 2020, 28, 1283–1291. [Google Scholar] [CrossRef]
- Gómez-Apo, E.; Mondragón-Maya, A.; Ferrari-Díaz, M.; Silva-Pereyra, J. Structural brain changes associated with overweight and obesity. J Obes 2021, Jul 16, 6613385. [Google Scholar] [CrossRef]
- Li, G.; Hu, Y.; Zhang, W.; Wang, J.; Ji, W.; Manza, P.; Volkow, N.D.; Zhang, Y.; Wang, G.J. Brain functional and structural magnetic resonance imaging of obesity and weight loss interventions. Mol Psychiatry 2023, 28, 1466–1479. [Google Scholar] [CrossRef]
- Patel, M.; Braun, J.; Lambert, G.W.; Kameneva, T.; Keatch, C.; Lambert, E. Central mechanisms in sympathetic nervous dysregulation in obesity. J Neurophysiol 2023. [Google Scholar] [CrossRef]
- Tadross, J.A.; Steuernagel, L.; Dowsett, G.K.C.; Kentistou, K.A.; Lundh, S.; Porniece, M.; Klemm, P.; Rainbow, K.; Hvid, H.; Kania, K.; et al. A comprehensive spatio-cellular map of the human hypothalamus. Nature 2025. [Google Scholar] [CrossRef]
- Buonfiglio, D.; Tchio, C.; Furigo, I.; Donato, J., Jr.; Baba, K.; Cipolla-Neto, J.; Tosini, G. Removing melatonin receptor type 1 signaling leads to selective leptin resistance in the arcuate nucleus. J Pineal Res 2019, 67, e12580. [Google Scholar] [CrossRef] [PubMed]
- Enriori, P.J.; Sinnayah, P.; Simonds, S.E.; Garcia Rudaz, C.; Cowley, M.A. Leptin action in the dorsomedial hypothalamus increases sympathetic tone to brown adipose tissue in spite of systemic leptin resistance. J Neurosci 2011, 31, 12189–12197. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.J.; Fontes, M.A.; Killinger, S.; Pawlak, D.B.; Polson, J.W.; Dampney, R.A. Cardiovascular responses evoked by leptin acting on neurons in the ventromedial and dorsomedial hypothalamus. Hypertension 2003, 42, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, J.R.; Miller, J.W.; Keogh, J.M.; Henning, E.; Satterwhite, J.H.; Cameron, G.S.; Astruc, B.; Mayer, J.P.; Brage, S.; See, T.C.; et al. Modulation of blood pressure by central melanocortinergic pathways. N Engl J Med 2009, 360, 44–52. [Google Scholar] [CrossRef]
- Lim, K.; Barzel, B.; Burke, S.L.; Armitage, J.A.; Head, G.A. Origin of aberrant blood pressure and sympathetic regulation in diet-induced obesity. Hypertension 2016, 68, 491–500. [Google Scholar] [CrossRef]
- Eikelis, N.; Lambert, G.; Wiesner, G.; Kaye, D.; Schlaich, M.; Morris, M.; Hastings, J.; Socratous, F.; Esler, M. Extra-adipocyte leptin release in human obesity and its relation to sympathoadrenal function. Am J Physiol Endocrinol Metab 2004, 286, E744–E752. [Google Scholar] [CrossRef]
- Myers, M.G., Jr.; Affinati, A.H.; Richardson, N.; Schwartz, M.W. Central nervous system regulation of organismal energy and glucose homeostasis. Nat Metab 2021, 3, 737–750. [Google Scholar] [CrossRef]
- Sewaybricker, L.E.; Huang, A.; Chandrasekaran, S.; Melhorn, S.J.; Schur, E.A. The significance of hypothalamic inflammation and gliosis for the pathogenesis of obesity in humans. Endocr Rev 2023, 44, 281–296. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Lambert, G.W.; Masuo, K.; Dawood, T.; Eikelis, N.; Nestel, P.J.; McGrane, M.T.; Mariani, J.A.; Socratous, F.; Chopra, R.; et al. Blunted sympathetic neural response to oral glucose in obese subjects with the insulin-resistant metabolic syndrome. Am J Clin Nutr 2009, 89, 27–36. [Google Scholar] [CrossRef]
- Guimaraes, P.S.; Huber, D.A.; Campagnole-Santos, M.J.; Schreihofer, A.M. Development of attenuated baroreflexes in obese Zucker rats coincides with impaired activation of nucleus tractus solitarius. Am J Physiol Regul Integr Comp Physiol 2014, 306, R681–R692. [Google Scholar] [CrossRef]
- Balasubramanian, P.; Asirvatham-Jeyaraj, N.; Monteiro, R.; Sivasubramanian, M.K.; Hall, D.; Subramanian, M. Obesity-induced sympathoexcitation is associated with Nrf2 dysfunction in the rostral ventrolateral medulla. Am J Physiol Regul Integr Comp Physiol 2020, 318, R435–R444. [Google Scholar] [CrossRef] [PubMed]
- Kishi, T.; Hirooka, Y.; Ogawa, K.; Konno, S.; Sunagawa, K. Calorie restriction inhibits sympathetic nerve activity via anti-oxidant effect in the rostral ventrolateral medulla of obesity-induced hypertensive rats. Clin Exp Hypertens 2011, 33, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Lambert, E.A.; Sari, C.I.; Eikelis, N.; Phillips, S.E.; Grima, M.; Straznicky, N.E.; Dixon, J.B.; Esler, M.; Schlaich, M.P.; Head, G.A.; et al. Effects of moxonidine and low-calorie diet: Cardiometabolic benefits from combination of both therapies. Obesity 2017, 25, 1894–1902. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Hu, Y.; Zhang, W.; Ding, Y.; Wang, Y.; Wang, J.; He, Y.; Lv, G.; von Deneen, K.M.; Zhao, Y.; et al. Resting activity of the hippocampus and amygdala in obese individuals predicts their response to food cues. Addict Biol 2021, 26, e12974. [Google Scholar] [CrossRef]
- Li, G.; Ji, G.; Hu, Y.; Liu, L.; Jin, Q.; Zhang, W.; Liu, L.; Wang, Y.; Zhao, J.; von Deneen, K.M.; et al. Reduced plasma ghrelin concentrations are associated with decreased brain reactivity to food cues after laparoscopic sleeve gastrectomy. Psychoneuroendocrinology 2019, 100, 229–236. [Google Scholar] [CrossRef]
- Lambert, E.; Lambert, G.; Ika-Sari, C.; Dawood, T.; Lee, K.; Chopra, R.; Straznicky, N.; Eikelis, N.; Drew, S.; Tilbrook, A.; et al. Ghrelin modulates sympathetic nervous system activity and stress response in lean and overweight men. Hypertension 2011, 58, 43–50. [Google Scholar]
- Wang, Y.; Ji, G.; Hu, Y.; Li, G.; Ding, Y.; Hu, C.; Liu, L.; Zhang, W.; von Deneen, K.M.; Han, Y.; et al. Laparoscopic sleeve gastrectomy induces sustained changes in gray and white matter brain volumes and resting functional connectivity in obese patients. Surg Obes Relat Dis 2020, 16, 1–9. [Google Scholar] [CrossRef]
- Custers, E.; Vreeken, D.; Kleemann, R.; Kessels, R.P.C.; Duering, M.; Brouwer, J.; Aufenacker, T.J.; Witteman, B.P.L.; Snabel, J.; Gart, E.; et al. Long-term brain structure and cognition following bariatric surgery. JAMA Netw Open 2024, 7, e2355380. [Google Scholar] [CrossRef]
- Simon, J.J.; Becker, A.; Sinno, M.H.; Skunde, M.; Bendszus, M.; Preissl, H.; Enck, P.; Herzog, W.; Friederich, H.C. Neural food reward processing in successful and unsuccessful weight maintenance. Obesity 2018, 26, 895–902. [Google Scholar] [CrossRef]
- Alhadeff, A.L.; Rupprecht, L.E.; Hayes, M.R. GLP-1 neurons in the nucleus of the solitary tract project directly to the ventral tegmental area and nucleus accumbens to control for food intake. Endocrinology 2012, 153, 647–658. [Google Scholar] [CrossRef]
- Rinaman, L. Ascending projections from the caudal visceral nucleus of the solitary tract to brain regions involved in food intake and energy expenditure. Brain Res 2010, 1350, 18–34. [Google Scholar] [CrossRef] [PubMed]
- Moiz, A.; Filion, K.B.; Tsoukas, M.A.; Yu, O.H.; Peters, T.M.; Eisenberg, M.J. Mechanisms of GLP-1 receptor agonist-induced weight loss: A review of central and peripheral pathways in appetite and energy regulation. Am J Med 2025. [Google Scholar] [CrossRef]
- Suda, Y.; Nakamura, K.; Matsuyama, F.; Hamada, Y.; Makabe, H.; Narita, M.; Nagumo, Y.; Mori, T.; Kuzumaki, N.; Narita, M. Peripheral-central network analysis of cancer cachexia status accompanied by the polarization of hypothalamic microglia with low expression of inhibitory immune checkpoint receptors. Mol Brain 2024, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Walton, E.; Bernardoni, F.; Batury, V.L.; Bahnsen, K.; Lariviere, S.; Abbate-Daga, G.; Andres-Perpina, S.; Bang, L.; Bischoff-Grethe, A.; Brooks, S.J.; et al. Brain structure in acutely underweight and partially weight-restored individuals with anorexia nervosa: A coordinated analysis by the ENIGMA Eating Disorders Working Group. Biol Psychiatry 2022, 92, 730–738. [Google Scholar] [CrossRef]
- Papassotiriou, I.; Spiliopoulou, S.; Dragonas, D.; Tsoutsoura, N.; Korompoki, E.; Manios, E. The relation between body mass index and target organ damage and the mediating role of blood pressure. Eur J Clin Nutr 2025. [Google Scholar] [CrossRef]
- Valenzuela, P.L.; Carrera-Bastos, P.; Castillo-Garcia, A.; Lieberman, D.E.; Santos-Lozano, A.; Lucia, A. Obesity and the risk of cardiometabolic diseases. Nat Rev Cardiol 2023, 20, 475–494. [Google Scholar] [CrossRef]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat Rev Endocrinol 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Alvarez, G.E.; Beske, S.D.; Ballard, T.P.; Davy, K.P. Sympathetic neural activation in visceral obesity. Circulation 2002, 106, 2533–2536. [Google Scholar] [CrossRef]
- Hillebrand, S.; de Mutsert, R.; Christen, T.; Maan, A.C.; Jukema, J.W.; Lamb, H.J.; de Roos, A.; Rosendaal, F.R.; den Heijer, M.; Swenne, C.A.; et al. Body fat, especially visceral fat, is associated with electrocardiographic measures of sympathetic activation. Obesity 2014, 22, 1553–1559. [Google Scholar] [CrossRef]
- Flores-Opazo, M.; Kopinke, D.; Helmbacher, F.; Fernandez-Verdejo, R.; Tunon-Suarez, M.; Lynch, G.S.; Contreras, O. Fibro-adipogenic progenitors in physiological adipogenesis and intermuscular adipose tissue remodeling. Mol Aspects Med 2024, 97, 101277. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Grima, M.T.; Eikelis, N.; Nestel, P.J.; Dawood, T.; Schlaich, M.P.; Chopra, R.; Masuo, K.; Esler, M.D.; Sari, C.I.; et al. The effects of weight loss versus weight loss maintenance on sympathetic nervous system activity and metabolic syndrome components. J Clin Endocrinol Metab 2011, 96, E503–508. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Maretich, P.; Kajimura, S. The common and distinct features of brown and beige adipocytes. Trends Endocrinol Metab 2018, 29, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Coelho, M.; Oliveira, T.; Fernandes, R. Biochemistry of adipose tissue: an endocrine organ. Arch Med Sci 2013, 9, 191–200. [Google Scholar] [CrossRef]
- Yahagi, N. Hepatic control of energy metabolism via the autonomic nervous system. J Atheroscler Thromb 2017, 24, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Bartness, T.J.; Liu, Y.; Shrestha, Y.B.; Ryu, V. Neural innervation of white adipose tissue and the control of lipolysis. Front Neuroendocrinol 2014, 35, 473–493. [Google Scholar] [CrossRef]
- Cypess, A.M.; Lehman, S.; Williams, G.; Tal, I.; Rodman, D.; Goldfine, A.B.; Kuo, F.C.; Palmer, E.L.; Tseng, Y.H.; Doria, A.; et al. Identification and importance of brown adipose tissue in adult humans. N Engl J Med 2009, 360, 1509–1517. [Google Scholar] [CrossRef]
- Vaughan, C.H.; Zarebidaki, E.; Ehlen, J.C.; Bartness, T.J. Analysis and measurement of the sympathetic and sensory innervation of white and brown adipose tissue. Methods Enzymol 2014, 537, 199–225. [Google Scholar] [CrossRef]
- Admiraal, W.M.; Holleman, F.; Bahler, L.; Soeters, M.R.; Hoekstra, J.B.; Verberne, H.J. Combining 123I-metaiodobenzylguanidine SPECT/CT and 18F-FDG PET/CT for the assessment of brown adipose tissue activity in humans during cold exposure. J Nucl Med 2013, 54, 208–212. [Google Scholar] [CrossRef]
- Green, A.L.; Bagci, U.; Hussein, S.; Kelly, P.V.; Muzaffar, R.; Neuschwander-Tetri, B.A.; Osman, M.M. Brown adipose tissue detected by PET/CT imaging is associated with less central obesity. Nucl Med Commun 2017, 38, 629–635. [Google Scholar] [CrossRef]
- Carey, A.L.; Formosa, M.F.; Van Every, B.; Bertovic, D.; Eikelis, N.; Lambert, G.W.; Kalff, V.; Duffy, S.J.; Cherk, M.H.; Kingwell, B.A. Ephedrine activates brown adipose tissue in lean but not obese humans. Diabetologia 2013, 56, 147–155. [Google Scholar] [CrossRef]
- Saito, M.; Okamatsu-Ogura, Y.; Matsushita, M.; Watanabe, K.; Yoneshiro, T.; Nio-Kobayashi, J.; Iwanaga, T.; Miyagawa, M.; Kameya, T.; Nakada, K.; et al. High incidence of metabolically active brown adipose tissue in healthy adult humans: effects of cold exposure and adiposity. Diabetes 2009, 58, 1526–1531. [Google Scholar] [CrossRef] [PubMed]
- Bahler, L.; Verberne, H.J.; Admiraal, W.M.; Stok, W.J.; Soeters, M.R.; Hoekstra, J.B.; Holleman, F. Differences in sympathetic nervous stimulation of brown adipose tissue between the young and old, and the lean and obese. J Nucl Med 2016, 57, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Finlin, B.S.; Memetimin, H.; Zhu, B.; Confides, A.L.; Vekaria, H.J.; El Khouli, R.H.; Johnson, Z.R.; Westgate, P.M.; Chen, J.; Morris, A.J.; et al. The beta3-adrenergic receptor agonist mirabegron improves glucose homeostasis in obese humans. J Clin Invest 2020, 130, 2319–2331. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Proenca, R.; Maffei, M.; Barone, M.; Leopold, L.; Friedman, J.M. Positional cloning of the mouse obese gene and its human homologue. Nature 1994, 372, 425–432. [Google Scholar] [CrossRef]
- Minocci, A.; Savia, G.; Lucantoni, R.; Berselli, M.E.; Tagliaferri, M.; Calo, G.; Petroni, M.L.; de Medici, C.; Viberti, G.C.; Liuzzi, A. Leptin plasma concentrations are dependent on body fat distribution in obese patients. Int J Obes Relat Metab Disord 2000, 24, 1139–1144. [Google Scholar] [CrossRef]
- Schwartz, M.W.; Peskind, E.; Raskind, M.; Boyko, E.J.; Porte, D., Jr. Cerebrospinal fluid leptin levels: relationship to plasma levels and to adiposity in humans. Nat Med 1996, 2, 589–593. [Google Scholar] [CrossRef]
- Rahmouni, K. Leptin-induced sympathetic nerve activation: Signaling mechanisms and cardiovascular consequences in obesity. Curr Hypertens Rev 2010, 6, 104–209. [Google Scholar] [CrossRef]
- Rahmouni, K.; Morgan, D.A. Hypothalamic arcuate nucleus mediates the sympathetic and arterial pressure responses to leptin. Hypertension 2007, 49, 647–652. [Google Scholar] [CrossRef]
- Rumantir, M.S.; Vaz, M.; Jennings, G.L.; Collier, G.; Kaye, D.M.; Seals, D.R.; Wiesner, G.H.; Brunner-La Rocca, H.P.; Esler, M.D. Neural mechanisms in human obesity-related hypertension. J Hypertens 1999, 17, 1125–1133. [Google Scholar] [CrossRef]
- Grassi, G.; Colombo, M.; Seravalle, G.; Spaziani, D.; Mancia, G. Dissociation between muscle and skin sympathetic nerve activity in essential hypertension, obesity, and congestive heart failure. Hypertension 1998, 31, 64–67. [Google Scholar] [CrossRef]
- Lafontan, M.; Langin, D. Lipolysis and lipid mobilization in human adipose tissue. Prog Lipid Res 2009, 48, 275–297. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suarez, V.J.; Redondo-Florez, L.; Beltran-Velasco, A.I.; Martin-Rodriguez, A.; Martinez-Guardado, I.; Navarro-Jimenez, E.; Laborde-Cardenas, C.C.; Tornero-Aguilera, J.F. The role of adipokines in health and disease. Biomedicines 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, K.; Sommer, M.; Strobel, S.; Thrum, S.; Bluher, M.; Wagner, U.; Rossol, M. Perturbation of the monocyte compartment in human obesity. Front Immunol 2019, 10, 1874. [Google Scholar] [CrossRef] [PubMed]
- Larabee, C.M.; Neely, O.C.; Domingos, A.I. Obesity: A neuroimmunometabolic perspective. Nat Rev Endocrinol 2020, 16, 30–43. [Google Scholar] [CrossRef]
- Huang, F.; Del-Rio-Navarro, B.E.; Leija-Martinez, J.; Torres-Alcantara, S.; Ruiz-Bedolla, E.; Hernandez-Cadena, L.; Barraza-Villarreal, A.; Romero-Nava, R.; Sanchez-Munoz, F.; Villafana, S.; et al. Effect of omega-3 fatty acids supplementation combined with lifestyle intervention on adipokines and biomarkers of endothelial dysfunction in obese adolescents with hypertriglyceridemia. J Nutr Biochem 2019, 64, 162–169. [Google Scholar] [CrossRef]
- Akiyoshi, H.; Gonda, T.; Terada, T. A comparative histochemical and immunohistochemical study of aminergic, cholinergic and peptidergic innervation in rat, hamster, guinea pig, dog and human livers. Liver 1998, 18, 352–359. [Google Scholar] [CrossRef]
- Jarhult, J.; Falck, B.; Ingemansson, S.; Nobin, A. The functional importance of sympathetic nerves to the liver and endocrine pancreas. Ann Surg 1979, 189, 96–100. [Google Scholar] [CrossRef]
- Mizuno, K.; Ueno, Y. Autonomic nervous system and the liver. Hepatol Res 2017, 47, 160–165. [Google Scholar] [CrossRef]
- Basu, R.; Chandramouli, V.; Dicke, B.; Landau, B.; Rizza, R. Obesity and type 2 diabetes impair insulin-induced suppression of glycogenolysis as well as gluconeogenesis. Diabetes 2005, 54, 1942–1948. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Grima, M.T.; Sari, C.I.; Eikelis, N.; Lambert, E.A.; Nestel, P.J.; Esler, M.D.; Dixon, J.B.; Chopra, R.; Tilbrook, A.J.; et al. Neuroadrenergic dysfunction along the diabetes continuum: a comparative study in obese metabolic syndrome subjects. Diabetes 2012, 61, 2506–2516. [Google Scholar] [CrossRef]
- Huggett, R.J.; Scott, E.M.; Gilbey, S.G.; Stoker, J.B.; Mackintosh, A.F.; Mary, D.A. Impact of type 2 diabetes mellitus on sympathetic neural mechanisms in hypertension. Circulation 2003, 108, 3097–3101. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Takamura, T.; Takeshita, Y.; Ryu, Y.; Misu, H.; Ota, T.; Tokuyama, K.; Nagasaka, S.; Matsuhisa, M.; Matsui, O.; et al. Ectopic fat accumulation and distant organ-specific insulin resistance in Japanese people with nonalcoholic fatty liver disease. PLoS One 2014, 9, e92170. [Google Scholar] [CrossRef] [PubMed]
- Hurr, C.; Simonyan, H.; Morgan, D.A.; Rahmouni, K.; Young, C.N. Liver sympathetic denervation reverses obesity-induced hepatic steatosis. J Physiol 2019, 597, 4565–4580. [Google Scholar] [CrossRef] [PubMed]
- Hampton, R.F.; Jimenez-Gonzalez, M.; Stanley, S.A. Unravelling innervation of pancreatic islets. Diabetologia 2022, 65, 1069–1084. [Google Scholar] [CrossRef]
- Almaca, J.; Weitz, J.; Rodriguez-Diaz, R.; Pereira, E.; Caicedo, A. The pericyte of the pancreatic islet regulates capillary diameter and local blood flow. Cell Metab 2018, 27, 630–644. [Google Scholar] [CrossRef]
- Mateus Goncalves, L.; Almaca, J. Functional characterization of the human islet microvasculature using living pancreas slices. Front Endocrinol (Lausanne) 2020, 11, 602519. [Google Scholar] [CrossRef]
- Sakamoto, K.; Butera, M.A.; Zhou, C.; Maurizi, G.; Chen, B.; Ling, L.; Shawkat, A.; Patlolla, L.; Thakker, K.; Calle, V.; et al. Overnutrition causes insulin resistance and metabolic disorder through increased sympathetic nervous system activity. Cell Metab 2025, 37, 121–137. [Google Scholar] [CrossRef]
- Scherrer, U.; Sartori, C. Insulin as a vascular and sympathoexcitatory hormone: implications for blood pressure regulation, insulin sensitivity, and cardiovascular morbidity. Circulation 1997, 96, 4104–4113. [Google Scholar] [CrossRef]
- Roatta, S.; Farina, D. Sympathetic actions on the skeletal muscle. Exerc Sport Sci Rev 2010, 38, 31–35. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Tripathy, D. Skeletal muscle insulin resistance is the primary defect in type 2 diabetes. Diabetes Care 2009, 32 Suppl 2, S157–163. [Google Scholar] [CrossRef]
- Eichmann, A.; Brunet, I. Arterial innervation in development and disease. Sci Transl Med 2014, 6, 252ps259. [Google Scholar] [CrossRef] [PubMed]
- Straka, T.; Vita, V.; Prokshi, K.; Horner, S.J.; Khan, M.M.; Pirazzini, M.; Williams, M.P.I.; Hafner, M.; Zaglia, T.; Rudolf, R. Postnatal development and distribution of sympathetic innervation in mouse skeletal muscle. Int J Mol Sci 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Delbono, O.; Rodrigues, A.C.Z.; Bonilla, H.J.; Messi, M.L. The emerging role of the sympathetic nervous system in skeletal muscle motor innervation and sarcopenia. Ageing Res Rev 2021, 67, 101305. [Google Scholar] [CrossRef] [PubMed]
- Bacurau, A.V.; Jardim, M.A.; Ferreira, J.C.; Bechara, L.R.; Bueno, C.R., Jr.; Alba-Loureiro, T.C.; Negrao, C.E.; Casarini, D.E.; Curi, R.; Ramires, P.R.; et al. Sympathetic hyperactivity differentially affects skeletal muscle mass in developing heart failure: role of exercise training. J Appl Physiol (1985) 2009, 106, 1631–1640. [Google Scholar] [CrossRef]
- Fonseca, G.; Santos, M.R.D.; Souza, F.R.; Costa, M.; Haehling, S.V.; Takayama, L.; Pereira, R.M.R.; Negrao, C.E.; Anker, S.D.; Alves, M. Sympatho-vagal imbalance is associated with sarcopenia in male patients with heart failure. Arq Bras Cardiol 2019, 112, 739–746. [Google Scholar] [CrossRef]
- Rodrigues, A.C.Z.; Messi, M.L.; Wang, Z.M.; Abba, M.C.; Pereyra, A.; Birbrair, A.; Zhang, T.; O'Meara, M.; Kwan, P.; Lopez, E.I.S.; et al. The sympathetic nervous system regulates skeletal muscle motor innervation and acetylcholine receptor stability. Acta Physiol (Oxf) 2019, 225, e13195. [Google Scholar] [CrossRef]
- Seals, D.R.; Esler, M.D. Human ageing and the sympathoadrenal system. J Physiol 2000, 528, 407–417. [Google Scholar] [CrossRef]
- Esler, M.D.; Turner, A.G.; Kaye, D.M.; Thompson, J.M.; Kingwell, B.A.; Morris, M.; Lambert, G.W.; Jennings, G.L.; Cox, H.S.; Seals, D.R. Aging effects on human sympathetic neuronal function. Am J Physiol 1995, 268, R278–R285. [Google Scholar] [CrossRef]
- Esler, M.D.; Thompson, J.M.; Kaye, D.M.; Turner, A.G.; Jennings, G.L.; Cox, H.S.; Lambert, G.W.; Seals, D.R. Effects of aging on the responsiveness of the human cardiac sympathetic nerves to stressors. Circulation 1995, 91, 351–358. [Google Scholar] [CrossRef]
- Kaye, D.M.; Vaddadi, G.; Gruskin, S.L.; Du, X.J.; Esler, M.D. Reduced myocardial nerve growth factor expression in human and experimental heart failure. Circ Res 2000, 86, E80–E84. [Google Scholar] [CrossRef]
- Iseki, K.; Ikemiya, Y.; Kinjo, K.; Inoue, T.; Iseki, C.; Takishita, S. Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int 2004, 65, 1870–1876. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; McCulloch, C.E.; Iribarren, C.; Darbinian, J.; Go, A.S. Body mass index and risk for end-stage renal disease. Ann Intern Med 2006, 144, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Chronic Kidney Disease Prognosis, C.; Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J.; Gansevoort, R.T. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [CrossRef]
- Hall, J.E.; do Carmo, J.M.; da Silva, A.A.; Wang, Z.; Hall, M.E. Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res 2015, 116, 991–1006. [Google Scholar] [CrossRef]
- Tu, J.; Chen, H.; Zeng, Q.; Chen, L.; Guo, Y.; Chen, K. Trends in obesity prevalence among adults with hypertension in the United States, 2001 to 2023. Hypertension 2025, 82, 498–508. [Google Scholar] [CrossRef]
- Lambert, E.; Sari, C.I.; Dawood, T.; Nguyen, J.; McGrane, M.; Eikelis, N.; Chopra, R.; Wong, C.; Chatzivlastou, K.; Head, G.; et al. Sympathetic nervous system activity is associated with obesity-induced subclinical organ damage in young adults. Hypertension 2010, 56, 351–358. [Google Scholar]
- Chagnac, A.; Zingerman, B.; Rozen-Zvi, B.; Herman-Edelstein, M. Consequences of glomerular hyperfiltration: The role of physical forces in the pathogenesis of chronic kidney disease in diabetes and obesity. Nephron 2019, 143, 38–42. [Google Scholar] [CrossRef]
- Agarwal, R.; Fouque, D. The foundation and the four pillars of treatment for cardiorenal protection in people with chronic kidney disease and type 2 diabetes. Nephrol Dial Transplant 2023, 38, 253–257. [Google Scholar] [CrossRef]
- Kenchaiah, S.; Evans, J.C.; Levy, D.; Wilson, P.W.; Benjamin, E.J.; Larson, M.G.; Kannel, W.B.; Vasan, R.S. Obesity and the risk of heart failure. N Engl J Med 2002, 347, 305–313. [Google Scholar] [CrossRef]
- Wong, C.Y.; O'Moore-Sullivan, T.; Leano, R.; Byrne, N.; Beller, E.; Marwick, T.H. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation 2004, 110, 3081–3087. [Google Scholar] [CrossRef]
- Schlaich, M.P.; Kaye, D.M.; Lambert, E.; Hastings, J.; Campbell, D.J.; Lambert, G.; Esler, M.D. Angiotensin II and norepinephrine release: interaction and effects on the heart. J Hypertens 2005, 23, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Schmermund, A.; Lerman, L.O.; Ritman, E.L.; Rumberger, J.A. Cardiac production of angiotensin II and its pharmacologic inhibition: effects on the coronary circulation. Mayo Clin Proc 1999, 74, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.; Ball, S.G.; Worthy, G.; Struthers, A.D.; Mary, D.A.; Greenwood, J.P. Hypertensive left ventricular hypertrophy: a mechanistic approach to optimizing regression assessed by cardiovascular magnetic resonance. J Hypertens 2012, 30, 2039–2046. [Google Scholar] [CrossRef] [PubMed]
- Cheng, D.C.Y.; Climie, R.E.; Shu, M.; Grieve, S.M.; Kozor, R.; Figtree, G.A. Vascular aging and cardiovascular disease: pathophysiology and measurement in the coronary arteries. Front Cardiovasc Med 2023, 10, 1206156. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol 2010, 55, 1318–1327. [Google Scholar] [CrossRef]
- Oren, A.; Vos, L.E.; Uiterwaal, C.S.; Grobbee, D.E.; Bots, M.L. Aortic stiffness and carotid intima-media thickness: two independent markers of subclinical vascular damage in young adults? Eur J Clin Invest 2003, 33, 949–954. [Google Scholar] [CrossRef]
- Sverrisdottir, Y.B.; Jansson, L.M.; Hagg, U.; Gan, L.M. Muscle sympathetic nerve activity is related to a surrogate marker of endothelial function in healthy individuals. PLoS ONE 2010, 5, e9257. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Sert-Kuniyoshi, F.H.; Sierra-Johnson, J.; Orban, M.; Gami, A.; Davison, D.; Singh, P.; Pusalavidyasagar, S.; Huyber, C.; Votruba, S.; et al. Modest visceral fat gain causes endothelial dysfunction in healthy humans. J Am Coll Cardiol 2010, 56, 662–666. [Google Scholar] [CrossRef]
- Huang, W.; Gan, Z.; Gao, Z.; Lin, Q.; Li, X.; Xie, W.; Gao, Z.; Zhou, Z.; Qiu, Z.; Qiu, W.; et al. Discrepancies between general and central obesity in arterial stiffness: observational studies and Mendelian randomization study. BMC Med 2024, 22, 325. [Google Scholar] [CrossRef]
- Lambert, E.A.; Phillips, S.; Belski, R.; Tursunalieva, A.; Eikelis, N.; Sari, C.I.; Dixon, J.B.; Straznicky, N.; Grima, M.; Head, G.A.; et al. Endothelial function in healthy young individuals Is associated with dietary consumption of saturated fat. Front Physiol 2017, 8, 876. [Google Scholar] [CrossRef]
- Xu, S.; Ilyas, I.; Little, P.J.; Li, H.; Kamato, D.; Zheng, X.; Luo, S.; Li, Z.; Liu, P.; Han, J.; et al. Endothelial dysfunction in atherosclerotic cardiovascular diseases and beyond: From mechanism to pharmacotherapies. Pharmacol Rev 2021, 73, 924–967. [Google Scholar] [CrossRef] [PubMed]
- Climie, R.E.; Alastruey, J.; Mayer, C.C.; Schwarz, A.; Laucyte-Cibulskiene, A.; Voicehovska, J.; Bianchini, E.; Bruno, R.M.; Charlton, P.H.; Grillo, A.; et al. Vascular ageing: moving from bench towards bedside. Eur J Prev Cardiol 2023, 30, 1101–1117. [Google Scholar] [CrossRef] [PubMed]
- Holwerda, S.W.; Luehrs, R.E.; DuBose, L.; Collins, M.T.; Wooldridge, N.A.; Stroud, A.K.; Fadel, P.J.; Abboud, F.M.; Pierce, G.L. Elevated muscle sympathetic nerve activity contributes to central artery stiffness in young and middle-age/older adults. Hypertension 2019, 73, 1025–1035. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



