Submitted:
19 March 2025
Posted:
20 March 2025
You are already at the latest version
Abstract
Telepresence robots can enhance social connection and support person-centered care in long-term care (LTC) homes. This study evaluates their impact in facilitating virtual visits between family caregivers and older residents in Canadian care homes. Telepresence robots were placed in residents’ rooms, allowing virtual visits at mutual convenience. A total of 18 residents and 17 family caregivers participated. Quantitative assessments included the Zarit Burden Interview, the De Jong Gierveld Loneliness Scale and the Quality of Life in Alzheimer’s Disease scale, while qualitative data were collected through interviews, field notes, and observations. Repeated ANOVA showed that using telepresence robots significantly reduced caregiver burden (p=0.008), improved residents' quality of life (p=0.028), and decreased resident loneliness (p=0.038). Older caregivers experienced the greatest burden reduction, with scores dropping from a mean of 25.0 at baseline to 16.1 at two months. Qualitative findings provided further context, revealing that residents felt more connected, close and engaged, while families found the robots facilitated continuity of care, complemented in-person visits, reduced stress and guilt and provided reassurance. These findings suggest that telepresence robots can enhance the well-being of both residents and caregivers in LTC homes, though future research should explore their long-term impact and technological limitations.
Keywords:
telepresence robots
; long-term care
; quality of life
; loneliness
; caregiver burden
1. Introduction
Loneliness in long-term care (LTC) remains an enduring and multifaceted challenge, intensified by the COVID-19 pandemic [1]. For residents in LTC settings, loneliness may extend beyond mere physical isolation, encompassing social disconnection and feelings of abandonment [2,3]. These factors collectively contribute to adverse health outcomes, including cognitive decline, depression, and reduced quality of life. Emerging evidence suggests that older men may be particularly vulnerable to loneliness in LTC settings. For example, Dahlberg et al. [4] and Wright et al. [5] reported older men, especially those who have lost social supports such as spouses, report higher levels of loneliness compared to women. This heightened vulnerability can be attributed to a confluence of factors, including the erosion of traditional social roles following retirement, a comparatively narrower social network, and societal expectations that discourage emotional expressiveness among men [6,7]. These issues may be further exacerbated by limited opportunities for spontaneous social engagement and meaningful interactions.
Family caregivers often experience substantial burdens during the transition of loved ones into LTC homes [8]. The reconfiguration of caregiving roles, from primary caregiver to a more peripheral yet emotionally invested visitor, faces unique challenges. For example, the feelings of guilt about placing their loved one into LTC, the loss of lifelong company at home, and the disrupted sense of purpose as a caregiver [9,10]. Such caregiver burden not only undermines the well-being of family members but also impacts residents’ quality of life. Strong family relationships are associated with enhanced emotional well-being, greater social connectedness, and improved overall quality of life among LTC residents [11].
In response to these dual challenges—resident loneliness and caregiver burden—technology-driven interventions offer promising solutions to facilitate meaningful social connections. Traditional approaches, such as telephone calls or video conferencing via handheld devices, often fall short due to technological barriers, sensory impairments, and the reliance on staff for operational assistance [12,13]. In this context, we have explored a more accessible option for virtual video calls by using telepresence robots [14]. These robotic systems allow for immersive, remote-controlled virtual visits, enabling easy, personalized interactions. Previous studies have demonstrated that telepresence robots help maintain social bonds, enhance residents’ sense of being valued and remembered, and support person-centered care [15,16]. From the residents’ perspective, telepresence robots nurture emotional closeness and meaningful engagement, while family members experience reduced stress, alleviated feelings of guilt, and reassurance regarding their loved one’s well-being.
While emerging qualitative evidence highlights the positive impact of telepresence robots, several concerns and barriers to implementation have also been noted [17,18]. Care facility staff have expressed concerns regarding potential resident confusion, privacy issues, and their own lack of skills and additional workload associated with managing the robots. Thus, systematic longitudinal assessments are needed to understand the long-term implications of using telepresence robots in LTC settings. This study addresses this gap by systematically examining the impact of telepresence robots on loneliness and quality of life among LTC residents, as well as the caregiver burden of their family caregivers. By integrating quantitative measures with rich qualitative insights, we aim to understand the broader implications of technology-driven interventions for improving the emotional and social well-being of older adults in LTC and their family caregivers. Our research questions are:
1. What are the experiences of residents and families in using telepresence robots?
2. Does the telepresence robot reduce loneliness, improve the quality of life in residents in LTC homes, and reduce the burden for family caregivers?
2. Methods
2.1. Design
We adopted a mixed-methods design, a convergent parallel mixed-methods approach under which quantitative and qualitative data were collected simultaneously and analyzed separately and independently [19](p. 280) [20](p. 519). Quantitative methods are advantageous in showing what relationships were established among variables; in contrast, qualitative methods are powerful in showing how and why these relationships develop [20](p. 519). With quantitative and qualitative data complementing each other, the approach allows us to draw on the strengths of both methods for a more comprehensive understanding of our research focus, which is the impacts of using telepresence robots on the emotional and social well-being of older adults in LTC and their family caregivers [21](p. 318). The approach also enables us to compare findings from both datasets with one another to gain better insights into the breadth and depth of individual experiences with telepresence robots and contextual factors [22]. Figure 1 shows the convergent parallel mixed-methods approach used in this study [23](p. 218).
2.2. Data Collection
2.2.1. Research Instruments
We used three survey instruments for the quantitative study: Zarit Burden Interview, DeJong Gierveld Loneliness Scale and Quality of Life –Alzheimer’s Disease (QOL-AD) scale. Firstly, the Zarit Burden Interview (12 items) [24] was used to measure caregiver burdens. The questionnaire has questions such as “How often do you feel that because of the time you spend with your relative, you do not have enough time for yourself?” “How often do you feel angry when you are around your relative?”. Participants could choose from “never,” “rarely,” “sometimes,” “quite frequently,” or “nearly always” (scored from 0 to 4 respectively) to answer. The higher the total score, the more burden the family caregiver has. Secondly, the 6-item DeJong Gierveld Loneliness Scale [25] was used to measure loneliness, with three items corresponding to emotional loneliness and social loneliness each. Participants could choose from “Yes,” “More or less,” and “No” for an answer that best described their feelings. Items for emotional loneliness were negatively worded (e.g., I experience a general sense of emptiness), and answers of “Yes” or “More or less” were scored three or two and “No” scored one. Questions for social loneliness were positively worded (e.g., There are many people I can trust completely), and the scoring was reversed. The higher score represents the greater loneliness. Lastly, the QOL-AD scale was used to measure participants’ quality of life [26]. The QOL-AD contains 13 items related to a group of life domains, including physical health, relationships, activities, and capabilities to perform some daily tasks. Participants could answer each question by choosing an answer from “poor,” “fair,” and “good” to “excellent,” with “poor” assigned 1 point and excellent assigned 4 points. A higher total score means a higher quality of life.
For qualitative data collection, we conducted semi-structured interviews with our participants as we asked them questions on the abovementioned scales. With questions such as “Can you tell me more about your experience of using the robot?” “Can you share some stories with us?” semi-structured interviews allowed us to follow up on experiences raised by our participants and gain rich, in-depth information about our study focus [27](p. 36). We also observed them during the data collection and took field notes to document our real-time observations and reflections, adding contextual depth to our data [28]. These qualitative methods complemented quantitative data to enrich the evidence given our research topic and enhanced the overall quality of our quantitative and qualitative data collected [29].
2.2.2. Setting
This study is part of a larger, three-year project that explores the experiences of residents, family caregivers, and staff in implementing telepresence robots in LTC settings for older people with dementia. We placed 20 robots in five LTC homes in an urban area of British Columbia, Canada. See Table 1 for detailed information about our partnered care sites.
2.2.3. Participant Recruitment and Sampling
We recruited participants with purposive sampling. The research team collaborated with staff champions from the recreation and rehabilitation departments of each care site to introduce the telepresence robot to residents and family caregivers and explain the study. Participants were intentionally recruited to reflect diverse racial and ethnocultural backgrounds, gender (male and female) and various age groups. We purposefully included residents with different mobility impairments requiring assistive devices like wheelchairs or walkers, as well as those living with various forms and stages of dementia. We had no participant drop-off during the two-month intervention.
This pre-post design, utilizing each participant as their own control, enhances statistical power even with a smaller sample size. The Partial Eta-Squared (η²p) values for caregiver burden (0.318), quality of life (0.191), and loneliness (0.203) in this study suggest large effect sizes, indicating substantial within-subject changes due to the intervention. Using G*Power (version 3.1) with parameters (α = 0.05, 1 - β = 0.80, and 3 measurements), the recommended sample size is 9, based on Cohen’s f calculated from the Partial Eta-Squared (η²p) values provided above. Given these strong effect sizes, the sample size of 35 (18 residents and 17 family caregivers) provided adequate power to detect meaningful changes.
2.2.4. Timeline
Data collection for this paper was between December 2022 and September 2023, which was the third phase of the larger project. Data collection for each participant was eight weeks. See Figure 2. For residents and patients, we collected data on their quality of life and loneliness at three points of time: before they started using the robot (T0), four weeks after using the robot (T1) and eight weeks after using the robot (T2). Similarly, we collected data on the caregiving burden from family caregivers at T0, T1 and T2. Notably, every participant’s T0 starts at a different time, as they started using the robot at a different time. For participants who participated in our study in the early stages of the larger project (i.e. before the third phase), their answers to these scales were retrospective.
We interviewed all residents in person as they preferred this approach. We scheduled data collection at the time and location at their convenience, often when they felt most energetic of the day and in their individual room at the care site. For family caregivers, we interviewed some of them in person during their visits to their loved ones in the care home. Interviews with other family caregivers were conducted remotely over Zoom or phone. Each interview lasted between 20 to 60 minutes. Data collected were recorded and transcribed verbatim. Data collection ceased when the research team agreed that the data was sufficient to answer our research questions.
2.2.5. The Research Team
Our team consists of multidisciplinary researchers and trainees. The Principal Investigator (PI), LH, is a professor in the School of Nursing at the University of British Columbia. LL is a professor in the School of Social Work at MacEwan University. The PI oversees the project and trains undergraduate and graduate trainees. JW, YZ, and LR are PhD students in nursing, medical science, and occupational therapy. JF is an undergraduate student in biomedical engineering. The team also involves patient partners and family caregivers to contribute lived experience expertise. Weekly research meetings allowed the team to discuss findings, critically challenge assumptions and deepen our understanding of the research topic from different perspectives. JW, LR and JF collected quantitative and qualitative data simultaneously. LL and YZ performed quantitative data analysis, while JW and LR led qualitative analysis.
2.3. Data Analysis
2.3.1. Quantitative Data Analysis
Statistical analyses were conducted using SPSS (version 29.0.2.0), with a significance level set at 0.05 for all two-tailed tests. First, descriptive analyses were performed to examine gender, age group, ethnicity, and family relationships, reporting counts and percentages to provide a comprehensive view of participants’ demographic characteristics. Descriptive statistics were then used to calculate the mean and standard deviation for the three scales (caregiver burden, quality of life, and loneliness) across three time points.
A repeated measures analysis of variance (ANOVA) was conducted to assess changes in each scale’s scores over time within the entire sample. If the assumption of sphericity was violated, a Greenhouse-Geisser correction was applied. When a significant effect was detected, Bonferroni post hoc tests were performed to determine which time points significantly differed. This analysis was then repeated for key sociodemographic subgroups, including binary gender (male and female), ethnicity (Asian and White), and age groups (for the caregiver burden scale only: younger than 60 years vs. 60 years and older). Cronbach’s alpha values indicated acceptable to high internal consistency for the scales. For the caregiver burden scale, reliability was 0.932 at Time 1, 0.895 at Time 2, and 0.870 at Time 3. For the loneliness scale, Cronbach’s alpha was 0.745 at Time 1, 0.643 at Time 2, and 0.654 at Time 3. The quality-of-life scale showed reliability values of 0.853 at Time 1, 0.804 at Time 2, and 0.911 at Time 3.
2.3.2. Qualitative Data Analysis
We followed the reflexive thematic analysis process proposed by Braun and Clark [30,31]. Step 1: LH trained the research team in mixed data analysis. Step 2: JW and LR familiarized with the qualitative data. Step 3: JW and LR coded qualitative data manually and developed initial themes. See Table 2: Examples of Coding. Step 4: In the research meeting, JW and LR presented themes, and the research team discussed and reviewed the themes. Step 5: Informed by the team discussion, the two trainees, JW and LR, refined the themes. Step 6: The team approved the updated themes and agreed on the final draft of the manuscript.
2.4. Data Integration
We compared, merged and interpreted quantitative and qualitative data to identify points of alignment and differences in findings [32]. Then, we developed narratives to explain how our quantitative and qualitative data complemented each other in the discussion, providing richer context and deeper insight.
2.5. Rigour
In our regular research meetings, we consistently involve patient partners, family caregivers, and clinicians to remain reflexive about our positions and assumptions about our research activities and participants. We involved the patient partner in the pilot testing survey and interview questions and reframed them accordingly to make these questions understandable for participants, especially patients and residents with dementia. We adopted multiple data collection methods, including surveys, interviews, field notes and observations, to gain a more comprehensive understanding of the research topic. In addition, LH trained the trainees using different methods to collect data from participants respectfully and make the data collection conversational and accessible.
2.6. Ethics
The study was approved by the Behavioral Research Ethics Board of the University of British Columbia. All our participants gave the research team informed consent before participating in the study. Pseudonyms were used for participants and LTC homes to protect confidentiality.
3. Result
The study included 35 participants, comprising 18 residents and 17 family members (see Table 3). Among the residents, males accounted for 55.6%, while females made up 44.4%. The majority of patients were aged 81 years or older (66.7%), followed by those aged 71–80 years (27.8%) and a smaller proportion aged 61–70 years (5.6%). In terms of ethnicity, 61.1% of patients identified as Asian, while 38.9% were white.
Among the family members, the gender distribution was predominantly female (82.3%), with males making up 17.6%. Family members’ ages varied, with the largest proportion in the 61–70 age group (29.4%), followed by 51–60 years (23.5%) and 31–50 years (23.5%). Smaller proportions were in the 71–80 (11.8%) and 21–40 (11.8%) age groups. Ethnically, 58.8% of family members identified as Asian, while 41.2% were white. Most of the caregivers were daughters to residents or patients (64.7%), followed by sons and other roles (spouse, granddaughter, friend).
3.1. Quantitative Results
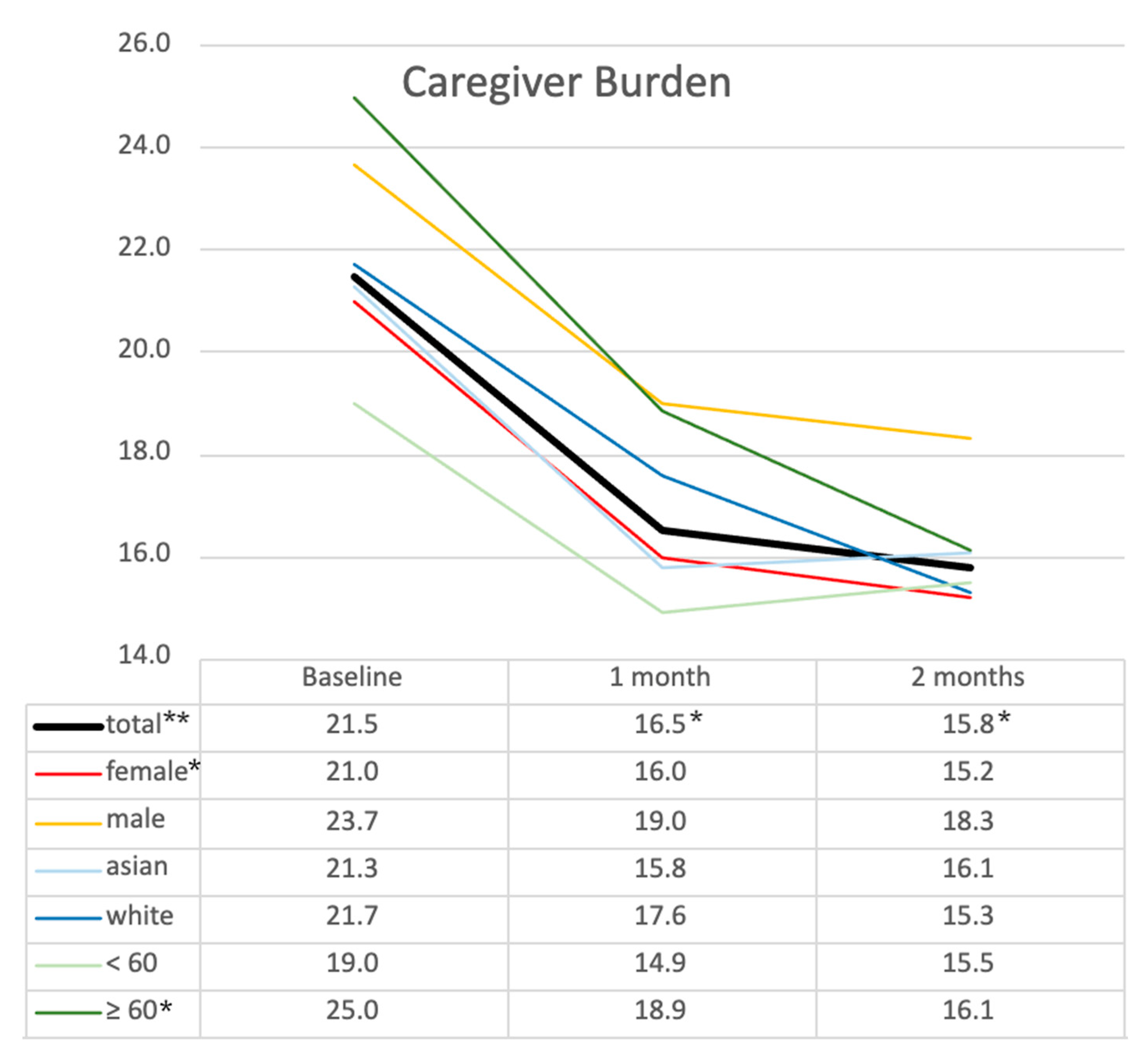
The results in Table 4 show significant changes in family caregiver burden, residents’ quality of life, and loneliness over three time points: Baseline (T0), 1 month after using a robot (T1), and 2 months after using a robot (T2). For family caregiver burden, the mean decreased from 21.5 ± 11.09 at T0 to 16.5 ± 7.92 at T1 and further to 15.8 ± 7.68 at T2. ANOVA revealed a significant overall difference (F(2) = 7.464, p = 0.008), with post hoc comparisons indicating significant reductions between T0 and T1 (p = 0.011) and T0 and T2 (p = 0.043). Subgroup analysis (Figure 2) revealed no statistical differences at T0 between subgroups based on gender, age, or ethnicity, although differences in mean values were observed. The highest burden score of 40 was reported by a spouse, followed by daughters with a mean of 22.1 and sons with a mean of 23.7, compared to a granddaughter with eight and a friend with 2. Male caregiver burden was also notably higher at 23.7 than in female caregivers at 21.0 (Figure 2). Female caregivers (n = 14) showed similar levels and trends to the total group, with a baseline score of 21.0, which decreased to 16.0 at 1 month and 15.2 at 2 months (p = 0.025). Caregivers over 60 reported a higher caregiver burden at all three time points compared to those under 60, although the differences were not statistically significant. The older adult subgroup began with the highest burden score of 25.0 at baseline, which decreased to 18.9 at 1 month and 16.1 at 2 months (p = 0.01). These findings suggest a significant reduction in caregiver burden over time across all groups, with the greatest benefit observed in the older adult caregiver subgroup.
Figure 2.
Changes in caregiver burden across demographic subgroups over time.* p < 0.05, ** p < 0.01 (statistical significance determined by ANOVA with post hoc test).
Figure 2.
Changes in caregiver burden across demographic subgroups over time.* p < 0.05, ** p < 0.01 (statistical significance determined by ANOVA with post hoc test).
Regarding quality of life, the mean increased from 29.9 ± 6.93 at T0 to 31.6 ± 6.55 at T1 and 32.2 ± 7.62 at T2. Although ANOVA showed a significant overall difference (F(2) = 4.024, p = 0.027), post hoc comparisons did not reveal significant differences between any pair of time points (Table 4). Subgroup analysis (Figure 3) indicated similar trends across different demographic groups without statistically significant differences, regardless of gender or ethnicity. Male residents and White residents consistently reported higher quality of life scores than female and Asian counterparts without statistically significant differences.
For resident loneliness scores, the mean decreased from 11.1 ± 3.43 at T0 to 9.9 ± 2.99 at T1 and slightly to 9.8 ± 2.73 at T2 (F(2) = 4.084, p = 0.026), with no further significant pairwise differences found between any time points (Table 4). Subgroup analysis (Figure 4) revealed a similar pattern across all groups. Specifically, within the ethnic subgroups, Asian residents experienced a greater decrease in loneliness, with scores dropping from 12.5 at T0 to 10.7 at T1, followed by a slight increase to 11.0 at T2 (p = 0.030). In contrast, the White subgroup did not report a reduction in loneliness at T1 but showed a significant decrease at T2, which differed from the trend observed in other subgroups. No significant differences in loneliness scores were found between male and female subgroups. These findings suggest that while loneliness decreased over time for all groups, the changes varied by ethnicity, with White residents showing a delayed improvement in loneliness.
Overall, a reduction in caregiver burden, improvement in quality of life and loneliness were reported during the implementation of the telepresence robot. Most of these improvements occurred within the first month after initiation and were sustained through the second month.
3.2. Qualitative Results
The data analysis of the qualitative data generated three themes on the impact of telepresence robots on residents and family caregivers (Refer to Table 5 for a summary of themes).
3.2.1. Impact on Residents
Promotes Connections and Nurtures Closeness
With their function for video calls, telepresence robots connect residents with their families and friends, spanning multiple generations. Family caregivers described sharing everyday experiences such as artwork, music, and family events. One family caregiver who lived far from the care home shared how she showed her artwork and played ukulele for her dad through the telepresence robot. She said, “He can get a feel of what is going on in my life.” (Candy, daughter of resident, White, Sunflower Residence). Residents expressed joy and closeness when engaging with the robot. A resident shared, “I have four grandchildren. Two of them will call in through the robot. I am happy when they call in. Usually, we will talk for a long time” (Winky, a resident, Asian, Tulip Residence). A family caregiver shared family moments through the robot with her father. She expressed, “When I show him the Christmas tree and different things going on in my life, he is happy. There’s one time when my sister showed my dad her daughter’s dance show, dancing ballet, my dad is happy.” (Cecilia, daughter of a resident, Asian, Tulip Residence)
Residents also preferred visual interactions offered by robots compared to traditional phone calls. For example, a resident stated, “The robot allows me to see the face of my daughter. Yea, I feel somehow happy with seeing my daughter. There are some differences between the phone and the robot as I can see her.” (Cherry, a resident, Asian, Tulip Residence)
Provides Meaningful Engagement
Telepresence robots offered residents opportunities for meaningful interactions and conversations, significantly reducing feelings of isolation. A resident expressed, “There are no people that I can chat with [in the care home]. On the robot, my granddaughter will ask me where I feel pain. I feel happy to talk to her through the robot.” (Winky, a resident, Asian, Tulip Residence). A daughter shared, “With more frequent calls through the robot, my dad can recall our conversations. He can chat and talk forever. It feels like an in-person visit to him” (Flora, daughter of a resident, White, Rose Residence). One caregiver described how frequent robot interactions enhanced a resident’s “sense of self and self-worth.” Another emphasized how visual interaction helped adapt communication strategies effectively. A family member shared, “The robot has helped in such a way that I can see her [the resident] when I’m asking her a question. I can see if she’s struggling with the answer, and then that means that I need to rephrase the question or talk about something different maybe” (Shereen, daughter of a resident, White, Sunflower Residence).
Acknowledges Robots’ Limitations
A few family members voiced the limitations of telepresence robots. As the family caregivers are the main controllers of the telepresence robots, the residents cannot initiate calls. The residents’ role is more passive in the call via telepresence robots. Therefore, some residents recognized the lack of control over the robot. A resident remarked, “If I don’t have the robot, that’s no big deal to me because I didn’t have this robot in my whole life. I can use the phone to call my family.” (Paul, a resident, Asian, Tulip Residence) Another resident commented, “The robot will move towards me when I am sitting. I don’t know how to use the robot. I feel annoyed with myself. I feel helpless. I feel useless. I have so much pain in my legs. No one can help me, not even the robot” (Cherry, a resident, Asian, Tulip Residence).
3.2.2. Impact on Family Caregivers
Reduces Stress and Guilt
Family caregivers reported the robot reduced stress and guilt associated with challenges in visiting care homes, especially during adverse weather and personal illness. Telepresence robots provided a practical alternative, easing caregiving burdens. One caregiver shared relief over less commuting, stating, “With the snow, I am not able to see her [the resident] for a while. I think about her [the resident] sitting in the nursing home by herself” (Catherine, friend of a resident, White, Jasmine Residence). Another family caregiver said, “I felt bad not seeing him [the resident] every day as he was expecting me. After I had been sick, it was becoming more challenging to maintain my visits at such a high frequency” (Lily, wife of a resident, White, Jasmine Residence). A resident’s son said, “The key benefit of the robot is time-saving for commute. The robot helps me to show up and be there more with my father” (Jeffrey, son of a resident, Asian, Tulip Residence). Another described, “The robot helps with relieving the pressure of driving. I have two young kids, and it’s hard having the time to drive to him [the resident] with two hours of travelling back and forth” (Janice, daughter of a resident, White, Zinnia Residence). Another family caregiver also shared how the telepresence robot supported her “visits to her mum” when she was sick. She said, “I was sick three weeks ago. I had a fever. Thank goodness! I have the [telepresence] robot. I can visit my mom.” (Ruby, daughter of a resident, Asian, Tulip Residence).
Enables Continuity in Caregiver’s Role and Complements In-Person Visits
Transferring to LTC homes can be a challenging transition period for residents and family caregivers. Family caregivers are usually highly involved in residents’ care before they move into LTC homes. Many caregivers in our study described how telepresence robots support the continuation of their caregiving roles and their involvement in the care of residents in LTC homes.
A daughter of a resident illustrated the continuity of her caregiving role and adaptation to the LTC routines of residents with the telepresence robot. She shared, “The robot helps with the feeling that I am still looking after Mom, seeing what she’s doing, and making sure that she knows that I am around. I can go on the robot and see her. And I know her routine. At least to say, ‘Hello mum’.” (Ruby, daughter of a resident, Asian, Tulip Residence)
A resident’s son also shared how he supported staff in the resident’s care. He said, “Before, when the staff was helping my dad, he would get very scared because he didn’t know who they were. With the telepresence robot, I am able to call in and help tell him who those people [the staff] are, and he feels better. He knows that his family is around, and he can calm down. I can show up on the robot and be there on demand.” (Jeffrey, son of a resident, Asian, Tulip Residence)
A family caregiver shared how telepresence robots allowed them to advocate for their loved ones in LTC for staff support during the COVID-19 pandemic. She shared, “The robot was really good when she [the resident] was confined because of the COVID outbreak on that floor [of the LTC home]. I went in [to the resident’s room] through the robot and found out that she [The resident] was confused and quite distressed. After I got off [logged out] from the robot, I asked the staff to talk to Ila. It was helpful as I could not go into the nursing home.” (Catherine, friend of a resident, White, Jasmine Residence)
Notably, most family caregivers emphasized that despite the presence of telepresence robots, they were still eager to visit their loved ones and have a personal touch. The telepresence robots were supplements to their in-person visits. A family caregiver emphasized, “Even though with the robot, I still come three times a week to visit the care home. The robot doesn’t replace the time that I need to come to the care home.” (Ruby, daughter of a resident, Asian, Tulip Residence) Another family caregiver echoed the preference of his mother, “The robot is a great addition. For my mom, she would prefer an in-person visit.” (Louis, son of a resident, Asian, Rose Residence)
Offers Reassurance on Residents’ Quality of Life
The telepresence robots helped reassure family caregivers about enhancing residents’ quality of life in LTC. One family caregiver shared, “The staff told me that [name of resident] is calmer and not as lonely, more settled.” (Lily, wife of a resident, White, Jasmine Residence) Another family caregiver described, “The robot really helps with his spirits and everything. It’s obviously better.” (Nancy, daughter of a resident, Asian, Jasmine Residence)
Knowing the benefits of the telepresence robots on residents had a positive impact on the caregivers. One of them smiled and said, “I think it helps mum…it really does help mum. She is quite happy when she sees me, even though I am not in person but on the robot. For me, knowing that Mum is more at ease as she knows that I am around is good for me, too. I feel happier, knowing that Mum is happy seeing me. I can tell that she is happy from her expression. She is not very verbal. For mum, she will be more grounded if she sees me more.” (Ruby, daughter of a resident, Asian, Tulip Residence)
4. Discussion and Implication
This study examined the impact of a telepresence robot intervention on family caregiver burden, residents’ quality of life, and loneliness. The findings demonstrated a significant reduction in caregiver burden, particularly during the first month of implementation, indicating immediate relief through improved communication, reduced logistical challenges, and increased reassurance for caregivers. Our qualitative insights reinforced the quantitative results, revealing reduced caregiver stress and guilt as caregivers provided emotional support and reduced residents’ anxiety using the telepresence robots. These findings align with Marvardi et al. [33], who highlighted caregiver burden as primarily influenced by residents’ behavioral disturbances and disability, alongside caregiver anxiety and depression [33]. Their findings align with our qualitative themes, which highlight the reduction of caregiver burden when caregivers could help decrease residents’ anxiety, calm the residents down and provide emotional support for residents through calling in with the telepresence robot. Importantly, while caregivers in our study emphasized that telepresence robots would not replace in-person visits, these robots offered additional benefits, such as reducing travel time, which reduced caregivers’ stress and guilt.
Previous research identified caregiver burden as closely related to residents’ neuropsychiatric symptoms and caregivers’ competence, with emotional burdens exacerbated by residents’ high affiliation and caregiver gender [34]. Our findings partially supported these conclusions. The highest burden scores in our study were reported by one individual spouse and older caregivers’ subgroup, aligning with earlier findings by Rinaldi et al. [35], in which older caregivers experience stress levels three times higher than younger groups, and children or spouses report burden-distress five to six times higher than other relatives. Although our study did not find statistically significant differences based on residents’ gender or caregiver affiliation due to the limited sample size, the highest burden score was reported by a spouse, followed by daughters and sons, compared to a granddaughter and a friend, which aligns with the above two research studies [34,35]. Notably, male caregivers reported higher initial burden levels than female caregivers, which is also consistent with prior research [35]. Older caregivers, who initially reported the highest burden, demonstrated the greatest reduction in burden following the intervention. This trend suggests that older caregivers, often facing higher stress and physical strain, may benefit most from interventions that ease perceived caregiving demands. An older adult spouse in our study expressed that hospitalization was once a barrier for her to visit the care home, which led to the feeling of guilt. Her physical decline since then also impacted the frequency with which she could visit the care home. While gender, age, and ethnicity did not significantly affect how caregivers reflected on their burden at the baseline, female caregivers and those over 60 appeared particularly receptive to technological support. This contributes new insights by showing that communication technology, like telepresence robots, plays a role in reducing caregiver burden alongside previously identified determinants like residents’ neuropsychiatric symptoms and caregivers’ competence. Our qualitative findings further support this conclusion, highlighting that relief from guilt and stress, reassurance from long-term care homes, and mediation in residents’ care planning—with the support and availability of telepresence robots as a communication technology—all contribute to alleviating caregiver burden.
Regarding residents’ quality of life and loneliness, a gradual improvement in the quality of life and reduction of loneliness was observed over time in our study, with the most significant changes within the first month. Due to the limited sample size, post hoc comparisons did not reveal statistically significant differences between time points. One research reported loneliness is closely associated with the quality of life in older adults [36], which aligned with our findings. Although one recent scoping review reported seldom studies focusing on the impact of assistive technology on the loneliness of residents with dementia [37], only one study in this review shows promising results of assistive technologies —not telepresence robots— which can reduce loneliness in people with dementia in long-term care [38]. Telepresence robots were reported in one review of their potential to enhance social connection, which contributes to the reduction of loneliness [39]. Our qualitative interviews also echoed this potential with the experiences using the telepresence robot shared by residents and family caregivers. For example, telepresence robots brought these individuals a sense of closeness, connected residents with their children, grandchildren, and even great-grandchildren, and allowed the sharing of instant life story updates between family caregivers and residents. Besides loneliness, the changes in quality of life were possibly influenced by additional factors such as resident’s baseline health conditions, social engagement, and individual preferences for virtual communication [40,41]. The qualitative data also reported and acknowledged the limitations of the telepresence robots’ impact on residents’ physical health and energy levels despite the other benefits they brought to residents’ and caregivers’ lives. Interestingly, male and White residents reported higher quality of life scores than their female and non-white counterparts, which may suggest potential cultural or gender-related variations in how residents perceive and engage with telepresence technology, requiring further investigation into individualized interventions tailored to different demographic groups.
For practice implications, the study suggests that telepresence robots can be a valuable tool for supporting family caregivers, particularly older caregivers who reported the highest initial burden. The sustained decrease in burden over time indicates that continuous use of telepresence robots may offer long-term benefits. Implementing these robots could assist caregivers who face emotional stress and logistical challenges. Given the positive outcomes for both residents and caregivers, policymakers and LTC administrators can consider integrating such technologies to enhance the well-being of residents and their families. The study also offers insights into the target populations that may best benefit from the use of telepresence robots. With limited resources, LTC administrators can explore how these technologies can be best used in their organizations, such as shared use of the robots or for residents who have older adult spouses or children. Furthermore, while the robots facilitate improved social connections, they should be used as a supportive, complementary communication tool rather than replacing the need for in-person visits.
For research implications, further studies should examine the long-term sustainability of the effects observed in this study regarding the reduction in caregiver burden, residents’ level of loneliness and the improvement in residents’ quality of life. Given the potential differences observed in subgroups, future research should include larger sample sizes and more rigorous study designs to better identify and target the most likely beneficiaries. Additionally, since the quality of life may be influenced by multiple factors, such as ethnocultural backgrounds and gender, further exploration of the relationship between telepresence robots and these determinants is warranted to understand their broader impact in detail. With the significant impact of telepresence robots on the older adult group, researchers can explore the potential challenges of using these technologies and strategies to best support older caregivers in using these robots. Researchers can also explore further the support of telepresence robots on intergenerational bonding between residents and their grandchildren.
Strengths and Limitations
This study utilized a mixed methods approach, which combines both qualitative and quantitative data to provide a more comprehensive understanding of the research problem. Our research team is composed of a diverse group of multidisciplinary researchers and trainees with expertise in nursing, medicine, occupational therapy, biomedical engineering, and social work, contributing to a more comprehensive investigation. Additionally, the team includes patient partners and family caregivers, who contributed their lived experience to this study. This engagement helps to ensure that our interventions and findings are relevant, practical, and sensitive to the needs of the participant.
Our study has the following limitations. This pre-post design study relies on each participant serving as their own control, which can increase statistical power with smaller sample sizes. However, the absence of a control group means that it is difficult to definitively attribute changes in outcomes solely to the intervention. For the quantitative study part, our sample size was constrained by the number of robots available. We have 20 robots in total. Further, our study was conducted in five different LTC homes based in urban areas of West Canada. The unique context may not be transferrable to LTC homes in rural areas or in other countries. Lastly, since finalizing this paper, our team has found out that the company that developed the telepresence robots used in our project has dissolved. Nevertheless, the findings were significant and important enough to highlight the positive outcomes benefiting residents in LTC. The findings published can provide insights for adopting or developing other similar products to be used in the long-term and facilitate the socialization of residents, their families and friends in LTC homes.
5. Conclusions
This two-month telepresence robot intervention demonstrated the potential to reduce family caregiver burden, enhance quality of life and improve loneliness in residents living with dementia in LTC homes. From the residents’ perspectives, the telepresence robot fosters a sense of connection, nurtures closeness, and provides meaningful engagement. From the families’ perspective, telepresence robots enable continuity in care, complement in-person visits, reduce stress and guilt, and offer comfort by reassurance of residents’ well-being, with older caregivers as the greatest beneficiaries. The study offers insights for policymakers and LTC administrators in planning and considering the adoption of similar technologies. Future research could explore the long-term impacts on the well-being of residents and their families, the impact of different factors on residents’ and family care partners’ perceptions of telepresence robots, how to better support older adult caregivers in using telepresence robots, and the robots’ potential in supporting intergenerational connections.
Supplementary Materials
Author Contributions
Conceptualization, L.H. and J.M.; methodology, L.H..; formal analysis, L.H., J.W., L.R., L.L., and Y.Z.; data curation, J.W. and Y.Z.; writing—original draft preparation, J.W., L.R., L.L., J.F., and Y.Z.; writing—review and editing, L.H. and J.M.; supervision, L.H. and L.L.; project administration, J.W. and L.R.; funding acquisition, L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Vancouver Foundation Participatory Action Research (PAR), grant number GR019971, Vancouver General Hospital Foundation and Richmond Hospital Foundation.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Behavioral Research Ethics Board of the University of British Columbia (H22-02402).
Informed Consent Statement
Written informed consent and assent were obtained from all subjects involved in the study. Informed consent and assent have been obtained from residents and family partners to publish this paper.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Acknowledgments
We extend our heartfelt gratitude to the residents, families, and staff of the long-term care homes for their invaluable contributions to this study.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ANOVA | Analysis of variance |
| LTC | Long-term care |
| PI | Principal investigator |
| QOL-AD | Quality of Life –Alzheimer’s Disease |
References
- White, E.M.; Wetle, T.F.; Reddy, A.; Baier, R.R. Front-Line Nursing Home Staff Experiences During the COVID-19 Pandemic. J Am Med Dir Assoc 2021, 22, 199–203. [CrossRef]
- Drageset, J.; Kirkevold, M.; Espehaug, B. Loneliness and Social Support among Nursing Home Residents without Cognitive Impairment: A Questionnaire Survey. Int J Nurs Stud 2011, 48, 611–619. [CrossRef]
- Paque, K.; Bastiaens, H.; Van Bogaert, P.; Dilles, T. Living in a Nursing Home: A Phenomenological Study Exploring Residents’ Loneliness and Other Feelings. Scand J Caring Sci 2018, 32, 1477–1484. [CrossRef]
- Dahlberg, L.; Andersson, L.; McKee, K.J.; Lennartsson, C. Predictors of Loneliness among Older Women and Men in Sweden: A National Longitudinal Study. Aging Ment Health 2015, 19, 409–417. [CrossRef]
- Wright, M.R.; Hammersmith, A.M.; Brown, S.L.; Lin, I.-F. The Roles of Marital Dissolution and Subsequent Repartnering on Loneliness in Later Life. The Journals of Gerontology: Series B 2020, 75, 1796–1807. [CrossRef]
- de Boise, S.; Hearn, J. Are Men Getting More Emotional? Critical Sociological Perspectives on Men, Masculinities and Emotions. Sociol Rev 2017, 65, 779–796. [CrossRef]
- Kemperman, A.; van den Berg, P.; Weijs-Perrée, M.; Uijtdewillegen, K. Loneliness of Older Adults: Social Network and the Living Environment. Int J Environ Res Public Health 2019, 16, 406. [CrossRef]
- Mueller, A.; Beach, S.R.; Bowers, B.J.; Fields, B. Relationship between Health Care Interactions and Care Partner Burden. Families, Systems, & Health 2022, 40, 225–231. [CrossRef]
- Fowler, J.; Blundell, B.; Morrisby, C.; Hendrick, A. ‘You’ve Got No Support’: The Experiences of Older Male Caregivers When Their Partner Enters Residential Care. J Gerontol Soc Work 2022, 65, 529–544. [CrossRef]
- Crawford, K.; Digby, R.; Bloomer, M.; Tan, H.; Williams, A. Transitioning from Caregiver to Visitor in a Long-Term Care Facility: The Experience of Caregivers of People with Dementia. Aging Ment Health 2015, 19, 739–746. [CrossRef]
- Street, D.; Burge, S.; Quadagno, J.; Barrett, A. The Salience of Social Relationships for Resident Well-Being in Assisted Living. J Gerontol B Psychol Sci Soc Sci 2007, 62, S129–S134. [CrossRef]
- Zamir, S.; Hennessy, C.H.; Taylor, A.H.; Jones, R.B. Video-Calls to Reduce Loneliness and Social Isolation within Care Environments for Older People: An Implementation Study Using Collaborative Action Research. BMC Geriatr 2018, 18, 62. [CrossRef]
- Chu, C.H.; Yee, A.; Stamatopoulos, V. Poor and Lost Connections: Essential Family Caregivers’ Experiences Using Technology with Family Living in Long-Term Care Homes during COVID-19. Journal of Applied Gerontology 2022, 41, 1547–1556. [CrossRef]
- Double Robotics. Double 3. The Future of Work Is Hybrid. Available online: https://www.doublerobotics.com (accessed on 10 March 2025).
- Hu, G.; Wong, J.; Ren, L.H.; Kleiss, S.; Berndt, A.; Wong, L.; Hussein, A.; Ahmed, N.; Mann, J.; Hung, L. Care Partner Experience with Telepresence Robots in Long-Term Care during COVID-19 Pandemic. Digit Health 2025, 11. [CrossRef]
- Hung, L.; Hu, G.; Wong, J.; Ren, H.; Ahmed, N.; Hussein, A.; Young, E.; Berndt, A.; Mann, J.; Corepal, R.; et al. Telepresence Robots in Long-Term Care Settings in British Columbia During the COVID-19 Pandemic: Analyzing the Experiences of Residents and Family Members. Gerontol Geriatr Med 2023, 9. [CrossRef]
- Niemelä, M.; van Aerschot, L.; Tammela, A.; Aaltonen, I.; Lammi, H. Towards Ethical Guidelines of Using Telepresence Robots in Residential Care. Int J Soc Robot 2021, 13, 431–439. [CrossRef]
- Moyle, W.; Jones, C.; Cooke, M.; O’Dwyer, S.; Sung, B.; Drummond, S. Connecting the Person with Dementia and Family: A Feasibility Study of a Telepresence Robot. BMC Geriatr 2014, 14, 7. [CrossRef]
- Teddlie, C.; Tashakkori, A. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences; Sage: Los Angeles, 2009.
- Hitchcock, J.H.; Onwuegbuzie, A.J. The Routledge Handbook for Advancing Integration in Mixed Methods Research; Routledge: London, 2022; ISBN 9780429432828.
- Ivankova, N. V.; Creswell, J.W.; Plano Clark, V.L. Foundations and Approaches to Mixed Methods Research. In First steps in research; Van Schaik publishers: Pretoria, 2016; pp. 305–336.
- Shorten, A.; Smith, J. Mixed Methods Research: Expanding the Evidence Base. Evidence Based Nursing 2017, 20, 74–75. [CrossRef]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; 5th ed.; SAGE Publications, 2018.
- Bédard, M.; Molloy, D.W.; Squire, L.; Dubois, S.; Lever, J.A.; O’Donnell, M. The Zarit Burden Interview. Gerontologist 2001, 41, 652–657. [CrossRef]
- De Jong Gierveld, J.; Van Tilburg, T. The De Jong Gierveld Short Scales for Emotional and Social Loneliness: Tested on Data from 7 Countries in the UN Generations and Gender Surveys. Eur J Ageing 2010, 7, 121–130. [CrossRef]
- Logsdon, R.G.; Gibbons, L.E.; McCurry, S.M.; Teri, L. Assessing Quality of Life in Older Adults With Cognitive Impairment. Psychosom Med 2002, 64, 510–519. [CrossRef]
- Olson, K. Essentials of Qualitative Interviewing.; Left Coast Press: Walnut Creek, 2011.
- Phillippi, J.; Lauderdale, J. A Guide to Field Notes for Qualitative Research: Context and Conversation. Qual Health Res 2018, 28, 381–388. [CrossRef]
- Els, R.C.; Meyer, H.W. The Influence of Leaders’ Attitudes and Commitment to Quality Management of Training on Organisational Excellence: A Mixed-Methods Study. Human Resource Development International 2025, 28, 79–109. [CrossRef]
- Braun, V.; Clarke, V. Reflecting on Reflexive Thematic Analysis. Qual Res Sport Exerc Health 2019, 11, 589–597. [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual Res Psychol 2006, 3, 77–101. [CrossRef]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving Integration in Mixed Methods Designs—Principles and Practices. Health Serv Res 2013, 48, 2134–2156. [CrossRef]
- Marvardi, M.; Mattioli, P.; Spazzafumo, L.; Mastriforti, R.; Rinaldi, P.; Polidori, M.C.; Cherubini, A.; Quartesan, R.; Bartorelli, L.; Bonaiuto, S.; et al. The Caregiver Burden Inventory in Evaluating the Burden of Caregivers of Elderly Demented Patients: Results from a Multicenter Study. Aging Clin Exp Res 2005, 17, 46–53. [CrossRef]
- van der Lee, J.; Bakker, T.J.E.M.; Duivenvoorden, H.J.; Dröes, R.-M. Do Determinants of Burden and Emotional Distress in Dementia Caregivers Change over Time? Aging Ment Health 2017, 21, 232–240. [CrossRef]
- Rinaldi, P.; Spazzafumo, L.; Mastriforti, R.; Mattioli, P.; Marvardi, M.; Polidori, M.C.; Cherubini, A.; Abate, G.; Bartorelli, L.; Bonaiuto, S.; et al. Predictors of High Level of Burden and Distress in Caregivers of Demented Patients: Results of an Italian Multicenter Study. Int J Geriatr Psychiatry 2005, 20, 168–174. [CrossRef]
- Vespa, A.; Spatuzzi, R.; Fabbietti, P.; Di Rosa, M.; Bonfigli, A.R.; Corsonello, A.; Gattafoni, P.; Giulietti, M.V. Association between Sense of Loneliness and Quality of Life in Older Adults with Multimorbidity. Int J Environ Res Public Health 2023, 20, 2615. [CrossRef]
- Budak, K.B.; Atefi, G.; Hoel, V.; Laporte Uribe, F.; Meiland, F.; Teupen, S.; Felding, S.A.; Roes, M. Can Technology Impact Loneliness in Dementia? A Scoping Review on the Role of Assistive Technologies in Delivering Psychosocial Interventions in Long-Term Care. Disabil Rehabil Assist Technol 2023, 18, 1107–1119. [CrossRef]
- Robinson, H.; MacDonald, B.; Kerse, N.; Broadbent, E. The Psychosocial Effects of a Companion Robot: A Randomized Controlled Trial. J Am Med Dir Assoc 2013, 14, 661–667. [CrossRef]
- Moyle, W.; Arnautovska, U.; Ownsworth, T.; Jones, C. Potential of Telepresence Robots to Enhance Social Connectedness in Older Adults with Dementia: An Integrative Review of Feasibility. Int Psychogeriatr 2017, 29, 1951–1964. [CrossRef]
- Beridze, G.; Ayala, A.; Ribeiro, O.; Fernández-Mayoralas, G.; Rodríguez-Blázquez, C.; Rodríguez-Rodríguez, V.; Rojo-Pérez, F.; Forjaz, M.J.; Calderón-Larrañaga, A. Are Loneliness and Social Isolation Associated with Quality of Life in Older Adults? Insights from Northern and Southern Europe. Int J Environ Res Public Health 2020, 17, 8637. [CrossRef]
- Boehlen, F.H.; Maatouk, I.; Friederich, H.-C.; Schoettker, B.; Brenner, H.; Wild, B. Loneliness as a Gender-Specific Predictor of Physical and Mental Health-Related Quality of Life in Older Adults. Quality of Life Research 2022, 31, 2023–2033. [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. International Journal for Quality in Health Care 2007, 19, 349–357. [CrossRef]
- O’cathain, A.; Murphy, E.; Nicholl, J. The Quality of Mixed Methods Studies in Health Services Research. J Health Serv Res Policy 2008, 13, 92–98. [CrossRef]
Figure 1.
Convergent parallel mixed-methods approach used in this study.
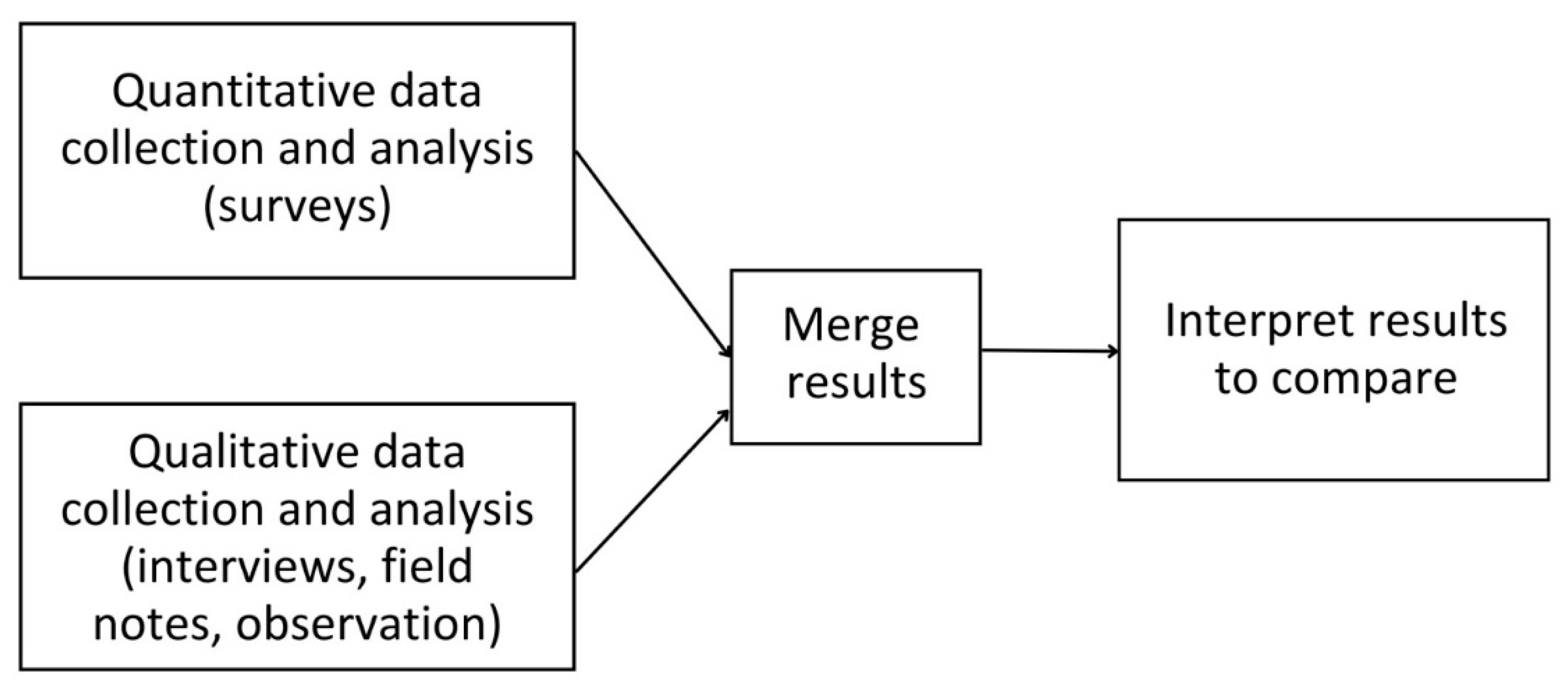
Figure 2.
Timeline for data collection for an individual participant.
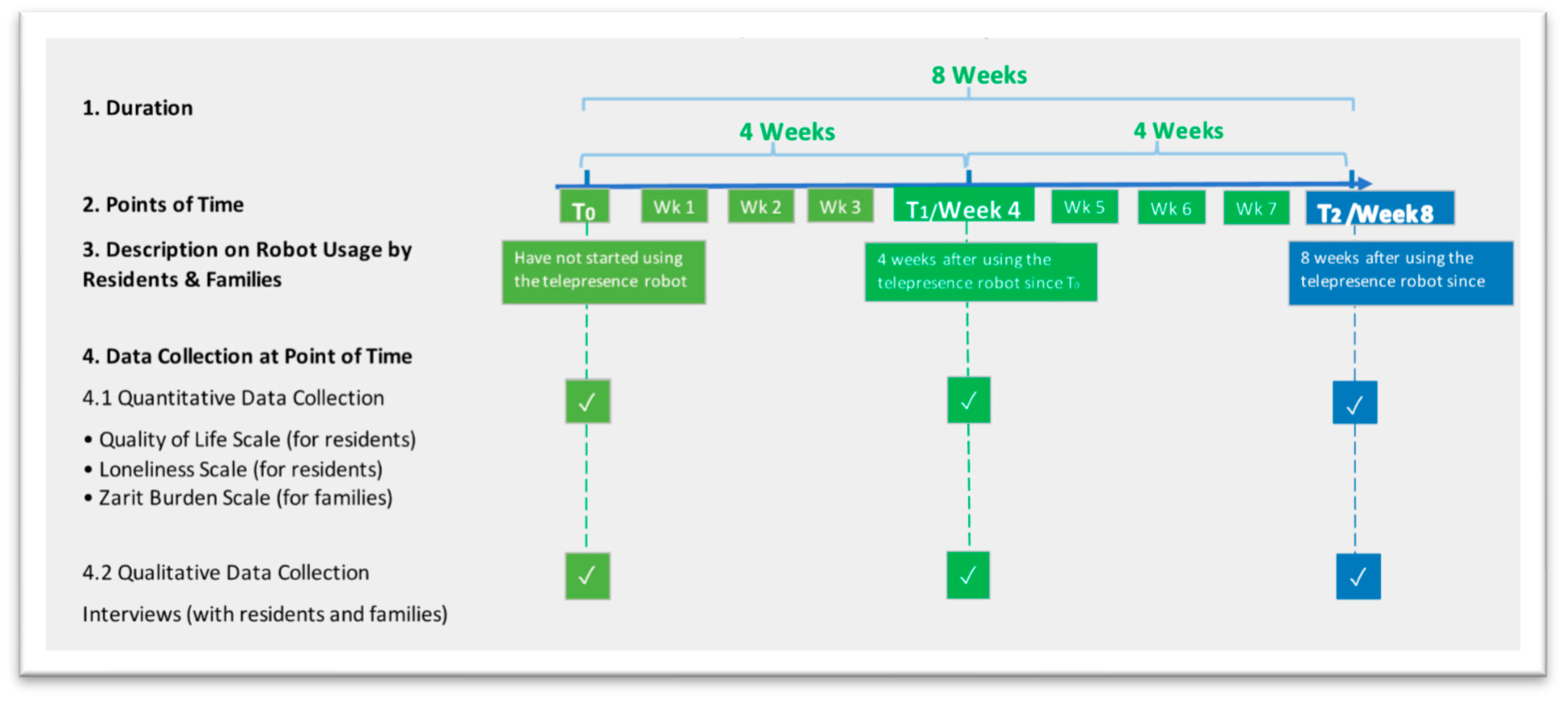
Figure 3.
Changes in quality of life across demographic subgroups over time. * p < 0.05 (statistical significance determined by ANOVA).
Figure 3.
Changes in quality of life across demographic subgroups over time. * p < 0.05 (statistical significance determined by ANOVA).
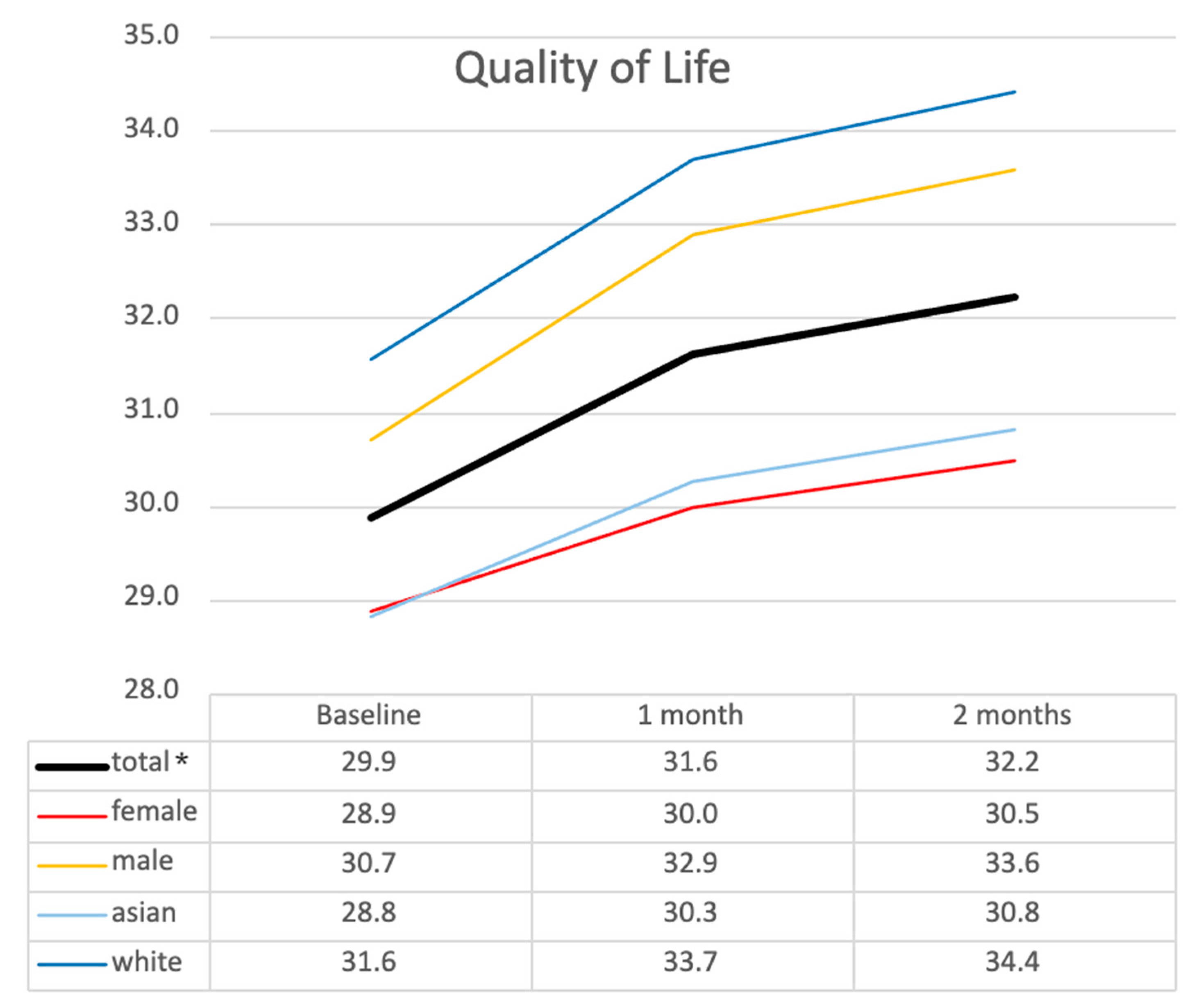
Figure 4.
Changes in loneliness across demographic subgroups over time. * p < 0.05 (statistical significance determined by ANOVA).
Figure 4.
Changes in loneliness across demographic subgroups over time. * p < 0.05 (statistical significance determined by ANOVA).
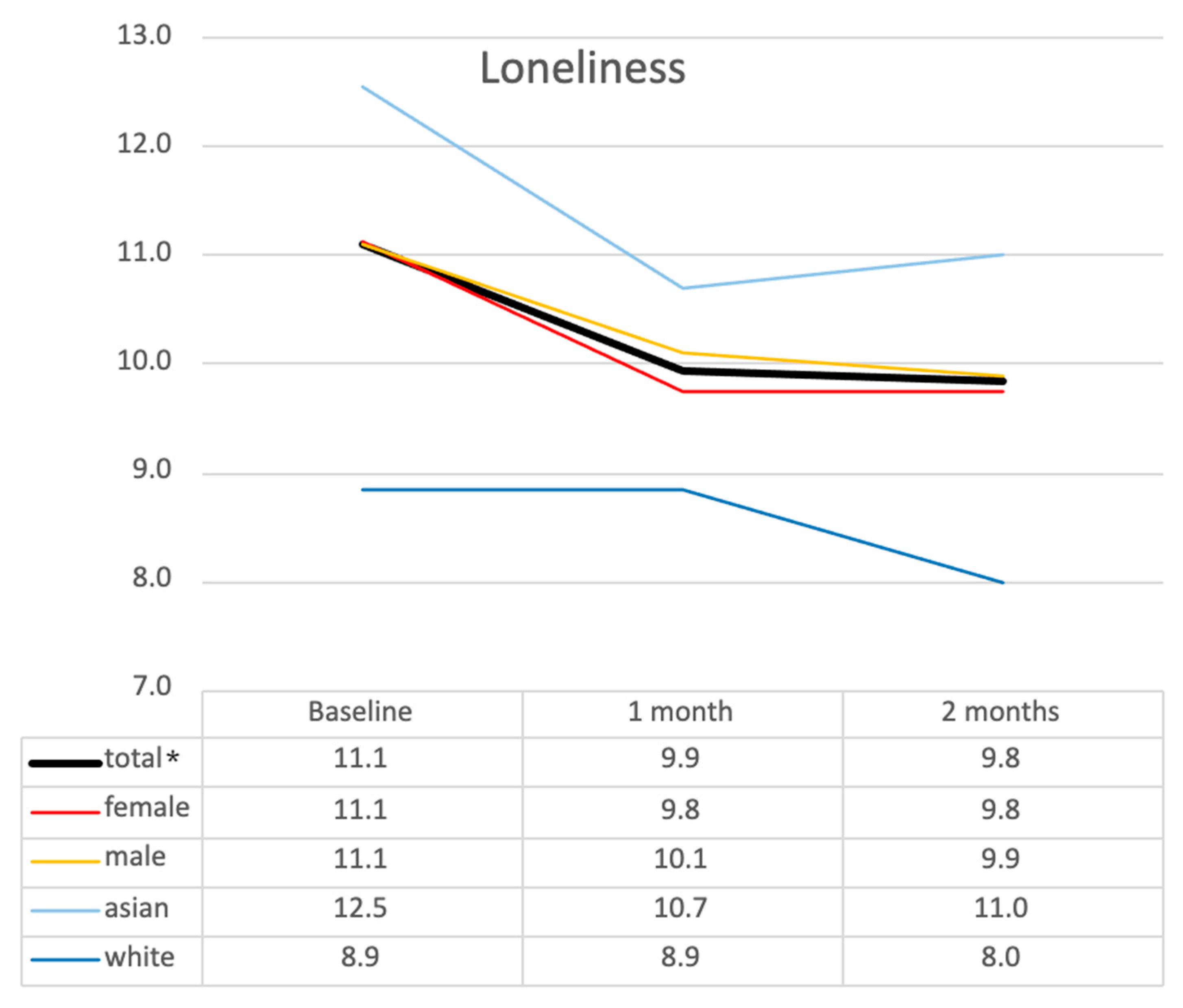

Table 1.
Detailed information of partnered care sites: types of rooms, staff-resident ratio and funding.
Table 1.
Detailed information of partnered care sites: types of rooms, staff-resident ratio and funding.
| Pseudonym of LTC Site | Types of Room Available | Staff-Resident Ratio | Funding |
|---|---|---|---|
| Jasmine Residence | Individual and Shared Room | Day: 1 staff member to 6 residents | Publicly funded |
| Evening: 1 staff member to 20 residents | |||
| Rose Residence | Individual and Shared Room | Day: 1 staff member to 6 residents | Publicly funded |
| Evening: 1 staff member to 8 residents | |||
| Night: 1 staff member to 25 residents | |||
| Zinnia Residence | Individual Room | Day: 3 nurses and 4 care aides (7 staff in total to 19 residents) | Publicly funded |
| Evening: 3 nurses and 3 care aides (6 staff in total to 19 residents) | |||
| Night: 2 nurses and 2 care aides (4 staff to 19 residents) | |||
| Tulip Residence | Individual Room | Day: 1 nurse and 2 to 3 care aides for 16 to 17 residents | Non-profit |
| Evening: 1 nurse and 2 to 3 care aides for 16 to 17 residents | |||
| Night: 1 staff (nurse or care aid) per care neighbourhood (16–27 residents) | |||
| Sunflower Residence | Individual Room | Long-term care: 1 Resident Care partner for 5–6 residents | Privately funded, for-profit |
Table 2.
Examples of coding.
| Quotes | Codes | Themes |
|---|---|---|
| The robot helps with relieving the pressure of driving and commuting. I have two young kids, and it’s hard having the time to drive to him [the resident] with two hours of travelling back and forth. It had been a hard time making time for myself and my kids… and it’s hard to see my dad. The robot visits help save us time for commuting |
|
Reduces Stress and Guilt |
| She [My granddaughter] will ask me where I feel pain. I feel happy to talk to her through the robot. |
|
Provides Meaningful Engagement |
Table 3.
Demographic characteristics of participants (n=35).
| Residents | Families | ||
|---|---|---|---|
| Gender | |||
| Male | 10 (55.6%) | Male | 3 (17.6%) |
| Female | 8 (44.4%) | Female | 14 (82.3%) |
| Age group | |||
| 61-70 years | 1 (5.6%) | 21-40 years | 2 (11.8%) |
| 71-80 years | 5 (27.8%) | 31-50 years | 4 (23.5%) |
| 81- years | 12 (66.7%) | 51-60 years | 4 (23.5%) |
| 61-70 years | 5 (29.4%) | ||
| 71-80 years | 2 (11.8%) | ||
| Ethnicity | |||
| White | 7 (38.9%) | White | 7 (41.2%) |
| Asian | 11 (61.1%) | Asian | 10 (58.8%) |
| Relationships | |||
| Daughter | 11 (64.7%) | ||
| Son | 3 (17.6%) | ||
| Spouse | 1 (5.9%) | ||
| Granddaughter | 1 (5.9%) | ||
| Friend | 1 (5.9%) | ||
| Total | 18 | Total | 17 |
Table 4.
Changes in caregiver burden, quality of life, and loneliness over time.
| Time Points | Mean ± SD | ANOVA F(df), P-value | Post Hoc Comparison (P-value) | |
|---|---|---|---|---|
| Caregiver Burden | T0 | 21.5 ± 11.09 | F(2) = 7.464, p = 0.008** | T0 vs. T1 (p = 0.011)* |
| T1 | 16.5 ± 7.92 | T0 vs. T2 (p = 0.043)* | ||
| T2 | 15.8 ± 7.68 | T1 vs. T2 (p = 1.000) | ||
| Quality of Life | T0 | 29.9 ± 6.93 | F(2) = 4.024, p = 0.027* | T0 vs. T1 (p = 0.109) |
| T1 | 31.6 ± 6.55 | T0 vs. T2 (p = 0.124) | ||
| T2 | 32.2 ± 7.62 | T1 vs. T2 (p = 1.000) | ||
| Loneliness | T0 | 11.1 ± 3.43 | F(2) = 4.084, p = 0.026* | T0 vs. T1 (p = 0.120) |
| T1 | 9.9 ± 2.99 | T0 vs. T2 (p = 0.085) | ||
| T2 | 9.8 ± 2.73 | T1 vs. T2 (p = 1.000) |
Note: ANOVA p-values indicate overall differences across time points. Post hoc comparisons were performed using Bonferroni correction. T0 = Baseline, T1 = 1 Month Follow-Up; T2 = 2 Month Follow-Up. *p < 0.05, **p < 0.01.
Table 5.
Summary of themes.
| Impact on Residents | Impact on Family Caregivers |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



