
Submitted:
18 March 2025
Posted:
18 March 2025
You are already at the latest version
Abstract
Objective: We aimed to explore the relevance of uncertain resection in lung cancer. Methods: We performed an exhaustive literature review of all studies comparing prognosis after resection according to IASLC classification. Results: Systematic review led to select 68 original studies included in this review. R(un) reclassification was mostly caused by a lack of hilar or mediastinal node dissection, or because of metasta-sis in the highest node. R(un) is a strong factor for higher recurrence and mortality, while its effects seem limited in early stages. Carcinoma in situ at bronchial margin resection (CIS BRM) does not show effect on survival, while positive pleural cytology (Cy+) and positive highest mediastinal lymph node (HMLN+) appear to be highly pre-dictive of recurrence and death. Conclusion: The R(un) classification of the IASLC 2005 appears highly relevant, espe-cially in locally advanced stages IIb-IIIA, and helps to discriminate patients with poor prognosis despite being classified as R0 according to UICC classification. The use of this more precise classification would allow for better stratification of recurrence risk and more effective use of adjuvant therapies. Cy+ patients should receive adjuvant chemotherapy, while CIS BRM patients could likely benefit from endoscopic surveil-lance to detect local recurrences. HMLN+ patients should be considered at high risk of recurrence, and adjuvant radiochemotherapy should be considered.
Keywords:
NSCLC
; oncology
; resected lung cancer
; uncertain resection
; mediastinal lymphadenectomy
; IASLC
1. Introduction
Treatment of early and locally advanced stage lung cancer primarily relies on surgical resection with the intention to remove all disease [1,2,3]. The quality of resection is assessed by the R criterion of the UICC TNM classification [4], which is divided into three categories: complete resection (R0), microscopic residue (R1), and macroscopic residue (R2). This criterion is a major prognostic factor and can alone determine access to adjuvant treatments [5,6]. However, a significant portion of resected patients classified as R0 experience recurrence and succumb to their disease, despite well-conducted surgery and apparently complete resection [7,8]. To better identify these at-risk patients, the IASLC proposed a fourth category for the R criterion in 2005: uncertain resection [R(un)] [9]. It includes patients who do not present proven residual tumor but for whom there is doubt about disease persistence. An uncertain resection is defined by a resection with margins proved to be free of disease microscopically, but the intraoperative lymph node evaluation has been less rigorous than systematic nodal dissection or lobe-specific systematic nodal dissection and/or the highest mediastinal node removed is positive (HMLN+) and/or the bronchial margin shows carcinoma in situ (CIS BRM) and/or the pleural lavage cytology is positive (R1 cy+).
According to IASLC classification, lobe specific systematic nodal dissection implies retrieving hilar nodes and, at least, three mediastinal nodal stations depending on the lobar location of the primary tumor, always including subcarinal nodes [7]: For right upper and middle lobes, two of the following three stations: superior paratracheal [2R], inferior paratracheal [4R] and pretracheal [2-4R]. For the right lower lobe, right inferior paratracheal nodes [4R], and either the paraoesophageal [8] or pulmonary ligament nodes [9]. For the left upper lobe, subaortic [5] and anterior mediastinal nodes [6]. For the left lower lobe, paraesophageal [8] and pulmonary ligament nodes [9]. The lymph node specimen should include, at least, six nodes, three removed from N1 stations and three removed from N2 stations.
This classification, which has been released almost twenty years ago, was intended to harmonize the criteria for resection quality on an international scale and to identify a new prognostic group of patients for whom local disease control appears uncertain. However, this classification still seems to be underutilized in practice compared to the classic R0-1-2 triad. As the 9th edition of the TNM is being prepared, an assessment seems necessary. Here, we propose a literature review to evaluate its relevance, focusing on R(un), which provides arguments in favor of a higher risk of recurrence among patients previously classified as R0.
2. Materials and Methods
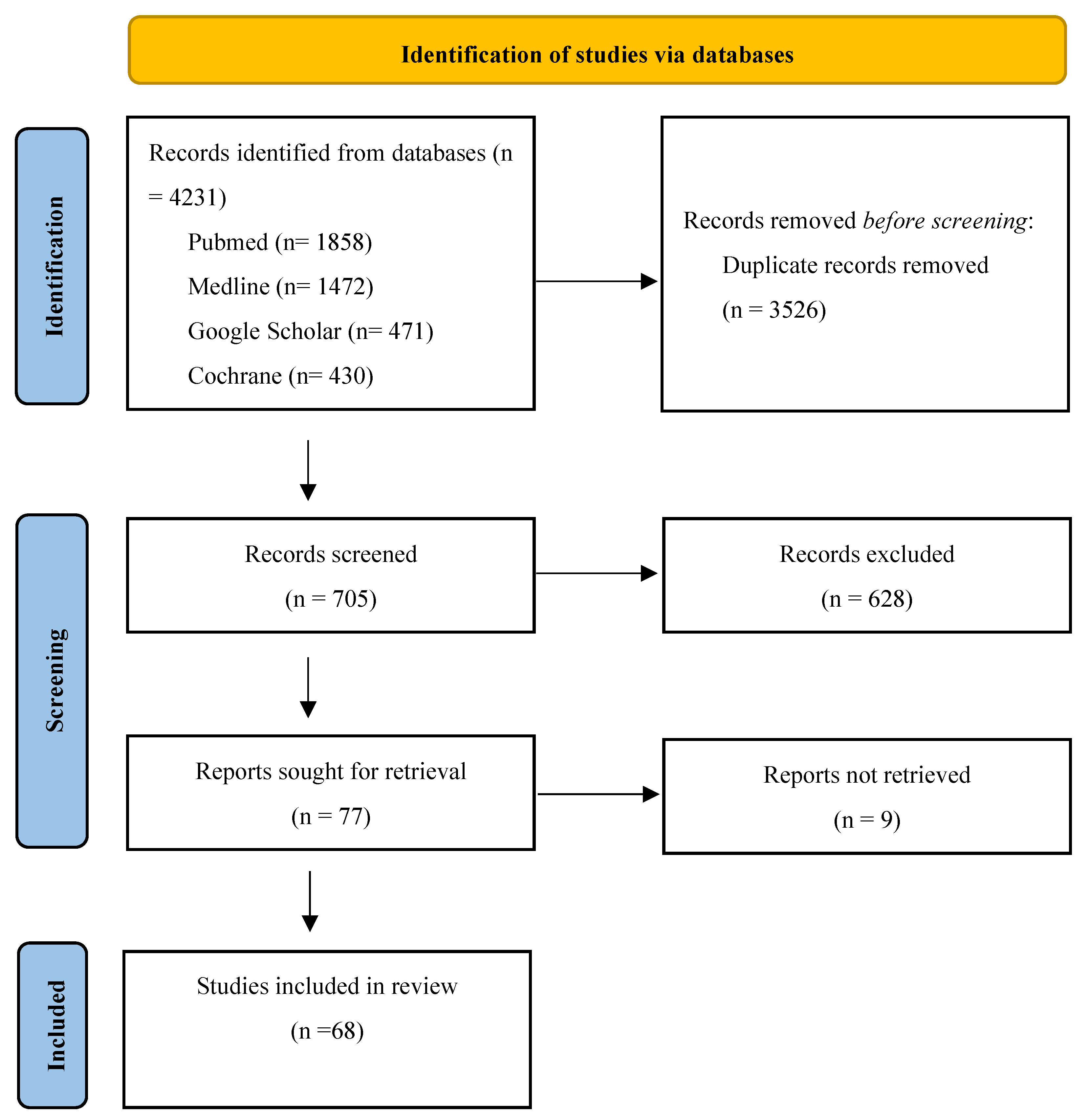
We conducted a systematic literature review and synthesized the results of all published series evaluating the prognostic value of R(un) according to the IASLC. Series were searched on PubMed, Cochrane, MEDLINE, and Google Scholar. We manually searched keywords “Lung cancer”, IASLC”, combined with the connector “AND” and additional keywords “uncertain resection”, “highest node”, “pleural cytology”, “carcinoma in situ”. PRISMA flowchart shows selecting process in figure 1 and 68 studies were selected for this review.
For more clarity, we will deliberately omit data comparing incomplete resection groups, as the prognostic impact of the latter is no longer in doubt.
Figure 1.
PRISMA Flowchart.
3. Results
We first described the literature background of IASLC classification, then we reviewed validations studies of R(un) and examined the impact of HMLN+, CIS BRM and Cy+ separately.
3.1. Roots of IASLC Classification
To better understand the relevance of the IASLC classification, it is first necessary to examine the literature upon which it relied to define R(un).
Naruke et al. [10] were the first, in 1978, to mention a "relatively curative" resection in which "all grossly visible tumor had been removed." They indeed considered that involvement beyond the visceral pleura or the presence of mediastinal lymph node metastases did not allow for a conclusion of complete removal of the tumor. Furthermore, radical lymph node dissection and clear resection margins were required. They demonstrated that N1 involvement (hilar, stations 10 to 12) or N2 involvement (mediastinal, stations 1 to 9) was associated with a 5-year survival rate lower than N0 patients (limited to intraparenchymal nodes, stations 13 and 14). This landmark publication fulfilled its objective of establishing the prognostic value of mediastinal lymph node involvement while proposing a lymph node mapping still used to this day but did not dwell on this definition of uncertain resection, which was more semantic at the time.
In 1998, the Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) published recommendations for standardizing the diagnosis and classification of lung cancer [11] and incorporated the work of Mountain [12] to define "presumed incomplete" surgery. It applies when margins are clear but with one of the following elements: the absence of radical lymph node dissection, the farthest positive lymph node (which can be the highest but also the lowest, in zone 9) if dissection was radical, and the presence of pleural effusion with positive cytology without tumor involvement of the pleura. The authors also proposed classifying atypical resections (wedge resections) as presumed incomplete surgeries. This definition is very similar to that proposed by the IASLC, differing only in the absence of margin abnormalities and the notion of positive pleural cytology without tumor involvement of the pleura. If carcinoma in situ at the margins is simply not mentioned, positive pleural cytology is accepted only in the absence of pleural involvement by the tumor because the authors believed it could be desquamations from the tumor or from lymphatics and/or peripheral lymph nodes, consisting of tumor cells incapable of migrating or causing pleural metastases. In case of pleural invasion by the tumor, the same cytology was then considered malignant, and the surgery deemed incomplete.
Regarding the CIS BRM component, it is based on the work of Snijder et al. [13] and Massard et al. [14], who showed that carcinoma in situ at bronchial margin primarily implied significant recurrence without demonstrating effect on survival. However, these are retrospective series with very small sample sizes, thus having a limited power level. Given the natural progression of these lesions [8,15], it is legitimate to consider the presence of carcinoma in situ at the bronchial resection margin as a potential poor prognostic factor.
Regarding the Cy+ component, numerous studies had already demonstrated that positive cytology in pleural lavage was an independent factor for poor prognosis [16,17,18], often associated with adenocarcinomas [19] of more advanced stages [20,21,22,23], with pleural exposure [24,25,26], N2 involvement [27], or vascular invasion [20]. All these publications, even with small sample sizes, have shown lower survival and higher recurrence rates in Cy+ patients.
3.2. Validation Studies
After the publication of the classification in 2005, several authors sought to verify the clinical relevance of this classification. These series are synthesized in Table 1. To date, only retrospective series are found, sometimes with significant sample sizes:
Gagliasso et al.[28] were the first to investigate uncertain resection by publishing a retrospective series of all patients who underwent surgery at their center in Italy over a period of 10 years, and by reclassifying the R criterion according to the IASLC. 185 patients (15%) out of 1277 patients were reclassified as R(un), in 97% of cases this reclassification was due to inadequate lymph node dissection (107/185, 56.6%) or involvement of the highest mediastinal lymph node (76/185, 41%). Survival analyses found a higher mortality rate in the R(un) group compared to the R0 group [Hazard Ratio (HR) 1.69, 95% CI: 1.412 - 2.024, p=0.0001] with a significantly decreased 5-year survival rate (37.3% vs 58.8%, median survival 39.9 months vs 80.1 months). It is noteworthy that patients classified as R(un) had more often undergone atypical resection than those in the R0 group (15% vs 1.3%), which could be a confounding factor as Wedges are associated with a poorer prognosis than anatomical resections. Nevertheless, after multivariate analysis, R(un) remained a significant predictor of mortality (adjusted HR 1.352, 95% CI: 1.101 – 1.661, p=0.004). In more detail, it can be noted that HMLN+ patients (n=76) had a 5-year survival rate of 28.8%, CIS BRM patients (n=5) of 40%, and those with inadequate dissection (n=107) of 44.2%.
Edwards et al.[29] then utilized the results of a retrospective international cohort, predominantly Japanese and used notably for the 8th TNM, for the purpose of validating the IASLC categorization. In this series of 14,712 patients (of whom 14,293 were initially classified as R0, accounting for 97.2% of the total population), 8,185 (56%) were reclassified as R(un), of which 8,174 were initially R0. Inadequate lymph node dissection and involvement of the highest lymph node accounted for 95.7% and 3.8% of the reasons for reclassification, respectively. While in the N0 group, the survival of R(un) patients was slightly but significantly reduced (5-year OS: 79% vs 82%, p=0.04), it appeared significantly impacted in N+ patients (HR 1.27, p<0.001; Median OS 50 vs 70 months; 5-year OS 45% vs 55%). Finally, there was a small but significant difference within the pT1-2aN0 subgroup (HR 1.22, p = 0.0007, 5-year OS 87% versus 83%) that the authors did not explain, but which might correspond to occult N+ involvement and/or Skip N2 in a group of patients usually not eligible for adjuvant chemotherapy.
In 2019, Osarogiagbon et al.[30] published a retrospective series based on the population of 12 American hospitals over 10 years, totaling 3,361 patients. This study revealed that 63.8% of R0 patients according to UICC definitions had to be reclassified as R(un); that is, 2,044 cases; almost always due to inadequate lymph node dissection (98%). They once again report higher mortality among R(un)-classified patients (adjusted HR 1.36, 95% CI 1.19 - 1.56, 5-year OS 54% vs 64%, median OS 69 months vs not reached). This relationship persists in the N0 (HR 1.31, 95% CI: 1.12 – 1.53, median OS 83 months vs not reached) and N+ (HR 1.24, 95% CI: 0.94 – 1.62, median OS 44 vs 62 months) subgroups. It is also notable that HMLN+ factor seems to emerge as a more significant mortality factor than inadequate dissection (HR 1.5, 95% CI: 1 – 2.31), without statistically differing from the R0-N2 group (HR 1.08, 95% CI: 0.71 – 1.67). Finally, the authors suggest that the absence of mediastinal dissection and complete absence of lymph node sampling would be leading mortality factors (HR 1.46, 95% CI: 1.24 – 1.73 and HR 1.79, 95% CI: 1.45 – 2.22), respectively.
Yun et al.[31] evaluated the IASLC classification focusing on pN2 patients, with a retrospective South Korean cohort of 1039 subjects. Among the R0 patients, 206 (21.8%) were reclassified as R(un) , exclusively for HLMN+ (89.8%) or inadequate lymph node dissection (10.2%), and 6 patients transitioned from R1 to R(un) due to CIS BRM. They reported inferior survival of the R(un) group compared to the R0 group in univariate analysis (HR: 1.25, 95% CI: 1.01 – 1.56, p=0.04, Median OS 55 vs 71 months, 5-year OS 45.8% vs 54.7%), but this difference faded after multivariate analysis, notably considering N2 subdivisions (HR: 1.06, 95% CI: 0.85 – 1.34, p = 0.595). Indeed, R(un) patients had significantly more N2a2 and N2b involvement, which have already been identified as mortality factors. It is also noteworthy that HMLN+ factor appears to have a significantly worse prognosis than inadequate lymph node dissection (Median OS 54 vs 97, 5-year OS 45.4 vs 64.6, p= 0.07), but this data should be interpreted cautiously given the small sample size of the inadequate lymph node dissection group (n=21). There was no data about CIS BRM patients.
Wang et al.[32] conducted a similar study on a local Chinese series of 2782 R0 patients according to UICC. After review, 885 (32%) were reclassified as R(un), among which only inadequate lymph node dissections (81%) and HMLN+ (19%) were found. The authors reported in multivariate analysis a better survival of R0 (adjusted HR: 1.302, 95% CI: 1.091–1.555, p = 0.003) but also a better recurrence-free survival (DFS) (adjusted HR: 1.177, 95% CI 1.045–1.380, p = 0.031). Within the R(un) group, HMLN+ seemed to present lower OS and DFS compared to inadequate lymph node dissection (5-year OS ~ 38% vs 75%, p < 0.001, based on Kaplan-Meier curve) (5-year DFS ~ 25% vs 72%, p < 0.001, based on Kaplan-Meier curve). In subgroup analysis, R(un) negatively impacted the survival and DFS of N0 (OS p = 0.002, DFS p = 0.033), N2 (OS and DFS p = 0.008), and Stage III patients (OS p = 0.002, DFS p = 0.003) but not N1 patients (OS p = 0.79, DFS p = 0.76) nor Stage I (OS p = 0.037, DFS p = 0.276) and II (OS p = 0.187, DFS p = 0.122) patients. Finally, the authors reported that segmentectomy, thoracotomy surgery, and left-sided localization would be risk factors for R(un) occurrence.
Ren et al.[33] published a retrospective chinese series of 5293 patients treated over a period of 4 years. Once again, they found 1371 patients reclassified as R(un) from the initial R0 group, accounting for 25.9% of its population, almost exclusively due to inadequate lymph node dissection (67.7%) or HMLN+ (37.2%). They reported lower OS (adjusted HR 1.41, 95% CI: 1.28 – 1.54, Median DFS 37 vs 57 months, p< 0.001), and DFS (adjusted HR 1.52, 95% CI: 1.38 – 1.67, 5-year OS 46% vs 71%, Median OS 35 months vs not reached, p < 0.001) among R(un) patients in a multivariate model. While HMLN+ involvement is presented as an independent prognostic factor for DFS (adjusted HR 1.21, 95% CI: 1.06 – 1.39, p = 0.003) and OS (adjusted HR 1.23, 95% CI: 1.07 – 1.42, p = 0.005), its effect seems weaker than R(un) N+ HMLN- involvement (adjusted HR DFS 1.37, 95% CI 1.1 – 1.71, p unavailable; adjusted HR OS 1.31, 95% CI 1.06 – 1.61, p unavailable). It is worth noting that in this study, all patients had undergone pleural lavage cytology, which was positive for only 11 patients.
Kadomatsu et al.[34] published a Japanese series of 355 R0 patients according to the UICC, of which 158 (44.5%) were reclassified as R(un), with 137 (87%) due to inadequate lymph node dissection. Survival figures for the overall R(un) group are not provided. However, there was no reported difference in survival within the stage I, stage II-III, and N0 subgroups. Only the N+ group differed, with lower survival in the R(un) group (adjusted HR 2.657, 95% CI: 1.197 – 5.899, p = 0.007; 5-year OS 43.4% vs 65%) with low sample sizes of 39 and 26 patients for these subgroups, requiring caution in interpreting these figures. No difference in DFS was reported by the authors.
Recently, Lee et al.[35], presenting a South Korean series of 910 patients including only clinical stage IIIB-N2 patients who received neoadjuvant radiochemotherapy followed by surgery. Here, 329 patients were reclassified as R(un), due to inadequate lymph node dissection (84.5%), and/or HMLN+ (31.6%). It is also interesting to note that 245 patients (28% of the UICC R0 population) were also reclassified as incomplete resection, mainly due to extracapsular lymph node invasion (ECE, 77%) and/or positive known nodes not removed (28.2%). Thus, a cohort initially composed of 96.3% UICC R0 finds itself in substantially comparable proportions between R0 (33.2%), R(un) (36.2%), and incomplete R (30.7%) according to IASLC. No significant difference is found in the R(un) group compared to the R0 group regarding OS (adjusted HR 1.22, 95% CI: 0.95 – 1.56, p = 0.114) or DFS (adjusted HR 1.25, 95% CI: 0.98 – 1.59, p = 0.113), although there is a trend toward poorer outcomes. Not surprisingly, R1/2 patients show markedly lower OS (adjusted HR 1.54, p = 0.001) and DFS (adjusted HR 1.51, p = 0.001) compared to the R0 group. Proven mediastinal involvement (ypN+) seems predictive of recurrence (adjusted HR 1.31, 95% CI: 0.96 – 1.8, p = 0.071) but not of death (adjusted HR 1.13, 95% CI: 0.81 – 1.57, p = 0.476), as does HMLN+ (adjusted DFS HR 1.18, 95% CI: 0.92 – 1.5, p = 0.183; adjusted OS HR 0.77, 95% CI: 0.59 – 1.02, p = 0.196). These results are difficult to interpret since the absence of significant differences could reflect the effect of neoadjuvant radio-chemotherapy, which may result in mediastinal downstaging, as observed in each group of this study (R0: 54% N0; R(un): 41.6% N0; R1/2: 14.3% N0), which included only cN2 patients. This downstaging could decrease the proportion of occult N+ in the R(un) group, thus bringing it closer to the R0 group, and thus blurring the survival differences usually observed. Finally, it is noteworthy that the authors report significantly better survival in the IASLC R0 group compared to the UICC R0 group (p = 0.011), which supports the idea of significant heterogeneity within the latter group.
Wen et al. [36] also described a series of 5200 patients, of whom 1727 were reclassified as R(un) (33%) due to insufficient LND (68.3%) or HMLN+ (38.3%) (CIS BRM = 3). They reported a lower OS (adjusted HR 1.4, 95% CI: 1.223 – 1.603, p < 0.001) and DFS (adjusted HR 1.28, 95% CI: 1.151 – 1.434, p < 0.001) in the R(un) group. In subgroup analysis, R(un) remained relevant for survival and DFS for all parameters studied (age, sex, smoking, histology) except for radiographic appearance and stage: it seems that R(un) with ground-glass opacities (HR 1.19, 95% CI: 0.78 – 1.81, p = 0.4) or stage I disease (HR 0.88, 95% CI: 0.68 – 1.14, p = 0.34) survive as well as their R0 counterparts. The DFS of R(un) with ground-glass opacities is comparable (HR 1.19, 95% CI: 0.88 – 1.62, p = 0.29), while a protective effect of R(un) is found in stage I (HR 0.81, 95% CI: 0.61 – 0.98, p = 0.024). However, it should be noted that stage I and ground-glass opacities were predominantly reclassified as R(un) due to insufficient LND, whereas stages II-III and solid nodules were more likely reclassified due to HMLN+. Finally, the authors showed that HMLN+ patients had lower OS than patients with insufficient LND (p < 0.0001).
Chen et al. [37] focused on patients who underwent lobectomy with bronchial resection-anastomosis. They report a series of 682 patients, of whom 631 were classified as R0 UICC, reclassified as 489 R0 (71.7%), 110 R(un) (16.1%), and 83 R1-2 (12.2%). The authors observed a lower disease-free survival (DFS) (adjusted HR 1.59, 95% CI: 1.09 - 2.31, p = 0.023) and overall survival (OS) (adjusted HR 1.54, 95% CI: 1.02 - 2.33, p = 0.040) in the R(un) group compared to R0. In subgroup analysis, this difference was observed in N2 patients (5-year DFS 29.1% vs 59.1%, adjusted p = 0.010; 5-year OS 43.5% vs 56.6%, adjusted p = 0.010). These findings need to be considered alongside the fact that 82 out of 110 patients in the R(un) group were reclassified as HMLN+, indicating N2 status. Consequently, N0 and N1 groups comprised only 16 and 5 patients, respectively, limiting the reliability of the results.
In 2025, a French study [38] reported R(un) as a worsening factor for OS (adjusted HR 1.26; 95% CI: 1.03 - 1.52, p<0.001) and DFS (adjusted HR 1.23; 95% CI: 1.03 - 1.46). Subgroup analyses among R(un) patients suggest HMLN+ and very poor LND (less than 3 lymph node or station 7 not examined) as a significant factor for low OS [HRs 3.35 (95% CI: 2.05 – 5.49) and 2.17 (95% CI: 1.39 – 3.38), respectively] and DFS [HRs 2.66 (95% CI: 1.71 – 4.15) and 2.05 (95% CI: 1.35 – 3.10) respectively].
Liu et al. [39] studied the impact of R(un) when associated with the new IASLC tumor gradation of adenocarcinomas [40], which mainly relies on anatomo-pathologic characteristics. They found that R(un) was associated with poor OS (Adjusted HR 1.57, 95% CI: 1.20 - 2.05, p= 0.001) and RFS (Adjusted HR 1.73, 95% CI: 1.37 - 2.19, p< 0.001) in the overall population but also showed that R(un) reduced OS and RFS in only in aggressive grade 3 tumors (OS 75.3% vs 56.5%, p< 0.001; RFS 68.3% vs 41.9%, p< 0.001).
3.3. The “Highest Mediastinal Lymph Node” Component
Some authors chose to focus on the prognostic impact of involvement of the highest lymph node, a criterion casting doubt on the persistence of lymphatic metastases despite well-performed mediastinal dissection. These series are summarized in Table 2.
Sakao et al.[41] published a series of 53 N2 patients, including 14 HMLN+ who were naive to any neoadjuvant and adjuvant therapy. They report a markedly lower survival among HMLN+ patients (adjusted HR 3.225, 95% CI: 1.153 – 9.009, p = 0.026). However, the dissection was carried out very aggressively, with HMLN defined as being located above the innominate vein trunk (stations R2 and L2), with authors even performing a median sternotomy for left lung tumors and harvesting nodes below the thyroid. These locations are rarely sampled in common practice and ultimately resemble N3 involvement, which could explain, in this small size series, the marked difference in survival among HMLN+ patients, some of whom could have occult N3.
Zheng et al.[42] report in their retrospective series of 549 patients, including 246 HMLN+, a similarly reduced survival among the latter compared to HMLN- patients (adjusted HR 1.584, 95% CI: 1.217 – 2.062, p < 0.0001; 5-year OS 13% vs 29%, Median OS 24.43 vs 36.48 months, p < 0.0001). Here, the dissection is carried out up to stations 2R and 4L, mostly outside the TABC according to the article's diagrams, representing a more conventional approach to dissection than in Sakao et al.'s series. However, it's notable that Skip N2 HMLN+ had significantly more severe mediastinal involvement than Skip N2 HMLN- since the number of mediastinal lymph node stations involved was higher in the former group (p<0.0001). While the number of skip N2 stations involved seems to be a mortality factor in this study (p< 0.0001), its effect is not found in multivariate analysis (adjusted HR 0.945, 95% CI 0.887 – 1.213, p= 0.224), reinforcing the impression of an effect primarily linked to HMLN+.
Park et al. [43] reported a retrospective series of 339 N2 patients, among whom 142 (42%) were HMLN+. Here, the authors differentiated between patients with the highest involved lymph node (2R or 4L, 5 or 6) and those with the farthest involved lymph node (either the highest or the lowest in station 9). The results were similar in both groups with a similar survival to the control group: adjusted HR 1.015 (95% CI: 0.751 - 1.371, p = 0.924), adjusted HR 1.050 (95% CI: 0.775 - 1.423, p = 0.755) respectively.
In a retrospective series of 266 pT1-4N2M0 patients, of whom 128 were HMLN+ (stations 2R, 4L, 5 or 6), Wang et al. [44] found no difference in survival (adjusted HR 1.00, 95% CI: 0.702 - 1.428, p = 0.99). It is notable here that there was a higher mortality among patients who received neoadjuvant therapy (adjusted HR 1.88, 95% CI 0.928 - 3.834, p= 0.079), which is consistent with more severe preoperative involvement and thus poorer prognosis.
Recently, Marziali et al. [45] published a retrospective series of 68 cN0, pN2 patients, with 31 HMLN+, reporting a lower OS (adjusted HR 2, 95% CI: 0.7 - 6.1, p = 0.002) and inferior DFS (adjusted HR 3.2, 95% CI: 1.4 - 7.4, p = 0.008) in the R(un). Here the definition of HMLN is different from other studies as lymph node dissection was sometimes performed in a lobe-specific manner. Thus, out of the 31 patients, 6 were HMLN+ in station 7: 2 for tumors of the left lower lobe, and 4 for tumors of the right lower lobe, the latter theoretically not corresponding to an HMLN+ but rather to inadequate dissection as it did not include station 4R.
Liu et al.[46] also published a retrospective series of 468 pT1-4N2 patients, including 219 HMLN+. They reported decreased overall survival (adjusted HR 1.45, 95% CI 1.07 – 1.99, p = 0.017) and recurrence-free survival (adjusted HR 1.26, 95% CI 0.94 – 1.68, p = 0.0115) in HMLN+ patients. This result is reinforced in the subgroup of stage IIIA patients (384 patients, 82.1% of the total cohort) for overall survival (adjusted HR 1.70, 95% CI 1.19 – 2.42, p = 0.003) and recurrence-free survival (adjusted HR 1.46, 95% CI 1.06 – 2.02, p = 0.002). These differences are not found in the IIIB patient subgroup, probably because the severity of the disease at this stage overshadows the prognostic impact of HMLN.

Table 2.
Published series regarding Highest Mediastinal Lymph Node.
| Répartition (%) | ||||||
|---|---|---|---|---|---|---|
| Author, year, country | Design | Patients (n) | HMLN - | HMLN + | HR DFS (p) | HR OS (p) |
| Wang et al.[44], 2021, China | Retrospective, Single Instutition | pT1-4N2M0 (266) | 138 (52%) | 128 (48%) | NA | 1(0,993) |
| Sakao et al.[41], 2006, Japan | Retrospective, Single Instutition | pT1-3N2M0 (53) | 39 (74%) | 14 (26%) | NA | 3,559 (0,0025) |
| Park et al.[43], 2019, South Korea | Retrospective, Single Instutition | pT1-4N2M0 (339) | 197 (58%) | 142 (42%) | 1 (0,99) | 1,085 (0,429) |
| Marziali et al.[45], 2023, Italy | Retrospective, Single Instutition | pT1-4N2M0 (68) | 37 (54%) | 31 (46%) | 3.2 (0,008) | 2 (0,002) |
| Zheng et al.[42], 2010, China | Retrospective, Single Instutition | pT1-4N2M0 (549) | 303 (55,2%) | 246 (44,8%) | NA | 1,584 (<0,0001) |
| Liu et al.[46], 2024 China |
Retrospective, Single Instutition | pT1-4N2M0 (486) | 249 (53,2%) | 219 (46.8%) | 1.26 (0,115) | 1,45 (0.017) |
HMLN : Highest Mediastinal lymph Node; HR: Hazard Ratio; DFS: Disease Free Survival; OS: Overall Survival; NA: Not Available.
3.4. The “Carcinoma In Situ at Bronchial Margin” Component
To date, there are very few series on CIS BRM. Indeed, the occurrence of this criterion remains extremely rare, even in large retrospective series [29,33]. There are about ten series [47,48,49,50,51,52,53,54,55,56,57] in which CIS BRM is reported in very small numbers, as shown in Table 3. Statistical tests are not available, but it is noted that the reported cases are almost always associated with a primary tumor of squamous cell carcinoma type. Ultimately, no author has been able to conclude a negative influence of CIS BRM on survival.
In 2017, Lee et al. [57] published a cohort of 1800 patients, including 18 with CIS BRM and 42 with extra-mucosal involvement of the bronchial margin (R1-EMD). The primary tumors of CIS BRM patients were predominantly squamous cell carcinomas (88.9%). The authors reported a higher local recurrence rate of CIS BRM compared to R0 (p= 0.008) without it affecting survival (adjusted HR 0.985, 95% CI: 0.373 - 2.602, p = 0.98).
3.5. The “Pleural Cytology” Component
Regarding Cy+, nearly twenty series, mainly retrospective, have been published after the release of the IASLC classification [58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76]. Although these series were not developed for the purpose of validating the IASLC classification, they constitute a dense literature in favor of this criterion for the R(un). On average, Cy+ patients represented 5% of the total sample size, and most series proposed pre-resection lavage (prePLC), performed just after thoracic access, sometimes followed by post-resection lavage (postPLC) before thoracic closure.
A meta-analysis conducted by Wang et al. [77] in 2016, comprising 28 studies with a total of 28,714 patients, including 1434 cases of Cy+, revealed that patients with positive pleural lavage cytology (PLC+) pre- and post-resection had significantly higher mortality compared to patients with negative cytology (PLC-): HR 2.89 (95% CI: 2.48 – 3.37, p < 0.00001), and HR 2.70 (95% CI: 1.90 – 3.83), respectively. This effect was reinforced when focusing on early Stage I: prePLC+: HR 3.29 (95% CI: 2.55 – 4.25, p < 0.00001), postPLC+: HR 4.85 (95% CI: 2.31 – 10.20, p < 0.0001). Similar figures were found concerning recurrence (all stages combined): prePLC+: RR 2.45 (95% CI: 1.91 – 3.15), postPLC+: RR 2.37 (95% CI: 1.11 – 5.09). Additionally, the authors also reported a significantly increased risk of pleural recurrence (RR 4.84, 95% CI: 3.03 – 7.73, p < 0.00001) and distant recurrence (RR 2.62; 95% CI: 1.72 – 4, p<0.00001) in the prePLC+ group. A similar effect was found in the postPLC+ group on pleural recurrence (HR 3.39, 95% CI: 1.26 – 9.10, p = 0.02) but not on distant recurrence (HR 1.7, 95% CI: 0.8 – 3.62, p = 0.17). However, the number of events and patients in this group were much lower than in the prePLC+ group, which could mask results due to lack of power.
Subsequent series have been published, yielding substantially similar results: Nakamura et al. [76] reported a prognostic contribution of postPLC+ (adjusted HR 2.12, 95% CI: 1.19 – 3.77, p= 0.01) but not of prePLC+ (adjusted HR 1.09, 95% CI: 0.56 – 2.12, p = 0.79) with a simplified lavage of 20ml saline solution. Onodera et al. [75] described a decreased DFS in both groups (5-year DFS prePLC+ 26.7% vs. 76.9%, p < 0.0001; 5-year DFS postPLC+ 14.3% vs. 76%, p < 0.0001), not significant in multivariate analysis (HR prePLC+ 1.82, p = 0.19 and HR postPLC+ 2.03, p = 0.14). Mizuno et al. [74] also showed decreased OS and DFS in PLC+ patients (5-year OS 61.5% vs 81.7%, p < 0.001; 5-year DFS 31.1% vs 75.7%, p < 0.001), persisting in multivariate analysis only for DFS (adjusted HR OS 1.34, 95% CI: 0.80 - 2.13, p = 0.25; adjusted HR DFS 1.70, 95% CI: 1.12 - 2.47, p = 0.013). These series are all subject to the same limitations, namely their retrospective nature and very small sample sizes in the PLC+ groups.
Very recently, Recuero Diaz et al. [78] published a multicenter prospective series of 684 patients, of which 15 were PLC+. These patients showed a higher prevalence of advanced stages (pIIB-IIIB, p= 0.02), pleural (p= 0.005) and vascular invasion (p= 0.02), N+ involvement (p <0.001), and larger tumor sizes (p= 0.005) with pT3-4 (p= 0.09) and poorly differentiated histology (p= 0.003). In multivariate analysis, PLC+ emerged as the major prognostic factor for recurrence (OR 3.46, 95% CI: 2.25 – 5.36, p < 0.001), surpassing N+ involvement, pTNM stage, and poorly differentiated histology, among others.
Therefore, Cy+ is a very strong independent prognostic factor, indicating both a tumor that is often more advanced or aggressive and favoring early recurrence and poor survival, placing patients in risk groups close to advanced stage III [26], even at stage I [71]. To account for this factor, some authors propose upgrading the tumor criterion (T) and considering adjuvant treatment [69,74], especially in early stages that may be falsely reassuring.
4. Discussion
Most published series find a negative prognostic impact of R(un) status. Uncertain resection according to the IASLC 2005 allows for the individualization of a group of patients with intermediate prognosis, worse than R0 but better than R1-2 [28,29], and therefore emerges as a relevant criterion that should raise concerns about early recurrence and increased mortality. However, various studies highlight that the R(un) encompasses a heterogeneous population, and the prognostic strength of the R(un) is often inferior to standard criteria such as TNM stage or N+ involvement.
From an epidemiological perspective, Wang et al. [32] report that segmentectomy, thoracotomy, and left-sided tumors are risk factors for the occurrence of R(un) . These are likely indirect markers: lymph node dissection may be less extensive in segmentectomy cases as it is considered less crucial in patients with small tumors. The left side is considered by the authors as more challenging for dissection due to nearby structures (thoracic duct, aortic arch, recurrent nerve...). Finally, thoracotomy is applied to patients with more advanced tumors, likely at higher risk of lymph node invasion and thus positive mediastinal lymph nodes and HMLN+. For HMLN+, risk factors also include cN+ involvement and severe mediastinal involvement (non-skip N2 and multiple N2) [41]. Cy+ appears to be favored by pleural and vascular involvement, occurring more frequently in larger tumors, with pN+ involvement, and low differentiation [78].
Furthermore, R(un) is a composite of several criteria themselves unequal. While the prognostic role of insufficient dissection and HMLN+ has been well-documented, CIS BRM remains a rare event. A review conducted on the subject by Vallières et al. [79] did not conclude to an effect on survival, although local recurrence seems slightly increased. The prognostic strength of this criterion remains to be determined, but it should be noted that CIS BRM is classified as R1 according to the UICC. Its migration to the R(un) seems therefore justified, pending further investigation to determine if this criterion indeed excludes a complete resection. As CIS BRM is located in the inner face of bronchial airways, it would be consistent to consider reinforced endoscopic surveillance for those patients.
The R(un) group is predominantly composed of patients who have not undergone sufficient lymph node dissection, making it a melting pot of true N0, true and occult N1, true and occult N2, with proportions impossible to specify. Thus, under-evaluated patients may not benefit from appropriate adjuvant therapies or surveillance, resulting in increased mortality in the R(un). The R(un) is also a good example of the Will Rogers phenomenon [80,81], whereby the prognosis of the R0 group improves due to the migration of cases with poorer prognosis to the new R(un), as well illustrated by Lee et al. [35] with R0 IASLC survival being better than that of the UICC R0 group (p= 0.011).
A portion of the R(un) is also represented by patients with the highest mediastinal lymph node involvement, which represents advanced N2 involvement and seems to have even more prognostic value when lymph node dissection is extensive [41,42]. This criterion is difficult to analyze as it heavily depends on the quality of dissection and must also consider N2 subdivisions, particularly the possible presence of skip N2, which notably affects prognosis [82,83]. Additionally, it is challenging for both the surgeon and pathologist to precisely identify the highest lymph node in the chain, as dissection is usually performed en bloc with mediastinal fat to limit the risk of rupture. As a result, most authors rather report the highest station involved, raising doubts about the possibility of residual involvement by contiguity but still providing an assessment of mediastinal involvement, as HMLN+ is often associated with multiple N2 involvement, the poor prognosis of which is increasingly documented [84,85]. This highlights the value of orienting lymph node dissection during surgery to properly mark the highest node removed.
On the contrary, the Cy+ criterion, although very rare in cases where pleural lavage is performed, appears to be a leading factor in mortality and recurrence. Its occurrence is more likely when the tumor invades the visceral pleura [78], raising the question of a pathophysiological continuum between this lavage cytology and the development of carcinomatous pleural effusion, classified as M1a. Nevertheless, Mizuno et al. [73], by performing intraoperative lavage analysis, showed that Cy+ patients had better survival than M1a patients (p< 0.001), while also detecting pleural dissemination in 9% of positive cases. This criterion is particularly relevant as it may affect tumors that solely invade the visceral pleura and are therefore classified as T2, for which adjuvant treatments are not routinely offered. Cy+ is thus a very strong independent prognostic factor, indicating both a more advanced or aggressive tumor, placing patients in risk groups akin to advanced stage III [26], even at stage I [74]. To account for this factor, some authors propose upstaging the T criterion of the tumor [67] and considering adjuvant treatment [69,74], especially in early stages that might appear falsely reassuring. Ogawa et al. [86] showed improved OS and DFS in patients who received adjuvant chemotherapy, which should encourage us to perform pleural lavage cytology. The question of whether those patients should receive adjuvant chemotherapy similarly to locally advanced stages or be treated as metastatic disease need to be explored.
The R(un) appears to be less discriminatory in stage I and ground-glass opacities [32,87,88]. This could be explained by a low probability of lymphatic invasion for these highly localized tumors [89]. Thus, Lee et al. [87] showed that less extensive dissection in Stage I and ground-glass opacities was not associated with poorer prognosis. This could explain the lack of difference in these subgroups [32,34,36,37]. In 2011, Darling et al. published the ACOSOG Z0030 trial [90] which demonstrated no difference in survival between systematic sampling (limited to one lymph node per area), pN0 confirmed intraoperatively, and radical lymph node dissection in cT1-2, N0 or non-hilar N1 patients. This finding has led some surgeons to debate the utility of lymph node dissection in early stages [91] and propose sampling for small peripheral tumors, cN0 [92]. This conservative approach, although interesting, requires perfect coordination and availability between the surgeon and pathologist, which can be challenging in routine practice. An alternative could be the use of intraoperative indocyanine lymphatic mapping [93,94], for example, to reduce the number of intraoperative analyses but this technique needs more investigations and proof or reliability.
The prognostic significance of R(un) becomes evident when advancing beyond Stage IIb, with larger tumors and a higher probability of lymphatic dissemination. For patients classified as N0, R(un) primarily reflects the quality of lymph node dissection, which is likely inadequate given the advancement of the disease. The imprecision of lymph node dissection may represent a missed opportunity for these patients, due to the persistence of potentially removable residual disease (especially skip N2) and understaging. For N1 and N2 patients, R(un) due to inadequate dissection or HMLN+ should also raise concerns about recurrence due to potential residual disease, prompting oncology teams to enhance surveillance and vigilance for recurrence.
One might also question the relevance of adjuvant radiotherapy: while this technique has not been proven effective routinely in the pN2R0 population in the Lung Art trial [95], its use is considered in guidelines, on a case-by-case basis, in the presence of significant risk factors for recurrence [96,97,98]. Indeed, the use of PORT in resected IIIA-N2 remains a very debated topic, and recent series on unselected patients failed to show improvements[99], but some wisely selected patients may benefit from it. Some authors suggest the use of risk scores, most of them taking account of the severity of mediastinal involvement [100,101,102]. Thus, HMLN+ patients may be good candidates, as Deng et al.[103] and Guo al.[104] reported improvements in OS and DFS after adjuvant chemoradation therapy. This point needs more explorations and may be supported by a randomized trial or assessed by a better stratification according to N2 subgroups in retrospective series, and was not, to our knowledge, addressed in the Lung Art Trial. Furthermore, current radiation therapy methods (i.e. intensity modulated radiation therapy) may offer better results on disease control and less toxicity, reinforcing their place in adjuvant strategy.
While the relevance of R(un) intersects with the debate on sampling in early stages, its importance in locally advanced stages seems indisputable, a fortiori in case of HMLN+. The literature provides evidence that the quality of resection and accuracy of lymph node staging are fundamental for the survival of these patients and that a large part of R(un) could be avoided. At a time when conservative approaches, whether in surgical approach [105] or parenchymal resection [106], are increasingly favoured, R(un) reminds us that not all patients are eligible for minimal dissection. IASLC classification remains underutilized because no therapeutic strategies are attached to it, but this could change in the near future as it has been advised to integrate it in the upcoming 9th TNM [107].
5. Conclusions
The uncertain R classification of the IASLC 2005 appears highly relevant, especially in locally advanced stages IIb-IIIA, and helps to discriminate patients with poor prognosis despite being classified as R0 according to previous UICC classifications. Its use in practice remains too limited due to the absence of clear therapeutic strategy changes. Furthermore, its composite nature of R(un) and the rarity of occurrence of some of its criteria prevent the design of prospective trial and series, necessary for its legitimacy. The use of this more precise classification would allow for better stratification of recurrence risk and more effective use of adjuvant therapies by thoracic oncology teams.
Finally, we support the idea that Cy+ patients should receive adjuvant chemotherapy, the format of which remains to be determined, while CIS BRM patients could likely benefit from diligent endoscopic surveillance to track local recurrence. Ultimately, HMLN+ patients should be considered as at high risk for recurrence, and adjuvant radio-chemotherapy should be discussed.
Author Contributions
Conceptualization, D.C., M.A. and A.L.; methodology, X.C. and A.E.; validation, X.C., M.A. and A.L.; investigation, X.C., B.L., A.E. and A.L.; resources, X.C., C.V. and A.L.; writing—original draft preparation, X.C. and A.L.; writing—review and editing, X.C., B.L., D.S., A.T., C.V., D.C., M.S., M.A. and A.L.; supervision, A.L.; project administration, A.L.; funding acquisition, D.C., B.L., A.T., D.S. and A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. Publication Charges were supported by Association Thorax à Tours.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NSCLC | Non-small cell lung cancer |
| UICC | Union Internationale Contre le Cancer |
| AJCC | American Joint Committee on Cancer |
| IASLC | International Association for the Study of Lung Cancer |
| R(un) HMLN CIS BRM R1 cy+ PLC HR OS DFS LND |
Uncertain Resection Highest Mediastinal Lymph Node Carcinoma In-Situ at Bronchus Resection Margin Pleural lavage positive cytology Pleural lavage cytology Hazard ratio Overall Survival Disease Free Survival Lymph Node Dissection |
References
- Jett, J.R.; Schild, S.E.; Kesler, K.A.; Kalemkerian, G.P. Treatment of Small Cell Lung Cancer: Diagnosis and Management of Lung Cancer, 3rd Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2013, 143, e400S–e419S. [Google Scholar] [CrossRef] [PubMed]
- Vansteenkiste, J.; Crinò, L.; Dooms, C.; Douillard, J.Y.; Faivre-Finn, C.; Lim, E.; Rocco, G.; Senan, S.; Van Schil, P.; Veronesi, G.; et al. 2nd ESMO Consensus Conference on Lung Cancer: Early-Stage Non-Small-Cell Lung Cancer Consensus on Diagnosis, Treatment and Follow-Up. Annals of Oncology 2014, 25, 1462–1474. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J Clin 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef] [PubMed]
- eUpdate – Early and Locally Advanced Non-Small-Cell Lung Cancer Available online:. Available online: https://www.esmo.org/guidelines/guidelines-by-topic/esmo-clinical-practice-guidelines-lung-and-chest-tumours/early-stage-and-locally-advanced-non-metastatic-non-small-cell-lung-cancer/eupdate-early-and-locally-advanced-non-small-cell-lung-cancer-nsclc-treatment-recommendations2 (accessed on 29 January 2024).
- Donington, J.S.; Kim, Y.T.; Tong, B.; Moreira, A.L.; Bessich, J.; Weiss, K.D.; Colson, Y.L.; Wigle, D.; Osarogiagbon, R.U.; Zweig, J.; et al. Progress in the Management of Early-Stage Non–Small Cell Lung Cancer in 2017. Journal of Thoracic Oncology 2018, 13, 767–778. [Google Scholar] [CrossRef]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann Glob Health 2019, 85, 8. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, Lucian. R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. Journal of Thoracic Oncology 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Rami-Porta, R.; Wittekind, C.; Goldstraw, P. Complete Resection in Lung Cancer Surgery: Proposed Definition. Lung Cancer 2005, 49, 25–33. [Google Scholar] [CrossRef]
- Naruke, T.; Suemasu, K.; Ishikawa, S. Lymph Node Mapping and Curability at Various Levels of Metastasis in Resected Lung Cancer. The Journal of Thoracic and Cardiovascular Surgery 1978, 76, 832–839. [Google Scholar] [CrossRef]
- Rami Porta, R. Normativa Actualizada (1998) Sobre Diagnóstico y Estadifícación Del Carcinoma Broncogénico. Archivos de Bronconeumología 1998, 34, 437–452. [Google Scholar] [CrossRef]
- Mountain, C.F. Surgical Therapy in Lung Cancer: Biologic, Physiologic, and Technical Determinants. Semin Oncol 1974, 1, 253–258. [Google Scholar] [PubMed]
- Snijder, R.J.; Brutel de la Rivière, A.; Elbers, H.J.; van den Bosch, J.M. Survival in Resected Stage I Lung Cancer with Residual Tumor at the Bronchial Resection Margin. Ann Thorac Surg 1998, 65, 212–216. [Google Scholar] [CrossRef]
- Massard, G.; Doddoli, C.; Gasser, B.; Ducrocq, X.; Kessler, R.; Schumacher, C.; Jung, G.M.; Wihlm, J.M. Prognostic Implications of a Positive Bronchial Resection Margin. Eur J Cardiothorac Surg 2000, 17, 557–565. [Google Scholar] [CrossRef]
- Wistuba, I.I.; Gazdar, A.F. LUNG CANCER PRENEOPLASIA. Annu. Rev. Pathol. Mech. Dis. 2006, 1, 331–348. [Google Scholar] [CrossRef]
- Buhr, J.; Berghäuser, K.H.; Morr, H.; Dobroschke, J.; Ebner, H.J. Tumor Cells in Intraoperative Pleural Lavage. An Indicator for the Poor Prognosis of Bronchogenic Carcinoma. Cancer 1990, 65, 1801–1804. [Google Scholar] [CrossRef]
- Kondo, H.; Asamura, H.; Suemasu, K.; Goya, T.; Tsuchiya, R.; Naruke, T.; Yamagishi, K.; Uei, Y. Prognostic Significance of Pleural Lavage Cytology Immediately after Thoracotomy in Patients with Lung Cancer. J Thorac Cardiovasc Surg 1993, 106, 1092–1097. [Google Scholar] [PubMed]
- Higashiyama, M.; Doi, O.; Kodama, K.; Yokouchi, H.; Tateishi, R.; Horai, T.; Ashimura, J.; Nagumo, S.; Naruse, Y. Pleural Lavage Cytology Immediately after Thoracotomy and before Closure of the Thoracic Cavity for Lung Cancer without Pleural Effusion and Dissemination: Clinicopathologic and Prognostic Analysis. Ann Surg Oncol 1997, 4, 409–415. [Google Scholar] [CrossRef]
- Eagan, R.T.; Bernatz, P.E.; Payne, W.S.; Pairolero, P.C.; Williams, D.E.; Goellner, J.R.; Piehler, J.M. Pleural Lavage after Pulmonary Resection for Bronchogenic Carcinoma. J Thorac Cardiovasc Surg 1984, 88, 1000–1003. [Google Scholar]
- Okada, M.; Sakamoto, T.; Nishio, W.; Uchino, K.; Tsuboshima, K.; Tsubota, N. Pleural Lavage Cytology in Non–Small Cell Lung Cancer: Lessons from 1000 Consecutive Resections. The Journal of Thoracic and Cardiovascular Surgery 2003, 126, 1911–1915. [Google Scholar] [CrossRef]
- Okumura, M.; Ohshima, S.; Kotake, Y.; Morino, H.; Kikui, M.; Yasumitsu, T. Intraoperative Pleural Lavage Cytolopgy in Lung Cancer Patients. The Annals of Thoracic Surgery 1991, 51, 599–604. [Google Scholar] [CrossRef]
- Pavia, R.; Mulè, V.; Angiò, L.; Monaco, F.; Smedile, F.; Fabiano, G.; Mondello, B.; Monaco, M. [Intraoperative pleural lavage for restaging of bronchogenic carcinoma]. Minerva Chir 2003, 58, 67–69. [Google Scholar] [PubMed]
- Vicidomini, G.; Santini, M.; Fiorello, A.; Parascandolo, V.; Calabrò, B.; Pastore, V. Intraoperative Pleural Lavage: Is It a Valid Prognostic Factor in Lung Cancer? The Annals of Thoracic Surgery 2005, 79, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Dresler, C.M.; Fratelli, C.; Babb, J. Prognostic Value of Positive Pleural Lavage in Patients with Lung Cancer Resection. The Annals of Thoracic Surgery 1999, 67, 1435–1439. [Google Scholar] [CrossRef]
- Riquet, M.; Badoual, C.; Le Pimpec Barthes, F.; Lhote, F.-M.; Souilamas, R.; Hubsch, J.-P.; Danel, C. Visceral Pleura Invasion and Pleural Lavage Tumor Cytology by Lung Cancer: A Prospective Appraisal. The Annals of Thoracic Surgery 2003, 75, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.; Ali, A.; Theodorou, P.; Nicholson, A.G.; Ladas, G.; Goldstraw, P. Intraoperative Pleural Lavage Cytology Is an Independent Prognostic Indicator for Staging Non–Small Cell Lung Cancer. The Journal of Thoracic and Cardiovascular Surgery 2004, 127, 1113–1118. [Google Scholar] [CrossRef]
- Kotoulas, C.; Lazopoulos, G.; Karaiskos, T.; Tomos, P.; Konstantinou, M.; Papamichalis, G.; Politi, D.; Lioulias, A. Prognostic Significance of Pleural Lavage Cytology after Resection for Non-Small Cell Lung Cancer. European Journal of Cardio-Thoracic Surgery 2001, 20, 330–334. [Google Scholar] [CrossRef]
- Gagliasso, M.; Migliaretti, G.; Ardissone, F. Assessing the Prognostic Impact of the International Association for the Study of Lung Cancer Proposed Definitions of Complete, Uncertain, and Incomplete Resection in Non-Small Cell Lung Cancer Surgery. Lung Cancer 2017, 111, 124–130. [Google Scholar] [CrossRef]
- Edwards, J.G.; Chansky, K.; Schil, P.V.; Nicholson, A.G.; Boubia, S.; Brambilla, E.; Donington, J.; Galateau-Sallé, F.; Hoffmann, H.; Infante, M.; et al. The IASLC Lung Cancer Staging Project: Analysis of Resection Margin Status and Proposals for Residual Tumor Descriptors for Non–Small Cell Lung Cancer. Journal of Thoracic Oncology 2020, 15, 344–359. [Google Scholar] [CrossRef]
- Osarogiagbon, R.U.; Faris, N.R.; Stevens, W.; Fehnel, C.; Houston-Harris, C.; Ojeabulu, P.; Akinbobola, O.; Lee, Y.-S.; Ray, M.A.; Smeltzer, M.P. Beyond Margin Status: Population-Based Validation of the Proposed IASLC Residual Tumor Classification Re-Categorization. J Thorac Oncol 2020, 15, 371–382. [Google Scholar] [CrossRef]
- Yun, J.K.; Lee, G.D.; Choi, S.; Kim, Y.-H.; Kim, D.K.; Park, S.-I.; Kim, H.R. A Validation Study of the Recommended Change in Residual Tumor Descriptors Proposed by the International Association for the Study of Lung Cancer for Patients With pN2 NSCLC. Journal of Thoracic Oncology 2021, 16, 817–826. [Google Scholar] [CrossRef]
- Wang, X.; Cai, J.-S.; Yang, F. Investigation of the Non-Small Cell Lung Cancer Patients with Uncertain Resection: A Population-Based Study. Lung Cancer 2022, 171, 47–55. [Google Scholar] [CrossRef]
- Ren, Y.; She, Y.; Tang, H.; Deng, J.; Jiang, G.; Wu, C.; Zhu, Y.; Zheng, H.; Chen, C. Prognostic Evaluation of the Proposed Residual Tumor Classification in a Chinese Non-Small Cell Lung Cancer Population. J Surg Oncol 2022, 125, 1061–1070. [Google Scholar] [CrossRef]
- Kadomatsu, Y.; Nakamura, S.; Ueno, H.; Goto, M.; Ozeki, N.; Fukumoto, K.; Fukui, T.; Suzuki, Y.; Chen-Yoshikawa, T.F. Prognostic Value of Uncertain Resection for Overall Survival in Non-Small Cell Lung Cancer. The Annals of Thoracic Surgery 2022, 114, 1262–1268. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.; Hong, Y.S.; Lee, G.; Kang, D.; Yun, J.; Jeon, Y.J.; Shin, S.; Cho, J.H.; Choi, Y.S.; et al. Validation of the IASLC Residual Tumor Classification in Patients With Stage III-N2 Non-Small Cell Lung Cancer Undergoing Neoadjuvant Chemoradiotherapy Followed By Surgery. Annals of Surgery 2023, 277, e1355. [Google Scholar] [CrossRef] [PubMed]
- Wen, Z.; Fu, F.; Zhao, Y.; Gao, Z.; Han, H.; Li, H.; Ye, T.; Hu, H.; Sun, Y.; Li, Y.; et al. Residual Tumor Descriptors Proposed by the International Association for the Study of Lung Cancer May Not Be Applicable to Stage I and Ground-Glass Opacity-Featured Non-Small Cell Lung Cancer. Transl Lung Cancer Res 2023, 12, 2157–2168. [Google Scholar] [CrossRef]
- Chen, T.; Zhong, Y.; Wen, J.; Deng, J.; She, Y.; Zhu, Y.; Chen, Q.; Wu, C.; Hou, L.; Jiang, L.; et al. Prognostic Significance of the Proposed Residual Tumor Classification in Patients With NSCLC After Sleeve Lobectomy. JTO Clin Res Rep 2023, 4, 100574. [Google Scholar] [CrossRef] [PubMed]
- Vergé, R.; Rouch, A.; Rabinel, P.; Renaud, C.; Cazaux, M.; Brouchet, L. Evaluation of Uncertain Resection for Localized Non-Small Cell Lung Cancer: The Crucial Prognosis of Suboptimal Lymph Node Assessment. Ann Thorac Surg 2025, S0003-4975(25)00170-5. [CrossRef]
- Liu, C.; Wang, L.-C.; Chang, J.-F.; Lin, K.-H.; Yeh, Y.-C.; Hsu, P.-K.; Huang, C.-S.; Hsieh, C.-C.; Hsu, H.-S. The Role of Extensive Lymph Node Dissection in the New Grading System for Lung Adenocarcinoma. Eur J Surg Oncol 2024, 50, 108540. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.L.; Ocampo, P.S.S.; Xia, Y.; Zhong, H.; Russell, P.A.; Minami, Y.; Cooper, W.A.; Yoshida, A.; Bubendorf, L.; Papotti, M.; et al. A Grading System for Invasive Pulmonary Adenocarcinoma: A Proposal From the International Association for the Study of Lung Cancer Pathology Committee. Journal of Thoracic Oncology 2020, 15, 1599–1610. [Google Scholar] [CrossRef]
- Sakao, Y.; Miyamoto, H.; Yamazaki, A.; Oh, T.; Fukai, R.; Shiomi, K.; Saito, Y. Prognostic Significance of Metastasis to the Highest Mediastinal Lymph Node in Nonsmall Cell Lung Cancer. Ann Thorac Surg 2006, 81, 292–297. [Google Scholar] [CrossRef]
- Zheng, H.; Hu, X.; Jiang, G.; Gao, W.; Jiang, S.; Xie, H.; Ding, J.; Chen, C. Define Relative Incomplete Resection by Highest Mediastinal Lymph Node Metastasis for Non-Small Cell Lung Cancers: Rationale Based on Prognosis Analysis. Lung Cancer 2011, 72, 348–354. [Google Scholar] [CrossRef]
- Park, S.Y.; Byun, G.E.; Lee, C.Y.; Lee, J.G.; Kim, D.J.; Paik, H.C.; Chung, K.Y. Clinical Implications of Uncertain Resection in Scenarios of Metastasis of the Highest or Most Distant Mediastinal Lymph Node Station Following Surgical Treatment of Non-Small-Cell Lung Cancer. Lung Cancer 2019, 138, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.D.; Liu, G.W.; Li, X.; Sui, X.Z.; Yang, F.; Wang, J. Propensity-Matched Analysis of Clinical Relevance of the Highest Mediastinal Lymph Node Metastasis. Ann Thorac Surg 2021, 111, 277–282. [Google Scholar] [CrossRef]
- Marziali, V.; Frasca, L.; Ambrogi, V.; Patirelis, A.; Longo, F.; Crucitti, P. Prognostic Significance of Uncertain Resection for Metastasis in the Highest Mediastinal Lymph Node after Surgery for Clinical N0 Non-Small Cell Lung Cancer. Front Surg 2023, 10, 1115696. [Google Scholar] [CrossRef]
- Liu, J.; Shi, Z.; Cao, B.; Wang, Z.; Zhang, N.; Liu, J. Prognostic Significance of the Highest Mediastinal Lymph Node Involvement in Patients with Stage III-N2 Non-Small Cell Lung Cancer. Ann Surg Oncol 2024. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Watanabe, S.; Kawachi, R.; Suzuki, K.; Asamura, H. The Impact of Residual Tumor Morphology on Prognosis, Recurrence, and Fistula Formation after Lung Cancer Resection. J Thorac Oncol 2008, 3, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Martini, N.; Beattie, E.J.; Cliffton, E.E.; Melamed, M.R. Radiologically Occult Lung Cancer: Report of 26 Cases. Surgical Clinics of North America 1974, 54, 811–823. [Google Scholar] [CrossRef]
- Soorae, A.S.; Stevenson, H.M. Survival with Residual Tumor on the Bronchial Margin after Resection for Bronchogenic Carcinoma. J Thorac Cardiovasc Surg 1979, 78, 175–180. [Google Scholar] [CrossRef]
- Law, M.R.; Hodson, M.E.; Lennox, S.C. Implications of Histologically Reported Residual Tumour on the Bronchial Margin after Resection for Bronchial Carcinoma. Thorax 1982, 37, 492–495. [Google Scholar] [CrossRef]
- Heikkilä, L.; Harjula, A.; Suomalainen, R.J.; Mattila, P.; Mattila, S. Residual Carcinoma in Bronchial Resection Line. Ann Chir Gynaecol 1986, 75, 151–154. [Google Scholar]
- Whyte, R.I.; Kaplan, D.K.; Sharpe, D.A.; Muehrcke, D.D.; Donnelly, R.J. Carcinoma of the Bronchus with Unsuspected Microscopic Resection-Line Involvement. Cancer 1988, 62, 1014–1016. [Google Scholar] [CrossRef]
- Lacasse, Y.; Bucher, H.C.; Wong, E.; Griffith, L.; Walter, S.; Ginsberg, R.J.; Guyatt, G.H. “Incomplete Resection” in Non-Small Cell Lung Cancer: Need for a New Definition. Canadian Lung Oncology Group. Ann Thorac Surg 1998, 65, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Ruffini, E.; Bongiovanni, M.; Cavallo, A.; Filosso, P.L.; Giobbe, R.; Mancuso, M.; Molinatti, M.; Oliaro, A. The Significance of Associated Pre-Invasive Lesions in Patients Resected for Primary Lung Neoplasms. Eur J Cardiothorac Surg 2004, 26, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Collaud, S.; Bongiovanni, M.; Pache, J.-C.; Fioretta, G.; Robert, J.H. Survival According to the Site of Bronchial Microscopic Residual Disease after Lung Resection for Non-Small Cell Lung Cancer. J Thorac Cardiovasc Surg 2009, 137, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Fernández, E.; de Castro, P.L.; Astudillo, J.; Fernández-Llamazares, J.; Bronchogenic Carcinoma Cooperative Group of the Spanish Society of Pneumology and Thoracic Surgery Bronchial Stump Infiltration after Lung Cancer Surgery. Retrospective Study of a Series of 2994 Patients. Interact Cardiovasc Thorac Surg 2009, 9, 182–186. [Google Scholar] [CrossRef]
- Lee, G.D.; Kim, D.K.; Jang, S.J.; Choi, S.H.; Kim, H.R.; Kim, Y.-H.; Park, S.-I. Significance of R1-Resection at the Bronchial Margin after Surgery for Non-Small-Cell Lung Cancer. European Journal of Cardio-Thoracic Surgery 2017, 51, 176–181. [Google Scholar] [CrossRef]
- Aokage, K.; Yoshida, J.; Ishii, G.; Enatsu, S.; Hishida, T.; Nishimura, M.; Nishiwaki, Y.; Nagai, K. The Impact on Survival of Positive Intraoperative Pleural Lavage Cytology in Patients with Non–Small-Cell Lung Cancer. The Journal of Thoracic and Cardiovascular Surgery 2010, 139, 1246–1252.e1. [Google Scholar] [CrossRef]
- Nakagawa, T.; Okumura, N.; Kokado, Y.; Miyoshi, K.; Matsuoka, T.; Kameyama, K. Clinical Relevance of Intraoperative Pleural Lavage Cytology in Non-Small Cell Lung Cancer. The Annals of Thoracic Surgery 2007, 83, 204–208. [Google Scholar] [CrossRef]
- Higashiyama, M.; Oda, K.; Okami, J.; Maeda, J.; Kodama, K.; Takenaka, A.; Nakayama, T.; Yoneda, G. Prognostic Value of Intraoperative Pleural Lavage Cytology for Lung Cancer without Carcinomatous Pleuritis: Importance in Patients with Early Stage Disease during Long-Term Follow-Up. European Journal of Cardio-Thoracic Surgery 2009, 35, 337–342. [Google Scholar] [CrossRef]
- Kawachi, R.; Nakazato, Y.; Masui, K.; Takei, H.; Koshi-ishi, Y.; Goya, T. Clinical Significance of Pleural Lavage Cytology for Non-Small Cell Lung Cancer: Is Surgical Resection Valid for Patients with Positive Pleural Lavage Cytology? Interactive CardioVascular and Thoracic Surgery 2009, 9, 265–268. [Google Scholar] [CrossRef]
- Nakamura, T.; Suzuki, K.; Mochizuki, T.; Ohde, Y.; Kobayashi, H.; Nakamura, H.; Toyoda, F. Prognostic Significance and Possibility in Guiding Adjuvant Therapy of the Pleural Lavage Cytology in Patients with Non-Small Cell Lung Cancer. Interact Cardiovasc Thorac Surg 2009, 8, 321–324. [Google Scholar] [CrossRef]
- Shintani, Y.; Ohta, M.; Iwasaki, T.; Ikeda, N.; Kanou, T.; Tomita, E.; Nakagawa, K.; Yasumitsu, T.; Ohno, Y. Intraoperative Pleural Lavage Cytology after Lung Resection as an Independent Prognostic Factor for Staging Lung Cancer. The Journal of Thoracic and Cardiovascular Surgery 2009, 137, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Kameyama, K.; Okumura, N.; Miyaoka, E.; Asamura, H.; Yoshino, I.; Tada, H.; Fujii, Y.; Nakanishi, Y.; Eguchi, K.; Mori, M.; et al. Prognostic Value of Intraoperative Pleural Lavage Cytology for Non–Small Cell Lung Cancer: The Influence of Positive Pleural Lavage Cytology Results on T Classification. The Journal of Thoracic and Cardiovascular Surgery 2014, 148, 2659–2664. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, Y.; Nakamura, H.; Miwa, K.; Adachi, Y.; Fujioka, S.; Haruki, T.; Horie, Y. Prognostic Significance of Pleural Lavage Cytology after Thoracotomy and before Closure of the Chest in Lung Cancer. Interactive CardioVascular and Thoracic Surgery 2009, 9, 102–106. [Google Scholar] [CrossRef]
- Baba, T.; Uramoto, H.; Kuwata, T.; Takenaka, M.; Chikaishi, Y.; Oka, S.; Nagata, Y.; Shigematsu, Y.; Shimokawa, H.; Nakagawa, M.; et al. Intrapleural Chemotherapy Improves the Survival of Non-Small Cell Lung Cancer Patients with Positive Pleural Lavage Cytology. Surg Today 2013, 43, 648–653. [Google Scholar] [CrossRef]
- Kaneda, M.; Yokoi, K.; Ito, S.; Niwa, H.; Takao, M.; Kondo, R.; Arimura, T.; Saito, Y. The Value of Pleural Lavage Cytology Examined during Surgery for Primary Lung Cancer. European Journal of Cardio-Thoracic Surgery 2012, 41, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, N.; Shiono, S.; Abiko, M.; Abe, M.; Watanabe, K.; Watanabe, I.; Uematsu, M.; Ogata, S.; Sato, T.; Tamura, G. Positive Intraoperative Pleural Lavage Cytology Is a Predictive Marker of Disease Recurrence in Stage I Lung Adenocarcinoma. Interactive CardioVascular and Thoracic Surgery 2014, 18, 621–625. [Google Scholar] [CrossRef]
- Mazza, F.; Ferrari, E.; Maineri, P.; Dozin, B.; Ratto, G.B. Pleural Lavage Cytology Predicts Recurrence and Survival, Even in Early Non-Small Cell Lung Cancer. Surg Today 2015, 45, 322–328. [Google Scholar] [CrossRef]
- HOKKA, D.; UCHINO, K.; TANE, K.; OGAWA, H.; TANE, S.; TANAKA, Y.; TAUCHI, S.; NISHIO, W.; YOSHIMURA, M.; MANIWA, Y. Pleural Lavage Cytology as an Independent Prognostic Factor in Non-Small-Cell Lung Cancer Patients with Stage I Disease and Adenocarcinoma. Mol Clin Oncol 2015, 3, 244–248. [Google Scholar] [CrossRef]
- Nakao, M.; Hoshi, R.; Ishikawa, Y.; Matsuura, Y.; Uehara, H.; Mun, M.; Nakagawa, K.; Okumura, S. Prognosis of Non-Small-Cell Lung Cancer Patients with Positive Pleural Lavage Cytology. Interactive CardioVascular and Thoracic Surgery 2015, 20, 777–782. [Google Scholar] [CrossRef]
- Tomizawa, K.; Nishino, M.; Sesumi, Y.; Kobayashi, Y.; Sato, K.; Chiba, M.; Shimoji, M.; Suda, K.; Shimizu, S.; Sato, T.; et al. Prognostic Impact of Pleural Lavage Cytology in Patients with Primary Lung Cancer. Lung Cancer 2016, 102, 60–64. [Google Scholar] [CrossRef]
- Mizuno, K.; Isaka, M.; Terada, Y.; Konno, H.; Mizuno, T.; Tone, K.; Kawata, T.; Nakajima, T.; Funai, K.; Ohde, Y. Intraoperative Rapid Diagnosis of Pleural Lavage Cytology in Non-Small Cell Lung Cancer. Gen Thorac Cardiovasc Surg 2024, 72, 127–133. [Google Scholar] [CrossRef]
- Mizuno, K.; Isaka, M.; Ono, M.; Hayakawa, T.; Terada, Y.; Yasuura, Y.; Kayata, H.; Konno, H.; Kojima, H.; Mizuno, T.; et al. Impact of Positive Pleural Lavage Cytology for Each Stage of Non-Small Cell Lung Cancer Patients. The Annals of Thoracic Surgery 2021, 111, 1696–1702. [Google Scholar] [CrossRef] [PubMed]
- Onodera, K.; Sakurada, A.; Hoshi, F.; Abe, J.; Hasumi, T.; Takahashi, S.; Saito, Y.; Okada, Y. Clinicopathological Features of Intraoperative Pleural Lavage Cytology for Non-Small Cell Lung Cancer. Gen Thorac Cardiovasc Surg 2020, 68, 164–169. [Google Scholar] [CrossRef]
- Nakamura, T.; Otsuki, Y.; Nakamura, H.; Funai, K. Pleural Lavage Cytology after Lung Resection in Patients with Non-Small Cell Lung Cancer and the Feasibility of 20 mL Saline Solution. Asian J Surg 2019, 42, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-M.; Ling, Z.-G.; Wu, Y.-B.; Cai, S.-Q.; Tang, Z.-M.; Wu, C.; Chen, Y.-Q. Prognostic Value of Pleural Lavage Cytology in Patients with Lung Cancer Resection: An Updated Meta-Analysis. PLoS One 2016, 11, e0157518. [Google Scholar] [CrossRef]
- Recuero Díaz, J.L.; Gatius Caldero, S.; Rosado Rodríguez, J.; Caamaño Villaverde, V.; Gómez de Antonio, D.; Tejerina, E.; Sánchez Moreno, L.; Martino González, M.; Moldes Rodríguez, M.; Abdulkader Nallib, I.; et al. Impact of Pleural Lavage Cytology Positivity on Early Recurrence After Surgery for Non-Small Cell Lung Cancer. Arch Bronconeumol. [CrossRef]
- Vallières, E.; Houtte, P.V.; Travis, W.D.; Rami-Porta, R.; Goldstraw, P. Carcinoma In Situ at the Bronchial Resection Margin: A Review. Journal of Thoracic Oncology 2011, 6, 1617–1623. [Google Scholar] [CrossRef]
- Feinstein, A.R.; Sosin, D.M.; Wells, C.K. The Will Rogers Phenomenon. New England Journal of Medicine 1985, 312, 1604–1608. [Google Scholar] [CrossRef]
- Riquet, M. Curage : Ô Désespoir, ô Will Rogers et Okies ! Revue des Maladies Respiratoires 2005, 22, 929–931. [Google Scholar] [CrossRef] [PubMed]
- Tsitsias, T.; Okiror, L.; Veres, L.; King, J.; Harrison-Phipps, K.; Routledge, T.; Pilling, J.; Bille, A. New N1/N2 Classification and Lobe Specific Lymphatic Drainage: Impact on Survival in Patients with Non-Small Cell Lung Cancer Treated with Surgery. Lung Cancer 2021, 151, 84–90. [Google Scholar] [CrossRef]
- Schlachtenberger, G.; Doerr, F.; Menghesha, H.; Heldwein, M.B.; Hagmeyer, L.; Michel, M.; Schaefer, S.C.; Wahlers, T.; Hekmat, K. Postoperative Long-Term Survival of Non-Small Cell Lung Cancer Patients with Skip-N2 Metastases. Surgical Oncology 2021, 38, 101505. [Google Scholar] [CrossRef]
- Yu, L.; Xu, J.; Qiao, R.; Zhong, H.; Han, B.; Zhong, R. Patterns of Recurrence and Survival Rate After Complete Resection of Pathological Stage N2 Small-Cell Lung Cancer. Front Oncol 2021, 11, 675354. [Google Scholar] [CrossRef] [PubMed]
- Stamatis, G.; Müller, S.; Weinreich, G.; Schwarz, B.; Eberhardt, W.; Pöttgen, C.; Aigner, C. Significantly Favourable Outcome for Patients with Non-Small-Cell Lung Cancer Stage IIIA/IIIB and Single-Station Persistent N2 (Skip or Additionally N1) Disease after Multimodality Treatment. Eur J Cardiothorac Surg 2022, 61, 269–276. [Google Scholar] [CrossRef]
- Ogawa, H.; Uchino, K.; Tanaka, Y.; Shimizu, N.; Okuda, Y.; Tane, K.; Tauchi, S.; Nishio, W.; Maniwa, Y.; Yoshimura, M. Efficacy of Adjuvant Chemotherapy for Lung Adenocarcinoma Patients with Positive Pleural Lavage Cytology Findings. Interactive CardioVascular and Thoracic Surgery 2015, 21, 34–39. [Google Scholar] [CrossRef]
- Lee, J.; Hong, Y.S.; Cho, J.; Lee, J.; Lee, G.; Kang, D.; Yun, J.; Jeon, Y.J.; Shin, S.; Cho, J.H.; et al. Reclassifying the International Association for the Study of Lung Cancer Residual Tumor Classification According to the Extent of Nodal Dissection for NSCLC: One Size Does Not Fit All. Journal of Thoracic Oncology 2022, 17, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Zhang, S.W.; Han, J.; Wang, Z.; Rong, Y.; Liu, J.F. [The impact of uncertainty resection on the prognosis of non-small cell lung cancer]. Zhonghua Wai Ke Za Zhi 2024, 62, 764–770. [Google Scholar] [CrossRef]
- Zhang, Y.; Fu, F.; Wen, Z.; Deng, L.; Wang, S.; Li, Y.; Chen, H. Segment Location and Ground Glass Opacity Ratio Reliably Predict Node-Negative Status in Lung Cancer. The Annals of Thoracic Surgery 2020, 109, 1061–1068. [Google Scholar] [CrossRef]
- Darling, G.E.; Allen, M.S.; Decker, P.A.; Ballman, K.; Malthaner, R.A.; Inculet, Richard. ; Jones, D.R.; McKenna, R.J.; Landreneau, R.J.; Rusch, V.W.; et al. Randomized Trial of Mediastinal Lymph Node Sampling Versus Complete Lymphadenectomy During Pulmonary Resection in the Patient with N0 or N1 (Less Than Hilar) Non-Small Cell Carcinoma: Results of the ACOSOG Z0030 Trial. J Thorac Cardiovasc Surg 2011, 141, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Murthy, S.C. Less Is More… (More or Less…). The Journal of Thoracic and Cardiovascular Surgery 2011, 141, 670–672. [Google Scholar] [CrossRef]
- Darling, G.E. Lymph Node Assessment in Early Stage Non-Small Cell Lung Cancer Lymph Node Dissection or Sampling? Gen Thorac Cardiovasc Surg 2020, 68, 716–724. [Google Scholar] [CrossRef]
- Marziali, V.; Frasca, L.; Longo, F.; Vega, R.; Crucitti, P. The Wide Range of Uses of Indocyanine Green in Thoracic Surgery: State of Art. Journal of Surgery 2022. [Google Scholar]
- Gregor, A.; Ujiie, H.; Yasufuku, K. Sentinel Lymph Node Biopsy for Lung Cancer. Gen Thorac Cardiovasc Surg 2020, 68, 1061–1078. [Google Scholar] [CrossRef]
- Le Pechoux, C.; Pourel, N.; Barlesi, F.; Lerouge, D.; Antoni, D.; Lamezec, B.; Nestle, U.; Boisselier, P.; Dansin, E.; Paumier, A.; et al. Postoperative Radiotherapy versus No Postoperative Radiotherapy in Patients with Completely Resected Non-Small-Cell Lung Cancer and Proven Mediastinal N2 Involvement (Lung ART): An Open-Label, Randomised, Phase 3 Trial. Lancet Oncol 2022, 23, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez De Dios, N.; Navarro-Martin, A.; Cigarral, C.; Chicas-Sett, R.; García, R.; Garcia, V.; Gonzalez, J.A.; Gonzalo, S.; Murcia-Mejía, M.; Robaina, R.; et al. GOECP/SEOR Radiotheraphy Guidelines for Non-Small-Cell Lung Cancer. World J Clin Oncol 2022, 13, 237–266. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, G.; Choy, H.; Bradley, J.; Rosenzweig, K.E.; Bogart, J.; Curran, W.J.; Gore, E.; Langer, C.; Louie, A.V.; Lutz, S.; et al. Adjuvant Radiation Therapy in Locally Advanced Non-Small Cell Lung Cancer: Executive Summary of an American Society for Radiation Oncology (ASTRO) Evidence-Based Clinical Practice Guideline. Practical Radiation Oncology 2015, 5, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Kris, M.G.; Gaspar, L.E.; Chaft, J.E.; Kennedy, E.B.; Azzoli, C.G.; Ellis, P.M.; Lin, S.H.; Pass, H.I.; Seth, R.; Shepherd, F.A.; et al. Adjuvant Systemic Therapy and Adjuvant Radiation Therapy for Stage I to IIIA Completely Resected Non–Small-Cell Lung Cancers: American Society of Clinical Oncology/Cancer Care Ontario Clinical Practice Guideline Update. JCO 2017, 35, 2960–2974. [Google Scholar] [CrossRef]
- Zhu, M.; Li, S.; Yuan, L.; Liu, S.; Li, J.; Zhang, D.; Chen, J.; Jiang, J.; Xu, Z. The High-Risk Features and Effect of Postoperative Radiotherapy on Survival for Patients with Surgically Treated Stage IIIA-N2 Non-Small Cell Lung Cancer. World Journal of Surgical Oncology 2023, 21, 238. [Google Scholar] [CrossRef]
- Zhang, C.-C.; Hou, R.-P.; Xia, W.-Y.; Zeng, W.-Q.; Liu, J.; Wang, J.-M.; Lv, C.-X.; Luo, Q.-Q.; Zhao, H.; Yu, W.; et al. Prognostic Index for Estimating the Survival Benefit of Postoperative Radiotherapy in Pathologic N2 Non–Small Cell Lung Cancer: A Real-World Validation Study. Lung Cancer 2021, 156, 100–108. [Google Scholar] [CrossRef]
- Zhang, C.-C.; Yu, W.; Zhang, Q.; Cai, X.-W.; Feng, W.; Fu, X.-L. A Decision Support Framework for Postoperative Radiotherapy in Patients with Pathological N2 Non-Small Cell Lung Cancer. Radiother Oncol 2022, 173, 313–318. [Google Scholar] [CrossRef]
- Zeng, W.-Q.; Feng, W.; Xie, L.; Zhang, C.-C.; Yu, W.; Cai, X.-W.; Fu, X.-L. Postoperative Radiotherapy for Resected Stage IIIA-N2 Non-Small-Cell Lung Cancer: A Population-Based Time-Trend Study. Lung 2019, 197, 741–751. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Wang, H.; Xiu, W.; Tian, X.; Gong, Y. Uncertain Resection of Highest Mediastinal Lymph Node Positive among pN2 Non-Small Cell Lung Cancer Patients: Survival Analysis of Postoperative Radiotherapy and Driver Gene Mutations. Jpn J Radiol 2023, 41, 551–560. [Google Scholar] [CrossRef]
- Guo, J.; Zhang, L.; Zhang, L.; Wu, J.; Xu, L.; E, H.; Li, C.; Wu, H.; Zhao, D.; Hu, Y.; et al. The Additional Radiotherapy to Adjuvant Chemotherapy Improves the Prognosis of Stage III-N2 with Highest Mediastinal Lymph Node Metastasis in Non-Small Cell Lung Cancer. J Cancer Res Clin Oncol 2023, 149, 13311–13321. [Google Scholar] [CrossRef] [PubMed]
- Nath, T.S.; Mohamed, N.; Gill, P.K.; Khan, S. A Comparative Analysis of Video-Assisted Thoracoscopic Surgery and Thoracotomy in Non-Small-Cell Lung Cancer in Terms of Their Oncological Efficacy in Resection: A Systematic Review. Cureus 2022, 14, e25443. [Google Scholar] [CrossRef] [PubMed]
- Altorki, N.; Wang, X.; Damman, B.; Mentlick, J.; Landreneau, R.; Wigle, D.; Jones, D.R.; Conti, M.; Ashrafi, A.S.; Liberman, M.; et al. Lobectomy, Segmentectomy, or Wedge Resection for Peripheral Clinical T1aN0 Non-Small Cell Lung Cancer: A Post Hoc Analysis of CALGB 140503 (Alliance). J Thorac Cardiovasc Surg 2024, 167, 338–347.e1. [Google Scholar] [CrossRef] [PubMed]
- Detterbeck, F.C.; Ostrowski, M.; Hoffmann, H.; Rami-Porta, R.; Osarogiagbon, R.U.; Donnington, J.; Infante, M.; Marino, M.; Marom, E.M.; Nakajima, J.; et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for Revision of the Classification of Residual Tumor After Resection for the Forthcoming (Ninth) Edition of the TNM Classification of Lung Cancer. J Thorac Oncol 2024, S1556-0864(24)00129-1. [CrossRef]
Table 1.
Published series regarding IASLC 2005 classification.
| Répartition (%) | Reason for reclassification (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author, year, country | Design | Patients (n) | R0 | R(un) | R1+2 | Insufficient LND | HMLN + | CIS BRM | Cy+ | HR OS (p) |
| Gagliasso et al.[28], 2017, Italy | Retrospective, Single Instutition | pT1-4N0-2M0 (1277) | 1003 (78,5%) | 185 (14,5%) | 89 (7%) |
107 (56,6%) | 76 (41%) |
5 (2,6%) |
NA | 1,69 (0,0001) |
| Edwards et al.[29], 2019, mainly Japan | Retrospective, International database | pT1-4N0-3M0 (14712) | 6070 (41%) | 8185 (56%) | 457 (3%) | 7824 (95,7%) | 312 (3,8%) | 11 (0,01%) |
34 (0,5%) |
N+ 1.27 (< 0.001) |
| Osarogiagbon et al.[30], 2019, USA | Retrospective, Population-based | Resected NSCLC (3361) | 1119 (33%) | 2044 (61%) | 198 (6%) | 2004 (98%) |
119 (5,8%) | 0 (0%) |
3 (0,1%) |
1,36 (<0,0001) |
| Yun et al.[31], 2021, South Korea | Retrospective, Single Instutition | pN2 NSLC(1039) | 432 (41,6%) | 212 (20,4%) | 395 (38%) | 21 (10,2%) |
185 (89,8%) | 6 (from R1) |
NA | 1.06 (0.595) |
| Wang et al.[32], 2022, China | Retrospective, Single Instutition | pT1-4N0-2M0 (2782) | 1897 (68%) | 885 (32%) | 0 (0%) | 717 (81%) |
168 (19%) | 0 | 0 | 1.302 (0,003) |
| Ren et al.[33], 2022, China | Retrospective, Single Instutition | Resected NSCLC (5293) | 3819 (72,1%) | 1371 (25,9%) | 103 (1,9%) | 929 (67,7%) |
511 (37,2%) | 2 | 11 | 1,41 (0,001) |
| Kadomatsu et al.[34], 2022, Japan | Retrospective, Single Instutition | Resected NSCLC (355) | 197 (55,5%) | 158 (44,5%) | 0 (0%) | 137 (87%) |
8 (5%) | 3 (2%) |
10 (6%) |
N+ 2,657 (0,007) |
| Lee et al.[35], 2023, South Korea | Retrospective, Single Instutition | Stage III-N2 (910) | 302 (33,2%) | 329 (36,2%) | 279 (30,7%) | 278 (84,5%) | 104 (31,6%) | 0 | NA | 1,18 (p for trend 0,002) |
| Wen et al.[36] 2023, China | Retrospective, Single Instutition | Resected NSCLC (5200) | 3228 (62%) | 1727 (33%) | 145 (5%) | 1179 (68,3%) | 663 (38,3%) | 3 (0,2%) | NA | 1,4 (<0,001) |
| Chen et al.[37], 2023 China | Retrospective, Single Instutition | Sleeve lobectomy (682) | 489 (71,7%) | 110 (16,1%) | 83 (12,2%) | 28 (25%) | 82 (74%) | 14 (12%) | 0 | 1,59 (0,023) |
| Vergé et al.[38], 2025 France |
Retrospective, Single Instutition | Resected cN0M0 (1108) | 732 (66.1%) | 291 (26.2%) | 85 (7.7%) | 251 (86.3%) | 40 (13,7%) | 2 (0.6%) | NA | 1.26 (<0.001) |
| Liu et al[39], 2024 Taiwan |
Retrospective, Single Instutition | Resected adenocarcinomas (1258) | 429 (33.9%) | 829 (65.9) | 0 (excluded) | 829 (100%) | NA | NA | NA | 1.57 (0.001) |
LND : Lymph Node dissection ; HMLN+ : Positive Highest Mediastinal Lymph Node; CIS BRM: Carcinoma In Situ at Bronchus Resection Margin; Cy+: Positive pleural Lavage Cytology; HR: Hazard Ratio; OS: Overall Survival; NA: Not Available.
Table 3.
Published series regarding CIS BRM.
| Author, year | Patients (n) | CIS (n) | SCC (n) | CIS % of Population | Local Recurrence (n) | 5-year survival CIS |
|---|---|---|---|---|---|---|
| Martini et al.[48], 1974 | 26 | 2 | 2 | 7.6 | 0 | NA |
| Soorae et al.[49], 1979 | 434 | 10 | 10 | 2.3 | NA | 70 |
| Law et al.[50], 1982 | 1000 | 9 | 9 | 0.9 | NA | 66.7 |
| Heikkila et al.[51], 1986 | 1069 | 5 | NA | 0.46 | NA | NA |
| Whyte et al.[52], 1988 | 560 | 2 | 2 | 0.36 | NA | NA |
| Lacasse et al.[53], 1998 | 399 | 3 | NA | 0.8 | NA | NA |
| Ruffini et al.[54], 2004 | 1090 | 5 | 5 | 0.45 | NA | NA |
| Kawaguchi et al.[47], 2008 | 4493 | 9 | 9 | 0.2 | 1 | 63 |
| Collaud et al.[55], 2009 | 584 | 3 | 3 | 0.5 | 2 | 100 |
| Fernandez et al.[56],2009 | 2994 | 52 | 45 | 1.7 | NA | NA |
| Total | 15,738 | 138 | 114 | 0.9 | / | / |
CIS : Carcinoma In Situ ; SCC : Squamous Cell Carcinoma ; NA : Not available.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



