Submitted:
14 March 2025
Posted:
17 March 2025
You are already at the latest version
Abstract
This study examines the extensive incidence of microplastics (MPs) within freshwater and Marine ecosystems, characterizing their distribution, composition, and potential health implications for immunosuppressed populations. Utilizing an extensive dataset curated through collaboration with global stakeholders, we systematically analyzed microplastic concentrations and types in various aquatic environments, correlating findings with prevailing environmental parameters such as temperature and turbidity. Our results indicate a pronounced presence of MPs in both Fresh water and Marine Water, with distinct variations. Freshwater ecosystems predominantly exhibited microplastics originating from urban wastewater and recreational activities, demonstrating higher concentrations of fragments and fibers indicative of local anthropogenic influences. In contrast, Marine environments showcased a more diverse spectrum of microplastic morphologies, including debris from larger plastic aggregates and microbeads, facilitated by extensive oceanic dispersal mechanisms. The analysis revealed significant bioaccumulation potential of these contaminants within aquatic organisms, raising concerns regarding food chain transfer and subsequent exposure risks to humans, particularly immunocompromised individuals. Pathological assessments suggest that MPs may exacerbate pre-existing health vulnerabilities by serving as vectors for harmful substances, including endocrine-disrupting chemicals, thus posing increased risks of impaired immune responsiveness and chronic inflammatory conditions. Given these findings, our research underscores the urgency for more rigorous monitoring protocols and public health strategies aimed at mitigating microplastic pollution and protecting at-risk populations. Thus, this investigation not only contributes to the growing body of knowledge regarding microplastic dynamics in aquatic ecosystems but also emphasizes the critical necessity for a multidisciplinary approach to address the intricate relationship between environmental contaminants and human health outcomes.
Keywords:
microplastics
; immunosuppressed population
; fresh water
; marine water
; post-organ transplant
; environmental pollution
Introduction
Microplastics (MPs) are small plastic particles measuring less than 5 millimeters (mm), commonly originating from various types of plastics used in everyday life. These fragments can ultimately find their way into the environment as waste, affecting places like the ocean, tap water, and soil [1]. Over the past few decades, the use of plastics has surged dramatically due to their affordability, lightweight nature, durability, and versatility. However, this increase in usage has led to escalating pollution issues resulting from improper plastic disposal. Currently, global plastic production is estimated at 270 million tons per year, while the associated waste generation is approximately 275 million tons [2]. The food chain becomes contaminated when microplastics enter through both natural foods and processed food products, typically during transportation, packaging, and storage. The danger posed by microplastics lies in their gradual degradation in the environment, which can assessments of the risks posed to both organisms and humans.
Humans are exposed to microplastics (MPs) through various pathways, including ingestion, inhalation, and skin contact, which can lead to their transfer into human tissues and organisms. It is estimated that the average person ingests approximately 0.1 to 5 grams of microplastics each week [3,4]. Individuals who primarily consume bottled water are estimated to ingest an additional 90,000 microplastic particles compared to those who only drink tap water, who consume approximately 4,000 extra particles. This highlights the significant difference in microplastic exposure based on the type of water consumed [5]. There is growing concern regarding plastic pollution from microplastics (MPs) in freshwater systems. Notably, microplastics larger than 200 μm have been found in the digestive tracts of 166 out of 240 samples of marine organisms that are safe for human consumption[6]. Given the extensive presence of microplastics (MPs) in both aquatic and terrestrial environments, their impact on organisms raises significant concerns. With water resources available to humans and marine life being contaminated with plastic pollution, it is crucial to maintain a robust immune defense system. This immunity is essential for protecting against the potential activation of immune responses and the associated toxicity from exposure to these foreign plastic particles in vertebrates[7,8]. The immune system consists of a variety of cells and factors that provide protection against foreign substances, including pathogens and microplastics (MPs). When MPs invade, innate immune cells, such as macrophages and neutrophils, are recruited to the site of exposure. These cells release inflammatory cytokines, such as IL-1β and TNF-α, to address the potential threat posed by the microplastics, thereby initiating an immune response to mitigate any harm[9]. Post-organ transplant patients are particularly susceptible to environmental contaminants, including microplastics (MPs), due to their reliance on immunosuppressive therapies that lower their immune function. This makes them more vulnerable to infections and impairs their ability to recover from cellular damage. The immunotoxic effects of MP uptake in cells primarily stem from oxidative stress, which is linked to the generation of reactive oxygen species (ROS) and danger-associated molecular patterns (DAMP). These DAMPs can activate innate immunity through toll-like receptors (TLRs), triggering a cascade of inflammatory responses that can further compromise the health of these vulnerable individuals. [10]. Exposure to microplastics (MPs) has been shown to up-regulate the expression of the TCIM (transcriptional and immune response regulator) gene[7], which promotes cell proliferation and inhibits apoptosis, serving as a protective mechanism for the body. It is crucial to understand the mechanisms underlying these adverse responses from microplastic ingestion, particularly in relation to organ systems in post-organ transplant patients, to effectively manage the associated health concerns.
Despite the widespread presence of MPs in the environment and their potential interactions with harmful pathogens, the combined effects of microplastic exposure on human health remain largely under-researched. This lack of knowledge poses serious risks, highlighting a critical need for more comprehensive studies that explore microplastic exposure, their bio-distribution in the body, and their interactions with the immune system to address potential immuno-safety issues effectively.
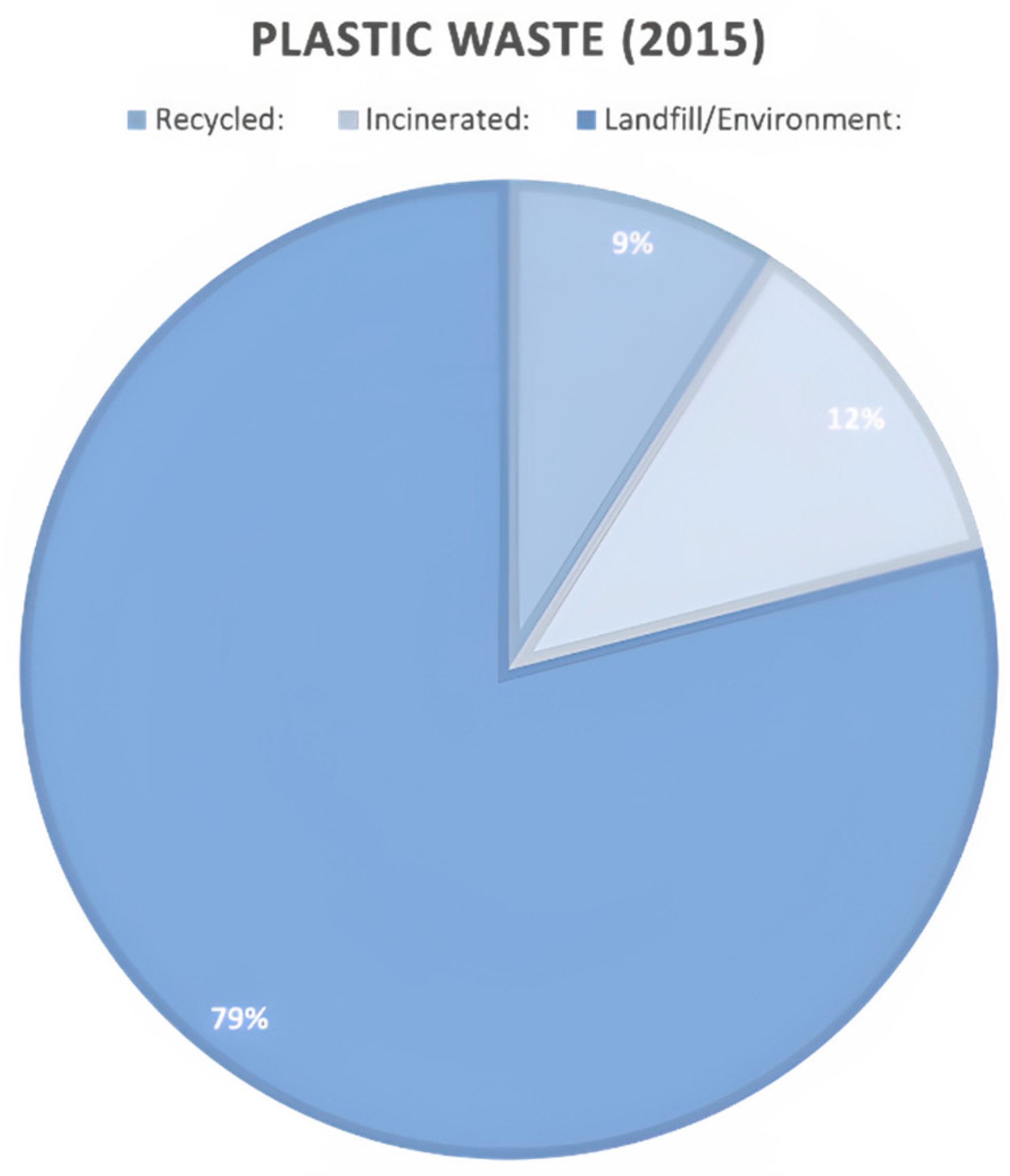
Figure 1.
Global Plastic Waste Disposal[11].
Figure 1.
Global Plastic Waste Disposal[11].
Methodology
Study Design
This review retained a comprehensive approach to evaluate the prevalence and characteristics of microplastics (MPs) in aquatic environments, leveraging data curated by Our World in Data in collaboration with global stakeholders. The focus encompassed diverse Freshwater and marine ecosystems, scrutinizing potential sources of MP contamination, which include industrial discharge, agricultural runoff, municipal waste output, and aquatic activities.
Ethical Considerations
The commitment of the study to adhere strictly to ethical guidelines in environmental research. Importantly, the research did not involve direct interaction with human or animal subjects, thereby mitigating ethical concerns related to the welfare of living beings. Furthermore, to ensure that the study protocols complied with established research standards, the methodologies were subject to review and approval by institutional review boards where applicable. This adherence not only reinforces the credibility of the research findings but also demonstrates a responsible approach towards conducting scientific inquiry, reflecting an awareness of ethical obligations in the realm of environmental science.
Health Risk Assessment
The Health Risk Assessment segment of this study employed a systematic and extensive review of current literature to evaluate the potential health implications of microplastic exposure, particularly focusing on populations that are immunocompromised, such as post-organ transplant patients. This assessment began with a detailed examination of various pathways through which microplastics can enter the human body, including ingestion through contaminated food and water, inhalation of airborne microplastics, and dermal contact. To quantitatively analyze the health risks associated with microplastics, we considered various factors, such as the concentrations of microplastics detected in water sources, the prevalence of these particles in food products, and the specific toxicity thresholds established in scientific literature. Comparisons were drawn with known biological effect thresholds to contextualize the implications of observed microplastic concentrations on health. Furthermore, the assessment investigated the bioaccumulation potential of microplastics in human tissues, considering how these particles could serve as vectors for harmful substances, including heavy metals and organic pollutants that adhere to their surfaces. This aspect is particularly critical for immunocompromised individuals, as their diminished ability to detoxify or excrete harmful substances may heighten the risk of adverse health effects. Incorporating data from toxicological studies, we evaluated how microplastics might induce inflammatory responses and other immune-toxic effects, thus potentially exacerbating existing health conditions in immunosuppressed populations.
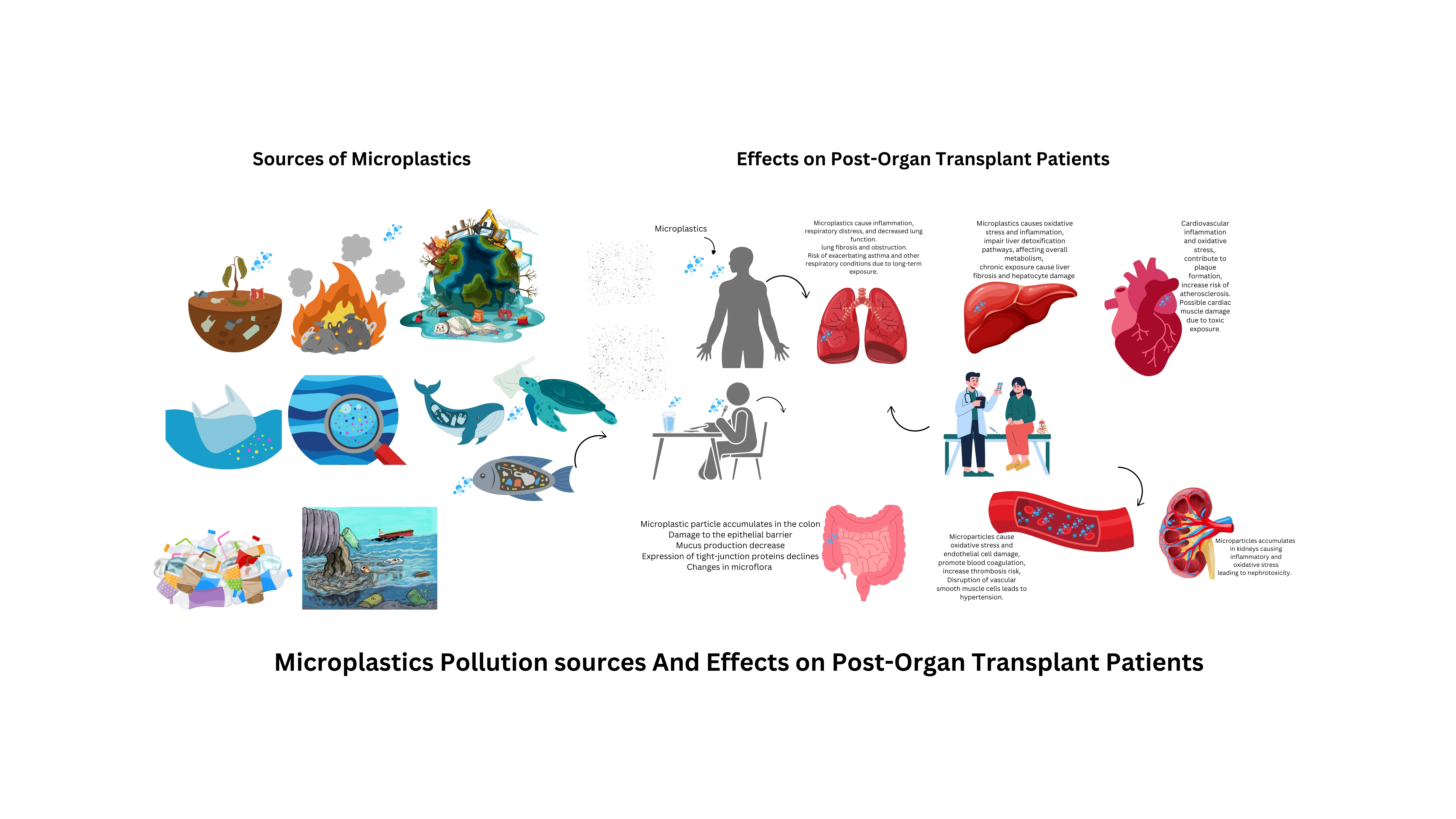
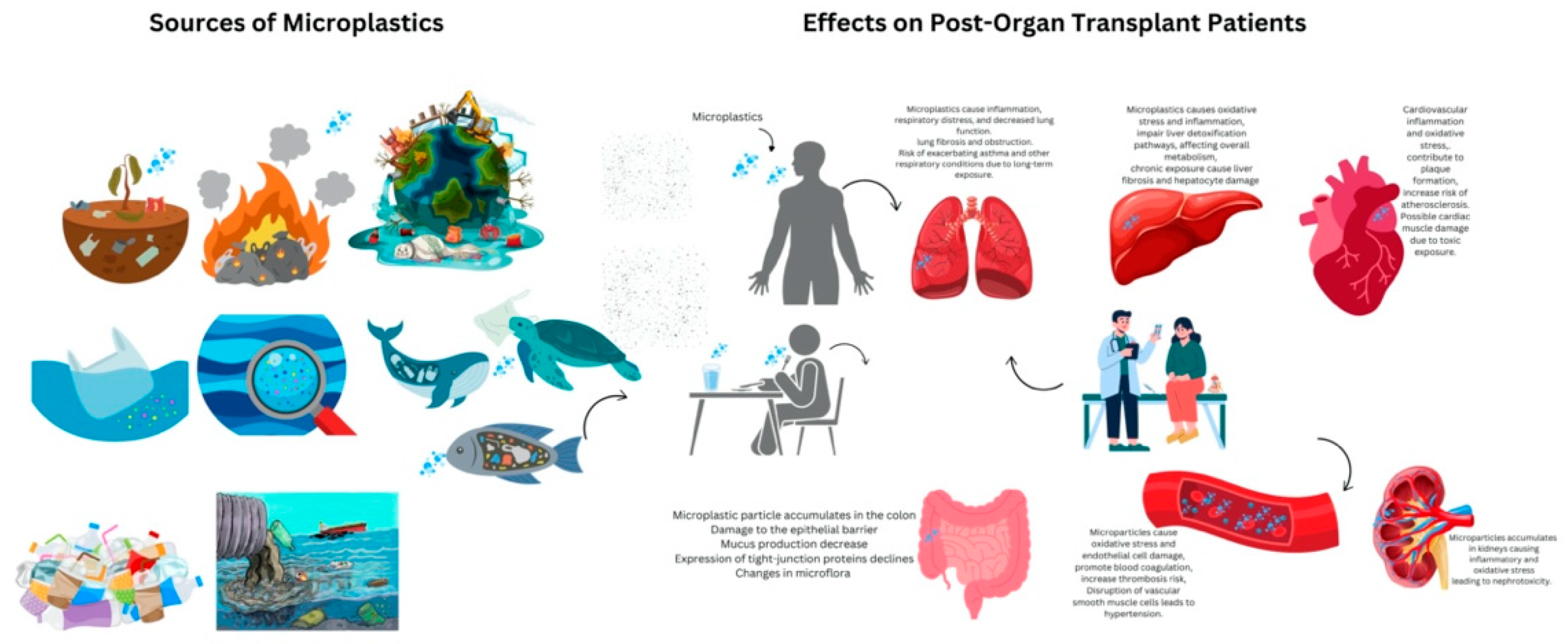
Figure 2.
Microplastics Pollution Sources and Effects on Post-Organ Transplant Patients.
Pathways of Microplastic Exposure
Microplastics (MPs) infiltrate our food and beverage systems primarily through two significant routes: packaging materials and environmental contamination. One of the most notable sources arises from food packaging, including plastic bottles, containers, and wraps[1]. During processes such as storage and heating, microplastic particles are released into these consumables. Numerous studies highlight that drinking water and beverages stored in plastic containers lead to the ingestion of substantial amounts of microplastics, with concentrations varying significantly based on factors such as brand, storage conditions, and the overall quality of packaging materials[12]. In addition to packaging, environmental contamination plays a crucial role in microplastic exposure. Seafood, in particular, is a major source due to ocean pollution by microplastics[13]. The use of contaminated water for irrigation further exacerbates the issue, contributing to the accumulation of microplastics in soil and resulting in indirect ingestion through the food chain[14]. While the general population faces risks of chronic microplastic exposure, organ transplant patients represent a uniquely vulnerable group due to their compromised immune systems and diminished capacity to detoxify environmental pollutants[15]. The excessive and long-term exposure to microplastics poses significant health hazards for the general populace, but immunosuppressed individuals experience particularly pronounced health issues. This underscores the urgent need for targeted research and intervention strategies to mitigate these risks and protect the health of at-risk populations.

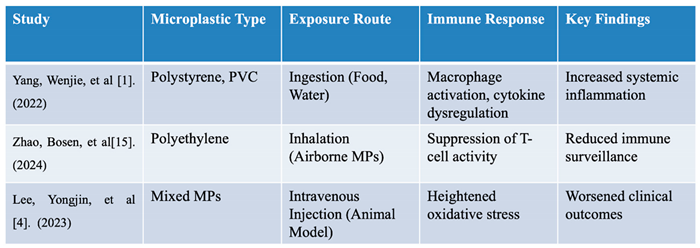
Table 1.
Key Studies on Microplastic Exposure and Immune System Impact.
Mechanisms of Microplastic Internalization
The continuous interaction between immune cells and external pathogens plays a crucial role in safeguarding health, particularly in the face of environmental contaminants such as microplastics (MPs). As the primary organs in direct contact with the external environment, the lungs and intestines are pivotal in the defense mechanisms against airborne and ingested pollutants[16,17]. In the pulmonary system, larger microplastic particles are generally removed through mucociliary clearance. However, smaller particles, especially those measuring less than 1μm, can evade these natural defenses. These diminutive MPs can penetrate bronchial epithelial cells, gaining access to endothelial cells and subsequently entering the circulatory system, thereby exposing the body to potential health hazards [1,16,18]. Notably, inhaled microplastics exhibit cytotoxic effects on human alveolar epithelial A549 cells. Once these particles are internalized, they disrupt essential cellular functions by inhibiting the cell cycle, triggering apoptosis, and promoting the expression of inflammation-related genes [19,20]. In the gastrointestinal tract, the uptake process diverges from the respiratory system. Here, M cells in the Peyer’s patches facilitate the endocytosis of microplastics, transporting them to mucosal lymphatic tissues [21]. Following inhalation or ingestion, microplastics can penetrate the air-blood barrier in the lungs or inflict damage on the gastrointestinal mucosa. Moreover, these particles have the potential to disseminate to vital organs including the liver, kidneys, and brain, subsequently activating the innate immune response. This immune activation may lead to dysfunction, particularly in cases of high exposure [22].
Impacts of Microplastics on Immune Function and Organ Systems
The innate immune system serves as the body's first line of defense against harmful microbes and is characterized as a non-specific immune response, reacting uniformly to all foreign organisms. Key players in this system are phagocytes, particularly white blood cells (leukocytes), which act as scavengers that engulf and digest antigens. Information regarding these antigens is presented on the surface of these scavenger cells, enabling recognition by the adaptive immune system [23]. Cytokines from the interleukin family are pivotal in modulating immune responses. Among the various immune cells, neutrophils stand out as the quickest responders, capable of forming phagosomes that non-specifically eliminate foreign pathogens, thereby playing a vital role in preventing immunotoxicity within the body. The interleukin one family cytokines play an important role during this process. Microplastics, particularly those originating from marine fiber fragments, are frequently ingested by aquatic species, such as fish. Common types of microplastics include polyethylene, polypropylene, and polystyrene, which can induce the release of neutrophil extracellular traps (NETs) [24] and enhance the degranulation of neutrophil granules. These microplastics can also enter the human body through inhalation and ingestion. Upon uptake, immune cells swiftly modulate transcriptional levels regarding enzymatic activities and cytokine release, evidenced by elevated levels of IL-1α and IL-1β following exposure to polystyrene (PS) microplastics [25]. Additionally, exposure adjusts the expression of genes associated with immune response, epithelial integrity, and lipid metabolism. In both fish and mouse models, high concentrations of polyethylene (PE) microplastics significantly alter the composition and diversity of the intestinal microbiome, inciting small intestine inflammation through the upregulation of TLR4, AP-1, and IRF5 [18]. Increased IL-1α levels in serum are noted, alongside diminished Th17 and Treg cell populations among CD4+ T lymphocytes post-exposure to microplastics [26]. For organ transplant recipients, the ingestion of microplastics poses substantial risks through interconnected pathways such as immune dysregulation, oxidative stress, cellular damage, and potential for bioaccumulation and toxicity. Research has shown the presence of various microplastic types in human stools, with a notable occurrence in patients suffering from IBD (inflammatory bowel disease), PP (polypropylene) predominantly showcasing at 62.8% and PET (polyethylene terephthalate) at 17.0% [27]. Microplastics instigate immune responses that can lead to chronic inflammation and activate immune cells, further perpetuating oxidative stress-related inflammatory pathways. Following MP uptake, immune cells exhibit noteworthy transcriptional changes, affecting both enzymatic activities and cytokine release. These particles can also inflict cellular injuries on innate immune cells involved in phagocytosis. Mitochondrial damage from airborne microplastics can incite oxidative stress that leads to cytotoxicity and inflammation through the MAPK and NF-κB signaling pathways. The NF-κB family is essential for regulating various immune mechanisms critical for inflammation, cell recruitment, and tissue microenvironment reshaping [28]. Recent studies have recorded significant alterations in populations of immunophenotypes, including CD4 and CD8 T lymphocytes, CD3+CD8+ T cells, CD19+ lymphocytes, dendritic cells, inflammatory monocytes, neutrophils, and anti-inflammatory macrophages [29,30]. Such immune responses can be particularly detrimental for transplant patients, highlighting the necessity of maintaining an intricate balance to prevent graft rejection. As macrophages, a key type of immune cell, react to microplastic exposure, they generate reactive oxygen species (ROS), fostering oxidative stress that damages DNA, lipids, and other cellular structures. This chronic oxidative stress can accelerate cellular aging and organ degeneration, possibly resulting in long-term health complications such as chronic allograft nephropathy, cardiovascular disease, and liver fibrosis. Addressing oxidative stress alongside immune responses is thus imperative. Moreover, increasing attention is being directed to the biological and immunological impacts following microplastic exposure. For example, amino-modified polystyrene microplastics (NH2-PSMPs) serve as a study model for assessing the effects of MPs on marine bivalves, which exhibit robust immune defenses against such materials [31]. Both polyvinyl chloride (PVC) and PE are noted for creating oxidative stress that leads to immune dysfunction in HKLs (head-kidney leucocytes) [32]. When polyethylene (PE) microplastics are administered orally to mice, the blood levels of neutrophils were found to increase, while there was a significant decrease in the overall white blood cell and lymphocyte counts. Concurrently, these PE microplastics were observed to migrate to the surface of mast cells within the mice's stomach, and abnormal accumulation of organelles, including mitochondria, was noted in spleen cells [33]. In related studies, polyvinyl chloride (PVC) and acrylonitrile butadiene styrene (ABS), another commonly used plastic, were utilized to investigate the effects of microplastics on human immune cells. Following exposure of peripheral blood mononuclear cells (PBMCs) to microplastics for 4–5 days, an activation of the cellular immune response was noted. Specifically, ABS and PVC were shown to stimulate the production of IL-6 and TNF-α, respectively, while both types suppressed histamine release. It was also observed that increasing concentrations of PVC microplastics led to a reduction in TNF-α and IL-2 levels, suggesting that microplastic exposure can trigger an immune response in human cells [34]. The effect of MPs on innate immunity memory is an emerging field with potential therapeutic applications that can help to understand the exact mechanism of interaction of plastic products with the human body.
Immunotoxicity of Microplastics Through Oxidative Stress
The immunotoxic effects associated with the uptake of microplastics (MPs) by cells are primarily induced by oxidative stress, which is driven by the generation of reactive oxygen species (ROS) and danger-associated molecular patterns (DAMP) [35]. The production of ROS occurs through two principal pathways: the impairment of the mitochondrial respiratory electron transport chain (ETC) and oxidative bursts triggered by NADPH oxidases (NOXs) following the entry of MPs into cells. DAMPs, in turn, have the potential to activate innate immune responses via toll-like receptors (TLRs), leading to a cascade of inflammatory reactions in immune cells [10,36]. Recent investigations into amino-modified polystyrene (NH2-PS) microplastics have demonstrated their detrimental effects across various trophic levels, particularly in metabolic processes. For instance, metabonomic analyses of freshwater cyanobacteria exposed to NH2-PS MPs for 48 hours revealed significant disruptions in arginine biosynthesis and glutathione metabolism. Specifically, this exposure down-regulated key metabolites such as L-glutamic acid, L-aspartic acid, and L-arginine, while concurrently up-regulating L-glutamine. Consequently, the release of O-phosphoethanolamine following NH2-PS MP exposure incited oxidative stress and membrane damage. Although this study was limited to short-term exposure, it sheds light on the toxic mechanisms exerted by freshwater phytoplankton and their potential implications for human health [37]. Moreover, the impact of microplastics extends to the promotion of cancer progression, particularly in human thyroid and lung malignancies, by influencing gene expression and exacerbating cancer deterioration [7]. The immunotoxic effects of microplastics (MPs) emphasize the significant interactions between these pollutants and the immune system. This situation reveals an urgent necessity for further research aimed at elucidating the immunotoxicity associated with these pervasive substances. A comprehensive understanding of the underlying mechanisms is vital for evaluating the broader health implications of microplastics and for formulating effective strategies to mitigate their detrimental effects. Table 2 summarizes the mechanism of MPs induced immunosuppression.
Role of Microplastic Endocrine Disruption and Bioaccumulation
Microplastics (MPs) are increasingly recognized as vectors for toxic chemicals, posing a significant threat to human and animal health. When these contaminated MPs enter the body, they can disrupt the endocrine system, impacting hormone-producing glands and their delicate signaling processes. They are called endocrine-disrupting chemicals or endocrine disruptors (EDs) [38]. These endocrine-disrupting chemicals (EDs) interfere with hormonal balance, crucial for overall health and particularly critical for vulnerable populations like post-transplant patients, where such disruptions can exacerbate pre-existing conditions like metabolic syndrome and cardiovascular diseases.[39]. Microplastics and endocrine disruptors (EDs) are contaminants of emerging concerns and ubiquitously present in aquatic ecosystems, establishing interactions that still are the subject of investigation due to their implications in the cotransport of pollutants[40]. These chemicals interfere with hormonal balance, which is crucial for recovery and overall health in post-transplant patients. Furthermore, MPs facilitate the bioaccumulation of toxic substances, including heavy metals and POPs (persistent organic pollutants), within tissues, especially detoxification organs like the liver and kidneys [41]. This accumulation further compromises organ function and increases the risk of chronic rejection in transplant recipients. The complex interactions between MPs and the bio-microenvironment present a major challenge in toxicity studies [15]. Like nanomaterials, MPs in biological fluids form a "biocorona" as immune proteins attach to their surfaces, a process influenced by particle size and charge. While MPs and EDs often coexist in soil, the impact of MPs on ED degradation and dissipation kinetics remains poorly understood, highlighting a critical gap in our knowledge regarding the combined toxicity of these emerging contaminants. EDs frequently coexist with MPs in soil environments. Specifically, the kinetic behavior of common EDs in MP-contaminated soil and the influence of MPs on their degradation require further investigation.
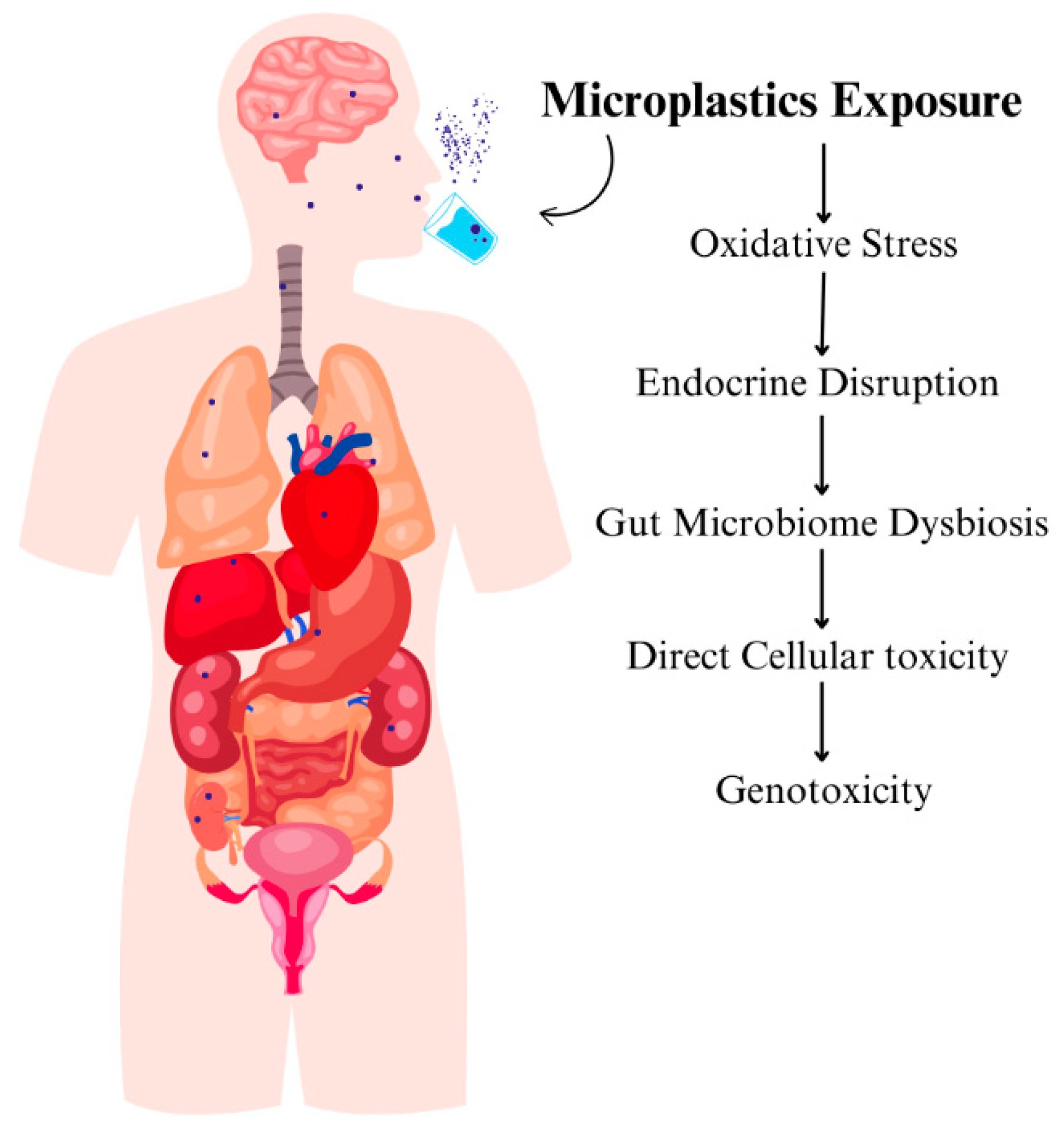
Figure 3.
Underlying Immune Responses Due to MPs exposure.
Discussion
Microplastics (MPs) have emerged as a significant environmental pollutant with potentially serious implications for both ecosystem health and human wellbeing, particularly among vulnerable populations, such as those who are immunosuppressed. This review examined the pathways of microplastic exposure, their environmental prevalence, and the potential health risks associated with their ingestion. Through this discussion, we elucidate the multifaceted nature of microplastics, their interactions within aquatic environments, and the corresponding implications for human health, especially for post-organ transplant patients. As evidenced by the research findings, microplastics are widely prevalent in both environments, albeit with differences in concentration, composition, and potential sources of contamination. In freshwater systems, the data exhibit significant microplastic concentrations, predominantly attributed to local runoff from agricultural activities, urban waste discharge, and recreational water use. This entry route amplifies the likelihood of ecosystem exposure, leading to the accumulation of microplastics in sediment and biota. Notably, small freshwater obligate species, such as certain fish and amphibians, may face increased risks as they ingest microplastics, which can compromise their health, growth, and reproductive success. Conversely, marine waters display a larger variety of microplastic shapes and types, driven by the ocean’s expansive transport mechanisms that distribute microplastics over greater distances. The predominant types in marine environments include fragments from the degradation of larger plastic items, fibers from textiles, and microbeads from personal care products. This diversity correlates with increased toxicity risks, not only due to the ingestion of microplastics by marine fauna but also because of the potential for bioaccumulation of toxic chemicals associated with these plastics, which may eventually reach humans through the seafood consumption pathway. Immunosuppressed individuals are particularly at risk from environmental exposure to microplastics. Following organ transplantation, patients are subjected to immunosuppressive therapies to prevent graft rejection, inherently compromising their immune defenses. This compromised state significantly limits their ability to detoxify and eliminate environmental toxins. Our findings indicate that microplastics may act as carriers for hazardous substances, including heavy metals and organic pollutants, which can exacerbate the health vulnerabilities already present in these patients. For instance, chronic exposure to microplastics can instigate systemic inflammatory responses and elicit immunotoxic effects that further deteriorate immune function, thus prolonging the susceptibility to infections and increasing the risk of complications during the critical post-transplant period. Moreover, the bioaccumulation of microplastics poses an additional concern, as their persistent nature can lead to elevated concentrations within human tissues. The presence of various microplastic types, particularly polypropylene (PP) and polyethylene terephthalate (PET), has been documented in the gastrointestinal tracts of patients, suggesting a potential pathway for systemic exposure following ingestion. The translocation of these particles into the bloodstream may facilitate the introduction of harmful pathogens or toxins, escalating risks of inflammatory responses and graft rejection as verified in recent observational studies. The immunological ramifications associated with microplastic exposure warrant scrutiny. Research demonstrates that MPs can activate innate immune responses through mechanisms involving toll-like receptors, thereby triggering inflammatory cascades that can overwhelm the already diminished immune capacity in transplant recipients. For example, increased levels of interleukin-1 alpha (IL-1α) and alterations in CD4+ T lymphocyte populations have been observed following microplastic exposure, indicating a dysregulated immune state that could predispose patients to chronic conditions[42].
The elevation of ROS levels in immunosuppressed individuals with already impaired cellular repair mechanisms can exacerbate tissue damage and inflammation, contributing to graft dysfunction and increasing vulnerability to opportunistic infections. Further complicating this dynamic is the impact of microplastics on the expression of key genes involved in immune regulation. Studies have shown that exposure to microplastics can up-regulate the expression of pro-inflammatory cytokines such as IL-6 and tumor necrosis factor-alpha (TNF-α). In immunosuppressed patients, this heightened inflammatory response can be particularly detrimental, as the delicate balance between immune activation and suppression is disrupted. The resulting chronic inflammation may not only impair graft survival but also increase the risk of developing post-transplant lymphoproliferative disorders (PTLD), a type of cancer associated with the immune response to foreign antigens [43,44].
Microplastics are ubiquitous in both freshwater and marine environments, arising from a variety of sources, including plastic waste, industrial discharges, and runoff from agricultural and urban areas. Recent studies estimate that approximately 8 million metric tons of plastics enter the oceans annually, contributing to the proliferation of microplastics as they degrade from larger plastic debris through mechanical, chemical, and photolytic processes[45] . Notably, MPs can vary significantly in shape, size, and polymer composition, with primary microplastics (manufactured small plastic particles) and secondary microplastics (degraded larger plastics) both contributing to environmental contamination. The widespread presence of these pollutants necessitates an understanding of their distribution dynamics and potential pathways of human exposure. Human exposure to microplastics primarily occurs through the consumption of contaminated food and drinking water. Evidence indicates that food packaging materials especially plastic containers are significant sources of microplastics in consumables. During food storage and preparation, MPs can leach into food items, especially when subjected to heat or prolonged contact with plastic materials [46]. Additionally, bottled water has been shown to contain microplastic concentrations that vary significantly based on brand and storage conditions, with one study reporting microplastic concentrations as high as 10.4 plastic particles per liter[47].
Environmental contamination also plays a critical role in the bioaccumulation of microplastics within aquatic food webs. Organisms at various trophic levels, from plankton to larger fish species, can inadvertently ingest microplastics, introducing these particles into the human food chain[48,49] . Figure 12 illustrates a comparative analysis of freshwater and marine water microplastics by shape type, emphasizing the sources of these pollutants, notably synthetic textiles and plastic degradation. As MPs accumulate within aquatic organisms, there is growing concern about the toxicological effects and potential transfer of harmful substances (like adsorbed pollutants or additives) to humans who consume these organisms. Moreover, the potential for microplastics to act as carriers for harmful substances is of significant concern. The leaching of toxic additives, such as plasticizers and stabilizers or even environmental contaminants adhered to the microplastics introduces additional challenges. These substances can further modulate immune responses by interfering with signaling pathways that govern immune cell activation and differentiation. For instance, compounds such as phthalates, commonly found within plastic materials, are known endocrine disruptors that can alter hormonal signaling pathways, leading to aberrant immune function. This disruption in communication can have far-reaching implications for allogeneic graft acceptance, potentially contributing to increased rates of rejection. The impact of microplastics on immune cell functionality, particularly macrophages and dendritic cells, also requires attention. These key players in the immune system are responsible for sensing environmental threats and orchestrating immune responses. Microplastic exposure has been shown to alter the antigen-presenting capabilities of dendritic cells, potentially impacting the ability to mount effective adaptive immune responses, which is crucial in immunocompromised individuals. Consequently, the impaired functionality of these cells can result in inadequate responses to infections, further complicating the health landscape for transplant patients.
The health implications of microplastic exposure, particularly for immunocompromised individuals, cannot be overstated. Studies have demonstrated that microplastics can provoke systemic inflammatory responses, disrupt gut microbiota, and elicit immunotoxic effects[50] . For immunosuppressed populations, such as post-organ transplant patients, the ingestion of microplastics may exacerbate existing health vulnerabilities. The presence of microplastics in the gut can facilitate the translocation of harmful pathogens or toxins into the bloodstream, potentially leading to complications such as chronic inflammation, infections, or even graft rejection [51,52]. Besides, the variability in individual responses to microplastic exposure may be influenced by genetic predispositions and the overall health status of a person, emphasizing the need for tailored risk assessments and health surveillance protocols for vulnerable groups. The interaction between microplastics and biochemicals in the body remains poorly understood, warranting further research to establish clear causal links between microplastic ingestion and specific health outcomes.
Despite the emerging evidence surrounding the health implications of microplastics, significant gaps remain in our understanding of their bio-distribution, long-term effects, and mechanisms of action within biological systems. The call for multidisciplinary research approaches that integrate toxicology, epidemiology, and environmental science is paramount to elucidate the complex interactions between microplastics, human health, and ecosystem dynamics [53]. Future studies should aim to implement longitudinal exposure assessments and experimental models that focus on immunotoxicity pathways related to microplastic ingestion. Such endeavors could lead to the identification of effective strategies to mitigate risks, enhance environmental resilience, and improve public health guidelines for affected populations. Understanding the interactions between microplastics and the immune system will aid in formulating appropriate dietary recommendations and public health interventions, particularly for immunocompromised individuals.
Conclusion
With widespread occurrence of microplastics in aquatic environments poses substantial challenges that affect not only ecological health but also critical human health outcomes. This article highlights the complex relationships between microplastics and aquatic ecosystem. The findings suggest that microplastics constitute a significant environmental hazard, particularly for immunocompromised individuals who may have heightened vulnerabilities to their detrimental effects. Microplastics threaten to alter immunological function, potentially leading to compromised immune responses, ineffective antigen presentation, and chronic inflammatory states. Such changes may heighten the risk of serious complications in susceptible populations, complicating their ability to respond to infections and exacerbating existing health issues. Therefore, it is crucial to address the synergistic threats posed by microplastics and their implications for human health through comprehensive research and proactive, multidisciplinary strategies aimed at reducing plastic pollution at its origin. Enhancing our understanding of the pathways by which microplastics affect both ecosystems and human health is essential for informing effective public health interventions and environmental policies. Prioritizing effective monitoring and mitigation strategies will be vital in protecting vulnerable groups while promoting the sustainability of aquatic ecosystems. As we deepen our investigation into microplastics, it becomes increasingly important to implement preventive measures that safeguard public health and preserve ecological integrity.
Abbreviation
Microplastics (MPs), Global Positioning System (GPS), Millimeters (mm), Toll-like receptors (TLRs), Fourier-transform infrared (FTIR), Neutrophil extracellular traps (NETs), Polypropylene (PP), Polystyrene (PS), Polyethylene (PE), Polyethylene terephthalate (PET), Polyvinyl chloride (PVC), Peripheral blood mononuclear cells (PBMCs), Acrylonitrile butadiene styrene (ABS), Reactive oxygen species (ROS), Amino-modified polystyrene microplastics (NH2-PSMPs), Post-transplant lymphoproliferative disorders (PTLD), Tumor necrosis factor-alpha (TNF-α), Danger-associated molecular patterns (DAMP), Interleukin-1 alpha (IL-1α), Endocrine-disrupting chemicals (EDs), Electron transport chain (ETC), IBD (inflammatory bowel disease), HKLs (head-kidney leucocytes), POPs (persistent organic pollutants).
References
- Yang, W.; Jannatun, N.; Zeng, Y.; Liu, T.; Zhang, G.; Chen, C.; Li, Y. Impacts of microplastics on immunity. Frontiers in toxicology 2022, 4, 956885. [Google Scholar] [PubMed]
- Jambeck, J.; Geyer, R.; Wilcox, C.; Siegler, T.; Perryman, M.; Andrady, A.; Narayan, R.; Law, K. Marine pollution. Plastic waste inputs from land into the ocean. Sci 2015, 347, 768–771. [Google Scholar]
- Senathirajah, K.; Attwood, S.; Bhagwat, G.; Carbery, M.; Wilson, S.; Palanisami, T. Estimation of the mass of microplastics ingested–A pivotal first step towards human health risk assessment. Journal of Hazardous Materials 2021, 404, 124004. [Google Scholar] [PubMed]
- Lee, Y.; Cho, J.; Sohn, J.; Kim, C. Health effects of microplastic exposures: current issues and perspectives in South Korea. Yonsei Medical Journal 2023, 64, 301. [Google Scholar]
- Mason, S.A.; Welch, V.G.; Neratko, J. Synthetic polymer contamination in bottled water. Frontiers in chemistry 2018, 6, 389699. [Google Scholar]
- Alfaro-Núñez, A.; Astorga, D.; Cáceres-Farías, L.; Bastidas, L.; Soto Villegas, C.; Macay, K.; Christensen, J.H. Microplastic pollution in seawater and marine organisms across the Tropical Eastern Pacific and Galápagos. Scientific reports 2021, 11, 6424. [Google Scholar]
- Limonta, G.; Mancia, A.; Benkhalqui, A.; Bertolucci, C.; Abelli, L.; Fossi, M.C.; Panti, C. Microplastics induce transcriptional changes, immune response and behavioral alterations in adult zebrafish. Scientific reports 2019, 9, 15775. [Google Scholar] [CrossRef]
- Li, L.a.; Xu, R.; Jiang, L.; Xu, E.G.; Wang, M.; Wang, J.; Li, B.; Hu, M.; Zhang, L.; Wang, Y. Effects of microplastics on immune responses of the yellow catfish Pelteobagrus fulvidraco under hypoxia. Frontiers in physiology 2021, 12, 753999. [Google Scholar] [PubMed]
- Lu, K.; Lai, K.P.; Stoeger, T.; Ji, S.; Lin, Z.; Lin, X.; Chan, T.F.; Fang, J.K.-H.; Lo, M.; Gao, L. Detrimental effects of microplastic exposure on normal and asthmatic pulmonary physiology. Journal of hazardous materials 2021, 416, 126069. [Google Scholar] [CrossRef]
- Gong, T.; Liu, L.; Jiang, W.; Zhou, R. DAMP-sensing receptors in sterile inflammation and inflammatory diseases. Nature Reviews Immunology 2020, 20, 95–112. [Google Scholar]
- Yang, Z.; Lü, F.; Zhang, H.; Wang, W.; Shao, L.; Ye, J.; He, P. Is incineration the terminator of plastics and microplastics? Journal of Hazardous Materials 2021, 401, 123429. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenberghe, L.; Janssen, C.R. Microplastics in bivalves cultured for human consumption. Environmental pollution 2014, 193, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Love, D.C.; Rochman, C.M.; Neff, R.A. Microplastics in seafood and the implications for human health. Current environmental health reports 2018, 5, 375–386. [Google Scholar] [CrossRef]
- Amobonye, A.; Bhagwat, P.; Raveendran, S.; Singh, S.; Pillai, S. Environmental impacts of microplastics and nanoplastics: A current overview. Frontiers in Microbiology 2021, 12, 768297. [Google Scholar] [CrossRef]
- Sykes, E.A.; Dai, Q.; Tsoi, K.M.; Hwang, D.M.; Chan, W.C. Nanoparticle exposure in animals can be visualized in the skin and analysed via skin biopsy. Nature communications 2014, 5, 3796. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.L.; Kelly, F.J. Plastic and human health: a micro issue? Environmental science & technology 2017, 51, 6634–6647. [Google Scholar]
- Zhao, B.; Rehati, P.; Yang, Z.; Cai, Z.; Guo, C.; Li, Y. The potential toxicity of microplastics on human health. Science of The Total Environment 2024, 912, 168946. [Google Scholar] [CrossRef]
- Zhang, M.; Gao, S.; Yang, D.; Fang, Y.; Lin, X.; Jin, X.; Liu, Y.; Liu, X.; Su, K.; Shi, K. Influencing factors and strategies of enhancing nanoparticles into tumors in vivo. Acta Pharmaceutica Sinica B 2021, 11, 2265–2285. [Google Scholar] [CrossRef]
- Forte, M.; Iachetta, G.; Tussellino, M.; Carotenuto, R.; Prisco, M.; De Falco, M.; Laforgia, V.; Valiante, S. Polystyrene nanoparticles internalization in human gastric adenocarcinoma cells. Toxicology in Vitro 2016, 31, 126–136. [Google Scholar] [CrossRef]
- Xu, M.; Halimu, G.; Zhang, Q.; Song, Y.; Fu, X.; Li, Y.; Li, Y.; Zhang, H. Internalization and toxicity: A preliminary study of effects of nanoplastic particles on human lung epithelial cell. Science of the Total Environment 2019, 694, 133794. [Google Scholar] [CrossRef]
- Mowat, A.M. Anatomical basis of tolerance and immunity to intestinal antigens. Nature Reviews Immunology 2003, 3, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Shen, R.; Yang, K.; Cheng, X.; Guo, C.; Xing, X.; Sun, H.; Liu, D.; Liu, X.; Wang, D. Accumulation of polystyrene microplastics induces liver fibrosis by activating cGAS/STING pathway. Environmental Pollution 2022, 300, 118986. [Google Scholar] [PubMed]
- McKechnie, J.L.; Blish, C.A. The innate immune system: fighting on the front lines or fanning the flames of COVID-19? Cell host & microbe 2020, 27, 863–869. [Google Scholar]
- Greven, A.C.; Merk, T.; Karagöz, F.; Mohr, K.; Klapper, M.; Jovanović, B.; Palić, D. Polycarbonate and polystyrene nanoplastic particles act as stressors to the innate immune system of fathead minnow (Pimephales promelas). Environmental toxicology and chemistry 2016, 35, 3093–3100. [Google Scholar]
- Jin, Y.; Xia, J.; Pan, Z.; Yang, J.; Wang, W.; Fu, Z. Polystyrene microplastics induce microbiota dysbiosis and inflammation in the gut of adult zebrafish. Environmental Pollution 2018, 235, 322–329. [Google Scholar]
- Li, B.; Ding, Y.; Cheng, X.; Sheng, D.; Xu, Z.; Rong, Q.; Wu, Y.; Zhao, H.; Ji, X.; Zhang, Y. Polyethylene microplastics affect the distribution of gut microbiota and inflammation development in mice. Chemosphere 2020, 244, 125492. [Google Scholar]
- Schwabl, P.; Köppel, S.; Königshofer, P.; Bucsics, T.; Trauner, M.; Reiberger, T.; Liebmann, B. Detection of various microplastics in human stool: a prospective case series. Annals of internal medicine 2019, 171, 453–457. [Google Scholar]
- Mohana, A.A.; Islam, M.M.; Rahman, M.; Pramanik, S.K.; Haque, N.; Gao, L.; Pramanik, B.K. Generation and consequence of nano/microplastics from medical waste and household plastic during the COVID-19 pandemic. Chemosphere 2023, 311, 137014. [Google Scholar]
- Djouina, M.; Vignal, C.; Dehaut, A.; Caboche, S.; Hirt, N.; Waxin, C.; Himber, C.; Beury, D.; Hot, D.; Dubuquoy, L. Oral exposure to polyethylene microplastics alters gut morphology, immune response, and microbiota composition in mice. Environmental Research 2022, 212, 113230. [Google Scholar]
- Chartres, N.; Cooper, C.B.; Bland, G.; Pelch, K.E.; Gandhi, S.A.; BakenRa, A.; Woodruff, T.J. Effects of Microplastic Exposure on Human Digestive, Reproductive, and Respiratory Health: A Rapid Systematic Review. Environmental Science & Technology 2024, 58, 22843–22864. [Google Scholar]
- Auguste, M.; Balbi, T.; Ciacci, C.; Canonico, B.; Papa, S.; Borello, A.; Vezzulli, L.; Canesi, L. Shift in immune parameters after repeated exposure to nanoplastics in the marine bivalve Mytilus. Frontiers in immunology 2020, 11, 426. [Google Scholar] [PubMed]
- Espinosa, C.; Beltrán, J.M.G.; Esteban, M.A.; Cuesta, A. In vitro effects of virgin microplastics on fish head-kidney leucocyte activities. Environmental Pollution 2018, 235, 30–38. [Google Scholar]
- Park, E.-J.; Han, J.-S.; Park, E.-J.; Seong, E.; Lee, G.-H.; Kim, D.-W.; Son, H.-Y.; Han, H.-Y.; Lee, B.-S. Repeated-oral dose toxicity of polyethylene microplastics and the possible implications on reproduction and development of the next generation. Toxicology letters 2020, 324, 75–85. [Google Scholar]
- Han, S.; Bang, J.; Choi, D.; Hwang, J.; Kim, T.; Oh, Y.; Hwang, Y.; Choi, J.; Hong, J. Surface pattern analysis of microplastics and their impact on human-derived cells. ACS Applied Polymer Materials 2020, 2, 4541–4550. [Google Scholar]
- AshaRani, P.; Low Kah Mun, G.; Hande, M.P.; Valiyaveettil, S. Cytotoxicity and genotoxicity of silver nanoparticles in human cells. ACS nano 2009, 3, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Bedard, K.; Krause, K.-H. The NOX family of ROS-generating NADPH oxidases: physiology and pathophysiology. Physiological reviews 2007, 87, 245–313. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.-J.; Li, J.-W.; Xu, E.G.; Sun, X.-D.; Zhu, F.-P.; Ding, Z.; Tian, H.; Dong, S.-S.; Xia, P.-F.; Yuan, X.-Z. Short-term exposure to positively charged polystyrene nanoparticles causes oxidative stress and membrane destruction in cyanobacteria. Environmental Science: Nano 2019, 6, 3072–3079. [Google Scholar]
- Pathak, D. Enemies of the hormones: microplastics and endocrine disruptors impacting public health. In Health and Climate Change, Elsevier: 2025; pp. 119-150.
- Puri, M.; Gandhi, K.; Suresh Kumar, M. A global overview of endocrine disrupting chemicals in the environment: Occurrence, effects, and treatment methods. International Journal of Environmental Science and Technology 2023, 20, 12875–12902. [Google Scholar] [CrossRef]
- Cortés-Arriagada, D.; Ortega, D.E.; Miranda-Rojas, S. Mechanistic insights into the adsorption of endocrine disruptors onto polystyrene microplastics in water. Environmental Pollution 2023, 319, 121017. [Google Scholar]
- Solleiro-Villavicencio, H.; Gomez-De León, C.T.; Del Río-Araiza, V.H.; Morales-Montor, J. The detrimental effect of microplastics on critical periods of development in the neuroendocrine system. Birth Defects Research 2020, 112, 1326–1340. [Google Scholar]
- Vezzulli, L.; Grande, C.; Reid, P.C.; Hélaouët, P.; Edwards, M.; Höfle, M.G.; Brettar, I.; Colwell, R.R.; Pruzzo, C. Climate influence on Vibrio and associated human diseases during the past half-century in the coastal North Atlantic. Proceedings of the National Academy of Sciences 2016, 113, E5062–E5071. [Google Scholar]
- Espinosa, C.; Cuesta, A.; Esteban, M.Á. Effects of dietary polyvinylchloride microparticles on general health, immune status and expression of several genes related to stress in gilthead seabream (Sparus aurata L.). Fish & shellfish immunology 2017, 68, 251–259. [Google Scholar]
- Cox, K.D.; Covernton, G.A.; Davies, H.L.; Dower, J.F.; Juanes, F.; Dudas, S.E. Human consumption of microplastics. Environmental science & technology 2019, 53, 7068–7074. [Google Scholar]
- Cordier, M.; Uehara, T. Will innovation solve the global plastic contamination: how much innovation is needed for that? 2024.
- Huang, W.; Wang, X.; Chen, D.; Xu, E.G.; Luo, X.; Zeng, J.; Huan, T.; Li, L.; Wang, Y. Toxicity mechanisms of polystyrene microplastics in marine mussels revealed by high-coverage quantitative metabolomics using chemical isotope labeling liquid chromatography mass spectrometry. Journal of hazardous materials 2021, 417, 126003. [Google Scholar] [PubMed]
- Rochman, C.; Tahir, A.; Williams, S.; Baxa, D.; Lam, R.; Miller, J. SJ 2015. Anthropogenic debris in seafood: Plastik debris and fibers from textiles in 59fish and bivalves sold for human consumption. Scientific reports 5.
- Ambrosini, R.; Azzoni, R.S.; Pittino, F.; Diolaiuti, G.; Franzetti, A.; Parolini, M. First evidence of microplastic contamination in the supraglacial debris of an alpine glacier. Environmental pollution 2019, 253, 297–301. [Google Scholar]
- Assas, M.; Qiu, X.; Chen, K.; Ogawa, H.; Xu, H.; Shimasaki, Y.; Oshima, Y. Bioaccumulation and reproductive effects of fluorescent microplastics in medaka fish. Marine Pollution Bulletin 2020, 158, 111446. [Google Scholar]
- Eriksen, M.; Lebreton, L.C.; Carson, H.S.; Thiel, M.; Moore, C.J.; Borerro, J.C.; Galgani, F.; Ryan, P.G.; Reisser, J. Plastic pollution in the world's oceans: more than 5 trillion plastic pieces weighing over 250,000 tons afloat at sea. PloS one 2014, 9, e111913. [Google Scholar]
- Abihssira-García, I.S.; Park, Y.; Kiron, V.; Olsvik, P.A. Fluorescent microplastic uptake by immune cells of atlantic salmon (Salmo salar L.). Frontiers in Environmental Science 2020, 8, 560206. [Google Scholar]
- Watson-Wright, W.M.; Wells, P.G.; Duce, R.A.; Gilardi, K.V.; Girvan, A.S.; Huber, M.E.; Kershaw, P.J.; Linders, J.B.; Luit, R.J.; Vivian, C.M. The UN Joint Group of Experts on the Scientific Aspects of Marine Environmental Protection (GESAMP)—An ocean science-policy interface standing the test of time. Marine Pollution Bulletin 2024, 199, 115917. [Google Scholar]
- Zhang, Y.; Kang, S.; Allen, S.; Allen, D.; Gao, T.; Sillanpää, M. Atmospheric microplastics: A review on current status and perspectives. Earth-Science Reviews 2020, 203, 103118. [Google Scholar]
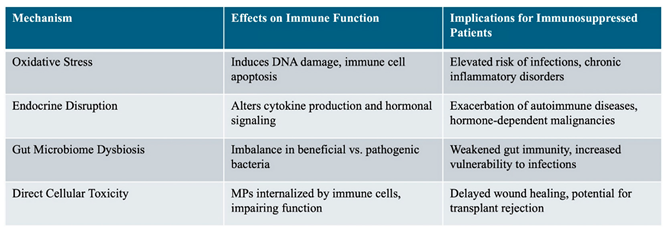
Table 2.
Mechanisms of Microplastic-Induced Immunosuppression.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



