
Submitted:
14 March 2025
Posted:
18 March 2025
You are already at the latest version
Abstract
Introduction: Lipomas are among the most encountered neoplasms in clinical practice, occurring mainly in adults between the fourth and sixth decades of life. Deep-seated lipomas in children are found in the thorax, chest wall, mediastinum, pleura, pelvis, retroperitoneum, and paratesticular area. Herein, we present a case of a three-year-old child with a giant mesenteric lipoma, along with a review of the literature on mesenteric lipomas in childhood. Case presentation: A three-year-old male toddler was referred to our hospital for severe, intermittent abdominal pain. Imaging studies at admission revealed a fat lesion occupying most of the peritoneal cavity and dislocating adjacent structures. An urgent laparotomy was performed. A giant lipoma arising from the mesentery and leading to the torsion of the mesenteric radix was confirmed and completely excised alongside an adherent small tract of jejunum. The child recovered uneventfully and is still being followed-up with no signs of recurrence. Discussion: Lipomas of the mesentery in children are very rare, and they are reported to be more common among children younger than three years of age. Mesenteric lipomas appeared to be more frequent in males than females. Even though they might be asymptomatic, voluminous lipomas can also create a lead point for intermittent torsion of the mass causing ischemia and infarction. Abdominal pain was the most frequent symptom, and the ileum was the tract of bowel more frequently involved by the tumor. Laparotomy was reported to be the preferable approach to safely remove this abdominal mass, especially in case of huge dimensions.
Keywords:
Mesentery
; lipoma
; Children
; Mesenteric torsion
; Management
1. Introduction
Lipomas are benign tumors of mature fat cells and are typically well-defined, enclosed in a fibrous capsule, and noninvasive. Lipomas are among the most encountered neoplasms in clinical practice. The prevalence is estimated to be around 1% of the entire population, with an incidence rate of around 2.1 per 1000 annually, occurring mainly in adults aged 40 to 60. They can arise anywhere in the body where fat cells are present and may cause variable and nonspecific symptoms, depending on size and location [1,2,3,4].
Lipomas are rare in the first 2 decades of life, may occur as single or multiple tumors, and can be located superficially or deeply in the body. Deep-seated lipomas in children are found in the thorax, chest wall, mediastinum, pleura, pelvis, retroperitoneum, and paratesticular area [5,6]. Particularly, lipomas of the mesentery involving the small bowel are very rare in children [1,6,7,8,9,10,11].
Mesenteric lipomas are slow-growing, soft, mobile masses that do not infiltrate the surrounding tissue; provided they allow bowel passage, they do not cause gastrointestinal symptoms [1,11]. Although mainly asymptomatic, nonspecific symptoms may occur, such as abdominal pain, vomiting, constipation, abdominal distension, and even partial or complete abdominal obstruction or volvulus [1,6,11,12,13].
Herein, we present a case of a 3-year-old male child with a giant mesenteric lipoma. A review of the literature regarding mesenteric lipomas in childhood was also performed.
2. Case Presentation
A 3-year-old male was referred to our hospital with severe, intermittent abdominal pain that started the night before, which raised suspicion of intestinal intussusception. During each painful episode, the child cried inconsolably and then became drowsy or fell asleep. No significant past medical or surgical history was reported, and the family history was unremarkable. The child presented a single episode of vomiting on the day of admission, with no other abdominal symptoms reported in the preceding days. On examination, the child was afebrile with stable vital signs. Abdominal palpation revealed diffuse fullness in the mid-abdomen without well-defined borders. Mild tenderness was noted, but no rebound tenderness or guarding occurred. Routine laboratory tests, including a complete blood count and basic metabolic panel, were within normal limits. Abdominal ultrasound demonstrated a hyperechoic intra-abdominal mass. A subsequent computed tomography (CT) scan confirmed a large, low-fat-density lesion measuring 13.2 × 4.5 × 12 cm, occupying most of the peritoneal cavity and dislocating adjacent structures (Figure 1). Although initial concerns included possible bowel obstruction or intussusception, no conclusive evidence of mechanical obstruction was found. Nonetheless, due to the acute presentation and escalating discomfort, an urgent laparotomy was performed for diagnostic and therapeutic purposes through a median incision under general anesthesia. Intraoperatively, a large, lobulated, yellow, soft mass arising from the mesentery was identified. Notably, a small jejunum tract was tightly adhered to the mass (Figure 2). The tumor was completely excised alongside the adherent small bowel, and an end-to-end anastomosis was created using interrupted absorbable stitches. Further investigation of the abdomen revealed a torsion of the mesentery radix that was recognized as the cause of a slightly bluish coloration of the small bowel loops. Once derotated, the whole small bowel recovered its normal coloration in a few seconds. Preoperative values of tumor markers were within normal ranges, and the pathohistological examination confirmed a giant lipoma 18.5 × 11.4 × 4.2 cm in size, weighing 548 grams, not infiltrating the adherent portion of the jejunum (14 cm in length), and with no evidence of malignancy (Figure 3). The child recovered uneventfully and was discharged home on the 8th postoperative day. At a 7-day follow-up, the patient was in good health with a satisfactory aesthetic result. The baby is still being followed up with no signs of recurrence.
3. Discussion
Lipomas of the mesentery in children are very rare, although they are among the most common neoplasms of mesenchymal origin. Interestingly, they are reported to be more common among children younger than 3 years [1,2,11,14]. Although they might be asymptomatic, frequent symptoms include progressive abdominal distension, abdominal pain, vomiting, constipation, feeling full after meals, and anorexia. Particularly, lesions exceeding 2 cm can cause abdominal pain, GI bleeding, intussusception, and bowel obstruction [1,11,14]. In 2003, Wolko and colleagues stated that it has not been fully explained how mesenteric lipomas can cause bowel obstruction. Additionally, they suggested that an obstruction may be caused by undue stress on the mesentery from the weight of the mass, which weakens and elongates the mesentery. This can also create a lead point for intermittent torsion of the mass. Furthermore, the twisting may cause tugging of the adjacent bowel, leading to obstruction [15]. However, Rwomurushaka et al. reported a partial intestinal obstruction resulting from extramural compression or a complete intestinal obstruction secondary to small bowel volvulus [2]. Notably, larger lipomas may twist around their vascular pedicle, causing ischemia and infarction [14].
Roentgenography may show a well-demarcated globular radiolucent mass clearly outlined by the greater density of the surrounding tissue [5,12]. However, the sonographic appearance of a mesenteric lipoma is that of a well-encapsulated echogenic mass with good through-transmission. Intraperitoneal lipomas can be confidently diagnosed when a homogeneous, highly echogenic encapsulated intra-abdominal mass is detected in children, especially if the mass is radiolucent on conventional radiographs [16]. On CT, the lipoma has typical fat tissue attenuation values from -80 to -120 HU. CT can also determine the omental or mesenteric origin of the lipoma and the precise anatomic features of the tumor. When performed, magnetic resonance imaging usually shows a homogenous signal intensity for the lipoma, identical to fat in all pulse sequences. This can help differentiate the lesion from adjacent structures and depict precise anatomic demarcations [17].
To obtain a comprehensive review of the literature, we searched the PubMed and Google Scholar databases using the following Medical Subject Heading terms: “lipoma,” “mesentery,” “child,” and “pediatric.” In summary, according to our review of the literature, mesenteric lipomas appeared slightly more frequent in males than females (13 males, 12 females, 1 not reported). The median age at presentation was 48 months (ranging from 9 months to 14 years), as in our case. Abdominal pain was the most frequent symptom, followed by abdominal distension and vomiting. The ileum was the intestinal tract more frequently involved by the tumor. Laparotomy was reported to be the preferable approach to safely remove the abdominal mass [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26] (Table 1). Notably, Stransky et al. and Ogilvy et al. published articles about mesenteric lipomas in children. However, since these articles could not be opened in any databases, we excluded them from our review [27,28]. A few more cases mentioned by Tayeh and colleagues and Turk and colleagues were published in languages other than English; thus, we did not add them to our table [6,11]. Moreover, in their review, Tayeh C et al. mentioned additional papers published in 2012 and 2014, but neither article could be found in any databases; therefore, we did not include them. Additionally, in 2016, Yang et al. published a paper on abdominal masses causing volvulus in children during a 20-year period in their hospital, where they noted five patients who had mesenteric lipomas. Since those cases were not described individually but as a group, we did not include them in this paper [29].
4. Conclusions
Mesenteric lipomas are rare in the pediatric population. They are usually asymptomatic but can cause unspecific symptoms such as abdominal pain, abdominal distension, vomiting, and constipation. Depending on their size and location, they can even lead to intestinal volvulus or obstruction. Although X-rays or ultrasound can provide helpful information, CT usually enables a more accurate description of the mass. Laparotomy with total removal of the lipoma, with or without bowel resection and an end-to-end anastomosis, is the treatment of choice in almost all cases. Particularly, we would warn pediatric surgeons not to underestimate a patient presenting with abdominal pain who alternates moments of agitation with moments of sudden falling asleep to avoid delaying a surgical exploration, with potentially devastating consequences.
Author Contributions
Conceptualization: A.B., D.C., and J.S.; methodology: Z.Z. and A.B.; investigation: Z.Z., R.B., and F.N.; data curation: Z.Z., A.B., D.C., and J.S.; formal analysis: R.B. and F.N.; validation: A.B., D.C., and J.S.; writing—original draft preparation: Z.Z., R.B., and F.N.; writing—review and editing: A.B., D.C., and J.S.; supervision: J.S.; this work has not been published previously and is not under consideration for publication elsewhere. All the authors approved the final version of the manuscript and attest that they meet the ICMJE criteria for authorship.
Funding
This work was supported by the Ministry of Health, Rome—Italy, in collaboration with the Institute for Maternal and Child Health IRCCS Burlo Garofolo, Trieste—Italy.
Institutional Review Board Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Conflict of Interests
None declared.
References
- Öztaş, T.; Asena, M. Mesenteric lipoma in a child: A case report. Pediatr. Acad. Case Rep. 2023, 2, 53–55. [CrossRef]
- Rwomurushaka, E.S.; Amsi, P.; Lodhia, J. Giant mesenteric lipoma in a pre-school child: a case report. J. Surg. Case Rep. 2024, 2024, rjae698. [CrossRef]
- Hashizume, N.; Aiko, T.; Fukahori, S.; Ishii, S.; Saikusa, N.; Koga, Y.; Higashidate, N.; Sakamoto, S.; Tsuruhisa, S.; Nakahara, H.; et al. Benign mesenteric lipomatous tumor in a child: a case report and literature review. Surg. Case Rep. 2020, 6, 1–6. [CrossRef]
- Azhar, M.; Zamir, N.; Jabbar, A. Giant Mesenteric Lipoma- A Rare Tumour Of Paediatric Age. J Ayub Med Coll Abbottabad. 2021, 33, 339-340.
- Ilhan, H.; Tokar, B.; Is̆iksoy, S.; Koku, N.; Pasaoglu, Ö. Giant mesenteric lipoma. J. Pediatr. Surg. 1999, 34, 639–640. [CrossRef]
- Tayeh, C.; Mneimneh, S.; El-Masri, R.; Daoud, N.; Rajab, M. Giant mesenteric lipoma: A case report and a review of the literature. J. Pediatr. Surg. Case Rep. 2015, 3, 166–170. [CrossRef]
- Malik, H.; Mirza, B.; Talat, N.; Zia, W.; Manzoor, A. Mesenteric Lipoma with Volvulus: A Rare Cause of Acute Abdomen in a Child. J. Coll. Physicians Surg. Pak. 2020, 30, 650–651. [CrossRef]
- Prince, T.C.; Shaffner, L.D. Mesenteric Lipoma in Children. Ann. Surg. 1956, 144, 913–914. [CrossRef]
- Kaniklides, C.; Frykberg, T.; Lundkvist, K. Paediatric Mesenteric Lipoma, An Unusual Cause of Repeated Abdominal Pain. Acta Radiol. 1998, 39, 695–697. [CrossRef]
- D, H.; B, R.; A, E.B.; Z, A.; M, K. The Mesenteric Lipoma in Children. Res. Pediatr. Neonatol. 2021, 5, 444–446. [CrossRef]
- Turk, E.; Edirne, Y.; Karaca, F.; Memetoglu, M.E.; Unal, E.; Ermumcu, O. A Rare Cause of Childhood Ileus: Giant Mesenteric Lipoma and a Review of the Literature. Eurasian J. Med. 2013, 45, 222–225. [CrossRef]
- Ozel, S.K.; Apak, S.; Ozercan, I.H.; Kazez, A. Giant Mesenteric Lipoma as a Rare Cause of Ileus in a Child: Report of a Case. Surg. Today 2004, 34, 470–472. [CrossRef]
- Maree, G.; Gawrieh, B.; Omran, A.; Ali, W. A rare lipoma site in a 1-year-old boy. J. Surg. Case Rep. 2021, 2021, rjab447. [CrossRef]
- Laguna, B.A.; Iyer, R.S.; Rudzinski, E.R.; Roybal, J.L.; Stanescu, A.L. Torsion of a giant mesocolic lipoma in a child with Bannayan-Riley-Ruvalcaba syndrome. Pediatr. Radiol. 2014, 45, 449–452. [CrossRef]
- Wolko, J.D.; Rosenfeld, D.L.; Lazar, M.J.; Underberg-Davis, S.J. Torsion of a giant mesenteric lipoma. Pediatr. Radiol. 2003, 33, 34–36. [CrossRef]
- Prando, A.; Wallace, S.; Marins, J.L.C.; Pereira, R.M.; de Oliveira, E.R.; Alvarenga, M. Sonographic features of benign intraperitoneal lipomatous tumors in children-report of 4 cases. Pediatr. Radiol. 1990, 20, 571–574. [CrossRef]
- Hamidi, H.; Rasouly, N.; Khpalwak, H.; Malikzai, M.O.; Faizi, A.R.; Hoshang, M.M.S.; Maroof, S.; Nasery, M.N.; Farzam, F.; Salehzai, M.; et al. Childhood giant omental and mesenteric lipoma. Radiol. Case Rep. 2016, 11, 41–44. [CrossRef]
- Selman, J.; Bender, J.R. Mesenteric Lipoma in a Child. Radiology 1948, 51, 66–70. [CrossRef]
- Gupta DK, Rohatgi M, Rao PS. Mesenteric lipoma. Indian Pediatr. 1988;25(10):1007-1009.
- Cherian, A.; Singh, S.J.; Broderick, N.; Zaitoun, A.M.; Kapila, L. Small bowel volvulus due to giant mesenteric lipoma. Pediatr. Surg. Int. 2004, 20, 869–871. [CrossRef]
- Kisra, M.; Ettayebi, F.; El Azzouzi, D.; Benhammou, M. Image of the Month—Answer. Arch. Surg. 2006, 141, 1046. [CrossRef]
- Srinivasan, K.; Gaikwad, A.; Ritesh, K.; Ushanandini, K. Giant omental and mesenteric lipoma in an infant. Afr. J. Paediatr. Surg. 2009, 6, 68–9. [CrossRef]
- Ahmed, I.; Singh, S.; Rawat, J.D. Chronic abdominal pain in a child. Saudi J. Gastroenterol. 2011, 17, 295–6. [CrossRef]
- Alireza R, Mohammad SS, Mehrzad M, Houman A. Midgut volvulus caused by mesenteric lipoma. Iran J Pediatr. 2013;23(1):121-123.
- Mozumder, M.R.; Afrin, R.; Biswas, T.; Haque, J.A.; Hoque, T.; Anjum, M.; Tofa, T.T. Mesenteric Lipoma in a Child- A Case Report. J. Dhaka Med Coll. 2024, 31, 258–263. [CrossRef]
- Garge, S.; Sharma, A.; Kelkar, H.; Jajodia, J. A Case of a Giant Mesentric Lipoma in a Two-year-old Child Presenting as Koch’s Abdomen. Apollo Med. 2024, 21, S11–S13. [CrossRef]
- Ogilvy, W.L.; Owen, H.F. Mesenteric lipoma in children. Can J Surg. 1960, 3, 344–6.
- Stransky E, Sevilla-Cabrera R. On a huge intraabdominal mesocolic lipoma in infancy. Ann Paediatr. 1962, 198, 24-34.
- Yang, C.; Wang, S.; Zhang, J.; Kong, X.R.; Zhao, Z.; Li, C.C. An unusual cause of paediatric abdominal pain: Mesenteric masses accompanied with volvulus. Turk. J. Gastroenterol. 2016, 27, 325–329. [CrossRef]
Figure 1.
Pre-operative Computed Tomography (TC). Axial (left), coronal (middle), and sagittal (right) scans showing a huge, low-fat-density neoformation and a sign consistent with mesenteric torsion (white arrow).
Figure 1.
Pre-operative Computed Tomography (TC). Axial (left), coronal (middle), and sagittal (right) scans showing a huge, low-fat-density neoformation and a sign consistent with mesenteric torsion (white arrow).
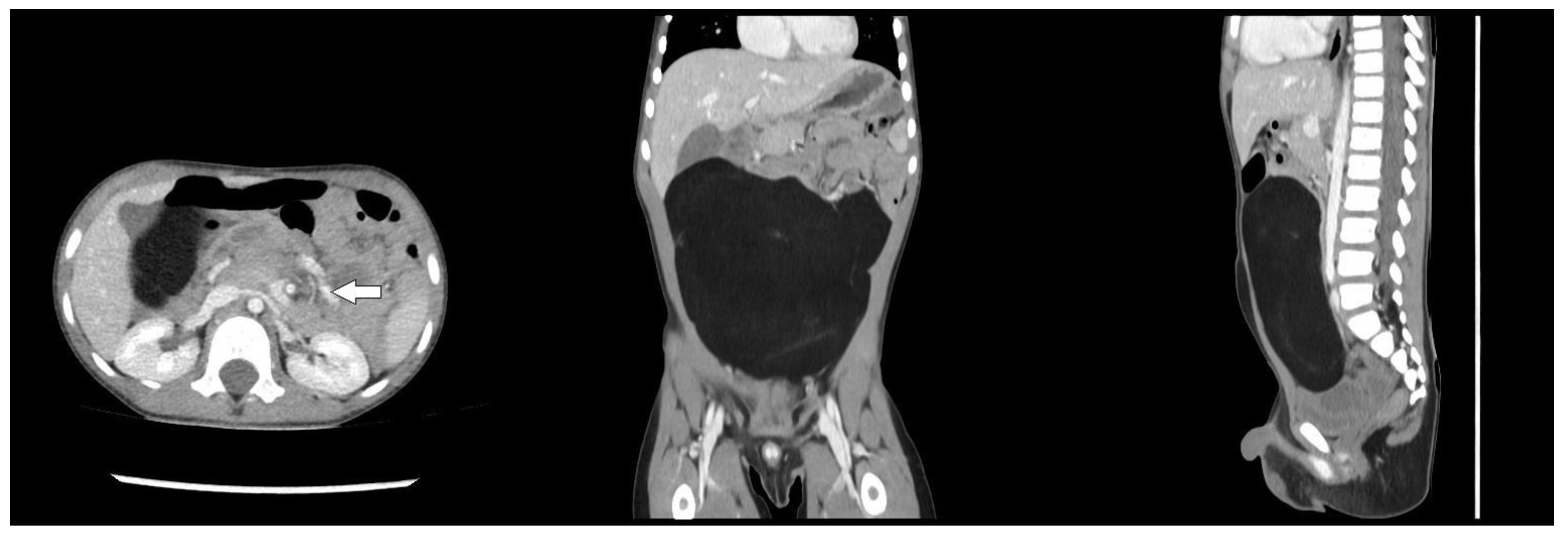
Figure 2.
Intraoperative close-up view (left) and macroscopic appearance (right) of a giant mesenteric lipoma involving a small tract of jejunum.
Figure 2.
Intraoperative close-up view (left) and macroscopic appearance (right) of a giant mesenteric lipoma involving a small tract of jejunum.
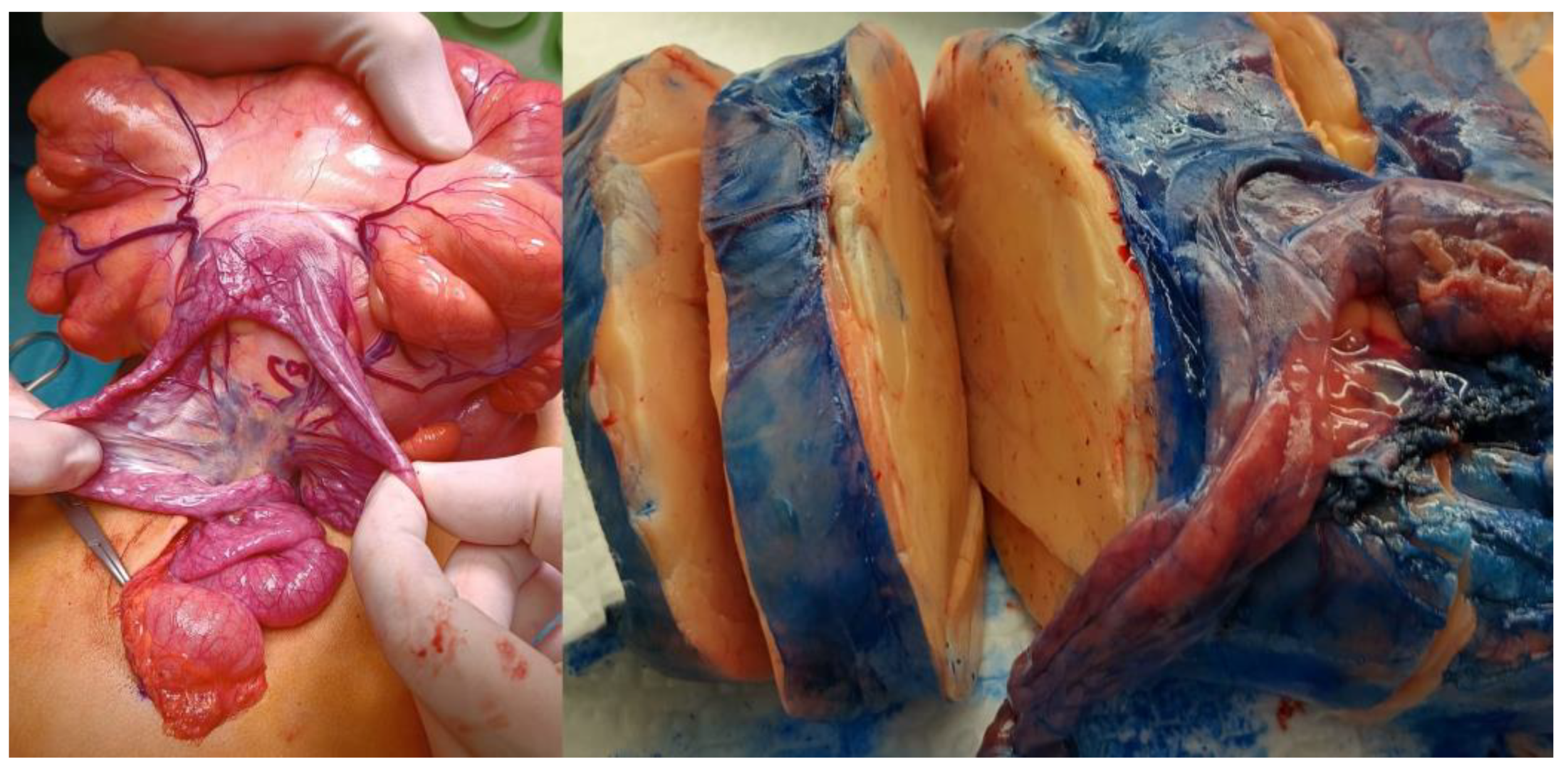
Figure 3.
Microscopic images of the mesenteric lipoma taken through a 10X. (left) and 20X (right) objectives on hematoxylin and eosin-stained histological sections.
Figure 3.
Microscopic images of the mesenteric lipoma taken through a 10X. (left) and 20X (right) objectives on hematoxylin and eosin-stained histological sections.
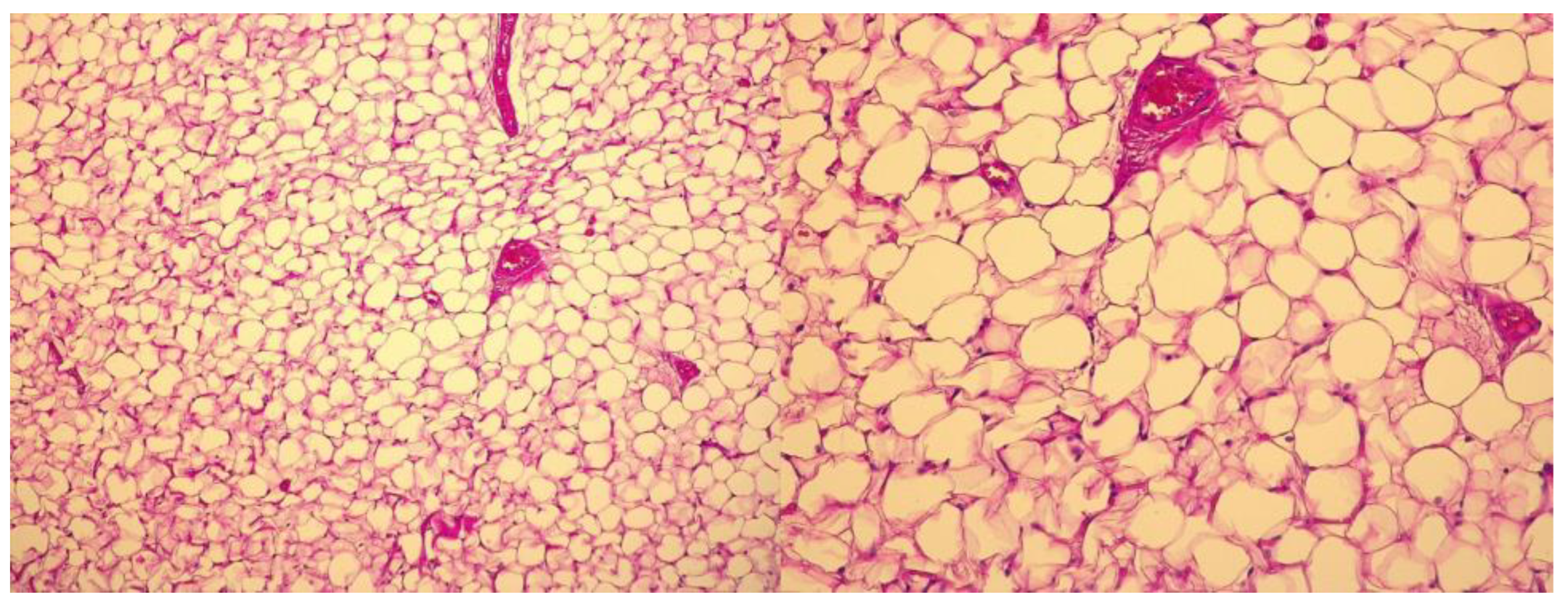

Table 1.
Previous cases of Pediatric Mesenteric Lipoma reported in the literature.
| Authors | Year | Age (months) | Sex | Comorbidities | Symptoms | Symptoms duration | Imaging | Tumor size (mm) | Tumor weight (gr) | Localization | Type of surgery | Intraoperative findings | Complications | LoS (days) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Selman J et al. (18) | 1947 | 48 | F | none | abdominal mass; nausea; vomiting | 4y | X-ray | NR | NR | ileum | laparotomy | NR | none | NR |
| Prince T C et al. (8) | 1956 | 10 | F | NR | abdominal mass | 3 m | X-ray | 200 | NR | ileum | laparotomy | NR | none | 7 |
| Gupta D K et al. (19) | 1988 | 14 | F | NR | NR | NR | NR | 150 | NR | ileum | NR | NR | NR | NR |
| Prando A et al. (16) | 1990 | 30 | M | NR | abdominal mass | NR | X-ray; US | 110x90x50 | NR | jejunum | NR | adherent to the wall of small bowel | NR | NR |
| Kaniklides C et al. (9) | 1998 | 132 | M | NR | abdominal pain; constipation | 8 y | X-ray; US; CT | 220x290x50 | 700 | mesentery | laparotomy | NR | NR | NR |
| Ilhan H et al. (5) | 1999 | 36 | M | none | abdominal distension | 6 m | US; CT | 310x230x120 | 2050 | mesentery | laparotomy | NR | none | 6 |
| Wolko J D et al. (15) | 2003 | 108 | M | Sorbital Intolerance | abdominal pain | 10 d | CT | 100x150 | NR | NR | NR | torsion of the lipoma; small bowel obstruction | none | NR |
| Ozel S K et al. (12) | 2004 | 84 | F | NR | abdominal pain; bilius vomiting | 4 d | X-ray; US; CT | 180x150x50 | NR | ileum | laparotomy | NR | NR | NR |
| Cherian A et al. (20) | 2004 | 168 | F | NR | abdominal pain; bilius vomiting | 8 h | X-ray | 160x150x75 | NR | ileum | laporoscopy; laparotomy | volvulus | none | 7 |
| Kisra M et al. (21) | 2006 | 168 | M | NR | NR | NR | NR | 124x68x110 | NR | ileum | NR | volvulus | NR | NR |
| Srinivasan K G et al. (22) | 2009 | 9 | NR | NR | abdominal distension; diarrhoea | 3 m | US; CT | NR | 1500 | omentum; mesentery; transverse colon | laparotomy | NR | NR | NR |
| Ahmed I et al. (23) | 2011 | 72 | M | none | abdominal pain; abdominal distension; constipation | 2 y | CT | NR | NR | ileum | laparotomy | NR | none | NR |
| Turk E et al. (11) | 2013 | 24 | F | none | abdominal pain, bilius vomiting | 24 h | X-ray; US | 160x150x80 | 770 | ileum | laparotomy | intestinal obstruction with necrosis | none | 5 |
| Alireza R et al. (24) | 2013 | 72 | F | NR | abdominal pain; nausea; vomiting | 2 d | X-ray; US; CT | 130x30x50 | NR | ileum | laparotomy | volvulus | none | NR |
| Tayeh C et al. (6) | 2015 | 24 | M | none | failure to thrive; abdominal distension | 1 y | X-ray; US | 220x190x90 | 1620 | ileum | laparotomy | NR | none | 6 |
| Laguna B A et al. (14) | 2015 | 72 | M | Bannayan-Riley-Ruvelbaca Syndrome | abdominal pain | 12 h | CT | 68x42x83 | NR | mesocolon | laparoscopy | torsion of the lipoma | NR | NR |
| Hamidi H et al. (17) | 2016 | 72 | F | NR | abdominal pain; abdominal distension | 4 y | US; CT | 280x240x100 | NR | NR | laparotomy | NR | none | NR |
| Hashizume N et al. (3) | 2020 | 36 | F | none | abdominal pain; abdominal distension | NR | US; CT; MRI | 80x60 | NR | ileum | laparotomy | NR | none | NR |
| Maree G et al. (13) | 2020 | 12 | M | NR | abdominal distension; diarrhoea | NR | US; CT | 90x110 | NR | jejunum | laparotomy | NR | none | 5 |
| Malik H et al. (7) | 2020 | 72 | F | NR | abdominal pain; vomiting; constipation | 24 h | X-ray | 100x80; 20x20 | NR | ileum | laparotomy | volvulus | none | NR |
| Azhar M et al. (4) | 2021 | 11 | M | none | abdominal distension; constipation; abdominal pain; vomiting | 4m | US; CT | 300x190x120 | NR | ileum | laparotomy | small bowel wrapped around tumor | none | 5 |
| Hanine D et al. (10) | 2021 | 60 | M | NR | abdominal pain | NR | X-ray; US; CT | NR | NR | ileum | laparotomy | NR | none | NR |
| Mozumder MR et al. (25) | 2022 | 96 | F | none | abdominal pain; vomiting | 1.5y | US; CT | 85x65x45 | 150 | ileum | laparotomy | NR | none | NR |
| Oztas T et al. (1) | 2023 | 48 | M | none | abdominal pain; vomiting | NR | X-ray; US; CT | 120x120x70 | NR | ileum | NR | volvulus | none | 6 |
| Rwomurushaka E S et al. (2) | 2024 | 36 | F | NR | abdominal distension; nausea | 1y | US; CT | 170x170x90 | NR | small bowel; mesentery | laparotomy | NR | none | 3 |
| Garge S et al. (26) | 2024 | 24 | M | NR | abdominal distension, abdominal pain, failure to thrive | 6 m | X-ray; US; CT | 150x60x100 | NR | ileum | laparotomy | NR | none | 5 |
Abbreviations: M=male; F=Female; NR=Not Reported; y=year(S); m=month(S); d=day(S); h=hour(S); US=Ultrasonography; CT= Computed Tomography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



