
Submitted:
13 March 2025
Posted:
14 March 2025
You are already at the latest version
Abstract
In dental clinics the risk of airborne infection is relevant. Microbiological air monitoring is a useful tool for evaluating the effectiveness of preventive measures and identifying at-risk situations. Active and passive sampling can be used to assess microbial air contamina-tion; however, optimal sampling methods and reference threshold values have not been established. Passive sampling has been standardized by the Index of Microbial Air con-tamination (IMA). This study aimed to review the use of the IMA standard for air quality assessment in dental clinics proposing IMA threshold values based on a meta-analysis. Scopus, PubMed, and Web of Science were analyzed for articles published until April 30, 2024, citing “Pasquarella C., et al., The index of microbial air contamination. J Hosp Infect 2000”. After applying the inclusion criteria, nine studies were considered. The mean IMA values before, during, and after dental procedures ranged from 2.4 to 38.3, 19 to 53.3, and 13 to 20, respectively. Seven studies were included in the meta-analysis, which had mean IMA values of 15.4, 33, and 16.7, respectively. Due to the ease of use, low cost, and com-parability of results, the IMA standard is recommended for the routine monitoring of mi-crobial air contamination.
Keywords:
air
; dental clinic
; IMA standard
; microbial contamination
; monitoring
; passive sampling
1. Introduction
Dental clinics are healthcare settings in which airborne infection risk is particularly relevant [1,2,3,4,5,6,7,8]. Patients and healthcare workers may be exposed to a wide variety of microorganisms that colonize or infect the oral cavity and respiratory tract or are carried in the water used during treatment [1,2,4,5,7,9,10,11,12,13]. Ablators, turbines, and air-water syringes may nebulize the saliva and microorganisms contained in the mouth of a patient, resulting in contamination of the surrounding air and surfaces [14,15,16,17,18]. In addition, water stagnation, biofilm production, and the inappropriate disinfection of dental unit water systems (DUWS) promote the proliferation of microorganisms, and contaminated water can be aerosolized and spread into the environment during dental procedures [10,19,20,21]. This suggests a potential risk of infection, particularly in patients who are immunocompromised; moreover, there may be an occupational risk because of the much greater exposure of healthcare workers [10,14,22,23,24]. The coronavirus disease 2019 pandemic has led to greater concern regarding the risk of the spread of airborne infections in dental clinics, and the recommendations for the prevention of airborne infections have been strengthened [4,5,25,26,27,28,29].
Minimizing microbial air contamination is essential for infection control [4,30], and microbial air monitoring is a useful tool for verifying the effectiveness of preventive measures and identifying at-risk situations, as an important component of risk management [26,31,32,33,34,35]. However, thus far, there has been no consensus regarding the optimal air sampling method and how to interpret the results to implement targeted preventive measures. Active and passive sampling approaches have been used [31,32,33,36]. Active sampling allows measurement of the concentration of culturable microorganisms in the air and is based on the use of devices that collect a known volume of air blown onto nutrient media; the results are expressed as colony forming units per cubic meter (cfu/m3) [31,32,33,37,38]. Several types of air samplers are available, with different engineering features and different biological and physical efficiencies, thus providing different results. The lack of standardization of the sampling parameters explains the variability of the results obtained using the same air sampler. Passive sampling measures the rate at which microorganisms settle on surfaces; it is based on sedimentation and relies on the use of settle plates exposed to air for a defined time; the results are expressed as cfu/plate/time. Passive sampling has been standardized by the Index of Microbial Air contamination (IMA) which corresponds to the number of cfu on a Petri dish with a diameter of 9 cm, containing nutrient agar, exposed to the air according to the 1/1/1 scheme (for 1 h, 1 m above the floor, and approximately 1 m from walls or major obstacles), and incubated at 36 ±1°C for 48 hours [39]. The IMA can also be expressed as cfu/m2or cfu/dm2.
Five classes of IMA have been defined in different environments at risk of infection, and the maximum acceptable values of IMA have been proposed for different risks of infection or contamination [39]. Infection control professionals should state the level of infection risk and adopt the corresponding maximum acceptable IMA value [39].
This study aimed to review the use of the IMA standard for air quality assessment in dental clinics and to propose threshold values based on a meta-analysis of the results obtained in the studies
2. Materials and Methods
Searches of Scopus, PubMed, and Web of Science were conducted for articles published until April 30, 2024, which citated the article “Pasquarella C., et al., The index of microbial air contamination. J Hosp Infect 2000;46,241-256”.
The inclusion criteria were: I) original studies, II) studies in English or Italian, III) studies performed in dental clinics, and IV) studies with the IMA standard, i.e., settle plates containing nutrient agar, placed in the dental unit, 1 m above the floor, within 1 m from the patient, and exposed for 1 h. Cited references in each study performed in dental clinics were also considered.
For each study, information on the country, type of study (single-center or multi-center), type of dental procedure, presence of a ventilation system, number of samples, sampling time, and IMA values were considered. Studies reporting the mean and standard deviation or median, minimum, and maximum IMA values were used for the meta-analysis.
The meta-analysis was conducted using R version 4.4.1 (R Development Core Team, 2024) [40] together with the R package “meta” (Guido Schwarzer, v. 7.0-0, 2024). In particular, the routine “metamean” was used to obtain an overall estimate from the studies. It calculates the common (not shown) and random effects meta-analyses of single untransformed means to determine the overall mean (MRAW); inverse variance weighting was used for pooling. The 95% confidence intervals (CIs) for individual studies were based on a standard normal distribution (default) or a t-distribution. Heterogeneity was evaluated using Cochrane Q statistics and the τ2, H2 and I2 indices indices. Statistical significance was set at p<0.05. A Forest plot was constructed for each analysis.
3. Results
A flow diagram of the review process is shown in Figure 1. The study by Pasquarella et al., “The index of microbial air contamination. J Hosp Infect 2000; 46:241-256” was cited in 240 articles from Scopus, 73 from PubMed, and 196 from Web of Science.
After screening the titles, 238 duplicates were identified and excluded. After the exclusion of non-original studies (e.g., reviews, book chapters, guidelines) (n=65), articles not in English or Italian (n=10), studies performed in non-healthcare settings (n=87), or in healthcare settings but not dental clinics (n=94), there were 15 studies performed in dental clinics [11,12,14,24,25,28,41,42,43,44,45,46,47,48,49,50]. Of these 15 studies, 10 were excluded for the following reasons: seven studies did not apply the IMA standard in all its parameters [12,24,25,28,41,42,50], one referred to an experimental simulation [45], one dealt only with fungal air contamination [49], and one focused on a specific microorganism, Staphylococcus arlettae [43]. Five studies met all the inclusion criteria [11,14,44,46,48]. A search of the cited references of the 15 studies performed in dental clinics identified four studies that also met the inclusion criteria [51,52,53,54]. Finally, nine studies were included in the review [11,14,44,46,48,51,52,53,54].
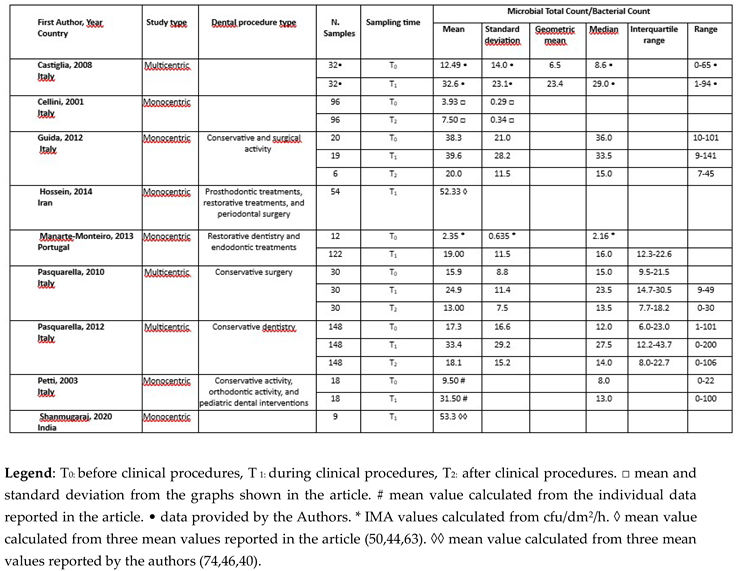
Table 1 shows the included studies listed in alphabetical order relative to the first author, reporting the year of publication, country, type of study (single-center or multi-center), type of dental procedure, number of samples, sampling time, and IMA values for bacteria or total viable count before (T0), during (T1), and after the procedure (T2).
The publication years ranged from 2001 to 2020. Seven studies were conducted in Europe, with six in Italy [11,14,46,51,52,54] and one in Portugal [44]. Two studies were conducted in Asia, with one in Iran [53] and one in India [48]. Most studies were single-center and three [11,14,46] were multi-center, including a maximum of 10 centers [11].
The number of air samples, collected in the dental units, within 1 m of the patient, ranged from 12 [44] to 148 [11] before the procedure (T0), from nine [48] to 148 [11] during the procedure (T1), and from six [52] to 148 [11] after the procedure (T2).
The types of dental procedures used are listed in Table 1. Conservative dentistry is the most frequently performed procedure.
Three studies [11,46,52] assessed microbial contamination under three sampling conditions: T0, T1, and T2; three [14,44,54] at T0 and T1; one at T0 and T2 [51]; and two only at T1 [48,53].
In seven studies [11,14,46,48,51,52,54] the total microbial count was determined, whereas in two studies [44,53] the bacterial count was determined. Table 1 shows the mean IMA values and, when available, the standard deviation, median, and range for each of the nine included studies. As in the study by Castiglia et al. (2008), which reported only the geometric mean, Table 1 shows the mean, standard deviation, median, and range values that were used in the meta-analysis and provided by the authors [14].
Figure 2 shows the mean IMA values obtained in different studies at T0, T1 and T2, in crescent order, referred to T1. The IMA values ranged from 2.35 [44] to 38.3 [52] at T0, from 19 [44] to 53.3 [48] at T1, and from 7.5 [51] to 20 [52] at T2.
The studies performed in Asia [48,53] reported the highest levels of microbial air contamination during procedures, with mean IMA values ranging from 40 to 74 in the study by Shanmugaraj and from 44 to 63 in the study by Hossein et al. (2014) [53].
Wide variability was observed in the increase in mean IMA values recorded before and during procedures, with differences ranging from 1.3 cfu (3.4%) [52] to 22 cfu (231.6%) [54], and the differences between values during procedures and after procedures ranged from 11.9 (91.5%) [46] to 19.6 (98%) [52].
Figure 3 shows the results of the meta-analysis, which included seven studies [11,14,44,46,48,52,54], of which there were six with data for T0 (before procedures), seven for T1 (during procedures), and three for T2 (after procedures).
The meta-analysis yielded an MRAW of 15.4 (95% CI: 6.3, 24.5) at T0, 33 (95% CI: 24.4, 41.6) at T1 and 16.7 (95% CI: 12.7, 20.8) at T2 (Figure 3). For the studies performed in Europe, the meta-analysis yielded an IMA value of 29, during procedures (Figure 4).
Only three studies [44,51,52] reported information on ventilation systems, without providing detail. Cellini et al. (2001) reported the presence of an air filtration system, Guida et al. (2012) reported the presence of an air conditioner, and Manarte-Monteiro et al. (2013) reported the presence of a regularly checked ventilation system [44,51,52].
4. Discussion
Dental clinics are environments at high risk of airborne infection for patients and healthcare workers. Many dental procedures produce aerosols (droplets, droplet nuclei, and splatters) that harbor various pathogenic microorganisms and may pose a risk for the spread of infections between patients and dentists [4,6,12,13,24]. The oral cavity of a patient is the main source of microorganisms; however, microorganisms can also be generated from dental unit waterlines, which can sometimes be highly contaminated [11,14]. Airborne microorganisms can settle on surfaces and be resuspended or transferred to patients through the hands of healthcare workers [55].
The presence of airborne microorganisms cannot be eliminated, but preventive interventions can be implemented to reduce the risk of disease transmission, and for this purpose several methods have been proposed [4,30]. However, it is important to verify the effectiveness of these interventions and identify at-risk situations. Microbiological air monitoring is a useful tool for achieving these aims [31,32,33]. To provide accurate and comparable results relevant to risk management, it is important to standardize the air sampling methods. To date, no generally accepted methods or threshold values are available for dental clinics. The passive air sampling method has been standardized with the IMA, defining the main parameters that can affect the results (exposure time, diameter of settle plates, and height of plate from the ground) [39], and it is the most commonly agreed measure [5].
This review aimed to assess, in the literature, the extent of use of the IMA standard [39] for air quality assessment in dental clinics, and to propose threshold values, based on the meta-analysis of results obtained in the studies.
In this review, only studies in which the IMA standard was fully applied, regarding, in particular, the size of the settle plate (9 cm diameter), exposure time (1 h), distance from the floor (1 m), and nutrient agar incubated at 37°C for 48 h. Plate count agar, tryptone soy agar, or blood agar plate were considered as nutrient agars with comparable results, if expressed as microbial total count and as bacterial count; in these incubation conditions, mainly bacteria grow, whereas other microorganisms, such as fungi, require selective media and appropriate incubation times and temperatures. Only the studies in which the IMA standard was measured within 1 m of the patients were considered, assuming this area to have the highest risk of infection.
Stringent inclusion criteria led to the exclusion of some studies in which the IMA standard was cited but not fully applied. For example, Zemouri et al. (2020) measured microbial load by exposing plates to the air for 30 min at a height of 80 cm from the floor; in the study by Decraene et al. (2008), settle plates were exposed at a distance of 244 cm from the chair of the dental unit; in the study by Suprono et al. (2022), settle plates were placed around the clinic area at varying distances and heights, without providing specific values [28,42,50].
The studies included in this review have provided a picture of microbial air contamination measured before, during, and after clinical procedures using a standardized passive sampling method.
As expected, an increase in microbial air contamination during dental procedures was observed, with variability in the IMA values. The percentage increase in the mean IMA values before and during procedures varied in different studies. The lowest change (3.39%) was observed in the study by Guida et al. (2012), in which a high level of microbial contamination was recorded before clinical procedures; the authors affirmed that this could be due to the status of the air conditioning systems, which were often turned off at the end of the daily procedures [52]. Despite all expectations, Kedjarune et al. (2000) reported higher microbial air contamination levels before clinical procedures than during clinical procedures, suggesting that this might indicate an overnight build-up of bacterial aerosols when ventilation systems were not operating [56]. Microbial air contamination during clinical procedures is mainly influenced by the presence of a ventilation system, the type of intervention, and the number of people present. Unfortunately, only a few studies have reported information on these variables; therefore, it was not possible to determine possible correlations. However, the lowest IMA values before and during procedures were reported by Manarte-Monteiro et al. (2012), in a study conducted in dental clinics supplied with a ventilation system that was regularly checked [44]. In the same study, IMA values were recorded during restorative dentistry and endodontic treatments; the latter provided a higher level of microbial air contamination than conservative treatments, and it was highlighted that the plate distance from the patient influenced the IMA values, with the highest contamination level at a distance of 0.5 m compared with a distance of 2 m. Hossein et al. (2014) also reported a higher bacterial load in periodontal procedures than in prosthodontic and restoration procedures [53].
Microbial air contamination decreased after procedures but there were only data from three studies. The mean IMA value was 16.7, which is similar to the IMA value obtained before clinical procedures (15.4).
The spread of airborne infections has long been one of the main concerns in the dental community because of the possible consequences for patients and healthcare workers. However, there are no recommended threshold values for microbial air contamination in dentistry. One of the aims of this study was to propose threshold values for microbial air contamination measured using the IMA standard. The IMA values before (15.4), during (33), and after (16.7) procedures, derived from the meta-analysis, can be used as threshold values in dental clinics. The most appropriate IMA value to be considered should be derived from the European studies (IMA, 29), excluding the study by Shanmugaray, with a mean IMA value of 53.3, which is significantly higher than the highest mean IMA value of 39.6 obtained in the European studies [48]. The IMA value of 29 is very close to the threshold value of 27.5, proposed by Pasquarella et al. (2012) based on the results from a multi-center Italian study, and slightly higher than an IMA of 25, cited by Kumbargere Nagraj et al. (2022) as a good performance indicator at a high-risk venue such as a dental clinic [5,11]. A limitation of the study was the small number of studies assessed; therefore, wider data collection is required to validate these proposed values, as current environmental conditions could be different from those in the years in which the studies included in this review were conducted. For example, the IMA of 25 initially proposed for operating rooms [39] is currently considered to be excessively high for modern operating rooms, where values less than 15 [47,57,58] can now be achieved.
In the studies by Petti et al. (2003) and Manarte-Monteiro et al. (2013) qualitative analyses were performed. In the study by Petti et al. (2003), staphylococci and streptococci were evaluated; Manarte-Monteiro et al. (2013) assessed the same organisms and micrococci in their study [44,54]. Streptococci indicate not only the presence of humans but may also be considered a good parameter to indicate the presence of aerosols originating from the oral cavity of patients, while staphylococci represent a less specific indicator, being present on the skin and mucosa and therefore more related to general human presence than to a dental procedure [54].
In five studies, active and passive sampling were used to evaluate microbial air contamination [11,14,46,52,54]. Petti et al. (2003) reported a significant correlation between active and passive sampling methods for high contamination levels, but no correlation for low contamination levels [54]. Pasquarella et al. (2012) reported a significant correlation between active and passive sampling, which was explored in depth in a subsequent study [59], showing different patterns of correlation, with the strongest correlation between cfu/m3 and IMA values when the highest microbial air contamination values were recorded [11]. Several factors can affect this relationship, such as particle size or ventilation parameters. For example, in an environment with a high concentration of microorganisms and high cfu/m3, there can be a low sedimentation rate because of the small size of the particle carrying the microorganisms. Considering the high fluctuation in microbial contamination in dental clinics owing to frequent aerosol production, the cumulative measurement of contamination provided by the use of settle plates exposed for 1 h was not correlated with the concentration measured using punctiform active sampling. A more probable correlation was found when the active sampling was performed at regular intervals during the 1 h exposure time of the settle plate [60], instead of performing punctiform active sampling measurement. Several studies have reported correlations between active and passive sampling [33,47,60,61,62,63,64,65,66]. However, it is questionable to assume that there is a predefined correspondence between active and passive sampling, as some authors have, expressing the results derived from the IMA standard in cfu/m3 by applying Omeliansky’s formula [67,68,69].
Active and passive sampling can be used for a general evaluation of microbial air quality, but they have specific aims, measuring different aspects of microbial air contamination. Active sampling measures the concentrations of microorganisms, and passive sampling measures the fall-out of biological particles, as a mirror of the airborne risk for critical surfaces. Passive sampling provides a measure of the contribution of airborne biocontamination to the biocontamination of surfaces, which is particularly relevant in dental clinics considering the important role of surfaces in the transmission of microorganisms. Some authors report that the use of settle plates is more appropriate than active sampling in dental clinics, as they provide a measure of contamination build-up during clinical procedures [12,42]. The use of settle plates, whose sampling efficiency is not influenced by engineering factors, standardized with the IMA, yields comparable results wherever and whenever they are obtained, providing the basis for the definition of threshold limits for effective risk prevention.
Some studies included in this review, in addition to evaluation of microbial air contamination using passive sampling with the IMA standard and active sampling, conducted microbial monitoring of surfaces, with nitrocellulose membranes or with RODAC plates, and microbial monitoring of DUWS [11,14,46,70]. This global approach provides a comprehensive evaluation of environmental quality in dental clinics.
5. Conclusions
This review provides an overview of the application of the IMA standard in dental clinics. As the IMA values are not dependent on engineering features and are derived from a standardized sampling method, it was possible to perform the meta-analysis to yield proposed reference threshold values. Expanding the data collection, to also include variables that affect microbial air contamination, could significantly contribute to the estimation of more appropriate threshold values In a context in which there are no generally accepted protocols for the evaluation of airborne microbial contamination, the IMA standard, which provides an estimation of the airborne risk of contamination for critical surfaces and cumulative measurements of microbial contamination, as well as low cost and ease of use, represents a valid tool to identify risks and to evaluate the effectiveness of prevention interventions; thus it can be proposed for routine microbial air monitoring.
Author Contributions
Conceptualization, C.P.; methodology, C.P., M.E.C., G.P., L.V. and R.A.; validation, C.P., I.V. and R.A.; investigation I.V., M.C.F. and C.P.; data curation, I.V. and G.P.; writing—original draft preparation, C.P. and I.V.; writing—review and editing, C.P., I.V., M.E.C., G.P., P.A., R.Z, M.C.F., L.V. and R.A.; visualization, C.P., I.V., M.E.C., G.P., M.C.F., L.V. and R.A.; supervision, C.P. and R.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable for studies not involving humans or ani-mals.
Informed Consent Statement
Not applicable for studies not involving humans. You might also choose to exclude this statement if the study did not involve humans.
Data Availability Statement
The data sets used in this article are not readily available because [including reason, e.g., the data are part of an ongoing study
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Centers for Disease Control and Prevention. Guidelines for Infection Control in Dental Health-Care Settings - 2003. MMWR 2003; 52(No RR-17):1-66. Available online: https://www.cdc.gov/mmwr/pdf/rr/rr5217.pdf. Accessed October 15, 2024.
- Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectation for Safe Care. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; October 2016. Available online: https://www.cdc.gov/dental-infection-control/media/pdfs/2024/07/safe-care2.pdf?CDC_AAref_Val=https://www.cdc.gov/oralhealth/infectioncontrol/pdf/safe-care2.pdf. Accessed October 15, 2024.
- Cole, E.C.; Cook, C.E. Characterization of infectious aerosols in healthcare facilities: an aid to effective engineering controls and preventive strategies. Am J Infect Control 1998, 26, 453-464. [CrossRef]
- Kumbargere Nagraj, S.; Eachempati, P.; Paisi, M.; Nasser M.; Sivaramakrishnan, G.; Verbeek, J.H. Interventions to reduce contaminated aerosols produced during dental procedures for preventing infectious diseases. Cochrane Database Syst Rev Oct 12 2020, 10(10), 1-122CD013686.
- Kumbargere Nagraj, S.; Eachempati, P.; Paisi, M.; Nasser, M.; Sivaramakrishnan, G.; Francis, T.; Verbeek, J.H. Preprocedural mouth rinses for preventing transmission of infectious diseases through aerosols in dental healthcare providers. Cochrane Database Syst Rev 2022, 8, 1-122. [CrossRef]
- Laheij, A.M.; Kistler, J.O.; Belibasakis, G.N.; Välimaa H.; de Soet J.J. European Oral Microbiology Workshop (EOMW). Healthcare-associated viral and bacterial infections in dentistry. J Oral Microbiol 2012, 4. [CrossRef]
- Van der Weijden, F. Aerosol in the oral health-care setting: a misty topic. Clin Oral Investig 2023, 27, 23-32.
- Zemouri C.; de Soet, H.; Crielaard, W.; Laheij, A. A scoping review on bioaerosols in healthcare and the dental environment. PLoS ONE 2017, 12, e0178007. [CrossRef]
- Centers for Disease Control and Prevention. Guidelines for Environmental infection Control in Health-Care Facilities. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). 2003. Update: July 2019. Available online: https://www.cdc.gov/infection-control/media/pdfs/Guideline-Environmental-H.pdf. Accessed October 15, 2024.
- Pankhurst, C.L.; Coulter, W.A. Do contaminated dental unit waterlines pose a risk of infection? J Dentistry 2007, 35, 712-720.
- Pasquarella, C.; Veronesi, L.; Napoli, C.; Castiglia, P.; Liguori, G.; Rizzetto, R.; Montagna, M.T.; Rizzetto, R.; Torre, I.; Righi, E.; Farruggia, P.; Tesauro, M.; Torregrossa, M.V.; Montagna M.T.; Colucci, M.E. et al. Microbial environment contamination in Italian dental clinics: A multicenter study yielding recommendations for standardized sampling methods and threshold values. Sci Total Environ 2012, 420, 289-299. [CrossRef]
- Rautemaa, R.; Nordberg, A.; Wuolijoki-Saaristo, K.; Meurman, J.H. Bacterial aerosols in a dental practice - a potential hospital infection problem? 2006, 64, 76-81. [CrossRef]
- Szymanska, J. Dental bioaerosols as an occupational hazard in a dentist’s workplace. Ann Agric Environ Med 2007, 14, 203-207.
- Castiglia, P.; Liguori, G.; Montagna, M.T.; Napoli, C.; Pasquarella, C.; Bergomi, M.; Fabiani, L.; Monarca, S.; Petti, S. Italian multicenter study on infection hazards during dental practice: control of environmental microbial contamination in public dental surgeries. BMC Public Health 2008, 8, 187-193. [CrossRef]
- Harrel, S.K.; Molinari, J. Aerosols and splatter in dentistry: a brief review of the literature and infection control implications. J Am Dent Assoc 2004, 135(4), 429-437.
- King, T.B.; Muzzin, K.B.; Berry, C.V.; Anders, L.M. The effectiveness of an aerosol reduction device for ultrasonic scalers. J Periodontol 1997, 68, 45-49. [CrossRef]
- Puljich, A.; Jiao, K.; Lee, R.S.; Walsh, L.J.; Ivanovski, S.; Han, P. Simulated and clinical aerosol spread in common periodontal aerosol-generating procedures. Clin Oral Investig 2022, 26, 5751-5762. [CrossRef]
- Timmerman, M.F.; Menso, L.; Steinfort, J.; van Winkelhoff, A.J.; van der Weijden, G.A. Atmospheric contamination during ultrasonic scaling. J Clin Periodontol 2004, 31, 458-462. [CrossRef]
- Kadailcifer, D.G.; Cotuk, A. Microbial contamination of dental unit waterlines and effect on quality of indoor air. Environ Monit Assess 2014, 186, 3431-3444.
- Szymanska, J. Biofilm and dental unit waterlines. Ann Agric Environ Med 2003, 10(2), 151-7.
- Szymańska, J.; Sitkowska, J. Bacterial contamination of dental unit waterlines. Environ Monit Assess 2013 May, 185(5), 3603-11. [CrossRef]
- Allsopp, J.; Basu, M.K.; Browne, R.M.; Burge, P.S.; Matthews, J.B. Survey of the use of personal protective equipment and prevalence of work-related symptoms among dental staff. Occup Environ Med 1997, 54, 125-134. [CrossRef]
- Araujo, M.W.; Andreana, S. Risk and prevention of transmission of infectious diseases in dentistry. Quintessence Int 2002, 33, 376-382.
- Polednik, B. Exposure of staff to aerosols and bioaerosols in a dental office. Building and Environment 2021, 187, 107388. [CrossRef]
- Bahador, M.; Alfirdous, R.A.; Alguria, T.A.; Griffin, I.; Tordik, P.A.; Martinho, F.C. Aerosols generated during endodontic treatment: a special concern during the Coronavirus Disease 2019 Pandemic. J Endod 2019, 47, 732-739. [CrossRef]
- Manea, A.; Crisan, D.; Baciut, G.; Baciut, M.; Bran, S.; Armencea, G.; Crisan, M.; Colosi, H.; Colosi, I.; Vodnar, D.; Aghorghiesei, A.; Aghorghiesei, O. The importance of atmospheric microbial contamination control in dental offices: Raised awareness caused by the SARS-CoV-2 Pandemic. Appl Sci 2021, 11, 2359. [CrossRef]
- Ralli, M.; Candelori, F.; Cambria, F.; Greco, A.; Angeletti, D.; Lambiase, A.; Campo, F.; Minni, A.; Polimeni, A.; De Vincentiis, M. Impact of COVID-19 pandemic on otolaryngology, ophthalmology and dental clinical activity and future perspectives. Eur Rev Med Pharmacol Sci 2020, 24, 9705-9971. [CrossRef]
- Suprono, M.S.; Savignano, R.; Won, J.B.; Lillard, S.; Zhong, Z.; Ahmed, A.; Roque-Torres, G.; Zhang, W.; Oyoyo, U.B.; Richardson, P.; Caruso, J.; Handysides, R.; Li, Y. Evaluation of microbial air quality and aerosol distribution in a large dental clinic. Am J Dent 2022, 35(5), 268-272.
- Wood D.; Da Silva K. A review of infection prevention and control guidelines for dental offices during the COVID-19 pandemic in mid-2020. Canadian Journal of Infection Control 2021, 36(3), 129-137.
- Li, Y.; Leung, G.M.; Tang, J.W.; Yang, X.; Chao, C.H.; Lin, J.Z.; Lu, J.W.; Nielsen, P.V.; Niu, J.; Qian, H.; Sleigh, A.C.; Su, H.J.; Sundell, J.; Wong, T.W.; Yuen, P.L. Role of ventilation in airborne transmission of infectious agents in the built environment - a multidisciplinary systematic review. Indoor Air 2007, 17, 2-18. [CrossRef]
- EN 17141:2020. Cleanrooms and associated controlled environments - Biocontamination control.
- ISO 14698-1:2003. Cleanrooms and associated controlled environments biocontamination control. Part 1: general principles and methods.
- Pasquarella, C.; Albertini, R.; Dall’Aglio, P.; Saccani, E.; Sansebastiano, G.E.; Signorelli, C. Air microbial sampling: The state of the art. Ig San Pubbl 2008, 64, 79–120.
- Pitzurra, M.; Savino, A.; Pasquarella, C. Microbiological environment monitoring (MEM). Ann Ig 1997, 9, 439–454.
- Whyte W.; Thomas A.M. Auditing the microbiological quality of the air in operating theatres. Bone Joint J 2024, 106-B(9), 887-891. [CrossRef]
- Viani, I.; Colucci, M.E.; Pergreffi, M.; Rossi, D.; Veronesi, L.; Bizzarro, A.; Capobianco, E.; Affanni, P.; Zoni, R.; Saccani, E.; Albertini, R.; Pasquarella C. Passive air sampling: the use of the index of microbial air contamination. Acta Biomed 2020, 91, 92-105. [CrossRef]
- Dybwad, M.; Skogan, G.; Blatny, J.M. Comparative Testing and Evaluation of Nine Different Air Samplers: End-to-End Sampling Efficiencies as Specific Performance Measurements for Bioaerosol Applications. Aerosol Science and Technology 2014, 48, 282-295.
- Whyte, W.; Green, G.; Albisu, A. Collection efficiency and design of microbial air samplers. Journal of Aerosol Science 2007, 38 (1), 97-110. ISSN 0021-8502. [CrossRef]
- Pasquarella, C.; Pitzurra, O.; Savino, A. The index of microbial air contamination. J Hosp Infect 2000, 46, 241–256. [CrossRef]
- R Development Core Team, 2024. A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available online: http://www.R-project.org/.
- Aquino de Muro, M.; Shuryak, I.; Uhlemann, A-C.; Tillman, A.; Seeram, D.; Zakaria, J.; Welch, D.; Erde, S.M.; Brenner, D.J. The abundance of the potential pathogen Staphylococcus hominis in the air microbiome in a dental clinic and its susceptibility to far-UVC light. MicrobiologyOpen 2023, 12, e1348. [CrossRef]
- Decraene V.; Ready, D.; Pratten, J.; Wilson, M. Air-borne microbial contamination of surfaces in a UK dental clinic. J Gen Appl Microbiol 2008, 54, 195-203. [CrossRef]
- Kherdekar, R.S.; Dixit, A.; Kothari, A.; Pandey K.P.; Advani, H.; Gaurav, A.; Omar, B.J. Unusually isolated Staphylococcus arlettae in intra-oral sutures - Case series. Access Microbiol 2023, 5, 000555.v4. [CrossRef]
- Manarte-Monteiro, P.; Carvalho, A.; Pina, C.; Olivira, H.; Conceicao Manso, M. Air quality assessment during dental practice: Aerosols bacterial counts in an universitary clinic. Rev Port Estomatol Med Dent Cir Maxillofac 2013, 54, 2-7. [CrossRef]
- Montalli, V.A.M.; Garcez, A.S.; de Oliveira, L.V.C.; Sperandio, M.; Napimoga, M.H.; Motta, R.H.L. A novel dental biosafety device to control the spread of potentially contaminated dispersion particles from dental ultrasonic tips. PLoS One 2021, 6(2), e0247029. [CrossRef]
- Pasquarella, C.; Veronesi, L.; Castiglia, P.; Liguori, G.; Montagna, M.T.; Napoli, C.; Rizzetto, R.; Torre, I.; Masia, M.D.; Di Onofrio, V.; Colucci, M.E.; Tinteri, C.; Tanzi, M. Italian multicentre study on microbial environmental contamination in dental clinics: a pilot study. Sci Total Environ 2010, 408, 4045-4051. [CrossRef]
- Pasquarella, C.; Vitali, P.; Saccani, E.; Manotti, P.; Boccuni, C.; Ugolotti, M.; Signorelli, C.; Mariotti, F.; Sansebastiano, G.E.; Albertini, R. Microbial air monitoring in operating theatres: experience at the University Hospital of Parma. J Hosp Infect 2012, 81(1), 50-7. [CrossRef]
- Shanmugaraj, G.B.; Rao, A. A study to assess the microbial profile and index of microbial air contamination in dental operatories. Indian J Dent Res 2020, 31, 465-469. [CrossRef]
- Vieira, C.D.; De Carvalho, M.A.; De Resende, M.A.; De Menezes Cussiol, N.A.; Alvarez-Leite, M.E.; Dos Santos, S.G.; de Oliveira, M.B.; De Magalhães, T.F.; Silva, M.X.; Nicoli, J.R.; de Macêdo Farias, L. Isolation of clinically relevant fungal species from solid waste and environment of dental health services. Lett Appl Microbiol 2010, 51, 370-376. [CrossRef]
- Zemouri, C.; Volgenant, C.M.C.; Buijs, M.J.; Crielaard, W.; Rosema, N.A.M.; Brandt, B.W.; Laheij, A.M.G.A.; De Soet, J.J. Dental aerosols: microbial composition and spatial distribution. J Oral Microbiol 2020, 12, 1762040. [CrossRef]
- Cellini, L.; Di Campli, E.; Di Candia, M.; Chiavaroli, G. Quantitative microbial monitoring in a dental office. Public Health 2001, 115, 301-305. [CrossRef]
- Guida M.; Gallé, F.; Di Onofrio, V.; Nastro, R.A.; Battista, M.; Liguori, R.; Battista, F.; Liguori, G. Environmental microbial contamination in dental setting: a local experience. J Prev Med Hyg 2012, 53, 207-212.
- Hossein, M.; Hossein, K.; Mojtaba, S.; Davood, E. Relation of bacteriological water and air quality in dentistry center. J Pure Appl Microbiol 2014, 8, 681-692.
- Petti, S.; Iannazzo, S.; Tarsitani, G. Comparison between different methods to monitor the microbial level of indoor air contamination in the dental office. Ann Ig 2003, 15, 725-733.
- Tellier, R.; Li, Y.; Cowling, B.J.; Tang, J.W. Recognition of aerosol transmission of infectious agents: a commentary. BMC Infect Dis 2019, 19, 101. [CrossRef]
- Kedjarune, U.; Kukiattrakoon, B.; Yapong, B.; Chowanadisai, S.; Leggat, P. Bacterial aerosols in the dental clinic: effects of time, position and type of treatment. Int Dent J 2000, 50, 103-107.
- Agodi, A.; Auxilia, F.; Barchitta, M.; Cristina, M.L.; D’Alessandro, D.; Mura, I.; Nobile, M.; Pasquarella, C. Italian Study Group of Hospital Hygiene. Operating theatre ventilation systems and microbial air contamination in total joint replacement surgery: results of the GISIO-ISChIA study. J Hosp Infect 2015, 90, 213-219. [CrossRef]
- Cristina, M.L.; Spagnolo, A.M.; Ottria, G.; Schinca, E.; Dupont, C.; Carbone, A.; Oliva, M.; Sartini, M. Microbial Air Monitoring in Turbulent Airflow Operating Theatres: Is It Possible to Calculate and Hypothesize New Benchmarks for Microbial Air Load? Int J Environ Res Public Health 2021 Oct 2, 18(19), 10379. PMID: 34639680; PMCID: PMC8507732. [CrossRef]
- Veronesi, L.; Colucci, M.E.; Napoli, C.; Castiglia, P.; Liguori, G.; Torre, I.; Righi, E.; Farruggia, P.; Tesauro, M.; Montagna, M.T.; Gallè, F.; Masia, M.D.; Di Onofrio, V.; Caggiano, G.; Tinteri, C.; Panico, M.; Pennino, F.; Cannova, L.; Pasquarella, C. Air microbial contamination in dental clinics: comparison between active and passive methods. Acta Biomed 2020 Apr 10, 91(3-S), 165-167. PMID: 32275284; PMCID: PMC7975899. [CrossRef]
- Perdelli, F.; Sartini, M.; Orlando, M.; Secchi, V.; Cristina, M.l. Relationship between settling microbial load and suspended microbial load in operating rooms. Ann Ig 2000, 12, 373-380.
- European Commission. EU Guidelines to Good Manufacturing Practice Medicinal Products for Human and Veterinary Use Revision to Annex 1. Manufacture of Sterile Medicinal Products. Brussels, 2022. 22 August. Available online: https://health.ec.europa.eu/system/files/2022-08/20220825_gmp-an1_en_0.pdf Accessed August 8, 2024.
- Napoli, C.; Marcotrigiano, V.; Montagna, M.T. Air sampling procedures to evaluate microbial contamination: a comparison between active and passive methods in operating theatres. BMC Public Health 2012, 2, 12, 594. [CrossRef]
- Orpianesi, C.; Cresci, A.; La Rosa, F.; Saltalamacchia, G.; Tarsi, R. Evaluation of microbial contamination in a hospital environment. Comparison between the Surface Air System and the traditional method. Nuovi Ann Ig Microbiol 1983, 34, 171-185.
- Pitzurra, M.; Morlunghi, P. Contaminazione microbica dell’aria atmosferica: correlazione fra due diverse metodiche di rilevazione. Ig Mod 1978, 71, 490-502.
- Verhoeff, A.P.; van Wijnen, J.H.; Bolej, J.S.; Brunekreef, B.; van Reenen-Hoekstra, E.S.; Samson, R.A. Enumeration and identification of airborne viable mould propagules in houses. A field comparison of selected techniques. Allergy 1990, 45, 275-284. [CrossRef]
- Whyte, W. Sterility assurance and models for assessing airborne bacterial contamination. Parenter Sci Technol 1986, o40, 188–97.
- Chawla, H.; Anand, P.; Garg, K.; Bhagat, N.; Varmani, S.G.; Bansal, T.; McBain, A.J.; Marwah, R.G. A comprehensive review of microbial contamination in the indoor environment: sources, sampling, health risks, and mitigation strategies. Front Public Health 2023, 11, 1285393. [CrossRef]
- Najotra, D.K.; Malhotra, A.S.; Slathia, P.; Raina, S.; Dhar, A. Microbiological Surveillance of Operation Theatres: Five Year Retrospective Analysis from a Tertiary Care Hospital in North India. Int J Appl Basic Med Res 2017, 7(3), 165-168. [CrossRef]
- Oulkheir, A.; Safouan, H.; El Housse, F.; Aghrouch, M.; Ounine, K.; Douira, A.; Chadli, S. Assessment of microbiological indoor air quality in a public hospital in the city of Agadir, Morocco. Periodicum Biologorum 2021, 123(1-2), 29-34. [CrossRef]
- Poletti, L.; Pasquarella, C.; Pitzurra, M.; Savino, A. Comparative efficiency of nitrocellulose membranes versus RODAC plates in microbial sampling on surfaces. J Hosp Infect 1999, 41(3), 195-201. [CrossRef]
Figure 1.
Flow diagram of the review.
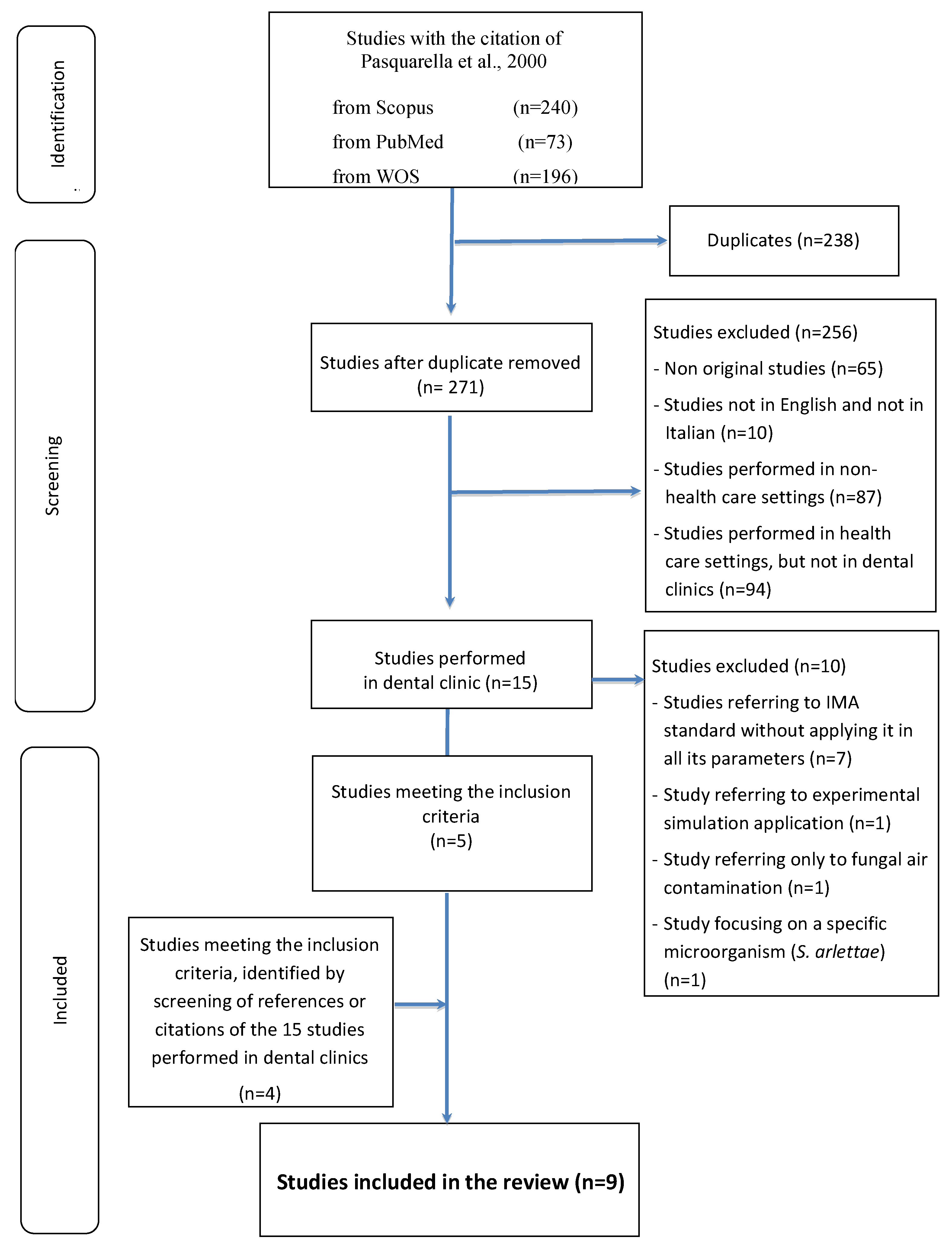
Figure 2.
Mean IMA values in the studies before (T0), during (T1), and after (T2) dental procedures.
Figure 2.
Mean IMA values in the studies before (T0), during (T1), and after (T2) dental procedures.
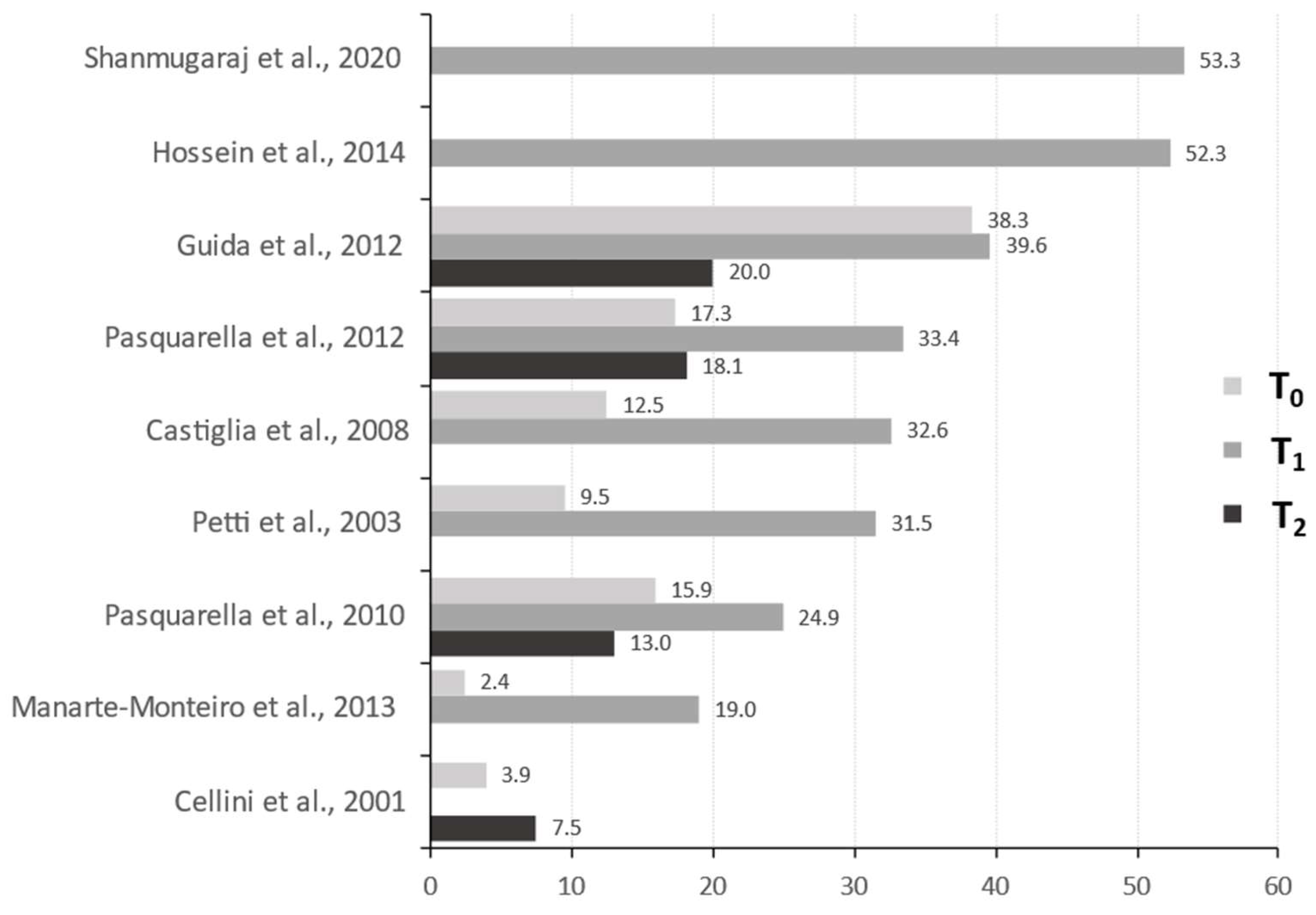
Figure 3.
Meta-analysis of the mean IMA values in the studies before (T0), during (T1), and after (T2) dental procedures.
Figure 3.
Meta-analysis of the mean IMA values in the studies before (T0), during (T1), and after (T2) dental procedures.
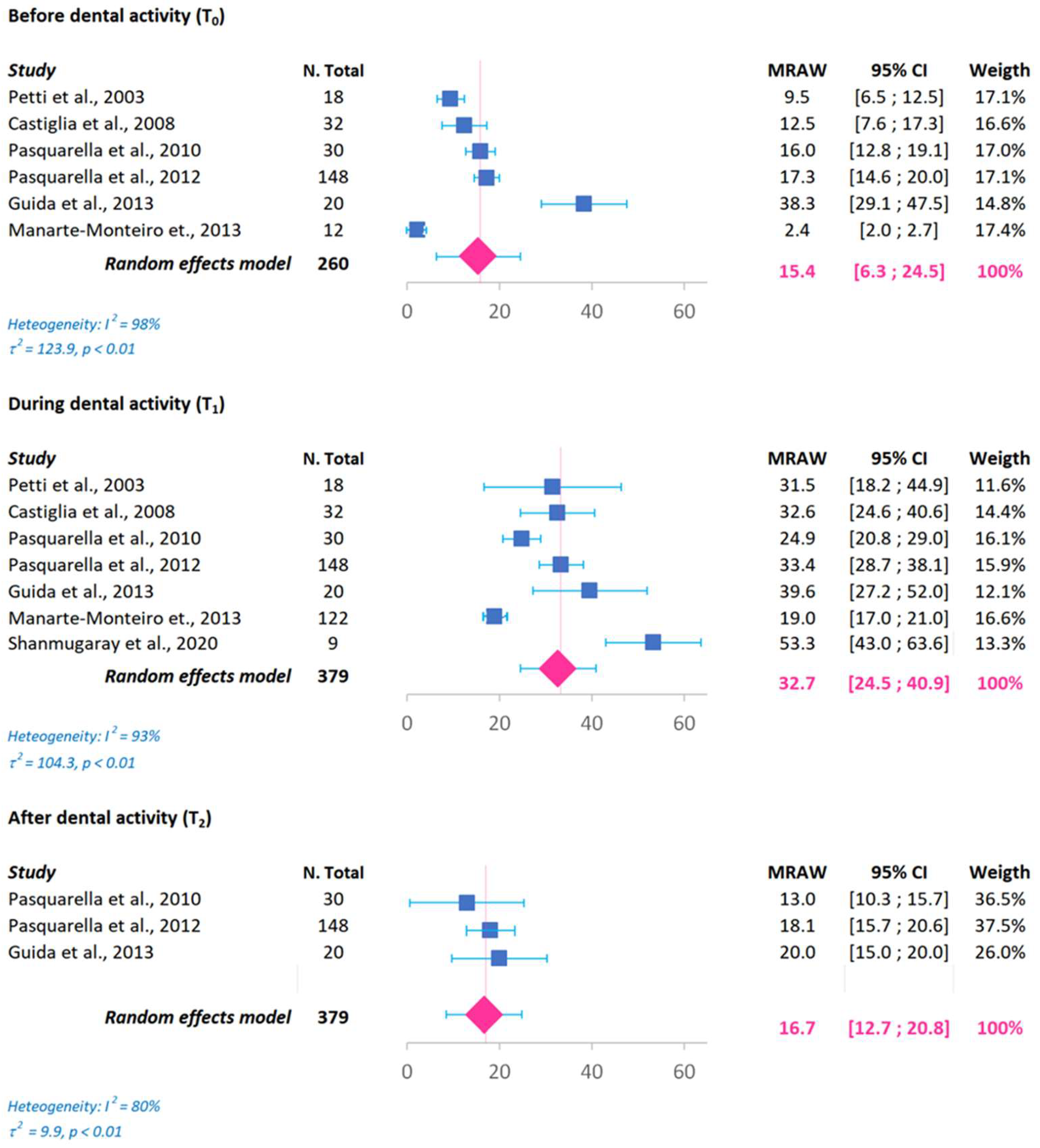
Figure 4.
Meta-analysis of the mean IMA values during (T1) dental procedures in European studies.
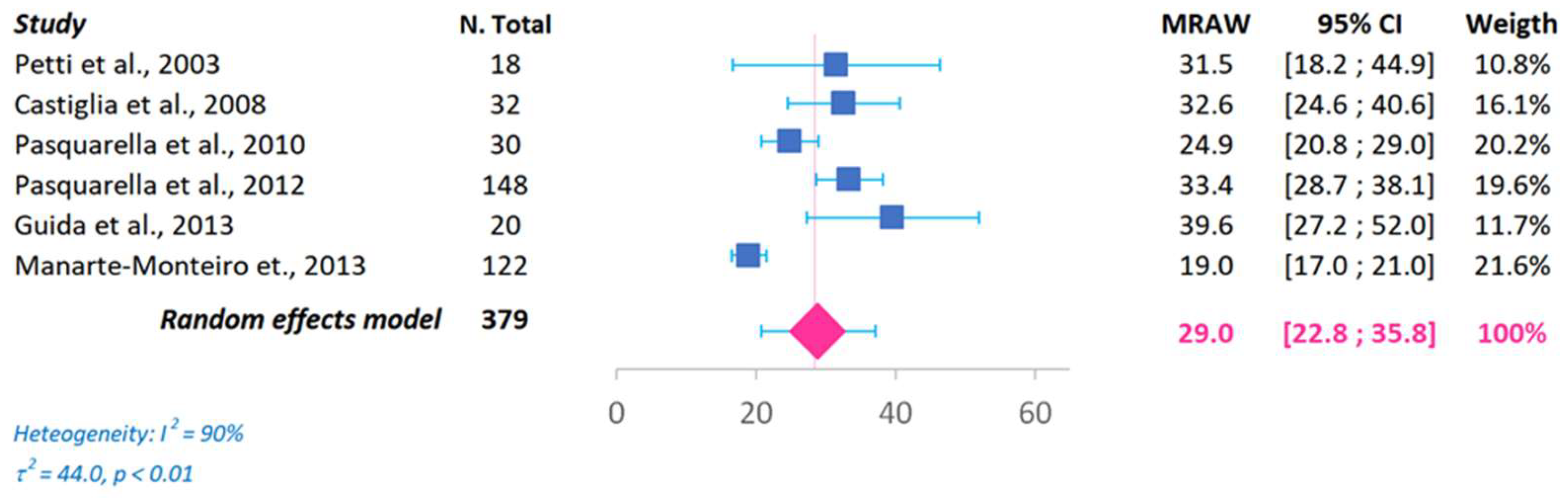

Table 1.
Characteristics of the studies using the Index of Microbial Air contamination (IMA) standard.
Table 1.
Characteristics of the studies using the Index of Microbial Air contamination (IMA) standard.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



