
Submitted:
13 March 2025
Posted:
13 March 2025
You are already at the latest version
Abstract
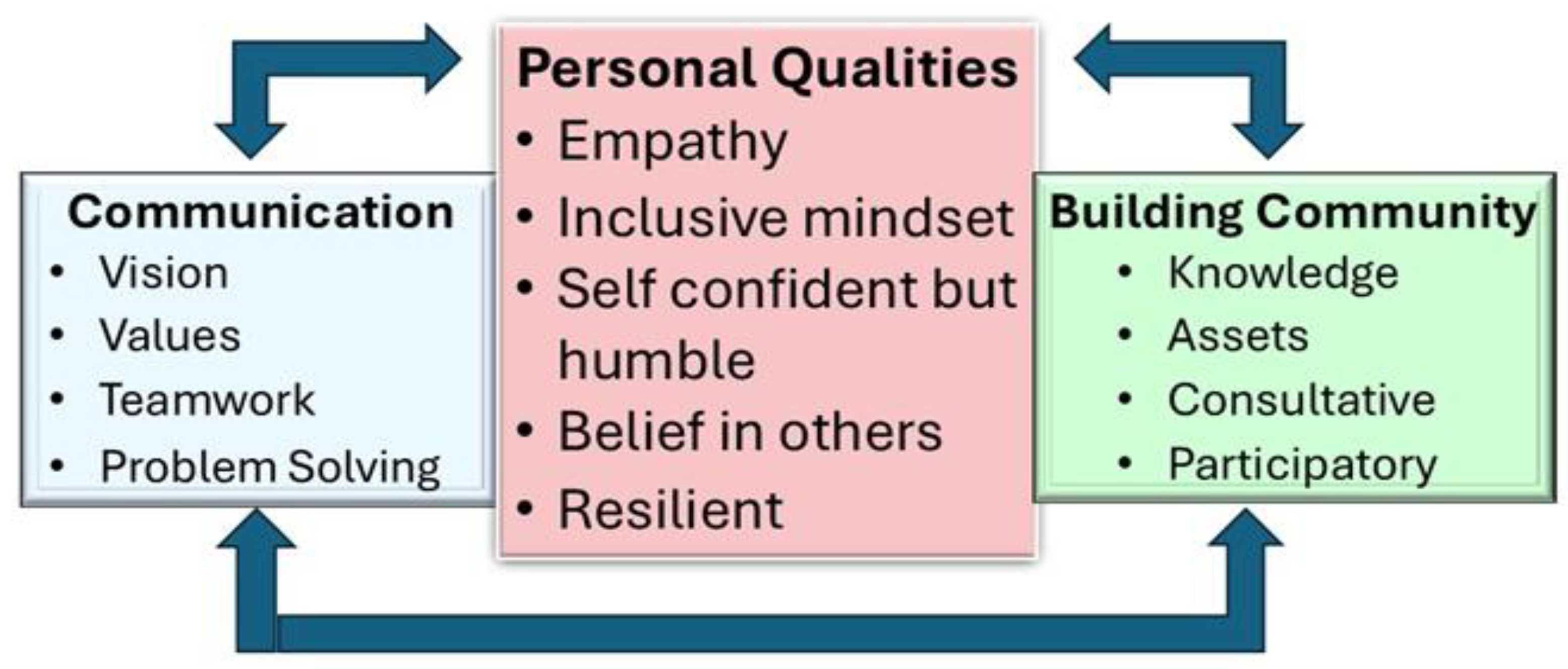
The health and social care needs of children and adults with disabilities are often neglected in many low and middle income countries. International opinion favours the creation of community-based supports rather than the institutional and clinic-based care that has dominated to date. However models of care that are reliant on community leadership have been slow to develop within and across less affluent countries. Moreover, the managerial models inherent in institutional based care are likely to be inadequate in such settings. The study aimed to explore the leadership qualities required in initiating and sustaining community-based supports. Face-to-face interviews were conducted with a purposeful sample of 16 leaders of projects in Africa, Asia and South America. They included people with sensorial, physical and intellectual disabilities as well as non-disabled leaders of local and national projects plus others whose leadership was at a regional or international level. Two main questions were addressed: what are the qualities required to function as a community leaders and how can these qualities be nurtured in low resourced settings. Thematic content analysis identified three core themes: first, personal qualities such as empathy with an understanding of the personal circumstances of persons in need of support, second, communicating clearly the vision and values informing their work, and thirdly, building and mobilising community support from families and neighbours. The nurturing of leadership comes through mentoring and coaching, the empowerment of others, networking opportunities and the development of inter-personal and communication skills. These themes were commonly expressed across the 16 leaders from all the participating nations and at all levels of responsibility which validates their universality. The findings are in marked contrast to current practices in health and social care that have valued professional expertise over lived experience, knowledge and technical skills over compassion and empathy, and the provision of person-centred ‘treatments’ over developing community and personal self-reliance. Nonetheless the challenges involved in establishing and sustaining new styles of leadership are many and will not be quickly resolved.
Keywords:
1. Background
1.1. Aims of the Study
2. Method
2.1. Sample
2.2. Procedure
2.3. Qualitative Analysis Using AI
2.4. Data Analysis
3. Findings
3.1. Personal Qualities of Leaders
A leader who listens to a voice that comes from the other people that you maybe leading and listening to them and taking actions towards those things. It shows braveness in you and shows kindness in you. And it also builds someone to be a role model of that person. (04)
The first thing is to be able to listen to what people are saying. Especially when you think about persons with disabilities, because they have a lot of grievances within themselves. Never be ..too hard on them because, you see, the issue is that these people are already broken. (02)
I think that the most important quality for leadership is empathy. You have to put your shoes in the others’ shoes … that’s really important. (12)
Leadership should be inclusive, and invite all people to the table. Not just to sit at the table, but to be a part of the discussion, or a part of the action. (16).
I think that the first and most important priority is to find someone who is a bridge builder, because essentially creating social inclusion means bringing together sometimes services, sometimes communities, sometimes neighbourhoods or groups of people or families who would not naturally find each other, or perhaps find communities of each other even if they were in the same physical space. (10)
Be confident of who you are. Be confident in what you do. Be confident when you speak. Be confident to fight for your rights. (04).
You should have the humility to learn from other people. (13)
A humble leader then is putting other people forward, is celebrating their work. It’s not taking all of the credit for themselves. (14)
I see a lot of qualities in many people, actually in all people. And it’s interesting because every person have like a different quality. Together it is like a (Jigsaw) puzzle inside all the group. (12)
A leader who listens to a voice that comes from other people that you are leading and listening to them and taking action towards those things. (04)
We work greatly with the self-respect with each person and to put value on what we are, what we have, and not in what we don’t have. (11)
Be someone who can keep the lines of communication open through thick and thin, accept criticism and be able to take accountability when needed. (05)
I persevered when there were troubles, because, I mean, organisations sometimes can find themselves in trouble. But we persevered together, and we endured together, we moved on. There were a lot of difficult times for the organisation. But they were able to see that I motivated them, I encouraged them. And they also encouraged others. (02)
What I would tell my fellow colleagues with intellectual disabilities is never give up. Never feel that you’re not home. Be confident of who you are. Be confident in what you do. Be confident when you speak. Be confident to fight for your rights. (04)
The self-confidence to be truly vulnerable, to admit when you don’t know something, to ask for help, to seek out advice, because it makes others know that they are truly participating. (10)
3.2. Communication
Spirit comes first before resources. If we have a spirit, we can collect resources, mobilise resources, but if we have resources but no spirit, then that leadership doesn’t work out. (01)
A leader does not mean that you have to just know how to read or write, but a leader should just know what to do and stand up for our rights. In Africa, it’s not easy to get a job. It’s not easy to have an education system. But we’re trying to find them, to advocate for ourselves to get meaningful roles, jobs, even education systems. (04)
When I speak about communication, it’s not a complicated purpose or technologies, because in the community, it’s people based. So how you talk to people, how you make them feel, how you convince them and how you make them feel to own that vision. (13)
Inclusion for us is such a kind of world where people living with and without disabilities can work together, can march together, can talk together, can laugh together, can cultivate friendship, and ultimately they can go and grow together at the same time.” (01)
Making inclusion an inherent value and .. meet up, discuss and maybe share the messages that you want to convey or that you want people to hear about and try to those messages in ways that can be accessible for people of all abilities. (05)
You have to cultivate your connections with the people you work with because these are the ones who will be going to work things out for your vision. The community develops you as a leader and then you develop community. (09)
You need to identify yourself as part of a community. You need to be taking active part of any actions that is meant to be destined for the well-being of the community and for you. (15)
A leader that’s able to make people come together to feel there’s a safe space to raise their concerns, to offer ideas. They have to get their hands dirty and be at the coalface of that work. (14)
Figuring out how you can do the best you can with what you have, and how you can creatively sort of exploit or see opportunities where others might not, is absolutely essential. (10)
Leadership is something, one could practise to be calculated risk takers, not kind of comfort seekers. (01)
One of the important assets to possess as a leader is the ability to be flexible and adaptive, which I believe people with disabilities have mastered. (05)
3.3. Building Community
It’s important for you to understand the DNA, the social fabric of that community, what makes them tick …the dynamics of that community. (10)
You need to identify yourself as part of a community. You need to be taking active part of any actions that is meant to be destined for the well-being of the community and for you. (15)
If you want to work to be great, work with those people who are in the local level, because they are the people who want the work to be done. (06)
Creating social inclusion means bringing together sometimes services, sometimes communities, sometimes neighbourhoods or groups of people or families who would not naturally find each other. (10)
It needs you to be open to new ideas, to new ways of thinking, and also to gather all those ideas and to process everything with your own ideas, your own way of being as a person. At the end you would be building community, not only for you, but also for the rest of the people that are part of the work that you are doing. (15)
A good leader also has to be a good follower… you are not leading a system or process, you are leading them through people. (09)
I think we can focus much more deeply on participatory forms of development and research to make sure that when we are going into a community and we’re talking about social inclusion, we have some ideas, we have some tools, but we don’t have a prescriptive process. We don’t just sort of hand over an instruction manual and say, this is how you do it. (10)
3.4. Styles of Leadership
The best leadership for me is what I call transformative leadership. It’s leadership that brings change and leadership that brings change is not the same as leadership that is for managing day-to-day tasks.” (13)
We should give, not just for leadership’s sake, but we should give them some sort of power to exercise so that they could exhibit their real abilities no matter whatever their physical limitations are. (01)
It’s a leader that listens to others. Compassion is the mainstay of what it would be, because if it’s not a compassionate leadership, then it’s not going to rally many people for the long term.” (14)
3.6. Nurturing Leadership
We all have the capacity and the ability to become a leader. The only thing is that you need to identify what is the cause that motivates you, that pulls those triggers inside of you that you say, okay, this is what I was looking for. This is something that really motivates me to do not even better, to do the best that I can. (15)
There was need to nurture another crop of leaders. So one thing that I decided to do was to identify those people that really showed interest in the organisation. And then apart from identifying them, I put them quite close to me so that they could learn the qualities of leading that organisation.” (02)
People can make mistakes because we are not gods, but we should make them learn from their mistakes. We cannot do anything about the past, but the only thing we can do is learn from that mistakes and help them nurture. (01)
I think a way is creating opportunities so they can share with people that feels the same as them. Learn good practises from the people around them. (11)
Coming to forums where we meet people from other areas also gives (leaders) a purpose for life in a way to say, okay, my fellows are doing it. Why not? Why can’t I? (08)
(Name) likes IT a lot that, you know, on all these platforms, he meets Google people. He’s inquisitive about it. Okay, how can I also use my IT to help me and also help other athletes? (08)
4. Discussion
4.1. Leadership Qualities
4.2. Nurturing and Developing Leaders
4.3. AI as a Tool in Research and Evaluation
4.4. Limitations and Future Research
4.5. Conclusions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation (2010) Community-based rehabilitation: CBR guidelines. Available at https://www.who.int/publications/i/item/9789241548052.
- Rifkin, S. B. (2018). Alma Ata after 40 years: Primary Health Care and Health for All—from consensus to complexity. BMJ global health, 3(Suppl 3), e001188. [CrossRef]
- Bitton, A. , Fifield, J., Ratcliffe, H., Karlage, A., Wang, H., Veillard, J. H.,... & Hirschhorn, L. R. (2019). Primary healthcare system performance in low-income and middle-income countries: a scoping review of the evidence from 2010 to 2017. BMJ Global Health, 4(Suppl 8), e001551. [CrossRef]
- Hone, T. , Gonçalves, J., Seferidi, P., Moreno-Serra, R., Rocha, R., Gupta, I.,... & Millett, C. (2024). Progress towards universal health coverage and inequalities in infant mortality: an analysis of 4· 1 million births from 60 low-income and middle-income countries between 2000 and 2019. The Lancet Global Health, 12(5), e744-e755. [CrossRef]
- Available at: https://www.worlddata.info/quality-of-life.php (last accessed 12 March, 2025).
- Zhou, M., & Shen, H. (2024). Forecasting the global burden of disease to 2050. The Lancet, 403(10440), 1961-1963. [CrossRef]
- Available at: https://sdgs.un.org/goals (last accessed 12 March, 2025).
- Malekpour, S., Allen, C., Sagar, A., Scholz, I., Persson, Å., Miranda, J. J., ... & Al-Ghanim, K. (2023). What scientists need to do to accelerate progress on the SDGs. Nature, 621(7978), 250-254. Available at: https://www.nature.com/articles/d41586-023-02808-x.
- World Health Organization. (2022). Global report on health equity for persons with disabilities. Geneva, World Health Organization.
- Roy, A. , Courtenay, K., Odiyoor, M., Walsh, P., Keane, S., Biswas, A.,... & Munir, K. (2021). Setting priorities for people with intellectual disability/intellectual developmental disorders across the lifespan: a call to action by the World Psychiatric Association. BJPsych international, 18(3), 54-57. [CrossRef]
- Lindsay, S. , Phonepraseuth, J., & Leo, S. (2024). Experiences and factors affecting poverty among families raising a child with a disability: a scoping review. Disability and Rehabilitation, 1-19. [CrossRef]
- Ohnmar, H. T. W. E. , Yuliawiratman, B. S., Tannor, A. Y., Asikin, M. Z. N., Elaine, S. O. H., De Groote, W.,... & Naicker, A. S. (2024). Barriers and facilitators for increased accessibility to quality rehabilitation services in low-and middle-income countries: a systematic review. European Journal of Physical and Rehabilitation Medicine, 60(3), 514. [CrossRef]
- World Health Organization; UNICEF. Global Report on Children with Developmental Disabilities: From the Margins to the Mainstream; World Health Organization: Geneva, Switzerland; United Nations Children’s Fund (UNICEF): New York City, NY, USA, 2023; Available online: https://www.who.int/publications/i/item/9789240080539 (last accessed on 12 March 2025).
- Sacks, E., Schleiff, M., Were, M., Chowdhury, A. M., & Perry, H. B. (2020). Communities, universal health coverage and primary health care. Bulletin of the World Health Organization, 98(11), 773. [CrossRef]
- Nuri, R.P.; Batorowicz, B.; Aldersey, H.M. Family support and family and child-related outcomes among families impacted by disability in low-and middle-income countries: A scoping review. J. Child Health Care 2020, 24, 637–654. [Google Scholar] [PubMed]
- UNICEF. Inclusive Interventions for Children with Disabilities: An Evidence and Gap Map from Low- and Middle-Income Countries; UNICEF Innocenti—Global Office of Research and Foresight: Rome, Italy, 2022; Available online: https://www.unicef-irc.org/publications/1537-inclusive-interventions-for-children-with-disabilities-in-low-and-middle-income-countries-an-evidence-gap-map.html (last accessed on 12 March, 2025).
- McConkey, R. (2024). Creating Family-Centred Support for Preschoolers with Developmental Disabilities in Low-Income Countries: A Rapid Review to Guide Practitioners. International Journal of Environmental Research and Public Health, 21(6), 651. [CrossRef]
- Essex, R., Kennedy, J., Miller, D., & Jameson, J. (2023). A scoping review exploring the impact and negotiation of hierarchy in healthcare organisations. Nursing Inquiry, 30(4), e12571. [CrossRef]
- Akmal, A. , Podgorodnichenko, N., Foote, J., Greatbanks, R., Stokes, T., & Gauld, R. (2021). Why is quality improvement so challenging? A viable systems model perspective to understand the frustrations of healthcare quality improvement managers. Health policy, 125(5), 658-664. [CrossRef]
- Czabanowska, K. (2014). Leadership in Public Health: reducing inequalities and improving health. Eurohealth, 20(3), 28-31. http://www.euro.who.int/__data/assets/pdf_file/0010/257743/EuroHealth_v20n3.
- The Oxford Character Project (2023). Character and global leadership: A survey of character-based leadership education and research in low- and middle-income countries. Available at: https://oxfordcharacter.org/research/character-global-leadership-report-2023.
- Eva, N. , Robin, M., Sendjaya, S., Van Dierendonck, D., & Liden, R. C. (2019). Servant leadership: A systematic review and call for future research. The leadership quarterly, 30(1), 111-132. [CrossRef]
- Bandura, A. (1977). Social learning theory. Oxford, England: Prentice-Hall.
- Green, D. How Change Happens; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- World Medical Association Declaration of Helsinki (2013). Ethical Principles for Medical Research Involving Human Subjects. Available at: https://www.wma.net/wp-content/uploads/2016/11/DoH-Oct2013-JAMA.
- Aung, Y. Y. , Wong, D. C., & Ting, D. S. (2021). The promise of artificial intelligence: a review of the opportunities and challenges of artificial intelligence in healthcare. British medical bulletin, 139(1), 4-15. [CrossRef]
- Qiao, S. , Fang, X., Garrett, C., Zhang, R., Li, X., & Kang, Y. (2024). Generative AI for Qualitative Analysis in a Maternal Health Study: Coding In-depth Interviews using Large Language Models (LLMs). medRxiv, 2024-09.
- Christou, P. A. (2023). How to use artificial intelligence (AI) as a resource, methodological and analysis tool in qualitative research?. Qualitative Report, 28(7).
- Braun, V., & Clarke, V. (2022). Conceptual and design thinking for thematic analysis. Qualitative Psychology, 9(1), 3–26. [CrossRef]
- Frechette, J. , Bitzas, V., Aubry, M., Kilpatrick, K., & Lavoie-Tremblay, M. (2020). Capturing lived experience: Methodological considerations for interpretive phenomenological inquiry. International Journal of Qualitative Methods, 19, 1609406920907254.
- Okpala, P. (2020). Increasing access to primary health care through distributed leadership. International Journal of Healthcare Management, 14(3), 914–919. [CrossRef]
- Ammerman, A. , Smith, T. W., & Calancie, L. (2014). Practice-based evidence in public health: improving reach, relevance, and results. Annual review of public health, 35(1), 47-63. [CrossRef]
- Langlois, E. V. , McKenzie, A., Schneider, H., & Mecaskey, J. W. (2020). Measures to strengthen primary health-care systems in low-and middle-income countries. Bulletin of the World Health Organization, 98(11), 781. [CrossRef]
- Karuga, R. , Kok, M., Luitjens, M., Mbindyo, P., Broerse, J. E., & Dieleman, M. (2022). Participation in primary health care through community-level health committees in Sub-Saharan Africa: a qualitative synthesis. BMC public health, 22(1), 359. [CrossRef]
- Karuga, R. , Khan, S., Kok, M., Moraa, M., Mbindyo, P., Broerse, J., & Dieleman, M. (2023). Teamwork in community health committees: a case study in two urban informal settlements. BMC health services research, 23(1), 1373. [CrossRef]
- Ludwick, T. , Morgan, A., Kane, S., Kelaher, M., & McPake, B. (2020). The distinctive roles of urban community health workers in low-and middle-income countries: a scoping review of the literature. Health policy and planning, 35(8), 1039-1052. [CrossRef]
- Demeke, G. W. , van Engen, M. L., & Markos, S. (2024). Servant leadership in the healthcare literature: a systematic review. Journal of healthcare leadership, 1-14. [CrossRef]
- Lorenzo, T. , Motau, J., van der Merwe, T., Janse van Rensburg, E., & Cramm, J. M. (2015). Community rehabilitation workers as catalysts for disability: inclusive youth development through service learning. Development in Practice, 25(1), 19-28. [CrossRef]
- Zhang, H. , Wu, C., Xie, J., Lyu, Y., Cai, J., & Carroll, J. M. (2023). Redefining qualitative analysis in the AI era: Utilizing ChatGPT for efficient thematic analysis. arXiv:2309.10771.
- World Health Organisation Guidance (2021). Ethics and governance of artificial intelligence for health. Geneva, World Health Organization.
- Ned, L. , Tiwari, R., Hess-April, L., Lorenzo, T., & Chikte, U. (2020). A situational mapping overview of training programmes for community-based rehabilitation workers in Southern Africa: strategies for strengthening accessible rural rehabilitation practice. Frontiers in Public Health, 8, 569279. [CrossRef]

| Code | Role | Country/ Region |
Personal Statement | Status | Gender |
| 01 | Co-founder of a youth-led, volunteer-based organisation called Rights as a Society | Nepal | I have a visual impairment and have graduated from University. I’m passionate about leadership entrepreneurship in grassroots movements, so that people with disabilities would be able to speak up for their rights and also they would be able to stand on their own feet. | Country National | Male |
| 02 | A disability activist and Disability Officer with the national office of an international NGO. | Zambia | Blind from when I was 10 years old, I graduated from University with a PhD and previously worked as a university lecturer. | Country National | Male |
| 03 | Social Advocate and founder of NGO to advise families on support services and companies to promote inclusive employment. | UAE | Recovered from brain injury as child. University degree in international relations. | Country national | Male |
| 04 | Member of Global Youth Council set up by international NGO and representing African Region | Sub Sharan Africa |
In my role I am representing my fellow colleagues with intellectual disability. And locally, back home, I am a sports assistant. I’m a health messenger and also the vice chairperson for the local athlete input council. | Regional National | Male |
| 05 | Senior social media editor in print and radio. | UAE | A wheelchair user, I use my current role to shape or reframe the media, pushing more inclusion and making the media more diverse | Country National | Female |
| 06 | Trainer of leaders in sports and self-employment | Sub-Sharan Africa | At my school I studied automotive engineering. I’ve been able to mentor around 20 students in my campus. We have an organisation there that we are running of helping young people to start their own businesses. | Regional National | Male |
| 07 | A psychologist and university teacher and researcher. A mother of a child with autism. | Zambia | To engage with parents and communities and to encourage them that there’s something they can do about it. | Country National | Female |
| 08 | Volunteer mentor to young adults with intellectual disability | Zimbabwe | A social worker with over 10 years of practice and a volunteer for the Lions Club International with a local sports organisation. Former cricketer. | Country national | Male |
| 09 | National Sports Director for an organisation serving people with intellectual disabilities | Pakistan | I have been working in my role since 2019 and before that as a sports development volunteer with the organisation for whom I work. I have had a strong passion for sports, for community development, leadership and they all come together in my present job. | Country national | Female |
| 10 | Country Director employed by International company/contractor working in-country on inclusion. | Uzbekistan | Adjunct university faculty member on doctoral Education Leadership Program. Previously worked in Central Asia, South Caucasus, Eastern Europe and Southeast Asia on inclusive education projects. | Expatriate to the country | Female |
| 11 | National co-ordinator of Inclusion project led by Sports NGO | Argentina | Qualified as psychopedagogue. Preparing training courses and guides for implementers of inclusion in schools across the county. | Country national | Female |
| 12 | Project co-ordinator of youth projects in our National sports NGO | El Salvador | I have experienced disability since birth through my uncle (who lives with an intellectual disability) my experience has made me passionate about advocating for human rights and constantly seeking new knowledge to change the world. | Country National | Female |
| 13 | Director for global development and government relations in a regional NGO. | Sub-Sharan Africa | I have been with the NGO for 17 years, having started as a volunteer, then paid manager, national director in one country and as a regional director for 5 years. | Regional Director | Female |
| 14 | Regional Director of International NGO responsible for planning, monitoring data and analytics. | South Asia | University graduate, with over 15 years experience with previous positions at HQ . | Expatriate to region | Male |
| 15 | Regional Officer for inclusion with an International sports NGO | Latin America | A university graduate with responsibility for inclusion in schools and promoting the leadership of people with intellectual disabilities. | Regional/National | Male |
| 16 | Chief inspirational officer and Board Member of an International NGO for sports and people with intellectual disability | Global | A person with intellectual disability whose been a sports participant and advocate since 1970 . | US citizen | Female |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



