Submitted:
12 March 2025
Posted:
13 March 2025
You are already at the latest version
Abstract
Background/Objectives: Advance care planning (ACP) is essential in ensuring that end-of-life (EOL) care aligns with patients' values and preferences. Despite its benefits, advance directive (AD) completion rates remain low, particularly among racial and ethnic minority populations. This study examines disparities in AD completion among patients with stage 4 solid tumor lung and gastrointestinal (GI) cancers and explores the role of caregivers in influencing patient decision-making. Methods: A cross-sectional, descrip-tive, correlational study utilizing secondary data analysis was conducted to assess pre-dictors of AD completion in a cohort of stage 4 solid tumor lung and GI cancer patients (n=235) and their caregivers (n=235). Patient and caregiver variables were analyzed to de-termine their impact on ACP engagement. Logistic regression analysis was used to iden-tify significant predictors of AD completion. Results: Among the study cohort, 67% (n=157) of patients had documented ADs. Disparities were evident, with non-White pa-tients 36% less likely to complete ADs compared to White patients. AD completion varied by socioeconomic status, with lower-income individuals demonstrating reduced engage-ment in ACP. Age and race were significant predictors of AD completion, with older age positively associated with completion (OR = 1.09). Findings highlight the need for targeted interventions to address inequities in ACP engagement. Conclusion: Nurses play a critical role in facilitating ACP discussions and addressing barriers to AD completion. Culturally sensitive, patient-centered interventions are necessary to bridge disparities and improve ACP engagement, particularly among historically underserved populations. Institutional policies should support nurses in integrating ACP discussions into routine care, ensuring equitable and patient-centered EOL decision-making.
Keywords:
ACP Conversations
; ACP documents
; clinical implications
; ancer
; end of life care
; health disparities
1. Introduction
Cancer progression significantly impacts patients and their families, often resulting in uncontrolled symptoms, the need for advance care planning (ACP), psychosocial and spiritual support, and complex treatment decisions [1,2,3,4]. Additionally, understanding prognosis and preparing for end-of-life (EOL) transitions are essential aspects of patient-centered care [5,6]. ACP ensures that patients receive medical interventions aligned with their values, goals, and preferences [7,8,9]. Despite the well-documented benefits of advance directives (ADs), completion rates remain low, with only one-third of adults having them in place [10,11,12].
Patients and families should be empowered to communicate their EOL treatment preferences, regardless of the care setting [13]. Many patients in the terminal phase of illness are not enrolled in hospice or palliative care, underscoring the need for healthcare professionals—particularly nurses—to facilitate these discussions across various healthcare environments [14,15,16]. Nurses are integral to the assessment of patient and caregiver understanding of diagnoses, prognoses, and treatment options [17,18,19]. Effective communication strategies equip nurses to lead these essential conversations, ensuring that patients’ voices are heard and respected in their care decisions [20,21,22].
Identifying and addressing patients’ goals of care in advanced cancer settings is critical for delivering high-quality healthcare [23,24,25,26]. However, multiple barriers hinder AD completion, including late-stage discussions, uncertainty regarding disease trajectory, complex family decision-making dynamics, and communication challenges between patients and providers [27,28]. Despite significant research on ACP, progress in overcoming these barriers remains limited.
2. Background
The growing population of older adults, particularly those over 65, has increased the demand for effective EOL communication between patients and healthcare providers [29,30]. Racial and ethnic disparities further complicate this issue. Studies indicate that White patients are more likely to discuss treatment limitations and complete ADs than Black and Hispanic patients [31,32,33,34]. Additionally, non-White patients are more likely to die in acute care settings and less likely to engage in EOL planning [35,36,37,38].
Beyond race and ethnicity, socioeconomic and cultural factors also influence EOL decision-making [39]. Mistrust of the healthcare system, religious and spiritual beliefs, literacy levels, and previous experiences with medical care impact patients’ willingness to engage in ACP. [40,41,42]. Additionally, the perception that ACP discussions are relevant only to those with terminal illnesses contributes to low participation rates [43,44]. Addressing these disparities requires culturally responsive, patient-centered interventions that prioritize trust-building and health education.
Given that many patients receive EOL care outside of specialized palliative or hospice settings, nurses across all specialties must be well-versed in assessing EOL preferences. Their role in patient advocacy, education, and communication uniquely positions them to facilitate ACP conversations, ensuring that care delivery aligns with patient values and preferences.
3. Methods
Our team conducted a study to examine factors that predict advance directive completion of stage 4 solid tumor Lung and GI cancer patients. The purpose of the original study was to understand how antecedent and process factors play a role in AD completion. This was a cross-sectional, descriptive, correlational study utilizing secondary data analysis. We examined how stage 4 solid tumor lung and GI cancer patients (n=235) and their caregivers (n=235) decided to complete or not to complete an advance directive. We postulated that caregiver factors influenced the patient to complete an advance directive. We examined patient and caregiver variables to understand their influence on patient EOL decision-making. The purpose of this article is to highlight the results of disparities in AD completion and make recommendations for clinical implications.
4. Results
Among the study cohort, 67% (n=157) of patients had documented ADs. However, significant disparities were evident. Of the patients with ADs, 28% (n=44) were non-White, including 24% African American, 50% Asian, and 50% Hispanic participants. AD completion rates varied by income, with 48% of those earning ≤$20,000, 52% earning $21,000–$49,999, and 56% earning $50,000 or more completing ADs. Logistic regression analysis identified age and race as significant predictors of AD completion, with older age positively associated with completion (OR = 1.09) and non-White patients exhibiting a 36% lower likelihood of AD completion compared to White patients. These findings highlight disparities in AD completion rates, emphasizing the necessity for targeted interventions to improve engagement in ACP among historically underserved populations. See Figure 1.
5. Discussion of Clinical Implications
The American Nurses Association (ANA) and the Hospice and Palliative Nurses Association (HPNA) emphasize the critical role of nurses in ACP facilitation [16,45,46]. Despite the availability of ADs for adults over 18, only a minority complete them, with older adults more likely to engage in ACP than younger populations. Racial and ethnic disparities persist, reinforcing the need for structured interventions that promote ACP engagement across diverse patient groups. Nurses must integrate discussions on EOL preferences into routine care while employing culturally sensitive communication strategies [47,48,49]. See Figure 2.
- Expanding nurses’ role in ACP and AD completion.
Nurses must proactively assess patients’ familiarity with ADs and provide tailored education to facilitate their completion [7]. This process involves initiating open-ended, nonjudgmental discussions that normalize ADs as a fundamental aspect of comprehensive healthcare planning. Many patients, particularly those from underrepresented populations, lack exposure to ACP or misunderstand its purpose [50]. By addressing misconceptions, nurses can play a pivotal role in fostering informed decision-making.
- Assessing patient readiness and knowledge
To effectively guide patients, nurses should assess their level of understanding and comfort with ACP discussions using the following inquiries:
- “Have you considered documenting your preferences for medical care in case you cannot communicate them in the future?”
- “Do you know what treatment options, including life-sustaining interventions, are available to you?”
- “Have you had conversations about your healthcare wishes with your family or designated caregivers?”
- Explaining the benefits of ADs
To encourage AD completion, nurses must emphasize its advantages, such as ensuring patient autonomy, reducing family burden, aligning treatment with personal values, and preventing unnecessary or undesired interventions. Providing real-world examples can help patients contextualize the importance of ACP.
- Facilitating AD completion
AD documents can appear complex and legally intimidating to many patients. Nurses can support patients in this process by:
- Simplifying AD forms through step-by-step guidance.
- Explaining legal terms in accessible language.
- Discussing treatment preferences in alignment with patient goals.
- Encouraging family involvement in ACP discussions.
- Addressing barriers to ACP completion
Barriers to AD completion include fear of discussing mortality, cultural and religious concerns, and distrust of the medical system. Nurses can mitigate these obstacles by:
- Creating a supportive environment for ACP discussions.
- Utilizing culturally competent communication strategies.
- Providing multilingual and literacy-friendly resources.
- Partnering with community organizations to extend outreach efforts.
- Leveraging interdisciplinary collaboration
Nurses can enhance ACP implementation by collaborating with palliative care teams, social workers, and legal advisors. Interdisciplinary efforts ensure a comprehensive approach to AD completion and patient-centered care planning [51].
- Future research directions
Although ADs are widely recognized as valuable, their completion rates remain low. Future research should explore the following:
- Evidence-based training programs for healthcare professionals in ACP facilitation.
- Policy changes integrating ACP into routine primary and specialty care.
- The role of technology and digital ACP tools in improving completion rates.
6. Conclusions
Nurses serve as critical facilitators in promoting ACP and ensuring patients’ EOL preferences are documented and honored. Culturally sensitive, proactive conversations regarding ACP are essential to bridging disparities in AD completion. Institutional policies must support nurses in integrating ACP discussions into clinical practice. By fostering trust, providing clear guidance, and leveraging interdisciplinary collaboration, nurses can significantly improve AD engagement and patient-centered EOL care.
Author Contributions
Each of the authors had the following contributions: Conceptualization, S.A. and D.G.; methodology, S.A.; software, S.A.; validation, S.A. and D.G.; formal analysis, S.A.; investigation, S.A.; resources, S.A.; data curation, S.A.; writing—original draft preparation, S.A. and D.G.; writing—review and editing, S.A., D.G., and S.D.; visualization, S.A. and S.D.; supervision, S.A.; project administration, S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the use of a secondary data analysis of de-identified data.
Informed Consent Statement
Patient consent was waived due to the work not including identified data.
Data Availability Statement
Data is not available at this time due to the author not owning the rights to the primary data set.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACP | Advance Care Planning |
| AD | Advance Directive |
| GI | Gastrointestinal |
| EOL | End of Life |
References
- Crawford GB, Dzierżanowski T, Hauser K, et al. Care of the adult cancer patient at the end of life: ESMO Clinical Practice Guidelines☆. ESMO Open. 2021;6(4):100225. [CrossRef]
- Aaron SP, Musacchio C, Douglas SL. Understanding Factors That Predict Advance Directive Completion. Palliat Med Rep. 2022;3(1):220-224. [CrossRef]
- Hui D, Heung Y, Bruera E. Timely Palliative Care: Personalizing the Process of Referral. Cancers. 2022;14(4):1047. [CrossRef]
- ‘My wife is my doctor at home’: A qualitative study exploring the challenges of home-based palliative care in a resource-poor setting. [CrossRef]
- Fenton ATHR, Fletcher KM, Kizildag D, et al. Cancer Caregivers’ Prognostic and End-of-Life Communication Needs and Experiences and their Impact. J Pain Symptom Manage. 2023;65(1):16-25. [CrossRef]
- Rodenbach R, Caprio T, Loh KP. Challenges in hospice and end-of-life care in the transfusion-dependent patient. Hematology. 2024;2024(1):340-347. [CrossRef]
- Rosa WE, Izumi S, Sullivan DR, et al. Advance Care Planning in Serious Illness: A Narrative Review. J Pain Symptom Manage. 2023;65(1):e63-e78. [CrossRef]
- Goswami, P. Advance Care Planning and End-Of-Life Communications: Practical Tips for Oncology Advanced Practitioners. J Adv Pract Oncol. 2021;12(1):89-95. [CrossRef]
- Sedini C, Biotto M, Crespi Bel’skij LM, Moroni Grandini RE, Cesari M. Advance care planning and advance directives: an overview of the main critical issues. Aging Clin Exp Res. 2022;34(2):325-330. [CrossRef]
- Bernard C, Tan A, Slaven M, Elston D, Heyland DK, Howard M. Exploring patient-reported barriers to advance care planning in family practice. BMC Fam Pract. 2020;21(1):94. [CrossRef]
- Yadav KN, Gabler NB, Cooney E, et al. Approximately One In Three US Adults Completes Any Type Of Advance Directive For End-Of-Life Care. Health Aff (Millwood). 2017;36(7):1244-1251. [CrossRef]
- Alanazi MA, Shaban MM, Ramadan OME, et al. Navigating end-of-life decision-making in nursing: a systematic review of ethical challenges and palliative care practices. BMC Nurs. 2024;23(1):467. [CrossRef]
- Ajibade, B. Assessing the patient’s needs and planning effective care. Br J Nurs Mark Allen Publ. 2021;30(20):1166-1171. [CrossRef]
- Binda F, Clari M, Nicolò G, et al. Quality of dying in hospital general wards: a cross-sectional study about the end-of-life care. BMC Palliat Care. 2021;20(1):153. [CrossRef]
- Haavisto E, Soikkeli-Jalonen A, Tonteri M, Hupli M. Nurses’ required end-of-life care competence in health centres inpatient ward – a qualitative descriptive study. Scand J Caring Sci. 2021;35(2):577-585. [CrossRef]
- Fliedner M, Halfens RJG, King CR, Eychmueller S, Lohrmann C, Schols JMGA. Roles and Responsibilities of Nurses in Advance Care Planning in Palliative Care in the Acute Care Setting: A Scoping Review. J Hosp Palliat Nurs. 2021;23(1):59. [CrossRef]
- George LS, Matsoukas K, McFarland DC, et al. Interventions to Improve Prognostic Understanding in Advanced Stages of Life-Limiting Illness: A Systematic Review. J Pain Symptom Manage. 2022;63(2):e212-e223. [CrossRef]
- Gray TF, Forst D, Nipp RD, Greer JA, Temel JS, El-Jawahri A. Prognostic Awareness in Caregivers of Patients with Incurable Cancer. J Palliat Med. 2021;24(4):561-569. [CrossRef]
- Lewandowska A, Rudzki G, Lewandowski T, Rudzki S. The Problems and Needs of Patients Diagnosed with Cancer and Their Caregivers. Int J Environ Res Public Health. 2021;18(1):87. [CrossRef]
- Chen W, Chung JOK, Lam KKW, Molassiotis A. End-of-life communication strategies for healthcare professionals: A scoping review. Palliat Med. 2023;37(1):61-74. [CrossRef]
- Potter JE, Elliott RM, Kelly MA, Perry L. Education and training methods for healthcare professionals to lead conversations concerning deceased organ donation: An integrative review. Patient Educ Couns. 2021;104(11):2650-2660. [CrossRef]
- Olsson MM, Windsor C, Chambers S, Green TL. A Scoping Review of End-of-Life Communication in International Palliative Care Guidelines for Acute Care Settings. J Pain Symptom Manage. 2021;62(2):425-437.e2. [CrossRef]
- Hoare S, Antunes B, Kelly MP, Barclay S. End-of-life care quality measures: beyond place of death. BMJ Support Palliat Care. Published online July 12, 2022. [CrossRef]
- Davidson BA, Puechl AM, Watson CH, et al. Promoting timely goals of care conversations between gynecologic cancer patients at high-risk of death and their providers. Gynecol Oncol. 2022;164(2):288-294. [CrossRef]
- McNiff KK, Caligiuri MA, Davidson NE, et al. Improving Goal Concordant Care Among 10 Leading Academic U.S. Cancer Hospitals: A Collaboration of the Alliance of Dedicated Cancer Centers. The Oncologist. 2021;26(7):533-536. [CrossRef]
- Patel MI, Khateeb S, Coker T. Association of a Lay Health Worker–Led Intervention on Goals of Care, Quality of Life, and Clinical Trial Participation Among Low-Income and Minority Adults With Cancer. JCO Oncol Pract. 2021;17(11):e1753-e1762. [CrossRef]
- Kim H, Flieger SP. Barriers to Effective Communication about Advance Care Planning and Palliative Care: A Qualitative Study. J Hosp Palliat Care. 2023;26(2):42-50. [CrossRef]
- Poveda-Moral S, Falcó-Pegueroles A, Ballesteros-Silva MP, Bosch-Alcaraz A. Barriers to Advance Care Planning Implementation in Health care: An Umbrella Review with Implications for Evidence-Based Practice. Worldviews Evid Based Nurs. 2021;18(5):254-263. [CrossRef]
- Fact Sheet: Aging in the United States. PRB. Accessed February 6, 2025. Available online: https://www.prb.org/resources/fact-sheet-aging-in-the-united-states/.
- Bureau, UC. Older Population and Aging. Census.gov. Accessed December 4, 2023. Available online: https://www.census.gov/topics/population/older-aging.html.
- Bazargan M, Bazargan-Hejazi S. Disparities in Palliative and Hospice Care and Completion of Advance Care Planning and Directives Among Non-Hispanic Blacks: A Scoping Review of Recent Literature. Am J Hosp Palliat Care. 2021;38(6):688-718. [CrossRef]
- Jones T, Luth EA, Lin SY, Brody AA. Advance Care Planning, Palliative Care, and End-of-life Care Interventions for Racial and Ethnic Underrepresented Groups: A Systematic Review. J Pain Symptom Manage. 2021;62(3):e248-e260. [CrossRef]
- Hong M, Kim K. Advance care planning among ethnic/racial minority older adults: Prevalence of and factors associated with informal talks, durable power of attorney for health care, and living will. Ethn Health. 2022;27(2):453-462. [CrossRef]
- Ashana DC, D’Arcangelo N, Gazarian PK, et al. “Don’t Talk to Them About Goals of Care”: Understanding Disparities in Advance Care Planning. J Gerontol A Biol Sci Med Sci. 2021;77(2):339-346. [CrossRef]
- Aaron SP, Gazaway SB, Harrell ER, Elk R. Disparities and Racism Experienced Among Older African Americans Nearing End of Life. Curr Geriatr Rep. 2021;10(4):157-166. [CrossRef]
- Hanna JR, Rapa E, Dalton LJ, et al. A qualitative study of bereaved relatives’ end of life experiences during the COVID-19 pandemic. Palliat Med. 2021;35(5):843-851. [CrossRef]
- Gazaway S, Chuang E, Thompson M, White-Hammond G, Elk R. Respecting Faith, Hope, and Miracles in African American Christian Patients at End-of-Life: Moving from Labeling Goals of Care as “Aggressive” to Providing Equitable Goal-Concordant Care. J Racial Ethn Health Disparities. 2023;10(4):2054-2060. [CrossRef]
- Cid M, Quan Vega ML, Yang Z, Guglielminotti J, Li G, Hua M. Disparities in end-of-life care for minoritized racial and ethnic patients during terminal hospitalizations in New York State. J Am Geriatr Soc. 2024;72(9):2690-2699. [CrossRef]
- Moss KO, Happ MB, Brody A. Nurses’ Role in Reducing Inequities for the Seriously Ill. J Gerontol Nurs. 2022;48(8):3-5. [CrossRef]
- Kunonga TP, Thomson KH, Beyer FR, Dawson S, Brittain K, Craig D. A Mixed Methods Systematic Review of the Effectiveness, Acceptability, and Feasibility of Advanced Care Plans for Older Adults Without Life-Limiting Conditions. J Long-Term Care. 2024;0. [CrossRef]
- Van Scoy LJ, Green MJ, Witt PD, et al. Low Skepticism and Positive Attitudes About Advance Care Planning Among African Americans: a National, Mixed Methods Cohort Study. J Gen Intern Med. 2021;36(3):705-712. [CrossRef]
- Catlett L, Campbell C. Advance Care Planning and End of Life Care Literacy Initiatives in African American Faith Communities: A Systematic Integrative Review. Am J Hosp Palliat Med. 2021;38(6):719-730. [CrossRef]
- Canny A, Mason B, Boyd K. Public perceptions of advance care planning (ACP) from an international perspective: a scoping review. BMC Palliat Care. 2023;22(1):107. [CrossRef]
- Association AM. Why You Should Talk to Patients About Advance Directives. Accessed February 26, 2025. Available online: https://edhub.ama-assn.org/pages/why-talk-to-patients-about-advance-directives.
- Nurse A. Calling for all nurses to lead and transform palliative care. American Nurse. May 10, 2017. Accessed February 11, 2025. Available online: https://www.myamericannurse.com/calling-nurses-lead-transform-palliative-care/.
- Moran S, Bailey ME, Doody O. Role and contribution of the nurse in caring for patients with palliative care needs: A scoping review. PLOS ONE. 2024;19(8):e0307188. [CrossRef]
- Islam Z, Pollock K, Patterson A, et al. Thinking ahead about medical treatments in advanced illness: a qualitative study of barriers and enablers in end-of-life care planning with patients and families from ethnically diverse backgrounds. Health Soc Care Deliv Res. 2023;11(7):1-135. [CrossRef]
- Brooks L, Manias E, Rasmussen B, Bloomer M. Practice recommendations for culturally-sensitive communication at the end of life. Aust Crit Care. 2024;37:S9. [CrossRef]
- Crooks J, Trotter S, OBE RB, Monaghan E, Clarke G, Patient Public Involvement Consortium. How does ethnicity affect presence of advance care planning in care records for individuals with advanced disease? A mixed-methods systematic review. BMC Palliat Care. 2023;22(1):43. [CrossRef]
- Shepherd V, Hood K, Wood F. ‘It’s not making a decision, it’s prompting the discussions’: a qualitative study exploring stakeholders’ views on the acceptability and feasibility of advance research planning (CONSULT-ADVANCE). BMC Med Ethics. 2024;25(1):80. [CrossRef]
- Wilkin K, Fang ML, Sixsmith J. Implementing advance care planning in palliative and end of life care: a scoping review of community nursing perspectives. BMC Geriatr. 2024;24(1):294. [CrossRef]
Figure 1.
Advance Directive Completion vs. Study Sample Distribution.
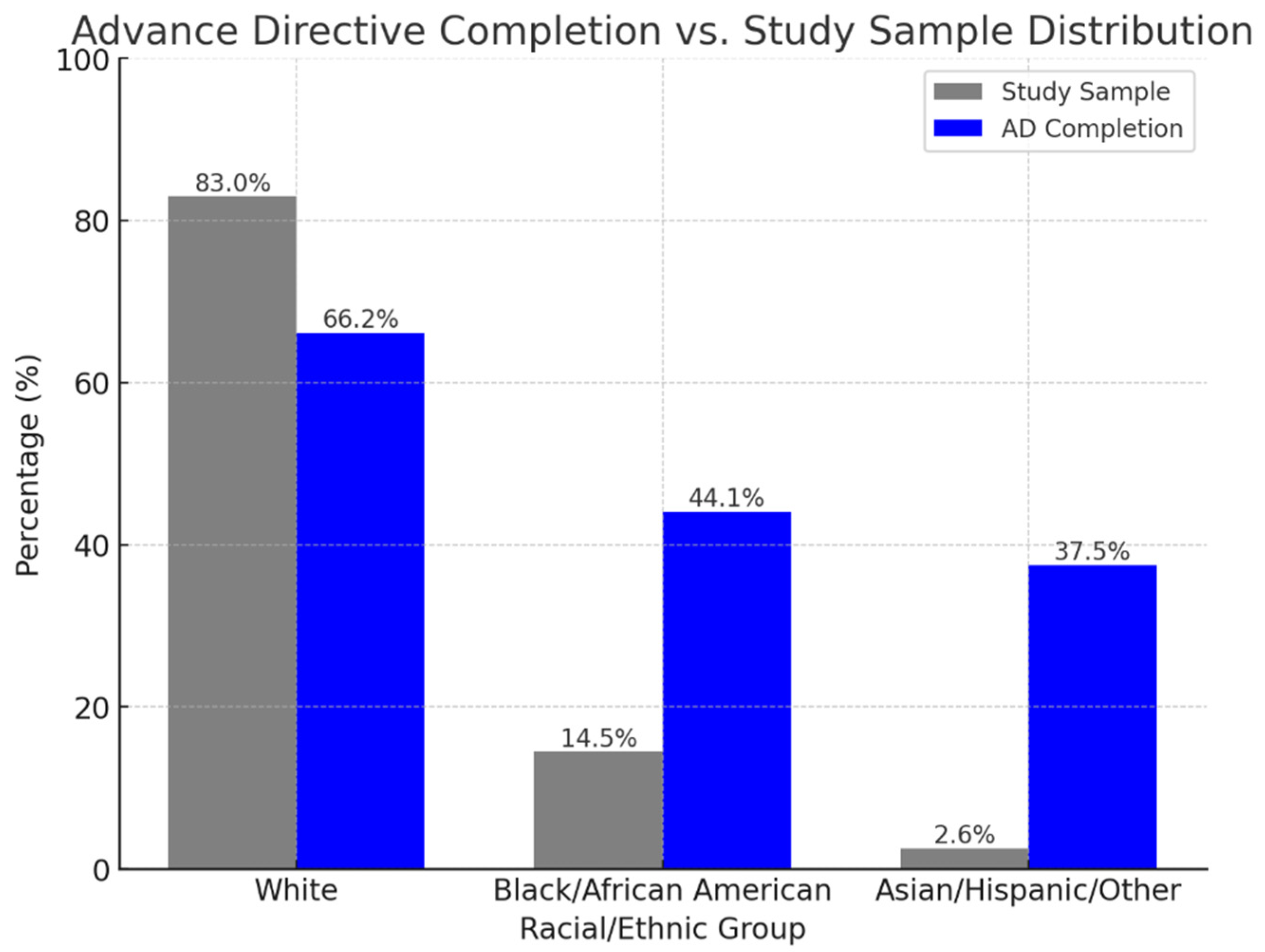
Figure 2.
Clinical Implications.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



