Submitted:
11 March 2025
Posted:
11 March 2025
You are already at the latest version
Abstract
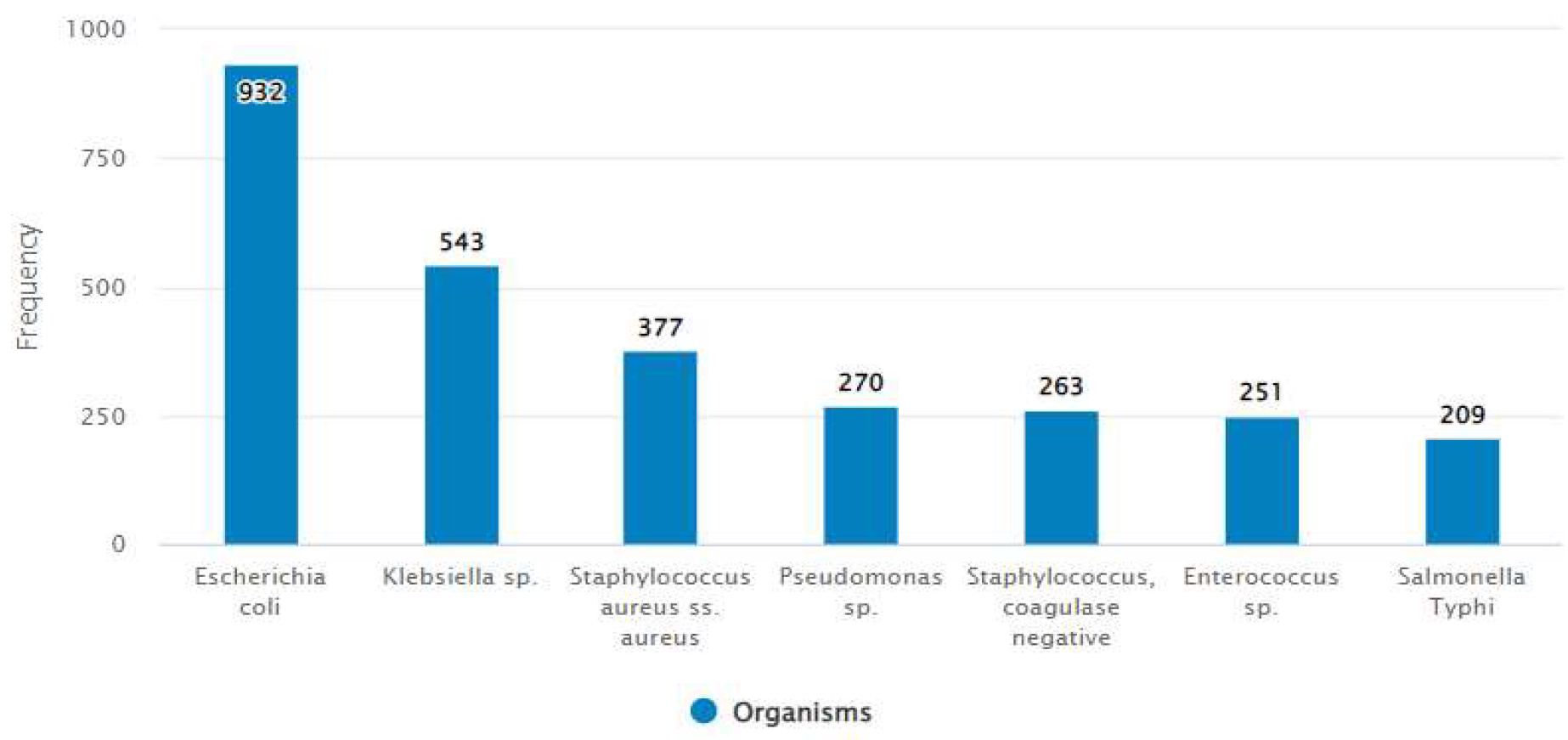
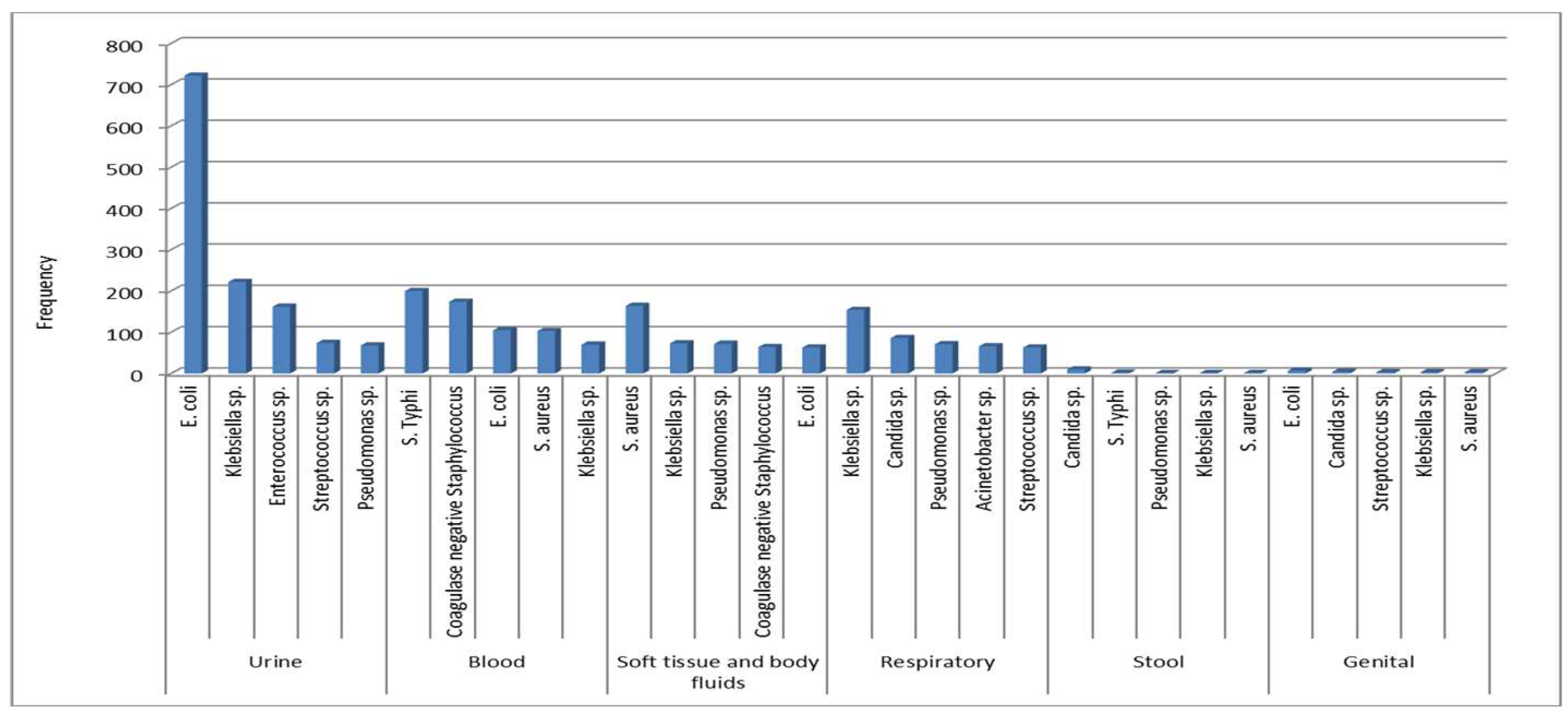
Background: It is essential to monitor causative agents of infections and antimicrobial resistance patterns to inform treatment and policy at the local level. In this study, we investigated the microbiological profile and antibiotic susceptibility pattern records in a tertiary care hospital. Materials and Method: This cross-sectional study was performed in a tertiary care hospital in Dhaka city, Bangladesh. The study utilized a retrospective descriptive research approach conducted between January 2018 and February 2021 in which culture results of blood, stool, urine, body fluid, genital, respiratory and soft tissue specimens were retrieved and analyzed. Results: A total of 26,825 samples were ana-lyzed; of which 3,779 records for microbial growth from clinical specimens were identi-fied, yielding a 14.09% isolation rate. Escherichia coli (E. coli), Klebsiella sp., Staphylo-coccus aureus, Pseudomonas sp., coagulase negative Staphylococcus, Salmonella Typhi and Enterococcus sp. were the most frequently isolated organisms among all specimens. E. coli, the most common causative organism of urinary tract infection (UTI) and genital infection, showed high resistance to co-trimoxazole (48%), ciprofloxacin (79%), and cephalosporins (63-65%) while the resistance rate to nitrofurantoin (7%), mecillinam (16%), aminoglycosides (7-18%), meropenem (8%) and colistin (0%) was low. In bloodstream infection, the most common microorganism found was S. Typhi. High sensitivity towards amoxicillin (100%), chloramphenicol (78%), co-trimoxazole (76%), cefixime (100%) and ceftriaxone (100%) were seen in S. typhi whereas almost all isolates were resistant to nalidixic acid (97%) and ciprofloxacin (96%). S. aureus, the predominant cause of soft tissue infection, was highly sensitive to co-trimoxazole (70%), doxycycline (86%), and linezolid (97%). Methicillin-resistant Staphylococcus aureus (MRSA) was 54%. The most common cause of respiratory infection was Klebsiella sp. The rate of resistance of Klebsiella sp. to third and fourth generation cephalosporins was approximately 65% and to ciprofloxacin and meropenem was 74% and 42% respectively. Pseudomonas sp., found commonly in urine, soft tissue, body fluids, and respiratory infections, were susceptible to ceftazidime, piperacillin/tazobactam and ciprofloxacin with resistance rate of 27%, 18% and 34% re-spectively. High resistance to meropenem was recorded for Pseudomonas sp. (30%) and Acinetobacter sp. (64%). Acinetobacter sp. showed low sensitivity (< 45%) to all of the tested antibiotics except colistin and tigecycline. Conclusion: This study highlights the high potential for infections associated with resistant microorganisms in the tertiary care hospital where samples for this study were collected. It is therefore recommended that judicious treatment following drug-susceptibility testing of isolates, regular surveillance programs, and strict infection control measures be put into place to address this increasing drug resistance problem.
Keywords:
1. Introduction
2. Materials and Methods
Study design and place
Data collection and processing
Statistical analysis
3. Results
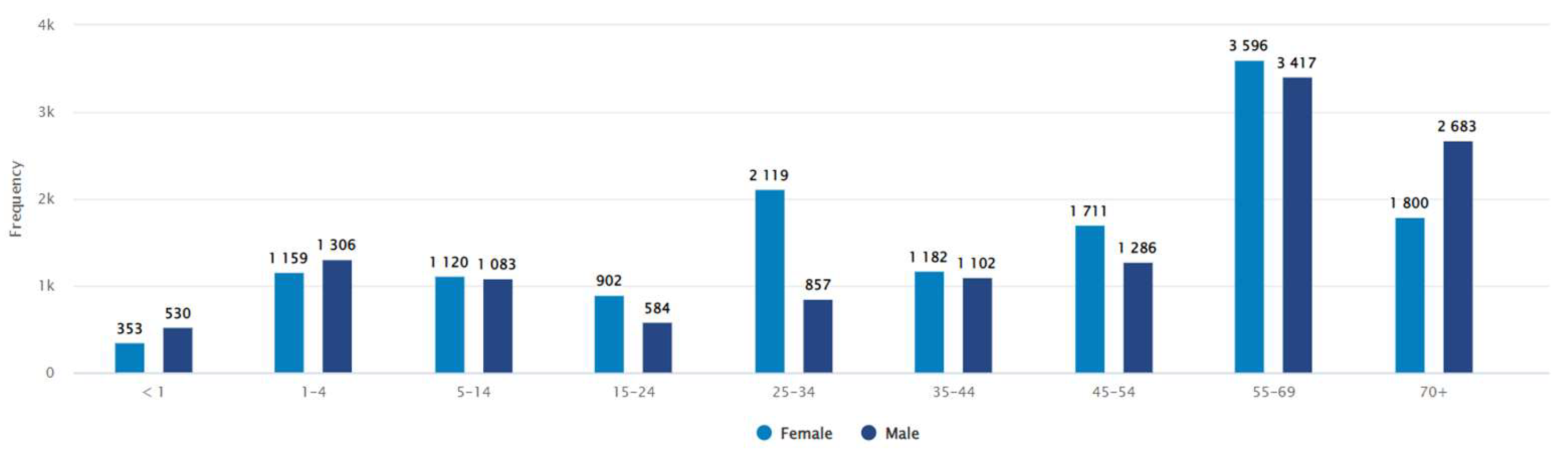
3.1. Demography and bacterial culture
3.1.1. Antibiotic susceptibility pattern
3.2. Figures, Tables and Schemes

| Specimen | All Isolates N (%) |
Positive culture n (%) |
Negative culture n (%) |
|---|---|---|---|
| Urine | 13059 (48.7) | 1549 (41) | 11510 (49.9) |
| Blood | 7274 (27.1) | 902 (23.9) | 6372 (27.6) |
| Soft tissue and body fluids | 2160 (8.1) | 567 (15) | 1593 (6.9) |
| Respiratory | 2012 (7.5) | 645 (17.1) | 1367 (5.9) |
| Stool | 1130 (4.2) | 17 (0.4) | 1113 (4.8) |
| Genital | 218 (0.8) | 23 (0.6) | 195 (0.8) |
| Others | 972 (3.6) | 76 (2) | 896 (3.9) |
| Total | 26825 | 3779 (14.09) | 23046 (85.91) |
| Organism | Number of patients* | AMC | AMK | AZM | CIP | CLI | CRO | CTX | CXM | DOX | FEP | FOX | GEN | LNZ | NET | NIT | PEN | SXT | TCY | TEC | VAN |
|
Staphylococcus aureus |
366 | 46 | 90 | 20 | 36 | 55 | 42 | 86 | 46 | 46 | 73 | 97 | 96 | 23 | 70 | 99 | 99 | ||||
|
Staphylococcus epidermidis |
260 | 39 | 91 | 16 | 46 | 61 | 38 | 92 | 39 | 39 | 68 | 96 | 97 | 32 | 63 | 100 | 100 | ||||
|
Enterococcus sp. |
247 | 72 | 25 | 9 | 15 | 11 | 30 | 31 | 63 | 29 | 68 | 98 | 61 | 74 | 66 | 10 | 38 | 90 | 99 | ||
|
Streptococcus pyogenes |
92 | 100 | 35 | 39 | 24 | 59 | 100 | 100 | 92 | 100 | 100 | 99 | 87 | 97 | 100 | 3 | 96 | 100 | |||
| Streptococcus agalactiae | 40 | 100 | 49 | 28 | 100 | 100 | 90 | 100 | 100 | 100 | 100 | 2 | 100 |
| Organism | Number of patients* | AMC | AMK | ATM | AZM | CAZ | CFM | CHL | CIP | COL | CRB | CRO | CTX | FEP | GEN | MEC | MEM | NAL | NET | NIT | PEF | SXT | TCY | TGC | TOB | TZP |
| Escherichia coli | 922 | 35 | 93 | 35 | 36 | 35 | 21 | 100 | 37 | 37 | 37 | 82 | 86 | 92 | 92 | 93 | 52 | 87 | 70 | 78 | ||||||
| Klebsiella pneumoniae | 489 | 36 | 59 | 38 | 36 | 35 | 26 | 100 | 37 | 36 | 38 | 52 | 62 | 58 | 57 | 29 | 44 | 71 | 35 | 48 | 47 | |||||
| Pseudomonas aeruginosa | 223 | 4 | 73 | 65 | 74 | 65 | 99 | 34 | 75 | 72 | 70 | 77 | 8 | 68 | 81 | |||||||||||
| Salmonella Typhi | 209 | 100 | 100 | 100 | 96 | 100 | 100 | 78 | 3 | 100 | 100 | 100 | 100 | 100 | 100 | 3 | 100 | 2 | 76 | 100 | 100 | |||||
| Acinetobacter sp. | 181 | 4 | 34 | 5 | 21 | 4 | 40 | 94 | 4 | 3 | 19 | 32 | 36 | 42 | 69 | 92 | 33 | 44 | ||||||||
| Enterobacter sp. | 139 | 53 | 91 | 64 | 66 | 51 | 66 | 90 | 66 | 65 | 69 | 85 | 80 | 96 | 90 | 51 | 77 | 55 | 82 | 91 | ||||||
| Proteus sp. | 53 | 74 | 82 | 79 | 79 | 74 | 28 | 2 | 76 | 76 | 83 | 67 | 98 | 85 | 32 | 50 | 75 | 94 | ||||||||
| Citrobacter freundii | 47 | 43 | 94 | 42 | 44 | 44 | 37 | 98 | 43 | 43 | 45 | 83 | 74 | 87 | 92 | 82 | 50 | 91 | 72 | 83 | ||||||
| Pseudomonas sp. | 35 | 51 | 41 | 62 | 72 | 46 | 54 | 46 | 74 | 46 | 92 | 41 | 88 | |||||||||||||
| Salmonella Paratyphi | 21 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BSH | Bangladesh Specialized Hospital |
| CAPTURA | Capturing Data on Antimicrobial Resistance Patterns and Trends in Use in Regions of Asia |
| IEDCR | Institute of Epidemiology Disease Control & Research |
| CDC | Communicable Disease Control |
| MoHFW | Ministry of Health and Family Welfare |
| QAAPT | Quick Analysis of Antimicrobial Patterns and Trends |
| CLSI | Clinical & Laboratory Standards Institute |
| VRSA | Vancomycin-resistant Staphylococcus aureus |
| MRSA | Methicillin-resistant Staphylococcus aureus |
References
- Rubin RP: A brief history of great discoveries in pharmacology: In celebration of the centennial anniversary of the founding of the American Society of Pharmacology and Experimental Therapeutics. Pharmacol Rev 2007, 59:289–359.
- Faryna A, Gilbert L, Wergowske, Kim G: Impact of therapeutic guidelines on antibiotic use by residents in primary care clinics. J Gen Intern Med 1987, 2:102–107.
- Subbalaxmi MV, Lakshmi V, Lavanya V. Antibiotic resistance--experience in a tertiary care hospital in south India. J Assoc Physicians India. 2010 Dec;58 Suppl:18-22. PMID: 21568007.
- Ehijie FO Enato and Ifeanyi E Chima. Evaluation of drug utilization patterns and patient care practices. West African Journal of Pharmacy 2011; 22(1): 36–41.
- Puca V, Marulli RZ, Grande R, Vitale I, Niro A, Molinaro G, Prezioso S, Muraro R, Di Giovanni P. Microbial Species Isolated from Infected Wounds and Antimicrobial Resistance Analysis: Data Emerging from a Three-Years Retrospective Study. Antibiotics (Basel). 2021 Sep 24;10(10):1162. [CrossRef] [PubMed] [PubMed Central]
- Lai PS, Bebell LM, Meney C, Valeri L, White MC. Epidemiology of antibiotic-resistant wound infections from six countries in Africa. BMJ Glob Health. 2018 Mar 6;2(Suppl 4):e000475. [CrossRef] [PubMed] [PubMed Central]
- Bassetti M, Di Biagio A, Rebesco B, Amalfitano ME, Topal J, Bassetti D. The effect of formulary restriction in the use of antibiotics in an Italian hospital. Eur J ClinPharmacol 2001; 57: 529-34.
- Alharbi AS. Bacteriological profile of wound swab and their antibiogram pattern in a tertiary care hospital, Saudi Arabia. Saudi Med J. 2022 Dec;43(12):1373-1382. [CrossRef] [PubMed]
- Biswas M, Roy DN, Tajmim A, Rajib SS, Hossain M, Farzana F, Yasmen N. Prescription antibiotics for outpatients in Bangladesh: a cross-sectional health survey conducted in three cities. Ann Clin Microbiol Antimicrob. 2014 Apr 22;13:15. [CrossRef] [PubMed] [PubMed Central]
- Pearson M, Chandler C. Knowing antmicrobial resistance in practice: a multi-country qualitative study with human and animal healthcare professionals. Glob Health Action. 2019;12(1):1599560. [CrossRef] [PubMed] [PubMed Central]
- Remesh A, Samna Salim AM, Gayathri UN, Retnavally KG: Antibiotics prescribing pattern in the in-patient departments of a tertiary care hospital. Pharma Pract 2013, 4:71–76.
- Minyahil A, Woldu, Sultan Suleman, Netsanet Workneh and Hafty barhane. Retrospective study of the pattern of Antibiotic Use in hawassa University Referral Hospital Pediartric ward, Southern Ethiopia. Journal of Applied Pharmaceutical Science 2013; 3(02): 93-98.
- Shadia, K., Borhan, S. B., Hasin, H., Rahman, S., Sultana, S., Barai, L., Jilani, M. A., & Haq, J. A. (2012). Trends Of Antibiotic Susceptibility Of Salmonella Enterica Serovar Typhi And Paratyphi In An Urban Hospital Of Dhaka City Over 6 Years Period. Ibrahim Medical College Journal, 5(2), 42–45. [CrossRef]
- Kot B. Antibiotic Resistance Among Uropathogenic Escherichia coli. Pol J Microbiol. 2019 Dec;68(4):403-415. Epub 2019 Dec 5. [CrossRef] [PubMed] [PubMed Central]
- Mulu W, Abera B, Yimer M, Hailu T, Ayele H, Abate D. Bacterial agents and antibiotic resistance profiles of infections from different sites that occurred among patients at Debre Markos Referral Hospital, Ethiopia: a cross-sectional study. BMC Res Notes. 2017 Jul 6;10(1):254. [CrossRef] [PubMed] [PubMed Central]
- Ahmed I, Rabbi MB, Sultana S. Antibiotic resistance in Bangladesh: A systematic review. Int J Infect Dis. 2019 Mar;80:54-61. Epub 2019 Jan 10. [CrossRef] [PubMed]
- Diekema D.J., Pfaller M.A., Shortridge D., Zervos M., Jones R.N. Twenty-Year Trends in Antimicrobial Susceptibilities Among Staphylococcus aureus from the SENTRY Antimicrobial Surveillance Program. Open Forum Infect. Dis. 2019;6:S47–S53. [PMC free article] [PubMed] [CrossRef] [Google Scholar]. [CrossRef]
- Linz MS, Mattappallil A, Finkel D, Parker D. Clinical Impact of Staphylococcus aureus Skin and Soft Tissue Infections. Antibiotics (Basel). 2023 Mar 11;12(3):557. [CrossRef] [PubMed] [PubMed Central]
- Cosgrove SE, Qi Y, Kaye KS, Harbarth S, Karchmer AW, Carmeli Y. The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges. Infect Control Hosp Epidemiol 2005;26(2):166–74.
- Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillinsusceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis 2003;36(1):53–9.
- Engemann JJ, Carmeli Y, Cosgrove SE, Fowler VG, Bronstein MZ, Trivette SL, et al. Adverse clinical and economic outcomes attributable to methicillin resistance among patients with Staphylococcus aureus surgical site infection. Clin Infect Dis 2003;36(5):592–8.
- Cetinkaya Y, Falk P, Mayhall CG. Vancomycin-resistant enterococci. Clin Microbiol Rev 2000;13(4):686–707.
- Orsi GB, Ciorba V. Vancomycin resistant enterococci healthcare associated infections. Annali di igiene: medicina preventiva e di comunita 2013;25 (6):485–92.
- Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis 2004;39 (3):309–17.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



