
Submitted:
10 March 2025
Posted:
11 March 2025
You are already at the latest version
Abstract
Background/Objectives: The timely initiation of antiretroviral therapy (ART) in persons living with HIV (PLWH) improves clinical outcomes. However, ART commencement is often delayed. Portugal, which has one of the highest new HIV diagnosis rates within the European Union, has limited available data. Evidence from 2017-2018 suggests that the average time to ART initiation exceeds the recommendations for optimal benefits. This study aimed to assess the number of days from the first hospital appointment to the commencement of ART among newly diagnosed PLWH in Portugal between 2017 and 2022 at the national level and across different hospitals within the country. Methods: A retrospective analysis of records from Portuguese public tertiary care hospitals, which manage the majority of HIV patients, was conducted. Descriptive statistics (measures of central tendency, dispersion, and frequency) were applied, along with association tests and a binary logistic regression model to examine factors influencing the timing of ART initiation. Results: A total of 2,229 cases from 19 hospitals were considered eligible. The median time interval between the first hospital appointment and ART initiation was 29.00 days, with a decreasing tendency between 2017 and 2022. Patients initiating therapy after 14 days had higher CD4 levels and lower viral loads compared to those starting within 14 days, with statistical significance. Conclusions: Continuous and regular monitoring of key indicators, such as the time to ART initiation, is pivotal for assessing the effectiveness of HIV treatment programs and pinpointing areas in need of improvement.
Keywords:
people living with HIV
; clinical care continuum
; rapid art initiation
; retrospective analysis
1. Introduction
The benefits of early antiretroviral therapy (ART) for persons living with HIV (PLWH), at the HIV diagnosis regardless of their CD4 cell count or clinical stage, are well documented in the literature [1,2,3,4,5,6,7,8,9,10,11]. These gains include improvement across a wide range of clinical outcomes, such as increased viral suppression and decreased onward HIV transmission, enhanced quality of life, and the prevention of AIDS- and non-AIDS-related morbidity and mortality. Early-start ART is especially valuable in settings where long delays are common due to extensive patient preparation before treatment initiation [2,8,12,13,14,15,16,17,18,19,20]. Same-day ART initiation is advocated by the World Health Organization (WHO) as a safe and effective strategy that can help to control the HIV epidemic [14,17,18,21,22]. Indeed, rapid ART initiation can play a crucial role in achieving the United Nations’ 95-95-95 targets for the HIV care cascade, which aim for 95% of all PLWH to be aware of their HIV status, 95% of diagnosed individuals to receive continued ART, and 95% of those on ART to achieve viral suppression [21,23].
Despite the benefits of early ART initiation, the HIV continuum of care encompasses several critical stages (i.e., awareness of symptoms, testing, diagnostic confirmation, linkage to care, clinical evaluation, and treatment initiation) each with barriers that may cumulatively delay ART initiation by weeks and significantly impact clinical outcomes [21,24]. These barriers can arise from various factors, including limited knowledge and understanding of HIV/AIDS (which can lead to engagement in risky behaviours and unawareness of the onset of concerning symptoms), stigma and discrimination that can deter individuals from seeking testing and treatment, overburdened healthcare systems, lengthy waiting times, geographic barriers, sociodemographic and economic disparities, or management of co-infections or comorbidities [25,26,27,28].
Several studies have demonstrated the potential of immediate ART initiation to shorten the time to viral suppression and improve retention in care among patients with early clinical HIV diseases [13,14,15]. Moreover, some countries have successfully implemented strategies to reduce the time from diagnosis to ART initiation, leading to significant benefits in treatment and prevention outcomes at the community level [29,30,31].
Time to ART initiation is a pivotal operational measure that can be used to assess current healthcare performance and guide quality improvement efforts focused on streamlining the way services are organized and delivered at the health facility level and the system-level [32,33,34,35]. Developing effective healthcare practice means more than reporting this measure yearly; it requires continuous monitoring at short time intervals to more accurately assess the impact of interventions and identify opportunities for improvement [35,36].
Portugal has one of the highest rates of new diagnoses of HIV infection and acquired immunodeficiency syndrome (AIDS) incidence in the European Union [37]. A national guideline issued in 2015 outlines the steps and the timeframe for the referral process after a reactive HIV test, though without a clear definition of the maximum time between linkage to hospital care and ART initiation [38]. A previous one-time evaluation of the time interval between HIV diagnosis and ART initiation in newly diagnosed patients, between 2015 and 2017 showed a mean treatment initiation delay of 76 days in 2015, decreasing to 69 and 68 days in 2016 and 2017, respectively [39].
Recognizing the critical importance of monitoring time to ART initiation, a pilot project was conducted in 2021 to set a national strategy for measuring time to ART initiation and demonstrate its relevance as a key performance indicator. The initiative covered the analysis of secondary data for the years 2017 and 2018 (the period shortly after the implementation of the national guideline of 2015), and encompassed 80% of newly diagnosed PLWH linked to care in Portuguese hospitals during that period. Findings indicated that ART commencement less than 14 days after the first hospital appointment only took place in 38.0% of the cases, while the median time until ART initiation was 21 days [40]. Although this represented the first systematic effort to start monitoring the referral process in Portugal, some reported data were incomplete or inaccurate.
Building on this foundation, a broader approach was implemented in 2022, covering a five-year timeframe (2017-2022), the entire HIV referral network for HIV infection, and assessing time to ART initiation after the COVID-19 pandemic. The relevance of this new study lies in the novel data generated, as there is a lack of regular monitoring of this type of information in the Portuguese context. Moreover, given that Portugal has a healthcare system that guarantees universal access to ART, assessing the impact of system-wide guidelines and policies on ART initiation timelines and associated delays throughout the process can provide valuable insights for settings with similar centralized healthcare infrastructures for HIV (and PLWH).
In this light, the results of the current study provide valuable lessons for healthcare policymakers and HIV care providers worldwide, especially those working in publicly funded healthcare settings aiming to improve time-sensitive interventions for HIV treatment.
Against this background, we aimed to: i) assess the time interval between the first hospital appointment and ART initiation among newly diagnosed PLWH in Portugal during the period spanning from 2017 to 2022 at the national level and across different hospitals within the country; ii) identify potential variations in the time to ART initiation across different hospitals and patient characteristics; iii) examine the trend in the time to ART initiation over time.
2. Materials and Methods
A retrospective analysis of records from Portuguese public tertiary care hospitals responsible for managing the care of most PLWH at Portugal’s mainland jurisdictional (country) level was conducted. Only cases of individuals aged 15 and older who were diagnosed with HIV with available data regarding the first hospital appointment between January 2017 and March 2022, and ART initiation occurring within twelve months of the first appointment were included. Patients for whom the date of HIV diagnosis or ART initiation could not be determined, patients who initiated treatment before the first appointment, or who had inconsistencies (which were unable to be resolved) in their reported data, were excluded.
2.1. Data Collection
The 25 major public referral hospitals for HIV treatment in mainland Portugal were invited to participate in the study (census approach). In Portugal, notifiable infectious diseases are not treated in private hospitals. After contacting the HIV department directors of each hospital by phone or email, a face-to-face meeting was held to discuss the study details for those who agreed to participate.
After confirming willingness to participate, formal authorization was obtained from the ethics committee of each hospital before data collection began. A structured data collection form was distributed by email and sent to the department directors. Data were collected by physicians from the participating hospitals and then manually checked for accuracy against the original clinical notes and records at the time of extraction and then anonymized before being sent to one designated member of the research team, by email. The anonymized data were referred to by the generic names “Centre A”, “Centre B”, etc., to avoid comparisons between centres with different structures.
2.2. Variables
The following data for each patient were manually extracted from hospital records: i) date of HIV diagnosis; ii) date of the first visit to a specialized HIV medical care centre; iii) date of ART initiation (i.e., date of ART prescription and/or collection); iv) first TCD4+ count; v) age at the time of commencement of ART; vi) country of birth; vii) sex; viii) age; and ix) source of referral (inpatient or non-governmental organization [NGO] referral).
For the time-based indicators, the time from the first appointment to the commencement of ART was calculated as the number of days between the date of the appointment to the first day of ART initiation.
The stage of HIV was categorized into three groups: A - asymptomatic, B - symptomatic, and C - late-stage HIV, adapting WHO’s clinical staging of HIV disease [27] and the classification adopted by the Directorate-General of Health [41], excluding the first stage of acute infection. The type of virus was classified into three groups: cases of HIV-1 infection, cases of HIV-2 infection and cases of HIV-1 and HIV-2 co-infection [42,43].
2.3. Data Analysis
Data cleaning procedures were implemented to eliminate inconsistencies or errors, including elimination of duplicates, missing and impossible values, entries not meeting the inclusion criteria (e.g., first hospital appointment before 2017 or after 2022, cases with ART initiation on the same day of or before the first appointment, or after six months) and entries with a previous HIV diagnosis. In addition, potentially identifiable variables were recoded using unique identification codes, and the same nomenclature was used for the same information to ensure consistency.
Data analysis was performed using SPSS Statistics for Windows, version 26.0. Descriptive statistics were used to summarize the data. For continuous variables, measures of central tendency (medians, and percentiles 25 and 75) and dispersion (standard deviation or interquartile range) were used. For categorical variables, the absolute number of individuals per category and respective percentages were determined. To assess associations between categorical variables, Pearson’s Chi-Square test was employed. When expected frequencies in contingency tables were below 5, the Fisher-Freeman-Halton Exact Test was applied. For comparisons of non-normally distributed continuous variables (viral load and CD4 count) across two groups (time to ART initiation: ≤14 days vs. >14 days [12]), the Mann-Whitney U test was used. Normality of the continuous variables was evaluated using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Finally, a binary logistic regression model was constructed to examine the relationship between time to ART initiation and disease stage, with odds ratios calculated to quantify the likelihood of delayed initiation. Multicollinearity was assessed to ensure model reliability. the significance level was set to 5%.
2.4. Ethical Considerations
The study was approved by the Ethics Committees of all participating hospitals.
3. Results
From the 3,434 cases received from the 19 participating hospitals, a total of 2,229 (64.9%) were considered eligible. The total number of received and eliminated cases, by stage of data cleaning is presented in Figure 1.
Overall, the median time interval between the first hospital appointment and ART initiation was 29.00 days (mean 39.00 days), with a range of 1 to 182 days (Table 1). A decreasing tendency in the median time until ART initiation over the years, with the lowest median time observed in 2022 (18 days) and the highest in 2017 (35 days). More than two thirds of the patients (77.0%) initiated ART more than 14 after the first appointment.
A statistically significant association between HIV stage and the time interval between the first consultation and the initiation of therapy was found, showing that the distribution of time intervals varies according to disease stages. Patients who started therapy 14 days after the first appointment tend to have higher CD4 levels compared to those who started earlier. A statistically significant difference in viral load distributions between the two groups was also found, as viral loads tend to be higher in the group that started therapy within 14 days compared to the group that started after 14 days (Table 2).
4. Discussion
The present study provides valuable insights into the time from first appointment to ART initiation among newly diagnosed PLWH in Portugal, spanning from 2017 to 2022. Overall, the median time to ART initiation was 29.00 days (almost four weeks), with a downward trend over the years, from 35 days in 2017 to 18 days in the beginning of 2022. This suggests an improvement in the timeliness of ART initiation over the past five-six years.
Moreover, in our study, patients with early ART initiation (14 days or less) after the first appointment had a lower viral load and a higher TCD4+ cell count, showing improved immune function and a reduced risk of HIV-related complications and transmission to others. This is particularly relevant as early start of ART for PLWH has already demonstrated well-established clinical benefits, including reduced risk of death, AIDS-related illnesses, serious non-AIDS illnesses, and sexual transmission of HIV due to behaviour modification, even though further research is necessary to determine the optimal timing of ART initiation [5,6,10,11,44,45]. While this study does not delve into the specific reasons, potential barriers to timely ART initiation may include inconsistencies in referral processes and protocols, unmet needs of specific populations, and psychosocial factors such as long wait times, inflexible appointment schedules, stigma, and an overburdened healthcare system facing high demand and limited response capacity due to healthcare worker shortages as doctors increasingly transition to private practice.
According to the European Centre for Disease Prevention and Control’s (ECDC) 2022 report, in most analysed countries in the European Union / European Economic Area, in 78% of the cases it took only four days after the HIV diagnosis until linkage to care, a number that increased to 98% for a linkage to care inferior to three months [46]. According to the ECDC’s report on HIV treatment and care, data from 2020 show that Portugal falls below (by less than 10%) the global 90-90-90 target in terms of the proportion of PLWH receiving ART [47].
Our study included a sample of new HIV diagnosis that represents 35.5% of Portuguese cases between 2017-2022. However, national statistics entail all diagnosed individuals (either in Portugal or not) and not only those newly diagnosed, which makes us believe that our samples can be largely representative of the Portuguese scenario. This was possible due to the inclusion of a large number of hospitals responsible for managing the care of most PLWH.
The period under analysis in this study reveals a decreasing trend in the median time between initial hospital appointments and ART initiation, which was not altered after 2020, with the onset of the COVID-19 pandemic. Other authors have confirmed this finding, as the pandemic imposed several structural changes in healthcare services that prioritized acute clinical situations like newly diagnosed PLWH [23,48]. The COVID-19 pandemic was also accompanied by a concerning decline in the absolute number of newly diagnosed HIV cases in 2020 and 2021 (the year 2022 was not representative since this study only included the first three months). As reported by the ECDC, the pandemic’s disruption had a significant impact on HIV testing and reporting [46,49].
The observed heterogeneity in practices across the assessed centres underscores the need to examine and study existing practices to identify the causes of variability, particularly at a national level. While local sociological factors may contribute, it is essential to investigate the organizational factors at the institutional level that drive these disparities. The National Program for HIV/AIDS Infection could play a valuable role in leading efforts to understand these differences and implement targeted improvements.
Overall, the findings of this study highlight the progress that has been made in Portugal in enhancing the timeliness of ART initiation among newly diagnosed PLWH. These results have significant implications for the development of national and regional strategies aimed at improving the timeliness of ART initiation among newly diagnosed PLWH in Portugal. These strategies should focus on reducing variability in ART initiation timelines across different hospitals and enhancing access to ART for underserved populations, such as younger patients and those referred from NGOs. Additionally, the findings of this study suggest that the national guideline for the referral process for newly diagnosed HIV patients should be updated to include a clear definition of the maximum time between linkage to hospital care and ART initiation. This would aid in ensuring that all PLWH have access to ART as soon as possible following their diagnosis.
Although this is the first attempt to longitudinally monitor the time until ART start in Portugal, the study is limited by the retrospective nature of data collection. This means that some data may be missing or inaccurate. Moreover, data was gathered from hospital records, therefore only covering the time after the first hospital appointment and until ART initiation, excluding data from the time of HIV diagnosis, in cases where the diagnosis was established before hospital appointment, re-scheduling of first appointments, and not assessing treatment adherence. Another limitation lies in the fact that the study only included patients who were diagnosed with HIV and initiated ART. Finally, out of the 25 hospitals invited to participate in this study, only 19 provided the necessary data. This limited participation may have hindered the ability to gather a more accurate picture of ART initiation for PLWH in Portugal. Despite the efforts from the research team, several barriers have contributed to this, namely difficulties in obtaining responses from hospital management boards, lack of cooperation from designated contact points for submitting the study to ethical committees, and instances where hospitals simply did not provide feedback after receiving the data request. Therefore, generalization of these findings to other populations should be approached with caution.
5. Conclusions
This study provides important information about the time from linkage to care to ART initiation in Portugal. The findings suggest that the time from hospital appointment to ART initiation is decreasing. However, there is still room for improvement, as advocated by the WHO. Continuous and regular monitoring and improvement of key indicators, such as the time to ART initiation, at short-time intervals, is pivotal for assessing the effectiveness of HIV treatment programs and pinpointing areas in need of improvement. This ongoing surveillance enables tracking progress, identifying potential bottlenecks in the care cascade, and implementing specific interventions to expedite ART commencement and optimize patient outcomes. Through consistent monitoring of these metrics, healthcare systems can ensure timely and effective treatment for PLWH, thereby reducing the risk of disease advancement and transmission.
Author Contributions
Conceptualization: FA, RC and VN; Data collection: AP, FM, JPC, JL, MA, IC, TT, IC, CS, AM, RP, AR, PS, IG, RCA, IP, AA, FR, PP, RD, GC, CP, NM, AR, JR, JF, MR, FF, DR, LP, CT, AAP, VA and RS; Formal analysis: CF, VN, RC and FA; Funding acquisition: FA and RC; Methodology: FA, RC and VN; Writing-original draft preparation: AV; Writing-review and editing: FA, AV, VN, CF, RC, AP, FM, JPC, JL, MA, IC, TT, IC, CS, AM, RP, AR, PS, IG, RCA, IP,AA, FR, PP, RD, GC, CP, NM, AR, JR, JF, MR, FF, DR, LP, CT, AAP, VA and RS; Supervision: FA, RC and VN. All authors have read and agreed to the published version of the manuscript.
Funding
This research received an external funding from Gilead Sciences Lda.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethics approvals were obtained from the following Ethics Committees: i) Unidade Local de Saúde de Matosinhos - Hospital de Pedro Hispano, ii) Centro Hospitalar de Vila Nova de Gaia/Espinho, iii) Centro Hospitalar Universitário de São João, iv) Centro Hospitalar Universitário do Porto, v) Centro Hospitalar do Tâmega e Sousa, vi) Centro Hospitalar do Baixo Vouga, vii) Hospital Distrital de Santarém, viii) Hospital de Vila Franca de Xira, ix) Centro Hospitalar Barreiro Montijo, x) Centro Hospitalar de Setúbal, xi) Hospital Garcia de Orta, xii) Centro Hospitalar Universitário Lisboa Norte - Hospital de Santa Maria, xiii) Centro Hospitalar Universitário de Lisboa Central - Hospital de São José, xiv) Centro Hospitalar Universitário de Lisboa Central - Hospital de Santo António dos Capuchos, xv) Centro Hospitalar Universitário de Lisboa Central - Hospital de Curry Cabral, xvi) Hospital Doutor Fernando da Fonseca, xvii) Unidade Local de Saúde do Baixo Alentejo, xviii) Centro Hospitalar Universitário do Algarve - Hospital de Faro, xix) Centro Hospitalar Universitário do Algarve - Hospital de Portimão.
Informed Consent Statement
Due to the retrospective and non-pharmacological nature of this study, in Portugal ethical clearance is not needed. The Ethics Committees waived informed consent as, according to Article 14(5)(b) of the General Data Protection Regulation, informed consent is not mandatory when obtaining consent is impossible, informing all subjects would be disproportionately effortful, or obtaining consent would pose objective difficulties that would impede the study. Additionally, the research serves a public interest and is retrospective in nature. This decision was expressed in the approval documents of each Ethics Committees. In addition, the general authorization for the use of anonymized demographical and clinical data was used.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank to Isabel Neves, Ludgero Vasconcelos, Rita Ferraz, José Vera, José Poças, Eugénio Teófilo, Patrícia Pacheco, Telo Faria, José Ferreira, Domitila Faria and Filomena Esteves for the administrative support, to Joana Pereira, João Barroso and João Ferreira de Sousa for data collection, to Helena Cortes Martins for providing data DGS / INSA 2017-2022, and to Ana Sequeira and Hugo Caldeira for technical assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hammer, S.M.; Squires, K.E.; Hughes, M.D.; Grimes, J.M.; Demeter, L.M.; Currier, J.S.; Eron, J.J.J.; Feinberg, J.E.; Balfour, H.H.J.; Deyton, L.R.; et al. A Controlled Trial of Two Nucleoside Analogues plus Indinavir in Persons with Human Immunodeficiency Virus Infection and CD4 Cell Counts of 200 per Cubic Millimeter or Less. New Engl. J. Med. 1997, 337, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Palella, F.J., Jr.; Delaney, K.M.; Moorman, A.C.; Loveless, M.O.; Fuhrer, J.; Satten, G.A.; Aschman, D.J.; Holmberg, S.D.; the HIV Outpatient Study Investigators. Declining Morbidity and Mortality among Patients with Advanced Human Immunodeficiency Virus Infection. N. Engl. J. Med. 1998, 338, 853–860. [Google Scholar] [CrossRef]
- Mateo-Urdiales A, Johnson S, Smith R, Nachega JB, Eshun-Wilson I. Rapid initiation of antiretroviral therapy for people living with HIV. Cochrane Database Syst Rev [Internet]. 2019 [cited 2024 Oct 12];2019. Available from: /pmc/articles/PMC6575156/.
- Kitahata, M.M.; Gange, S.J.; Abraham, A.G.; Merriman, B.; Justice, A.C.; Hogg, R.S.; Deeks, S.G.; Eron, J.J.; Brooks, J.T.; Rourke, S.B.; et al. Effect of Early versus Deferred Antiretroviral Therapy for HIV on Survival. New Engl. J. Med. 2009, 360, 1815–1826. [Google Scholar] [CrossRef]
- Andrade, H.B.; Shinotsuka, C.R.; da Silva, I.R.F.; Donini, C.S.; Li, H.Y.; de Carvalho, F.B.; Brasil, P.E.A.A.D.; Bozza, F.A.; Japiassu, A.M. Highly active antiretroviral therapy for critically ill HIV patients: A systematic review and meta-analysis. PLOS ONE 2017, 12, e0186968. [Google Scholar] [CrossRef]
- Lundgren JD, Babiker AG, Gordin F, Emery S, Grund B, Sharma S, et al. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. 2015;373:795–807.
- Temprano ANRS 12136 Study Group. A trial of early antiretrovirals and isoniazid preventive therapy in Africa. N Engl J Med. 2015;373:808–22.
- Samji, H.; Cescon, A.; Hogg, R.S.; Modur, S.P.; Althoff, K.N.; Buchacz, K.; Burchell, A.N.; Cohen, M.; Gebo, K.A.; Gill, M.J.; et al. Closing the Gap: Increases in Life Expectancy among Treated HIV-Positive Individuals in the United States and Canada. PLOS ONE 2013, 8, e81355. [Google Scholar] [CrossRef]
- Lohse, N.; Obel, N. Update of Survival for Persons With HIV Infection in Denmark. Ann. Intern. Med. 2016, 165, 749–750. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Verma, A.; Kashyap, M.; Gautam, P. ART in Prevention of Mother-to-Child Transmission of HIV. J. Obstet. Gynecol. India 2020, 70, 18–22. [Google Scholar] [CrossRef]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H.; et al. Prevention of HIV-1 Infection with Early Antiretroviral Therapy. N. Engl. J. Med. 2011, 365, 493–505. [Google Scholar] [CrossRef]
- Zolopa, A.R.; Andersen, J.; Komarow, L.; Sanne, I.; Sanchez, A.; Hogg, E.; Suckow, C.; Powderly, W. Early Antiretroviral Therapy Reduces AIDS Progression/Death in Individuals with Acute Opportunistic Infections: A Multicenter Randomized Strategy Trial. PLOS ONE 2009, 4, e5575. [Google Scholar] [CrossRef]
- Koenig, S.P.; Dorvil, N.; Dévieux, J.G.; Hedt-Gauthier, B.L.; Riviere, C.; Faustin, M.; Lavoile, K.; Perodin, C.; Apollon, A.; Duverger, L.; et al. Same-day HIV testing with initiation of antiretroviral therapy versus standard care for persons living with HIV: A randomized unblinded trial. PLOS Med. 2017, 14, e1002357–e1002357. [Google Scholar] [CrossRef]
- Pilcher, C.D.; Ospina-Norvell, C.F.-P.; Dasgupta, A.B.; Jones, D.; Hartogensis, W.; Torres, S.M.; Calderon, F.M.; Demicco, E.; Geng, E.; Gandhi, M.; et al. The Effect of Same-Day Observed Initiation of Antiretroviral Therapy on HIV Viral Load and Treatment Outcomes in a US Public Health Setting. Am. J. Ther. 2017, 74, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Mendez-Lopez, A.; McKee, M.; Stuckler, D.; Granich, R.; Gupta, S.; Noori, T.; Semenza, J. Population uptake and effectiveness of test-and-treat antiretroviral therapy guidelines for preventing the global spread of HIV: an ecological cross-national analysis. HIV Med. 2019, 20, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Ford, N.; Migone, C.; Calmy, A.; Kerschberger, B.; Kanters, S.; Nsanzimana, S.; Mills, E.J.; Meintjes, G.; Vitoria, M.; Doherty, M.; et al. Benefits and risks of rapid initiation of antiretroviral therapy. AIDS 2018, 32, 17–23. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy. Geneva; 2017.
- Ford, N.; Vitoria, M.; Doherty, M. Providing antiretroviral therapy to all who are HIV positive: the clinical, public health and programmatic benefits of Treat All. J. Int. AIDS Soc. 2018, 21, e25078. [Google Scholar] [CrossRef] [PubMed]
- Njuguna, I.N.; Cranmer, L.M.; O Otieno, V.; Mugo, C.; Okinyi, H.M.; Benki-Nugent, S.; Richardson, B.; Stern, J.; Maleche-Obimbo, E.; Wamalwa, D.C.; et al. Urgent versus post-stabilisation antiretroviral treatment in hospitalised HIV-infected children in Kenya (PUSH): a randomised controlled trial. Lancet HIV 2018, 5, e12–e22. [Google Scholar] [CrossRef]
- Grant PM, Zolopa AR. When to start ART in the setting of acute AIDS-related opportunistic infections: The time is now! Curr HIV/AIDS Rep. 2012;9:251–8.
- Boyd, M.; Boffito, M.; Castagna, A.; Estrada, V. Rapid initiation of antiretroviral therapy at HIV diagnosis: definition, process, knowledge gaps. HIV Med. 2019, 20, 3–11. [Google Scholar] [CrossRef]
- Bogdanić, N.; Bendig, L.; Lukas, D.; Zekan, Š.; Begovac, J. Timeliness of antiretroviral therapy initiation in the era before universal treatment. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Joint United Nations Programme on HIV/AIDS. Prevailing against pandemics by putting people at the centre: World AIDS Day report 2020 [Internet]. 2020. Available from: https://aidstargets2025.unaids.org/assets/images/prevailing-against-pandemics_en.
- Gardner, E.M.; McLees, M.P.; Steiner, J.F.; del Rio, C.; Burman, W.J. The Spectrum of Engagement in HIV Care and its Relevance to Test-and-Treat Strategies for Prevention of HIV Infection. Clin. Infect. Dis. 2011, 52, 793–800. [Google Scholar] [CrossRef]
- Genberg, B.L.; Lee, Y.; Rogers, W.H.; Wilson, I.B. Four Types of Barriers to Adherence of Antiretroviral Therapy are Associated with Decreased Adherence Over Time. AIDS Behav. 2015, 19, 85–92. [Google Scholar] [CrossRef]
- Croome, N.; Ahluwalia, M.; Hughes, L.D.; Abas, M. Patient-reported barriers and facilitators to antiretroviral adherence in sub-Saharan Africa. AIDS 2017, 31, 995–1007. [Google Scholar] [CrossRef]
- Moges, N.A.; Adesina, O.A.; A Okunlola, M.; Berhane, Y. Barriers and Facilitators of Same-Day Antiretroviral Therapy Initiation Among People Newly Diagnosed with HIV in Ethiopia: Qualitative Study Using the Transtheoretical Model of Behavioral Change. J. Multidiscip. Heal. 2020, 13, 1801–1815. [Google Scholar] [CrossRef]
- Patel, R.C.; Odoyo, J.; Anand, K.; Stanford-Moore, G.; Wakhungu, I.; Bukusi, E.A.; Baeten, J.M.; Brown, J.M. Facilitators and Barriers of Antiretroviral Therapy Initiation among HIV Discordant Couples in Kenya: Qualitative Insights from a Pre-Exposure Prophylaxis Implementation Study. PLOS ONE 2016, 11, e0168057. [Google Scholar] [CrossRef]
- Esber, A.L.; Coakley, P.; A Ake, J.; Bahemana, E.; Adamu, Y.; Kiweewa, F.; Maswai, J.; Owuoth, J.; Robb, M.L.; Polyak, C.S.; et al. Decreasing time to antiretroviral therapy initiation after HIV diagnosis in a clinic-based observational cohort study in four African countries. J. Int. AIDS Soc. 2020, 23, e25446. [Google Scholar] [CrossRef] [PubMed]
- Medland, N.A.; Chow, E.P.F.; McMahon, J.H.; Elliott, J.H.; Hoy, J.F.; Fairley, C.K. Time from HIV diagnosis to commencement of antiretroviral therapy as an indicator to supplement the HIV cascade: Dramatic fall from 2011 to 2015. PLoS ONE 2017, 12, e0177634. [Google Scholar]
- Lockman, S.; Holme, M.P.; Makhema, J.; Bachanas, P.; Moore, J.; Wirth, K.E.; Lebelonyane, R.; Essex, M. Implementation of Universal HIV Testing and Treatment to Reduce HIV Incidence in Botswana: the Ya Tsie Study. Curr. HIV/AIDS Rep. 2020, 17, 478–486. [Google Scholar] [CrossRef]
- Chen, Q.; Liu, J.; Fu, X.; Yang, F.; Liu, Q.; Li, J.; Tan, Z.; Li, J.; Lin, K.; Yan, Y.; et al. Effect of Late Testing and Antiretroviral Treatment on Mortality Among People Living With HIV in the Era of Treat-All in Guangdong Province, China, 1992–2018: A Cohort Study. Front. Public Heal. 2022, 10, 851117. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Xiao, X.; Zhang, C.; Xie, Y.; Wang, H. Prevalence of delayed antiretroviral therapy initiation among people living with HIV: A systematic review and meta-analysis. PLOS ONE 2023, 18, e0286476. [Google Scholar] [CrossRef]
- Alejos B, Díez C, Galindo MJ, Lopez JC, Hernando V, Ayerdi O, et al. Linkage to care and time to viral suppression in PWH in Spain: 2004-2020. Top Antivir Med. 2022;30:358–358.
- Hill, J.E.; Stephani, A.-M.; Sapple, P.; Clegg, A.J. The effectiveness of continuous quality improvement for developing professional practice and improving health care outcomes: a systematic review. Implement. Sci. 2020, 15, 1–14. [Google Scholar] [CrossRef]
- Powers KA, Miller WC. Building on the HIV cascade: a complementary “HIV States and Transitions” framework for describing HIV diagnosis, care, and treatment at the population level. J Acquir Immune Defic Syndr. 2015;69:341–7.
- Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90: An ambitious treatment target to help end the AIDS epidemic. 2014.
- Ministério da Saúde. Diário da República n.o 228/2015, 1o Suplemento, Série II de 2015-11-20, Despacho n.o 13447-C/2015. Portugal; 2015.
- Ministério da Saúde. Direção-Geral da Saúde. Infeção VIH e SIDA: Desafios e Estratégias. Lisboa; 2018.
- Nicolau, V.; Cortes, R.; Lopes, M.; Virgolino, A.; Santos, O.; Martins, A.; Faria, N.; Reis, A.P.; Santos, C.; Maltez, F.; et al. HIV Infection: Time from Diagnosis to Initiation of Antiretroviral Therapy in Portugal, a Multicentric Study. Healthcare 2021, 9, 797. [Google Scholar] [CrossRef]
- Ministério da Saúde., Direção-Geral da Saúde, Instituto Nacional de Saúde Doutor Ricardo Jorge. Infeção VIH e SIDA em Portugal – 2022. 2022.
- Robertson, D.L.; Hahn, B.H.; Sharp, P.M. Recombination in AIDS viruses. J. Mol. Evol. 1995, 40, 249–259. [Google Scholar] [CrossRef]
- Sharp, P.M.; Hahn, B.H. Origins of HIV and the AIDS Pandemic. Cold Spring Harb. Perspect. Med. 2011, 1, a006841–a006841. [Google Scholar] [CrossRef] [PubMed]
- Grinsztejn, B.; Hosseinipour, M.C.; Ribaudo, H.J.; Swindells, S.; Eron, J.; Chen, Y.Q.; Wang, L.; Ou, S.-S.; Anderson, M.; McCauley, M.; et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect. Dis. 2014, 14, 281–290. [Google Scholar] [CrossRef] [PubMed]
- A Levy, J. Caution: should we be treating HIV infection early? Lancet 1998, 352, 982–983. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. HIV/AIDS surveillance in Europe 2022 - 2021 data [Internet]. 2022. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/2022-Annual_HIV_Report_final.pdf.
- European Centre for Disease Prevention and Control. ECDC Special report: Continuum of HIV care - Monitoring implementation of the Dublin Declaration on Partnership to fight HIV/AIDS in Europe and Central Asia: 2021 progress report [Internet]. 2021. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/Dublin-Continuum-of-HIV-care-2021-progress-report-final-with-covers-updated.pdf.
- Ben Farhat, J.; Hessamfar, M.; Farbos, S.; Desclaux, A.; Dumondin, G.; Ferrand, H.; Greib, C.; Castan, B.; Rispal, P.; Duffau, P.; et al. Time to Treatment Initiation and HIV Viral Suppression in People Diagnosed With HIV-1 During COVID-19 Pandemic in Ex-Aquitaine, France (ANRS CO3 AQUIVIH-NA Cohort-QuAliCOV Study). Am. J. Ther. 2024, 95, 1–5. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. World AIDS Day 2022: WHO/Europe and ECDC report reveals increasing numbers living with undiagnosed HIV in the Region [Internet]. 2022. Available from: https://www.ecdc.europa.eu/en/news-events/hiv-increasing-numbers-living-undiagnosed.
Figure 1.
Study flowchart with included and excluded cases of persons living with HIV.
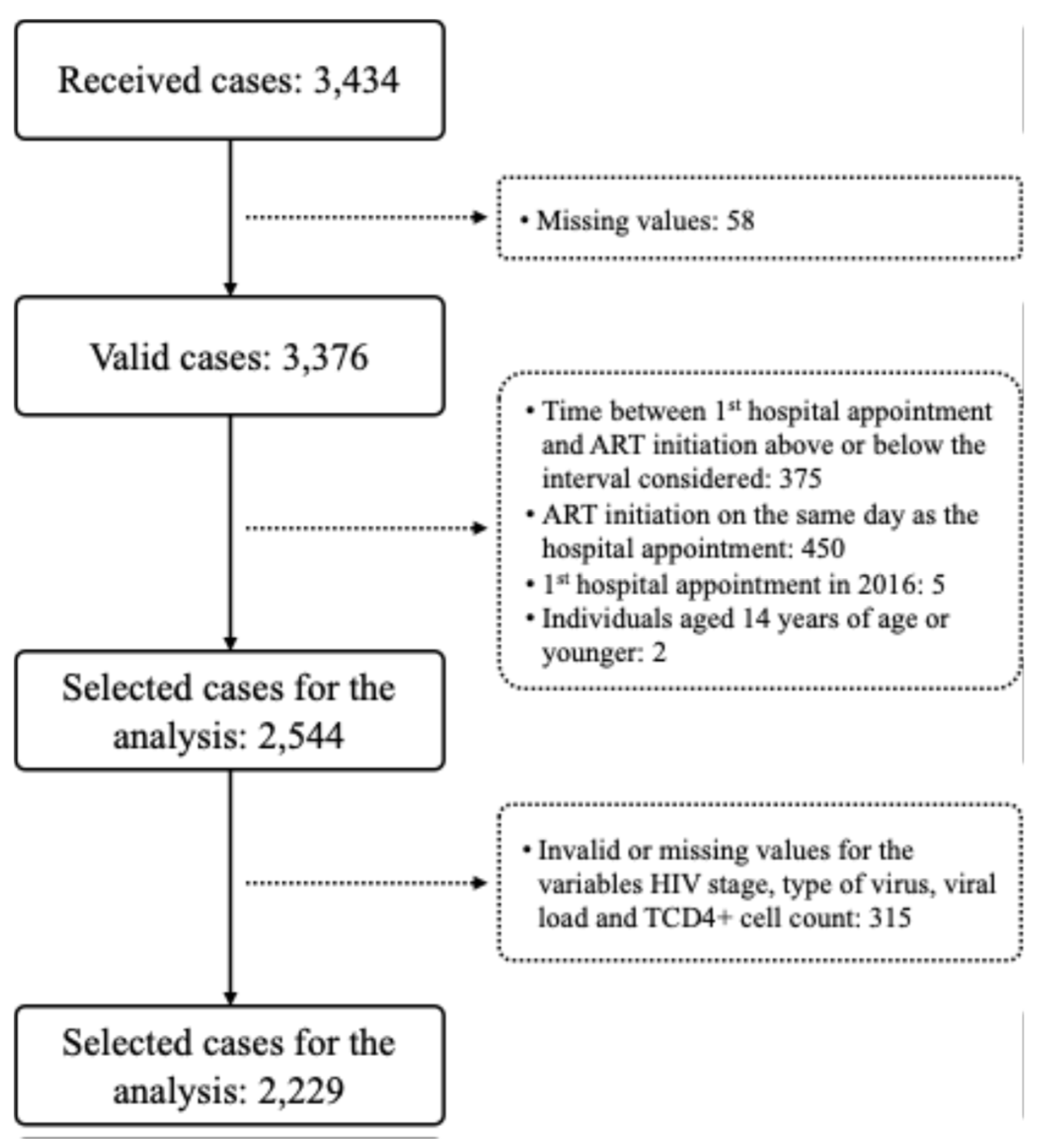

Table 1.
Time (days) until ART initiation, over the years (n=2,229).
| Year of the first appointment | N | Median (IQR) | Mean (standard deviation) | Range (minimum-maximum) |
|---|---|---|---|---|
| 2017 | 493 | 36.00 (33.00) | 48.74 (48.15) | 1-364 |
| 2018 | 497 | 30.00 (23.00) | 39.54 (36.59) | 1-309 |
| 2019 | 428 | 29.00 (30.50) | 39.73 (42.07) | 1-355 |
| 2020 | 348 | 21.00 (28.00) | 36.62 (46.83) | 1-351 |
| 2021 | 353 | 22.00 (23.00) | 31.99 (39.08) | 1-351 |
| 2022 | 110 | 21.00 (22.00) | 26.15 (27.73) | 1-222 |
| Total | 2,229 | 29.00 (30.00) | 39.30 (42.52) | 1-354 |
Note: IQR, interquartile range.
Table 2.
Clinical characteristics of patients on ART, between 2017 and 2022 (n=2,229).
| Total N |
≤14 days n (%) |
>14 days n (%) |
p-value | |
|---|---|---|---|---|
| HIV stage | ||||
| A | 1512 | 1196 (79.1%) | 316 (20.9%) | |
| B | 458 | 354 (77.3%) | 104 (22.7%) | <.001 |
| C | 259 | 155 (59.8%) | 104 (40.2%) | |
| Type of virus | ||||
| HIV1 | 2190 | 1676 (76.5%) | 514 (23.5%) | |
| HIV2 | 3 | 27 (75.0%) | 1 (33.3%) | .902 |
| HIV1 and 2 | 36 | 2 (66.7%) | 9 (25.0%) | |
| Viral load | ||||
| Mean (SD) | 756,175 (4,409,505) | 637,216 (4232190) | 1,1432,246 (4,927,177) | |
| Median (IQR) | 83,100 (319,702) | 70,718 (245,472) | 138,000 (570,850) | <.001 |
| Minimum-maximum | 0-101,000,000 | 0-101,000,000 | 37-100,000,000 | |
| TCD4+ cell count Mean (SD) Median (IQR) Minimum-maximum |
377.52 (331.06) 338.00 (353) 1-9210 |
392.74 (349.28) 353.23 (345) 2-9210 |
328.01 (257.29) 292.50 (367) 1-1362 |
<.001 |
Note: ER, emergency room; HIV, human immunodeficiency virus; IQR, interquartile range; NA, not available; NGO, non-governmental organization; SD, standard deviation. In bold, statistically significant values.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



