
Submitted:
08 March 2025
Posted:
11 March 2025
You are already at the latest version
Abstract
Applying digital health interventions (DHIs) in primary health care (PHC) is a possible strategy for achieving universal health coverage (UHC). Australia’s implementation of DHIs in PHC has shown both successes and challenges across diverse populations. This scoping review synthesised evidence from 60 studies, focusing on digital health interventions, PHC, successful care measurement, and the Australian context. Findings indicated that DHIs improved healthcare accessibility and efficiency but still face challenges in ensuring quality care, particularly for Culturally and Linguistically Diverse (CALD) and First Nations populations due to language barriers and regional digital gaps. Ineffective governance, limited resources, and increased workloads further hinder DHI implementation. While DHIs presented high-quality outcomes for the general population and some CALD groups, affordability remains a barrier for others. Tailored or co-designed DHIs for minority populations show more tremendous community engagement success compared to general interventions. To conclude, DHIs for PHC in Australia enhance healthcare delivery but require addressing inequities in access, governance, and resource allocation to ensure inclusive progress toward UHC. Policymakers and healthcare managers must prioritise these gaps to create more equitable healthcare systems.
Keywords:
Digital Health
; Primary Health Care
; Universal Health Coverage
; Australia
1. Introduction
Universal Health Coverage (UHC) refers to providing every person who needs health services with high-quality care without financial hardship [1]. As the World Health Organisation (WHO) concluded, Primary health care (PHC) is the most effective and cost-efficient method to achieve UHC [2]. The declaration of Alma-Ata in 1978 defined PHC as essential health care (usually at a fundamental level), which is universally accessible to the community with full community participation and affordable price [3].
Digital health uses information communication technologies (ICT) to assist health and health-related fields [4]. Digital health interventions can support clients, health service providers, and health systems or resource managers; they can also support a wide range of activities related to health data [5]. WHO highlighted the importance of digital health because it may help more significant numbers of people access some health services that were previously unavailable or unaffordable to them [6], which matches the Idea of UHC and PHC that provides affordable health services and increases accessibility [3]. Current evidence partially supports the idea of WHO that digital health can offer high-gain opportunities in specific segments; for instance, eHealth applications can increase the efficiency of general practitioners (GPs) by reducing the need for physical consultations and increasing the level of satisfaction of patients through 24/7 applicability as well as more straightforward and easier access [7]. Because related electronic devices have become more common at the health system level, primary health care assisted by digital techniques can cover more people, which was significant progress in PHC and UHC [8]. However, some researchers questioned the effectiveness and accuracy of current evidence [7,8]. This is because the nature of health systems across various countries and the building blocks of systems (such as health care delivery and health financing) are different; the generalisability of evidence would be limited [7,8,9,10]. Therefore, developing country-specific knowledge would be necessary to assess the success and challenges of digital health interventions in PHC. Furthermore, due to the inequity and inequality across populations under one health system [8,10], identifying a specific disadvantaged population for research would be meaningful. Health systems usually have poor consideration of linguistic and cultural diversity worldwide, and this problem is critical in digital health interventions to achieve UHC [8], so research on the population affected by this problem would be necessary.
Australia has applied efforts to build a PHC network to achieve UHC and has achieved some success. By 2021, 38.4% of health expenditure in Australia will be allocated to primary health care [11]. A Medicare system funded by the state or federal government was built to provide free or affordable health services and then reduce the out-of-pocket health expenditure of patients (Although some marginal groups still reported the price is unaffordable); most informants of this research presented strong satisfactory towards current Medicare system in Australia [12,13]. Privately operated GPs, which are Medicare-funded, deliver most of PHC services; some population groups or functions that were not covered by GPs would be supplemented by targeted public funding for services, which increased the range of coverage of PHC [13]. However, some challenges still exist, such as some patients, including First Nations peoples, face inequity when they need to access services like dental care and face non-communicable diseases [13]. Other challenges of PHC in Australia include poor leadership infrastructure, lack of training and clear job descriptions for health workers, community trust towards health services, and weak client engagement [12]. Overall, although some challenges are persistently hindering for the delivery of PHC services in Australia.
However, compared to the general population, priority populations, including people from Culturally and Linguistically Diverse (CALD) and First Nations backgrounds, the situation may be worse due to health inequity [14,15,16]. This is because economic issues such as poverty [17] or complex historical, geographic and socio-cultural factors, including colonisation and racism [18] faced by First Nations peoples, are systematically generating barriers to this population to obtain quality primary care. CALD people face similar circumstances, such as unequal distribution of power and resources, preventing them from equally accessing quality primary care [19]. Currently, the role of applying digital health in primary care is uncertain; the implementation of digital health can help disadvantaged population groups access quality health care [20] or reinforce the existing health inequity [8,21], and as we know, if DHIs have unique effects on the successes or challenges across among priority populations (First Nations and CALD populations) in Australia is still unclear.
To provide a deeper understanding of the role of DHIs in primary care and inform healthcare managers to address health inequities, this scoping review will examine the successes and challenges of digital health interventions in improving access to primary health care across different populations in Australia.
2. Materials and Methods
2.1. Searching strategies
We conducted a search on four online databases: PubMed, Web of Science, Embase, Google Scholar, and one grey literature source, Australian Telehealth Society, to find research studies or articles related to the implementation of DHIs in the PHC area, the search terms were organised around three main themes: Digital health interventions, Primary health care, measurement of successful care, Australia background. Only database articles published in the last ten years (from 2014 to 2024) would be selected to ensure the timeliness of selected studies. There is no published time limit on grey literature. Boolean operators, truncations, and search terms were tailored to each database. Refer to the table in supplementary file S1 for details of searching strategies.
2.2. Study Selection
Selected papers would be imported into EndNote 20, and then duplicates would be removed. Afterwards, the titles and abstracts would be screened. Articles irrelevant to this study topic or have insufficient information in the title and/or abstract would be excluded. The quality of selected articles would be examined based on the Mixed Methods Appraisal Tool [22]. After the data screening, the final list will be checked and discussed. If there are no more disagreements, reviewers will conduct a full-text review independently. We obtained 1451 search results from PubMed, 916 results from Web of Science, 910 results from Embase, 17900 results from Google Scholar, and 45 from the Australian Telehealth Society [Figure 1 for a detailed search and screening process].
2.3. Data extraction and analysis
One reviewer extracted data based on study characteristics (author, year of publication, jurisdictions (states and territories), research focus duration of the study, study type/design, study participants (Which group of CALD people), sample size, The digital health interventions used, key findings and conclusions in the study). After the extraction, reviewers would recheck to ensure the content was accurate and complete. A thematic analysis was applied to gather articles presenting similar patterns around one theme and then identify successes and challenges of digital health interventions in improving access to primary health care among priority populations in Australia.
The health system building blocks, including Health Services Delivery, Health workforce, Health Governance and stewardship, and Health Information system, which the World Health Organisation concluded, were used as themes to help organise our findings [23]. In addition, community engagement, as an essential indicator of primary health, would also be selected as another significant theme [3].
The structure of this scoping review would follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist [24].
3. Results
3.1. Characteristics of included studies.
After excluding duplicate publications or articles with relatively low relevance to the current topic, 60 articles were selected. Of the chosen articles, 3 were cohort studies [25,26,27], 1 was a commentary article [28], 10 were critical, systematic or scoping reviews [29,30,31,32,33,34,35,36,37,38], 5 were cross-sectional studies [39,40,41,42,43], 5 were feasibility or pilot studies [44,45,46,47,48], 2 were government or organisation reports [49,50], 4 studies applied mixed-methods [51,52,53,54], 1 was randomised-controlled trails [55], 5 were studies applied other quantitative methods [56,57,58,59,60], 22 were qualitative studies [61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82], 2 studies have not specified their methodology or used different methods [83,84]. Refer to Supplementary Material 1 for detailed characteristics of selected studies and Table 1 for the overview of findings.
3.2. Critical characteristics of studies, success, and challenges of using digital health methods to promote primary health care in Australia.
3.2.1. Health service delivery (organised around the population)
For the general population, many successes were achieved regarding the efficiency of PHC delivery. For instance, both a new telehealth model in Central Australia [58] and a method of using apps and audio-visual media to provide nutrition education [75] were reported successful due to their time-saving function and improved efficiency. Two more DHIs in other PHC areas caused increased efficiency and extra fees, considering the additional cost was low. It would not affect the affordability of services; the overall success was supported [28,60].
Significantly, DHIs improved patients’ access to PHC services during Covid-19 [69]. DHIs also made PHC services accessible to older patients [69], persons disadvantaged due to socioeconomic, geographic or other reasons [27], and customers living in remote or regional areas [27,50]. What’s more, current PHC services delivery assisted by DHIs have good coordination with emergency referral stream operated by specialists [58], other health organisations and government departments [50] and PHC delivered by face-to-face services [69]. Notably, high comprehensiveness could be indicated by a single DHI that can provide symptom monitoring and management, goal setting, behavioural activation, and motivational counselling services [37], or DHI could deliver detailed risk assessment procedures in place for any patient who is at risk of suicide intention [27].
Overall, the use of telehealth in rural/remote Australia was increasing, which was a positive signal [31], but some mental health care providers suggested that the current telehealth method is not a standalone replacement for traditional professional management but instead a tool to support treatments [76]. Another challenge was the utilisation of a more effective telehealth method; video telehealth had significantly lower utilisation than traditional telephone telehealth [41]. As a feasibility test reported, too many study participants (older adults) never used mobile apps or dropped out, and too few used the app weekly, resulting in their ineffective intervention [44].
In the aspect of service quality, patients received quality and effective health care delivered through mobile apps and digital mental health interventions [27,76], a health education delivered through a social media campaign [50] and a Health Care Homes program assisted by digital technologies [84]. Nevertheless, ineffectiveness in some PHC areas was revealed, such as cardiovascular disease and diabetes management [44], could not support some complex clinical assessments [68] or failed to provide enough novelty, which is an important contributor to consumers’ engagement in an Infant health app [47]. Although few participants in a study reported negative experiences with their health Apps, concerns about addiction were raised by nonusers, indicating a challenge to the person-centeredness of service delivery that DHIs need to be more responsible for their clients [76].
For both the general population and a certain number of First Nations peoples living with them (usually in rural/remote contexts), some positive and similar comments were left on the improved accessibility of PHC brought by DHIs and emphasised it was meaningful to rural [36] and have geographical remoteness as well as no enough health staffs [80], reduced the health inequalities between metropolitan counterparts [45]. Another DHI, the virtual integrated general practices, also contributed to the success of the quality-of-service delivery that achieved its objectives, increasing participants’ willingness to use and improving efficiency by reducing the cost of travelling [45]. Besides, there is success in utilisation. Current health communication to cancer survivors is mainly delivered by digital health methods, and online resources are very important for those clients [34]. However, the services delivered by DHIs have low coverage and do not include relevant chronic and emergency care [12].
For HDIs that mainly deliver PHC services to First Nations peoples, there were successes in the quality of PHC service. An online alcohol and drug control program mentioned that the health education materials in this project presented a high level of written communication, good readability and usability [51]; First Nations-specific telehealth services improved First Nations patients’ confidence, then obtained positive health outcomes [51]. The efficiency improvement was also mentioned by First Nations peoples, who said that DHIs saved travel time, which can be reallocated to health service delivery [71]. However, the challenges to accessibility, such as language barriers in some DHIs [71] or the knowledge barrier caused by the use of complex medical jargon [51], still exist. Another challenge is the utilisation of telehealth is lower compared to face-to-face primary care [54]; as an article explained, some DHIs were a way to augment rather than replace face-to-face services [71].
For the general population, including a certain number of CALD people, DHIs were normally successful in improving efficiency among this research population. Telehealth reduced the economic burden on travel, parking, and accommodation, saved time, and improved overall efficiency, but the long waiting time can be challenging [81].
Overall, increased access to care is a common advantage of telehealth [81]; it could improve access to PHC for some vulnerable groups and rural area residents [42]. DHIs also provide people with impaired physical mobility an alternative way to access health services [79]. In addition, a cancer care website improved accessibility through its interactive functions [48]. However, for older adults, technical difficulties in login and website navigation performed as barriers to accessibility [48]; DHIs reduced access for CALD patients due to their non-English background was also reported [42].
There was a positive outcome regarding service quality, with DHIs being useful for some administrative work, such as organising follow-up appointments or facilitating return visits [79]. However, using digital methods to care for chronic disease in overweight and obese patients, except for a minor outcome, health literacy and diet at six months were positive, and the DHI did not affect most major outcomes [55]. Other quality problems of applied DHIs, including telehealth, did not perform well for complex or sensitive issues [81], health information delivered by social media is usually low quality [56], and missed or delayed diagnoses [42]. Patients did not receive centralised support or navigation, and poor quality of communication is another challenge [64], which also causes discomfort among CALD patients [64,81]. When searching for health information, the utilisation of telehealth or face-to-face GP service is nearly equal [56]. However, participants with CALD backgrounds have lower utilisation of DHIs; older adults and residents from rural areas are less likely to use PHC delivered through videos [25].
For the CALD population, the quality of PHC services delivered by digital methods is important. Some successes were achieved by using DHIs for health education to CALD people through the improvement of interested health outcomes, health literacy and intention to conduct cervical screening [46], which idea supported by another breast cancer health communication program that applying DHIs can improve the health knowledge and screening rates of breast cancer among CALD women [53]. However, some quality issues in translation were reported by CALD people seeking information resources on digital platforms [63] and maternity care mediated by telephone interpretation services [67]. Significantly, insufficient health information from social media became a common challenge specified by selected articles [61,83]; sometimes, bad-quality information even caused negative effects [43].
DHIs improved access to PHC services [29] and pre-travel health information [78]. A group of CALD parents outlined that online health information on child obesity could be accessed quickly, and video-based health education could also help those parents cross the language barrier [43]. However, due to the low availability or efficiency of Healthcare-specific interpreters [65] or considering that English sources were in a predominant position, CALD people still find it harder to access a broader range of information from domestic and international sources [26,43,74,77]. Furthermore, a challenging trend of DHI utilisation was revealed in CALD communities, including face-to-face interviews were more preferred to deliver PHC services [62], and DHIs were less likely to be used [83] compared to the general population or some CALD people from English-speaking countries [26].
Characteristics of DHI, including privacy and confidentiality, can facilitate CALD patients to reduce their shame and overcome previous experiences of being discriminated against [29], then improve the person-centeredness of services. Using social media and online messages to conduct health education was particularly acceptable among young CALD people [70], and online health education platforms run by health professionals or governments gained acceptance from the general CALD population [43]. However, ensuring health service delivery could cover all social groups in the targeted population (CALD population) was a critical challenge. For instance, during the online COVID-19 health communication program, a problem was presented: Health resources are mainly allocated to “high volume” CALD communities rather than “high demand” communities [77].
3.2.2. Health Workforce
Although online training for health workers has been successful in health services such as end-of-life care, the effectiveness of this DHI is still uncertain [57]. In another aspect of the supplies for health workers (human resources or funding), digital health can be used to overcome the challenges in areas such as staff shortages in aged care and rural/remote settings, then improve the accessibility of sleep care GP services [40]. Still, some healthcare providers expressed frustration about telehealth funding and its impact on facilitating their practices [68]. Notably, COVID-19 increased health providers’ skills in telehealth methods and eventually contributed to the success of multiple DHIs and service qualities [40].
Also, challenges were presented as low availability of training and tools, such as no proper tools to use, including limited appropriate technologies to support practitioners in delivering services [68] or difficulty finding appropriate technology due to the lack of efficiency or safety information [40]. Health worker training issues, including PHC providers having low familiarity with new digital health technologies [68,82], problematic training affordability [40], Extra workload and limited time brought by DHIs [40], are also presented as challenges for patients to access quality primary care. For health workers who provide DHIs in rural areas that have a relatively high proportion of First Nations residents (nearly 15%), the inadequate rural health workforce, as a health resource barrier, became a major challenge [33]. A study on health workers who mainly deliver services to First Nations peoples reported a similar challenge: additional staff are needed to support patients’ telehealth appointments [71]. The same study also illustrated other challenges, including the extra workload brought by telehealth and interpreters not being trained to translate some medical jargon, which may relate to language barriers caused by low translation quality [71]. Remarkably, DHIs enabled vulnerable staff to safely continue delivering services to their regular clients during the COVID-19 Pandemic, which is considered a success [71].
3.2.3. Health Information System (HIS)
For the general population, applying DHIs in PHC delivery enabled data collection and analysis during the health intervention, improved efficiency and expanded the data source simultaneously [27,75]. An article highlighted the success of the current health record system, “My Health Record”, in increasing the accessibility of health data for both patients and healthcare providers [39]. However, online platforms that could promote real-time share of health information have not been established in some specific PHC areas [57], and inequity of access for consumers with limited resources still exists [39], which were reported as challenges.
Research with the context of rural/remote Australia and includes Aboriginal health practitioners as participants and another research on HIS specifically designed for the First Nations peoples presented similar ideas that the functions of current HIS can ensure healthcare providers’ access to good quality data and improve their PHC delivery performance [38,80]. Moreover, the current Health information system in NT that has a data management function can lead to substantial improvements in the delivery of PHC. However, a key challenge was the lack of connectivity between HIS across different services [33]. In addition, in regional areas, healthcare providers faced challenges, including difficulties in operating the HIS, which resulted in low workflow efficiency and increased risk of errors [80] or inappropriate tools used, causing low data management efficiency [38], which eventually reduces the efficiency of service delivery. Besides, the current HIS is deeply connected with other health system components; any attempt at change or improvement would cause a severe documentation burden and then become a new challenge [38].
3.2.4. Medicine, Vaccines, diagnostic and technologies
In the area of nutrition education for the Australian general population, some digital technologies (such as photographs and nutrient analysis software) were considered successful in improving the efficiency and effectiveness of service delivery [75]. However, the challenge in technology affordability was that the high price of technology (retina camera) is commercially not practical for large-scale use for healthcare providers, resulting in a low eye screening rate [82]. Besides, technological infrastructure for videoconferencing to access GP services is unaffordable for disadvantaged patients with low socioeconomic status [41].
Accessibility and quality of technologies are the challenges faced by both people from the general population group and the First Nations people group. For example, the general population and First Nations peoples as participants reported the accessibility and utilisation of telehealth hardware (such as smartphone ownership) were low among the research population [49], especially in rural or remote Australia [66]. Also, the system-level uptake of telehealth technologies is slow [49], which caused the low accessibility of digital health services mediated by those infrastructures [66]. The quality of some current technologies is low, including unstable internet in rural or remote Australia [80], absence of some essential functions (for instance, auto-reminders) of technologies [66] and current technologies are usually designed for general purpose rather than specialised for clinical purpose [49], which may lead to the low quality of health services [49,66]. Research on First Nations peoples reported similar challenges: poor accessibility/utilisation of technologies (low smartphone ownership) and low quality of technology, such as bad internet in living areas of some First Nations peoples, causing poor communication audio quality in telehealth [71].
General and CALD participants outlined the lack of hardware devices to apply DHIs [64] and bad technology quality (phone call dropped), which can significantly reduce the experienced quality of care [81] as perceived challenges. Among research mainly designed for CALD patients, a study focused on electronic mental diagnosis methods suggests the test results generated from computerised neuropsychological assessments (CNAs) were more stable and accurate, then improved the overall quality of PHC [59]. The challenge of low availability and accessibility of telehealth devices (smartphones) exists in CALD patients as well [77] and might be even worse than in the general population [63]. Challenges included the quality issues of technologies, such as some DHIs being susceptible to technological difficulties [46] and an unstable Internet connection [35].
3.2.5. Community engagement
Some First Nations peoples received GP services delivered by mobile apps and found the apps are positioned in a way that counters rural community-centred norms, values, and culture and reduces community involvement, which presented not only a low person-centredness in service delivery but also a significant signal of the absence of community engagement [36]. Another challenge for some DHIs, such as cardiac rehabilitation services assisted by digital systems, local health providers and community leaders pointed out the need to improve coordination with different social groups, programs and service providers [66]. However, some successful community engagement has been achieved, such as healthcare providers developed online health education material with local First Nations communities, then eventually delivering services tailored for First Nations peoples with high cultural appropriateness and person-centeredness [51], or recruited First Nations researchers in the design process, then helped First Nations peoples overcome shame or previous experience of being discriminated [52] and enables First Nations peoples to access service in their country, then reduce their mental distress and alienation [32].
A co-design online health education program emphasised the success of involvement and empowerment of the CALD community members [46]. Moreover, when conducting health communication about COVID-19 in CALD communities, social media apps were heavily relied on to deliver health information and provide a platform for the officials to cooperate with local community leaders [77]. However, some DHIs presented a lack of community engagement through failure to provide culturally appropriate materials; for example, most DHIs aimed at suicide protection were designed for the general population, and they may not be able to cover the needs of minority groups, including CALD people [30]. Moreover, CALD patients reported a diabetes mobile app failed to provide details about culturally relevant foods and reduced the overall service quality [63]. Also, current LGBTQ+ health services websites could not satisfy the cultural needs of the Australian CALD LGBTIQ+ patients, increasing their social isolation [72].
4. Discussion
4.1. Summary of Findings
This scoping review identified the successes and challenges of applying digital health interventions in improving access to primary health care (PHC) among priority populations in Australia. In the aspect of health services delivery, the accessibility of health services obtained successes across the types of studies that involved the general population but were challenging in studies specifically designed for CALD or First Nations populations. For general and First Nations populations, the quality of PHC services delivered by DHIs is at a satisfactory level; although the DHIs presented some effectiveness for CALD people, the quality of the cultural- and language-specific content is usually low. All three populations reported improved efficiency brought by DHIs. However, the utilisation of quality DHIs is generally low between First Nations and CALD populations. To other health system building blocks, deeply related to Primary health service delivery, Ineffective health governance related to DHIs was presented as a challenge across all three populations. Health workforce using DHIs presented similar challenges across general and First Nations populations, including extra workload and inadequate supplies, and similar successes under COVID-19 settings. However, as special health workers, the interpreters are involved in special challenges for the First Nations population. The current HIS is successful for all populations in its main functions, but low inter-sector cooperation and inequities in accessing HIS between cities and rural/remote areas still exist for First Nations Peoples and some parts of general populations. Among both general and CALD populations, current technologies can improve overall quality but are insufficient in specific areas. However, for CALD and First Nations populations, the affordability of technologies limited their access to PHC. Although DHIs can improve community engagement with First Nations and CALD people through tailored and co-designed DHIs, for DHIs designed for the general population but applied to minority populations, there is a challenge of delivering PHCs in a way that priority populations can culturally accept. Moreover, current DHIs cannot cover all target population groups, such as “low volume” CALD groups or First Nations people.
The overview of the successes and challenges across building blocks and populations was listed in the table in Supplementary file S1. Current evidence suggests the challenges and successes of applying DHIs for priority populations to access the PHC are generally inconclusive; this finding is similar to previous reviews [8,85,86]. However, there are some critical patterns across the findings that were remarkable and useful for improving the access of PHC delivered by DHIs to the priority populations and will be interpreted with the comparison to existing research:
4.2. Tailored designs in DHIs are needed to help priority populations overcome cultural barriers.
Cultural barriers still exist and prevent both CALD and First Nations people from using DHIs to access quality PHC services. However, this barrier can be reduced with further DHIs tailored to the priority populations. We synthesised that many Patients from priority populations reported challenges on a lack of content with cultural appropriateness, and such failure of DHIs to satisfy the cultural needs of priority populations significantly limited the access of those people to quality health services [30,36,63,72]. This relation explains that an imprecise representation of the culture is related to fear towards DHIs or past traumas [87]. Interestingly, a common feature was revealed: Most of those DHIs facing challenges on cultural barriers were designed for the general public rather than tailored explicitly to priority populations. In contrast, patients from priority populations usually reported that DHIs tailored to them successfully reduced cultural barriers [32,46,51,52]. An idea of tailored design is key to overcoming cultural barriers, and it can be revealed. International evidence supported this idea that tailored DHIs improved access to services in particularly underserved groups, and a higher degree of target population involvement and co-design can reinforce this improvement [88,89]. The success of tailored design can be explained by such design usually involves co-design with members from priority populations or other forms of high community engagement, which engages First Nations and CALD peoples meaningfully in research, documenting their experiences and needs on different health areas, then ensures their cultural needs are acknowledged in those DHIs [90]. Although further studies on the role of tailored designs still need to be scrutinised to obtain a better understanding and improve the impact of these designs [89], the importance of tailored designs discovered from current evidence could provide insight for health managers or providers to deliver primary care assisted by DHIs to priority communities.
4.3. Language barriers faced by CALD and First Nations peoples are still significant.
Two important sub-themes were discovered from existing studies: challenges related to interpreters and a lack of community language resources. Both sub-themes suggest that the language barriers faced by CALD and First Nations populations are still significant. Many patients from priority populations faced language problems. The studies selected by us show in current DHIs, interpreters use the telephone or other online platforms such as Zoom to participate in health service delivery [65,71] or health education programs, and health providers translate English health information into community languages [26,43,74,77] are major ways used to address the language barrier. However, current evidence shows the interpreter service may present low quality, efficiency, or availability, especially when complex medical jargon or rural/remote context is involved. Also, community language resources are absent or have poor translation quality. As other studies agreed, such challenges limited the progress of addressing current language barriers, limiting priority populations’ ability to use DHIs to access quality PHC services [91,92,93]. Although there are alternative options to overcome the language barrier which were not mentioned in the articles selected by us, such as using translation apps to ensure the service could be delivered without interpreters [94,95], those two articles related to this option did not mention there is a large-scale use of this method existing. In addition, some evidence suggests that such alternative options could have severe accuracy problems [96,97], which may help explain why this alternative method did not affect the conclusion on language barriers made by our study. Hence, this research emphasises that language barriers are still challenging for priority populations, and an explanation was provided. As a cross-sectional study suggests, future improvements may still need to focus on creating supporting infrastructure and health e-literacy at system levels and facilitating interpreters to support telehealth interactions [91].
4.4. The role of DHIs in relation to the regional digital divide faced by First Nations peoples.
Poor internet connection is an important challenge to applying DHIs in priority studies. In studies, our research synthesised that such insufficient DHI technology infrastructure is significantly severe among First Nations peoples, indicating the regional digital divide is still lasting. According to the article we selected, some challenges of technological infrastructure are faced by First Nations peoples, such as unstable internet [71,80] or inadequate hardware or devices to receive DHIs [25,66]. Notably, nearly all of the research was done in a rural/remote context. This challenge is shared by other local residents who are more likely to belong to the general population group [25,66,80]. The listed evidence suggests that although developing digital health methods can help overcome the geographical barrier, the digital divide between rural areas and city areas may still be significant, contributing to the challenges faced by First Nations Peoples in using DHIs to access quality PHC services. This idea was supported by previous studies [98,99]. Furthermore, the idea claimed by an article that COVID-19 ensure the funding of rural digital health, hence a key barrier preventing telehealth from securing its place in rural areas would be addressed [100]. Our evidence opposed this claim that the funding problem is still a concern for rural healthcare providers using DHIs [68]. Notably, admitting the significance of the digital divide does not mean denying the potential DHIs in overcoming this barrier. With the development in the digital health area, multiple successes in improving rural access to PHC services mediated by DHIs were listed in our results section [27,32,36,45,50,71,80]. The idea that the gap between urban and rural areas has not been reduced [99] can be opposed, and DHIs’ ability to overcome the regional digital divide could be supported. To conclude, the role of the regional digital divide in our topic has been examined. Efforts from healthcare providers and managers are needed to address this gap and improve the health and well-being of First Nations peoples.
4.5. Limitations
This scoping review has some limitations. Firstly, many of the selected articles (36%) are qualitative studies. Because one qualitative study could generate multiple ideas, collecting and presenting all those ideas would be extremely hard. Hence, this study only selected those “most relevant points”. Such a process may result in data loss and may cause some deviations from the real situation. To overcome this limitation, further studies can limit the inclusion of studies to ensure the proportion of other types of studies. Since the methodology is a scoping review, no standardised measurement exists to examine the effect size of each success and challenge. Therefore, we can only map the results obtained from different studies and explain patterns rather than explaining to what extent current DHIs are successful or facing challenges. Based on this limitation, a further systematic review of this topic would be recommended to obtain a more “quantified” result. Moreover, as some selected studies indicated, the First Nations and CALD peoples have a broad label, and the successes and challenges may vary across different sub-groups in each population. Therefore, more detailed and more profound studies on each population and its sub-groups are welcomed.
5. Conclusions
Digital health interventions hold promise in bolstering access to quality primary care for patients. Nonetheless, formidable challenges persist within various healthcare subdomains, spanning different health systems building blocks and demographic groups, rendering the overall evidence inconclusive and uncertain. Nonetheless, amid this complexity, certain noteworthy trends emerge. For instance, digital health interventions demonstrate the potential to mitigate language and cultural barriers encountered by priority populations and address the digital disparity among First Nations communities. Analysis of existing research reveals that despite the critical importance of high-quality interpreters and translated materials in facilitating access for priority populations, proposed alternative approaches have not substantially impacted the efficacy of digital health interventions. While the regional digital divide remains pronounced, digital health interventions exhibit promise in surmounting this obstacle. Cultural barriers persist, but tailored designs of digital health interventions offer promise in assisting priority populations in overcoming this challenge. These underlying patterns of success and challenge furnish a nuanced comprehension of the role of digital health interventions in primary care, thereby equipping healthcare managers with insights to combat health disparities across diverse demographics.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, File S1: Searching strategy and details of database articles.
Author Contributions
Conceptualization, R.K. and Y.A.; methodology, R.K., Y.A. and S.Z.; formal analysis, S.Z.; writing—original draft preparation, S.Z.; writing—review and editing, R.K. and Y.A.; supervision, R.K. and Y.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analysed in this study. Data sharing is not applicable to this research.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DHIs | Digital Health Interventions |
| PHC | Primary Health Care |
| CALD | Culturally and Linguistically Diverse |
References
- World Health Organization. Universal health coverage (UHC) 2023 [cited 7 January, 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc).
- World Health Organization. Universal Health Coverage n.a. [cited 7 January, 2024. Available from: https://www.who.int/health-topics/universal-health-coverage#tab=tab_1.
- World Health Organization. Declaration of Alma-Ata International Conference on Primary Health Care; Alma-Ata, USSR,1978.
- World Health Organization. Global diffusion of eHealth: making universal health coverage achievable: report of the third global survey on eHealth. World Health Organization; 2016.
- World Health Organization. Classification of digital health interventions v1.0. 2018.
- World Health Organization. Global strategy on digital health 2020-2025. 2021.
- Kasteleyn MJ, Versluis A, van Peet P, Kirk UB, van Dalfsen J, Meijer E, et al. SERIES: eHealth in primary care. Part 5: A critical appraisal of five widely used eHealth applications for primary care - opportunities and challenges. Eur J Gen Pract. 2021;27(1):248-56.
- Erku D, Khatri R, Endalamaw A, Wolka E, Nigatu F, Zewdie A, et al. Digital Health Interventions to Improve Access to and Quality of Primary Health Care Services: A Scoping Review. International journal of environmental research and public health. 2023;20(19):6854. [CrossRef]
- Sanyal C, Stolee P, Juzwishin D, Husereau D. Economic evaluations of eHealth technologies: A systematic review. PLoS One. 2018;13(6):e0198112-e. [CrossRef]
- Srivastava D, Van Kessel R, Delgrange M, Cherla A, Sood H, Mossialos E. A Framework for Digital Health Policy: Insights from Virtual Primary Care Systems Across Five Nations. PLOS digital health. 2023;2(11):e0000382-e. [CrossRef]
- Health AIo, Welfare. Health expenditure Australia 2020-21. Canberra: AIHW; 2022.
- Endalamaw A, Erku D, Khatri RB, Nigatu F, Wolka E, Zewdie A, et al. Successes, weaknesses, and recommendations to strengthen primary health care: a scoping review. Arch Public Health. 2023;81(1):100-. [CrossRef]
- Fisher M, Freeman T, Mackean T, Friel S, Baum F. Universal Health Coverage for Non-communicable Diseases and Health Equity: Lessons From Australian Primary Healthcare. Int J Health Policy Manag. 2022;11(5):690-700. [CrossRef]
- Bradley C, Hengel B, Crawford K, Elliott S, Donovan B, Mak DB, et al. Establishment of a sentinel surveillance network for sexually transmissible infections and blood borne viruses in Aboriginal primary care services across Australia: The ATLAS project. BMC Health Serv Res. 2020;20(1):769-. [CrossRef]
- Henderson J, Javanparast S, MacKean T, Freeman T, Baum F, Ziersch A. Commissioning and equity in primary care in Australia: Views from Primary Health Networks. Health Soc Care Community. 2018;26(1):80-9. [CrossRef]
- Marcus K, Balasubramanian M, Short SD, Sohn W. Dental hesitancy: a qualitative study of culturally and linguistically diverse mothers. BMC Public Health. 2022;22(1):2199-. [CrossRef]
- Davy C, Harfield S, McArthur A, Munn Z, Brown A. Access to primary health care services for Indigenous peoples: A framework synthesis. Int J Equity Health. 2016;15(1):1-9. [CrossRef]
- Ong KS, Carter R, Kelaher M, Anderson I. Differences in primary health care delivery to Australias Indigenous population: A template for use in economic evaluations. BMC Health Serv Res. 2012;12(1):307-. [CrossRef]
- Scanlon B, Durham J, Wyld D, Roberts N, Toloo GS. Exploring equity in cancer treatment, survivorship, and service utilisation for culturally and linguistically diverse migrant populations living in Queensland, Australia: a retrospective cohort study. International journal for equity in health. 2023;22(1):175-. [CrossRef]
- Foley K, Freeman T, Ward P, Lawler A, Osborne R, Fisher M. Exploring access to, use of and benefits from population-oriented digital health services in Australia. Health Promot Int. 2021;36(4):1105-15. [CrossRef]
- Ziebland S, Hyde E, Powell J. Power, paradox and pessimism: On the unintended consequences of digital health technologies in primary care. Soc Sci Med. 2021;289:114419-. [CrossRef]
- Pace R, Pluye P, Bartlett G, Macaulay AC, Salsberg J, Jagosh J, et al. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int J Nurs Stud. 2012;49(1):47-53. [CrossRef]
- World Health Organization. Everybody’s business--strengthening health systems to improve health outcomes: WHO’s framework for action. 2007.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement (Reprinted from Annals of Internal Medicine). Physical therapy. 2009;89(9):873-80.
- Dai Z, Sezgin G, Hardie RA, McGuire P, Pearce C, McLeod A, et al. Sociodemographic determinants of telehealth utilisation in general practice during the COVID-19 pandemic in Australia. Intern Med J. 2023;53(3):422-5. [CrossRef]
- Sezgin G, Dai Z, McLeod A, Pearce C, Georgiou A. Difference in general practice telehealth utilisation associated with birth country during COVID-19 from two Australian states. Ethics Med Public Health. 2023;27:100876. [CrossRef]
- Staples LG, Webb N, Asrianti L, Cross S, Rock D, Kayrouz R, et al. A Comparison of Self-Referral and Referral via Primary Care Providers, through Two Similar Digital Mental Health Services in Western Australia. Int J Environ Res Public Health. 2022;19(2). [CrossRef]
- Estai M, Kruger E, Tennant M, Bunt S, Kanagasingam Y. Challenges in the uptake of telemedicine in dentistry. Rural Remote Health. 2016;16(4):3915. [CrossRef]
- Baker AEZ, Procter NG, Ferguson MS. Engaging with culturally and linguistically diverse communities to reduce the impact of depression and anxiety: a narrative review. Health & Social Care in the Community. 2016;24(4):386-98. [CrossRef]
- Bowden M, McCoy A, Reavley N. Suicidality and suicide prevention in culturally and linguistically diverse (CALD) communities: A systematic review. International Journal of Mental Health. 2020;49(4):293-320. [CrossRef]
- Bradford NK, Caffery LJ, Smith AC. Telehealth services in rural and remote Australia: a systematic review of models of care and factors influencing success and sustainability. Rural Remote Health. 2016;16(4):3808.
- Caffery LJ, Bradford NK, Wickramasinghe SI, Hayman N, Smith AC. Outcomes of using telehealth for the provision of healthcare to Aboriginal and Torres Strait Islander people: a systematic review. Aust N Z J Public Health. 2017;41(1):48-53. [CrossRef]
- Edelman A, Grundy J, Larkins S, Topp SM, Atkinson D, Patel B, et al. Health service delivery and workforce in northern Australia: a scoping review. Rural Remote Health. 2020;20(4):6168. [CrossRef]
- Goodwin BC, Zajdlewicz L, Stiller A, Johnston EA, Myers L, Aitken JF, et al. What are the post-treatment information needs of rural cancer survivors in Australia? A systematic literature review. Psychooncology. 2023;32(7):1001-12. [CrossRef]
- Luu B, Fox L, McVeigh MJ, Ravulo J. Effectively supporting Culturally and Linguistically Diverse (CALD) young people with their mental health and wellbeing - does this matter or exist in Australia? Social Work in Mental Health. 2023.
- O’Sullivan B, Couch D, Naik I. Using Mobile Phone Apps to Deliver Rural General Practitioner Services: Critical Review Using the Walkthrough Method. JMIR Form Res. 2022;6(1):e30387. [CrossRef]
- Parker S, Prince A, Thomas L, Song H, Milosevic D, Harris MF. Electronic, mobile and telehealth tools for vulnerable patients with chronic disease: a systematic review and realist synthesis. BMJ Open. 2018;8(8):e019192. [CrossRef]
- Sibthorpe B, Gardner K, Chan M, Dowden M, Sargent G, McAullay D. Impacts of continuous quality improvement in Aboriginal and Torres Strait islander primary health care in Australia. J Health Organ Manag. 2018;32(4):545-71. [CrossRef]
- Carroll J, Butler-Henderson K. MyHealthRecord in Australian Primary Health Care: An Attitudinal Evaluation Study. J Med Syst. 2017;41(10):158. [CrossRef]
- Cheung JM, Menczel Schrire Z, Aji M, Rahimi M, Salomon H, Doggett I, et al. Embedding digital sleep health into primary care practice: A triangulation of perspectives from general practitioners, nurses, and pharmacists. Digit Health. 2023;9:20552076231180970. [CrossRef]
- Fisher K, Tapley A, Ralston A, Davey A, Fielding A, van Driel M, et al. Video versus telephone for telehealth delivery: a cross-sectional study of Australian general practice trainees. Fam Pract. 2023. [CrossRef]
- Halcomb EJ, Ashley C, Dennis S, McInnes S, Morgan M, Zwar N, et al. Telehealth use in Australian primary healthcare during COVID-19: a cross-sectional descriptive survey. BMJ Open. 2023;13(1):e065478. [CrossRef]
- Jawad D, Taki S, Baur L, Rissel C, Mihrshahi S, Wen LM. Resources used and trusted regarding child health information by culturally and linguistically diverse communities in Australia: An online cross-sectional survey. International Journal of Medical Informatics. 2023;177. [CrossRef]
- Buss VH, Varnfield M, Harris M, Barr M. Remotely Conducted App-Based Intervention for Cardiovascular Disease and Diabetes Risk Awareness and Prevention: Single-Group Feasibility Trial. JMIR Hum Factors. 2022;9(3):e38469. [CrossRef]
- Lepre B, Job J, Martin Z, Kerrigan N, Jackson C. The Queensland Virtual Integrated Practice (VIP) partnership program pilot study: an Australian-first model of care to support rural general practice. BMC Health Serv Res. 2023;23(1):1183. [CrossRef]
- Power R, Ussher JM, Hawkey A, Missiakos O, Perz J, Ogunsiji O, et al. Co-designed, culturally tailored cervical screening education with migrant and refugee women in Australia: a feasibility study. Bmc Womens Health. 2022;22(1). [CrossRef]
- Taki S, Lymer S, Russell CG, Campbell K, Laws R, Ong KL, et al. Assessing User Engagement of an mHealth Intervention: Development and Implementation of the Growing Healthy App Engagement Index. JMIR Mhealth Uhealth. 2017;5(6):e89. [CrossRef]
- Tiong SS, Koh ES, Delaney G, Lau A, Adams D, Bell V, et al. An e-health strategy to facilitate care of breast cancer survivors: A pilot study. Asia Pac J Clin Oncol. 2016;12(2):181-7. [CrossRef]
- Australasian Telehealth Society. Telehealth and the NBN: A submission to the Australian House of Representatives Infrastructure and Communications Committee Inquiry into the role and potential benefits of the National Broadband Network 2011 Febuary.
- WA Country Health Service. Telehealth Awareness Week 2018. Government of Western Australia; 2018 25-29 June.
- Amanda R, Rana K, Saunders P, Tracy M, Bridges N, Poudel P, et al. Evaluation of the usability, content, readability and cultural appropriateness of online alcohol and other drugs resources for Aboriginal and Torres Strait Islander Peoples in New South Wales, Australia. BMJ Open. 2023;13(5):e069756. [CrossRef]
- Lee KSK, Wilson S, Perry J, Room R, Callinan S, Assan R, et al. Developing a tablet computer-based application (’App’) to measure self-reported alcohol consumption in Indigenous Australians. BMC Med Inform Decis Mak. 2018;18(1):8.
- Macnamara J, Camit M. Effective CALD community health communication through research and collaboration: an exemplar case study. Communication Research and Practice. 2017;3(1):92-112. [CrossRef]
- Osborn E, Ritha M, Macniven R, Agius T, Christie V, Finlayson H, et al. “No One Manages It; We Just Sign Them Up and Do It”: A Whole System Analysis of Access to Healthcare in One Remote Australian Community. Int J Environ Res Public Health. 2022;19(5). [CrossRef]
- Parker SM, Barr M, Stocks N, Denney-Wilson E, Zwar N, Karnon J, et al. Preventing chronic disease in overweight and obese patients with low health literacy using eHealth and teamwork in primary healthcare (HeLP-GP): a cluster randomised controlled trial. BMJ Open. 2022;12(11):e060393. [CrossRef]
- Bowden JL, Lamberts R, Hunter DJ, Melo LR, Mills K. Community-based online survey on seeking care and information for lower limb pain and injury in Australia: an observational study. BMJ Open. 2020;10(7):e035030. [CrossRef]
- Ding J, Johnson CE, Saunders C, Licqurish S, Chua D, Mitchell G, et al. Provision of end-of-life care in primary care: a survey of issues and outcomes in the Australian context. BMJ Open. 2022;12(1):e053535. [CrossRef]
- Green D, Russell DJ, Zhao Y, Mathew S, Fitts MS, Johnson R, et al. Evaluation of a new medical retrieval and primary health care advice model in Central Australia: Results of pre- and post-implementation surveys. Aust J Rural Health. 2023;31(2):322-35. [CrossRef]
- Page ZA, Croot K, Sachdev PS, Crawford JD, Lam BP, Brodaty H, et al. Comparison of Computerised and Pencil-and-Paper Neuropsychological Assessments in Older Culturally and Linguistically Diverse Australians. Journal of the International Neuropsychological Society. 2022;28(10):1050-63.
- Snoswell CL, Caffery LJ, Whitty JA, Soyer HP, Gordon LG. Cost-effectiveness of Skin Cancer Referral and Consultation Using Teledermoscopy in Australia. JAMA Dermatol. 2018;154(6):694-700. [CrossRef]
- Alqahtani AS, Sheikh M, Wiley K, Heywood AE. Australian Hajj pilgrims’ infection control beliefs and practices: Insight with implications for public health approaches. Travel Med Infect Dis. 2015;13(4):329-34. [CrossRef]
- Alzubaidi H, Mc Namara K, Browning C. Time to question diabetes self-management support for Arabic-speaking migrants: exploring a new model of care. Diabet Med. 2017;34(3):348-55. [CrossRef]
- Ayre J, Bonner C, Bramwell S, McClelland S, Jayaballa R, Maberly G, et al. Implications for GP endorsement of a diabetes app with patients from culturally diverse backgrounds: a qualitative study. Australian Journal of Primary Health. 2020;26(1):52-7. [CrossRef]
- Carrigan A, Roberts N, Clay-Williams R, Hibbert P, Austin E, Pulido DF, et al. What do consumer and providers view as important for integrated care? A qualitative study. BMC Health Serv Res. 2023;23(1):11. [CrossRef]
- Easpaig BNG, Tran Y, Winata T, Lamprell K, Pulido DF, Arnolda G, et al. Providing outpatient cancer care for CALD patients: a qualitative study. Bmc Research Notes. 2021;14(1). [CrossRef]
- Field P, Franklin RC, Barker R, Ring I, Leggat PA. Cardiac rehabilitation in rural and remote areas of North Queensland: How well are we doing? Aust J Rural Health. 2022;30(4):488-500.
- Hughson JA, Marshall F, Daly JO, Woodward-Kron R, Hajek J, Story D. Health professionals’ views on health literacy issues for culturally and linguistically diverse women in maternity care: barriers, enablers and the need for an integrated approach. Australian Health Review. 2018;42(1):10-20.
- James S, Ashley C, Williams A, Desborough J, McInnes S, Calma K, et al. Experiences of Australian primary healthcare nurses in using telehealth during COVID-19: a qualitative study. BMJ Open. 2021;11(8):e049095. [CrossRef]
- Javanparast S, Roeger L, Kwok Y, Reed RL. The experience of Australian general practice patients at high risk of poor health outcomes with telehealth during the COVID-19 pandemic: a qualitative study. BMC Fam Pract. 2021;22(1):69. [CrossRef]
- Kearns R, Gardner K, Silveira M, Woodland L, Hua M, Katz M, et al. Shaping interventions to address waterpipe smoking in Arabic-speaking communities in Sydney, Australia: a qualitative study. BMC Public Health. 2018;18(1):1379. [CrossRef]
- Mathew S, Fitts MS, Liddle Z, Bourke L, Campbell N, Murakami-Gold L, et al. Telehealth in remote Australia: a supplementary tool or an alternative model of care replacing face-to-face consultations? BMC Health Serv Res. 2023;23(1):341.
- McCulloch K, Murray K, Cassidy E. Bridging Across the Digital Divide: Identifying the Extent to Which LGBTIQ plus Health Service Websites Engage Culturally and Linguistically Diverse (CALD) Users. Journal of Homosexuality. 2023;70(11):2395-417. [CrossRef]
- O’Callaghan C, Dharmagesan GG, Roy J, Dharmagesan V, Loukas P, Harris-Roxas B. Enhancing equitable access to cancer information for culturally and linguistically diverse (CALD) communities to complement beliefs about cancer prognosis and treatment. Support Care Cancer. 2021;29(10):5957-65. [CrossRef]
- O’Callaghan C, Tran A, Tam N, Wen LM, Harris R. Promoting the get healthy information and coaching service (GHS) in Australian-Chinese communities: facilitators and barriers. Health Promot Int. 2022;37(2). [CrossRef]
- O’Connor R, Slater K, Ball L, Jones A, Mitchell L, Rollo ME, et al. The tension between efficiency and effectiveness: a study of dietetic practice in primary care. J Hum Nutr Diet. 2019;32(2):259-66. [CrossRef]
- Pung A, Fletcher SL, Gunn JM. Mobile App Use by Primary Care Patients to Manage Their Depressive Symptoms: Qualitative Study. J Med Internet Res. 2018;20(9):e10035. [CrossRef]
- Seale H, Harris-Roxas B, Heywood A, Abdi I, Mahimbo A, Chauhan A, et al. Speaking COVID-19: supporting COVID-19 communication and engagement efforts with people from culturally and linguistically diverse communities. BMC Public Health. 2022;22(1):1257. [CrossRef]
- Seale H, Kaur R, Mahimbo A, MacIntyre CR, Zwar N, Smith M, et al. Improving the uptake of pre-travel health advice amongst migrant Australians: exploring the attitudes of primary care providers and migrant community groups. BMC Infect Dis. 2016;16:213. [CrossRef]
- Song HJ, Dennis S, Levesque JF, Harris MF. What matters to people with chronic conditions when accessing care in Australian general practice? A qualitative study of patient, carer, and provider perspectives. BMC Fam Pract. 2019;20(1):79. [CrossRef]
- Tan MS, Patel BK, Roughead EE, Ward M, Reuter SE, Roberts G, et al. Opportunities for clinical decision support targeting medication safety in remote primary care management of chronic kidney disease: A qualitative study in Northern Australia. J Telemed Telecare. 2023:1357633x231204545. [CrossRef]
- Toll K, Spark L, Neo B, Norman R, Elliott S, Wells L, et al. Consumer preferences, experiences, and attitudes towards telehealth: Qualitative evidence from Australia. PLoS One. 2022;17(8):e0273935. [CrossRef]
- Watson MJG, McCluskey PJ, Grigg JR, Kanagasingam Y, Daire J, Estai M. Barriers and facilitators to diabetic retinopathy screening within Australian primary care. BMC Fam Pract. 2021;22(1):239.
- Mistry SK, Harris E, Harris MF. Learning from a codesign exercise aimed at developing a navigation intervention in the general practice setting. Family Practice. 2022;39(6):1070-9.
- True A, Janamian T, Dawda P, Johnson T, Smith G. Lessons from the implementation of the Health Care Homes program. Med J Aust. 2022;216 Suppl 10(Suppl 10):S19-s21. [CrossRef]
- Agarwal S, Agarwal S, Glenton C, Henschke N, Tamrat T, Bergman H, et al. Tracking health commodity inventory and notifying stock levels via mobile devices: a mixed methods systematic review. Cochrane Database Syst Rev. 2020;2020(10):CD012907-CD. [CrossRef]
- Lall P, Rees R, Law GCY, Dunleavy G, Cotič Ž, Car J. Influences on the implementation of mobile learning for medical and nursing education: Qualitative systematic review by the digital health education collaboration. J Med Internet Res. 2019;21(2):e12895-e. [CrossRef]
- Whitehead L, Talevski J, Fatehi F, Beauchamp A. Barriers to and Facilitators of Digital Health Among Culturally and Linguistically Diverse Populations: Qualitative Systematic Review. J Med Internet Res. 2023;25(1):e42719-e. [CrossRef]
- Gonzalez C, Early J, Gordon-Dseagu V, Mata T, Nieto C. Promoting Culturally Tailored mHealth: A Scoping Review of Mobile Health Interventions in Latinx Communities. J Immigr Minor Health. 2021;23(5):1065-77. [CrossRef]
- Radu I, Scheermesser M, Spiess MR, Schulze C, Händler-Schuster D, Pehlke-Milde J. Digital Health for Migrants, Ethnic and Cultural Minorities and the Role of Participatory Development: A Scoping Review. International journal of environmental research and public health. 2023;20(20):6962. [CrossRef]
- Botfield JR, Newman CE, Lenette C, Albury K, Zwi AB. Using digital storytelling to promote the sexual health and well-being of migrant and refugee young people: A scoping review. Health education journal. 2018;77(7):735-48.
- Gallegos-Rejas VM, Kelly JT, Lucas K, Snoswell CL, Haydon HM, Pager S, et al. A cross-sectional study exploring equity of access to telehealth in culturally and linguistically diverse communities in a major health service. Australian health review. 2023;47(6):721-8. [CrossRef]
- Gallegos-Rejas VM, Kelly JT, Snoswell CL, Haydon HM, Banbury A, Thomas EE, et al. Does the requirement for an interpreter impact experience with telehealth modalities, acceptability and trust in telehealth? Results from a national survey including people requiring interpreter services. Journal of Telemedicine and Telecare. 2023;29(10_suppl):24S-9S. [CrossRef]
- Heinrichs DH, Kretzer MM, Davis EE. Mapping the online language ecology of multilingual COVID-19 public health information in Australia. European journal of language policy. 2022;14(2):133-62. [CrossRef]
- Freyne J, Bradford D, Pocock C, Silvera-Tawil D, Harrap K, Brinkmann S. Developing digital facilitation of assessments in the absence of an interpreter: Participatory design and feasibility evaluation with allied health groups. JMIR Form Res. 2018;20(1):e1-e. [CrossRef]
- Hwang K, Williams S, Zucchi E, Chong TWH, Mascitti-Meuter M, LoGiudice D, et al. Testing the use of translation apps to overcome everyday healthcare communication in Australian aged-care hospital wards—An exploratory study. Nurs Open. 2022;9(1):578-85. [CrossRef]
- Beh THK, Canty DJ. English and Mandarin translation using Google Translate software for pre-anaesthetic consultation. Anaesth Intensive Care. 2015;43(6):792-3.
- Panayiotou A, Gardner A, Williams S, Zucchi E, Mascitti-Meuter M, Goh AMY, et al. Language translation apps in health care settings: Expert opinion. JMIR Mhealth Uhealth. 2019;7(4):e11316-e. [CrossRef]
- Koh A, Swanepoel DW, Ling A, Ho BL, Tan SY, Lim J. Digital health promotion: promise and peril. Health Promot Int. 2021;36(Supplement_1):i70-i80. [CrossRef]
- Walker J. ‘It keeps dropping out!’: The need to address the ongoing digital divide to achieve improved health and well-being benefits for older rural Australians. Australas J Ageing. 2017;36(4):262-3. [CrossRef]
- Warr D, Luscombe G, Couch D. Hype, evidence gaps and digital divides: Telehealth blind spots in rural Australia. Health (London). 2023;27(4):588-606. [CrossRef]
Figure 1.
PRISMA flow diagram of screening and selection process.
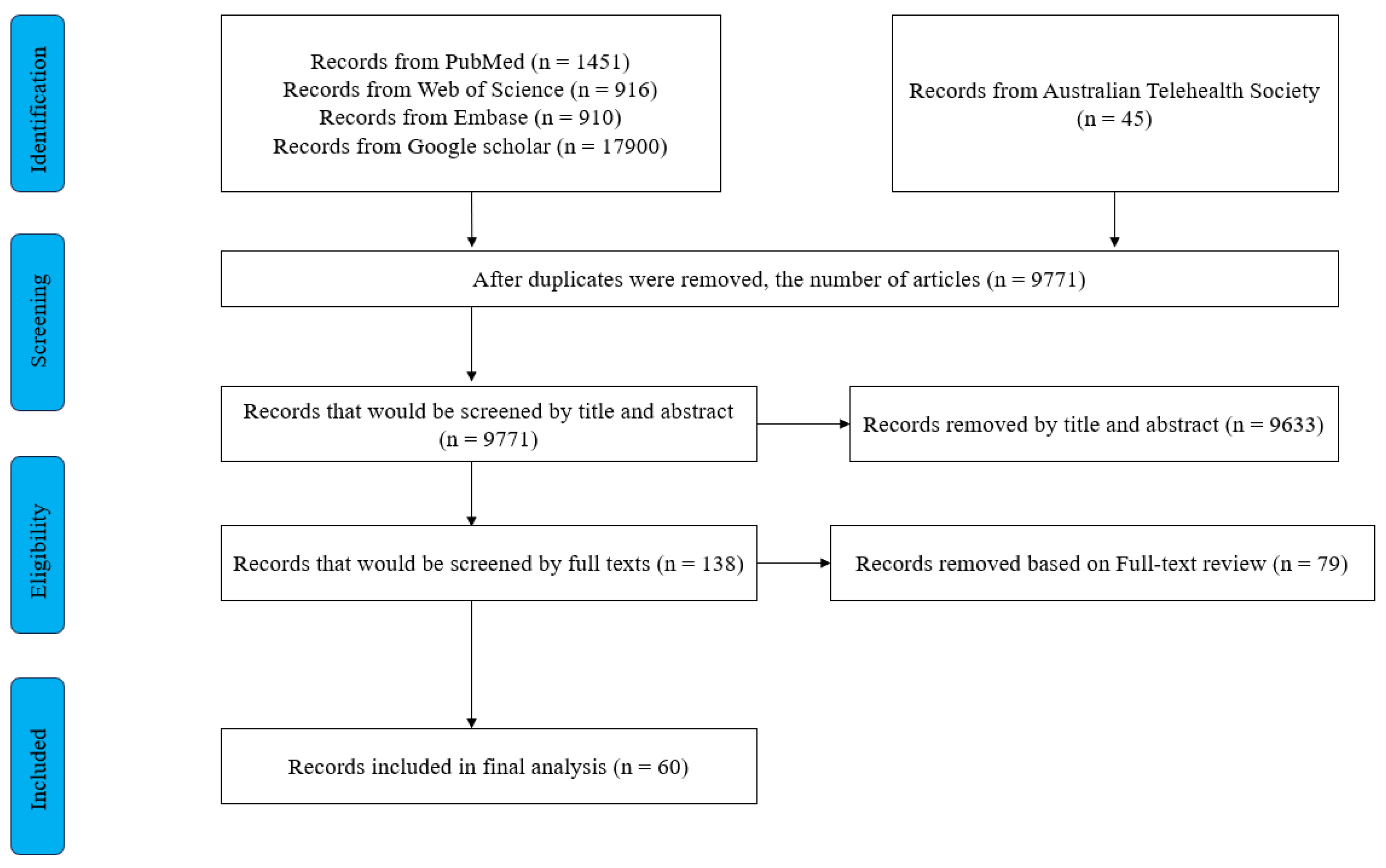

Table 1.
Summary of findings derived from the included studies in the review.
| Health System Building Blocks (Number of Relevant Studies) | Populations (Number of Relevant Studies) |
Successes | Challenges |
|---|---|---|---|
| Governance and stewardship for health systems [3] | General [3] | n/a | 1. The overall health governance was fragmented [49]. 2. Lack of transparency and consistency across policies [58]. 3. lack of regulatory control over information on the online platform [56]. |
| First Nations peoples [1] | n/a | 1. First Nations peoples’ health problems have not been addressed at a national level [49]. | |
| CALD [1] | n/a | 1. lack of regulatory control over information on the online platform [56]. | |
| Health workforce [6] | General [4] | 1. Online training has been implemented [57]. 2. DHIs could help overcome staff shortages [40]. 3. Skill improvements in using DHIs stimulated by Covid-19 [40]. |
1. Current funding for health workers could not satisfy the extra needs brought by DHIs [68]. 2. No appropriate technology to use [40,68]. 3. Training affordability and extra workload [40]. 4. Hard to establish familiarity with new technologies [68,82]. |
| First Nations peoples [2] | 1. Enable vulnerable health workers access to patients during the COVID-19 [71]. | 1. Inadequate rural health workforce [33,71]. 2. Extra workload and low translation skills [71]. |
|
| Health Information System [7] | General [4] | 1. Current HIS improved efficiency and expanded the data source [27,75]. 2. Current HIS increased the accessibility for both patients and healthcare providers [39]. |
1. Real-time sharing of health information function was unavailable in some areas [57]. 2. Some disadvantaged patients could not access some HIS [39]. |
| First Nations peoples [3] | 1. Current HIS ensures healthcare providers access good quality data [38,80]. 2. Substantial improvements in providing PHC have been led [33]. |
1. The lack of connectivity between HISs across different services is challenging [33]. 2. Staff perceived difficulties in operating the HIS, then caused negative results [80]. 3. Inappropriate tools are used in operating HIS [38]. 4. Updating the current HIS is difficult [38]. |
|
| Medicine, Vaccines, diagnostics and technologies [14] | General [3] | 1. Some technologies were considered to assist clinical practice [75]. | 1. Low affordability of technologies for some healthcare providers or patients [41,82] |
| First Nations peoples [4] | n/a | 1. low accessibility and utilisation of telehealth hardware [49,66,71]. 2. The system-level uptake of telehealth technologies is slow [49]. 3. In rural areas, the quality of some current technologies is low [80] 4. Some technologies do not have some essential functions [66]. 5. Current technologies seldom specialised for clinical purposes [49]. |
|
| CALD [7] | 1. Current mental diagnosis delivered by DHIs is more accurate and stable [59]. | 1. Low availability or low quality of hardware devices to apply DHIs [35,46,63,64,77,81]. | |
| Health service delivery [51] | General [15] | 1. DHIs increased the overall efficiency of PHC delivery [28,58,60,75]. 2. DHIs improved patients’ access to PHC, especially for disadvantaged patients or those in the COVID-19 context [27,50,69]. 3. DHIs have good coordination with other levels of care and organisations [50,58,69]. 4. DHIs could support a wide range of health services, indicating high comprehensiveness [27,37]. 5. The use of DHIs in rural/remote Australia is increasing [31]. 6. Patients received quality PHC delivered by DHIs [27,50,76,84]. |
1. DHIs could only be tools to support treatments [76]. 2. The utilisation of more effective DHIs is low [41] 3. For elderly patients, the utilisation of DHIs is low [44]. 4. DHIs presented ineffectiveness in some PHC areas [44,47,68]. 5. Concerns raised on DHIs due to the fear of addiction [76]. |
| First Nations peoples [6] | 1. DHIs improved rural access to PHCs [36,45,80]. 2. Another DHI improved the quality-of-service delivery [45,51]. 3. Online resources were widely used [34]. 4. DHIs improved First Nations peoples’ efficiency in accessing PHC services [71]. |
1. DHIs could not cover some emergency care [12]. 2. Challenges in accessibility caused by language or knowledge barriers still exist [51,71]. 3. The utilisation and independence of DHIs are low [54,71]. |
|
| CALD [22] | 1. DHIs successfully improved the efficiency of health service delivery [81]. 2. The overall access to health services was improved [29,42,48,78,79,81] 3. DHIs contributed to the success of health communication programs [46,53]. 4. Current DHIs were helpful in assisting administrative work [79]. 5. Except for searching for health information [56], the utilisation of DHIs among CALD people is low [25]. 6. DHIs can help CALD people overcome the language barrier [43]. 7. Characteristics of DHI, including privateness and confidentiality, showed high person-centeredness [29]. 8. Some online health education programs gained acceptance from CALD communities [43,70]. |
1. Technical difficulties became barriers to accessibility [48] 2. Language barrier still exists [42]. 3. DHIs could be low-quality or ineffective in multiple situations [42,55,56,64,81]. 4. The low translation quality is especially critical for CALD people [63,67]. 5. Low-quality online health information caused negative effects [43,61,83]. 6. Due to problems with interpreters or English sources of online health information in the predominant position, the language barrier has not been completely overcome [26,43,65,74,77] 7. There is a challenging trend of DHI utilisation in CALD communities [26,62,83]. 8. Some CALD communities with high health demands have been ignored [77]. |
|
| Community engagement [10] | First Nations peoples [5] | 1. However, some successful community engagement has been achieved by DHIs tailored for First Nations peoples [32,51,52]. | 1. Digital GP apps are designed in a way that is against community values and reduces community involvement [36]. 2. The coordination with different social groups needed to be improved [66]. |
| First Nations peoples [6] | 1. Successes in involvement and empowerment were emphasised on a tailored program [46]. 2. Social media apps provided a platform to cooperate with local community leaders [77]. |
1. Some DHIs failed to satisfy the cultural needs of CALD people [30,63,72]. |
* Tables may have a footer.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



