
Submitted:
11 March 2025
Posted:
11 March 2025
You are already at the latest version
Abstract
Health disparities among populations across geographic regions, demographic and socio-economic groups are well documented; however, ecological studies which visually demonstrate health disparities associated with structural racism among racialized populations are limited. The purpose of this study was to examine low birthweight (LBW) as a measurable indicator of disproportionate health impacts across three race/ethnicity groups- non-Hispanic Black, Hispanic and non-Hispanic White in the United States. We begin by providing the contextual background of structural racism through a literature review, and then more specifically, we examine LBW as a selected health indicator characterized with a socio-biological pathway of structural racism leading to health disparities. To visualize this pathway of impacts, publicly available US County Health Ranking data for LBW, at the county level in two US States, Tennessee and Ohio, were analyzed to uncover ecological (area-based) outcomes. Significant correlation and scatter plots provided evidence of LBW as a racially sensitive health indicator associated with impacts of structural racism. These were further notable through examination of mediating socio-economic (e.g. race/ethnicity, income, education, and employment) and environmental factors such as housing issues as well as other underlying health conditions. Our case study provided a window for more fully visualizing disparity across Non-Hispanic Black, Hispanic, Non-Hispanic White populations as demonstrated by the prevalence of LBW and its mediating factors at the county level. Potentially important policy implications are identified through our study findings that are salutary and/or reductive for addressing impacts of structural racism.
Keywords:
Strutural racism
; determinants of health disparity
; low birthweight
1. Background
Health inequities, the differences in health outcomes between populations are avoidable and preventable, and are therefore unjust [1]. The evidence of extant disparities in health indicators, including morbidity and mortality among populations across geographic regions, demographic groups and socio-economic factors has been officially reported in the United States (US) [2] and Canada [3,4] in the North American context. Whereas both countries are grappling with the extant structural racism, the research on the associations of health disparities in Canada [5,6]; and particularly in US life expectancy at the county level [7] among racial-ethnic groups, has been reported. More specifically, several studies have reported racial discrimination against Black and African American people leading to health disparities embedded in a structural manner in the US society [8,9,10,11,12]. Structural racism refers to the totality of ways in which societies embody racial discrimination through mutually reinforcing systems of housing, education, employment, earnings, benefits, credit, media, health care and criminal justice, while these patterns and practices in vogue at the system level, in turn, reinforce discriminatory beliefs, values and distribution of resources [10]. A recent cross-disciplinary scoping review of literature has comprehensively presented theoretical underpinning and impacts of structural racism associated with health disparities across populations [13]. Yet, visualization of evidence from ecological links to indicators of structural racism associated with health disparities among racialized populations has been limited.
Birth outcomes such as low birthweight (LBW) have been one of the components to serve as barometer of health system performance [14] and are generally reported as indicators of poor infant health status of populations. Birth outcomes are significant risk factors for infant mortality, reflecting a serious public health concern that could have severe lifelong health impacts in terms of quality of life and costly societal burden [15,16]. In high-income North America, the US ranked the highest prevalence of LBW, 8.26% (95% UI, 8.15–8.36), as reported [14]. It is well documented in the US that racial disparities in birth outcomes are attributed to interpersonal and structural racism, but not due to other causes such as discrete genetic differences [15,17,18]; yet the visualization of such disparities at the area-based ecological level has not been evidently demonstrated in the literature to inform the local area-level policy planning for reparative changes.
An overwhelming body of empirical evidence shows, there exists an association of local area (neighborhood) adversity factors such as poverty, segregation, crime, and eviction rates with poor infant outcomes [10,19]. Pervasive socioeconomic differences occurring across race/ethnic subgroups are associated with resulting measures of disadvantage in birth outcomes, which continue from childhood to adulthood [20]. The physical, social, and political environments which are currently characterized through the contemporary social determinants of health are fundamentally rooted in structural racism [19]. For example, Black mothers are reported typically twice as likely to give birth to a LBW infant than their White counterparts; this Black-White disparity is due to impact of interpersonal or structural racism along with other risk factors such as mother’s age, education, smoking, access to prenatal care, etc. [15,17,21].
One of the challenges of studying effects of structural racism on health is identifying appropriate geographical units for aggregation of the data to demonstrate its area-based impacts [16]. Thus, research to confirm the role of racism and to evaluate trends in the impact of racism on health outcomes by geographical areas has been hampered by the challenge of measuring racism [15]. In the empirical measurement of structural racism with its complex, insidious, and ecologic nature, residential segregation has been used as key exposure factor and is highly predictive of a range of adverse birth outcomes [22], whereby three area-based measures of racial/ethnic composition make up as an indicator for residential segregation: the proportion of residents who are non-Hispanic Black, the proportion of residents of color, and the Index of Concentrations at the Extreme (ICE). The ICE measure captures geographical social polarization by looking at extremes of privilege and deprivation within a given neighborhood or census tract. In addition, exploitative revenue generation (the practice of using excessive municipal fines and fees) have disproportionate impact on residents of color and are associated with preterm and LBW. [22] The discrete residential segregation in certain areas over time could potentially turn into area-based ecological diffusion of its impacts across a geographic jurisdiction. Therefore, we hypothesized that a measurable indicator can be identified at the county level for visualizing ecological impacts of structural racism in health outcomes such as LBW such that the ecological evidence can be used in local level planning for reparative policy changes.
Thus, thepurpose of this study is to examine and visualize ecological distribution of low birthweight as an indicator of health disparity that shows a component evidence of structural racism across the populations of three race/ethnicity groups acros counties of Tennessee and Ohio states. Additionally, we examine some of the related multidimensional mediating factors at the county level within the two states.
2. Materials and Methods
The methodological framework of this study was developed simply to visualize how the structural racism extant theoretically in several studies reported in the literature actually manifests into area-based ecological vivid reality in the racialized population of African American people compared to other racial groups of non-Hispanic White people and Hispanic people in the US. We undertook LBW which is considered sentitive of being impacted by structural racism as its selected measurable indicator. As described below, we first reviewed peer reviewed literature found through a search in order to provide a contextual background for our study, then followed by analysis of LBW rate data across counties of two States.
2.1. Literature Review
We carried out a review of peer reviewed health science literature published from 2000 to 2023 that were indexed in PubMed® online literature data-base hosted by US National Library of Medicine, comprising more than 37 million citations for biomedical literature from MEDLINE, life science journals, and online books. The literature review was intended to contextualize the US background of structural racism as a determinant of health disparity measurable by low birthweight as a selected health indicator and the socio-biological pathways of structural racism associated with health disparities. Using three specific search terms, “Low birthweight”, “United States”, “Structural racism” in the PubMed platform, we found a total of 21 directly relevant peer reviewed articles after removing duplicate or non-relevant entries. We extracted strikingly relevant excerpts from the full text of the selected articles and searched for relevant themes to identify socio-economic and politico-legal inequity factors, and mediating factors associated with low birthweight resulting from structural racism so as to guide the next steps in our study, i.e., data analysis and interpretation. Our review of literature was intended to highlight the background context of the pervasive impact of structural racism systemically on adverse birth outcomes, particularly low birthweight among Black populations in the US.
2.2. Ecological Health Disparity Analysis of County Level Data
Using publicly available US County Health Ranking data for the year 2021 extracted from the 2023 Annual Report of the Wisconsin University Population Health Initiative (URL Link for 2023 County Health Rankings National Findings Report - County Health Rankings & Roadmaps: https://www.countyhealthrankings.org/findings-and-insights/2023-county-health-rankings-national-findings-report), an ecological health disparity analysis was carried out for area-based case-studies of two selected States, one State in the deep South and another in the North, respectively, Tennessee and Ohio. The two states represent two different paths in the history of racial slavery in the US— Tennessee as a slave state deeply embedded in the Southern plantation system and Ohio as a free state with abolitionist influences. However, both states grappled with racial discrimination long after slavery was formally abolished. The two states provide appropriate representative samples for structural racism in the US. While the first author explored and conducted this research while being stationed in Tennessee as a visiting scholar to the US, he also had the opportunity to make location visit to Ohio, providing him a first-hand sense of the current geography and populations of both states during the time of this study in the fall 2023. The charts on the LBW data reported for all counties of the two States, measured in proportion of livebirths were plotted against the proportions of non-Hispanic Black, Hispanic and non-Hispanic White population by county to examine trends associated across the two variables. Correlation analyses using SPSS software were conducted between LBW and the proportion of three racial-ethnic groups and selected other indicators that were hypothesized to have some link with the structural racism. Low birthweight is considered as a racism sensitive health indicator, with its socio-economic and politico-legal policy inequities and mediating factors (e.g., race/ethnicity, income, education, and employment) and environmental factors (e.g., severe housing problems). We used the theoretical framework of structural racism with respect to measuring its area-based ecological impact on LWB across counties, wheras the area-based racial segregation as reviewed in the literature [22,23] would be localized within certain parts of the county. Thus, we were able to visualize disparity in the prevalence of LBW among non-Hispanic Black, Hispanic, non-Hispanic White populations across the whole counties in the State. Finally, we have drawn potential policy implications for reparative change based on our findings for addressing the impacts of structural racism.
3. Results and Discussion
3.1. Literature Review for Contextual Background of Low Birthweight as Pathway for Structural Racism
We reviewed the health science literature published from 2000–2023 indexed in PubMed to contextualize the US background of structural racism as a determinant of health disparity measurable specifically by low birthweight (LBW) and its socio-biological pathways of structural racism associated with health disparities. We found a total of 21 directly relevant peer reviewed articles after removing duplicate or non-relevant entries. We extracted strikingly relevant excerpts from the full text of the selected articles and searched for relevant thematic factors that we identified as influencing factors or having a mediating effect on LBW and resulting from structural racism. We tabulated these factors into a summary table (Table 1) to guide the next steps in data analysis and interpretation for this study.
The included studies (Table 1) highlight the pervasive impact of structural racism on low birthweight and other adverse birth outcomes, particularly among Black populations in the US.
Furthermore, five from the above-stated 21 selected US studies identified state or county level polices facilitating structural racism [15,17,18,19,22,29,33] that were negatively associated with LBW requiring public policy reform, while positive impact of policies were also reported [18,33] on Safe Babes, Safe Mom and Paid Parent Leave supporting the birthing mothers. Other state and county level policy related causes of structural racism negatively impacting birth weights reported in the literature include multiple level structural racism [21] and county-level eviction rates [36]. A Minnesota study showed that higher risk of LBW for US-born Black compared to their White counterparts was explained by multidimensional structural racism of various typologies based on residential, income, education, employment, home ownership and criminal justice inequities [24,25], while inequities in three commonly known determinants of health- education, income and employment associated with structural racism resulting in LBW as birth outcome were also reported [26]. Residential segregation typology of this association was also reported by other studies as well [23,36]. Criminal justice inequity was reported as a typology of structural racism associated with LBW by four studies [16,24,26,27]. Heteropatriarchal structural sexism were identified to explain structural racism associated with LBW in two studies [28,30]. The reported vulnerability factors of birthing mothers subject to impacts of structural racism on the birth outcome of LBW include their mental distress [27,34], life course impact such as Adverse Childhood Experiences (ACEs) and Adverse Adult Experiences (AAEs) [31]. The study that considered the status of prenatal mental health and substance use [34] indicated important implications for pregnant women as well as their developing children, and found positive associations between life course impact such as maternal childhood adversity (i.e., Adverse Childhood Experiences-ACEs) with prenatal mental health and substance use outcomes (e.g., severe anxiety, mood dysregulation measured by Mood Disorder Questionnaire- MDQ, marijuana use) among urban, low income, mostly minority women such as Black women. Further reports indicated the life course perspective with poorer birthing outcomes among Black people [31]. This originated from heightened exposure to stressors as adverse experiences early in life followed by cumulative exposure to the stressors later in life over time. Experiences of Discriminations (EoDs) at various settings such as school, job hiring, work, housing, medical care, sales & service, banking & mortgage, and in public settings and police or courts could impact on the psychophysiological status of pregnant women, leading to impairment of vasodilation during pregnancy [32]. This study found that impaired vasodilation during pregnancy as a potential mediating factor in the hypertension-related health disparities between African American women and European American women, and exposures to discrimination were associated with higher total peripheral resistance during pregnancy in the former with potential impact on the birth weight of their offspring [32].
While the report that Black mothers had dramatically higher rates of very low birthweight (VLBW) than White mothers [35], it was also reported that between 1989 and 2019 the relative odds that first births were VLBW increased by roughly 16 percent (from 0.030 to 0.034) for Black mothers and 13 percent (from 0.010 to 0.012) for White mothers. In addition, they showed that the maternal age-specific rate of VLBW had a widening gap with higher rates with the increasing age of the Black mothers compared to White mothers in 2017–2019. In summary, the most current literature provides the framework for using LBW as a lens for examining health disparities such that LBW is characterized as a socio-biological pathway of structural racism. The framework necessitates visualization of this health disparities at the ecological level as vivid evidence of the impact of structural racism.
A pictorial chart model (Figure 1) was derived, summarizing the indicators of structural racism identified from the literature review, visualizing how it shows up in the characteristics of the population, how it impacts on socio-economic and politico-legal inequities and mediating factors which, in turn, lead to health disparity outcome such a low birthweight. The positive (+ve) mediatring factors are salutary to health equity, whereas negative (-ve) once are associated with health disparity.
3.2. Ecological Case-Study of Two US Counties
County level ecological socio-demographic and health characteristics of Tennessee and Ohio are summarized in Table 2. Tennessee in the South and Ohio in the North in the US are fairly comparable states in their demographic composition, despite the former being smaller than the latter in population size. The former has also a relatively larger proportion of racialized populations, especially the non-Hispanic Black and has relatively lower status in health indicators such as birth outcomes, life expectancy, chronic disease especially diabetes that are generally reported to be linked with the impacts of structural racism. Especially among birth outcomes, LBW, can be considered as a case example indicator of health impact of structural racism in its local-area based ecological analysis by counties, in both States showing certain distribution patterns as presented in scatter plots (Figure 2). In both States, the rate of LBW was lower in the counties that have lower proportion of non-Hispanic Black populations and increased with the proportion of that population within the county. Also in both States, the reverse pattern of lower LBW rate was observed with the increasing proportion of non-Hispanic White population, while Hispanic population did not show any significant pattern. These plots were consistent with the Pearsons correlations of LBW rate, which were significantly positive with the proportion of non-Hispanic Black population (P < 0.01) and significantly negative with the proportion of non-Hispanic White population (P < 0.01), whereas Hispanic population was statistically non-significant in both States. It must be noted that non-Hispanic Black population had suffered from extreme racial discrimination with the historical enslavement, followed by a series of racially discriminatory policies as illustrated in Figure 1, and their health outcomes such as LBW had been severely impacted by the socio-economic and politico-legal policy inequities and associated mediating factors. On the other hand, Hispanic population might not have been subjected to racial discrimination practices that were of the same type or severity as the former. We suggest that this would help explain the difference in the health outcomes between the two populations.
Using Pearson’s correlation analysis, further exploration of selected measurable indicators that have been generally considered examples of mediating factors associated with the impacts of structural racism (Table 2) showed that Education (Highschool completion in TN, Highschool graduation in OH, school segregation), Income (Income inequality, Median household income, Children s poverty, Unemployment, Food insecurity, and Health (Life expectancy, Frequent physical stress, Diabetes prevalence, HIV prevalence) were all significantly correlated towards disadvantageousness for LBW. The selection of these measurable indicators for correlation analysis as presented in Table 3 was an opportunistic exercise, as the indicators were intuitively selected based on their relevance to the findings of literature review with respect to impact of structural racism on the selected health outcome, LBW, from the available indicators in the database used.
Our ecological analyses of LBW demonstrated through our case studies provide visualized evidence of extant health disparity, particularly between non-Hispanic White and non-Hispanic Black populations to the disadvantageousness of the latter. We were able to identify the nature of health disparity structurally embedded in the influencing factors measurable at the county level as elucidated by the racially disproportionate ecological distribution of LBW. Particularly, our case studies support the notion that residential segregation is a reflection and reinforcement of structural and institutional racism resulting from racialized and economically segregated neighborhoods [10,23,24].
Mehra et al. introduced five distinct modes of operationalizations of segregation that could explain its impact at the county level [23]. These five modes that could be calculated for indexing cross micro-level spatial units (e.g., neighborhoods) within macro-level spatial units (e.g., regions), are comprised of Exposure—the degree of neighborhood isolation or interaction of minority with majority groups; Evenness—the degree to which each neighborhood has the same proportion of minority and majority members for even distribution; Clustering—the degree to which minority neighborhoods are contiguous and tightly clustered; Concentration—the degree to which minority members occupy a small proportion of the total area of a region; and Centralization—the degree to which a minority group is centrally located within a region. These modes of segregation could explain how the proportions of LBW rate are positively and significantly correlated with the proportion of non-Hispanic Black population and negatively correlated with non-Hispanic White population, in both states studied. However, interestingly in our case studies, the Hispanic population did not show these patterns of significant health disparity at the ecological level, even though they could have been subjected to county-level exploitative revenue generation through fees and fines as described by Davies et al. [22]. Yet, it is important to note that Hispanics have not previously been reported to have these five modes of segregation, and the racial discrimination against them was not the same in term of its form and severity as in Hispanic Black population to cause similar impact at the ecological level, and this may be an area for future study.
The disproportionate representation of Black people in the U.S. penal system demonstrates longstanding mechanisms underlying inequities in incarceration (dating back to Colonialism) and health at the population level [10].The ecological concentration of incarceration measured as county level prison rates has been reported to be associated with racial disparities in adverse birth outcome such as LBW mediated through two pathways- community level mental-stress and reduced health care access [27].
Inequity in education has been identified in the literature [24,26], and constitutes one determinant of the multidimensional structural racism typology which could be a factor explaining birth inequities leading to higher risk of LBW for US-born Blacks [24]. This further resonates with our county-level results showing significant correlations of LBW with degree of High School completion in Tennessee, High School graduation in Ohio and degree of school segregation in both States as valid indicators of education (Table 2). Likewise, our background literature review for conceptualization indicated income, poverty and employment as three other determinants of the multidimensional structural racism typology, explaining higher risk of LBW among Blacks [24,25,26,29]. These findings were consistent with significantly positive correlations of LWB with income inequality (negative correlation with median household income), child poverty and unemployment at the county-level in both the States (Table 2).
Closely related with the residential segregation, homeownership has been well documented as one of the major components embedded in the structural racism in the US leading to health disparity such as impacting negatively on birth outcomes in the Black population [9,19,25,26]. This pattern of relationships has been consistently elucidated by the significant correlations of LBW negatively with homeownership and positively with severe housing problems at the county level in both the States.
Some of the factors intrinsic to the birthing Black mothers reported in the literature influencing their disproportionate rate of LWB include life course impacts of Adverse Childhood Experiences (ACEs) and Adverse Adult Experiences [31,34], prenatal mental health and substance use [34], maternal age at first births [35], as well as the epigenetic legacy of enslavement and ongoing cultural loss [21], which are all factors that are structural in nature. Furthermore, significant correlations of LBW found with other selected health status indicators- such as being negatively correlated with life expectancy, and positively with frequent physical distress, HIV prevalence and food insecurity at the county level in both States could indicate their respective association embedded as factors mediating structural racism, similar to those of community level mental stress and reduced health care access reported [27].
Allostatic load. In the recent scoping review, it was surmised in a recent study [13] that Black Americans suffered from chronic stresses on ongoing basis, bearing higher allostatic load as compared to White individuals. The concept of allostatic load, first introduced by McEwen and Stellar [37], is the physio-pathological impact of wear and tear resulting from chronic stresses on a number of organs and tissues that can predispose the organism to disease. It is crucial in understanding health inequalities, particularly in the context of our study on LBW among non-Hispanic Black women compared to their non-Hispanic White counterparts. It refers to the physiological cost of chronic exposure to fluctuating or heightened neural and neuroendocrine responses due to repeated or chronic environmental stressors [38]. Ethnicity has been associated with varying levels of allostatic load, with Black Americans generally exhibiting higher levels than Whites [38], while everyday racial discrimination, as well as institution-specific structural discrimination, differentially affect allostatic load among Black women, with higher levels reported in those experiencing greater perceived racial or social adversities throughout their lives [38]. While general population studies consistently show that low socioeconomic status, impoverished neighborhoods, and low educational attainment increase allostatic load through the mechanism of neuronal and hormonal responses to the chronic stresses caused by those factors, the evidence of specific impact of allostatic load on birth outcomes is limited, warranting further investigation to establish a clear understanding of the associated multidimensional factors.
Finally, state or county-level policies reported in our review as having salutary impact against structural racism including aid to needy families, housing assistance, Medicaid, minimum wage, earned income tax credits [17], political representation of racialized minorities [19], the Safe Babies, Safe Moms initiative [18], paid parental leave [33], community building as well as culturally centered care [21] could have reparative impacts on health disparity measured by the indicator such as LBW. On the other hand, implementation of these policies has the potential to not only positively impact but at the same time reinforce structural racism, such as the case of racialized police use of force [16], reductive racial bias by the state [15], exploitative revenue generating county-level fees and fines (Davis et al., 2023), county-level housing eviction rates [36]. As such, policy implementation could have reductive association leading to higher LBW rate in counties with higher proportion of racialized population.
Some of the limitations of our study include the list of variables included in the correlations analysis of LBW was not exhaustive enough to draw the comprehensive web of mechanisms through socio-economic and politico-legal policy inequity pathways and mediating factors of structural racism impacting on racial health disparity in LBW. Our analyses were intended to simply examine individual association of the variables without exploring their interdependence. A robust analysis of desirable data involving structural equation modeling would be a future aspirational exercise for deriving comprehensive results on the mechanism of the whole system of structural racism. In summary, structural racism creates a web of interrelated factors including socioeconomic inequities, reduced healthcare access, residential segregation, chronic stress, and biological mechanisms that collectively contribute to the higher incidence of LBW among non-Hispanic Black mothers. Addressing this multi-factorial issue requires comprehensive reparative policy changes for interventions aimed at reducing racial disparities and promoting health equity.
4. Conclusions
Addressing health disparities associated with the multidimensional factors embedded in structural racism in a society requires multifaceted policy interventions, community-level changes, and systemic reforms targeting the various dimensions of structural racism, including labor markets, residential segregation, income inequality, and political representation. Effective solutions must also consider the historical context and cumulative stressors affecting marginalized communities through intergenerational trauma leading to allostatic load. The background literature review and ecological analysis of LBW in our case studies generally resonated with each other in providing evidence of extant health disparity associated with structural racism, particularly between non-Hispanic White and non-Hispanic Black populations to the disadvantageousness of the latter. More so, racially disproportionate county-level distribution of LBW along with various influencing and mediating factors elucidate the nature of health disparity structurally embedded in US society. Racially disproportionate ecological concentration of the rates of residential segregation, incarceration, inequities in education, income and employment, some measurable birthing mother traits, racially biased policies at the state or county level constitute the components of structural racism that lead to disparity in health such as measured in LBW and need policy change considerations. In summary, structural racism creates a web of interrelated factors including socioeconomic inequities, reduced healthcare access, residential segregation, chronic stress, and biological mechanisms that collectively contribute to the higher incidence of low birthweight among the non-Hispanic Black mothers. Further research for modeling empirical evidence at the ecological level using more exhaustive lists of influencing and mediating factors is needed to draw comprehensive mechanisms and pathways. Structural racism impacts health disparity measured by LBW as a marker such that the policy implications for change can be formulated to the reparative advantage of the affected county areas, especially those counties that have higher proportion of non-Hispanic Black population. Addressing health disparities as impacts of structural racism requires multifaceted policy interventions, community-level changes, and systemic reforms targeting the various dimensions of structural racism, including labor markets, residential segregation, income inequality, and political representation. Effective solutions must also consider the historical context and cumulative stressors affecting racialized communities.
Authors Contributions: This paper was an outcome of the research conducted by D.P.R., the PI and first author in the capacity as the Fulbright Canada Research Chair in Race and Health Policy at the University of Memphis, Cecil C. Humphreys School of Law, Memphis, Tennessee, United States during his scholarly visit term in 2023. Specific author contributions are: Conceptualization: D.P.R. and K.T.S.; Data curation and Analysis: D.P.R.; Funding acquisition: D.P.R. and K.T.S.; Literature search/Investigation/Methodology: D.P.R.; Project Administration: D.P.R. and K.T.S.; Resources: D.P.R. and K.T.S.; Validation: D.P.R., L.L.L., C.L.F. and K.T.S.; Data visualization: D.P.R.; Writing-original draft: D.P.R.; Writing—review & editing: D.P.R., L.L.L., C.L.F. and K.T.S. All authors have read and agreed to the published version of the manuscript.
Funding
The core competitive funding for Fulbright Canada Research Chair’s scholarly visit to the Cecil C. Humphreys School of Law, University of Memphis was sponsored by the Fulbright Canada Foundation. Other funding support include visit to Fulbright Enhancement Seminar in Cleveland, Ohio sponsored by United States Fulbright Program. Logistic support was provided by the University of Memphis School of Law.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
No new data collected from any subjects.
Data Availability Statement
1. We reviewed peer reviewed articles found in our search at PubMed. 2. We used publicly available US County Health Ranking data for the year 2021 extracted from the 2023 Annual Report of the Wisconsin University Population Health Initiative (URL Link for 2023 County Health Rankings National Findings Report - County Health Rankings & Roadmaps: https://www.countyhealthrankings.org/findings-and-insights/2023-county-health-rankings-national-findings-report.
Acknowledgments
The first author thankfully acknowledges the support of Prof. Shanthi Johnson (Vice-President for Research and Innovation, University of Windsor), Dr. William Osei (Advisor, Emotional Well Being Institute Canada) and (Wendy Kebwaro, Executive Director, BCCDC) for my nomination for Fulbright Canada Research Chair program and collegial cooperation and logistic support of Faculty and Staff at the Cecil C. Humphreys School of Law, University of Memphis, including Daniel Kiel, Jodi Wilson, Daniel Schaffzin, LaVaire Lockhart, Karol Landers, Christopher Whitehead and Ryan Jones.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Whitehead, M. The concepts and principles of equity and health. Int J Health Serv. 1992, 22, 429–445. [CrossRef]
- US CDC. CDC Health Disparities and Inequalities Report United States, 2011. Centers for Disease Control and Prevention, US Department of Health and Human Services, Atlanta, GA.
- PHAC. Key Health Inequalities in Canada: A National Portrait. Ottawa: Public Health Agency of Canada. 2018. Available online: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/science-research/key-health-inequalities-canada-national-portrait-executive-summary/key_health_inequalities_full_report-eng.pdf.
- Rasali, D.; Kao, D.; Fong, D.; Qiyam, L. Priority Health Equity Indicators for British Columbia: Preventable and Treatable Premature Mortality. BC Center for Disease Control, Provincial Health Services Authority, Vancouver, B.C. 2019.
- Rasali, D.; Li, C.; Mak, S.; Rose, C.; Janjua, N.; Patrick, D. Correlations of COVID-19 incidence with neighborhood demographic factors in BC. Annals of Epidemiology 2021, 61, 17. [CrossRef]
- Brown, T.H.; Homan, P.A. Frontiers in measuring structural racism and its health effects. Health Serv Res. 2022, 57, 443–447. [CrossRef]
- GBD US Health Disparities Collaborators. Life expectancy by county, race, and ethnicity in the USA, 2000 19: A systematic analysis of health disparities. The Lancet, 2022, 400, 25–38. [CrossRef]
- Gee, G.C.; Ford, C.L. Structural racism and health inequities. Du Bois Review: Social Science Research on Race 2011, 8, 115–132. [CrossRef]
- Krieger, N. Discrimination and Health Inequities. Int. J. Health Services 2014, 44, 643–710.
- Bailey, Z.D.; Krieger, N.; Ag nor, M.; Graves, J.; Linos, N.; Bassett, M.T. Structural Racism and Health Inequities in the USA: Evidence and Interventions. The Lancet 2017, 389, 1453–1463. [CrossRef]
- Sweeting, J.A.; Akinyemi, A.A.; Holman, E.A. Parental Preconception Adversity and Offspring Health in African Americans: A Systematic Review of Intergenerational Studies. Trauma, Violence, & Abuse 2023, 24, 1677–1692. [CrossRef]
- Williams, D.R.; Lawrence, J.A.; Davis, B.A. Racism and Health: Evidence and Needed Research. Annual Review of Public Health 2019, 40, 105–125. [CrossRef]
- Rasali, D.P.; Woodruff, B.M.; Alzyoud, F.A.; Kiel, D.; Schaffzin, K.T.; Osei, W.D.; Ford, C.L.; Johnson, S. Cross-Disciplinary Rapid Scoping Review of Structural Racial and Caste Discrimination Associated with Population Health Disparities in the 21st Century. Societies 2024, 14, 186. [CrossRef]
- Global Nutrition Target Collaborators. Global, regional, and national progress towards the 2030 global nutrition targets and forecasts to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2025 Dec 21;404, 2543-2583. [CrossRef]
- Nguyen, T.T.; Adams, N.; Huang, D.; Glymour, M.M.; Allen, A.M.; Nguyen, Q.C. The Association Between State-Level Racial Attitudes Assessed From Twitter Data and Adverse Birth Outcomes: Observational Study. JMIR Public Health Surveill, 2020, 6, e17103. [CrossRef]
- Chegwin, V.; Teitler, J.; Muchomba, F.M.; Reichman, N.E. Racialized police use of force and birth outcomes. Social Science & Medicine 2023, 321, 115767. [CrossRef]
- Pearlman, J.; Robinson, D.E. State Policies, Racial Disparities, and Income Support: A Way to Address Infant Outcomes and the Persistent Black-White Gap? J Health Politics, Policy & Law 2022, 47, No. 2, April. [CrossRef]
- Patchen, L.; McCullers, A.; Beach, C.; Browning, M.; Porter, S.; Danielson, A.; Asegieme, E.; Richardson, S.R.; Jost, A.; Jensen, C.S.; Ahmed, N. Safe Babies, Safe Moms: A Multifaceted, Trauma Informed Care Initiative. Maternal & Child Health J. 2023, Nov. [CrossRef]
- Stanhope, K.K.; Kapila, P.; Umerani, A.; Hossain, A.; Salah, M.A.; Singisetti, V.; Carter, S.; Boulet, S.I. Political representation and perinatal outcomes to Black, White, and Hispanic people in Georgia: A cross-sectional study. Annals Epid. 2023, 87, 38–44. [CrossRef]
- Blumenshine, P.; Egerter, S.; Barclay, C.J.; Cubbin, C.; Braveman, P.A. Socioeconomic disparities in adverse birth outcomes: A systematic review. American Journal of Preventive Medicine 2010, 39, 263–272. [CrossRef]
- Bridgeman-Bunyoli, A.M.; Cheyney, M.; Monroe, S.M.; Wiggins, N.; Vedam, S. Preterm and low birthweight birth in the United States: Black midwives speak of causality, prevention, and healing. Birth 2022, 49, 526–539. [CrossRef]
- Davis, B.A.; Arcaya, M.C.; Williams, D.R.; Krieger, N. The impact of county-level fees & fines as exploitative revenue generation on US birth outcomes 2011 2015. Health & Place 2023, 80, 102990. [CrossRef]
- Mehra, R.; Boyd, L.M.; Ickovics, J.R. Racial residential segregation and adverse birth outcomes: A systematic review and meta-analysis. Soc. Sci. & Med. 2017, 191, 237e250. [CrossRef]
- Chantarat, T.; Van Riper, D.C.; Hardeman, R.R. Multidimensional structural racism predicts birth outcomes for Black and White Minnesotans. Health Serv. Res. 2022a, 57, 448-457. [CrossRef]
- Chantarat, T.; Mentzer, K.M.; Van Riper, D.C.; Hardeman, R.R. Where are the labor markets?: Examining the association between structural racism in labor markets and infant birth weight. Health & Place 2022b, 74, 102742. [CrossRef]
- Wallace, M.E.; Mendola, P.; Liu, D.; Grantz, K.L. Joint Effects of Structural Racism and Income Inequality on Small-for-Gestational-Age Birth. Am. J. Public Health 2015, 105, 1681–1688. [CrossRef]
- Sonderlund, A.L.; Williams, N.L.; Charifson, M.; Ortiz, R.; Sealy-Jefferson, S.; De Leon, E.; Schoenthaler, A. Structural racism and health: Assessing the mediating role of community mental distress and health care access in the association between mass incarceration and adverse birth outcomes. SSM - Population Health 2023, 24, 101529. [CrossRef]
- Everett, B.G.; Limburg, A.; Homan, P.; Philbin, M.M. Structural Heteropatriarchy and Birth Outcomes in the United States. Demography 2022, 59, 89–110. [CrossRef]
- Chambers, B.D.; Erausquin, J.T.; Tanner, A.E.; Nichols, T.R.; Brown-Jeffy, S. Testing the Association Between Traditional and Novel Indicators of County-Level Structural Racism and Birth Outcomes among Black and White Women. J. Racial and Ethnic Health Disparities 2018, 5, 966–977. [CrossRef]
- Nagle, A.; Samari, G. State-level structural sexism and cesarean sections in the United States. Soc Sci. 2021, 289, 114406. [CrossRef]
- Mersky, J.P.; Jeffers, N.K.; Lee, C.P.; Shlafer, R.J.; Jackson, D.B.; G mez, A. Linking Adverse Experiences to Pregnancy and Birth Outcomes: A Life Course Analysis of Racial and Ethnic Disparities Among Low? Income Women. J Racial & Ethnic Health Disparities 2023, June. [CrossRef]
- Christian, L.M.; Koenig, J.; Williams, D.P.; Kapuku, G.; Thayer, J.F. Impaired vasodilation in pregnant African Americans: Preliminary evidence of potential antecedents and consequences. Psychophysiology 2012, 58, e13699. [CrossRef]
- Karasek, D.; Raifman, S.; Dow, W.H.; Hamad, R.; Goodman, J.M. Evaluating the Effect of San Francisco s Paid Parental Leave Ordinance on Birth Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 11962. [CrossRef]
- Jasthi, D.L.; Nagle-Yang, D.; Frank, S.; Masotya, M.; Huth-Bocks, A. Associations Between Adverse Childhood Experiences and Prenatal Mental Health and Substance Use Among Urban, Low? Income Women. Community Mental Health Journal 2012, 58, 595–605. [CrossRef]
- Geronimus, A.T.; Bound, J.; Hughes, L. Trend Toward Older Maternal Age Contributed To Growing Racial Inequity In Very-Low-Birthweight Infants In: The US. Health Aff (Millwood), 2023, 42, 674–682. [CrossRef]
- Harville, E.W.; Wallace, M.E.; Theall, K.P. Eviction as a social determinant of pregnancy health: County-level eviction rates and adverse birth outcomes in the United States. Wiley-Health Soc Care Community 2022, 30, e5579–e5587. [CrossRef]
- McEwen, B.S.; Stellar, E. Stress and the individual. Mechanisms leading to disease. Arch Intern Med. 1993, 153, 2093–3101. [CrossRef]
- Guidi, J.; Lucente, M.; Sonino, N.; Fava, G.A. Allostatic Load and Its Impact on Health: A Systematic Review. Psychother. Psychosom. 2021, 90, 11–27. [CrossRef]
Figure 1.
A model illustrating structural racism impacting socio-economic, politico-legal and mediating factors leading to low birthweight as a health disparity in racialized population from, synthesized from the literature reviewed as presented in Table 1.
Figure 1.
A model illustrating structural racism impacting socio-economic, politico-legal and mediating factors leading to low birthweight as a health disparity in racialized population from, synthesized from the literature reviewed as presented in Table 1.
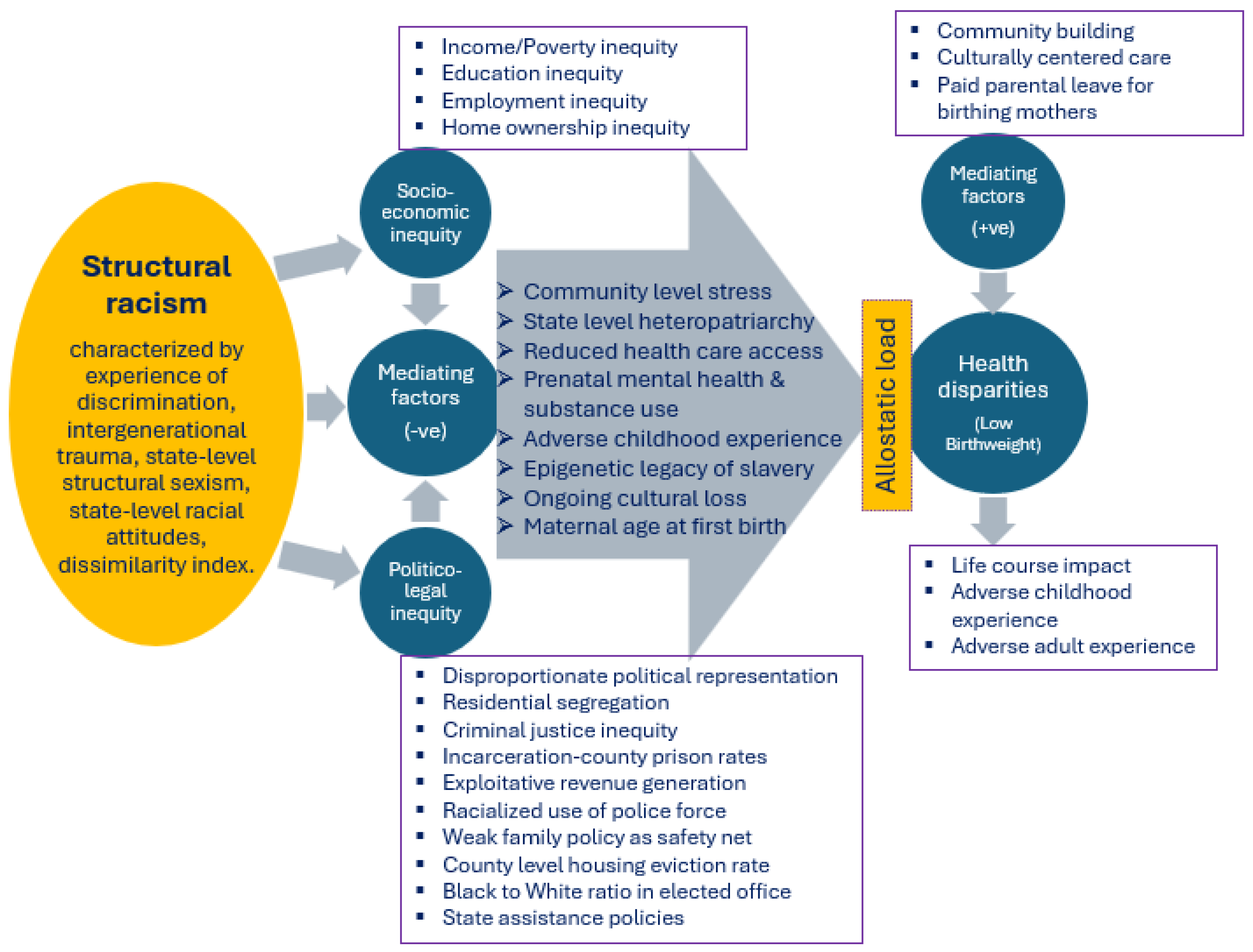
Figure 2.
Scatter plots and trend lines of low birthweight rate by the county’s proportion of non-Hispanic Black, Hispanic and non-Hispanic White populations in Tennessee (TN) and Ohio (OH) states.
Figure 2.
Scatter plots and trend lines of low birthweight rate by the county’s proportion of non-Hispanic Black, Hispanic and non-Hispanic White populations in Tennessee (TN) and Ohio (OH) states.
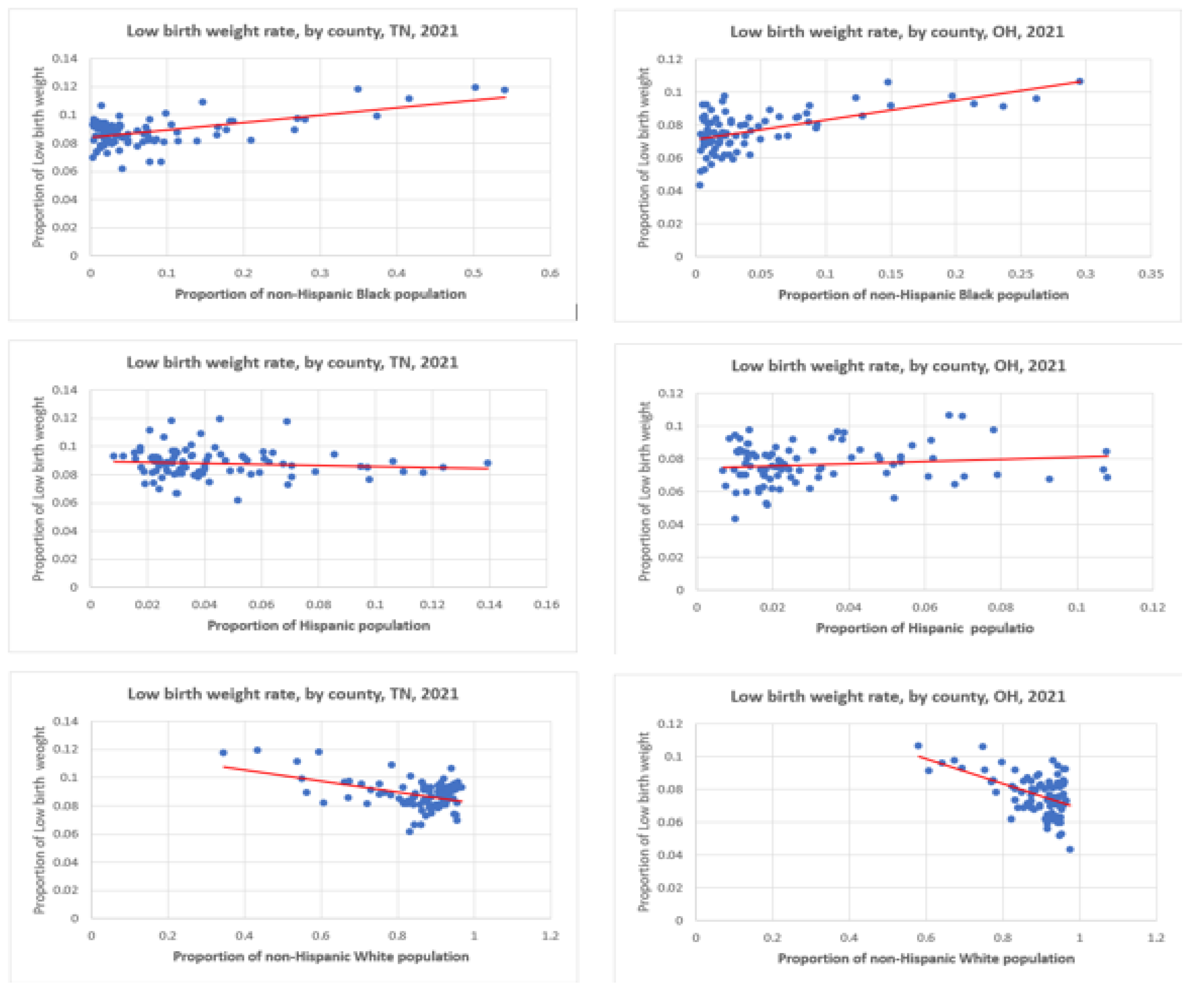

Table 1.
Summary of Included US Studies with Indicators of Structural Racism associated with ow Birthweight.
Table 1.
Summary of Included US Studies with Indicators of Structural Racism associated with ow Birthweight.
| Author(s) (Year of Publication) |
Indicator(s) of Structural Racism as Mediating Factors of Impact on Low Birthweight | Extract from the Relevant Findings |
|---|---|---|
| Chantarat et al. (2022a) |
|
|
| Chantarat et al. (2022b) |
|
|
| Wallace et al. (2015) |
|
|
| Sonderlund et al. (2023) |
|
|
| Everett et al. (2022) |
|
|
| Chambers et al. (2018) |
|
|
| Mehra et al., (2017) |
|
|
| Chegwin et al, (2023) |
|
|
| Nagle and Samari (2019) |
|
|
| Pearlman and Robinson (2022) |
|
|
| Nguyen et al. (2020) |
|
|
| Patchen et al. (2023) |
|
|
| Mersky et al. (2023) |
|
|
| Stanhope et al. (2023) |
|
|
| Bridgeman-Bunyoli et al. (2022) |
|
|
| Christian et al. (2021) |
|
|
| Davis et al. (2023) |
|
|
| Karasek et a. (2022) |
|
|
| Jasthi et al. (2022) |
|
|
| Geronimus et al. (2023) |
|
|
| Harville et al. (2022) |
|
|
Table 2.
Socio-demographic and health characteristics of Tennessee and Ohio, by county, 2021.
| Socio-demographic and Health Data | US States | |
|---|---|---|
| Ohio (n = 88) | Tennessee (n = 95) | |
| State total population | 11,780,017 | 6,975,218 |
| % non-Hispanic Black | 12.82 | 16.61 |
| % Hispanic | 4.32 | 6.11 |
| % Asian | 2.66 | 2.02 |
| % non-Hispanic White | 77.67 | 73.08 |
| Poor or Fair Health, % | 14.50 | 15.70 |
| Low Birthweight, % births | 8.56 | 9.13 |
| Teen Births, per 1000 live births | 20.90 | 27.17 |
| Life Expectancy, years | 76.52 | 75.33 |
| Diabetes Prevalence, % | 10.90 | 12.50 |
| Air Pollution Particulate Matter (PM2.5) | 8.9 | 7.6 |
| Severe Housing Problems, % | 13.06 | 13.43 |
Table 3.
Pearson’s corrections of low birthweight rate with three race/ethnicity groups and selected measures of structural racism in Tennessee and Ohio, 2021.
Table 3.
Pearson’s corrections of low birthweight rate with three race/ethnicity groups and selected measures of structural racism in Tennessee and Ohio, 2021.
| Tennessee | Ohio | |||||
|---|---|---|---|---|---|---|
| R | P-value | (n) | R | P-value | (n) | |
| Non-Hispanic Black | 0.557 ** | 0 | 95 | 0.584 ** | 0 | 88 |
| Hispanic | -0.102 | 0.326 | 95 | 0.127 | 0.239 | 88 |
| Non-Hispanic White | -0.459 ** | 0 | 95 | -0.512 ** | 0 | 88 |
| High School Completion | -0.202 * | 0.05 | 95 | 0.116 | 0.283 | 88 |
| High School Graduation | -0.203 | 0.054 | 90 | -0.401 ** | 0 | 88 |
| School Segregation | 0.249 * | 0.018 | 90 | 0.485 ** | 0 | 87 |
| Income Inequality | 0.263 * | 0.01 | 95 | 0.594 ** | 0 | 88 |
| Median Household Income | -0.294 ** | 0.004 | 95 | -0.391 ** | 0 | 88 |
| Children in Poverty | 0.379 ** | 0 | 95 | 0.600 ** | 0 | 88 |
| Unemployment | 0.559 ** | 0 | 95 | 0.539 ** | 0 | 88 |
| Homeownership | -0.404 ** | 0 | 95 | -0.548 ** | 0 | 88 |
| Severe Housing Problems | 0.473 ** | 0 | 95 | 0.526 ** | 0 | 88 |
| Life Expectancy | -0.348 ** | 0.001 | 95 | -0.549 ** | 0 | 88 |
| Frequent Physical Distress | 0.329 ** | 0.001 | 95 | 0.260 * | 0.015 | 88 |
| Diabetes Prevalence | 0.620 ** | 0 | 95 | 0.529 ** | 0 | 88 |
| HIV Prevalence | 0.398 ** | 0 | 91 | 0.528 ** | 0 | 86 |
| Food Insecurity | 0.339 ** | 0.001 | 95 | 0.528 ** | 0 | 88 |
R = Pearson’s correlation co-efficient with ** highly significant at P-value < 0.01 and * significant at P-value < 0.05; n = number of counties within the state.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



