
Submitted:
07 March 2025
Posted:
10 March 2025
You are already at the latest version
Abstract
This study aims to evaluate the micro-tensile bond strength of two types of composites for indirect restoration luted to enamel and dentin by self-adhesive cement. Sixteen flat enamel and dentin surfaces of human molar were cemented to equal flat specimens from laboratory composite Signum ceramics and CAD/CAM block Cerasmart. Half of the specimens of the group were thermocycling. After that, the samples were prepared for µTBS. From the micro-tensile bond strength tests, we found that thermocycling significantly reduced the adhesive bond. Dentin bonds better to conventional laboratory composites. Enamel bonds are better than composite blocks for milling.
Keywords:
micro-tensile bond strength
; composite inlay
; CAD/CAM
; restorative dentistry
1. Introduction
Nowadays, the use of dental amalgams is limited, with a tendency towards its complete removal as a restorative material. Direct and indirect composites [1,2] are used for restoring vital posterior teeth with extensive destruction, corresponding to a minimally invasive work technique. Despite the progress in the development of direct composite materials, they still have several disadvantages that make them unsuitable for obturation with significant loss of hard dental tissues. Polymerization shrinkage is a major problem, leading to the formation of a marginal gap, microleakage and the occurrence of secondary carious lesions [3,4]. The linear polymerization shrinkage of composite materials containing Bis-GMA is between 0.3-1.5% [5], and the volumetric shrinkage is 1.5-3.5% [6].
Composite materials for indirect restorations are divided into two groups: laboratory (used by dental technicians for layer-by-layer restorations) and computer-aided design/computer-aided manufacturing (CAD/CAM) blocks, which are milled by machines. These materials can be called hybrid ceramics, but their composition is close to direct composites [7]. Indirect restoration methods improve composite materials' physicochemical properties, reducing polymerisation shrinkage and marginal gaps. These types of materials are prepolymerized [8], and the changes regarding shrinkage occur only in the thin layer of the cement. Laboratory composites are two generations. The second generation is more widely used in dental practice, such as Signum ceramics (Heraeus Kulzer), Artglass (Heraeus Kulzer), and Belleglass HP (Kerr). These are hybrid materials combining the qualities of ceramic and composite materials [9]. The inorganic component in their composition is approximately twice as much as the organic one, and as a result, their mechanical properties and wear resistance are improved.
With the improvement of dental medicine technologies, CAD/CAM systems emerged in the 1980s [10,11]. The computer-generated design for inlays, overlays, and onlays is then fed to a CAD/CAM machine. The machine mills the final restoration from composite blocks. This improves the accuracy of the obtained restoration to the cavity shape, adjacent teeth and antagonists [12]. The first composite blocks for CAD/CAM machines were introduced in 2000. They are similar in content to direct composite materials, but their light polymerisation is performed in the factory [13,14]. This significantly improves their mechanical properties and reduces their shrinkage [15]. The retention of indirect restorations is mainly achieved through adhesion [16]. The strength of the adhesive bond is crucial for the longevity of indirect restorations. The adhesion of conventional CAD/CAM restorations is directly related to their cementation to the hard dental tissues [17,18,19,20]. In recent years, self-adhesive cement is most often used to bond aesthetic indirect restoration [17,19,21]. There is a lack of data in the literature regarding the investigation of the strength of the adhesive bond of new composite materials (conventional and milling blocks) after thermocycling, and those regarding the bond with different dental structures - enamel and dentin, are insufficient. This study aims to evaluate the tensile bond strength of the adhesive bond between enamel or dentin and two composite materials reinforced with ceramic particles - laboratory and milling blocks, with and without thermocycling.
2. Materials and Methods
The Medical University – Sofia Research Ethics Committee approved the project (approval number 53). Thirty-two extracted human molars were used for the in vitro study. The micro-tensile bond strength (µTBS) was evaluated on 80 specimens made of enamel/dentin and two types of composite materials for indirect restorations - CERASMART milling blocks (GC Europe, Leuven, Belgium) and the conventional laboratory composite Signum ceramics (Heraeus Kulzer, Hanau, Germany).
2.1. Fabrication of Composite Samples
One of the composites - CERASMART (GC Europe, Leuven, Belgium), represents CAD/CAM blocks. Sixteen cylindrical standard models with a height of 4 mm and a length of 8 mm were made from them. The other material is the conventional laboratory composite Signum ceramics (Heraeus Kulzer, Hanau, Germany). The material is initially polymerised in a pre-made model for the final fabrication of analogous standard models. For this purpose, the CAD/CAM blocks are also used to make negative silicone impressions (matrices). Their resulting models are placed in a test silicone to create a mould for the conventional laboratory composite - Signum ceramic. After the silicone mass hardens, the milling material is removed, and the traditional laboratory composite - Signum ceramics is applied to the prepared form in two portions sequentially. Each portion is polymerised for 6 s, and after removing the specimen from the mould, a final polymerisation is performed for 90 s in a Hi-Light power 3D (Heraeus Kulzer, Hanau, Germany) oven. This technology makes sixteen specimens from each group of composite material.
2.2. Preparation of Enamel Specimens
The enamel surface on 16 molars was separated buccally and lingually using a diamond bur. Then, they are divided into four equal groups (x4 specimens in each). Composite blocks with a height of 4 mm from the laboratory composite Signum ceramics are cemented to groups A and B, and CAD/CAM blocks (CERASMART) again with a height of 4 mm using the self-adhesive cement iCEM self-adhesive (Heraeus Kulzer, Hanau, Germany) to groups C and D. The enamel surface is not treated (according to the manufacturer's instructions), and the composite materials are sandblasted (50µm Al2O3) at 3 atm for 20 s, followed by silanisation. The test bodies from groups A and C are subjected to thermal loading (for 1000 cycles) using a Thermocycler (SD Mechatronik, Munich, Germany) at bath temperatures of 5 and 55°C. The stay in the hot and cold baths is 30 s, and the holding time before immersion in one of them is 15 s. After the thermocycling stage, each specimen is embedded in an epoxy block. Using a Leica SP 1600 microtome, under continuous water cooling, this block is cut into three mutually perpendicular planes until miniature test bodies (specimens) for physicomechanical testing are obtained. The dimensions of the square cross-section are 2x2 mm. The test bodies from groups B and D are also embedded in resin but are not subjected to thermocycling ageing. They are directly cut into specimens. For µTBS evaluation (Figure 1), the specimens are appropriately positioned in an LMT 100 stand (LAM. Technologies, Firenze FI, Italy) and subjected to static tensile loading at a 0.5 mm/min speed. The registered maximum value of the force (N) resisting the test body, divided by its initial cross-sectional area (S), is the tensile strength with a dimension of MPa.
2.3. Preparation of Dentin Specimens
The occlusal third on 16 teeth is removed using a diamond bur. The aim is to expose the dentin. The lower third of the crown is also removed. The dentin surface is examined using magnification (x9) for the absence of enamel and pulp tissue. The prepared dentin specimens are divided into four equal groups (x4 specimens each). Composite blocks with a height of 4 mm from the laboratory composite Signum ceramics are cemented to groups E and F. CAD/CAM blocks CERASMART to groups G and H, using the self-adhesive cement iCem. The dentin surface doesn`t require pretreatment according to the manufacturer's instructions for the cementing agent, and the composite materials are sandblasted (50µm Al2O3) at 3 atm for 20 s, followed by silanisation. The dentin plates in groups E and F are similarly cemented to 8 composite Signum ceramics samples, and those in groups G and H to 8 CERASMART standards using the self-adhesive cement iCem. The dentin specimens from groups E and G, as the enamel specimens, are subjected to thermocycling loading under the conditions described. All specimens (including those from groups F and H) are individually embedded in activated epoxy resin and left for 72 hours after the thermocycling effect. A similar preparation of specimens for determining the adhesive strength follows. The tests are performed under the same conditions, and the data obtained are processed analogously (Fig. 1).
3. Results
The mean and standard deviations of µTBS values are shown in Table 1. The Independent Samples T-test result revealed that thermocycling significantly affected the µTBS (p< 0.05) in all the groups except Signum ceramis bond to dentin. Thermocycling reduces the tensile bond strength. A comparison of the results between enamel/dentin specimens with/without thermocycling, cemented to the two types of composite material. The data show the opposite for dentin specimens - the tensile strength is higher for composite 1 (Signum ceramis). Statistical processing of this data was performed. The distribution in the groups was found to be normal, and their dispersion was equal. The statistical processing results show no statistically significant difference in micro-tensile strength between composite 1 (Signum ceramis) and 2 (Cerasmart) cemented to enamel, regardless of whether they were thermocycling. The observed difference is of a random (non-systematic) nature. However, a statistically significant difference in micro-tensile strength in favor of Signum ceramics is proven for dentin, regardless of whether the specimens were thermocycling. This second conclusion can be asserted with 99% probability. Summarising the findings, it can be said that thermocycling leads to fatigue of the hard dental tissue/composite material bond and a decrease in micro-tensile strength. This difference is statistically evident in 3 out of 4 tested tooth groups. It does not occur only in the dentin-composite 1 (Signum ceramis) bond. At the same time, the lowest micro-tensile strength values are observed after thermocycling the specimens made after cementing dentin to the Cerasmart composite block. Composite material 1 (Signum ceramics) has a stronger adhesive bond to dentin, and composite material 2 (Cerasmart) to enamel.
4. Discussion
The adhesion of indirect restorations to hard dental tissues is crucial for their longevity. Nowadays, self-adhesive cement is most widely used [22]. Most of the research found in the literature concerns the study of the bond between the resin cement and enamel/dentin. The role of these bonding agents is very complex, as they must establish a connection with the hard dental tissues and the composite material. Several quantitative methods for determining the strength of the adhesive bond are described in the literature: shear strength, micro-shear strength, tensile strength, micro-tensile strength [17,23,24,25,26]. The macro testing requires an adhesion area exceeding 3 mm2, while micro tests require less than 3 mm2 [27]. According to Griffit [28], the strength of the measured adhesive bond decreases with an increasing area of the tested specimens. Different methods for evaluating the strength of the adhesive bond also affect the results. Not many studies in literature use other tests to assess adhesion to enamel and dentin [17,23]. The specimens in this study were prepared according to the standardised guidelines and methodologies described in the literature [17,29,30]. Our study evaluated the adhesive strength by measuring the µTBS in MPa. Measuring micro-tensile strength is a more complex process involving the preparation of many specimens from a smaller amount of material. It is performed in a smaller area, contributing to a more uniform stress distribution [31]. Fewer material defects are observed on the smaller area of the specimens [23]. In this methodology, adhesive-type fractures are more common and cohesive-type fractures are less common [31]. This makes it more reliable [32], and the micro-tensile strength values are higher than macro-tensile strength [23]. The adhesive strength found in the literature varies between 9 and 45.3 MPa and depends on the testing method and the composition of the material [33]. In our study, specimens that fractured before testing were not considered, and values of 0 MPa were not included. In some studies, these specimens are also excluded [23,34], while in others they are concluded [35]. Enamel specimens are more prone to fracture before testing compared to dentin specimens. Enamel has a higher hardness than dentin: 270-350 KHN and 50-70 KHN [36], which leads to debonding of the hard dental tissues from the specimen during its cutting. In our study, specimens made of Cerasmart material bonded better to enamel than those made of Signum ceramics material. Since the experimental setup was performed under the same conditions for both groups, it can be argued that the Cerasmart material bonds more strongly to the self-adhesive cement iCEM. Adhesion to the enamel surface is more easily achieved and more reliable. Enamel comprises 94-96% inorganic components, 1-4% water, and 4-5% organic components [23]. It has higher intermolecular forces and higher surface energy. There are three models by which the structure of enamel can be altered by phosphoric acid, and adhesion can be achieved: by attacking the prisms' core, the prisms' periphery, or a combination of both [23]. Modern self-adhesive cement does not require etching of the enamel surface, as it contains acidic methacrylate groups [37]. In our study, we followed this work protocol as in most studies found in the literature [33,38]. However, some authors report higher micro-tensile strength values after pretreatment of the enamel surface with 37% phosphoric acid [37].
Adhesion to dentin is more complex, as it is a porous, moist structure consisting of hydroxyapatite particles in a collagen matrix. The organic component reduces the bond strength. Dentin tubules are wider and more permeable near the pulp. The water content is lower on the surface and increases at depth. In addition to these physiological differences, the dentin structure undergoes changes with increasing age or due to the presence of a carious process. An increase in thickness and a decrease in permeability are observed. All these factors make the dentin structure more complex for achieving satisfactory adhesion [23,26]. The micro-tensile strength values for dentin should be lower compared to enamel. In our study, the dentin surface was not treated with etching acid before cementation of the composite material. Interestingly, the micro-tensile strength values for dentin cemented to composite material 1 (Signum ceramis) are higher than those for enamel. Similar results are reported in a review study by Scherrer et al. [39] and Bracher et al. [23]. According to the authors, the results are due to the formation of microcracks during the cutting of the enamel specimens. De Munck et al. found that a self-adhesive cement bond is better for dentin than enamel [37]. They suggest selective etching only of the enamel surface [37], as dentin treatment yields worse results than enamel treatment [37]. Further research on the selective etching of the enamel surface would improve the cementation protocol for indirect composite restorations.
The dentin and Signum ceramic samples showed the highest micro-tensile bond strength values. The dentin surface bonds better than the enamel surface with the tested cement. This dependence was not observed in the Cerasmart material samples. The enamel bonds better than dentin with resin cement. Since the primary goal in cavity preparation is to maximise enamel preservation in the peripheral connection, cementation of Cerasmart restorations would yield a more reliable result.
The cement used in this study is self-adhesive. They do not require preliminary enamel/dentin surface treatment, which facilitates the work protocol and reduces postoperative sensitivity [38]. The bond formed with the tooth structure (dentin/enamel) is micro-mechanical and chemical. It is achieved between the cement's multifunctional acid monomers and the tooth structure's hydroxyapatite crystals [38]. Most studies report that despite the good qualities of self-adhesive cements, they still have a weaker adhesive bond than conventional cements, which require etching and applying a bonding agent [35,40,41]. Other studies show that self-adhesive types of cement bond are better than those requiring total etching [31,42]. Some authors reported that the acid methacrylate esters cannot fully penetrate the partially dissolved contaminant layer. As a result, voids are formed, and the bond strength between the cement and dentin is reduced [43].
The treatment of the inner surface of indirect restorations also affects the adhesive bond strength. The composite material samples we prepared were first subjected to sandblasting with Al2O3, which achieves a micro-mechanical bond, and then silane was applied to achieve a chemical bond. Most studies indicated that this significantly increases the bond strength between the tooth structure and the composite material [38]. De Angelis et al. reported lower micro-tensile bond strength values for composite material to dentin – 6.46 MPa, compared to our values – 18.65 MPa and 12.08 MPa, when treated with Al2O3 without silane application [35]. Other authors also obtained lower values, as they did not use silane [41]. They used the same cement as us – iCem (Heraeus Kulzer). Fuentes et al. didn’t observe a significant change in adhesive bond strength after silane application [40].
Thermal cycling is one of the most used methods that imitates clinical conditions and induces mechanical stress. Most studies found in the literature don’t evaluate the adhesive bond strength after thermal fatigue, limiting the data obtained [17,30,42]. In our study, the adhesive bond strength systematically decreased after thermal cycling. This dependence was statistically significant in three studied groups – Signum ceramis/enamel, Cerasmart/enamel, and Cerasmart/dentin. In the Signum ceramis/dentin samples, a decrease in µTBS was again observed, but it was not statistically significant. The other authors also reported a substantial change in adhesive bond strength after thermal cycling [38,44]. Three possible mechanisms by which temperature changes lead to a decrease in adhesive bond strength are: significant differences in the thermal expansion of different substrates (enamel/dentin/composite material) lead to the destruction of the adhesive bond [38]; degradation of the cement due to the destruction of the filler/matrix bond; release of monomer from the cement upon temperature increase [38]. Other authors claim that thermal cycling does not affect the adhesive bond strength [45]. Abo-Hamar et al. reported a significant change in enamel samples' thermal cycling but not dentin samples [46]. The adhesive bond strength values we obtained show that it decreases significantly after temperature changes, except for the composite material 1 group (Signum ceramics) cemented to dentin.cc
5. Conclusions
Within the limitations of this in vitro study, it was concluded that
- Thermal fatigue of the material leads to decreased micro-tensile bond strength values for all materials tested.
- Dentin bonds better to conventional laboratory composites.
- Enamel bonds are better than composite blocks for milling.
Author Contributions
Conceptualization, V.P. and J.K.; methodology, V.P.; investigation, V.P.; resources, V.P.; data curation, J.K.; writing—original draft preparation, V.P.; writing—review and editing, J.K. and S.Y.; visualisation, V.P.; supervision, J.K. All authors have read and agreed to the published version of the manuscript.
Funding
The Bulgarian Ministry of Education and Science funded this research under the National Program “Young Scientists and Postdoctoral Students—2.”
Institutional Review Board Statement
The use of extracted teeth was approved by the Medical University – Sofia Research Ethics Committee (approval number 53).
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- El-Askary, F.; Hassanein, A.; Aboalazm, E.; Al-Haj Husain, N.; Özcan, M. A Comparison of Microtensile Bond Strength, Film Thickness, and Microhardness of Photo-Polymerized Luting Composites. Materials 2022, 15, 3050. [CrossRef]
- Haruyama, A.; Muramatsu, T.; Kameyama, A. The Effect of Silane Treatment of a Resin-Based Composite on Its Microtensile Bond Strength to a Ceramic Restorative Material. Appl. Sci. 2024, 14, 9178. [CrossRef]
- Cassin, A.M.; Pearson, G.J. Microleakage studies comparing a one-visit indirect composite inlay system and a direct composite restorative technique. J Oral Rehabil 1992 May; 19(3):265–270. [CrossRef]
- De Andrade, O.S.; de Goes, M.F.; Montes, M.A. Marginal adaptation and microtensile bond strength of composite indirect restorations bonded to dentin treated with adhesive and low-viscosity composite. Dent Mater 2007 Mar; 23(3):279–287.
- Kwon, H.J.; Ferrance, J.; Kang, K.; Dhont, J.; Lee, I.B. Spatio-temporal analysis of shrinkage vectors during photo-polymerization of composite. Dent Mater 2013; 29(12):1236-1243. [CrossRef]
- Boaro, L.C.; Goncalves, F.; Guimares, T.C.; Ferracane, J.L.; Pfeifer, C.S.; Braga, R.P. Sorption, solubility, shrinkage and mechanical properties of low-shrinkage commercial resin composites. Dent Mater 2013; 29(4):398-404.
- Lauvahutanon, S.; Takahashi, H.; Shiozawa, M.; Iwasiki, N.; Asahawa, Y.; Oki, M.; Finger, W.; Arksornnukit, M. Mechanical properties of composite resin blocks for CAD/CAM. Dent Mater 2014; 33(5): 705-710. [CrossRef]
- Nguyen, J.F.; Migonney, V.; Ruse, N.D.; Sadoun, M. Resin composite blocks via high-pressure high-temperature polymerization.Dent Mater 2012; 28:529-534. [CrossRef]
- Mandikos, M.N.; McGivney, G.P.; Davis, E.; Bush, P.J; Carter, J.M. A comparison of the wear resistance and hardness of indirect composite resins. J Prost Dent 2001; 85(4):386-395. [CrossRef]
- Dikici, B.; Türke¸s Ba¸saran, E.; Can, E. Does the Type of Resin Luting Material Affect the Bonding of CAD/CAM Materials to Dentin? Dent. J. 2025, 13, 41.
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: current status and future perspectives from 20 years of experience. Dent Mater 2009; 28:44-56. [CrossRef]
- Boitile, P.; Mawusii, B.; Tapie, L.; Fromentin, O. A systematic review of CAD/CAM fit restoration evaluations. J Оral Rehabil 2014; 41:853-874. [CrossRef]
- Giordano, R. Materials for chairside CAD/CAM-produced restorations. J Am Dent Assoc 2006; 137:14S-21S. [CrossRef]
- ParadigmTM MZ100 Block: Technical Product Profile. St. Paul, MN: 3M ESPE; 2000. [CrossRef]
- Awada, A.; Nathanson, D. Mechanical properties of resin-ceramic CAD/CAM restorative materials. J Prosthet Dent 2015; 114: 587–593.
- Antoniou, I.; Mourouzis, P.; Dionysopoulos, D.; Pandoleon, P.; Tolidis, K. Influence of Immediate Dentin Sealing on Bond Strength of Resin-Based CAD/CAM Restoratives to Dentin: A Systematic Review of In Vitro Studies. Biomimetics 2024, 9, 267. [CrossRef]
- Bellan, M.C.; Cunha, P.F.J.S.D.; Tavares, J.G.; Spohr, A.M.; Mota, E.G. Microtensile bond strength of CAD/CAM materials to dentin under different adhesive strategies. Braz Oral Res. 2017; 18(31): e109. [CrossRef]
- Kaptan, A.; Bektaş, O.; Eren, D.; Doğan, D. Influence of different surface sreatments to Self-adhesive resin cement to CAD-CAM materials bonding. ODOVTOS Int J Dental Sc 2023;25-1:22-32.
- Papadopoulos, K.; Pahinis, K.; Saltidou, K.; Dionysopoulos, D.; Tsitrou, E. Evaluation of the Surface Characteristics of Dental CAD/CAM Materials after Different Surface Treatments. Materials (Basel). 2020 Feb 22;13(4):981. [CrossRef]
- Manso, A.P.; Carvalho, R.M. Dental Cements for Luting and Bonding Restorations: Self-Adhesive Resin Cements. Dent Clin North Am. 2017 Oct; 61(4): 821–834.
- Wu, C.-Y.; Nakamura, K.; Miyashita-Kobayashi, A.; Haruyama, A.; Yokoi, Y.; Kuroiwa, A.; Yoshinari, N.; Kameyama, A. The Effect of Additional Silane Pre-Treatment on the Microtensile Bond Strength of Resin-Based Composite Post-andCore Build-Up Material. Appl. Sci. 2024, 14, 6637. [CrossRef]
- Awad, M.M.; Alhalabi, F.; Alshehri, A.; Salem, M.A.; Robaian, A.; Alghannam, S.; Alayad, A.S.; Almutairi, B.; Alrahlah, A. Silane-Containing Universal Adhesives Influence Resin-Ceramic Microtensile Bond Strength. Coatings 2023, 13, 477. [CrossRef]
- Bracher, L.; Ozcan, M. Adhesion of resin composite to enamel and dentin: a methodological assessment. J Adhes Sci Technol. 2018;32:258–271. [CrossRef]
- Chin, A.; Ikeda, M.; Takagaki, T.; Nikaido, T.; Sadr, A.; Shimada, Y.; Tagami, J. Effects of Immediate and Delayed Cementations for CAD/CAM Resin Block after Alumina Air Abrasion on Adhesion to Newly Developed Resin Cement. Materials 2021, 14, 7058. [CrossRef]
- Gerdzhikov, I.; Uzunov, T.; Radeva, E. Evaluation of Microtensile Bond Strength of Luting Cements to Zirconia Ceramics. Wulfenia.2021, 28(12):2-11.
- Sano, H.; Chowdhury, A.F.M.A.; Saikaew, P.; Matsumoto, M.; Hoshika, S.; Yamauti, M. The microtensile bond strength test: Its historical background and application to bond testing. Jpn Dent Sci Rev. 2020 Dec;56(1):24-31. [CrossRef]
- Van Meerbeek, B.; Peumans, M.; Poitevin, A.; Mine, A.; Van Ende, A.; Neves, A.; De Munck, J. Relationship between bond-strength tests and clinical outcomes. Dent Mater. 2010 Feb;26(2):e100-21. [CrossRef]
- Griffith, A.A. The phenomena of rupture and flow in solids. Philos Trans R Soc London, Ser A. 1920;221:168–198.
- Armstrong, S.; Breschi, L.; Özcan, M.; Pfefferkorn, F.; Ferrari, M.; Van Meerbeek, B. Academy of Dental Materials guidance on in vitro testing of dental composite bonding effectiveness to dentin/enamel using micro-tensile bond strength (μTBS) approach. Dent Mater. 2017 Feb;33(2):133-143. [CrossRef]
- Gailani, H.F.A.; Benavides-Reyes, C.; Bolaños-Carmona, M.V.; Rosel-Gallardo, E.; González-Villafranca, P.; González-López, S. Effect of Two Immediate Dentin Sealing Approaches on Bond Strength of Lava™ CAD/CAM Indirect Restoration. Materials. 2021 Mar 26;14(7):1629.
- Magdy, N.; Rabah, A. Evaluation of micro-tensile bond strength of indirect resin composite inlay to dentin. Int J Health Sci Res. 2017; 7(5):105-115.
- Betamar, N.; Cardew, G.; van Noort, R. Influence of specimen designs on the microtensile bond strength to dentin. J Adhes Dent. 2007;9:159–168.
- De Munck, J.; Mine, A.; Poitevin, A.; Van Ende, A.; Cardoso, M.V.; Van Landuyt, K.L.; Peumans, M.; Van Meerbeek B. Meta-analytical review of parameters involved in dentin bonding. J Dent Res. 2012 Apr;91(4):351-7. [CrossRef]
- Goracci, C.; Cury, A.H.; Cantoro, A.; Papacchini, F.; Tay, F.R.; Ferrari, M. Microtensile bond strength and interfacial properties of self-etching and self-adhesive resin cements used to lute composite onlays under different seating forces. J Adhes Dent. 2006 Oct;8(5):327-35.
- De Angelis, F.; Minnoni, A.; Vitalone, L.M.; Carluccio, F.; Vadini, M.; Paolantonio, M.; D'Arcangelo, C. Bond strength evaluation of three self-adhesive luting systems used for cementing composite and porcelain. Oper Dent. 2011 Nov-Dec;36(6):626-34.
- Meredith, N.; Sherriff, M.; Setchell, D.J.; Swanson, S.A. Measurement of the microhardness and young's modulus of human enamel and dentine using an indentation technique. Arch Oral Biol. 1996;41:539–545. [CrossRef]
- De Munck, J.; Vargas, M.; Van Landuyt, K.; Hikita, K.; Lambrechts, P.; Van Meerbeek, B. Bonding of an auto-adhesive luting material to enamel and dentin. Dent Mater. 2004 Dec;20(10):963-71.
- Gamal, R.; Gomaa, Y.; Abdellatif, M. Microtensile bond strength and scanning electron microscopic evaluation of zirconia bonded to dentin using two self-adhesive resin cements; effect of airborne abrasion and aging. Fut Dent J 2017; 3(2):55-60. [CrossRef]
- Scherrer, S.S.; Cesar, P.F.; Swain, M.V. Direct comparison of the bond strength results of the different test methods: a critical literature review. Dent Mater. 2010;26:78–93. [CrossRef]
- Fuentes, M.V.; Escribano, N.; Baracco, B.; Romero, M.; Ceballos, L. Effect of indirect composite treatment micro effect of indirect composite treatment microtensile bond strength of self-adhesive resin cements. J Clin Exp Dent 2015.
- Roperto, R.; Akkus, A.; Akkus, O.; Lang, L.; Sousa-Neto, M.D.; Teich, S.; Porto. T.S. Effect of different adhesive strategies on microtensile bond strength of computer aided design/computer aided manufacturing blocks bonded to dentin. Dent Res J (Isfahan). 2016;13(2):117-123. [CrossRef]
- Türkmen, C.; Durkan, M.; Öksüz, M. Shear Bond Strength of Indirect Composites Luted with Three New Self-Adhesive Resin Cements to Dentin. J Adh 2009;85(12):919-931. [CrossRef]
- Rodrigues, R.F.; Ramos, C.M.; Francisconi, P.A.; Borges, A.F. The shear bond strength of self-adhesive resin cements to dentin and enamel: An in vitro study. J Prosthet Dent. 2015;113:220–7.
- Berkman, M.; Tuncer, S.; Tekçe, N.; Karabay, F.; Demirci, M. Microtensile bond strength between self-adhesive resin cements and resin based ceramic CAD/CAM block. Int. J Dental Sc 2020;23(1): 116-125. [CrossRef]
- Amaral, F.L.; Colucci, V.; Palma-Dibb, R.G.; Corona, S.A. Assessment of in vitro methods used to promote adhesive interface degradation: a critical review. J Esthet Restor Dent. 2007;19:340–354. [CrossRef]
- Abo-Hamar S.E.; Hiller, K.A.; Jung, H.; Federlin, M.; Friedl, K.H.; Schmalz, G. Bond strength of a new universal self-adhesive resin luting cement to dentin and enamel.Clin Oral Invest. 2005;9:161–167. [CrossRef]
Figure 1.
Scheme for preparing enamel specimens for microtensile testing and microtensile strength testing. Legend: E - enamel, D – dentin, C1 - composite 1 (Signum ceramis), C2 - composite 2 (Cerasmart), t° - thermocycling.
Figure 1.
Scheme for preparing enamel specimens for microtensile testing and microtensile strength testing. Legend: E - enamel, D – dentin, C1 - composite 1 (Signum ceramis), C2 - composite 2 (Cerasmart), t° - thermocycling.
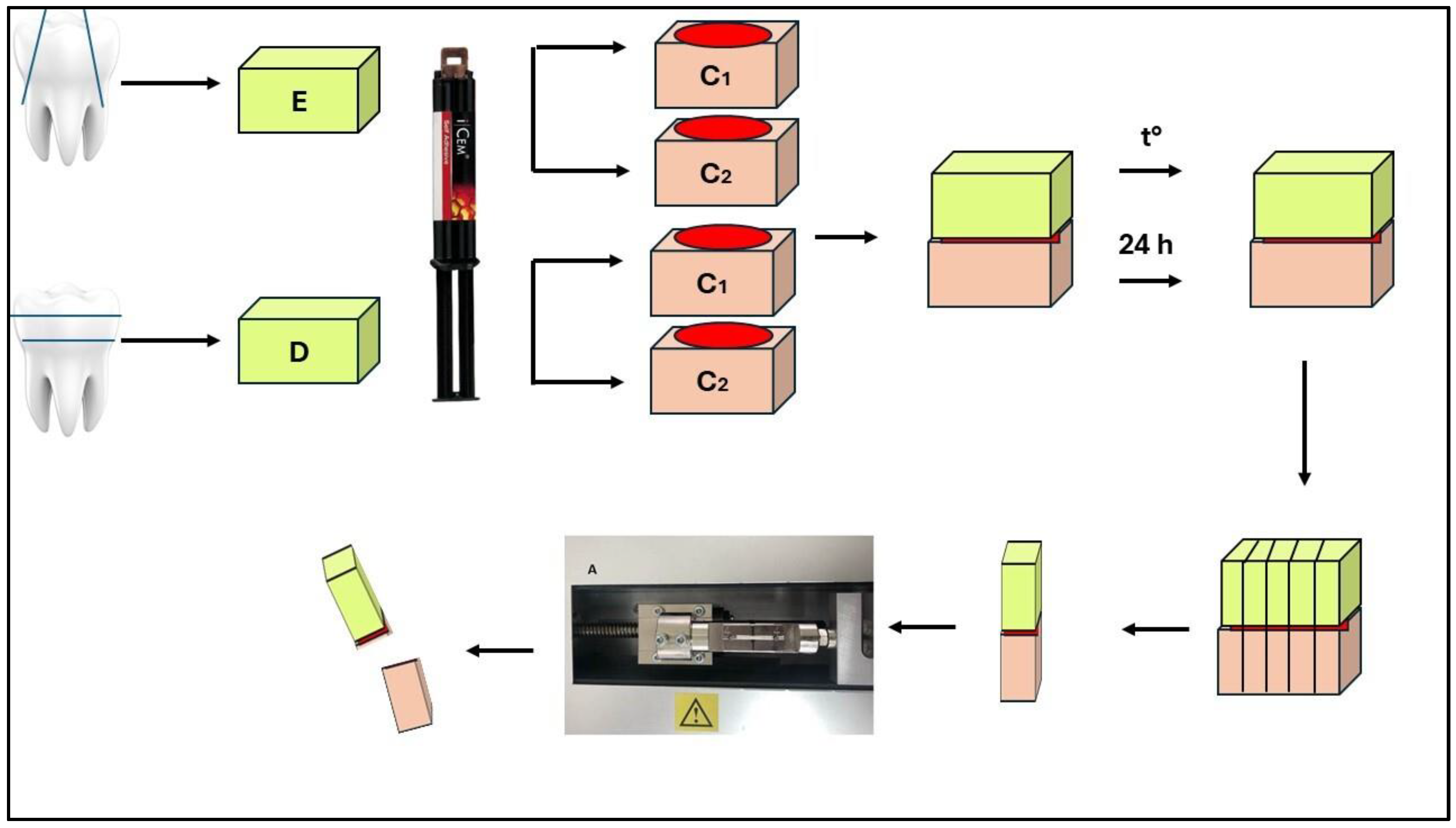

Table 1.
Statistical analysis results of the difference between micro-tensile strength in thermocycled and non-thermocycling specimens.
Table 1.
Statistical analysis results of the difference between micro-tensile strength in thermocycled and non-thermocycling specimens.
| Group | Initial Mean ± SD (MPa) |
Agining Mean ± SD (MPa) |
Group | Initial Mean ± SD (MPa) |
Agining Mean ± SD (MPa) |
|---|---|---|---|---|---|
| S/E | 12.22±2.12A, a | 8.53±1.93B, a | S/D | 18.65±3.98A, a | 16.96±3.66A, a |
| C/E | 14.58±3.37A, a | 10.60±2.17B, a | C/D | 12.08±2.53A, b | 6.17±1.28B, b |
Legend: S – Signum ceramics, C – Cerasmart, E – enamel, D-dentin. *Groups with different letters indicate statistically significant differences. Different superscript uppercase letters in each row for each material indicate significant differences with agining (p<0.05). Different superscript lowercase letters in each column for each composite material indicate significant differences (p<0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



