Submitted:
05 March 2025
Posted:
06 March 2025
You are already at the latest version
Abstract
immunotherapy alone or incombination with chemotherapy or radioitherapy is in the front line treatment for melanoma and lung cancer.However, its role in prostate cancer is usually as fourth line treatment. It is usual employed in patients with metastasis, after androgen blockade and chemotherapy. This article reviews the immunosuppressive effects of prostate cancer and possible uses of various types of immunotherapy. It als considers when would be the optimal time to employ this type of therapy.
Keywords:
prostate cancer
; immunotherapy
; cancer vaccines
; biochemical failure
; metastasis
Introduction
In 2022 of all the men diagnosed with cancer 14% of these were prostate cancer [1] while in American men this figure accounted for 19% of all cancers, representing 9% of all cancer deaths [2]. However, for those patients with localized cancer treated with curative radical prostatectomy or external beam radiotherapy or brachytherapy the 5-year survival rate is over 99% [3]. During follow-up serial measurements of the serum PSA are made, to determine the absence or presence of biochemical recurrence. This has been defined as a serum PSA >0.2ng/mL after radical prostatectomy [4] or according to the ASTRO II (American Society for Therapeutic Radiology and Oncology) guidelines an increase of the serum PSA of 2ng/mL above the nadir level achieved after radiotherapy was defined as biochemical recurrence [5]. The presence of biochemical recurrence implies the dissemination of cancer cells to distant tissues before curative treatment. Moreno et al. reported the dissemination of prostate cancer cells first to the neurovascular structures and then into the circulation [6.] It has even been reported that circulating tumour cells can be detected before a prostate biopsy, highlighting their early dissemination into the circulation [7]. It has been estimated that approximately 106 cancer cells per gram of the primary tumour are released into the circulation over a 24-hour period [8]. However, the metastatic process is inefficient, the majority of these circulating tumour cells are destroyed by the sheer forces found in the circulation or by the innate and/or acquired immune systems with only an estimated 0.01% of these cells survive [9]. Some of these cancer cells are able to implant in distant tissues and survive. They enter a varying latency period or dormancy before “awaking” to proliferate and grow.
To understand the rational of immunotherapy it is necessary to understand the complex interactions between the cancer cells, both in the primary tumour and distant micro-metastasis and the immune system.
Modulation of the Immune System by the Primary Tumour
Primary prostate cancer is made of different subpopulations of tumour cells. This heterogeneous population has differing genotypic and phenotypic characteristics and therefore differing biological properties [10]. Not only this, but the cancer cells reside in the tumour micro-environment (TME). This TME is compose of host cells, fibroblasts, immune cells, blood vessels, endothelial cells and the extracellular matrix for example. Paget in 1891 thought of the hypothesis of the idea of the soil and seed, those seeds (cancer cells) which fell on stony ground would not germinate or proliferate, while those that fell on fertile ground would germinate, proliferate and eventually cause metastatic disease [11,12]. The interactions between the different TME components is dynamic and changes with time. This multi-factoral process has been described as an ecosystem, classifying it as a “multidimensional, spatiotemporal unity of ecology and evolution” [13]. In this ecosystem there is an intraspecific relationship, that is communication between cells and an interspecific relationship between the cancer cells and host factors. It has further been described that this ecosystem represents the total of the primary, regional, distal and systemic “onco-spheres”, each with its own local .microenvironment, niches, immune, nervous and endocrine systems [14]
The immune response can be basically split into two, firstly the component which is responsible for the elimination of the cancer cells. This is composed of the innate immune response, whereby natural killer cells (NK-cells) play a cytotoxic role in order to eliminate tumour cells and the acquired immune response carried out by CD8 positive cytotoxic T-lymphocytes while dendritic cells present neo-antigens to the cytotoxic T-cells to enhance the immune response. On the other hand there are immune cells which inhibit the effector cells. This include CD4, FOXP3 positive regulatory T-lymphocytes (Tregs), myeloid derived suppresser cells (MDSC) recruited from the bone marrow and Tumour Associated Macrophages. The balance between cytotoxic cells and suppressor cells will determine if the tumour cells are eliminated or not. As previously mentionerd the tumour onco-sphere is complex and dynamic, with various mechanisms which affect this balance.
It is important that this ecosystem has multiple interactions but for the purpose of describing the role of each of factor it is necessary to limit this to the individual components.
1) prostate cancer cells: Tumour cells can directly affect the immune system both cytotoxic and immunosuppressive systems. Using single-cell RNA sequencing and multicolour flow cytometry is has been reported that high grade localized prostate cancer is highly infiltrated with exhausted cytotoxic T-cells which expressed TIM3,TOX, PD-1, CTLA4, CXCL13 and other markers of immune exhaustion in high levels, as well as MDSC and Tregs. This contrasted with the results found in low grade prostate cancer where the inverse was found with the ratio of cytotoxic T-cells relative to Tregs and MDSC. In high grade prostate cancer Tumour Infiltrating Lymphocytes (TILs) expressed high levels of the androgen receptor and prostate specific membrane antigen but less PSA antigen when compared to low grade prostate cancer [15]. PTEN is a tumour suppressor gene, it loss has been reported to be in the order of 20-30% of newly diagnosed prostate cancers. The loss of the PTEN gene increases with disease progression and its inactivation has been reported to paradoxically cause immunosuppression [16]. Tregs were found to be significantly increased in PTEN negative prostate cancer, but this was dependent on the site of sampling. In bone metastasis it caused a decrease in cytotoxic T-cells, in liver metastasis it caused the Tregs to be increased, while in lymph nodes cytotoxic T-cells were increased. These different alterations in the immune function also highlights the importance of the TME, with PTEN loss causing different effects depending on the surrounding tissue.
The BRCA mutations cause defects in the reparation of damaged DNA. The location of immune cells in wild type BRCA 1/2 tumours is predominately extra-tumoral contrasting with an intratumoral location in mutated forms. The ratio of intra to extratumoral location of immune cells was significantly higher in mutated tumours, especially for CD4, CD8 and FOXP3 lymphocytes. However, the FOXP3 to cytotoxic T-cells ratio was significantly higher in BRCA mutated cancer, impling a more immunosuppressed TME [17].
The extracellular matrix is a complex system of proteins, glycoproteins and proteoglycans, which from aggregates such as sheet-lime networks and fibrils. In addition, it has biophysical properties such as molecular density, rigidity and tensional forces [18].
Matrix metalloproteinase 2 (MMP-2) is a type IV collagenase, its expression in prostate cancer cells is associated with a worse prognosis [19,20] Not all prostate cancer cells express MMP-2, those which do are able to pass through the basement membrane and the extracellular matrix and enter the circulation, cells that are MMP-2 negative may disseminate in a form of Indian file through the tract left by MMP-2 positive cells. The multiple interactions between the tumour and stromal cells causes a re-programming of the phenotypic characteristics of both components [19,20] MMP-2 in degrading the extracellular matrix the metalloproteinases trigger the proteolysis of cytokines and their respective receptors such as tumora necrosis factor receptor R, interleukin 6R, and 2R [21] In addition, MMP-2 causes TH2 polarizacion of macrophages from the TH1 subtype, therefore restricting the anti-tumour immune response It is also able to cleave the interleukin-2-R-alpha receptor which in doing so suppresses the proliferation of cytotoxic T-cells as a result of increased apoptosis [22]. In addition to causing local immunosuppression they also cause immunosuppression at distant sites by the release of exosomes into the circulation. These exosomes are released by a process of exocytosis entering the circulation and thus are able to reach distant tissues. Exosomes are membrane bound vesicles with a diameter of approximately 50-100 nm in diameter, they fuse with the tumour cell plasma membrane and are this able to disseminate into the circulation. Exosomes are thought to be important in both the communication between cancer cells and in the remodellling of the TME [23]. Due to the differential expression of the expression of integrins on their membrane this may in part their role in the organotropic distribution of metastasis, [24]. The exosomes fuse directly with the the membrane of target cells, releasing their contents. Into the normale cells occupying the TME [25]. The exosomal contents then cause immune dysfunction; firstly they cause the differencation of bone marrow monocytes into MDSCs causing local immunosuppression and these cells also migrate to the primary tumour enhancing the immunosuppressive TME [26,27].
Secondly, they selectively affect T-cell maturation, decreasing the number and activity of cytotoxic T-cells [28], increase the proliferation of CD4+ T-cells [28], decrease the cytotoxic capabilities of NK-cells [25] and conversion of immature B-lymphocytes into regulatory B-cells [29]. Finally they increase the proliferation and activity of Tregs [30], the activity of MDSC [31] and increased immunosuppression caused by regulatory B-lymphocytes [29].
As a result of these changes the immunosuppression of the pre-metastatic niche makes fertile soil for future circulating tumour cells (the seeds) to implant in these distant sites.
Fibroblasts maintain the arquiecture of the TME, the definition of a fibroblast is somewhat difficult, mostly deriving from the embryonic mesoderm, although some derive from the neural crest. As they lack cell specific biomarkers they are often defined by their morphology, localizacion in the tissue and a lack of epithelial, mesenchymal and white cell markers (Figure 1).
The Role of Immunotherapy and Immunomodulation
Although the use of immunotherapy has changed the treatments used and the prognosis, especially in renal cell cancer and bladder cancer [32,33], this has not been the case in patients with cancer of the prostate [34]. There are differing reasons, the mechanisms of immunosuppression classifies prostate cancer as immunologically “cold” with a TME that is essentially immunosuppressive [35]. This immunological TME changes with time, the primary tumour being “colder” than metastatic disease [36]. In metastatic bone disease the immunosuppression mechanisms and lack of cytotoxic cell activation results in a TME immunosuppressive and immunotherapy is much less effective than in other solid tumours [37]. Thus the identification of biomarkers that characterize both the molecular, phenotypic and biological properties that may predict the benefit of immunotherapy are required [38]. Most reports of the activity of immunotherapy have been in patients with castration resistant metastatic prostate cancer, whom have relapsed after first and second line anti-androgens and/or chemotherapy with a taxane. This is in contrast with the early use of immunotherapy in malignancies such as the use of trastuzumab in HER-2 positive breast cancer and the anti-CD20 monoclonal antibody rituximab in non-Hodgkins lymphoma. Secondly it is possible in patients with macro-metastatic disease, as revealed by imaging studies, may not permit the entry of large molecules such as antibodies or the TME is sufficiently immunosuppressive that cytotoxic immune cells are not able to enter the metastasis in order to eliminate the tumour cells.
Sipuleucel-T ia an autologous cellular immunotherapy used in patients with metastatic castration resistant prostate cancer. These patients may be asymptomatic or with a minimum of symptoms. Sipuleucel-T was shown to reduce the risk of death and an increased overall survival as compared with a placebo in the Immunotherapy for prostate adenocarcinoma treatment phase 3 trial (IMPACT) in 2010 [39]. Based on these reported results the use of Sipuleucel-T has been included multiple clinical guidelines for the treatment of these patients [40,41,42,43,44]. In the IMPACT trial a retrospective analysis of metastatic castration resistant prostate cancer who had a low baseline PSA level, defined as < 22.1 ng/mL, the use of Sipuleucel-T was reported to have an overall survival of 13 months greater than the placebo group [45]. Sipuleucel-T stimulates an anti-tumour immunological response. Autologous antigen presenting cells are obtained from pecific prostate cancer patient susing leukopheresis, the mononuclear cells obtained are incubated with a recombinant protein for 36-44 hours. This recombinant protein PA2024 is compromised ot two components; firstly prostatic acid phosphatase (PAP) which is expressed in the majority of prostate carcinomas and at very low levels in other tissues. Secondly, PAP is conjugated with granulocyte-macrophage stimulating factor (GM-CSF) [46]. This conjugate increases the antigen uptake by antigen presenting cells [46]. This infusion of Sipeluecel-T contains not only cytotoxic T-cells, but also CD4 T-cells, NK cells, antigen presenting cells and B-cells. Upregulation of serial CD54 measuremnts is used to monitor the activation of antigen presenting cells. The first infusion acts as a primer and the second and third as a boost. This increase of CD54 acitivation was associated with an increased overall survival [47]. In a subgroup of patients from the IMPACT trial, the immune response to Sipeleucin-T was maintained 26 weeks after its administration [46].
Fong et al. [48] published a multicentre phase II study of using Sipeluecel-T as neoadjuvant treatment prior to radical prostatectomy for localized prostate cancer. This included a control group who did not receive Sipelucel T. From the biopsy and radical prostatectomy samples, immunocytological staining assessed the type and distribution of cells from the immune system. It was reported that in the post prostatectomy samples patients had increased T-cells at the cancer margen as compared with the biopsy sample, but only in those patients who had had prior treatment with Sipeluce-T which increased the number of CD4+ FOXP3 – helper T cells and cytotoxic T-cells. Although Tregs were also increased the only formed a small fraction of the total of recruited T-cells. There was no effect on NK-cell populations as would be expected. Approximately 50% of the CD3 T-cells expressed PD-1 and also expressed Ki-67 with the implication that they were not exhausted T-cells.This reported result pose sthe question of whether if combined with other therapies which can increase the immune response of T-cell such as ipilimumab or with therapies which target PD-1/PD-L1 may increase the response rates. In the case of metastatic disease, the TME is different and changes in the T-cell subpopulations may be different. Galen et al. [49] showed that the TME of metastatic lesions were immunologically colder than the primary tumour. The onco-sphere is more immunosuppressive with a lower infiltration by lymphocytes and thus T-cell and NK-cell activation is significantly reduced producing immunotolerance and a decreased effect of immunotherapies [50]. However combininig Sipuleucil-T with other therapies may improve progression free survivial with less toxicity. Trials involving the combination with atezolizumab or with radium-223 are ongoing [51,52].
G-VAX is a vaccine using genetically modified irradiated prostate cancer cells using two cell lines, one hormone sensitive, the other hormone resistant. These modified cancer cells express GM-CSF. Theoretically this type of vaccine should increase the differentiation of antigen presenting dendritic cells [53]. However the results in asymptomatic and symptomatic patients with metastatic castrate resistant prostate cancer did not show an improved overall survival when compared with G-VAX plus docetaxel, or docetaxol alone. Both the VITAL 1 and VITAL 2 trials were halted before completion due to an increased death rate of patients treated with G-VAX and no increase in the overall survival rates [54].
PROSTVAC-VF is a recombinant vaccine based on a poxvirus which has been modified with a PSA transgene to improve immunostimulation. It also contains molecules that increase the immune reponse, such as lymphocyte function associated antigen 3 (CD58), CD80 and the intracellular adhesion molecule, ICAM-1 or CD54 [55]. This combination is supposed to generate a stonger immune response against tumour cells, however in clinical trials this has not been seen to be thec ase [56]. As such the the use of this vaccine alone has not beendemonstrated to be clinically useful. Although in phase II trials promising results were seen but theres were not confirmed in phase III trials [56]. However, when used in combination with a taxane the results suggested an improved progression free survival as compared with the use of a taxane alone [57]. The use of this vaccine with the concurrent use of immune checkpoint inhibitors; monoclonal antibodies that target receptors that are essential for a successful immune reponse [58], are undergoing. In patients with localized cancer and castration resistant prostate cancer this vaccine is being use in combinationwith nivolumab (NCT02933255) and in hormone sensitive prostate with either nivolumab or ipimumab (NCT035632217).
Check point inhibitors are monoclonal antibodies which are able to target receptors that play an important role in the immune response [58]. Two pathways of these immune checkpoints that have been studied are associated with cytotoxic T-cell associated protein 4 (CTLA-4) and the programmed cell death protein 1 (PD-1) [59,60,61]. CTLA-4 is confined to the T-cell surface membrane; this protein competes with CD28, a costimulatory receptor, to bind to CD80/CD86 ligands. These two ligands are present on the surface membrane of antigen presenting cells [59]. The result of this CTLA-4-CD80-CD86 complex is a decrease in T-cell proliferation and the production of Inerleukin-2. These two processes are stimulated if CD28 binds to the CD80/CD86 complex [61]. Differing from CTLA-4 the PD-1 protein is found on the surface membrane of activated T-cells and binds to the PD-L1 and PD-L2 receptors. Both PD-L1 and PD-L2 are frequently upregulated on antigen presenting cells and cancer cells [62,63]. However, there is a decrease in cytokine production and decreased PD-1 positive T-cell proliferation, activity and their survival in the TME as a result of this treatment [64,65]. In patients with aggressive prostate cancer the upregulation of either of these ligands is associated with a worse prognosis [65]. Bypassing the inhibitory effects of these ligands using antibodies which target these ligands may enhance the immune response against cancer cell.
The results of monotherapy with the monoclonal antibody ipilimumab, a CTLA-4 blocker, in two phase III trials have been reported. In the CA184-43 trial ipilimumab together with radiotherapy to one bone metastasis was used following progression after docetaxel and compared with placebo together with radiotherapy [66]. The CA184-095 trail compared ipilimumab versus placebo before treatment with docetaxol with the hypothesis that docetaxol is immunosuppressive. However, neither of the two trials was there a benefit of adding ipilimumab to the patients treatment. However, in the final analysis there was a significant difference of long term survivors in the ipilimumab arm when given after docetaxol chemotherapy [68]. It has reported that docetaxol ris able to remodel the TME, causing an increased intratumoral infiltration by T-lymphocytes and upregulation of both PD-1 and PD-L1. In men with metastatic castration resistant prostate cancer the combined therapy produced a longer progression free surivial than with anti-PD-1 blockage as monotherapy. Thus, combining therapies may produce beneficial results for these patients [69]. However, the combination of iplilmumab together with sipuleucel-T in patients with metastatic castration resistant prostate cancer only produced a low rate of responses. A lower frequency of circulating T-lymphocytes expressing CTLA-4 or prior radiotherapy increased the response rate in these patients [70].
The use of anti-PD1 and anti-PD-L1 are limited to clincal trials in men with metastiatic castration resistant prostate cancer. In phase I trials of the use of the anti-PD-1 inhibitor in 17 patients, the use of anti-PD-1 nivolumab [71] treatment failed to show an objective response. This was also true for the anti-PD-L1 inhibitor avelumab [72] in a group of 18 patients. In the KEYNOTE trial phase I the anti-PD-1 antibody pembroizumab had some success, with a limited response rate of approximately 17% in those patients positive for PD-L1 expession [73]. In patients pretreated con docetaxol the response was also poor; independente on PD-L1 positivity [73]. The KEYNOTE-199 trial equally reported a low response rates in patients previously treated with docetaxol, achieving a 3-5% response rate following the use of pembiolizumab [74]. In the KEYNOTE-641 and IMbasador trials combining atezlizumab or pembilizumab with enzalutamide showed no improvement in terms of overall survival as compared with enzalutamide alone [75,76]. A phase 3 randomised trial conducted in 2017 used pililumumab monotherapy in high doses, 10mg/kg ascompared to placebo. There was no diiference in the overall survival between the two groups; 28.7 versus 29.7 moths respectively. In terms of progression free survival this was reported as 5.6 versus 3.8 months respectively and higher drcrese in the levels of PSA. The treatment group had an increased frequency of 3-4 grade adverse effects and also an increased death rate in the treatment group. This highlights the difference in a stastically significant difference and a clinically significant difference. Inspite of ongoing research to identify new immune checkpoint targets, such as the lymphocyte activation of gene 3, the T-cell immunoglobulin , the C- dormain of the gene 3 lymphocyte activation of the gene 3 and the immunoglobulin suppressor effect of T-cell activation via the V-dormain are under study as an independiente monotherapy or in combination with checkpoint inhibitors (ref)
Bispecific Antibodies That Target Costimulatory Recpetors of T-Cells
The evolving array of precision anti-tumor immunotherapy capable of targeting two epitopes in a single ttreatment is evolving and may play a crucial role in anti-cancer therapies [77,78]
These bispecific antibodies incorporate the epitope binding domains of two monoclonal antibodies. Firstly, against a specific cancer cell epitope, such as PMSA and a costimulatory T-cell receptor enabling the T-cell to bind to the tumour cell and thus improves its cytotoxic role [79,80]
These bivalente monoclonal antibodies are obtained against monospecific epitopes or even tri-espectific T-cell antibodies (BiTEs and TriTEs [81] It is pivotal that the optimization of the manufacturing process is to achieve the optimal binding of the antibody to the desired epitope, the stability of the molecule and its pharmakinetics. The dual targeting of the cancer cell with the direct contact with the T-cell produces the activation, proliferation and cytotoxicity of these cells which are antigen dependente. Thus by binding of the antibody to the tumour antigen such as PSMA, the crosslinking between the T-cell and tumour cell improves the cytotoxicity of the T-cell; a type of immunological symbiosis. This results via CD28 or CD3 which cativates the adjacent T-cells, resulting in an antigen-specific T-cell immune response directly against cells expressing this epitope. These BITEs have been used in pre-clinical trials [82] which have been reported to cause significant anti-tumoral effects in mouse xenograft models.In these in vivo experiments there was a dose dependente inhibition of tumour growth, although in tumours expressing a lower level of the selected epitope the therapy had a decreased effect [82]. Figure 2 shows the action of Bites with T-cell activation which elinates the tumour cell.
Newer BiTEs have a longer half-life, such as AMG160 which by binding to the PMSA epitope induces T-cell activation and the elimination of the tumour cell [83]. At the ESMO 2020 congress a Phase 1 clinical trial reported a dpse dependent PSA reduction in 68% of patients and a reduction of > 50% in 34% of participating patients. However, some 26% of patients experienced the cytokine release syndrome which most severe during the first cycle of treatment [84]. The use of treatments with BiTEs and the cytokine release syndrome has been recently reviewed [85]. It is a systemic inflammatory response with a large rapid release of cytokines into the circulation by the immunological system which may result in multi-organ failure,with lung, liver and/or kidney failure and ultimately may lead to the death of the patient. This has been reported in treatments with immune checkpoint inhibitors, BiTEs and more frequently with CAR-T cells. A multicentre phase I study of AMG340 an anti-PMA- CD3 BiTE is ongoing as well as the anti-PMSA-CD28 plus the anti-PD1 antibody ceiplimab.
Other potential tumour epitopes such as Glypican-1, disintegrin and metalloproteinase 17 and anti prostate cancer stem cell are being developed [86]. Other developments include the use of subcuteanous treatments and the use of inyectable biopolymer depots to provide a more sustained releapse of the BiTE [86].
Chimeric Antigen Receptor (CAR) T-Cell Therapy
The patientsT-cells are removed using leukopheresis and are modified genetically to express synthetic receptors directed against tumour specific epitopes. After undergoing culture to expand their numbers, they are re-infused into the patient where in a MHC independent mode they can potentially eliminate the tumour cells. [87]. Seocond and third generation CATs contain intracellular costimulatory domains to further entance both the activation and proliferation of CAR-T cells [88,89]. Third generation CAR-T cells appear to have an increased activity against cancer cells as compared to second generation CAR-T cells, at least in pre-clinical trials [90].
The heterogeneity of tumour epitopes makes the design of CAR-T cells more difficult; plus the fact that these epitopes must not be or very lowly expressed in normal cells to prevent tissue damage. PMSA and prostate stem cell antigen have been used along with costimulants such as tumour growth factor-β in an effort to overcome the imunosuppressive TME [91]. Synergy with the addition of zoledronate was seen when gamma-delta CAR-T cells were used to target prostate cancer cells, the CAR T cells recomenzing the phosphoantigens in the TME [92]. I has been reported that CAR-T cells which are engineered to express cytokines , IL-12, IL15 or CCL19 give the CAR-T cells a higher proliferation rate, persistence in the animal model and higher anti tumoral capacities than conventional CAR-T cells [93].
Preclinical studies using mice xenograft models to determine dosage and toxicity are ongoing. To improve the effectiveness of CAR-T therpy chermotherapy to cause lymphodepletion has been investigated, normally using cyclophosphamide and or fludarabine infusions for 3 dias, starting five days before the infusion of the CAR-T cells. The hypothesis of this Phase 1 trial is that pre-treatment with chemotherapy may decrease the number ot Tregs and there would be less inhibition of the CAR modified T-cells [94].
However CAR-T therapy has its side effects; allergic reactions, septicaemia por the immunosuppression, cytopenias, the immune effector cell causing neurotoxiciy and the cytokine release syndrome. These last two adverse effects were though tto be the principal reasons for the death of patients [95]. In addition if the cancer cells do not express the targeted epitope and/or is immunosuppressive to such an exent the efficacy of CART treatment may be limited.
PMSA Linked Radionuclides
The expression of the PMSA epitope is increased in approximately 75-95 of patients ith metastatic castration resistant prostate cancer. PMSA antibodies linked to a beta-emitting radionuclide such as lutetium 177 (177Lu) and yrium 90 (90Y) have been shown in phase I and phase II trials to have activity against PMSA expressing cancer cells as well as a dose dependent response [96,97,98]. The PSMA epitope is expressed in nearly all of these cancer cells, however the use of PSMA imaging by PSMA PET-CAT or using whole body single photon gamma camera computerized tomography has not been shown to be useful in detecting PMSA expressing tumours. The use of this therapy has been based on the response seen by imaging studies. It has been hypothisized that the higher the expression of PMSA on the cancer cells the better is the response. With higher doses of 177 Lu even patients with a negative imaging study responded. The authors suggested that micrometastic disease was eliminated or decreased and was too small to be detected by imaging studies [99]. No differences in progression free survival was detected between patients treated with cabazitaxel or 177Lu-PMSA in patients that progressed after docetaxol chemotherapy [100]. It is interesting that the authors mention micro-metastatic disease, as the 2022 US Food and Drug Administration [101] and European Medicines Agency [102] approved it use as a last line therapy after progression of the disease folloing androgen deprivation and taxane based hemotherapy. After the anti PSMA antibody binds to the cancer cell the radionuclide enters the cell dispersing throught the cytoplasm. The beta irradiation by damaging the DNA leads to the elimination of the cancer cell. The low penetration of these radiactive particles limits damage to neighbouring normal tissues [103].
Androgen Deprevation Therapy
Sin the pioneering work of Huggins and Hodges where in 1941 they showed that surgical castration prolonged dprogression free survival and overall survival in men with meastatic prostgate prostate cancer, androgen deprivation has been the cornerstone of prostate cancer treatment [104]. The devopment and use of steroidal (megestrol, cypertone and medroxyprogestone) plus androgen receptor antagonists such as flutamide and biclutamide were developed in the 1960s and 70s. These efective androgen receptor blockers inhibit the binding of testosterone and dihydrotestosoterone (DHT) to the androgen receptor. However, their usage prolongs the progression free surivial for approxomately 3-5 years, whereby the selection of resistant cells and changes in the androgen recptor leads to resistant tumour cells. With the devopment of GnRH agonsits such as leuprolide and gosserelin and GnLH antagonist such as degarelix, which is inyectable or the newer oralrelugolix, these treatments are often used in combination with androgen receptor blockage. The newer drus such as abiterone and enzutamide are normally used as second line therapy although the new NCCN guidelines [40] suggest that they may de used as first line treatment. After progression chemotherapy with or without androgen deprevation therapy is recommended. Immunotherapy remains as fourth line therapy. The important question is if it is known that androgen receptor blockade in its mainy forms eventually causing castration rsistent prostate cancer why is it be used as frontline therapy [105].
Should Immunotherapy Be Used as Frontline Treatment for Biochemical Relapse? Are We Not Seeing the Woods for the Trees?
In patients with biochemical relapse androgen deprivation therapy is front line treatment. Thes patients are asymptomatic, and do not have metastasis as shown in imaging studies. This called called minimal residual disease (MRD) whereby although there is a rising serum PSA level no metastatic disease can be detected. However the serum PSA levels are rising which means that the micrometastasis are proliferating, growing, disseminating to eventually form metastasis. As far back as 1992 Moreno et al. reported the detected of prostate cancer cells in the circulation after urative treatment [6]. It has also been reorted that these disseminated tumour cells or micrometastasis that are detected in the bonemarrow form a latent reserve fotrthe future development of macrometastasis [106]. In breast trustuzumab an anti-HER-2 monoclonal antibody is uded in the advujant setting, even though there is no evidence of metastatic disease. Furthermore its use produces a similar disease free survivla in those patients who not only express HER-2 in the primary tumour but even in those negative for the expression of HER-2 [107,108]. In patients with HER-2 posiitve gastric cancer trastuzumab has been incorporated as part of the first line therapy in combination with chemotherapy [109].
In patients with pathologically organ confined prostate cancer who were treated with radical prostectomy, one month after treatment three types of MRD were described. [110]. Firstly those patients who were negative for bone marrow micro-metastasis and CTC, classified as Group I (figures 3-6.)
Group II was formed by men with only bone marrow micro-metastasis detected, which may be single cells expressing PSA or larger group of PSA expressing cells detected
Figure 4.
Bone marrow biopsia showing a few PSA epressing cells implamted in the bone marrow.
Figure 5.
Bone marrow micro-metastasis with multiple PSA expressing cells.
Figure 6.
Circulating tumour cell xpressing PSA (red) and matrix metalloproteinase-2 (black).
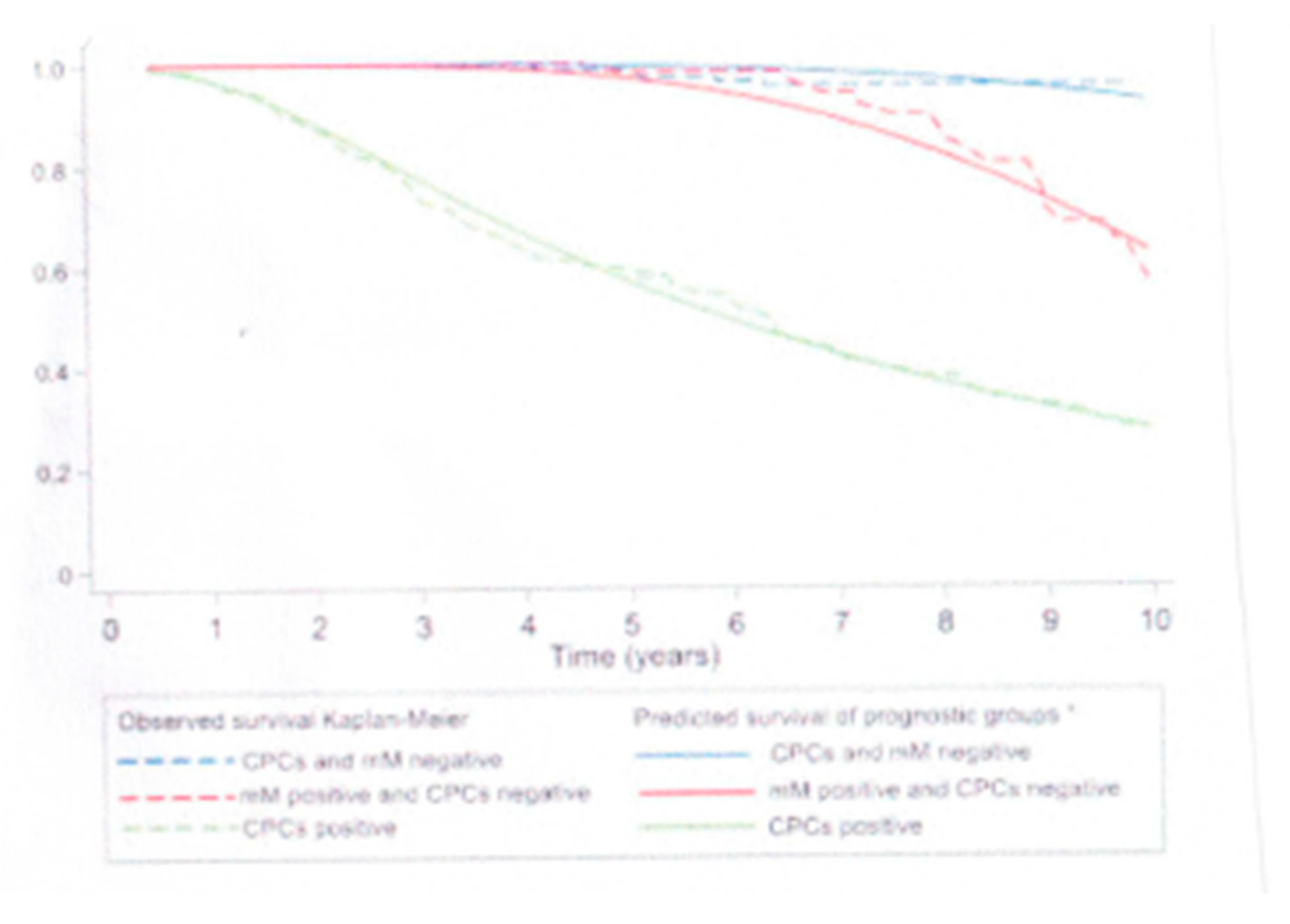
Figure 7.
Kaplam Meier survivale curves for a median time of ten years after radical prostatectomy for pathologcal organ confined prostate cancer.
Figure 7.
Kaplam Meier survivale curves for a median time of ten years after radical prostatectomy for pathologcal organ confined prostate cancer.
Finally group III MRD patients who had CTCs detected independent of whether there were bone marrow micro-mateastasis detected.
However, at this time, there is no agreement on the best method of detecting CTCs, which underlines one hurdle for this form of MRD classification. In support of this hypothesis, Bueniket et al. [111] suggested that the use of immunotherapy in patients with MRD may be more effective as adjuvant therapy after curative treatment or as first line treatment after after biochemical failure than compared with fourth line treatment when there is metastatic disease. There is a certain logic to this hypothesis; firstly in MRD the tumour load is minimal implying that the immunosuppression caused by the tumour cells is less and the anti-tumour immune response could be more efective. Secondly, if Group III MRD patients can be converted to Group II or better still Group I, tha latency period may be prolonged and the patient remains asymotmatic, delaying to the progression to biocehmical failure. Thirdly, even if used at the time of biochemical failure and there is no evidence of metastatic disease and maybe equally as effective.
Future Developments and the Use of Immunotherapy in Patients with Prostate Cancer
The development of new agents using pre-clinical and Phase I and II clinical trials may decrease the risk of developing metastatic disease or prolong the dormancy period. Double blind, randomized placebo controlled multicentre trials need to be conducted to find when it is most appropriate to use immunotherapy in patients treated with curative therapy for prostate cancer.
References
- Sridaran, D.; Bradshaw, E.; DeSelm, C.; Pachynski, R.; Mahajan, K.; Mahajan, N.P. Prostate cancer immunotherapy: Improving clinical outcomes with a multi-pronged approach. Cell Rep. Med. 2023, 4, 101199. [Google Scholar] [CrossRef] [PubMed]
- Siegel RI, Miller KD, JemalA, 2018 Cancer Statistics. CA Cancer J Clin 2018; 68: 7-30.
- Nelson, P.S. Molecular States Underlying Androgen Receptor Activation: A Framework for Therapeutics Targeting Androgen Signaling in Prostate Cancer. J. Clin. Oncol. 2012, 30, 644–646. [Google Scholar] [CrossRef] [PubMed]
- Mir, M.C.; Li, J.; Klink, J.C.; Kattan, M.W.; Klein, E.A.; Stephenson, A.J. Optimal Definition of Biochemical Recurrence After Radical Prostatectomy Depends on Pathologic Risk Factors: Identifying Candidates for Early Salvage Therapy. Eur. Urol. 2013, 66, 204–210. [Google Scholar] [CrossRef]
- Roach, M.; Hanks, G.; Thames, H.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef]
- Moreno, J.G.; Croce, C.M.; Fischer, R.; Monne, M.; Vihko, P.; Mulholland, S.G.; Gomella, L.G. Detection of hematogenous micrometastasis in patients with prostate cancer. 1992, 52, 6110–6112.
- Murray NP, Reyes E, Orellana N, Fuentealba, C., Jacob, O. Head to head of the Chun Nomogram, percentago free PSA and primary circulating postate cells to predict thew presence of prostate cancer at repeat biopsy. APJACPn2016; 17: 2559-2563.
- Chang YS, di Tomaso E, McDonald DM, Jone R, Jasin RK, Munn LL. Mosaic blood vessels in tumors: Frequency of cancer cells in contact with flowing blood. Proc Natl Acad Sci USA 2000; 97: 14608-14613.
- Fidler, I.J. Metastasis: Quantitative Analysis of Distribution and Fate of Tumor Emboli Labeled With 125I-5-Iodo-2′ -deoxyuridine23. JNCI J. Natl. Cancer Inst. 1970, 45, 773–782. [Google Scholar] [CrossRef]
- Song H, Weinstein HNW, Allegakoen P, Wadsworth II MH, Xie J, Yang H,Castro EA, Lu L, Stohr BA, Feny FY,et al. Single-cell analysis of human. Primary prostate cancer reveals the heterogeneity of tumor-associated epithlial cell states. Nat Commun 2022; 13: 141.
- Paget, S. The distribution of secondary growths in cancer of the breast. Lancet 1889, 133, 571–573. [Google Scholar] [CrossRef]
- Fildler IJ, Poste, G. The “seed And soli” hypothesis revisited. Lancet Oncol 2008; 9; 8.
- Luo, W. Nasopharyngeal carcinoma ecology theory: Cancer as multidimensional spatiotemporal “unity of ecology and evolution” pathological ecosystem. Theranostics 2023, 13, 1607–1631. [Google Scholar] [CrossRef]
- Chen, X., Song, E. The theory of tumour ecosystem. Cancer Commun 2022; 42: 587-608.
- Adorno Febles VR, Hao Y, Ahsan A, Wu J, Qian Y, Zhong H,Loeb S, Makova AV, Lepor, A., Wysock J et al. Single-cell analysis of localized prostate cancer patients links high Gleason score with an immunosuppressive profile Prostate 2023; 83: 840-849.
- Vidotto, T.; Saggioro, F.P.; Jamaspishvili, T.; Chesca, D.L.; de Albuquerque, C.G.P.; Reis, R.B.; Graham, C.H.; Berman, D.M.; Siemens, D.R.; Squire, J.A.; et al. PTEN-deficient prostate cancer is associated with an immunosuppressive tumor microenvironment mediated by increased expression of IDO1 and infiltrating FoxP3+ T regulatory cells. Prostate 2019, 79, 969–979. [Google Scholar] [CrossRef]
- Jenzer, M.; Keß, P.; Nientiedt, C.; Endris, V.; Kippenberger, M.; Leichsenring, J.; Stögbauer, F.; Haimes, J.; Mishkin, S.; Kudlow, B.; et al. The BRCA2 mutation status shapes the immune phenotype of prostate cancer. Cancer Immunol. Immunother. 2019, 68, 1621–1633. [Google Scholar] [CrossRef]
- Eble, J.A.; Niland, S. The extracellular matrix in tumor progression and metastasis. Clin. Exp. Metastasis 2019, 36, 171–198. [Google Scholar] [CrossRef]
- Ross JS, Kaur, P.Sheehan CE, Fisher HA, Kaufman RA Jr, Kallakury BV. Prognostic significance of metalloproteinase 2 and tissue inhibitor of metalloproteinase 2 expression in prostate cancer. Mod. Pathol. 2003, 16, 198–205.
- Trudel, D.; Fradet, Y.; Meyer, F.; Harel, F.; Têtu, B. Significance of MMP-2 expression in prostate cancer: An immunohistochemical study. Cancer Res. 2003, 63, 8511–8515. [Google Scholar] [PubMed]
- Nissinen, L., Kahari VM. MMPs in inflammation. Biochem Biophys Acta 2014; 1840: 2571-2580.
- Lee BK, Kim MJ, Jang HS, Lee HR, Ahn KM, Lee JH, Choung PH, Kim MJ et al. High concentrations of MMP-2 and MMP-9 reduce NK mediated cytotoxicity against oral squamous cell carcinoma line. In Vivo 2008; 22: 593-598.
- Kahlert C, Kalluri R Exosomes in tumor microenvironment influence cancer progression and metastasis. J Mol Med 2013; 91: 431-437.
- Hoshino, A.; Costa-Silva, B.; Shen, T.-L.; Rodrigues, G.; Hashimoto, A.; Mark, M.T.; Molina, H.; Kohsaka, S.; Di Giannatale, A.; Ceder, S.; et al. Tumour exosome integrins determine organotropic metastasis. Nature 2015, 527, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Syn, N.; Wang, L.; Sethi, G.; Thiery, J.-P.; Goh, B.-C. Exosome-Mediated Metastasis: From Epithelial–Mesenchymal Transition to Escape from Immunosurveillance. Trends Pharmacol. Sci. 2016, 37, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Xiang, X.; Poliakov, A.; Liu, C.; Liu, Y.; Deng, Z.-B.; Wang, J.; Cheng, Z.; Shah, S.V.; Wang, G.-J.; Zhang, L.; et al. Induction of myeloid-derived suppressor cells by tumor exosomes. Int. J. Cancer 2009, 124, 2621–2633. [Google Scholar] [CrossRef]
- Morrissey, S.M.; Zhang, F.; Ding, C.; Montoya-Durango, D.E.; Hu, X.; Yang, C.; Wang, Z.; Yuan, F.; Fox, M.; Zhang, H.-G.; et al. Tumor-derived exosomes drive immunosuppressive macrophages in a pre-metastatic niche through glycolytic dominant metabolic reprogramming. Cell Metab. 2021, 33, 2040–2058.e10. [Google Scholar] [CrossRef]
- Wieckowski, E.U.; Visus, C.; Szajnik, M.; Szczepanski, M.J.; Storkus, W.J.; Whiteside, T.L. Tumor-Derived Microvesicles Promote Regulatory T Cell Expansion and Induce Apoptosis in Tumor-Reactive Activated CD8+ T Lymphocytes. J. Immunol. 2009, 183, 3720–3730. [Google Scholar] [CrossRef]
- Figueiro F, Muller L, Funk S, Jackson EK, Battastini AM, Whiteside TL. Phenotypic and functional characteristics of CD39 high human regulatory B-cells (Breg) Oncoimmunology 2016; 5:e1082703.
- Schuler, P.J.; Saze, Z.; Hong, C.-S.; Muller, L.; Gillespie, D.G.; Cheng, D.; Harasymczuk, M.; Mandapathil, M.; Lang, S.; Jackson, E.K.; et al. Human CD4+CD39+ regulatory T cells produce adenosine upon co-expression of surface CD73 or contact with CD73+ exosomes or CD73+ cells. Clin. Exp. Immunol. 2014, 177, 531–543. [Google Scholar] [CrossRef]
- Xiang, X.; Poliakov, A.; Liu, C.; Liu, Y.; Deng, Z.-B.; Wang, J.; Cheng, Z.; Shah, S.V.; Wang, G.-J.; Zhang, L.; et al. Induction of myeloid-derived suppressor cells by tumor exosomes. Int. J. Cancer 2009, 124, 2621–2633. [Google Scholar] [CrossRef]
- Braun, D.A.; Bakouny, Z.; Hirsch, L.; Flippot, R.; Van Allen, E.M.; Wu, C.J.; Choueiri, T.K. Beyond conventional immune-checkpoint inhibition—Novel immunotherapies for renal cell carcinoma. Nat. Rev. Clin. Oncol. 2021, 18, 199–214. [Google Scholar] [CrossRef]
- Rhea LP, Mendez-Marti S, Kim D, Aragon-Ching JB. Role of immunotherapy in bladder cancer. Cancer Treat Res Commun 2021;26: 100296.
- Bansal, D.; Reimers, M.A.; Knoche, E.M.; Pachynski, R.K. Immunotherapy and Immunotherapy Combinations in Metastatic Castration-Resistant Prostate Cancer. Cancers 2021, 13, 334. [Google Scholar] [CrossRef]
- Movassaghi, M.; Chung, R.; Anderson, C.B.; Stein, M.; Saenger, Y.; Faiena, I. Overcoming Immune Resistance in Prostate Cancer: Challenges and Advances. Cancers 2021, 13, 4757. [Google Scholar] [CrossRef] [PubMed]
- Galon, J.; Bruni, D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat. Rev. Drug Discov. 2019, 18, 197–218. [Google Scholar] [CrossRef] [PubMed]
- Jiao, S.; Subudhi, S.K.; Aparicio, A.; Ge, Z.; Guan, B.; Miura, Y.; Sharma, P. Differences in Tumor Microenvironment Dictate T Helper Lineage Polarization and Response to Immune Checkpoint Therapy. Cell 2019, 179, 1177–1190.e13. [Google Scholar] [CrossRef] [PubMed]
- López-Campos, F.; Gajate, P.; Romero-Laorden, N.; Zafra-Martín, J.; Juan, M.; Polo, S.H.; Moreno, A.C.; Couñago, F. Immunotherapy in Advanced Prostate Cancer: Current Knowledge and Future Directions. Biomedicines 2022, 10, 537. [Google Scholar] [CrossRef]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T Immunotherapy for Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in prostate cancer version 1:2023. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx (accessed on November 2024).
- McNeel DG, Bander NH,, Beer TM, Drake CG, Fang L, Harrelson S, Kanttoff PV, Mdan RA, Oh WK et al. The Society for Immunotherapy for the treatment of prostate carcinoma. J Immunother cancer 2016; 4: 92.
- Cookson, M.S.; Roth, B.J.; Dahm, P.; Engstrom, C.; Freedland, S.J.; Hussain, M.; Lin, D.W.; Lowrance, W.T.; Murad, M.H.; Oh, W.K.; et al. Castration-Resistant Prostate Cancer: AUA Guideline. J. Urol. 2013, 190, 429–438. [Google Scholar] [CrossRef]
- Basch, E.; Loblaw, D.A.; Oliver, T.K.; Carducci, M.; Chen, R.C.; Frame, J.N.; Garrels, K.; Hotte, S.; Kattan, M.W.; Raghavan, D.; et al. Systemic Therapy in Men With Metastatic Castration-Resistant Prostate Cancer: American Society of Clinical Oncology and Cancer Care Ontario Clinical Practice Guideline. J. Clin. Oncol. 2014, 32, 3436–3448. [Google Scholar] [CrossRef]
- Parker C, Gillessen S, Heidenreich A, Horwich A: ESMO Guidelines Committee. Cancer of the prostate : ESMO guidelines clinical practice guidelines for diagnosis, treatment and followup. Ann Oncol 2015; 26 (suppl 5): v69-v77.
- Schellhammer, P.F.; Chodak, G.; Whitmore, J.B.; Sims, R.; Frohlich, M.W.; Kantoff, P.W. Lower Baseline Prostate-specific Antigen Is Associated With a Greater Overall Survival Benefit From Sipuleucel-T in the Immunotherapy for Prostate Adenocarcinoma Treatment (IMPACT) Trial. Urology 2013, 81, 1297–1302. [Google Scholar] [CrossRef]
- Sims, R.B. Development of sipuleucel-T: Autologous cellular immunotherapy for the treatment of metastatic castrate resistant prostate cancer. Vaccine 2011, 30, 4394–4397. [Google Scholar] [CrossRef]
- Stewart FP, Dela Rosa C, Sheikh NA, McNeel DG, Frohlich MW, Urdal DL et al. Correlation between product parameters and overall survival in three trials of sipuleuce-T, an autologous active cancer chemotherapy for the treatment of prostate cancert. J Clin Oncol 2010: 28: (15s) abstract 4552.
- Fong, L.; Carroll, P.; Weinberg, V.; Chan, S.; Lewis, J.; Corman, J.; Amling, C.L.; Stephenson, R.A.; Simko, J.; Sheikh, N.A.; et al. Activated Lymphocyte Recruitment Into the Tumor Microenvironment Following Preoperative Sipuleucel-T for Localized Prostate Cancer. JNCI J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef]
- Galon, J.; Bruni, D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat. Rev. Drug Discov. 2019, 18, 197–218. [Google Scholar] [CrossRef] [PubMed]
- Jiao, S.; Subudhi, S.K.; Aparicio, A.; Ge, Z.; Guan, B.; Miura, Y.; Sharma, P. Differences in Tumor Microenvironment Dictate T Helper Lineage Polarization and Response to Immune Checkpoint Therapy. Cell 2019, 179, 1177–1190.e13. [Google Scholar] [CrossRef] [PubMed]
- Rosser C,J, Hirasawa Y, Acaba JD, Tamura DJ, Pal SK, Huang J, Scholz MC, Dorffet TB. Phase 1b study assessing different sequencing regimens of atezolizumab (anti-PD-L1)and spipuleucin T (Sip-T) ikn patients who have asympotomatic or minimally symptomatic metastatic castrate resistant prostate cancer. J Clin Oncol 2020; 38: e17564.
- Marshall, C.H.; Fu, W.; Wang, H.; Park, J.C.; DeWeese, T.L.; Tran, P.T.; Song, D.Y.; King, S.; Afful, M.; Hurrelbrink, J.; et al. Randomized Phase II Trial of Sipuleucel-T with or without Radium-223 in Men with Bone-metastatic Castration-resistant Prostate Cancer. Clin. Cancer Res. 2021, 27, 1623–1630. [Google Scholar] [CrossRef]
- Warren, T.L.; Weiner, G.J. Uses of granulocyte-macrophage colony-stimulating factor in vaccine development. Curr. Opin. Hematol. 2000, 7, 168–173. [Google Scholar] [CrossRef]
- Joniau, S.; Abrahamsson, P.-A.; Bellmunt, J.; Figdor, C.; Hamdy, F.; Verhagen, P.; Vogelzang, N.J.; Wirth, M.; Van Poppel, H.; Osanto, S. Current Vaccination Strategies for Prostate Cancer. Eur. Urol. 2012, 61, 290–306. [Google Scholar] [CrossRef]
- Handa, S.; Hans, B.; Goel, S.; Bashorun, H.O.; Dovey, Z.; Tewari, A. Immunotherapy in prostate cancer: Current state and future perspectives. Ther. Adv. Urol. 2020, 12. [Google Scholar] [CrossRef]
- Gulley, J.L.; Borre, M.; Vogelzang, N.J.; Ng, S.; Agarwal, N.; Parker, C.C.; Pook, D.W.; Rathenborg, P.; Flaig, T.W.; Carles, J.; et al. Phase III Trial of PROSTVAC in Asymptomatic or Minimally Symptomatic Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2019, 37, 1051–1061. [Google Scholar] [CrossRef]
- Arlen, P.M.; Gulley, J.L.; Parker, C.; Skarupa, L.; Pazdur, M.; Panicali, D.; Beetham, P.; Tsang, K.Y.; Grosenbach, D.W.; Feldman, J.; et al. A randomized phase II study of concurrent docetaxel plus vaccine versus vaccine alone in metastatic androgen-independent prostate cancer. Clin. Cancer Res. 2006, 12, 1260–1269. [Google Scholar] [CrossRef]
- Granier C, Badoual C, De Guillebon E, Blanc C,, Roussel H,S, Colin E, Saldmann A, Gey A, Oudard S, Tartour E,. Mechanisms of action and use of checkpoint inhibitors in cancer. ESMO open 2017; 2: e000213.
- Huang J, Wang L, Cong Z, Amoozgar Z, Kiner E, Xing D, Orsulic S, Matulonis U,Goldberg MS. The PARP1 inhibitor BMN 673 exhibits immunoregulatory effects in BRCA-1 -/- murine model of ovarian cancer. Biochem Biophys Res Commun 2015; 463: 551-556.
- Farhangnia, P.; Ghomi, S.M.; Akbarpour, M.; Delbandi, A.-A. Bispecific antibodies targeting CTLA-4: Game-changer troopers in cancer immunotherapy. Front. Immunol. 2023, 14, 1155778. [Google Scholar] [CrossRef]
- Isaacsson V, Antonarkis ES. PD-1/PD-L1 pathway inhibitors in advanced prostate cancer. Expert Rev Clin Pharmacol 2018; 11: 475-486.
- Xu Y, Song G,Xie S, Jiang W, Chen X, Chu M, Hu X,Wang ZW. The roles of PD-1/PD-L1 in the prognosis and immunotherapy of prostate cancer. Mol Ther 2021; 29: 1958-1969.
- Leng, C.; Li, Y.; Qin, J.; Ma, J.; Liu, X.; Cui, Y.; Sun, H.; Wang, Z.; Hua, X.; Yu, Y.; et al. Relationship between expression of PD-L1 and PD-L2 on esophageal squamous cell carcinoma and the antitumor effects of CD8+ T cells. Oncol. Rep. 2015, 35, 699–708. [Google Scholar] [CrossRef]
- Salmaninejad A, Valilou SF, Shabgah AG, Aslani S, Alimandani M, Pasdar A, Sahebkar, A. PD-1/PD-L1 pathway: Basic biology and role in cancer immunotherapy. J Cell Phsiol 2019; 234: 16824-16837.
- Lotfinejad, P.; Kazemi, T.; Mokhtarzadeh, A.; Shanehbandi, D.; Niaragh, F.J.; Safaei, S.; Asadi, M.; Baradaran, B. PD-1/PD-L1 axis importance and tumor microenvironment immune cells. Life Sci. 2020, 259, 118297. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Dai, Z.; Wu, W.; Wang, Z.; Zhang, N.; Zhang, L.; Zeng, W.-J.; Liu, Z.; Cheng, Q. Regulatory mechanisms of immune checkpoints PD-L1 and CTLA-4 in cancer. J. Exp. Clin. Cancer Res. 2021, 40, 1–22. [Google Scholar] [CrossRef]
- Kwon ED, Drake CG, Scher HI, Fizazi K, Bossi A, Van der Eeertwegh AJ, Krainer M, Houede N, Santos R, Mahammedi, H. Ipilimumab versus placebo after radiotherapy in patitents with metastastic castration-resistant prostate cancer that had progressed after docetaxol chemotherapy (CA184-03): A multicentre randomized double blind phase 3 trial. Lancet Oncol 2014; 15: 700-712.
- Beer, T.M.; Logothetis, C.; Sharma, P.; Bossi, A.; McHenry, B.; Fairchild, J.P.; Gagnier, P.; Chin, K.M.; Cuillerot, J.-M.; Fizazi, K.; et al. CA184-095: A randomized, double-blind, phase III trial to compare the efficacy of ipilimumab versus placebo in asymptomatic or minimally symptomatic patients (pts) with metastatic chemotherapy-naive castration-resistant prostate cancer (CRPC). J. Clin. Oncol. 2012, 30, TPS4691. [Google Scholar] [CrossRef]
- Fizazi, K.; Drake, C.G.; Beer, T.M.; Kwon, E.D.; Scher, H.I.; Gerritsen, W.R.; Bossi, A.; Eertwegh, A.J.v.D.; Krainer, M.; Houede, N.; et al. Final Analysis of the Ipilimumab Versus Placebo Following Radiotherapy Phase III Trial in Postdocetaxel Metastatic Castration-resistant Prostate Cancer Identifies an Excess of Long-term Survivors. Eur. Urol. 2020, 78, 822–830. [Google Scholar] [CrossRef]
- Ma, Z.; Zhang, W.; Dong, B.; Xin, Z.; Ji, Y.; Su, R.; Shen, K.; Pan, J.; Wang, Q.; Xue, W. Docetaxel remodels prostate cancer immune microenvironment and enhances checkpoint inhibitor-based immunotherapy. Theranostics 2022, 12, 4965–4979. [Google Scholar] [CrossRef]
- Sinha, M.; Zhang, L.; Subudhi, S.; Chen, B.; Marquez, J.; Liu, E.V.; Allaire, K.; Cheung, A.; Ng, S.; Nguyen, C.; et al. Pre-existing immune status associated with response to combination of sipuleucel-T and ipilimumab in patients with metastatic castration-resistant prostate cancer. J. Immunother. Cancer 2021, 9, e002254. [Google Scholar] [CrossRef]
- Topalin SL. Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD, Sosman SA, Atkins MB el at. Safety, activity and immune correlates of Anti-PD-1 antibody in cancer. N Eng J Med 2012; 366: 2443-2454.
- Fakhrejehani F, Madan RA, Dahut WL, Karzai F, Cordes LM, Schlom J, Liow E, Bennett C, ZhengT, Yu J et al. Avelumab in metastatic castration-resistant prostate cancer J Clin Oncol 2017; 35: 159.
- Hoimes CJ, Graff JN, Tagawa ST, Hwang C, Kilari D, Ten Tije AJ, Omlin AU, McDermott RS, Vaishampayan UN, Elliot T et al. KEYNOTE-199 cohort (C) Phase II study of pembrolizumam (pembro) plus enzalutamide (enzo) for enzo resistante metastatic castration resistant prostate cancer. J Cin Oncol 2020; 38: 5543.
- Antonarakis E, Piulats J, Gross-Goupil M, Goh J, Vaishampayan U, De Wit R, Alanko T, FukasawanS, Tabata T, Feyerabend S Pembrolizumab monotherapy for treatment-refractory for docetaxol-pretreated metastatic castration resistant prostate cancer. Updated analyses with 4 years of follow-up from cohorts 1-3 of the KEYNOTE-199 study. Ann Oncol 2021; 32: S651-S652.
- Graff JN, Liang LW, Kim, J., Stenzel, A. Keynote-641: A phase 3 study of pembrolizumumab plus enzalutamide for metastatic asgration resisitant prostate cancer: Futr Oncol 2021; 17: 3107-3026.
- Powles T, Yuen KC, Gillessen S, Kadel EE 3rd; Rathkopf D, Matsubara N, Drake CG, Fizazi K, Piulats JM, Wysocki PJ et al. Atezolizumaba with enzautamide versus enzautamide alone in metastatic castration resistant prostate cancer. A randomized phase 3 trial. Nat Med 2022; 28: 144-153.
- Blanco B, Dominguez-Alonso C, Alvarez -Vallina, L. Bispecific immunomodulatory antibodies for cancer immunotherapy. Clin Cancer Res 2021; 27: 5457-5464).
- Heuls AM, Coupet TA, Sentman CL: Bispecific T-cell engagers for cancer immunotherapy. Immunol Cell Biol 2015; 93: 290-296).
- Zhou, S.-J.; Wei, J.; Su, S.; Chen, F.-J.; Qiu, Y.-D.; Liu, B.-R. Strategies for Bispecific Single Chain Antibody in Cancer Immunotherapy. J. Cancer 2017, 8, 3689–3696. [Google Scholar] [CrossRef]
- Gaspar M, Pravin J, Rodriques L, Uhlenbroich S, Everett KL, Wollerton F, Morrow M, Tuna M, Brevis, N. CD137/OX40 bispecfic antibody induces potent antitumor activity that is dependent on target coengagement. Cancer Immunol Res 2020; 8: 781-793.
- Lee SC, MA JS, Kim SC, Laborda E, Choi SH, Hampton EN, Yun H, NunezV, Muldong MT, Wu CN. A PMSA targeted bispecific antidody for prostate cancer driven by a small-moecular targeting ligand, Sci Adv 2021; 7: eab8193.
- Chiu D, Tavara R, Haber L, Aina OH, Vazzana K, Ram P, Danton M, Finney J, Jalal S, Krueger P A PMSA targeting CD3 bisoecific antibody induces antitumor responses that are enhanced by 4-1BB costimulation. Cancer Immunol Res 2020; 8: 595-608.
- Deegan P, Thomas O, Noal-Stevaux, O., Li, S. Wahl J, Bogner P, Aeffner F, Friedrich, M., Liao MZ, Mattes, K. The PSMA targeting half-life extended BiTE therapy AMG 160 has potent antitumoral activity in pre-clincal models of metastatic castration resistant prostate cancer. Clin Cancer Res 2021; 27: 2928-2937.
- Miyahira, A.K.; Soule, H.R. The 27th Annual Prostate Cancer Foundation Scientific Retreat Report. Prostate 2021, 81, 1107–1124. [Google Scholar] [CrossRef]
- Shah, D.; Soper, B.; Shopland, L. Cytokine release syndrome and cancer immunotherapies—Historical challenges and promising futures. Front. Immunol. 2023, 14, 1190379. [Google Scholar] [CrossRef]
- Yan, T., Zhu, L., Chen, J. Current advances and challenges in CAR-T therapy for solid tumors. Tumor associated antigens and the tumor microenvironment, Exp Hematol Oncol 2023; 12: 14.
- George P, Dasyam N, Giunti G, Mester B, Bauer E, Andrews B, Perera T, Ostapowicz T, Frampton, C., Li, P.,. Third generation anti CD19 chimeric antigen receptor T-cells incorporating a TRL2 domain for relapsed or refactory B-cel lymphoma: A phase I clinical trial protocol (ENABLE) BMJ Open 2020; 10: e034629.
- Roselli E, Boucher JC, Li G, Kotani H, Spitler K, Reid K, Cervantes EV, Bulliard Y, Tu N, Lee SB. 4-1BB and otimized CD28 costimulation enhances function of human mono-spefic and bi-specific thrd-generation CAR T cells. J Immunother Cancer 2021; 9: e003354.
- Ramos, C.A.; Rouce, R.; Robertson, C.S.; Reyna, A.; Narala, N.; Vyas, G.; Mehta, B.; Zhang, H.; Dakhova, O.; Carrum, G.; et al. In Vivo Fate and Activity of Second- versus Third-Generation CD19-Specific CAR-T Cells in B Cell Non-Hodgkin’s Lymphomas. Mol. Ther. 2018, 26, 2727–2737. [Google Scholar] [CrossRef]
- Kloss, C.C.; Lee, J.; Zhang, A.; Chen, F.; Melenhorst, J.J.; Lacey, S.F.; Maus, M.V.; Fraietta, J.A.; Zhao, Y.; June, C.H. Dominant-Negative TGF-β Receptor Enhances PSMA-Targeted Human CAR T Cell Proliferation And Augments Prostate Cancer Eradication. Mol. Ther. 2018, 26, 1855–1866. [Google Scholar] [CrossRef] [PubMed]
- Frieling JS, Tordesilla L, Bustos XE, Ramello MC, Bishop RT, Cianne JE, Snedal SA, Li T, Lo CH, de la Iglesia, J. gamma-delta enriched CAR-T therapy for bone metastastic castrate resistant prostate cancer. Sci Adv 2023; ): eadf0108.
- Zhang, Y.; Zhuang, Q.; Wang, F.; Zhang, C.; Xu, C.; Gu, A.; Zhong, W.H.; Hu, Y.; Zhong, X. Co-expression IL-15 receptor alpha with IL-15 reduces toxicity via limiting IL-15 systemic exposure during CAR-T immunotherapy. J. Transl. Med. 2022, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Dorff TB, Blanchard S, Martirosyan H, Adkins L, Dhapola G, Moriarty A, Wagner JR, Chaudhry A, D} Apuzzo M, Kuhn, P. Phase 1 study of PSCA-targetted CAR T cell therapy for metastatic Castration resistant prostate cancer (mCRPC) J Clin Oncol 2022; 40: 91.
- Pennisi, M.; Jain, T.; Santomasso, B.D.; Mead, E.; Wudhikarn, K.; Silverberg, M.L.; Batlevi, Y.; Shouval, R.; Devlin, S.M.; Batlevi, C.; et al. Comparing CAR T-cell toxicity grading systems: Application of the ASTCT grading system and implications for management. Blood Adv. 2020, 4, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Milowsky, M.I.; Nanus, D.M.; Kostakoglu, L.; Vallabhajosula, S.; Goldsmith, S.J.; Bander, N.H. Phase I Trial of Yttrium-90—Labeled Anti—Prostate-Specific Membrane Antigen Monoclonal Antibody J591 for Androgen-Independent Prostate Cancer. J. Clin. Oncol. 2004, 22, 2522–2531. [Google Scholar] [CrossRef]
- Hofman MS, Violet J, Hicks RJ, Ferdinandus J, Thang SP, Akhust T, Iravani A, Kong G, Ravi Kumar A, Murphy DG et al. [177Lu]-PSMA-617 radionuclide treatment in patients metastatic resistant prosateancer (luPSMA trial); a single centre, single arm, phase 2 study. Lancet Oncol 2018; 19: 825-833.
- Niaz MJ, Batra JS, Walsh RD, Ramirez-Font MK, Vallabhaajosulo S, Jhanwar YS, Molina AM, Nanus DM, Osborne JR, Bando NH et al., Pilot study of hyperfractionated dosing of lutetium-177-labelled anti.prostate specific membrane antigen momoclonal antibody J591 (1777Lu-J5911 for metastatic castration reistnat prostate cancer. Oncologist 2020; 25; 477-e895.
- Vlachostergios PJ, Niaz MJ, Skafida M, Mossallaie SA, Thomas C, Christos PJ, Osborne JR, Molina AM, Nanus DM, Bander NH, Tagawa ST. Imaging expression of prostate specific membrane antigen and response to PMSA targeted beta-emitting radionuclie therapies in metastatic castration resistant prostate cancer. Prostate 2021; 81: 279-285.
- Hofman MS, Emmett L, Vilet J, Iravani A, Joshua AM, Goh JC, Pattison DA, Tan TH, Kirkwood ID, Ng s et al. TheraP: A randomized phase 2 trial of 177 Lu-PMSA-617 theranostics vs cabazitaxel in progressive castration resistnante prostate cancer, (Clinical trial protocol ANZUP 1603) BJU Int 2019; 124 Suppl1: 5-13.
- US Food and Drug ASministration(FDA). FDA approves Pluvicto for metastatic castratin resistant prostate cancer. News release march 23, 2022, accessed december 2024 https://www.fda.gov/drugs/resources-information.approved-drugs/fda-approves-pluvicto-metastatic-castration-resistant-prostate-cancer.
- European Medicines Agency (EMA). Pluvicto: EPAR-medicine overview. European public assessment report December 21 Accessed December 2024.
- https://www.ema.europa.eu/en/documents/overview/pluvict0-par-medicine-overview_en.pdf.
- Arbuznikova, D.; Eder, M.; Grosu, A.-L.; Meyer, P.T.; Gratzke, C.; Zamboglou, C.; Eder, A.-C. Towards Improving the Efficacy of PSMA-Targeting Radionuclide Therapy for Late-Stage Prostate Cancer—Combination Strategies. Curr. Oncol. Rep. 2023, 25, 1363–1374. [Google Scholar] [CrossRef]
- Studies on prostatic cancer I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. 1941. 2002; 168: 9-12.
- Desai, K.; McManus, J.M.; Sharifi, N. Hormonal therapyfor prostate cancer. Endocr. Reiews 42, 354–373.
- Pantel, K.; Alix-Panabières, C. Bone marrow as a reservoir for disseminated tumor cells: A special source for liquid biopsy in cancer patients. BoneKEy Rep. 2014, 3, 584. [Google Scholar] [CrossRef]
- Sun GY, Jing H, Wang SL, Song YW, Jun, J., Fang H et al. Trastuzumab provides a comparable prognosis in patients with HER-2 positve breast cancer to those with HER-2 negative breast cancer: Post hoc analyses of a randomised controlled trial of post mastectomy hypofractionated radiotherapy. Front. Oncol. 2021, 10, 605750.
- Wu XQ, Ge, YP, Gong XL, Liu, Y., Bai CM. Advances in the treatment of human epidermal growth factor receptor2 positive gastric cancer. Zhongguo Yi Xue Ke Xue Yuan Xue Bao2022; 44: 899-905.
- Murray, N.P.; Aedo, S.; Fuentealba, C.; Reyes, E.; Salazar, A.; Lopez, M.A.; Minzer, S.; Orrego, S.; Guzman, E. Subtypes of minimal residual disease, association with Gleason score, risk and time to biochemical failure in pT2 prostate cancer treated with radical prostatectomy. ecancermedicalscience 2019, 13, 934. [Google Scholar] [CrossRef]
- Bubenik, J.; Simová, J. Minimal residual disease as the target for immunotherapy and gene therapy of cancer (Review). Oncol. Rep. 2005, 14, 1377–1380. [Google Scholar]
Figure 1.
Effects of prostate cancer on he immune system.
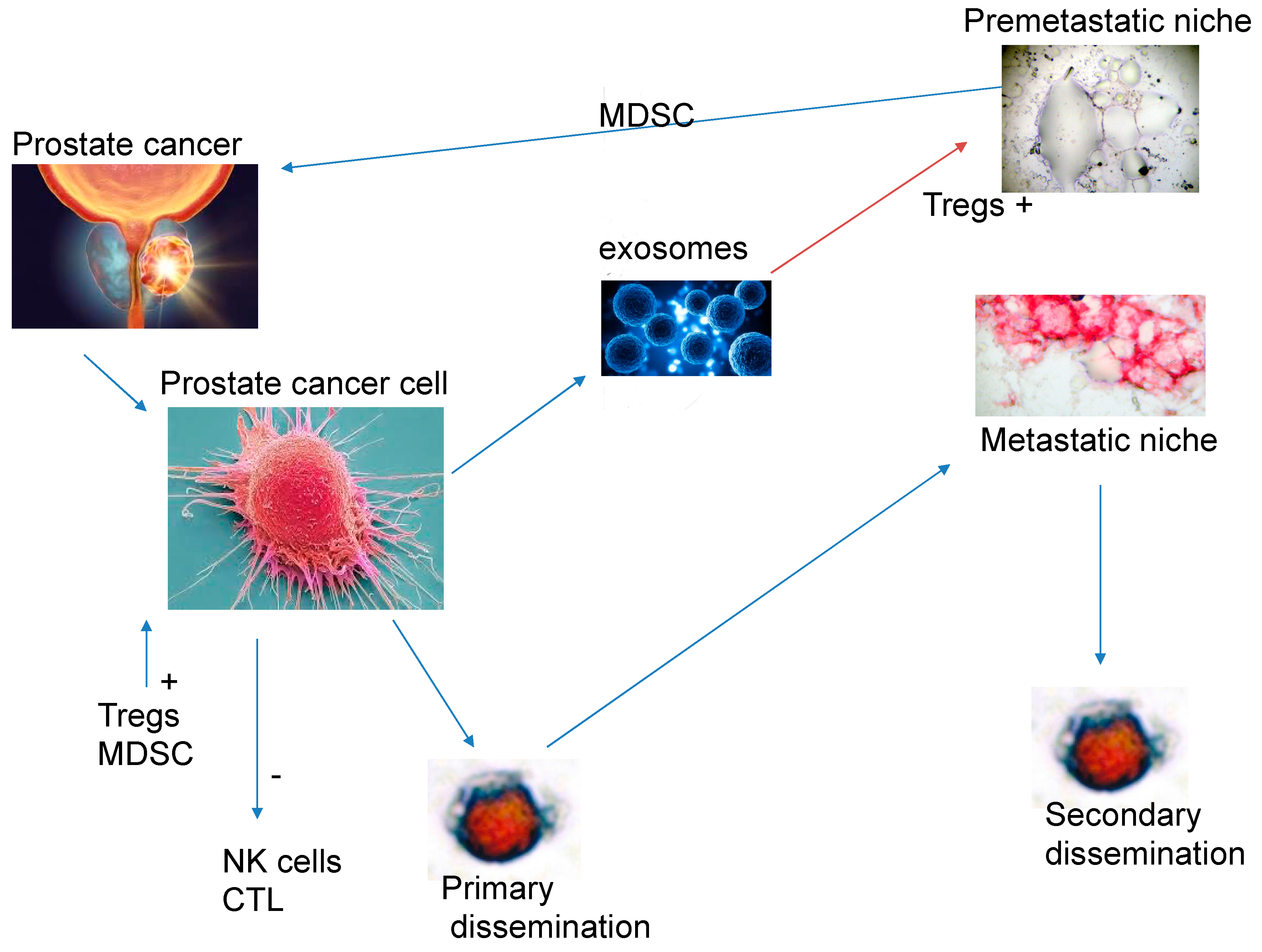
Figure 2.
The action of a BiTE expressing bivalent antidoies against PMSA and permitting the binding to T-cell CD3 epitope.
Figure 2.
The action of a BiTE expressing bivalent antidoies against PMSA and permitting the binding to T-cell CD3 epitope.

Figure 3.
Bone marrow biopsy sample negative for PSA expressing cells.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



