Submitted:
04 March 2025
Posted:
05 March 2025
You are already at the latest version
Abstract
This review examines the potential of herbal medicines in treating hypothyroidism, a condition marked by a deficiency of thyroid hormones. Hypothyroidism is common in the United States, affecting approximately 4.6% of the population, with higher rates observed in females and the elderly. The review aims to provide a thorough overview of the current state of research on herbal treatment for hypothyroidism. Despite these promising findings, the review highlights the limitations of current research, including the lack of large-scale, high-quality clinical trials and concerns regarding long-term safety and efficacy. The review emphasizes the need for further rigorous research to validate the benefits and safety of these herbal medicines and to explore their mechanisms of action in greater detail. By addressing these gaps in knowledge, the review aims to contribute to the development of more effective and safer treatment options for patients with hypothyroidism. The outcomes of this review for the field of study include the potential inclusion of herbal medicines into treatment protocols, offering a natural and potentially safer alternative to conventional thyroid treatments. Future research directions suggested by the review include conducting large-scale randomized controlled trials and investigating the interactions between herbal medicines and conventional treatments.
Keywords:
Hypothyroidism
; Thyroid-stimulating hormone
; thyroid function
1. Introduction
Hypothyroidism is a major public health issue in the United States, affecting a substantial portion of the population. The prevalence of hypothyroidism in the USA is around 4.6%, with 4.3% attributed to subclinical hypothyroidism and 0.3% to overt hypothyroidism [1]. The prevalence of overt and subclinical hypothyroidism in the USA is reported to be 0.4% and 9%, respectively [2]. Recent studies have shown that the prevalence of hypothyroidism has increased markedly over the past two decades, with almost 10% of the US population affected between 2009-2012, and this percentage increasing to 11.7% by 2019 [3]. This increase is particularly notable among females and those older than 60 years of age [3].
Hypothyroidism is caused by a deficiency of thyroid hormones due to various factors. The most common cause in iodine-sufficient areas is Hashimoto's thyroiditis, an autoimmune condition [4,5]. In iodine-deficient regions, the primary cause is iodine deficiency [6,7]. Other causes include autoimmune thyroiditis, thyroidectomy, thyroid ablation, and certain medications [8]. Environmental factors such as thyroid-disrupting chemicals, iodine supply variations, and drugs interfering with thyroid function also contribute to hypothyroidism [9]. Additionally, autoimmune thyroiditis, iodine deficiency, radioiodine ablation, and surgery are significant causes in the elderly population [10]
The current standard treatment for hypothyroidism involves the use of synthetic thyroid hormones, such as levothyroxine. While effective, these treatments can have side effects and are dependent on a stable supply chain. This has led to an interest in exploring alternative treatments, including herbal medicines, which may offer a more natural and potentially safer approach to managing hypothyroidism. Herbal medicines have shown promise in improving thyroid function and normalizing thyroid hormone levels.
Despite the promising potential of these herbal medicines, there are limitations to their current use. The lack of large-scale, high-quality clinical trials and concerns regarding long-term safety and efficacy need to be addressed through rigorous research. Future studies should focus on validating the benefits and safety of these herbal medicines and exploring their mechanisms of action in greater detail. By addressing these gaps in knowledge, we can better incorporate herbal medicines into treatment protocols, offering patients a natural and potentially safer alternative for managing hypothyroidism.
This review aims to provide a thorough overview of the current state of research on herbal medicines for treating hypothyroidism, discussing their potential benefits, limitations, and future directions. By examining the evidence and identifying areas for further research, we hope to contribute to the development of more effective and safer treatment options for patients with hypothyroidism.
2. Herbal Treatment for Hypothyroidism
Hypothyroidism results from a deficiency of thyroid hormones due to various factors. Iodine is a significant factor [6,7], though autoimmune conditions can also be causal [4,5]. Environmental factors such as thyroid-disrupting chemicals, iodine supply variations, and drugs interfering with thyroid function also contribute to hypothyroidism [9].
Normal thyroid function depends on a variety of trace elements for thyroid hormone synthesis and metabolism, which interact with each other and are in a dynamic balance [11]. Thyroid hormones are known for controlling the metabolism of lipids, carbohydrates, proteins, minerals, and electrolytes, and for regulating body temperature. Normal thyroid status depends on the chemical/elemental composition of body fluids and tissues, which changes depending on physiological state, lifestyle, and environment [12].
2.1. Biomarkers for Diagnosing Hypothyroidism
Hypothyroidism is primarily diagnosed through the measurement of thyroid hormones and thyroid-stimulating hormone (TSH). The most common biomarkers include serum levels of T3, T4, and TSH. In primary hypothyroidism, there is a reduction in T4 and T3 with a corresponding increase in serum TSH [13]. These biomarkers are essential for confirming the diagnosis and guiding treatment. The measurement of serum TSH levels is the most common method for determining thyroid hormone status. Elevated TSH levels indicate hypothyroidism, while low levels suggest hyperthyroidism. Direct tests include measuring T3, T4, free-T4, free-T3, T4 resin uptake, free T4 index, T4 binding globulin, and anti-TPO [13]. These tests provide a thorough assessment of thyroid function and help in diagnosing hypothyroidism accurately. This review, for the sake of brevity, focuses on interventions which have been tested for their impact on TSH.
3. Interventions for Hypothyroidism
We perform a literature search on the interventions that can result in an improvement in thyroid function, as measured by TSH levels. Several herbal and nutraceutical interventions have been tested for their impact on hypothyroidism. These are included below in Table 1 and Figure 1 for those reporting their values as a change in TSH.
The treatments from the search with the greatest effect on TSH are included below, the four interventions with the largest clinical effects, with 95% CIs not crossing zero. These interventions are selenomethione, shadhushana charna, ginger, and ashwagandha.
3.1. Selenomethionine
Selenomethionine is a an organic form of the trace element selenium which is conjugated with the amino acid methionine, helping with bioavailability and absorbtion. The thyroid gland of an adult human contains the highest concentration of selenium out of any organ in the body [36]. A class of proteins called selenoproteins are synthesized using selenium, and several of these are involved in thyroid hormone metabolism [36]. Selenomethionine supplementation, especially when coupled with myo-inositol, was shown to produce a lowering of TSH relative to the control group [14].
3.2. Shadushana Churna
Shadushana Churna (SC) is a polyherbal formulation used in Ayurvedic medicine, composed of the elements in Table 2 [16]. In a trial comparing the effects of SC with Vyoshadi Guggulu (VG), SC reduced TSH by 26.29% or 1.892ng/mL while VG reduced TSH by 16.61% or 1.156ng/mL. The decrease for each therapy was significant, however, the difference of decrease in TSH between SC and VG was not statistically signicant.
3.3. Ginger
Ginger, or Zingiber officinale, a common ingredient in many dishes, may exert anti-hypothyroid effects via anti-inflammatory or anti-oxidant pathways [39], or potentially through metabolic regulation[40] or protection of the thyroid gland from damage [41].
A double blind placebo controlled trial observed significant improvements in TSH levels with ginger supplementation -1.84ng/mL relative to placebo (p<0.001), when patients were given 500mg of ginger twice per day for 30 days [17]. These findings suggest possible clinical utility for ginger in treating hypothyroidism.
3.4. Ashwagandha
Ashwagandha (Withania somnifera) is an adaptogenic herb known for its potential role in modulating thyroid function through various physiological mechanisms [42]. Its bioactive compounds, including withanolides, alkaloids, and saponins, contribute to its therapeutic effects. Withanolides exhibit anti-inflammatory and antioxidant properties, alkaloids provide neuroprotective effects, and saponins enhance Ashwagandha’s adaptogenic properties, helping the body cope with physiological stress [43]. Given these properties, Ashwagandha has been increasingly studied for its ability to support thyroid regulation.
Ashwagandha influences thyroid function through multiple pathways. Research suggests that it can stimulate the secretion of thyroid hormones, increasing T3 and T4 levels [43]. Additionally, its adaptogenic effect reduces cortisol, mitigating stress-induced suppression of thyroid function. Its strong antioxidant profile also helps protect thyroid cells from oxidative damage [43]. A randomized, double-blind, placebo-controlled trial by Sharma et al. (2017) found that daily supplementation of 600 mg of Ashwagandha for eight weeks resulted in a 41.5% increase in T3, a 16% increase in T4, and a significant reduction in TSH (p < 0.001), with minimal transient adverse effects [44]. Another 60-day clinical study by Lopresti et al. (2023) demonstrated a 23% reduction in morning cortisol levels, improved stress markers, and indirect support for thyroid function [45].
4. Conclusions
This work aims to provide guidance for the development of integrative treatements for hypothyroidism. Several herbas and nutraceuticals may be beneficial for cases of hypothyroidism, and we have provided an overview of the current studies on non-pharmaceutical agents for the treatment of hypothyroidism. The most promising agents include selenomethione, shadhushana charna, ginger, and ashwagandha. These agents, as well as the others identified, albeit with lower priorirty, should be subject to further validation. The treatment of hypothyroidism is a pressing chronic condition for people in developed countries, even with abundant trace minerals (such as iodine) for proper thyroid function.
The above treatments are non-pharmaceutical and may be able to be used as part of an integrative treatment plan, as these approaches are gaining popularity [46], and may avoid the side effects of pharmaceuticals used for hypothyroidism [47]. Furthermore, for cases of subclinical hypothyroidism, as affects 4.3% of Americans [1], a lesser degree of intervention can correct thyroid function, and nutraceuticals may be useful in that role.
References
- Zúñiga, D.; Balasubramanian, S.; Mehmood, K.T.; Al-Baldawi, S.; Zúñiga Salazar, G. Hypothyroidism and Cardiovascular Disease: A Review. Cureus 2024, 16, e52512. [Google Scholar] [CrossRef] [PubMed]
- Shu, Q.; Kang, C.; Li, J.; Hou, Z.; Xiong, M.; Wang, X.; Peng, H. Effect of Probiotics or Prebiotics on Thyroid Function: A Meta-Analysis of Eight Randomized Controlled Trials. PLOS ONE 2024, 19, e0296733. [Google Scholar] [CrossRef]
- Vol 16 Issue 8, p. 5-6. American Thyroid Association.
- Chiovato, L.; Magri, F.; Carlé, A. Hypothyroidism in Context: Where We’ve Been and Where We’re Going. Adv Ther 2019, 36, 47–58. [Google Scholar] [CrossRef]
- Hennessey, J.V.; Espaillat, R. Subclinical Hypothyroidism: A Historical View and Shifting Prevalence. Int J Clin Pract 2015, 69, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Cherim, A.; Petca, R.-C.; Dumitrascu, M.-C.; Petca, A.; Candrea, E.; Sandru, F. Thyroid Disorders in Systemic Sclerosis: A Comprehensive Review. J Clin Med 2024, 13, 415. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Leung, A.A.C. Evaluation and Management of the Child with Hypothyroidism. World J Pediatr 2019, 15, 124–134. [Google Scholar] [CrossRef]
- Bashkin, A.; Nodelman, M. [THE CLINICAL APPROACH TO DIAGNOSIS AND TREATMENT OF HYPOTHYROIDISM]. Harefuah 2017, 156, 322–325. [Google Scholar]
- Vigone, M.C.; Di Frenna, M.; Weber, G. Heterogeneous Phenotype in Children Affected by Non-Autoimmune Hypothyroidism: An Update. J Endocrinol Invest 2015, 38, 835–840. [Google Scholar] [CrossRef]
- Vacante, M.; Biondi, A.; Basile, F.; Ciuni, R.; Luca, S.; Di Saverio, S.; Buscemi, C.; Vicari, E.S.D.; Borzì, A.M. Hypothyroidism as a Predictor of Surgical Outcomes in the Elderly. Front Endocrinol (Lausanne) 2019, 10, 258. [Google Scholar] [CrossRef]
- Zhou, Q.; Xue, S.; Zhang, L.; Chen, G. Trace Elements and the Thyroid. Front Endocrinol (Lausanne) 2022, 13, 904889. [Google Scholar] [CrossRef]
- Błażewicz, A.; Wiśniewska, P.; Skórzyńska-Dziduszko, K. Selected Essential and Toxic Chemical Elements in Hypothyroidism-A Literature Review (2001-2021). Int J Mol Sci 2021, 22, 10147. [Google Scholar] [CrossRef] [PubMed]
- Sharma, H.; Kakadiya, J. Different Novel Biomarkers Involved in Diagnosing Hypothyroidism. The Egyptian Journal of Internal Medicine 2023, 35, 28. [Google Scholar] [CrossRef]
- Zuhair, V.; Shaikh, A.T.; Shafi, N.; Babar, A.; Khan, A.; Sadiq, A.; Ashraf, M.A.; Nihan, K.; Hamza, M.; Khalid, B.; et al. Role of Supplementation with Selenium and Myo-Inositol vs. Selenium Alone in Patients of Autoimmune Thyroiditis: A Systematic Review and Meta-Analysis 2024.
- Farhangi, M.A.; Dehghan, P.; Tajmiri, S.; Abbasi, M.M. The Effects of Nigella Sativa on Thyroid Function, Serum Vascular Endothelial Growth Factor (VEGF) – 1, Nesfatin-1 and Anthropometric Features in Patients with Hashimoto’s Thyroiditis: A Randomized Controlled Trial. BMC Complement Altern Med 2016, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.B.; Padhar, B.C.; Meena, H.M.L.; Mathur, S.K. Efficacy of Vyoshadi Guggulu and Shadushana Churna in the Management of Subclinical Hypothyroidism: An Open Labelled Randomized Comparative Pilot Clinical Trial. AYU (An International Quarterly Journal of Research in Ayurveda) 2020, 41, 181. [Google Scholar] [CrossRef]
- Ashraf, H.; Heydari, M.; Shams, M.; Zarshenas, M.M.; Tavakoli, A.; Sayadi, M. Efficacy of Ginger Supplementation in Relieving Persistent Hypothyroid Symptoms in Patients with Controlled Primary Hypothyroidism: A Pilot Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Evidence-Based Complementary and Alternative Medicine 2022, 2022, 5456855. [Google Scholar] [CrossRef]
- Sharma, A.K.; Basu, I.; Singh, S. Efficacy and Safety of Ashwagandha Root Extract in Subclinical Hypothyroid Patients: A Double-Blind, Randomized Placebo-Controlled Trial. The Journal of Alternative and Complementary Medicine 2018, 24, 243–248. [Google Scholar] [CrossRef]
- Luo, J.; Zhou, L.; Sun, A.; Yang, H.; Zhang, P.; Liu, K.; Yu, X.; Lin, Y.; Huang, Y.; Han, L. Herbal Medicine for Hashimoto’s Thyroiditis: A Systematic Review and Network Meta-Analysis. Journal of Ethnopharmacology 2024, 323, 117663. [Google Scholar] [CrossRef]
- Wei, M.; Ma, W.; Zhang, W.; Yin, D.; Tang, Y.; Jia, W.; Jiang, Y.; Wang, C.; Gong, Y. Efficacy and Safety of Ophiocordyceps Sinensis in the Treatment of Hashimoto’s Thyroiditis: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2023, 14. [Google Scholar] [CrossRef]
- An, J.H.; Kim, Y.J.; Kim, K.J.; Kim, S.H.; Kim, N.H.; Kim, H.Y.; Kim, N.H.; Choi, K.M.; Baik, S.H.; Choi, D.S.; et al. L-Carnitine Supplementation for the Management of Fatigue in Patients with Hypothyroidism on Levothyroxine Treatment: A Randomized, Double-Blind, Placebo-Controlled Trial. Endocrine Journal 2016, 63, 885–895. [Google Scholar] [CrossRef]
- Zhao, G.; Wang, Z.; Ji, J.; Cui, R. Effect of Coffee Consumption on Thyroid Function: NHANES 2007-2012 and Mendelian Randomization. Front. Endocrinol. 2023, 14. [Google Scholar] [CrossRef]
- Zavros, A.; Andreou, E.; Aphamis, G.; Bogdanis, G.C.; Sakkas, G.K.; Roupa, Z.; Giannaki, C.D. The Effects of Zinc and Selenium Co-Supplementation on Resting Metabolic Rate, Thyroid Function, Physical Fitness, and Functional Capacity in Overweight and Obese People under a Hypocaloric Diet: A Randomized, Double-Blind, and Placebo-Controlled Trial. Nutrients 2023, 15, 3133. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Wei, J.; Wang, L.; Wang, Q.; Zhao, J.; Chen, S.; Wei, F. Effects of Selenium Supplementation on Graves’ Disease: A Systematic Review and Meta-Analysis. Evidence-Based Complementary and Alternative Medicine 2018, 2018, e3763565. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.F.; Venn, B.J.; Manning, P.J.; Cameron, C.M.; Skeaff, S.A. Iodine Supplementation of Mildly Iodine-Deficient Adults Lowers Thyroglobulin: A Randomized Controlled Trial. The Journal of Clinical Endocrinology & Metabolism 2016, 101, 1737–1744. [Google Scholar] [CrossRef]
- Javidi, N.; Khorasani, Z.M.; Salari, R.; Niroumand, S.; Yousefi, M. Achievements in Hypothyroidism Treatment with Herbal Medicine: A Systematic Review of Randomized Controlled Trials. Current Drug Discovery Technologies 2023, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, E.; Golgiri, F.; Janani, L.; Moradi, N.; Fallah, S.; Abiri, B.; Vafa, M. Randomized Study of the Effects of Zinc, Vitamin A, and Magnesium Co-Supplementation on Thyroid Function, Oxidative Stress, and Hs-CRP in Patients with Hypothyroidism. Biol Trace Elem Res 2021, 199, 4074–4083. [Google Scholar] [CrossRef]
- Yavari, M.; Akbari, M.; Ramezani Ahmadi, A.; Siavash Dastjerdi, M.; Hashemi, M.S. Investigating the Effect of Combined Use of Selenium and Myo-Inositol Supplements on Thyroid Function and Autoimmune Characteristics in Thyroid Disorders: A Systematic Review and Meta-Analysis. Expert Review of Endocrinology & Metabolism 2024, 19, 269–277. [Google Scholar] [CrossRef]
- Nordio, M. A Novel Treatment for Subclinical Hyperthyroidism: A Pilot Study on the Beneficial Effects of l-Carnitine and Selenium. Eur Rev Med Pharmacol Sci 2017, 21, 2268–2273. [Google Scholar]
- Jiang, H.; Chen, X.; Qian, X.; Shao, S. Effects of Vitamin D Treatment on Thyroid Function and Autoimmunity Markers in Patients with Hashimoto’s Thyroiditis—A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Pharmacy and Therapeutics 2022, 47, 767–775. [Google Scholar] [CrossRef]
- Wang, S.; Wu, Y.; Zuo, Z.; Zhao, Y.; Wang, K. The Effect of Vitamin D Supplementation on Thyroid Autoantibody Levels in the Treatment of Autoimmune Thyroiditis: A Systematic Review and a Meta-Analysis. Endocrine 2018, 59, 499–505. [Google Scholar] [CrossRef]
- Dineva, M.; Fishpool, H.; Rayman, M.P.; Mendis, J.; Bath, S.C. Systematic Review and Meta-Analysis of the Effects of Iodine Supplementation on Thyroid Function and Child Neurodevelopment in Mildly-to-Moderately Iodine-Deficient Pregnant Women. The American Journal of Clinical Nutrition 2020, 112, 389–412. [Google Scholar] [CrossRef]
- Hoang, T.D.; Olsen, C.H.; Mai, V.Q.; Clyde, P.W.; Shakir, M.K.M. Desiccated Thyroid Extract Compared with Levothyroxine in the Treatment of Hypothyroidism: A Randomized, Double-Blind, Crossover Study. J Clin Endocrinol Metab 2013, 98, 1982–1990. [Google Scholar] [CrossRef]
- Shimomura, Y.; Kobayashi, I.; Maruto, S.; Ohshima, K.; Mori, M.; Kamio, N.; Fukuda, H. Effect of Gamma-Oryzanol on Serum TSH Concentrations in Primary Hypothyroidism. Endocrinol Jpn 1980, 27, 83–86. [Google Scholar] [CrossRef]
- Dai, X.; Zhou, Y.; Yu, X. [Effect of ginseng injection in treating congestive heart failure and its influence on thyroid hormones]. Zhongguo Zhong Xi Yi Jie He Za Zhi 1999, 19, 209–211. [Google Scholar] [PubMed]
- Wang, F.; Li, C.; Li, S.; Cui, L.; Zhao, J.; Liao, L. Selenium and Thyroid Diseases. Front Endocrinol (Lausanne) 2023, 14, 1133000. [Google Scholar] [CrossRef] [PubMed]
- Lyons, M.P.; Papazyan, T.T.; Surai, P.F. Selenium in Food Chain and Animal Nutrition: Lessons from Nature -Review-. Asian-Australasian Journal of Animal Sciences 2007, 20, 1135–1155. [Google Scholar]
- Schrauzer, G.N. Selenomethionine: A Review of Its Nutritional Significance, Metabolism and Toxicity. The Journal of Nutrition 2000, 130, 1653–1656. [Google Scholar] [CrossRef] [PubMed]
- Al-Amoudi, W.M. Toxic Effects of Lambda-Cyhalothrin, on the Rat Thyroid: Involvement of Oxidative Stress and Ameliorative Effect of Ginger Extract. Toxicol Rep 2018, 5, 728–736. [Google Scholar] [CrossRef]
- Jafarnejad, S.; Keshavarz, S.A.; Mahbubi, S.; Saremi, S.; Arab, A.; Abbasi, S.; Djafarian, K. Effect of Ginger (Zingiber Officinale) on Blood Glucose and Lipid Concentrations in Diabetic and Hyperlipidemic Subjects: A Meta-Analysis of Randomized Controlled Trials. Journal of Functional Foods 2017, 29, 127–134. [Google Scholar] [CrossRef]
- Mohammed, E.T.; Hashem, K.S.; Ahmed, A.E.; Aly, M.T.; Aleya, L.; Abdel-Daim, M.M. Ginger Extract Ameliorates Bisphenol A (BPA)-Induced Disruption in Thyroid Hormones Synthesis and Metabolism: Involvement of Nrf-2/HO-1 Pathway. Sci Total Environ 2020, 703, 134664. [Google Scholar] [CrossRef]
- Institute of Functional Medicine Specialization The Efficacy of Ashwagandha Root Extract for Hypothyroidism. [Internet]. Available from: Https://Institutodeespecializacionenmedicinafuncional.Com.
- Ashwagandha in hypothyroidism Available from: Ashwagandha in Hypothyroidism.Pdf.
- Sharma, A.K.; Basu, I.; Singh, S. Efficacy and Safety of Ashwagandha Root Extract in Subclinical Hypothyroid Patients: A Double-Blind, Randomized Placebo-Controlled Trial. The Journal of Alternative and Complementary Medicine 2018, 24, 243–248. [Google Scholar] [CrossRef]
- Arumugam, V.; Vijayakumar, V.; Balakrishnan, A.; B Bhandari, R.; Boopalan, D.; Ponnurangam, R.; Sankaralingam Thirupathy, V.; Kuppusamy, M. Effects of Ashwagandha (Withania Somnifera) on Stress and Anxiety: A Systematic Review and Meta-Analysis. EXPLORE 2024, 20, 103062. [Google Scholar] [CrossRef] [PubMed]
- Song, E.; Ang, L.; Lee, M.S. Increasing Trends and Impact of Integrative Medicine Research: From 2012 to 2021. Integr Med Res 2022, 11, 100884. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.A.; Stem, L.A.; Bruehlman, R.D. Hypothyroidism: Diagnosis and Treatment. afp 2021, 103, 605–613. [Google Scholar]
Figure 1.
Herbal and nutraceutical treatments for HT as a forest plot with 95% confidence intervals.
Figure 1.
Herbal and nutraceutical treatments for HT as a forest plot with 95% confidence intervals.
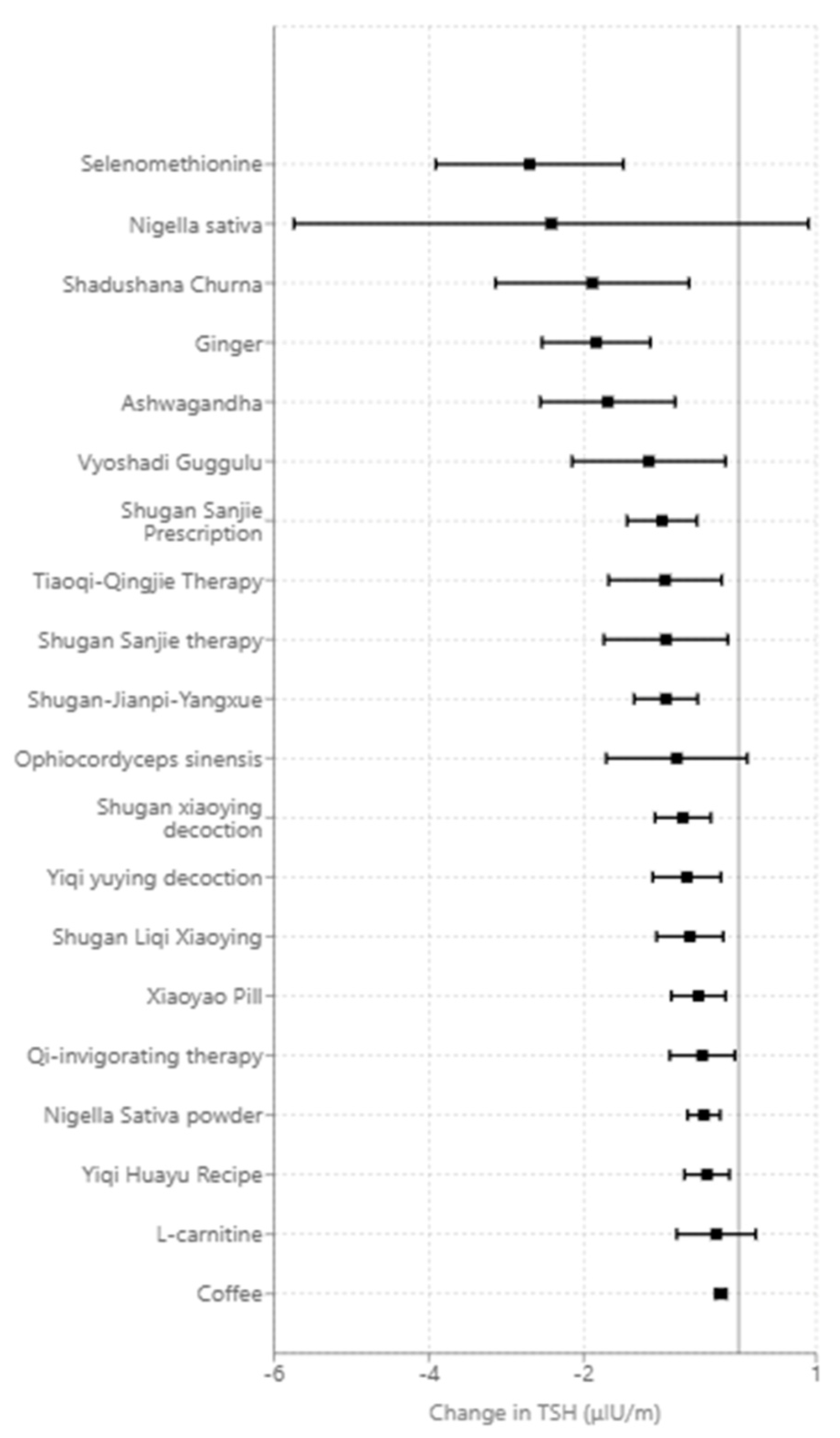

Table 1.
Herbal medicines tested for efficacy in hypothyroidism.
| Intervention | Impact on Thyroid Stimulating Hormone (TSH) (μIU/m) relative to placebo or baseline |
|---|---|
| Selenomethionine and myo-inositol | -3.10 [-4.25,-1.95] [14] |
| Selenomethionine | -2.70[-3.91,-1.49] [14] |
| Nigella sativa | -2.42 [−5.74,0.90] n.s. [15] |
| Shadushana Churna | -1.89[-3.14,−0.64] [16] |
| Ginger | -1.84 [-2.54,-1.14] [17] |
| Ashwagandha | -1.69[-2.56, -0.82] [18] |
| Vyoshadi Guggulu | -1.16[-2.15,-0.16] [16] |
| Shugan Sanjie Prescription | -0.99 [-1.44, -0.68] [19] |
| Tiaoqi-Qingjie Therapy | -0.95 [-1.68, -0.54] [19] |
| Shugan Sanjie therapy | -0.94 [-1.74, -0.50] [19] |
| Shugan-Jianpi-Yangxue medicine | -0.94 [-1.35, -0.66] [19] |
| Ophiocordyceps sinensis | -0.80[-1.71,0.11] n.s. [20] |
| Shugan xiaoying decoction | -0.72 [-1.08, -0.48] [19] |
| Yiqi yuying decoction | -0.67 [-1.11, -0.40] [19] |
| Shugan Liqi Xiaoying formula | -0.63 [-1.06, -0.38] [19] |
| Xiaoyao Pill | -0.52 [-0.87, -0.31] [19] |
| Qi-invigorating phlegm and Blood-Activating Therapy | -0.47 [-0.89, -0.25] [19] |
| Nigella Sativa powder | -0.45 [-0.66, -0.30] [19] |
| Yiqi Huayu Recipe | -0.41 [-0.70, -0.24] [19] |
| L-carnitine | -0.29[-0.80, 0.22] n.s. [21] |
| Coffee | -0.23[-0.30, -0.16] [22] |
| Zinc and Selenium | n.s. [23] |
| Selenium | n.s. [24] |
| Iodine | n.s. [25] |
| Probiotics | n.s. [2] |
| Mentha x Piperita | n.s. [26] |
| Zinc, Vitamin A, and Magnesium Co-supplementation | n.s. [27] |
| Selenium and Myo-inositol | n.s. [28] |
| l-carnitine and selenium | n.s. [29] |
| Vitamin D | n.s. [30]n.s. [31] |
| Iodine | n.s. [32] |
| Thyroid extract | n.s. [33] |
| Gamma-oryzanol (rice bran extract_ | n.s. [34] |
| Ginseng | n.s. [35] |
* Case study.
Table 2.
The composition of Shushanda Churna. Reproduced from [16] under a Creative Commons Attribution-NonCommercial-ShareAlike License (CC BY-NC-SA).
Table 2.
The composition of Shushanda Churna. Reproduced from [16] under a Creative Commons Attribution-NonCommercial-ShareAlike License (CC BY-NC-SA).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



