Submitted:
05 March 2025
Posted:
05 March 2025
Read the latest preprint version here
Abstract
Background: Nepal’s diverse geography creates significant challenges for healthcare accessibility, particularly for neonatal care. Rural areas, especially in the mountainous regions, face severe healthcare gaps due to isolation, inadequate infrastructure, and a shortage of skilled staff. Strengthening healthcare in these underserved regions is essential to reducing neonatal mortality.
Methods: A comprehensive literature search identified studies on neonatal mortality and interventions, particularly Helping Babies Breathe (HBB), analyzed using a narrative synthesis approach. The review examined disparities in neonatal health outcomes, regional differences, and barriers to healthcare access.
Findings: The review identified key themes related to healthcare disparities, neonatal mortality, and birth outcomes in Nepal's remote regions. Geographical isolation, inadequate healthcare infrastructure, and cultural barriers contribute to persistently high neonatal mortality, particularly in mountainous areas such as Jumla and Dolpa, where rates exceed 60 per 1,000 live births. HBB has shown a significant impact, reducing neonatal mortality by up to 60% when effectively implemented. However, infrastructural gaps, lack of emergency transport, and the uneven distribution of skilled birth attendants (SBAs) remain critical challenges. Addressing these disparities requires expanded training, increased availability of neonatal resuscitation equipment, and culturally sensitive healthcare strategies.
Recommendations: Future research should explore sustainable neonatal resuscitation training, telemedicine support, and emergency referral systems to improve neonatal survival in remote Nepal. Further studies on healthcare infrastructure gaps and policy-driven interventions are needed to enhance maternal and newborn care.
Conclusions: While HBB and other neonatal interventions have demonstrated success in reducing neonatal mortality, their impact is limited by persistent disparities in healthcare infrastructure, workforce availability, and geographic inaccessibility. To achieve sustainable reductions in neonatal mortality, a multi-faceted approach combining expanded SBA training, improved emergency healthcare infrastructure, and community-based interventions is essential.
Keywords:
Neonatal mortality
; Nepal
; Remote regions
; Rural healthcare
; Healthcare disparities
; Health equity
; Skilled birth attendants (SBAs)
; Neonatal resuscitation
; Helping Babies Breathe (HBB)
; Resource-limited settings
; Comprehensive Emergency Obstetric and Neonatal Care (CEmONC)
1. Introduction
1.1. Geographical Barriers to Healthcare Access
Nepal’s geography presents significant challenges to healthcare accessibility, particularly in the provision of neonatal care. The country is divided into three main regions: the Terai (plains), hilly region, and mountainous region. While the Terai and lower hilly regions have relatively better healthcare services, mountainous areas, which cover 15% of Nepal’s landmass, face extreme barriers due to their harsh climate, rugged terrain, and sparse population distribution [1,2]. Many communities in these remote regions, including districts such as Dolpa and Jumla, have limited access to essential health services, resulting in critical delays in receiving medical care [3,4].
The geographical isolation of Nepal’s mountainous regions means that reaching a healthcare facility often requires several hours or even days of travel on foot. The lack of roads and emergency transportation further exacerbates the challenge, increasing the likelihood of adverse neonatal outcomes [5,6]. In some cases, air transport is the only viable option for emergency medical evacuations, yet it remains rare and costly [7]. The combination of these factors contributes directly to high neonatal mortality rates, with some districts reporting rates exceeding 60 per 1,000 live births [8]. Addressing these barriers requires improvements in local healthcare infrastructure, emergency transport systems, and the availability of trained healthcare personnel in remote areas. A study in 2000 suggested that up to 36,443 neonatal deaths in Nepal could be prevented by 2030 if comprehensive interventions were implemented to enhance healthcare accessibility [6]. Recent research from Indonesia reinforces this, highlighting that rapid access to quality institutional delivery care is a key determinant of neonatal survival in underserved regions, where targeted improvements in healthcare infrastructure and skilled birth attendance have the potential to avert thousands of preventable deaths [9].
1.2. Healthcare Infrastructure and Access in Nepal
Nepal’s healthcare system remains highly centralized, with most advanced medical facilities located in urban centers, leaving rural and mountainous regions severely under-resourced [10]. As of 2021, Nepal had 3,789 health posts, 3,176 sub-health posts, 125 hospitals, and 203 primary healthcare centers [10]. Health posts serve as the primary healthcare provider for many rural populations, yet they often face shortages of trained staff and medical supplies, reducing their effectiveness in addressing neonatal health needs [11].
Despite the existence of a referral system linking health posts to district and regional hospitals, its implementation is ineffective in many remote regions. In districts such as Mugu and Humla, the nearest hospitals are over eight hours away on foot, and emergency transportation is virtually nonexistent [12]. This lack of access leads many women to rely on untrained traditional birth attendants, increasing the risk of complications during childbirth [13]. Furthermore, cultural preferences for home births persist, as hospital deliveries are often perceived as inaccessible or unnecessary [14]. Historically, the absence of skilled birth attendants (SBA) in these settings has resulted in a higher prevalence of neonatal complications, including asphyxia, infection, and hypothermia [6].
Efforts to improve neonatal health outcomes must focus on expanding the number of trained birth attendants [7], ensuring a steady supply of essential neonatal care equipment [15], and developing a more efficient emergency transport infrastructure [2]. Without these improvements, the disparities in neonatal survival rates between urban and rural regions will remain a persistent challenge.
1.3. Neonatal Mortality and Health Disparities in Remote Nepal
While Nepal has made progress in reducing overall neonatal mortality, significant regional disparities remain. The national neonatal mortality rate (NMR) stands at 21 per 1,000 live births, yet in remote mountainous regions, the rate surpasses 60 per 1,000 [7,8]. Dolpa district, in particular, reports an NMR of 67 per 1,000 live births, one of the highest in the country. The broader mountain region maintains an average neonatal mortality rate of 46 per 1,000, nearly double the national average [13]. These statistics demonstrate the stark inequalities in neonatal health outcomes between urban and remote areas.
A major factor contributing to high neonatal mortality in remote Nepal is the prevalence of home births, often occurring in unsafe environments such as animal sheds due to traditional beliefs and customs [6]. In some regions, over 60% of neonatal deaths are linked to preventable causes such as hypothermia, infection, and birth asphyxia, conditions that could be managed effectively with basic neonatal care [14]. The lack of skilled healthcare providers further exacerbates these challenges, as many births occur without medical assistance [16].
The absence of emergency transport and delays in seeking care mean that even when complications arise, timely medical intervention is rarely available [17]. In areas such as Mugu and Humla, women must walk long distances to reach a hospital, often arriving too late for life-saving interventions [7,15]. Strategies to address these disparities should include increasing the number of trained healthcare workers in rural districts [18], expanding neonatal resuscitation programs such as Helping Babies Breathe (HBB) [19] and developing community-based healthcare initiatives that respect cultural practices while promoting safe birth practices [20]. Without targeted interventions, neonatal mortality rates in Nepal’s remote regions will remain unacceptably high, exacerbating existing health inequities between urban and rural populations.
2. Methods
This review employs a narrative synthesis approach to analyze disparities in neonatal mortality and healthcare access in Nepal’s remote regions. Due to the heterogeneity of study designs, populations, and interventions, a quantitative meta-analysis was not feasible. Instead, Popay et al.’s Narrative Synthesis Framework [21] was utilized, as it provides a structured methodology to integrate findings from diverse studies and systematically identify thematic patterns across different contexts [22].
2.1. Search Strategy and Study Selection
A systematic literature search was conducted using electronic databases (PubMed, CINAHL, Embase, and Scopus) to identify relevant studies published within the last 25 years. Boolean operators (AND/OR) were applied to refine the search strategy, ensuring comprehensive coverage of key topics. The following search terms were used:
- ‘neonatal mortality’ OR ‘infant mortality’
- ‘neonatal resuscitation’ OR ‘Helping Babies Breathe (HBB)’
- ‘newborn care’ OR ‘birth outcomes’
- ‘healthcare disparities’ OR ‘healthcare access’
- ‘skilled birth attendants’ OR ‘healthcare workers’
- ‘remote regions’ OR ‘rural healthcare’ OR ‘resource-limited settings’
- ‘geographical barriers’ OR ‘terrain’ OR ‘infrastructure challenges’
- ‘Nepal’ AND ‘hilly regions’ OR ‘mountainous regions’
- ‘antenatal care’ OR ‘delivery practices’
- ‘cultural barriers’ OR ‘socio-cultural factors’ OR ‘ethnic groups’
- ‘healthcare interventions’ OR ‘healthcare programs’
The search strategy was adapted to match each database’s syntax. No language restrictions were applied, although non-English studies were included only if English translations were available.
2.1.1. Inclusion and Exclusion Criteria
Studies eligible for this review focused on neonatal health in Nepal’s rural and remote regions, particularly in hilly and mountainous districts. Research on interventions such as HHB, antenatal care, birth practices, and SBAs was included if it explicitly reported neonatal mortality, birth outcomes, or healthcare disparities in these regions.
Various study designs were considered, including:
- Quantitative and qualitative studies
- Randomized controlled trials
- Observational studies
Studies were excluded if they did not focus specifically on neonatal health in Nepal. However, research addressing maternal health was included if neonatal and maternal findings were reported separately. Studies that did not differentiate between hilly and mountainous areas were still considered if they focused on rural and remote healthcare challenges in Nepal.
2.2. Data Extraction and Analysis
Data from the selected studies were extracted using a standardized data extraction form, capturing information such as:
- Study design and population
- Neonatal mortality rates and birth outcomes
- Healthcare access and service availability
- Effectiveness of interventions
- Geographical and cultural factors influencing neonatal healthcare
A narrative thematic analysis was conducted to identify commonalities and variations in neonatal mortality trends, intervention effectiveness, and policy gaps contributing to persistent disparities. The PRISMA flowchart was used to guide the study selection process, ensuring transparency and methodological rigor (see Figure 1).
Findings were synthesized across both qualitative and quantitative studies, combining statistical trends with contextual healthcare challenges to provide a holistic understanding of neonatal healthcare disparities in Nepal’s remote settings.
2.3. Narative Synthesis
Narrative synthesis is particularly relevant in healthcare and policy research, where interventions and contextual factors vary widely [23]. This approach facilitates an in-depth interpretation of complex health disparities and policy gaps by identifying relationships and trends in neonatal healthcare provision within Nepal’s rural and mountainous regions.
2.3.1. The Four-Stage Narrative Synthesis Framework
Following Popay et al.’s framework [21], the synthesis was conducted in four distinct stages:
2.3.2. Preliminary Synthesis
A comprehensive literature search was conducted using PubMed, CINAHL, Embase, and Scopus to identify studies focusing on neonatal mortality and healthcare disparities in remote regions of Nepal. Articles were screened according to predefined eligibility criteria (detailed in Section 2.1.1), and key themes were identified using an inductive coding approach. A narrative summary of findings was compiled to highlight emerging patterns related to healthcare accessibility, effectiveness of interventions, and regional disparities in neonatal care.
2.3.3. Exploring Relationships Within and Between Studies
To further analyze cross-study relationships, findings were categorized and stratified based on:
- Study type (qualitative vs. quantitative)
- Geographical region (hilly vs. mountainous)
- Type of intervention (e.g., HBB, SBA programs)
This thematic classification allowed for the examination of how geographical, infrastructural, and cultural disparities impact neonatal mortality. Differences in neonatal outcomes between rural and urban settings were also evaluated, considering healthcare infrastructure, socio-cultural influences, and study heterogeneity.
2.3.4. Critical Appraisal of Studies
To ensure the credibility and reliability of the synthesis, all included studies underwent critical appraisal using a modified Critical Appraisal Skills Programme (CASP) checklist for qualitative and observational research [24]. Key areas assessed included:
- Study design and methodology
- Sample size and representativeness
- Intervention effectiveness and bias evaluation
Particular attention was given to the risk of bias, including small sample sizes, self-reported data limitations, and potential publication bias favouring urban-based healthcare interventions.
2.4. Synthesis and Presentation of Findings
The final synthesis integrated key insights into four overarching themes:
- Regional disparities in neonatal mortality and birth outcomes
- Impact of neonatal resuscitation programs such as HBB
- Infrastructure and resource gaps in neonatal healthcare
- Geographical barriers to healthcare access
To enhance clarity, data were systematically tabulated, highlighting key differences in neonatal outcomes across Nepal’s rural districts. A conceptual model was also developed to illustrate the interconnections between these themes, offering a comprehensive synthesis of neonatal healthcare disparities and intervention effectiveness.
3. Results
A total of 334 papers were retrieved across four major databases, with 62 from Scopus, 84 from Embase, 96 from PubMed, and 92 from CINAHL. After removing 248 duplicates, 86 unique studies remained for evaluation. The initial title and abstract screening led to the exclusion of 54 papers, leaving 32 studies for full-text review. Following a detailed assessment, 11 additional studies were excluded, resulting in a final sample of 21 relevant studies that met the inclusion criteria.
The included studies represent a range of methodological approaches, including cross-sectional analyses, qualitative interviews, mixed-methods research, spatial assessments of healthcare accessibility, and community-based prospective cohort studies. These studies provide comprehensive insights into neonatal mortality rates, birth outcomes, healthcare disparities, and the effectiveness of interventions across different regions of Nepal. Key themes emerging from the synthesis include regional disparities in neonatal mortality and birth outcomes, the impact of neonatal resuscitation programs such as HBB, infrastructure and equipment gaps in neonatal healthcare, and geographic barriers to healthcare access (see Table 1).
4. Discussion
This review synthesizes findings from the included studies examining neonatal mortality and healthcare disparities in remote regions of Nepal. The analysis highlights four key themes influencing neonatal health outcomes: regional disparities in neonatal mortality and birth outcomes, the impact of neonatal resuscitation programs such as HBB, infrastructure and resource gaps in neonatal healthcare, and geographical barriers to healthcare access. Together, these themes illustrate the structural and systemic barriers that contribute to high neonatal mortality rates in remote areas.
4.1. Regional Disparities in Neonatal Mortality and Birth Outcomes
Significant regional disparities in neonatal mortality and birth outcomes persist across Nepal, particularly between remote mountainous areas and more accessible rural or urban regions. Bhattarai et al. [25] found that low birth weight prevalence was notably higher in hilly and mountain regions, with disparities influenced by maternal age, caste, and antenatal care access. Similarly, Karki and Kittel [8] reported persistently high neonatal mortality rates in Dolpa, where cultural resistance to institutional births and a reliance on untrained birth attendants continue to hinder neonatal survival.
The risks associated with traditional birthing practices remain significant. In 2000, Thapa et al. [6] documented that neonatal mortality was nearly three times higher in births occurring in animal sheds compared to home deliveries, primarily due to unsanitary conditions, lack of skilled attendance, and increased risks of infections and hypothermia. More recent studies suggest that some women in remote areas of Nepal still give birth in animal sheds, despite efforts to discourage the practice. A study by Sharma et al. in 2016 [34] documented that some rural communities in Nepal continue to practice childbirth in animal sheds, influenced by cultural traditions and beliefs about impurity during childbirth. The study emphasized that giving birth in unsanitary conditions increases the risk of neonatal infections and sepsis, reinforcing findings from Thapa et al. [6].
Another report by Devkota and Bhatta in 2011 [35] found that in certain districts, women still deliver in animal sheds, particularly in areas with limited access to maternal health services. The study highlighted that these births often go unattended, increasing the likelihood of perinatal complications and neonatal mortality. Additionally, in 2022 Joshi [36] explored the Chhaupadi practice, where women are relegated to sheds during menstruation and childbirth. While government efforts have sought to eliminate this custom, some communities persist in following these traditional restrictions, leading to continued unsafe birth practices.
These studies confirm that despite being widely discouraged, animal-shed births remain a reality in some remote Nepalese communities, reinforcing the need for community-based maternal health interventions and improved access to skilled birth attendants. Kaphle et al. [20] further emphasized that cultural norms in Mugu often conflicted with medical recommendations, preventing women from seeking timely maternal care.
The availability of SBAs varies significantly by region, impacting neonatal outcomes. Choulagai [26] found that only 48% of births in mid- and far-western Nepal were attended by SBAs, with distance from healthcare facilities and lack of transport cited as the main barriers. In Solukhumbu, Thomas et al. [32] reported that 35.7% of births occurred in health facilities, but many women still opted for home births due to limited transportation and facility shortages. Schoenhals et al. [29] similarly found that 70% of births in Solukhumbu were home deliveries, with many lacking skilled medical assistance.
Regional disparities extend to healthcare accessibility and neonatal survival rates. Kc et al. [27] found that neonatal mortality declined overall between 2001 and 2016, yet wealth-based disparities widened, with poorer families projected to meet neonatal survival targets much later than wealthier groups. Without equitable access to quality neonatal care, neonatal mortality in Nepal’s most remote districts is likely to remain high.
4.2. Impact of Neonatal Resuscitation Programs Such as HBB
The HBB program has shown measurable success in reducing neonatal deaths due to birth asphyxia, yet implementation challenges persist. Naresh et al. [19] reported that HBB training reduced neonatal mortality by 60% when properly implemented. However, the effectiveness of HBB is compromised by healthcare worker turnover and lack of refresher training, particularly in rural health posts [31].
Despite high resuscitation equipment availability, many healthcare workers struggle to use it effectively. Pandey et al. [17] found that 91.6% of health facilities stocked neonatal resuscitation bags, yet skill retention among healthcare workers was poor, limiting the program’s overall effectiveness. Singh and Shankar [30] further highlighted gaps in CPR knowledge among healthcare providers, finding that only 12.8% of Nepalese health assistants had received CPR training and none had practical experience in performing resuscitation.
In facilities where HBB is implemented, gaps in follow-up care and neonatal referrals reduce its long-term impact. Ghimire et al. [7] reported that although neonatal asphyxia cases declined in HBB-trained centers, limited access to emergency referrals meant that many neonates still faced postnatal complications. Expanding in-situ mentorship programs, as suggested by Maru et al. [28], could enhance HBB effectiveness by reinforcing hands-on training in neonatal resuscitation.
Addressing these HBB-related challenges requires sustained refresher training, incentives for rural postings, and improved referral networks for high-risk neonates. Without these systemic improvements, the impact of HBB will remain limited in the most vulnerable communities.
4.3. Infrastructure and Resource Gaps in Neonatal Healthcare
Severe infrastructure and resource shortages continue to undermine neonatal survival in Nepal’s remote regions. Bhattarai et al. [25] found that many health facilities lacked essential neonatal care infrastructure, including electricity, incubators, and sterile equipment. Similarly, Tuladhar [33] reported that by 2021, only 2.2% of health facilities stocked all essential neonatal medicines, demonstrating a major gap in facility readiness for neonatal emergencies.
Facilities in high-mortality districts, such as Dolpa and Jumla, are particularly ill-equipped for neonatal care. Karki and Kittel [8] noted frequent medicine shortages, while Tamang et al. [31] found that most facilities lacked functional incubators and transport services. Thomas et al. [32] further highlighted staff shortages, with no trained obstetric and neonatal emergency personnel available at many rural health posts.
Inconsistent Comprehensive Emergency Obstetric and Neonatal Care (CEmONC) services exacerbate neonatal mortality risks. Acharya et al. [18] found that only 16.1% of Nepalese health facilities were equipped to manage assisted vaginal deliveries, highlighting critical gaps in facility readiness. The expansion of CEmONC services, as recommended by Maru et al. [28], has been shown to increase institutional births and reduce neonatal deaths in under-resourced districts.
To strengthen neonatal care, investments must focus on improving health facility readiness, expanding CEmONC services, and ensuring a consistent supply of essential medicines and neonatal equipment..
4.4. Geographical Barriers to Healthcare Access
Geographic isolation remains one of the most significant barriers to neonatal healthcare in Nepal. Paudel et al. [16] found that in remote villages of Jumla, women frequently travel 7-8 hours on foot to reach the nearest health facility, delaying critical care for high-risk births. Similar challenges were observed in Dolpa, where poor road infrastructure and harsh terrain prevent timely maternal care access [8].
The absence of emergency transport significantly affects neonatal survival. Tamang et al. [31] found that 20 out of 31 health facilities in Jumla lacked ambulances, severely limiting referral services. Cao et al. [2] further demonstrated that motorized transport access significantly reduced neonatal mortality, yet mountainous districts still lacked basic transport infrastructure.
Expanding community-based birthing centers in remote areas could reduce reliance on long-distance travel for safe deliveries. Additionally, investing in rural ambulance networks and mobile health outreach programs, as recommended by Shrestha and Jung [13], could help bridge accessibility gaps and provide essential neonatal follow-up care.
5. Recommendations
Future research should prioritize the development of sustainable neonatal resuscitation training models tailored to the challenges faced by healthcare workers in remote Nepal. While programs such as HBB have demonstrated success, studies indicate that skill retention declines over time without reinforcement, especially in settings where access to refresher training is limited [19,30]. Future research should explore innovative, low-resource approaches to continuous neonatal resuscitation training, assessing their effectiveness in improving skill retention and reducing neonatal mortality over the long term.
The impact of digital and remote learning tools in neonatal resuscitation training requires further investigation, particularly in regions with limited internet connectivity and inconsistent electricity access. Research should evaluate the effectiveness of offline-accessible training solutions, determining their feasibility for healthcare workers in geographically isolated areas. Additionally, studies examining healthcare worker engagement, usability, and knowledge retention in relation to digital learning models would provide valuable insights into scaling training programs efficiently in low-resource settings.
Future studies should explore the role of telemedicine and mobile health initiatives in bridging gaps in neonatal emergency care. Given the widespread geographic barriers to healthcare access in Nepal [2,17,27], research should examine how real-time clinical support and remote neonatal case discussions influence healthcare worker decision-making and neonatal outcomes. Evaluating community-based interventions that integrate telehealth support for birth attendants and midwives could provide actionable strategies to reduce neonatal deaths in the most underserved regions.
There is a pressing need to investigate how healthcare infrastructure and supply chain inefficiencies impact neonatal care in Nepal’s high-mortality districts. While previous studies have documented severe shortages of essential medicines, neonatal equipment, and trained personnel [25,33], research should move beyond identifying gaps and focus on evaluating intervention models that strengthen supply chains, improve healthcare facility readiness, and optimize resource allocation. Understanding the cost-effectiveness and scalability of such interventions is crucial for their successful implementation in low-resource settings.
Future research should assess the effectiveness of alternative models for emergency transport and referral systems in reducing neonatal mortality. Geographic isolation remains a critical barrier to healthcare access in Nepal’s rural districts, yet studies examining rural ambulance networks, air transport feasibility, and mobile maternal health units remain limited [16,31]. Investigating how community-driven transport interventions influence neonatal survival rates would provide key evidence for addressing emergency referral challenges in remote settings.
Long-term studies are needed to evaluate the broader policy and governance structures affecting neonatal health in Nepal, particularly in relation to health system accountability, funding mechanisms, and rural healthcare workforce retention [13]. Research should explore how provincial and national health policies influence neonatal outcomes, with an emphasis on identifying effective policy reforms that strengthen maternal and newborn healthcare delivery in Nepal’s most at-risk regions.
6. Conclusions
The findings from this review highlight four major barriers to neonatal healthcare in Nepal’s remote regions. Stark regional disparities persist in neonatal survival rates, exacerbated by socioeconomic inequities and cultural birth practices. While neonatal resuscitation programs such as HBB have demonstrated effectiveness, training gaps and healthcare worker turnover reduce their long-term impact. Infrastructure and resource limitations severely restrict neonatal care capacity, while geographic barriers continue to prevent timely healthcare access.
Addressing these systemic challenges requires comprehensive, multi-level interventions, including expanded SBA training, enhanced emergency transport systems, and investments in healthcare infrastructure. While existing programs such as HBB and CEmONC have shown promise, their success depends on addressing underlying systemic inequities in Nepal’s most underserved regions.
Author Contributions
Conceptualization, VK; methodology, VK; formal analysis, VK; writing—original draft preparation, VK.; writing—review and editing, RG & AG. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bhattarai, K. and D. Conway, Contemporary environmental problems in Nepal: Geographic perspectives. 2021, Springer Cham: Switzerland.
- Cao, W.R., et al., Equity of geographical access to public health facilities in Nepal. BMJ Glob Health, 2021. 6(10). [CrossRef]
- Hodge, A., et al., Utilisation of health services and geography: deconstructing regional differences in barriers to facility-based delivery in Nepal. Matern Child Health J, 2015. 19(3): p. 566-77. [CrossRef]
- Wasti, S.P., et al., Overcoming the challenges facing Nepal's health system during federalisation: An analysis of health system building blocks. Health Res Policy Syst, 2023. 21(1): p. 117. [CrossRef]
- Rublee, C., et al., Three Climate and Health Lessons from Nepal Ahead of COP28. NAM Perspect, 2023. 2023. [CrossRef]
- Thapa, N., et al., Infant death rates and animal-shed delivery in remote rural areas of Nepal. Social Science & Medicine, 2000. 51(10): p. 1447-1456. [CrossRef]
- Ghimire, P.R., et al., Factors Associated With Perinatal Mortality in Nepal: Evidence From Nepal Demographic and Health Survey 2001–2016. BMC Pregnancy and Childbirth, 2019. 19(1). [CrossRef]
- Karki, B.K. and G. Kittel, Neonatal mortality and child health in a remote rural area in Nepal: a mixed methods study. BMJ Paediatr Open, 2019. 3(1): p. e000519. [CrossRef]
- Kalter, H.D., et al., Modified Pathway to Survival highlights importance of rapid access to quality institutional delivery care to decrease neonatal mortality in Serang and Jember districts, Java, Indonesia. J Glob Health, 2023. 13: p. 04020. [CrossRef]
- Kuikel, B.S., et al., A critical analysis of health system in Nepal: Perspective's based on COVID-19 response. Dialogues Health, 2023. 3: p. 100142. [CrossRef]
- Parajuli, R., et al., Challenges and opportunities for implementing digital health interventions in Nepal: A rapid review. Front Digit Health, 2022. 4: p. 861019. [CrossRef]
- Khadka, K.B., et al., Newborn morbidities and care procedures at the special newborn care units of Gandaki Province, Nepal: A retrospective study. BMC Pregnancy and Childbirth, 2024. 24(1): p. 883. [CrossRef]
- Shrestha, G., et al., Free Newborn Care Services: A New Initiative in Nepal. Journal of Nepal Health Research Council, 2018. 16(3): p. 340-344.
- Khatri, R.B., et al., Newborn Health Interventions and Challenges for Implementation in Nepal. Frontiers in Public Health, 2016. 4. [CrossRef]
- Khanal, V., S. Bista, and S.R. Mishra, Prevalence of and factors associated with home births in western Nepal: Findings from the baseline of a community-based prospective cohort study. Clinical Epidemiology and Global Health, 2024. 27: p. 101594. [CrossRef]
- Paudel, M., et al., Health system barriers influencing perinatal survival in mountain villages of Nepal: Implications for future policies and practices. Journal of Health, Population and Nutrition, 2018. 37(1): p. 16. [CrossRef]
- Pandey, A.R., et al., Service availability and readiness for basic emergency obstetric and newborn care: Analysis from Nepal Health Facility Survey 2021. PLOS ONE, 2023. 18(8): p. e0282410. [CrossRef]
- Acharya, K., et al., Basic emergency obstetric and newborn care service availability and readiness in Nepal: Analysis of the 2015 Nepal Health Facility Survey. PloS one, 2021. 16(7): p. e0254561. [CrossRef]
- Naresh, P., et al., Newborn Resuscitation Scale Up and Retention Program Associated with Improved Neonatal Outcomes in Western Nepal. Int J Pediatr Res, 2022. 8: p. 087.
- Kaphle, S., H. Hancock, and L.A. Newman, Childbirth traditions and cultural perceptions of safety in Nepal: Critical spaces to ensure the survival of mothers and newborns in remote mountain villages. Midwifery, 2013. 29(10): p. 1173-1181. [CrossRef]
- Popay, J., et al., Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme Version, 2006. 1(1): p. b92.
- Snilstveit, B., S. Oliver, and M. Vojtkova, Narrative approaches to systematic review and synthesis of evidence for international development policy and practice. Journal of Development Effectiveness, 2012. 4(3): p. 409-429. [CrossRef]
- Rodgers, M., et al., Testing methodological guidance on the conduct of narrative synthesis in systematic reviews: Effectiveness of interventions to promote smoke alarm ownership and function. Evaluation, 2009. 15(1): p. 49-73.
- CASP, Critical Appraisal Skills Programme (CASP) Qualitative Checklist. Available at: https://casp-uk.net, 2020.
- Bhattarai, B., et al., Association of geographic distribution and birth weight with sociodemographic factors of the maternal and newborn child of hilly and mountain regions of eastern Nepal: a cross-sectional study. BMJ Paediatr Open, 2022. 6(1). [CrossRef]
- Choulagai, B., Barriers to using skilled birth attendants' services in mid- and far-western Nepal: A cross-sectional study. BMC International Health and Human Rights, 2013. 13(1). [CrossRef]
- Kc, A., et al., Scaling up quality improvement intervention for perinatal care in Nepal (NePeriQIP): Study protocol of a cluster randomised trial. BMJ global health, 2017. 2(3): p. e000497-e000497. [CrossRef]
- Maru, S., et al., Impact of the roll out of comprehensive emergency obstetric care on institutional birth rate in rural Nepal. BMC Pregnancy and Childbirth, 2017. 17(1). [CrossRef]
- Schoenhals, S., et al., Critical Assessment of Maternal-Newborn Care Delivery in Solukhumbu, Nepal. Annals of Global Health, 2017. 83(1): p. 202-202. [CrossRef]
- Singh, B. and P.R. Shankar, Knowledge regarding cardiopulmonary resuscitation among health assistants in Nepal: A cross-sectional study. PLOS ONE, 2023. 18(11): p. e0293323. [CrossRef]
- Tamang, P., et al., Health facility preparedness of maternal and neonatal health services: A survey in Jumla, Nepal. BMC Health Services Research, 2021. 21(1): p. 1023. [CrossRef]
- Thomas, J.W., et al., Analysis of the Perinatal Care System in a Remote and Mountainous District of Nepal. Matern Child Health J, 2022. 26(10): p. 1976-1982. [CrossRef]
- Tuladhar, S., Changes in health facility readiness for obstetric and neonatal care services in Nepal: An analysis of cross-sectional health facility survey data in 2015 and 2021. BMC Pregnancy and Childbirth, 2024. 24(1). [CrossRef]
- Sharma, S., et al., Dirty and 40 days in the wilderness: Eliciting childbirth and postnatal cultural practices and beliefs in Nepal. BMC Pregnancy and Childbirth, 2016. 16(1): p. 147. [CrossRef]
- Devkota, M. and M. Bhatta, Newborn Care Practices of Mothers in a Rural Community in Baitadi, Nepal. Health Prospect, 2018. 10: p. 5–9. [CrossRef]
- Joshi, S., Chhaupadi practice in Nepal: A literature review. World Medical & Health Policy, 2022. 14(1): p. 121-137. [CrossRef]
Figure 1.
PRISMA Flowchart for study selection.
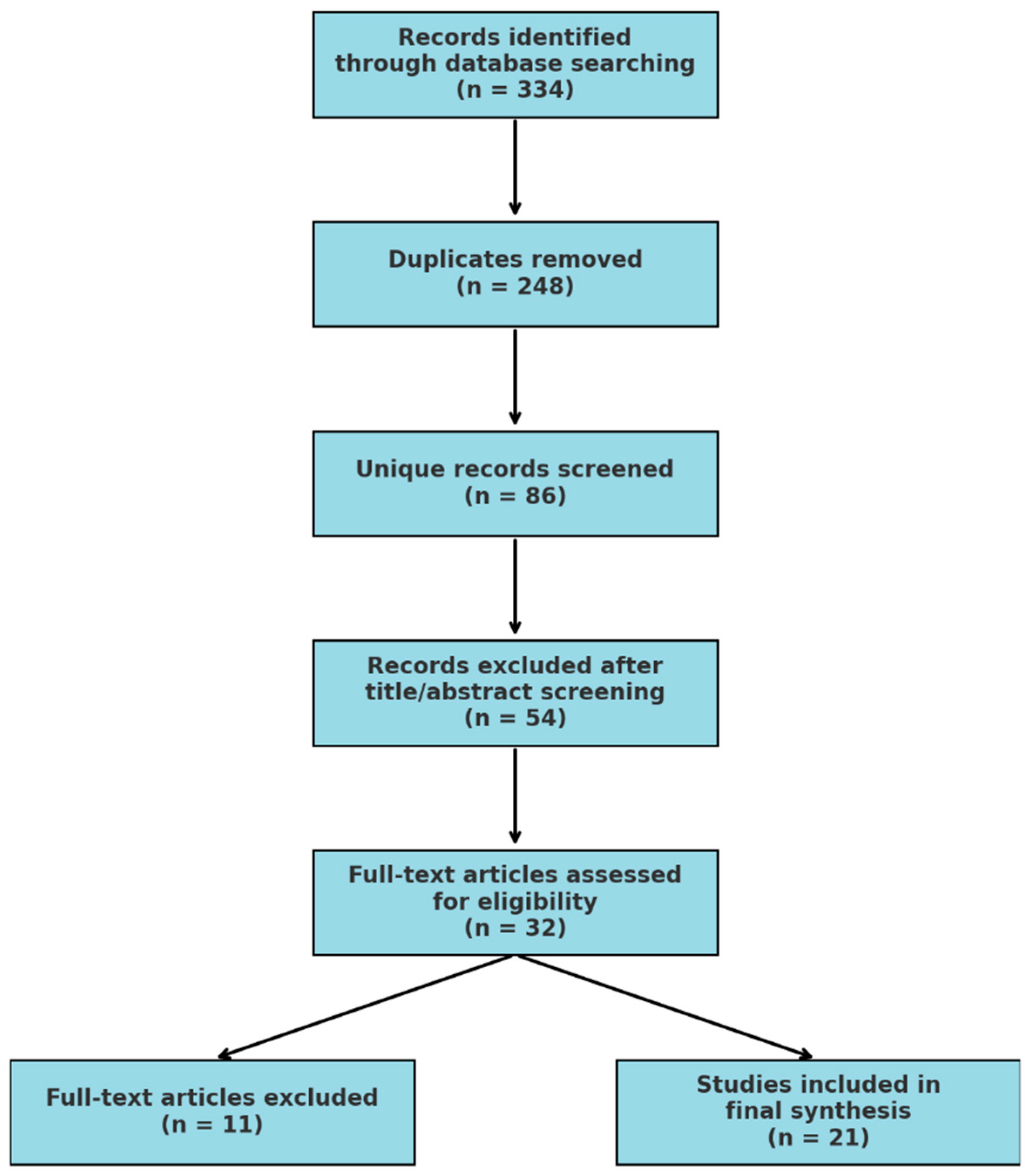

Table 1.
Summary of included papers.
| Author Year | Study Design | Study Population | Key Themes | Findings | Study Quality and Bias |
| Acharya, et al. (2021)[18] |
Cross-sectional | 457 health facilities across Nepal | Healthcare infrastructure, facility readiness, emergency obstetric care | Hospitals had higher neonatal care readiness. Only 16.1% offered assisted vaginal birth, 10% provided anticonvulsants. Readiness linked to staffing levels, 24-hour service, and newborn death review. | Moderate risk of bias due to self-reported facility readiness assessments |
| Bhattarai, et al. (2022)[25] |
Cross-sectional. | 1,386 term singleton births from 4 hospitals in eastern Nepal | Geographic disparities, birth weight, maternal factors | Low birth weight was higher in hilly regions (6.6%). Dalit ethnicity, low maternal age, and higher antenatal visits associated with hilly region births. | Low risk; large dataset but limited causal inferences |
| Cao, et al. (2021)[2] |
Spatial analysis | 5,553 public health facilities, 2020 population data | Healthcare access, geographic barriers | 92.54% of population accessed facilities within 15 min via motorized transport. Accessibility declined for higher-level facilities. Recommended new health centers in underserved areas. | Moderate risk due to reliance on modeled transport data |
| Choulagai(2013)[26] | Cross-sectional | 2,481 women who gave birth in last 12 months in three districts | Skilled birth attendants, barriers to healthcare access | 48% used SBAs. Barriers included distance (45%) and transport issues (21%). Antenatal care improved SBA utilization. | Low risk; strong sample representation but lacks qualitative depth |
| Ghimire (2019)[7] |
Demographic health survey analysis | 23,335 pregnancies from Nepal Demographic Health Survey | Neonatal mortality trends, regional disparities | Perinatal mortality rate was 42 per 1,000 births. Higher mortality in mountainous regions, younger mothers, poor sanitation. | Low risk; robust dataset but lacks intervention-specific data |
| Kaphle, et al. (2013)[20] |
Qualitative | 25 pregnant/postnatal women, 16 healthcare/community stakeholders in Mugu | Cultural barriers, birth practices | Animal-shed births preferred due to spiritual beliefs, leading to neonatal risks. Cultural beliefs conflicted with medical advice. | Moderate risk due to small sample size and subjective reporting |
| Karki & Kittel (2019)[8] |
Mixed-methods | 12,287 people from Dolpa district | Neonatal mortality, cultural influences, healthcare access | Neonatal mortality rate was 67 per 1,000. Cultural mistrust of modern medicine and poor health infrastructure led to increased deaths. | Moderate risk; strong sample but relies on retrospective data |
| Kc, et al. (2017)[27] |
Secondary analysis | Women aged 15-49 from Nepal Demographic and Health Surveys (2001, 2006, 2011, 2016) | Neonatal mortality trends, socioeconomic disparities | Neonatal mortality decreased between 2001 and 2016, but disparities widened between wealth quintiles. Tetanus vaccination, maternal education, and household conditions were key predictors of neonatal mortality. | Low risk; robust dataset but limited ability to analyze causal relationships |
| Khanal, et al. (2024)[15] |
Prospective cohort | 735 mother-infant pairs in western Nepal | Home births, healthcare utilization | 11.8% had home births. Low antenatal care increased likelihood of home birth. Higher wealth correlated with hospital births. | Low risk; strong methodology but lacks long-term neonatal tracking |
| Khatri, et al. (2022)[14] |
Cross-sectional | 901 antenatal care facilities and 454 perinatal service providers | Healthcare infrastructure, service quality | Structural quality scores were higher for private facilities; government-run facilities in rural areas showed poor readiness for maternal and newborn care. | Moderate risk; self-reported facility assessments limit objectivity |
| Maru, et al. (2017)[28] |
Pre-post intervention | 210 postpartum women in rural Nepal | Emergency obstetric care, birth facility utilization | Institutional birth rates rose from 30% to 77% after CEmOC introduction. Availability improved birth planning and safety perceptions. | Low risk; rigorous comparison but limited to one hospital area |
| Naresh, et al. (2022)[19] |
Prospective observational | 18 health facilities assessing 49,809 births | Newborn resuscitation, HBB | HBB training reduced neonatal deaths and birth asphyxia. Skill retention remained high over 24 months. | Low risk; large dataset, but results may not generalize to non-participating regions |
| Pandey, et al. (2023)[17] |
Cross-sectional | 804 health facilities in Nepal. | Emergency obstetric care, facility readiness | Service availability for neonatal care remains inadequate. Only 43.7% of facilities met Comprehensive Emergency Obstetric and Neonatal Care (CEmONC) standards. | Moderate risk due to facility-reported data |
| Paudel, et al. (2018)[16] |
Qualitative | 42 interviews with women who experienced perinatal deaths and 20 interviews with healthcare workers | Healthcare system barriers, perinatal mortality | Poor governance, lack of community engagement, and weak health system accountability contributed to high perinatal mortality in remote villages. | Moderate risk; small sample limits generalizability |
| Schoenhals, et al. (2017)[29] |
Cross-sectional | 122 women who gave birth in the past 24 months in Solukhumbu District | Maternal-newborn health practices | Only 26% of births occurred in health facilities, with 70% at home. Limited access to skilled birth attendants contributed to neonatal complications. | Moderate risk; small sample size but relevant to high-altitude populations |
| Shrestha & Jung (2023)[13] |
Quasi-experimental | Rural Nepalese children from Nepal Living Standards Survey data | Healthcare reform, gender-based disparities | Healthcare reform reduced infant mortality for boys but had no significant effect on girls, suggesting persistent societal gender biases in healthcare access. | Moderate risk; reliance on secondary data may not capture all confounders |
| Singh & Shankar (2023)[30] |
Cross-sectional | 500 health assistants registered with Nepal Health Professional Council | CPR knowledge among healthcare workers | Only 12.8% had CPR training; none had performed CPR. Training gaps highlight urgent need for competency development. | Low risk; strong methodology but limited to one profession |
| Tamang, et al. (2021)[31] |
Descriptive cross-sectional | 31 state-run health facilities in Jumla District | Facility preparedness, medicine availability | Many facilities lacked essential neonatal medicines and transport services. Emergency preparedness was inadequate in most centers. | Moderate risk; self-reported data may limit reliability |
| Thapa, et al. (2000)[6] |
Community-based retrospective | 3,007 live-born children from 772 mothers in Jumla, Nepal | Animal-shed births, neonatal mortality | Neonatal mortality was significantly higher for births occurring in animal sheds compared to homes. Lack of hygiene and medical care contributed to higher risk. | Moderate risk; older dataset but relevant to cultural birth practices |
| Thomas, et al. (2022)[32] |
Cross-sectional | 487 households and 19 health facilities in Solukhumbu District | Facility readiness, SBA availability | Only 35.7% of births occurred in health facilities. Lack of trained obstetric and neonatal staff hindered service readiness. | Low risk; large sample, but self-reported barriers may introduce bias |
| Tuladhar (2024)[33] |
Cross-sectional | Survey data from 2015 and 2021 assessing facility readiness | Neonatal service provision, healthcare trends | By 2021, only 2.2% of facilities stocked all essential neonatal medicines. Readiness for neonatal care remained critically low, particularly in rural areas. | Moderate risk; government survey data may not reflect all local disparities |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



