Submitted:
04 March 2025
Posted:
05 March 2025
You are already at the latest version
Abstract
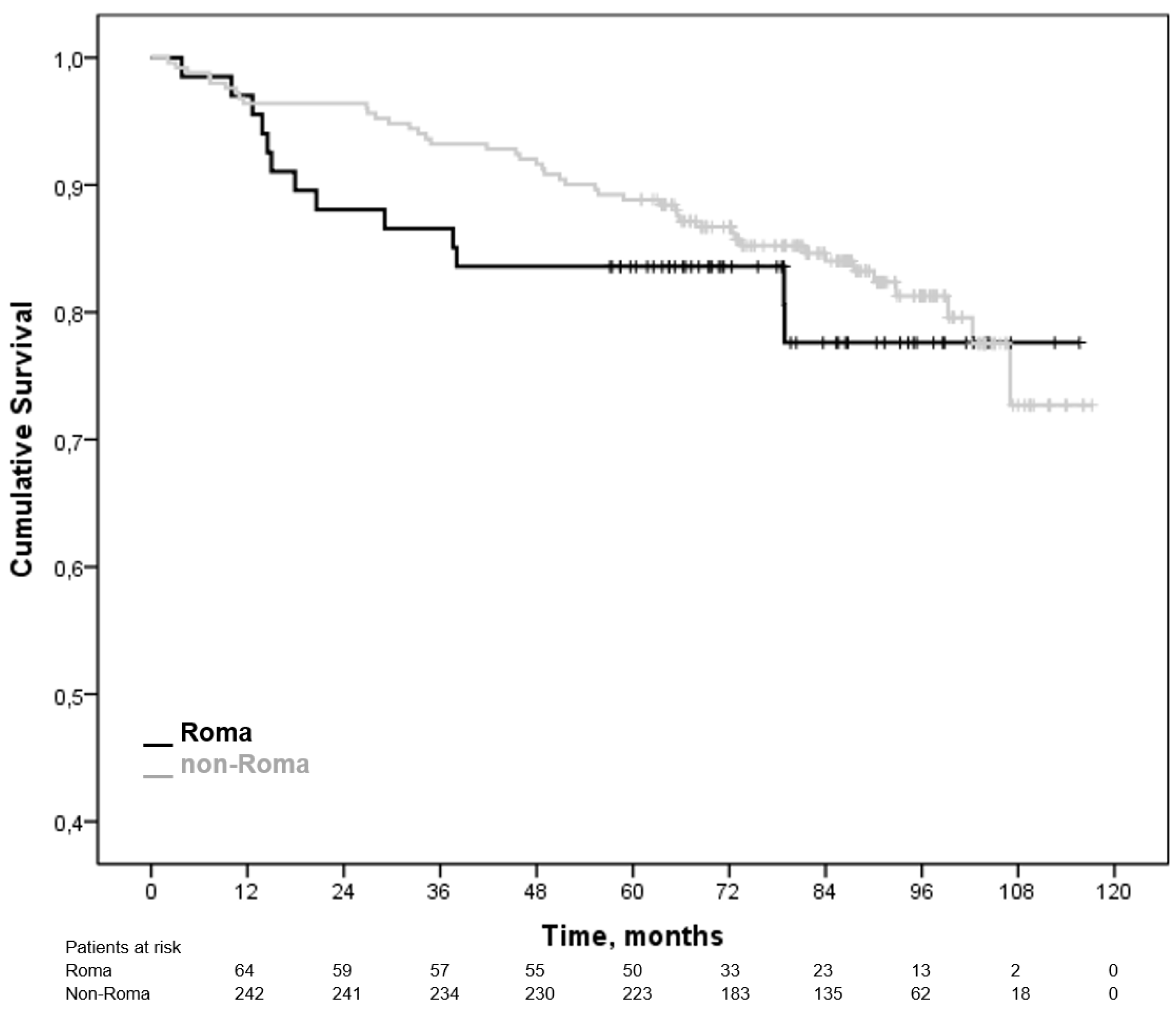
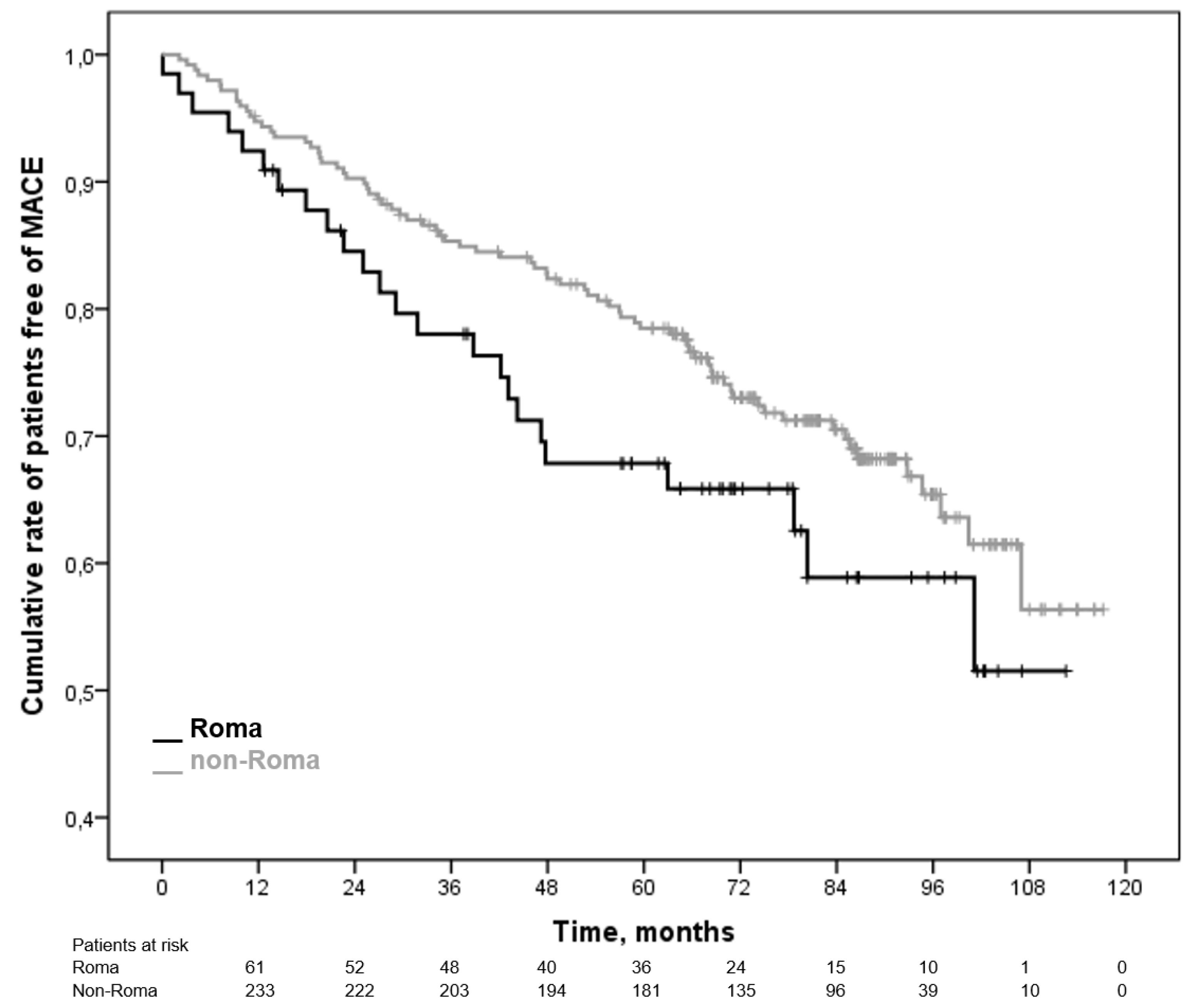
Background: Clinical and treatment characteristics, and outcomes of Roma patients with acute myocardial infarction (AMI) have not been appropriately investigated. Methods: We retrospectively analyzed 67 Roma patients and 251 non-Roma patients with AMI in one hospital center in Croatia in a period from 2011 to 2015, and followed-up for a median of 84 months. Results: Roma patients had significantly more unfavorable risk factors at admission, more complex coronary artery disease measured by Syntax score, and lower left ventricular ejection fraction at discharge. There were no differences in rates of revascularization after index coronary angiography. Roma patients had significantly worse therapy adherence at last follow-up. Death and composite major adverse cardiac event (MACE) were not significantly more frequent in Roma patients compared to non-Roma (HR 1.11, 95% CI 0.63-1.93 for death, and HR 1.19, 95% CI 0.83-1.70 for MACE). More Roma patients experienced stroke and repeated myocardial infarction during follow-up (10% vs 4.5%, and 15% vs 10%, respectively) but that difference was not significant. Lower left ventricular ejection fraction was independently associated with mortality and MACE within whole cohort. Multivariate regression model for MACE among patients that had reliable data on therapy adherence showed significant independent impact of low therapy adherence. Conclusion: Roma patients with AMI in Croatia have significantly more unfavorable risk profile at admission and worse medical therapy adherence after discharge, but receive appropriate revascularization and experience no excess mortality during long-term follow-up. Their MACE rates could be improved with better patient education and stronger therapy adherence monitoring.
Keywords:
1. Introduction
2. Materials and Methods
Study Population
Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of interest
References
- Khan MA, Hashim MJ, Mustafa H, Baniyas MY, Al Suwaidi SKBM, AlKatheeri R, Alblooshi FMK, Almatrooshi MEAH, Alzaabi MEH, Al Darmaki RS, Lootah SNAH. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus. 2020;12:e9349. [CrossRef]
- Freund KM, Jacobs AK, Pechacek JA, White HF, Ash AS. Disparities by race, ethnicity, and sex in treating acute coronary syndromes. J Womens Health (Larchmt). 2012;21:126-132. [CrossRef]
- Hall SL, and Lorenc T. Secondary prevention of coronary artery disease. Am Fam Physician. 2010;81:289-296.
- Rasmussen JN, Chong A, Alter DA. Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA. 2007;297:177–186. [CrossRef]
- Borrell LN, and Lancet EA. Race/ethnicity and all-cause mortality in US adults: revisiting the Hispanic paradox. Am J Public Health. 2012;102:836–843. [CrossRef]
- Kohler IV, and Preston SH. Ethnic and religious differentials in Bulgarian mortality, 1993-98. Popul Stud. 2011;65:91–113. [CrossRef]
- Gniwa Omezzine R, Akkara A, Abdelkafi Koubaa A, Belguith Sriha A, Rdissi A, Amamou K. Predictors of Poor Adherence to Hypertension Treatment. Tunis Med. 2019;97:564-571.
- Lauffenburger JC, Robinson JG, Oramasionwu C, Fang G. Racial/Ethnic and gender gaps in the use of and adherence to evidence-based preventive therapies among elderly Medicare Part D beneficiaries after acute myocardial infarction. Circulation. 2014;129:754-63. [CrossRef]
- Ringold D, Orenstein MA, Wilkens E. Roma in an expanding Europe: breaking the poverty cycle. Washington: The World Bank; 2005.
- Fundación Secretariado Gitano. Health and the Roma community, analysis of the situation in Europe: Bulgaria, Czech Republic, Greece, Portugal, Romania, Slovakia, Spain. Madrid: Fundacion Secretariado Gitano; 2009.
- Vozarova de Courten B, de Courten M, Hanson RL, Zahorakova A, Egyenes HP, Tataranni PA, et al. Higher prevalence of type 2 diabetes, metabolic syndrome and cardiovascular diseases in gypsies than in nongypsies in Slovakia. Diabetes Res Clin Pract. 2003;62:95-103. [CrossRef]
- Sudzinova A, Nagyova I, Rosenberger J, Studencan M, Vargova H, Middel B, van Dijk JP, Reijneveld SA. Seven years' mortality in Roma and non-Roma patients after coronary angiography. Eur J Public Health. 2015;25:765-769. [CrossRef]
- Thuijs DJFM, Kappetein AP, Serruys PW, Mohr FW, Morice MC, Mack MJ, Holmes DR Jr, Curzen N, Davierwala P, Noack T, et al; SYNTAX Extended Survival Investigators. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet. 2019;394:1325-1334. [CrossRef]
- Morisky DE, and DiMatteo MR. Improving the measurement of self-reported medication nonadherence: final response. J Clin. Epidem 2011;64:255–267. [CrossRef]
- Graham G, Xiao YY, Rappoport D, Siddiqi S. Population-level differences in revascularization treatment and outcomes among various United States subpopulations. World J Cardiol. 2016;8:24-40. [CrossRef]
- Karkabi B, Zafrir B, Jaffe R, Shiran A, Jubran A, Adawi S, Ben-Dov N, Iakobishvili Z, Beigel R, Cohen M, Goldenberg I, Klempfner R, Flugelman MY, Rubinshtein R. Ethnic Differences Among Acute Coronary Syndrome Patients in Israel. Cardiovasc Revasc Med. 2020 Nov;21(11):1431-1435. [CrossRef]
- Wechkunanukul K, Grantham H, Damarell R, Clark RA. The association between ethnicity and delay in seeking medical care for chest pain: a systematic review. JBI Database System Rev Implement Rep. 2016 Jul;14(7):208-35. [CrossRef] [PubMed]
- Anderson L, Thompson DR, Oldridge N, Zwisler AD, Rees K, Martin N, Taylor RS. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2016;CD001800. [CrossRef]
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. [CrossRef]
- Dzayee DAM, Moradi T, Beiki O, Alfredsson L, Ljung R. Recommended drug use after acute myocardial infarction by migration status and education level. Eur J Clin Pharmacol 2015;71:499–505. [CrossRef]
- Ringba¨ck Weitoft G, Ericsson O, Lo¨froth E, Rose´n M. Equal access to treatment? Population-based follow-up of drugs dispensed to patients after acute myocardial infarction in Sweden. Eur J Clin Pharmacol 2008;64:417–424. [CrossRef]
- Frederiksen HW, Zwisler AD, Johnsen SP, Öztürk B, Lindhardt T, Norredam M. Differences in initiation and discontinuation of preventive medications and use of non-pharmacological interventions after acute coronary syndrome among migrants and Danish-born. Eur Heart J. 2018 Jul 1;39(25):2356-2364. [CrossRef] [PubMed]
- Graham G. Racial and Ethnic Differences in acute coronary syndrome and myocardial infarction within the United States: from demographics to outcomes. Clin Cardiol. 2016;39:299-306. [CrossRef]
- Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, et al. ESC Scientific Document Group, 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). European Heart Journal, 2020; ehaa575. [CrossRef]
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. [CrossRef]
- Ibrahimov F, Yilmaz Y, Ismayilov I, Musayev K, Musayev OO, Alasgarli S, Shahbazova S, Isgenderova M, Jahangirov T. Comparing 5-year outcomes of aorta-coronary bypass surgery and percutaneous coronary intervention performed with new-generation drug-eluting stents in non-diabetic patients with multivessel acute coronary syndrome patients and intermediate syntax score. Medeni Med J. 2020;35(2):121-127. [CrossRef]
- Fiatal S, Pikó P, Kósa Z, Sándor J, Ádány R. Genetic profiling revealed an increased risk of venous thrombosis in the Hungarian Roma population. Thromb Res. 2019 Jul;179:37-44. Epub 2019 May 2. [CrossRef] [PubMed]
- Pikó P, Fiatal S, Kósa Z, Sándor J, Ádány R. Genetic factors exist behind the high prevalence of reduced high-density lipoprotein cholesterol levels in the Roma population. Atherosclerosis. 2017 Aug;263:119-126. Epub 2017 May 26. [CrossRef] [PubMed]

|
Patients’ characteristic, N (%) |
Ethnicity | |||
| Roma N=67 |
Non-Roma N=251 |
P value | ||
| Type of ACS | STEMI | 44 (66) | 185 (73) | 0.362 |
| NSTEMI | 23 (34) | 66 (27) | ||
| Index year of treatment | 2011-2013 | 30 (45) | 175 (66) | 0.003 |
| 2014-2015 | 37 (55) | 86 (34) | ||
| ECG localization | Anterior/septal | 20 (30) | 72 (29) | 0.263 |
| Inferior | 29 (43) | 104 (41) | ||
| Posterior/lateral | 7 (10) | 13 (5) | ||
| None (unidentified) | 11 (17) | 62 (25) | ||
| CAD severity | One-vessel | 18 (27) | 141 (56) | <0.001 |
| Two-vessel | 27 (40) | 69 (28) | ||
| Multivessel | 19 (28) | 30 (12) | ||
| No obstructive CAD | 3 (5) | 11 (4) | ||
| Left-main disease | 5 (7) | 10 (4) | 0.326 | |
| Syntax score, median (range) | 18 (0-48) | 11 (0-36) | <0.001 | |
| Treatment | PCI | 52 (78) | 221 (89) | 0.023 |
| CABG | 8 (12) | 8 (3) | ||
| OMT | 7 (10) | 19 (8) | ||
| Age, median (range) | 59 (39-86) | 58 (27-86) | 0.598 | |
| Male gender | 47 (70) | 175 (70) | 1.000 | |
| Family history for CAD/MI | 14 (21) | 81 (32) | 0.074 | |
| Hypertension | 37 (55) | 127 (51) | 0.582 | |
| Diabetes mellitus | Admission | 16 (24) | 46 (18) | 0.213 |
| Last follow-up, N/N’ (%) | 23/53 (43) | 62/210 (30) | 0.070 | |
| Active tobacco use | Admission | 49 (73) | 125 (50) | 0.001 |
| Last follow-up, N/N’ (%) | 28/53 (53) | 54/210 (26) | <0.001 | |
| Dyslipidemia | 14 (21) | 35 (14) | 0.183 | |
| Previous stroke/TIA | 5 (8) | 14 (6) | 0.565 | |
| Peripheral artery dise | 8 (12) | 29 (12) | 1.000 | |
| Body mass index, kg/m2, median (range) | 27.6 (22.5-35.8) | 27 (18.4-41.5) | 0.185 | |
| CrCl at admission, ml/min/1.73m2, median (range) | 79.6 (34.7-100.5) | 87 (24.2-184.5) | 0.800 | |
| HbA1c at admission, %, median (range) | 6.1 (4.9-10.4) | 5.5 (4.5-12.9) | <0.001 | |
| LDL-C at admission, mmol/L, median (range) | 3.8 (1.0-6.6) | 3.7 (0.7-8.9) | 0.789 | |
| Triglycerides at admission, mmol/L, median (range) | 1.8 (0.4-16.1) | 1.5 (0.3-8.9) | 0.017 | |
| CRP at admission, mg/dl, median (range) | 3.5 (0.2-198) | 4.4 (0.5-101) | 0.682 | |
| LVEF at discharge, %, median (range) | 52 (30-75) | 57 (24-78) | 0.015 | |
| Unemployed | 32 (48) | 30 (12) | <0.001 | |
| Income below poverty line | 34 (51) | 30 (12) | <0.001 | |
| Education | None | 15 (22.5) | 1 (0.5) | <0.001 |
| Elementary school | 37 (55) | 56 (22) | ||
| High school | 15 (22.5) | 128 (51) | ||
| University | 0 | 66 (26.5) | ||
| Therapy adherence (MMAS-8) | Low, N/N’ (%) | 29/53 (55) | 60/210 (28) | <0.001 |
| Moderate, N/N’ (%) | 23/53 (43) | 101/210 (48) | ||
| High, N/N’ (%) | 2/53 (2) | 50/210 (24) | ||
| Specific drug adherence at last follow-up | DAPT for 12 months, N/N’ (%) | 36/53 (68) | 180/210 (86) | 0.004 |
| Statin, N/N’ (%) | 32/53 (60) | 169/210 (81) | 0.003 | |
| ACEI/ARB, N/N’ (%) | 41/53 (76) | 161/210 (78) | 0.966 | |
| Beta-blocker, N/N’ (%) | 40/53 (75) | 173/201 (82) | 0.247 | |
| Death during follow-up | 13 (19) | 44 (18) | 0.722 | |
| MACE during follow-up | Composite | 25 (37) | 79 (31) | 0.381 |
| Stroke | 7 (10) | 11 (4.5) | 0.072 | |
| Repeat MI | 10 (15) | 25 (10) | 0.272 | |
| Other | 8 (12) | 43 (17) | 0.089 | |
| Regression model | Multivariate Cox regression, HR (95% CI) | ||
| Death | MACE | ||
| Model A | Roma vs. non-Roma | 1.228 (0.656-2.297) | 1.445 (0.907-2.312) |
| Model B | Roma vs. non-Roma | 1.040 (0.473-2.286) | 1.263 (0.718-2.221) |
| Syntax score | 1.018 (0.986-1.051) | 1.028 (1.005-1.051)* | |
| LVEF | 0.958 (0.919-0.977)* | 0.967 (0.946-0.989)* | |
| Model C | Roma vs. non-Roma | 5.025 (0.756-33.423) | 1.682 (0.805-3.515) |
| Syntax score | 0.969 (0.908-1.035) | 1.022 (0.994-1.051) | |
| LVEF | 0.911 (0.855-0.971)* | 0.970 (0.946-0.995)* | |
| Income below poverty line | 2.835 (0.696-11.549) | 0.868 (0.448-1.682) | |
| Active tobacco use | 0.453 (0.181-2.444) | 0.894 (0.520-1.538) | |
| HbA1c | 1.488 (0.970-2.280) | 0.958 (0.779-1.178) | |
| Triglycerides | 0.263 (0.062-1.123) | 0.935 (0.796-1.137) | |
| Model D | Roma vs. non-Roma | N/A | 1.203 (0.553-2.621) |
| Syntax score | 1.028 (0.998-1.059) | ||
| LVEF | 0.984 (0.958-1.011) | ||
| Income below poverty line | 0.845 (0.413-1.727) | ||
| Active tobacco use | 0.861 (0.486-1.524) | ||
| HbA1c | 0.948 (0.756-1.189) | ||
| Triglyceride level | 0.943 (0.759-1.172) | ||
| Low adherence to medical therapy | 5.810 (1.295-26.061)* | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



