
Submitted:
04 March 2025
Posted:
04 March 2025
You are already at the latest version
Abstract
Background/Objectives: Femoral head avascular necrosis (FAN) is a serious orthopedic disorder that causes the death of bone tissue as an outcome of occlusion or insufficiency of the vessels supplying blood to the femoral head. It is especially common in middle-aged men. Factors such as alcohol consumption, corticosteroid use, trauma, and systemic diseases have influential roles in the development of FAN, and the ensuing vascular disruptions can also negatively affect the patient’s broader systemic vascular health. Erectile dysfunction (ED) is a condition caused by impairment of the penile blood flow, which reduces quality of life in men and has psychosocial effects. This study examined the potential relationship between FAN and ED in consideration of the similar pathophysiological mechanisms of these conditions.
Methods: The research was planned as a retrospective case-control study and conducted between January 2020 and December 2023. FAN was diagnosed based on the Ficat-Arlet classification using plain radiography and magnetic resonance imaging, and staging was performed with expert clinical evaluations. The International Index of Erectile Function (IIEF) scale was administered to evaluate ED. Data from 50 patients with FAN and 50 healthy men were evaluated using appropriate statistical methods including the Student t-test, Shapiro-Wilk test, Kruskal-Wallis test, and Dunn and Spearman correlation analysis.
Results: The analysis revealed that an increase in FAN stage was associated with a significant increase in ED severity. The prevalence of ED among FAN patients was significantly higher compared to the control group with the Spearman correlation coefficient obtained for FAN stage and IIEF score (r=-0.631; p=0.001) supporting the significant relationship between these two conditions. There was no significant difference between the groups in age distribution.
Conclusions: This study demonstrated that with the progression of FAN, systemic vascular deterioration affects penile blood flow, increasing the severity of ED. This finding highlights the common pathophysiological mechanisms of FAN and ED and reveals the importance of early diagnosis and multidisciplinary treatment approaches. This relationship should be examined in detail with larger samples and prospective designs in future studies.
Keywords:
Femur avascular necrosis
; erectile dysfunction
; Ficat Classification
1. Introduction
Femoral head avascular necrosis (FAN), particularly seen in middle-aged men, is a serious orthopedic condition involving the death of bone tissue as a result of occlusion or insufficiency of the vessels supplying blood to the femoral head [1]. Various risk factors such as corticosteroid use, alcohol consumption, trauma, and systemic diseases have influential roles in the development of FAN. Cases of FAN are increasing over time and the complications have devastating effects on quality of life. However, early diagnosis and accurate staging could change the course of the disease [2].
Epidemiologically, FAN is seen at varying rates around the world but its frequency increases in men in the high-risk group between the ages of 20 and 40. Studies have shown that the presence of the abovementioned risk factors significantly increases the incidence of the disease in comparison to individuals lacking those risk factors [3]. Furthermore, pathological differences are clearly observed between the early and advanced stages when FAN patients are evaluated with clinical staging. Staging is therefore an effective prognostic tool in the management of the disease and plays a key role in determining treatment strategies [4].
Erectile dysfunction (ED) is the most common sexual dysfunction in men and has negative effects on quality of life and psychosocial status [5]. The pathogenesis of ED arises from a combination of vascular, neurogenic, hormonal, and psychological factors and its prevalence increases with age. Approximately 20% of men over the age of 40 have symptoms of ED, but recent studies also show that the prevalence is rapidly increasing in young adults [6]. A majority of ED cases have a vascular basis and disorders of the vascular system are highly effective in its emergence.
We hypothesized a potential relationship between these two clinical conditions, particularly considering the common mechanism of vascular dysfunction. The vascular damage and disruptions of the microcirculation that occur with FAN can have negative effects not only on bone tissue but also on the broader systemic vascular network. The present study accordingly aimed to clarify the possible common mechanisms of these two different but interrelated diseases by evaluating their pathophysiological and clinical manifestations while drawing attention to the importance of multidisciplinary approaches in treatment strategies. Detailed examination of the epidemiology of both FAN and ED is critical for identifying risk groups and developing proactive strategies for treatment.
2. Materials and Methods
2.1. Study Design
Patients were evaluated retrospectively in this study. The Scientific Research Ethics Committee of the University of Health Sciences Erzurum Faculty of Medicine approved the research (Reference No. 34922). The study was subsequently conducted between January 2020 and December 2023 in the Orthopedics and Traumatology Clinic of the University of Health Sciences Erzurum City Hospital. All analyzed patients were male and had been admitted to outpatient clinics for non-traumatic elective purposes.
The study comprised two groups, with one consisting of 50 patients with FAN and the other consisting of 50 healthy individuals in a control group for comparison. Patients with FAN were evaluated according to the Ficat-Arlet classification using a combination of plain radiographs, magnetic resonance imaging (MRI), and clinical features. With this classification system, cases of FAN are staged with scores ranging from 1 to 4, with higher scores reflecting more severe FAN. The healthy individuals in the control group also underwent plain radiography, MRI, and clinical examination to confirm stage 0 according to the Ficat-Arlet classification.
Both groups were evaluated for ED using the International Index of Erectile Function (IIEF) scale. With this 5-item scale, scores ranging from 1 to 5 are obtained. Patients with no ED complaints receive a score of 5, while those with very severe ED symptoms receive a score of 1.
Ficat-Arlet staging was performed by an orthopedist and traumatologist, while IIEF scores were calculated by a urologist.
2.2. Patients and Control Group
Non-trauma patients with a minimum of 12 months of orthopedic follow-up were analyzed in this study. All included patients had plain radiographs, MRI scans, and clinical follow-up examinations available in their records. Patients with FAN for whom Ficat-Arlet staging could not be performed were excluded.
Furthermore, the urological anamnesis of each patient was recorded and the IIEF scale was administered, and then serum testosterone levels were measured in the morning on an empty stomach. Only individuals with normal serum testosterone levels were included in the analysis. Those with testicular failure that could lead to primary ED, those with multiple sclerosis or Parkinson’s disease, those who had undergone radical pelvic surgery (radical prostatectomy, cystectomy, etc.) or had a history of pelvic radiation, and those using antidepressant drugs or other substances that could cause ED were excluded. The average age of all individuals in both groups was 44.91 years, reflecting the demographic group of young middle age. Individuals under 25 years of age or over 60 were not included in either group. In selecting the upper age limit, it was aimed to exclude the higher rates of FAN and ED seen in individuals ≥60 years of age, as the prevalence of both disorders increases with age. In selecting the lower limit of 25 years, it was aimed to create homogeneous groups of sexually active individuals with appropriate urological development.
2.3. Imaging Protocols
2.3.1. MRI
MRI constitutes the most sensitive imaging technique for the evaluation of FAN, possessing sensitivity of 70-100% and specificity of 90-100%. Since bilateral involvement may be observed in cases of FAN, both hips were included in the field of view of the MRI sequences evaluated in this study. Only patients with confirmed unilateral avascular necrosis were analyzed. Evaluations were based on T1 and T2 sequences. Hyperintense areas such as those affected by early-stage edema, indicated by lower T1 signals, were examined. In T2 sequences, increased intensity between normal bone marrow and ischemic areas was noted and specific evaluations of hip osteonecrosis were performed.
2.3.2. X-rays
Anteroposterior pelvic radiography was performed for all patients. The sphericity of the femoral head, osteoarthritic and secondary degenerative changes, osteochondral structures, and the presence of subchondral fractures were examined. The possible presence of osteopenia, sclerosis, subchondral cyst, crescent sign, cortical collapse, and degenerative changes, all of which are important in Ficat-Arlet staging, was carefully examined on each plain radiograph.
2.4. Data Analysis
To evaluate the data obtained in this study, NCSS 2020 Statistical Software (NCSS LLC, Kaysville, UT, USA) was utilized for statistical analysis. While quantitative variables are presented using mean, standard deviation, median, minimum, and maximum values, qualitative variables are presented as frequencies and percentages in line with descriptive statistical methods. Shapiro-Wilk tests and box-plot graphics were utilized to facilitate evaluations of the compliance of all data with normal distribution. Subsequently, Student t-tests were used for quantitative evaluations of normally distributed data from two groups, while Kruskal-Wallis tests were used for comparisons of non-normally distributed variables from three or more groups and the Dunn test was used to identify the groups from which differences arose. Spearman correlation analysis was performed to evaluate possible relationships between variables. Fisher-Freeman-Halton tests were performed for comparisons of qualitative data. All results were evaluated with 95% confidence intervals and a significance level of p<0.05.
3. Results
The research was finalized with a total of 100 male participants. Ages ranged from 29 to 60 years with a mean age of 44.91±7.37 (Table 1).
According to the obtained IIEF scores, 4.0% (n=4) of the participants had severe ED (score of 1), 9% (n=9) had an ED score of 2, 15% (n=15) had a score of 3, 25% (n=25) had a score of 4, and 47% (n=47) had no ED symptoms (score of 5) (Figure 2).
While half of the analyzed individuals were FAN patients (50%, n=50), 50% (n=50) constituted the healthy control group (Table 2).
The ages of the participants did not differ with statistical significance between the groups (p>0.05). However, IIEF scores were significantly different between patients with FAN and the healthy control group (p=0.001). The rates of mild to moderate ED as reflected by scores of 2-4 were higher among FAN patients compared to the control group, while the rate of individuals with no ED symptoms (score of 5) was higher in the control group (Figure 3).
FAN stages were found to vary significantly by age. Specifically, patients with stage 4 FAN according to the Ficat-Arlet classification were statistically significantly older than those with stage 1 or stage 2 FAN (p=0.004 and p=0.001; p<0.01) (Table 3 and Figure 4).
IIEF scores, reflecting the extent of ED, did not differ significantly according to age (p>0.05).
4. Discussion
In this retrospective case-control study, the relationship between FAN and ED was examined. The findings revealed the existence of a statistically significant negative relationship between FAN stages and IIEF scores (r=-0.631; p=0.001). In other words, as FAN progresses, the severity of ED increases as a result of the deterioration of systemic vascular health and negative effects on penile blood flow.
The similar pathophysiological mechanisms of FAN and ED reflect the ways in which these two diseases are related to each other. Several of the risk factors for the development of FAN, such as corticosteroid use, alcohol consumption, and systemic diseases, disrupt the blood flow to bone tissue and trigger avascular necrosis. The pathogenesis of ED is similarly largely based on vascular dysfunction. Dysregulated modulation of vascular endothelial growth factor (VEGF) and microcirculation disorder constitute common foundations of these diseases [1,2].
In this study, the finding of a higher rate of ED in the patient group versus the control group supports the possibility of FAN causing not only local bone damage but also systemic vascular damage. FAN is a condition that generally occurs as a result of reduced blood flow and it may be associated with systemic vascular complications. In particular, systemic diseases such as diabetes are known to have influential roles in the development of FAN. Lai et al. examined the relationship between diabetes and FAN and stated that vascular complications may be effective in the disease process [7]. It is thought that, particularly in advanced stages of FAN, deterioration in the vascular system may increase the severity of ED by restricting penile blood flow. The present study accordingly highlights the common vascular pathophysiologies of FAN and ED and demonstrates the importance of a multidisciplinary treatment approach.
In our review of the literature, no study was found that directly addressed the relationship between FAN and ED. However, vascular endothelial damage plays a decisive role in the pathophysiologies of both diseases. In line with this common mechanism, extracorporeal shock wave therapy (ESWT) has been reported to provide beneficial results in the treatment of both FAN and ED [8,9]. ESWT is used for both diseases because shock waves trigger neovascularization by increasing VEGF expression within the tissue, thereby improving blood flow [10,11]. The positive effects of ESWT in treating both diseases support the existence of overlapping pathophysiologies between FAN and ED and reveal that evaluating these clinical conditions together is important for the planning of effective treatment strategies.
There is no definitively proven treatment for FAN, neither pharmacologically nor surgically. The literature reports that anticoagulants, bisphosphonates used to inhibit bone destruction, prostaglandin analogs, antiplatelet drugs such as acetyl salicylate, and many other agents are being used for the treatment of FAN [12,13,14,15,16,17,18]. However, no treatment has been shown to offer high levels of evidence and these treatments have side effects [19]. One previous study involving the administration of sildenafil to rats showed increased levels of VEGF and osteopontin in the early period following ischemic trauma to the femoral head together with a corresponding increase in the production of new non-calcified (osteoid) bone tissue and matrix, verifying that sildenafil may facilitate the regeneration of bone tissue in cases of ischemic trauma [20]. In another study, vardenafil was shown to have a beneficial impact on bone union and promote the early stages of fracture healing, when vasodilation is more necessary in a setting of increased inflammation [21]. The first-line treatment of ED traditionally entails oral drug therapy with agents such as apomorphine or sildenafil, but two new phosphodiesterase 5 (PDE5) inhibitors, tadalafil and vardenafil, were shown to provide better selectivity [22]. The strong relationship observed in our study between FAN and ED, the positive effects of PDE5 inhibitors on avascular necrosis and bone fracture healing in previous experimental studies, and the successful results previously obtained with PDE5 inhibitors in the treatment of ED signify the potential of these inhibitors for future use in the treatment of patients with FAN. Prospective randomized double-blind and controlled studies are needed to determine the true clinical effectiveness of these compounds, but the present study is important in terms of offering guidance for future research in this area.
However, the present study also has methodological limitations to be acknowledged. Its retrospective design and small sample size may have affected the generalizability of the findings. Future studies comprising larger patient populations, prospective designs, and the inclusion of additional variables such as hormonal profiles and microcirculation parameters would support a more thorough understanding of the relationship between FAN and ED.
In conclusion, this study has demonstrated that ED severity increases with increasing FAN stages, and the similar vascular pathophysiological mechanisms of these two diseases explain that relationship. Our findings emphasize the crucial value of early diagnosis and multidisciplinary treatment strategies in the management of both diseases. In addition, the early evaluation and management of ED in patients diagnosed with FAN will play an important role in improving their quality of life.
Author Contributions
Conceptualisation, E.Ö.- H.U.Ö. and N.A.; Data curation, E.Ö.-A.A.Ö,-F.E.T; and E.D.; Formal analysis, E.Ö.-A.A.Ö. and E.D.; Methodology, E.Ö.-H.U.Ö. and N.A.; Supervision, E.Ö.-F.E.T. and N.A.; Validation, E.Ö.-A.A.Ö.-F.E.T.-N.A.-H.U.Ö. and E.D.; visualisation,A.A.Ö; Writing—original draft, E.Ö..-H.U.Ö; Writing—review and editing, E.Ö.,-A.A.Ö,- F.E.T.,-N.A.,-H.U.Ö. and E.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Institutional ethics committee (Erzurum Medical Faculty Scientific Research Ethics Committee for Clinical Research: 34922).
Informed Consent Statement
Patient consent was waived due to the research’s retrospective nature and the medical imaging’s anonymisation.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| FAN | Femoral head avascular necrosis |
| ED | Erectile dysfunction |
| IIEF | The International Index of Erectile Function |
| MRI | Magnetic resonance imaging |
| VEGF | Vascular endothelial growth factor |
| ESWT | Extracorporeal shock wave therapy |
| PDE 5 | Phosphodiesterase 5 |
References
- Mwale F, Wang H, Johnson AJ, Mont MA, Antoniou J. Abnormal vascular endothelial growth factor expression in mesenchymal stem cells from both osteonecrotic and osteoarthritic hips. Bull NYU Hosp Jt Dis. 2011;69(Suppl. 1):S56-61.
- Moya-Angeler J. Current concepts on osteonecrosis of the femoral head. World J Orthop. 2015;6:590-601. [CrossRef]
- Konarski W, Poboży T, Śliwczyński A, Kotela I, Krakowiak J, Hordowicz M, et al. Avascular necrosis of femoral head—Overview and current state of the art. Int J Environ Res Public Health. 2022;19:7348. [CrossRef]
- Petek D, Hannouche D, Suva D. Osteonecrosis of the femoral head: pathophysiology and current concepts of treatment. EFORT Open Rev. 2019;4:85-97. [CrossRef]
- Varela CG, Yeguas LAM, Rodríguez IC, Vila MDD. Penile Doppler ultrasound for erectile dysfunction: Technique and interpretation. AJR Am J Roentgenol. 2020;214:1112-1121. [CrossRef]
- Pantazis A, Franco I, Gitlin J. Erectile dysfunction in adolescents and young adults. Curr Urol Rep. 2024;25:225-232. [CrossRef]
- Lai SW, Lin CL, Liao KF. Real-world database examining the association between avascular necrosis of the femoral head and diabetes in Taiwan. Diabetes Care. 2019;42:39-43. [CrossRef]
- Wang CJ, Cheng JH, Huang CC, Yip HK, Russo S. Extracorporeal shockwave therapy for avascular necrosis of femoral head. International Journal of Surgery. 2015;24(Pt. B):184-187. [CrossRef]
- Fojecki GL, Tiessen S, Osther PJS. Extracorporeal shock wave therapy (ESWT) in urology: A systematic review of outcome in Peyronie’s disease, erectile dysfunction and chronic pelvic pain. World J Urol. 2017;35:1-9.
- Chawla ST, Shahan J, Soutipan N, Sorkhi SR, Choi YS, Bae WJ, et al. Radial type low-intensity extracorporeal shockwave therapy enhances penile microvascular perfusion in an aging rat model: A novel interventional strategy to treat erectile dysfunction. World J Mens Health. (in press). [CrossRef]
- Ma HZ, Zeng BF, Li XL. Upregulation of VEGF in subchondral bone of necrotic femoral heads in rabbits with use of extracorporeal shock waves. Calcif Tissue Int. 2007;81:124-131. [CrossRef]
- Ajmal M, Matas AJ, Kuskowski M, Cheng EY. Does statin usage reduce the risk of corticosteroid-related osteonecrosis in renal transplant population? Orthop Clin North Am. 2009;40:235-239.
- Chotanaphuti T, Thongprasert S, Laoruengthana A. Low molecular weight heparin prevents the progression of precollapse osteonecrosis of the hip. J Med Assoc Thai. 2013;96:1326-1330.
- Glueck CJ, Freiberg RA, Sieve L, Wang P. Enoxaparin prevents progression of stages I and II osteonecrosis of the hip. Clin Orthop Relat Res 2005;(435):164-170. [CrossRef]
- Glueck CJ, Freiberg RA, Wissman R, Wang P. Long term anticoagulation (4-16 years) stops progression of idiopathic hip osteonecrosis associated with familial thrombophilia. Adv Orthop 2015;2015:138382. [CrossRef]
- Pengde K, Fuxing P, Bin S, Jing Y, Jingqiu C. Lovastatin inhibits adipogenesis and prevents osteonecrosis in steroid-treated rabbits. Joint Bone Spine. 2008;75:696-701. [CrossRef]
- Pritchett JW. Statin therapy decreases the risk of osteonecrosis in patients receiving steroids. Clin Orthop Relat Res 2001;(386):173-178. [CrossRef]
- Agarwala S, Shetty V, Karumuri LK, Vijayvargiya M. Patellar resurfacing versus nonresurfacing with patellaplasty in total knee arthroplasty. Indian J Orthop 2018;52:393-398. [CrossRef]
- Lee YJ, Cui Q, Koo KH. Is there a role of pharmacological treatments in the prevention or treatment of osteonecrosis of the femoral head?: A systematic review. J Bone Metab. 2019;26:13-18. [CrossRef]
- Hines JT, Jo WL, Cui Q, Mont MA, Koo KH, Cheng EY, et al. Osteonecrosis of the femoral head: An updated review of ARCO on pathogenesis, staging and treatment. J Korean Med Sci. 2021;36:e177. [CrossRef]
- Atcı T, Alagöz E, Yaprak Saraç E, Özbay H, Daşcı MF, Acar A, et al. Effects of different vardenafil doses on bone healing in a rat fracture model. Jt Dis Relat Surg. 2021;32:313-322. [CrossRef]
- Rodríquez Vela L, Gonzalvo Ibarra A, Pascual Regueiro D, Rioja Sanz LA. Disfunción eréctil [Erectile dysfunction]. Actas Urol Esp. 2002;26:667-690.
Figure 1.
Distribution of femoral head avascular necrosis (FAN) stages according to the Ficat-Arlet classification.
Figure 1.
Distribution of femoral head avascular necrosis (FAN) stages according to the Ficat-Arlet classification.
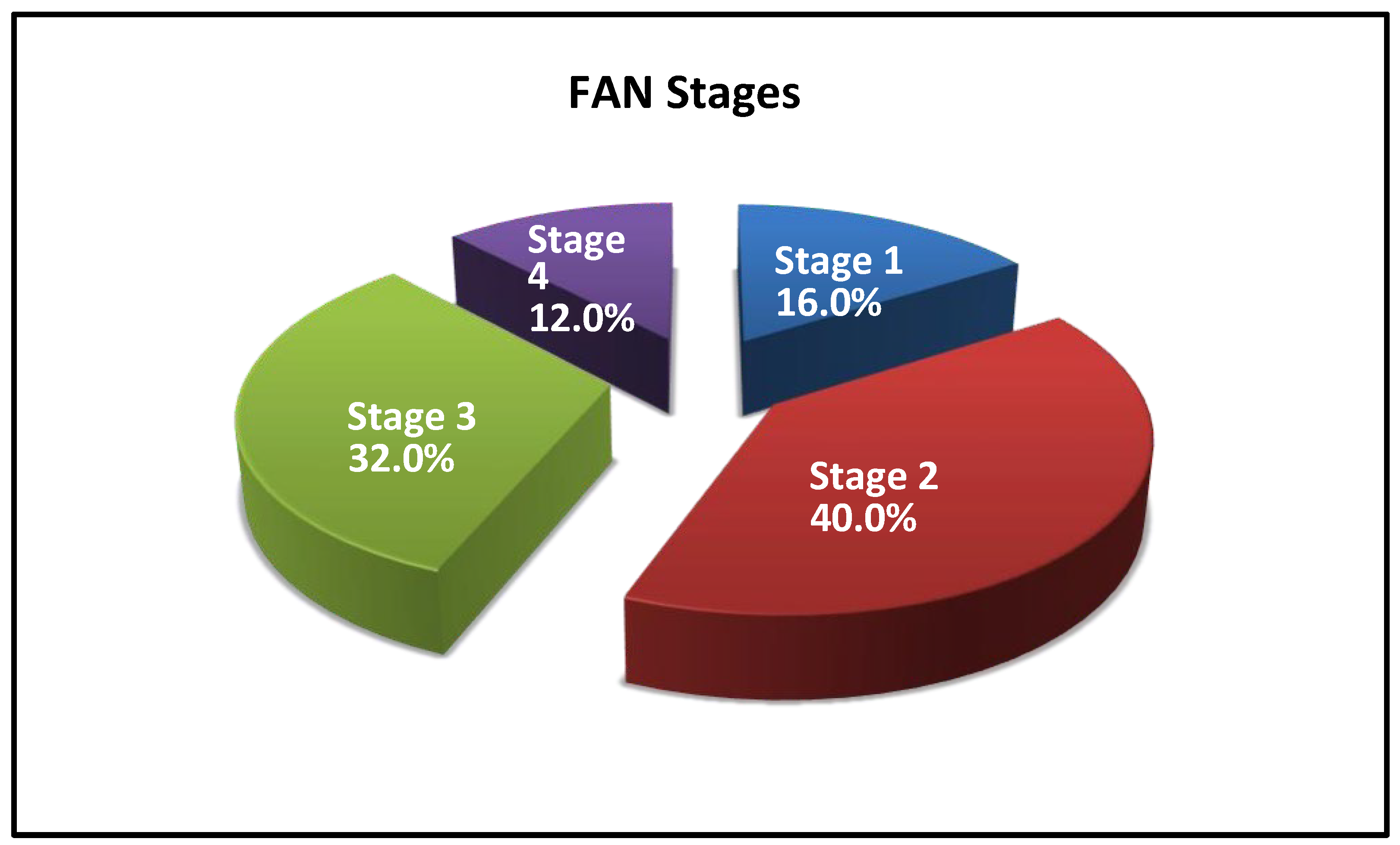
Figure 2.
Distribution of IIEF scores, reflecting the extent of erectile dysfunction (ED).
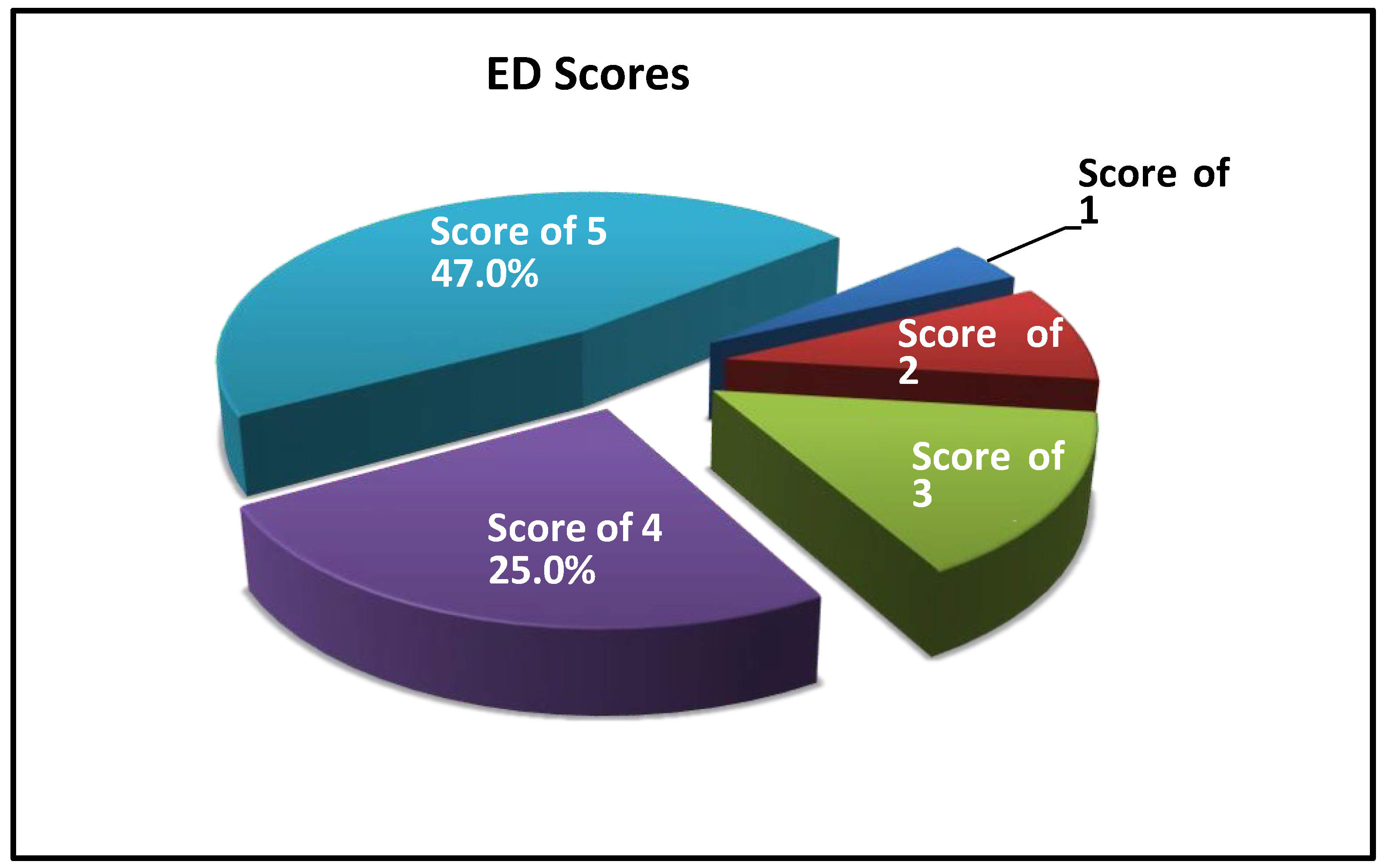
Figure 3.
Distribution of IIEF scores by groups, reflecting the extent of erectile dysfunction (ED).
Figure 3.
Distribution of IIEF scores by groups, reflecting the extent of erectile dysfunction (ED).
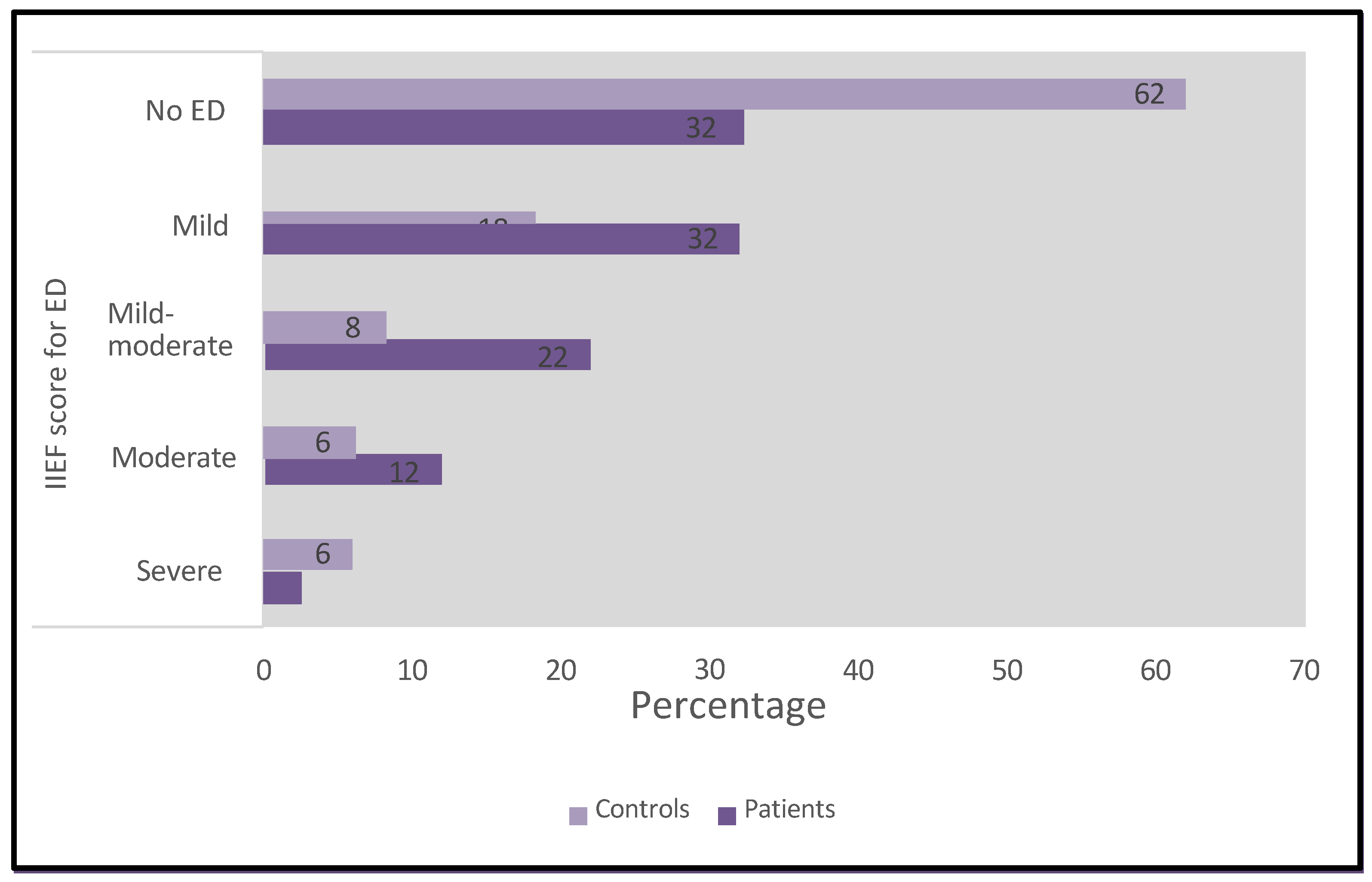
Figure 4.
Variations in FAN stage according to age.
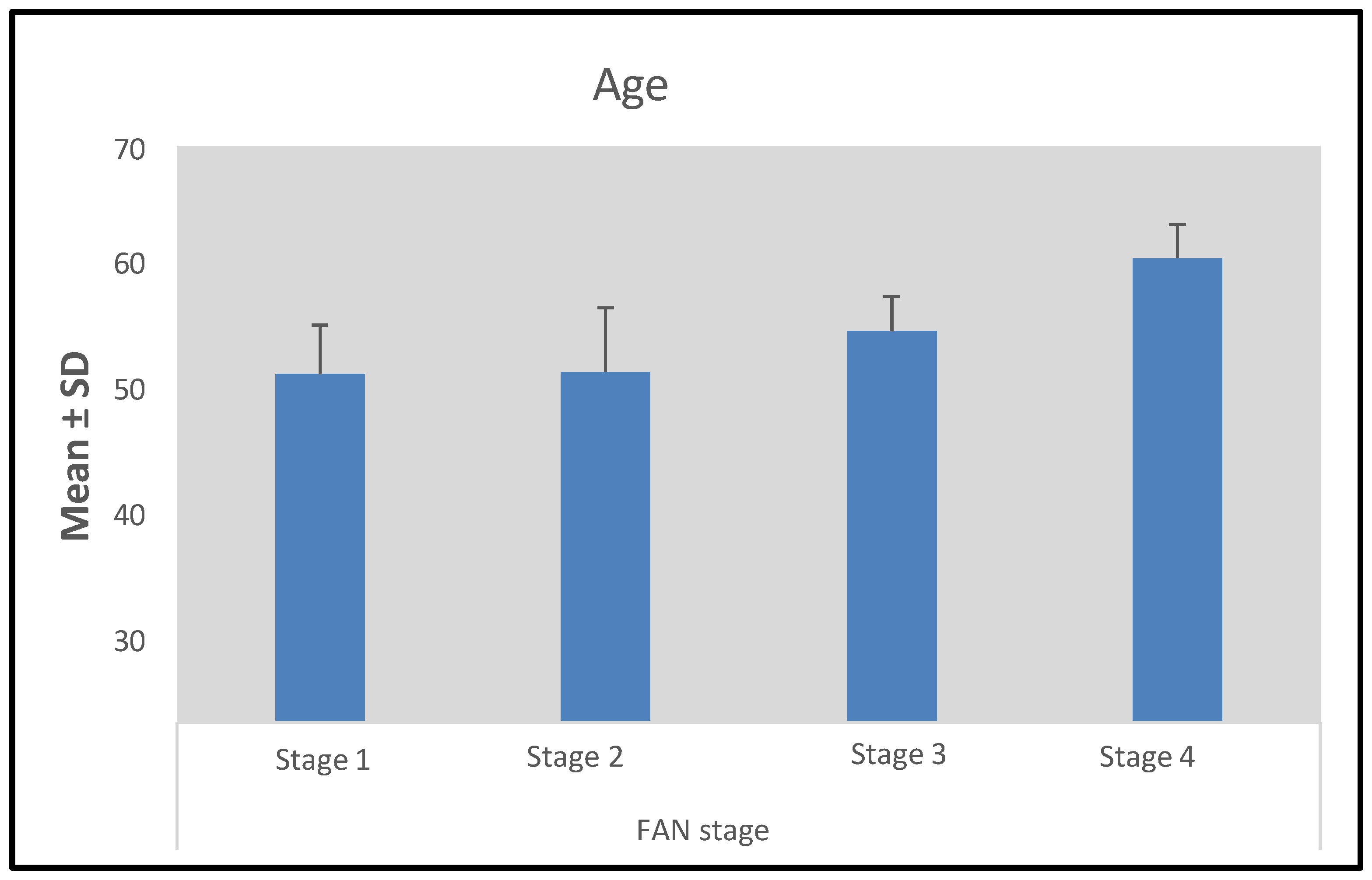
Figure 5.
Relationship between FAN stage and IIEF score. While higher FAN scores indicate more severe FAN, lower IIEF scores indicate more severe ED.
Figure 5.
Relationship between FAN stage and IIEF score. While higher FAN scores indicate more severe FAN, lower IIEF scores indicate more severe ED.
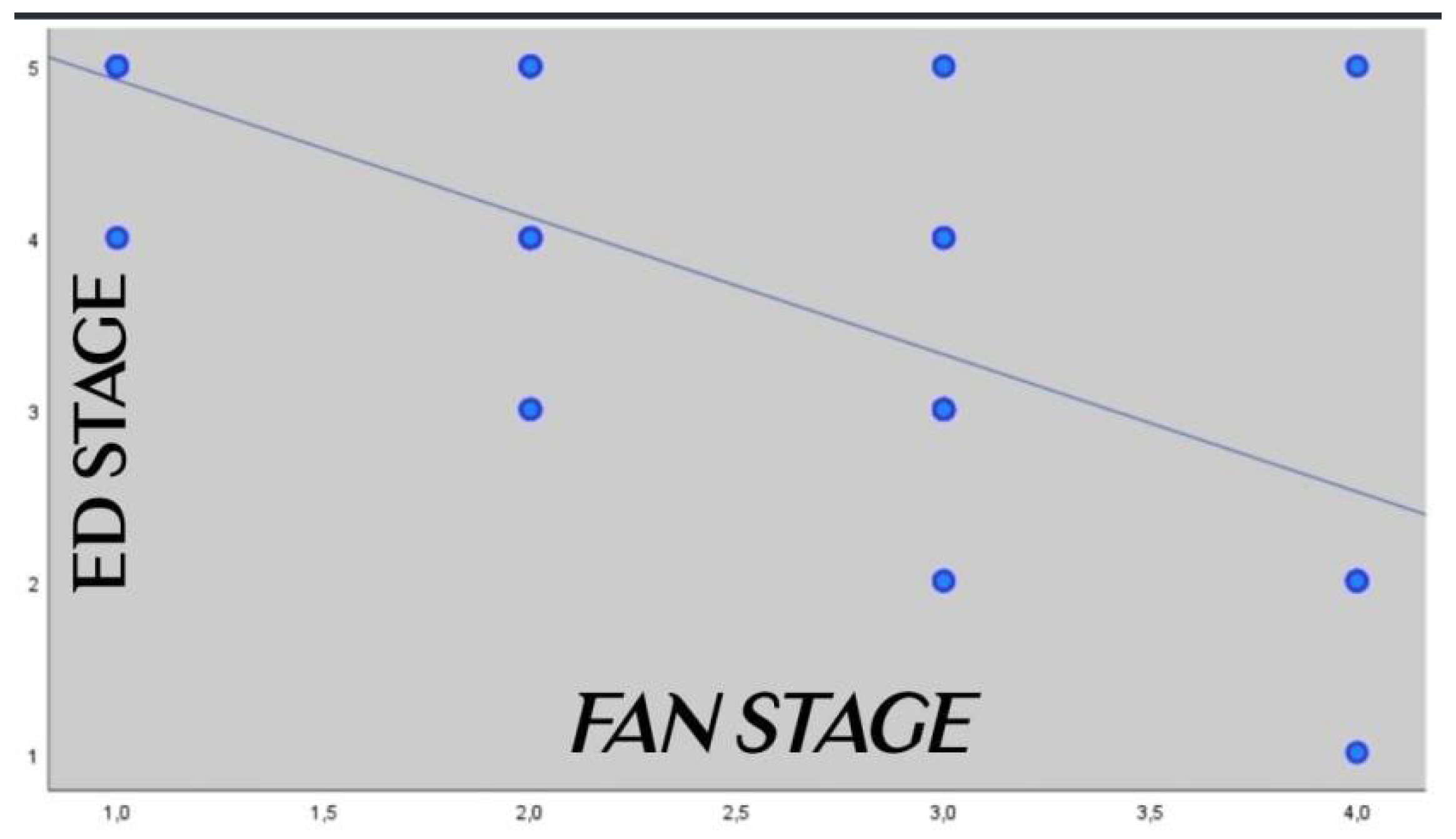

Table 1.
Descriptive data of all participants.
| n (%) | ||
|---|---|---|
| Years | Mean ± SD | 44.91±7.37 |
| Median (range) | 45 (29-60) | |
| FAN stage | 1 (mild) | 8 (16.0) |
| 2 | 20 (40.0) | |
| 3 | 16 (32.0) | |
| 4 (severe) | 6 (12.0) | |
| IIEF score | 1 (severe ED) | 4 (4.0) |
| 2 | 9 (9.0) | |
| 3 | 15 (15.0) | |
| 4 | 25 (25.0) | |
| 5 (no ED) | 47 (47.0) | |
| Group | Patients | 50 (50.0) |
| Control group | 50 (50.0) |
According to the FAN staging, stage 1 disease (mild) was detected in 16% (n=8) of the cases, stage 2 in 40% (n=20), stage 3 in 32% (n=16), and stage 4 (severe) in 12.0% (n=6) (Figure 1).
Table 2.
Comparisons of descriptive characteristics by groups.
| Patients (n=50) | Controls (n=50) | p | ||
|---|---|---|---|---|
| Age | Mean ± SD | 45.86±7.54 | 43.96±7.16 | 0.199 a |
| Median (range) | 47 (29-60) | 45 (29-57) | ||
| FAN stage | 1 (mild) | 8 (16.0) | 0 (0.0) | - |
| 2 | 20 (40.0) | 0 (0.0) | ||
| 3 | 16 (32.0) | 0 (0.0) | ||
| 4 (severe) | 6 (12.0) | 0 (0.0) | ||
| IIEF score | 1 (severe ED) | 1 (2.0) | 3 (6.0) | 0.001 b,** |
| 2 (moderate) | 6 (12.0) | 3 (6.0) | ||
| 3 (mild-moderate) | 11 (22.0) | 4 (8.0) | ||
| 4 (mild) | 16 (32.0) | 9 (18.0) | ||
| 5 (no ED) | 16 (32.0) | 31 (62.0) |
a: Student t-test; b: Fisher-Freeman-Halton test; **: p<0.01.
Table 3.
Comparison of FAN stages and IIEF scores by age.
| Age | ||||
|---|---|---|---|---|
| Mean ± SD | Median (range) | pc | ||
|
FAN stage (n=50) |
1 (mild) | 42.38±5.97 | 42.5 (34-53) | 0.001** |
| 2 | 42.65±7.79 | 42 (29-55) | ||
| 3 | 47.63±4.22 | 49 (41-53) | ||
| 4 (severe) | 56.5±4.09 | 58 (50-60) | ||
| IIEF score (n=100) | 1 (severe ED) | 49.50±8.19 | 51.5 (38-57) | 0.053 |
| 2 (moderate) | 50.89±7.32 | 51 (41-60) | ||
| 3 (mild-moderate) | 46.93±3.92 | 47 (41-55) | ||
| 4 (mild) | 43.48±7.23 | 44 (29-55) | ||
| 5 (no ED) | 43.49±7.62 | 43 (32-58) |
c: Kruskal-Wallis test and Dunn-Bonferroni test; **: p<0.01.
Table 4.
Relationship between FAN stage and erectile dysfunction.
| FAN stage | ||
|---|---|---|
| IIEF score | r | -0.631 |
| p | 0.001** |
Spearman correlation coefficient; **: p<0.01.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



