
Submitted:
03 March 2025
Posted:
05 March 2025
You are already at the latest version
Abstract
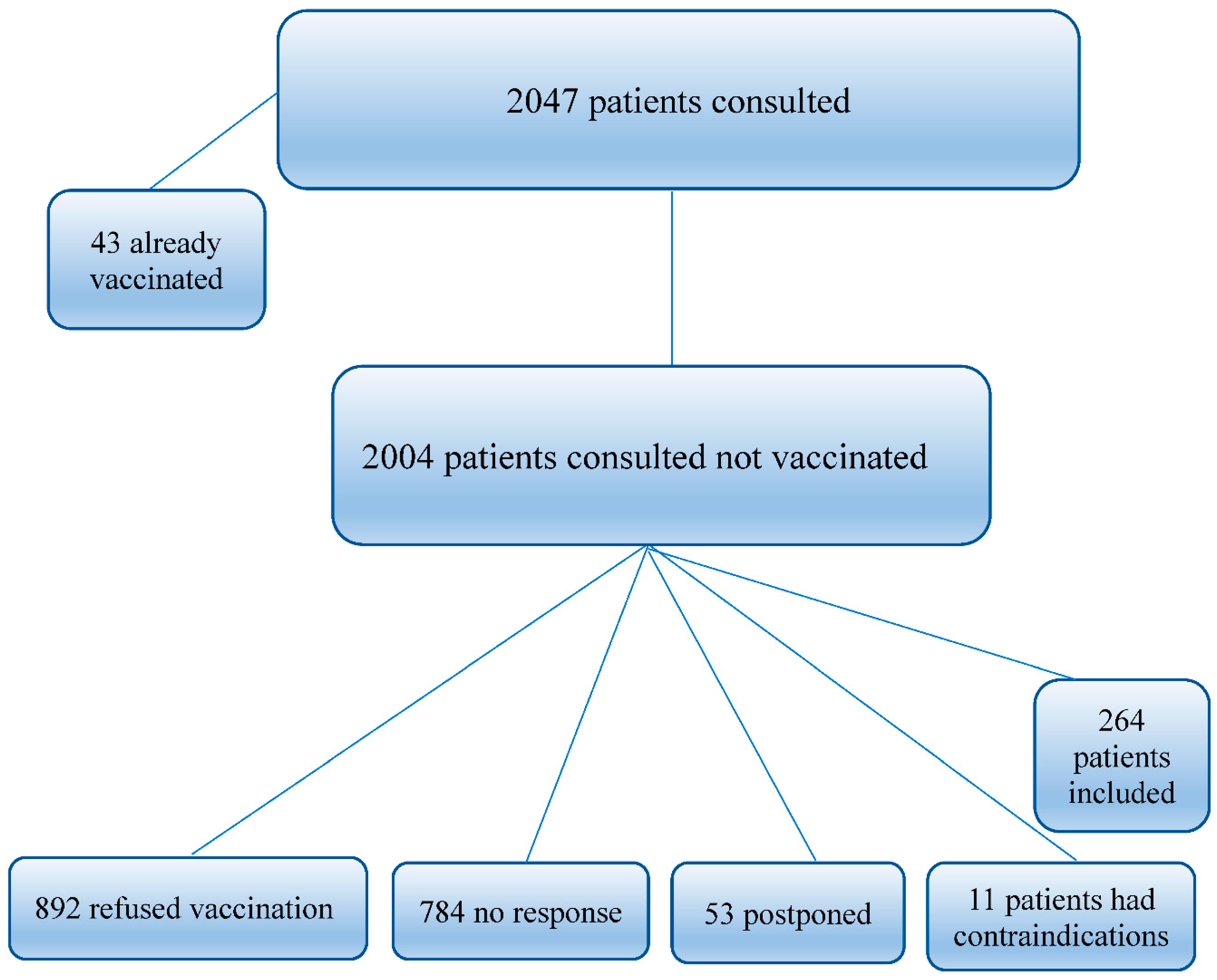
Background: Viral infections are very severe infections and can be responsible for death, as is the case with influenza infection; which during a short period of spread can cause significant deaths in the general population, and in immunocompromised patients in particular; as is the case with cancer patients; weakened by the disease and viral infection too. Patients with cancer are at high risk of severe infections complications. Among people with immunosuppression due to chemotherapy, corticosteroid treatment, or immunotherapy, high rates of influenza infection and related complications are frequently observed. In Algeria, the influenza vaccine is recommended for people aged 65 and over, as well as for those with chronic medical conditions who are at high risk of complications. It is offered by the government free of charge to elderly and other risk groups and distributed through general hospitals and pharmacists Material and methods: The medical oncology department of the Establishment DIDOUCHE Mourad, Constantine, launched a vaccination campaign for eligible patients, during the vaccination campaign initiated by the Algerian Ministry of Health during seasonal infection from October to December, each year. During two (02) months of medical oncology consultations (November 2024 to December 2024), 2047 patients were consulted and 264 patients were concerned by the vaccination. The findings emphasize the crucial role of healthcare professionals in advocating for influenza vaccination among cancer patients and the need for collaboration with health authorities to improve vaccination coverage Results: For a total of 2047 patients consulted (whose 43 (2,10 %) were already vaccinated), 892 (43.57%) patients refused the idea of vaccination. 784 (38.29%) patients did not want to comment yet at the time of the consultation and preferred to continue their treatments, 53 (2.58%) were postponed for bone marrow aplasia. 11 (0.53%) patients had contraindications to vaccination including 3 (27.27%) egg allergy, 2 (18.18%) tuberculosis, 2 (18.18%) febril neutropenia ,2 (18.18%%) recent ischemic stroke (less than 20 days), 1 (9.09%) on treatment with Rituximab and 1 (9,09%) patient had a recent Guillan Barre Syndrom. (less than 6 weeks). 264 cancer patients ((12.89%) were included in the study of adherence to a vaccination campaign launched in medical oncology department of the hospital establishment DIDOUCHE Mourad, Constantine 189 (71.60%) patients were women and 75 (28.40%) patients were men. Different tumor localizations were noted. As a result, the influenza vaccination campaign coverage in our study was 13,17 % for all ages of cancer patients included and 48,86 % for those ≥ 65 years. Discussion: The influenza vaccination coverage was low among cancer patients. Influenza non-vaccination in the previous season was the strongest predictor of not receiving influenza vaccination in the current season. The main reasons for the low level of vaccination coverage rate that emerged in our study were having no-informations for indication to cancer patients (41,28%), fear of side effects (31,43%) getting medical treatment for cancer (chemotherapy, targeted therapy or immunotherapy ) (9,46%), lack of efficacy (9,09%), and no-need (8,71%). Nevertheless, after having informations and advice by medical oncologists, all patients stated that they will get vaccine next year. Conclusion: Vaccination against influenza in patients with cancer is a serious issue that presents many challenges, mainly in association with the immunocompromised state of these patients. Owing to disease and/or treatment-associated immunosuppression, patients with cancer are vulnerable to infectious diseases and are at high risk of developing infection- related complications, including those associated with influenza. Vaccination against common preventable diseases, including seasonal influenza, is therefore highly recommended in these patients.
Keywords:
Background
Material and Methods
Results

| SEX | N | % |
| WOMEN | 189 | 71,60 |
| MEN | 75 | 28,40 |
| TOTAL | 264 | 100% |
| Characteristics by age, group and sex | ||||
| Age range | Women total | Men total | TOTAL | % |
| 18-24 years old | 1 | 1 | 2 | 0,75 |
| 25-29 years old | 2 | 1 | 3 | 1,13 |
| 30-34 years old | 2 | 2 | 4 | 1,51 |
| 35-39 years old | 8 | 8 | 3,03 | |
| 40-44 years old | 5 | 3 | 8 | 3,03 |
| 45-49 years old | 13 | 1 | 14 | 5,30 |
| 50-54 years old | 20 | 4 | 24 | 9,09 |
| 55-59 years old | 30 | 7 | 37 | 14,01 |
| 60-64 | 21 | 14 | 35 | 13,25 |
| 65 years & more | 87 | 42 | 129 | 48,86 |
| TOTAL | 189 | 75 | 264 | 100 |
| Tumor types of the vaccinated population | ||
| TUMOR TYPE | N | % |
| Breast | 115 | 43,56 |
| Colorectal | 47 | 17,80 |
| Prostate | 18 | 6,81 |
| Ovary | 12 | 4,54 |
| Lung | 11 | 4,16 |
| Sarcoma | 9 | 3,4 |
| Pancreatic | 7 | 2,65 |
| Gastric | 5 | 1,89 |
| UCNT | 4 | 1,51 |
| Testicular | 3 | 1,13 |
| Kidney | 3 | 1,13 |
| Others (GIST, LNH, Bladder, Endometer | 30 | 11,36 |
Discussion
| Causes of non-vaccination | N | % |
| Fear of side effects | 83 | 31,43 |
| Lack of efficacy | 24 | 9.09 |
| No need | 23 | 8,71 |
| No-information | 109 | 41,28 |
| In -chemotherapy, or Immunotherapy | 25 | 9,46 |
| TOTAL | 264 | 100 |
Conclusion
References
- Cooksley, C.; Avritscher, E.; Bekele, B.; Rolston, K.; Geraci, J.; Elting, L. Epidemiology and outcomes of serious influenza-related infections in the cancer population. Cancer. 2005;104:618-28. [CrossRef]
- Bitterman, R.; Eliakim-Raz, N.; Vinograd, I.; Zalmanovici Trestioreanu, A.; Leibovici, L.; Paul, M. Influenza vaccines in immunosuppressed adults with cancer. CD008983Cochrane Database Syst Rev 2018;2. [CrossRef]
- European Centre for Disease Prevention and Control. Seasonal influenza vaccination and antiviral use in Europe – Overview of vaccination recommendations and coverage rates in the EU Member States for the 2013–14 and 2014–15 influenza seasons 2016.
- Vinograd I, Baslo R, Eliakim-Raz N, Farbman L, Taha A, Sakhnini A, et al. Factors associated with influenza vaccination among adult cancer patients: a case-control study. Clin Microbiol Infect 2014;20(9):899–905 . [CrossRef]
- The coverage of influenza vaccination and predictors of influenza non-vaccination in Danish cancer patients: A nationwide register-based cohort study Lau Amdisen a, , Lars Pedersen a, Niels Abildgaard b, Christine Stabell Benn c,d , Mikael Rørth a ,Deirdre Cronin-Fenton a , Signe Sørup a Vaccine 42 (2024) 1690–1697.
- Perception about influenza pneumococcal vaccines vaccination coverage among patients with malignancies their family members, Y. Urun, H. Akbulut, A. Demirkazik, F. Cay Senler, G. Utkan, H. Onur, F. Icli Ankara University School of Medicine, Department of Medical Oncology, Ankara, Turkey JBUON 2013; 18(2): 511-515 ISSN: 1107-0625 •.
- Beck CR, McKenzie BC, Hashim AB et al. Influenza vaccination for immunocompromised patients: sys- tematic review and meta-analysis from a public health policy perspective. PLoS One 2011; 6(12): p e29249. [CrossRef]
- Pollyea, D.A.; Brown, J.M.; Horning, S.J. Utility of influ- enza vaccination for oncology patients. J Clin Oncol 2010; 28: 2481-2490.
- Ring, A.; Marx, G.; Steer, C.; Harper, P. Influenza vaccina- tion and chemotherapy: a shot in the dark? Support Care Cancer 2002; 10: 462-465.
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: a sys- tematic review and meta-analysis. Lancet Infect Dis 2012; 12: 36-44.
- Casper, C.; Englund, J.; Boeckh, M. How I treat influen- za in patients with hematologic malignancies. Blood 2010; 115: 1331-1342.
- Avritscher EB, Cooksley CD, Geraci JM et al. Cost-ef- fectiveness of influenza vaccination in working-age cancer patients. Cancer 2007; 109: 2357-2364.
- World Health Organisation (2018) Influenza (Seasonal) Fact sheet. Accessed 15 Nov 2019.
- Kunisaki KM, Janoff EN (2009) Influenza in immunosuppressed populations: a review of infection frequency, morbidity, mortality, and vaccine responses. Lancet Infect Dis 9:493–504.
- Zbinden D, Manuel O (2014) Influenza vaccination in immuno- compromised patients: efficacy and safety. Immunotherapy 6: 131–139.
- Ortbals, D.W.; Liebhaber, H.; Presant, C.A.; Van Amburg, A.L.I.I.I.; Lee, J.Y. Influ-enza immunization of adult patients with malignant diseases. Ann Intern Med. 1977;87:552–7.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



