
Submitted:
01 March 2025
Posted:
03 March 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic has significantly impacted global health, particularly influencing healthcare-seeking behavior in rural areas where infrastructure and literacy are limited. However, empirical studies on the role of knowledge of COVID-19 symptoms in health facility visits remain scarce. Applying the Health Belief Model, this study hypothesizes that greater knowledge of symptoms of COVID-19 enhances the likelihood of visiting healthcare facilities in rural India due to increased perceived susceptibility and severity, thereby encouraging a timely medical visit. Utilizing a dataset of 1,950 respondents from the 2020 Round 1 of the COVID-19 Related Shocks Survey in Rural India, conducted by the World Bank and its collaborators, mean comparison tests and probit regression analysis were employed to investigate this relationship. The findings indicate that greater knowledge of the symptoms of COVID-19 significantly increases the likelihood of visits to the health facility. Additional factors influencing healthcare utilization include age, age squared, female gender, rich states, higher household consumption expenditure, no schooling and few interaction terms. The robustness of these findings was confirmed through Maximum Likelihood Estimation. The results underscore the importance of targeted health education and awareness campaigns to enhance health literacy and promote timely healthcare-seeking behavior during pandemics, especially in resource-limited rural settings.
Keywords:
COVID-19
; rural India
; COVID-19 symptoms knowledge
; health facility visit
1. Introduction
The COVID-19 pandemic has significantly impacted global health, and healthcare-seeking behaviors play a crucial role in controlling the spread of the disease [1]. In rural areas, where the healthcare infrastructure is often limited, individuals' awareness of COVID-19 symptoms is vital for timely medical attention [2]. Knowledge of symptoms such as fever, cough, difficulty breathing, and loss of taste or smell can directly influence decisions to visit healthcare facilities [3]. Although numerous studies have explored factors influencing healthcare utilization/avoidance during the pandemic [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23], the specific impact of knowledge of COVID-19 symptoms on health facility visits in rural developing countries remains underexplored. This gap is particularly critical in rural India, where health literacy is often lower, and access to medical facilities is restricted by geographical and socio-economic factors [24,25,26,27]. Knowledge of COVID-19 symptoms can be considered a health literacy indicator, reflecting an individual's ability to understand and act upon health information [28]. In such settings, knowledge of COVID-19 symptoms can encourage timely healthcare-seeking behaviors [29]. The Health Belief Model (HBM) emphasizes that knowledge and perceptions significantly shape healthcare utilization [30,31]. This model highlights that understanding symptoms influences perceptions of risk and the likelihood of seeking medical attention [32,33,34,35]. This study addresses the gap by applying the Health Belief Model (HBM) framework to hypothesize that greater knowledge of COVID-19 symptoms enhances the likelihood of visiting health facilities in rural areas, thereby improving early detection and reducing disease transmission.
The Health Belief Model (HBM) serves as a robust theoretical framework for understanding how individual beliefs and perceptions about health influence their behaviors. Developed by social psychologists in the 1950s, the HBM posits that health-related behaviors are determined by an individual's perception of four key constructs: perceived susceptibility, perceived severity, perceived benefits, and perceived barriers [30]. In the context of COVID-19, perceived susceptibility refers to an individual's belief about the likelihood of contracting the virus [36], while perceived severity refers to their understanding of the serious consequences associated with the infection [37]. Knowledge of COVID-19 symptoms can significantly influence these perceptions, since recognizing specific symptoms such as fever, cough, and difficulty breathing can increase an individual's sense of susceptibility and severity, prompting them to take preventive actions and seek medical attention. The HBM also emphasizes perceived benefits and perceived barriers as crucial determinants of health behaviors. Perceived benefits refer to an individual's belief in the efficacy of taking specific actions to reduce the threat of illness [38]. In this case, greater awareness of COVID-19 symptoms can improve the perceived benefits of visiting healthcare facilities for early diagnosis and treatment. However, perceived barriers include factors that may hinder people from seeking medical care [39], such as fear of exposure to the virus in healthcare facilities, lack of transportation, or financial constraints. By increasing knowledge of the symptoms of COVID-19, public health interventions can address these barriers by providing clear information about the importance of early detection and the availability of safe and accessible healthcare services. This approach is particularly relevant in settings with limited healthcare infrastructure, where timely healthcare-seeking behaviors are essential to control the spread of the virus and improve health outcomes. By applying the HBM framework, this study aims to uncover the impact of symptom awareness on healthcare utilization. Studying this association will provide valuable insights into the need to improve knowledge of COVID-19 symptoms as a proxy for health literacy in the pandemic context. These findings can ultimately contribute to better management of the COVID-19 pandemic in vulnerable rural communities by promoting timely utilization of healthcare and strengthening health literacy.
Among all potential variables, the knowledge of the symptoms of COVID-19 is a crucial determinant for visits to health facilities during the pandemic. COVID-19 presents with a variety of symptoms that can vary in severity from mild to severe. Key symptoms include fever, cough, and difficulty breathing, which are common in many respiratory diseases, but COVID-19 also has unique symptoms such as loss of taste or smell, which are less common in other illnesses [40]. Additionally, COVID-19 can cause gastrointestinal symptoms such as nausea and diarrhea, as well as neurological symptoms such as headache and fatigue [41,42]. This distinct combination of symptoms allows people to identify the potential severity of their condition and differentiate it from other illnesses such as the common cold or influenza [43]. Understanding these key symptoms provides individuals with immediate and actionable information needed to make informed decisions about seeking medical care. Unlike other factors such as socioeconomic status, access to healthcare, or psychological barriers, direct awareness of symptoms has an immediate impact on healthcare-seeking behavior [44]. Recognizing symptoms such as fever, cough, and difficulty breathing enables individuals to comprehend the urgency of their condition and the need for professional medical intervention [3]. This direct link between symptom recognition and healthcare-seeking behavior is critical in rural settings, where delays in seeking care can lead to worse health outcomes due to limited healthcare resources [45]. Previous research has shown that awareness of symptoms significantly influences health behaviors, particularly in the context of infectious diseases. For instance, studies have shown that people with greater awareness of disease symptoms are more likely to seek timely medical care, thereby improving health outcomes [46,47]. In the context of COVID-19, this awareness can drive timely utilization of healthcare, which is essential for early detection and treatment, ultimately reducing the spread of the virus and mitigating its impact on vulnerable populations. Therefore, by focusing on the awareness of symptoms, this study addresses a fundamental aspect of public health education that can drive timely utilization of healthcare.
This study contributes to the literature in three ways. First, it provides pioneering empirical evidence of the role of knowledge of symptoms of COVID-19 (a proxy of health literacy) in the influence of healthcare visits during the pandemic. Second, it uses a nationally representative large-scale dataset of rural India with approximately 2000 participants, allowing for a comprehensive analysis of the role of knowledge of COVID-19 symptoms in visits to health facilities. This approach improves the robustness of our findings, strengthens the generalizability of the results to the broader rural Indian population, and provides a more nuanced understanding of the dynamics during the pandemic. Third, it highlights the significance of understanding COVID-19 symptoms in rural settings, where healthcare infrastructure is often limited, and health literacy is generally lower. By identifying specific barriers and facilitators to healthcare-seeking behaviors, this study offers targeted recommendations for public health interventions to enhance knowledge of COVID-19 symptoms. These interventions aim to improve health literacy and encourage timely utilization of healthcare in vulnerable populations.
2. Literature Review
The literature on healthcare-seeking behavior during the COVID-19 pandemic highlights various factors influencing individuals' decisions to seek or avoid medical care. This section synthesizes key studies that examine the impact of COVID-19 on healthcare utilization in different regions and populations. The studies are summarized in Table 1, providing a comprehensive overview of their objectives, methodologies, countries of focus, and key findings. This table aims to present a clear comparison of the literature, facilitating the identification of common themes and gaps in existing research.
3. Materials and Methods
3.1. Data
This study utilizes data from the first round of the "COVID-19 Shocks in Rural India" survey, conducted by the World Bank in collaboration with IDinsight, Ministry of Rural Development (India) and the Development Data Lab (DDL). Data collection took place between 5-10, May 2020 in six Indian states: Jharkhand, Rajasthan, Uttar Pradesh, Andhra Pradesh, Bihar, and Madhya Pradesh. The survey employed a computer-assisted telephone interview (CATI) methodology to ensure data collection despite mobility restrictions during the pandemic. The dataset consists of 4,550 observations and 234 variables, covering a wide range of topics such as health, migration, labor and income, agriculture, relief, and consumption. Sampling was conducted using a multi-stage cluster design, drawing from various pre-existing survey frames, including voter rolls and frontline health worker registries, ensuring state-representative rural samples. To improve the reliability and representativeness of the dataset, post-stratified weights were applied, correcting for potential biases in caste and religious representation using 2011 Census data. The survey questions were structured according to predefined modules, ensuring a systematic approach to data collection across states. The questionnaire followed a modular design covering health, migration, labor, agriculture, and relief access, allowing consistency in thematic data collection. Missing data was addressed through multiple imputation techniques, where feasible, and topcoding was applied to select indicators to mitigate the influence of extreme values. Robust statistical controls were incorporated in the analysis, adjusting for key socio-demographic factors such as gender, age, education, household size, and consumption level. The final analytical sample excludes observations with missing values on primary variables of interest, ensuring a robust and consistent dataset to evaluate the impact of knowledge about COVID-19 symptom on healthcare-seeking behavior in rural India. Hence, after removing missing variables, the final sample consisted of 1,950 observations, representing 42.85% of the valid responses from 4,550 observations. More than half of the observations were dropped, which could have affected the efficiency and overall representativeness of the results. To assess whether this might have occurred, we checked the distribution of the data before and after dropping the observations with missing values but observed no significant difference in distribution (mean and standard deviation) that could have materially affected our results (see Table A1 in the Appendix A). Thus, the final data of this study appeared to be sufficient and representative enough to provide unbiased results
3.2. Variables
The study's dependent variable is a dichotomous measure named "health facility visit”, based on a module question related to health that ask, “In the last three months, have you visited a health facility or camp for yourself (or for your children)?” The variable is defined with a "Yes" (1) for those who affirmed the visit and a "No" (0) for those who did not. The sample for this study included 4,550 respondents who provided either a "Yes" or "No" answer to this question.
The main explanatory variable is derived from a health-related module question: "What symptoms of coronavirus/COVID-19 have you heard about?" Respondents could select from a list of 12 symptoms: fever, cough, tiredness, difficulty breathing, muscle pain/body aches, loss of appetite, sore throat, diarrhea, nausea, nasal and throat congestion, loss of smell and taste, and others. Each symptom was coded as a binary variable in the original dataset. The intended approach was to create a composite measure called "COVID-19 symptoms knowledge," where each symptom known by the respondent would be assigned a value of 1, which would result in a composite score ranging from 0 to 12. However, before proceeding with the composite measure, it was necessary to assess the internal consistency of the binary responses. Cronbach's alpha was calculated to determine whether the items (symptoms) consistently measured the same construct. The resulting scale reliability coefficient was 0.5963, which is below the acceptable benchmark of 0.7. This low alpha suggests that the items may not be strongly correlated with each other or consistently measure a single underlying construct. Therefore, the symptoms may not form a reliable composite measure of knowledge of symptoms of COVID-19. The results of the Cronbach’s Alpha test are presented in Table 2.
To address the issue of weak test scale, the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was calculated to assess the suitability of the data for factor analysis. The overall KMO value was 0.679, indicating a marginally adequate sample for the factor analysis. The individual KMO values for each variable are presented in Table 3.
Given the results of the KMO test, exploratory factor analysis (EFA) was conducted using principal factors to examine whether the symptoms naturally clustered into factors. This analysis aimed to identify whether different symptoms were grouped together to form separate factors, guiding the decision to use the full set of symptoms, a subset, or multiple factors in the analysis. Utilizing EFA, we aimed to ensure that the explanatory variable 'COVID-19 symptoms knowledge' was based on a reliable and valid representation of respondents' awareness of COVID-19 symptoms. The results of the EFA identified a factor with an eigenvalue greater than 1 (1.51692), which explained most of the variance of the symptoms. The factor loadings for each symptom are presented in Table 4.
The results of the EFA indicate that Factor 1 largely explains symptoms such as fever, cough, tiredness, difficulty in breathing, and muscle or body pain, with factor loadings ranging from 0.34 to 0.68. These symptoms are more closely related to the respiratory and general symptoms of COVID-19. Given the stronger correlations of these symptoms, we created a new composite variable, "COVID-19 respiratory and general symptoms knowledge," using only the most strongly correlated symptoms (fever, cough, difficulty in breathing, muscle pain/body aches, and tiredness) from Factor 1. To create the new composite variable, each of the five selected symptoms was coded as a binary variable, with a value of 1 if the respondent was aware of the symptom and 0 otherwise. The composite score was then calculated by adding the binary scores for the selected symptoms for each respondent. This resulted in a composite score ranging from 0 to 5, representing the total number of symptoms the respondent was aware of. This approach provides a cleaner and more reliable measure of the knowledge of COVID-19 symptoms knowledge by focusing on the most strongly correlated respiratory and general symptoms.
Finally, we control demographic and socioeconomic factors to isolate the independent impact of knowledge of respiratory and general symptoms of COVID-19 on the visit to the health facility. Our study used several control variables: female gender, age, age squared, education, state of residency, household size, government transfer, monthly consumption expenditure, and few interaction terms. Table 5 provides detailed definitions and measurements of the dependent, independent, and control variables.
3.3. Descriptive Statistics
According to the descriptive statistics presented in Table 6, approximately 34.15% of the respondents visited a health facility within the last three months, and on average, the respondents reported having knowledge of nearly 2 out of 5 forms of COVID-19 respiratory or general symptoms. Furthermore, the average respondent was 38.09 years old, and the females constituted 10% of the sample. The level of education varied, with 28.36% having received higher education (high school and more) and 16% not having attended school. The average household size was 6.29 members, and approximately 64% of the respondents lived in the rich states of Andhra Pradesh, Madhya Pradesh, Rajasthan, or Uttar Pradesh. The average household expenditure was approximately Rs.10,471.34 and the government transfer recipients comprised 60% of the respondents. Regarding the interaction variables, the mean values are as follows: the interaction of household size and government transfer is 3.84, the knowledge of COVID-19 respiratory and general symptoms and female is 0.16, and the age and high school education or more is 9.82.
To compare the average values of the two datasets and determine whether they came from the same population, ANOVA and t-tests were conducted for the probability of visiting a health facility, distributed by age group, rich states, and without schooling status. The results of these tests are shown in Table 7 and Table 8, along with the test statistics and the significance levels.
Table 7 presents the distribution of visits to health facilities in five main age groups. While age is often considered a significant factor in determining health-seeking behavior, our results of the ANOVA test indicate otherwise. We observe that age does not significantly influence whether individuals visit health facilities. This finding suggests that age alone is not a strong predictor of health facility visits and may need to be combined with other demographic variables to demonstrate a more pronounced effect.
Table 8 shows that, at the 5% significance level, the percentage of individuals visiting health facilities is significantly higher in rich states compared to other states. This could potentially be due to better access to healthcare resources and financial ability. Similarly, a noticeable difference in no schooling with health facility visitation can be observed at 10% significance. More specifically, the percentage of individuals without schooling status is less likely to visit health facilities, as compared to those who have attended school. This may imply that individuals without formal education might face barriers to accessing health facilities or may have less awareness of the importance of seeking medical care.
3.4. Methods
We employed probit regression to investigate the association between the knowledge of respiratory and general symptoms of COVID-19 and visits to health facility. Probit regression was particularly suitable for this study because it models binary outcomes by estimating the probability of an event (e.g., the likelihood of visiting a health facility) under the assumption of a normally distributed latent variable. Furthermore, our choice of the probit model is based on its wide acceptance in health studies [49,50,51,52]. In Lal et al. [53], the probit model was used to explain the association between financial literacy and health-seeking behaviors, such as health checkup. Given these precedents, the use of probit regression in this context is both plausible and well-supported, allowing us to effectively analyze the relationship between the knowledge of COVID-19 symptoms and visits to the health facility. The econometric model of our analysis is stated in Equation 1.
where indicates the health facility visit behavior of the th respondent, represents the respondents COVID-19 respiratory and general symptoms knowledge, is a vector of the respondents’ demographic and socioeconomic characteristics, and is the error term.
We created three models for Equation 1, each with a distinct control variable. We provided an example of our model requirements for Eq. (1) below. Equations (2), (3), and (4), represent Models 1, 2, and 3, respectively.
To identify and correct for high intercorrelations among two or more independent variables in all models, we conducted correlation and multicollinearity tests. For example, individuals with a high level of education may have high knowledge on COVID-19 respiratory and general symptoms, or those with a high consumption expenditure may have greater access to healthcare information and resources. By conducting these tests, we ensured that our models did not suffer from multicollinearity, which could potentially bias the results and affect the reliability of our findings. The Correlation Matrix and the Variance Inflation Test (VIF) are presented in Table 9 and Table 10.
The correlation matrix revealed a weak relationship between the relative movements of two variables in all models (substantially lower than 0.70). Furthermore, the variance inflation factor tests of the explanatory variables showed an insignificant presence of multicollinearity in all models (less than 10). We also examined the marginal effects of the probit regression results to understand the impact of explanatory variables on the probability of visiting a health facility. By analyzing the marginal effects, we were able to quantify the change in probability associated with variations in each independent variable, providing a more intuitive interpretation of the probit regression coefficients.
Although potential endogeneity is a concern in terms of omitted variable bias and reverse causality, we believe that this is not going to affect our results, for several reasons. First, we included important factors that might influence individuals’ health facility visit behavior. These comprise various socio-economic and demographic characteristics of individuals that are widely used in various health-economics studies to explain phenomena. Second, the theoretical background discussed in the introduction section and the literature review section lay the basis for how COVID-19 respiratory and general symptoms knowledge could influence health facility visit behavior and why reverse causality is less likely to occur.
Additionally, we conducted a robustness check using Maximum Likelihood Estimation (MLE). This technique is widely used in health-related observational studies and is a standard method for parameter estimation and inference in statistics [54]. The MLE method estimates the parameter values that maximize the likelihood function, ensuring the best fit for the data [55]. MLE possesses many optimal properties, including sufficiency (providing complete information about the parameters), consistency (yielding asymptotically correct results), efficiency (achieving minimum variance), and asymptotic normality [54,55]. By employing MLE, we enhanced the robustness of our analysis, ensuring that our findings on the association between knowledge of respiratory and general symptoms of COVID-19 and visits to the health facilities are reliable and well-supported.
4. Results
In an effort to understand the relationship between the visits to the health facility and the knowledge of respiratory and general symptoms of COVID-19, we conducted a cross-sectional probit regression analysis, the results of which are presented in Table 11. The findings indicate that the knowledge of respiratory and general symptoms of COVID-19 significantly predicts the visits to the health facility in all models. This is evident from the positive coefficients, which are significant at the 10% level in Model 1 and Models 3, and 5% level in Model 2, suggesting that respondents with higher levels of knowledge of the symptoms of COVID-19 are more inclined to visit health facilities during the pandemic. The positive association between the knowledge of COVID-19 symptoms and the visit to the health facility underscores the importance of health education and awareness campaigns in rural areas, not only to increase the health literacy, but also to make a timely visit to the healthcare facilities, which is crucial for early diagnosis and effective management of the disease,
Regarding demographic variables, it is observed that age has a non-linear relationship with health facility visits, initially decreasing the likelihood of visits with increasing age, but after a certain point, the likelihood of visiting a health facility increases as age continues to rise, which is only significant in Model 3 at the 10% level. Female respondents are more prone to visit health facilities during the pandemic, and the results are consistent across Model 2 and Model 3 at 10% and 1% significance level, respectively. As for the negative 10% significance level interaction term between female and COVID-19 symptoms knowledge in Model 3, it suggests that for females, higher knowledge of COVID-19 symptoms is associated with a reduced likelihood of visiting health facilities compared to males. The interaction term of age and higher level of schooling do not exhibit a significant association to the visit to health facility.
When considering socio-economic variables, it is observed that those individuals from the rich states and who have a high household consumption expenditure have a positive association with health facility visits at 1% and 5%, respectively. Additionally, the positive 10% significance level interaction term between household size and government transfer in Model 3 suggests that for a respondent with a higher household size, getting a government transfer is more likely to contribute to a health facility visit during the pandemic. However, those respondents who did not attend school are less likely to visit a health facility moderated at a 10% significance level. Variables such as high school or more, household size, and government transfer do not independently have a pronounced effect on health facility visits, indicating that their influence may be more nuanced and potentially dependent on interactions with other factors. This interpretation highlights the complexity of health-seeking behavior and the need to consider multiple dimensions and interactions in the analysis.
After running the probit regression, we also conducted a marginal effects estimation to assess the probability of visiting a health facility based on the main explanatory variable, the knowledge of the symptoms of COVID-19, along with other control variables. The main results indicate that knowledge of COVID-19 symptoms knowledge significantly increases the probability of visiting a health facility. Specifically, a one-unit increase in knowledge is associated with a 1.5% increase in the probability of visiting a health facility in Model 1, a 2.0% increase in Model 2, and a 1.5% increase in Model 3. These effects are statistically significant at the 5% level in Models 1 and 2, and at the 10% level in Model 3. This positive association underscores the importance of health education and awareness campaigns in promoting health-seeking behavior, particularly during the pandemic. The results of the Marginal Effects estimation are presented in Table 12.
To further validate our earlier findings, we conducted a robustness test using Maximum Likelihood Estimation (MLE) to examine the relationship between the knowledge of respiratory and general symptoms of COVID-19 and the behavior of visit to the health facility among the respondents. The results, as presented in Table 13, reaffirm the importance of knowledge of COV1D-19 symptoms in predicting the visit to the health facility in all models. Additionally, the signs and significance levels of all other control variables in the MLE models are consistent with the probit regression results. This consistency further reinforces the robustness of our findings, providing confidence in the reliability of the estimated effects.
5. Discussion
Our probit regression analysis provides robust evidence that individuals with greater knowledge of COVID-19 respiratory and general symptoms are significantly more likely to visit health facilities during the pandemic. Furthermore, as part of robustness checks, we employed Maximum Likelihood Estimation, and this alternative measure yielded consistent results, reinforcing the association between knowledge of COVID-19 symptoms and increased likelihood of visiting a health facility. This consistency across different measures confirms the robustness of our findings and confirms our hypothesis, underscoring the critical role of health education in promoting proactive health-seeking behavior in rural areas. Additionally, this empirical validation substantiates the behavioral health theory of the Health Belief Model proposed by Rosenstock [56] , highlighting the importance of perceived knowledge and awareness in motivating individuals to take preventive health actions. The results emphasize that when individuals recognize the severity and susceptibility associated with COVID-19 and understand the benefits of early diagnosis and treatment, they are more inclined to engage in health-seeking behavior, such as visiting healthcare facilities.
This finding resonates with the broader context of our study, particularly within the rural Indian economy, which underscores the significance of understanding how the knowledge of the basic symptoms of COVID-19, driven by targeted health education, awareness campaigns, and the demographic and socioeconomic background of the individual, manifests in health-promoting behavior during times of crisis. During the COVID-19 pandemic, rural India faced unique challenges, including limited healthcare infrastructure and accessibility. The Government of India responded by increasing COVID-19 testing facilities, treatment options, vaccination drives, developing new health infrastructure, as well as boosting the already existing health infrastructure in the villages [57,58,59]. Through these initiatives, the issue of limited health facilities and access was significantly diminished in rural areas [60,61,62]. However, a critical challenge remained: the lack of knowledge about COVID-19 symptoms among rural populations [63,64,65]. Many rural residents, unaware of the symptoms of COVID-19, often mistook them for common illnesses and did not seek medical attention [66]. This lack of awareness led to delays in diagnosis and treatment, exacerbating the spread of the virus. Conversely, individuals in rural India with higher literacy levels or better knowledge of COVID-19 symptoms were more likely to have appropriate behavior and proper practices in the population [67,68], including visiting health facilities for diagnosis and treatment. This aligns with existing literature that broadly links health awareness or literacy with increased and timely medical intervention, reducing disease burden and improving health outcomes [69,70]. By bridging the knowledge gap through targeted education and awareness campaigns, rural populations can be empowered to make informed health decisions, such as visiting health facilities, ultimately strengthening community resilience in the face of public health crises [71]
In addition to focusing on the association between the knowledge of COVID-19 symptoms and the behavior of the visit to the health facility, we determine probability of health facility visit based on other demographic factors such as age, gender, and few interaction variables. Our analysis indicates that age exhibits a non-linear relationship with health facility visits. Initially, as age increases, the probability of visiting a health facility decreases. However, beyond a certain age threshold, the likelihood of seeking medical attention begins to increase. These findings are supported by studies that demonstrate a significant and pronounced non-linear relationship between age and health outcomes [72]. Additionally, research shows that patient age is linearly and positively correlated with satisfaction with healthcare before 65 years and negatively thereafter, suggesting a non-linear influence of age on health-seeking behavior [73]. Furthermore, our findings show that females are more likely to visit health facilities during the pandemic. Research suggests that women are generally more proactive in seeking healthcare services due to their role as primary caregivers and their holistic approach to health [74,75]. However, the interaction term between the knowledge of the COVID-19 symptoms and female suggests that females with a higher knowledge of the symptoms of COVID-19 are less likely to visit health facilities compared to males. This counterintuitive finding may be explained by the increased burden of caregiving responsibilities and household duties during the pandemic, which could limit women's ability to seek healthcare despite their knowledge [76,77]. Additionally, women may prioritize the health of their family members over their own, leading to reduced personal healthcare visits [78,79]
Among the socioeconomic variables, our analysis revealed that individuals from wealthier states like Madhya Pradesh, Andhra Pradesh, Rajasthan, and Uttar Pradesh, as well as those with higher monthly expenditures, are more likely to visit health facilities during the pandemic. This trend is attributed to their financial capacity for healthcare [80,81], superior healthcare infrastructure [82], better health and financial literacy [83,84], and the likelihood of having health insurance [85]. Additionally, higher monthly consumption expenditure allows prioritizing health needs [86], including visiting health facilities during the pandemic and getting specialized and expedited treatment. Consequently, these factors collectively increase the utilization of health facilities and improve health outcomes. Moreover, the interaction between household size and government transfer suggests that larger households benefit more from government transfers, as these transfers help alleviate financial constraints, making it easier for them to afford healthcare services [87,88,89]. Additionally, government transfers can help offset the economic impact of the pandemic, allowing larger households to prioritize healthcare expenditures and access necessary medical services [90]. Lastly, our analysis found that individuals with no educational background are less likely to visit health facilities during the pandemic. Lack of education correlates with lower health literacy, making it difficult to understand the importance of seeking medical care and navigating the healthcare system [91,92]. Limited access to information about healthcare services and government programs further hinders their ability to seek care. Additionally, lower educational attainment is associated with lower socioeconomic status, creating financial barriers to accessing healthcare [93,94].
Although this study provides valuable insights, it has some limitations. First, our analysis was based on probability of health facility visit data from a single wave of 2020 rural India survey, restricting the depth of longitudinal evidence available on health facility visit behavior. Therefore, future research should employ broader data collection methods and longitudinal studies, exploring how visit behavior in health facility evolves among individuals with higher levels of COVID-19 symptoms knowledge, as the pandemic situation gradually improves. Second, our study does not include certain critical variables, such as household income, household assets, marital status, and psychological variables such as risk aversion, myopic thinking, impatience/ impulsiveness, as questions involving these variables were not included in the questionnaire. These variables would have provided a more comprehensive understanding of the multifaceted factors that contribute to health-seeking behavior from the psychological and financially dynamic family setup viewpoint. Third, the data for this study were collected from only six states in rural India, which may limit the generalizability of the findings to other states not included in the sample. Lastly, this research did not establish a causal relationship between our primary independent variable (knowledge of COVID-19 symptoms) and the dependent variable (health facility visit) due to the cross-sectional nature of the study. However, the goal of this study was not to determine causality between the independent and dependent variables; rather, we aimed to examine if the primary explanatory variable predicts health facility visit behavior during the pandemic in rural India. Although there are limitations, the study offers valuable insights into COVID-19-induced healthcare visits in rural India. It sets the groundwork for future research to address these limitations and improve our understanding of healthcare-seeking behaviors during public health crises.
6. Conclusions
Drawing on behavioral health theories such as the Health Belief Model, this study is a pioneer in its area by focusing in-depth on knowledge of COVID-19 symptoms as an important predictor of health facility visits. It provides empirical evidence suggesting that people with higher knowledge of COVID-19 symptoms are more likely to engage in health facility visit behavior during crises in rural India. This can be explained within the four constructs of the Health Belief Model. Firstly, respondents with knowledge of COVID-19 symptoms are more likely to perceive themselves as susceptible to the virus, aligning with the perceived susceptibility construct of the Health Belief Model. This heightened awareness increases their likelihood of seeking medical attention, as they believe they are at risk. Secondly, with a thorough understanding of COVID-19 symptoms, the respondents might perceive the potential health consequences of contracting the virus as severe, which aligns with the perceived severity construct. This belief can lead them to seek immediate medical care to avoid severe outcomes. Thirdly, knowledgeable respondents may recognize the benefits of seeking early medical intervention, corresponding to the perceived benefits construct. They understand that early detection and treatment can improve health outcomes, which motivates them to utilize healthcare facilities. Lastly, while there may be potential barriers to accessing healthcare, such as financial constraints and travel difficulties, the urgency driven by their knowledge of symptoms might help respondents overcome these barriers, aligning with the perceived barriers construct. Their heightened concern and perceived severity of the situation can outweigh these obstacles, leading to increased healthcare utilization. By connecting these findings to the constructs of the Health Belief Model, the study provides a deeper understanding of the behavioral and cognitive factors that influence visits to health facilities during the pandemic. This strengthens the theoretical foundation of the research and highlights the practical implications of improving health literacy. Among the control variables, certain demographic and socioeconomic characteristics, namely age, age squared, female gender, interaction term between female and COVID-19 symptoms knowledge, rich states, higher household consumption expenditure, interaction term between household size and government transfer and no schooling significantly affected health facility visit behavior during the pandemic. This accentuates the multifaceted nature of respondents’ health decision-making processes, highlighting the importance of considering a wide range of control variables to effectively understand and promote health seeking behaviors, such as visit to the health facility during the outbreaks, for early diagnosis and treatment.
The findings of this study underscore the critical importance of health literacy for individuals in rural India. Knowledge of symptoms of COVID-19 directly influences the likelihood of seeking prompt medical care, which can improve health outcomes and reduce the spread of the virus. Rural residents should prioritize staying informed about health issues and understanding symptoms to make proactive decisions about their health in case of any outbreaks. This emphasizes the need for accessible health education programs that cater to various levels of literacy and cultural contexts within rural communities to empower individuals to take charge of their health. For government bodies, the study highlights the crucial role of public health education in managing and mitigating health crises in rural India. Governments should invest in widespread health literacy programs, especially targeting rural areas, to ensure that populations are well-informed about symptoms and the importance of early medical intervention. While health literacy programs undoubtedly boost the general awareness of symptoms and preventative measures for any outbreaks, for this knowledge-driven behavior to translate into actual healthcare visits, it is crucial to also reduce barriers to accessing healthcare. Thus, policy measures should focus on providing affordable healthcare services, improving transportation infrastructure, and increasing the availability of medical facilities in remote areas. Additionally, governments can collaborate with local organizations and community leaders to tailor health education initiatives to the specific needs and challenges of different rural communities. Researchers can build upon this study by exploring the long-term impact of health literacy, using COVID-19 symptoms knowledge or any other relevant variable as a proxy, on healthcare-seeking behavior and health outcomes in rural India. Future research should consider incorporating a broader range of variables, such as household income and assets, marital status, and psychological factors, as well as including a broader geographic range to provide a more comprehensive understanding of the determinants of visits to health facilities, as well as to enhance the representativeness of the results. Longitudinal studies could provide deeper insights into how knowledge of COVID-19 symptoms evolves and affects behavior over time. Researchers should also examine the effectiveness of various health education strategies in different cultural and socioeconomic contexts within rural India to identify the most impactful approaches to improving health literacy. By addressing these implications, individuals, governments, and researchers can work together to improve health literacy, reduce health disparities, and improve public health outcomes in rural India.
Author Contributions
Conceptualization, S.L. and Y.K.; Methodology, S.L., Y.K., N.C., R.C. and R.S.; Software, S.L.; Validation, S.L., Y.K. and R.S.; Formal Analysis, S.L., N.C., and R.C.; Investigation, S.L.; Resources, Y.K.; R.S., N.C and R.C.; Data Curation, S.L.; Writing—Original Draft Preparation, S.L., N.C., and R.C.; Writing—Review and Editing, Y.K. and R.S.; Visualization, S.L.; Supervision, Y.K.; Project Administration, S.L. and Y.K.; Funding Acquisition, Y.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The article processing charge (APC) was waived by COVID-MDPI.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
Data are available upon request.
Acknowledgments
We would like to express our gratitude to COVID-MDPI for waiving the article processing charge (APC) for this manuscript. Their support has greatly facilitated the publication of this research.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HBM | Health Belief Model |
| MLE | Maximum Likelihood Estimation |
| COVID-19 | Coronavirus Disease of 2019 |
Appendix A

Table A1.
Comparison of sample distribution before and after dropping missing observations
| Variable | Before | After | ||
|---|---|---|---|---|
| Mean | Std. Dev. | Mean | Std.Dev. | |
| Health facility visit | 0.3242 | 0.4682 | 0.3415 | 0.4743 |
| COVID-19 respiratory and general symptoms knowledge | 1.8309 | 1.3659 | 1.8969 | 1.3519 |
| Age | 37.7387 | 13.1062 | 38.0872 | 12.8127 |
| Age squared | 1595.9390 | 1130.4550 | 1614.715 | 1104.909 |
| Female | 0.1185 | 0.3232 | 0.1000 | 0.3001 |
| Rich state | 0.6978 | 0.4593 | 0.6354 | 0.4814 |
| High school or more | 0.3031 | 0.4597 | 0.2836 | 0.4509 |
| No school | 0.1424 | 0.3495 | 0.1600 | 0.3667 |
| Household size | 6.4523 | 3.2521 | 6.2882 | 2.8031 |
| Government transfer | 0.5911 | 0.4917 | 0.6000 | 0.4900 |
| Household consumption expenditure | ₹10070.54 | ₹10896.31 | ₹10,471.34 | ₹11,465.25 |
| Inter_HS> | 3.8581 | 4.0011 | 3.8431 | 3.8214 |
| Inter_Fem&CovidRespGen | 0.1764 | 0.6803 | 0.1615 | 0.6455 |
| Inter_Age&HighSch | 10.4247 | 17.2461 | 9.8236 | 17.0400 |
References
- Filip, R. , Gheorghita Puscaselu, R., Anchidin-Norocel, L., Dimian, M., & Savage, W. K. (2022). Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. In Journal of Personalized Medicine (Vol. 12, Issue 8). MDPI. [CrossRef]
- Ali, J. , Singh, S., & Khan, W. Health awareness of rural households towards COVID-19 pandemic in India: Evidence from Rural Impact Survey of the World Bank. Journal of Public Affairs 2022, e2819. [Google Scholar] [CrossRef]
- Zhang, Q. , Feng, S., Wong, I. O. L., Ip, D. K. M., Cowling, B. J., & Lau, E. H. Y. A population-based study on healthcare-seeking behaviour of persons with symptoms of respiratory and gastrointestinal-related infections in Hong Kong. BMC Public Health 2020, 20. [Google Scholar] [CrossRef]
- Splinter, M. J. , Velek, P., Kieboom, B. C. T., Ikram, M. A., de Schepper, E., Ikram, M. K., & Licher, S. Healthcare avoidance during the early stages of the COVID-19 pandemic and all-cause mortality: a longitudinal community-based study. British Journal of General Practice 2023, BJGP.2023.0637. [Google Scholar] [CrossRef]
- Huang, W. L. , Liao, S. L., Huang, H. L., Tsai, P. J., Huang, H. H., Lu, C. Y., & Ho, W. S. Impact of post-COVID-19 changes in outpatient chronic patients’ healthcare-seeking behaviors on medical utilization and health outcomes. Health Economics Review 2024, 14. [Google Scholar] [CrossRef]
- Oduro, M. S. , Peprah, P., Morgan, A. K., & Agyemang-Duah, W. Staying in or out? COVID-19-induced healthcare utilization avoidance and associated socio-demographic factors in rural India. BMC Public Health 2023, 23. [Google Scholar] [CrossRef]
- Pujolar, G. Oliver-Anglès, A., Vargas, I., & Vázquez, M. L. (2022). Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. In International Journal of Environmental Research and Public Health (Vol. 19). MDPI. [CrossRef]
- Bastani, P. , Mohammadpour, M., Samadbeik, M., Bastani, M., Rossi-Fedele, G., & Balasubramanian, M. Factors influencing access and utilization of health services among older people during the COVID − 19 pandemic: a scoping review. Archives of Public Health 2021, 79. [Google Scholar] [CrossRef]
- Zhang, J. , Xu, Z., Wei, X., Fu, Y., Zhu, Z., Wang, Q., Wang, Q., Liu, Q., Guo, J., Hao, Y., & Yang, L. Analysis of health service utilization and influencing factors due to COVID-19 in Beijing: a large cross-sectional survey. Health Research Policy and Systems 2024, 22. [Google Scholar] [CrossRef]
- Rezaei, Z. , Lotfi, F., Bayati, M., & Kavosi, Z. The effect of Covid-19 pandemic on healthcare utilization in public vs private centers in Iran: a multiple group interrupted time-series analysis. BMC Health Services Research 2023, 23. [Google Scholar] [CrossRef]
- Hung, K. K. C. , Walline, J. H., Chan, E. Y. Y., Huang, Z., Lo, E. S. K., Yeoh, E. K., & Graham, C. A. Health Service Utilization in Hong Kong During the COVID-19 Pandemic – A Cross-sectional Public Survey. International Journal of Health Policy and Management 2022, 11, 508–513. [Google Scholar] [CrossRef]
- Splinter, M. J. , Velek, P., Kamran Ikram, M., Kieboom, B. C. T., Peeters, R. P., Bindels, P. J. E., Arfan Ikram, M., Wolters, F. J., Leening, M. J. G., de Schepper, E. I. T., & Licher, S. Prevalence and determinants of healthcare avoidance during the COVID-19 pandemic: A population-based cross-sectional study. PLoS Medicine 2021, 18. [Google Scholar] [CrossRef]
- Soares, P. , Leite, A., Esteves, S., Gama, A., Laires, P. A., Moniz, M., Pedro, A. R., Santos, C. M., Goes, A. R., Nunes, C., & Dias, S. Factors associated with the patient’s decision to avoid healthcare during the COVID-19 pandemic. International Journal of Environmental Research and Public Health 2021, 18. [Google Scholar] [CrossRef]
- Sahakyan, S. , Muradyan, D., Giloyan, A., & Harutyunyan, T. Factors associated with delay or avoidance of medical care during the COVID-19 pandemic in Armenia: results from a nationwide survey. BMC Health Services Research 2024, 24. [Google Scholar] [CrossRef]
- Czeisler, M. É. , Marynak, K., Clarke, K. E. N., Salah, Z., Shakya, I., Thierry, J. M., Ali, N., McMillan, H., Wiley, J. F., Weaver, M. D., Czeisler, C. A., Rajaratnam, S. M. W., & Howard, M. E. Delay or Avoidance of Medical Care Because of COVID-19–Related Concerns — United States, June 2020. MMWR. Morbidity and Mortality Weekly Report 2020, 69, 1250–1257. [Google Scholar] [CrossRef] [PubMed]
- Islam, M. I. , Freeman, J., Chadwick, V., & Martiniuk, A. Healthcare Avoidance before and during the COVID-19 Pandemic among Australian Youth: A Longitudinal Study. Healthcare (Switzerland) 2022, 10. [Google Scholar] [CrossRef]
- Arnetz, B. B. , Goetz, C., vanSchagen, J., Baer, W., Smith, S., & Arnetz, J. E. Patient-reported factors associated with avoidance of in-person care during the COVID-19 pandemic: Results from a national survey. PLoS ONE 2022, 17. [Google Scholar] [CrossRef]
- Kang, L. , Li, C., & Du, H. Predictors of Medical Care Delay or Avoidance Among Chinese Adults During the COVID-19 Pandemic. Patient Preference and Adherence 2023, 17, 3067–3080. [Google Scholar] [CrossRef]
- Lee, M. , & You, M. Avoidance of healthcare utilization in south korea during the coronavirus disease 2019 (Covid-19) pandemic. International Journal of Environmental Research and Public Health 2021, 18. [Google Scholar] [CrossRef]
- Lopes, S. , Soares, P., Gama, A., Pedro, A. R., Moniz, M., Laires, P., Goes, A. R., Nunes, C., & Dias, S. Association between perception of COVID-19 risk, confidence in health services and avoidance of emergency department visits: results from a community-based survey in Portugal. BMJ Open 2022, 12. [Google Scholar] [CrossRef]
- Smolić, Š. , Fabijančić, M., & Blaževski, N. How did fear of COVID-19 affect access to healthcare in Central and Eastern Europe? Findings from populations aged 50 or older after the outbreak. Eastern European Economics 2023, 61, 571–590. [Google Scholar] [CrossRef]
- Farrer, L. M. , Batterham, P. J., Gulliver, A., Morse, A., Calear, A. L., McCallum, S., Banfield, M., Shou, Y., Newman, E., & Dawel, A. The Factors Associated With Telehealth Use and Avoidance During the COVID-19 Pandemic: Longitudinal Survey. Journal of Medical Internet Research 2023, 25. [Google Scholar] [CrossRef]
- Wang, Z. , Tang, Y., Cui, Y., Guan, H., Cui, X., Liu, Y., Liu, Y., Kang, Z., Wu, Q., Hao, Y., & Liu, C. Delay in seeking health care from community residents during a time with low prevalence of COVID-19: A cross-sectional national survey in China. Frontiers in Public Health 2023, 11. [Google Scholar] [CrossRef]
- Pung, P. (2021, June 4). FMC Raises COVID-19 Awareness in Rural India. Https://Www.Fmc.Com/En/Articles/Fmc-Raises-Covid-19-Awareness-Rural-India?Form=MG0AV3.
- Biswas, P. (2020, July 1). Knowledge gap on Covid-19 exists in rural communities: UoH study - Times of India. Https://Timesofindia.Indiatimes.Com/Education/News/Knowledge-Gap-on-Covid-19-Exists-in-Rural-Communities-Uoh-Study/Articleshow/76731518.Cms?Form=MG0AV3.
- Passi, R. , Kaur, M., Lakshmi, P. V. M., Cheng, C., Hawkins, M., & Osborne, R. H. Health literacy strengths and challenges among residents of a resource-poor village in rural India: Epidemiological and cluster analyses. PLOS Global Public Health 2023, 3. [Google Scholar] [CrossRef]
- Player, J. (2019, December). Healthcare Access in Rural Communities in India - Ballard Brief. Https://Ballardbrief.Byu.Edu/Issue-Briefs/Healthcare-Access-in-Rural-Communities-in-India?Form=MG0AV3.
- Murakami, K. , Kuriyama, S., & Hashimoto, H. General health literacy, COVID-19-related health literacy, and protective behaviors: evidence from a population-based study in Japan. Frontiers in Public Health 2023, 11. [Google Scholar] [CrossRef]
- Carter, P. , Megnin-Viggars, O., & Rubin, G. J. (2021). What Factors Influence Symptom Reporting and Access to Healthcare During an Emerging Infectious Disease Outbreak? A Rapid Review of the Evidence. In Health Security (Vol. 19, pp. 353–363). Mary Ann Liebert Inc. [CrossRef]
- Rosenstock, I. M. Historical Origins of the Health Belief Model. Health Education & Behavior 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Jones, C. L. , Jensen, J. D., Scherr, C. L., Brown, N. R., Christy, K., & Weaver, J. The Health Belief Model as an Explanatory Framework in Communication Research: Exploring Parallel, Serial, and Moderated Mediation. Health Communication 2015, 30, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Agyemang-Duah, W. , & Rosenberg, M. W. Healthcare utilization among informal caregivers of older adults in the Ashanti region of Ghana: a study based on the health belief model. Archives of Public Health 2023, 81. [Google Scholar] [CrossRef]
- Alhalaseh, L. , Fayoumi, H., & Khalil, B. The Health Belief Model in predicting healthcare workers’ intention for influenza vaccine uptake in Jordan. Vaccine 2020, 38, 7372–7378. [Google Scholar] [CrossRef]
- Wong, L. P. , Alias, H., Wong, P. F., Lee, H. Y., & AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Human Vaccines and Immunotherapeutics 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Luquis, R. R. , & Kensinger, W. S. Applying the Health Belief Model to assess prevention services among young adults. International Journal of Health Promotion and Education 2019, 57, 37–47. [Google Scholar] [CrossRef]
- An, S. , Schulz, P. J., & Kang, H. Perceived COVID-19 susceptibility and preventive behaviors: moderating effects of social support in Italy and South Korea. BMC Public Health 2023, 23. [Google Scholar] [CrossRef]
- DeDonno, M. A. , Longo, J., Levy, X., & Morris, J. D. Perceived Susceptibility and Severity of COVID-19 on Prevention Practices, Early in the Pandemic in the State of Florida. Journal of Community Health 2022, 47, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Buehler, A. , Malone, M., & Majerus-Wegerhoff, M. (2006). Patterns of responses to symptoms in rural residents: The Symptom-Action-Time-Line process. In Springer Publishing Company. ASME.
- Janz, N. K. , & Becker, M. H. The Health Belief Model: A Decade Later. Health Education & Behavior 1984, 11, 1–47. [Google Scholar] [CrossRef]
- CDC. (2024, June 13). About COVID-19. Https://Www.Cdc.Gov/Covid/about/Index.Html.
- Watson, S. & Benisek, A. (2024, October 29). GI Symptoms and Coronavirus (COVID-19). Https://Www.Webmd.Com/Covid/Covid19-Digestive-Symptoms?Form=MG0AV3.
- Mlynaryk, N. (2022, June 16). COVID-19 on the Brain: Neurological Symptoms Persist in Majority of Long-Haulers. Https://Health.Ucsd.Edu/News/Press-Releases/2022-06-15-Covid-19-on-the-Brain-Neurological-Symptoms-Persist-in-Majority-of-Long-Haulers/?Form=mg0av3.
- Mayo Clinic. (2024, November 27). COVID-19, cold, allergies and the flu: What are the differences? Https://Www.Mayoclinic.Org/Diseases-Conditions/Coronavirus/in-Depth/Covid-19-Cold-Flu-and-Allergies-Differences/Art-20503981?Form=MG0AV3.
- Gilliland, M. J. , Phillips, M. M., Raczynski, J. M., Smith, D. E., Cornell, C. E., & Bittner, V. (1999). Health-Care-Seeking Behaviors. In Handbook of Health Promotion and Disease Prevention (pp. 95–121). Springer US. [CrossRef]
- Hou, Y. , Li, W., Li, S., Chen, L., An, J., & Lu, S. Enhancing healthcare utilization and reducing preventable hospitalizations: exploring the healthcare-seeking propensity of patients with non-communicable diseases in Rural China. BMC Public Health 2025, 25, 323. [Google Scholar] [CrossRef]
- Martin, R. , & Leventhal, H. (2008). Symptom perception and health care-seeking behavior. In Handbook of clinical health psychology: Volume 2. Disorders of behavior and health. (pp. 299–328). American Psychological Association. [CrossRef]
- Riegel, B. , de Maria, M., Barbaranelli, C., Matarese, M., Ausili, D., Stromberg, A., Vellone, E., & Jaarsma, T. Symptom Recognition as a Mediator in the Self-Care of Chronic Illness. Frontiers in Public Health 2022, 10. [Google Scholar] [CrossRef]
- Gupta, C. (2025, February 21). Top 10 richest states in India by GDSP and GDP per capita, as of 2024. Https://Indianexpress.Com/Article/Trending/Top-10-Listing/Top-10-Richest-States-in-India-by-Gdsp-and-Gdp-per-Capita-as-of-2024-9601172/.
- Lal, S. , Nguyen, T. X. T., Sulemana, A. S., Khan, M. S. R., & Kadoya, Y. Time Discounting and Hand-Sanitization Behavior: Evidence from Japan. Sustainability (Switzerland) 2023, 15. [Google Scholar] [CrossRef]
- Khan, M. S. R. , Nguyen, T. X. T., Lal, S., Watanapongvanich, S., & Kadoya, Y. Hesitancy towards the Third Dose of COVID-19 Vaccine among the Younger Generation in Japan. International Journal of Environmental Research and Public Health 2022, 19. [Google Scholar] [CrossRef]
- Nguyen, T. X. T. , Lal, S., Abdul-Salam, S., Khan, M. S. R., & Kadoya, Y. Financial Literacy, Financial Education, and Cancer Screening Behavior: Evidence from Japan. International Journal of Environmental Research and Public Health 2022, 19. [Google Scholar] [CrossRef]
- Sulemana, A. S. , Lal, S., Nguyen, T. X. T., Khan, M. S. R., & Kadoya, Y. Pandemic Fatigue in Japan: Factors Affecting the Declining COVID-19 Preventive Measures. Sustainability (Switzerland) 2023, 15. [Google Scholar] [CrossRef]
- Lal, S. , Nguyen, T. X. T., Sulemana, A. S., Khan, M. S. R., & Kadoya, Y. Does financial literacy influence preventive health check-up behavior in Japan? a cross-sectional study. BMC Public Health 2022, 22. [Google Scholar] [CrossRef]
- Myung, I. J. Tutorial on maximum likelihood estimation. Journal of Mathematical Psychology 2003, 47, 90–100. [Google Scholar] [CrossRef]
- Miura, K. An Introduction to Maximum Likelihood Estimation and Information Geometry. Interdisciplinary Information Sciences 2011, 17, 155–174. [Google Scholar] [CrossRef]
- Rosenstock, I. M. The Health Belief Model and Preventive Health Behavior. Health Education & Behavior 1977, 2, 354–386. [Google Scholar] [CrossRef]
- Government of India. (2020a). PM to launch High Throughput COVID. Https://Www.Pib.Gov.in/Newsite/PrintRelease.Aspx?Relid=210269&form=MG0AV3.
- WHO. (2020, August 16). How India scaled up its laboratory testing capacity for COVID19. Https://Www.Who.Int/India/News/Feature-Stories/Detail/How-India-Scaled-up-Its-Laboratory-Testing-Capacity-for-Covid19?Form=MG0AV3.
- Government of India. (2020b, July 27). PM launches High Throughput COVID testing facilities at Kolkata, Mumbai and Noida. Https://Pib.Gov.in/PressReleasePage.Aspx?PRID=1641550&form=MG0AV3.
- Ministry of Health and Family Welfare. (2024, July 26). Government of India has taken several initiatives through ‘Whole of Government’ approach during the COVID. Https://Pib.Gov.in/Pressreleaseshare.Aspx?PRID=2037420&form=MG0AV3.
- Rangarajan, R. (2021, July 15). Addressing the gap in diagnostic services in rural India - ET HealthWorld. Https://Health.Economictimes.Indiatimes.Com/News/Diagnostics/Addressing-the-Gap-in-Diagnostic-Services-in-Rural-India/84420975?Form=MG0AV3.
- Sharma, A. (2021, May 16). Focus on awareness, increase testing and more: Centre’s guidelines on COVID management in rural, peri-urban areas. Https://English.Jagran.Com/India/Focus-on-Awareness-Increase-Testing-and-More-Centres-Guidelines-on-Covid-Management-in-Rural-Periurban-Areas-10026754?Form=MG0AV3.
- Kordi, F. , Lakeh, N. M., Pouralizadeh, M., & Maroufizadeh, S. Knowledge and behaviors of prevention of COVID-19 and the related factors in the rural population referred to the health centers: a cross-sectional study. BMC Nursing 2023, 22. [Google Scholar] [CrossRef]
- Naresh, S. J. , Reddy, M. M., Suryanarayana, R., Bhattacharyya, A., & T Kamath, P. B. Awareness, practices, and myths related to coronavirus disease-19 among rural people in Kolar District, South India: A community-based mixed-methods study. Journal of Education and Health Promotion 2022, 11, 57. [Google Scholar] [CrossRef]
- Noronha, R. (2021, May 10). Ground report: How Covid-19 has affected India’s rural areas. Https://Www.Indiatoday.in/Magazine/Cover-Story/Story/20210510-Ground-Report-How-Covid-19-Has-Affected-India-s-Rural-Areas-1796993-2021-05-01.
- Behl, A. (2021, May 13). Lack of awareness, poor enforcement of curbs in rural areas leading to more deaths, allege residents. Https://Www.Hindustantimes.Com/Cities/Gurugram-News/Lack-of-Awareness-Poor-Enforcement-of-Curbs-in-Rural-Areas-Leading-to-More-Deaths-Allege-Residents-101620927291536.Html.
- Joshi, B. N. , Bhavya M K, Prusty, R. K., Tandon, D., Kabra, R., Allagh, K. P., & Khan, S. Knowledge, perception and practices adapted during COVID-19: A qualitative study in a district in Maharashtra, India. The Journal of Community Health Management 2024, 11, 157–164. [Google Scholar] [CrossRef]
- Chaudhary, K. , Dhatrak, A., Shyam Sundar, R. N., & Suresh, S. B. Knowledge, attitudes and practices of rural population towards COVID-19 appropriate behaviour in pandemic situation: a cross-sectional study in central India. International Journal of Community Medicine and Public Health 2022, 9, 4641. [Google Scholar] [CrossRef]
- Gupta, S. , Chakraborty, A., Biswas, R., Baur, B., & Banerjee, R. How effective are health awareness campaigns in India among young citizens? National Journal of Physiology, Pharmacy and Pharmacology 2023, 1. [Google Scholar] [CrossRef]
- Sharma, I. P. , Chaudhry, M., Sharma, D., & Kaiti, R. Mobile health intervention for promotion of eye health literacy. PLOS Global Public Health 2021, 1. [Google Scholar] [CrossRef]
- Khatri, R. B. , Endalamaw, A., Erku, D., Wolka, E., Nigatu, F., Zewdie, A., & Assefa, Y. Preparedness, impacts, and responses of public health emergencies towards health security: qualitative synthesis of evidence. Archives of Public Health 2023, 81. [Google Scholar] [CrossRef]
- Monaghan, C. , de Andrade Moral, R., & Power, J. M. Modelling the Non-linear Associations between Age and Health: Implications for Care. Age and Ageing 2024, 53. [Google Scholar] [CrossRef]
- Moret, L. , Nguyen, J. M., Volteau, C., Falissard, B., Lombrail, P., & Gasquet, I. Evidence of a non-linear influence of patient age on satisfaction with hospital care. International Journal for Quality in Health Care 2007, 19, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Rudoy, J. , & Leis, H. (2020). Females are Discontent but Darn Proactive About Their Health and Healthcare. Https://Www.Oliverwyman.Com/Our-Expertise/Perspectives/Health/2019/Mar/Females-Are-Unhappy-but-Darn-Proactive-about-Their-Health-and-He.Html.
- NeuroLaunch editorial team. (2024, September 22). Health-Seeking Behavior: Factors Influencing Healthcare Decisions and Outcomes. Https://Neurolaunch.Com/Health-Seeking-Behavior/?Form=MG0AV3.
- Pinchoff, J. , Santhya, K. G., White, C., Rampal, S., Acharya, R., & Ngo, T. D. Gender specific differences in COVID-19 knowledge, behavior and health effects among adolescents and young adults in Uttar Pradesh and Bihar, India. PLoS ONE 2020, 15. [Google Scholar] [CrossRef]
- Wenham, C. (2020, September 30). The gendered impact of the Covid-19 crisis and post-crisis period | Think Tank | European Parliament. Https://Www.Europarl.Europa.Eu/Thinktank/En/Document/IPOL_STU(2020)658227.
- Rakotosamimanana, S. , Mangahasimbola, R. T., Ratovoson, R., & Randremanana, R. V. Determinants of COVID-19-related knowledge and disrupted habits during epidemic waves among women of childbearing age in urban and rural areas of the Malagasy Middle East. BMC Public Health 2023, 23. [Google Scholar] [CrossRef]
- Murray, S. , Edison, S., & Sofia, A. (2024, May). New Data: Moms Prioritize Household Healthcare Over Their Own. Https://Www.Pymnts.Com/Study_posts/New-Data-Moms-Prioritize-Household-Healthcare-over-Their-Own/?Form=MG0AV3.
- Selvaraj, S. , Karan, A. K., Mao, W., Hasan, H., Bharali, I., Kumar, P., Ogbuoji, O., & Chaudhuri, C. Did the poor gain from India’s health policy interventions? Evidence from benefit-incidence analysis, 2004–2018. International Journal for Equity in Health 2021, 20. [Google Scholar] [CrossRef]
- Manchanda, N. , & Rahut, D. B. Inpatient Healthcare Financing Strategies: Evidence from India. European Journal of Development Research 2021, 33, 1729–1767. [Google Scholar] [CrossRef]
- Kumar, A. & Gupta, S. (2012, July 2). Health Infrastructure in India: Critical Analysis of Policy Gaps in the Indian Healthcare Delivery. Https://Www.Vifindia.Org/Occasionalpaper/2012/Health-Infrastructure-in-India-Critical-Analysis-of-Policy-Gaps-in-the-Indian-Healthcare-Delivery.
- Rani, M. , & Siwach, M. Financial Literacy in India: A Review of Literature. Economic and Regional Studies / Studia Ekonomiczne i Regionalne 2023, 16, 446–458. [Google Scholar] [CrossRef]
- Gangwar, R. , & Singh, R. (2018). Analyzing Factors Affecting Financial Literacy and Its Impact on Investment Behavior Among Adults in India. SSRN Electronic Journal. [CrossRef]
- Aashima,; Sharma, R. Inequality and disparities in health insurance enrolment in India. Journal of Medicine, Surgery, and Public Health 2023, 1, 100009. [Google Scholar] [CrossRef]
- Dehury, R. K. , Ahmad, I., Behera, M. R., Samal, J., Manchana, V., Mohammed, J., Dehury, P., Behera, D., Desouza, N. V. e., & Dondapati, A. Assessment of out-of-pocket (OOP) expenditures on essential medicines for acute and chronic illness: a comparative study across regional and socioeconomic groups in India. BMC Public Health 2025, 25. [Google Scholar] [CrossRef]
- The Hans India. (2024, December 10). The Influence of Government Policies on Healthcare Financing in India: A Focus on Ayushman Bharat. Https://Www.Thehansindia.Com/Life-Style/Health/the-Influence-of-Government-Policies-on-Healthcare-Financing-in-India-a-Focus-on-Ayushman-Bharat-928656?Form=MG0AV3.
- Sahoo, N. (2023). An Examination of India’s Federal System and its Impact on Healthcare. [CrossRef]
- de Foo, C. , Verma, M., Tan, S. Y., Hamer, J., van der Mark, N., Pholpark, A., Hanvoravongchai, P., Cheh, P. L. J., Marthias, T., Mahendradhata, Y., Putri, L. P., Hafidz, F., Giang, K. B., Khuc, T. H. H., van Minh, H., Wu, S., Caamal-Olvera, C. G., Orive, G., Wang, H., … Legido-Quigley, H. Health financing policies during the COVID-19 pandemic and implications for universal health care: a case study of 15 countries. The Lancet Global Health 2023, 11, e1964–e1977. [Google Scholar] [CrossRef]
- Li, Y. , & Huang, L. Assessing the impact of public transfer payments on the vulnerability of rural households to healthcare poverty in China. BMC Health Services Research 2022, 22. [Google Scholar] [CrossRef]
- Raghupathi, V. , & Raghupathi, W. The influence of education on health: An empirical assessment of OECD countries for the period 1995-2015. Archives of Public Health 2020, 78. [Google Scholar] [CrossRef]
- Stormacq, C. , van den Broucke, S., & Wosinski, J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promotion International 2019, 34, E1–E17. [Google Scholar] [CrossRef] [PubMed]
- Aikens NL, Barbarin O. Socioeconomic Differences in Reading Trajectories: The Contribution of Family, Neighborhood, and School Contexts. Journal of Educational Psychology. 2008, 100, 235–51.
- Von Wagner, C. , Knight, K., Steptoe, A., & Wardle, J. Functional health literacy and health-promoting behaviour in a national sample of British adults. Journal of Epidemiology and Community Health 2007, 61, 1086–1090. [Google Scholar] [CrossRef]
Table 1.
Literature Review Table on factors influencing health seeking behavior during the pandemic.
Table 1.
Literature Review Table on factors influencing health seeking behavior during the pandemic.
| Study | Focus (Aim) | Method (Design, Sample Size) | Methodology | Country | Key Findings |
|---|---|---|---|---|---|
| Arnetz, B. B. et al. (2022) | Identify patient-reported factors associated with avoidance of in-person care during COVID-19 | Nationwide online survey, Recruitment via Research Match and Facebook, N = 3840 | Multivariable logistic regression analysis | USA | Avoidance is positively associated with younger age, inability to afford care, greater stress related to COVID, frequent discussions, negative healthcare experience, poor safety awareness, and low communication effectiveness |
| Bastani, P. et al. (2021) | Explore factors affecting healthcare access and utilization for older people during COVID-19 | Scoping review, Systematic search of PubMed, Web of Science, Scopus, and Embase, N = 50 articles | Thematic analysis | USA and India | Positive association between access/utilization and literacy, education, aging attitudes, service availability, policies, and social determinants |
| Czeisler, M. É. et al. (2020) | Investigate delay or avoidance of medical care due to COVID-19 concerns | Cross-sectional survey, online (web-based survey), N = 4,975 | Multivariable Poisson regression | USA | Avoidance is higher in younger adults, unpaid caregivers, individuals with underlying medical conditions, and people of black origin, covered health insurance status |
| Farrer, L. M. et al. (2023) | Examine factors associated with telehealth use and avoidance | Longitudinal survey, online (Email), N = 706 | Logistic regression | Australia | The acceptance of telehealth was higher for those who had used it before, telehealth reduces health care, avoidance was associated with younger age, speaking a language other than or in addition to English, having a current medical diagnosis, and lower levels of acceptability of telehealth. |
| Huang, W. L. et al. (2024) | Impact of post-COVID-19 changes on chronic patients' healthcare-seeking behavior | Cross-sectional in person survey, N = 9,058 | Repeated Measures ANOVA and Generalized Estimating Equation | Taiwan | Chronic patients with irregular outpatient visits had 5.85 fewer annual outpatient visits. Older age, female gender, lower socioeconomic status, and more severe pre-existing conditions were statistically significant factors contributing to reduced outpatient visits and poorer health outcomes.Limited access to healthcare facilities and telemedicine services, and less adherence to medical advice were significant predictors of reduced outpatient visits and poorer health outcomes |
| Hung, K. K. C. et al. (2022) | Analyze self-reported health service utilization in Hong Kong during COVID-19 | Cross-sectional telephone survey, Online, N = 765 | Binary logistic regression analyses | Hong Kong | The factors associated with avoiding medical consultation included being female, married, completing higher education, and those who reported a “large/very large” impact of COVID-19 on their mental health |
| Islam, M. I. et al. (2022) | Examine factors affecting healthcare avoidance among Australian youth pre- and during COVID-19 | Longitudinal in-person survey, N = 1,110 | Bivariate analyses and multiple logistic regression models | Australia | The factors most strongly associated with the avoidance of healthcare during the COVID-19 pandemic were the gender of female gender, an ongoing medical condition, and moderately high psychological distress |
| Kang, L. et al. (2023) | Identify predictors of medical care delay or avoidance in Chinese adults | Cross-sectional survey, N = 4,369 | Logistic regression | China | Older adults and adults with chronic diseases were less likely to delay or avoid medical care during the pandemic, individuals who had completed more than three years of care.College, employed adults, and current smokers in rural areas showed a higher likelihood of delaying or avoiding medical care |
| Lee, M. & You, M. (2021) | Examine the influence of socio-demographic and health-related factors on the avoidance of healthcare utilization | Cross-sectional survey, Online, N = 1,000 | Logit regression | South Korea | Sociodemographic characteristics (e.g., gender, age, income level, and residential area) were related to healthcare avoidance. Among the investigated influencing factors, residential areas highly affected by COVID-19 (i.e., Daegu/Gyeoungbuk region) had the most significant effect on healthcare avoidance |
| Lopes, S. et al. (2022) | To examine the association between the perception of COVID-19 risk, confidence in health services and avoidance of emergency department (ED) visits | Community-based cross sectional online survey, N = 987 | Logistic regression models | Portugal | The odds of avoiding ED were higher for participants who did not have confidence in the response of the health service to conditions outsideCOVID-19 and lower for those who perceived a low risk of being infected in a health provider. Self-reported worse health status increased odds of ED avoidance |
| Oduro, M. S. et al. (2023) | COVID-19-induced healthcare utilization avoidance in rural India | Cross-sectional survey, N = 2,000 | Multivariable Binary Logistic Regression Model via Multiple Imputation | India | Residents of Bihar State are more likely to avoid healthcare during COVID-19 compared to those in Andhra Pradesh. Additionally, individuals with education beyond high school, those using government healthcare facilities, and agricultural daily wage laborers also have higher odds of avoiding healthcare during the pandemic. |
| Pujolar, G. et al. (2022) | The objective is to synthesize the available knowledge on access to health care for non-COVID-19 conditions and to identify knowledge gaps. | Scoping review, Systematic search, N = 53 articles | Scoping review of the literature and PRISMA guide | Various | The most frequent access barrier described for non-COVID-19 conditions related to services was a lack of resources, while barriers related to the population were predisposing (fear of contagion, stigma, or anticipating barriers) and enabling characteristics (worset socioeconomic status and an increase in technological barriers). |
| Rezaei, Z. et al. (2023) | Effect of COVID-19 on healthcare utilization in Iran’s public vs private centers | Time series, Health records data, N = 2,700,000 | Multiple Group Interrupted Time Series Analysis | Iran | The study found that the COVID-19 pandemic significantly decreased healthcare utilization in Iran, with public healthcare centers experiencing a more substantial decline than private centers. |
| Sahakyan, S. et al. (2024) | Assess the prevalence of and risk factors associated with the avoidance or delay of medical care | Cross sectional telephone survey, N = 3,483 | Logistic regression analysis | Armenia | Overall, younger age, being female, higher monthly expenditures, higher perceived threat, and not being vaccinated were associated with avoidance or delay in medical care. |
| Smolić, Š. et al. (2023) | Impact of COVID-19 fear on forgoing healthcare access in Central/Eastern Europe (50+ age) | Cross-national panel survey using telephone interviews, N = 13,033 | Multivariate logistic regression | Central/Eastern Europe | The results suggested that women, younger older adults, more educated individuals, those in poorer health, and those with more chronic health conditions were more likely to avoid healthcare |
| Soares, P. et al. (2021) | Identify factors associated with a patient’s decision to avoid and/or delay healthcare during the COVID-19 pandemic. | Community based survey, Various Online platforms, N = 2,000 | Poisson regression | Portugal | Healthcare avoidance was more common among women, those with low confidence in the response of the healthcare system, individuals who lost income, experienced negative emotions due to distancing measures, completed the questionnaire before mid-June 2021, and perceived worse health, inadequate government measures, unclear information, and higher risks of COVID-19 infection and complications. |
| Splinter, M. J. et al. (2021) | Prevalence and determinants of healthcare avoidance during COVID-19 from patient perspective | Cross-sectional population-based in-person survey, N = 4.656 | Logistic regression | Netherlands | The determinants related to avoidance were older, female sex, low educational level (primary education versus higher vocational/university), poor self-appreciated health, unemployment, smoking, concern about contracting COVID-19, symptoms of depression and anxiety |
| Splinter, M. J. et al. (2024) | To determine the association between healthcare avoidance during the early stages of the COVID-19 pandemic and all-cause mortality. | Longitudinal community-based in-person survey, N = 5,656 | Multivariable Cox proportional hazards regression | Netherlands | Those who avoided health care reported more often symptoms of depression and anxiety and more often rated their health as poor to fair |
| Wang, Z. et al. (2023) | Investigate delay in healthcare-seeking during low COVID-19 prevalence | Cross-sectional national survey, Online, N = 1,317 | Logistic regression | China | Fear of infection, middle age, lower levels of perceived controllability of COVID-19, living with chronic conditions, pregnancy or co-habiting with a pregnant woman, access to internet-based medical care, and higher risk level in the region were significant predictors of the delay in seeking health care |
| Zhang, J. et al. (2024) | Examine health service utilization and COVID-19 in Beijing | Cross-sectional survey, Online, N = 53,924 | Multivariate Tobit regression | China | Factors affecting health service utilization include being female, older than 60 years, non-healthcare workers, rich self-rated income level, having underlying disease, living alone, depressive symptoms and healthy lifestyle habits, as well as longer infection duration, higher infection numbers and severe symptoms. |
Table 2.
Cronbach's Alpha Test Results.
| Item | Obs | Sign | Item-test Correlation | Item-rest Correlation | Average Interitem Covariance | Alpha if Item Deleted |
|---|---|---|---|---|---|---|
| Fever | 1950 | + | 0.7265 | 0.5237 | 0.0071069 | 0.4873 |
| Cough | 1950 | + | 0.7471 | 0.5678 | 0.0069213 | 0.4736 |
| Tired | 1950 | + | 0.4190 | 0.2637 | 0.0113556 | 0.5724 |
| Breath | 1950 | + | 0.5874 | 0.3443 | 0.0092194 | 0.5528 |
| Pain | 1950 | + | 0.4737 | 0.2701 | 0.0106615 | 0.5697 |
| Appetite | 1950 | + | 0.2982 | 0.2055 | 0.0125156 | 0.5868 |
| Throat | 1950 | + | 0.4409 | 0.2335 | 0.0110594 | 0.5793 |
| Diarrhea | 1950 | + | 0.0937 | 0.0436 | 0.013396 | 0.6011 |
| Nausea | 1950 | + | 0.1108 | 0.0618 | 0.0133638 | 0.6004 |
| Congestion | 1950 | + | 0.2900 | 0.0965 | 0.0126046 | 0.6070 |
| Smell | 1950 | + | 0.1104 | 0.0331 | 0.013386 | 0.6029 |
| Other | 1950 | + | 0.1162 | 0.0034 | 0.0130539 | 0.5997 |
| Test scale | 0.0112255 | 0.5963 |
Table 3.
Kaiser-Meyer-Olkin (KMO) Measure of Sampling Adequacy.
| Variable | KMO |
|---|---|
| Fever | 0.6541 |
| Cough | 0.6347 |
| Tired | 0.7104 |
| Difficulty breathing | 0.7748 |
| Muscle pain/body aches | 0.7909 |
| Loss of appetite | 0.6791 |
| Sore throat | 0.8270 |
| Diarrhea | 0.5378 |
| Nausea | 0.5055 |
| Nasal and throat congestion | 0.5922 |
| Loss of smell and taste | 0.4515 |
| Other | 0.5331 |
| Overall | 0.6790 |
Table 4.
Factor Loadings from Exploratory Factor Analysis.
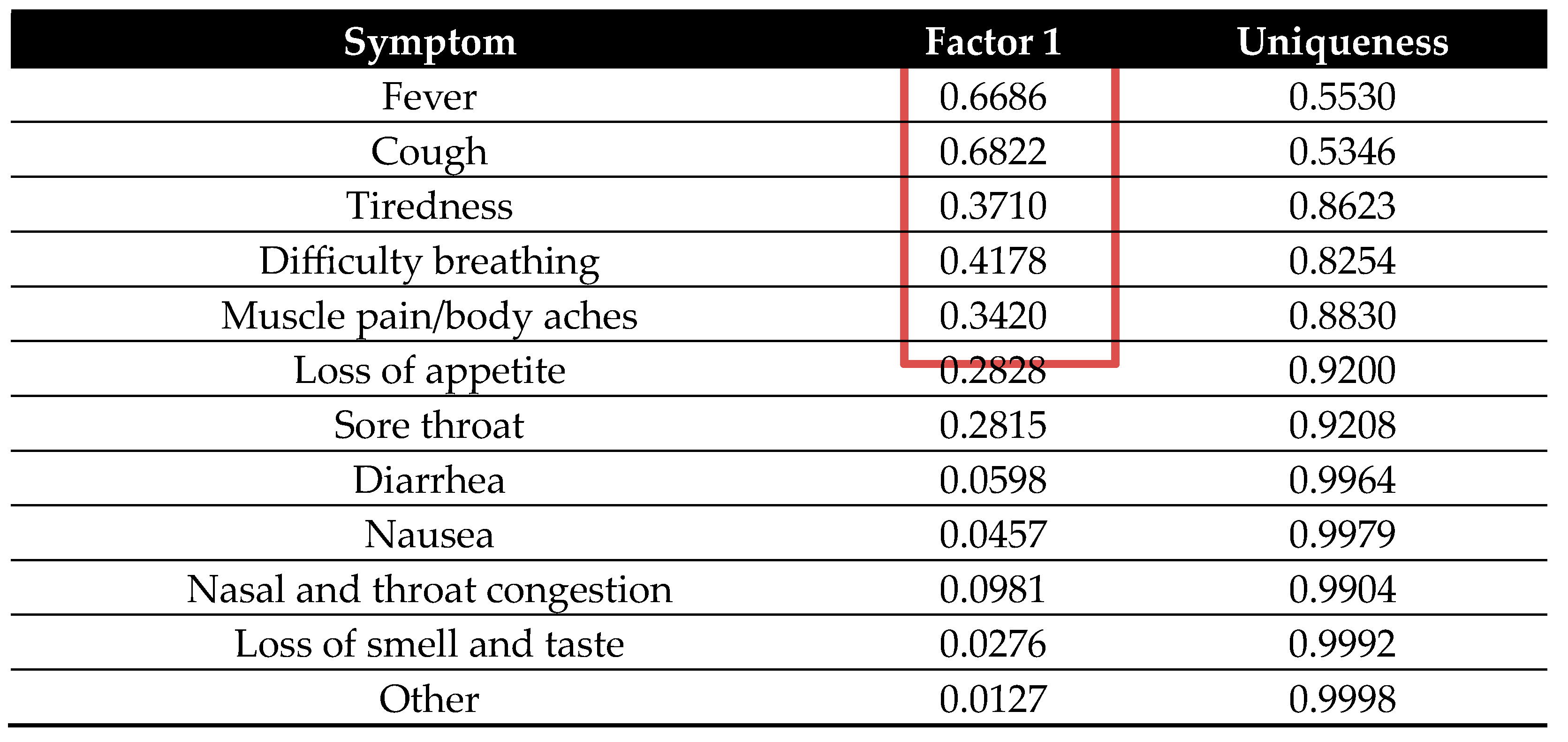 |
Table 5.
Variable definitions.
| Dependent variable | |
|---|---|
| Health facility visit | Binary variable: 1 indicates that the respondents visited health facilities in the last three months, and 0 otherwise |
| Independent variables | |
| COVID-19 respiratory and general symptoms knowledge | A composite score (0-5) indicating knowledge of key COVID-19 symptoms: fever, cough, difficulty breathing, muscle pain, and tiredness. Each symptom is coded as binary (1 = aware, 0 = not aware) |
| Age | Continuous variable: age of the respondents |
| Age squared | Continuous variable: Square of each age |
| Female | Binary variable: Equal to 1 if the respondents are females, 0 otherwise |
| No school | Binary variable: Equal to 1 if the respondents did not attend school, 0 otherwise |
| High school or more | Binary variable: Equal to 1 if the respondent attended a high school or more, 0 otherwise |
| Rich state | Binary variable: Equal to 1 if the respondent is from the states of Andhra Pradesh, Madhya Pradesh, Rajasthan or Uttar Pradesh, 0 otherwise[1]. |
| Household size | Continuous variable: Total number of people living in a household |
| Government transfer | Binary variable: Equal to 1 if the respondent received money in their bank account from the government as part of the relief fund, 0 otherwise |
| Household consumption expenditure | Continuous variable: Respondents’ own consumption expenditure measured in rupees |
| Inter_HS> | Interaction term of household size and government transfer |
| Inter_Fem&CovidRespGen | Interaction term of female and COVID-19 respiratory and general symptoms knowledge |
| Inter_Age&HighSch | Interaction term of age and high school or more |
Table 6.
Descriptive statistics.
| Variable | Mean | Std. Dev. | Min | Max |
|---|---|---|---|---|
| Dependent variable | ||||
| Health facility visit | 0.3415 | 0.4743 | 0 | 1 |
| Main independent variable | ||||
| COVID-19 respiratory and general symptoms knowledge | 1.8969 | 1.3519 | 0 | 5 |
| Other control variables | ||||
| Age | 38.0872 | 12.8127 | 18 | 91 |
| Age squared | 1614.715 | 1104.909 | 324 | 8281 |
| Female | 0.1000 | 0.3001 | 0 | 1 |
| Rich state | 0.6354 | 0.4814 | 0 | 1 |
| High school or more | 0.2836 | 0.4509 | 0 | 1 |
| No school | 0.1600 | 0.3667 | 0 | 1 |
| Household size | 6.2882 | 2.8031 | 1 | 25 |
| Government transfer | 0.6000 | 0.4900 | 0 | 1 |
| Household consumption expenditure | ₹10,471.34 | ₹11,465.25 | ₹300 | ₹150,000 |
| Inter_HS> | 3.8431 | 3.8214 | 0 | 25 |
| Inter_Fem&CovidRespGen | 0.1615 | 0.6455 | 0 | 5 |
| Inter_Age&HighSch | 9.8236 | 17.0400 | 0 | 82 |
| Observations | 1950 | |||
Table 7.
ANOVA analysis of age-related variations in health facility visits.
| Health facility visit | Age groups | |||||
|---|---|---|---|---|---|---|
| 18–29 | 30–39 | 40–49 | 50–59 | 60+ | Total | |
| 0 | 357 | 386 | 289 | 151 | 101 | 1,284 |
| % | 64.44 | 67.36 | 67.68 | 66.52 | 59.76 | 65.85 |
| 1 | 197 | 187 | 138 | 76 | 68 | 666 |
| % | 35.56 | 32.64 | 32.32 | 33.48 | 40.24 | 34.15 |
| Total | 554 | 573 | 427 | 227 | 169 | 1,950 |
| % | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| F-statistics | 1.13 | |||||
Table 8.
T-test analysis of health facility visits across rich states and no schooling status.
| Health facility visit | Rich states | No school | |||
|---|---|---|---|---|---|
| 0 | 1 | 0 | 1 | Total | |
| 0 | 500 | 784 | 1064 | 220 | 1284 |
| % | 70.32 | 63.28 | 64.96 | 70.51 | 65.85 |
| 1 | 211 | 455 | 574 | 92 | 666 |
| % | 29.68 | 36.72 | 35.04 | 29.49 | 34.15 |
| Total | 711 | 1239 | 1638 | 312 | 1950 |
| % | 100 | 100 | 100 | 100 | 100 |
| Mean Difference | t-value = -3.1648** | t-value = 1.8973* | |||
Table 9.
Correlation Matrix test results.
| Variables | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Health facility visit | 1.000 | ||||||||||||
| (2) COVID-19 symptoms knowledge | 0.044 | 1.000 | |||||||||||
| (3) Age | 0.013 | -0.008 | 1.000 | ||||||||||
| (4) Female | 0.019 | -0.069 | -0.098 | 1.000 | |||||||||
| (5) Rich state | 0.072 | 0.059 | 0.193 | -0.216 | 1.000 | ||||||||
| (6) High school or more | 0.008 | 0.268 | -0.169 | -0.073 | -0.029 | 1.000 | |||||||
| (7) No school | -0.043 | -0.214 | 0.169 | 0.176 | 0.040 | -0.275 | 1.000 | ||||||
| (8) Household size | 0.038 | 0.035 | -0.040 | -0.062 | -0.043 | 0.011 | -0.031 | 1.000 | |||||
| (9) Government transfer | 0.023 | 0.018 | -0.028 | -0.028 | 0.040 | -0.058 | -0.003 | 0.051 | 1.000 | ||||
| (10) Household consumption expenditure | 0.072 | 0.103 | 0.043 | -0.059 | 0.081 | 0.106 | -0.057 | 0.159 | -0.057 | 1.000 | |||
| (11) Inter_HS> | 0.051 | 0.034 | -0.029 | -0.053 | 0.009 | -0.040 | -0.026 | 0.486 | 0.821 | 0.013 | 1.000 | ||
| (12) Inter_Fem&CovidRespG | 0.002 | 0.156 | -0.103 | 0.751 | -0.159 | -0.013 | 0.053 | -0.027 | -0.010 | -0.022 | -0.020 | 1.000 | |
| (13) Inter_Age&HighSch | 0.014 | 0.254 | 0.058 | -0.087 | -0.009 | 0.917 | -0.252 | -0.007 | -0.092 | 0.113 | -0.071 | -0.035 | 1.000 |
Table 10.
Variance Inflation test (VIF) results.
| Variable | VIF | 1/VIF |
|---|---|---|
| High school or more | 9.21 | 0.108520 |
| Inter_Age&HighSch | 9.02 | 0.110889 |
| Inter_HS> | 7.84 | 0.127562 |
| Government transfer | 6.03 | 0.165956 |
| Female | 2.63 | 0.380815 |
| Household size | 2.61 | 0.383621 |
| Inter_Fem&CovidRespGen | 2.57 | 0.389641 |
| Age | 1.57 | 0.638345 |
| COVID-19 respiratory and general symptoms knowledge | 1.23 | 0.814225 |
| No school | 1.18 | 0.846097 |
| Rich state | 1.11 | 0.904194 |
| Household consumption expenditure | 1.06 | 0.942358 |
| Mean VIF | 3.84 | |
Table 11.
Probit Regression Estimation results.
| Variables | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Dependent variable: Probability of visiting a health facility | |||
| COVID-19 respiratory and general symptoms knowledge | 0.0421* | 0.0555** | 0.0418* |
| (0.0215) | (0.0235) | (0.0240) | |
| Age | -0.0169 | -0.0233* | |
| (0.0125) | (0.0132) | ||
| Age squared | 0.0002 | 0.0003* | |
| (0.0001) | (0.0001) | ||
| Female | 0.2786* | 0.4357*** | |
| (0.1516) | (0.1567) | ||
| Inter_Fem&CovidRespGen | -0.1079 | -0.1238* | |
| (0.0716) | (0.0724) | ||
| Inter_Age&HighSch | -0.0000 | 0.0044 | |
| (0.0018) | (0.0052) | ||
| Rich state | 0.2279*** | ||
| (0.0651) | |||
| High school or more | -0.2091 | ||
| (0.2002) | |||
| No school | -0.1710* | ||
| (0.0887) | |||
| Household size | -0.0088 | ||
| (0.0172) | |||
| Government transfer | -0.1843 | ||
| (0.1477) | |||
| Household consumption expenditure | 0.0000** | ||
| (0.0000) | |||
| Inter_HS> | 0.0407* | ||
| (0.0217) | |||
| Constant | -0.4888*** | -0.2307 | -0.2209 |
| (0.0506) | (0.2556) | (0.2966) | |
| Observations | 1,950 | 1,950 | 1,950 |
| Log likelihood | -1250 | -1247 | -1231 |
| Chi2 statistics | 3.835 | 9.890 | 41.99 |
| p-value | 0.0502 | 0.129 | 6.56e-05 |
| Robust standard errors in parentheses | |||
| *** p<0.01, ** p<0.05, * p<0.1 | |||
Table 12.
Marginal Effects Estimation results.
| Variables | dy/dx | dy/dx | dy/dx |
| Model 1 | Model 2 | Model 3 | |
| Dependent variable: Probability of visiting a health facility | |||
| COVID-19 respiratory and general symptoms knowledge | 0.015** | 0.020** | 0.015* |
| (0.008) | (0.009) | (0.009) | |
| Age | -0.006 | -0.008* | |
| (0.005) | (0.005) | ||
| Age squared | 0.000 | 0.000* | |
| (0.000) | (0.000) | ||
| Female | 0.102* | 0.157** | |
| (0.055) | (0.056) | ||
| Inter_Fem&CovidRespGen | -0.039 | -0.045* | |
| (0.026) | (0.026) | ||
| Inter_Age&HighSch | -0.000 | 0.002 | |
| (0.001) | (0.002) | ||
| Rich state | 0.082*** | ||
| (0.023) | |||
| High school or more | -0.075 | ||
| (0.072) | |||
| No school | -0.062* | ||
| (0.032) | |||
| Household size | -0.003 | ||
| (0.006) | |||
| Government transfer | -0.066 | ||
| (0.053) | |||
| Household consumption expenditure | 0.000** | ||
| (0.000) | |||
| Inter_HS> | 0.015* | ||
| (0.008) | |||
| Observations | 1,950 | 1,950 | 1,950 |
| Robust standard errors in parentheses | |||
| *** p<0.01, ** p<0.05, * p<0.1 | |||
Table 13.
Maximum Likelihood Estimation results.
| Variables | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Dependent variable: Probability of visiting a health facility | |||
| COVID-19 respiratory and general symptoms knowledge | 0.0419** | 0.0540*** | 0.0382* |
| (0.0182) | (0.0198) | (0.0204) | |
| Age | -0.0170 | -0.0234* | |
| (0.0125) | (0.0133) | ||
| Age squared | 0.0002 | 0.0003* | |
| (0.0001) | (0.0001) | ||
| Female | 0.2911* | 0.4354*** | |
| (0.1522) | (0.1568) | ||
| Inter_Fem&CovidRespGen | -0.1137 | -0.1247* | |
| (0.0719) | (0.0723) | ||
| Inter_Age&HighSch | -0.0002 | 0.0045 | |
| (0.0018) | (0.0052) | ||
| Rich state | 0.2218*** | ||
| (0.0656) | |||
| High school or more | -0.2158 | ||
| (0.2003) | |||
| No school | -0.1651* | ||
| (0.0897) | |||
| Household size | -0.0083 | ||
| (0.0171) | |||
| Government transfer | -0.1813 | ||
| (0.1480) | |||
| Household consumption expenditure | 0.0000** | ||
| (0.0000) | |||
| Inter_HS> | 0.0404* | ||
| (0.0216) | |||
| Constant | -0.5043*** | -0.2466 | -0.2244 |
| (0.0510) | (0.2558) | (0.2949) | |
| Observations | 1,950 | 1,950 | 1,950 |
| Log likelihood | -1249 | -1246 | -1231 |
| Chi2 statistics | 5.332 | 11.71 | 41.47 |
| p-value | 0.0209 | 0.0687 | 7.99e-05 |
| Standard errors in parentheses | |||
| *** p<0.01, ** p<0.05, * p<0.1 | |||
1 These four states were grouped as 1 because they are classified among the top 10 states with the highest GDP per capita in the country [48] . |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



