Submitted:
01 March 2025
Posted:
03 March 2025
You are already at the latest version
Abstract
Background: Extrapulmonary neuroendocrine carcinomas (EP-NECs) are rare, aggressive malignancies with no standardized treatment approach. Although platinum-based chemotherapy is considered the first-line therapy, overall survival (OS) and progression-free survival (PFS) remain limited. This study aims to evaluate the clinical and pathological characteristics of EP-NEC patients, their treatment responses, and survival outcomes. Methods: This retrospective observational study included 29 EP-NEC patients diagnosed and followed between 2015 and 2024. Clinical and demographic data, tumor localization, disease stage, administered treatments, and survival outcomes were analyzed. Kaplan-Meier survival analysis was used to assess OS and PFS, with subgroup comparisons performed via the log-rank test. Results: The most common primary tumor sites were the pancreas (21%), prostate (17%), and cervix (14%). At diagnosis, 55.2% of patients had metastatic disease. First-line platinum-based chemotherapy achieved an objective response rate of 82.1%, with a median PFS of 8.16 months and a median OS of 14.16 months. Surgical intervention significantly improved survival (p = 0.020), while a high Ki-67 proliferation index (>80%) was associated with worse PFS (p = 0.032). Other factors, including smoking status and liver-directed therapies, had no significant impact on survival. Conclusion: EP-NECs present with poor prognosis despite platinum-based chemotherapy achieving high response rates. Surgical resection improves survival outcomes, whereas high Ki-67 expression is associated with worse prognosis. These findings highlight the need for further research into novel therapeutic strategies for EP-NECs.
Keywords:
Extrapulmonary neuroendocrine carcinoma
; platinum-based chemotherapy
; survival analysis
; Ki-67 index
; surgical intervention
1. Introduction
Extrapulmonary neuroendocrine carcinomas (EP-NECs) are extremely rare and can develop in various parts of the gastrointestinal (GI) tract. In the squamous-lined regions of the GI tract, such as the esophagus and anus, they predominantly exhibit small-cell histology[1]. Within the jejunum and ileum, EP-NECs account for only 1% of all neuroendocrine tumors[2]. Additionally, extrapulmonary small-cell carcinomas can arise in the bladder (0.3%–1% of cases), cervix (1% of cases), and prostate (2% of cases)[3]. These tumors are characterized by rapid proliferation, high mitotic rates, and poor differentiation, leading to limited treatment options and poor prognosis[4,5].
EP-NECs are aggressive epithelial cancers with immunohistochemical expression of neuroendocrine (NE) markers (chromogranin A, synaptophysin, or neuron cell adhesion molecule), and a proliferation (Ki-67) index of >20%[6]. In addition, EP-NECs lack the typical organoid-like growth pattern of low-grade, well-differentiated neuroendocrine tumors (WD-NETs) and are therefore defined as poorly differentiated. Similar to their pulmonary counterparts, EP-NECs can exhibit a “small-cell” (SC) morphology, characterized by diffuse sheets of cells with scant cytoplasm and fusiform nuclei with inconspicuous nucleoli and finely granular chromatin, or a “large-cell” morphology, with nests- or trabeculae-like patterns of round/polygonal cells, moderate amounts of cytoplasm, and large nuclei with prominent nucleoli and vesicular chromatin[7].
Patients with an EP-NEC diagnosis mostly present with metastatic disease and have an average life expectancy of less than 12 months[8]. Treatment options for these patients remain limited; surgery is the mainstay of treatment in localized disease, while platinum-based chemotherapy is the only standard-of-care first-line palliative treatment, unchanged for the past three decades[1]. Although radiological responses are observed in up to ~70% of patients receiving first-line platinum-based chemotherapy, disease progression occurs rapidly, with a median progression-free survival (PFS) of 4–9 months[9,10]. Several chemotherapy regimens have been explored after platinum-based chemotherapy failure in small retrospective studies or non-randomized trials, but none have become standard practice to date[11].
Despite their histological similarities to small-cell lung cancer (SCLC), EP-NECs lack a standardized treatment approach. Current therapeutic strategies primarily rely on platinum-based chemotherapy, mirroring SCLC treatment guidelines[6,12,13]. However, retrospective studies indicate that response rates in EP-NECs are lower compared to SCLC, with a median progression-free survival (PFS) of 4–9 months and an overall survival (OS) ranging from 5 to 16 months[13-15]. Recent advancements in molecular profiling have highlighted the genetic heterogeneity of EP-NECs, distinguishing them from their pulmonary counterparts. Key genetic alterations, including TP53, RB1, MYCN amplification, and BRAF mutations, suggest potential therapeutic targets beyond conventional chemotherapy[16]. While platinum-based chemotherapy remains the standard first-line treatment, its long-term efficacy is limited, necessitating further exploration of molecularly targeted therapies and immunotherapy approaches[17,18].
Furthermore, while EP-NECs have historically been treated as a single disease entity, evidence from large datasets suggests significant variability in survival and treatment outcomes within the EP-NEC spectrum, indicating underlying biological heterogeneity[8,19]. The anatomical site of origin and a Ki-67 threshold of 55% have emerged as key prognostic factors. Ki-67 index of <55% was associated with significantly longer OS but a lower likelihood of response to platinum-based chemotherapy compared to patients with a Ki-67 index of ≥55%[19,20].
This study aims to evaluate the clinical characteristics of EP-NEC patients, assess treatment responses, and identify prognostic factors associated with survival outcomes. By integrating findings from contemporary literature, this research seeks to highlight the urgent need for novel therapeutic strategies beyond traditional chemotherapy.
2. Materials and Methods
This study was designed as a retrospective observational analysis. A total of 29 patients diagnosed with EP-NEC between 2015 and 2024 and followed up during this period were included in the study. Patients with pulmonary neuroendocrine carcinoma or those with histopathological evidence of mixed tumors were excluded.
Clinical and demographic data, date of diagnosis, disease stage at presentation, administered treatments, progression timelines, and survival outcomes were reviewed. Demographic data, including age, sex, smoking history, and Eastern Cooperative Oncology Group (ECOG) performance status(PS), were recorded. Primary tumor localization, disease stage at diagnosis (local, locoregional, metastatic), and metastatic sites (liver, bone, lymph nodes, etc.) were evaluated. The administration of surgery, chemotherapy, radiotherapy, and immunotherapy, along with treatment responses, were documented.
Data were analyzed using SPSS v27.0 (IBM Corp.). Categorical variables were presented as frequencies and percentages, while continuous variables related to survival times were reported as means and medians. The relationship between clinicopathological features and survival was evaluated using univariate and multivariate Cox proportional hazards models. The type I error level was set at 5%. Additionally, OS ve PFS analysis was performed using Kaplan–Meier curves and a log-rank test.
This study was reviewed and approved by the Non-Interventional Clinical Research Ethics Committee of Istanbul Medipol University (Approval No: 150, Date: 06.02.2025). All research procedures were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
3. Results
This study included 29 patients diagnosed with EP-NECs, with a nearly equal gender distribution and a median age of 60.14 years (range: 29–82). At initial diagnosis, 55.2% of patients had metastatic disease, while 10.3% had localized and 34.5% had locoregional disease. The majority of patients (69%) were non-smokers. The Ki-67 proliferation index was greater than 80% in 75% of patients. Treatment approaches varied, including curative-intent radiotherapy (39.3%), concurrent chemoradiotherapy (25%), liver-directed therapies (6.9%), and surgical resection (31%). All patients received platinum-based chemotherapy, with 51.7% receiving cisplatin-etoposide and 48.3% receiving carboplatin-etoposide. Detailed demographic and clinical characteristics are summarized in Table 1.
The most common primary tumor site was the pancreas (21%), followed by the prostate (17%) and cervix (14%). Other frequently affected sites included the bladder (10%), stomach (7%), colon (4%), and liver (4%). Less common primary tumor locations involved the rectum, gallbladder, thyroid, breast, parotid gland, and head-neck region, each accounting for approximately 3–4% of cases (Figure 1). Among the 16 patients diagnosed with metastatic disease, the most common sites of metastasis were the bone (27.6%), liver (13.8%), lymph nodes (13.8%), lung (10.3%), and brain (3.4%) (Figure 2).
The response to first-line therapy was notable, with a complete response (CR) in 12 patients (42.9%), partial response (PR) in 11 patients (39.3%), and progressive disease (PD) in 5 patients (17.9%), yielding an overall objective response rate (ORR) of 82.1%. Second-line chemotherapy was administered to 15 patients (51.7%) and included irinotecan (17.2%), cisplatin-etoposide (6.9%), and other regimens such as paclitaxel and oxaliplatin plus capesitabine (CAPOX) (17.2%). Response rates for second-line therapy showed PR in 3 patients (10.3%), stable disease (SD) in 1 patient (3.4%), and PD in 7 patients (24.1%). Third-line chemotherapy was given to 10 patients (34.5%) with a median of 3 cycles per patient. Immunotherapy was administered to 3 patients (10.3%), where one patient exhibited stable disease (SD) and another experienced disease progression (Table 2).
At the median follow-up 25.6 months(range: 6.5-33.2) median PFS was 8.16 months (CI 95% 1.88–14.45, Figure 3). The median OS was 14.16 months (CI 95% 5.92-31.31, Figure 4). The univariate analysis of PFS and OS identified key prognostic factors. For PFS, ECOG performance status (p = 0.005), surgical history (p = 0.020), and Ki-67 index (p = 0.032) were statistically significant prognostic factors. In other words, poor ECOG PS (2 vs 0-1) and lack of surgery were associated with worse PFS, while patients with a lower Ki-67 (<80%) had slightly better outcomes. Although not statistically significant, first-line chemotherapy choice (Cisplatin-Etoposide vs. Carboplatin-Etoposide) showed a numerical trend favoring Cisplatin-Etoposide (13.1 vs. 7.1 months, p = 0.182).
For OS, no variables reached statistical significance, but first-line chemotherapy (Cisplatin-Etoposide vs. Carboplatin-Etoposide) and disease stage showed numerically meaningful differences. Patients receiving Cisplatin-Etoposide had longer OS (26.4 vs. 11.7 months, p = 0.180), and those with local disease survived longer (52.2 months) than those with locoregional (12.4 months) or metastatic disease (11.8 months) (p = 0.520).
These findings suggest that ECOG-PS, surgical intervention, and tumor proliferation index significantly influenced PFS, while chemotherapy choice and disease stage may have an impact on OS. Detailed results of the univariate analysis for PFS and OS are available in Table 3 and Table 4, respectively.
Multivariate analysis revealed that Ki-67 index, surgical intervention, and immunotherapy status were independent prognostic factors for PFS. Patients with a high Ki-67 index (≥60%) had significantly worse PFS (p = 0.000), indicating its role in tumor aggressiveness. Surgical resection was associated with a significant improvement in PFS (p = 0.030), emphasizing the potential survival benefit of surgery in selected patients. Additionally, patients who did not receive ICIs had an increased risk of progression (p = 0.035).
In contrast, ECOG PS (p = 0.463) and the choice of first-line chemotherapy regimen (Cisplatin-Etoposide vs. Carboplatin-Etoposide, p = 0.475) did not show significant associations with PFS. These findings underscore the impact of tumor biology and treatment approach on disease progression (Table 3).
Multivariate analysis revealed that none of the evaluated factors were independent predictors of OS (p > 0.05). However, certain variables exhibited numerical trends. The choice of first-line chemotherapy (Cisplatin-Etoposide vs. Carboplatin-Etoposide) showed a tendency towards improved OS in patients receiving Cisplatin-Etoposide (26.4 vs. 11.7 months, p = 0.331), though this was not statistically significant. Similarly, patients undergoing surgical intervention demonstrated better survival outcomes (26.4 vs. 11.8 months, p = 0.705), yet the effect was not statistically significant in the multivariate model. The Ki-67 index was not a significant predictor of OS (p = 0.645). These findings suggest that while surgical resection and chemotherapy choice may influence survival, their effects were not robust enough to reach statistical significance in the current dataset (Table 4).
4. Discussion
EP-NECs are rare and aggressive malignancies with limited treatment options. Despite the use of platinum-based chemotherapy as the first-line treatment, survival outcomes remain poor. Our study, consistent with existing literature, highlights the challenges in managing EP-NECs and underscores the need for more effective therapeutic strategies.
In our cohort, first-line platinum-based chemotherapy demonstrated a high ORR (82.1%), compatible with prior reports that show initial response rates of up to 70–80% [21]. [21]. However, disease progression occurred rapidly, in our study, with a median PFS of 8.16 months and median OS of 14.16 months, which are relatively favorable compared to other studies that reported PFS ranging from 5.83 to 9 months and OS between 13.6 and 16 months [21,22]. This variability may stem from differences in patient characteristics, treatment approaches, and disease burden at the diagnosis. Notably, patients who underwent surgical resection had significantly improved survival outcomes (p = 0.02), supporting the notion that resection should be considered in selected cases where feasible[23].
Survival outcomes in EP-NEC remain poor suboptimal despite current treatment strategies. Multiple studies have reported median PFS and OS values in patients receiving platinum-based chemotherapy. To provide a comparative perspective on survival outcomes across different studies, we have compiled relevant data from the literature, including our study, in the table below. This table summarizes survival rates and treatment responses in metastatic EP-NEC patients, offering insights into prognosis and therapeutic efficacy (Table 5).
A key prognostic factor identified in our study was the Ki-67 proliferation index, with 75% of patients exhibiting Ki-67 >80%, a finding consistent with previous research[18]. High Ki-67 expression was associated with significantly worse PFS (p = 0.032), reinforcing its role in risk stratification and treatment planning. These findings emphasize the need for a more personalized approach to EP-NEC management, particularly for patients with highly proliferative tumors.
Our study also evaluated treatment beyond first-line therapy. Second-line chemotherapy resulted in partial response in only 10.3% of patients, while 24.1% had disease progression, suggesting diminishing efficacy with successive lines of treatment. Third-line therapy yielded no partial responses, with only 6.9% of patients achieving stable disease, indicating a critical need for alternative approaches in refractory EP-NEC cases.
Our multivariate analysis further supports the significance of these prognostic factors. The Ki-67 index was identified as the strongest predictor of PFS, with higher values correlating with significantly shorter survival durations. This aligns with prior studies suggesting that highly proliferative tumors exhibit increased resistance to systemic therapies. Surgical resection remained a critical factor, demonstrating an independent association with improved PFS. These findings reinforce the notion that, despite the aggressive nature of EP-NECs, surgery should be considered in carefully selected cases where resection is feasible.
Interestingly, our analysis also indicated a potential role for immunotherapy in delaying disease progression, as patients who did not receive immunotherapy had significantly worse PFS. While the role of immune checkpoint inhibitors in EP-NECs remains controversial, emerging evidence suggests that specific molecular subgroups may derive benefit from such therapies. Further prospective trials are warranted to evaluate the efficacy of immunotherapy in EP-NEC patients.
Multivariate analysis did not identify any independent predictors of OS. However, numerical trends suggested that Cisplatin-Etoposide might be associated with better survival compared to Carboplatin-Etoposide, and surgical intervention showed a potential benefit, though neither reached statistical significance. Interestingly, the Ki-67 index was not an independent prognostic factor, highlighting the complexity of EP-NECs. These findings emphasize the need for larger studies integrating molecular profiling to improve treatment strategies.
Immune checkpoint inhibitors (ICIs) remains a controversial approach for EP-NECs. In our study, three patients who received immunotherapy beyond the third line setting experienced disease progression as the best response. This observation aligns with findings from previous reports demonstrating limited benefit of ICIs in EP-NECs, particularly in tumors with low PD-L1 expression[18]. The KEYNOTE-158 trial similarly reported a low response rate (3.7%) with pembrolizumab in neuroendocrine neoplasms[32]. Given these results, ICIs may be more effective in specific molecular subgroups rather than as a generalized treatment for all EP-NECs. Future research should focus on biomarker-driven patient selection and combination strategies with DNA repair inhibitors or chemotherapy to enhance response rates[33].
Molecular profiling has revealed substantial heterogeneity in EP-NECs, suggesting that different biological subtypes may require distinct therapeutic approaches[33]. The classification proposed by Frizziero et al. (2022) categorizes EP-NECs into SCLC-like, non-neuroendocrine cancer-like, and tumor-agnostic groups, each with unique molecular features and potential therapeutic targets. This framework may help refine treatment algorithms:
- SCLC-like EP-NECs, frequently harboring TP53 and RB1 mutations, may benefit from DNA repair-targeted therapies.
- Non-neuroendocrine cancer-like EP-NECs, with frequent KRAS and BRAF mutations, could be targeted with BRAF and MEK inhibitors.
- Tumor-agnostic EP-NECs, characterized by epigenetic alterations, might respond to EZH2 inhibitors[33].
Given the poor prognosis associated with current treatments, alternative strategies such as targeted therapies and novel ICIs combinations warrant further investigation. Agents such as AURKA inhibitors (for MYCN-amplified tumors), PARP inhibitors, and epigenetic modulators have shown preclinical promise[33]. However, their clinical efficacy remains to be validated in prospective studies.
5. Conclusion
EP-NECs remain a rare and highly aggressive malignancy with limited treatment options. Despite achieving high ORR with platinum-based chemotherapy, the prognosis for EP-NEC patients remains poor, with a median PFS of 8.16 months and a median OS of 14.16 months in our cohort. These findings underscore the urgent need for more effective therapeutic strategies.
Our study highlights the importance of surgical resection in improving survival outcomes. Patients who underwent surgery had significantly longer survival compared to those who did not, suggesting that surgical intervention should be considered in carefully selected cases. However, due to the aggressive nature of EP-NECs, surgical resection is often not feasible, emphasizing the need for additional systemic therapies.
Given the poor prognosis associated with current treatment modalities, the development of novel therapeutic strategies is imperative. Multicenter clinical trials, biomarker-driven therapies, and personalized treatment approaches are needed to optimize patient outcomes. Collaborative efforts between oncologists, molecular biologists, and clinical researchers will be essential in advancing the management of EP-NECs and improving survival rates for affected patients.
Author Contributions
Conceptualization, H.M. M.M.M., E.S, A.B., Ö.Y, Ö.A, Ö.FÖ. J.H.; methodology, H.M. M.H.Y. E.S software, H.M., E.S., M.M.M.,A.B., Ö.A.,Ö.FÖ.,J.H., validation, H.M. E.E.D.,M.H.Y., H.Ö., formal analysis, H.M. H.Ö., investigation, H.M.; resources, H.M., A.B; data curation, H.M. M.H.Y, E.E.D.,H.Ö, Ö.A. J.H., Ö.FÖ.,Ö.Y.,.; writing—original draft preparation, H.M.,A.B; writing—review and editing, H.M.; visualization, H.M.; supervision, A.B..; project administration, H.M., E.S.,; All authors have read and agreed to the published version of the manuscript.
Funding
None
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the . Ethical approval was obtained from the institutional review board (Approval No: 150, Date: 06.02.2025).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data of this study is available from the corresponding author upon a reasonable request.
Acknowledgments
None
Conflicts of Interest
The authors declare no conflict of interest
References
- Shia, J.; Tang, L.H.; Weiser, M.R.; Brenner, B.; Adsay, N.V.; Stelow, E.B.; Saltz, L.B.; Qin, J.; Landmann, R.; Leonard, G.D. Is nonsmall cell type high-grade neuroendocrine carcinoma of the tubular gastrointestinal tract a distinct disease entity? The American journal of surgical pathology 2008, 32, 719–731. [Google Scholar] [CrossRef]
- Qubaiah, O.; Devesa, S.S.; Platz, C.E.; Huycke, M.M.; Dores, G.M. Small intestinal cancer: a population-based study of incidence and survival patterns in the United States, 1992 to 2006. Cancer epidemiology, biomarkers & prevention 2010, 19, 1908–1918. [Google Scholar]
- Walenkamp, A.M.; Sonke, G.S.; Sleijfer, D.T. Clinical and therapeutic aspects of extrapulmonary small cell carcinoma. Cancer treatment reviews 2009, 35, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.R.; Coppola, D.; Klimstra, D.S.; Phan, A.T.; Kulke, M.H.; Wiseman, G.A.; Kvols, L.K. The NANETS consensus guidelines for the diagnosis and management of poorly differentiated (high-grade) extrapulmonary neuroendocrine carcinomas. Pancreas 2010, 39, 799–800. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.-N.; Rashid, A. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. Journal of clinical oncology 2008, 26, 3063–3072. [Google Scholar] [CrossRef]
- Garcia-Carbonero, R.; Sorbye, H.; Baudin, E.; Raymond, E.; Wiedenmann, B.; Niederle, B.; Sedlackova, E.; Toumpanakis, C.; Anlauf, M.; Cwikla, J. ENETS consensus guidelines for high-grade gastroenteropancreatic neuroendocrine tumors and neuroendocrine carcinomas. Neuroendocrinology 2016, 103, 186–194. [Google Scholar] [CrossRef]
- McNamara, M.G.; Frizziero, M.; Jacobs, T.; Lamarca, A.; Hubner, R.A.; Valle, J.W.; Amir, E. Second-line treatment in patients with advanced extra-pulmonary poorly differentiated neuroendocrine carcinoma: a systematic review and meta-analysis. Therapeutic advances in medical oncology 2020, 12, 1758835920915299. [Google Scholar] [CrossRef]
- Lantuejoul, S.; Fernandez-Cuesta, L.; Damiola, F.; Girard, N.; McLeer, A. New molecular classification of large cell neuroendocrine carcinoma and small cell lung carcinoma with potential therapeutic impacts. Translational lung cancer research 2020, 9, 2233. [Google Scholar] [CrossRef]
- Walter, T.; Tougeron, D.; Baudin, E.; Le Malicot, K.; Lecomte, T.; Malka, D.; et al. Poorly differentiated gastro-entero-pancreatic neuroendocrine carcinomas: are they really heterogeneous? Insights from the FFCD-GTE national cohort. European Journal of Cancer 2017, 79, 158–165. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Burke, A.P.; Marx, A.; Nicholson, A.G. Introduction to the 2015 World Health Organization classification of tumors of the lung, pleura, thymus, and heart. Journal of Thoracic Oncology 2015, 10, 1240–1242. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C. AJCC cancer staging manual; Springer, 2017; Vol. 1024. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). European journal of cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Moertel, C.G.; Kvols, L.K.; O'Connell, M.J.; Rubin, J. Treatment of neuroendocrine carcinomas with combined etoposide and cisplatin. Evidence of major therapeutic activity in the anaplastic variants of these neoplasms. Cancer 1991, 68, 227–232. [Google Scholar] [CrossRef]
- Terashima, T.; Morizane, C.; Hiraoka, N.; Tsuda, H.; Tamura, T.; Shimada, Y.; Kaneko, S.; Kushima, R.; Ueno, H.; Kondo, S. Comparison of chemotherapeutic treatment outcomes of advanced extrapulmonary neuroendocrine carcinomas and advanced small-cell lung carcinoma. Neuroendocrinology 2012, 96, 324–332. [Google Scholar] [PubMed]
- Heetfeld, M.; Chougnet, C.N.; Olsen, I.H.; Rinke, A.; Borbath, I.; Crespo, G.; Barriuso, J.; Pavel, M.; O'Toole, D.; Walter, T. Characteristics and treatment of patients with G3 gastroenteropancreatic neuroendocrine neoplasms. Endocrine-related cancer 2015, 22, 657–664. [Google Scholar] [PubMed]
- Yamaguchi, T.; Machida, N.; Morizane, C.; Kasuga, A.; Takahashi, H.; Sudo, K.; Nishina, T.; Tobimatsu, K.; Ishido, K.; Furuse, J. Multicenter retrospective analysis of systemic chemotherapy for advanced neuroendocrine carcinoma of the digestive system. Cancer science 2014, 105, 1176–1181. [Google Scholar] [CrossRef]
- Yachida, S.; Totoki, Y.; Noë, M.; Nakatani, Y.; Horie, M.; Kawasaki, K.; Nakamura, H.; Saito-Adachi, M.; Suzuki, M.; Takai, E. Comprehensive genomic profiling of neuroendocrine carcinomas of the gastrointestinal system. Cancer discovery 2022, 12, 692–711. [Google Scholar]
- Govindan, R.; Aggarwal, C.; Antonia, S.J.; Davies, M.; Dubinett, S.M.; Ferris, A.; Forde, P.M.; Garon, E.B.; Goldberg, S.B.; Hassan, R.; et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of lung cancer and mesothelioma. Journal for ImmunoTherapy of Cancer 2022, 10, e003956. [Google Scholar] [CrossRef]
- McNamara, M.G.; Scoazec, J.-Y.; Walter, T. Extrapulmonary poorly differentiated NECs, including molecular and immune aspects. Endocrine-Related Cancer 2020, 27, R219–R238. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. REporting recommendations for tumor MARKer prognostic studies (REMARK). Breast cancer research and treatment 2006, 100, 229–235. [Google Scholar]
- de M Rêgo, J.F.; de Medeiros, R.S.S.; Braghiroli, M.I.; Galvão, B.; Neto, J.E.B.; Munhoz, R.R.; Guerra, J.; Nonogaki, S.; Kimura, L.; Pfiffer, T.E. Expression of ERCC1, Bcl-2, Lin28a, and Ki-67 as biomarkers of response to first-line platinum-based chemotherapy in patients with high-grade extrapulmonary neuroendocrine carcinomas or small cell lung cancer. ecancermedicalscience 2017, 11, 767. [Google Scholar] [CrossRef]
- Jesinghaus, M.; Konukiewitz, B.; Keller, G.; Kloor, M.; Steiger, K.; Reiche, M.; Penzel, R.; Endris, V.; Arsenic, R.; Hermann, G. Colorectal mixed adenoneuroendocrine carcinomas and neuroendocrine carcinomas are genetically closely related to colorectal adenocarcinomas. Modern Pathology 2017, 30, 610–619. [Google Scholar] [PubMed]
- Frizziero, M.; Kilgour, E.; Simpson, K.L.; Rothwell, D.G.; Moore, D.A.; Frese, K.K.; Galvin, M.; Lamarca, A.; Hubner, R.A.; Valle, J.W. Expanding therapeutic opportunities for extrapulmonary neuroendocrine carcinoma. Clinical Cancer Research 2022, 28, 1999–2019. [Google Scholar]
- Celik, E.; Samanci, N.S.; Derin, S.; Bedir, S.; Degerli, E.; Oruc, K.; Oztas, N.S.; Alkan, G.; Senyigit, A.; Turna, H. A single center’s experience of the extrapulmonary neuroendocrine carcinomas. Northern Clinics of Istanbul 2022, 9, 35. [Google Scholar] [PubMed]
- Weaver, J.M.J.; Hubner, R.A.; Valle, J.W.; McNamara, M.G. Selection of Chemotherapy in Advanced Poorly Differentiated Extra-Pulmonary Neuroendocrine Carcinoma. Cancers 2023, 15, 4951. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.; Krapcho, M.; Garshell, J.; Miller, D.; Altekruse, S. Surveillance, Epidemiology, and End Results (SEER) Program (www. seer. cancer. gov) SEER* Stat Database: Incidence-SEER 18 Regs Research Data+ Hurricane Katrina Impacted Louisiana Cases, Nov 2015 Sub (2000-2013)<Katrina/Rita Population Adjustment>-Linke. 2015. Rita population adjustment¿ e Linke 2015.
- Sorbye, H.; Welin, S.; Langer, S.W.; Vestermark, L.W.; Holt, N.; Osterlund, P.; Dueland, S.; Hofsli, E.; Guren, M.; Ohrling, K. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): the NORDIC NEC study. Annals of oncology 2013, 24, 152–160. [Google Scholar]
- Machida, N.; Yamaguchi, T.; Kasuga, A.; Takahashi, H.; Sudo, K.; Nishina, T.; Tobimatsu, K.; Ishido, K.; Furuse, J.; Boku, N. Multicenter retrospective analysis of systemic chemotherapy for advanced poorly differentiated neuroendocrine carcinoma of the digestive system. American Society of Clinical Oncology: 2012.
- Bernick, P.; Klimstra, D.; Shia, J.; Minsky, B.; Saltz, L.; Shi, W.; Thaler, H.; Guillem, J.; Paty, P.; Cohen, A. Neuroendocrine carcinomas of the colon and rectum. Diseases of the colon & rectum 2004, 47, 163–169. [Google Scholar]
- Smith, J.D.; Reidy, D.L.; Goodman, K.A.; Shia, J.; Nash, G.M. A retrospective review of 126 high-grade neuroendocrine carcinomas of the colon and rectum. Annals of Surgical Oncology 2014, 21, 2956–2962. [Google Scholar]
- Fujii, H.; Aotake, T.; Horiuchi, T.; Chiba, Y.; Imamura, Y.; Tanaka, K. Small cell carcinoma of the gallbladder: a case report and review of 53 cases in the literature. Hepato-gastroenterology 2001, 48, 1588–1593. [Google Scholar]
- Strosberg, J.R.; Cheema, A.; Weber, J.; Han, G.; Coppola, D.; Kvols, L.K. Prognostic validity of a novel American Joint Committee on Cancer Staging Classification for pancreatic neuroendocrine tumors. Journal of Clinical Oncology 2011, 29, 3044–3049. [Google Scholar]
- Garcia-Carbonero, R.; Capdevila, J.; Crespo-Herrero, G.; Díaz-Pérez, J.; Del Prado, M.M.; Orduña, V.A.; Sevilla-García, I.; Villabona-Artero, C.; Beguiristain-Gómez, A.; Llanos-Muñoz, M. Incidence, patterns of care and prognostic factors for outcome of gastroenteropancreatic neuroendocrine tumors (GEP-NETs): results from the National Cancer Registry of Spain (RGETNE). Annals of oncology 2010, 21, 1794–1803. [Google Scholar]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.-P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair–deficient cancer: results from the phase II KEYNOTE-158 study. Journal of Clinical Oncology 2020, 38, 1–10. [Google Scholar] [PubMed]
- Frizziero, M.; Kilgour, E.; Simpson, K.L.; Rothwell, D.G.; Moore, D.A.; Frese, K.K.; Galvin, M.; Lamarca, A.; Hubner, R.A.; Valle, J.W.; et al. Expanding Therapeutic Opportunities for Extrapulmonary Neuroendocrine Carcinoma. Clinical Cancer Research 2022, 28, 1999–2019. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Location of the primary tumor in all cases (local/regional and metastatic disease).
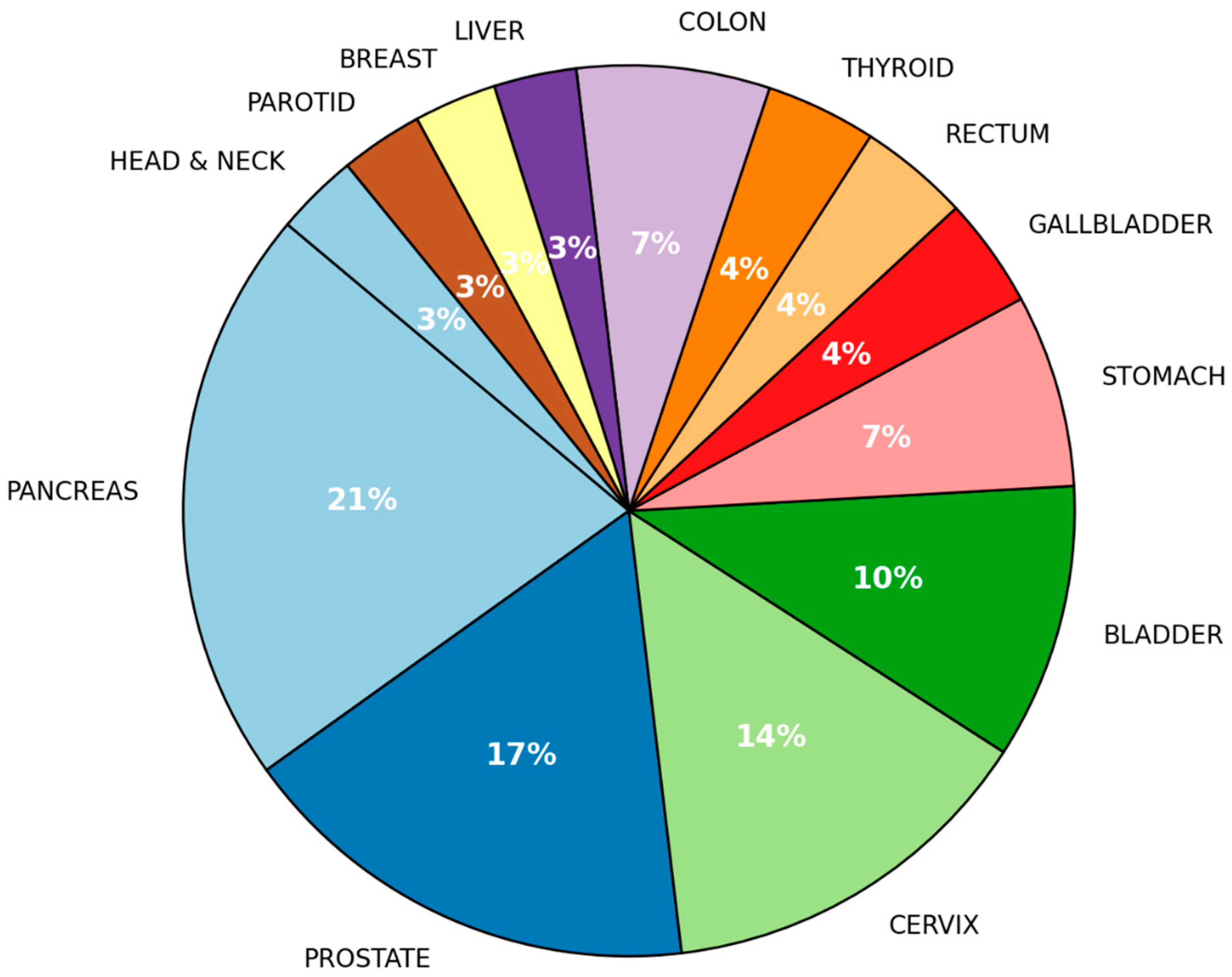
Figure 2.
Frequency of metastasis sites.
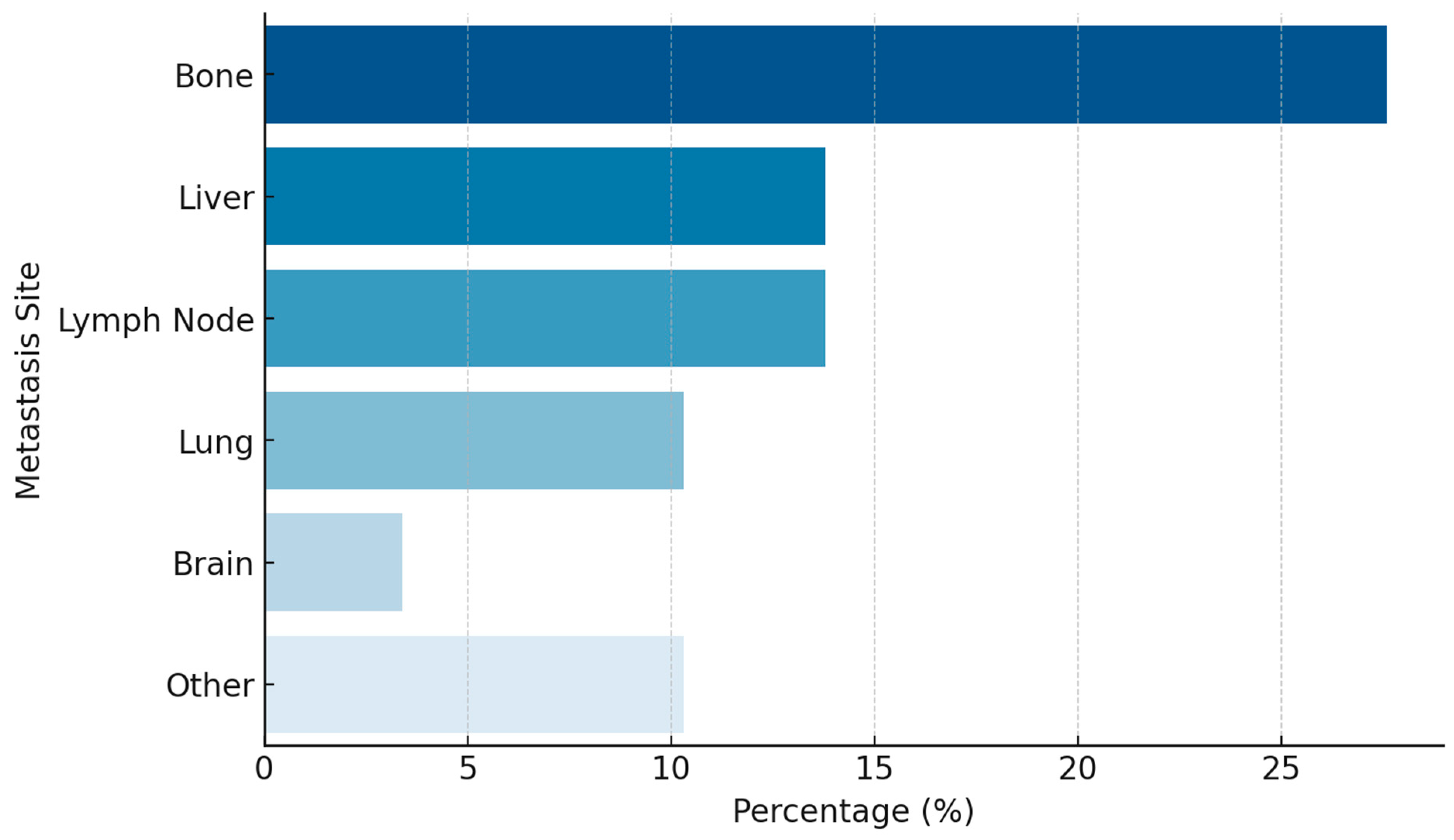
Figure 3.
Progression-Free Survival.
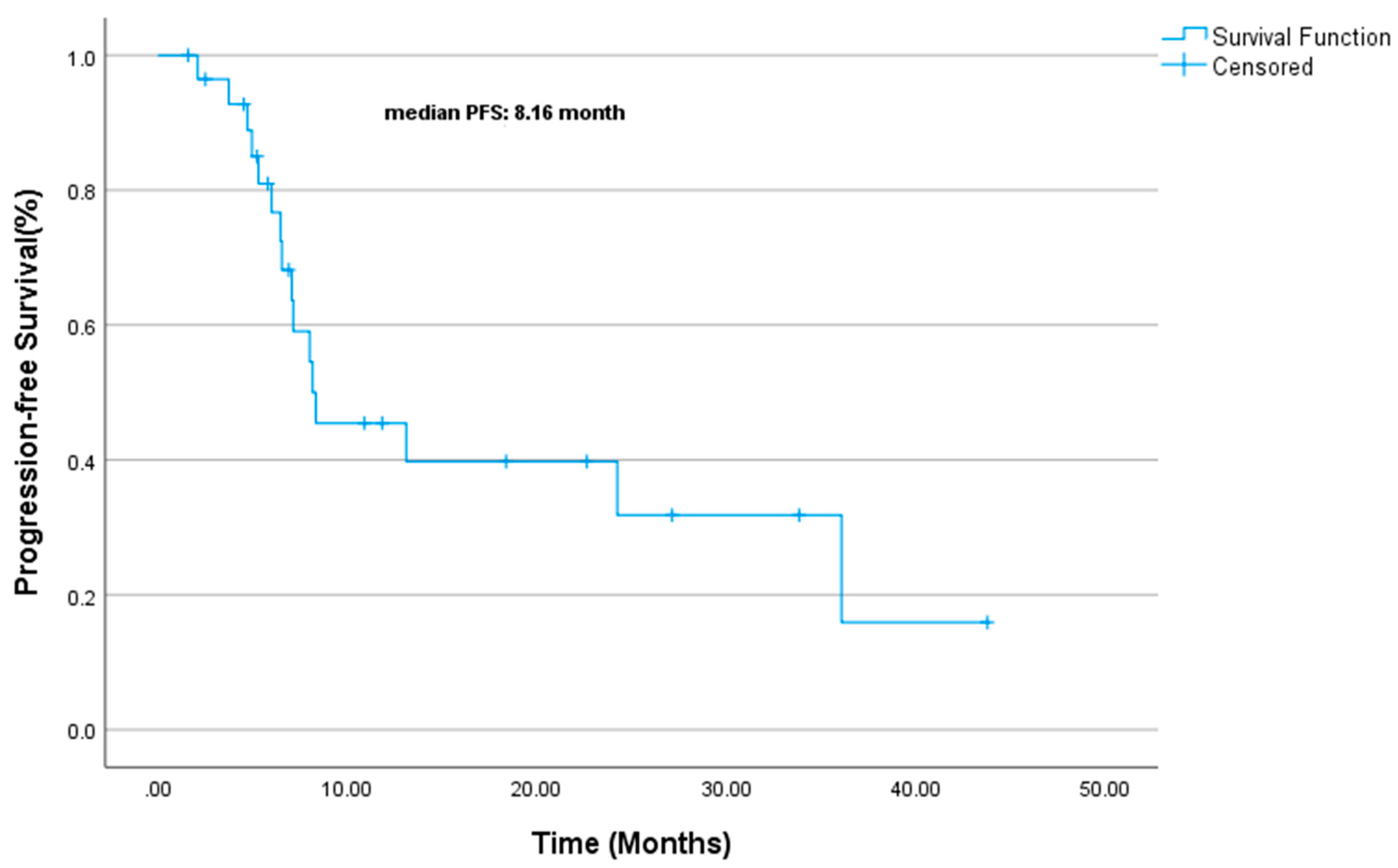
Figure 4.
Overall Survival.
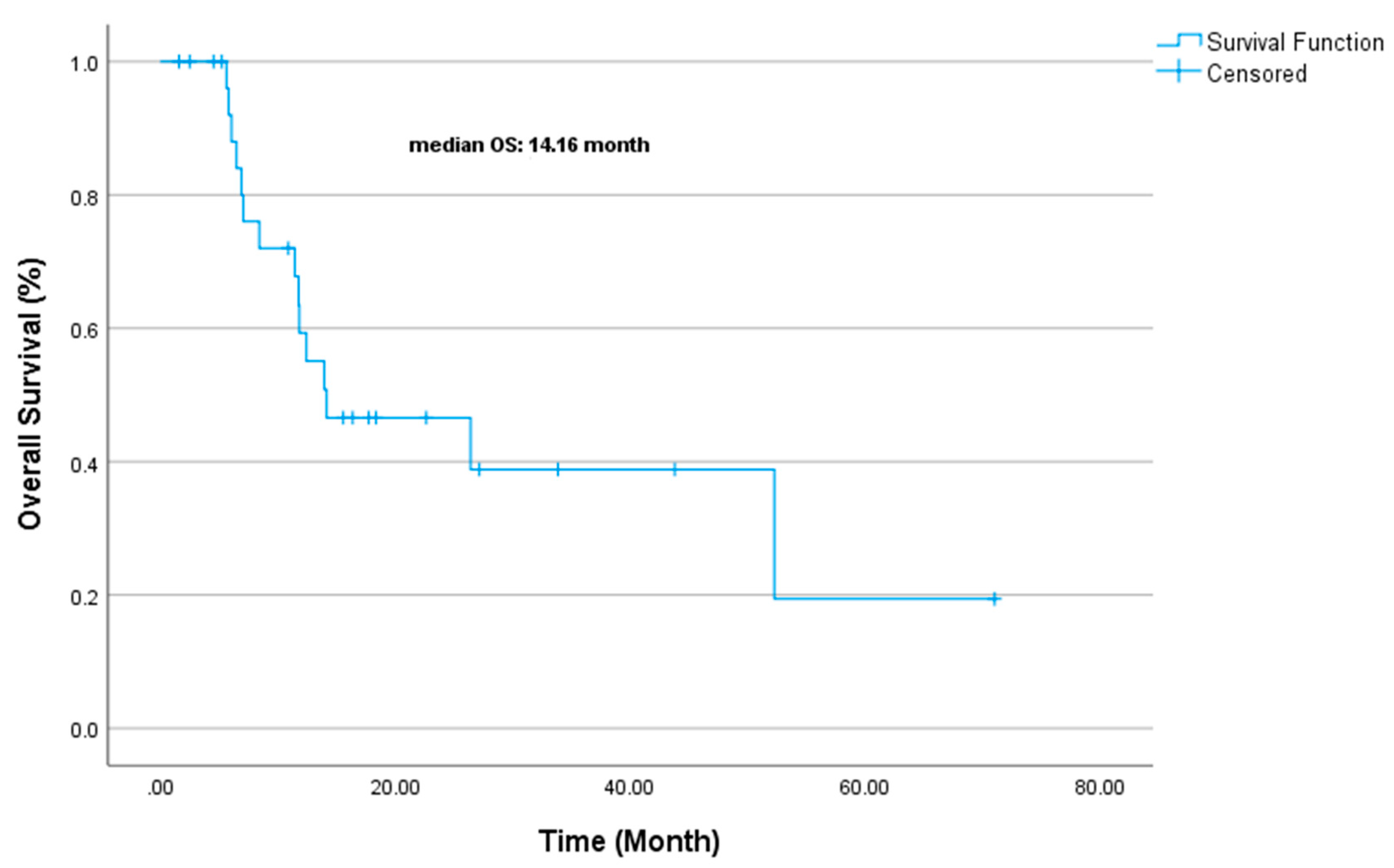

Table 1.
Baseline clinic and demographic characteristics of patients.
| Variable | (%) |
|---|---|
| Age | |
| Median Age (Range) | 60.14 (29-82) |
| ECOG PS | |
| 0 | 82.8 |
| 1 | 10.3 |
| 2 | 6.9 |
| Sex | |
| Female | 48.3 |
| Male | 51.7 |
| Smoking | |
| Yes | 31.0 |
| No | 69.0 |
| Stage at first diagnosis | |
| Localized | 10.3 |
| Locoregional | 34.5 |
| Metastatic | 55.2 |
| Ki-67 | |
| >80 | 75.0 |
| 60–80 | 25.0 |
| Surgery | |
| Yes | 31.0 |
| No | 69.0 |
| Curative RT | |
| Yes | 39.3 |
| No | 58.6 |
| Concurrent CRT | |
| Yes | 25.0 |
| No | 75.0 |
| Liver-Directed Therapy | |
| Yes | 6.9 |
| No | 93.1 |
| 1st Line Chemotherapy | |
| Cisplatin+Etoposide | 51.7 |
| Carboplatin+Etoposide | 48.3 |
| 2nd Line Chemotherapy | |
| Cisplatin+Etoposide | 6.9 |
| Irinotecan | 17.2 |
| Paclitaxel | 3.4 |
| CAPOX | 3.4 |
| 3rd Line Therapy | |
| Chemotherapy | 34.5 |
| Immunotherapy | 10.3 |
| CAPOX: Oxaliplatin plus capecitabine RT: Radiotherapy CRT: Chemoradiotherapy ECOG PS: Eastern Cooperative Oncology Group Performance Status | |
Table 2.
Treatment Response Rates by Therapy Line.
| Therapy Line | N (%) |
|---|---|
| 1st Line | |
| Complete Response (CR) | 12 (42.9%) |
| Partial Response (PR) | 11 (39.3%) |
| Progressive Disease (PD) | 5 (17.9%) |
| Objective Response Rate (ORR) | %82.1 |
| 2nd Line | |
| Partial Response (PR) | 3 (10.3%) |
| Stable Disease (SD) | 1 (3.4%) |
| Progressive Disease (PD) | 7 (24.1%) |
| 3rd Line | |
| Partial Response (PR) | 0(0%) |
| Stable Disease (SD) | 2 (6.9%) |
| Progressive Disease (PD) | 3 (10.3%) |
| Immunotherapy | |
| Partial Response (PR) | 0(0%) |
| Stable Disease (SD) | 1 (33.3%) |
| Progressive Disease (PD) | 2 (66.6%) |
Table 3.
PFS Analysis Results.
| Variable | PFS Duration (Median, Months) | Univariate p-Value | Multivariate HR (95% CI) | Multivariate p-Value |
| Gender | 0.747 | - | - | |
| Male | 8.3 mo. | |||
| Female | 8 mo. | |||
| Stage | 0.442 | - | - | |
| Local | 24.2 mo. | |||
| Locoregional | 8.1 mo. | |||
| Metastatic | 8 mo. | |||
| ECOG-PS | 0.005 | 1.452 (0.537–3.926) | 0.463 | |
| ECOG PS-0 | 8.1 mo. | |||
| ECOG PS-1 | 8.3 mo. | |||
| ECOG PS-2 | 2.1 mo. | |||
| Smoking Status | 0.539 | - | - | |
| Non-smoker | 8.1 mo. | |||
| Smoker | 7.1 mo. | |||
| Surgical History | 0.02 | 7.291 (1.212–43.862) | 0.03 | |
| No Surgery | 8 mo. | |||
| Surgery | NR | |||
| Concurrent CRT | 0.847 | - | - | |
| No Concurrent CRT | 8.3 mo. | |||
| Concurrent CRT | 8.1 mo. | |||
| First-line CT (Cis-Eto vs Carbo-Eto) | 0.182 | - | - | |
| Cis-Eto: | 13.1 mo. | |||
| Carbo-Eto | 7.1 mo. | |||
| Ki-67 | 0.032 | NE | 0.0 | |
| Ki67<80 | 36 mo. | |||
| Ki-67 ≥ 80: 8 mo. | 8 mo. | |||
| CT: Chemotherapy RT: Radiotherapy CRT: Chemoradiotherapy Cis-Eto: Cisplatin etoposide Carbo-Eto: Carboplatin Etoposide ECOG-PS: Eastern Cooperative Oncology Group Performance Status NR: Not Reached NE: Not Estimable | ||||
Table 4.
OS Analysis Results.
| Variable | OS Duration (Median, Months) | Univariate p-Value | Multivariate Exp(B) | Multivariate p-Value |
| Gender | 0.451 | - | - | |
| Male | 11.8 mo. | |||
| Female | 26.4 mo. | |||
| Stage | 0.520 | - | - | |
| Local | 52.2 mo. | |||
| Locoregional | 12.4 mo. | |||
| Metastatic | 11.8 mo. | |||
| ECOG-PS | 0.448 | 1.106 | 0.825 | |
| ECOG PS-0 | 13.9 mo. | |||
| ECOG PS-1 | NR | |||
| ECOG PS-2 | 6.5 mo. | |||
| Smoking Status | 0.418 | - | - | |
| Non-smoker | 26.4 mo. | |||
| Smoker | 11.7 mo. | |||
| Surgical History | 0.385 | 1.324 | 0.705 | |
| No Surgery | 11.8 mo. | |||
| Surgery | 26.4 mo. | |||
| Concurrent CRT | 0.581 | - | - | |
| No Concurrent CRT | 14.1 mo. | |||
| Concurrent CRT | 14.1 mo. | |||
| First-line CT (Cis-Eto vs Carbo-Eto) | 0.180 | 0.508 | 0.331 | |
| Cis-Eto: | 26.4 mo. | |||
| Carbo-Eto | 11.7 mo. | |||
| Ki-67 | 0.959 | 1.405 | 0.645 | |
| Ki67<80 | 26.4 mo. | |||
| Ki-67 ≥ 80: 8 mo. | 11.8 mo. | |||
| CT: Chemotherapy RT: Radiotherapy CRT: Chemoradiotherapy Cis-Eto: Cisplatin etoposide Carbo-Eto: Carboplatin Etoposide ECOG-PS: Eastern Cooperative Oncology Group Performance Status NR: Not Reached NE: Not Estimable | ||||
Table 5.
Survival Data of Patients with Metastatic Gastroenteropancreatic Neuroendocrine Carcinomas.
Table 5.
Survival Data of Patients with Metastatic Gastroenteropancreatic Neuroendocrine Carcinomas.
| Reference | No. of Patients | Cohort | Primary Site | Median PFS (months) | Median OS (months) | 2-Year Survival (%) | 3-Year Survival (%) |
|---|---|---|---|---|---|---|---|
| Yao 2008[5] | 2027 | All NEC (Including Lung) | Mixed | - | 5 (4.5-5.5) | - | - |
| SEER Program 2013[24] | 1389 | GEP-NEC | GEP | - | 5 (4.7-5.4) | 11 | 8 |
| Sorbye 2013[25] | 252 | GEP-NEC (Chemotherapy Treated) | GEP | - | 11 (9.4-12.6) | 14 | 9.5 |
| Sorbye 2013[25] | 53 | GEP-NEC (No Treatment) | GEP | - | 1 (0.3-1.8) | - | - |
| Machida 2012[26] | 258 | GEP-NEC (Chemotherapy Treated) | GEP | - | 11.5 | - | - |
| Bernick 2004[27] | 38 | Colorectal Small Cell NEC | Colon & Rectum | - | 10.5 (6.7-19) | 26 | 13 |
| Smith 2013[28] | 126 | Colorectal NEC | Colon & Rectum | - | 13 | 5 | - |
| Fujii 2001[29] | 53 | Gallbladder, Small Cell NEC (Chemotherapy Treated) | Gallbladder | - | 8 | 0 | - |
| Strosberg 2011[30] | 32 | Pancreatic NEC | Pancreas | - | 21 | - | - |
| Garcia-Carbonero 2010[31] | 85 | GEP-NEC | GEP | - | 1.7 | - | - |
| Celik et al. (2022)[22] | 47 | EP-NEC (Chemotherapy Treated) | Stomach (27.6%), Unknown Primary (23.4%), Pancreas (10.6%) | 5.83 (4.46-7.20) | 13.6 (9.01-18.18) | - | - |
| NEC, Neuroendocrin carcinoma CI, confidence interval GEP-NEC, gastroenteropancreatic neuroendocrine carcinoma SEER, Surveillance, Epidemiology, and End Results | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



