
Submitted:
27 February 2025
Posted:
28 February 2025
You are already at the latest version
Abstract
Exclusive breastfeeding (EB), feeding an infant solely breast milk, has been recommended worldwide, due to its health benefits for infants and mothers. However, EB rates remain low, due to several socio-demographic, occupational, and cultural factors. Our aim was to investigate the factors associated with EB amongst Arab mothers living in Israel: i.e., age, education, religiosity, employment status, and the number of children which impact breastfeeding practices. Data were collected through surveys from Arab mothers of different religious and geographical backgrounds. We found that older maternal age, higher levels of religiosity, and an increased number of children were positively associated with EB. Employment reduced EB. Muslim mothers were more likely to combine breastfeeding with formula; Christian and Druze mothers showed higher EB rates. Geographical disparities were also noted. This study highlights the complex interplay of socio-demographic and cultural factors that impact breastfeeding practices amongst Arab mothers in Israel, with significant implications for policy development and maternal support programs. We underscore the importance of incorporating religious and cultural considerations into breastfeeding promotion strategies. Public health initiatives should target support for working mothers by advocating extended maternity leave and breastfeeding-friendly workplace policies. Furthermore, community-based interventions should engage family members in supporting breastfeeding mothers.
Keywords:
exclusive breastfeeding
; Arab mothers
; religiosity
; maternal health
; breastfeeding duration
; cultural beliefs
; employment status
; socio-demographic factors
; child nutrition
; Israel
1. Introduction
The practice of exclusive breastfeeding (EB) from birth to four months of age is common worldwide. Health organizations, such as the World Health Organization (WHO) and the Israeli Ministry of Health, recommend EB up to 6 months of age as the ideal goal, which will be followed by the introduction of solid foods and continued breastfeeding. Before six months, infants are typically not yet developmentally ready to handle solid foods, thus, rendering breastfeeding the ideal source of nutrition at this stage. EB also provides natural antibodies which bolster the infant’s immune system.
The first two years of the baby’s life are critical, and proper nutrition is essential for proper growth and development (Black et al., 2008). Inadequate nutrition increases the risk of both short- and long-term morbidity and mortality, i.e., wasting (low weight for height), stunting (delayed growth), obesity, cognitive impairment, diminished future physical work capacity, and, in female infants, fertility problems (Black et al., 2008; Prado & Dewey, 2014; Ottolini et al., 2020). Moreover, poor early nutrition can lead to the development of unhealthy eating habits that may persist throughout life (Birch et al., 2007). According to data from the WHO and the World Bank, 6.8% of children under 5 years old suffer from wasting, and ~22% experience stunting. The majority of these cases occur in children from developing or third-world countries (mostly, Africa and Asia). However, these conditions are also present in developed countries, with prevalence rates of stunting and wasting at 4% and 0.4%, respectively. Globally, a common nutritional problem is food insecurity, defined as limited or uncertain availability of safe and adequate food or an unreliable ability to acquire food through socially acceptable means. In Israel, a developed country, ~21% of children suffer from food insecurity, with approximately half of these children experiencing severe food insecurity (World Health Organization, 2023).
Childhood obesity, on the other hand, is a more prevalent phenomenon found in developed countries: 7.6% vs. 3.4% in developing countries National Insurance Institute, 2021). Among breastfeeding’s numerous advantages for both infants and mothers is the reduced risk of obesity as well as development of an emotional bond/attachment between mother and infant. Moreover, there is a decreased risk of breast and ovarian cancer for the mother (Dieterich et al., 2013; Ip et al., 2009; Wallenborn et al., 2021). Studies have shown that breastfed infants have a 26% lower likelihood of suffering from obesity or overweight (Victora et al., 2016; Quigley et al., 2016; Rito et al., 2019).
Research has also indicated that EB offers additional benefits, including a reduced risk of mortality in infants due to sudden infant death syndrome (SIDS). A meta-analysis conducted in the USA found that the risk of SIDS was reduced by 45% in infants who were breastfed (either exclusively or partially); in infants breastfed for at least two months, the risk decreased by 62%, and in infants who were breastfed for a certain amount of time, by 73% (Hauck et al., 2011; Thompson et al., 2017). Meek & Noble found that EB may bestow a protective effect against the development of asthma, eczema, lower respiratory tract infections, and type 1 diabetes (Meek & Noble, 2022). Despite the advantages associated with EB, a significant percentage of women worldwide do not breastfeed.
Only three developed countries (USA, Spain, and France) have reported that >80% of mothers have ever breastfed Perez-Escamilla et al., 2023). In 2020, according to the Center for Disease Control’s (CDC) data from the USA, breastfeeding initiation rate was 83.1%, with significant differences observed across various socio-economic groups (90.1%, among women in the highest socio-economic versus 75.4% in the lowest socio-economic bracket). The breastfeeding initiation rate among university-educated women was 91.9%, compared to 72.5% who did not complete high school Centers for Disease Control and Prevention, 2023). These data indicate that only 45.3% of infants received EB at 3 months; 25.4% at 6 months of age (Centers for Disease Control and Prevention, 2023). According to the Global Breastfeeding Collective of the WHO and UNICEF, only 48% of infants under 6 months are EB (Global Breastfeeding Collective, 2023). To encourage breastfeeding, many hotlines for breastfeeding mothers have been set up internationally, i.e., the Australian Breastfeeding Association website, which enumerates the advantages of breastfeeding for both mothers and infants and offers help with related problems (Australian Breastfeeding Association website).
1.1. Breastfeeding Practice in Israel
A national health and nutrition survey conducted in Israel between 2019 and 2020 found that the percentage of women practicing EB for a duration of 4 to <6 months was 28.8% (Specht et al., 2018). In another survey conducted in Israel, it was reported that the initiation rate of breastfeeding was ~90%, for all women who began EB in the hospital. However, the rates of EB significantly declined during the postpartum period (during maternity leave). The survey indicated that the primary reason for discontinuing breastfeeding was the difficulty in breastfeeding, i.e., physiological issues and problems with milk supply (National Program for Nutrition and Health Surveys, 2019).
Various factors influence the duration of EB, i.e., demographic and biological, perceptions and beliefs, social, and hospital-related. Demographic factors include age (older women are expected to breastfeed more than younger women); education level (the higher the education, the greater the likelihood of EB); and income level (as income increases, the likelihood of breastfeeding also increases (Victora et al., 2016; Perez-Escamilla et al., 2023). Biological factors primarily relate to the ability to produce milk or a sufficient milk quantity. Moreover, research has shown that mothers who are obese at the time of pregnancy exhibit a lower likelihood of breastfeeding. Factors related to the mother’s perceptions and beliefs include feelings of self-efficacy (the higher the self-efficacy, the greater the likelihood of breastfeeding) (Meek & Noble, 2022); Perez-Escamilla et al., 2023).
Social factors include the mother’s employment status, duration of maternity leave, and support from her partner. Hospital-related factors include policies (such as rooming-in and early initiation of breastfeeding) (Zimmerman et al., 2022; Dieterich et al., 2022). It is essential to raise awareness as to the long-term importance of breastfeeding during the mother’s visits to well-baby clinics. The WHO, the American Academy of Pediatrics (AAP), and the Israeli Ministry of Health recommend EB for the first six months following the birth of the infant [Dieterich et al., 2022; WHO , 2022; Meek et al., 2020; Ministry of Health, 2021; Sundararajan & Rabe, 2021).
1.2. Religious Significance Attributed to Breastfeeding
In the Israeli Arab community (Islam, Christianity, and Druze), breastfeeding holds a significant symbolic value due to religious reasons, hence, we focused on three groups: a non-conservative, conservative, and religious group. A majority of Arab women do not participate in the labor force remaining at home to raise their children. Consequently, breastfeeding is perceived as a fundamental and important issue, similar to global trends, as a result of its health benefits for both infants and mothers. However, also within this community, cultural, social, and economic factors affect the attitudes and practices related to breastfeeding.
In terms of traditional and religious significance, breastfeeding is regarded in Islam as a blessed duty. The Quran specifies the duration of breastfeeding in the verse: “Mothers may breastfeed their children for two complete years for whoever wishes to complete the nursing” (Surat Al-Baqarah [2:233]) (The Noble Qur’an. Surat Al-Baqarah). Breastfeeding is considered a religious obligation of the mother towards the child; however, the child may be transitioned to artificial feeding, if necessary for the child’s welfare . If a mother is unable to breastfeed her child, another woman (wet nurse) is appointed to the role and establishes a bond of “milk kinship” between the infant, wet nurse, and family, a relationship that is recognized in Islam and precisely defined by religious law, giving breastfeeding a spiritual value.(Sivertsev, 2022).
In Christianity, breastfeeding symbolizes maternal care, love, and the spiritual grace conferred by both the mother and the Church. It also serves as a symbol of the spiritual relationship between the believer and the Church. In the Catholic tradition, Mary is often portrayed as the ideal mother. Images of Mary breastfeeding the infant Jesus are perceived as a representation of how she provides life to her son, both physically and spiritually (Mehrpisheh, et al. 2020). In the Druze community, breastfeeding is perceived as an essential part of raising a child, encompassing both physical and cultural values . Similar to many other cultures, breastfeeding is considered an integral part of a mother’s responsibility towards her child, signifying closeness and love (Alchalel et al., 2024).
1.3. Family and Social Factors
In many Arab families, regardless of religious beliefs, there is strong support for breastfeeding from extended family members, such as grandmothers and aunts, who provide guidance on the benefits and techniques of breastfeeding. There is often encouragement to breastfeed for extended periods, and in some cases, even beyond the first year of the child’s life. However, the level of familial support and influence may vary across families. Furthermore, various social factors also impact breastfeeding, i.e., education, age, socio-economic status, ethnic background, health, and cultural beliefs. Socio-economic status also plays a pivotal role. For example, in the United States and the United Kingdom, non-white ethnic groups, particularly, those of Caribbean descent, tend to have lower breastfeeding rates. Cultural beliefs, in particular, exert a significant influence on the likelihood of breastfeeding (Dorri et al., 2022).
Because breastfeeding in the Israeli Arab community is regarded as a key element with significant health, cultural, and religious value, research has reported a steady increase in breastfeeding rates among Israeli Arab women, with studies showing that in the initial months following childbirth, breastfeeding rates rise to between 85% and 90%. Among Muslim women, there is a tendency to breastfeed for extended periods of time, sometimes up to a year or beyond (Mehrpisheh et al., 2020; Alchalel et al., 2024; Dorri et al., 2022; Arif et al., 2021).
Breastfeeding rates among Christian Arab women are lower than among Muslim women, yet, above the national average. Research has shown that the breastfeeding rate among Christian women ranges from 70% to 80% during the initial months postpartum, with a gradual decline, thereafter, similar to trends observed in other populations [34]. Furthermore, among Druze women, breastfeeding rates are also high, reaching ~85% to 90% in the months following childbirth. Similar to their Muslim counterparts, Druze women perceive breastfeeding as having significant cultural and communal value. Nonetheless, there is a decline in breastfeeding rates associated with the adoption of modern lifestyles and economic pressures, i.e., the necessity to return to work (Alchalel et al., 2024; Dorri et al.,2022; Arif et al., 2021; Laksono et al., 2021).
Overall, breastfeeding rates are relatively high across all groups, with the highest rates observed among Druze women, followed by Muslim women, and lastly, Christian women. There is a general trend of declining breastfeeding rates over time, correlated with the increasing complexity of modern life. The relationship between poverty, women’s occupations, and EB has been extensively studied. Health-related initiatives, such as the WHO Code and the Baby-Friendly Hospital Initiative have addressed these factors [35]. Analyzing economic gradient data can further clarify the impact of education and occupation on breastfeeding trends (Carandang et al., 2021).
Therefore, the objective of this study was to examine the impact of socio-demographic, occupational, and religious characteristics on the rates of EB among Israeli Arab mothers (Muslim, Christian, and Druze). We investigated how factors such as age, education, marital status, income level, and profession affect a mother’s decision to EB. Additionally, we explored the relationship between the mothers’ level of religiosity and EB rates, endeavoring to understand the contributions of these factors to the duration and/or continuation of EB and related public health policies.
The research hypotheses were:
- H1: As the mother’s age increases, the likelihood of EB and its duration increases.
- H2: The more previous births (i.e., children), the likelihood of EB and its duration increases.
- H3: There are differences in the rate of EB and its duration based on ethnic group affiliation and geographical region.
- H4: As the mother’s education level increases, the likelihood of EB and its duration increases.
- H5: As the mother’s religiosity level increases, the likelihood of EB and its duration increases.
- H6: There are differences in the rates of EB and its duration based on the type of breastfeeding instructional trainings/courses the mother had received.
- H7: Working reduced the likelihood of both EB and its duration, further decreasing as the workload (scope) increases.
- H8: An association exists between the mother’s education level and the factors which foster breastfeeding and those that lead to its cessation.
While hypotheses H1-H4 addresses aspects that have been studied to some extent in the existing literature, they remain integral to our study because they provide validation of previously observed trends among the underrepresented population of Arab mothers in Israel. Furthermore, they allow for a comparative analysis to assess whether these well-documented relationships hold within our specific sample or show unique patterns affected by religiosity, employment status, or regional factors, thus, serving as a foundation for understanding the broader interplay of factors crucial for interpreting findings from the newer hypotheses (H5-H8) and ensuring a comprehensive analysis.
2. Methods
2.1. Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the Ramat Gan Academic College, approval code #2023-1010, approval date: July 20, 2023. Part I of Appendix A: Informed Consent Form for Online Studies, explains to each participant who answered the questionnaire that “by clicking the ‘I agree’ button, you express your consent to participate in the study”. Thereby, every respondent to the questionnaire gave her informed consent (Appendix A for Informed Consent Form).
2.2. Participants
The sample consisted of 274 married Israeli Arab women between the ages of 21-48 (M = 31.05, SD = 5.21). Of these, 186 (67.9%) respondents were Muslim, 40 (14.6%) Christian, and 48 (17.5%) Druze. Their religiosity level ranged from 1 to 5 ( M = 4.55 and SD = 0.74, Cronbach’s Alpha Coefficient, α = .83), indicating a considerably religious participant group. Most lived in the north (80.3%), several from the south (12.85%) and the rest from the center of the country (6.9%). Education-wise, more than half were academics (58.4%); 9.9% did not finish high-school; 23.4% completed high-school, and 8.4% had learned in a tertiary education setting.
Workwise, most were salaried part-/full-time employees (64.2%), 29.6% were unemployed, and the rest, self-employed (6.2%). Some participants did not work prior to the current birth (30.7%), whereas, 29.6%, worked full time (100%), 24.1%, worked 75%, 12% worked 50%, and 3.6% worked 25%. When asked, 37.2% reported that they planned on returning to work after giving birth, 28.5% had already returned to work, 8.8% stated that they would not return, and 25.5% were uncertain. Moreover, when asked, the respondents declared that they planned to return to work when their baby reached the age of: (1) One month (0.4%); (2) 2 months (0.4%); (3) 3 months (7.3%); (4) 4-6 months (15%); (5) 6 months and above (40.9%); 36.1% stated that they would not return to work. Household-wise, 38.3% had had no children before their recent delivery, 19.3% had only one child prior to their recent delivery, 17.5% had two children, and 24.8%, three children. Typically, the participants housed one more individual in their home (2.2%), 2 individuals (8%), 3 individuals (23.4%), and > 4 (66.4%).
2.3. Measures
The research questionnaire was based on a survey from the local National Center for Disease Control (ICDC) reporting on baby nutrition. The questionnaire was then approved by five experts in the field, and translated into Arabic (the native language of the participants). This was done to ensure maximum accessibility and more accurate and representative responses. Prior to distributing the survey, a pilot questionnaire which had been answered by 40 individuals was collected in order to assess the questionnaire. Subsequently, minor changes were made.
The survey comprised three sections: (1) socio-demographical information (i.e.,., age, marital status, educational level); (2) baby nutrition-related questions (i.e.,., type/method of feeding, duration of breastfeeding, instructional training regarding breastfeeding); and (3) the impact of factors that either foster or halt breastfeeding habits (Appendix A).
2.4. Procedure
The target population for this study were Arab women (Muslim, Christian, and Druze) from the age of 18, who had given birth within the past year and breastfed their infants for at least four months postpartum. The research tool was a questionnaire composed by a team of family health nurses from the Israeli Ministry of Health and validated by experts in the field of breastfeeding: three family health nurses and two family health specialists. The questionnaire was originally written in Hebrew and translated into Arabic, then back translated and reviewed by translators who specialize in questionnaire language to ensure that it was easy to understand. The initial sample included questionnaires filled in by 300 participants; however, 26 questionnaires were excluded due to incomplete responses. Consequently, the final sample comprised responses from 274 participants who met the predetermined inclusion criteria. These participants were drawn from three different regions of Israel (north, central, and south) and represented a variety of age groups and socioeconomic backgrounds.
The sampling method utilized a snowball approach, wherein, participants assisted the researchers in recruiting other potential participants through their personal networks. Additionally, the questionnaire link was made available online, and physical copies were distributed by well-baby clinics (Tipat Chalav) nurses to breastfeeding women. Exclusion criteria were a minimum age of 18, having given birth within the year and breastfed the infants for at least four months. The researchers had no prior relationship or familiarity with any of the participants, all of whom received detailed information about the study. Anonymity and confidentiality were assured, and participants were informed that their involvement would not provide any personal benefits or advantages but, would contribute to the advancement of general knowledge in this area of research.
There were no known risks associated with participation in the study; however, as with any online activity, there was a potential risk of privacy breaches. Researchers made every effort to mitigate this risk by ensuring that the questionnaires were completed anonymously, with personal details used solely for research purposes.
Participants were informed that additional information could be obtained from the Ethics Committee via an inquiry form at the conclusion of the study. The research team could also be contacted through the email address provided in the questionnaire. Participants retained the right to discontinue the survey at any stage. Informed consent was explicitly obtained through a designated question at the beginning of the survey. Only after providing their informed consent could they access the questionnaire link and proceed to complete the survey.
2.5. Data Analysis
Statistical analyses were performed using the SPSS-PC (v28) Statistical Package. Prior to the analysis, data cleaning and distribution characteristics including tests of normality were examined. Descriptive statistics were used to describe the sample. The significance level was set at p < .05.
3. Results
3.1. Hypotheses Testing
In order to test hypothesis H1, the assessment of age differences between: (1) the three different breastfeeding methods (i.e., complete reliance on baby food and/or supplements, EB, or integrated/combined EB and baby food) and (2) breastfeeding duration, one-way analyses of variance (one-way ANOVAs), were employed.
In assessing the association between age and breastfeeding methods (exclusive; N =165, M = 31.73, SD = 4.76/combined; N =66, M =30.00, SD = 4.92/baby food; N =43, M = 0.05, SD = 7.00), the results indicated a significant main effect: F(2, 271) = 3.60, p <.05. Hence, in order to gauge the source of these significant differences, Tukey’s HSD post-hoc tests were performed, revealing only that those who preferred EB were slightly older than those who opted for combined breastfeeding (p <.05). No other significant differences were discovered between these groups.
In assessing the association between age and breastfeeding duration during the last 4 months (did not breastfeed at all; N =19, M =28.95, SD = 3.52/up to 1 month; N =10, M =27.20, SD = 4.61/up to 2 months; N =6, M =27.33, SD =5.05/up to 3 months; N =25, M =32.20, SD = 8.73/up to 4 months; N =20, M =28.45, SD =5.83/above 4 months; N =194, M =31.69, SD = 4.46), the results indicated a significant main effect: F(5, 268) =4.40, p <.01. In order to gauge the source of these significant differences, Tukey’s HSD post-hoc tests were performed, revealing that those who breastfed for >4 months were slightly older than those who did so up to 4 months (p <.05) and up to 1 month (p <.05). No other significant differences were discovered between these groups.
In order to test hypothesis H2, the assessment of the association between the number of children prior to the recent delivery and (1) the three different breastfeeding methods (i.e., only baby food, EB, integrated/combined breastfeeding) and (2) breastfeeding duration, chi-square tests were performed. Statistically significant differences were found among the different breastfeeding methods: χ2 (6, N =274) =41.15, p <.01, rc =.27. Results indicated that: (1) those with no children before the current delivery, preferred baby food or combined breastfeeding; (2) those with 1 child did not have a specific preference; (3) those with 2 children preferred combined breastfeeding; and (4) those with 3 children preferred EB. Statistically significant differences were also found among the different breastfeeding methods: χ2 (6, N =274) =41.15, p <.01, rc =.27.
In order to test hypothesis H3, the assessment of the association between ethnic affiliation (Muslim-Arabs/Christian-Arabs/Druze) or geographic region (north, center and south of the country) and (1) the three different breastfeeding methods (i.e., only baby food, EB, integrated/combined breastfeeding) and (2) breastfeeding duration, chi-square tests, were performed.
Statistically significant differences were found among the different ethnic groups: χ2 (4, N =274) =31.93, p <.01, rc =.24. Results indicated that: (1) Muslim Arab women preferred baby food or combined breastfeeding; whereas, (2) Christian Arabs and (3) Druze both preferred EB. Statistically significant differences were found among the different ethnic groups: χ2 (10, N =274) =22.73, p <.01, rc =.20. Results indicated that: (1) Muslim Arab women preferred to breastfeed for up to 3 and 4 months; whereas (2) Christian Arabs and (3) Druze both preferred to breastfeed for >4 months. Statistically significant differences were found among the different regions: χ2 (4, N =274) =14.70, p <.01, rc =.16. Results indicated that: (1) those living in the north of the country preferred EB; (2) those living in the center preferred to use baby food; and (3) those living in the south preferred combined breastfeeding. Statistically significant differences were found among the different regions: χ2 (10, N =274) =25.36, p <.01, rc =.22. Results indicated that: (1) those living in the north of the country preferred to breastfeed for >4 months; (2) those living in the center did not have a specific preference; whereas (3) those living in the south preferred to breastfeed up to 3 and 4 months.
In order to test hypothesis H4, the assessment of the association between educational level (non-academic/academic) and (1) the three different breastfeeding methods (i.e., only baby food, EB, integrated/combined breastfeeding) and (2) breastfeeding duration, chi-square tests were performed. No statistically significant differences were found among the educational levels of the groups in relation to breastfeeding methods: χ2 (2, N =274) =4.01, p >.05, rc =.12 and no statistically significant differences were found among the educational levels of the groups in relation to breastfeeding duration: χ2 (2, N =274) =2.49, p >.05, rc =10.
In order to test hypothesis H5, the assessment of religiosity level differences between (1) the three different breastfeeding methods (i.e., only baby food, EB, integrated/combined breastfeeding) and (2) breastfeeding duration, one-way analyses of variance (one-way ANOVAs), were employed.
In gauging the association between religiosity level and breastfeeding methods (exclusive; N = 65, M =4.70, SD = 0.65/combined; N =66, M =4.37, SD =0.71/baby food; N =43, M =4.27, SD =0.97), the results indicated a significant main effect: F(2, 271) =8.70, p <.01. Hence, in order to reveal the source of these significant differences, Tukey’s HSD post-hoc tests were performed, finding that those who preferred EB reported higher religiosity levels than (1) those who preferred combined breastfeeding (p <.01) and (2) only baby food (p <.01). No other significant differences were discovered between these groups.
In gauging the association between religiosity level and breastfeeding duration during the last 4 months (did not breastfeed at all; N =19, M =3.97, SD =1.24/up to 1 month; N =10, M = 4.27, SD =1.05/up to 2 months; N =6, M =3.61, SD =0.83/up to 3 months; N =25, M =4.55, SD = 0.48/up to 4 months; N =20, M =4.35, SD =.90/above 4 months; N =194, M =4.67, SD =0.61), the results indicated a significant main effect: F(5, 268) =6.54, p <.01. In order to reveal the source of these significant differences, Tukey’s HSD post-hoc tests were performed, indicating only that those who breastfed for >4 months reported a higher religiosity level than (1) those who preferred not to breastfeed (p <.01) and (2) those who breastfed up to 2 months (p <.01). No other significant differences were discovered between these groups.
In order to test hypothesis H6, the assessment of the association between prior instruction(s) received regarding breastfeeding (did not receive any/group instructional program/personal or private instructional program) and (1) the three different breastfeeding methods (i.e., only baby food, EB, integrated/combined breastfeeding) and (2) breastfeeding duration, chi-square tests were performed. No statistically significant differences were found among the instructional groups in relation to breastfeeding methods: χ2 (4, N =274) =4.28, p >.05, rc =.09. In addition, no statistically significant differences were found among the instructional groups in relation to breastfeeding duration: χ2 (10, N =274) =7.90, p >.05, rc =.12.
In order to test hypothesis H7, the assessment of the association between employment status (unemployed/part- or full-time salaried employee/self-employed) and (1) the three different breastfeeding methods (i.e., only baby food, EB, integrated/combined breastfeeding), chi-square tests were performed. No statistically significant differences were found among the different breastfeeding methods: χ2 (4, N =274) =17.08, p <.01, rc =.18. Results indicated that: (1) those who were unemployed preferred EB; (2) those who were self-employed preferred to opt for baby food only or combined breastfeeding; and (3) salaried employees preferred combined breastfeeding. However, in testing whether these results changed under different employment/job percentage (0% or unemployed/part-time as 25% job/50%/75%/full-time with 100% employment), it was discovered that the results (previous paragraph) did not change at all based on the job scope, and stayed relatively similar across all the work percentage groups, respectively: (1) χ2 =4.57, p >.05, for the unemployed group; (2) χ2 =4.02, p >.05, for the 25% part-timers; (3) χ2 =0.49, p >.05, for the 50% part-timers; (4) χ2 =6.35, p >.05, for the 75% part-timers; and (5) χ2 =1.96, p >.05, for the full-timers.
Lastly, in order to test hypothesis H8, the assessment of the differences between educational levels (non-academic/academic) on (1) the reasons for fostering the mothers to breastfeed their infant and (2) the reasons leading them to stop breastfeeding, descriptive statistics, independent-samples t-tests and chi-square tests were performed. Notable, the 9 reasons fostering the mothers to breastfeed their infant were rated on a 3-point Likert-type scale (0 =did not influence my decision to breastfeed my baby; 1 =somewhat influenced my decision; 2 =influenced my decision a great deal). Moreover, the 6 reasons leading to a halt in breastfeeding were calculated on a dichotomous scale (0 = was not a reason to stop breastfeeding; 1 = was a reason to stop breastfeeding). The 3-point Likert scale was chosen for its simplicity and clarity and to minimize participant confusion and response fatigue, thus, enabling clear categorization of levels of influence,
Depicted in Figure 1 are the reasons, in a descending order, based on the mean scores, favoring breastfeeding. As can be seen, the two most prominent participant-reported reasons favoring breastfeeding were: (1) wanting to maintain the baby’s health (M =1.87); and (2) wanting to develop a more intimate relationship/attachment with the baby (M =1.84).
Portrayed in Figure 2 are the participant-reported reasons leading to a halt in breastfeeding in a descending order based on relative frequencies. “Reported reasons” was used to describe the participants’ self-identified reasons for ceasing breastfeeding, as collected through the survey instrument. This phrasing reflects the subjective nature of the responses provided by the participants. As can be seen, the most prominent reported reason to halt breastfeeding was the quality of the milk/the amount of milk produced by the mother herself (50.7%).
Independent-sample t-tests revealed several significant differences between academics and non-academics for fostering breastfeeding. The results are presented in Table 1. As can be learned from the statistically significant effects: (1) non-academics were more influenced by their family members to breastfeed than academics; (2) academics were more influenced by instructional training programs than non-academics; (3) non-academics were more influenced by successful previous breastfeeding than academics; (4) non-academics were more influenced by financial constraints (i.e., EB does not require ‘special’ funds) than academics; and (5) academics tended to be more influenced by information obtained from the literature, internet or media.
4. Discussion
EB offers significant health benefits for both infants and mothers, applicable in both the short- and long term. Breast milk provides essential nutrition and protection against infections and diseases (Adokiya et al., 2023), containing antibodies, cytokines, and antimicrobial compounds that support the infant’s immune system and facilitate its development. Breastfeeding reduces the risk of SIDS, with the risk being even lower with EB. Furthermore, EB protectively affects the development of asthma, eczema, type 1 diabetes, and other diseases. Infants who are breastfed have a lower risk of obesity. Furthermore, studies have shown that women who breastfeed, experience lower incidence rates of breast and ovarian cancer (Lokossou et al., 2022; Gavine et al., 2022; Gianni et al., 2019).
In 2003, the WHO recommended EB for infants up to 6 months of age (Gavine et al., 2022; Gianni et al., 2019). In Israel, a survey showed that the breastfeeding initiation rate is ~90%, with all women who began breastfeeding in the hospital reporting practicing EB. However, EB rates dropped significantly during maternity leave, largely due to challenges such as milk supply issues and technical difficulties with breastfeeding (Zimmerman et al., 2022).
According to data from the 2nd National Health and Nutrition Survey, the percentage of women practicing EB at 4 to 6 months postpartum was only 28.8% (National Program for Nutrtion and Health Surveys, 2020; Ministry of Health, 2023). Following these findings, a quality indicator was established within Israel’s National Program for Quality Indicators in Well-Baby Clinics (“Tipat Chalav”), focusing on “the rate of women practicing EB up to 4 months.” Data from 2022 showed that the national rate for EB up to 4 months was 22%, whereas, the rate among Arab Israeli women was even lower, 14% (Alchalele et al., 2024). These findings highlight Arab Israeli women as a group at an increased risk for lower rates of EB. This population’s specific characteristics and challenges should be investigated to better understand and address the factors affecting EB within this demographic, in line with the quality index’s goal of improving early nutrition and breastfeeding rates across Israel.
The largest Arab population in Israel is concentrated in the Northern District, towns and villages. Arab citizens of Israel, who are primarily Muslim, Christian, and Druze, make up 21% of the overall population of Israel (Central Bureau of Statistics, 2020). The current study emphasizes the complex effects of religious beliefs, socio-demographic factors, and cultural norms on breastfeeding patterns among Arab mothers in Israel. These findings provide insights into the key factors shaping breastfeeding behavior, including religiosity, education, age, number of children, employment, and family support.
To elaborate, one of the central findings of this study is the strong association between high levels of religiosity and longer durations of EB. This finding aligns with the religious traditions in Islam, Christianity, and Druze communities, who recommend breastfeeding and regard it as a health and spiritual obligation of the mother towards the child. The religious value attributed to breastfeeding serves as a significant motivator for its continuation, particularly, in religious communities where faith plays a central role in daily life. This finding underscores the powerful impact of religious beliefs on the health of both the mothers and infants.
As the mother’s age increases, the likelihood of EB and its duration increases. Based on the data analyzed herein, we found that the relationship between the mother’s age and breastfeeding was significant. Older mothers tended to practice EB more often and for longer periods of time than younger mothers, as evidenced by the ANOVA findings showing significant differences in breastfeeding methods and duration between the different age groups. The post hoc analysis further confirmed that mothers who practiced EB were slightly older than those who used combined feeding methods, thus suggesting that older mothers may have more experience, patience, or access to resources that encourage EB. Moreover, as the mother has had more previous births (i.e., more children), the likelihood of EB and its duration increases.
Chi-square tests revealed statistically significant differences in breastfeeding practices based on the number of children a mother had birthed before her recent delivery. Mothers with more children, particularly, those with three or more children, showed a stronger preference for EB compared to mothers with fewer or no prior children. This could be attributed to increased confidence and experience in breastfeeding as a mother has more children, as well as greater familiarity with overcoming initial breastfeeding challenges.
Furthermore, differences were found relating to the rate of EB and the duration of breastfeeding based on belonging to an ethnic group and/or geographic region. Ethnic and regional differences were observed to statistically and significantly impact both breastfeeding methods and duration. Muslim Arab mothers were more likely to combine breastfeeding with baby formula, whereas, Christian and Druze mothers favored EB. Geographically, mothers from northern Israel were more likely to practice EB compared to those from the central or southern regions. These differences most likely reflected cultural and religious practices, as well as access to breastfeeding support services that vary by region and ethnicity.
Moreover, as the educational level of the mother increased, the probability of EB and its duration increased. Contrary to expectations, the relationship between education level and breastfeeding was not as strong as hypothesized. Chi-square tests indicated no statistically significant difference between education levels and breastfeeding methods or duration. However, the effect of education may be more pronounced during the initiation phase, and less so in the continuation phase. Other factors such as family support and employment status might play a larger role in the continuation of EB over time.
Furthermore, as the mother’s level of religiosity increased, the likelihood of EB and its duration increased. The study found a significant association between higher religiosity and EB. Mothers with higher levels of religiosity were more likely to practice EB and for longer durations, thus, reflecting the religious beliefs in the Arab Muslim, Christian, and Druze communities that encourage breastfeeding as a spiritual and health-related obligation. These findings underscore the importance of integrating religious considerations into public health strategies that aim to promote breastfeeding.
However, as opposed to our hypothesis, no statistically significant differences were found as to the type of breastfeeding training mothers received and their breastfeeding methods or duration. Whereas, breastfeeding courses and training may provide initial support, they did not seem to affect long-term breastfeeding behavior in this sample, hence, suggesting that while training may help with initiation, other factors such as family support, personal experience, and cultural norms may play a more substantial role in sustaining EB.
In line with our other hypotheses, working reduced the likelihood of both EB and its duration, further decreasing as workload (volume) increased. The results indicated that employment status significantly affected breastfeeding practices. Unemployed mothers were more likely to practice EB, whereas, mothers who were employed, especially, those with full-time jobs, tended to opt for combined feeding methods. Employment-related factors such as lack of time and unsupportive workplace conditions contributed to early cessation of breastfeeding. These findings highlight the need for workplace policies that support breastfeeding, such as extended maternity leave and on-site breastfeeding facilities.
There is also the relationship between the mother’s level of education and the factors that foster breastfeeding or lead to its termination. Education level played a role in the reasons for fostering or halting breastfeeding. Non-academic mothers were more likely to be influenced by family members and financial constraints, whereas, academic mothers were more likely to be influenced by breastfeeding literature and medical advice. Academic mothers were more likely to cite fatigue, lack of time, or work-related issues as reasons for stopping breastfeeding, thus, indicating the importance of targeted interventions addressing the specific challenges faced by working mothers.
We found significant importance in familial support, particularly, the roles of grandmothers and older women within the family in encouraging breastfeeding. In the Arab society, where strong familial support networks exist, this encouragement plays a central role in preserving traditional breastfeeding patterns, thus, underscoring the importance of community intervention programs that include family members as part of the breastfeeding education process, thus, enabling a more comprehensive support system for breastfeeding.
We identified several challenges that led to the cessation of breastfeeding, including difficulties in milk supply, fatigue, and the pressure of returning to work. These challenges are particularly pronounced among mothers with lower levels of education, highlighting the need for targeted interventions to provide both practical and emotional support for continued breastfeeding.
In summary, this study has provided evidence supporting most of the hypotheses, particularly, those related to age, number of children, religiosity, and employment status. Yet, the effect of educational level and breastfeeding training on breastfeeding practices was less pronounced than expected, suggesting the need for further research and targeted interventions to promote long-term EB.
4.1. Policy Recommendations
Our findings emphasize the need to integrate religious and cultural factors into breastfeeding promotion programs within religious communities. Healthcare professionals should be aware of the religious and cultural significance of breastfeeding and provide support to mothers in alignment with their beliefs. As such, encouraging EB should commence early in the pregnancy, during hospitalization, and continue after discharge within the community. This can be achieved through resource utilization for both group and individual guidance, facilitating mother-infant proximity post-delivery, thus, empowering mothers to enhance their self-efficacy in continuing breastfeeding. Furthermore, raising awareness among mothers and their surroundings as to the benefits of maintaining EB, as well as the drawbacks of premature cessation, will aid in adopting health-promoting behaviors through breastfeeding and prevent its early discontinuation.
Collaborative efforts should be established among all members of the healthcare team (physicians, nurses, dietitians, and social workers) and workplaces to implement supportive breastfeeding processes, with the all-encompassing goal of safeguarding public health. Policies that allow for flexible work arrangements, longer maternity leave, and physical conditions that facilitate breastfeeding can ease the burden on mothers and encourage the continuation of breastfeeding.
The current research suggests that breastfeeding patterns among Arab mothers in Israel are influenced by a combination of religious beliefs, social factors, and demographic characteristics. Addressing existing challenges, particularly, in the workplace and the lack of professional support, may lead to improved breastfeeding rates and positively impact the health of both mothers and infants.
4.2. Limitations and Future Research Recommendations
The sampling method employed in the study utilized a snowball sampling technique; participants recruit additional participants from their personal networks. This method may introduce bias in sample selection, as the sample may not necessarily represent the broader population, but, is instead based on existing social networks. We recommend that future studies employ randomized or stratified sampling methods to ensure a more representative sample. Alternatively, combining snowball sampling with other probability-based sampling techniques could reduce bias and increase generalizability.
Geographic limitations of the sample were noted, as most participants resided in northern Israel, which could affect the generalizability of the findings to other populations in different geographic areas of the country. To mitigate such biases, the survey was distributed across all residential areas of the Arab population. Fortunately, it achieved a satisfactory representation from all segments of the population, reflecting the diversity of the Arab community in Israel in terms of origin and place of residence. We recommend that future research aim for a more geographically diverse sample, potentially including participants from different regions of Israel or outside the country. Researchers could also explore regional differences by comparing findings from northern and southern Israel to assess variations.
Since participants were asked to retrospectively report on breastfeeding after childbirth, there is a likelihood of memory bias that may affect the accuracy of the reports, particularly, regarding the duration of breastfeeding and the reasons for its cessation. We recommend that to reduce memory bias, future research could prospectively collect data, by following participants from childbirth through the breastfeeding period. Alternatively, researchers could use mixed methods, incorporating qualitative interviews to validate quantitative reports.
Furthermore, the study focused on Arab mothers in Israel, therefore, the findings may not be applicable or representative of other populations, even within Israel or in the broader global context, thereby, limiting generalizability of the findings to other populations. We recommend conducting similar studies (i.e., systematic replications) with diverse ethnic and religious groups, both within Israel and in other countries, to determine whether the findings are culturally specific or universally applicable. Cross-cultural comparisons could also be valuable.
From a cultural/religious aspect, although the study emphasized religious and cultural beliefs, we did not explore in depth the interaction between these and other factors, such as modern social norms and global effects, which may alter breastfeeding patterns in specific populations. We recommend that future research explore the dynamic relationship between traditional cultural/religious beliefs and factors, such as media, globalization, and socioeconomic factors, to understand how these affect breastfeeding practices. This can be achieved through longitudinal studies and in-depth qualitative research.
5. Conclusions
We examined the impact of religious beliefs and socio-demographic factors on breastfeeding patterns among Arab mothers in Israel, focusing on Muslim, Christian, and Druze populations. We explored how religion, age, education, number of children, and employment impact the choice of exclusive or combined breastfeeding, finding a direct correlation between high levels of religiosity and longer durations of EB, particularly, among Druze and Muslim women. Additional factors affecting breastfeeding duration include family support, especially from older women in the family, as well as economic and employment-related factors. Working mothers were more likely to combine breastfeeding with infant formula.
The research revealed that the motivations for continued breastfeeding were primarily centered around child health and the intimate bond between mother and child. Conversely, a lack of breast milk was the most common reason cited for ceasing breastfeeding. We underscore the need for broader, multidisciplinary support from the healthcare system and employers for breastfeeding mothers, as well as programs tailored to the religious and cultural backgrounds of the studied populations.
Supplementary Materials
The online questionnaire as supplementary material and supporting information can be downloaded at: Preprints.org.
Author Contributions
Conceptualization, M.T. and K.A.,; methodology, M.T., S.B., O.Y., M.S.,; formal analysis, M.S.,S.B., M.T., K.A.; investigation, K.A., M.T., O.Y.; writing-original draft preparation, O.Y. and M.T.; writing-review and editing, M.T.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the Ramat Gan Academic College, approval code #2023-1010, approval date: July 20, 2023. On the Appendix A: Informed consent form for online studies, Part I: Informed Consent Form for Online Studies it is written to each participant who answered the questionnaire that “by clicking the “I agree” button, you express your consent to participate in the study. Thereby, each patient who filled out the questionnaire had given his/her informed consent.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. The participants were given a detailed explanation of the study in their native language (Arabic or English) and were asked online to provide an informed consent form.
Data Availability Statement
Individual level data cannot be made publicly available due to legal and ethical restrictions. Aggregative data might be provided upon reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Acknowledgments
We thank the hospitals, nurses, and supervisors for their support.
Appendix A: Informed Consent Form for Online Studies
Part I: Informed Consent Form for Online Studies
Greetings,
You are invited to participate in a study entitled “Characteristics and Factors Israeli Arab Mothers Related to Exclusive Breastfeeding. This study was conducted by researchers from the Ramat Gan Academic College and The Academic College of Tel Aviv-Jaffa. We thank you for dedicating your time and participating in the study.
The purpose of the study is to investigate the factors associated with exclusive breastfeeding among Arab mothers living in Israel.
The time required to fill out the questionnaire is approximately 15 minutes. The questionnaire is anonymous and will be filled out anonymously. Your answers are completely confidential, and will not be used in any way, except for research purposes.
You do not have to answer all the questions. If you feel uncomfortable, you may stop filling out the questionnaire at any stage.
By agreeing to fill out this questionnaire, you declare that you are over 18 years old.
It is assumed that participating in the research will not bring you any personal profit or advantage, however, we hope that your participation will contribute to the general knowledge in this research field.
It should be noted that we are not aware of any risks by participating in the study, but, as with any online activity, there is a certain risk of breach of privacy. We have made every effort to reduce this risk by having the questionnaire filled out anonymously and to not use the details, except, for the purpose of the study.
At the conclusion of the study, you will be able to receive more information from the Ethics Committee of The Israel Academic College, Ramat Gan, using the debriefing form. In addition, you can contact the research team by email:
We thank you very much for filling out the questionnaires in full.
Sincerely yours,
Dr. Khaled Awawdi : Awawdi.h@iac.ac.il Dr. Tarabeih Mahdi: mahdita@mta.ac.il
By clicking the “I agree” button, you express your consent to participate in the study. By clicking on the “I do not agree” button, you terminate your participation in the study.
Appendix B
Part A: Socio-Demographic and Employment Characteristics
- Age: ___________________
-
Marital Status:
- Married or living with a partner
- Single
- Divorced or separated
- Widowed
-
What is your nationality?
- Arab Muslim
- Arab Christian
- Arab Druze
-
Region?
- North
- Central
- South
-
Level of Religiosity. Please circle the extent to which you agree with the following statements. 1 = Strongly disagree, 5 = Strongly agree.
- Do you believe in religious values?
- Do you act according to traditional religious values?
- Do you observe the commandments of your faith?
-
How many children do you have prior to your last birth? (not including your most recent child)?
- 0
- 1
- 2
- 3
- 4 or more
-
How many people permanently live in your household?
- 1
- 2
- 3
- 4 or more
-
What is your level of education?
- Primary
- Secondary
- Academic
-
Did you work before the birth and what are the characteristics of your job?
- I did not work
- Self-employed
- Employed
-
Did you work before the birth or until shortly before, and what was the extent of your work? (If you are employed at a different percentage than listed below, please mark the higher percentage.)
- I did not work
- I worked, full-time 100%
- I worked, 75% part-time
- I worked, 50% part-time
- I worked, 25% part-time
-
Do you intend to return to work?
- Yes
- No
- I don’t know
- I have already returned to work
-
At what age of the baby do you intend to return to work or have you returned to work?
- 1 month
- 2 months
- 3 months
- Between 4 to 6 months
- 6 months
- I do not plan to return to work
-
The average income for a family was recently determined as between 12,000 shekels and 15,000 shekels. How would you rate your family’s income?
- Below average
- Average income
- Above average
Part B: Details on Infant Feeding
Exclusive breastfeeding is defined as the natural feeding of breast milk or expressed breast milk without any supplementation of infant formula (IF), including any formula given in the hospital after birth.
-
During your prenatal follow-up or your stay in the hospital, did you receive guidance on breastfeeding, and in what form?
- I did not receive any dialogue or guidance on breastfeeding.
- I received a group dialogue or guidance on breastfeeding.
- I received an individual dialogue or assistance regarding breastfeeding.
-
What was the nature of the feeding your infant received since the last birth during the past four months?
- Infant formula (IF) only.
- Partial/combined breastfeeding with IF.
- Exclusive breastfeeding (breast milk and/or expressed breast milk) only.
-
If your infant’s feeding method during the past four months was based on exclusive breastfeeding, how long did the breastfeeding last?
- I did not breastfeed at all.
- Up to one month.
- Up to two months.
- Up to three months.
- Up to four months.
- More than four months.
- If the feeding method for your baby over the past four months, or part of that time, was based on exclusive breastfeeding, please indicate the degree of influence each of the following factors had on your decision to breastfeed:
| Factors affecting decision to breastfeed | Did not impact my decision | Had some impact on my decision | Had a significant impact on my decision |
| 1. Family members (Mother, Mother-in-law, Sisters) | 0 | 1 | 2 |
| 2. Health Clinic Nurse | 0 | 1 | 2 |
| 3. Hospital Staff | 0 | 1 | 2 |
| 4. Childbirth Preparation Course | 0 | 1 | 2 |
| 5. Successful Previous Experience with Breastfeeding with a Previous Child | 0 | 1 | 2 |
| 6. Economic Consideration (breast milk is free) | 0 | 1 | 2 |
| 7. Desire for Good Bonding with the Child | 0 | 1 | 2 |
| 8. Maintaining the Health of Your Baby | 0 | 1 | 2 |
| 9. Information from the Internet, Literature, and Media | 0 | 1 | 2 |
- 5.
- If the feeding method for your baby over the past four months, or part of that time, was based on exclusive or partial breastfeeding, please indicate for each of the following reasons whether it was a reason for you to stop breastfeeding:
| Reasons affecting decision to stop breastfeeding | Was NOT a reason to stop | WAS a reason to stop |
| 1. Because you did not have enough milk or the milk was not good and the baby constantly needed formula supplementation. | 0 | 1 |
| 2. Because of health issues of the baby: illness, hospitalization, or medication that prevented the baby from breastfeeding. | 0 | 1 |
| 3. Because of your own health issues: illness, hospitalization, or medication that prevented you from breastfeeding. | 0 | 1 |
| 4. Due to fatigue, discomfort, lack of time, or dissatisfaction with the breastfeeding experience. | 0 | 1 |
| 5. Due to lack of support and guidance from professionals for continuing breastfeeding. | 0 | 1 |
| 6. Because returning to work and work conditions were not supportive enough for continuing breastfeeding or expressing milk. | 0 | 1 |
References
- Adokiya, M.N., Bukari, M., Ndago, J.A., Kuganab-Lem, R.B., Garti, H., Konlan, M.Y., Amoasah, A.A., & Ali, Z. (2023). Exclusive.
- Breastfeeding among Beneficiaries of a Nutrition Enhancement Programme and its Associated Factors in Ghana. PLoS ONE, 18(5), e0286546. [CrossRef]
- Alchalel, S., Zaitoon, H., Gover, A., Simmonds, A., Toropine, A., & Riskin, A. (2024). The Impact of Religious Beliefs on Early Lactation in Israeli Mothers. Breastfeeding Medicine, 19, 525-533. [CrossRef]
- Arif, S., Khan, H., Aslam, M., & Farooq, M. (2021). Factors Influencing Exclusive Breastfeeding Duration in Pakistan: A Population-Based Cross-Sectional Study. BMC Public Health, 21, 1–10. [CrossRef]
- Australian Breastfeeding Association. Website. https://www.breasfeeding.asn.au/.
- Birch, L., Savage, J.S., & Ventura, A. (2007). Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Canadian Journal of Dietetic Practice and Research, 68, s1–s56.
- Black, R.E., Allen, L.H., Bhutta, Z.A., Caulfield, L.E., de Onis, M., Ezzati, M., Mathers, C., & Rivera, J. (2008). Maternal and Child Undernutrition Study Group. Maternal and Child Undernutrition: Global And Regional Exposures and Health Consequences. Lancet, 371, 243–260. [CrossRef]
- Carandang, R.R., Sakamoto, J.L., Kunieda, M.K., Shibanuma, A., Yarotskaya, E., Basargina, M., & Jimba, M. (2021). Roles of the Maternal and Child Health Handbook and Other Home-Based Records on Newborn and Child Health: A Systematic Review. International Journal of Environmental Research and Public Health, 18, 7463. [CrossRef]
- Centers for Disease Control and Prevention (CDC). (2020). Rates of any and Exclusive Breastfeeding by Sociodemographic Characteristic among Children Born in 2020. Available online: https://www.cdc.gov/breastfeeding/data/nis_data/rates-any-exclusive-bf-socio-dem-2020.htm (accessed on 2 August 2023).
- Centers for Disease Control and Prevention (CDC). (2020). Results: Breastfeeding Rates. Available online: https://www.cdc.gov/breastfeeding/data/nis_data/results.html (accessed on 2 August 2023).
- Central Bureau of Statistics. Population, by District, Sub-District and Religion. 2020. Available online: https://www.cbs.gov.il/he/publications/DocLib/2022/2.ShnatonPopulation/st02_15x.xls (accessed on 22 February 2024).
- Dieterich, C.M., Felice, J.P., O’Sullivan, E., & Rasmussen, K.M. (2013). Breastfeeding and Health Outcomes for the Mother-Infant Dyad. Pediatric Clinics of North America, 60, 31–48. [CrossRef]
- Dieterich, R.R., Sereika, S., & Demirci, J. (2022). Early postpartum patterns of breastfeeding exclusivity and perceived insufficient milk by pre-pregnancy body mass index. Journal of Obstetric Gynecologic and Neonatal Nursing, 51, 205–217. [CrossRef]
- Dorri, R.A., Donnelly, T.T., McKiel, E., & Bouchal, S.R. (2022). Family and Religion’s Influence on Arab Immigrant Mothers’ Initiation and Exclusive Breastfeeding. International Journal of Healthcare, 8, 1–9. [CrossRef]
- Gavine, A., Shinwell, S.C., Buchanan, P., Farre, A., Wade, A., Lynn, F., Marshall, J., Cumming, S.E., Dare, S., & McFadden, A. (2022). Support for Healthy Breastfeeding Mothers with Healthy Term Babies. The Cochrane Database of Systematic Reviews, 10, CD001141. [CrossRef]
- Gianni, M.L., Bettinelli, M.E., Manfra, P., Sorrentino, G., Bezze, E., Plevani, L., Cavallaro, G., Raffaeli, G., Crippa, B.L., Colombo, L., Morniroli, D., Liotto, N., Roggero, P., Villamor, E., Marchisio, P., & Mosca, F. (2019). Breastfeeding Difficulties and Risk for Early Breastfeeding Cessation. Nutrients, 11, 2266. [CrossRef]
- Global Breastfeeding Collective (2023). Global Breastfeeding Scorecard, 2023: Rates of Breastfeeding Increase Around the World Through Improved Protection and Support. World Health Organization (WHO); United Nations Children’s Fund (UNICEF) Available online: https://www.unicef.org/media/150586/file/Global%20breastfeeding%20scorecard%202023.pdf.
- Hauck, F.R., Thompson, J.M., Tanabe, K.O., Moon, R.Y., & Vennemann, M.M. (2011). Breastfeeding and Reduced Risk of Sudden Infant Death Syndrome: A Meta-Analysis. Pediatrics, 128, 103–110. [CrossRef]
- Ip, S., Chung, M., Raman, G., Trikalinos, T.A., & Lau, J. (2009). A Summary of the Agency for Healthcare Research and Quality’s Evidence Report on Breastfeeding in Developed Countries. Breastfeeding Medicine, 4 (Suppl 1), S17–S30. [CrossRef]
- Laksono, A.D., Wulandari, R.D., Ibad, M., & Kusrini, I. (2021). The Effects of Mother’s Education on Achieving Exclusive Breastfeeding in Indonesia. BMC Public Health, 21, 1–6. [CrossRef]
- Lokossou, G.A.G., Kouakanou, L., Schumacher, A., & Zenclussen, A.C. (2022). Human Breast Milk: from Food to Active Immune Response with Disease Protection in Infants and Mothers. Frontiers in Immunology, 13, 849012. [CrossRef]
- Meek, J.Y., Feldman-Winter, L., & Noble, L. (2020). Optimal Duration of Breastfeeding. Pediatrics, 146, e2020018809. [CrossRef]
- Meek, J.Y.& Noble, L. (2022). Policy Statement: Breastfeeding and the Use of Human Milk. Pediatrics, 150, e2022057988. [CrossRef]
- Mehrpisheh, S., Memarian, A., Ameri, M., & Saberi Isfeedvajani, M. (2020). The Importance of Breastfeeding Based on Islamic rules and Qur’an. Hospital Practices and Research, 5, 37–41. [CrossRef]
- Ministry of Health, Israel. National plan dimensions of quality. Available online: https://www.health.gov.il/Subjects/Patient_Safety/hospitals/National_plan_dimensions_of_quality/Pages/05-16-2-01-001.aspx (accessed 2023).
- Ministry of Health, Israel. (2021). Available online. https://www.gov.il/BlobFolder/policy/bz01-2021/he/files_circulars_bz_bz01_2021.pdf.
- National Insurance Institute. Food Security in Israel: Annual Report. (2021). Available online: https://www.btl.gov.il/Publications/research/ Documents/ bitconTzonti%202021.pdf.
- National Program for Nutrition and Health Surveys (MABAT) – Infant Nutrition 2019–2020. Available online: https://www.gov.il/BlobFolder/reports/mabat-infant2/he/files_ publications_units_ICDC_ mabat-infant2-2019-2020.pdf.
- Ottolini, K.M., Andescavage, N., Keller, S., & Limperopoulos, C. (2020). Nutrition and the Developing Brain: the Road to Optimizing Early Neurodevelopment: A Systematic Review. Pediatric Research, 87, 194–201. [CrossRef]
- Pérez-Escamilla, R., Tomori, C., Hernández-Cordero, S., Baker, P., Barros, A.J., Bégin, F., & Richter, L. (2023). Breastfeeding: Crucially Important, but Increasingly Challenged in a Market-Driven World. Lancet , 401, 472–485. [CrossRef]
- Prado, E.L. & Dewey, K.G. (2014). Nutrition and Brain Development in Early Life. Nutrtion Reviews, 72, 267–284. [CrossRef]
- Quigley, M.A., Carson, C., Sacker, A., & Kelly, Y. (2016). Exclusive Breastfeeding Duration and Infant Infection. European Journal of Clinical Nutrition, 1420–1427. [CrossRef]
- Rito, A.I., Buoncristiano, M., Spinelli, A., Salanave, B., Kunešová, M., Hejgaard, T., García Solano, M., Fijałkowska, A., Sturua, L., Hyska, J., Kelleher, C., Duleva, V., Musić Milanović, S., Farrugia Sant’Angelo, V., Abdrakhmanova, S., Kujundzic, E., Peterkova, V., Gualtieri, A., Pudule, I., et al. (2019). Association Between Characteristics at Birth, Breastfeeding and Obesity in 22 Countries: The WHO European Childhood Obesity Surveillance Initiative - COSI 2015/2017. Obesity Facts, 12, 226–243. [CrossRef]
- Sivertsev, A. (2022). Households, Sects, and the Origins of Rabbinic Judaism; Brill: Leiden, The Netherlands, 102.
- Specht, I.O., Rohde, J.F., Olsen, N.J., & Heitmann, B.L. (2018). Duration of Exclusive Breastfeeding may be Related to Eating Behaviour and Dietary Intake in Obesity Prone Normal Weight Young Children. PLoS ONE, 13, e0200388. [CrossRef]
- Sundararajan, S., & Rabe, H. (2021). Prevention of Iron Deficiency Anemia in Infants and Toddlers. Pediatric Research, 89, 63–73. [CrossRef]
- The Noble Qur’an. Surat Al-Baqarah, 2:233. Available online: https://quran.com/2/233.
- Thompson, J.M.D., Tanabe, K., Moon, R.Y., Mitchell, E.A., McGarvey, C., Tappin, D., Blair, P.S., & Hauck, F.R. (2017). Duration of Breastfeeding and Risk of SIDS: An Individual Participant Data Meta-Analysis. Pediatrics, 140, e20171324. [CrossRef]
- Victora, C.G., Bahl, R., Barros, A.J., França, G.V., Horton, S., Krasevec, J., Murch, S., Sankar, M.J., Walker, N., Rollins, N.C., & Lancet Breastfeeding Series Group. (2016). Breastfeeding in the 21st Century: Epidemiology, Mechanisms, and Lifelong Effect. Lancet, 387, 475–490. [CrossRef]
- Wallenborn, J.T., Levine, G.A., Carreira Dos Santos, A., Grisi, S., Brentani, A., & Fink, G. (2021). Breastfeeding, Physical Growth, and Cognitive Development. Pediatrics, 147, e2020008029. [CrossRef]
- WHO (2023). Levels and Trends in Child Malnutrition: UNICEF/WHO/The World Bank Group Joint Child Malnutrition estimates: key findings of the 2023 editions. World Health Organization. Available online: https://www.who.int/publications/i/item/9789240073791.
- WHO Recommendations on Maternal and Newborn Care for a Positive Postnatal Experience (2022). World Health Organization. Available online: https://www.who.int/publications/i/item/9789240045989.
- Zimmerman, D.R., Kaplan, M., Shoob, H., Freisthler, M., Toledano, M., & Stein-Zamir, C. (2022). Breastfeeding Challenges and Support in a High Initiation Population. Israel Journal of Health Policy Research, 11, 31. [CrossRef]
Figure 1.
Reasons to foster breastfeeding (mean scores).
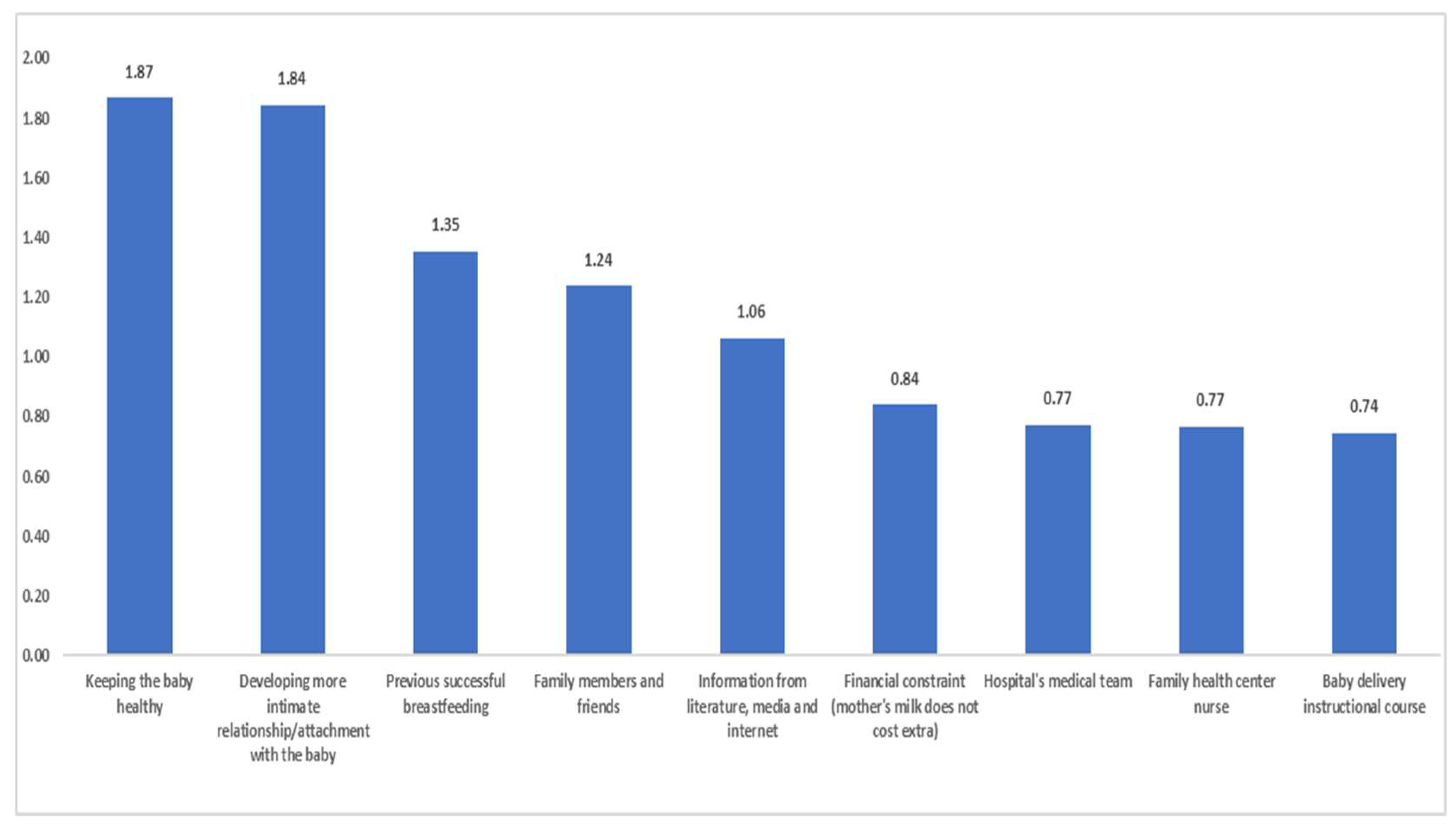
Figure 2.
Participant-reported reasons to halt breastfeeding with relative frequencies (proportions).
Figure 2.
Participant-reported reasons to halt breastfeeding with relative frequencies (proportions).
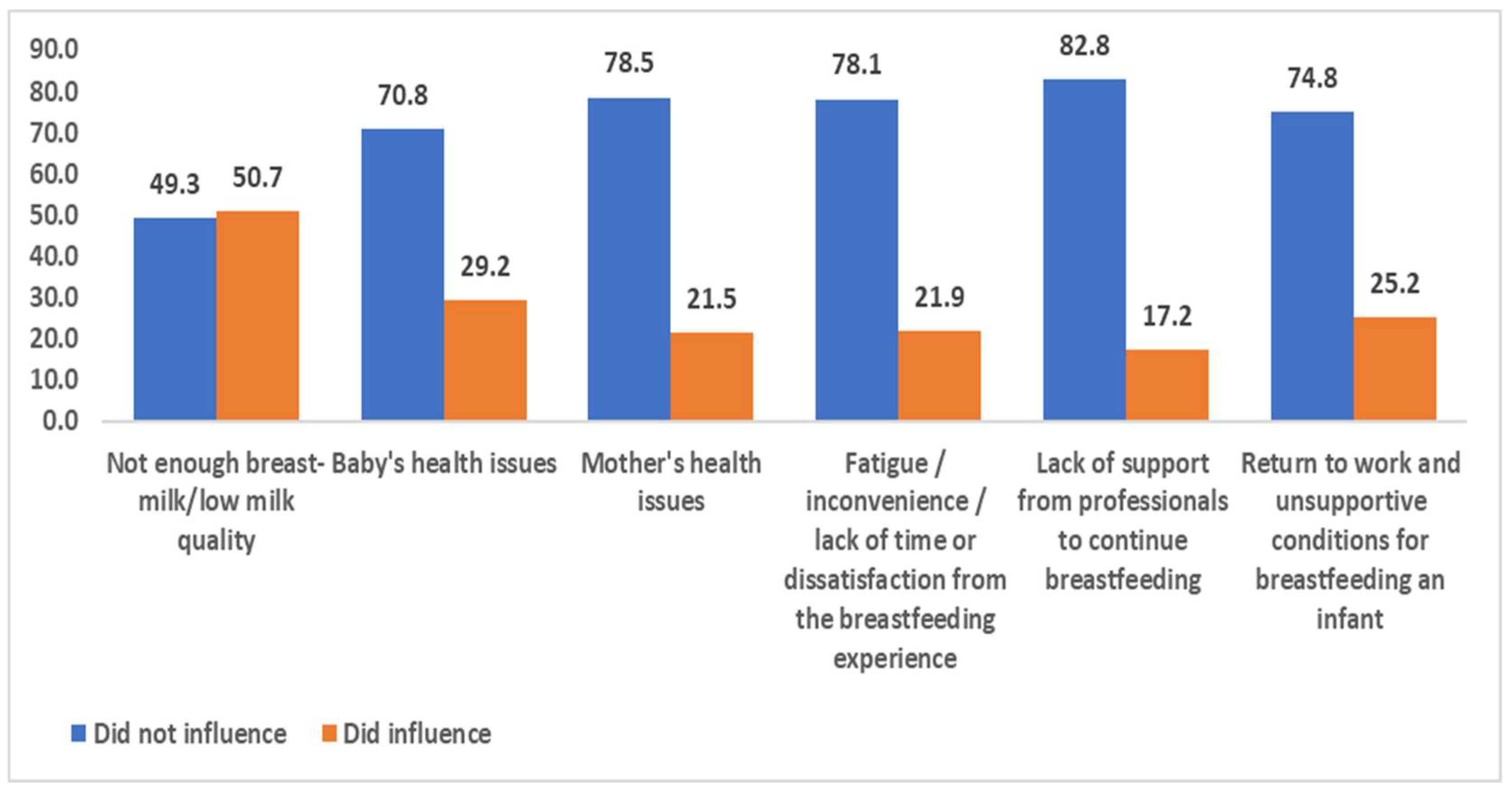

Table 1.
Independent-sample t-tests results, means and standard deviations describing the factors that foster breastfeeding.
Table 1.
Independent-sample t-tests results, means and standard deviations describing the factors that foster breastfeeding.
| Reason | Group | N | M | SD | t-test |
|---|---|---|---|---|---|
| Family members and friends | Non-academic | 114 | 1.38 | 0.81 | t = 2.26, p < .05 |
| Academic | 160 | 1.14 | 0.90 | ||
| Family health center nurse | Non-academic | 114 | 0.71 | 0.75 | t = 0.98, p > .05 |
| Academic | 160 | 0.81 | 0.83 | ||
| Hospital’s medical team | Non-academic | 114 | 0.70 | 0.75 | t = 1.28, p > .05 |
| Academic | 160 | 0.83 | 0.81 | ||
| Baby delivery instructional course | Non-academic | 114 | 0.56 | 0.76 | t = 3.13, p < .01 |
| Academic | 160 | 0.88 | 0.85 | ||
| Previous successful breastfeeding | Non-academic | 114 | 1.59 | 0.77 | t = 3.79, p < .01 |
| Academic | 160 | 1.19 | 0.92 | ||
| Financial constraint (mother’s milk does not cost extra) | Non-academic | 114 | 1.16 | 0.94 | t = 5.00, p < .01 |
| Academic | 160 | 0.61 | 0.85 | ||
| Developing a more intimate relationship or attachment with the baby | Non-academic | 114 | 1.81 | 0.56 | t = 1.00, p > .05 |
| Academic | 160 | 1.87 | 0.45 | ||
| Keeping the baby healthy | Non-academic | 114 | 1.85 | 0.50 | t = 0.52, p > .05 |
| Academic | 160 | 1.88 | 0.45 | ||
| Information from literature, media and internet | Non-academic | 114 | 0.78 | 0.89 | t = 4.58, p < .01 |
| Academic | 160 | 1.26 | 0.84 |
Chi-square tests indicated several significant associations (between educational level and reasons leading to a halt in breastfeeding). We found that: (1) non-academics believed that the quality of the milk/the amount of milk produced by the mother herself was an important reason to halt breastfeeding, as opposed to academics who believed the opposite (χ2 =6.21, p <.01); (2) non-academics believed that the health issues of the baby were an important reason to halt breastfeeding, as opposed to academics who did not believe so (χ2 =11.75, p <.01); (3) no significant association was found with regard to health issues of the mother as a reason between educational groups (χ2 = 1.06, p >.05); (4) academics believed that the fatigue/inconvenience/lack of time or dissatisfaction from the breastfeeding experience was an important reason to halt breastfeeding, as opposed to non-academics who did not believe so (χ2 = 4.26, p < .05); (5) no significant association was found with regard to lack of support from professionals to continue breastfeeding as a reason between educational groups (χ2 = 2.19, p >.05); and (6) academics believed that the return to work and unsupportive conditions for breastfeeding an infant was an important reason to halt breastfeeding, as opposed to non-academics who did not believe so (χ2 = 3.59, p < .05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



