
Submitted:
27 February 2025
Posted:
27 February 2025
You are already at the latest version
Abstract
Phosphoinositide 3-kinase (PI3K) and PTEN-induced kinase 1 (PINK1) are key regulators of metabolism and mitochondrial quality control. This study assessed their immunoexpression in 22 patients with lung adenocarcinoma and resected brain metastases treated with curative intent (2007–2017) and evaluated their prognostic significance. Tissue microarrays of primary tumors and matched metastases were analyzed using the H-score method. PI3K expression was significantly higher in primary tumors than in metastases (96.8 ± 57.9 vs. 43.5 ± 62.3; p = 0.003) and in stage IV adenocarcinomas (113.3 ± 56.3 vs. 61.4 ± 47.1; p = 0.043). PINK1 expression showed no significant variation across disease stages. Univariate analysis identified older age (>55 years), PI3K overexpression (HR = 7.791, 95% CI 1.718–36.432; >50 points), and PINK1 overexpression (>100 points) in primary tumors as predictors of poor overall survival (HR = 2.236, 95% CI 1.109–4.508; p = 0.025). Multivariate analysis confirmed PINK1 overexpression in primary tumors as an independent prognostic factor (HR = 4.328, 95% CI 1.264–14.814; p = 0.020). These findings suggest that PI3K and PINK1 may serve as prognostic biomarkers in lung adenocarcinoma with brain metastases, highlighting the need for research on their role in tumor progression and therapeutic response.
Keywords:
PI3K
; PINK1
; adenocarcinoma
; brain
; lung
; immunohistochemistry
; metastasis
; surgery
1. Introduction
Lung cancer constitutes a critical global health concern due to its high incidence and mortality rates. According to estimates from the International Agency for Research on Cancer's (IARC) GLOBOCAN 2020, lung cancer remains the leading cause of cancer-related deaths worldwide [1]. Unfortunately, lung cancer is frequently diagnosed at a locally advanced or advanced stage, significantly limiting treatment options[2]. Among the histological subtypes, lung adenocarcinoma is the most prevalent, representing approximately 40% to 50% of all cases and contributing significantly to cancer-related mortality globally[3]. It is the most common subtype to be diagnosed in people who have never smoked[4]. Adenocarcinoma is particularly common among women, with an increasing incidence observed in specific regions such as East Asia, driven by oncogenic mutations, most often involving EGFR[5]. Brain metastases (BM) develop in a substantial proportion of patients with lung adenocarcinoma, representing a severe clinical problem due to poor prognosis and limited therapeutic options[6]. Approximately 30% of patients with non-small cell lung cancer (NSCLC) develop brain metastases. Of these, nearly half exhibit brain involvement at the time of diagnosis, whereas the remainder acquire metastatic lesions during the therapeutic course[7]. Hence, brain metastases are expected to increase following prolonged overall survival in the future. Most patients with brain metastases have oligometastases[8]. For these patients, local treatment of brain metastases improves symptom control, quality of life, and survival time. Current treatment strategies for brain oligometastases include surgery, radiation therapy, and systemic treatments such as targeted therapies and immune checkpoint inhibitors[9]. Despite advancements, brain metastases remain associated with dismal outcomes[10,11].
Phosphoinositide 3-kinase (PI3K) is a critical component of the PI3K/AKT/mTOR signaling pathway, frequently activated in various malignancies[12]. Aberrant activation of PI3K contributes to oncogenic processes, including cell proliferation, survival, angiogenesis, and metabolic adaptation[13]. In lung adenocarcinoma, PI3K pathway alterations have been associated with poor prognosis and therapeutic resistance[14]. Targeting this pathway is an area of ongoing research, with several inhibitors currently in clinical trials[15,16].
Mitophagy, a selective form of autophagy responsible for eliminating damaged mitochondria, plays an important homeostatic function in cells and tissues maintaining the integrity of the mitochondrial pool by eliminating old and/or damaged mitochondria[17,18]. Therefore, defects in mitophagy could lead to a failure in proper reprograming of cellular metabolism, control of cell fate determination, attenuation of inflammation and response to DNA damage[18]. PTEN-induced kinase-1 (PINK1) is a key regulator of the canonical mitophagy pathway, initiating the process by recruiting Parkin, an E3 ubiquitin ligase, to the outer mitochondrial membrane[19]. PINK1 signaling has been shown to modulate several cellular processes, including mitochondrial dynamics, bioenergetics, and oxidative stress responses[20]. Dysregulation of mitophagy has been implicated in cancer, with PINK1 playing a dual role depending on the cellular context. In some cancers, PINK1 acts as a tumor suppressor by preserving mitochondrial integrity, while in others, it promotes tumorigenesis by enabling metabolic reprogramming and resistance to apoptosis [21,22,23,24].
Recent studies have highlighted the interaction between PI3K/AKT/mTOR pathway and PINK1 activity, suggesting that their crosstalk may play a crucial role in tumor progression and therapeutic resistance[25,26]. For instance, PINK1 enhances AKT activity by regulating PTEN, the main inhibitor of the PI3K/AKT/mTOR pathway[24,26]. Besides, PINK1 has been associated with glycolysis regulation and modulation of PI3K signaling, promoting cancer cell survival and proliferation[27,28]. Moreover, PINK1 and PI3K may influence the tumor microenvironment, particularly through their interactions with immune cells and their role in controlling the inflammatory response [29,30]. These findings underscore the potential of PINK1 and PI3K as prognostic biomarkers and therapeutic targets. Finally, one hallmark of cancer is metabolic reprogramming, with mitochondria playing a key role in supporting tumor growth. PINK1-mediated mitophagy and the PI3K/AKT pathway may contribute to metabolic plasticity in lung adenocarcinoma, promoting cell survival under stress[31].
In this study, we aimed to investigate the immunoexpression of PI3K and PINK1 in lung adenocarcinomas with brain metastases and assess their potential prognostic significance. We also explored the association of PI3K and PINK1expression with clinicopathological features, patient outcomes and PD-L1 immunoexpression.
2. Materials and Method
2.1. Patients and Samples
A total of 22 consecutive patients with suitable material of lung adenocarcinomas and resected BM, treated with curative intent between 2007 and 2017, were retrospectively selected from the Department of Pathology electronic database at the Hospital Universitario Central de Asturias. The follow-up period lasted until 2025. All patients were managed with conventional treatment strategies before the immunotherapy era, receiving standard approaches such as surgery, chemotherapy, and radiotherapy when indicated[32,33,34]. All the electronic medical records were reviewed to determine whether outcomes of interest occurred. All the tumors were excised with conventional surgery. In fact, for cases diagnosed at stage IV, surgical management always prioritized the resection of brain metastases before addressing the primary tumor. Patients with partial or subtotal resections, or those with limited material, were excluded. The original archived H&E slides were reviewed and diagnoses were established following the latest WHO guideline[35]. Information about the tumor stage was obtained from the date of the diagnosis. Clinical patient-related data were collected. Patient age was defined as the age at the time of diagnosis, either by lung or brain excisional biopsy. All patients had a history of heavy smoking, with a cumulative exposure of more than 30 pack-years. Comprehensive molecular profiling was performed, including immunohistochemistry (IHC) for relevant biomarkers and PCR-based analysis. All patients were found to be negative for alterations that would qualify them for targeted therapy. Ethics approval was obtained from the Ethics Committee of Hospital Universitario Central de Asturias (Reference No. 88/18), and the study was conducted in accordance with the Declaration of Helsinki.
2.2. Histopathologic Evaluation
Each sample was analyzed by two independent observers (and a third one in the case of strong disagreement), confirmed the diagnosis and registered the following histopathologic features using hematoxylin-eosin-stained slides: degree of differentiation classified as well differentiated (1), moderately differentiated (2) and poorly differentiated (3); absence or presence and percentage of necrosis, and mitotic activity by 10 high power fields.
2.3. Tissue Microarray Construction
Tissue microarrays (TMAs) were constructed from tissue blocks used for routine pathological evaluation. Morphologically representative areas were selected from each individual tumor paraffin block. Areas in each case with the most representative histology to overcome tumor heterogeneity were selected, and three 3 mm tissue cores were taken from each donor block and extruded into the recipient array. Thus, TMAs were created containing three tissue cores from each of the 22 lung adenocarcinomas and their respective 22 BM. In addition, each TMA included two cores of normal placenta and cerebral tissue as internal controls. A section from each microarray was stained with H&E to check the adequacy of tissue sampling. After 5 minutes at 60°C, the TMA blocks were subsequently cut using a microtome into 3μm thick sections and mounted on glass slides in preparation for immunohistochemistry.
2.4. Immunohistochemistry
For expression analysis by inmunohistochemistry we used the EnVision FLEX High pH (Link) Kit (Agilent-Dako, K800021. Santa Clara, CA. USA) and Dako Autostainer system. Paraffin embedded tissue sections (3µm) were deparaffinized, rehydrated and epitope retrieval by heat induction (HIER) at 95ºC for 20 min and ph 9 (Agilent-Dako) in the Pre-Treatment Module, PT-LINK (Agilent-Dako). Endogenous peroxidase activity was blocked with EnVision™ FLEX Peroxidase-Blocking Reagent (DM821) for 5 min. The sections were incubated with rabbit Anti-PI3K monoclonal antibody (Cell Signaling Technology, ref: 4249S, Danvers, Massachusetts, USA) at 1:50 dilution during 30min; rabbit Anti-PINK-1 policlonal antibody (BC100-494, NobusBiologicals. Madrid. Spain) at 1:200 dilution during 30min; and mouse Anti–PD-L1 monoclonal antibody (22C3, Dako, Denmark), at 1:200 dilution during 30min. The antigen-antibody reaction was detected with the Dako EnVision + Dual Link System-HRP (Agilent-Dako). The signal was detected using diaminobenzidine chromogen as substrate in Dako EnVision™ FLEX/HRP (Agilent-Dako). Counterstaining with hematoxylin was the final step. Negative controls were processed by omitting the primary antibody. Normal placental and cerebral tissues were used as positive controls. After the whole process, sections were dehydrated and mounted with permanent medium (Agilent-Dako mounting medium, CS703). The sections were studied and photographed under a light microscope (Nikon - Eclipse 80i).
2.5. Immunohistochemistry Assessment
Immunoexpression of the proteins were evaluated by two independent observers (and a third one in the case of strong disagreement) without any prior knowledge of each patient's clinical information and outcome. We used a semiquantitative approach called H-score (or “histo” score) as described elsewhere[22,36,37]. The final score gives more relative weight to higher intensity staining in each tumor sample. Then, the sample can then be categorized in a qualitative variable and considered positive or negative based on a specific discriminatory threshold. Besides, the final score was the mean of three cores analyzed for each case. In addition, excellent agreement was obtained for the immunohistochemistry assessment by the observers (k = 0.783), based on a hierarchical kappa test. Strong disagreement was considered for those cases evaluated with more than 30 points of difference. Discrepant cases were reevaluated, and the disagreement resolved.
2.6. Statistical Analysis
Baseline demographic and clinical characteristics of the patients and pathological data were summarized with standard descriptive statistics. The primary endpoint analyzed was overall survival (OS), defined as the time from the date of diagnosis confirmed by excisional biopsy to the date of death or the last recorded follow-up. All deaths were tumor related. All parameters were tested for normal distribution by the Shapiro-Wilk test. Therefore, depending on their symmetry and nature, variables were described by using mean ± standard deviation, percentage, medians with 25 and 75 percentiles or relative and absolute frequencies. The association between categorical variables was analysed using the χ2 test. For statistical analysis involving quantitative variables, non-parametric test such as the Kruskal–Wallis test (the nonparametric version of the ANOVA). Bonferroni correction was performed due to multiple statistical tests. Dunn test was performed as a post-hoc tests after a significant Kruskal-Wallis test. Pearson´s correlation test was carried out to analyse the statistical relationship, or association, between two continuous variables. For analysis of the survival data of patients, the Kaplan-Meier curves and the log-rank test were performed. Crude and adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated by using of the Cox proportional-hazards model. The simultaneous prognostic effect of various factors was determined in a multivariate analysis by using of the Cox proportional-hazard regression model. All reported p values are 2-sided, and values below 0.05 were considered statistically significant. All analyses were made by using IBM SPSS Statistics 27 (institutional license from the University of Oviedo).
3. Results
3.1. Clinicopathological Features of Cases
Twenty-two consecutive patients with lung adenocarcinoma and BM, for whom suitable tumor material was available, were enrolled in the study. Patients were categorized into two groups based on BM at diagnosis: stage IV or other stages, according to their main clinicopathological features, as summarized in Table 1. Except for survival, adjuvant therapy, PI3K expression in the primary tumor, and PDL1 expression in BM, there were no significant differences between the two groups regarding clinicopathological characteristics. Patients in Stage I-III showed significantly longer overall survival compared to those in Stage IV (p = 0.031). Adjuvant therapy was more frequently administered in Stage IV patients (p = 0.014). The expression of PI3K in primary tumors was significantly higher in Stage IV cases (p = 0.043) and was more than twice as high as in BM samples (p = 0.003). Additionally, PDL1 expression in BM was significantly different between the groups (p = 0.035). Non-significant differences were observed regarding age, gender, primary tumor location, BM location, tumor size, differentiation grade, necrosis and mitotic activity.
Several significant correlations were identified between clinicopathological variables in lung adenocarcinoma and its BM (Table 2). A significant moderate negative correlation between OS and patient age was noted (r = -0.590; p = 0.016), indicating that older patients had shorter OS. A quite strong positive correlation was observed between mitotic activity in the primary tumor and tumor size (r = 0.673; p = 0.004), suggesting that larger tumors exhibited higher mitotic activity. Furthermore, mitotic activity in brain metastases showed a significant moderate positive correlation with mitotic activity in the primary tumor (r = 0.594; p = 0.015), highlighting a link between proliferative activity in both sites. Additionally, PI3K expression in the primary tumor displayed a significant positive correlation with PI3K expression in BM (r = 0.556; p = 0.025), suggesting a consistent activation pattern of this pathway in primary and metastatic lesions.
3.2. Immunohistochemical Study of Proteins
A mean immunoexpression of 96.8 ± 57.9 points for PI3K in primary lung adenocarcinomas and 43.5 ± 62.3 points in BM was determined, with statistically significant differences between both tumor sites (p = 0.003) (Table1). Cytoplasmic staining with variable nuclear positivity for PI3K was observed among tumor samples (Figure 1A-C). Regarding PINK1, no significant differences were found between primary tumors (76.8 ± 40.0) and BM (77.5 ± 44.8; p = 0.793) (Table 1). The immunostaining pattern for PINK1 varied among tumor samples, showing weak to moderate or intense cytoplasmic positivity (Figure 1D-F). These findings indicate a significant reduction of PI3K expression in metastatic lesions, while PINK1 levels remain stable regardless of the tumor site.
PD-L1 expression was evaluated in both primary lung adenocarcinomas and their corresponding BM. Positive immunostaining (PD-L1 >1%) was detected in 40.9% of primary tumors and 36.4% of BM, without statistically significant differences between both sites (p = 0.307). In addition, no positive cases were identified in BM from stage I-III lung adenocarcinomas, with significant differences compared to stage IV cases (p = 0.035) (Table 1). (Figure S1 shows images of the immunohistochemical analysis).
3.3. Survival Curves, Univariate and Multivariate Analysis
Kaplan-Meier survival analysis was performed to evaluate the prognostic impact of PI3K PINK1 and PD-L1 expression on OS in lung adenocarcinoma patients with BM. The analysis was conducted in both primary tumors and metastatic lesions; however, significant results were only observed in the primary tumors. The results demonstrated that patients with more than 50 points of PI3K expression in the primary tumor exhibited significantly reduced OS compared to those with lower PI3K levels (p = 0.002, Figure 2A). Regarding PINK1 expression, patients with more than 90 points in the primary tumor had significantly lower OS compared to those with 90 or fewer points (p = 0.044, Figure 2B). When stratified into three groups, patients with PI3K expression between 60 and 150 points had the worst OS, followed by those with more than 150 points (p = 0.008, Figure 2C). Similarly, when PINK1 expression was categorized into three groups, patients with more than 100 points were significantly associated with poorer survival outcomes (p = 0.049, Figure 2D). These findings suggest that both PI3K and PINK1 overexpression in primary tumors may be linked to worse prognosis in lung adenocarcinoma patients with BM. Kaplan-Meier survival analysis was also performed to assess the prognostic significance of PD-L1 expression. The results indicated that patients with PD-L1 positive tumors had significantly reduced OS compared to those with PD-L1 negative tumors (p = 0.048, Supplementary Figure 2). This finding suggests that PD-L1 positivity may be associated with worse prognosis in this patient cohort.
Univariate analysis showed that older age (>55 years) (HR = 7.014, 95% CI 1.485-33.139; p = 0.014), more than 50 points of PI3K expression in the primary tumor (HR = 7.791, 95% CI 1.718-36.432; p = 0.008), and more than 100 points of PINK1 expression in the primary tumor (HR = 2.236, 95% CI 1.109-4.508; p = 0.025) were significantly associated with poor OS. Additionally, in the multivariate model, PINK1 overexpression in the primary tumor remained an independent prognostic factor for OS (HR = 4.328, 95% CI 1.264-14.814; p = 0.020) (Table 3).
4. Discussion
Lung cancer is the leading cause of cancer-related mortality worldwide and remains a major public health concern[1]. Lung adenocarcinoma, like other types of lung cancer, is often diagnosed at locally advanced or advanced stage, which limits treatment options[2].
Therefore, disease stage is a key prognostic factor, significantly impacting survival outcomes[38]. Particularly, lung adenocarcinoma with brain metastases has historically posed a significant challenge in oncology due to its poor prognosis, complex molecular landscape and the difficulty of its treatment[6]. In fact, in this case series, for patients diagnosed at stage IV, surgical management always prioritized the resection of brain metastases before addressing the primary tumor[8]. In this work, we have studied the immunohistochemical expression of the kinase PI3K, PINK1 and PD-L1 in a specific subset of patients with lung adenocarcinomas, only those who underwent surgical resection of their BM, to better describe molecular alterations at this stage of advanced disease.
We hereby stratified our twenty-two cases by disease stage and identified relevant findings. Patients diagnosed at earlier stages (I-III) had more than twice the OS compared to those diagnosed at Stage IV. A recent multicenter study in China analyzing 7,311 lung cancer patients confirmed that disease stage is a crucial predictor of survival, with significant differences in 5-year overall survival rates across stages I to IV. This highlights the impact of early-stage diagnosis and suggests that aggressive screening strategies may benefit high-risk populations, such as heavy smokers, to improve patient outcomes [39]. Adjuvant therapy was administered to most patients in this cohort, with a statistically significant difference between Stage IV and Stage I-III cases. We observed that patients with advanced-stage disease are more likely to receive adjuvant therapy, likely reflecting the greater tumor burden and the necessity of multimodal approaches in Stage IV disease. Previous studies have demonstrated that combining systemic therapy with RT can improve survival in NSCLC patients with brain metastases [40]. The higher percentage of patients in Stage I-III not receiving adjuvant therapy (42.8%) is because surgical resection was the primary treatment. Furthermore, the rise of targeted therapies and immune checkpoint inhibitors is reshaping treatment paradigms, particularly in patients with specific molecular alterations [11].
Microscopic examination of the tumors did not show significant differences concerning grade and necrosis. However, Stage IV tumors exhibited higher mitotic activity in both primary and metastatic sites compared to Stage I-III tumors. The direct relationship between mitotic activity and stage IV lung adenocarcinoma is not clearly established in the current literature. Although it is reasonable to assume that tumors in advanced stages may exhibit higher mitotic activity due to their aggressive nature, additional studies are needed to confirm this specific association. Unlike mitotic count, the tumor proliferative marker Ki-67 has been associated with a poorer prognosis in lung cancer[41]. The PI3K H-score showed a statistically significant increase, nearly doubling from Stage I-III tumors to Stage IV tumors. It is known that the activation of the PI3K/AKT pathway acts as an inducer of the epithelial-mesenchymal transition process during lung tumor metastasis[42]. Besides, the PI3K H-score showed a statistically significant decrease of more than a half from primary tumors to brain metastases. This reduction may indicate a biological shift in metastatic lesions that could influence therapeutic resistance, potentially affecting response to PI3K inhibitors[43]. PI3K has been extensively studied in various primary tumors and metastatic tissues, emerging as a master regulator of brain metastasis-promoting macrophages and microglia. It plays a pivotal role in shaping the tumor microenvironment, thereby facilitating metastatic colonization within the central nervous system[24,44]. Additionally, patients with Stage IV tumors exhibited higher PD-L1 expression compared to Stage I-III cases, especially in brain metastases, which may indicate a more immunosuppressive tumor microenvironment facilitating tumor progression and immune evasion. This suggests that tumors diagnosed at an advanced stage exhibit a more pronounced immune evasion phenotype, potentially affecting their response to immune checkpoint inhibitors (ICIs)[45]. Concerning PINK1 immunohistochemical expression, we did not observe significant differences between groups, including disease stages and primary tumors compared to BM. However, we previously reported significantly higher levels of PINK1 immunoexpression in liver metastases from colorectal carcinomas compared to primary tumors of the colon[22]. Besides, a current pan-cancer analysis revealed that PINK1 mRNA expression was reduced across multiple cancer types compared to normal tissues, including brain, breast, colorectal, esophageal, head and neck, liver, and ovarian cancers, as well as leukemia and melanoma, while elevated expression was observed in diffuse large B-cell lymphoma[29]. In NSCLC, PINK1 exhibited significant overexpression in both NSCLC tissues and cell lines, showing a correlation with the clinicopathological features of the disease[46]. Building upon these findings, we further investigated PINK1 expression by directly comparing its levels in tumor tissues from both primary and metastatic lesions, aiming to explore its potential applicability in routine pathological practice.
Although PINK1 inhibits PTEN, the key inhibitor of PI3K/AKT pathway, we did not observe any positive correlations in the immunohistochemical expression between the two molecules in either primary tumors or BM. This suggests the presence of more complex regulatory mechanisms that may attenuate this effect[47].
Survival analysis revealed that PI3K and PINK1 expression levels in primary lung adenocarcinomas were significantly associated with OS when patients were stratified according to specific cutoff points. These findings were also consistent with univariate Cox regression analyses. In contrast, we previously observed that immunohistochemical expression in metastatic tissue was not significantly associated with survival[22]. Furthermore, PINK1 expression in primary tumors emerged as an independent predictor of OS in the multivariate model. Similar findings were reported by Meng Wang et al. in primary lung adenocarcinomas[48]. Additionally, we previously reported analogous findings in metastatic colorectal carcinomas with resected liver metastases[22]. The molecular profile of advanced-stage cancer is gaining increasing relevance, sometimes outweighing conventional clinical and histopathological features. While the role of PI3K and PINK1 across various cancer types remains partially understood, previous studies have shown that PI3K acts as a master regulator of brain metastasis facilitating metastatic colonization. On the other hand, PINK1 has shown context-dependent effects, promoting cell migration and proliferation in lung cancer while exhibiting a protective role in other malignancies such as blood, brain, and breast cancers[29,48].
Taken together, these findings suggest that PI3K and PINK1 alterations are associated with carcinogenesis, particularly in lung adenocarcinomas with BM, potentially due to their roles in mitophagy, metabolic reprogramming, and modulation of the tumor microenvironment. From a translational perspective, therapies targeting these pathways, such as PI3K inhibitors or mitophagy modulators like metformin, may hold promise for improving patient outcomes, particularly in those with lung adenocarcinoma and BM exhibiting high PI3K and PINK1 expression[49,50].
We acknowledge several limitations in our study. First, there are potential biases inherent to its retrospective nature. Second, the study is restricted to a specific subset of lung cancer patients, namely those with BMs, and the evaluation of protein immunoexpression in non-metastatic lung adenocarcinomas was not addressed. Third, these findings are based on patients treated at a university hospital; thus, the proportion of tumors with poor prognosis might be higher due to referral bias compared to routine ambulatory practice. Fourth, the study was conducted at a single center. Fifth, the immunohistochemical analysis was performed using tissue microarrays; however, protein immunoexpression patterns were relatively homogeneous and consistent across the three representative tissue cores selected from each tumor.
5. Conclusions
In conclusion, the data presented herein, derived from a highly specific subset of patients with lung adenocarcinomas and resected BM, revealed that the immunohistochemical expression of PINK1, evaluated using the H-score and stratified into three groups (<50, 50–100, and >100), was a significant independent prognostic predictor for OS when assessed in primary tumors but not in metastatic tissue. Similarly, PI3K expression in primary tumors emerged as a significant prognostic factor, with higher H-scores associated with poorer survival outcomes. These findings highlight the potential complementary role of both PINK1 and PI3K as biomarkers for risk stratification in lung adenocarcinomas with BM. In addition, these results support the potential utility of PI3K-targeted therapies and mitophagy modulators in selected patient subgroups. Besides, PD-L1 expression reinforces the need for personalized approaches in immunotherapy. Nevertheless, these results require validation in prospective studies that also include lung adenocarcinomas with metastases to other anatomical sites, further supporting the clinical utility of PINK1 and PI3K immunoexpression for prognostic assessment. Ultimately, this evidence could also provide the rationale for exploring therapeutic strategies aimed at modulating PINK1 and PI3K expression in patients with lung adenocarcinomas and resected brain metastases.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This research was funded in part by Instituto de Salud Carlos III (ISCIII), grant number FISS-21-RD21/0002/0041; by Agencia de Ciencia, Competitividad Empresarial e Innovacion Asturiana, grant number SEK-25-GRU-GIC-24-069; and by the Instituto de Investigación Sanitaria del Principado de Asturias (ISPA) under the project name "ISPA EMERGENTES IFV 2020" to I.F.V. Noelia Blanco was funded by Spanish Ministry of Universities, grant number FPU20/06016. Daniela Corte and Andrea Navarro were funded by Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union, grants number PT20/00161 and PT23/00077.
Authors' contributions
MRV, AAFV and IFV reviewed the diagnoses of lung adenocarcinomas and their brain metatases and carried out the TMA preparations. Immunohistochemistry was carried out by MDCT and ANL. Data analyses were performed by JSJ, KMPB and NBA. MRV, AAFV and IFV carried out and interpreted the staining, contributed to data analyses, and drafted the manuscript. SFM, JML and LMQ provided technical support and critically reviewed the manuscript. Funding acquisition by JML and IFV. IFV coordinated the study. All authors read and approved the final manuscript.
Ethical Approval and Consent to participate
Ethics approval was obtained from the Hospital Universitario Central de Asturias Committee and the study was performed in accordance with the Declaration of Helsinki.
Human Ethics
All procedures involving experiments on human subjects are done in accord with the ethical standards of the Committee on Human Experimentation of the institution in which the experiments were done or in accord with the Helsinki Declaration of 1975.
Consent for publication
The authors read and approved the final manuscript for publication. All authors have contributed to the work and agree with the presented findings.
Availability of supporting data
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
Principado de Asturias BioBank, financed jointly by Servicio de Salud del Principado de Asturias and Instituto de Salud Carlos III, and integrated in the Spanish National Biobanks and Biomodels Network. We acknowledge Dr. Rodrigo Eduardo Ugalde-Herrá for his support in the development of TMA preparations.
Competing interests
The authors declare that there are no conflicts of interest. The authors have no connection to any companies or products mentioned in this article.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal, A., et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021; 71 (3):209-249. [CrossRef]
- Polanco D, Pinilla L, Gracia-Lavedan E, Mas A, Bertran S, Fierro, G., et al. Prognostic value of symptoms at lung cancer diagnosis: a three-year observational study. J Thorac Dis 2021; 13 (3):1485-1494. [CrossRef]
- Luo G, Zhang Y, Rumgay H, Morgan E, Langselius O, Vignat, J., et al. Estimated worldwide variation and trends in incidence of lung cancer by histological subtype in 2022 and over time: a population-based study. Lancet Respir Med 2025. [CrossRef]
- Myers DJ, Wallen JM. Lung Adenocarcinoma. StatPearls. Treasure Island (FL)2025.
- Ha SY, Choi SJ, Cho JH, Choi HJ, Lee, J., Jung, K., et al. Lung cancer in never-smoker Asian females is driven by oncogenic mutations, most often involving EGFR. Oncotarget 2015; 6 (7):5465-5474. [CrossRef]
- Sumiyoshi K, Yatsushige H, Shigeta K, Aizawa Y, Fujino A, Ishijima, N., et al. Survival prognostic factors in nonsmall cell lung cancer patients with simultaneous brain metastases and poor performance status at initial presentation. Heliyon 2024; 10 (18):e38128. [CrossRef]
- Waqar SN, Samson PP, Robinson CG, Bradley J, Devarakonda S, Du L, et al. Non-small-cell Lung Cancer With Brain Metastasis at Presentation. Clin Lung Cancer 2018; 19 (4):e373-e379. [CrossRef]
- Yen CT, Wu WJ, Chen YT, Chang WC, Yang SH, Shen SY, et al. Surgical resection of brain metastases prolongs overall survival in non-small-cell lung cancer. Am J Cancer Res 2021; 11 (12):6160-6172.
- Li, Y., Yan, B., He, S. Advances and challenges in the treatment of lung cancer. Biomed Pharmacother 2023; 169:115891.
- Sperduto PW, Mesko S, Li J, Cagney D, Aizer, A., Lin NU, et al. Survival in Patients With Brain Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Definition of the Eligibility Quotient. J Clin Oncol 2020; 38 (32):3773-3784. [CrossRef]
- Myall NJ, Yu H, Soltys SG, Wakelee HA, Pollom, E. Management of brain metastases in lung cancer: evolving roles for radiation and systemic treatment in the era of targeted and immune therapies. Neurooncol Adv 2021; 3 (Suppl 5):v52-v62. [CrossRef]
- Martini M, De Santis MC, Braccini L, Gulluni F, Hirsch, E. PI3K/AKT signaling pathway and cancer: an updated review. Ann Med 2014; 46 (6):372-383. [CrossRef]
- Yu JS, Cui, W. Proliferation, survival and metabolism: the role of PI3K/AKT/mTOR signalling in pluripotency and cell fate determination. Development 2016; 143 (17):3050-3060. [CrossRef]
- Sanaei MJ, Razi S, Pourbagheri-Sigaroodi A, Bashash, D. The PI3K/Akt/mTOR pathway in lung cancer; oncogenic alterations, therapeutic opportunities, challenges, and a glance at the application of nanoparticles. Transl Oncol 2022; 18:101364. [CrossRef]
- Glaviano A, Foo ASC, Lam HY, Yap KCH, Jacot, W., Jones RH, et al. PI3K/AKT/mTOR signaling transduction pathway and targeted therapies in cancer. Mol Cancer 2023; 22 (1):138. [CrossRef]
- Yu, L., Wei, J., Liu, P. Attacking the PI3K/Akt/mTOR signaling pathway for targeted therapeutic treatment in human cancer. Semin Cancer Biol 2022; 85:69-94. [CrossRef]
- Chourasia AH, Boland ML, Macleod KF. Mitophagy and cancer. Cancer & metabolism 2015; 3:4.
- Drake LE, Springer MZ, Poole LP, Kim CJ, Macleod KF. Expanding perspectives on the significance of mitophagy in cancer. Seminars in cancer biology 2017; 47:110-124. [CrossRef]
- Gladkova C, Maslen SL, Skehel JM, Komander, D. Mechanism of parkin activation by PINK1. Nature 2018; 559 (7714):410-414. [CrossRef]
- Gan ZY, Callegari S, Cobbold SA, Cotton TR, Mlodzianoski MJ, Schubert AF, et al. Activation mechanism of PINK1. Nature 2022; 602 (7896):328-335.
- Bernardini JP, Lazarou, M., Dewson, G. Parkin and mitophagy in cancer. Oncogene 2017; 36 (10):1315-1327.
- Celis-Pinto JC, Fernández-Velasco AA, Corte-Torres MD, Santos-Juanes J, Blanco-Agudín N, Piña Batista KM, et al. PINK1 Immunoexpression Predicts Survival in Patients Undergoing Hepatic Resection for Colorectal Liver Metastases. Int J Mol Sci 2023; 24 (7). [CrossRef]
- Panigrahi DP, Praharaj PP, Bhol CS, Mahapatra KK, Patra, S., Behera BP, et al. The emerging, multifaceted role of mitophagy in cancer and cancer therapeutics. Semin Cancer Biol 2020; 66:45-58. [CrossRef]
- Blazquez R, Wlochowitz D, Wolff A, Seitz S, Wachter A, Perera-Bel J, et al. PI3K: A master regulator of brain metastasis-promoting macrophages/microglia. Glia 2018; 66 (11):2438-2455. [CrossRef]
- Chen C, Xiang A, Lin X, Guo, J., Liu, J., Hu, S., et al. Mitophagy: insights into its signaling molecules, biological functions, and therapeutic potential in breast cancer. Cell Death Discov 2024; 10 (1):457. [CrossRef]
- Zheng F, Zhong J, Chen K, Shi Y, Wang F, Wang S, et al. PINK1-PTEN axis promotes metastasis and chemoresistance in ovarian cancer via non-canonical pathway. J Exp Clin Cancer Res 2023; 42 (1):295. [CrossRef]
- Agnihotri S, Golbourn B, Huang X, Remke M, Younger S, Cairns RA, et al. PINK1 Is a Negative Regulator of Growth and the Warburg Effect in Glioblastoma. Cancer Res 2016; 76 (16):4708-4719. [CrossRef]
- Li J, Xu X, Huang H, Li L, Chen, J., Ding Y, et al. Pink1 promotes cell proliferation and affects glycolysis in breast cancer. Exp Biol Med (Maywood) 2022; 247 (12):985-995. [CrossRef]
- Zhu L, Wu W, Jiang S, Yu S, Yan, Y., Wang, K., et al. Pan-Cancer Analysis of the Mitophagy-Related Protein PINK1 as a Biomarker for the Immunological and Prognostic Role. Front Oncol 2020; 10:569887. [CrossRef]
- Heavey S, O'Byrne KJ, Gately, K. Strategies for co-targeting the PI3K/AKT/mTOR pathway in NSCLC. Cancer Treat Rev 2014; 40 (3):445-456. [CrossRef]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov 2022; 12 (1):31-46. [CrossRef]
- Tambo Y, Sone T, Nishi K, Shibata K, Kita T, Araya T, et al. Five-year efficacy and safety of pembrolizumab as first-line treatment in patients with non-small cell lung cancer with PD-L1 tumor proportion score ≥50 %: A multicenter observational study. Lung Cancer 2025; 201:108422. [CrossRef]
- Rudin CM, Awad MM, Navarro A, Gottfried M, Peters, S., Csőszi, T., et al. Pembrolizumab or Placebo Plus Etoposide and Platinum as First-Line Therapy for Extensive-Stage Small-Cell Lung Cancer: Randomized, Double-Blind, Phase III KEYNOTE-604 Study. J Clin Oncol 2020; 38 (21):2369-2379. [CrossRef]
- Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med 2015; 372 (21):2018-2028.
- Board WHOCoTE. Thoracic Tumours. Lyon, France: International Agency for Research on Cancer; 2021.
- Camacho-Urkaray E, Santos-Juanes J, Gutierrez-Corres FB, Garcia B, Quiros LM, Guerra-Merino, I., et al. Establishing cut-off points with clinical relevance for bcl-2, cyclin D1, p16, p21, p27, p53, Sox11 and WT1 expression in glioblastoma - a short report. Cellular oncology (Dordrecht) 2018; 41 (2):213-221. [CrossRef]
- Fernandez-Vega I, Santos-Juanes J, Camacho-Urkaray E, Lorente-Gea L, Garcia B, Gutierrez-Corres FB, et al. Miki (Mitotic Kinetics Regulator) Immunoexpression in Normal Liver, Cirrhotic Areas and Hepatocellular Carcinomas: a Preliminary Study with Clinical Relevance. Pathology oncology research : POR 2020; 26 (1):167-173. [CrossRef]
- Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 2016; 11 (1):39-51. [CrossRef]
- He S, Li H, Cao M, Sun D, Yang, F., Yan, X., et al. Survival of 7,311 lung cancer patients by pathological stage and histological classification: a multicenter hospital-based study in China. Transl Lung Cancer Res 2022; 11 (8):1591-1605. [CrossRef]
- Kim MH, Kim SH, Lee MK, Eom JS. Recent Advances in Adjuvant Therapy for Non-Small-Cell Lung Cancer. Tuberc Respir Dis (Seoul) 2024; 87 (1):31-39. [CrossRef]
- Martin B, Paesmans M, Mascaux C, Berghmans T, Lothaire, P., Meert AP, et al. Ki-67 expression and patients survival in lung cancer: systematic review of the literature with meta-analysis. Br J Cancer 2004; 91 (12):2018-2025. [CrossRef]
- Moghbeli, M. PI3K/AKT pathway as a pivotal regulator of epithelial-mesenchymal transition in lung tumor cells. Cancer Cell Int 2024; 24 (1):165. [CrossRef]
- Li H, Wen X, Ren Y, Fan Z, Zhang, J., He, G., et al. Targeting PI3K family with small-molecule inhibitors in cancer therapy: current clinical status and future directions. Mol Cancer 2024; 23 (1):164. [CrossRef]
- Brastianos PK, Carter SL, Santagata S, Cahill DP, Taylor-Weiner, A., Jones RT, et al. Genomic Characterization of Brain Metastases Reveals Branched Evolution and Potential Therapeutic Targets. Cancer Discov 2015; 5 (11):1164-1177. [CrossRef]
- Fares J, Ulasov I, Timashev, P., Lesniak MS. Emerging principles of brain immunology and immune checkpoint blockade in brain metastases. Brain 2021; 144 (4):1046-1066. [CrossRef]
- Zhang R, Gu J, Chen J, Ni J, Hung, J., Wang, Z., et al. High expression of PINK1 promotes proliferation and chemoresistance of NSCLC. Oncol Rep 2017; 37 (4):2137-2146. [CrossRef]
- Fu D, Hu Z, Xu X, Dai X, Liu, Z. Key signal transduction pathways and crosstalk in cancer: Biological and therapeutic opportunities. Transl Oncol 2022; 26:101510. [CrossRef]
- Wang M, Luan S, Fan X, Wang J, Huang J, Gao X, et al. The emerging multifaceted role of PINK1 in cancer biology. Cancer Sci 2022; 113 (12):4037-4047. [CrossRef]
- Zeng S, Gan HX, Xu JX, Liu JY. Metformin improves survival in lung cancer patients with type 2 diabetes mellitus: A meta-analysis. Med Clin (Barc) 2019; 152 (8):291-297.
- Zhang B, Leung PC, Cho WC, Wong CK, Wang, D. Targeting PI3K signaling in Lung Cancer: advances, challenges and therapeutic opportunities. J Transl Med 2025; 23 (1):184. [CrossRef]
Figure 1.
Immunostaining for PI3K and PINK1 proteins in primary lung adenocarcinomas, measured by the H-score. Images show PI3K expression (A-C) and PINK1 expression (D-F) at 400× magnification. Representative cases are shown with negative or low expression (A, D), moderate expression (B, E) and high expression (C, F). Scale bars in A-F = 40 μm.
Figure 1.
Immunostaining for PI3K and PINK1 proteins in primary lung adenocarcinomas, measured by the H-score. Images show PI3K expression (A-C) and PINK1 expression (D-F) at 400× magnification. Representative cases are shown with negative or low expression (A, D), moderate expression (B, E) and high expression (C, F). Scale bars in A-F = 40 μm.
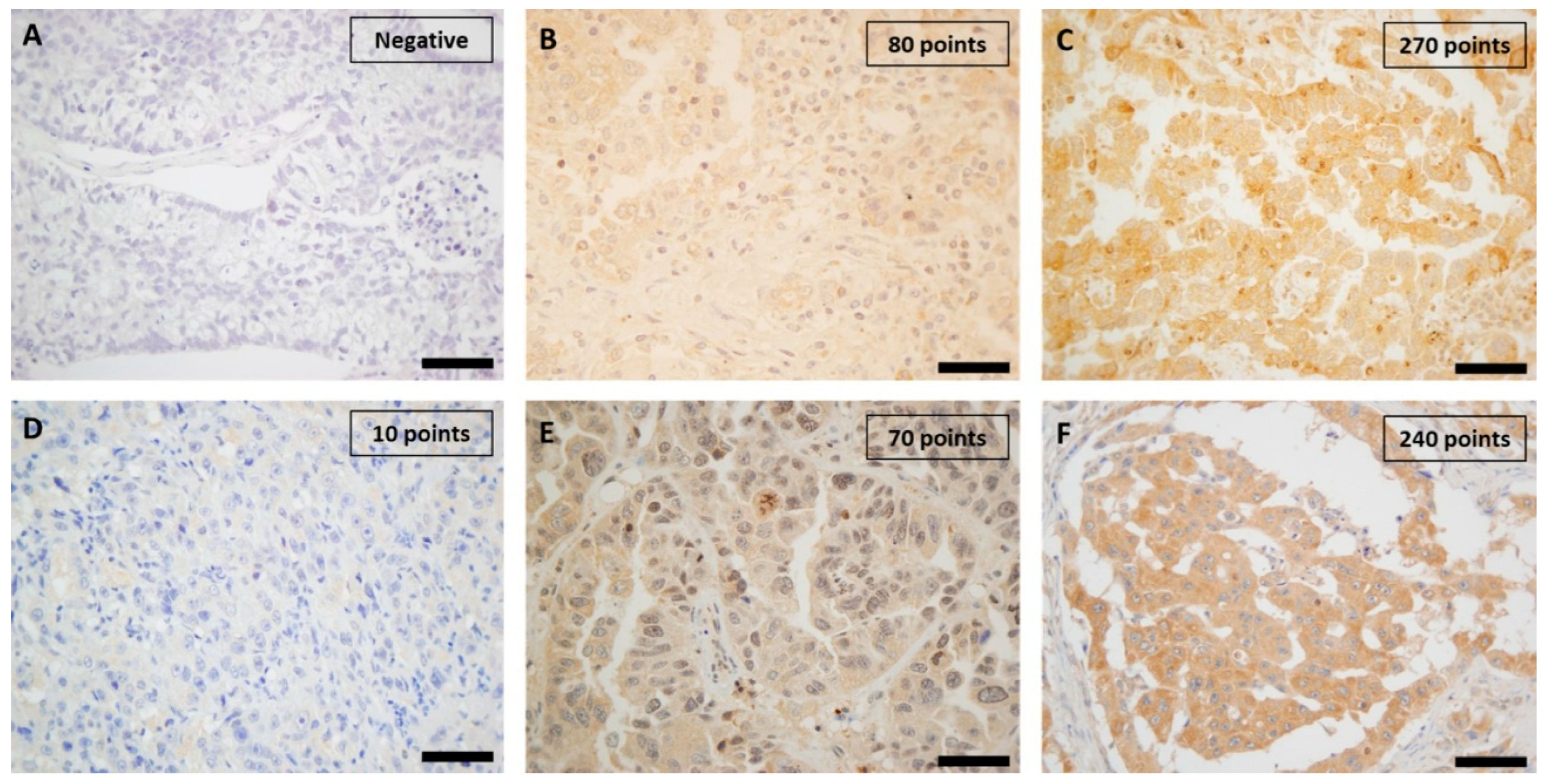
Figure 2.
Kaplan-Meier survival estimates for PI3K and PINK1 expression in primary lung adenocarcinomas. (A) PI3K expression grouped by H-score values ≤50 and >50 points, showing significantly better OS for cases with lower expression (p=0.002). (B) PINK1 expression grouped by H-score values ≤90 and >90 points, with higher survival in the low-expression group (p=0.044). (C) PI3K expression categorized into three groups: ≤60, 60-150, and >150 points, highlighting significantly better OS for cases with H-scores ≤60 points (p=0.008). (D) PINK1 expression stratified into three groups: ≤50, 50-100, and >100 points, showing improved survival in cases with H-scores ≤50 points (p=0.049).
Figure 2.
Kaplan-Meier survival estimates for PI3K and PINK1 expression in primary lung adenocarcinomas. (A) PI3K expression grouped by H-score values ≤50 and >50 points, showing significantly better OS for cases with lower expression (p=0.002). (B) PINK1 expression grouped by H-score values ≤90 and >90 points, with higher survival in the low-expression group (p=0.044). (C) PI3K expression categorized into three groups: ≤60, 60-150, and >150 points, highlighting significantly better OS for cases with H-scores ≤60 points (p=0.008). (D) PINK1 expression stratified into three groups: ≤50, 50-100, and >100 points, showing improved survival in cases with H-scores ≤50 points (p=0.049).
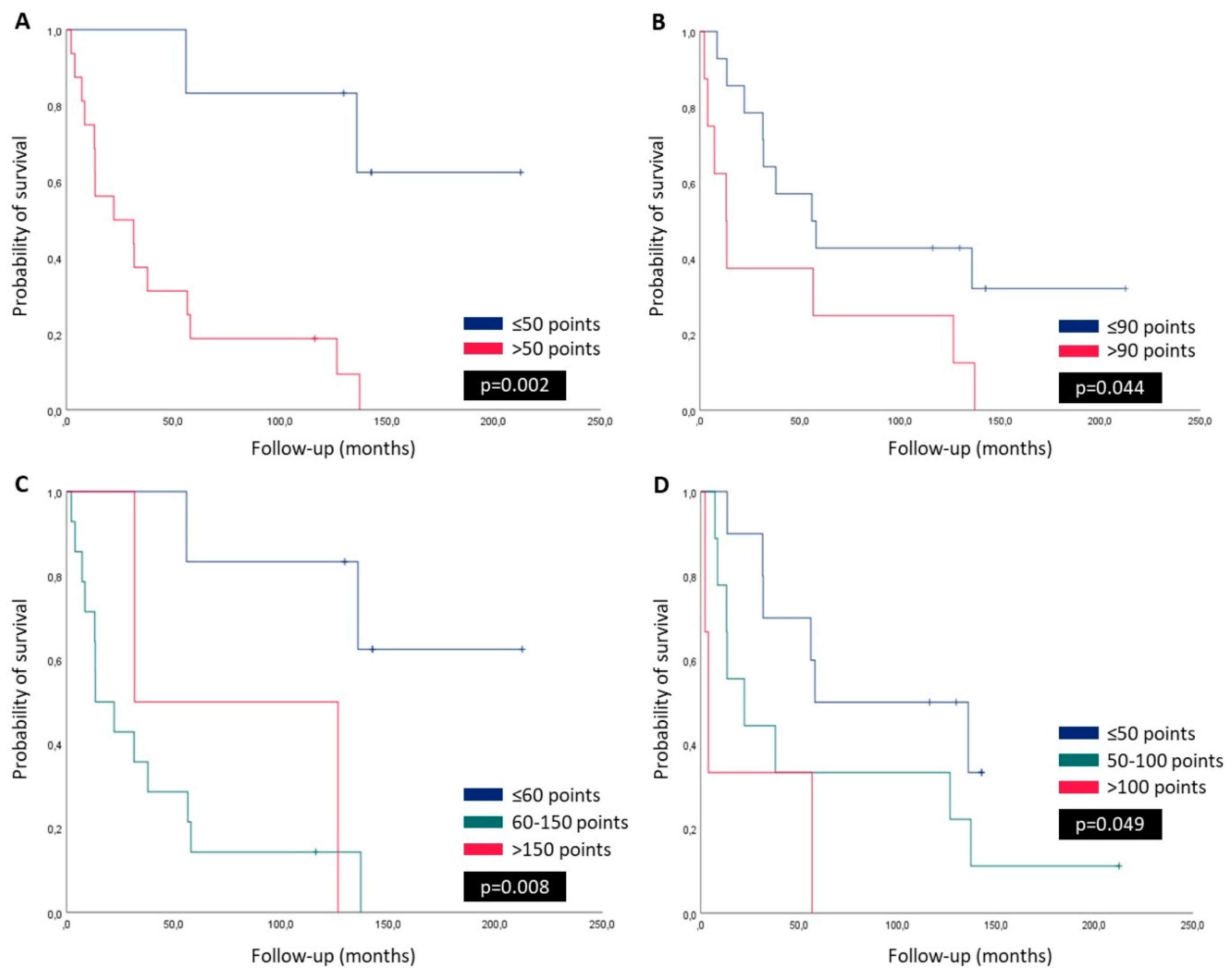

Table 1.
Patient demographics and histopathological differences based on brain metastasis at diagnosis.
Table 1.
Patient demographics and histopathological differences based on brain metastasis at diagnosis.
| Total | Stage IV | Stage I-III | P valor | |
|---|---|---|---|---|
| Patients | 22 | 15 (68.2%) | 7 (31.8%) | - |
| Age (years) | 58.7 ± 8.7 | 60.7 ± 5.4 | 54.4 ± 12.7 | 0.113 |
|
Gender -male -female |
11 (50%) 11 (50%) |
8 (53.3%) 7 (46.7%) |
3(42.9%) 4 (57.1%) |
0.975 |
|
Status -alive -dead |
5 (22.7%) 17 (77.3%) |
2 (13.3%) 13 (86.7%) |
3 (42.9%) 4 (57.1%) |
0.321 |
|
Primary tumor location -Superior lobes -Other sites |
12 (54.5%) 10 (45.5%) |
9 (60%) 6 (40%) |
3 (42.9%) 4 (57.1%) |
0.361 |
|
Brain metastases location -Fronto-temporal lobes -Other sites |
17 (77.3%) 5 (22.7%) |
11 (73.3%) 4 (26.7%) |
6 (85.7%) 1 (14.3%) |
0.348 |
| Tumor size in primary tumor (cm) | 3.5 ± 1.4 | 3.6 ± 1.4 | 3.1 ± 1.6 | 0.449 |
|
Survival (months) -OS |
68.1 ± 62.4 |
50.0 ± 52.5 |
106.9 ± 68.0 |
0.031 |
|
Adjuvant therapy -No -RT and/or CT -RT and CT |
3 (13.6%) 14 (63.7%) 5 (22.7%) |
0 12 (80%) 3 (20%) |
3 (42.8%) 2 (28.6%) 2 (28.6%) |
0.014 |
|
Grade in primary tumor -Well -Moderate -Poor |
7(31.8%) 8(36.4%) 7 (31.8%) |
4 (26.7%) 6 (40%) 5 (33.3%) |
3 (42.8%) 2 (28.6%) 2 (28.6%) |
0.741 |
|
Grade in brain metastasis -Well -Moderate -Poor |
3 (13.6%) 1 (4.6%) 18 (81.8%) |
2 (13.3%) 0 13 (86.7%) |
1 (14.3%) 1 (14.3%) 5 (71.4%) |
0.447 |
|
Necrosis in primary tumor -No -<25% -25%/50% -50%/75% ->75% |
4 (18.2%) 7 (31.8%) 7 (31.8%) 3 (13.6%) 1 (4.6%) |
6 (40%) 3(20%) 4 (26.6%) 1 (6.7%) 1 (6.7%) |
3 (42.8%) 2 (28.6%) 1 (14.3%) 1 (14.3%) 0 |
0.294 |
|
Necrosis in brain metastasis -No -<25% -25%/50% -50%/75% ->75% |
11 (50%) 5 (22.7%) 4 (18.2%) 0 2(9.1%) |
6 (40%) 3 (20%) 4 (26.6%) 0 2 (13.4%) |
5 (71.4%) 2 (28.6%) 0 0 0 |
0.420 |
|
Mitotic activity (per 10 HPF) -Primary tumor -Brain metastases |
18.0 ± 18.4 20.7 ± 16.5 |
22.8 ± 19.8 23.0 ± 18.6 |
7.7 ± 9.5 15.7 ± 10.2 |
0.343 0.026 0.285 |
|
PI3K (H-Score): -Primary tumor -Brain metastases |
96.8 ± 57.9 43.5 ± 62.3 |
113.3 ± 56.3 54.3 ± 70.2 |
61.4 ± 47.1 18.3 ± 28.6 |
0.003 0.043 0.319 |
|
PINK1 (H-Score): -Primary tumor -Brain metastases |
76.8 ± 40.0 77.5 ± 44.8 |
79.3 ± 39.9 75.7 ± 45.4 |
71.4 ± 43.0 81.7 ± 47.5 |
0.793 0.677 0.412 |
|
PDL1 (positive >1% tumor): -Primary tumor -Brain metastases |
9 (40.9%) 8 (36.4) |
7(46.7%) 8(53.3) |
2 (28.6%) 0 |
0.985 0.307 0.035 |
Values in bold are statistically significant, p <0.05. OS: Overall survival; RT: Radiotherapy; CT: Chemotherapy; HPF: High power field. The underlined p-values represent the results of the statistical analysis comparing the variables of the primary tumor and the variables of the brain metastasis.
Table 2.
Pearson´s correlation test for clinicopathological data and PI3K and PINK1 immunoexpresion in lung adenocarcinomas and their brain metastases.
Table 2.
Pearson´s correlation test for clinicopathological data and PI3K and PINK1 immunoexpresion in lung adenocarcinomas and their brain metastases.
| Age | Tumor size | OS | Mitosis primary tumor | Mitosis brain metastases | PI3K primary tumor | PI3K brain metastases | PIKN1 primary tumor | |
|---|---|---|---|---|---|---|---|---|
| Tumor size | r=-0.117 p=0.665 | - | - | - | - | - | - | - |
| OS | r=-0.590 p=0.016 | r=-0.109 p=0.687 | - | - | - | - | - | - |
| Mitosis primary tumor | r=-0.351 p=0.183 | r=0.673 p=0.004 | r=-0.032 p=0.908 | - | - | - | - | - |
| Mitosis brain metastases | r=-0.486 p=0.056 | r=0.173 p=0.521 | r=0.193 p=0.474 | r=0.594 p=0.015 | - | - | - | - |
| PI3Kprimary tumor | r=0.402 p=0.122 | r=0.041 p=0.880 | r=-0.468 p=0.068 | r=0.179 p=0.508 | r=-0.009 p=0.975 | - | - | - |
| PI3Kbrain metastases | r=0.013 p=0.963 | r=-0.180 p=0.505 | r=-0.289 p=0.277 | r=0.107 p=0.692 | r=0.246 p=0.358 | r=0.556 p=0.025 | - | - |
| PINK1 primary tumor | r=0.180 p=0.505 | r=0.223 p=0.406 | r=-0.385 p=0.140 | r=0.410 p=0.115 | r=0.145 p=0.593 | r=0.372 p=0.156 | r=0.023 p=0.934 | - |
| PINK1brain metastases | r=0.149 p=0.582 | r=0.135 p=0.617 | r=-0.185 p=0.492 | r=-0.284 p=0.287 | r=-0.134 p=0.620 | r=0.117 p=0.667 | r=0.247 p=0.356 | r=0.045 p=0.869 |
Values in bold are statistically significant, p <0.05; OS: Overall survival; r= Pearson´s correlation coefficient.
Table 3.
Univariate and multivariate analyses of variables associated with overall survival.
| Variables | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p value | HR | 95% CI | p value | |
| Age, years | 1.074 | 1.014-1.138 | 0.015 | |||
| Age, years (≤55 vs. >55) | 7.014 | 1.485-33.139 | 0.014 | 2.502 | 0.302-20.750 | 0.395 |
| Gender (male vs. female) | 2.009 | 0.758-5.326 | 0.161 | |||
| Primary tumor location (superior lobes vs. others) | 0.653 | 0.226-1.889 | 0.431 | |||
| Brain metastases location (frontotemporal lobes vs. others) | 1.243 | 0.460-3.361 | 0.668 | |||
| Tumour size (≤3cm vs. >3cm) | 1.552 | 0.585-4.116 | 0.377 | |||
| Stage (IV vs. others) | 2.902 | 0.923-9.128 | 0.068 | 4.896 | 0.890-26.941 | 0.065 |
| Adjuvant therapy (yes vs. no) | 1.161 | 0.538-2.505 | 0.704 | |||
| Mitotic activity primary tumor (≤15 vs. >15) | 0.716 | 0.270-1.901 | 0.502 | |||
| Mitotic activity brain metastases (≤15 vs. >15) | 0.795 | 0.287-2.202 | 0.660 | |||
| PI3K primary tumor | 1.008 | 1.000-1.015 | 0.038 | |||
| PI3K primary tumor; score (≤50 vs. >50) | 7.791 | 1.718-36.432 | 0.008 | 0.864 | 0,058-12.786 | 0.915 |
| PI3K primary tumor; score (<60 vs. 60-150 vs. >150) | 2.295 | 1.135-4.638 | 0.021 | |||
| PINK1 primary tumor | 1.013 | 1.000-1.026 | 0.042 | |||
| PINK1 primary tumor; score (≤90 vs. >90) | 2.589 | 0.992-6.759 | 0.052 | |||
| PINK1 primary tumor; score (<50 vs. 50-100 vs. >100) | 2.236 | 1.109-4.508 | 0.025 | 4.328 | 1.264-14.814 | 0.020 |
| PDL1 primary tumor; score (negative vs. positive) | 2,497 | 0.947-6.585 | 0.064 | 3.210 | 0.768-13.408 | 0.110 |
Cox regression model. CI – confidence interval, HR – hazard ratio. Values in bold are statistically significant, p <0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



