
Submitted:
25 February 2025
Posted:
27 February 2025
You are already at the latest version
Abstract
Emerging zoonotic fungal diseases represent a significant public health challenge in Africa, highlighting the complex interplay between human, animal, and environmental health. This review examines the distribution of various medically important fungi with zoonotic potential, including Emergomyces, Blastomyces, Coccidioides, Cryptococcus, dermatophytes, Histoplasma, Sporothrix, Talaromyces, Paracoccidioides, Aspergillus, and Malassezia in Africa. The evidence suggests that many of these infections are underdiagnosed due to the lack of surveillance and diagnostic capabilities, particularly in immunocompromised populations. The rise in these fungal infections, often linked to increasing HIV prevalence and environmental factors, emphasizes the need for comprehensive public health strategies. Effective interventions should focus on enhancing surveillance, raising awareness, improving diagnostic capacity, and fostering collaboration across health sectors through a One Health approach to mitigate the risks associated with these emerging pathogens.
Keywords:
Zoonotic fungal diseases
; Africa
; public health
; One Health approach
; surveillance
; diagnostic capacity
1. Introduction
Fungal infections represent a significant and often overlooked public health challenge globally [1]. With approximately one billion individuals affected by fungal diseases each year, resulting in an estimated 1.5 million deaths, the impact of these infections is profound [2]. Over the past century, there has been a marked increase in both the prevalence of fungal infections and associated fatalities [3]. This rise has been particularly pronounced among immunocompromised individuals, leading to the emergence of several new and previously known fungal infections[4]. Notably, a subset of these infections is classified as zoonotic, meaning they can be transmitted from animals to humans [5].
Zoonotic diseases, traditionally viewed as predominantly viral or bacterial in nature, encompass a significant number of fungal infections that have drawn less attention in public health discussions [6,7]. Animals have been identified as key reservoirs for many infectious diseases, accounting for approximately 75% of all emerging infections. The transmission of fungal pathogens from animals to humans is a growing concern, particularly in regions like Africa, where close human-animal interactions are prevalent [8,9]. This paper aims to provide an extensive overview of zoonotic fungal pathogens relevant to the African continent, examining their geographical distribution, and the public health implications associated with these infections.
Table 1 Demonstrating Zoonotic fungal diseases and their causative agents, hosts range, epidemiological and clinical characteristics.
2. Medically Important Fungi with the Potential of Zoonotic Transmission to Humans in Africa:
2.1. Emergomycosis
Emergomycosis is a serious fungal infection caused by a group of fungi known as Emergomyces, which was previously referred to as Emmonsia [10]. There are five known species of this fungus, including Es. Pasteurianus, Es. Africanus, Es. Canadensis, Es. Orientalis, and Es. Europaeus. Emergomyces can be found worldwide, but certain species, like Es. Pasteurianus and Es. Africanus, are predominantly found in Africa, particularly in South Africa, where the highest number of cases has been recorded [11]. Es. Africanus is a recently identified species that appears to only exist in southern Africa [12]. This fungus is thermally dimorphic, meaning it can change form depending on temperature. It primarily affects individuals with advanced HIV, and infections occur when fungal spores are inhaled from the soil [10]. Cases of emergomycosis have been documented on four continents: Asia, Europe, Africa, and North America [13]. Given the increase in global HIV cases, it is likely that emergomycosis exists in many areas without being reported, leading to underdiagnosis. To date, all reported cases have come from South Africa (Figure 1), with no other African countries reporting infections.
2.2. Blastomycosis:
Blastomycosis is a fungal infection that occurs when spores from the Blastomyces species, commonly found in soil, are inhaled [14]. In Africa, the primary causative agent is Blastomyces percursus [15]. The infection typically presents as pulmonary disease, which can progress to skin lesions, and may also affect other organs such as the brain. Remarkably, extra-pulmonary manifestations are the most common form of blastomycosis. Pulmonary involvement, when assessed through imaging, shows signs such as alveolar infiltrates, consolidation, and cavitation on chest radiographs [16,17]. Reported cases of blastomycosis have emerged from several African countries, including Kenya, Mozambique, Rwanda, Tanzania, Uganda, Zambia, Zimbabwe, The Gambia, Ghana, Liberia, Nigeria, Angola, the Democratic Republic of the Congo, South Africa, Algeria, Egypt, the Libyan Arab Jamahiriya, Morocco, and Tunisia (Fig.1). Awareness and monitoring of this infection are crucial, particularly in areas where exposure to contaminated soil is prevalent.
2.3. Coccidomycosis:
Coccidioidomycosis, commonly known as Valley Fever, is caused by inhaling spores from the Coccidioides fungi [18]. C. immitis and C. posadasii are two significant species associated with this disease [19]. C. posadasii thrives in arid areas of the southwestern United States, northern Mexico, and South America, while C. immitis is primarily found in California's San Joaquin Valley [19]. Coccidioidomycosis transmission predominantly occurs during the dry summer and late fall months, when soil disturbances such as wind and storms are frequent. Rarely, infection can also result from contact with contaminated materials [20]. Its prevalence is extremely low outside the Americas, but cases have been documented among travelers returning from endemic regions in Asia and Europe [20]. In Africa, Coccidioidomycosis has been reported in Ethiopia, Sudan, Uganda, Zimbabwe, Ghana, Nigeria, Egypt and Senegal (Fig.1). Public health initiatives should focus on improving awareness and education about this disease, especially for individuals traveling to endemic areas and for those living in regions where the Coccidioides fungi are present.
2.4. Cryptococosis
Cryptococcosis has emerged as one of the most lethal fungal diseases globally, with the annual death toll exceeding 180,000 [21]. This disease is particularly dangerous as it affects both immunocompromised and immunocompetent individuals, often by causing meningoencephalitis in HIV-positive patients. The primary causative agent is Cryptococcus neoformans, while Cryptococcus gattii has been increasingly observed in healthy individuals, leading to pulmonary infections. Since its first case was reported in the mid-1980s, the incidence of cryptococcosis has risen, underscoring the necessity for heightened public health measures [22]. In Africa, the disease has been reported in multiple countries, including Burundi; Djibouti; Eritrea; Ethiopia; Kenya; Madagascar; Malawi; Mozambique; Rwanda; Sudan; Tanzania; Uganda; Zambia; Zimbabwe; Burkina Faso; Cameroon; Côte d’Ivoire; Ghana; Guinea-Bissau; Mali; Nigeria; Senegal; Sierra Leone; Central African Republic; Democratic Republic of the Congo; Equatorial Guinea; Gabon; Lesotho; Swaziland; Botswana; Namibia; South Africa; Algeria; Egypt; Libyan Arab Jamahiriya; Morocco and Tunisia (Fig.1).
2.5. Dermatophytosis
Dermatophytosis, commonly referred to as ringworm or tinea, is a prevalent fungal infection observed globally [23]. However, recent trends indicate significant changes in the epidemiology of this disease [23]. The types of fungal species causing dermatophytosis now vary greatly across different countries. This shift has been associated with factors such as inappropriate treatment practices, high population density, international travel, and migration [23,24]. Additionally, the increasing popularity of pets has led to the emergence of new species, such as Trichophyton erinacei and Trichophyton benhamiae, which are contributing to a rise in zoonotic infections [25,26]. The rising incidence of dermatophytosis raises serious public health concerns as the costs associated with treatment can be substantial and prolonged. Such factors often lead to non-adherence to prescribed therapies, resulting in potential resistance to antifungal medications [23,27]. A particularly alarming situation has emerged with a large-scale outbreak of dermatophytosis currently ongoing in India, which is beginning to spread to other regions, including parts of Africa [28,29]. This outbreak is characterized by human-to-human transmission, typical of dermatophytes that primarily infect humans, yet it exhibits a severity of symptoms usually associated with zoophilic dermatophytes [30]. The outbreak has been linked to a novel species known as Trichophyton indotineae, which demonstrates enhanced virulence compared to the previously widespread species, Trichophyton mentagrophytes and Trichophyton interdigitale [29,31].
Research suggests that T. mentagrophytes, which typically infects wild animals, is adapting, moving to domestic animals, and behaving as an anthropophilic clonal variant. This Indian strain has shown a concerning trend of increased antifungal resistance, likely due to the overuse of common antifungal agents by the public, complicating control efforts and leading to a rising incidence of the disease [5].
In Africa, dermatophytosis has been reported in numerous countries, highlighting the need for greater awareness and intervention. Countries affected include Burundi, Djibouti, Eritrea, Ethiopia, Kenya, Madagascar, Malawi, Mauritius, Mayotte, Mozambique, Réunion, Rwanda, Somalia, Sudan, Tanzania, Uganda, Zambia, Benin, Burkina Faso, Cameroon, Cabo Verde, Côte d’Ivoire, Ghana, Guinea-Bissau, Liberia, Mali, Mauritania, Nigeria, Senegal, Togo, Angola, Chad, the Democratic Republic of the Congo, South Africa, Algeria, Egypt, the Libyan Arab Jamahiriya, Morocco, and Tunisia (Fig.1).
2.6. Histoplasmosis
Histoplasmosis is a significant fungal infection primarily found in the Ohio and Mississippi river valleys of the United States, as well as in various regions across Central and South America, Western, Southern, Eastern, and Central Africa, and Southeast Asia [32]. The infection is caused by two distinct varieties of the fungus Histoplasma capsulatum: Histoplasma capsulatum var. capsulatum (Hcc): This is the classical form of the disease. Histoplasma capsulatum var. duboisii (Hcd): This variety is associated with the African form of histoplasmosis [33]. Transmission of histoplasmosis predominantly occurs through the inhalation of microconidia, the airborne spores of the fungus [33]. A key risk factor for developing severe histoplasmosis is HIV/AIDS, which has led to the classification of the disease as an AIDS-defining illness since Globally, it is estimated that around 500,000 individuals are diagnosed with histoplasmosis each year. Of these cases, approximately 100,000 progress to disseminated histoplasmosis, and around 25,000 individuals succumb to the infection [34]. The disease is increasingly being recognized in various parts of the world. While histoplasmosis was initially endemic to regions such as the Ohio and Mississippi river valleys, and sub-Saharan Africa, its reach has expanded to the Caribbean, Southeast Asia, and throughout South and Central America.
The prevalence of histoplasmosis may be underestimated due to frequent misdiagnosis, as it is often confused with conditions such as tuberculosis or emergomycosis. Moreover, in many countries, the requirement for reporting histoplasmosis infections to health authorities is not mandatory, hindering accurate tracking of the disease's distribution and prevalence. Histoplasmosis has been reported in numerous countries across Africa, including: Ethiopia, Kenya, Rwanda, Tanzania, Uganda, and Somalia; South Africa, Zimbabwe, Zambia, Mozambique, Malawi, and Angola; Burkina Faso, Cameroon, Côte d’Ivoire, The Gambia, Ghana, Guinea, Guinea-Bissau, Liberia, Mali, Mauritania, Nigeria, Senegal, Sierra Leone, and Togo; Egypt, Morocco, and Tunisia (Fig.1).
2.7. Sporotrichosis
Sporotrichosis is a sub-acute to chronic fungal infection caused by thermal dimorphic fungi belonging to the genus Sporothrix [35]. This disease is predominantly found in tropical and subtropical regions and is typically transmitted through traumatic injury that allows fungal spores to enter the host, classifying it as an implantation mycosis [35].
The clinical manifestations of sporotrichosis can be broadly categorized into skin, mucosal, systemic, and immunoreactive forms. The most common presentations include cutaneous or subcutaneous lesions and lymphadenopathy, particularly in cases of disseminated disease [36,37]. Although sporotrichosis is rarely life-threatening, it can lead to significant morbidity and a marked decline in quality of life. The ecological niche of Sporothrix fungi is primarily found in soil and decaying plant matter [35]. Infection often occurs during activities such as farming, gardening, animal husbandry, and mining, where there is increased risk of exposure to the spores. Zoonotic transmission is also prevalent, with cases frequently linked to interactions with infected animals.
Recently, sporotrichosis has been recognized as one of the deep mycoses classified among neglected tropical diseases. The ecology and epidemiology of this infection exhibit variations across different geographical regions, contributing to its distinct patterns of occurrence. Reported cases of sporotrichosis have emerged from various countries, including Ethiopia, Madagascar, Mozambique, Sudan, Uganda, Zambia, Zimbabwe, Ghana, Niger, Nigeria, Sierra Leone, the Democratic Republic of the Congo, South Africa, Egypt, Libya, and Morocco (Fig.1).
2.8. Talaromycosis:
Talaromycosis, formerly referred to as penicilliosis, is a fungal infection stemming from the organism Talaromyces marneffei (previously known as Penicillium marneffei) [38]. This disease is primarily found in East and Southeast Asia and is classified as a neglected tropical illness [38].
Patients may exhibit a variety of symptoms, including non-painful skin lesions, particularly on the face and neck, fever, anemia, swollen lymph nodes, and hepatic involvement. It predominantly affects individuals with weakened immune systems, such as those living with HIV/AIDS, cancer patients, individuals who have undergone organ transplants, those on long-term corticosteroid therapy, the elderly, malnourished persons, or individuals with autoimmune disorders [39].
Talaromyces marneffei is notable for being the only thermally dimorphic fungus within the Talaromyces genus [39,40]. This means that, like many other dimorphic fungi, it exists as a mold in external environments but transforms into small, round yeast cells when it infects a host's tissues. Although there is limited information available regarding its natural habitat, the fungus has been retrieved from soil samples [39,40]. Research suggests that heavy rainfall may create conditions conducive to the growth and spread of this fungus. The transmission of the infection is believed to occur through the inhalation of fungal spores that originate from unidentified sources in the environment. The incubation period for Talaromyces marneffei can differ, and it is possible for the infection to remain dormant and asymptomatic for extended periods [39,40]. Cases have also been identified in various regions across Africa, including Uganda, Burkina Faso, Ghana, Nigeria, Togo, and South Africa (Fig.1).
2.9. Lobomycosis
Lobomycosis, a rare cutaneous fungal infection primarily caused by Lacazia loboi, Its distribution is almost exclusive in the Americas, and it has a particularly high prevalence in the Amazon basin [41]. Cases of lobomycosis have been reported only in dolphins and humans [41]. The fungus had been demonstrated in the soil and vegeatation, as well as aquatic environments [41]. In Africa, it has been reported in South Africa (Fig.1). With limited cases documented, this infection emphasizes a gap in our understanding of its transmission dynamics and risk factors within the region. Further investigation is warranted to develop appropriate public health responses.
2.10. Paracoccidioidomycosis
Paracoccidioidomycosis is a systemic fungal infection caused by two thermally dimorphic fungi: Paracoccidioides brasiliensis and Paracoccidioides lutzii. It primarily occurs in the humid subtropical regions of Latin America, including Brazil, Argentina, Colombia, and Venezuela, as well as parts of Central America [42]. The natural habit of the fungus is still undetermined however, it hypothesized that the fungus is able to survive and proliferate in the soil [43]. The fungus is then enter via the respiratory tract or injuries through the skin and mucous membrane [43].
The lungs are the main site of infection, which typically results from inhaling conidia and mycelial fragments. In many cases, the infection is asymptomatic. There are two main forms of paracoccidioidomycosis: the acute/subacute form, often referred to as juvenile paracoccidioidomycosis, and the chronic form, also known as adult paracoccidioidomycosis [44]. The acute or subacute forms account for approximately 10% of clinical cases and are typically seen in children and adolescents under 16 years old, affecting both genders equally. Common clinical features include lymphadenopathy, hepatosplenomegaly, fever, weight loss, malaise, and various skin lesions, while respiratory symptoms and mucous membrane involvement are rare [45]. In contrast, the chronic form is more common in adults over 16, with a notable male-to-female ratio of 20:1, likely due to the inhibitory effects of estrogen on the conversion of mycelial forms to yeast. Patients may exhibit primary lung infections, cough, dyspnea, fever, weight loss, and complications related to chronic lung disease, including fibrosis and emphysema. Additional symptoms may involve mucous membrane lesions, skin lesions, and cervical lymphadenopathy. Risk factors for developing paracoccidioidomycosis include agricultural occupations, malnutrition, smoking, and alcohol use [46,47].
Notably, paracoccidioidomycosis has not been documented in Africa, raising questions about whether the disease is genuinely absent from the continent or whether underreporting and inadequate surveillance have led to missed cases.
2.11. Aspergillosis
Aspergillosis is an infection caused by a group of molds known as Aspergillus, which are commonly found in the environment [48]. These fungi are prevalent in soil, plant debris, and decaying organic matter [48]. While most people inhale Aspergillus spores without any ill effects, individuals with weakened immune systems, pre-existing lung diseases, or certain risk factors may develop health issues ranging from allergic responses to severe respiratory infections [49].
Aspergillus species are distributed widely across the globe, thriving in both indoor and outdoor environments. They are especially prominent in tropical and subtropical regions, where humidity and temperature favor their growth. In many countries across Africa, including those listed such as Burundi; Djibouti; Eritrea; Ethiopia; Kenya; Madagascar; Malawi; Mozambique; Rwanda; Somalia; Sudan; Tanzania; Uganda; Zambia; Zimbabwe; Benin; Burkina Faso; Cameroon; Cabo Verde; Côte d’Ivoire; Ghana; Guinea-Bissau; Liberia; Mali; Nigeria; Senegal; Sierra Leone; Angola; Central African Republic; Democratic Republic of the Congo; Lesotho; Swaziland; Botswana; Namibia; South Africa; Algeria; Egypt; Libyan Arab Jamahiriya; Morocco; and Tunisia (Fig.1).
2.12. Eumycetoma
Eumycetoma is a chronic granulomatous infectious disease characterized by a triad of symptoms: painless swelling, the presence of discharging sinuses, and the discharge of "grains," which are the causative agents encased in a protective matrix [50]. This condition involves a complex array of pathogens, with over 60 different fungal species associated with its development, presenting a significant challenge to global health [50].
The agents responsible for eumycetoma can infect a wide variety of hosts, including humans, animals, and plants, as well as impacting agricultural and food products [50]. The disease is prevalent in diverse environmental settings worldwide, making its control and management crucial. The impact of eumycetoma extends beyond individual health, affecting animal and environmental health, as well as socio-cultural and economic factors, thereby threatening food security and safety.
Recent reports indicate a troubling rise in eumycetoma incidence rates, along with an increasing diversity of hosts and geographical spread. Contributing factors to this trend include climate change, globalization, poor living conditions, and inadequate hygiene and sanitation practices. These elements create an environment conducive to the spread of eumycetoma and amplify its impact on communities.
Eumycetoma has been documented in numerous countries across Africa, including Eritrea; Ethiopia; Kenya; Madagascar; Mauritius; Rwanda; Somalia; Sudan; Tanzania; Uganda; Cameroon; The Gambia; Ghana; Guinea; Guinea-Bissau; Liberia; Mali; Mauritania; Niger; Nigeria; Senegal; Togo; Angola; Chad; Democratic Republic of the Congo; Republic of Congo; Namibia; South Africa; Algeria; Egypt; Libyan Arab Jamahiriya; Morocco; and Tunisia (Fig.1).
2.13. Malassezia Infection (pityriasis)
Malassezia infections, commonly known as pityriasis, are conditions caused by the Malassezia genus of fungi, which are part of the normal skin flora in humans and other mammals [51]. These lipid-dependent yeasts are naturally found on the skin surface and can sometimes lead to various skin disorders, including pityriasis versicolor, a condition characterized by discolored patches on the skin [51]. While Malassezia is ubiquitous, its infections have been reported in various countries across globe, indicating a widespread presence and potential for infection. The primary causative agents of pityriasis are species of the Malassezia genus, with Malassezia furfur being the most frequently implicated [51]. Malassezia infections are primarily associated with humans, but they can also affect other mammals, including dogs and cats [52]. In humans, the infections can occur in individuals of any age, but are more frequently observed in adolescents and young adults, possibly due to hormonal changes affecting sebum production [52]. The transmission of Malassezia infections is not fully understood as the fungi are commonly present on the skin without causing harm. Pityriasis versicolor is considered not contagious, but similar conditions may arise in susceptible hosts due to environmental triggers [52]. This infection had been reported in Ethiopia; Kenya; Madagascar; Malawi; Mauritius; Mayotte; Rwanda; Sudan; Tanzania; Uganda; Zambia; Cameroon; Côte d’Ivoire; The Gambia; Ghana; Liberia; Mali; Nigeria; Senegal; Angola; Central African Republic; Chad; Democratic Republic of the Congo; Gabon; Algeria; Egypt; Libyan Arab Jamahiriya; Morocco and Tunisia (Fig.1).
3. Conclusions and Future Perspective:
The rising incidence of zoonotic fungal diseases across Africa poses a significant challenge to public health systems, emphasizing the urgent need for a comprehensive and integrated strategy for disease prevention and management. The emergence of infections such as emergomycosis, blastomycosis, coccidioidomycosis, cryptococcosis, dermatophytosis, histoplasmosis, sporotrichosis, and eumycetoma underscores the intricate connections between human, animal, and environmental health, as encapsulated by the One Health framework. Since approximately 75% of emerging infectious diseases originate from animal reservoirs, it is vital to enhance surveillance systems and deepen our understanding of these zoonotic fungal pathogens to prevent future outbreaks and protect public health.
To effectively address this multi-dimensional public health threat, targeted interventions are necessary. Key actions include the development of robust surveillance mechanisms to monitor fungal infections in humans, animals, and the environment, ensuring timely identification and response to emerging threats. Public health entities should collaborate closely with veterinary services and environmental agencies to establish comprehensive surveillance networks that facilitate proactive measures.
Increased awareness among healthcare professionals, veterinarians, and the public regarding zoonotic fungal infections is of paramount importance. Educational campaigns should emphasize prevention strategies, proper hygiene practices, and the critical need for early medical intervention.
Enhancing access to healthcare, particularly in rural and underserved regions, will significantly improve diagnostic capacity and treatment options. Training healthcare workers to promptly recognize signs of fungal infections can lead to timely treatment, ultimately reducing complications and fatalities. Furthermore, investing in research to understand the epidemiology, ecology, and transmission dynamics of zoonotic fungal diseases will provide essential insights to inform public health policies. Collaboration with academic institutions and international organizations will stimulate the development of innovative solutions and treatments.
Improving diagnostic capacity is crucial in addressing the burden of zoonotic fungal diseases in Africa, where there is a significant lack of diagnostic tools for fungal infections [53]. A comprehensive survey conducted in 2023 across 47 African countries assessed the diagnostic capabilities for skin fungal diseases and revealed notable disparities in availability and quality [53]. Only 15% of the countries offer skin biopsies in the public sector, while 45% do so in the private sector. However, 46% of countries perform skin biopsies regularly, mainly in university hospitals. Direct microscopy is utilized in only 42% of public sector facilities, with 21% not employing this method at all. Fungal cultures are conducted in 44% of public sector facilities, but 20% lack fungal culture services entirely, and 44% do not offer this in either the public or private sectors. Histopathological examinations are frequently used in 40% of public sector countries, but 20% do not utilize this essential diagnostic method. Economic barriers, particularly the cost of diagnostics, significantly hinder accessibility, resulting in underutilization of available services. To address these gaps, investment in advanced laboratory technologies and infrastructure is necessary, alongside the implementation of comprehensive training programs for healthcare providers in diagnostic methodologies. Establishing specialized regional laboratories capable of conducting advanced tests and providing rapid results will support timely clinical decision-making and response to outbreaks. Additionally, promoting awareness of the importance of fungal diagnostics among healthcare providers and patients, as well as implementing strategies to subsidize costs, can further improve the utilization rates of essential diagnostic services. By enhancing the diagnostic capacity for zoonotic fungal diseases, healthcare systems in Africa can facilitate early detection and effective management of these emerging threats, ultimately reducing their public health impact.
Moreover, emphasizing a One Health approach will foster collaboration across disciplines, integrating human, animal, and environmental health into one cohesive strategy. Such initiatives can help mitigate the risks associated with zoonotic diseases while enhancing overall health outcomes for communities.
In conclusion, the public health implications of emerging zoonotic fungal diseases in Africa necessitate immediate and coordinated actions. By leveraging the One Health approach, we can establish a proactive framework that recognizes the interconnectedness of health sectors, thereby improving disease prevention and control strategies. Strengthening this framework will ultimately enhance health security for individuals, animals, and ecosystems across the African continent, empowering communities to better withstand the challenges posed by these emerging pathogens.
Author Contributions
Conceptualization, A.A.; methodology, A.A.; and E.E.S; validation, A.A., E.E.S. and N.S.M.; formal analysis, A.A., E.E.S. and N.S.M.; investigation, A.A., E.E.S. and N.S.M.; resources, A.A., E.E.S. and N.S.M.; data curation, A.A., E.E.S. and N.S.M.; writing—original draft preparation, A.A., E.E.S. and N.S.M.; writing—review and editing, A.A., E.E.S. and N.S.M.; visualization, A.A., E.E.S. and N.S.M.; supervision, A.A.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
All data used for the development of this review is available online.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AIDS | Acquired immunodeficiency syndrome |
| CNS | Central nervous system |
| HIV | Human Immunodeficiency virus |
Appendix A
Appendix A
Data set for the diversity and distribution of Zoonotic fungal diseases in Africa.
References
- Rodrigues, M.L.; Nosanchuk, J.D. Fungal Diseases as Neglected Pathogens: A Wake-Up Call to Public Health Officials. In Advances in Clinical Immunology, Medical Microbiology, COVID-19, and Big Data; Jenny Stanford Publishing, 2021 ISBN 978-1-00-318043-2.
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and Multi-National Prevalence of Fungal Diseases—Estimate Precision. Journal of Fungi 2017, 3, 57. [Google Scholar] [CrossRef]
- Rayens, E.; Norris, K.A. Prevalence and Healthcare Burden of Fungal Infections in the United States. Open Forum Infectious Diseases, 2022; 9, ofab593. [Google Scholar] [CrossRef]
- Low, C.-Y.; Rotstein, C. Emerging Fungal Infections in Immunocompromised Patients. F1000 Med Rep 2011, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Kundu, R.; Bansal, Y.; Singla, N. The Zoonotic Potential of Fungal Pathogens: Another Dimension of the One Health Approach. Diagnostics 2024, 14, 2050. [Google Scholar] [CrossRef]
- Rahman, M.T.; Sobur, M.A.; Islam, M.S.; Ievy, S.; Hossain, M.J.; El Zowalaty, M.E.; Rahman, A.T.; Ashour, H.M. Zoonotic Diseases: Etiology, Impact, and Control. Microorganisms 2020, 8, 1405. [Google Scholar] [CrossRef]
- One Health: Fungal Pathogens of Humans, Animals, and Plants: Report on an American Academy of Microbiology Colloquium Held in Washington, DC, on October 18, 2017; American Academy of Microbiology Colloquia Reports; American Society for Microbiology: Washington (DC), 2019.
- Carpouron, J.E.; de Hoog, S.; Gentekaki, E.; Hyde, K.D. Emerging Animal-Associated Fungal Diseases. Journal of Fungi 2022, 8, 611. [Google Scholar] [CrossRef]
- Esposito, M.M.; Turku, S.; Lehrfield, L.; Shoman, A. The Impact of Human Activities on Zoonotic Infection Transmissions. Animals 2023, 13, 1646. [Google Scholar] [CrossRef]
- Vinayagamoorthy, K.; Gangavaram, D.R.; Skiada, A.; Prakash, H. Emergomycosis, an Emerging Thermally Dimorphic Fungal Infection: A Systematic Review. Journal of Fungi 2023, 9, 1039. [Google Scholar] [CrossRef]
- He, D.; Quan, M.; Zhong, H.; Chen, Z.; Wang, X.; He, F.; Qu, J.; Zhou, T.; Lv, X.; Zong, Z. Emergomyces Orientalis Emergomycosis Diagnosed by Metagenomic Next-Generation Sequencing. Emerg Infect Dis 2021, 27, 2740–2742. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Lerm, B.; Hoving, J.C.; Kenyon, C.; Horsnell, W.G.; Basson, W.J.; Otieno-Odhiambo, P.; Govender, N.P.; Colebunders, R.; Botha, A. Emergomyces Africanus in Soil, South Africa. Emerg Infect Dis 2018, 24, 377–380. [Google Scholar] [CrossRef]
- Samaddar, A.; Sharma, A. Emergomycosis, an Emerging Systemic Mycosis in Immunocompromised Patients: Current Trends and Future Prospects. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- Miceli, A.; Krishnamurthy, K. Blastomycosis. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Schwartz, I.S.; Muñoz, J.F.; Kenyon, C.R.; Govender, N.P.; McTaggart, L.; Maphanga, T.G.; Richardson, S.; Becker, P.; Cuomo, C.A.; McEwen, J.G.; et al. Blastomycosis in Africa and the Middle East: A Comprehensive Review of Reported Cases and Reanalysis of Historical Isolates Based on Molecular Data. Clinical Infectious Diseases 2021, 73, e1560–e1569. [Google Scholar] [CrossRef]
- Pullen, M.F.; Alpern, J.D.; Bahr, N.C. Blastomycosis—Some Progress but Still Much to Learn. Journal of Fungi 2022, 8, 824. [Google Scholar] [CrossRef]
- Linder, K.A.; Kauffman, C.A.; Miceli, M.H. Blastomycosis: A Review of Mycological and Clinical Aspects. Journal of Fungi 2023, 9, 117. [Google Scholar] [CrossRef]
- Akram, S.M.; Koirala, J. Coccidioidomycosis. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Kirkland, T.N.; Fierer, J. Coccidioides Immitis and Posadasii; A Review of Their Biology, Genomics, Pathogenesis, and Host Immunity. Virulence 2018, 9, 1426–1435. [Google Scholar] [CrossRef]
- Crum, N.F. Coccidioidomycosis: A Contemporary Review. Infect Dis Ther 2022, 11, 713–742. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, V.; Chaturvedi, S. Cryptococcus Gattii: A Resurgent Fungal Pathogen. Trends in Microbiology 2011, 19, 564–571. [Google Scholar] [CrossRef]
- Pescador Ruschel, M.A.; Thapa, B. Cryptococcal Meningitis. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Kruithoff, C.; Gamal, A.; McCormick, T.S.; Ghannoum, M.A. Dermatophyte Infections Worldwide: Increase in Incidence and Associated Antifungal Resistance. Life (Basel) 2023, 14, 1. [Google Scholar] [CrossRef]
- Keshwania, P.; Kaur, N.; Chauhan, J.; Sharma, G.; Afzal, O.; Alfawaz Altamimi, A.S.; Almalki, W.H. Superficial Dermatophytosis across the World’s Populations: Potential Benefits from Nanocarrier-Based Therapies and Rising Challenges. ACS Omega 2023, 8, 31575–31599. [Google Scholar] [CrossRef]
- Segal, E.; Elad, D. Human and Zoonotic Dermatophytoses: Epidemiological Aspects. Front Microbiol 2021, 12, 713532. [Google Scholar] [CrossRef]
- Kottferová, L.; Molnár, L.; Major, P.; Sesztáková, E.; Kuzyšinová, K.; Vrabec, V.; Kottferová, J. Hedgehog Dermatophytosis: Understanding Trichophyton Erinacei Infection in Pet Hedgehogs and Its Implications for Human Health. J Fungi (Basel) 2023, 9, 1132. [Google Scholar] [CrossRef]
- Aimoldina, A.; Smagulova, A.; Batpenova, G.; Konnikov, N.; Algazina, T.; Jetpisbayeva, Z.; Azanbayeva, D.; Amantayev, D.; Kiyan, V. Mycological Profile and Associated Factors Among Patients with Dermatophytosis in Astana, Kazakhstan. J Fungi (Basel) 2025, 11, 65. [Google Scholar] [CrossRef]
- Verma, S.; Madhu, R. The Great Indian Epidemic of Superficial Dermatophytosis: An Appraisal. Indian J Dermatol 2017, 62, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Uhrlaß, S.; Verma, S.B.; Gräser, Y.; Rezaei-Matehkolaei, A.; Hatami, M.; Schaller, M.; Nenoff, P. Trichophyton Indotineae-An Emerging Pathogen Causing Recalcitrant Dermatophytoses in India and Worldwide-A Multidimensional Perspective. J Fungi (Basel) 2022, 8, 757. [Google Scholar] [CrossRef]
- Deng, R.; Wang, X.; Li, R. Dermatophyte Infection: From Fungal Pathogenicity to Host Immune Responses. Front Immunol 2023, 14, 1285887. [Google Scholar] [CrossRef] [PubMed]
- Sonego, B.; Corio, A.; Mazzoletti, V.; Zerbato, V.; Benini, A.; di Meo, N.; Zalaudek, I.; Stinco, G.; Errichetti, E.; Zelin, E. Trichophyton Indotineae, an Emerging Drug-Resistant Dermatophyte: A Review of the Treatment Options. J Clin Med 2024, 13, 3558. [Google Scholar] [CrossRef]
- Akram, S.M.; Koirala, J. Histoplasmosis. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Ocansey, B.K.; Kosmidis, C.; Agyei, M.; Dorkenoo, A.M.; Ayanlowo, O.O.; Oladele, R.O.; Darre, T.; Denning, D.W. Histoplasmosis in Africa: Current Perspectives, Knowledge Gaps, and Research Priorities. PLoS Negl Trop Dis 2022, 16, e0010111. [Google Scholar] [CrossRef]
- Falci, D.R.; Monteiro, A.A.; Braz Caurio, C.F.; Magalhães, T.C.O.; Xavier, M.O.; Basso, R.P.; Melo, M.; Schwarzbold, A.V.; Ferreira, P.R.A.; Vidal, J.E.; et al. Histoplasmosis, An Underdiagnosed Disease Affecting People Living With HIV/AIDS in Brazil: Results of a Multicenter Prospective Cohort Study Using Both Classical Mycology Tests and Histoplasma Urine Antigen Detection. Open Forum Infect Dis 2019, 6, ofz073. [Google Scholar] [CrossRef]
- Barros, M.B. de L.; de Almeida Paes, R.; Schubach, A.O. Sporothrix Schenckii and Sporotrichosis. Clin Microbiol Rev 2011, 24, 633–654. [Google Scholar] [CrossRef]
- Martínez-Herrera, E.; Arenas, R.; Hernández-Castro, R.; Frías-De-León, M.G.; Rodríguez-Cerdeira, C. Uncommon Clinical Presentations of Sporotrichosis: A Two-Case Report. Pathogens 2021, 10, 1249. [Google Scholar] [CrossRef]
- Orofino-Costa, R.; Macedo, P.M. de; Rodrigues, A.M.; Bernardes-Engemann, A.R. Sporotrichosis: An Update on Epidemiology, Etiopathogenesis, Laboratory and Clinical Therapeutics. An Bras Dermatol 2017, 92, 606–620. [Google Scholar] [CrossRef]
- Wang, F.; Han, R.; Chen, S. An Overlooked and Underrated Endemic Mycosis-Talaromycosis and the Pathogenic Fungus Talaromyces Marneffei. Clin Microbiol Rev 2023, 36, e0005122. [Google Scholar] [CrossRef]
- Mahajan, M. Talaromyces Marneffei. Emerg Infect Dis 2021, 27, 2278. [Google Scholar] [CrossRef]
- Pruksaphon, K.; Nosanchuk, J.D.; Ratanabanangkoon, K.; Youngchim, S. Talaromyces Marneffei Infection: Virulence, Intracellular Lifestyle and Host Defense Mechanisms. Journal of Fungi 2022, 8, 200. [Google Scholar] [CrossRef]
- Francesconi, V.A.; Klein, A.P.; Santos, A.P.B.G.; Ramasawmy, R.; Francesconi, F. Lobomycosis: Epidemiology, Clinical Presentation, and Management Options. Therapeutics and Clinical Risk Management 2014, 10, 851–860. [Google Scholar] [CrossRef]
- Cordova, L.A.; Torres, J. Paracoccidioidomycosis. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Brummer, E.; Castaneda, E.; Restrepo, A. Paracoccidioidomycosis: An Update. Clin Microbiol Rev 1993, 6, 89–117. [Google Scholar] [CrossRef] [PubMed]
- Burger, E. Paracoccidioidomycosis Protective Immunity. J Fungi (Basel) 2021, 7, 137. [Google Scholar] [CrossRef]
- Marques, S.A.; Lastória, J.C.; Camargo, R.M.P. de; Marques, M.E.A. Paracoccidioidomycosis: Acute-Subacute Clinical Form, Juvenile Type. An Bras Dermatol 2016, 91, 384–386. [Google Scholar] [CrossRef]
- Bongomin, F.; Kibone, W.; Okot, J.; Nsenga, L.; Olum, R.; Baluku, J.B. Fungal Diseases in Africa: Epidemiologic, Diagnostic and Therapeutic Advances. Ther Adv Infect Dis 2022, 9, 20499361221081441. [Google Scholar] [CrossRef]
- Bongomin, F.; Ekeng, B.E.; Kibone, W.; Nsenga, L.; Olum, R.; Itam-Eyo, A.; Kuate, M.P.N.; Pebolo, F.P.; Davies, A.A.; Manga, M.; et al. Invasive Fungal Diseases in Africa: A Critical Literature Review. Journal of Fungi 2022, 8, 1236. [Google Scholar] [CrossRef]
- Mousavi, B.; Hedayati, M.T.; Hedayati, N.; Ilkit, M.; Syedmousavi, S. Aspergillus Species in Indoor Environments and Their Possible Occupational and Public Health Hazards. Curr Med Mycol 2016, 2, 36–42. [Google Scholar] [CrossRef]
- Sisodia, J.; Bajaj, T. Allergic Bronchopulmonary Aspergillosis. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Siddig, E.E.; Ahmed, A. The Urgent Need for Developing and Implementing a Multisectoral One Health Strategy for the Surveillance, Prevention, and Control of Eumycetoma. IJID One Health 2024, 100048. [Google Scholar] [CrossRef]
- Gaitanis, G.; Magiatis, P.; Hantschke, M.; Bassukas, I.D.; Velegraki, A. The Malassezia Genus in Skin and Systemic Diseases. Clinical Microbiology Reviews 2012, 25, 106–141. [Google Scholar] [CrossRef] [PubMed]
- Hobi, S.; Cafarchia, C.; Romano, V.; Barrs, V.R. Malassezia: Zoonotic Implications, Parallels and Differences in Colonization and Disease in Humans and Animals. Journal of Fungi 2022, 8, 708. [Google Scholar] [CrossRef] [PubMed]
- Badiane, A.S.; Ramarozatovo, L.S.; Doumbo, S.N.; Dorkenoo, A.M.; Mandengue, C.; Dunaisk, C.M.; Ball, M.; Dia, M.K.; Ngaya, G.S.L.; Mahamat, H.H.; et al. Diagnostic Capacity for Cutaneous Fungal Diseases in the African Continent. International Journal of Dermatology 2023, 62, 1131–1141. [Google Scholar] [CrossRef]
Figure 1.
Showing the distributions and diversity of Medically important zoonotic fungal diseases among different African countries.
Figure 1.
Showing the distributions and diversity of Medically important zoonotic fungal diseases among different African countries.
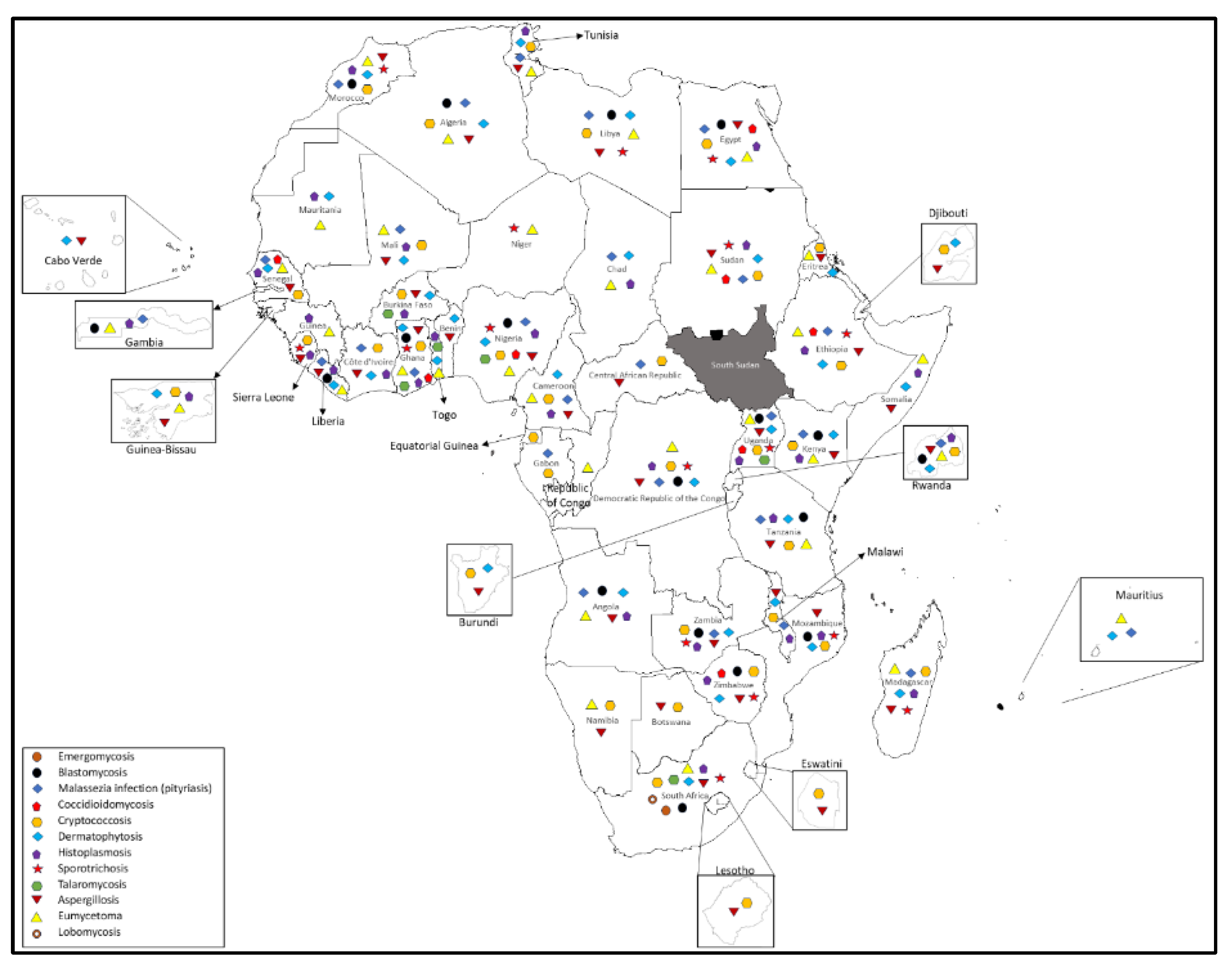

Table 1.
Demonstrating Zoonotic fungal diseases and their causative agents, hosts range, epidemiological and clinical characteristics.
Table 1.
Demonstrating Zoonotic fungal diseases and their causative agents, hosts range, epidemiological and clinical characteristics.
| Disease | Causative agents | Animal hosts | Mode of transmission | Clinical manifestation in Animals | Clinical manifestation in human |
| Emergomycosis | Emmonsia spp | Rodents | Inhalation of the fungus | Deep mycosis | Disseminated mycosis |
| Blastomycosis | Blastomyces dermatitidis | Cats, dogs, horses and marine mammals | Inhalation of airborne conidia | Cutaneous, pulmonary, disseminated infection | Cutaneous, pulmonary, disseminated infection |
| Coccidomycosis |
Coccidioides immitis; Coccidioides posadasii |
Cattles, Cats, dogs, horses, snakes, reptiles and marine mammals | Inhalation of conidia and skin trauma | Self-limiting to chronic. Dissemination | Cutaneous, pulmonary, disseminated infection |
| Cryptococosis |
Cryptococcus neoformans; Cryptococcus gattii |
Cattles, goats, Cats, dogs, horses and marine mammals | Inhalation of the fungus; implantation of the fungus into the skin | Respiratory tract, CNS, eyes, and skin. | Cutaneous, eye, respiratory and central nervous system infection |
| Dermatophytosis |
Microsporum spp.; Trichophyton spp |
Cats, dog, cattle, goats, horses, Camels, pigs, rodents, bats | Direct contact with the infected animals or material contaminated from the site of the infection | Ring lesion with central healing and crusts at the peripheral area, some degree of folliculitis |
Tinea |
| Histoplasmosis | Histoplasma capsulatum | Cattle, sheep, horses, dogs, cats, birds, bats, rats, skunks, and opossums | Inhalation of the fungus | Cutaneous, pulmonary, disseminated infection | Cutaneous, pulmonary, disseminated infection |
| Sporotrichosis |
Sporothrix schenckii; Sporothix brasiliensis |
dogs, cats, horses, cows, camels, dolphins, goats, mules, birds, pigs, rats, armadillos | direct inoculation of the organism into skin wounds via contact with plants, soil, or penetrating foreign bodies | lymphocutaneous, cutaneous, and disseminated | lymphocutaneous, cutaneous, and disseminated |
| Talaromycosis | Talaromyces marneffei | Bamboo rats, dogs and cats | Unknown; but it hypothesize that by inhalation of the fungus from the environment | Cutaneous, respiratory and disseminated disease | Cutaneous, respiratory and disseminated disease |
| Lobomycosis | Lacazia loboi | Dolphins | Traumatic inoculation | Cutaneous disease | Cutaneous disease |
| Paracoccidomycosis |
Paracoccidioides brasiliensis; Paracoccidioides lutzii |
Dogs, armadillos and monkeys | Inhalation of the fungus, Inoculation of the organism into the subcutaneous tissues | Cutaneous (skin ulcers), adenitis, and disseminated disease | Mucocutenous, respiratory and disseminated disease |
| Aspergillosis | Aspergillus spp. | Domestic animals (dogs, horse, cats, poultry), birds, and wildlife | Inhaling airborne spores | Pulmonary mainly; cutaneous; and disseminated | Pulmonary mainly; cutaneous; and disseminated |
| Eumycetoma | More than 70 fungal species most prevalent one including Madurella spp.,; Falciformispora spp.,; Fusarium spp., Medicopsis spp., | Cats, Dogs, Horses, Turtles, Fish, Cattle, Tiger | Inoculation of the causative agents into the subcutaneous tissue | Subcutaneous disease mainly, however disseminated infection can also occur | Subcutaneous disease if the disease affected the extremities; respiratory (Lung involvement); CNS |
| Malassezia infection (pityriasis) |
Mallasezia spp. | Dogs, cats, cows, sheep, pig, horse, wild animals |
Normal commensals of the skin | Dermatitis, alopecia, stenosis, otitis externa |
Chronic superficial disease of the skin (pityriasis versicolor), folliculitis, seborrhoeic dermatitis and dandruff, fungaemia |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



