Submitted:
24 February 2025
Posted:
25 February 2025
You are already at the latest version
Abstract
Background: Echinacea purpurea is widely utilized in dietary supplements, nutraceuticals, and herbal medicine, yet its effectiveness and safety for children remain debated. Objective: To evaluate the effectiveness and safety of E. purpurea in the treatment of upper respiratory tract infection (URTI) and otitis media (OM) in children. Data sources: Embase, Cochrane Central Register of Controlled Trials (CENTRAL), ClinicalTrials.gov, PubMed from January 2000 to December 2023. Methods: This systematic review and meta-analysis were conducted and reported according to the PRISMA 2020 Checklist and Cochrane Training 2022 guidelines. Results: 9 randomized controlled trials with 1518 participants in the treatment group, 1651 participants in the placebo control group, met the selection criteria. Products derived from E. purpurea are highly diverse, utilizing different plant parts such as roots, leaves, and flowers, available in various dosage forms like capsules and extracts, and manufactured in numerous countries worldwide. Risk of bias was assessed according to the PEDro scale with 3 studies of excellent quality, 5 studies of high quality and 1 study of moderate quality.The meta-analysis found that E. purpurea significantly benefits URTI, reducing treatment duration (SMD = -0.19, 95% CI [-0.30; -0.09], p < 0.01), incidence (RR = 0.81, 95% CI [0.75; 0.87]), and antibiotic use (RR = 0.18, 95% CI [0.13; 0.25], p < 0.01). However, adverse events were moderately increased (RR = 1.38, 95% CI [1.08; 1.78]), though generally mild. For OM, E. purpurea lowered episode incidence (RR = 0.56, 95% CI [0.44; 0.73], p < 0.01) but did not shorten treatment duration (p = 0.10). Its effectiveness may be limited due to OM's bacterial etiology, often requiring antibiotics. While E. purpurea may help reduce recurrence, it is unlikely to speed recovery. Further research on optimal formulations and dosages is needed.The publication bias of pooled results as assessed by the funnel plot showed that the studies had certain bias, largely due to heterogeneity between studies. Conclusion: The meta-analysis of nine studies found that E. purpurea was effective in reducing the duration of treatment, the incidence of episodes, and antibiotic usage for URTI in children, with some positive effects on OM. This study systematically evaluates the efficacy and safety of E. purpurea in treating URTI and OM in children, providing evidence-based insights to guide clinical decisions and inform healthcare professionals and parents considering its use. However, the safety profile remains unclear, particularly regarding adverse events. Further research is required to standardize methodologies and confirm these results.
Keywords:
children
; common cold
; Echinacea purpurea
; otitis media
; upper respiratory tract infection
1. Introduction
In recent years, there has been growing interest in the use of dietary supplements, nutriceuticals or herbal medicine to support health and well-being. Echinacea purpurea, a member of the Echinacea genus, is known by its immune-stimulating compounds, antioxidants, antibacterial, antiviral, and antiparasitic properties [1,2]. These attributes render it pertinent in various commercial formulations, often recommended for addressing respiratory issues, urinary tract infections, and chronic wounds [3,4].
Upper respiratory tract infection (URTI) are prevalent illnesses characterized by symptoms such as nasal congestion, runny nose, sore throat, cough, and mild fever [5,6]. Viral infnections, including rhovirus, parainfluenza, respiratory syncytial virus, influenza, adenovirus, and coronaviruses are common causative agents transmitted through contact with infected individuals' nasal secretions and saliva [7]. The common cold is a prevalent form of URTI, primarily caused by viruses, with symptoms largely similar to those of URTIs. Weather changes, particularly during the cold season, often weaken the immune system and increase the risk of catching a cold, subsequently elevating the risk of upper respiratory tract infections.
Otitis media (OM) is a notable URTI complication, particularly in young children, often occurring after prolonged flu or cold episodes. Despite the challenges posed by the immature immune system in children, antibiotics are frequently prescribed for URTI and OM treatment, though their efficacy against viral infections [8,9].
To address medication side effects, natural products are increasingly preferred for pediatric conditions, with Echinacea purpurea emerging as a popular herbal supplement used to treat URTIs due to its immune-stimulating properties [1,10]. Despite its widespread use, multiple studies on efficacy of E. purpurea for treating URTIs show mixed results, and the effectiveness and safety of E. purpurea in pediatric populations remain unclear [11,12]. The widespread use of E. purpurea as a dietary supplement for immune support in children has garnered both endorsement and caution, given varying findings on its safety and efficacy. While some studies report only minor side effects, such as mild gastrointestinal discomfort or skin reactions, others underscore the importance of considering product variability and its potential impact on safety. This study aims to clarify the efficacy and safety profile of E. purpurea for managing URTIs and complications related to OM in children, with a focus on its role within nutrition and herbal supplementation.
Children and adults exhibit significant differences in immune responses to illnesses and treatments, including the use of E. purpurea. In children, the underdeveloped immune system heightens vulnerability to pathogens and potential side effects of therapeutic interventions. Conversely, adults possess a mature immune system, enabling more robust responses to stimuli with reduced risk. Active components in E. Purpurea, such as alkamides, polysaccharides, and phenolic acids, exert immunomodulatory effects but may overstimulate the immature immune systems of children, potentially leading to side effects such as rash, urticaria, or gastrointestinal disturbances, which are less common in adults [4,13,14]. Hence, research on Echinacea products must account for the unique physiological and immunological characteristics of pediatric populations, avoiding direct extrapolations from adult studies
2. Methods
Study design: The study adheres to the PRISMA 2020 checklist and Cochrane Training (Version 6.3, 2022) for a robust systematic review and meta-analysis, registered on PROSPERO (ID: CRD42024502333).
Participants: Randomized Controlled Trials (RCTs) evaluating efficacy of E. purpurea in treating URTIs and OM in children.
Scope: Unrestricted language search from January 2000 to December 2023, sourcing studies from Embase, Cochrane CENTRAL, ClinicalTrials.gov, and PubMed.
PICOS Questions:
Population (P): Children (1-12 years) with URTI or OM. Intervention (I): E. purpurea. Comparison (C): Placebo. Outcome (O): Treatment duration, the incidence of at least one episode, adverse events (AE), and antibiotic usage. Study design (S): RCTs
Search and Data Collection
Strategy: Studies from January 2000 to December 2023 accessed via PubMed, Cochrane, ClinicalTrials.gov, and Embase. Keywords include Echinacea purpurea, children, Upper respiratory tract infection, common cold, and otitis media. The search strategy is detailed in Supplementary document 1. Data collection procedures followed the methodology previously outlined in reference [15].
Selection and Exclusion Criteria
Research inclusion: A randomized, placebo-controlled trial assessing preparations containing E. purpurea for the prevention and/or treatment of URTI and/or OM complications in children. The study should provide comprehensive information on two groups: the treatment group and the control group, with outcomes measured in at least one of the following areas: duration of treatment, incidence rate of at least one episode, antibiotic usage rate, or adverse events. The participants are children under 12 years of age, with health status ranging from healthy to those with URTI, the common cold, or OM complications.
Research exclusion: Survey studies. Non-clinical research. Uncontrolled trials. Conference abstracts without comprehensive research papers. Studies lacking detailed information on the treatment and control groups, where results are presented only in graphs or figures without specific numerical data.
Process: Covidence tool [16] (Cochrane) used for study selection. Two independent reviewers screened studies, with discrepancies resolved by a third reviewer.
Data collection: Two variables considered: continuous (Mean±SD) the results were analyzed using the relative risk (RR) outcome measure, offering insight into the relative probability of events occurring between two groups; and binary (N%) the analysis was conducted using the standardized mean difference (SMD), with different scales, providing a standardized measure of effect size. Extracted independently by two groups, discrepancies resolved by a fifth reviewer.
Publication quality assessment: The quality of the included studies was assessed using the PEDro scale [17], which comprises 11 items, 10 of which are scored. For this study, the PEDro scale was adapted to evaluate each criterion based on the information provided in the articles and the corresponding PEDro guidelines, with responses recorded as either 'Yes' or 'No.' Scores were categorized as follows: Low (0–3), Moderate (4–5), Good (6–8), and Excellent (9–10). A detailed summary table of the quality assessment for each study is provided, with comprehensive evidence for each criterion included in Supplementary document 2, in alignment with Cochrane recommendations. Any discrepancies during the assessment process were resolved through consultation with a third independent reviewer.
Meta-analysis: R Studio and meta packages used. Fixed and random-effects models applied, providing pooled effect estimates with risk ratios and standard mean differences. Heterogeneity assessed with I2.
Although sensitivity analyses are typically recommended to assess the stability of results in meta-analyses, the limited number of studies in our dataset did not meet the minimum threshold for reliable sensitivity analysis outcomes.
Bias evaluation: Publication bias assessed using funnel plots and Egger regression test [18], evaluating asymmetry for continuous and binary variables.
3. Result
3.1. Study Selection
The process of selecting studies is detailed in Figure 1. The research team identified 131 studies through a thorough search of reliable sources. After using Covidence to semi-automatically eliminate duplicate studies, the number reduced to 104. These studies underwent further screening based on titles and abstracts, with 71 articles excluded for reasons outlined in Figure 1. Following careful full-text review, an additional 24 articles were excluded, including 2 studies involving subjects over 12 years old, 8 studies with inappropriate designs, 2 non-trial reports, 10 studies lacking outcome variables related to URTI or OM, and 2 studies found to be duplicates with different titles by the same author group. Finally, 9 RCTs were selected for conducting meta-analysis.
3.2. Study Characteristics
The characteristics of the studies are detailed in Table 1. The participants in the studies were healthy children aged 1-12 years. The studies utilized E. purpurea and a combination of E. purpurea and E. angustifolia, using various parts such as root and aerial part. Among the 9 RCTs, four studies used E. purpurea products manufactured in the United States [10,19,20,21], two RCTs used products from Switzerland [22,23], and the remaining three studies were from the United Kingdom, Russia, and Germany [24,25,26]. The predominant formulation was liquid dosage, with two RCTs in tablet form [22,23] and two studies in nasal drop form [21,26]. Four studies used E. purpurea with alcohol [10,22,23,26], three studies used alcohol-free E. purpurea [20,24,25] and two studies used Echinacea with other supplements (vitamin C, propolis, and a few minor plant species, accounting for a small proportion) [19,21].
3.3. Risk of Bias in Studies
Table 2 summarizes the quality of the studies included in the comprehensive analysis. The quality scores ranged from 5 to 10 on the PEDro scale, with an average score of 7.56. Three studies [10,20,24] obtained excellent quality scores (9 or 10), five studies [19,22,23,25,26] were of high quality (scores between 6 and 8), and one study [21] was of moderate quality (score of 5).
3.4. Results of Meta-Analysis
3.4.1. URTI Meta-Analysis
- The treatment time:
Performing a comprehensive analysis with five studies [19,20,22,23,25] evaluating the duration of URTI treatment using E. purpurea in children, as results shown in Figure 2A. The data indicated statistically significant analysis (p < 0.01), with a standardized mean difference (SMD) of -0.19 and a confidence interval (CI) of 95% = [-0.30; -0.09]). There was a high heterogeneity among studies (I2 = 91%). Surveys of studies using large numbers [20,25] showed results that improved URTI treatment time but were not statistically significant. However, studies by Cohen and Ogal both show clear effectiveness. Therefore, it was concluded that E. purpurea is effective in reducing the duration of URTI treatment in children.
-Adverse event:
The meta-analysis of six studies [20,22,23,24,25,26] assessing the safety of E. purpurea in URTI treatment is presented in Figure 2B. The results indicated low heterogeneity (I2 = 33%). The fixed-effect model with a risk ratio (RR) of 1.38; CI 95% = [1.08; 1.78], and the random-effect model with RR = 1.45; CI 95% = [0.95; 2.22]. Thus, the use of E. purpurea tends to be safe, causing fewer side effects than placebo, but no statistical significance with the p-value of 0.19 (> 0.05).
To provide a comprehensive overview of safety, the research team synthesized and classified the adverse effects experienced by children in the studies. The severity classification was aligned for compatibility with a previously established grading system [27]. The summary table (Table 3) shows that most reported adverse effects were mild, with minimal and non-serious impact. Severe reactions were not reported in any of the studies included.
- The incidence of at least one:
Conducting a meta-analysis with five studies [19,20,22,23,25] (Figure 2C) revealed that the use of E. purpurea could significantly reduce the incidence of at least one episode of URTI in children (p < 0.01). The data also showed a relative risk of RR = 0.81; CI 95% = [0.75; 0.87], and a random-effect model with RR = 0.82; CI 95% = [0.64; 1.05]. However, the heterogeneity among studies was very high (I2 = 90%). Notably, one study indicated that the placebo group had a lower incidence than the intervention group [23].
-The antibiotic use:
Four studies [21,22,23,26] evaluating the impact of E. purpurea on the antibiotic prescription rate in URTI treatment were comprehensively analyzed (Figure 2D). The results showed significant heterogeneity (I2 = 79%), and the outcomes were statistically significant (p < 0.01). The overall effect model with RR = 0.18; CI 95% = [0.13; 0.25], and the random-effect model with RR = 0.27; CI 95% = [0.10; 0.72] indicated a clear reduction in antibiotic usage with the use of E. purpurea in URTI treatment for children.
3.4.2. Meta-Analysis for OM Treatment
- Duration of treatment:
Conducting a meta-analysis of two studies [10,21] for data on the duration of OM treatment in children using E. purpurea showed inconclusive impact (Figure 3A). The heterogeneity was relatively moderate (I2 = 64%), and the combined studies did not show statistically significant results (p = 0.10 > 0.05), with a SMD of 0.05 and a CI of 95% = [-0.14; 0.24]. The study with substantial weight [21] did not demonstrate a significant positive effect.
- The incidence of at least one:
Three studies [10,19,22] analyzing the rate of at least one episode of OM in children using E. purpurea were comprehensively analyzed (Figure 3B). The results indicated a statistically significant reduction in at least one episode of OM (p < 0.01), with high heterogeneity among studies (I2 = 88%). The overall effect model with RR = 0.56; CI 95% = [0.44; 0.73], and the random-effect model with RR = 0.74; CI 95% = [0.34; 1.62] suggested a positive impact. The study with substantial weight [19,22] demonstrated a significant reduction in the rate of at least one episode of OM.
3.5. Quality Assessment of Meta-Analyses
For URTI analysis: Funnel plots for URTI studies (Figure 4) showed asymmetry, indicating potential publication bias. Evaluation of safety and antibiotic usage did not reveal significant publication bias.
For OM complications: Funnel plots for OM-related analyses (Figure 5) suggested potential publication bias, particularly in the analysis of OM treatment duration. The assessment of at least one episode of OM showed an asymmetrical funnel plot but with no significant publication bias.
4. Discussion
4.1. Study Findings
The aim of this study was to determine the effectiveness of E. purpurea in children with URTI and complications such as OM. After an exhaustive search of reliable sources, 131 records were identified. Following the removal of duplicates and meticulous screening of titles, abstracts, and full texts, 9 eligible studies were included in the comprehensive analysis.
The studies included in the analysis utilized various E. purpurea products derived from roots, seeds, above-ground parts, or the entire plant during flowering. All 9 studies employed E. purpurea, except for a 2004 study by Cohen et al. [19], which used a combination of the upper part of E. purpurea and the root of E. angustifolia. Factors such as the type of E. purpurea product, the part of the plant used, and combinations with other supplements can significantly impact the efficacy of Echinacea. Specifically, studies using E. purpurea alone or in combination with E. angustifolia, and utilizing different parts of the plant such as the root or aerial parts, suggest that each part may uniquely affect the immune system. The root is generally considered to contain more active compounds, yet the aerial parts also exhibit certain effects [12]. Additionally, differences in chemical composition between E. purpurea and E. angustifolia may lead to variations in therapeutic effectiveness, warranting further analysis to identify the most suitable plant type or part for children. Moreover, combining E. purpurea with other supplements like vitamin C, honey, and various minor herbs appears to enhance its effects. This combination could potentially offer superior immune support compared to Echinacea alone [28]. This could inform future research and product development in the field.
The studies included in the analysis examined various E. purpurea products derived from roots, seeds, aerial parts, or the entire plant during flowering. Of the nine studies, all employed E. purpurea, except for one study by Cohen et al. (2004) [19], which used a combination of the aerial part of E. purpurea and the root of E. angustifolia. Factors such as the type of E. purpurea product, specific plant parts used, and combinations with other supplements can significantly influence the efficacy of Echinacea. Studies utilizing E. purpurea alone or in combination with E. angustifolia, and employing different plant parts, such as the root or aerial parts, suggest that each part may uniquely impact immune function. While the root is typically considered to contain higher levels of active compounds, the aerial parts also demonstrate certain beneficial effects [12]. Furthermore, differences in chemical composition between E. purpurea and E. angustifolia could lead to variations in therapeutic outcomes, warranting further analysis to determine the most appropriate plant type or part for pediatric use. Additionally, combining E. purpurea with supplements like vitamin C, honey, and other minor herbs appears to enhance its effects, potentially offering stronger immune support than Echinacea alone [28]. These insights could guide future research and product development in this field.
The products originated from different countries, with variations in formulations and dosages for different age groups. Liquid formulations were the predominant form, while tablet and nasal drop forms were also used. The formulation of Echinacea can significantly affect its absorption and duration of action. Liquid forms are typically absorbed more quickly, providing immediate effects, whereas tablets may offer prolonged effects due to slower absorption. Additionally, nasal drop formulations can directly target the respiratory system, which is particularly beneficial for treating symptoms like colds or respiratory infections. Optimizing the formulation for specific clinical situations is crucial. E. purpurea products from countries such as the United States, Switzerland, the United Kingdom, Russia, and Germany may yield different results due to varying manufacturing processes, including cultivation, harvesting, extraction, and formulation methods. For instance, studies showing better efficacy from a particular country could reflect the quality of the product or adherence to GMP standards in production. Furthermore, children aged 1-12 are a key demographic because their immune systems and development are still maturing. As a result, immune-supporting products like E. purpurea may have different effects compared to adults.
The risk of bias assessment using the PEDro scale indicated relatively high-quality studies, with 3 achieving excellent scores, 5 scoring high, and only 1 considered of moderate quality. Detail description of bias assessment can be located in Supplementary document 2.
The results of a meta-analysis of URTI in children show that E. purpurea helps reduce treatment time, reduces the incidence of at least one episode, and reduces the rate of antibiotic use which is relatively clear with p-values having statistical significance. Observation of studies on adverse events shows that using E. purpurea tends to be safer than the placebo group (the most common side effects are rash, and urticaria), however this result is not statistically significant (p-value > 0.05). A careful examination of individual studies with significant weight reveals that the incidence of rash and urticaria is higher in the E. purpurea group compared to the placebo group. Therefore, parents are advised to consult healthcare professionals and carefully consider before administering it to children.
For OM complications in children, a review of the significant weight studies found that E. purpurea was associated with a statistically significant reduction in the incidence of at least one episode. Regarding treatment time, E. purpurea did not reduce the number of treatment days, but this result was not statistically significant.
The effectiveness of E. purpurea for OM may be limited due to the different pathophysiology of OM compared to URTI, as OM often has a bacterial rather than viral etiology, requiring antibiotic intervention in severe cases. These findings support the potential role of E. purpurea as an adjunctive treatment for URTI in children. In contrast, the analysis of OM complications yielded less conclusive results. The stronger effects for URTI may be due to its viral etiology, which aligns with E. purpurea's immune-modulating properties. In contrast, OM often has a bacterial component, which may limit E. purpurea’s ability to reduce treatment duration once an infection occurs.These findings suggest that while E. purpurea may help reduce recurrence rates of OM, it is unlikely to accelerate recovery once an infection has occurred. Further research is needed to determine optimal formulations and dosages for OM treatment.
Publication bias assessment indicated some degree of bias in studies related to URTI treatment, potentially influenced by high heterogeneity. However, studies involving adverse events showed no significant publication bias, suggesting the accuracy of the findings.
4.2. Significance of the Study
Our study not only focused on evaluating the effectiveness of E. purpurea in URTI but also investigated its impact on the significant co-occurring condition of OM. Given the high prevalence and infectious risk of these conditions in children, identifying an effective treatment is crucial for reducing symptom severity and duration. Additionally, the sensitivity of children aged 1 - 12 years to medication, coupled with incomplete development of certain organs, emphasizes the importance of safe and effective treatment choice [29,30].
The study results indicate that E. purpurea shows potential in reducing treatment duration, disease incidence, and the need for antibiotics in managing URTI in children. These findings suggest that E. purpurea could be a valuable adjunctive treatment option, helping to mitigate antibiotic overuse in pediatric care a crucial consideration given the rising concern over antibiotic resistance.
Moreover, the use of E. purpurea may contribute to reducing healthcare costs associated with URTI treatment, OM while providing safer and more effective options for healthcare providers in pediatric care. However, to ensure the safe and effective use of this herbal remedy, further in-depth studies are required to clarify safety concerns, particularly regarding potential adverse effects such as rash and urticaria.
Additionally, this research opens opportunities for the development of other herbal products and contributes to improving public health management by reducing the risk of antibiotic misuse. The findings may also encourage further clinical trials and research into other plant species, potentially leading to new herbal-based treatments that are both effective and safe for children.
It is noteworthy that most studies were conducted in Europe and North America. Future research assessing the efficacy of E. purpurea in Asian countries, where the plant is prevalent [31,32,33], would be intriguing, especially considering the high prevalence of respiratory diseases in Asian children [34,35].
4.3. Differences from Previous Studies
As of the time of conducting this study, our investigation has concluded in five meta-analyses, including three scrutinies centered on the treatment of colds [36,37,38] and two on the management of URTI [11,39].
Regarding treatment time, the research results (Figure 2A) are similar to studies [36,37,38] which all show that using E. purpurea helps reduce URTI treatment time. In which a meta-analysis by Shah SA [38], showed that E. purpurea was effective in reducing the duration of colds by 1.4 days, the group of authors K Linde and colleagues [37] showed an improvement in symptoms. clearly over each period of 2 - 4 days and 5 - 10 days. Different from the results of the research group, David's results showed that E. purpurea did not affect the duration of URTI treatment (SD = -0.12, CI 95% = [0.93; 1.22]) [11].
In assessing adverse events of trial products, scrutiny may be directed towards participant attrition rates, the incidence of adverse events or undesirable effects. The results (Figure 2B) show that E. purpurea tends to be safe, with few side effects when used in children (the most common side effects are rash and urticaria), but this result is not clear as indicated by the p value > 0.05, which is consistent with the studies of Marlies Karsch-Völk and K Linde [36,37] generally intimate a lower incidence of adverse effects in the Echinacea intervention group compared to the placebo cohort, albeit with an inconsistent clarity in this observation. Findings of Marlies Karsch-Völk [36] unveil a notable divergence in the frequency of patients reporting adverse effects between the placebo group (32.6%) and the treatment group (34.1%) (OR = 1.28, CI 95% = [1.02; 1.60], p = 0.03). Sholto David's study again provided evidence that adverse events with E. purpurea were lower than placebo, with a larger number of participants experiencing at least one adverse event in the E. purpurea group (RR = 1 .11, CI 95% = [0.94; 1.31]) [11].
Concerning the incidence of at least one episode of the common cold, RR outcomes of Marlies Karsch-Völk [36] do not evince a statistically significant effect relative to the placebo. Conversely, investigation of Shah SA demonstrates a conspicuous 58% reduction in the incidence of patients contracting the common cold (OR = 0.42, CI 95% = [0.25; 0.71], p < 0.001 [38]. Other study of Linde similarly intimates a marginally lower risk of experiencing at least one cold episode with the E. purpurea preparation under scrutiny compared to the placebo (relative risk 0.80 to 0.88) [37]. Our study findings (Figure 2C) align with the conclusions drawn by Shah SA and K Linde, substantiating the premise that E. purpurea mitigates the incidence of at least one URTI infection in the pediatric demographic [37,38].
URTI is one of the common reasons for prescribing antibiotics to patients although the majority of URTI are caused by viruses and most resolve spontaneously unless due to complications such as acute OM with effusion, tonsillitis, sinusitis, so indiscriminate use of antibiotics is ineffective and inappropriate [40,41]. Research results (Figure 2D) show the positive effect of E. purpurea in reducing the rate of antibiotic use. Choosing E. purpurea is a solution that contributes to more treatment alternatives and helps reduce the overuse of antibiotics in children. These results are similar to the 2019 study of David's group [11].
Echinacea purpurea is also as the popular ingredient in dietary supplements and nutraceuticals primarily for its immune-enhancing effects [42]. Common forms of Echinacea purpurea supplements include capsules, tablets, tinctures, and teas [43]. Research has demonstrated various health benefits associated with its use. For instance, a study by Hao indicated that dietary supplementation with 200 mg/kg of Echinacea purpurea polysaccharide notably alleviated the reduction in colon length, weight loss, and histopathological damage in mice with dextran sulfate sodium-induced colitis [44]. Additionally, E. purpurea has been utilized as a nutritional supplement during the COVID-19 pandemic. A study in Saudi Arabia found that supplementing dairy products with Echinacea increased the proportion of participants using it for COVID-19 treatment, from 7.5% to 11.9% [45]. The active compounds in E. purpurea, such as polysaccharides, alkamides, and phenolic acids, are believed to stimulate the immune system by increasing the production of white blood cells and enhancing their activity [1,46].
In herbal supplement or medicine, E. purpurea is used not only for immune support but also for its anti-inflammatory and antioxidant properties [47,48]. The anti-inflammatory properties are largely attributed to the plant's alkamides and caffeic acid derivatives, which may help modulate the inflammatory response of the body [49]. Furthermore, antioxidant activity of Echinacea helps protect cells from oxidative stress, which is implicated in numerous chronic diseases [50,51].
The findings from this meta-analysis may significantly contribute to the field of nutrition by consolidating clinical information that supports guideline recommendations on dietary supplements and nutraceuticals to boost immune function and reduce antibiotic dependence, which is crucial given the growing concerns about antibiotic resistance [52]. For nutritional products, safety is paramount. Guidelines that emphasize the importance of dietary supplements should be evidence-based [53], and our findings provide robust data to support recommendations for the appropriate use of E. purpurea in children, ensuring both efficacy and safety [52,54]. This endorsement by regulatory agencies further strengthens the role of E. purpurea in nutrition and treatment strategies to prevent and manage URTIs in children.
4.4. Strengths and Limitations
This study is the first to comprehensively synthesize evidence on E. purpurea in children, contributes valuable insights for researchers and practitioners seeking safe and effective treatments. The homogeneity in intervention selection, participant criteria, and stringent target group selection enhances the robustness of the findings.
However, the limitation lies in the relatively small number of included studies, potentially limiting the persuasiveness of the conclusions. The research period spanned over 20 years, yet the number of eligible studies remained limited due to the lack of extensive research on E. purpurea in pediatric populations. While the small number of studies may affect statistical significance and trend detection, pooling individual studies with smaller sample sizes creates a larger composite sample, enhancing reliability for identifying significant associations. Each selected study meets strict quality and reliability standards, ensuring that the analysis is grounded in high-quality data.
The observed heterogeneity among studies also poses a challenge to result interpretation. The results (Figures 2A, 2C, 2D and 3A) show high heterogeneity (I2), limiting the findings due to variations in patient characteristics, product properties, dosage, formulation, and methodologies across studies. This diversity reflects clinical and scientific practice but challenges the consistency of results. Although subgroup analysis is commonly employed to address heterogeneity, it was not feasible in this study due to the limited number of studies and significant variability in study design. To improve the reliability and comparability of results, future studies should aim to standardize methods and variables. Sensitivity analysis should also be considered to assess the stability and robustness of aggregated results. However, for sensitivity analysis to be objective and effective, it typically requires a minimum of 10 studies [55]. To address these limitations, rigorous selection criteria were used, along with a thorough assessment of study quality using the PEDro scale. Heterogeneity (I²) has been transparently reported to provide context for the variability across studies. These limitations emphasize the need for further research with a larger and more homogeneous dataset to allow meaningful subgroup analyses.
To enhance the generalizability and applicability of findings, future studies should include diverse geographic regions to achieve a more comprehensive understanding of the efficacy of E. purpurea across various populations. Increasing statistical power through larger sample sizes is essential to provide more robust and conclusive evidence regarding its effectiveness in managing URTIs and OM in pediatric populations. Further research is needed to conduct a more nuanced investigation into the specific impact of E. purpurea on OM treatment duration to derive definitive conclusions in this area.
The ethical considerations surrounding the use of E. purpurea in children should not be overlooked. The variability in formulations, the potential for immune overstimulation, and the lack of standardized dosing present challenges that warrant caution. Given that mild adverse reactions such as rash and gastrointestinal discomfort have been reported, healthcare professionals should guide parents in making informed decisions. Regulatory bodies should also work towards establishing more stringent quality control measures to ensure the safe and effective use of E. purpurea in pediatric populations.
Long-term studies are critical for evaluating the sustained efficacy and safety of E. purpurea, particularly in children who experience recurrent respiratory infections. Investigating the efficacy of different Echinacea species and formulations is also crucial to understanding the variability in their therapeutic effects on pediatric respiratory health. Moreover, future research should include stratified analyses to assess age-related variations in safety and efficacy, comparing outcomes between younger children (1–5 years) and older children (6–12 years). Longitudinal studies focusing on recurrent infections in children are recommended to comprehensively evaluate the long-term safety and effectiveness of E. purpurea. These multidimensional and rigorous approaches will provide a deeper and more precise understanding of E. purpurea’s role in pediatric healthcare, contributing to evidence-based guidance for its clinical application.
5. Conclusions
This meta-analysis highlights the potential of E. purpurea as a dietary intervention for managing pediatric URTIs and otitis media OM. The findings suggest that E. purpurea may effectively reduce treatment duration, the incidence of URTIs and OM episodes, and antibiotic usage. These results indicate that E. purpurea could contribute to mitigating the burden of pediatric respiratory infections while promoting antimicrobial stewardship and reducing reliance on synthetic medications.
From a nutritional perspective, E. purpurea offers a promising avenue for integrating phytotherapeutics into pediatric care. Its immune-modulating properties and natural origins align well with current trends in clinical nutrition, emphasizing safe and holistic approaches to health. However, significant concerns remain regarding the variability in formulations, inconsistent safety profiles, and limited data on long-term effects. Mild adverse events such as rash, urticaria, and gastrointestinal discomfort were noted, but the overall safety profile warrants further investigation.
Future research should prioritize rigorous and standardized methodologies to evaluate E. purpurea across diverse populations, stratify analyses by age groups, and explore its long-term impact. Additionally, studies should aim to better understand the nutritional and immunological mechanisms underlying its efficacy. These efforts will provide robust evidence to guide its integration into clinical nutrition practice.
In conclusion, while E. purpurea demonstrates significant potential as a nutritional intervention for pediatric respiratory health, its use must be informed by comprehensive research. Healthcare providers should carefully balance its benefits against unresolved safety concerns, ensuring that its application aligns with evidence-based nutritional strategies.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Attached supplementary document 1 (search_algorithm.docx). Attached supplementary document 2 (risk_of_bias_assessment.xlsx)
Author Contributions
TMH Vu: Writing – review & editing, Writing – original draft, Data curation, Conceptualization. PMK Doan: Formal analysis, Data curation. TTD Nguyen: Software, Formal analysis, Data curation. TTT Bui: Writing – originaldraft, Data curation. THL Ha: Validation, Data curation. TKQ Hoang: Review & editing, Writing – original draft, Visualization, Conceptualization. IP Taufani: Review & editing, Data curation. HA Ha: Conceptualization, Supervision, Review & editing, Writing – original draft, Visualization. TPT Pham: Conceptualization, Supervision, Review & editing, Writing – original draft, Visualization.
Funding
This research received no financial support.
Data Availability Statement
All data were included in the article.
Acknowledgements
Not applicable.
Conflicts of Interest
The authors declare no competing interest.
Abbreviations
CI, confidence interval; OM, otitis media; RCT, randomized controlled trials; RR, risk ratio; SMD, standardized mean difference; URTI, upper respiratory tract infection.
References
- Crawford C, Brown LL, Costello RB, Deuster PA. Select Dietary Supplement Ingredients for Preserving and Protecting the Immune System in Healthy Individuals: A Systematic Review. Nutrients. 2022 Nov 1;14(21):4604. [CrossRef]
- Quynh, Thuy D, Khiem V, Thien N, Ha HA. Phytochemical Profiling of Echinacea Genus: A mini Review of Chemical Constituents of Selected Species. 2023.
- Sumer J, Keckeis K, Scanferla G, Frischknecht M, Notter J, Steffen A, et al. Novel Echinacea formulations for the treatment of acute respiratory tract infections in adults-A randomized blinded controlled trial. Front Med (Lausanne). 2023;10:948787. [CrossRef]
- Burlou-Nagy C, Bănică F, Jurca T, Vicaș LG, Marian E, Muresan ME, et al. Echinacea purpurea (L.) Moench: Biological and Pharmacological Properties. A Review. Plants (Basel). 2022 May 5;11(9):1244. [CrossRef]
- DeGeorge KC, Ring DJ, Dalrymple SN. Treatment of the Common Cold. Am Fam Physician. 2019 Sep 1;100(5):281–9.
- Thomas M, Bomar PA. Upper Respiratory Tract Infection. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Apr 28]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK532961/.
- Abdel-Naby Awad OG. Echinacea can help with Azithromycin in prevention of recurrent tonsillitis in children. Am J Otolaryngol. 2020;41(4):102344.
- Khan EA, Raja MH, Chaudhry S, Zahra T, Naeem S, Anwar M. Outcome of upper respiratory tract infections in healthy children: Antibiotic stewardship in treatment of acute upper respiratory tract infections. Pak J Med Sci. 2020;36(4):642–6. [CrossRef]
- Korppi M, Heikkilä P, Palmu S, Huhtala H, Csonka P. Antibiotic prescribing for children with upper respiratory tract infection: a Finnish nationwide 7-year observational study. Eur J Pediatr. 2022;181(8):2981–90. [CrossRef]
- Wahl RA, Aldous MB, Worden KA, Grant KL. Echinacea purpurea and osteopathic manipulative treatment in children with recurrent otitis: a randomized controlled trial. BMC Complementary and Alternative Medicine. 2008 Oct 2;8(1):56. [CrossRef]
- David S, Cunningham R. Echinacea for the prevention and treatment of upper respiratory tract infections: A systematic review and meta-analysis. Complement Ther Med. 2019 Jun;44:18–26. [CrossRef]
- Vu TMH, Hoang TV, Nguyen TQH, Doan PMK, Nguyen TTD, Bui TTT, et al. Echinacea purpurea: An overview of mechanism, efficacy, and safety in pediatric upper respiratory infections and otitis media. International Journal of Plant Based Pharmaceuticals. 2024 Jun 16;4(2):90–100. [CrossRef]
- Maggini V, Bandeira Reidel RV, De Leo M, Mengoni A, Rosaria Gallo E, Miceli E, et al. Volatile profile of Echinacea purpurea plants after in vitro endophyte infection. Nat Prod Res. 2020 Aug;34(15):2232–7. [CrossRef]
- Petrova A, Ognyanov M, Petkova N, Denev P. Phytochemical Characterization of Purple Coneflower Roots (Echinacea purpurea (L.) Moench.) and Their Extracts. Molecules. 2023 Jan;28(9):3956.
- Pham TPT, Hoang TV, Cao PTN, Le TTD, Ho VTN, Vu TMH, et al. Comparison of Omega-3 polyunsaturated fatty acids bioavailability in fish oil and krill oil: Network Meta-analyses. Food Chemistry: X. 2024 Dec;24:101880. [CrossRef]
- Covidence [Internet]. [cited 2024 May 14]. Covidence - Better systematic review management. Available from: https://www.covidence.org/.
- Blobaum P. Physiotherapy Evidence Database (PEDro). J Med Libr Assoc. 2006 Oct;94(4):477–8.
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997 Sep 13;315(7109):629–34.
- Cohen HA, Varsano I, Kahan E, Sarrell EM, Uziel Y. Effectiveness of an herbal preparation containing echinacea, propolis, and vitamin C in preventing respiratory tract infections in children: a randomized, double-blind, placebo-controlled, multicenter study. Arch Pediatr Adolesc Med. 2004 Mar;158(3):217–21.
- Taylor JA, Weber W, Standish L, Quinn H, Goesling J, McGann M, et al. Efficacy and safety of echinacea in treating upper respiratory tract infections in children: a randomized controlled trial. JAMA. 2003 Dec 3;290(21):2824–30.
- Wustrow TPU, Otovowen Study Group. Alternative versus conventional treatment strategy in uncomplicated acute otitis media in children: a prospective, open, controlled parallel-group comparison. Int J Clin Pharmacol Ther. 2004 Feb;42(2):110–9. [CrossRef]
- Ogal M, Johnston SL, Klein P, Schoop R. Echinacea reduces antibiotic usage in children through respiratory tract infection prevention: a randomized, blinded, controlled clinical trial. Eur J Med Res. 2021 Apr 8;26(1):33.
- Weishaupt R, Bächler A, Feldhaus S, Lang G, Klein P, Schoop R. Safety and Dose-Dependent Effects of Echinacea for the Treatment of Acute Cold Episodes in Children: A Multicenter, Randomized, Open-Label Clinical Trial. Children (Basel). 2020 Dec 15;7(12):292.
- Barrett B. Efficacy and safety of echinacea in treating upper respiratory tract infections in children: a randomized controlled trial. J Pediatr. 2004 Jul;145(1):135–6. [CrossRef]
- Weber W, Taylor JA, Stoep AV, Weiss NS, Standish LJ, Calabrese C. Echinacea purpurea for prevention of upper respiratory tract infections in children. J Altern Complement Med. 2005 Dec;11(6):1021–6. [CrossRef]
- Spasov AA, Ostrovskij OV, Chernikov MV, Wikman G. Comparative controlled study of Andrographis paniculata fixed combination, Kan Jang and an Echinacea preparation as adjuvant, in the treatment of uncomplicated respiratory disease in children. Phytother Res. 2004 Jan;18(1):47–53.
- Sayegh AS, Eppler M, Sholklapper T, Goldenberg MG, Perez LC, La Riva A, et al. Severity Grading Systems for Intraoperative Adverse Events. A Systematic Review of the Literature and Citation Analysis. Annals of Surgery [Internet]. 2023 Apr 27 [cited 2024 Nov 1]; Available from: https://journals.lww.com/10.1097/SLA.0000000000005883. [CrossRef]
- Schoop R, Klein P, Suter A, Johnston SL. Echinacea in the prevention of induced rhinovirus colds: A meta-analysis. Clinical Therapeutics. 2006 Feb 1;28(2):174–83. [CrossRef]
- Tyler S. Chapter 13: Physical Development in Early Childhood. 2020 May 26 [cited 2024 Jan 14]; Available from: https://uark.pressbooks.pub/hbse1/chapter/physical-development-in-early-childhood_ch_13/.
- Erceg D, Jakirović M, Prgomet L, Madunić M, Turkalj M. Conducting Drug Treatment Trials in Children: Opportunities and Challenges. Pharm Med [Internet]. 2024 May 10 [cited 2024 May 14]; Available from: . [CrossRef]
- Applequist W. Echinacea. The Genus Echinacea. ebot. 2005 Jan;59(1):98–98.
- Liu YC, Zeng JG, Chen B, Yao SZ. Investigation of Phenolic Constituents in Echinacea purpurea Grown in China. Planta Med. 2007 Dec;73(15):1600–5. [CrossRef]
- Bałan BJ, Różewski F, Zdanowski R, Skopińska-Różewska E. Review paper<br>Immunotropic activity of Echinacea. Part I. History and chemical structure. Cent Eur J Immunol. 2012;37(1):45–50.
- Liu Q, Qin C, Du M, Wang Y, Yan W, Liu M, et al. Incidence and Mortality Trends of Upper Respiratory Infections in China and Other Asian Countries from 1990 to 2019. Viruses. 2022 Nov 18;14(11):2550. [CrossRef]
- Jin X, Ren J, Li R, Gao Y, Zhang H, Li J, et al. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. EClinicalMedicine. 2021 Jul;37:100986. [CrossRef]
- Karsch-Völk M, Barrett B, Kiefer D, Bauer R, Ardjomand-Woelkart K, Linde K. Echinacea for preventing and treating the common cold. Cochrane Database Syst Rev. 2014 Feb 20;2014(2):CD000530.
- Linde K, Barrett B, Wölkart K, Bauer R, Melchart D. Echinacea for preventing and treating the common cold. Cochrane Database Syst Rev. 2006 Jan 25;(1):CD000530.
- Shah SA, Sander S, White CM, Rinaldi M, Coleman CI. Evaluation of echinacea for the prevention and treatment of the common cold: a meta-analysis. Lancet Infect Dis. 2007 Jul;7(7):473–80. [CrossRef]
- Anheyer D, Cramer H, Lauche R, Saha FJ, Dobos G. Herbal Medicine in Children With Respiratory Tract Infection: Systematic Review and Meta-Analysis. Acad Pediatr. 2018;18(1):8–19. [CrossRef]
- Kenealy T, Arroll B. Antibiotics for the common cold and acute purulent rhinitis. Cochrane Database Syst Rev. 2013 Jun 4;2013(6):CD000247.
- Sur DKC, Plesa ML. Antibiotic Use in Acute Upper Respiratory Tract Infections. Am Fam Physician. 2022 Dec;106(6):628–36.
- Abdel Rahman AN, Khalil AA, Abdallah HM, ElHady M. The effects of the dietary supplementation of Echinacea purpurea extract and/or vitamin C on the intestinal histomorphology, phagocytic activity, and gene expression of the Nile tilapia. Fish Shellfish Immunol. 2018 Nov;82:312–8. [CrossRef]
- Echinacea Extract - an overview | ScienceDirect Topics [Internet]. [cited 2024 May 16]. Available from: https://www.sciencedirect.com/topics/medicine-and-dentistry/echinacea-extract.
- Wei FH, Xie WY, Zhao PS, Gao W, Gao F. Echinacea purpurea Polysaccharide Ameliorates Dextran Sulfate Sodium-Induced Colitis by Restoring the Intestinal Microbiota and Inhibiting the TLR4-NF-κB Axis. Nutrients. 2024 Apr 26;16(9):1305. [CrossRef]
- Hafiz NM, El-Readi MZ, Esheba G, Althubiti M, Ayoub N, Alzahrani AR, et al. The use of the nutritional supplements during the covid-19 outbreak in Saudi Arabia: A cross-sectional study. Complement Ther Med. 2023 Mar;72:102917. [CrossRef]
- Kim H, Calderón AI. Rational and Safe Use of the Top Two Botanical Dietary Supplements to Enhance the Immune System. Comb Chem High Throughput Screen. 2022;25(7):1129–30. [CrossRef]
- Choudhary S, Khan S, Rustagi S, Rajpal VR, Khan NS, Kumar N, et al. Immunomodulatory Effect of Phytoactive Compounds on Human Health: A Narrative Review Integrated with Bioinformatics Approach. Curr Top Med Chem. 2024 Mar 27. [CrossRef]
- Elvir Lazo OL, White PF, Lee C, Cruz Eng H, Matin JM, Lin C, et al. Use of herbal medication in the perioperative period: Potential adverse drug interactions. Journal of Clinical Anesthesia. 2024 Aug;95:111473.
- Kakouri E, Talebi M, Tarantilis PA. Echinacea spp.: The cold-fighter herbal remedy? Pharmacological Research - Modern Chinese Medicine. 2024 Mar;10:100397.
- Adebimpe Ojo C, Dziadek K, Sadowska U, Skoczylas J, Kopeć A. Analytical Assessment of the Antioxidant Properties of the Coneflower (Echinacea purpurea L. Moench) Grown with Various Mulch Materials. Molecules. 2024 Feb 22;29(5):971.
- Abdel-Wahhab KG, Elqattan GM, El-Sahra DG, Hassan LK, Sayed RS, Mannaa FA. Immuno-antioxidative reno-modulatory effectiveness of Echinacea purpurea extract against bifenthrin-induced renal poisoning. Sci Rep. 2024 Mar 11;14(1):5892. [CrossRef]
- Dehn Lunn A. Reducing inappropriate antibiotic prescribing in upper respiratory tract infection in a primary care setting in Kolkata, India. BMJ Open Qual. 2018 Nov;7(4):e000217.
- Djaoudene O, Romano A, Bradai YD, Zebiri F, Ouchene A, Yousfi Y, et al. A Global Overview of Dietary Supplements: Regulation, Market Trends, Usage during the COVID-19 Pandemic, and Health Effects. Nutrients. 2023 Jul 26;15(15):3320. [CrossRef]
- Brykman MC, Streusand Goldman V, Sarma N, Oketch-Rabah HA, Biswas D, Giancaspro GI. What Should Clinicians Know About Dietary Supplement Quality? AMA J Ethics. 2022 May 1;24(5):E382-389.
- Mathur MB, VanderWeele TJ. Sensitivity analysis for publication bias in meta-analyses. Journal of the Royal Statistical Society Series C, Applied Statistics. 2020 Aug 28;69(5):1091. [CrossRef]
Figure 1.
Flow diagram of study selection.
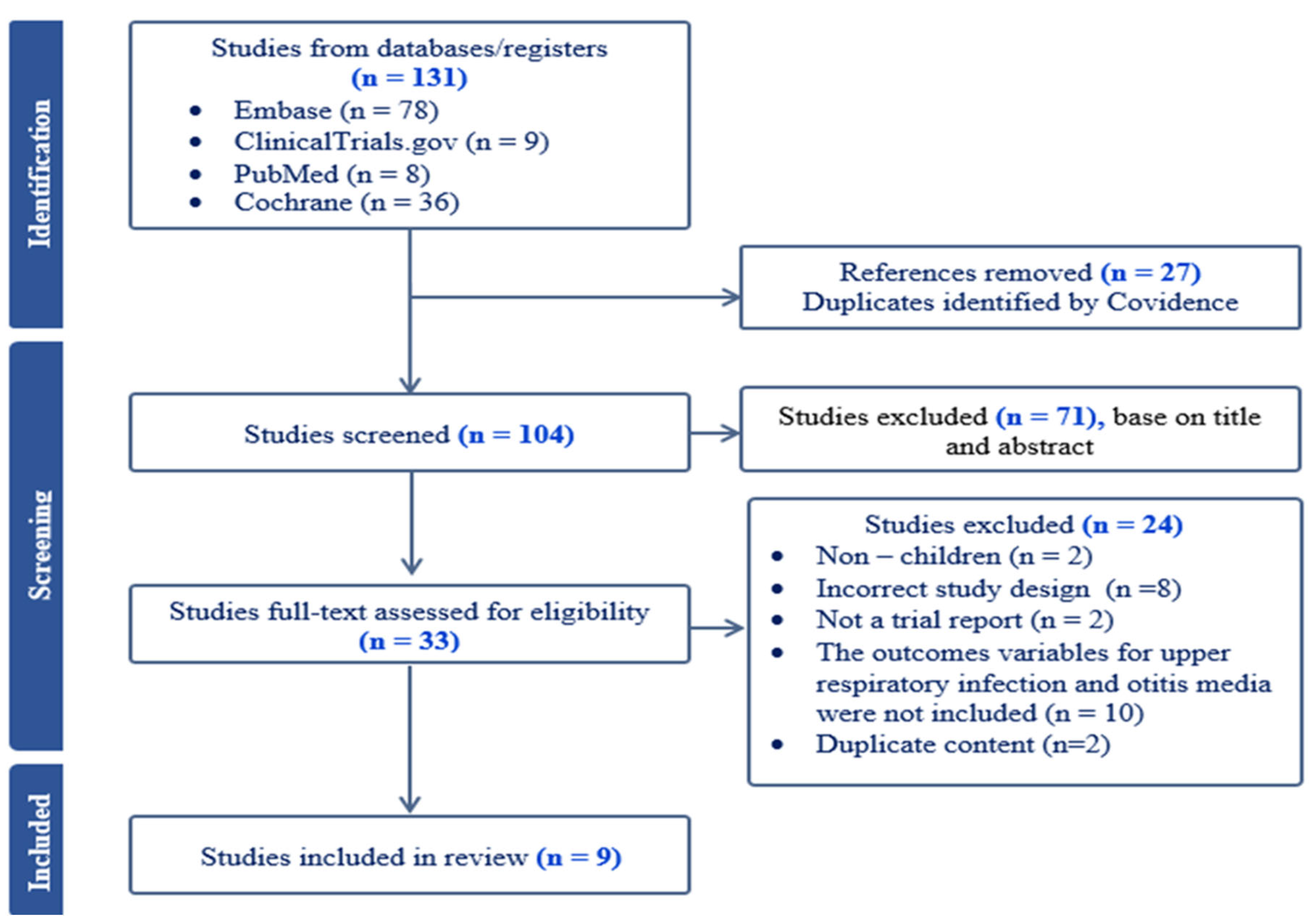
Figure 2.
A meta-analysis on the effect of Echinacea purpurea in (A) the treatment time (B) Adverse event (C) the incidence of at least one (D) The antibiotic use rates of upper respiratory infections in children.
Figure 2.
A meta-analysis on the effect of Echinacea purpurea in (A) the treatment time (B) Adverse event (C) the incidence of at least one (D) The antibiotic use rates of upper respiratory infections in children.
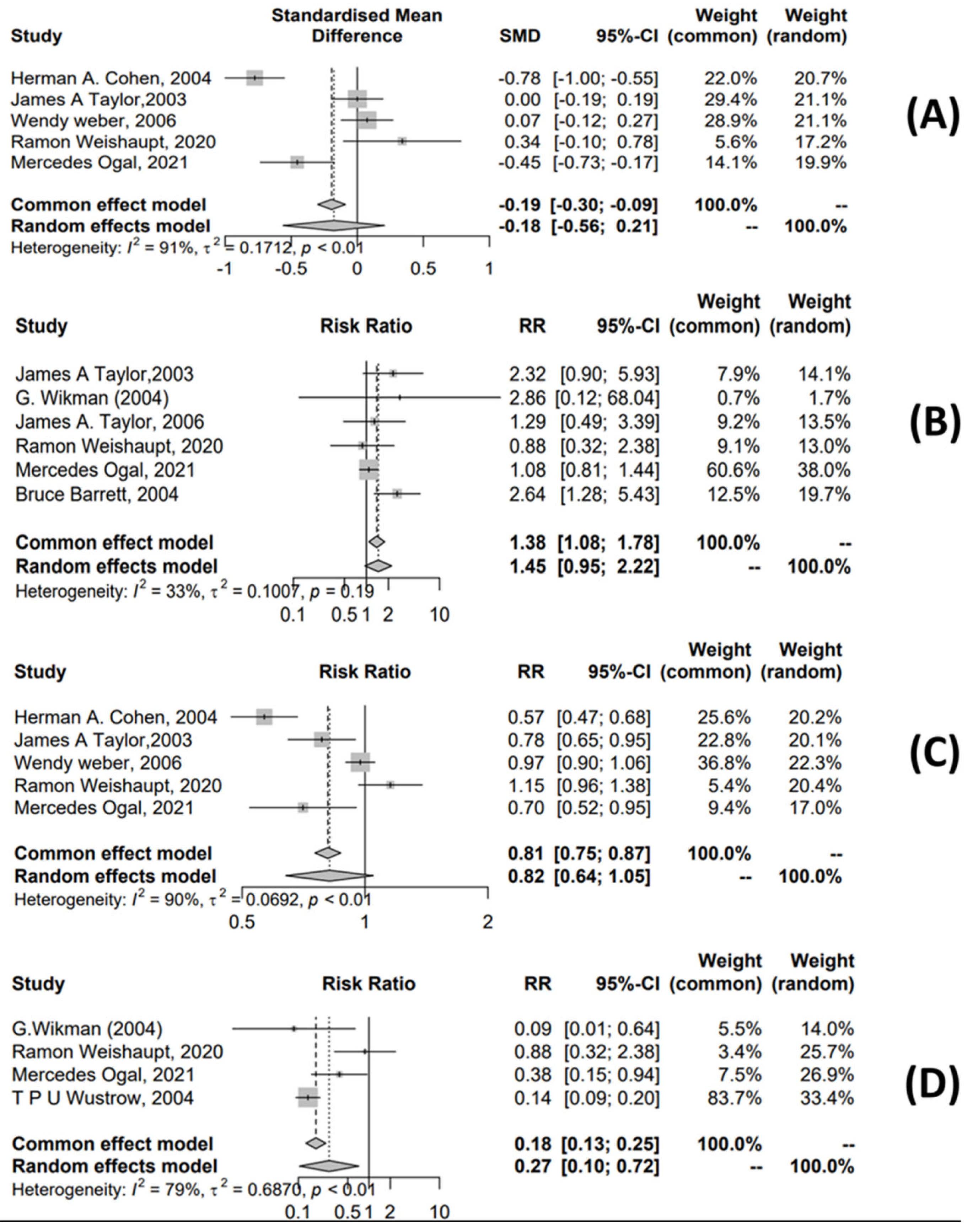
Figure 3.
A meta-analysis on the effects of Echinacea purpurea and duration of treatment (A) and the incidence of at least one episode (B) for otitis media in children.
Figure 3.
A meta-analysis on the effects of Echinacea purpurea and duration of treatment (A) and the incidence of at least one episode (B) for otitis media in children.
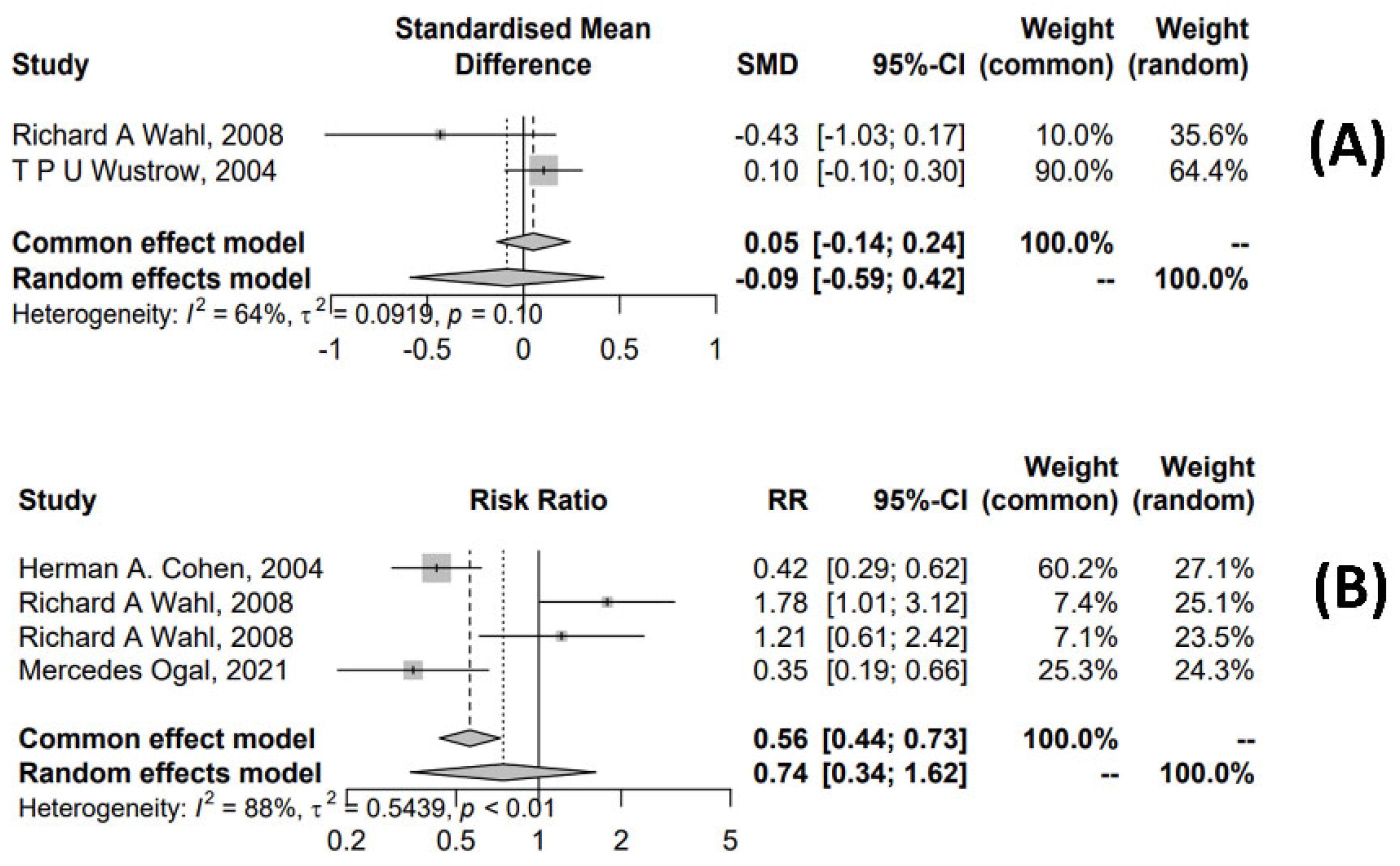
Figure 4.
Funnel plot on the (A): effect of Echinacea purpurea on the treatment time of upper respiratory infections in children, (B): safety of Echinacea purpurea in the treatment of upper respiratory infections in children, (C): relationship of Echinacea purpurea and the incidence of at least one upper respiratory tract infection in children, (D): effects of Echinacea purpurea and the rate of antibiotic use in the treatment of upper respiratory infections in children.
Figure 4.
Funnel plot on the (A): effect of Echinacea purpurea on the treatment time of upper respiratory infections in children, (B): safety of Echinacea purpurea in the treatment of upper respiratory infections in children, (C): relationship of Echinacea purpurea and the incidence of at least one upper respiratory tract infection in children, (D): effects of Echinacea purpurea and the rate of antibiotic use in the treatment of upper respiratory infections in children.
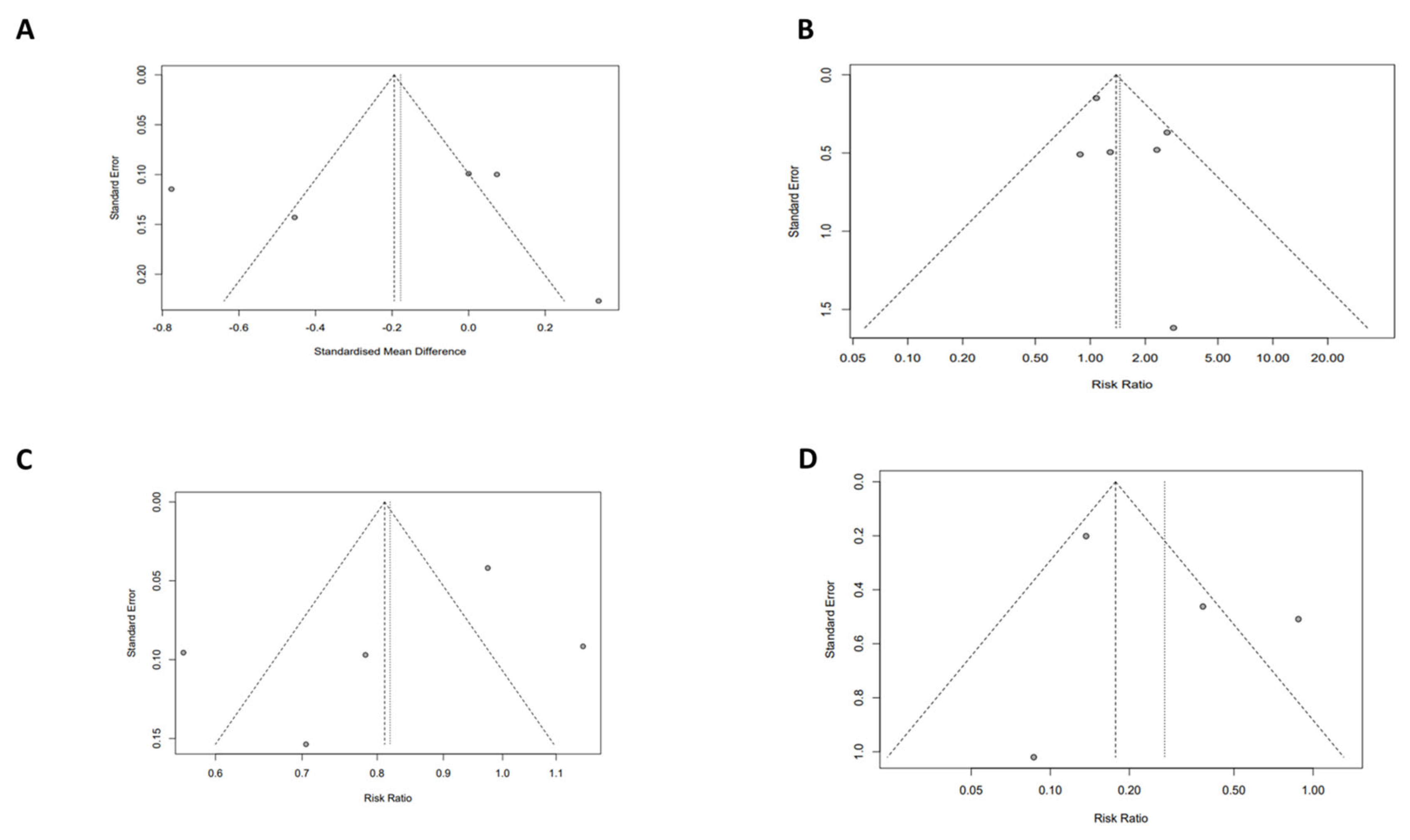
Figure 5.
Funnel plot on the (A): effects of Echinacea purpurea and treatment time for otitis media in children, (B): relationship of Echinacea purpurea and the incidence of at least one otitis media in children.
Figure 5.
Funnel plot on the (A): effects of Echinacea purpurea and treatment time for otitis media in children, (B): relationship of Echinacea purpurea and the incidence of at least one otitis media in children.
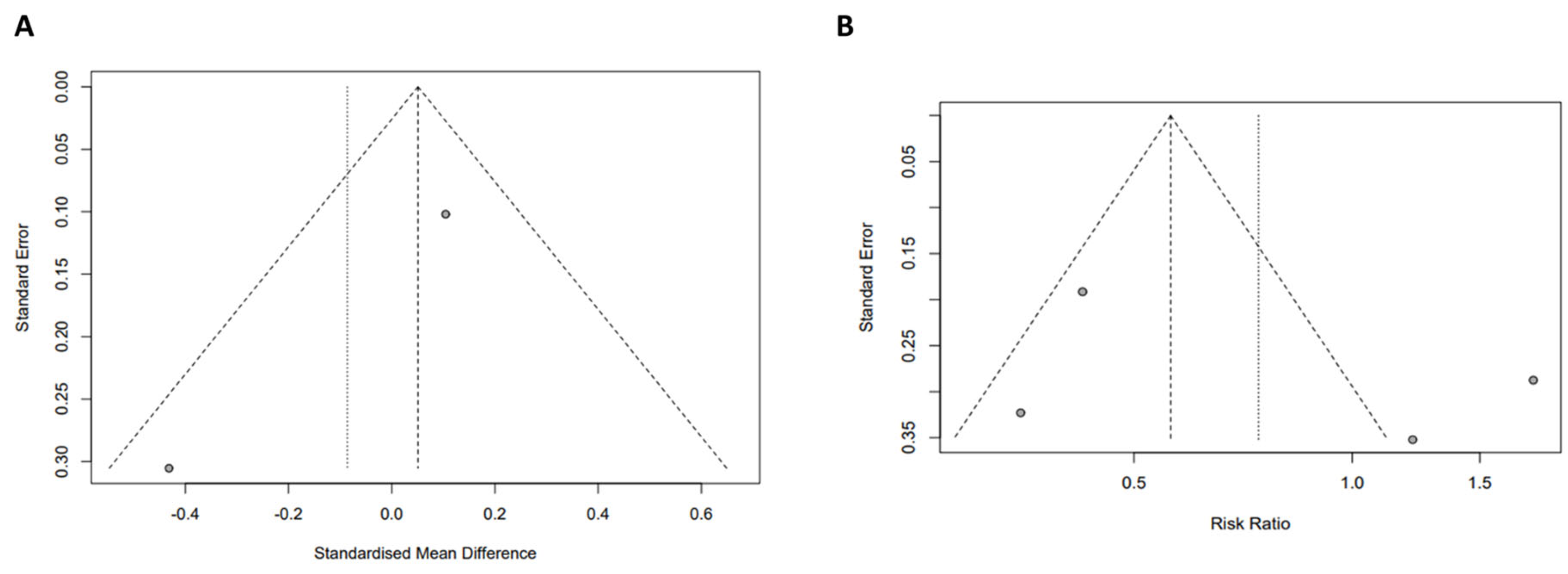

Table 1.
Characteristics of included studies.
| Study | Patient population |
Species, part | Dose | Dosage form, Manufac-turer | Patient number | Research group characteristics | Outcome | ||
|---|---|---|---|---|---|---|---|---|---|
| Treat-ment | Placebo | Treatment | Placebo | ||||||
| Barrett B., 2004 [24] | 2-11 years URTI |
E. purpurea aerial parts |
Not reported | -Solution -England |
337 | 370 | Not reported | Not reported | -Treatment time -Adverse event |
| Cohen H.A., 2004 [19] | 1-5 years -URTI and OM |
E. purpurea aerial parts, E. angustifolia root |
-1-3 years: 2x5 mL/day -4-5 years: 2x7,5mL/day |
-Solution -USA |
215 | 215 | Echinacea, propolis, vitamin C | Propolis, vitamin C | -Treatment time -Number of times having at least one episode |
| Ogal M., 2021 [22] | 4-12 years -URTI and OM |
-E. purpurea root, aerial parts |
-Echinacea: 3x400mg/day -Vitamin C: 3x50mg/day |
-Tablet Switzerland |
104 | 99 | Echinacea, ethanolic | Vitamin C (axit ascorbic and canxi ascorbate) | -Treatment time -Adverse event -Number of times having at least one episode -Rate of antibiotic use |
| Taylor J.A., 2003 [20] | 2-11 years URTI |
-E. purpurea, the above-ground herb harvested at flowering | -2-5 years: 7,5mL/day (2 x 3,75 mL/day) -6-11 years: 10mL/day (2x5mL/day) |
-Solution -USA |
337 | 370 | Echinacea non-alcohol | Syrup | -Treatment time -Adverse event -Number of times having at least one episode |
| Wahl R.A., 2008 [10] | 1-5 years URTI and OM |
-E. purpurea, the fresh roots and dried mature seeds |
3x0,5mL/day during first 3 day, then 3x0,25mL/day in the next 7 days | -Solution -USA |
44 |
46 | Echinacea, ethanol | Ethanol, filtered water, food coloring and thickeners | -Treatment time -Adverse events -Number of times having at least one episode |
| G. Wikman, 2004 [26] | 4-11 years URTI |
- E. purpurea (part not specified) |
-Echinacea: 10 drops (3 times/day) -Andrographis paniculata: 3x2 capsules/day |
-Nasal drops -Russia -Tablet - Sweden |
94 | 39 | Echinacea, ethanol, Andrographis paniculata (N.) | Warm drinks, throat gargles, antiseptic nose drops, and paracetamol at a dose of 500 mg 3 times a day in cases of fever and severe headache |
-Adverse event -Rate of antibiotic use |
| Weber W., 2006 [25] | 2-11 years URTI |
-E. purpurea, the above-ground plant parts harvested at flowering |
-2-5 years: 87,75mg ( 2 x ¾ teaspoon/ day) -6-11 years: 117mg (2x1 teaspoon/day) |
-Solution -Germany |
263 | 261 | Echinacea non-alcohol | Placebo liquid | -Treatment time -Adverse events -Number of times having at least one episode |
| Weishaupt R., 2020 [23] | 4-12 years URTI |
-E. purpurea root | -Low dose: 3 capsules/day -Hight dose: 5 capsules/day |
-Tablet - Switzerland |
79 | Echinacea, ethanolic | -Treatment time -Adverse events -Number of times having at least one episode -Rate of antibiotic use |
||
| Wustrow T.P.U., 2004 [21] | 1-10 years OM |
-E. purpurea (part not specified) |
Not reported | -Nasal drops -Germany |
194 | 196 | Alternative treatment with medicine Otovowen contain hightly concentrated liquid plant extracts of Echinacea and some other plant species |
Conventional treatment not treated with medicine Otovowen | -Treatment time -Rate of antibiotic use |
Abbreviations: OM, otitis media; URTI, upper respiratory tract infection.
Table 2.
Quality of articles (PEDro scale).
| PEDro criteria | Study | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Barrett 2004 [24] | Cohen 2004 [19] | Ogal 2021 [22] | Taylor 2003 [20] | Wahl 2008 [10] | Wikman 2004 [26] | Weber 2006 [25] | Weishaupt 2020 [23] | Wustrow 2004 [21] | |
| 1. Eligibility* | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 2. Randomization | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 |
| 3. Concealed allocation | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 |
| 4. Baseline comparability | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 5. Blind subject | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 |
| 6. Blind therapist | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 |
| 7. Blind assessor | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 |
| 8. Adequate follow-up | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 |
| 9. Intention-to-treat analysis | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 10. Between-group comparisons | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 11. Point estimate variability | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Total score | 9/10 | 8/10 | 7/10 | 9/10 | 10/10 | 6/10 | 8/10 | 6/10 | 5/10 |
| Study quality | Excellent | Good | Good | Excellent | Excellent | Good | Good | Good | Moderate |
Note: *Criterion 1 is not used to calculate the total PEDro score.
Table 3.
Observed adverse reactions in children using E. purpurea.
| Adverse reactions | Severity | Detailed description | References |
|---|---|---|---|
| Allergic reactions | Mild | Mild urticaria; itchiness; rash; choking | [20,22,25,26] |
| Gastrointestinal Issues | Mild-Moderate | Vomiting; diarrhea; stomachache | [20,22,23] |
| Infections | Moderate | Stomatitis; conjunctivitis | (23) |
| Fever | Mild | Some users may experience mild fever, though this is uncommon; scarlet fever | [22,23] |
| Dizziness | Mild | Some individuals may feel mild dizziness after taking E. purpurea | (23) |
| Drowsiness or Insomnia | Mild-Moderate | Some users may feel drowsy, while others might experience insomnia | (20) |
| Headaches | Mild-Moderate | Mild to moderate headaches may occur, particularly with prolonged use of E. purpurea | [20,22] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



