Submitted:
24 February 2025
Posted:
26 February 2025
You are already at the latest version
Abstract
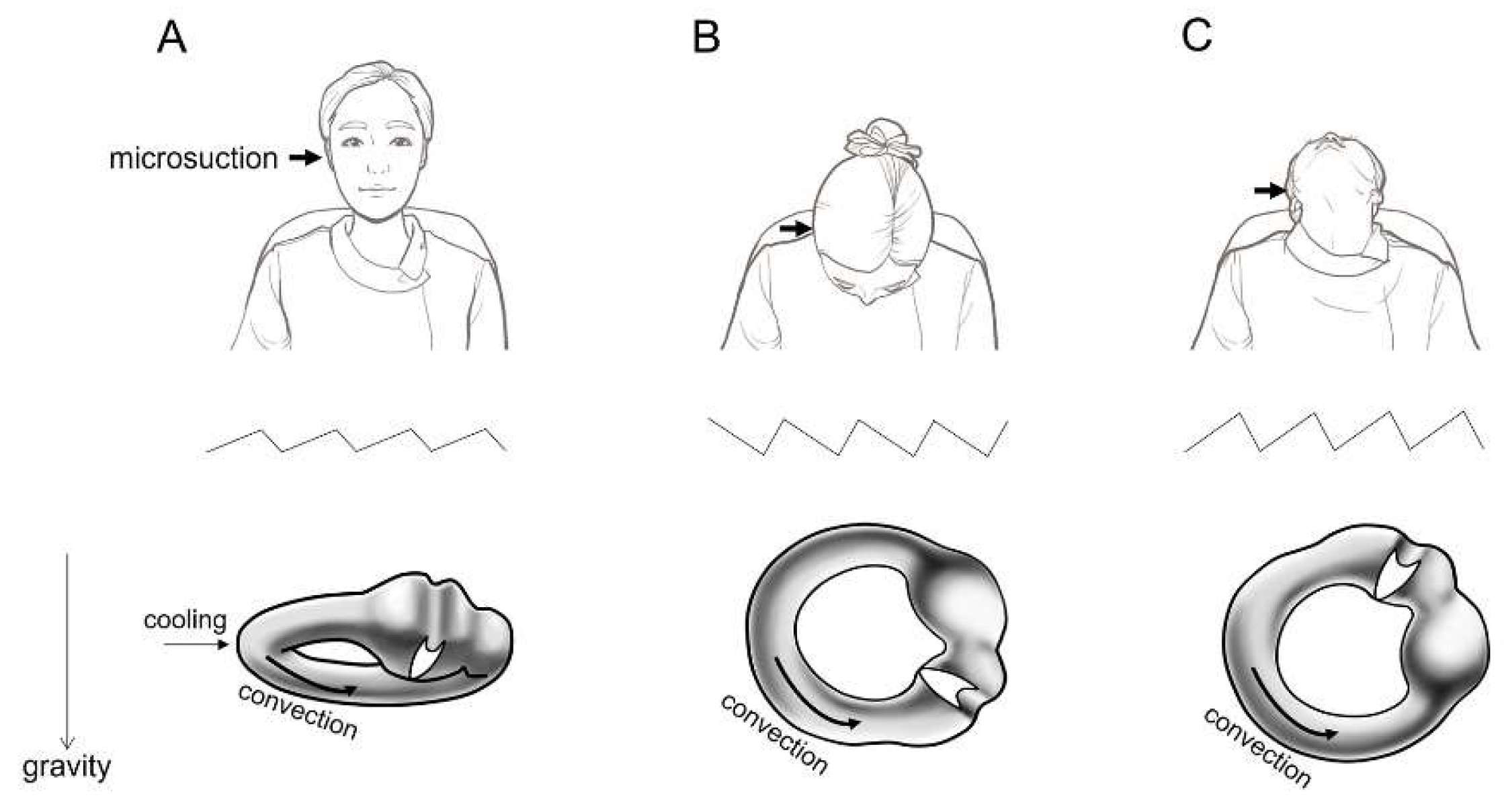
Background/Objectives: Aural toilet using microsuction is a common procedure in ENT clinics, and vertigo is a frequent complaint during this procedure. This study aimed to investigate the characteristics and incidence of microsuction-induced nystagmus and vertigo based on the appearance of the tympanic membrane (TM). Methods: In 85 patients with various TM appearances, microsuction-induced vertigo and nystagmus were assessed. Results: Microsuction elicited nystagmus in 95% (81 of 85) of patients and vertigo in 36% (31 of 85). The nystagmus direction was towards the ipsilateral ear in a bowing position and towards the contralateral ear in a leaning position. The proportion of patients who complained of rotatory vertigo was significantly higher in those with TM perforation, open cavity mastoidectomy, and adhesive otitis media (74%, 26 of 35) compared to those without TM perforation group (10%, 5 of 50) (P < 0.001, X2 test). Conclusions: Aural toilet using microsuction commonly induces due to convection in the lateral semicircular canal endolymph caused by the cooling effect. While microsuction-induced nystagmus was observed in most patients, the incidence of vertigo varied depending on the TM condition. Clinicians should closely monitor patients for vertigo during the procedure, and methods to prevent microsuction-induced vertigo should be explored.
Keywords:
1. Introduction
2. Materials and Methods
3. Results
3.1. Patients and TM appearance
3.2. Microsuction-induced nystagmus and vertigo
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TM | Tympanic membrane |
| EAC | External auditory canal |
References
- Clegg AJ, Loveman E, Gospodarevskaya E, Harris P, Bird A, Bryant J, et al. The safety and effectiveness of different methods of earwax removal: a systematic review and economic evaluation. Health Technol Assess. 2010;14(28):1-192. [CrossRef]
- Pothier DD, Hall C, Gillett S. A comparison of endoscopic and microscopic removal of wax: a randomised clinical trial. Clin Otolaryngol. 2006;31(5):375-80. [CrossRef]
- Addams-Williams J, Howarth A, Phillipps JJ. Microsuction aural toilet in ENT outpatients: a questionnaire to evaluate the patient experience. Eur Arch Otorhinolaryngol. 2010;267(12):1863-6. [CrossRef]
- Bende M. Warm air for prevention of vertigo. Laryngoscope. 1988;98(6 Pt 1):687. [CrossRef]
- Bhutta MF, Head K, Chong LY, Daw J, Schilder AG, Burton MJ, et al. Aural toilet (ear cleaning) for chronic suppurative otitis media. Cochrane Database Syst Rev. 2020;9(9):Cd013057.
- Dundas-Grant J. Case of Vertigo on Suction in a Patient with Adhesive Processes in the Middle Ear, following Scarlet Fever: Presumably Malleo-Incudal Ankylosis. Proc R Soc Med. 1928;21(12):1933. [CrossRef]
- Dundas-Grant J. Case of Vertigo on Suction in a Patient with absence of the Stapes. (Previously shown November 17, 1911). Proc R Soc Med. 1928;21(12):1933.
- Gray RF, Nicolaides AR. Vertigo following aural suction: can it be prevented? Clin Otolaryngol Allied Sci. 1988;13(4):285-8.
- McInerney NJ, O'Keeffe N, Mackle T. Aural microsuction: an analysis of post-procedure patient safety incidents. Ir J Med Sci. 2024;193(2):945-7.
- Nicolaides AR, Gray RF. Aural suction without vertigo. Clin Otolaryngol Allied Sci. 1990;15(2):137-40.
- Prowse SJ, Mulla O. Aural microsuction for wax impaction: survey of efficacy and patient perception. J Laryngol Otol. 2014;128(7):621-5. [CrossRef]
- Sarode D, Asimakopoulos P, Sim DW, Syed MI. Aural microsuction. Bmj. 2017;357:j2908.
- Kim CH, Lee J, Choi B, Shin JE. Nystagmus in adult patients with acute otitis media or otitis media with effusion without dizziness. PLoS One. 2021;16(5):e0250357.
- Barany R. Physiologie und pathologie (funktions-prufung) des bogengang-apparates beim menschen: kliniche studien. F Deuticke. 1907.


| Appearance of TM (n = 85) | Patients showing nystagmus (number of patients, %) |
Patients experiencing vertigo (number of patients, %) |
| No TM perforation | ||
| Normal TM (n = 35) | 34 (97%) | 3 (9%) |
| Normal postoperative TM after canal wall up mastoidectomy (n = 7) | 7 (100%) | 2 (29%) |
| Otitis media with effusion (n = 8) | 5 (63%) | 0 (0%) |
| TM perforation | ||
| Chronic suppurative otitis media (n = 14) | 14 (100%) | 9 (64%) |
| Middle ear cholesteatoma with/without laby- rinthine fistula (n = 5) | 5 (100%) | 5 (100%) |
| Ventilation tube in situ (n = 6) | 6 (100%) | 3 (50%) |
| TM without perforation after open cavity mastoid- ectomy (n = 6) | 6 (100%) | 5 (83%) |
| Adhesive otitis media (n = 4) | 4 (100%) | 4 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



