Submitted:
20 February 2025
Posted:
21 February 2025
You are already at the latest version
Abstract
Background and aims: Prostatectomy is a common surgical procedure for prostate cancer, the most frequently diagnosed cancer in the male population. The choice of anaesthetic technique has a significant impact on postoperative pain management. The changes in recommendations between 2015 and 2021 prompted this study to evaluate the impact of intrathecal morphine administration in combination with general anaesthesia compared to general anaesthesia alone on postoperative analgesic consumption and associated side effects. Material and Methods: A single center retrospective cohort study was conducted, analysing data from 202 patients who underwent prostatectomy between 2015 and 2021. Patients were divided into two groups: 147 patients received intrathecal morphine combined with general anaesthesia, while 49 patients received general anaesthesia alone. Key postoperative parameters, including Numerical Rating Scale (NRS) scores, analgesic consumption, and side effects (e.g., nausea, pruritus, hypotension, respiratory depres-sion) were evaluated. Statistical analyses were performed using Mann-Whitney U-tests and multiple regression models. Results: The group receiving intrathecal morphine showed a significant decrease in NRS pain scores at rest and during movement (p < 0.001). The need for postoperative analgesics, especially opioids such as piritramide, was reduced in this group. No significant increase in serious side effects such as respiratory depression was observed. Conclusion: The present study investigates the potential of intrathecal morphine combined with general anaesthesia as a promising approach to improve pain management in prostatectomy patients. By reducing pain intensity, this method shows significant clinical benefits. In addition, the absence of a significant increase in serious adverse events reinforces the safety of this approach. However, further studies are warranted to assess long-term outcomes and explore optimal dosing strategies. The re-introduction of this anaesthetic technique has great potential to improve patient recovery and satisfaction following major surgery.
Keywords:
intrathecal morphine
; prostatectomy
; general anaesthesia
; postoperative pain
; analgesic consumption
; side effects
; numerical rating scale (NRS)
; spinal anaesthesia
; retrospective cohort study
; pain management
1. Introduction
Prostate cancer is the most commonly diagnosed malignancy in men and a leading cause of cancer-related mortality worldwide [1,2]. In Germany, prostatectomy is a commonly performed surgical procedure, with 21,850 cases documented in 2016 alone [3]. The rising prevalence of prostate cancer has been attributed to the increasing use of prostate-specific antigen (PSA) screening, a practice that has improved early detection but also raised concerns about overdiagnosis [4,5,6].
Effective postoperative pain management is critical to improving recovery after prostatectomy [7,8]. Inadequate management of postoperative pain can impede mobilisation, prolong healing and increase the risk of complications, including deep vein thrombosis and pulmonary embolism [9,10]. Spinal anaesthesia, consisting of the local anaesthetics bupivacaine and morphine in combination with general anaesthesia (GA), has been adopted as standard practice in many institutions [11], including the Cologne Hospital, Holweide, Germany, with the aim of improving pain management.
Although the analgesic benefits of intrathecal morphine (ITM) are well documented, its use is not without risk. Adverse effects such as pruritus, nausea and respiratory depression have been reported [12,13]. In addition, international guidelines differ in their recommendations for the use of ITM in prostatectomy due to these potential complications. For example, the European Association of Urology (EAU) guidelines emphasise the importance of balancing pain management with minimising side effects [4]. Similarly, the PROSPECT guidelines, as established by Lemoine et al. in 2021 [7], conversely advise against its use due to the unresolved issue of its side effects and the unstudied duration of its effect [7]. While Joshi et al. (2015) [14] highlighted the efficacy of ITM in reducing postoperative pain, they also emphasised the need for caution regarding its associated side effects, particularly in the context of prostatectomy. In contrast to Lemoine et al. (2021), Joshi et al. (2015) recommended ITM for prostatectomy, citing its analgesic effect and the low side effects when applied correctly [7,14]. Enhanced recovery after surgery protocols emphasise the need for multimodal approaches to optimise patient outcomes while minimising risks [15]. These protocols highlight the potential of combining GA with ITM to achieve superior postoperative pain management and accelerated recovery [15].
This study investigates the efficacy and safety of ITM in combination with GA for prostatectomy. Specifically, it compares this approach to GA alone, focusing on postoperative pain management, analgesic consumption, and the incidence of side effects. The results of this study are intended to provide evidence to guide clinical decision making and improve patient care.
2. Materials and Methods
This retrospective, single-centre study was conducted at Cologne-Holweide Hospital, Germany, to evaluate the efficacy and safety of ITM in combination with GA in patients undergoing open radical prostatectomy. The study was conducted in accordance with the Declaration of Helsinki and the European Union's General Data Protection Regulation (GDPR), and ethical approval was granted by the Ethics Committee of the University of Witten/Herdecke (approval number S-240/2024). Data collection and analysis took place between September 2024 and January 2025, with data from patients treated between 2015 and 2021.
The study included 202 patients with diagnosed and histologically confirmed prostate cancer who underwent open radical prostatectomy. Patients were included in the study if they had complete and consistent documentation in their medical records. Patients with incomplete data or who underwent additional surgical procedures unrelated to prostate cancer were excluded from the study. To protect the confidentiality of the patients, the data were anonymised and access to the records was restricted to authorised personnel who had received training in data protection.
Patient data were extracted from both electronic and paper records archived in the hospital's CCP® system. The variables extracted included demographic information (age, height, weight), preoperative parameters (comorbidities, Numerical Rating Scale (NRS) chronic pain score, previous opioid use and home medication), intraoperative clinical parameters and postoperative outcomes.
The present study was designed to compare two different groups of patients: those who received GA alone and those who received GA in combination with ITM. In the GA+ITM group, spinal anaesthesia was administered using 0.3 mg intrathecal morphine combined with bupivacaine under strict aseptic conditions. General anaesthesia was induced by intravenous administration of propofol (2-3 mg/kg), sufentanil (0.25-0.75 µg/kg) or fentanyl (2 μg/kg) and cisatracurium (0.15 mg/kg). It should also be noted that the volatile anaesthetics sevoflurane or desflurane were used during the maintenance phase of anaesthesia in this study. Maintenance of anaesthesia was achieved by the use of intravenous agents and volatile anaesthetics, which were tailored to the clinical condition of the patient.
The intraoperative monitoring protocol was standardised and included non-invasive and invasive blood pressure measurement, electrocardiography and pulse oximetry. The intraoperative fluid management strategy included the administration of crystalloids while blood products were administered as needed based on estimated blood loss and anemia (hemoglobin below 8 g/dl). Vasopressors such as cafedrine/theodrenaline or noradrenaline were administered as required to maintain haemodynamic stability. Prophylactic dexamethasone (4-8 mg) was also given as a co-analgesic respectively to prevent nausea and vomiting.
Postoperatively, patients were monitored in the recovery room for vital signs, respiratory function and pain management. Pain intensity was assessed at rest and during mobilisation using the NRS. Following NRS measurement, analgesic regimens were administered, including intravenous piritramide, metamizole, and oral oxycodone, with naloxone administered as needed to counter opioid side effects. Nausea and vomiting were treated with dimenhydrinate, ondansetron, metoclopramide and promethazine. Postoperative complications, including pruritus, respiratory depression, haemodynamic instability and surgical complications, were meticulously documented along with the procedures performed. Patients were then transferred to the Intermediate Care Unit (IMC)) or Intensive Care Unit (ICU) for further monitoring, depending on clinical need and clinic resources.
The total duration of hospitalisation, days on ICU/IMC, complications such as paravasation, wound dehiscence, postoperative urinary output and haematuria, were meticulously documented. Pain management and mobilisation status were also tracked on the first postoperative day. Data on analgesic requirements and their correlation with pain scores were collected to evaluate the efficacy of the anaesthetic techniques. The analysis was conducted utilising SPSS version 29 (IBM). The patient characteristics were summarised using descriptive statistics, while the Mann-Whitney U test was applied to compare non-parametric variables between the two groups. A multiple linear regression analysis was performed to identify predictors of postoperative pain and analgesic consumption. A p-value of less than p< 0.05 was considered to be statistically significant. The study adhered to the European Association of Urology (EAU) guidelines on prostate cancer treatment from Mottet et al. [4] and the PROSPECT guidelines for pain management after prostatectomy Lemoine et al. [7], incorporating evidence from Joshi et al. [14] regarding the use of ITM.
The anonymised dataset and detailed protocols for data collection and analysis are available upon request, with the aim of facilitating replication and further research. While this study provides valuable insights, its retrospective nature and the reliance on pre-existing records present inherent limitations. Nevertheless, efforts were made to minimise biases and ensure the accuracy of collected data.
3. Results
3.1. Demographic Data
In the period between 2015 and 2021, a total of 202 patients underwent radical prostatectomy at Cologne Hospital, Holweide, Germany. With regard to the anaesthetic technique employed, 147 patients received a combination of ITM and GA, while 49 patients underwent general anaesthesia alone. In six cases, the type of anaesthesia used could not be determined. The mean age of patients in the spinal and general anaesthesia group was 68.18 ± 7.697 years, compared to 70.27 ± 6.984 years in the general anaesthesia-only group. Further analysis revealed comparable body weights and heights between the two groups, with average weights of 85.64 ± 17.043 kg and 84.29 ± 13.995 kg, and mean heights of 175.91 cm.
The duration of hospital stay was found to be reduced in the combined anaesthesia group (12.41 ± 4.668 days) in comparison to the general anaesthesia-only group (14.37 ± 7.857 days). The length of stay in the ICU or IMC prior to transfer to a standard ward was comparable between the two groups (0.94 ± 0.751 vs. 0.87 ± 0.647 days).

Table 1.
Demographic data presentation of data as number n or mean value ± standard deviation.
| ITM | No – ITM | |
|---|---|---|
| n | 147 | 49 |
| Age (Years) | 68.18 ± 7.697 | 70.27 ± 6.984 |
| Weight (Kg) | 85.64 ± 17.043 | 84.29 ± 13.995 |
| Height (cm) | 175.91 ± 9.485 | 175.91 ± 8.070 |
| Hospital Stay (days) | 12.41 ± 4.668 | 14.37 ± 7.857 |
| ICU / IMC Stay (days) | 0.94 ± 0.751 | 0.87 ± 0.647 |
3.2. Pain Assessment and Analgesic Administration
The pain assessment was conducted utilising NRS at two distinct time points: within the recovery room and on the IMC or ICU. The study collected data from 138 patients who received ITM in combination with GA and 43 patients who underwent GA alone; however, a total of 21 patients were excluded from the study due to missing values. Furthermore, 32 patients were excluded from the NRS analysis in the recovery room due to incomplete data, leaving 130 patients in the morphine group and 40 in the non-morphine group.
3.2.1. Recovery Room Pain Assessment and Medication Administration
In the recovery room, patients who received ITM reported an average NRS score of 1.05 (Mdn. = 0.00) at rest and 1.22 (Mdn. = 0.00) during movement. The mean number of analgesic medications administered was found to be 0.2246 (Mdn. = 0.00), with administration occurring approximately 4 hours and 22 minutes (Mdn. = 4:15) after the ITM application. The mean doses of analgesics administered to this group were as follows: 1.18 mg piritramide (Mdn. = 0.00), 0.04 g metamizole (Mdn. = 0.00), 0.00 mg morphine (Mdn. = 0.00) intravenously, and 0.07 mg oxycodone (Mdn. = 0.00) orally.
In contrast, patients who did not receive ITM exhibited higher mean NRS scores in the recovery room: 2.20 (Mdn. = 3.00) at rest and 2.18 (Mdn. = 2.00) during movement. The group received an average number of 0.6744 analgesic medications (Mdn. = 1.00) approximately 4 hours and 32 minutes (Mdn. = 4:30) after surgery. The mean doses of analgesics administered to this group were as follows: 3.62 mg piritramide (Mdn. = 3.00), 0.05 g metamizole (Mdn. = 0.00), 0.12 mg morphine (Mdn. = 0.00) intravenously, and 0.29 mg oxycodone (Mdn. = 0.00) orally.
A Mann-Whitney U test was performed to evaluate potential differences in analgesic administration, NRS scores at rest and during movement in the recovery room and IMC/ICU, timing of initial analgesic administration, and analgesic doses between the two groups. The distributions of these variables differed significantly between the groups (Kolmogorov-Smirnov p < 0.05).
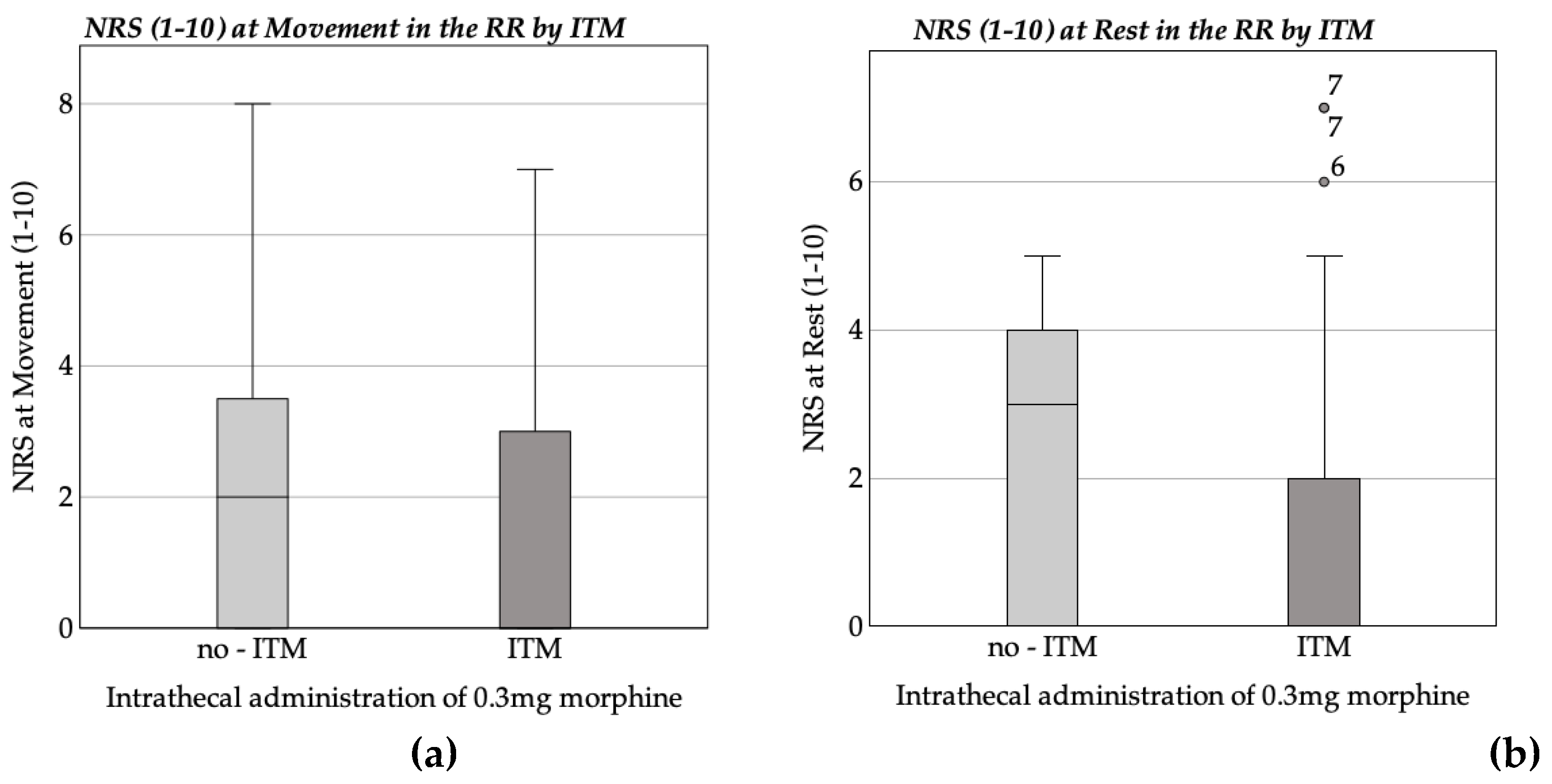
A significant difference was observed in the NRS scores at rest in the recovery room between the intrathecal morphine group (MRank = 78.36) and the non-morphine group (MRank = 108.71) (U = 1671.500, Z = -3.851, p < 0.001, r = -0.295). This outcome is further interpreted in accordance with Cohen's (1988) classification system for correlation strength [16], indicating a moderate correlation (r = 0.3) for NRS scores at rest in the recovery room. The Mann-Whitney U-test revealed no statistically significant difference between the groups in relation to the NRS scores during movement in the recovery room. The ITM group (MRank = 71.60) and the no morphine group (MRank = 84.58) gave U = 1771.500, Z = -1.920 and a p-value of 0.055.
Figure 1.
Boxplot of: NRS at rest and movement in the recovery room (RR). (a) average NRS at movement in the recovery room by ITM; (b) average NRS at rest in the recovery room by ITM.
Figure 1.
Boxplot of: NRS at rest and movement in the recovery room (RR). (a) average NRS at movement in the recovery room by ITM; (b) average NRS at rest in the recovery room by ITM.
A multiple linear regression analysis was conducted in order to investigate the predictors of the NRS score (1–10) at rest in the recovery room. The model demonstrated a significant overall explanation of variance (F(14, 138) = 2.223, p = 0.009), with a total variance explained of R² = 0.184 (adjusted R² = 0.101).
The analysis identified several significant predictors. ITM was found to be associated with a lower NRS score (b = -1.156, SE = 0.345, β = -0.269, t = -3.353, p = 0.001). Furthermore, the analysis revealed a negative correlation between age and the NRS score, with a significant regression coefficient of -0.069 and a p-value of 0.002. Among the intraoperative medications, fentanyl administration demonstrated a significant negative association with the NRS score (b = -1843.000, SE = 0.884, β = -0.168, t = -2.085, p = 0.039).
The analysis revealed that additional factors, including weight, propofol, midazolam, thiopental, sufentanil, and piritramide administration, as well as comorbidities (arterial hypertension, diabetes mellitus, hypothyroidism, and COPD), did not demonstrate significant effects on the NRS score (all p > 0.05) at rest. Furthermore, the elapsed time post-intravenous administration of ITM was not a significant predictor (b = -0.079, SE = 0.181, β = -0.386, t = -0.435, p = 0.749).
Table 2.
Results of the Multiple Linear Regression Analysis for Predictors of NRS- Scores at Rest in the recovery room (N = 153).
Table 2.
Results of the Multiple Linear Regression Analysis for Predictors of NRS- Scores at Rest in the recovery room (N = 153).
| NRS (1-10) at Rest in the recovery room | |||||
| Coefficients | b | SE | β | t | p |
| (Constant) | 9.246 | 1.992 | 4.641 | <.001 | |
| ITM | -1.156 | .345 | -.269 | -3.353 | .001 |
| Age | -.069 | .021 | -.275 | -3.223 | .002 |
| Weight | -.010 | .009 | -.091 | -1.076 | .284 |
| Propofol | -.004 | .002 | -.149 | -1.652 | .101 |
| Midazolam | -.005 | .005 | -.091 | -1.144 | .254 |
| Thiopental | -.010 | .006 | -.128 | -1.577 | .117 |
| Sufentanil | -.082 | .148 | -.048 | -.553 | .581 |
| Piritramide | .034 | .046 | .059 | .726 | .469 |
| Fentanyl. | -1843,000 | .884 | -.168 | -2.085 | .039 |
| Arterial Hypertony Diabetes Mellitus Hypothyroidism COPD Time after ITM |
-.079 .181 -.386 -4.85 -2.217E-5 |
.294 .490 .563 .749 .000 |
-.022 .030 -.055 -.056 -.041 |
-.269 .369 -.686 -.647 -.522 |
.788 .713 .494 .518 .603 |
| Remarks: N = 153; R² = 0.184; corr. R² = 0.101; F(14, 138) = 2.223; p = 0.009 | |||||
A multiple linear regression model was developed in order to ascertain the factors that exert an influence on NRS scores (1–10) during movement in the recovery room. The model demonstrated a substantial explanation of variance in NRS scores, F(14, 138) = 1.791, p = 0.045, with a total variance explained of R² = 0.154 (adjusted R² = 0.068).
The analysis yielded several key findings, highlighting that ITM was significantly associated with reduced NRS scores during movement (b = -0.872, SE = 0.394, β = -0.181, t = -2.214, p = 0.028). Additionally, the analysis revealed a significant negative impact of age on the outcomes (β = -0.290, t = -3.344, p = 0.001). The analysis revealed no significant association between NRS scores during movement and other variables, including weight, midazolam, thiopental, sufentanil, and piritramide administration, as well as comorbidities such as arterial hypertension, diabetes mellitus, hypothyroidism, and COPD (all p > 0.05). The time elapsed since ITM administration was also not a significant predictor (p = 0.801).
Table 3.
Results of the multiple linear regression analysis for rredictors of NRS Scores at movement in the recovery room (N = 153).
Table 3.
Results of the multiple linear regression analysis for rredictors of NRS Scores at movement in the recovery room (N = 153).
| NRS (1-10) at Movement in the recovery room | |||||
| Coefficients | b | SE | β | t | p |
| (Constant) | 9.614 | 2.275 | 4.226 | <.001 | |
| ITM | -.872 | .394 | -.181 | -2.214 | .028 |
| Age | -.082 | .025 | -.290 | -3.344 | .001 |
| Weight | -.009 | .010 | -.078 | -.903 | .368 |
| Propofol | -.005 | .003 | -.162 | -1.758 | .081 |
| Midazolam | -.006 | .005 | -.092 | -1.132 | .260 |
| Thiopental | -.010 | .007 | -.125 | -1.520 | .131 |
| Sufentanil | -.124 | .168 | -.064 | -.733 | .465 |
| Piritramide | .051 | .053 | .078 | .952 | .343 |
| Fentanyl | -1.727 | 1.009 | -.141 | -1.711 | .089 |
| Arterial Hypertony | -.108 | .336 | -.027 | -.321 | .749 |
| Diabetes Mellitus | .302 | .559 | .044 | .541 | .590 |
| Hypothyroidism | -.478 | .643 | -.061 | -.743 | .458 |
| COPD | -.083 | .856 | -.009 | -.097 | .923 |
| Time after ITM | 1.223E-5 | .000 | .020 | .252 | .801 |
| Remarks: N = 153; R² = 0.154; corr. R² = 0.068; F (14, 138) = 1.791; p = 0.045 | |||||
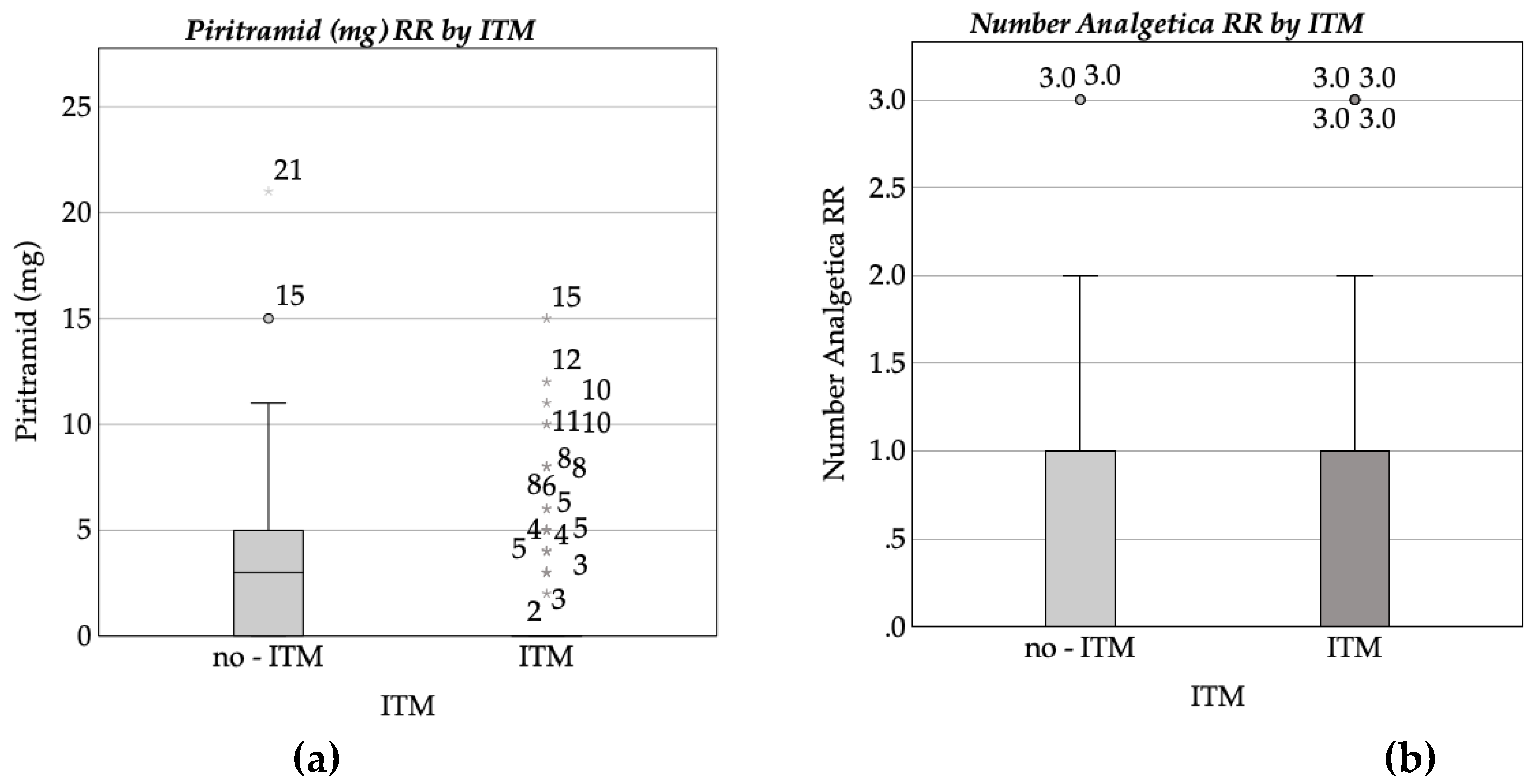
Patients who received ITM required a lower amount of analgesics in the recovery room compared to those who did not receive ITM. The mean piritramide dose was 1.18 mg (SD = 2.76) in the ITM group, compared to 3.62 mg (SD = 4.50) in the control group. A similar observation was made with the total number of analgesics administered, which was markedly lower in the ITM group (M = 0.22, SD = 0.45) compared to the non-ITM treated group (M = 0.67, SD = 0.61). Furthermore, no intravenous morphine was required in the intrathecal morphine group (M = 0.00, SD = 0.00), while the control group had a mean morphine dose of 0.12 mg (SD = 0.76). A significant difference in the total dosage of piritramide administered in the recovery room was observed between the two groups. The Mann-Whitney U test yielded a significant result, U = 1838.000, Z = -4.684, p < 0.001, indicating that the treatment group received lower piritramide dosages (Mdn. rank = 82.82) compared to the control group (Mdn. rank = 117.26). According to the guidelines established by Cohen (1988) [16], the effect size corresponds to a moderate correlation. A significant discrepancy was identified between the treatment group (Mdn. rank = 82.39) and the control group (Mdn. rank = 118.63) with regard to the number of analgesics administered in the recovery room. The Mann-Whitney U test yielded U = 1779.000, Z = -4.944, p < 0.001, with an effect size of r = -0.367, thus confirming a moderate correlation (Cohen, 1988) [16].
Figure 2.
Boxplot of: (a) Intravenous piritramide dose (mg) administered in the recovery room (RR) by intrathecal morphine (ITM) administration status; (b) Number of analgesics administered in the recovery room (RR) by intrathecal morphine (ITM) administration status.
Figure 2.
Boxplot of: (a) Intravenous piritramide dose (mg) administered in the recovery room (RR) by intrathecal morphine (ITM) administration status; (b) Number of analgesics administered in the recovery room (RR) by intrathecal morphine (ITM) administration status.
A multiple linear regression analysis was performed in order to ascertain the predictors of piritramide dosage (mg) in the recovery room. The model, incorporating ITM, patient characteristics (age, weight), comorbidities, and intraoperative medications, did not attain statistical significance (F(14, 129) = 1.466, p = 0.133) and accounted for a mere 13.7% of the variance (R² = 0.137; adjusted R² = 0.044).
ITM (p = 0.296), age (p = 0.430), weight (p = 0.139), and comorbidities demonstrated no statistically significant associations with piritramide dosage. Among the intraoperative medications, sufentanil approached significance (p = 0.083). The complete regression results can be found in Appendix A.1.
A multiple linear regression analysis was conducted in order to identify predictors of the number of analgesics administered in the recovery room. The model incorporated a range of variables, including intrathecal morphine administration, patient characteristics (age, weight), comorbidities (e.g., arterial hypertension, diabetes mellitus, hypothyroidism, COPD), intraoperative medication dosages, and the timing of pain measurement and analgesic administration.
The regression model did not attain statistical significance (F(14, 129) = 1.223, p = 0.266) and explained a mere 11.7% of the variance in the number of analgesics administered (R² = 0.117; adjusted R² = 0.021). None of the predictors demonstrated a significant association with the outcome variable (p > 0.05), although weight (p = 0.099), propofol dosage (p = 0.077), and arterial hypertension (p = 0.086) approached significance. The comprehensive results of the regression analysis are presented in Appendix A.2.
The timing of pain measurements and administration of analgesics was then compared between two groups: patients receiving ITM (N = 136) and those not receiving ITM (N = 42). Descriptive statistics showed a mean time of 4:22 hours (± 0:52) for the ITM group and a mean time of 4:32 hours (±1:09) for the non-ITM group. The Mann-Whitney U-test yielded a U-value of 2559.500 with a Z-score of -1.017 and a p-value of 0.309, indicating that there was no statistically significant difference between the groups in terms of the timing of pain measurement and medication administration (p > 0.05).3.2.2. IMC / ICU pain assessment and medication administration.
The investigation encompassed the evaluation of pain parameters within the IMC and the ICU, with the NRS being utilised to assess pain levels at rest and during movement. The time interval to the initial administration of analgesics was also determined. Furthermore, the total quantity of analgesics administered, along with the dosages of specific medications such as piritramide, metamizole, oxycodone, oxycodone/naloxone, tilidin, and ibuprofen, were documented. A subsequent analysis identified significant differences in the distribution of these variables between the treatment and control groups using the Kolmogorov-Smirnov test (p < 0.05).
The NRS at rest data set comprised 149 patients, with 38 patients in the control group (no ITM) and 111 patients in the treatment group (ITM). The control group reported a mean NRS of 1.24 (Mdn. = 0.00), while the treatment group reported a mean NRS of 0.77 (Mdn. = 0.00). However, the Mann-Whitney U test revealed no statistically significant difference between the groups (U = 1758, Z = -1.89, p = 0.05). Furthermore, an additional analysis of the NRS during movement data set, encompassing 149 patients (39 in the control group and 110 in the treatment group), was conducted. The mean NRS was 1.72 (Mdn. = 0.00) in the control group compared to 0.90 (Mdn. = 0.00) in the treatment group. However, once more, no significant difference was observed (U = 1771, Z = -1.92, p = 0.05).
A further comparison was made between the two groups with regard to the total number of analgesics administered on the IMC/ICU. The treatment group (N = 124) received an average of 0.92 analgesics (Mdn. = 1.00), while the control group (N = 44) received 0.95 analgesics (Mdn. = 1.00). The Mann-Whitney U test revealed that there was no significant difference between the groups (U = 2696, Z = -0.13, p = 0.89).
In the course of the analysis of the effects of specific analgesics, the treatment group received, on average, 0.77 mg of piritramide (Mdn. = 0.00), 0.51 g of metamizole (Mdn. = 0.00), and 1.69 mg of oxycodone (Mdn. = 0.00), 0.32 mg of oxycodone/naloxone (Mdn. = 0.00), 1.61 mg of tilidin (Mdn. = 0.00), and 4.88 mg of ibuprofen (Md = 0.00). In comparison, the control group received 1.27 mg of piritramide (Mdn. = 0.00), 0.53 g of metamizole (Mdn. = 0.00), and 1.14 mg of oxy codone (Mdn. = 0.00), 0.45 mg of oxycodone/naloxone (Mdn. = 0.00), 2.27 mg of tilidin (Mdn. = 0.00), and no ibuprofen. The application of statistical tests revealed no significant differences in the dosage of piritramide (U = 2389.5, Z = -1.67, p = 0.095), metamizole (U = 2725, Z = 0.012, p = 0.990), oxycodone (U = 2595.5, Z = -0.775, p = 0.438), or oxycodone/naloxone (U = 2438.5, Z = -0.751, p = 0.452).
The temporal parameters surrounding the initial administration of analgesics were also subjected to rigorous scrutiny. In the treatment group, the administration of analgesics occurred, on average, 11:30 hours (Mdn. = 11:15) after surgery, while in the control group, analgesics were administered after 12:54 hours (Mdn. = 11:00). This discrepancy did not attain statistical significance (U = 2438.5, Z = -0.751, p = 0.452).
In summary, the results of the Mann-Whitney U test demonstrate that there are no statistically significant differences between the treatment and control groups with regard to NRS scores, the total number of analgesics administered, or the dosages of specific analgesics on the IMC/ICU ward.
3.3. Complications and side effects
3.3.1. Hemodynamic Complications
The investigation of hemodynamic effects following the intrathecal administration of 0.3 mg of morphine involved the analysis of heart rates (bpm) and blood pressure (mmHg) values across multiple time points, in conjunction with the utilisation of circulatory support medications. The investigation involved the measurement of vital signs at several time points, including baseline, immediately following the intervention, and at regular intervals of 5, 10, 15, 20, 25, and 30 minutes, as well as at 6, 12, and 24 hours after the application of the intervention.
Heart rate measurements included 43 patients in the control group and 128 in the morphine group at baseline. No significant differences in heart rate were observed between the two groups at baseline (U = 2727, Z = -0.125, p = 0.901) or at subsequent intervals of 5, 10, 15, or 20 minutes (all p > 0.4). A marginal difference was observed at 30 minutes (U = 2818, Z = -1.74, p = 0.08), but this did not reach statistical significance.
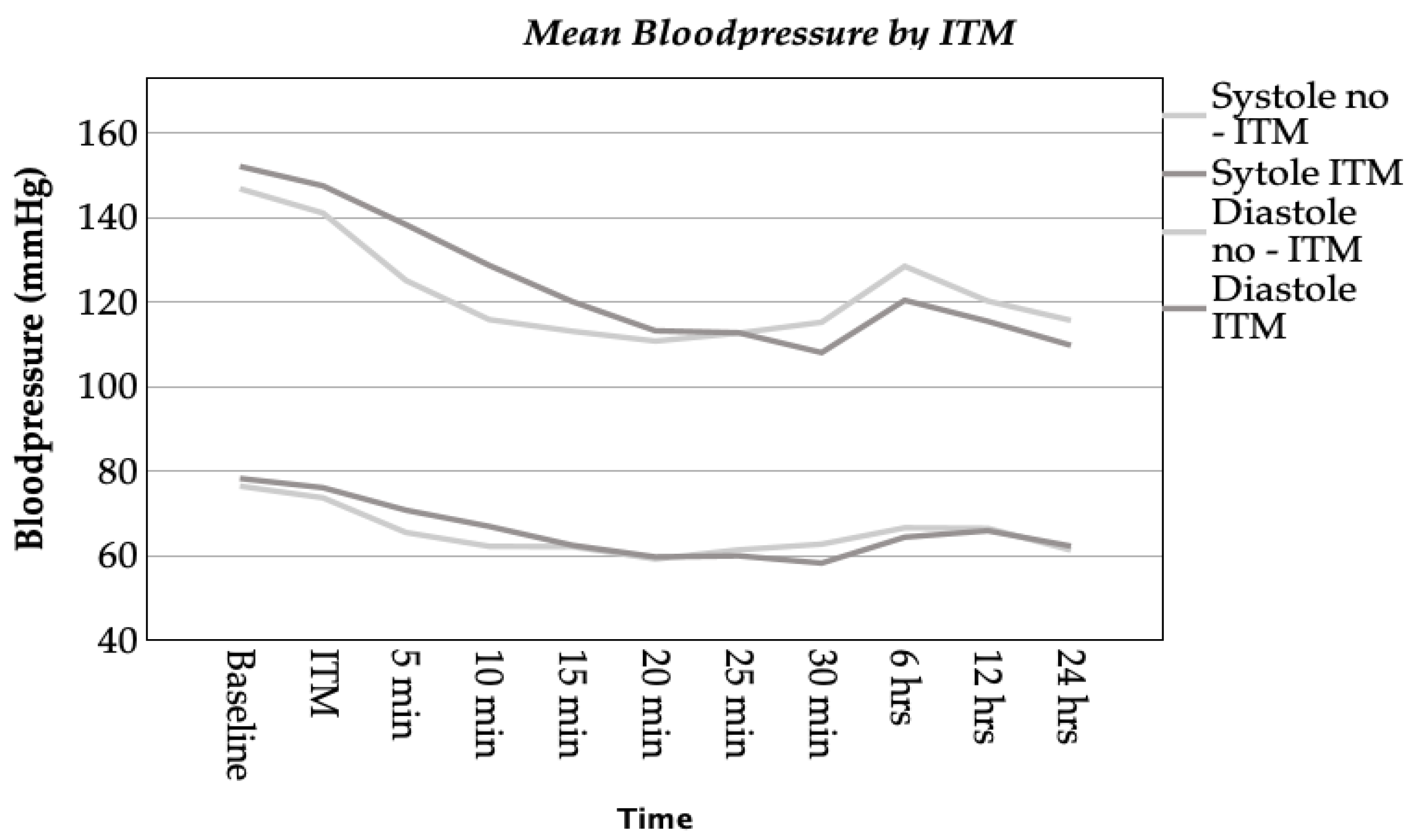
A comprehensive evaluation of blood pressure values was conducted, encompassing both systolic and diastolic parameters. At five minutes post-intervention, a significant difference was observed in systolic blood pressure (U = 2386, Z = -2.524, p = 0.012, r = 0.198), with higher values recorded in the morphine group. A similar trend was observed in diastolic blood pressure, with a significant difference noted (U = 2564, Z = -1.968, p = 0.049, r = 0.155). At 10 minutes, systolic blood pressure remained significantly elevated in the morphine group (U = 2287, Z = -2.901, p = 0.004, r = 0.213), while diastolic differences did not reach significance (p = 0.092). No significant differences in blood pressure were observed at 20, 25, or 30 minutes, or at later time points (all p > 0.1).
The analysis of blood pressure 30 minutes after the administration of 0.3 mg (ITM) revealed significant associations with systolic and diastolic blood pressure values. A multiple linear regression model for systolic blood pressure explained 6.7% of the variance (R² = 0.067; adjusted R² = 0.023), though the overall model was not statistically significant (F(8, 169) = 1.51, p = 0.156). However, ITM exhibited a significant negative correlation with systolic blood pressure (b = -7.471, SE = 3.037, β = -0.187, t = -2.460, p = 0.015).
Conversely, intraoperative atropine administration exhibited a significant correlation with reduced systolic blood pressure (b = -48.827, SE = 22.771, β = -0.164, t = -2.144, p = 0.033). The impact of other factors, including age, weight, arterial hypertension, diabetes mellitus, Akinor®, and noradrenaline, was not significant (p > 0.2).
With regard to diastolic blood pressure, the regression model explained 9.0% of the variance (R² = 0.09; adjusted R² = 0.047) and was statistically significant (F(8, 169) = 2.087, p = 0.039). ITM was once again found to be significantly associated with lower diastolic blood pressure (b = -5.426, SE = 1.869, β = -0.218, t = -2.903, p = 0.004). Furthermore, intraoperative atropine use exhibited a substantial negative impact on diastolic blood pressure (b = -33.135, SE = 14.013, β = -0.178, t= -2.365, p = 0.019). In a manner analogous to that of systolic blood pressure, other variables, including age, weight, arterial hypertension, diabetes mellitus, Akinor®, and noradrenaline, were not found to be significantly associated with diastolic blood pressure (p > 0.3). Detailed statistical results for systolic and diastolic blood pressure can be found in Appendix A.3 and Appendix A.4, respectively.
Figure 3.
Line chart of mean blood pressure at various time points relative to ITM administration: 5 minutes before ITM (-5), at ITM, and 5, 10, 15, 20, 25, 30 minutes, 6 hours, 12 hours, and 24 hours after ITM.
Figure 3.
Line chart of mean blood pressure at various time points relative to ITM administration: 5 minutes before ITM (-5), at ITM, and 5, 10, 15, 20, 25, 30 minutes, 6 hours, 12 hours, and 24 hours after ITM.
The intraoperative utilisation of circulatory support medications, encompassing Akinor®, atropine, and noradrenaline, was the subject of a comprehensive evaluation. The Mann-Whitney U test revealed no statistically significant differences in Akinor® usage between the groups (p = 0.321). However, a significant difference was observed for atropine, with a lower dose administered in the morphine group (U = 3358, Z = -3.005, p = 0.003, r = 0.215).
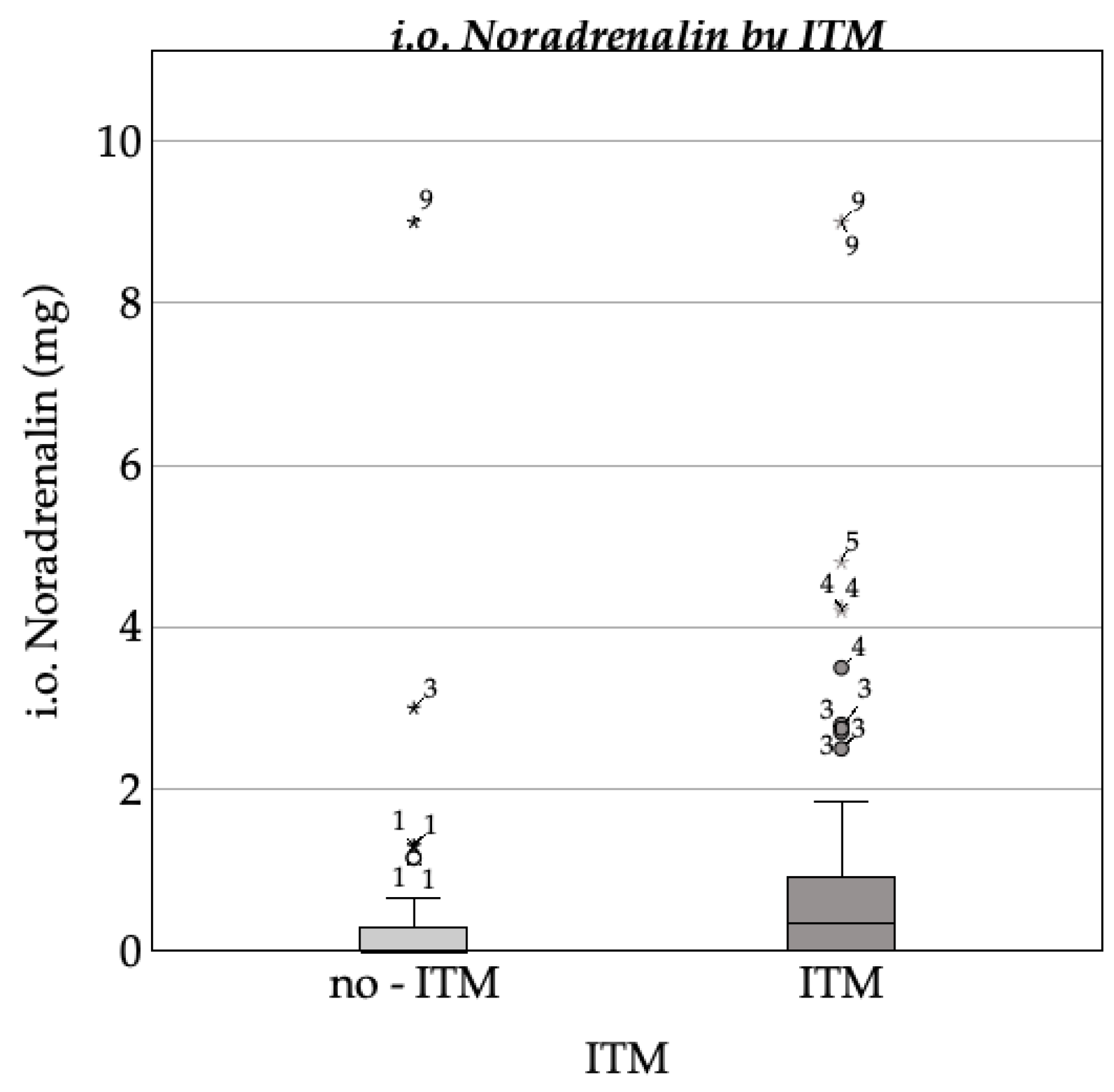
A high mean rank for noradrenaline use was observed in the morphine group in comparison to the control group (U = 2565, Z = -2.964, p = 0.003, r = 0.213).
The regression analysis for the intraoperative administration of noradrenaline included ITM, patient characteristics (age, weight), comorbidities (arterial hypertension, diabetes mellitus), and the intraoperative use of Akinor® and atropine. The model explained only 1.9% of the variance in noradrenaline dosage (R² = 0.019; adjusted R² = -0.022) and was not statistically significant (F(7, 171) = 0.461, p = 0.861). None of the predictors demonstrated a significant association with the noradrenaline dose. Intrathecal morphine (p = 0.320), age (p = 0.862), weight (p = 0.367), arterial hypertension (p = 0.463), diabetes mellitus (p = 0.648), Akinor® (p = 0.727), and atropine (p = 0.588) were all nonsignificant. Detailed results can be found in Appendix A.5.
Figure 4.
Boxplot of mean cumulated noradrenalin by ITM.
The present study focused on the temporal parameters of circulatory medication administration. The mean time to administration was found to be longer in the morphine group (22.52 min, SD = 37.96) compared to the control group (11.98 min, SD = 54.10). However, this difference was not found to be statistically significant (U = 2921, Z = -1.552, p = 0.121).
3.3.2. Respiratory Complications
The analysis of oxygen saturation included patients from both the control group (without ITM) and the intervention group (with ITM). Measurements were conducted at baseline, during morphine administration, and at intervals of 15, 30 minutes, 6, 12, and 24 hours post-intervention. It was noted that the sample size decreased over time due to limited data availability.
In the control group, mean oxygen saturation ranged from 97.80% preoperatively (Mdn. = 98.00%) to 98.94% at 15 minutes, peaking at 99.00% at 30 minutes (Mdn. = 99.00%), and declining to 96.00% at 6 hours and 97.25% at 24 hours. In the intervention group, the mean oxygen saturation at the preoperative stage was found to be marginally lower at 97.42% (Mdn. = 98.00%), peaking at 99.77% at 30 minutes (Mdn = 99.00%) and declining to 96.67% at 6 hours and 96.06% at 24 hours. The Mann-Whitney U test revealed no statistically significant differences in oxygen saturation between the groups at any time point (e.g., preoperative: U = 2604.5, p = 0.455; at 30 minutes: U = 3449.0, p = 0.722).
Figure 5.
Line chart of mean oxygen saturation over time for patients with and without ITM administration. Measurements were taken at baseline, during ITM administration, and at intervals of 15 minutes, 30 minutes, 6 hours, 12 hours, and 24 hours post-intervention.
Figure 5.
Line chart of mean oxygen saturation over time for patients with and without ITM administration. Measurements were taken at baseline, during ITM administration, and at intervals of 15 minutes, 30 minutes, 6 hours, 12 hours, and 24 hours post-intervention.
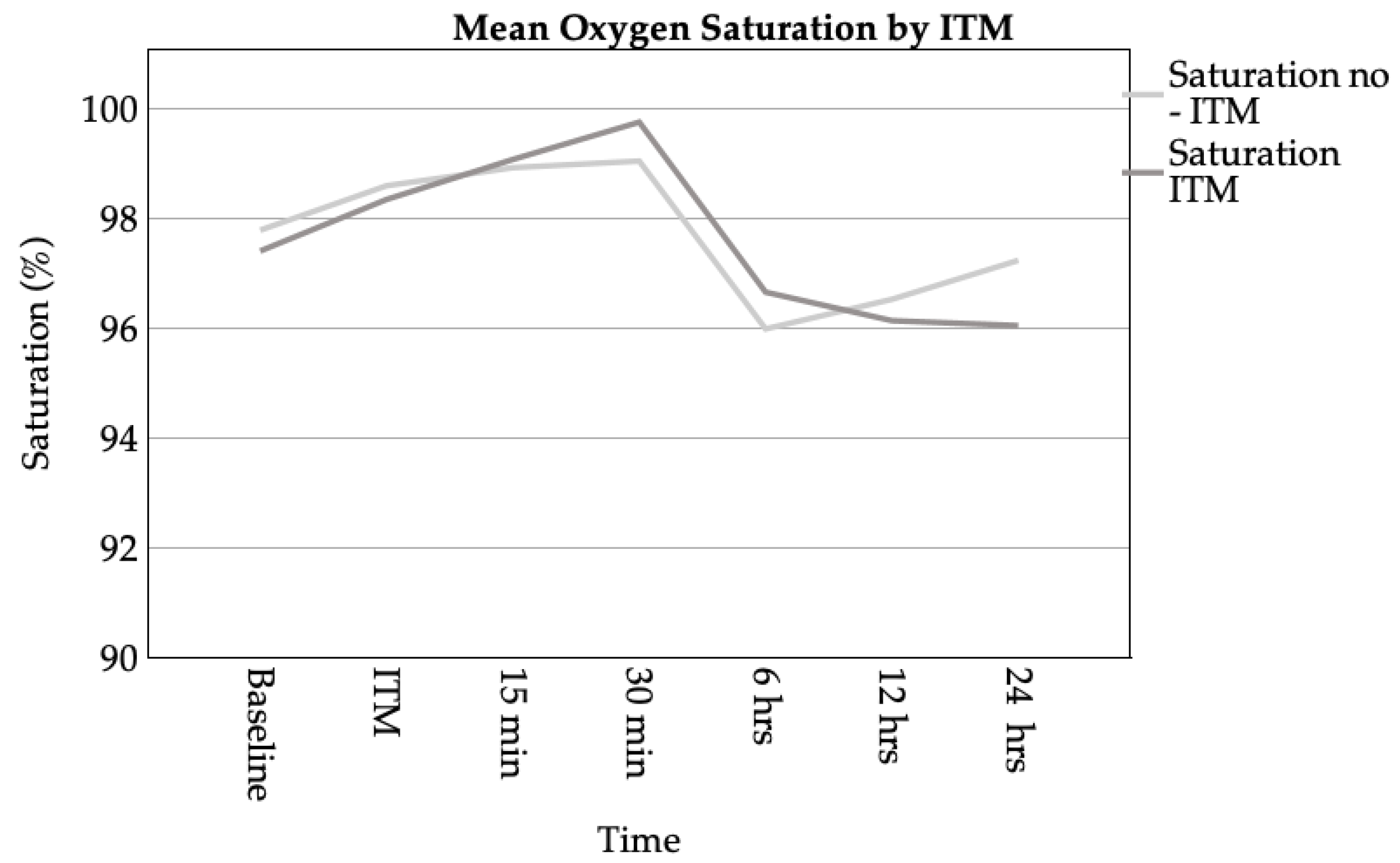
The analysis of oxygen supplementation was conducted at 6 and 12 hours following the intervention. It was observed that both groups exhibited a mean flow rate of 1.55 L/min at 6 hours (Mdn. = 2.00 L/min). At 12 hours, the control group received an average of 1.10 L/min (Mdn. = 1.00 L/min), while the intervention group received 1.35 L/min (Mdn. = 2.00 L/min). The Mann-Whitney U test revealed no statistically significant differences between the groups at either 6 hours (p = 0.653) or 12 hours (p = 0.664).
3.3.3. Hospital Stay
The Mann-Whitney U test was performed to compare the length of hospital stay between patients who received ITM (N = 147) and those who did not (N = 49). Descriptive statistics showed that patients without ITM had a mean hospital stay of 14.37 days (± 7.86), while patients with ITM had a mean hospital stay of 12.41 days (± 4.67). The Mann-Whitney U-test yielded a U-value of 3057.000, a Z-score of -1.611 and a p-value of 0.107, indicating no statistically significant difference in hospital stay between the groups (p > 0.05).
The analysis of hospital stay duration incorporated a range of predictors, including ITM, patient characteristics (age, weight), comorbidities (arterial hypertension, diabetes mellitus), intraoperative noradrenaline utilisation, NRS at rest and movement , the timing of the initial analgesic in the recovery room, and the number of days until transfer to a regular ward. The multiple linear regression model explained 17.4% of the variance in hospital stay duration (R² = 0.174; adjusted R² = 0.114) and was statistically significant (F(10, 138) = 2.9, p = 0.002).
Among the predictors, diabetes mellitus demonstrated a significant positive association with hospital stay, increasing the duration by an average of 5.26 days (b = 5.262, SE = 1.448, β = 0.294, t = 3.635, p < 0.001). Conversely, ITM administration was associated with a reduction in hospital stay duration by approximately 1.74 days; however, this effect did not reach statistical significance (b = -1.743, SE = 0.952, β = -0.152, t = -1.830, p = 0.069). A positive association between weight and hospital stay was observed; however, this effect did not reach statistical significance (β = 0.142, t = 1.731, p = 0.086). The remaining variables, encompassing age, arterial hypertension, intraoperative noradrenaline, pain scores both at rest and during movement, the timing of the initial analgesic administration in the recovery room, and the days until transfer to a regular ward, were found to have a non-significant impact on the prediction of hospital stay duration (p > 0.1 for all). Detailed results are presented in Appendix A.6.
3.3.4. Effect of Intrathecal Morphine on Postoperative Nausea and Vomiting
Postoperative symptoms of nausea and vomiting in the recovery room were analysed in 178 patients, including 43 in the control group (no ITM) and 135 in the intervention group (with ITM).
In the control group, the mean incidence of emesis was 0.00 (Mdn. = 0.00), and nausea was 0.05 (Mdn = 0.00). The median time of occurrence for nausea was recorded as 5:30 hours postoperatively. The anti-emetic medications administered included dimenhydrinate (mean = 10.07 mg), with minimal use of other agents.
In the intervention group, the mean incidence of emesis was 0.01 (Mdn. = 0.00), and the mean incidence of nausea was 0.06 (Mdn. = 0.00). The median time of occurrence for emesis was recorded as 4:13 hrs. The anti-emetic medications administered included dimenhydrinate (mean = 9.00 mg) and butylscopolamine (mean = 16.00 mg), with limited use of other agents.
The Mann-Whitney U test was employed to evaluate the differences between the control group (no ITM) and the intervention group (with ITM) in the recovery room in terms of the incidence of nausea and emesis, as well as the administration of anti-emetic medications.
The investigation revealed no statistically significant difference between the groups in terms of emesis in the recovery room (U = 2859.500, Z = -0.800, p = 0.423). The mean ranks were 88.50 for the control group and 89.82 for the morphine group. Similarly, no significant difference was found for nausea in the recovery room (U = 2888.000, Z = -0.306, p = 0.760), with mean ranks of 89.16 and 90.26, respectively.
On the IMC / ICU ward, a non-significant trend towards a difference in nausea incidence was observed (U = 2399.000, Z = -1.512, p = 0.130), with mean ranks of 77.79 for the control group and 85.50 for the morphine group. The temporal dynamics of nausea following intrathecal morphine administration also did not exhibit a significant difference (U = 21.000, Z = -0.840, p = 0.401), with mean ranks of 9.00 hrs for the control group and 12.45 hrs for the morphine group.
For the occurrence of emesis within the ward setting, no statistically significant differences were observed (U = 2360.000, Z = -0.233, p = 0.816), with mean ranks of 79.50 for the control group and 80.83 for the morphine group. Furthermore, the temporal dynamics of emesis following morphine administration did not demonstrate a statistically significant variation (U = 73.000, Z = -0.665, p = 0.506), with mean ranks of 18.57 hrs and 15.92 hrs, respectively.
The analysis of anti-emetic medication doses also revealed no significant differences between the groups. For dimenhydrinate, the Mann-Whitney U test yielded U = 2415.000 (Z = -0.400, p = 0.689), and for ondansetron, U = 2460.000 (Z = -0.568, p = 0.570). Analogous non-significant outcomes were identified for butylscopolamine, metoclopramide, and promethazine. A slight trend was observed for promethazine (U = 2418.000, Z = -1.761, p = 0.078), but this was not statistically significant. The total number of anti-emetic medications administered was not found to be significantly different (U = 2420.000, Z = -0.363, p = 0.717), with mean ranks of 84.00 for the control group and 82.02 for the morphine group.
The results of the linear regression analysis for predicting postoperative emesis in the recovery room are summarised as follows. The regression model incorporated the following predictor variables: ITM, age, weight, NRS at rest (1–10), NRS during movement (1–10), timing of pain assessment and analgesic administration in the recovery room, sufentanil dose, fentanyl dose, nausea in the recovery room, diabetes mellitus, and intraoperative dexamethasone dose.
The model accounted for 29.1% of the variance in emesis (R² = 0.291, adjusted R² = 0.236), with a statistically significant fit (F(11, 141) = 5.269, p < 0.001). The standard error of the estimate was 0.100. The detailed results of the regression analysis are presented in Appendix A.6 and summarised in the table below.
Multiple linear regression analysis was performed to identify predictors of nausea in the RR. The model included ITM, fentanyl , sufentanil, dexamethasone, age, weight, rest and movement pain scores at RR, time to first analgesic administration in the RR, and diabetes mellitus. The overall model was not statistically significant (F(10, 142) = 0.793, p = 0.635, R² = 0.053, adjusted R² = -0.014), indicating that the included variables did not explain a meaningful proportion of the variance in postoperative nausea.
Among the predictors, ITM did not show a significant association with nausea in the RR (B = 0.058, p = 0.211), suggesting that its administration did not have a significant impact on postoperative nausea in this cohort. Similarly, other variables including dexamethasone (B = -0.003, p = 0.512), sufentanil (B = -0.002, p = 0.894) and pain scores did not reach statistical significance. Age, weight and diabetes mellitus also showed no significant influence. Detailed results of the regression analysis can be found in Appendix A.7.
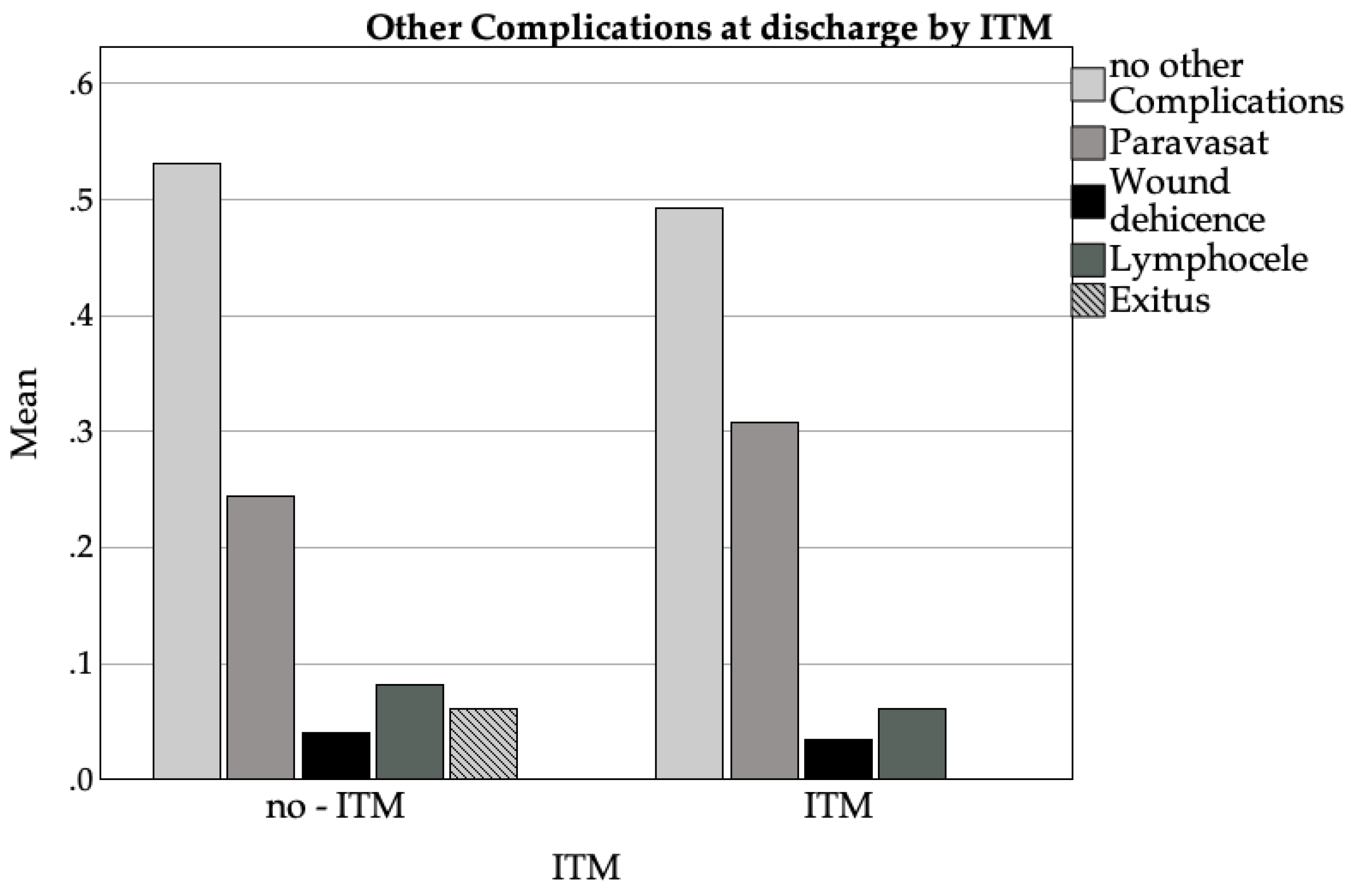
3.3.5. Other Complications
The following section will analyse the complications listed in the discharge summary.
Among patients who did not receive ITM (N = 49), 53% experienced no further documented complications (Mdn. = 0.53, SD = .504), while Vesicoureteral anastomotic insufficiency (paravasation) occurred in 24% (Mdn. = .24, SD = .434), lymphoceles in 8% (Mdn = 0.08, SD = .277), and wound dehiscence in 4%. Postoperative delirium was not observed. In the ITM group (N = 146), no complications occurred in 49% (Mdn. = .49, SD = .502), Vesicoureteral anastomotic insufficiency (paravasation) occurred in 31% (Mdn. = 0.31, SD = .463), and lymphoceles occurred in 6% (Mdn. = 0.06, SD = .241). Wound dehiscence occurred in 3% of cases and postoperative delirium in 1%. Across both groups (N = 195), 50% exhibited no complications, 29% experienced vesicoureteral anastomotic insufficiency (paravasation) and 7% demonstrated lymphocele, and 2% died.
Mortality occurred in 3 patients (1.5%), while 98.5% (N = 198) survived. One case was missing, resulting in a total of N = 202 recorded cases. The cause of death of the three deceased patients was documented as cardiac arrest in the relevant discharge reports.
Patients without ITM had a mortality rate of 6% (mean = 0.06, SD = 0.242,), while no deaths occurred in the ITM group (mean = 0.00, SD = 0.000, N = 146). The overall mortality rate was 2% (mean = 0.02, SD = 0.123, N = 195).
The Mann-Whitney U test revealed no significant differences between the groups with regard to the majority of complications. For the category of "no complications," the mean ranks were 100.73 (without ITM) and 97.08 (with ITM) (U = 3443.000, p = 0.651). The Mann-Whitney U test further revealed no statistically significant differences for the occurrence of paravasation (U = 3350.500, p = 0.400), wound dehiscence (U = 3443.000, p = 0.651), postoperative delirium (U = 3443.000, p = 0.651), and the majority of other categories (all p > 0.05).
Figure 6.
Bar chart of the distribution of side effects reported in the discharge summaries grouped by intrathecal morphine (ITM) administration.
Figure 6.
Bar chart of the distribution of side effects reported in the discharge summaries grouped by intrathecal morphine (ITM) administration.
4. Discussion
Intrathecal morphine is a potent option for the management of postoperative pain due to its unique pharmacological profile. Its hydrophilic nature leads to slow clearance from the cerebrospinal fluid (CSF) and significant rostral spread, resulting in prolonged analgesia but also a reported higher risk of side effects such as pruritus, nausea, and respiratory depression [1,2,3]. Morphine exerts its primary effects through μ-opioid receptors (MORs), resulting in a reduction in neurotransmitter release and a decrease in neuronal excitability [4,5]. The medication under scrutiny in this study has been demonstrated to achieve effective analgesia at a receptor occupancy level of 80%, a distinction that sets it apart from other opioids [6]. The prolonged effects of morphine are further enhanced by its slow systemic diffusion, although this process concomitantly increases the risk of delayed respiratory depression [7]. Morphine-6-glucuronide (M6G), a metabolite of morphine, contributes marginally to analgesia [8].
The findings of this study corroborate the efficacy of ITM in diminishing post-operative pain intensity and opioid consumption, with patients receiving ITM reporting significantly lower NRS scores both at rest and during movement in the immediate postoperative period, consistent with findings from prior studies [25,26]. Furthermore, the requirement for supplemental analgesics, including piritramide and metamizole, was significantly reduced in the morphine group. This finding is consistent with earlier research indicating that intrathecal morphine significantly delays the time to first analgesic request [27,28]. In the recovery room, patients who received ITM exhibited an average NRS score of 1.05 at rest and 1.22 during movement. Patients in the ITM group demonstrated a reduced requirement for analgesics, with a mean piritramide dose of 1.18 mg compared to 3.62 mg in the non-morphine group. Furthermore, the Mann-Whitney U test revealed a statistically significant difference in the total number of analgesics administered between the morphine group (mean = 0.22) and the control group (mean = 0.67). The Mann-Whitney U test also revealed statistically significant differences in analgesic consumption and NRS scores at rest, with moderate effect sizes according to Cohen's guidelines [16].
In contrast, the non-morphine group exhibited significantly higher pain scores and analgesic consumption, indicating a greater reliance on postoperative opioid administration. This finding emphasises the benefits of ITM in reducing immediate postoperative analgesic requirements, which is particularly relevant in minimising i.v.-opioid-related side effects such as sedation and respiratory depression. The findings of this study are in accordance with the guidelines proposed by Joshi et al. (2015) and Lemoine et al. (2021) [9,10], which underscore the significance of incorporating neuraxial opioid techniques into multimodal analgesic regimens for achieving optimal postoperative pain management. Lemoine et al. emphasise that the decrease in systemic opioid requirements, as evidenced by this study, is associated with a reduced occurrence of sedation and respiratory complications, thereby validating the safety profile of intrathecal morphine [9]. Nevertheless, Lemoine et al. advocate a high level of vigilance with regard to the risk of dose-dependent side effects and the insufficiently investigated duration of the analgesic effect [9]. Consequently, they advise against the continued use of ITM in radical prostatectomy in 2021, despite the recommendation by Joshi et al. in 2015, which was based on its analgesic effect and low side effects when ITM is used correctly [7].
In the context of the IMC/ICU, no substantial disparities were identified between the morphine and non-morphine groups with respect to NRS scores, the aggregate amount of analgesics administered, or the specific dosages of particular analgesics. These findings suggest that while ITM provides robust analgesia in the immediate postoperative phase, its effects may diminish over time as systemic analgesics become the primary mode of pain management. These observations are consistent with those of previous studies, which reported that the analgesic efficacy of intrathecal morphine is most pronounced within the first 12 to 24 -36 hours post-surgery [1,3,11].
The prolonged analgesic duration of ITM, attributable to its hydrophilicity and slow systemic clearance, underscores its utility in managing postoperative pain in high-risk surgical populations [17,18]. Nevertheless, the optimal dose remains a subject of debate, with higher doses having been associated with an increased incidence of side effects without proportional improvements in analgesia [29]. The intrathecal 0.3 mg morphine utilised in this study exceeds the doses recommended in current guidelines, including the dose recommended by Joshi et al. (2015) [11] and the doses investigated by Lemoine et al. (2021) for the PROSPECT Guidelines [7]. The abovementioned authors propose the utilisation of reduced doses, ranging from 0.1 to 0.2 mg, as a means to attain a harmonious equilibrium between efficacy and safety, emphasising the importance of minimising dose-related adverse effects while ensuring sufficient analgesia is maintained [7,14].
The present study set out with the objective of investigating the haemodynamic, respiratory and other complications associated with intrathecal morphine administration. The haemodynamic effects comprised alterations in heart rate and blood pressure, which were analysed at the baseline and at multiple intervals post-intervention. No significant differences in heart rate were observed between the morphine and non-morphine groups across all measured time points. However, subsequent analysis of blood pressure revealed transient increases in systolic and diastolic values at 5 and 10 minutes post-intervention in the morphine group. These differences were not sustained at later intervals. Regression analysis identified a significant association between intrathecal morphine and lower systolic and diastolic blood pressure at 30 minutes post-intervention, consistent with findings from Joshi et al. (2015). [14], Lemoine et al. (2021) [7], and Ummenhofer et al. (2000) [17]. These findings are consistent with those reported by Reise and Van Aken (2011), who observed that neuraxial opioids can induce transient hemodynamic changes, particularly when administered concomitantly with local anaesthetics [15]. This observation emphasises the importance of meticulous monitoring during neuraxial opioid application [12]. Nevertheless, the findings of this study suggest that, while transient hemodynamic alterations occur, these are not sustained beyond the initial postoperative period. Consequently, prolonged monitoring beyond the RR does not appear to be necessary.
Furthermore, Zand et al. (2015) [13] emphasise that, when appropriately dosed, intrathecal morphine can maintain haemodynamic stability by reducing the requirement for systemic opioid administration, which often causes larger fluctuations in blood pressure and heart rate. The current findings, in conjunction with the observations of Zand et al. [13], confirm that intrathecal morphine does not lead to clinically relevant hemodynamic instability requiring prolonged postoperative monitoring beyond the RR.
Respiratory complications, including oxygen desaturation and the need for supplemental oxygen, were minimal and showed no significant differences between the groups. The mean oxygen saturation levels were comparable across both groups at all time points, corroborating previous studies that report a low incidence of respiratory compromise with intrathecal morphine at doses below 0.3 mg [19,23]. However, Koning et al. consider 2022 respiratory depression to be the most severe side effect of ITM administration [23]. This method of administration carries the risk of delayed respiratory depression [12]. Due to its pharmacological properties, intrathecally administered morphine has a long-lasting presence in the cerebrospinal fluid, which leads to a duration of action of up to 36 hours [17,19]. The incidence of respiratory depression after a dose of less than 1 mg of intrathecally administered morphine varies between 0.5 and 3.0% in studies with a total of 492 and 5705 patients, respectively [12,29,31,32]. This variation in incidence can be attributed to the heterogeneity in the definition of respiratory depression [33]. In a similar vein, Sultan et al. emphasised in 2011 that appropriate dosing and vigilant postoperative monitoring can effectively mitigate respiratory risks [19]. The findings of this study indicate the absence of any respiratory depressions, a phenomenon that may be attributable to the constraints imposed by the modest sample size and the relatively low incidence documented by Koning et al. in 2020. This finding is consistent with Mugabure Bujedo's conclusion that the risk of respiratory depression can be effectively mitigated through appropriate dosing and monitoring protocols [18].
Postoperative nausea and vomiting (PONV) were evaluated in both groups, and while no significant differences were observed in the incidence or timing of nausea and emesis, the use of anti-emetic medications, including dimenhydrinate and butylscopolamine, was similar. The studies by Deer et al. (2017), Prager et al. (2014) and Dhawan (2021) documented that nausea and vomiting can be considered possible side effects of morphine [34,35,36]. A study by Thay et al. also demonstrated an incidence of 11.2% for pruritus, as well as postoperative nausea and vomiting, in a group of 124 patients who received intrathecal morphine application during a caesarean section [37]. The aforementioned authors' description of the side effects of nausea and vomiting is not evident in this study; however, the results are consistent with those of Koning et al. from 2022 and Rathmell et al. from 2005, who emphasise the effectiveness of multimodal PONV prevention strategies in patients receiving neuraxial opioids [23,27]. The importance of effective PONV management in improving patient satisfaction and recovery outcomes is also emphasised by Joshi et al. [14].
The present study found no significant differences between the groups in terms of complications documented in discharge summaries, including vesicoureteral anastomotic insufficiency (paravasation), lymphoceles, and wound dehiscence. Zand et al. reported analogous findings regarding wound complications in 2015, emphasising that intrathecal morphine does not significantly increase the risk of surgical site issues [30]. The incidence of paravasation and lymphoceles in this study is consistent with previously published data, which emphasise that these complications are predominantly associated with surgical technique rather than analgesic modality [38,39]. The safety profile of intrathecal morphine is therefore supported, provided that appropriate monitoring protocols are implemented, as recommended by Joshi et al. (2015) [14]. The current findings are also in alignment with Stein et al. (1995), who discussed the manageable risk-benefit profile of intrathecal opioid administration in perioperative care [20].
The present study is subject to several limitations, which must be given due consideration. Firstly, the retrospective nature of the study design limits the ability to establish causality and increases the potential for selection bias. Additionally, the single-centre nature of the study implies limitations in terms of its generalisability to other institutions or patient populations. The absence of randomisation further reduces the strength of comparisons between groups, as confounding variables may not have been evenly distributed. While all patients underwent general anaesthesia, variations in anaesthesia protocols, including induction agents and intraoperative medications, were not standardised. The retrospective study design precluded meticulous adherence to the recovery room protocols. The retrospective study design precluded meticulous adherence to the recovery room protocols. It is important to acknowledge that limited measuring points were utilised in the analysis. This methodological decision inevitably introduces a certain degree of imprecision into the results.
The lack of documentation concerning preoperative home medications, which have the capacity to influence postoperative outcomes, introduces an unaccounted source of variability. In addition, the inconsistent documentation of precise operation times limits the evaluation of the impact of surgical duration on outcomes. Additionally, the documentation of urinary output side effects was inadequate, resulting in their exclusion from the statistical analysis. The reduced sample size and unequal distribution between the treatment and control groups have furthermore been demonstrated to reduce statistical power and limit the robustness of conclusions drawn. Moreover, the evaluation of pruritus, a prevalent side effect of intrathecal morphine, was impeded by the absence of systematic documentation in patient records[3]. These limitations underscore the necessity for prospective, multicentre, randomised controlled trials to validate these findings and furnish more robust evidence for clinical practice.
5. Conclusions
Intrathecal morphine, when administered concomitantly with GA, has been shown to significantly enhance postoperative pain management in patients undergoing prostatectomy. The present study demonstrates that ITM is associated with reduced pain intensity, lower postoperative analgesic consumption, and delayed time to the first request for analgesics without a significant increase in severe side effects. Specifically, patients receiving ITM reported lower NRS pain scores at rest and during movement in the recovery room and required fewer supplemental opioids, such as piritramide.
The occurrence of haemodynamic and respiratory complications was minimal and manageable, which is consistent with extant literature that highlights the safety of intrathecal morphine when administered at appropriate doses. The transient fluctuations in blood pressure and the absence of clinically significant respiratory depression further substantiate the safety profile of intrathecal morphine. Furthermore, the incidence of common side effects such as PONV did not differ significantly between the groups, indicating that intrathecal morphine does not exacerbate these outcomes when combined with multimodal management strategies, including preoperative antiemetic therapy.
The findings indicate that a dose of 0.3mg morphine, while effective, may exceed current guideline recommendations, which advocate for lower doses to minimise side effects. Future research should focus on optimising dosing strategies to balance efficacy and safety, and consequently, the duration of action necessitates further analysis. Despite the limitations of this retrospective study, including its single-centre design, lack of randomization, and unequal group sizes, the results provide a compelling argument for the inclusion of intrathecal morphine in multimodal analgesic protocols for prostatectomy.
The need for further research is evident, and the design of prospective, multicentre studies with standardised protocols is recommended to validate these findings, evaluate long-term outcomes, and refine dosing recommendations. The application of intrathecal morphine in clinical practice holds significant potential to enhance postoperative recovery, reduce opioid-related adverse effects, and improve patient satisfaction in major surgical procedures.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee University Witten / Herdecke (protocol code Number S-240/2024 at 3 October 2024.
Informed Consent Statement
Patient consent was waived for this study due to its retrospective nature and the anonymization of all patient data prior to analysis. The data were collected and processed in such a way that individual patients could no longer be identified, ensuring compliance with data protection regulations. This approach adheres to the stipulations outlined in the ethical approval obtained for the study. The hospitals involved in the study are obligated under §21 of the German Hospital Remuneration Act (Krankenhausentgeltgesetz) to transmit certain patient data, such as age, gender, postal code, diagnosis group (ICD-10), comorbidities, and other factors, to the Institute for the Hospital Remuneration System (InEK). This transmission suggests that patient consent for the use of these data in a de-identified manner has already been implicitly granted. Furthermore, the study maximized data security measures to minimize any risk of privacy breaches. The study protocol was reviewed and approved by the data protection officer of Holweide Hospital. It complies with the Declaration of Helsinki (World Medical Association, 2013).
Data Availability Statement
Should further elucidation be required to support the findings of this study, the corresponding author is available to provide the necessary data upon reasonable request.
Acknowledgments
The author wishes to express their gratitude to the Statistic Consultancy of the University of Witten Herdecke, with particular thanks to Dr. Sabrina Voß.
Conflicts of Interest
The authors declare no conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
| CSF | Cerebrospinal fluid |
| DVT | Deep Venous Thrombosis |
| EAU | European Association of Urology |
| GA | General Anaesthesia |
| GDPR | Union’s General Data Protection Regulation |
| ITM | Intrathecal Morphin |
| IMC | Intermediate Care Unit |
| ICU | Intensive Care Unit |
| Kg | Kilogram |
| Mdn | Median |
| Mg | Milligram |
| ml | Millilitres |
| NRS | Numeric Rating Scale |
| PONV | Postoperative nausea and vomiting |
| RR | Recovery Room |
Appendix A
Appendix A.1
| Piritramide dosis in the recovery room | |||||||
| Coefficients | b | SE | β | t | p | ||
| (Constant) | 1.975 | 2.173 | .909 | .365 | |||
| ITM | -.380 | .362 | -.091 | -1.050 | .296 | ||
| Age | -.018 | .023 | -.071 | -.791 | .430 | ||
| Weight | .017 | .011 | .139 | 1.487 | .139 | ||
| Propofol | -.003 | .003 | -.114 | -1.158 | .249 | ||
| Midazolam | -.004 | .005 | -.078 | -.916 | .361 | ||
| Thiopental | -.004 | .006 | -.059 | -.683 | .496 | ||
| Sufentanil | .262 | .150 | .160 | 1.745 | .083 | ||
| Piritramide | -.046 | .049 | -.082 | -.939 | .349 | ||
| Fentanyl | -.319 | .957 | -.029 | -.333 | .739 | ||
| Arterial Hypertony | -.572 | .304 | -.162 | -.1884 | .0.62 | ||
| Diabetes Mellitus | -.531 | .579 | -0.80 | -.917 | .361 | ||
| Hypothyroidism | -.134 | .569 | -.020 | -.235 | .814 | ||
| COPD | .756 | .768 | -.092 | .984 | .327 | ||
| Time after ITM | -1.197E-5 | .000 | -.024 | -.277 | .782 | ||
| Remarks: N = 144; R² = .137; corr. R² = .044; F(14, 129) = .466; p = .132 | |||||||
Appendix A.2
| Number of analgetica in the recovey room | ||||||
| Coefficients | b | SE | β | t | p | |
| (Constant) | 0.883 | .924 | .955 | .341 | ||
| ITM | 0.054 | .154 | .031 | .350 | .727 | |
| Age | -0.005 | .010 | -.047 | -.516 | .607 | |
| Weight | .008 | .005 | .158 | 1.661 | .099 | |
| Propofol | -.002 | .001 | -.177 | -1.782 | .077 | |
| Midazolam | .000 | .002 | -.007 | -.082 | .935 | |
| Thiopental | -.004 | .003 | -.133 | -1.527 | .129 | |
| Sufentanil | .015 | .064 | .021 | .232 | .817 | |
| Piritramide | -.028 | .021 | -.121 | -1.362 | .175 | |
| Fentanyl | -.498 | .407 | -.108 | -1.223 | .224 | |
| Arterial Hypertony | -.223 | .129 | -.150 | -1.728 | .086 | |
| Diabetes Mellitus | -.230 | .246 | -.082 | -.932 | .353 | |
| Hypothyroidism | -.097 | .242 | -.035 | -.399 | .690 | |
| COPD | -.059 | .327 | -.017 | -.182 | .856 | |
| Time after ITM | -1.242E-5 | .000 | -.058 | .676 | .500 | |
| Remarks: N = 144; R² = .117; corr. R² = .021; F(14, 129) = 1.223; p = .266 | ||||||
Appendix A.3
| Systole at 30min | |||||
| Coefficients | b | SE | β | t | p |
| (Constant) | 118.183 | 15.395 | 7.677 | <.001 | |
| ITM | -7.471 | 3.037 | -.187 | -2.460 | .015 |
| Age | .076 | .183 | .032 | 0.413 | .680 |
| Weight | -.097 | .081 | -.092 | -1.201 | .231 |
| Arterial Hypertony | 2.853 | 2.644 | .082 | 1.079 | .282 |
| Diabetes Mellitus | .710 | 4.338 | .013 | 0.164 | .870 |
| Akinor | .039 | .180 | .016 | 0.216 | .829 |
| Atropine | -48.827 | 22.771 | -.164 | -2.144 | .033 |
| Noradrenalin | -.258 | .968 | -.020 | -0.267 | .790 |
| Remarks: N = 178; R² = .067; corr. R² = .023; F(8, 169) = 1.51; p = .156 | |||||
Appendix A.4
| Diastole at 30min | |||||
| Coefficients | b | SE | β | t | p |
| (Constant) | 74.093 | 9.475 | 7.820 | <.001 | |
| ITM | -5.426 | 1.869 | -.218 | -2.903 | .004 |
| Age | -.096 | .112 | -.064 | -.854 | .395 |
| Weight | -.044 | .050 | -.067 | -.880 | .380 |
| Arterial Hypertony | 1.649 | 1.627 | .076 | 1.014 | .312 |
| Diabetes Mellitus | 2.641 | 2.670 | .075 | .989 | .324 |
| Akinor | -.106 | .110 | -.072 | -.960 | .339 |
| Atropine | -33.135 | 14.013 | -.178 | -2.365 | .019 |
| Noradrenalin | .435 | .596 | .054 | .730 | .466 |
| Remarks: N = 178; R² = .09; corr. R² = .047; F(8, 169) = 2.087; p = .039 | |||||
Appendix A.5
| Noradrenalin dosis | |||||
| Coefficients | b | SE | β | t | p |
| (Constant) | .706 | 1.205 | .86 | .559 | |
| ITM | .239 | .239 | .077 | .997 | .320 |
| Age | .003 | .014 | .014 | .175 | .862 |
| Weight | -.006 | .006 | -.071 | -.905 | .367 |
| Arterial Hypertony | .153 | .209 | .057 | .736 | .463 |
| Diabetes Mellitus | -.157 | .343 | -.036 | -.458 | .648 |
| Akinor | .005 | .014 | .027 | .349 | .727 |
| Atropine | -.978 | 1800 | -.042 | -.543 | .588 |
| Remarks: N = 179; R² = .019; corr. R² = -.022; F(7, 171) = .461; p = .861 | |||||
Appendix A.6
| Hospital Stay | |||||
| Coefficients | b | SE | β | t | p |
| (Constant) | 9,982 | 5.428 | 1.839 | .068 | |
| ITM | -1,743 | .952 | -.152 | -1.830 | .069 |
| Age | .008 | .057 | .012 | .146 | .884 |
| Weight | .040 | .023 | .142 | 1.731 | .086 |
| Arterial hypertension | -.676 | .794 | -.069 | -.852 | .396 |
| Diabetes Mellitus | 5.262 | 1.448 | .294 | 3.635 | <.001 |
| Noradrenalin | -.040 | .277 | -.011 | -.146 | .885 |
| First in RR after Surgery | .071 | .000 | .049 | .613 | .541 |
| NRS at rest (1-10) | .412 | .554 | .154 | .744 | .458 |
| NRS at movement (1-10) | -.629 | .484 | -.263 | -1.300 | .196 |
| Days until regular ward | -1.025 | .799 | -.105 | -1.282 | .202 |
| Remarks: N = 149; R² = .174; corr. R² = .114; F(10, 138) = 2.9; p = .002 | |||||
Appendix A.7
| Nausea in the recovery room | |||||
| Coefficients | b | SE | β | t | p |
| (Constant) | .225 | .223 | 1010.000 | .314 | |
| ITM | .027 | .041 | .051 | .649 | .517 |
| Age | -.002 | .002 | -.078 | -1034.000 | .303 |
| Weight | -.001 | .001 | -.040 | -.525 | .601 |
| Pain at rest RR (NRS 1–10) | .013 | .024 | .109 | .554 | .580 |
| Pain during movement RR(NRS 1–10) | -.009 | .022 | -.077 | -.398 | .691 |
| Time until first action at RR | .000 | .000 | .002 | .031 | .975 |
| Sufentanil dose | -.003 | .016 | -.015 | -.197 | .844 |
| Fentanyl dose | .101 | .105 | .074 | .957 | .340 |
| Diabetes mellitus | -.037 | .059 | -.049 | -.621 | .535 |
| Dexamethasone | -.001 | .005 | -.011 | -.137 | .892 |
| Emesis RR | .936 | .149 | .477 | 6.272 | <.001 |
| Remarks: N = 153; R² = .259; corr. R² = .202; F(11, 141) = 4.491; p < .001 | |||||
References
- Alenezi, B.; Alsubhi, M.H.; Jin, X.; He, G.; Wei, Q.; Ke, Y. Global Development on Causes, Epidemiology, Aetiology, and Risk Factors of Prostate Cancer: An Advanced Study. Highlights Med. Med. Sci. 2021, 17. [Google Scholar] [CrossRef]
- Mottet, N.; Cornford, P.; Briers, E.; Santis, M.D.; Gillessen, S.; Grummet, J.; Henry, A.M. EAU-EANM-ESTRO-ESUR-ISUP-SIOG GUIDELINES ON PROSTATE CANCER. 2023, 17–21, 55–61, 85.
- Groeben, C.; Koch, R.; Baunacke, M.; Flegar, L.; Borkowetz, A.; Thomas, C.; Huber, J. Entwicklung Der Operativen Uroonkologie in Deutschland – Vergleichende Analysen Aus Populationsbasierten DatenTrends in Uro-Oncological Surgery in Germany—Comparative Analyses from Population-Based Data. Urol. 2021, 60. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Autorino, R.; Kaouk, J.H.; Stolzenburg, J.-U.; Gill, I.S.; Mottrie, A.; Tewari, A.; Cadeddu, J.A. Current Status and Future Directions of Robotic Single-Site Surgery: A Systematic Review. Eur. Urol. 2013, 63, 266–280. [Google Scholar] [CrossRef]
- Ilic, D.; Djulbegovic, M.; Jung, J.H.; Hwang, E.C.; Zhou, Q.; Cleves, A.; Agoritsas, T.; Dahm, P. Prostate Cancer Screening with Prostate-Specific Antigen (PSA) Test: A Systematic Review and Meta-Analysis. BMJ 2018, 362, k3519. [Google Scholar] [CrossRef]
- Lemoine, A.; Witdouck, A.; Beloeil, H.; Bonnet, F. ; PROSPECT Working Group Of The European Society Of Regional Anaesthesia And Pain Therapy (ESRA) PROSPECT Guidelines Update for Evidence-Based Pain Management after Prostatectomy for Cancer. Anaesth. Crit. Care Pain Med. 2021, 40, 100922. [Google Scholar] [CrossRef]
- Wu, C.L.; Rowlingson, A.J.; Partin, A.W.; Kalish, M.A.; Courpas, G.E.; Walsh, P.C.; Fleisher, L.A. Correlation of Postoperative Pain to Quality of Recovery in the Immediate Postoperative Period. Reg. Anesth. Pain Med. 2005, 30, 516–522. [Google Scholar] [CrossRef]
- Baumann, F.; Schüle, K. Bewegungstherapie Und Sport Bei Krebs. Leitfaden Für Die Praxis; Deutscher Ärzteverlag, 2008.
- Wani, M.; Al-Mitwalli, A.; Mukherjee, S.; Nabi, G.; Somani, B.K.; Abbaraju, J.; Madaan, S. Venous Thromboembolism (VTE) in Post-Prostatectomy Patients: Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 3979. [Google Scholar] [CrossRef]
- Naghibi, K.; Saryazdi, H.; Kashefi, P.; Rohani, F. The Comparison of Spinal Anesthesia with General Anesthesia on the Postoperative Pain Scores and Analgesic Requirements after Elective Lower Abdominal Surgery: A Randomized, Double-Blinded Study. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2013, 18, 543–548. [Google Scholar]
- Gehling, M.; Tryba, T. Risks and Side-Effects of Intrathecal Morphine Combined with Spinal Anaesthesia: A Meta-Analysis. Anaesthesia 2009, 64. [Google Scholar] [CrossRef]
- Onodera, H.; Ida, M.; Naito, Y.; Kinomoto, A.; Kawaguchi, M. Respiratory Depression Following Cesarean Section with Single-Shot Spinal with 100 Μg Morphine. J. Anesth. 2023, 37, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Joshi, G.P.; Jaschinski, T.; Bonnet, F.; Kehlet, H. ; PROSPECT collaboration Optimal Pain Management for Radical Prostatectomy Surgery: What Is the Evidence? BMC Anesthesiol. 2015, 15, 159. [Google Scholar] [CrossRef] [PubMed]
- Freise, H.; Van Aken, H.K. Risks and Benefits of Thoracic Epidural Anaesthesia. Br. J. Anaesth. 2011, 107, 859–868. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; L. Erlbaum Associates: Hillsdale, N.J., 1988.
- Ummenhofer, W.C.; Arends, R.H.; Shen, D.D.; Bernards, C.M. Comparative Spinal Distribution and Clearance Kinetics of Intrathecally Administered Morphine, Fentanyl, Alfentanil, and Sufentanil. Anesthesiology 2000, 92, 739–753. [Google Scholar] [CrossRef]
- Mugabure Bujedo, B. A Clinical Approach to Neuraxial Morphine for the Treatment of Postoperative Pain. Pain Res. Treat. 2012, 2012, 612145. [Google Scholar] [CrossRef]
- Sultan, P.; Gutierrez, M.C.; Carvalho, B. Neuraxial Morphine and Respiratory Depression: Finding the Right Balance. Drugs 2011, 71, 1807–1819. [Google Scholar] [CrossRef]
- Stein, C.; Schäfer, M.; Hassan, A.H. Peripheral Opioid Receptors. Ann. Med. 1995, 27, 219–221. [Google Scholar] [CrossRef]
- De Gregori, S.; De Gregori, M.; Ranzani, G.N.; Allegri, M.; Minella, C.; Regazzi, M. Morphine Metabolism, Transport and Brain Disposition. Metab. Brain Dis. 2012, 27, 1–5. [Google Scholar] [CrossRef]
- Verscheijden, L.F.M.; Litjens, C.H.C.; Koenderink, J.B.; Mathijssen, R.H.J.; Verbeek, M.M.; de Wildt, S.N.; Russel, F.G.M. Physiologically Based Pharmacokinetic/Pharmacodynamic Model for the Prediction of Morphine Brain Disposition and Analgesia in Adults and Children. PLOS Comput. Biol. 2021, 17, e1008786. [Google Scholar] [CrossRef]
- Koning, M.V.; Reussien, E.; Vermeulen, B.A.N.; Zonneveld, S.; Westerman, E.M.; de Graaff, J.C.; Houweling, B.M. Serious Adverse Events after a Single Shot of Intrathecal Morphine: A Case Series and Systematic Review. Pain Res. Manag. 2022, 2022, 4567192. [Google Scholar] [CrossRef]
- Wittwer, E.; Kern, S.E. Role of Morphine’s Metabolites in Analgesia: Concepts and Controversies. AAPS J. 2006, 8, E348–E352. [Google Scholar] [CrossRef] [PubMed]
- Andrieu, G.; Roth, B.; Ousmane, L.; Castaner, M.; Petillot, P.; Vallet, B.; Villers, A.; Lebuffe, G. The Efficacy of Intrathecal Morphine With or Without Clonidine for Postoperative Analgesia After Radical Prostatectomy. Anesth. Analg. 2009, 108, 1954. [Google Scholar] [CrossRef] [PubMed]
- Kurzova, A.; Malek, J.; Klezl, P.; Hess, L.; Sliva, J. A Single Dose of Intrathecal Morphine Without Local Anesthetic Provides Long-Lasting Postoperative Analgesia After Radical Prostatectomy and Nephrectomy. J. Perianesth. Nurs. 2024, 39, 577–582. [Google Scholar] [CrossRef]
- Rathmell, J.P.; Lair, T.R.; Nauman, B. The Role of Intrathecal Drugs in the Treatment of Acute Pain. Anesth. Analg. 2005, 101. [Google Scholar] [CrossRef]
- Ozbek, H.; Deniz, M.N.; Erakgun, A.; Erhan, E. Comparison of 75 and 150 Μg Doses of Intrathecal Morphine for Postoperative Analgesia after Transurethral Resection of the Prostate under Spinal Anesthesia. J. Opioid Manag. 2013, 9, 415–420. [Google Scholar] [CrossRef]
- Meylan, N.; Elia, N.; Lysakowski, C.; Tramèr, M.R. Benefit and Risk of Intrathecal Morphine without Local Anaesthetic in Patients Undergoing Major Surgery: Meta-Analysis of Randomized Trials. Br. J. Anaesth. 2009, 102, 156–167. [Google Scholar] [CrossRef]
- Zand, F.; Amini, A.; Asadi, S.; Farbood, A. The Effect of Methylnaltrexone on the Side Effects of Intrathecal Morphine after Orthopedic Surgery under Spinal Anesthesia. Pain Pract. Off. J. World Inst. Pain 2015, 15, 348–354. [Google Scholar] [CrossRef]
- Koning, M.V.; Klimek, M.; Rijs, K.; Stolker, R.J.; Heesen, M.A. Intrathecal Hydrophilic Opioids for Abdominal Surgery: A Meta-Analysis, Meta-Regression, and Trial Sequential Analysis. Br. J. Anaesth. 2020, 125, 358–372. [Google Scholar] [CrossRef]
- Gwirtz, K.H.; Young, J.V.; Byers, R.S.; Alley, C.; Levin, K.; Walker, S.G.; Stoelting, R.K. The Safety and Efficacy of Intrathecal Opioid Analgesia for Acute Postoperative Pain: Seven Years’ Experience with 5969 Surgical Patients at Indiana University Hospital. Anesth. Analg. 1999, 88, 599–604. [Google Scholar] [CrossRef]
- Ko, S.; Goldstein, D.H.; VanDenKerkhof, E.G. Definitions of “Respiratory Depression” with Intrathecal Morphine Postoperative Analgesia: A Review of the Literature. Can. J. Anaesth. 2003, 50, 679–688. [Google Scholar] [CrossRef]
- Deer, T.R.; Pope, J.E.; Hayek, S.M.; Lamer, T.J.; Veizi, I.E.; Erdek, M.; Wallace, M.S.; Grider, J.S.; Levy, R.M.; Prager, J.; et al. The Polyanalgesic Consensus Conference (PACC): Recommendations for Intrathecal Drug Delivery: Guidance for Improving Safety and Mitigating Risks. Neuromodulation J. Int. Neuromodulation Soc. 2017, 20, 155–176. [Google Scholar] [CrossRef] [PubMed]
- Prager, J.; Deer, T.; Levy, R.; Bruel, B.; Buchser, E.; Caraway, D.; Cousins, M.; Jacobs, M.; McGlothlen, G.; Rauck, R.; et al. Best Practices for Intrathecal Drug Delivery for Pain. Neuromodulation J. Int. Neuromodulation Soc. 2014, 17, 354–372. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, R.; Daubenspeck, D.; Wroblewski, K.E.; Harrison, J.-H.; McCrorey, M.; Balkhy, H.H.; Chaney, M.A. Intrathecal Morphine for Analgesia in Minimally Invasive Cardiac Surgery: A Randomized, Placebo-Controlled, Double-Blinded Clinical Trial. Anesthesiology 2021, 135, 864–876. [Google Scholar] [CrossRef] [PubMed]
- Thay, Y.; Goh, Q.; Han, R.; Sultana, R.; Sng, B. Pruritus and Postoperative Nausea and Vomiting after Intrathecal Morphine in Spinal Anaesthesia for Caesarean Section: Prospective Cohort Study. Proc. Singap. Healthc. 2018, 27, 201010581876034. [Google Scholar] [CrossRef]
- Hauri, D.; Jäger, P. Checkliste Urologie, 4th ed.; Thieme Verlag: Stuttgart, 2000.
- Gardner, T.A.; Bissonette, E.A.; Petroni, G.R.; McClain, R.; Sokoloff, M.H.; Theodorescu, D. Surgical and Postoperative Factors Affecting Length of Hospital Stay after Radical Prostatectomy. Cancer 2000, 89, 424–430. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



