Submitted:
18 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
Drug discovery has undergone a remarkable transformation over the centuries, evolving from empirical observations and natural product isolation to high-throughput screening and molecular design. This review provides a historical overview of key milestones in drug development, tracing the journey from traditional practices to modern computational techniques. Emphasizing the increasing role of Artificial Intelligence (AI), the review explores how machine learning, deep learning, and generative algorithms are revolutionizing the field of drug discovery and development. AI's ability to analyze complex datasets, predict drug-target interactions, and optimize lead compounds has accelerated the drug discovery pipeline and personalized medicine and drug repurposing efforts. While the advantages of AI include cost-effectiveness, enhanced efficiency, and expanded chemical space exploration, its limitations, such as data dependency and interpretability, are also discussed. This review aims to contextualize the evolution of drug discovery while highlighting AI's transformative potential in addressing contemporary challenges in healthcare.
Keywords:
Artificial intelligence (AI)
; Pharmaceutical industry
; Drug development
; Machine Learning (ML)
1. Introduction
One might define a drug as a molecule or a material used to prevent, treat, diagnose, or relieve the symptoms of a disease or natural condition [1]. The usage of drugs can be traced back to ancient times when humans relied primarily on herbs to treat various diseases. Written records of medicinal drugs have been found in multiple ancient cultures, including those of Greece, Egypt, India, and China. During the medieval period, both Arabic and European nations explored the study of drugs [2].
The Renaissance marked the beginning of scientific inquiry into medicine. Still, it was not until the 19th century that medicine became truly scientific with the discovery and development of antiseptics, vaccines, and anesthetics [3]. Drugs have also been used for recreational and ceremonial purposes for thousands of years, whether naturally occurring, like cannabis and opium, or synthetically created, such as LSD and ecstasy. Today, both medicinal and recreational drugs are significant global industries [4].
The drug development process has a rich history that spans millions of years. It began with using natural products and evolved into a complex, multistage process involving a range of scientific disciplines. However, the first real application of the drug development and discovery process can be traced back to the 19th century, when most nations started relying on medicinal chemists’ knowledge to develop potential drugs [5].
As the abstract mentions, drug discovery and development is lengthy and costly. Therefore, there is a need to create more sophisticated tools to assist in the process. To answer this problem, scientists have resorted to tools like machine learning and artificial intelligence to enhance the drug development process [6]. Considered a subfield of artificial intelligence (AI) and computer science, machine learning employs data and algorithms to allow artificial intelligence to replicate human learning, therefore progressively increasing its accuracy [7].
Integrating AI into the drug discovery and development process marks a new era in drug discovery, offering unprecedented opportunities to enhance efficiency, reduce costs, and improve the success rates of new therapies.
In addition, AI in drug discovery can help address global health challenges, including finding treatments for rare diseases and diseases prevalent in low-resource settings. It also opens up new possibilities for faster and more inclusive solutions to medical challenges.
By leveraging AI, the pharmaceutical industry can move toward more intelligent, data-driven drug discovery, ultimately improving patient outcomes and making treatments more accessible. Therefore, this brief review provides the historical context of drug development and examines how AI is transforming the drug development industry.
2. A Brief History of Drug Discovery and Development
2.1. Early Stage of Drug Discovery
Drug discovery and development can be traced back to ancient times when humans used plants, animal organs, or minerals to treat their fellow’s ailments. Back then, drug discovery was a trial-and-error process that included assessing how a patient reacted after injecting the drug [8,9,10]. While these folk medicines likely developed independently in various civilizations, there are striking similarities, such as using identical herbs to treat similar ailments. This shared knowledge is probably the result of ancient traders, who may have played a key role in spreading medical knowledge during their journeys [11].
The Middle Ages saw a rise in uncommon diseases in many parts of Europe, and some of the new diseases included but were not limited to leprosy, which is a chronic and infectious medical condition caused by a bacterium called Mycobacterium leprae [12]. Leprosy affects the skin, making it patchy and causing it to lose pigmentation.
Smallpox is also one of the ancient diseases that existed for roughly 3,000 years, killing millions of people in the process. Smallpox was caused by the variola virus and was eradicated in the 1980s [13].
In addition, tuberculosis (TB) was also discovered in ancient Europe. A bacterial infection caused by Mycobacterium tuberculosis is transmitted through the air [14]. TB settles in the lungs and grows due to the mode of infection, which occurs when an individual breathes.
The bacterium can travel through the bloodstream to other internal organs, including the brain, spine, and kidneys, from the lungs [15].
Scabies is also one of the diseases discovered in the early years of civilization. It is caused by tiny parasitic mites called Sarcoptes scabiei [16], which burrow into the host’s skin and lay eggs, resulting in itchy and sore skin. This can ultimately lead to severe disease and kidney-related issues [17].
Bubonic plague is one of the few zoonotic diseases (diseases transmitted between animals and humans) discovered during early civilization. The disease is caused by a bacterium called Yersinia pestis and is transmitted by fleas that infest rodents and other animals [18]. The condition manifests as enlarged lymph nodes, which may reach the size of chicken eggs and are located in the groin, armpit, or neck. Additional symptoms include fever, chills, headache, fatigue, and myalgia [19].
The aforementioned diseases resulted in the deaths of many European citizens, and it was this tragedy that led to a shift in the way drugs were discovered and developed. This change established scientific thought as the basis for drug discovery and development [20].
2.2. Keynote Discoveries in Drug Development
Numerous keynote discoveries have marked the drug discovery process since the early 18th century. Some may have been recorded, but most may not have been for various reasons. This article briefly overviews key discoveries in drug discovery and development.
As mentioned earlier, leprosy was first identified in the early millennium period. During the Middle Ages, the Norwegian scientist Gerhard Armauer Hansen discovered that it was caused by Mycobacterium leprae [21]. His research enabled scientists to thoroughly understand the disease’s transmission mechanisms, allowing them to develop drugs that could potentially treat leprosy [22].
To find a cure for leprosy, a medicine called dapsone was developed. However, the bacterium that causes leprosy developed resistance to the medicine, leading to further investigation. In 1935, Daniel Bovet and his colleagues at the Pasteur Institute used sulfanilamide (a synthetic antibiotic used to treat bacterial infections) as a chemotherapeutic agent for treating bacterial infections [23]. However, sulfanilamide was first synthesized in 1908 by an Austrian chemist called Paul Josef Jakob Gelmo [24].
Ernest Fourneau of France and Gladwin Buttle independently discovered that dapsone could also be used for chemotherapeutic purposes that same year [25], but it was first discovered in 1908 by Emil Fromm and J. Wittmann, chemists at the University of Freiburg [26].
Smallpox is believed to have existed for more than 3,000 years, and it was such a brutal disease that killed 3 out of every 10 people who had it [27]. The initial treatment for smallpox was inoculation. However, in 1796, Edward Jenner, a British physician and scientist, successfully discovered and developed the smallpox vaccine. Following this discovery, vaccines began to be used to combat most infectious diseases [13,29].
As of 2021, brincidofovir (TEMBEXA) was approved for treating smallpox because it showed promising results in halting the spread of the smallpox virus and alleviating symptoms in animals infected with similar illnesses.
Finding the right treatment for tuberculosis has proven to be quite a challenge in modern times. People often relied on plant-based concoctions, dietary interventions, and climatic prescriptions [13], yet all these approaches proved futile as individuals continued to die regardless. In the early 1930s, however, an American scientist named Selman Waksman identified Streptomycin (SM), the first aminoglycoside antibiotic found to treat TB [31].
Streptomycin is currently used as an integral component of the multi-drug regimen for TB of the lungs. In the quest to find a rapid cure for tuberculosis, the para-amino salt of salicylic acid (PAS) was produced by Jorgen Lehman, a Swedish scientist, and a combination of SM and PAS has been found to be quite effective in the treatment of clinical tuberculosis [12]. Today, the general treatment of tuberculosis is an intensive two-month course of therapy that includes the following drugs: isoniazid, rifampicin (or Rifampin), pyrazinamide, and ethambutol [34].
One antibiotic that should be used as a first line of defense against active Mycobacterium tuberculosis (TB) infection is isoniazid (INH). INH has played a crucial role in tuberculosis treatment plans for many years [13].
Rifampin is an antibiotic that belongs to the rifamycin family. To put it simply, it inhibits bacterial development. This antibiotic can only treat bacterial illnesses. Viruses (like the flu or the common cold) are immune to it. Antibiotics lose their efficacy against subsequent infections when used for unnecessary purposes [13].
Pyrazinamide is an antibiotic used with other medications to treat tuberculosis (TB). It works by stopping the growth of bacteria [35]. This antibiotic treats only bacterial infections and does not work for viral infections (such as the common cold or flu).
Ethambutol is a bacteriostatic drug that inhibits cell wall synthesis and is used to manage and treat tuberculosis (TB). The mechanism of action, dosing considerations, pharmacokinetics, adverse event profiles, contraindications, boxed warnings, and monitoring strategies are highlighted within a multi-drug treatment [36].
In the late 1700s, another British physician named William Withering extracted digitalis from foxglove. It was discovered that digitalis had the potential to cure or treat dropsy, a condition in which excess fluid accumulates in the soft tissues of the heart, resulting in heart failure [37].
In the mid-1700s, another British physician and scientist named John Hunter discovered bone remodeling. After studying the repair and regeneration of bone marrow, he also examined the regeneration of bone cartilage and the repair of tendons. This discovery led to the development of numerous new surgical procedures; he also provided detailed anatomical descriptions [38].
In 1786, one of the Scottish physicians, James Lind, discovered that scurvy can be treated by supplementing the diet with citrus fruits. Scurvy manifests as a sickness when the body does not get enough vitamin C (ascorbic acid) from food and this affects the production of collagen which is a protein that aids in maintaining the skin, blood vessels, bones, and cartilage and its production requires vitamin C. Lind’s discovery concluded that scurvy can be treated by supplementing the diet with citrus fruits, and this study was one of the first to be conducted under very controlled clinical conditions. It was after this study that clinical experiments began to be conducted to test new medicines [39].
2.3. Evolution of Pharmaceutical Practices
While immense work was done on drug discovery from the 1700s to the late 1800s, the 1900s saw a boom in drug discovery based solely on systematic research. This drug discovery era included the discovery of drugs such as aspirin, extracted from the bark of a willow tree and used to treat fever [45]. Alexander Fleming found that penicillium mold was effective against Staphylococcus germs (Fleming, 1952) [45]. Ten years later, Ernst Chain and Howard Florey rediscovered this fact, and their work led to the large-scale production of penicillin [46].
As mentioned, most drugs utilized before the 19th century were herbs or extracts from botanical species. However, the 19th century saw an increase in the use of synthetic drugs produced using chemical methods. Most drugs were used for therapeutic purposes rather than completely curing diseases.
Screening natural materials and extracting their active components for illness treatment became the primary focus of drug development activities in the early 1930s [47]. Most of the time, these active components are chemical mimics of substances found in nature, known as new chemical entities (NCEs), which undergo rigorous testing to confirm their safety, potency, and efficacy.
By the late 1970s, cellular and molecular biology advancements improved DNA recombination products, marking the birth of the biotechnology industry [48,49,50]. The pharmaceutical industry, combined with breakthroughs in gene therapy, an understanding of pathological processes, and insights from the Human Genome Project, has opened numerous opportunities for creating drugs that specifically target the root causes of diseases.
3. Conventional Drug Discovery and Development Process
Conventional Drug Discovery and Development (DDD) is described as an important yet complex process for researching and developing new therapeutics. This process has led to novel cures for some of the world’s most prevalent diseases [51]. However, the drug discovery and development process remain lengthy, costly, and challenging; it involves five main stages.
- The pre-discovery stage entails conducting basic research to understand the mechanisms that result in the occurrence of diseases while also identifying possible targets, such as proteins. It is the stage at which scientists conduct basic research to understand the disease and formulate an appropriate target molecule [52].
- The drug discovery stage is the most important of all the stages, as it entails researching possible drug molecules (chemical or biological) that may have the potential to cure the investigated disease or at least alleviate the symptoms [53]. This stage is crucial because it allows for the discovery of target and lead molecules, followed by the validation and synthesis of drug candidates. The ultimate stage of the phase is drug development [54].
- The preclinical development stage entails studying the mode of action of drug candidates and researching the potential toxicity of the developed drugs; that is, researchers gather crucial data on medication safety, feasibility, and repeated testing—usually in laboratory animals—during this stage, which precedes clinical trials (testing in humans) [55].
- The clinical stage involves conducting the study by testing the safety of the developed drugs in humans. If the tests prove successful, the study is expanded to include many more participants to determine the drug’s effectiveness when consumed by numerous people with various traits, such as body weight, and so on [5].
- The reviewing, approval, and post-market monitoring stage entails the approval or disapproval of the developed drug, including conducting surveillance to confirm the efficacy and safety of pharmaceutical products and to detect the occurrence of diseases caused by adverse reactions [56].
Figure 2 below summarizes the drug discovery and development value chain and depicts the various stages involved in the conventional drug discovery and development process. Stage one is the drug pre-discovery stage and entails screening a large library of available molecules to test their ability to modify the target, and molecules that pass the screening phase are taken to stage two of the process which entails structure confirmation and synthesis of the molecules. Stage three is the most crucial stage as it entails modification of the synthesized lead molecules, and it is from this group of molecules that potential drug molecules are selected and taken to stage 4 of the process. The fourth stage involves in vivo analyses of the potential drug molecules to test their pharmacokinetics and toxicity and successful drug candidates will then be taken for clinical studies [53].
4. Integration of AI in Drug Development
As previously mentioned, the drug development process is quite lengthy, tedious, and, most importantly, costly. The end-to-end DDD process takes approximately 10 to 15 years and costs USD 2 billion to produce one successful drug molecule [57,58,59]. Hence, there is a need for innovative approaches to accelerate and streamline drug discovery. Luu and his colleagues [60] describe drug design and development as discovering novel medicinal substances by integrating computational, experimental, clinical, and translational models [61].
One way to streamline and accelerate drug discovery is by using artificial intelligence, a computational process that combines computer science and mathematics. The program utilizes large datasets to enable problem-solving. The pharmaceutical industry has increasingly investigated the role of artificial intelligence (AI) and other innovative technologies to assist in the accelerated discovery of effective treatment therapies [62].
4.1. AI Technologies and Their Applications
One solution for efficient drug development is repurposing or reoptimizing existing drugs. Artificial intelligence (AI) and generative machine learning (GML) can expedite drug discovery, ensuring the successful development of new drugs with significantly reduced time, costs, and failure rates. The section below discusses some parameters of AI and GML used in drug discovery and development.
- (i)
- Machine learning (ML) is a branch of AI that enables systems to learn from provided data and improve their performance based on that data without requiring additional programming [63]. ML’s application in drug discovery involves identifying potential drug candidates by predicting ligand-receptor interactions. ML also has the potential to predict ADMET (Absorption, Distribution, Metabolism, Excretion, and Toxicity) conditions, which are pharmacokinetic parameters that affect a drug’s safety, efficacy, and clinical success. These parameters help avoid late-stage drug failures by flagging poor ADMET conditions early [64].
- (ii)
- Deep learning (DL) is a branch of machine learning that uses artificial neural networks to teach computers to perform tasks that humans can do [65]. One major application of DL in drug development is its ability to generate novel drug candidates with desired properties. Additionally, DL can analyze large datasets from imaging and genomic data related to drug efficacy and safety [6].
- (iii)
- Reinforcement learning is a branch of machine learning that teaches computer software to make optimal decisions. DL’s application in drug discovery includes predicting synthetic pathways for synthesizing new molecules and iteratively modifying compounds to improve their efficacy or reduce their toxicity [66].
- (iv)
- Generative models are machine-learning models that design new molecules with properties and constraints similar to those of the molecules used to train the models. Their advantage lies in expanding the molecule bank by creating novel molecules; they also have the potential to tailor molecules for specific therapeutic agents [67].
- (v)
- Bioinformatics is a branch of molecular biology that extensively analyzes biological data using various computational tools to manage and interpret it. This discipline provides information such as DNA and amino acid sequences and annotations about those sequences [61].
- (vi)
- Cheminformatics is a field focused on solving chemical problems using computers. It involves tasks such as coding chemical structures, modeling properties, and developing databases [68].
- (vii)
- Molecular descriptors are quantitative measures of molecular properties, such as molecular weight, geometry, and polarity. Their advantage is that they simplify complicated molecular structures into numerical values, enabling model training. They also allow for determining the bioactivity of designed molecules [69].
- (viii)
- Molecular fingerprints (e.g., chemical fingerprints and pharmacophore fingerprints) are techniques that describe a molecule’s structure by converting it into bit strings. They aid in drug development by facilitating similarity-based searches of molecules, and they are also useful for the virtual screening and clustering of molecules with similar activity profiles [70].
- (ix)
- Molecular docking scores are computer-generated estimates of how strong the binding affinity of a small drug molecule to the target molecule is. The score is derived from computer simulations and often guides prioritizing molecules with high binding affinities [71]. For instance, Pang and Kozikowski successfully utilized computer-based molecular docking to predict through rigid docking, the bound pose of huperzine A, [72] thereby dramatically reducing the time needed to conduct molecular docking experimentally. Computer-based molecular docking was also used successfully in the identification of common chemoresistance-associated genes that impact cancer survival [73].
- (x)
- Drug screening (also known as toxicity test) is a process used to determine the presence of drugs or chemicals in a person’s body. It can be used to identify illegal drugs, monitor drug use, or assess the effects of an overdose. Various AI parameters such as molecular descriptors and dataset parameters have been utilized during drug screening.
Some of them include molecular descriptors (e.g., physicochemical descriptors properties, structural descriptors, and pharmacophore features) which are numerical values that represent the chemical properties of a molecule. These descriptors predict a molecule’s properties, classify chemical structures, and understand how molecules interact [74].
Dataset descriptors are also used during drug screening. They are modifiable fields that can be added to a dataset worksheet. Their advantage is that they can replace values in calculations, allowing users to make changes readily. They also improve data quality, resulting in robust model training [75].
- (xi)
- Fragmentation-Based Drug Discovery (FBDD) is rapidly progressing as another option for innovative and efficient early-stage de novo drug discovery [76,77]. “The main goal of de novo [drug discovery] is to generate chemically sound and original structures predicted to have desired physicochemical and biological properties” [78].
FBDD seeks to build drug-like molecules from pieces of other molecules known as fragments [79].
Due to the small size of the fragments, a molecule can be created to bind to multiple targets on the therapeutic site by leveraging each fragment’s ability to bind to a different site on the target [67,80,81].
Fragment-based techniques provide a creative method of identifying new molecules with higher binding affinity and improved therapeutic properties [82]. The FBDD approach can generate new molecules from a small dataset.
4.2. Advantages of AI in Drug Discovery
Artificial intelligence has opened a window of opportunity for accelerated drug design and development. This section briefly discusses the opportunities that artificial intelligence offers for drug discovery.
Accelerated drug discovery: AI has the potential to accelerate drug discovery by analyzing a large amount of data. This would enable scientists to identify drugs that may cure new diseases and help reduce the time spent on experimental trials [83].
Improved drug design accuracy: AI has the potential to analyze data more accurately and efficiently than traditional methods, such as the trial-and-error experimentation process previously used in drug development. It also aids in prediction reliability by utilizing high-dimensional data and advanced algorithms [79].
Broad application ability: AI can be applied in various fields, including small molecule design, biologics, and therapeutics. It can rapidly process data, enabling researchers to make informed decisions during lead optimization [84].
Integration of multimodal data and expansion of the chemical space: AI has the potential to combine chemical, biological, and clinical data to create holistic models for drug discovery and uncover novel lead compounds [85].
Artificial intelligence is also pivotal in gene editing, as it is widely used to develop gene therapies. One major contribution of AI to drug development is its cost-effectiveness, which reduces resource expenditure by prioritizing promising candidates and minimizing experimental failures [86].
4.3. Challenges of AI in Drug Discovery
One of the major challenges with AI-assisted drug discovery models is that they require a large, labeled training dataset of existing drugs (molecules) from which to learn to generate a new set of molecules based on the input molecules [87]. Unfortunately, this is not always readily available in drug discovery.
While numerous studies have demonstrated the application of generative machine learning in drug discovery, all have relied on a large input (training) dataset of molecules. These models have generally used a complete, unfiltered, publicly available drug database containing hundreds of thousands of molecules [88,89] as their input dataset. Arguably, this approach is ineffective for targeted or condition-specific drug discovery, which typically involves a relatively small dataset.
Another limitation of AI is its inability to fully account for the complexity of biological systems, leading to potential prediction inaccuracies. Most AI models are ‘black boxes’; thus, it is challenging to understand how these models make decisions [90]. One major challenge is that regulatory agencies require robust validation and clear evidence for AI-predicted drug candidates, which can be time-consuming. Therefore, researchers utilizing AI for drug development must verify the information gathered using AI-related tools [91].
4.3. Case Studies
As of today, Insilico Medicine, a biotechnology company based in Hong Kong and New York, is one of the few companies that have taken an AI-generated drug to the clinical trials phase. The company has successfully developed a drug called INS018-055, a small-molecule inhibitor that shows promising signs for treating idiopathic pulmonary fibrosis, a chronic pulmonary disease affecting more than 5 million people worldwide [92].
Other pharmaceutical companies actively using AI to discover new drugs are Exscientia and Sumitomo Dainippon Pharma. The company successfully designed and developed DSP-1181, a drug with the potential to treat obsessive-compulsive disorder, which causes people to experience repeated unwanted thoughts [93].
The drug (DSP-1181) is one of the few AI-generated drugs that have reached clinical trials, and the process took less than 12 months, significantly faster than traditional methods.
Atomwise partnered with IBM Watson to develop new active antibiotics against antibiotic-resistant bacteria. AI was utilized to screen billions of compounds, focusing on those with favorable docking properties [94]. This process identified and validated several lead compounds for antibacterial activity.
AI also has the potential to be used in vaccine development, and DeepMind’s AlphaFold has explored this field by predicting protein structures to assist in vaccine and therapeutic design. AlphaFold successfully predicted 3D protein structures with unprecedented accuracy, and this approach has accelerated the understanding of viral mechanisms and immune responses [95].
This phenomenal progress showcased by various pharmaceutical companies is a testament to the fact that artificial intelligence is the future of drug development. It is believed that utilizing AI-powered tools could catalyze the creation of new pharmaceutical drugs within the next decade.
4.4. Comparison Between AI-Enhanced Drug Discovery and Traditional Drug Discovery
As of today, researchers classify drug discovery into two components, traditional and AI-enhanced drug discovery, with the former being based solely on trial and error (through a range of scientific experiments) to identify potential drug candidates, while the latter uses artificial intelligence (AI) to analyze data and identify new potential drug candidates. AI-enhanced drug discovery accelerates drug development, reduces costs, and increases efficiency compared to traditional methods. However, traditional approaches remain essential for the validation and regulatory approval of new drug leads. Therefore, combining both methods offers the best results for modern drug development. Table 1 gives a brief comparison of AI-enhanced vs traditional drug discovery [96,97,98].
5. Conclusion
Progress in drug discovery can be traced as far back as the implementation of civilization by the human species. Human beings use herbs, certain animal organs, and some minerals for the treatment of various ailments. While the process has faced many challenges from the very beginning, there is reason to believe that the integration of artificial intelligence and other machine learning tools in drug development has the potential to change this tedious field by accelerating the entire drug discovery process—from initial discovery to post-market surveillance. By harnessing the power of AI, pharmaceutical companies can develop new drugs more quickly and efficiently while reducing costs and improving patient outcomes. As AI technology continues to advance, its role in drug development is expected to grow, driving further innovations in the field of medicine.
Acknowledgments
The authors thank the University of Johannesburg for its financial support.
References
- Ritter, J. M., MacEwan, D., Flower, R., Robinson, E., Henderson, G., Fullerton, J., Loke, Y. K., Rang and Dale’s pharmacology, 10th ed, London New York Oxford, 2024.
- Dias D. A., Urban, S., Roessner, U., Metabolites, 2012, 2(2), 303-336.
- Paterson, G., R., Neilson, J. B., Roland, C. G., Canadian Medical Association Journal, 1982, 127 (10), 948.
- Crocq, M. A., Dialogues in Clinical Neuroscience, 2007, 9(4), 355-61.
- Atanasov, A. G., Waltenberger, B., Pferschy-Wenzig, E. M., Linder, T., Wawrosch, C., Uhrin, P., Temml, V., Wang, L., Schwaiger, S., Heiss, E. H., Rollinger, J. M., Schuster, D., Breuss, J. M., Bochkov. V., Mihovilovic, M. D., Kopp, B., Bauer, R., Dirsch, V. M., Stuppner, H., Advanced Biotechnology, 2015, 33(8), 1582-1614.
- Paul, D., Sanap, G., Shenoy, S., Kalyane, D., Kalia, K., Tekade, R. K., Drug Discovery Today, 2021, 26(1), 80-93.
- Matt, C., What is Machine Learning? Definition, Types, Tools & More, Accessed 23 September 2024, @11: 00 am.
- Kinghorn, A.D., Pan, L., Fletcher, J.N., Chai, H., Journal of Natural Products, 2011,74,1539–1555.
- Singh, S., Kumar, R., Payra, S., Singh, S. K., Cureus, 2023, 15(8), e44359.
- Gad, H. A., El-Ahmady, S. H., Abou-Shoer, M. I., Al-Azizi, M.M., Phytochemical Analysis, 2013, 24(1),1–24.
- Noohi, M., Inavolu, S.S., Sujant, M., Springer Nature, 2022, 65(3), 399–411.
- Underwood, E., Ashworth, R., Philip, R., Robert, G., Guthrie, Douglas, J., Thomson, W.
- Woodruff, H. B., Selman, A., Waksman, Applied and Environmental Microbiology, 2014, 80 (1), 2-8.
- Riedel, S., Proceedings (Baylor University, Medical Center), Vol. (18), 1, 2005, 21–25.
- Kirian, M., “Notifiable disease”, Encyclopedia Britannica, 21 June 2024, https://www.britannica.com/science/notifiable-disease. Accessed 6 August 2024.
- Serrano-Coll, H., Cardona-Castro, N., Journal of Wound Care. Vol 31 (6), 2022, S32–S40.
- Gordon, S. V., Parish, T., Microbiology, 164 (4), 2018, 437–439.
- Bates, B., Bargaining for Life, A Social History for Tuberculosis, 1876-1938. Philadelphia: University of Pennsylvania Press, 1992.
- Arlian, L., Annual Review of Entomology, 1989, 34, 139–61.
- McMichael, A.J., BMC Biology,2010, 8(108), 1-3.
- Murray R. L., Crane, J. S., Scabies. StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544306/.
- Steven, L., Percival, D., Williams, W., Microbiology of waterborne diseases: microbiological aspects and risks, 2nd edition, Academic Press, Boston, Massachusetts, London (England), 2014.
- Santacroce, L., Del Prete, R., Charitos, I. A., Bottalico L., Le Infezioni in Medicina, 2021, 29 (4), 623-632.
- Christensen, S. B., Molecules, 2021, 7:26(19), 6057.
- Gelmo, P., Journal of Practical Chemistry, 1908, 77, 369-382.
- Bennett, B. H., Parker, D. L., Robson, M., Public Health Reports, 2008, 123(2), 198-205.
- Barr, J., Journal of the History of Medicine and Allied Sciences, 2011, 66(4), 425-467.
- Pai, V.V., Rao, P.N., Agarwal, A.K., Darlong, J.,Kar, H.K., Narang, T.,Phiske, M.M., Jayashree, P.K., Reddy, S.A., Sarah, N., Chugh, R., Sunkara, G., Pathak, H., Borde, P.P., Kota, J., Modali, S., Indian Journal of Leprosy, 2023, 95, 293-297.
- Fenner, F., Henderson, D. A., Arita, I., Ježek, Z., Ladnyi, I. D., Smallpox and its eradication. History of International Public Health, Geneva, World Health Organization,1988, 6, 209–44.
- Wilson, P. K., “William Withering”. Encyclopedia Britannica, 22 April 2024, https://www.britannica.com/biography/William-Withering. Accessed 6 August 2024.
- Granupas, European Medicines Agency, 2018, Accessed: 15/08/2024 at 3:25 pm.
- Sterling, T. R., Villarino, M. E., Borisov, A. S., Shang, N., Gordin, F., Bliven-Sizemore, E., The New England Journal of Medicine, 2011, 365 (23), 2155–66.
- National Center for Biotechnology Information, Retrieved September 24, 2024, from https://pubchem.ncbi.nlm.nih.gov/compound/Pyrazinamide.
- Lee, N., Patel, P., Nguyen, H., In: StatPearls [Internet], StatPearls Publishing, 2024, Available from: https://www.ncbi.nlm.nih.gov/books/NBK559050/.
- Tröhler, U., Journal of the Royal Society of Medicine, 2007, 100(3),155-6.
- Winters, William L. “Cardiology”. Encyclopedia Britannica, 26 Apr. 2019, https://www.britannica.com/science/cardiology. Accessed 23 September 2024.
- Evans, C. H., Journal of Orthopedic Research, 2007, 25(4), 556-60.
- Carpenter K. J., Annals of Nutrition and Metabolism, 2012, 61(3), 259-64.
- Sandhu, G. K., Journal of Global Infectious Diseases, 2011, 3 (2),143–50.
- O’Connor, C., Patel, P., Brady, M. F., Isoniazid. In: StatPearls [Internet], StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557617/.
- Flemming, A., British Medical Journal, 1952, 2(4778), 269-273.
- Maclagan, T., The Journal of Rheumatology, 1876, 1, 342–4.
- Flemming, A., British Journal of Experimental Pathology, 1929, 10, 226–36.
- American Chemical Society, Discovery and Development of penicillin, http://www.acs.org/content/acs/en/education/whatischemistry/landmarks/flemingpenicillin.html (accessed: 6 August 2024).
- Mushtaq, S, Abbasi B, H., Uzair, B., Abbasi, R., International Online Journal for Advances in Sciences, 2018, 17, 420-425.
- Loban, P.E., and Kaiser, A.D., Journal of Molecular Biology, 1973, 78, 453–471.
- Bolivar, F., Rodriguez, R.L., Greene, P.J., Betlach, M.C., Heyneke, H.L., Boyer, H.W., Gene, 1977, 2, 95–113.
- Novick, R.P., Clowes, R.C., Cohen, S.N., Curtiss, R., Datta, N., and Falkow, S., Bacteriological Reviews, 1976, 40, 168.
- Sikora, S., Hurley, B., and Tharakan, A. G., “Intelligent drug discovery: Powered by AI,” 2019.
- Mohs, R.C., Greig, N.H., Alzheimer and Dementia Journals, 2017, 11;3(4), 651-657.
- Wouters, O. J., McKee, M., Luyten, J., The Journal of the American Medical Association, 2020, 3;323(9), 844-853.
- Brown, D. G., Wobst, H. J., Kapoor, A., Kenna, L. A., Southall N., Nature Reviews Drug Discovery, 2022, 21(11), 793-794.
- Umscheid, C. A., Mitchell, M.D., Doshi, J.A., Agarwal, R., Williams, K., Brennan, P. J., Infection Control & Hospital Epidemiology, 2011, 32(2),101-14.
- Lombardino, J. G., Lowe III, J. A., Nature Reviews, Drug Discovery, 2004, 3, 853-862.
- Markan, U., Pasupuleti, S., Pollard, C.M., Perez, A., Aukszi, B., Lymperopoulos, A., Therapeutic Advances in Cardiovascular Diseases, 2019, 13(6), 1-7.
- Drug Bank, “ATC Classification: C09.” [Online]. Available: https, Accessed: 26 July 2024.
- Luu, K.T., Kraynov, E., Kuang B., Vicini P., Zhong W.Z., Journal of the American Association of Pharmaceutical Scientists, 2013, 15, 551–558.
- Zong, W.Z., Zhou, S.F., International Journal of Molecular Sciences. 2014,15, 20072–20078.
- Mohsen, S., Behrooz, A., Roza, D., Cognitive Robotics, 2023, 3, 54-70.
- Guan, L., Yang, H., Cai, Y., Sun, L., Di, P., Li, W., Liu, G., Tang, Y., Medicinal Chemistry Communications, 2018, 10(1), 148-157.
- Kufel, J., Bargieł-Łączek, K., Kocot, S., Koźlik, M., Bartnikowska, W., Janik, M., Czogalik, Ł., Dudek, P., Magiera, M., Lis, A., Paszkiewicz, I., Nawrat, Z., Cebula, M., Gruszczyńska, K., Diagnostics (Basel), 2023,3:13(15), 2582.
- Singh, R.J., Lebeda, A., Tucker O., Chapter 2, Medicinal plants—nature’s pharmacy, Medicinal plants, Boca Raton, CRC Press, 2012, 13–51.
- Zeng, X., Wang, F., Luo, Y., Kang, S. G., Tang, J., Lightstone, F. C., Fang, E. F., Cornell, W., Zhang, X. C., Wu, C. K., Yi, J. C., Zeng, X. X., Yang, C. Q., Lu, A. P., Hou, T. J., Cao, D. S., Pushing the Boundaries of Molecular Property Prediction for Drug Discovery with Multitask Learning BERT Enhanced by SMILES Enumeration. Research, 2022.
- Engel, T., Journal of Chemical Informatics and Models, 2006, 46 (6), 2267–2277.
- Muegge, I., Mukherjee, P., Expert Opinion on Drug Discovery, 2016, 11(2), 137- 48.
- Agu, P. C., Afiukwa, C. A., Orji, O. U., Ezeh, E. M., Ofoke, I. H., Ogbu, C. O., Ugwuja, E. I., Aja, P. M., Scientific Reports, 2023, 17:13(1), 13398.
- Pang, Y. P., Kozikowski, A. P., Journal of Computer-Aided Molecular Design, 1994, 8(6), 669-81.
- Thipani Madhu M., Balaji, O., Kandi, V., Ca J., Harikrishna, G. V., Metta N, Mudamanchu, V. K., Sanjay, B. G., Bhupathiraju, P. A., A Narrative Review of Chondrocalcinosis, 2024,16(6), e63448.
- Guha R, Willighagen, E., Current Topics in Medicinal Chemistry, 2012, 12(18), 1946-1956.
- Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., McGuinness, L. A., Stewart, L. A., Thomas, J., Tricco, A. C., Welch, V. A., Whiting, P., McKenzie, J. E., British Medical Journal, 2021, 29(372), 60.
- Russell, S. J., Norvig., P., Artificial Intelligence, A modern approach, 2021, 4th ed., Hoboken, Pearson.
- Bian, Y., (Sean) Xie, X.Q., “Computational Fragment-Based Drug Design: Current Trends, Strategies, and Applications,” American Association of Pharmaceutical Scientists, 2018, (20) 59,1–11.
- Erlanson, D.A., McDowell, R.S., Brien, T.O., Journal of Medicinal Chemistry, 2004, (47)14,10–12.
- Vora, L. K., Gholap, A. D., Jetha, K., Thakur, R. R. S., Solanki, H. K., Chavda, V. P., Pharmaceutics, 2023, 10:15(7), 1916.
- Vamathevan, J., Clark, D., Czodrowski, P., Dunham, I., Ferran, E., Lee, G., Li, B., Madabhushi, A., Shah, P., Spitzer, M., Zhao, S., Nature Reviews: Drug Discovery, 2019, 18(6), 463-477.
- Feng, R., New Milestone in AI Drug Discovery, 2023, https://insilico.com/blog/first_phase2: Accessed August 2024.
- Liebman, M., Chemistry International, (44) (1), 2022, 16-19.
- Blanco-González, A., Cabezón, A., Seco-González, A., Conde-Torres, D., Antelo-Riveiro, P., Piñeiro, Á., Garcia-Fandino, R., Pharmaceuticals (Basel), 2023, 18:16(6), 891.
- Hughes, J. P., Rees, S., Kalindjian, S. B., Philpott, K. L., British Journal of Pharmacology, 2011, 162(6), 1239-49.
- Han, R., Yoon, H., Kim, G., Lee, H., Lee, Y., Pharmaceuticals (Basel), 2023, 6:16(9), 1259.
- Quazi, S., Medical Oncology, 2022, 15:39(8), 120.
- Zhavoronkov, A., Ivanenkov, Y. A., Aliper, A., Veselov, M. S., Aladinskiy, V. A., Aladinskaya, A. V., Terentiev, V. A., Polykovskiy, D. A., Kuznetsov, M. D., Asadulaev, A., Volkov, Y., Zholus, A., Shayakhmetov, R. R., Zhebrak, A., Minaeva, L. I., Zagribelnyy, B. A., Lee, L. H., Soll, R., Madge, D., Xing, L., Guo, T., Aspuru-Guzik, A., Nature Biotechnology, 2019, (9), 1038-1040.
- Dara, S., Dhamercherla, S., Jadav, S. S., Babu, C. M., Ahsan, M. J., Artificial Intelligence Reviews, 2022, 55(3), 1947-1999.
- Drews, J., Drug discovery, 2000, 287(5460), 1960-4.
- Hassija, V., Chamola, V., Mahapatra, A., Cognitive Computing, 2024, 16, 45–74.
- Seema, Y., Abhishek, S., Rishika, S., Jagat, P. Y., Intelligent Pharmacy, 2024, 2(3), 367-380.
- Feng, R., New Milestone in AI Drug Discovery, 2023, https://insilico.com/blog/first_phase2: Accessed August 2024.
- Balfour, H., DSP-1181: drug created using AI enters clinical trials. European Pharmaceutical Review – News on 4 February DSP-1181, 2020: drug created using AI enters clinical trials. europeanpharmaceuticalreview.com.
- Bess, A., Berglind, F., Mukhopadhyay, S., Brylinski, M., Griggs, N., Cho, T., Galliano, C., Wasan, K. M., Drug Discovery Today, 2022, 27(4), 1099-1107.
- Desai, D., Kantliwala, S. V., Vybhavi, J., Ravi, R., Patel, H., Patel, J., Review of AlphaFold 3, Cureus: Journal of Medical Science, 2024, 16(7), e63646.
- Shang, Z., Chauhan, V., Devi, K., Patil, S., Journal of Multidisciplinary Healthcare, 2024, 15(17), 4011-4022.
- Aiumtrakul, N., Thongprayoon, C., Suppadungsuk, S., Krisanapan, P., Miao, J., Qureshi, F., Cheungpasitporn, W., Journal of Personalized Medicine, 2023, 30:13(10),1457.
- Visan, A. I., Negut, I., Life (Basel), 2024, 7:14(2), 233.
Figure 1.
2-dimensional structures of some of the keynote discoveries in drug development.
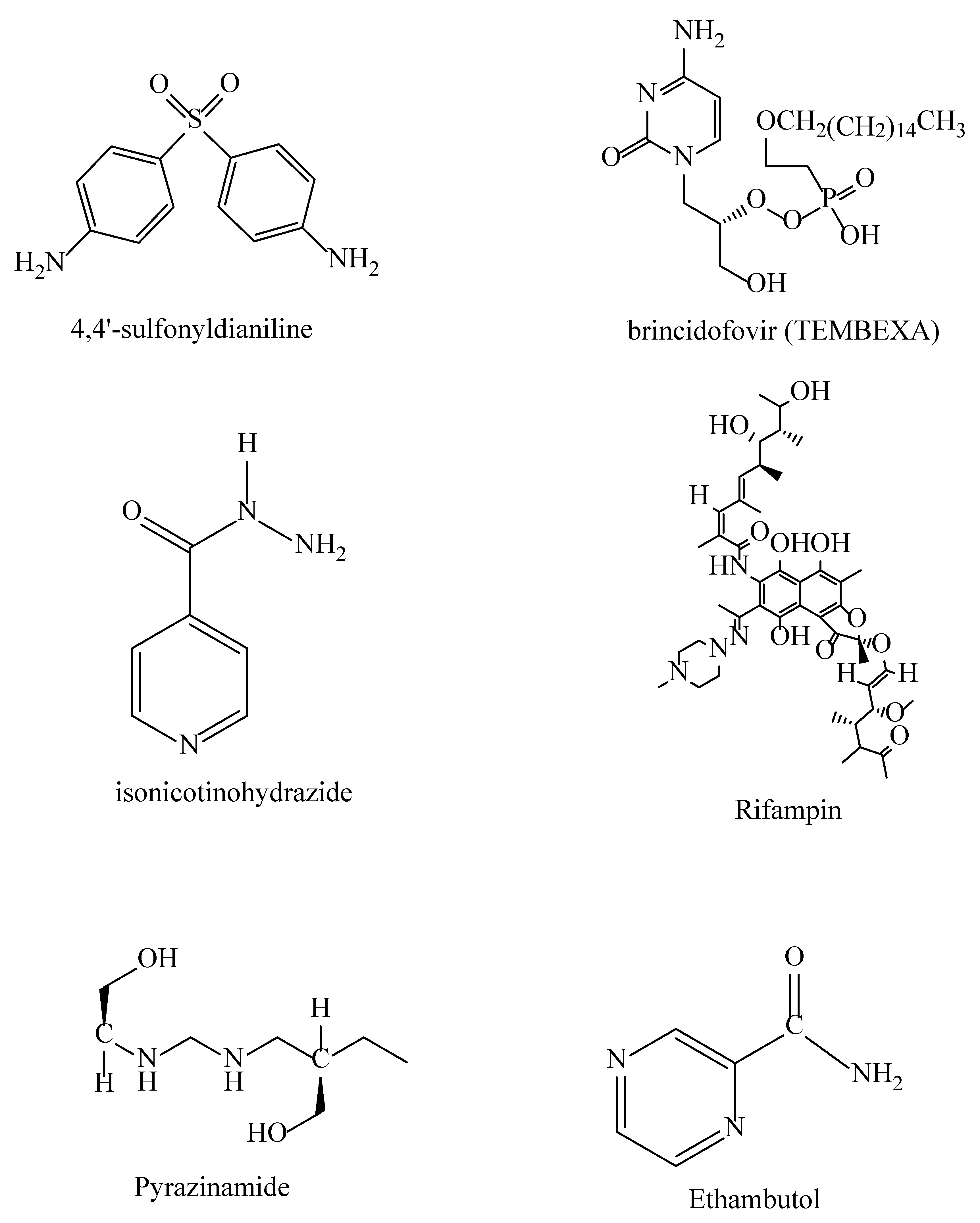
Figure 2.
Summary of the drug discovery and development process.
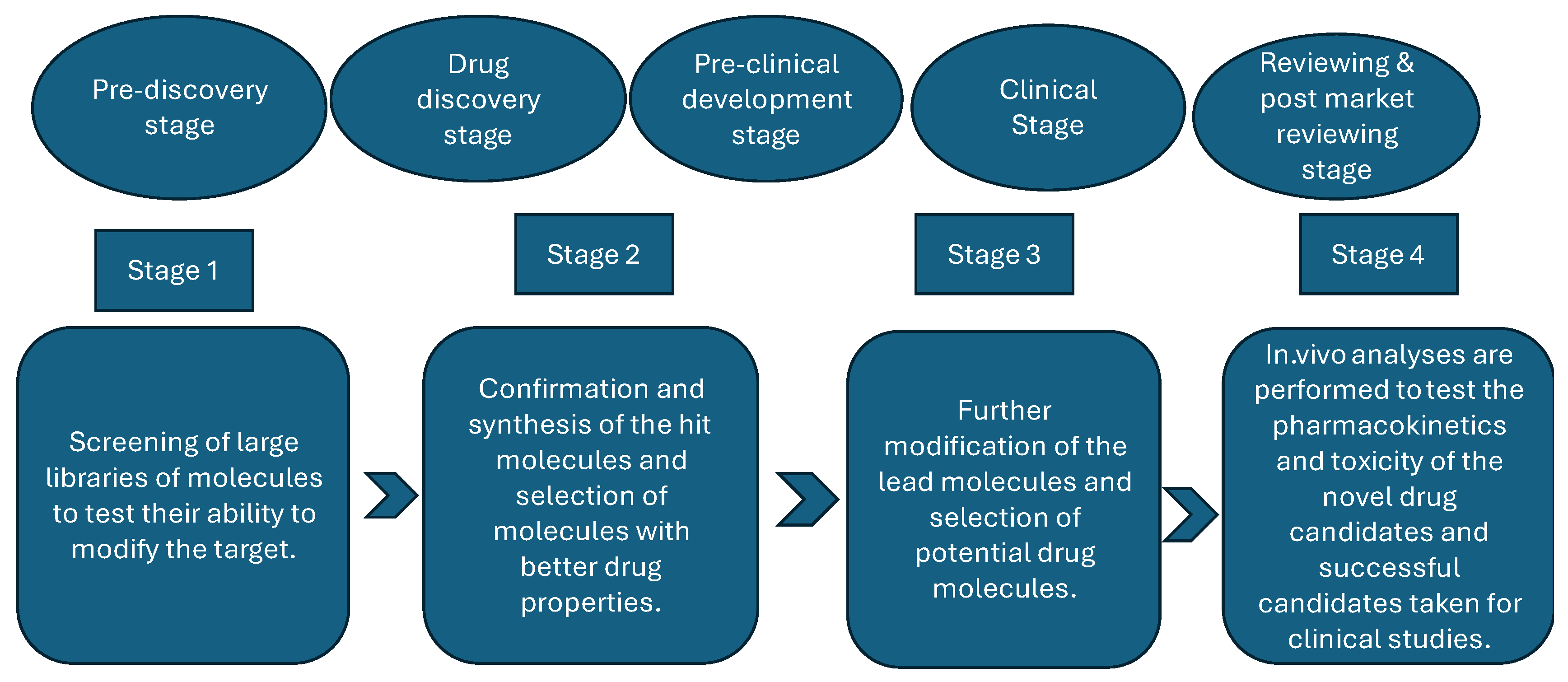

Table 1.
Traditional Drug Discovery vs AI-Enhanced Drug Discovery.
| Aspect | Traditional Drug discovery | AI-enhanced drug discovery |
|---|---|---|
| Cost of production | It is quite slow since it involves many manual processes and trial and error. | Quite fast since most of the processes are automated, resulting in large amounts of data being processed quickly. |
| Reaction accuracy | Reactions are less accurate because they rely solely on humans Capabilities. |
It has the potential to increase reaction accuracy by accurately predicting reaction interactions. |
| Screening | Physical high-throughput screening takes longer and is expensive. | Virtual screening of millions of compounds in a short time time. |
| Lead Optimization | Requires manual labor and intensive effort optimization. | AI-driven algorithms optimize lead compounds more efficiently. |
| Innovation | Innovation is driven more by established scientific paradigms. | AI can identify novel drug candidates and mechanisms that humans cannot easily identify and observe. |
| Drug Repurposing | Drug repurposing is slower due to limited experimental evidence insights. | AI can identify existing drugs for new uses by analyzing large datasets. |
| Target Identification | Relies heavily on human hypotheses and experiment validation. | AI can quickly identify new drug targets using complex data patterns. |
| Personalization | Limited ability to tailor drugs to individual genetics profiles. | Can assist in developing personalized therapies based on patient’s data. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



