
Submitted:
19 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
Background/Objectives: A relatively small number of studies have evaluated the effec-tiveness of interventions designed to ameliorate family burden and to improve family functioning for families with a child with ASD. This study aims to investigate whether a long-term multi-family group psychoeducational intervention, originally developed for families with a member with a psychiatric disorder, can assist parents of children with ASD to improve family functioning; family rituals; family burden; to understand the etiology, the characteristics, and treatment options for ASD; and to manage social- and self-stigmatization.
Method: We compared an intervention group (N=3 couples – 6 parents) with a waitlist control group (N=3 couples – 6 parents) by administering psychometric scales to evaluate the effectiveness of the intervention on (a) family functioning, (b) family rituals, and (c) family burden. Qualitative analysis of pre- and post-intervention semi-structured interviews assessed (a) the participants' understanding of the nature, causes, and treatments for ASD and (b) management of social- and self-stigmatization in families with a child with ASD.
Results: Quantitative pre and post-test group comparisons as well as qualitative thematic analysis revealed significant decreases in all parameters under study for the treatment group.
Conclusions: Our findings provide pilot evidence that long-term group psychoeduction,
originally designed for families with a member with a psychiatric disorder,may provide an efficacious treatment choice toward improving the general functioning of families with a child with ASD. Systematic replications of this psychoeducational intervention merit attention.
Keywords:
autism spectrum disorder
; group psychoeducation
; family functioning
; family rituals
; family burden
; stigma management
1. Introduction
Autism spectrum disorder (ASD) is classified as a neurodevelopmental disorder characterized by persistent impairment in communication and social interaction; restricted, repetitive patterns of behavior, interests, or activities; and sensory sensitivities [1]. Recent epidemiological studies estimate ASD prevalence worldwide to be around 1%, consistently increasing over the past 15–20 years [2,3]. There are also much higher estimates of its prevalence. For example, 2,85% of 8-year-old students in the USA are diagnosed with ASD[4]. Provided the chronic and often lifelong nature of ASD, individuals with this diagnosis may require long-term care and support for which family members undertake responsibility. Active involvement of family members in the implementation of therapeutic protocols has been shown to enhance the development and prognosis of children with ASD [5,6,7]. Nevertheless, there is a scarcity of programs that provide proper, on-going, and systematic support to enhance parenting skills and alleviate stress and depression that are particularly elevated in parents of children with ASD – even more so than in parents with children other disabilities [8].
It has been extensively documented that parents who raise a child with ASD are chronically exposed to high levels of stress [6], due to various psychosocial challenges stemming from the child's social, communicative, and behavior difficulties and from the limited access to comprehensive therapeutic interventions and rehabilitation services for individuals with ASD [9,10,11,12,13]. Chronic stress is detrimental for the parents' health and quality of life, and has been associated with somatic symptoms, anxiety, depression, and poorer perceived general health compared to the general population [12,14]. Chronic stress has adverse effects not only on the parents, but also on the family member diagnosed with ASD [6,15]. It is undoubted that people with ASD are recipients of stress but also impose stress on other family members [16]. Expressed Emotion (EE) (which refers to negative emotional intensity in the family context and is a risk factor for relapse) is another factor with adverse impact on the family dynamics and on the person with ASD since it has been proven to exacerbate or maintain behavior problems and autistic symptomatology [17,18,19]. On the other hand, longitudinal studies have shown that parents’ warmth and positive attitude toward their children with ASD is associated with decreasing behavior problems [6,20].
The cumulative effects of emotional strain, financial difficulties, social challenges, and psychosomatic symptoms are referred to as "family burden" [21,22,23,24,25,26]. Researchers distinguish between objective burden, defined as manifested disorder-associated costs to families (e.g., financial issues), and subjective burden, defined as each family's interpretation of hardships associated with facing a serious disorder [25]. Family burden or the difficulties associated with raising a child with ASD may impose difficulties on the family’s daily functioning and its overall social adjustment, such as the family’s engagement in social rituals, traditions, ceremonial activities, vacations, and recreational social activities, which are all important for maintaining family cohesion and stability [27]. .
It has also been demonstrated that raising a child with ASD imposes strain on the marital relationship – leading to disruption of family cohesion – and also has a negative impact on the interaction and communication among family members themselves (including the extended family), and between family members and neighbors and friends which may lead to psychosocial disengagement or marginalization of the family [10,28]. Nevertheless, aside from evaluating burden and strain imposed on families, it is important to explore parameters that may improve the quality of family functioning. The McMaster Model of Family Functioning [29] provides a comprehensive description of six dimensions pertaining to the functioning of the family system and thus may be used for families with a member with a chronic disability [30]. The dimensions of the McMaster Model are evaluated by the Family Assessment Device [29].
Another adversity, that families raising a child with ASD need to cope with, is stigma. Described as an attribute that is deeply discrediting, with components such as labelling, stereotyping, separating, status loss, and discrimination, social stigma leads to poorer quality of life for families with children with ASD [31]. Self-stigma is the most debilitating type of stigmatization since the person who experiences self-stigma is adopting an “illness identity” – a devalued view of oneself that overshadows every other identity [32].
Despite the identification of a host of difficulties that may be associated with raising a child with ASD, and the undoubted benefits of parent training and support services, a relatively small number of studies have evaluated the effectiveness of interventions designed to ameliorate parents’ psychological difficulties, to reduce family burden, and to improve family functioning and family atmosphere for families with a child with ASD [12,33,34,35,36]. Stressful life events may often not be avoided, yet, improving coping mechanisms that help reduce family burden may be a realistic goal for families of individuals with ASD.
Due to the scarcity of studies addressing the improvement of family functioning, and provided the benefits of having a warm and supportive family atmosphere, it was considered important to explore the literature for interventions whose effectiveness is well documented (evidence-based) with clinical populations other than ASD. One example of such interventions is family psychoeducation that has been adapted to involve, not only the person with a serious mental illness, but also members of his/her family. Falloon & Liberman [37] developed and introduced a psychoeducation intervention that addresses families with a member with schizophrenia. Family psychoeducation entails didactic and therapeutic elements that aim to inform family members about the illness and to guide them on how to improve the family functioning, to handle and cope with the illness, and to manage social and self-stigma. The psychoeducational process typically includes: (a) briefing about the illness, (b) training in problem-solving, (c) practicing effective communication, and (d) learning to assert one's needs [30,38].
Empirical studies and meta-analyses – conducted with populations from the USA, Australia, and Europe – have demonstrated that parent support programs, implemented to parents of children with ASD, lead to improved parental psychosocial outcomes [39]. In addition, participation in psychoeducational programs can reduce family burden, improve coping, enhance family organization and coherence, and reduce social and self-stigma [30,40,41,42,43]. Family psychoeducation formats vary, including long vs. brief, single-family vs. multi-family group, and peer-led vs. professional-led programs [6].
Family psychoeducation has also been shown to reduce family stress and improve outcomes in other populations with various diagnosis, such as cancer, asthma, and mood disorders [44,45,46,47,48,49,50,51,52,53]. Pertaining to the diagnosis of ASD, Dawalt et al. [6] provided a preliminary evaluation of a controlled multi-family group psychoeducation intervention addressing parents of adolescents with ASD, with promising outcomes, since improvements were noted in parental depressive symptoms and problem-solving skills following treatment. Nevertheless, the majority of psychoeducation programs address the children’s needs and aim to support children with ASD rather than their parents [27], who need to increase their competence in parenting a child with ASD, overcome social isolation, and decrease their stress levels [27]. Thus, the need to design psychoeducational interventions that primarily address parental functioning in families with a child with ASD remains prevalent.
The present study aimed to investigate the effectiveness of a long-term multi-family group psychoeducational intervention, originally designed for parents of individuals with schizophrenia [30,38], to parents of children with ASD. Hence, the originality of the present study lies on: (a) the systematic adaptation and application of an evidence-based psychoeducational intervention, designed originally for families with a member with Schizophrenia, to parents of children with ASD and (b) the extensive focus of the psychoeducation program on the improvement of the systemic properties of the family of a child with ASD (parental communication and affective responsiveness skills, problem solving skills, adherence to family rituals, social and self-stigma management, and stress management). Finally, considering the international focus on parent support programs, the importance of this study lies on the need to assess the efficacy of programs in countries such as Greece, where there aren’t but a handful of studies in psychoeducational services for parents and no intervention studies for parents of children with ASD.
We compared an intervention group with a waitlist control group by administering psychometric scales to evaluate outcomes in (a) family functioning (problem-solving, communication, roles, behavior control, affective responsiveness, and involvement per the McMaster family model), assessed by the Family Assessment Device [27]; (b) family engagement in rituals and routines, assessed by the Family Rituals Scale [55]; and (c) family burden (psychological, financial, health, and social hardships), assessed by Family Burden Scale [25]. A qualitative analysis, based on pre- and post-intervention focus group data, was conducted to evaluate the participants' (a) understanding of the nature, causes, and treatments for ASD and (b) management of social stigma and self-stigma.
2. Materials and Methods
2.1. Participants
Six couples – parents of children diagnosed with ASD – that were all attending educational and therapeutic programs, at the Institute of Systemic Behavior Analysis (ISBA), located in Athens, Greece and at the Day Center Hara II (DCH II) in Larissa, Greece – participated in this study. The participation of the parents in the study was voluntary. The demographic characteristics of the participants and their offsprings are depicted in Table 1.
2.2. Settings and Researchers
For a period of over twelve months, the members of the treatment group met regularly at the ISBA, where psychoeducational group sessions were held in an office area. The control group received individual psychological counselling, provided at the Day Center Hara II by a psychologist who was specialized in autism. Couples from the control group were registered on a waitlist to receive group psychoeducation in the year to come.
The psychoeducational treatment sessions were conducted by the two authors of the present article who were highly experienced clinical psychologists, both holders of a doctoral degree in Behavior Analysis and certified in family psychotherapy (systemic and behavioral approach).
The first author served as the primary observer, responsible for data collection and analysis of all research sessions. There were also two psychology undergraduate students who served as secondary independent observers and were trained systematically for the purposes of the present study.
2.3. Assessment Instruments
2.3.1. Standardized Assessment Measures
To assess the effectiveness of treatment, performances of the two groups were compared across both quantitative and qualitative measures. Participants in both the treatment and the control group were pre-and post-tested with three self-reported questionnaires, each measuring a separate family parameter: family functioning (Family Assessment Device), family rituals and routines (Family Rituals Scale), and family burden (Family Burden Scale). For the purposes of the qualitative assessment, we conducted individualized semi-structured interviews with each participant pre and post treatment on the following topics: (a) understanding of the nature, causes, and treatments of ASD and (b) ways of managing social stigma and self-stigma associated with raising a child with ASD.
2.3.1.1. Family Functioning
The Family Assessment Device (FAD) was used to assess family functioning [27]. FAD is a self-reported, paper-and-pencil, 60-item questionnaire that assesses one’s perception of his/her family across seven dimensions: a) Problem Solving: skills to manage issues that threaten the functional capacity of the family and the integrity of the family unit. b) Communication: verbal interactions among family members that permeate clear messages (c) Roles: concretely-stated and equally-distributed assignment of responsibilities among family members, providing nurturance and support to one another, promoting personal development for each family member, following up on whether tasks assigned are carried out responsibly. (d) Affective Responsiveness: the extent to which each family member has affective reactions that are congruent to social context. (e) Affective involvement: the extent to which family members are interested and show respect to each other’s actions or concerns. Family well-being corresponds to intermediate levels of involvement, low and high scores of involvement are associated with dysfunction. (f) Behavioral Control: the standards for the behavior that the family sets for its members which may be flexible, rigid, indifferent, or chaotic. The scale is scored in the direction of dysfunction, with rating 4 reflecting high levels of dysfunction. The Greek version of FAD shows high subscale internal consistency (Cronbach’s a > 0.7) [56]. The FAD subscales are psychometrically sound (Cronbach’s a from 0.72 to 0.92)). Cutoff scores for normal family functioning are: ≥2 for the General Family Functioning, 2.3 for Family Roles, 2.2 for Communication, Problem-Solving, Affective Responsiveness, 2.1 for Affective Involvement, and 1.9 for Behavior Control.
2.3.1.2. Family Rituals
The Family Rituals Scale (FRS) [55] is an eleven-item, self-reported questionnaire that measures three types of family activities that increase members’ participation in family rituals and routines: (a) family traditions on religious holidays, (b) family celebrations and trips, and (c) patterned routines. The scale is scored in the direction of dysfunction, with 11 being the regular practice of family rituals and 44 being the absence of family rituals. The scale shows adequate internal consistency (Cronbach’s alpha = 0.89). The cutoff score for FRS is 18.
2.3.1.3. Family Burden
The Family Burden Scale (FBS) [25] is a twenty-three-item scale that measures the burden experienced by caregivers of individuals with psychiatric disorders. It measures burden across four dimensions: (a) impact on daily activities/social life, (b) incidence of aggressive, violent episodes, (c) impact on physical and mental health of the caregiver, (d) impact on financial status/financial problems due to the patient’s illness. The first, second, and fourth dimensions provide measures of objective burden, whereas the third is a measure of subjective burden. The scale is scored in the direction of dysfunction and shows adequate internal consistency (Cronbach’s a = 0.85). The cutoff score is 24.
2.3.2. Qualitative Assessment
2.3.2.1. Semi-Structured Interview
A semi-structured interview was conducted with each one of the participating parents (treatment and control group), before and after the intervention. The interview was based on a set of 6 open-ended questions, organized around two main topics: (a) parents’ understanding of the nature of their offspring’s disorder (e.g., etiology, symptoms, treatment, and prognosis of ASD) and (b) self and social stigma management (e.g., what they think of themselves as parents of an individual with ASD, or what they believe other people think of them as parents with an offspring with ASD).
2.4. Design and Procedure
A controlled group trial with a pre- and post-measures quasi-experimental design was used to assess the effectiveness of the treatment procedure. Couples were assigned to one of two groups matched by city of origin (Athens or Larissa), age, years of education, and year of initial diagnosis of their offspring. The treatment group (N =6, three couples received intensive psychoeducational therapy, and the control group (N= 6, three couples) received standard counseling, provided by a psychologist at a daycare center. Taking into consideration the small sample sizes per group of participants (N=6) [57] a t-test for analyzing independent samples was conducted, showing equality of means for age, years of education, and years of diagnosis between the two groups (p > 0.2), thus making the two groups relatively homogeneous.
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the research ethics committee of the National and Kapodistrian University of Athens (NKUA) and of the ISBA (project identification code and date: 78/7-9-2017). Parents were contacted, in person, to discuss the purpose and procedures of the study. Written informed consent was obtained from all twelve parents prior to the beginning of the study.
All six couples (treatment and control group) were pre and post tested using both quantitative and qualitative means of assessment. Standardized tests were self- administered in a private room in paper and pencil format. Semi-structured interviews yielded the data used for qualitative analysis. pertaining to the participants' (a) understanding of the nature, causes, and treatments of ASD, and (b) ways of managing social stigma and self-stigma associated with raising a child with ASD. The interview was audiotaped for data-collection purposes and had no time limit (average interview time: 60 min.) The off springs received ASD specialized treatment services throughout the study at the ISBA (treatment group) and DCH-II (control group).
The three couples who participated in the treatment group received 23 biweekly 90-min sessions conducted by two experienced clinical psychologists, who were also the study coordinators, both holders of doctoral degrees in Applied Behavior Analysis for children with ASD, both certified in family psychotherapy (systemic and behavioral approach).
The content and format of the psychoeducation program was based on the behavioral-family-therapy protocol developed by Falloon and his associates [30,58,59]. Proper adjustments of the protocol were made by the study coordinators to address the needs of children with ASD, based on parental reports and relevant studies with parents of children with ASD [9,10,11,12,13,60,61]. Parental reports were systematically drawn from semi-structured individual interviews during which the parents discussed questions, posed by the coordinators, and addressed difficulties that families encountered at that time. During all treatment and focus group sessions parents and therapists sat in a circle to ensure full attendance of the group process by all group members. The content of the intervention after adaptations was as follows: (a) to provide parents with information about the nature, the causes, and treatment of ASD, (b) to assist them in developing coping skills that would help them deal with social and self-stigma, (c) to train them in techniques for improving communication and problem-solving, and (d) to assist them in developing behavior management skills. To meet the protocol’s aims, several techniques were used including modeling, role-playing, positive feedback, and promoting generalization through homework assignments. Participants were also provided with educational material associated with the content of the therapeutic sessions that was provided either printed or in reference to internet websites. The content and structure of the program are summarized in Table 2.
2.5. Data Collection and Analysis
For data collection and analysis purposes, all sessions were audio taped, scored, and analyzed by independent observers to ensure adherence to the implementation of the treatment protocol (treatment fidelity) and reliability of treatment outcomes. Analysis of the quantitative and qualitative data will be presented in this section separately and in detail. Data were also collected on communication and problem solving skills training of the parents for interobserver agreement purposes.
2.5.1. Quantitative Analysis
SPSS 18.0 J for Windows was used to assess the questionnaire scores. Two types of nonparametric statistical tests were conducted. Specifically, for the purpose of comparing before and after treatment effects within each group, mean scores before and after treatment were compared using the Wilcoxon matched-pairs signed-ranks test, since it is a test suggested for repeated measurements on single small samples, when the population from which they are drawn cannot be assumed to be normally distributed[57]. Mean score comparisons within groups for the total scores were conducted for the Family Assessment Devise (FAD), the Family Rituals Scale (FRS), and the Family Burden Scale (FBS). For the FAD and the FBS, post-hoc before-after within group comparisons, using the Wilcoxon matched-pairs signed-ranks test, were conducted for all their subscales’ mean scores. To compare between groups (the psychoeducation group and the standard-care control group) mean scores before and after treatment, on the same three questionnaires, the non-parametric statistical-hypothesis Mann-Whitney U-Test was conducted since it is one of the most frequently used nonparametric significance tests for equal small sample sizes.
2.5.2. Qualitative Analysis
Patterns of answers, that were provided during the structured interviews before and after the intervention from both the treatment and the control group, were identified, coded, and categorized. The identified themes were the following: (a) Understanding ASD (etiology, characteristics, treatment, and prognosis) and (b) social- and self-stigma management.
3. Results
The quantitative and qualitative results of the present study are presented separately. The quantitative outcomes are the product of statistical analysis comparing pre- and post-treatment data collected from the three questionnaires (FAD, FRS and FBS) using within- and between-groups comparisons. Qualitative outcomes are yielded from systematic identification, coding, and categorization of data collected during semi-structured interviews conducted with each participating parent (pre-and post-treatment) data collected from within- and between-groups comparisons that were conducted with each of the six couples of parents before and after the intervention. The IOA for standardized -measure outcomes (quantitative data) and for qualitative data derived from semi-structured interviews and focus groups was 100%. For treatment fidelity purposes, interobserver agreement (IOA) data were collected on 70% of the treatment sessions. IOA ranged from 80 to 100% with an average of 92%.
3.1. Quantitative Outcomes
3.1.1. Family Assessment Device
Table 3 depicts the mean scores (SD) on the subscales of the FAD before and after the intervention within the treatment group (N=6) and within the control group (N=6), as well as the cutoff scores on each sub-scale for normal family functioning. The results of the Wilcoxon matched-pairs signed-ranks test analysis (z-values and p-values) are recorded for each family subscale mean score differences, within each of the two groups. Pre-intervention mean scores indicated family functioning at pathological levels across all family dimensions for both groups, with the exception of Emotional Involvement, which was within normal range (cutoff=2,10) for both treatment (M=1,92; SD=0,2) and control group (M=2,01; SD=0,3 ). Problem Solving was referred to as the most abnormal dimension of family functioning for both treatment (M=2,83; SD=0,37, and control group (M=2,65; SD=0,2; cutoff=2,20).
For the treatment group, the Wilcoxon matched-pairs signed-ranks test comparisons of all pre- and post-treatment mean sub-scale scores showed a statistically significant (p<0.05) decrease across all seven family dimensions, except for Emotional Involvement (p=0,6), (which was already within normal family functioning levels (M<2,10) prior to intervention). Additionally, the post-intervention mean scores for the treatment group dropped under the cutoff scores across all family functioning dimensions, indicating normal levels of family functioning following intervention, with one exception. The mean family subscale scores for Behavior Control remained at marginally dysfunctional levels (M =1,98; SD=0.1; cutoff score= 1.90). For the control group, there were no statistically significant mean differences (p < 0.05) on the Wilcoxon matched-pairs signed-ranks test comparisons on any of the pre- and post-treatment mean sub-scale scores. The mean scores of the control group remained at dysfunctional levels (higher than the cutoff scores) across all family functioning dimensions, except for the Emotional Involvement sub-scale (M=2,06; SD=0,4), which was already within normal range before the intervention.
Table 3 also depicts the results of the Mann-Whitney U-Test (Average Ranks and p values) comparing the mean scores of all family-functioning subscales at pre- and post-test between treatment and control group. Statistical significance was set at p < 0.05. There were no statistically significant differences between the two groups at pre-test (p > 0.05), showing no between-group systematic differences in any of the family-functioning dimensions before intervention. When the two groups were compared post-treatment, however, the treatment group’s Average Ranks scores in all family-functioning dimensions were lower than those of the control group at a statistically significant level (p < 0.05). Figure 1 and Figure 2 depict pre- and post-treatment mean scores across all dimensions of family functioning of the FAD for the treatment and the control group accordingly.
3.1.2. Family Rituals Scale (FRS) and Family Burden Scale (FBS)
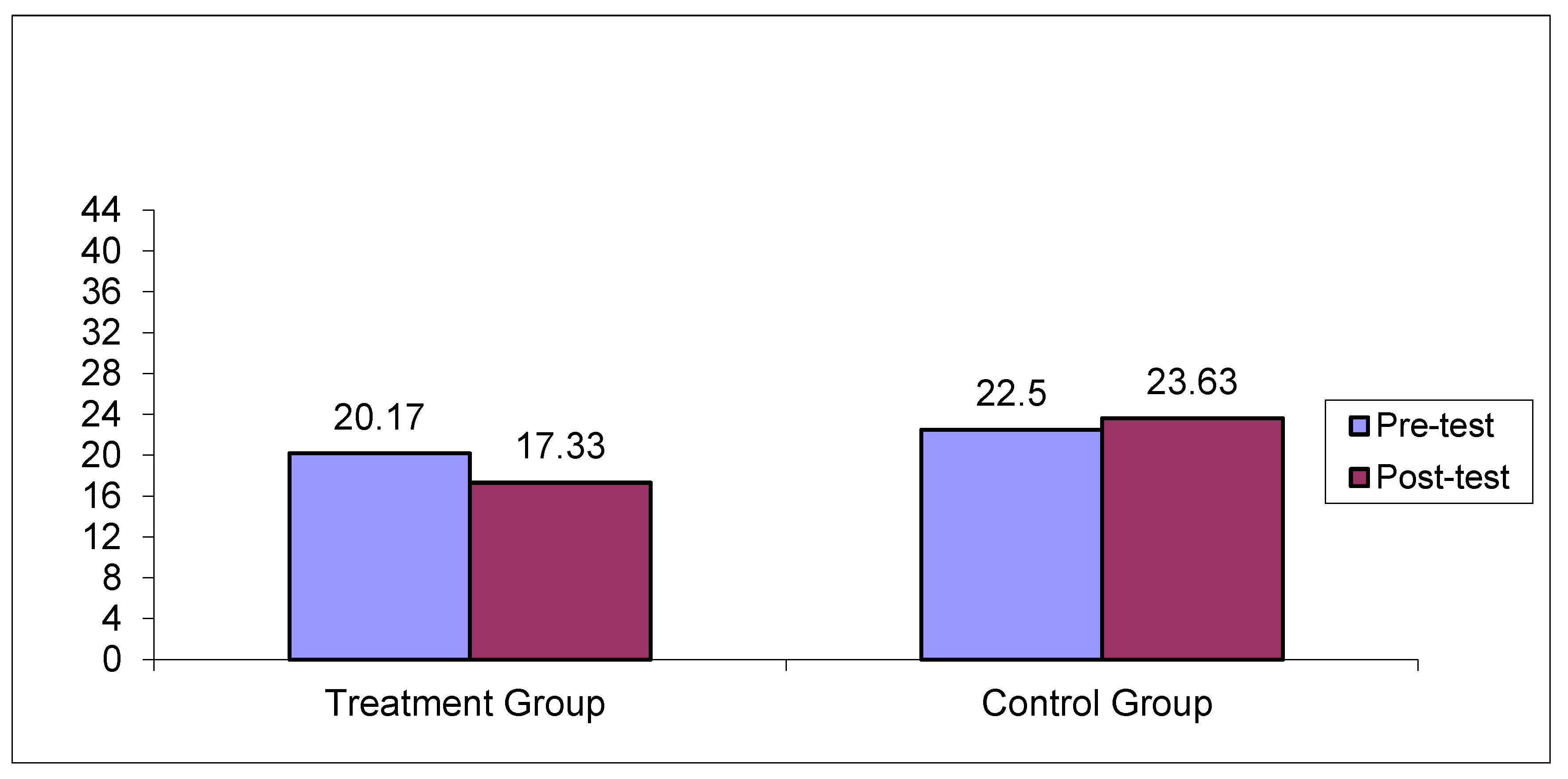
Table 4 depicts the pre- and post-treatment mean scores (SD) on the FRS and the FBS as well as on all their subscales, within the treatment group (N=6) and within the control group (N=6), and it also depicts the cutoff scores on both scales. In addition, results of the Wilcoxon matched-pairs signed-ranks test analysis (z-values and p-values) are depicted on Table 4 for FRS and FBS total scale and subscales mean score differences within and between groups Results showed that there was statistically significant improvement at p < .05 for the FRS mean scores after treatment for the treatment group, (pre-test M=20.17; SD=2.56), post-test M=17.33; SD=2.16, z=-2.27, p=0.02), while for the control group pre and post-test mean score differences where of no statistical significance (pre-test M=22.50; SD=4.2, post-test M=23.63; SD=4.16, z=-1.61, p=0.08). The findings were similar for FBS. Specifically, for the treatment group, there was statistically significant improvement at p < .05 for the FBS total mean score after treatment (pre-test M=21.50; SD= 5.11, post-test M=13.5; SD=4.03, z=-2.22, p=0.026), while for the control group pre and post-treatment total FBS mean score differences where not statistically significant (pre-test M=22.30; SD=3.2, post-test M=25.55; SD=3.6, z=-1.02, p=0.07). Subscale pre and post mean score comparisons for the treatment group showed statistically significant decrease of family burden across the three out of four family burden dimensions: Social Life (pre-test M=8.70;SD=2.7, post-test M=6.63; SD=3.9, z=-2.73, p=0.03, Aggressiveness subscale mean scores (pre-test M=3.30; SD=2.7, post-test M=2.37;SD=1.8, z=-2.6, p=0.04), Health subscale mean scores (pre-test M=7.25; SD=2.1, post-test M=3.13; SD=2.05, z=-2.17, p=0.011). Nevertheless, Financial Burden subscale mean scores difference was not statistically significant for the treatment group (p>.05).For the Control group pre and post-test FBS mean sub-scale score differences where not statistically significant for any of the four dimensions (p>.05).
Finally, Table 4 depicts the Mann Wittney U test comparisons of the mean scale and subscales scores on the FRS and the FBS at pre- and post-test, between the treatment group (N=6) and the control group (N=6). There were no statistically significant differences between the two groups at pre-test (p>.05), showing no systematic differences in level of disruption of family rituals and family burden between the two groups. Nevertheless, mean scores between the two groups differed significantly (p<.05), in favour of the treatment group, after the psychoeducational therapeutic intervention, in both FRS and FBS and its subscales, except for the mean scores on the financial-burden subscale (p>.05). Graphs 3 and 4 depict pre- and post-treatment total mean scores for the FBS and the FRS scales for the treatment and the control group, respectfully.
Figure 3.
Pre and post- test mean scores on the FBS across treatment and control group.
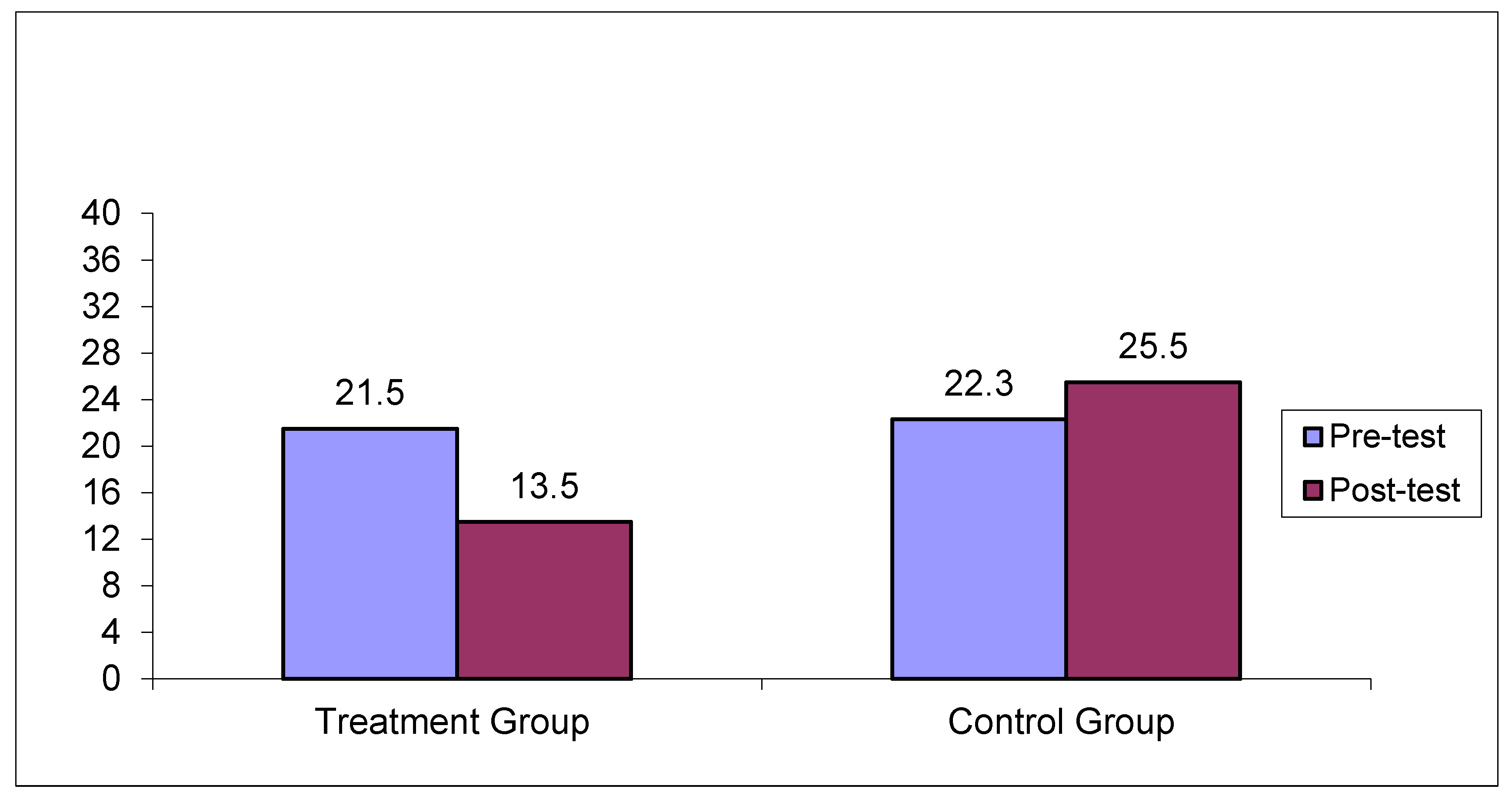
Figure 4.
Pre and post- test mean scores on the FRS across treatment and control group.
As mentioned in the data collection and analysis section, data were systematically collected on communication and problem-solving skills of the parents who participated in the treatment group. All parents demonstrated great improvement in all those skills. Interobserver agreement on data collected during parent training ranged from 90-100% agreement.
3.2. Qualitative Analysis of Parents’ Self-Reports
Table 5 depicts the qualitative analysis conducted on the answers of parents of the treatment group that were provided during the semi-structured interviews before and after treatment in relation to knowledge about ASD and to stigma management.
3.2.1. Knowledge About ASD
3.2.1.1. Understanding of the Causes of ASD
Parents’ answers regarding the possible causes of ASD, prior to intervention, for both the treatment and the control group (N=12), may be categorized around two themes: (a) environmental and psychological factors (e.g., “I was working a lot during pregnancy”, “I was spending too much time on the internet”, “My son regressed when he was vaccinated”, “stressful events during pregnancy, like my fathers’ death”, “I think he took after his father’s personality”, etc.) and (b) vagueness and general confusion (e.g., “It is a very confusing disorder and I find it hard to understand”). After study completion, the parents’ answers in the treatment group (N=6) shifted towards genetic/neurobiological explanations for the etiology of ASD (e.g., “genetic disorder of a very complex nature, “It is a brain dysfunction that happened before birth”). Contrary to the treatment group, no thematic changes were detected in the answers of the control group after treatment.
3.2.1.2. Symptomatology of ASD
Before treatment, parents’ descriptions of their offspring’s symptoms, both in the treatment and the control group (N=12), were organized around personality characteristics: (e.g., “my child is an introvert” “He is very stubborn” etc.). After intervention, parents in the treatment group (N=6) were able to describe the main neurodevelopmental characteristics of ASD (difficulties in communication, emotional expression, play and social skills, behavioral issues etc.), while there were no thematic shifts in the control group.
3.2.1.3. Treatment of ASD
Prior to intervention, parents, in both the treatment and the control group (N=12), considered medication as the only possible effective treatment, while they were simultaneously seeking for a miraculous solution. Following treatment, parents in the treatment group identified the importance of intensive psychoeducational programs for the child and the family (structure, routines, intensive educational programs, alternative communication programs, behavior support programs together with a supportive family atmosphere, etc.). No thematic shifts were identified for the control group.
3.2.2. Stigma Management
3.2.2.1. Social Stigma Management
Before the intervention, parents’ answers regarding social stigma management, in both the treatment and the control group, were organized around two main patterns: (a) social withdrawal and avoidance of public places and (b) shame for their child’s behavior and/or anger for other people staring at or avoiding the child and the family. Following treatment, the parents’ answers in the treatment group (N=6) shifted towards three major themes: (a) social networking with other families with a child with ASD, (b) strengthening of family cohesion through family outdoors activities, and (c) social networking with relatives and members of their community and a need to inform people about their child’s disability. No thematic changes were detected in the answers of the control group following the introduction of treatment.
3.2.2.2. Self-Stigma Management
Before the intervention, parents’ answers regarding self-stigma management, both in the treatment and the control group (N=12) evolved around two main themes: (a) self-blame, guilt, sense of failure in the parental role, and (b) increased levels of parental stress due to lack of skills for managing their child’s behavior, meeting financial needs, and planning for their child’s future. After the intervention, parents’ self-reports for the treatment group (N=6) shifted towards two new themes (a) a sense of empowerment in the parental role and a need to advocate for their child with a sense of pride for being a parent of a child with ASD and (b) a sense of efficacy in the parental role, through a better understanding of the nature of ASD, in general, and their child’s needs, in particular. No thematic changes were identified in the control group.
4. Discussion
Families of children with ASD experience unique stressors in their daily lives since autism has pervasive effects across all the domains of child development. The complexity of the disorder, the disruption of family functioning, the social isolation due to social- and self-stigmatization, and a host of other factors lead to high stress levels and to family burden [62].
The aim of the present study was to investigate the effectiveness of a long-term, multi-family, group psychoeducational intervention on assisting parents of children with ASD to surpass parental and family difficulties, associated with the diagnosis of ASD. Specifically, both quantitative and qualitative means of assessment were utilized to assess the effectiveness of the intervention.
The quantitative analysis included three standardized scales that were administered to both the treatment and control groups prior and after applying the intervention. The results revealed that there were no systematic differences between the two groups prior to intervention. Thus, we may ascertain that differences between the two groups, following the intervention, may be attributed to the psychoeducational program that was applied [63].
Following the intervention, systematic changes were not noted in the control group for any of the three standardized scales that were administered. On the other hand, several systematic improvements were achieved by the treatment group. Those improvements were statistically significant and may be summarized as follows:
- On the FAD, prior to intervention, the scores obtained place family functioning within pathological levels in six out of seven family function subscales for both groups. These results are consistent with findings of previous studies that report high stress levels, negative emotional intensity and marital communication and problem-solving difficulties in parents of children with ASD [6,10,17,18,19,28,33]. Following intervention, scores within normal range were obtained on the six aforementioned sub-scales only for the treatment group. Specifically, the following areas were improved: emotional responsiveness, communication, behavior control and allocating roles and responsibilities, and problem solving. To our knowledge, this is the first study that demonstrates improved communication and problem-solving skills in parents of children with ASD, following the application of a psychoeducational treatment program, in contrast to prior findings [6,63,64]. As pointed out, lack of improvement in those two domains may have been attributed to the short duration of the psychoeducational intervention applied in earlier studies. The effectiveness of the present psychoeducational model may be attributed to its duration (long-term application) and to the fact that it included group psychological counselling and social support among group members [64,66].
- On the FRS, prior to intervention, the scores obtained indicated serious disruption in family rituals and routines. These findings were anticipated, since the FRS assesses engagement of family members in activities, such as family traditions or religious holidays, family celebrations and trips, and patterned routines (e.g., eating together on Sundays, cooking special meals, going out on weekends) – areas in which most families with a child with ASD encounter great disruption [50]. Following intervention, statistically significant improvements were noted in all the aforementioned areas. These findings are consistent with prior findings pertaining to psychoeducational therapeutic programs applied to families of other clinical populations [25,30].
- On the FBS, which assesses subjective and objective burden, it is worth noting that prior to treatment parental burden was within marginal normal range (slightly below the cutoff point). This finding was unexpected, in light of the relevant literature worldwide that underlines high levels of family burden due to the strain associated with raising a child with ASD [10,14,67,68,69]. This finding may be attributed to the fact that the children of all families who participated had been receiving behavior analytic treatment for several years. Thus, service needs of the children of those families were met to a satisfactory degree, which, according to empirical findings, is an important factor for reducing family burden[70]. Additional tentative explanations relate to culturally bound differences, since anecdotal data suggest that Mediterranean parents, and particularly mothers, refuse to perceive or to admit that their offspring with a handicap is a “burden” [24,30]. Following intervention, statistically significant reductions were noted by all parents in (a) family social isolation, (b) behavior outbursts of the child with ASD, and (c) the emergence of psychosomatic health issues as a result of extending provision of care. This is a crucial finding since there is limited evidence about the effectiveness of group psychoeducation programs in decreasing objective and subjective burden of families with a member with ASD [33,68,71].
Qualitative data were collected for both the treatment and the control groups and were obtained through individual semi-structured interviews before and after intervention. Prior to intervention, no systematic differences were noted between the two groups. Following intervention, no systematic changes were reported by the control group, whereas several improvements were reported by the participants of the treatment group. Specifically, the following improvements were reported:
- Parents reported more accurate information about the etiology and the characteristics of ASD and appreciated the importance of early intervention and of parent training in behavior management and in problem-solving with the aim to achieve optimal outcomes. Those findings are consistent with the existing literature related to the benefits of psychoeducation and parent training on parental skills and knowledge pertaining to ASD [33,72,73].
- Thematic analysis of parental reports reflected major improvements on social- and on self-stigma management. Namely, parents shifted from parental social withdrawal, avoidance of public places, shame, and embarrassment for their child’s behavior to active social networking with other group members and relatives and a proactive tendency to inform other people about their offspring’s disability, mainly by organizing outdoor activities and by participating actively in public events. Pertaining to self-stigma, parents shifted from self-blame, a sense of failure in the parental role, fear of social judgement and social rejection to a sense of efficacy in the parental role and a sense of pride for being a parent of a child with ASD. Those shifts may work as a buffer against cultural reactions to aberrant behavior (e.g., staring, rude comments, or avoiding interaction), since having a more accurate understanding of ASD is identified as one of the critical factors for empowering families against stigma [33,72,73].
4.1. Study Limitations and Implications for Future Research
The current study has several limitations. The first limitation pertains to the small size and to the non-random selection of the sample. Both of those limitations compromise the generalization or the external validity of the findings. It would be important for future research to replicate the present study with a larger sample.
Another factor that limits the external validity of the present study is the familiarity of the participants with the research settings. Parents’ attendance and commitment to the psychoeducational group sessions was high, which may be attributed to this familiarity and may have led to the establishment of a strong therapeutic alliance between the therapists who led the sessions and the group members. Thus, the findings of the present study may not be generalized to services offered in settings that are unfamiliar to the participating parents. Furthermore, the extent to which previously existing therapeutic alliance and trust contributed to the effectiveness of the group intervention is not systematically assessed in this study and remains to be examined in future research [33,50].
Post-treatment assessment was conducted one month following completion of the intervention but long-term maintenance was not systematically assessed. There are only anecdotal data that provide support for maintenance. Specifically, the participating parents reported that they continued to have a closer and mutually supportive relationship with their spouse. In addition, the participating couples reported that they developed social ties amongst themselves. It would be important to investigate whether long-term psychoeducation could possibly help parents to maintain self-determination, a sense of coherence, family empowerment, peer-to-peer support, and long-lasting coping with stigma.
The duration of the group therapeutic intervention was over 12 months and was carried out on a bi-weekly basis. It would be important to investigate whether a more cost-effective, short-term group psychoeducational program could lead to similar outcomes. According to prior research, it was suggested that a minimum of an 18-month duration was necessary for the therapeutic effects of a psychoeducational program to be maintained [38]. In addition, manualizing the treatment protocol may contribute to replication of the present study with greater precision [33]. In summary, future research efforts may address issues that improve the external validity of the findings and assess the effectiveness of the different parameters of the intervention as a means of building group family psychoeducational interventions that address the needs of families of children with ASD. Finally, it would be worth investigating sociodemographic and other family or child variables (e.g., age or severity of difficulties) that may attribute to treatment outcomes.
5. Conclusion
This study aimed to fill a research gap in supporting families of children with ASD through the application of a group psychoeducation intervention that was designed to address specifically the needs of such families, and draws from prior evidence-based research with families with a member with other chronic disorders. The analysis of both quantitative and qualitative data of this pilot study replicate prior findings about the importance of psychoeducational interventions and provides evidence that long-term group family psychoeducation, promoting a better awareness of ASD and its treatment, the development of effective communication and problem-solving skills among family members, and the management of stigma may greatly improve family dynamics in terms of improving engagement in family rituals and routines and overall family functioning, as well as minimizing family burden, which are all factors positively associated with the family’s quality of life and may serve as the foundation for social rehabilitation of families raising a child with ASD.
Author Contributions
Conceptualization, Angeliki Gena, and Ioanna Tsiouri; methodology, Angeliki Gena and Ioanna Tsiouri; software, Ioanna Tsiouri; validation, Angeliki Gena and Ioanna Tsiouri and two undergraduate students; Formal analysis, Ioanna Tsiouri (two undergraduate students); Investigation, Angeliki Gena and Ioanna Tsiouri; resources, Angeliki Gena; data curation, Ioanna Tsiouri; writing—original draft preparation, Ioanna Tsiouri; writing—review and editing, Angeliki Gena ; visualization, Ioanna Tsiouri.; supervision, Angeliki Gena ; project administration, Angeliki Gena; funding acquisition, N/A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the research ethics committee of the National and Kapodistrian University of Athens (NKUA) and of the ISBA (project identification code and date: 78/7-9-2017).
Informed Consent Statement
Parents were contacted, in person, to discuss the purpose and procedures of the study. Written informed consent was obtained from all twelve parents prior to the beginning of the study and written informed consent has been obtained from the parents to publish this paper.
Data Availability Statement
The raw data supporting the conclusions of this article are unavailable due to privacy and ethical restrictions applied, because of the sensitivity of parental reports and the small size of the research sample. .
Acknowledgments
The authors would like to thank the parents, who voluntarily participated in this research project, as well as the undergraduate students who voluntarily supported the data collection and served as interobservers for reliability purposes.
Conflicts of Interest
“The authors declare no conflicts of interest.”.
Abbreviations
The following abbreviations are used in this manuscript:
| ASD | Autism spectrum disorder |
| ISBA | Institute of systemic behavior analysis |
| DCH II | Day Center Hara II |
| FAD | Family assessment device |
| FRS | Family ritual scale |
| FBS | Family burden scale |
| NKUA | National and kapodistrian university of Athens |
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders-DSM-5-TR. 5th ed.; American Psychiatric Publishing, Washington DC., 2022; pp.125-132. [CrossRef]
- World Health Organization. Autism spectrum disorders. Available online: https://communitymedicine4asses.wordpress.com/2023/03/31/who-updates-fact-sheet- on-autism-29-march-2023/ (accessed on 29 October 2024).
- Zhou, H.; Xu, X.; Yan, W.; Zou, X.; Wu, L.; Luo, X. & LATENT-NHC Study Team. Prevalence of autism spectrum disorder in China: a nationwide multi-center population- based study among children aged 6 to 12 years. Neuroscience Bulletin 2020, 36, 961–97. [Google Scholar] [CrossRef]
- Maenner, M.J.; Warren, Z.; Williams, A.R.; Amoakohene, E.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Fitzgerald, R.T.; Furnier, S.M.; Hughes, M.M.; Ladd-Acosta, C.M.; McArthur, D.; Pas, E.T.; Salinas, A.; Vehorn, A.; Williams, S.; Esler, A.; Grzybowski, A.; Hall-Lande, J.; Nguyen, R.H.N.; … Shaw, K.A. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. Morbidity and mortality weekly report. Surveillance summaries Washington, D.C. 2002, 72, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Fenning, R.M.; & Butter, E.M. ; Johnson, E.M. Butter, & L. Scahill (Eds.), Parent training for autism spectrum disorder. In C. R.; Johnson, E.M. Butter, & L. Scahill (Eds.), Parent training for autism spectrum disorder: Improving the quality of life for children and their families. American Psychological Association, 2020; Johnson, E.M. Butter, &. [Google Scholar] [CrossRef]
- DaWalt, L.S.; Greenberg, J.S.; & Mailick, M.R. ; & Mailick, M. R. Transitioning Together: A Multi-family Group Psychoeducation Program for Adolescents with ASD and Their Parents. Journal of autism and developmental disorders, 2018, 48, 251–263. [Google Scholar] [CrossRef]
- Pillay, M.; Alderson-Day, B.; Wright, B.; Williams, C.; Urwin, B. Autism Spectrum Conditions--enhancing Nurture and Development (ASCEND): an evaluation of intervention support groups for parents. Clinical child psychology and psychiatry 2011, 16, 5–20. [Google Scholar] [CrossRef]
- Rivard, M.; Terroux, A.; Parent-Boursier, C.; Mercier, C. Determinants of stress in parents of children with autism spectrum disorders. Journal of Autism and Developmental Disorders 2014, 44, 1609–1620. [Google Scholar] [CrossRef]
- Bishop-Fitzpatrick, L.; Mazefsky, C.A.; Minshew, N.J.; Eack, S.M. The Relationship Between Stress and Social Functioning in Adults With Autism Spectrum Disorder and Without Intellectual Disability. Autism Res, 2015, 8:164-173. [CrossRef]
- Gena, A.; Balamotis, G. H Oikogeneia tou Paidiou me Aftismo. Tomos A΄. Oi Goneis. Gutenberg, Athens, Greece, 2013; 124-127.
- Hayes, S.A.; Watson, S.L. The impact of parenting stress: a meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. Journal of autism and developmental disorders 2013, 43, 629–642. [Google Scholar] [CrossRef]
- Ruiz-Robledillo, N.; Moya-Albiol, L. Lower electrodermal activity to acute stress in caregivers of people with autism spectrum disorder: an adaptive habituation to stress. Journal of autism and developmental disorders 2015, 45, 576–588. [Google Scholar] [CrossRef]
- Gau, S.S.F.; Chou, M.C.; Chiang, H.L.; Lee, J.C.; Wong, C.C.; Chou, W.J.; Wu, Y.Y. Parental adjustment, marital relationship, and family function in families of children with autism. Research in Autism spectrum disorders 2011, 6, 263–270. [Google Scholar] [CrossRef]
- Lavelle, T.A.; Weinstein, M.C.; Newhouse, J.P.; Munir, K.; Kuhlthau, K.A.; Prosser, L.A. Economic burden of childhood autism spectrum disorders. Pediatrics 2011, 133, e520–e529. [Google Scholar] [CrossRef]
- Kavaliotis, P. Accurate Diagnosis of the Syndrome in Children with Autism Spectrum Disorders and Parents’ Resilience. Journal of Educational and Developmental Psychology 2017, 7, 218. [Google Scholar] [CrossRef]
- Piro-Gambetti, B.; Greenlee, J.; Hickey, E.J.; Putney, J.M.; Lorang, E.; Hartley, S.L. Parental Depression Symptoms and Internalizing Mental Health Problems in Autistic Children. Journal of autism and developmental disorders 2023, 53, 2373–2383. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.K.; Seltzer, M.M.; & Greenberg, J.S. ;& Greenberg, J. S. Longitudinal effects of adaptability on behavior problems and maternal depression in families of adolescents with autism. Journal of Family Psychology 2011, 25, 601–609. [Google Scholar] [CrossRef]
- Greenberg, L.S.; Pascual-Leone, A. Emotion in psychotherapy: A practice-friendly research review. J. Clin. Psychol. 2006, 62: 611-630. [CrossRef]
- Hastings, R.P.; Lloyd, T. (Expressed emotion in families of children and adults with intellectual disabilities. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13: 339-345. [CrossRef]
- Woodman, A.C.; Smith, L.E.; Greenberg, J.S.; Mailick, M.R. Contextual Factors Predict Patterns of Change in Functioning over 10 Years Among Adolescents and Adults with Autism Spectrum Disorders. Journal of autism and developmental disorders 2016, 46, 176–189. [Google Scholar] [CrossRef]
- Jungbauer, J.; Wittmund, B.; Dietrich, S.; Angermeyer, M.C. Subjective burden over 12 months in parents of patients with schizophrenia. Archives of psychiatric nursing 2003, 17, 126–134. [Google Scholar] [CrossRef]
- Lauber, C.; Nordt, C.; Falcato, L.; Rössler, W. Do people recognize mental illness? Factors influencing mental health literacy. European archives of psychiatry and clinical neuroscience 2003, 253, 248–251. [Google Scholar] [CrossRef]
- Magliano, L.; Fiorillo, A.; De Rosa, C.; Maj, M.; Family burden and social network in schizophrenia, vs. physical diseases: preliminary results from an Italian national study. Acta Psychiatrica Scandinavica 2006, 113: 60-63. [CrossRef]
- Grandón, P.; Jenaro, C.; Lemos, S. Primary caregivers of schizophrenia outpatients: burden and predictor variables. Psychiatry research 2008, 158, 335–343. [Google Scholar] [CrossRef]
- Madianos, M.; Economou, M.; Dafni, O.; Koukia, E.; Palli, A.; Rogakou, E. (Family disruption, economic hardship and psychological distress in schizophrenia: can they be measured? . European psychiatry : the journal of the Association of European Psychiatrists 2004, 19, 408–414. [Google Scholar] [CrossRef]
- Nasr, T.; Kausar, R. Psychoeducation and the family burden in schizophrenia: a randomized controlled trial. Annals of general psychiatry 2009, 8, 17. [Google Scholar] [CrossRef]
- Ağırkan, M.; Koç, M.; Avcı, Ö.H. How effective are group-based psychoeducation programs for parents of children with ASD in Turkey? A systematic review and meta-analysis. Research in Developmental Disabilities 2023, 139, 104554. [Google Scholar] [CrossRef]
- Gupta, A.; Singhal, N. Psychosocial support for families of children with autism. Asia Pacific Disability Rehabilitation Journal 2005, 16, 62–83. [Google Scholar]
- Epstein, N.B.; Baldwin, L.M.; Bishop, D.S. The McMaster family assessment device. Journal of marital and family therapy 1983, 9, 171–180. [Google Scholar] [CrossRef]
- Tsiouri, I.; Gena, A.; Economou, M.P.; Bonotis, K.S.; Mouzas, O. Does Long-Term Group Psychoeducation of Parents of Individuals with Schizophrenia Help the Family as a System? A Quasi-Experimental Study. International Journal of Mental Health 2015, 44, 316–331. [Google Scholar] [CrossRef]
- Tsujita, M.; Homma, M.; Kumagaya, S.I.; Nagai, Y. (Comprehensive intervention for reducing stigma of autism spectrum disorders: Incorporating the experience of simulated autistic perception and social contact. PloS one 2023, 18, e0288586. [Google Scholar] [CrossRef]
- Dubreucq, J.; Plasse, J.; Franck, N. Self-stigma in Serious Mental Illness: A Systematic Review of Frequency, Correlates, and Consequences. Schizophrenia bulletin 2021, 47, 1261–1287. [Google Scholar] [CrossRef]
- Kollia, S.E.; Tsirempolou, E.; Gena, A. Encouraging the efforts of the family system: A psychoeducational therapeutic intervention for parents of children with Autism Spectrum Disorder (ASD). Cogn.-Behav. Res. Ther 2020, 6, 47–51. [Google Scholar]
- Lopez, J.; Crespo, M.; Zarit, S. (Assessment of the Efficacy of a Stress Management Program for Informal Caregivers of Dependent Older Adults. The Gerontologist 2007, 47, 205–214. [Google Scholar] [CrossRef]
- Sorrell, J.M. Moving beyond caregiver burden: identifying helpful interventions for family caregivers. Journal of psychosocial nursing and mental health services 2014, 52, 15–18. [Google Scholar] [CrossRef]
- Van Mierlo, L.D.; Van der Roest, H.G.; Meiland, F.J.; Dröes, R.M. Personalized dementia care: proven effectiveness of psychosocial interventions in subgroups. Ageing research reviews 2010, 9, 163–183. [Google Scholar] [CrossRef]
- Falloon, I.R.; Liberman, R.P. Interactions between drug and psychosocial therapy in schizophrenia. Schizophrenia bulletin 1983, 9, 543–54. [Google Scholar] [CrossRef]
- Falloon, I.R. Family interventions for mental disorders: efficacy and effectiveness. World psychiatry : official journal of the World Psychiatric Association (WPA) 2003, 2, 20–28. [Google Scholar]
- Yu, Y.; McGrew, J.H.; Boloor, J. Effects of caregiver-focused programs on psychosocial outcomes in caregivers of individuals with ASD: A meta-analysis. Journal of Autism and Developmental Disorders 2019, 49, 4761–4779. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.M.; Hogarty, G.E.; Reiss, D.J. Family treatment of adult schizophrenic patients: A psycho-educational approach. Schizophrenia Bulletin 1980, 6, 490–505. [Google Scholar] [CrossRef] [PubMed]
- Falloon, I.R.H.; McGill, C.W.; Boyd, J.L.; Pederson, J. Family management in the prevention of morbidity of schizophrenia: social outcome of a two-year longitudinal study. Psychological Medicine 1987, 17, 59–66. [Google Scholar] [CrossRef]
- Lucksted, A.; McFarlane, W.; Downing, D.; Dixon, L. Recent Developments in Family Psychoeducation as an Evidence-Based Practice. Journal of Marital and Family Therapy 2012, 38: 101-121. [CrossRef]
- Tessier, A.; Roger, K.; Gregoire, A.; Desnavailles, P.; Misdrahi, D. Family psychoeducation to improve outcome in caregivers and patients with schizophrenia: a randomized clinical trial. Frontiers in psychiatry 2023, 14, 1171661. [Google Scholar] [CrossRef]
- Bäuml, J.; Froböse, T.; Kraemer, S.; Rentrop, M.; & Pitschel-Walz, G. Psychoeducation: a basic psychotherapeutic intervention for patients with schizophrenia and their families. Schizophrenia bulletin 2006, 32(suppl_1), S1-S9. [CrossRef]
- Chiquelho, R.; Neves, S.; Mendes, A.; Relvas, A.P.; Sousa, L. ProFamilies: a psycho-educational multi-family group intervention for cancer patients and their families. European journal of cancer care 2011, 20, 337–344. [Google Scholar] [CrossRef]
- McFarlane, W.R.; Dixon, L.; Lukens, E.; Lucksted, A. Family psychoeducation and schizophrenia: a review of the literature. Journal of marital and family therapy, 2003, 29, 223–245. [Google Scholar] [CrossRef]
- Motlova, L.; Dragomirecka, E.; Spaniel, F. Relapse prevention in schizophrenia: does group family psychoeducation matter? One-year prospective follow-up field study. Int J Psychiatry Clin Pract. 2006, 10:38-44. [CrossRef]
- Pilling, S.; Bebbington, P.; Kuipers, E. Psychological treatments in schizophrenia: Meta-analysis of family intervention and cognitive behaviour therapy. Psychol Med. 2002, 32:763-782. [CrossRef]
- Rummel-Kluge, C.; Kissling, W. Psychoeducation in schizophrenia: new developments and approaches in the field. Current opinion in psychiatry 2008, 21, 168–172. [Google Scholar] [CrossRef]
- Solomon, A.H.; Chung, B. Understanding autism: how family therapists can support parents of children withautism spectrum disorders. Family process 2012, 51, 250–264. [Google Scholar] [CrossRef]
- Tanrıverdi, D.; Ekinci, M. The effect psychoeducation intervention has on the caregiving burden of caregivers for schizophrenic patients in Turkey. International Journal of Nursing Practice 2012, 18: 281-288. [CrossRef]
- Young, M.E.; Fristad, M.A. Evidence based treatments for bipolar disorder in children and adolescents. Journal of Contemporary Psychotherapy: On the Cutting Edge of Modern Developments in Psychotherapy 2007, 37, 157–164. [Google Scholar] [CrossRef]
- Young, D.K.; Ng, P.Y.; & Cheng, D. ; & Cheng, D. Psychoeducation Group on Improving Quality of Life of Mild Cognitive Impaired Elderly. Research on Social Work Practice 2019, 29, 303–310. [Google Scholar] [CrossRef]
- Bearss, K.; Johnson, C.; Smith, T.; Lecavalier, L.; Swiezy, N.; Aman, M.; Scahill, L. Effect of parent training vs parent education on behavioral problems in children with autism spectrum disorder: A randomized clinical trial. Jama 2015, 313, 1524–1533. [Google Scholar] [CrossRef]
- Madianos, M.; Economou, M. Schizophrenia and family rituals: measuring family rituals among schizophrenics and “normals. ” European Psychiatry 1994, 9, 45–51. [Google Scholar] [CrossRef]
- Statharou, A.; Papathanasiou, I.; Gouva, M. ; Masdrakis,V. Interdisciplinary Health Care 2011, 3(2), 59–69. [Google Scholar]
- DeWinter, J., (2013) “Using the Student's t-test with extremely small sample sizes”, Practical Assessment, Research, and Evaluation 18: 10.
- Falloon IRH.; Boyd JL.; McGill CW.. Family Management in the Prevention of Morbidity of Schizophrenia: Clinical Outcome of a Two-Year Longitudinal Study. Arch Gen Psychiatry. 1985, 42:887–896. [CrossRef]
- Falloon, I.R.; McGill, C.W.; Matthews, S.M.; Keith, S.J.; & Schooler, N.R. ; & Schooler, N. R. Family treatment for schizophrenia : the design and research application of therapist training models. The Journal of psychotherapy practice and research( 1996, 5, 45–56. [Google Scholar]
- Dieleman, L.M.; Moyson, T.; De Pauw, S.S.W.; Prinzie, P.; Soenens, B. Parents' Need-related Experiences and Behaviors When Raising a Child With Autism Spectrum Disorder. Journal of pediatric nursing 2018, 42, e26–e37. [Google Scholar] [CrossRef]
- DePape, A.M.; Lindsay, S. Parents' experiences of caring for a child with autism spectrum disorder. Qualitative health research 2015, 25, 569–583. [Google Scholar] [CrossRef]
- Bonis, S. Stress and Parents of Children with Autism: A Review of Literature. Issues in Mental Health Nursing 2016, 37, 153–3. [Google Scholar] [CrossRef]
- Scholtz, S.E.; de Klerk, W.; de Beer, L.T. The Use of Research Methods in Psychological Research: A Systematised Review. Frontiers in research metrics and analytics 2020, 5, 1. [Google Scholar] [CrossRef]
- Ardic, A.; Cavkaytar, A. The effect of the psychoeducational group family education program for families of children with ASD on parents: A pilot study. International Journal of Early Childhood Special Education 2019, 11, 1–17. [Google Scholar] [CrossRef]
- Güler, G.; Bedel, A. The Effect of Group Guidance Program on Family Stress and Burnout Levels for Parents of Children with Special Needs. Psycho-Educational Research Reviews 2024, 13, 77–89. [Google Scholar] [CrossRef]
- Dixon, L.; Adams, C. ; & Lucksted, AUpdate on family psychoeducation for schizophrenia. Schizophrenia bulletin 2000, 26, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Bhuiyan, M.R. ; Islam, M. Z. Coping Strategies for Financial Burden of Family for the Children with Autism Spectrum Disorder. Bangladesh Armed Forces Medical Journal 2024, 56, 56, 38–44. [Google Scholar] [CrossRef]
- Zhao, Y.; Lu, F.; Wang, X.; Luo, Y.; Zhang, R.; He, P.; Zheng, X. The economic burden of autism spectrum disorder with and without intellectual disability in China: A nationwide cost-of-illness study. Asian journal of psychiatry 2024, 92, 103877. [Google Scholar] [CrossRef] [PubMed]
- Picardi, A.; Gigantesco, A.; Tarolla, E.; Stoppioni, V.; Cerbo, R.; Cremonte, M.; Alessandri, G.; Lega, I.; Nardocci, F. Parental Burden and its Correlates in Families of Children with Autism Spectrum Disorder: A Multicentre Study with Two Comparison Groups. Clinical practice and epidemiology in mental health: CP&EMH 2018, 14, 143–176. [Google Scholar] [CrossRef]
- Montenegro, M.C.; Abdul-Chani, M.; Valdez, D.; Rosoli, A.; Garrido, G.; Cukier, S.; Paula, C.S.; Garcia, R.; Rattazzi, A.; Montiel-Nava, C. Perceived Stigma and Barriers to Accessing Services: Experience of Caregivers of Autistic Children Residing in Latin America. Research in developmental disabilities 2022, 120, 104123. [Google Scholar] [CrossRef]
- Kaçan, H.; Gümüş, F.; Bayram Değer, V. Effect of individual psychoeducation for primary caregivers of children with autism on internalized stigma and care burden: a randomized controlled trial. International Journal of Developmental Disabilities 2023, 1–10. [Google Scholar] [CrossRef]
- McAleese, A.; Lavery, C.; & Dyer, K.F. ; & Dyer, K. F. Evaluating a psychoeducational, therapeutic group for parents of children with autism spectrum disorder. Child Care in Practice 2014, 20, 162–181. [Google Scholar]
- O'Donovan, K.L.; Armitage, S.; Featherstone, J.; McQuillin, L.; Longley, S.; Pollard, N. Group-based parent training interventions for parents of children with autism spectrum disorders: A literature review. Review Journal of Autism and Developmental Disorders 2019, 6, 85–95. [Google Scholar] [CrossRef]
- Deguchi, N.K.; Asakura, T.; Omiya, T. Self-Stigma of Families of Persons with Autism Spectrum Disorder: a Scoping Review. Rev J Autism Dev Disor. 2021, 8, 373–388. [Google Scholar] [CrossRef]
- Salleh, N.S.; Abdullah, K.L.; Yoong, T.L.; Jayanath, S.; Husain, M. Parents' Experiences of Affiliate Stigma when Caring for a Child with Autism Spectrum Disorder (ASD): A Meta-Synthesis of Qualitative Studies. Journal of pediatric nursing 2020, 55, 174–183. [Google Scholar] [CrossRef]
Figure 1.
Pre and post test mean scores across all FAD dimensions within the treatment group.
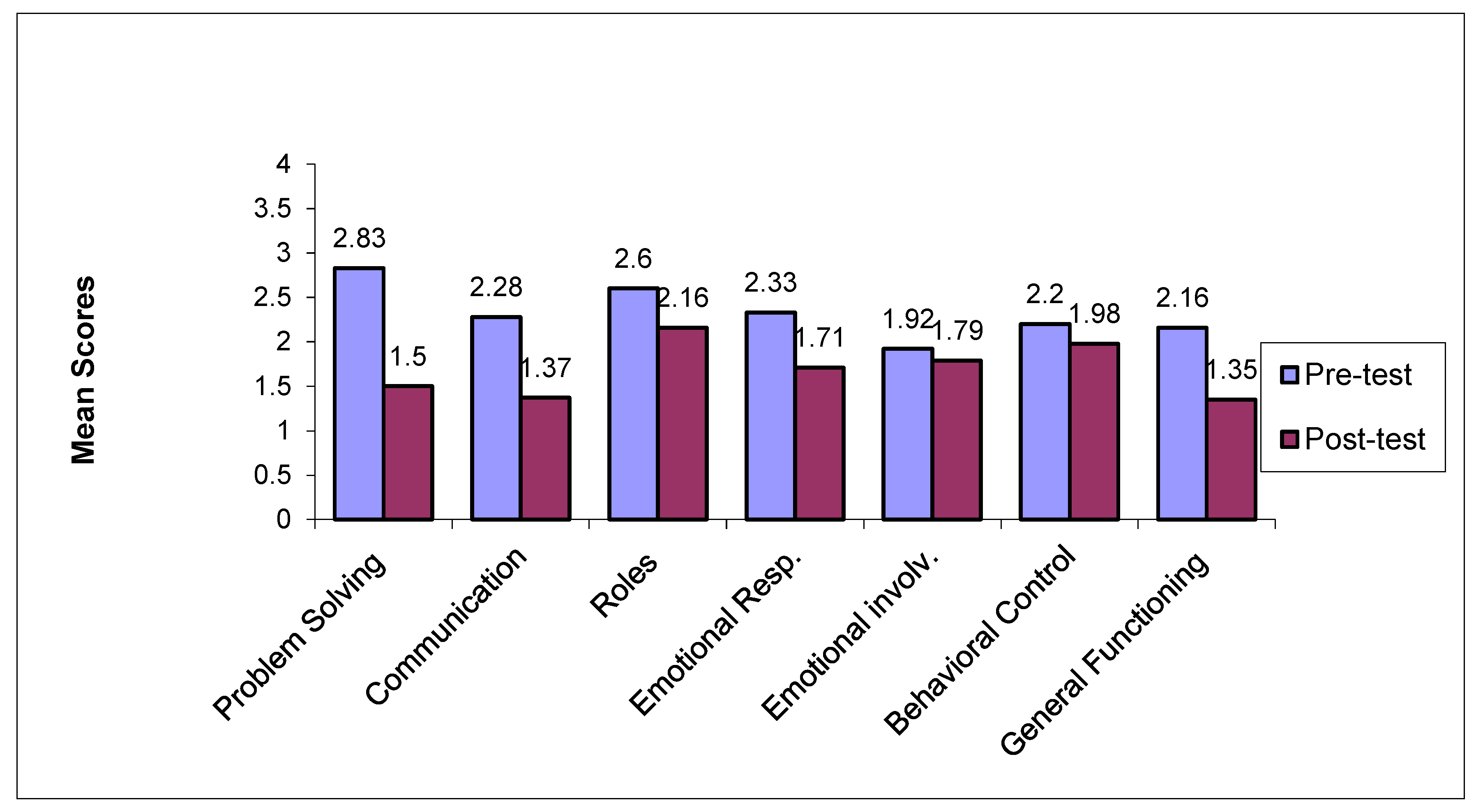
Figure 2.
Pre and post test mean scores across all FAD dimensions within the control group.
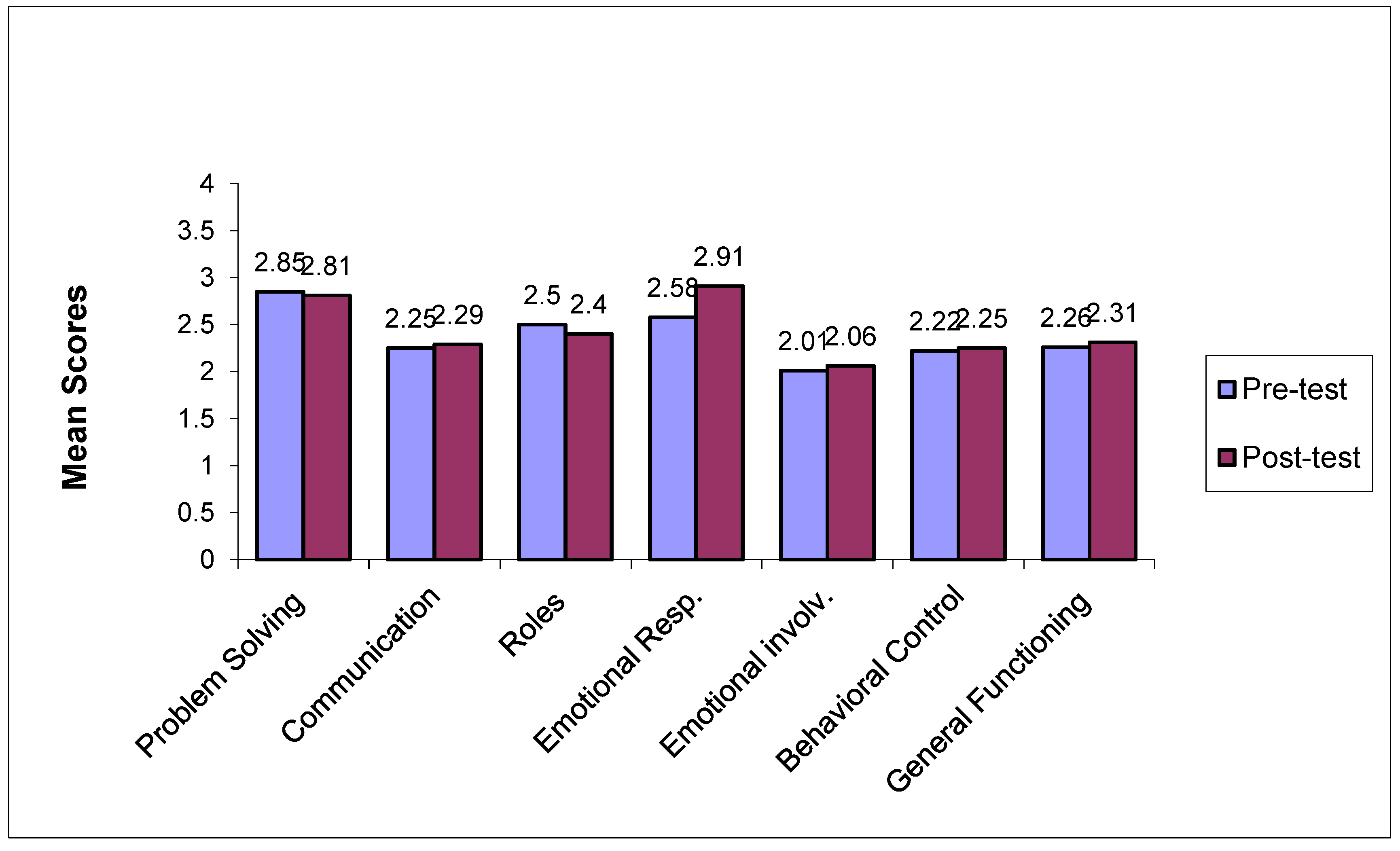

Table 1.
Sociodemographic Characteristics of the participating parents and their offsprings.
| Treatment Group N = 6 |
Control Group N = 6 |
Total Sample N = 12 |
||||
|---|---|---|---|---|---|---|
|
Sociodemographic Characteristics Parents |
M, or N | SD, or % | M, or N | SD, or % | M, or N | SD, or % |
| Fathers | 3 | 50% | 3 | 50% | 6 | 50% |
| Mothers | 3 | 50% | 3 | 50% | 6 | 50% |
| Age (M ± SD) | 40.83 | ±3.66 | 41.17 | ±4.6 | 41.00 | ±3.9 |
| Years of formal education (M ± SD) |
14.67 | ±4.0 | 13.33 | ±2.8 | 14.00 | ±3.3 |
|
Sociodemographic Characteristics of offsprings with ASD |
||||||
| Age (M ± SD) |
7.34 | ±2.55 | 6.45 | ±3.4 | 7.11 | ±3.2 |
| Years since initial diagnosis (M ± SD) |
5.00 | ±0.8 | 4.33 | ±1.3 | 4.67 | ±1.1 |
| Received specialized treatment services | ISBA | DCH II | ||||
| Intensity of treatment | < 3 hours per day | <3 hours per day | ||||
Table 2.
Content and Structure of Group Psychoeducational Intervention (treatment group).
| Topics per session | Sessions |
|---|---|
| A. Pre-test assessment | |
Individualized semi-structured interviews with each member of group to assess:
|
1 session per participant |
| Treatment group psychoeducational therapeutic program |
Duration (in 90 minute sessions) |
|
1 group session |
|
1 group session |
|
3 group sessions |
|
3 group session s |
|
10 group sessions |
|
5 group sessions |
|
1 group session |
| Total numberof treatment sessions | 23 group sessions |
| Post-test assessment | |
Individualized semi-structured interviews with each member of the group to assess
|
1 session per participant |
Table 3.
Mean scores on the FAD subscales pre and post-intervention for the treatmentgroup (N=6) and the control group (N=6).
Table 3.
Mean scores on the FAD subscales pre and post-intervention for the treatmentgroup (N=6) and the control group (N=6).
| Treatment Group (N=6) |
Control Group (N=6) |
Average Rank Between the two groups comparisons** |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| FAD subscales |
Pre-test Mean (±SD) |
Post-test Mean (±SD) |
z value* (p<.05) |
Pre-test Mean(±SD) |
Post-test Mean(± SD) |
z value* (p<.05) |
Treatment Group (N=6) |
Control Group (N=6) |
P |
|
|
Problem solving Cut-off=2.20 |
2.83 (0.37) | 1.50 ( 0.18) | -2.22 (p=.011) |
2.85 (0.4) | 2.81 (0.23) | –1.83 (p = 0.08) |
Pre | 8.39 | 8.61 | 0.668 |
| Post | 5.50 | 12.50 | 0.001 | |||||||
|
Communication Cut-off=2.20 |
2.28 (0.52) | 1.37 (0.29) | –2.21 (p = .017) |
2.25 (0.5) | 2.29 (0.3) | –0.61 (p = 0.32) |
Pre | 7.21 | 7.65 | 0.773 |
| Post | 3.50 | 11.20 | 0.01 | |||||||
|
Roles Cut-off=2.30 |
2.6 (0.3) | 2.16 (0.3) | –2.20 (p =0.011) |
2.5 (0.3) | 2.4 (0.3) | –0.41 (p = 0.43) |
Pre | 9.56 | 7.44 | 0.342 |
| Post | 8.42 | 8.58 | 0.08 | |||||||
|
Emotional response Cut-off =2.20 |
2.33 (0.7) | 1.71 (0.5) | –1.68 (p = .011) |
2.58 (0.3) | 2.91 (0.4) | –1.73 (p = 0.16) |
Pre | 8.44 | 8.56 | 0.923 |
| Post | 4.81 | 8.19 | 0.001 | |||||||
|
Emotional involvement Cut-off =2.10 |
1.92 (0.2) | 1.79 (0.1) | –2.03 (p = .611) |
2.01 (0.3) | 2.06 (0.4) | –1.41 (p = 0.72) |
Pre | 9.63 | 9.38 | 0.382 |
| Post | 5.00 | 9.12 | 0.002 | |||||||
|
Behavioral control Cut-off =1.90 |
2.20 (0.2) | 1.98 (0.1) | –1.92 (p = 0.04) |
2.22 (0.2) | 2.25 (0.2) | –0.32 (p = 0.12) |
Pre | 8.38 | 8.14 | 0.959 |
| Post | 6.15 | 8.08 | 0.05 | |||||||
|
General Functioning Cut-off =2.00 |
2.16 (0.3) | 1.35 (0.2) | –2.03 (p =0.012) |
2.26 (0.3) | 2.31 (0.3) | –0.08 (p = 0.33) |
Pre | 8.18 | 8.13 | 0.738 |
| Post | 5.44 | 8.56 | 0.007 | |||||||
* Wilcoxon matched pair signed rank test comparisons of pre and post-test scores within the treatment group and within the control group. ** Mann-Whitney U-test comparisons between the two groups at pre-test and post-test. .
Table 4.
Mean scores on the FRS and FBS and its subscales pre and post-intervention for the treatment group (N=6) and the control group (N=6).
Table 4.
Mean scores on the FRS and FBS and its subscales pre and post-intervention for the treatment group (N=6) and the control group (N=6).
|
Scales |
Treatment Group (N=6) |
Control Group (N=6) |
Average Rank Between the two groups comparisons** |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre-test Mean (±SD) | Post-test Mean (±SD) |
z value* (p<.05) |
Pre-test Mean (±SD) |
Post-test Mean (± SD) |
z value* (p<.05) |
Treatment Group (N=6) |
Control Group (N=6) |
P | ||
|
FRS Total Cut off score=18 |
20.17 (2.56) | 17.33 (2.16) | –2.27 (p = 0.027) |
22.50 (4.2) | 23.63 (4.2) | –1.61 (p = 0.08) |
Pre | 6.89 | 6.43 | 0.77 |
| Post | 4.38 | 12.23 | 0.01 | |||||||
|
FBS Total Cut off score=24 |
21.50 (5.11) | 13.5 (4.03) |
–2.22 (p = 0.026) |
22.30 (3.2) | 25.55 (3.6) | –1.02 (p = 0.06) |
Pre | 7.23 | 8.09 | 0.65 |
| Post | 6.62 | 11.94 | 0.02 | |||||||
| FBS Social life |
8.7 0(2.7) | 6.63 (3.9) | –2.73 (p = 0.03) |
9.53 (2.3) | 10.20 (2.2) | –0.33 (p = 0.14) |
Pre | 7.01 | 7.19 | 0.89 |
| Post | 6.19 | 10.31 | 0.04 | |||||||
| FBS Aggres/ness |
3.30 (2.7) | 2.37 (1.8) | –2.6 (p = 0.04) |
3.47 (4.2) | 3.80 (2.6) | –0.15 (p = 0.52) |
Pre | 6.54 | 6.76 | 0.89 |
| Post | 5.10 | 11.00 | 0.01 | |||||||
| FBS Health |
7.25 (2.1) | 3.13 (2.5) | –2.7 (p = 0.011) |
7.63 (3.5) | 8.00 (2.6) | –0.82 (p = 0.14) |
Pre | 8.55 | 8.14 | 0.83 |
| Post | 5.04 | 10.54 | 0.01 | |||||||
| FBS Financial |
2.25 (1.5) | 1.87 (1.3) | –1.4 (p > 0.05) |
2.37 (1.3) | 2.55 (1.3) | –0.34 (p = 0.53) |
Pre |
7.79 | 8.01 | 0.92 |
| Post | 7.12 | 8.31 | 0.69 | |||||||
*Wilcoxon matched pair signed rank test comparisons of pre and post-test scores within the treatment group and within the control group. ** Mann-Whitney U-test comparisons between the two groups at pre-test and post-test.
Table 5.
Pre and post treatment parents’ self-reports related to comprehension of the nature, causes, treatment of ASD and social and self-stigma management.
Table 5.
Pre and post treatment parents’ self-reports related to comprehension of the nature, causes, treatment of ASD and social and self-stigma management.
| 1.Knowledge about ASD | ||||
|---|---|---|---|---|
| Before N=12 (common themes for both treatment and control group) |
After N=6 (only treatment group/no pattern shift for control group) |
|||
| Areas | Themes | Example Quotes | Themes | Example Quotes |
| 1.1. Causes | -Psychological-Environmental | “I was stressed out during pregnancy, because of my father’s death”. “I spent too much time on the internet” “I was working long hours”: |
-Neurobiological -Genetic nature |
“Genetic disorder of a very complex nature” “It is a brain dysfunction that happened before birth” “ It is a metabolic disorder –an infection of the brain” |
| -Confusion -Luck or destiny |
“For me it is a confusing disorder that I find hard to understand” “Nobody knows, it was meant to happen to us” |
|||
| 1.2. Symptoms | Personality traits | “My child is an introvert person” “He is very self-absorbed” “He is very immature” “He is very stubborn” “He does not take no for an answer” |
Neurodevelopmental characteristics | “It is a developmental disorder that affects behavior at many levels (communication, emotional expression, play skills, social relations, self-help skills” “It is a neurological health issue. My daughter cannot communicate what she wants and this is why she has a lot of behavior issues”. |
| 1.3. Treatment | -Medical solution -Miracle |
“I hope for a miracle cure” “I pray to God, every day, for him to get well” |
-Psychoeductional programs for the child and the family | “I believe in intensive structured educational programs” “I believe in structure and everyday routines in conjunction with a supportive family atmosphere “ |
| 2. Stigma management | ||||
| 2.1. Social stigma | -Social withdrawal -Shame, anger, guilt |
”I avoid going to the playground with my child” “We are not invited anymore by relatives during the holidays” “I often feel embarrassed when I am in public places with my child “I feel that other people feel sorry for me” “I get really angry when people are staring at us! “ |
-Social networking within the group -Family activities -Social networking with the community and relatives -Need to educate community about ASD |
“I really enjoyed spending the holidays with one of the other families that I met during the group program“ “We are planning a family summer vacation” “We have invited my brother’s family over for Christmas” “I now believe that people understand how difficult raising a child with ASD might be and that they respect me” “I believe that ignorance is the reason for social stigma and that we should inform people about our child’s ASD” |
| 2.2. Self-stigma | -Sense of failure as a parent - Self-blame, self-pity -Increased parental stress |
“I believe that god is punishing me.” “I constantly feel guilty for not doing enough for my child” “I feel that everything is lost” “I feel stressed, wondering whether there is anything else I can do for my child that I cannot financially afford.” “I really don’t know how to handle his behaviors” “I am really worried about the future” |
-Empowerment -Need for advocacy |
“I am very proud that I have a special child, and I think that my son is proud of his parents too” “I really don’t care how other people see us. I just want my child to be happy” |
| -Satisfaction from the parental role | “I feel that we make one small step forward, everyday” “As a father I feel that I respond more and more to my child’s needs. “ |
|||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



