Submitted:
19 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
Myocardial infarction with nonobstructive coronary arteries (MINOCA) is an increasingly recognized condition, with a higher incidence in women, characterized by myocardial injury without significant coronary artery obstruction. Sex-specific differences play a critical role in its pathophysiology, clinical presentation, and response to treatment. While the underlying mechanisms of MINOCA are diverse—including coronary microvascular dysfunction, coronary spasm, plaque rupture, coronary dissection, and thromboembolism—women are more frequently affected by non-atherosclerotic causes, particularly coronary microvascular dysfunction and spontaneous coronary dissection. Etiological investigations, including coronary angiography with intracoronary imaging, functional tests and physiology assessment, are crucial for identifying underlying causes, and advanced non-invasive techniques, such as cardiac magnetic resonance imaging, provide valuable insights. Current therapeutic strategies, including antiplatelet agents, beta-blockers, and statins, are largely extrapolated from studies in obstructive coronary artery disease, with limited evidence on their efficacy in MINOCA, particularly in women. This review explores sex-specific differences in the pathophysiology, diagnostic evaluation, and management of MINOCA, emphasizing the need for tailored approaches to improve outcomes.
Keywords:
MINOCA
; myocardial infarction
; nonobstructive coronary arteries
; pathophysiology
; sex difference
; coronary microvascular dysfunction
; coronary spasm
; vasomotor function tests
; cardiac magnetic resonance imaging
; women
1. Introduction
Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA) refers to a clinical syndrome where patients present with myocardial injury despite the absence of hemodynamically significant coronary lesions (stenosis < 50%) on angiography [1]. It is a heterogeneous condition encompassing diverse pathophysiological mechanisms that lead to myocardial ischemia and necrosis in the absence of significant coronary obstruction. MINOCA can be further categorized into cases with no or minimal atherosclerosis (0–30% stenosis) and those with mild atherosclerosis (30–49% stenosis) [2]. Given its diverse etiologies, MINOCA should be considered an operational diagnosis that requires a systematic approach to identify the underlying cause in each patient. Establishing the diagnosis requires meeting the criteria for acute myocardial infarction (MI), as defined by the Fourth Universal Definition of Myocardial Infarction, while ruling out obstructive coronary artery disease [3]. Despite growing recognition, MINOCA remains underdiagnosed and frequently misclassified due to the complexities involved in identifying its underlying causes. Certain patient populations, particularly postmenopausal women, appear to be disproportionately affected [4]. This sex-related disparity highlights the need to explore potential differences in pathophysiological mechanisms, clinical presentation, and treatment response. While MINOCA can result from coronary plaque disruption, coronary spasm, coronary microvascular dysfunction, thromboembolism, and spontaneous coronary artery dissection (SCAD), emerging evidence suggests that women are more frequently affected by coronary microvascular dysfunction and vasospastic mechanisms, whereas men are more likely to have thromboembolic or atherosclerotic causes [5]. Given the increasing recognition of MINOCA, particularly among women, a deeper understanding of its pathophysiological mechanisms is essential for improving diagnostic accuracy and clinical management. Moreover, the absence of standardized treatment protocols and the potential differences in therapeutic response between men and women underscore the need for continued research in this field. This review provides a comprehensive examination of the epidemiology, pathophysiology, clinical presentation, diagnostic modalities, and management strategies for MINOCA, with a particular emphasis on sex-related differences. By exploring the unique characteristics of MINOCA in women, we aim to enhance awareness, improve patient care, and contribute to the development of sex-specific diagnostic and therapeutic strategies.
2. Epidemiology
MINOCA accounts for approximately 5% to 10% of all acute myocardial infarction (MI) cases. A meta-analysis encompassing 28 studies from 1995 to 2013 estimated that MINOCA represents around 6% of all myocardial infarctions [6]. Demographically, MINOCA patients tend to be younger, than those with myocardial infarction due to obstructive coronary artery disease (MI-CAD), with a mean age of 59 years compared to 61 years in MI-CAD patients. Notably, women are disproportionately affected, with multiple studies reporting that over 50% of MINOCA patients are female [7]. A comprehensive meta-analysis revealed that women constitute approximately 59.5% of MINOCA cases [8], despite representing only 25% of MI-CAD cases. Women presenting with MI are more than twice as likely as man to be diagnosed with MINOCA, whereas men are more frequently diagnosed with MI-CAD. The sex-related differences in MINOCA incidence may be attributed to distinct underlying pathophysiological mechanisms that are more prevalent in women, including coronary vasospasm and microvascular dysfunction [9]. Additionally, spontaneous coronary artery dissection (SCAD) occurs more frequently in women, particularly during the peripartum period [10]. These findings highlight the necessity of integrating sex-specific considerations into the diagnosis, management, and research of MINOCA to improve outcomes for this predominantly female patient population. In terms of cardiovascular risk factors, typically exhibit fewer traditional risk factors and a lower prevalence of prior or concurrent cardiovascular diseases compared to MI-CAD patients. However, hypertension appears to be equally prevalent in both groups [6,7]. Ethnically, MINOCA is more frequently observed among individuals of Black, Māori, or Pacific descent, as well as those of Hispanic ethnicity. Once considered a benign condition, MINOCA is now recognized as carrying significant long-term cardiovascular risk. A meta-analysis of 44 studies reported an annual mortality rate of 2.0% among MINOCA patients [11]. Additionally, affected individuals face an increased risk of recurrent MI, heart failure, and stroke [12]. Notably, the peak cardiac troponin level during a MINOCA event correlates with long-term mortality [13]. A systematic review found that the 12-month all-cause mortality for suspected MINOCA patients was 3.4%, with a major adverse cardiovascular event (MACE) rate of 9.6% [14]. These findings underscore the importance of recognizing MINOCA as a significant clinical entity requiring thorough evaluation and management.
3. Pathophysiology
The pathophysiology of MINOCA is diverse, encompassing both atherosclerotic and non-atherosclerotic mechanisms that contribute to myocardial ischemia and necrosis. A comprehensive understanding of these underlying processes is essential for accurate diagnosis and effective management. Sex-related differences have been increasingly recognized in the prevalence and mechanisms underlying MINOCA, with women more frequently affected by non-atherosclerotic causes, particularly coronary microvascular dysfunction, vasospasm and spontaneous coronary artery dissection and men more frequently affected by atherosclerotic causes.
3.1. Atherosclerotic Causes of Myocardial Necrosis
- Coronary plaque disruption
Coronary plaque disruption is frequently observed in patients with MINOCA and encompasses plaque rupture, plaque erosion, and calcified nodules. These disruptions can lead to luminal thrombus formation or plaque hemorrhage, either with or without concurrent coronary spasm. Plaque rupture, the most common cause of coronary thrombosis in men, occurs when a structural defect in the fibrous cap exposes the thrombogenic lipid-rich core of the atherosclerotic plaque to the bloodstream. Thrombi often contain dislodged plaque material, indicating that rupture and thrombosis occurred simultaneously. This process is associated with fibrous cap thinning, primarily driven by two mechanisms: (i) the depletion of vascular smooth muscle cells (VSMCs) within the fibrous cap, and (ii) macrophage infiltration leading to degradation of the collagen-rich cap matrix [15]. Plaque erosion is the second leading cause of coronary thrombosis. Unlike plaque rupture, it involves endothelial cell loss or dysfunction without a visible structural defect in the plaque. Although the underlying mechanisms remain incompletely understood, endothelial cell apoptosis and detachment from the extracellular matrix appear to play a role [16]. Additionally, vasospasm has been proposed as a contributor to endothelial damage and subsequent thrombosis [17]. Calcified nodules represent a less common cause of coronary thrombosis. Dysfunctional or sparse endothelial cells overlying these nodules can increase the risk of thrombosis. On optical coherence tomography (OCT), calcified nodules appear as signal-poor regions with irregular borders protruding into the arterial lumen. While angiography may suggest plaque disruption, such as through the presence of haziness or small filling defects, a definitive diagnosis requires intracoronary imaging. OCT, with its superior near-field resolution, or high-definition intravascular ultrasound (IVUS), are the preferred modalities. A large OCT-based study by Reynolds et al. identified a culprit lesion in 46.2% of women (67 of 145) with MINOCA, with plaque erosion being the most common findings [18]. Smaller studies have also demonstrated the utility of OCT in detecting etiologic plaques in suspected MINOCA cases [19,20].
3.2. Non-Atherosclerotic Causes of Myocardial Necrosis
- Coronary Artery Spasm
Coronary artery spasm can occur at different levels of the coronary circulation, affecting either the epicardial arteries or the coronary microvasculature. Epicardial coronary spasm is characterized by a transient near-total or complete (≥90% constriction), occlusion of large, proximal coronary artery, accompanied by angina and ischemic electrocardiographic changes, either occurring spontaneously or in response to a provocative stimulus. Vasospastic angina (VSA), also known as Prinzmetal angina, is a clinical syndrome defined by: (i) typical symptoms of vasospasm, (ii) documented myocardial ischemia during spontaneous episodes, and (iii) confirmed coronary artery spasm. Although spontaneous epicardial vasospasms can occur, provocative testing is often necessary to confirm heightened vasoreactivity and is recommended in patients with suspected VSA (class I) [21]. The two primary mechanisms underlying epicardial spasm are endothelial dysfunction and heightened VSMC reactivity [22]. Microvascular coronary spasm affects the small resistance vessels of the coronary circulation (diameter <200 μm), impairing myocardial perfusion despite the absence of significant stenosis in the epicardial arteries. This condition is a key mechanism underlying CMD, as will be further discussed in the following section, and is more prevalent among women. Patients with microvascular spasm often experience angina at rest or during emotional stress. A meta-analysis encompassing 25 studies with 14,554 patients found that epicardial spasm was more prevalent in men (61%), whereas microvascular spasm was more common in women (64%) [23]. Additionally, women are more likely to exhibit heightened coronary vascular sensitivity, experiencing pathological responses to lower doses of acetylcholine compared to men [24]. Smoking has been identified as a significant risk factor for epicardial spasm in young women, with an odds ratio of 7.7 for smokers women versus non-smokers women [25]. Identifying vasospasm is crucial, as it necessitates specific therapeutic strategies, including the use of calcium channel blockers and nitrates to prevent recurrent episodes [26], as we will later discuss.
- Coronary Microvascular Dysfunction
CMD is a condition characterized by four key criteria: (i) myocardial ischemia-related symptoms, (ii) the absence of obstructive CAD, (iii) objective evidence of myocardial ischemia, and (iv) impaired coronary microvascular function. The dysfunction of coronary microcirculation can be identified through various parameters, including: (i) a reduced coronary flow reserve (CFR) of less than 2.0 in response to a vasodilator, assessed via Doppler or thermodilution techniques; (ii) increased microvascular resistance, indicated by an index of microvascular resistance (IMR) exceeding 25; (iii) the coronary slow-flow phenomenon, defined as a thrombolysis in myocardial infarction (TIMI) frame count greater than 25; or (iv) microvascular spasm confirmed by provocative testing [27]. The gold standard for diagnosing CMD is invasive coronary function testing, which is advised for patients experiencing persistent angina despite nonobstructive coronary findings (class 2a recommendation) [28]. Noninvasive imaging alternatives include positron emission tomography (PET, class 2a), stress cardiac magnetic resonance (CMR) imaging (class 2a), and stress echocardiography with coronary flow velocity reserve measurement (class 2b) [28,29]. CMD s significantly more prevalent among women with MINOCA compared to men, reflecting sex-specific differences in coronary physiology and endothelial function. In a cohort of 40 female MINOCA patients who underwent stress CMR, two-thirds displayed inducible perfusion defects, suggesting the presence of CMD [30]. Among women with stable CMD, approximately 8% exhibited myocardial scarring on CMR in the Women’s Ischemia Syndrome Evaluation (WISE) study [31]. CMD results from either functional or structural abnormalities, or a combination of both [29]. Functional disturbances can involve excessive vasoconstriction due to microvascular spasm or impaired vasodilatory capacity [32]. The underlying mechanisms for increased microvascular constriction include Rho-kinase–mediated phosphorylation of myosin light-chain, inflammatory processes within the coronary microcirculation, and an increased presence of vasoconstrictive substances such as serotonin [33,34]. Impaired vasodilation in CMD may be due to endothelial dysfunction with reduced synthesis or effectiveness of vasodilatory molecules such as nitric oxide (NO), prostaglandins, and endothelium-derived hyperpolarizing factors [35]. Impaired vasodilation may be also endothelium-independent, with a diminished response to vasodilatory agents (such as adenosine, dipyridamole, and papaverine) and excessive sympathetic nervous system activity [29]. Structural changes, including luminal narrowing, vascular remodeling, reduced microvascular density, or extramural compression, may also contribute to CMD by increasing coronary microvascular resistance. Estrogen plays a crucial role in maintaining endothelial function by enhancing nitric oxide production and suppressing angiotensin 1 receptors and angiotensin-converting enzyme, thereby mitigating vasoconstriction induced by the renin-angiotensin system. Consequently, estrogen deficiency has been linked to increased endothelial dysfunction. This is one of the reasons why CMD is more frequent among post-menopausal women.
- Coronary embolism and thrombosis
Coronary thromboembolism is a less common but recognized cause of MINOCA. It can be categorized into three primary types: direct, iatrogenic, and paradoxical [36]. Direct embolism originates from embolic material dislodged from left-sided cardiac structures, including mural thrombi, infectious endocarditis, or intracardiac tumors such as myxomas [37]. Individuals with underlying cardiac conditions, such as cardiomyopathies (with or without impaired left ventricular function), atrial fibrillation, valvular disease, or coronary artery ectasia, have a heightened risk of direct embolism due to blood stagnation and reduced flow [36]. Although rare, infective endocarditis can also lead to coronary embolism, particularly in cases involving mitral valve infection, Staphylococcus aureus or fungal pathogens, and vegetations exceeding 10 mm in size [38]. Additionally, nonbacterial thrombotic endocarditis, or marantic endocarditis, has been reported as an infrequent cause of embolism [39]. Among cardiac tumors, myxomas with a villiform texture are more prone to embolization than those with smooth surfaces [37]. Iatrogenic coronary embolism typically occurs during coronary interventions but can also arise in the context of cardiac surgery or valvular procedures [36]. In contrast, paradoxical embolism results when embolic material from the systemic venous circulation bypasses pulmonary filtration due to a right-to-left shunt, such as a patent foramen ovale or atrial septal defect [40]. In situ coronary thrombosis may also be associated with inherited or acquired hypercoagulable disorders, the most frequent etiology among female population. Genetic predisposition to thrombosis was identified in 14% of MINOCA patients undergoing thrombophilia screening post-infarction, with abnormalities including factor V Leiden mutation, deficiencies in proteins C and S, and prothrombin gene mutations [6,41]. Acquired prothrombotic states that increase the risk of coronary thrombosis include conditions such as thrombotic thrombocytopenic purpura, antiphospholipid syndrome, heparin-induced thrombocytopenia, and myeloproliferative neoplasms [42]. In a prospective study of 84 MINOCA patients, 15.5% were diagnosed with antiphospholipid syndrome [43].
- Spontaneous Coronary Artery Dissection
SCAD refers to the separation of the coronary artery wall layers, accompanied by intramural hemorrhage, without any evidence of atherosclerotic disease, physical injury, or iatrogenic causes [2]. SCAD is increasingly recognized as a cause of acute myocardial infarction, necessitating a high level of suspicion, particularly in young women [44,45]. Over 90% of SCAD patients are female, with a significant proportion presenting before 50 years of age[46,47]. SCAD-related MI is estimated to account for 1%-5% of all AMI cases, rising to 35% in women under 50 years of age [31,44]. SCAD-related obstruction arises from the separation of the media and adventitia, leading to intramural hematoma formation. The "outside-in" hypothesis posits that the primary event is s vasa vasorum rupture, whereas the "inside-out" hypothesis suggests an intimal tear as the initial trigger [48,49]. SCAD may arise due to an underlying vasculopathy triggered by various stressors, such as catecholamine surges, emotional stress, intense physical exertion, sympathomimetic drug use, or hormonal changes [44,49]. Fibromuscular dysplasia was identified in 72% of patients from a cohort of 168 individuals with SCAD, with approximately half reporting a physical or emotional trigger [44]. Female sex hormones and pregnancy are also linked to SCAD, with most pregnancy-related MI events occurring within the first week postpartum [47]. The presence of coronary artery tortuosity (e.g., corkscrew appearance, multivessel symmetrical tortuosity) should raise suspicion for SCAD. To confirm the diagnosis, intravascular imaging techniques, such as OCT and IVUS, may be required to reveal the absence of significant atherosclerotic plaque and the presence of a dissection or intramural hematoma. OCT, with its higher spatial resolution, is often the preferred imaging method in suspected SCAD cases, though it should be used cautiously to avoid exacerbating the dissection by high-pressure contrast injection [50].
Figure 1 shows MINOCA pathophysiological mechanism.
3.3. Supply-Demand Mismatch
Supply-demand mismatch, known as type II MI, may lead to MINOCA. Approximately 50% of patients with type II MI do not have significant CAD, and they can be classified as MINOCA [4]. Stressors that reduce oxygen supply, like severe bradyarrhythmias, respiratory failure with profound hypoxemia, or significant anemia, can trigger a MINOCA. Conversely, stressors that increase oxygen demand, such as sustained tachyarrhythmias, extreme hypertension, or thyrotoxicosis, can also contribute [2]. In patients with stable CAD, an acute stress event causing ischemic symptoms may lead to MINOCA due to the inability of the heart to meet increased oxygen demands or further compromise in supply caused by the stressor. Depending on the clinical scenario, coronary angiography may be necessary to evaluate the presence of underlying CAD.
3.4. MINOCA Mimics
Several conditions that cause myocardial injury can be mistaken for MINOCA. In a study by Reynolds et al., 20.7% of patients with suspected MINOCA (24 out of 116) had nonischemic patterns on CMR imaging, such as myocarditis, takotsubo syndrome (TTS), or nonischemic cardiomyopathy [18].
4. Clinical Presentation
Patients with MINOCA commonly report chest pain that can resemble classic angina, often presenting as a pressure-like or constrictive discomfort in the chest, radiating to the left arm, jaw, or back. This pain may be precipitated by exertion or emotional stress and relieved by rest or nitroglycerin, like obstructive myocardial infarction. However, a significant proportion of patients, particularly women (69% compared to 58% of men), describe atypical symptoms such as nausea, epigastric discomfort, dizziness, dyspnea, or profound fatigue. These non-specific presentations frequently lead to misdiagnosis or a delay in seeking medical attention, as they are often attributed to non-cardiac conditions such as anxiety, musculoskeletal disorders, or gastrointestinal conditions. Emotional stress is a well-recognized precipitant, particularly in women [51]. Dyspnea is a common complaint especially in microvascular dysfunction. Some patients experience palpitations, which may be indicative of concurrent arrhythmic activity, particularly in cases of coronary spasm. Autonomic symptoms, including diaphoresis, nausea, and vomiting, are also frequently reported and may be more pronounced in women. The variability in symptom onset suggests that different pathophysiological mechanisms. Electrocardiographic (ECG) findings in MINOCA are variable and depend on the underlying pathophysiology. Many patients present with ST-segment elevation, while others exhibit non-ST elevation changes or non-specific T-wave abnormalities. ST-segment elevation is more commonly seen in cases associated with coronary spasm, whereas patients with microvascular dysfunction often demonstrate T-wave inversions or subtle ischemic changes. In some instances, ECG findings are normal at presentation. The presence of transient ECG abnormalities, such as dynamic ST-segment changes, suggests an underlying vasospastic component [18]. The degree of troponin elevation varies, and lower peak levels may be observed in cases driven by microvascular dysfunction rather than epicardial coronary occlusion. The discrepancy between symptom severity, ECG findings, and troponin levels often raises diagnostic uncertainty, necessitating further imaging and functional testing to establish the underlying etiology [6]. Another sex-specific consideration is that there are several nontraditional cardiac risk factors unique to or predominant in women, including early menopause or menarche, gestational diabetes mellitus, hypertension, preeclampsia, and eclampsia during pregnancy, as well as systemic inflammatory disorders. These factors contribute to endothelial dysfunction and microvascular abnormalities, increasing the susceptibility of women to MINOCA.
5. Diagnosis
The European Society of Cardiology (ESC) was the first international organization to develop formal diagnostic criteria for MINOCA [1]. Their proposed definition consists of three key components: (i) fulfillment of the criteria for acute myocardial infarction as outlined in the Third Universal Definition of Myocardial Infarction [1], (ii) confirmation of non-obstructive coronary arteries based on angiographic assessment, ensuring that no major epicardial coronary vessel has stenosis exceeding 50%, and (iii) exclusion of other overt clinical conditions that could account for the acute presentation. A fundamental aspect of this definition is the presence of myocardial injury, as evidenced by elevated cardiac troponin levels above the 99th percentile upper reference limit, with a characteristic rise and fall on serial testing. However, while troponin elevation signifies myocardial injury, it is not specific to ischemia, as non-ischemic conditions also lead to similar biomarker elevations. Recognizing this limitation, the Fourth Universal Definition of Myocardial Infarction, developed by a joint task force of the ESC, American College of Cardiology (ACC), American Heart Association (AHA), and World Heart Federation (WHF), introduced a revised framework for distinguishing myocardial injury from myocardial infarction [3]. Accordingly, the term MINOCA should be reserved exclusively for cases where an ischemic origin is identified as the cause of the clinical presentation. This necessitates a meticulous diagnostic approach when evaluating patients with suspected MI who lack significant coronary artery stenosis. To establish a diagnosis of MINOCA, clinicians must systematically rule out extracardiac causes of myocardial injury – such as sepsis, pulmonary embolism, aortic dissection – through the evaluation of clinical context, laboratory test and echocardiography. Subsequently, CMR can rule out cardiac causes of myocardial injury – such as myocarditis, TTS, and cardiomyopathies – and confirm myocardial infarction. Once these possibilities have been methodically ruled out through appropriate diagnostic investigations, a definitive diagnosis of MINOCA as a working diagnosis can be established. Finally, to define the underlying etiology it’s necessary to perform intravascular imaging (OCT and IVUS), intracoronary functional test (Ach/ergonovine) and coronary physiology assessment (FFR, CMR, IMR).
CMR is highly recommended as a critical tool in diagnosing MINOCA, as it can rule out conditions like myocarditis, TTS, and cardiomyopathies, as well as confirm MI. The reported prevalence of TTS and myocarditis in patients diagnosed with MINOCA at CMR varies significantly in the literature, ranging from 2% to 27% for TTS and 7% to 63% for myocarditis [6,20,52,53]. These differences can be attributed to factors such as the selection criteria for study participants, the timing of the CMR assessment, and the specific CMR techniques and diagnostic criteria employed. CMR with LGE allows for the evaluation of infarct location and size. However, in a significant proportion of cases (ranging from 8% to 73%) where myocarditis or TTS is excluded by CMR, a localized infarct is not detected by LGE [6,20,52,53,54]. Contemporary LGE imaging, using sequences with an average voxel size of 1.4×1.8×6 (-8) mm, requires a minimum of 0.2 g of infarcted myocardial tissue to be visible [55]. This threshold is higher than the amount of damaged myocardium needed to cause small but notable increases in cardiac troponin levels, which may account for the lack of visible infarction on CMR in many MINOCA patients. Nonetheless, it remains possible that the elevated troponin levels in these cases could be due to factors other than ischemic necrosis. Standard CMR protocols provide comprehensive evaluation of both cardiac anatomy and function, utilizing steady-state free precession (SSFP) MRI or cine imaging. They also assess tissue properties, with T2-weighted imaging sequences (T2w) and T2-weighted fat-suppressed sequences (T2wSTIR) being valuable for identifying localized edema. Additionally, T1-weighted imaging following LGE helps detect areas of acute cellular membrane damage or chronic myocardial scarring. The distribution of LGE can differentiate between myocardial infarction, which typically shows subendocardial or transmural enhancement, and myocarditis, which often exhibits a subepicardial or mid-wall pattern. TTS typically presents with apical and mid-ventricular edema, accompanied by transient dyskinesia in these regions, while the basal segments exhibit hyperkinesia, and no LGE is observed. Advancements in MRI technology have enhanced diagnostic accuracy. Parametric T1-mapping, which calculates extracellular volume (ECV), along with T2-mapping sequences, allows for precise pixel-by-pixel analysis of myocardial tissue characteristics. This approach assesses both extracellular and intracellular features, such as water content, which can indicate inflammation or edema. Moreover, T1 and T2 mapping can detect diffuse changes like generalized fibrosis, which are not visible with LGE [56]. The updated Lake Louise Criteria for CMR in myocardial inflammation incorporates mapping sequences, refining the imaging diagnosis by considering both T1 criteria (e.g., presence of LGE or increased T1-mapping or ECV values) and T2 criteria (e.g., hyperintensity in T2wSTIR or elevated T2-mapping values)[57]. The introduction of free-breathing LGE techniques has notably improved spatial resolution, making it five times more effective and allowing for the detection of smaller areas of necrosis. In a recent study, incorporating this enhanced sequence into standard imaging protocols enabled a definitive diagnosis in 48% of MINOCA patients who initially had normal scans [58]. The diagnostic accuracy of CMR is maximized when performed within 7 to 14 days of symptom onset. Delayed imaging can lead to the disappearance of certain pathological markers, such as myocardial edema in myocarditis. A study by Dastidar et al. compared retrospective scans of MINOCA patients and found that early CMR (within two weeks of admission) reduced inconclusive results from 43% to 16% [59]. This improvement was primarily due to better detection of Takotsubo syndrome and myocarditis. In patients with a MINOCA diagnosis, serial CMR scans revealed that myocardial edema and epicardial LGE patterns resolved in about one-quarter of cases within three weeks of admission. However, CMR is not universally accessible, so its use cannot be considered a mandatory diagnostic step for MINOCA.
Invasive testing includes intravascular imaging (OCT and IVUS), intracoronary functional testing (Ach, ergonovine) and coronary physiology assessment (FFR, CMR, IMR).
- Intravascular imaging (OCT and IVUS)
OCT is a high-resolution imaging technique used to characterize coronary plaque. It utilizes near-infrared light to capture detailed images of plaque components (fibrous cap, thrombus, and calcification) and the vessel wall (intima, media, adventitia). OCT offers better resolution (15-20 µm) than angiography. While well-established for assessing obstructive CAD, its role in MINOCA management remains underexplored. Few studies have shown OCT's effectiveness in detecting plaque rupture or thrombi in MINOCA cases, offering insights into its potential prognostic value. Yamamoto et al. (2019) reported that OCT identified abnormal findings in 25% of MINOCA patients with ischemic symptoms but angiographically non-obstructive lesions, including thrombus and plaque rupture [60]. In a comparison study, Usui et al. (2017) found that women with MINOCA had a higher prevalence of ruptured plaques and intraplaque hemorrhage, whereas women with obstructive CAD had more persistent thrombi [61]. Taruya et al. (2016) demonstrated OCT's prognostic value, finding hidden high-risk lesions in 51% of MINOCA patients. During follow-up, 10% of patients with these high-risk lesions developed ACS [62]. Similarly, a study by Mas-Lladò et al. (2020) revealed that OCT identified atherosclerotic plaques, spontaneous coronary dissection, and no findings in some MINOCA patients, further confirming its diagnostic utility [63]. A larger study by Zeng et al. (2022) found that 33.7% of MINOCA cases had atherosclerotic causes, with worse clinical outcomes compared to non-atherosclerotic causes, such as spontaneous dissection or coronary spasm [64]. Patients with atherosclerotic MINOCA had more adverse events, including major cardiac events, revascularizations, and rehospitalizations. In the context of SCAD, OCT provides valuable information for assessing the length of intramural hematomas, the extent of luminal compromise, and the thickness of a dissected tear. However, the risk of worsening the false lumen during contrast injection should be considered [65]. Limitations of OCT are related to the evaluation of proximal part of left main or right coronary artery or in case of coronary ectasia. IVUS employs a specialized catheter with a miniaturized ultrasound probe, offering a resolution of 100 μm. It uses ultrasonic technology, such as piezoelectric or capacitive micromachined ultrasound transducers, to visualize the endothelium through the blood column. Though IVUS can categorize atheromatous plaques into four types—soft, fibrous, calcified, and mixed—its spatial resolution limits detailed plaque classification. Research tools like Near-Infrared Spectroscopy (NIRS)-IVUS can provide insights into plaque lipid content. While OCT offers higher resolution for detailed endoluminal imaging, IVUS provides deeper tissue penetration (4-8 mm versus OCT’s 1-3 mm), making it effective for exploring outer plaque layers and assessing lipid content and vessel remodeling. IVUS is also better at visualizing calcified lesions and doesn't require contrast administration, making it the preferred option for patients with chronic kidney disease. IVUS is well-established for managing obstructive CAD during percutaneous revascularization, but its role in MINOCA management remains underexplored
- Intracoronary functional test (Ach, ergonovine)
Intracoronary acetylcholine testing is currently the preferred method to evaluate coronary epicardial and microvascular endothelium-dependent vasodilation and vasospasm. It involves intracoronary acetylcholine boluses (20–200 mcg) and subsequent assessment of the coronary response using invasive contrast angiography. The test is considered positive for macrovascular spasm if symptoms occur, accompanied by ischaemic ECG changes and an angiographic ≥90% reduction of the coronary lumen [66]. If the lumen reduction is <90%, the diagnosis of microvascular spasm is made. The vasospastic effect of Ach is rapidly transient and can, if needed, be reversed by intracoronary administration of nitroglycerine, which also allows assessment of endothelium-independent epicardial coronary vasodilation. Large registries have demonstrated that intracoronary acetylcholine bolus up to maximum 200 mcg in stable patients has a sustainable safety profile [67,68]. It should be performed after at least 24 hours of wash-out from CCB and nitrates. Use of intracoronary ergonovine boluses (20-60 mcg) is a possible alternative.
- Coronary physiology assessment (FFR, CMR, IMR)
For assessing flow-limiting obstructive coronary artery disease, fractional flow reserve (FFR) is used. FFR is the ratio of distal coronary pressure to aortic pressure at maximal hyperemia, with abnormal FFR values defined as ≤0.80, or a non-hyperemic pressure ratio ≤0.89. These values must be interpreted within the context of the individual patient's clinical situation. Data from stable patients suggest that up to a quarter of those with 30%-50% stenosis show functionally significant lesions when assessed using FFR. If FFR is utilized, it is recommended that only those with an FFR >0.80 be included as part of the MINOCA diagnosis [69]. Studies typically use a CFR cut-off of 2.0 for thermodilution or 2.5 for Doppler flow velocity as markers of prognostic significance [61,70]. Microvascular resistance is assessed by combining pressure and flow data. The index of microvascular resistance (IMR) is calculated as the product of distal coronary pressure during maximal hyperemia and the hyperaemic mean transit time. An IMR ≥25 indicates microvascular dysfunction. Alternatively, the hyperaemic myocardial velocity resistance (HMR) index is based on Doppler flow, calculated by dividing intracoronary pressure by hyperaemic flow velocity. Research has shown that an HMR >1.9 is a strong predictor of recurrent chest pain in patients with angina and non-obstructive coronary arteries. Together, CFR, IMR, and FFR provide comprehensive diagnostic information regarding endothelial-independent CMD, endothelium-dependent microvascular function, vasospastic responses, and low-grade stenoses. CMD is characterized by decreased CFR and increased microvascular resistance (IMR, HMR).
Figure 2 shows clinical algorithm for the diagnosis of myocardial infarction with nonobstructive coronary artery disease.
6. Management
Currently, no randomized clinical trials have been published on the treatment of MINOCA. As a result, existing guidelines rely primarily on expert consensus rather than high-quality evidence. The complexity of MINOCA as a heterogeneous condition further complicates treatment decisions, as the precise underlying cause is often undetermined in routine clinical practice. Acute-phase management primarily aims to alleviate symptoms, as no intervention has been demonstrated to limit infarct size in MINOCA. Long-term low-dose aspirin is generally recommended for secondary prevention [2]. However, the role of DAPT remains controversial, with no observational studies indicating a significant reduction in cardiovascular risk [71,72,73,74,75]. Conversely, statin therapy has been associated with lower mortality and reduced MACE, with effects comparable to those observed in randomized trials of secondary prevention in traditional myocardial infarction [71,72,73,74,75]. Similarly, angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) have demonstrated positive associations with improved outcomes [71,72,73,74,75]. Beta-blockers, on the other hand, have shown inconsistent results, with most studies failing to establish a clear survival benefit, although a large study by Lindahl et al. suggested a non-significant trend toward improved outcomes [71]. Data on calcium channel blockers remain limited, with no conclusive evidence of long-term MACE reduction [72,74]. Beyond pharmacological strategies, non-drug interventions have been poorly studied, though one investigation suggested that structured physical exercise may provide benefits in MINOCA patients [76]. Additionally, life-style regulation – including healthy diet, exercise, weight control, smoking cessation and stress management activities- and mitigation of modifiable cardiovascular risk factors—including blood pressure control, diabetes control, lipid-lowering therapy—are essential to optimize long-term outcomes.
Patients diagnosed with an underlying cause for MINOCA benefit from cause-directed treatment; however, even when an etiology is suspected, the optimal management approach remains unclear.
For MINOCA cases attributed to plaque disruption the recommended treatment includes a period of DAPT, followed by lifelong monotherapy, alongside high-intensity statins—even in individuals with minimal plaque burden—β-blockers, and ACEIs or ARBs. While the observational cohort study of patients from the SWEDEHEART registry did not show a clear benefit of dual antiplatelet therapy, this analysis included the entire MINOCA population without distinguishing between those with confirmed plaque disruption and those with other underlying causes of MINOCA[71]. The use of a second antiplatelet agent could be justified by extrapolating data from acute myocardial infarction trials, which did not require confirmation of obstructive CAD but demonstrated an added benefit from combining a P2Y12 receptor inhibitor with aspirin [77,78]. Limited evidence exists regarding the efficacy of PCI either with or without drug-eluting stents, in managing culprit lesions in MINOCA cases caused by plaque disruption. Due to this lack of robust data, expert panels and guideline committees have not endorsed PCI as a standard approach for treating MINOCA-related lesions [1,2]. Prati et al. evaluated the efficacy of dual DAPT compared to PCI with stenting in 31 patients who had plaque erosion identified via OCT. After a median follow-up period of 753 days, all participants remained symptom-free [79]. This research was the first to propose a non-invasive therapeutic alternative for individuals presenting with acute coronary syndromes despite the absence of significant arterial obstruction. Subsequently, the EROSION trial reinforced these findings, demonstrating that patients managed conservatively with DAPT, without undergoing PCI, experienced a favorable clinical course [80]. At one-year follow-up, the need for repeat revascularization was observed in only 5.7% of cases, supporting the viability of a medication-based approach in select patients with non-obstructive coronary lesions. In an OCT investigation, Imola et al. assessed the impact of stent placement in the management of ambiguous or intermediate coronary lesions in a cohort of 40 individuals. The application of drug-eluting stents was carried out according to protocol when local thrombosis was observed, secondary to ulceration or erosion. After an average follow-up of 4.6±3.2 months, no incidents of death, acute myocardial infarction, or stent thrombosis were recorded [81].
If vasospasm (epicardial or microvascular) is the underlying mechanism, calcium channel blockers (dihydropyridine and non-dihydropyridine) are the most effective symptomatic therapy, preventing recurrent symptoms and arrhythmias, and improving mortality. It may be necessary to administer unusually high dosages of calcium antagonist (2 × 200 mg diltiazem daily or higher up to 960 mg daily) or even a combination of non-dihydropyridine (such as diltiazem) with dihydropyridine calcium blockers (such as amlodipine). Low-dose aspirin is also effective in treating coronary vasospasm by inhibiting thromboxane-A2-mediated-vasoconstriction. Nitrates may be considered as adjunctive therapies. While short-acting sublingual and intracoronary nitrates are effective in providing rapid relief, the advantages of long-acting nitrates remain uncertain, potentially due to the development of tolerance [82]. Other drugs that have been found to effectively relieve coronary spasm include nicorandil (a potassium channel activator with nitrate-like effects) and cilostazol (a phosphodiesterase type 3 inhibitor) [82]. ACEIs/ARBs therapy are recommended, and statin use should be initiated if coexisting atherosclerosis is present.
In patients with microvascular dysfunction, among the standard antianginal treatments, calcium channel blockers and β-blockers have been shown to effectively reduce symptoms, while nitrates are less effective [83]. Furthermore, several small randomized controlled trials have highlighted the effectiveness of various non-traditional antianginal treatments, alongside standard post-MI treatment with ACEI/ARB and statins. These therapies work by improving endothelial function (e.g., l-arginine [84]) and promoting microvascular vasodilation (e.g., dipyridamole [85], ranolazine [86]). These treatments may alleviate symptoms but data demonstrating functional improvement are predominantly restricted to CMD patients with stable angina [83,84,87]. Additionally, some studies propose that the combination of an aldosterone antagonist with either ACEI or ARB could provide enhanced clinical outcomes in CMD [88].
In patients with SCAD, stenting carries a higher risk of complications as it may exacerbate the dissection both upstream and downstream of the affected vessel [47,89,90,91]. As a result, a conservative approach without angioplasty is typically recommended for most patients. PCI should be reserved for cases with high-risk anatomical features, such as severe lesions in the proximal left main or left anterior descending artery, low TIMI grade, or ongoing ischemia with hemodynamic instability [92]. The challenges of the procedure, the ongoing healing process, and the frequent distal nature of SCAD lesions support this cautious approach. While several strategies have been employed in PCI for SCAD, there are no definitive studies proving the superiority of one method over others. A common technical approach is the use of current-generation drug-eluting stents, and in the absence of significant atherosclerosis, bioresorbable scaffolds may offer a promising alternative [93]. Using cutting balloons for dilatation, with or without stenting, can help fenestrate the intramural hematoma and expand the true vessel lumen [94]. Coronary artery bypass grafting (CABG) is not an optimal treatment, as grafts often fail over time due to healing processes in the grafted arteries, which may lead to competitive flow and eventual occlusion; it should be reserved for stable patients with high-risk clinical features and either an ostial LAD lesion or ≥ 2 proximal lesions when PCI is not feasible or left main dissection involving the LAD or left circumflex artery [95]. Long-term beta-blocker therapy is a reasonable option [92]. A large cohort study found that SCAD survivors who were treated with beta-blockers had a lower risk of recurrence [89]. Since thrombus plays a minimal role in SCAD pathophysiology, the use of antiplatelet therapy remains contentious: theoretically it increases the risk of bleeding and worsen the hematoma or dissection area, however, the intimal tear may have prothrombotic properties, making the use of a moderately potent P2Y12 inhibitor like clopidogrel a justifiable option.
Coronary thrombosis/embolism management should focus on addressing the underlying prothrombotic condition. It’s typically managed with antithrombotic and, at times, antiplatelet treatments. In some cases, additional therapies are necessary; for instance, thrombotic thrombocytopenic purpura (TTP) is treated with plasma infusions and apheresis for plasma exchange, alongside supportive therapies like steroids and rituximab. This approach has significantly improved survival rates for TTP patients [96]. Patients with heparin-induced thrombocytopenia (HIT) should avoid future exposure to heparin. Given the complexity of these conditions, it is advisable to consult a hematologist for further management. Treatment should also include ACEI/ARB therapy and statins for secondary prevention.
When MINOCA results from an imbalance between myocardial oxygen supply and demand, treatment should be tailored to the specific etiology. Additional cardioprotective therapies should be individualized to each patient’s clinical scenario.
As we have seen, evidence-based treatments for MINOCA are lacking. A randomized clinical trial is now ongoing, the MINOCA-BAT (Randomized Evaluation of Beta-Blocker and ACEI/ARB Treatment in MINOCA Patients); it seeks to enroll at least 3,500 patients and will investigate the effects of ACE inhibitors/ARBs and β-blockers versus placebo on cardiovascular outcomes and overall mortality over one year [97]. The primary outcome of MINOCA-BAT is mortality or readmission due to MI, stroke or heart failure, and the trial is due to complete in 2025. The results of that study may affect future treatment guidelines for patients with MINOCA. Another interesting trial is ongoing, the WARRIOR (Women’s Ischemia Trial to Reduce Events In Non-Obstructive CAD); it’s a multicenter, prospective study designed to assess the effectiveness of intensive medical therapy —consisting of high-intensity statins and ACEIs or ARBs—against usual care in 4,422 symptomatic women with a diagnosis of INOCA (anginal symptoms and/or signs of ischemia and no obstructive coronary artery disease) in the United States in terms of MACE and mortality over 3 years. The Precision Medicine with Zibotentan in Microvascular Angina (PRIZE) trial holds future promise (NCT04097314). Zibotentan is an oral, endothelin A receptor antagonist that may provide benefit by opposing the reported vasoconstrictor response of coronary micro vessels to endothelin
Given the gaps in evidence, further research is essential to refine treatment strategies and establish more precise management recommendations.
7. Other Sex-Related Considerations
Sex-specific disparities in symptom manifestation, in the accuracy of diagnostic tests, and key determinants of triage, evaluation, and early intervention in women with myocardial ischemia may contribute to less favorable clinical outcomes. Additionally, women experience distinct risk factors that are often overlooked in standard clinical assessments. These include early menopause or menarche, gestational diabetes, pregnancy-related hypertensive conditions (such as preeclampsia and eclampsia), delivering small-for-gestational-age infants, placental abruption, and pregnancy loss, all of which are linked to an increased risk of cardiovascular disease. Women are less frequently referred for diagnostic evaluations and commonly receive inadequate secondary prevention therapies. Compared to men, women have shorter survival rates following PCI and CABG. Despite presenting with symptoms indicative of myocardial ischemia, women continue to be underdiagnosed, undertreated, and are less likely to be directed toward cardiac rehabilitation. Raising awareness of sex-specific variations in ischemic heart disease among both healthcare professionals and the public is vital for improving adherence to preventative, diagnostic, and therapeutic protocols. Expanding sex- and gender-specific cardiovascular research beyond traditional biomedical models to incorporate social determinants of health will support the formulation of tailored health policies. These initiatives will contribute to developing a patient-centered, sex- and gender-sensitive approach to cardiovascular care, ultimately fostering improved outcomes for women. Achieving equitable cardiovascular care for women necessitates a comprehensive strategy that includes public health campaigns, implementation of sex-specific guidelines, and increased female participation in clinical research. Enhancing awareness of unique cardiovascular risk factors and atypical myocardial infarction presentations in women is critical. However, recognition of these differences remains insufficient [98]. Of concern, even when the symptoms are recognized, only half seek medical attention [99]. The adoption of sex-specific clinical guidelines is crucial in closing this gap. Recent surveys indicate that only 22% of primary care physicians and 42% of cardiologists feel adequately equipped to assess cardiovascular risk in female patients [98]. Furthermore, nearly 70% of postgraduate trainees report insufficient exposure to sex-based medical concepts in their education [100]. Identification of at-risk women remains inadequate, with only 44% of primary care physicians and 53% of cardiologists utilizing the therosclerotic cardiovascular disease (ASCVD) risk calculator for female patients [98]. Despite directives from institutions such as the National Institutes of Health (NIH) and the European Commission’s Horizon 2020 program mandating the inclusion of women in clinical trials, female representation remains disproportionately low. A review of cardiovascular disease prevention guidelines found that women made up just 25% of the participants in 156 analyzed trials [101]. Innovative strategies such as oversampling, targeted recruitment of female subgroups, providing incentives for researchers to ensure female inclusion, and leveraging social media for recruitment may improve female participation in clinical studies. Addressing these inequities is essential to advancing cardiovascular health in women and ensuring equal access to evidence-based medical care [102].
8. Conclusions
MINOCA represents a complex and heterogeneous clinical entity with significant sex-specific implications in terms of pathophysiology, diagnosis, and management. Women are disproportionately affected and often present with nontraditional risk factors and atypical symptoms, leading to frequent misdiagnosis and suboptimal treatment. The current diagnostic and therapeutic paradigms, largely extrapolated from obstructive coronary artery disease research, fail to adequately address the unique characteristics of MINOCA in women.
To improve outcomes, a multifaceted approach is required, integrating enhanced clinician awareness, refined diagnostic strategies, and evidence-based, sex-specific treatment protocols. Increased investment in research focused on female cardiovascular health, greater inclusion of women in clinical trials, and the implementation of tailored prevention and management strategies are critical steps toward achieving equitable care. By addressing these gaps, the medical community can ensure that women with MINOCA receive timely and appropriate care, ultimately reducing morbidity and mortality associated with this condition.
Author Contributions
Conceptualization, C.T. and F.G.; Methodology, A.M. and M.V.; Software, C.T. and M.V; Writing—Original Draft Preparation, C.T. and C.G.; Writing—Review & Editing P.M and F.G.; Visualization, M.V. and A. M.; Supervision, P.M. and C.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio ALP, et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J. 2017 Jan 14;38(3):143–53. [CrossRef]
- Tamis-Holland JE, Jneid H, Reynolds HR, Agewall S, Brilakis ES, Brown TM, Lerman A, Cushman M, Kumbhani DJ, Arslanian-Engoren C, Bolger AF, Beltrame JF; American Heart Association Interventional Cardiovascular Care Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; and Council on Quality of Care and Outcomes Research. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation. 2019 Apr 30;139(18):e891-e908. [CrossRef]
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 2018 Nov 13;138(20):e618–51. [CrossRef]
- Lindahl B, Baron T, Albertucci M, Prati F. Myocardial infarction with non-obstructive coronary artery disease. EuroIntervention. 2021 Dec 3;17(11):e875-e887. Erratum in: EuroIntervention. 2022 Apr 01;17(17):e1366. doi: 10.4244/EIJ-D-21-0042C. [CrossRef]
- Boivin-Proulx LA, Haddad K, Lombardi M, Chong AY, Escaned J, Mukherjee S, et al. Pathophysiology of Myocardial Infarction With Nonobstructive Coronary Artery Disease: A Contemporary Systematic Review. CJC Open. 2024 Feb;6(2Part B):380–90. [CrossRef]
- Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic Review of Patients Presenting With Suspected Myocardial Infarction and Nonobstructive Coronary Arteries. Circulation. 2015 Mar 10;131(10):861–70. [CrossRef]
- Eggers KM, Hjort M, Baron T, Jernberg T, Nordenskjöld AM, Tornvall P, et al. Morbidity and cause-specific mortality in first-time myocardial infarction with nonobstructive coronary arteries. J Intern Med. 2019;285(4):419–28. [CrossRef]
- Ang SP, Chia JE, Krittanawong C, Lee K, Iglesias J, Misra K, et al. Sex Differences and Clinical Outcomes in Patients With Myocardial Infarction With Nonobstructive Coronary Arteries: A Meta-Analysis. J Am Heart Assoc. 2024 Aug 6;13(15):e035329. [CrossRef]
- Pacheco C, Luu J, Mehta PK, Wei J, Gulati M, Merz CNB. INOCA and MINOCA: Are Women’s Heart Centres the Answer to Understanding and Management of These Increasing Populations of Women (and Men)? Can J Cardiol. 2022 Oct;38(10):1611–4. [CrossRef]
- Cano-Castellote M, Afanador-Restrepo DF, González-Santamaría J, Rodríguez-López C, Castellote-Caballero Y, Hita-Contreras F, et al. Pathophysiology, Diagnosis and Treatment of Spontaneous Coronary Artery Dissection in Peripartum Women. J Clin Med. 2022 Nov 10;11(22):6657. [CrossRef]
- Pelliccia F, Pasceri V, Niccoli G, Tanzilli G, Speciale G, Gaudio C, et al. Predictors of Mortality in Myocardial Infarction and Nonobstructed Coronary Arteries: A Systematic Review and Meta-Regression. Am J Med. 2020 Jan 1;133(1):73-83.e4. [CrossRef]
- Nordenskjöld AM, Lagerqvist B, Baron T, Jernberg T, Hadziosmanovic N, Reynolds HR, Tornvall P, Lindahl B. Reinfarction in Patients with Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): Coronary Findings and Prognosis. Am J Med. 2019 Mar;132(3):335-346. [CrossRef]
- Hjort M, Lindahl B, Baron T, Jernberg T, Tornvall P, Eggers KM. Prognosis in relation to high-sensitivity cardiac troponin T levels in patients with myocardial infarction and non-obstructive coronary arteries. Am Heart J. 2018 Jun 1;200:60–6. [CrossRef]
- Pasupathy S, Lindahl B, Litwin P, Tavella R, Williams MJA, Air T, et al. Survival in Patients With Suspected Myocardial Infarction With Nonobstructive Coronary Arteries: A Comprehensive Systematic Review and Meta-Analysis From the MINOCA Global Collaboration. Circ Cardiovasc Qual Outcomes. 2021 Nov;14(11):e007880. [CrossRef]
- Davies MJ. The pathophysiology of acute coronary syndromes. Heart. 2000 Mar 1;83(3):361–6. [CrossRef]
- White SJ, Newby AC, Johnson TW. Endothelial erosion of plaques as a substrate for coronary thrombosis. Thromb Haemost. 2018 Mar 20;115:509–19. [CrossRef]
- Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006 Apr 18;47(8 Suppl):C13-18. [CrossRef]
- Reynolds HR, Maehara A, Kwong RY, Sedlak T, Saw J, Smilowitz NR, et al. Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction With Nonobstructive Coronary Arteries in Women. Circulation. 2021 Feb 16;143(7):624–40. [CrossRef]
- Opolski MP, Spiewak M, Marczak M, Debski A, Knaapen P, Schumacher SP, et al. Mechanisms of Myocardial Infarction in Patients With Nonobstructive Coronary Artery Disease: Results From the Optical Coherence Tomography Study. JACC Cardiovasc Imaging. 2019 Nov 1;12(11, Part 1):2210–21. [CrossRef]
- Gerbaud E, Arabucki F, Nivet H, Barbey C, Cetran L, Chassaing S, et al. OCT and CMR for the Diagnosis of Patients Presenting With MINOCA and Suspected Epicardial Causes. JACC Cardiovasc Imaging. 2020 Dec 1;13(12):2619–31. [CrossRef]
- Beltrame JF, Crea F, Kaski JC, Ogawa H, Ong P, Sechtem U, et al. International standardization of diagnostic criteria for vasospastic angina. Eur Heart J. 2017 Sep 1;38(33):2565–8. [CrossRef]
- Montone RA, Niccoli G, Fracassi F, Russo M, Gurgoglione F, Cammà G, et al. Patients with acute myocardial infarction and non-obstructive coronary arteries: safety and prognostic relevance of invasive coronary provocative tests. Eur Heart J. 2018 Jan 7;39(2):91–8. [CrossRef]
- Woudstra J, Vink CEM, Schipaanboord DJM, Eringa EC, den Ruijter HM, Feenstra RGT, et al. Meta-analysis and systematic review of coronary vasospasm in ANOCA patients: Prevalence, clinical features and prognosis. Front Cardiovasc Med. 2023;10:1129159. [CrossRef]
- Park JY, Choi SY, Rha SW, Choi BG, Noh YK, Kim YH. Sex Difference in Coronary Artery Spasm Tested by Intracoronary Acetylcholine Provocation Test in Patients with Nonobstructive Coronary Artery Disease. J Intervent Cardiol. 2022;2022:5289776. [CrossRef]
- Caralis DG, Deligonul U, Kern MJ, Cohen JD. Smoking is a risk factor for coronary spasm in young women. Circulation. 1992 Mar;85(3):905–9. [CrossRef]
- Scalone G, Niccoli G, Crea F. Editor’s Choice- Pathophysiology, diagnosis and management of MINOCA: an update. Eur Heart J Acute Cardiovasc Care. 2019 Feb;8(1):54–62. [CrossRef]
- Ong P, Camici PG, Beltrame JF, Crea F, Shimokawa H, Sechtem U, et al. International standardization of diagnostic criteria for microvascular angina. Int J Cardiol. 2018 Jan 1;250:16–20. [CrossRef]
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Nov 30;144(22):e368–454. [CrossRef]
- Del Buono MG, Montone RA, Camilli M, Carbone S, Narula J, Lavie CJ, et al. Coronary Microvascular Dysfunction Across the Spectrum of Cardiovascular Diseases: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021 Sep 28;78(13):1352–71. [CrossRef]
- Mauricio R, Srichai MB, Axel L, Hochman JS, Reynolds HR. Stress Cardiac MRI in Women With Myocardial Infarction and Nonobstructive Coronary Artery Disease. Clin Cardiol. 2016 Oct;39(10):596–602. [CrossRef]
- Wei J, Bakir M, Darounian N, Li Q, Landes S, Mehta PK, et al. Myocardial Scar Is Prevalent and Associated With Subclinical Myocardial Dysfunction in Women With Suspected Ischemia But No Obstructive Coronary Artery Disease: From the Women’s Ischemia Syndrome Evaluation-Coronary Vascular Dysfunction Study. Circulation. 2018 Feb 20;137(8):874–6. [CrossRef]
- Crea F, Camici PG, Bairey Merz CN. Coronary microvascular dysfunction: an update. Eur Heart J. 2014 May;35(17):1101–11. [CrossRef]
- Godo S, Takahashi J, Yasuda S, Shimokawa H. Role of Inflammation in Coronary Epicardial and Microvascular Dysfunction. Eur Cardiol. 2021 Feb;16:e13. [CrossRef]
- Odaka Y, Takahashi J, Tsuburaya R, Nishimiya K, Hao K, Matsumoto Y, et al. Plasma concentration of serotonin is a novel biomarker for coronary microvascular dysfunction in patients with suspected angina and unobstructive coronary arteries. Eur Heart J. 2017 Feb 14;38(7):489–96. [CrossRef]
- Takahashi J, Suda A, Nishimiya K, Godo S, Yasuda S, Shimokawa H. Pathophysiology and Diagnosis of Coronary Functional Abnormalities. Eur Cardiol. 2021 Feb;16:e30. [CrossRef]
- Raphael CE, Heit JA, Reeder GS, Bois MC, Maleszewski JJ, Tilbury RT, et al. Coronary Embolus: An Underappreciated Cause of Acute Coronary Syndromes. JACC Cardiovasc Interv. 2018 Jan 22;11(2):172–80. [CrossRef]
- El Sabbagh A, Al-Hijji MA, Thaden JJ, Pislaru SV, Pislaru C, Pellikka PA, et al. Cardiac Myxoma: The Great Mimicker. JACC Cardiovasc Imaging. 2017 Feb;10(2):203–6. [CrossRef]
- Zhao J, Yang J, Chen W, Yang X, Liu Y, Cong X, et al. Acute myocardial infarction as the first sign of infective endocarditis: a case report. J Int Med Res. 2020 Dec;48(12):300060520980598. [CrossRef]
- Karameh M, Golomb M, Arad A, Kalmnovich G, Herzog E. Multi-Valvular Non-bacterial Thrombotic Endocarditis Causing Sequential Pulmonary Embolism, Myocardial Infarction, and Stroke: A Case Report and Literature Review. Cureus. 2022 Dec;14(12):e32261. [CrossRef]
- Talebi S, Jadhav P, Tamis-Holland JE. Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease (MINOCA): a Review of the Present and Preview of the Future. Curr Atheroscler Rep. 2021 Jul 6;23(9):49. [CrossRef]
- Pasupathy S, Rodgers S, Tavella R, McRae S, Beltrame JF. Risk of Thrombosis in Patients Presenting with Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA). TH Open Companion J Thromb Haemost. 2018 Apr;2(2):e167–72. [CrossRef]
- Shen YM, Nagalla S. Hypercoagulable Workup in Thrombotic Cardiovascular Diseases. Circulation. 2018 Jul 17;138(3):229–31. [CrossRef]
- Stepien K, Nowak K, Wypasek E, Zalewski J, Undas A. High prevalence of inherited thrombophilia and antiphospholipid syndrome in myocardial infarction with non-obstructive coronary arteries: Comparison with cryptogenic stroke. Int J Cardiol. 2019 Sep 1;290:1–6. [CrossRef]
- Saw J, Starovoytov A, Aymong E, Inohara T, Alfadhel M, McAlister C, et al. Canadian Spontaneous Coronary Artery Dissection Cohort Study: 3-Year Outcomes. J Am Coll Cardiol. 2022 Oct 25;80(17):1585–97. [CrossRef]
- García-Guimaraes M, Bastante T, Macaya F, Roura G, Sanz R, Barahona Alvarado JC, et al. Spontaneous coronary artery dissection in Spain: clinical and angiographic characteristics, management, and in-hospital events. Rev Espanola Cardiol Engl Ed. 2021 Jan;74(1):15–23. [CrossRef]
- Lewey J, El Hajj SC, Hayes SN. Spontaneous Coronary Artery Dissection: New Insights into This Not-So-Rare Condition. Annu Rev Med. 2022 Jan 27;73:339–54. [CrossRef]
- Tweet MS, Hayes SN, Codsi E, Gulati R, Rose CH, Best PJM. Spontaneous Coronary Artery Dissection Associated With Pregnancy. J Am Coll Cardiol. 2017 Jul 25;70(4):426–35. [CrossRef]
- Waterbury TM, Tweet MS, Hayes SN, Eleid MF, Bell MR, Lerman A, et al. Early Natural History of Spontaneous Coronary Artery Dissection. Circ Cardiovasc Interv. 2018 Sep;11(9):e006772. [CrossRef]
- Hayes SN, Tweet MS, Adlam D, Kim ESH, Gulati R, Price JE, et al. Spontaneous Coronary Artery Dissection: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020 Aug 25;76(8):961–84. [CrossRef]
- Alfonso F, Paulo M, Gonzalo N, Dutary J, Jimenez-Quevedo P, Lennie V, et al. Diagnosis of spontaneous coronary artery dissection by optical coherence tomography. J Am Coll Cardiol. 2012 Mar 20;59(12):1073–9. [CrossRef]
- La S, Beltrame J, Tavella R. Sex-specific and ethnicity-specific differences in MINOCA. Nat Rev Cardiol. 2024 Mar;21(3):192–202. [CrossRef]
- Collste O, Sörensson P, Frick M, Agewall S, Daniel M, Henareh L, et al. Myocardial infarction with normal coronary arteries is common and associated with normal findings on cardiovascular magnetic resonance imaging: results from the Stockholm Myocardial Infarction with Normal Coronaries study. J Intern Med. 2013;273(2):189–96. [CrossRef]
- Dastidar AG, Baritussio A, De Garate E, Drobni Z, Biglino G, Singhal P, et al. Prognostic Role of CMR and Conventional Risk Factors in Myocardial Infarction With Nonobstructed Coronary Arteries. JACC Cardiovasc Imaging. 2019 Oct 1;12(10):1973–82. [CrossRef]
- Mahmoudi M, Harden S, Abid N, Peebles C, Nicholas Z, Jones T, et al. Troponin-positive chest pain with unobstructed coronary arteries: definitive differential diagnosis using cardiac MRI. Br J Radiol. 2012 Aug 1;85(1016):e461–6. [CrossRef]
- Kramer CM, Barkhausen J, Bucciarelli-Ducci C, Flamm SD, Kim RJ, Nagel E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J Cardiovasc Magn Reson. 2020 Jan 20;22(1):17. [CrossRef]
- Ferreira VM, Schulz-Menger J, Holmvang G, Kramer CM, Carbone I, Sechtem U, et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J Am Coll Cardiol. 2018 Dec 18;72(24):3158–76. [CrossRef]
- Cundari G, Galea N, De Rubeis G, Frustaci A, Cilia F, Mancuso G, et al. Use of the new Lake Louise Criteria improves CMR detection of atypical forms of acute myocarditis. Int J Cardiovasc Imaging. 2021 Apr 1;37(4):1395–404. [CrossRef]
- Lintingre PF, Nivet H, Clément-Guinaudeau S, Camaioni C, Sridi S, Corneloup O, et al. High-Resolution Late Gadolinium Enhancement Magnetic Resonance for the Diagnosis of Myocardial Infarction With Nonobstructed Coronary Arteries. JACC Cardiovasc Imaging. 2020 May 1;13(5):1135–48. [CrossRef]
- Dastidar AG, Rodrigues JCL, Johnson TW, De Garate E, Singhal P, Baritussio A, et al. Myocardial Infarction With Nonobstructed Coronary Arteries: Impact of CMR Early After Presentation. JACC Cardiovasc Imaging. 2017 Oct 1;10(10, Part A):1204–6. [CrossRef]
- Yamamoto MH, Maehara A, Song L, Matsumura M, Chin CY, Losquadro M, et al. Optical Coherence Tomography Assessment of Morphological Characteristics in Suspected Coronary Artery Disease, but Angiographically Nonobstructive Lesions. Cardiovasc Revascularization Med Mol Interv. 2019 Jun;20(6):475–9. [CrossRef]
- Usui E, Murai T, Kanaji Y, Hoshino M, Yamaguchi M, Hada M, et al. Clinical significance of concordance or discordance between fractional flow reserve and coronary flow reserve for coronary physiological indices, microvascular resistance, and prognosis after elective percutaneous coronary intervention. EuroIntervention J Eur Collab Work Group Interv Cardiol Eur Soc Cardiol. 2018 Sep 20;14(7):798–805. [CrossRef]
- Taruya A, Tanaka A, Nishiguchi T, Ozaki Y, Kashiwagi M, Yamano T, et al. Lesion characteristics and prognosis of acute coronary syndrome without angiographically significant coronary artery stenosis. Eur Heart J Cardiovasc Imaging. 2020 Feb 1;21(2):202–9. [CrossRef]
- Mas-Lladó C, Maristany J, Gómez-Lara J, Pascual M, Alameda MDM, Gómez-Jaume A, et al. Optical Coherence Tomography for the Diagnosis of Exercise-Related Acute Cardiovascular Events and Inconclusive Coronary Angiography. J Intervent Cardiol. 2020;2020:8263923. [CrossRef]
- Zeng M, Zhao C, Bao X, Liu M, He L, Xu Y, et al. Clinical Characteristics and Prognosis of MINOCA Caused by Atherosclerotic and Nonatherosclerotic Mechanisms Assessed by OCT. JACC Cardiovasc Imaging. 2023 Apr;16(4):521–32. [CrossRef]
- Barbieri L, D’Errico A, Avallone C, Gentile D, Provenzale G, Guagliumi G, et al. Optical Coherence Tomography and Coronary Dissection: Precious Tool or Useless Surplus? Front Cardiovasc Med. 2022;9:822998. [CrossRef]
- Vrints C, Andreotti F, Koskinas KC, Rossello X, Adamo M, Ainslie J, Banning AP, Budaj A, Buechel RR, Chiariello GA, Chieffo A, Christodorescu RM, Deaton C, Doenst T, Jones HW, Kunadian V, Mehilli J, Milojevic M, Piek JJ, Pugliese F, Rubboli A, Semb AG, Senior R, Ten Berg JM, Van Belle E, Van Craenenbroeck EM, Vidal-Perez R, Winther S; ESC Scientific Document Group. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024 Sep 29;45(36):3415-3537. [CrossRef]
- Takagi Y, Yasuda S, Takahashi J, Tsunoda R, Ogata Y, Seki A, et al. Clinical implications of provocation tests for coronary artery spasm: safety, arrhythmic complications, and prognostic impact: Multicentre Registry Study of the Japanese Coronary Spasm Association. Eur Heart J. 2013 Jan 21;34(4):258–67. [CrossRef]
- Ong P, Athanasiadis A, Borgulya G, Vokshi I, Bastiaenen R, Kubik S, et al. Clinical usefulness, angiographic characteristics, and safety evaluation of intracoronary acetylcholine provocation testing among 921 consecutive white patients with unobstructed coronary arteries. Circulation. 2014 Apr 29;129(17):1723–30. [CrossRef]
- Curzen N, Rana O, Nicholas Z, Golledge P, Zaman A, Oldroyd K, et al. Does routine pressure wire assessment influence management strategy at coronary angiography for diagnosis of chest pain?: the RIPCORD study. Circ Cardiovasc Interv. 2014 Apr;7(2):248–55. [CrossRef]
- AlBadri A, Bairey Merz CN, Johnson BD, Wei J, Mehta PK, Cook-Wiens G, et al. Impact of Abnormal Coronary Reactivity on Long-Term Clinical Outcomes in Women. J Am Coll Cardiol. 2019 Feb 19;73(6):684–93. [CrossRef]
- Lindahl B, Baron T, Erlinge D, Hadziosmanovic N, Nordenskjöld A, Gard A, et al. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. Circulation. 2017 Apr 18;135(16):1481–9. [CrossRef]
- Kovach CP, Hebbe A, O’Donnell CI, Plomondon ME, Hess PL, Rahman A, et al. Comparison of Patients With Nonobstructive Coronary Artery Disease With Versus Without Myocardial Infarction (from the VA Clinical Assessment Reporting and Tracking [CART] Program). Am J Cardiol. 2021 May 1;146:1–7. [CrossRef]
- Abdu FA, Liu L, Mohammed AQ, Xu B, Yin G, Xu S, et al. Effect of Secondary Prevention Medication on the Prognosis in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. J Cardiovasc Pharmacol. 2020 Dec;76(6):678. [CrossRef]
- Ciliberti G, Verdoia M, Merlo M, Zilio F, Vatrano M, Bianco F, et al. Pharmacological therapy for the prevention of cardiovascular events in patients with myocardial infarction with non-obstructed coronary arteries (MINOCA): Insights from a multicentre national registry. Int J Cardiol. 2021 Mar 15;327:9–14. [CrossRef]
- Paolisso P, Bergamaschi L, Saturi G, D’Angelo EC, Magnani I, Toniolo S, et al. Secondary Prevention Medical Therapy and Outcomes in Patients With Myocardial Infarction With Non-Obstructive Coronary Artery Disease. Front Pharmacol [Internet]. 2020 Jan 31 [cited 2025 Feb 7];10. Available from: https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2019.01606/full. [CrossRef]
- Eggers KM, Hadziosmanovic N, Baron T, Hambraeus K, Jernberg T, Nordenskjöld A, et al. Myocardial Infarction with Nonobstructive Coronary Arteries: The Importance of Achieving Secondary Prevention Targets. Am J Med. 2018 May 1;131(5):524-531.e6. [CrossRef]
- Chen ZM, Jiang LX, Chen YP, Xie JX, Pan HC, Peto R, et al. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet Lond Engl. 2005 Nov 5;366(9497):1607–21. [CrossRef]
- Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001 Aug 16;345(7):494–502. [CrossRef]
- Prati F, Uemura S, Souteyrand G, Virmani R, Motreff P, Di Vito L, et al. OCT-Based Diagnosis and Management of STEMI Associated With Intact Fibrous Cap. JACC Cardiovasc Imaging. 2013 Mar 1;6(3):283–7. [CrossRef]
- Xing L, Yamamoto E, Sugiyama T, Jia H, Ma L, Hu S, et al. EROSION Study (Effective Anti-Thrombotic Therapy Without Stenting: Intravascular Optical Coherence Tomography–Based Management in Plaque Erosion). Circ Cardiovasc Interv. 2017 Dec;10(12):e005860. [CrossRef]
- Imola F, Mallus MT, Ramazzotti V, Manzoli A, Pappalardo A, Di Giorgio A, et al. Safety and feasibility of frequency domain optical coherence tomography to guide decision making in percutaneous coronary intervention. EuroIntervention J Eur Collab Work Group Interv Cardiol Eur Soc Cardiol. 2010 Nov;6(5):575–81. [CrossRef]
- Beltrame JF, Crea F, Kaski JC, Ogawa H, Ong P, Sechtem U, et al. The Who, What, Why, When, How and Where of Vasospastic Angina. Circ J Off J Jpn Circ Soc. 2016;80(2):289–98. [CrossRef]
- Beltrame JF, Crea F, Camici P. Advances in coronary microvascular dysfunction. Heart Lung Circ. 2009 Feb;18(1):19–27. [CrossRef]
- Lerman A, Burnett JC, Higano ST, McKinley LJ, Holmes DR. Long-term L-arginine supplementation improves small-vessel coronary endothelial function in humans. Circulation. 1998 Jun 2;97(21):2123–8. [CrossRef]
- Kurtoglu N, Akcay A, Dindar I. Usefulness of oral dipyridamole therapy for angiographic slow coronary artery flow. Am J Cardiol. 2001 Mar 15;87(6):777–9, A8. [CrossRef]
- Saha S, Ete T, Kapoor M, Jha PK, Megeji RD, Kavi G, et al. Effect of Ranolazine in Patients with Chest Pain and Normal Coronaries- A Hospital Based Study. J Clin Diagn Res JCDR. 2017 Apr;11(4):OC14–6. . [CrossRef]
- Kilic S, Aydın G, Çoner A, Doğan Y, Arican Özlük Ö, Çelik Y, et al. Prevalence and clinical profile of patients with myocardial infarction with non-obstructive coronary arteries in Turkey (MINOCA-TR): A national multi-center, observational study. Anatol J Cardiol. 2020 Feb;23(3):176–82. [CrossRef]
- Suhrs HE, Michelsen MM, Prescott E. Treatment strategies in coronary microvascular dysfunction: A systematic review of interventional studies. Microcirc N Y N 1994. 2019 Apr;26(3):e12430. [CrossRef]
- Saw J, Aymong E, Sedlak T, Buller CE, Starovoytov A, Ricci D, et al. Spontaneous Coronary Artery Dissection. Circ Cardiovasc Interv. 2014 Oct;7(5):645–55. [CrossRef]
- Nakashima T, Noguchi T, Haruta S, Yamamoto Y, Oshima S, Nakao K, et al. Prognostic impact of spontaneous coronary artery dissection in young female patients with acute myocardial infarction: A report from the Angina Pectoris–Myocardial Infarction Multicenter Investigators in Japan. Int J Cardiol. 2016 Mar 15;207:341–8. [CrossRef]
- Tweet MS, Hayes SN, Pitta SR, Simari RD, Lerman A, Lennon RJ, Gersh BJ, Khambatta S, Best PJ, Rihal CS, Gulati R. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation. 2012 Jul 31;126(5):579-88. [CrossRef]
- Adlam D, Alfonso F, Maas A, Vrints C, Writing Committee. European Society of Cardiology, acute cardiovascular care association, SCAD study group: a position paper on spontaneous coronary artery dissection. Eur Heart J. 2018 Sep 21;39(36):3353–68. [CrossRef]
- Macaya F, Salinas P, Gonzalo N, Camacho-Freire S, Jackson R, Massot M, et al. Long-term follow-up of spontaneous coronary artery dissection treated with bioresorbable scaffolds [Internet]. [cited 2025 Feb 7]. Available from: https://eurointervention.pcronline.com/article/long-term-follow-up-of-spontaneous-coronary-artery-dissection-treated-with-bioresorbable-scaffolds.
- Alkhouli M, Cole M, Ling FS. Coronary artery fenestration prior to stenting in spontaneous coronary artery dissection. Catheter Cardiovasc Interv. 2016;88(1):E23–7. [CrossRef]
- Saw J, Mancini GBJ, Humphries KH. Contemporary Review on Spontaneous Coronary Artery Dissection. J Am Coll Cardiol. 2016 Jul 19;68(3):297–312. [CrossRef]
- Saha M, McDaniel JK, Zheng XL. Thrombotic thrombocytopenic purpura: pathogenesis, diagnosis and potential novel therapeutics. J Thromb Haemost JTH. 2017 Oct;15(10):1889–900. [CrossRef]
- Nordenskjöld AM, Agewall S, Atar D, Baron T, Beltrame J, Bergström O, et al. Randomized evaluation of beta blocker and ACE-inhibitor/angiotensin receptor blocker treatment in patients with myocardial infarction with non-obstructive coronary arteries (MINOCA-BAT): Rationale and design. Am Heart J. 2021 Jan 1;231:96–104. [CrossRef]
- Bairey Merz CN, Andersen H, Sprague E, Burns A, Keida M, Walsh MN, et al. Knowledge, Attitudes, and Beliefs Regarding Cardiovascular Disease in Women: The Women’s Heart Alliance. J Am Coll Cardiol. 2017 Jul 11;70(2):123–32. [CrossRef]
- Mosca L, Hammond G, Mochari-Greenberger H, Towfighi A, Albert MA, American Heart Association Cardiovascular Disease and Stroke in Women and Special Populations Committee of the Council on Clinical Cardiology, Council on Epidemiology and Prevention, Council on Cardiovascular Nursing, Council on High Bloo. Fifteen-year trends in awareness of heart disease in women: results of a 2012 American Heart Association national survey. Circulation. 2013 Mar 19;127(11):1254–63, e1-29. [CrossRef]
- Dhawan S, Bakir M, Jones E, Kilpatrick S, Merz CNB. Sex and gender medicine in physician clinical training: results of a large, single-center survey. Biol Sex Differ. 2016;7(Suppl 1):37. [CrossRef]
- Melloni C, Berger JS, Wang TY, Gunes F, Stebbins A, Pieper KS, et al. Representation of women in randomized clinical trials of cardiovascular disease prevention. Circ Cardiovasc Qual Outcomes. 2010 Mar;3(2):135–42. [CrossRef]
- Tweet MS, Gulati R, Aase LA, Hayes SN. Spontaneous coronary artery dissection: a disease-specific, social networking community-initiated study. Mayo Clin Proc. 2011 Sep;86(9):845–50. [CrossRef]
Figure 1.
MINOCA pathophysiological mechanisms.
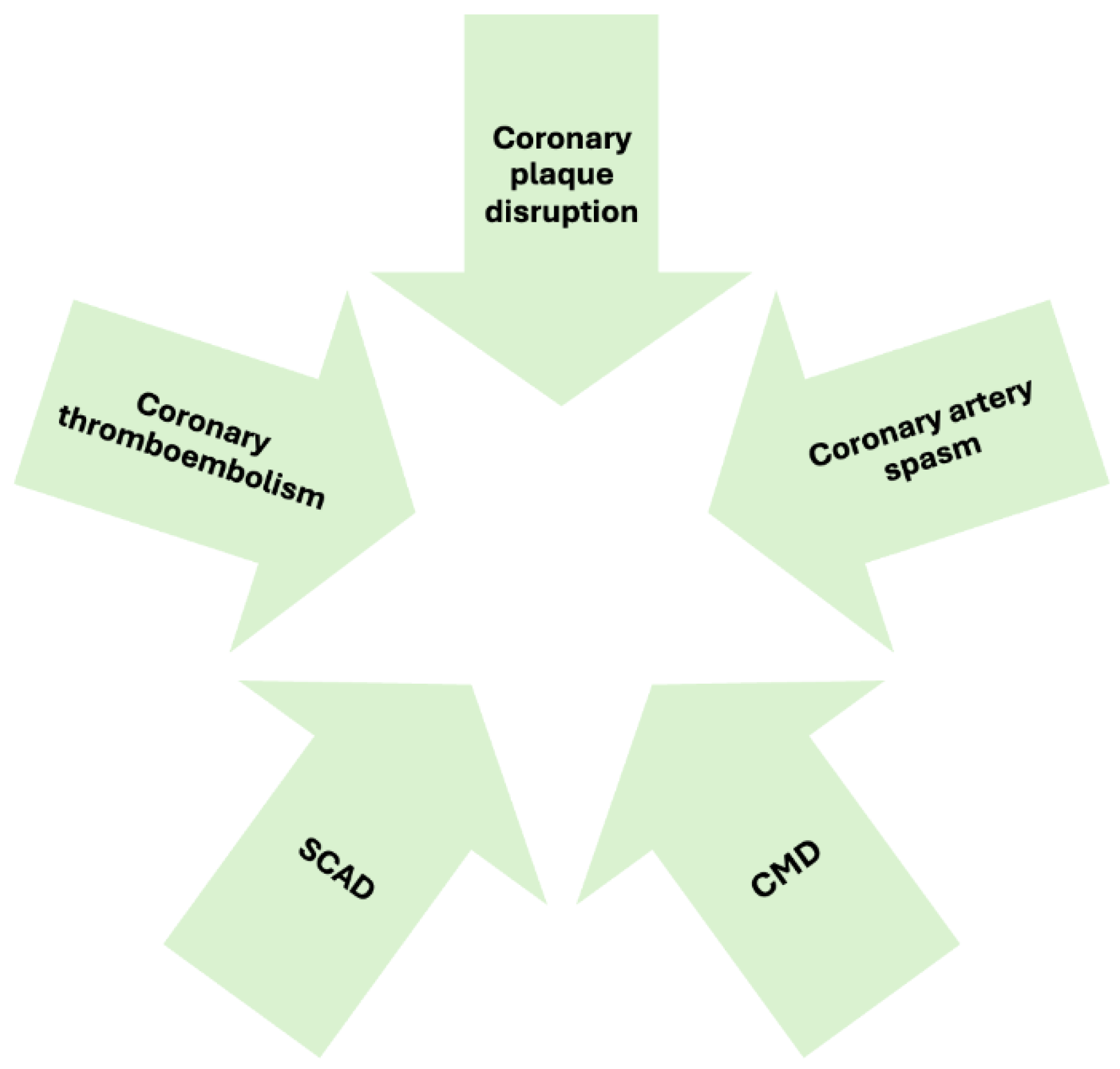
Figure 2.
Clinical algorithm for the diagnosis of myocardial infarction with nonobstructive coronary artery disease.
Figure 2.
Clinical algorithm for the diagnosis of myocardial infarction with nonobstructive coronary artery disease.
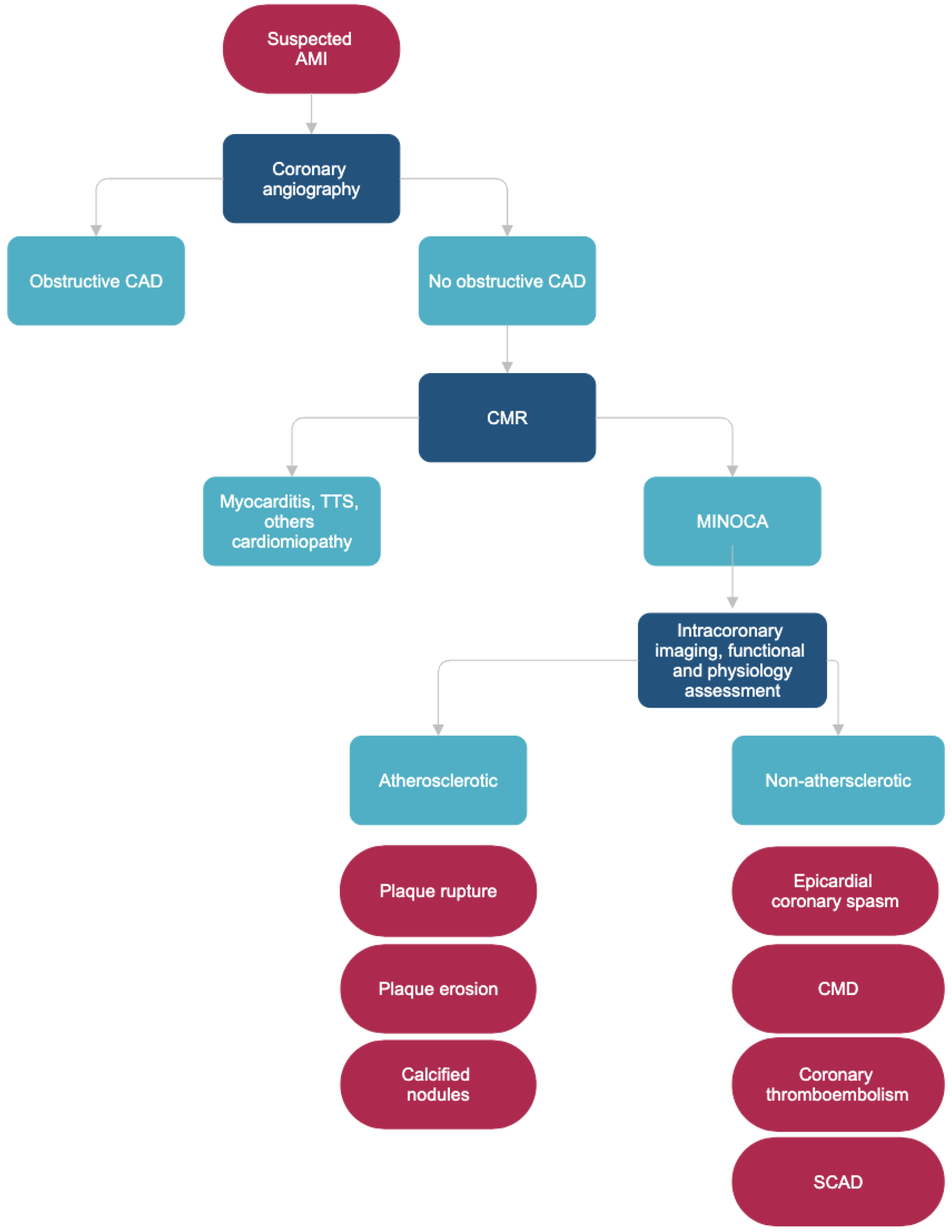
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



