Submitted:
21 February 2025
Posted:
21 February 2025
You are already at the latest version
Abstract
Background: Septal accessory pathways (APs) are challenging ablation targets. The study aims to contribute to the pediatric literature by presenting our long-term experience of septal AP ablations with limited fluoroscopy. Methods: This is a retrospective study of all patients who underwent septal AP ablations from July 2012 to July 2023 at a single center. Results: We identified 298 septal AP connections in 291 (11.8 ± 4.9 years) patients. Seventy-nine (27%) cases were diagnosed with supraventricular tachycardia, and 225 (73%) cases were diagnosed with Wolff-Parkinson-White syndrome (WPW). The AP locations were posteroseptal (n=159;54%), anteroseptal (n=86;30%), and midseptal (n=46;16%). Of those diagnosed with WPW, 61 (28%) had high-risk AP and 90 (40%) were adenosine responsive. Cryoablation was used in 190 (66%), radiofrequency ablation (RFA) was used in 36 (12.5%), and both were used in 62 (21.5%) patients. The overall acute success rate of initial procedures was 89.6% (The acute success rate of cryoablation=86.6%; RFA=94.1%). During a mean follow-up of 88.5±33.0 months, the overall recurrence rate was 11.3%, with the highest at the right-posteroseptal location. An irrigated-tip RFA was preferred during redo procedures in 20 (45%) cases. The long-term success rate was 99% when the repeat procedures were considered. No complications were observed. Conclusions: Due to the higher recurrence rates in septal AP ablations compared to other locations, repeated procedures might be needed to achieve definitive long-term success. This study indicates that similar acute and long-term success rates can be achieved with cryoablation compared to RFA, with the significant benefit of increased safety.
Keywords:
Cryoablation
; irrigated-tip radiofrequency ablation
; recurrence
1. Introduction
Septal accessory pathways (APs) are challenging targets, representing 30% of all APs [1]. Ablation of anteroseptal and midseptal APs increases the risk of atrioventricular (AV) block due to their proximity to the normal AV conduction system. However, AV block may also occur in other septal locations. In contrast, the complex anatomy of the posteroseptal space presents a risk of coronary injury [2].
Radiofrequency catheter ablation (RFA) is the preferred treatment for eliminating accessory pathways (APs) [3]. However, RFA for septal APs is linked to higher complication rates than other locations [4]. Since 2003, cryoablation has emerged as a safe alternative to RFA for several arrhythmogenic substrates, particularly in the septal region [5,6,7,8]. The pediatric literature indicates that cryoablation has higher recurrence rates compared to RFA. Nevertheless, some benefits of cryothermal energy, such as lesion reversibility, a reduced risk of thrombus formation, and improved catheter stability, make it a favorable option when the AP is near the AV node or bundle of His [6,8,9].
Although many expert consensus reports on the management of AP in the pediatric population estimate an overall acute procedural success rate of 95%, septal AP ablation presents lower acute success rates with higher recurrence rates when evaluated over a more extended follow-up period [10,11,12]. Many patients require multiple procedures to achieve definitive success.
This study aims to contribute to pediatric literature by sharing our long-term experience with septal AP ablations using limited fluoroscopy at a single center. Consequently, we evaluated the initial and repeat procedures regarding techniques and strategies to understand better the factors that may have influenced long-term outcomes.
2. Materials and Methods
2.1. Patients and Study Design
This retrospective, single-center study involved reviewing the clinical and procedural reports of patients who underwent electrophysiological studies (EPS) for septal atrioventricular reentrant tachycardia substrates mediated by APs in the Pediatric Cardiology/Electrophysiology Department of Medipol University in Istanbul, Turkey, between July 2012 and July 2023. Data collection was performed using FileMaker® software and included the following variables: patient characteristics, type of access, location of APs, presence of additional arrhythmia substrates, type of catheter and energy used, imaging modality used to guide the procedure, transseptal puncture, procedure duration, fluoroscopy duration, and complications. Initial ablation data were incorporated for patients who underwent second or third ablation procedures due to recurrent or unsuccessful attempts. The study received approval from our institution’s ethical committee.
2.2. Procedure
Informed written consent was obtained from all patients’ legal guardians, and retrospective case analysis was conducted under a consent waiver approved by the local institutional research committee.
Antiarrhythmic medications were discontinued at least five half-lives prior to the procedure. All procedures were conducted under general anesthesia using an EnSite 3D electroanatomic system (St. Jude Medical, Inc., St. Paul, MN, USA) with limited fluoroscopy. A comprehensive electrophysiological study (EPS) was initiated to identify the arrhythmia substrate and evaluate its characteristics. Initially, a risk assessment was performed for manifest AP (Wolff-Parkinson-White syndrome [WPW]). Risk stratification was based on consensus guidelines established by experts from the Pediatric and Congenital Electrophysiology Society in collaboration with the Heart Rhythm Society in 2012, along with the study published by Etheridge et al. in 2018. The shortest pre-excitatory RR interval (SPERRI), the anterograde effective refractory period of the AP (APERP), and the shortest paced cycle length with preexcitation during rapid atrial pacing (SPPCL) ≤ 250 ms are considered to carry an increased risk for sudden cardiac death. Borderline risk is defined as values for APERP, SPERRI, and SPPCL between 250 and 300 ms.13,14
Delta wave mapping and retrograde mapping during supraventricular tachycardia (SVT) and/or V-pace were utilized in patients with manifest APs), whereas the latter two techniques were employed in patients with concealed APs. Additionally, a qS pattern in the unipolar electrogram was targeted during sinus rhythm or atrial pacing in patients with manifest APs. Electroanatomic mapping assisted in identifying potential targets within a 3D geometric framework.
The location of APs was defined as follows [11].
1. Anteroseptal (AS) if earliest ventricular activation during anterograde conduction or earliest retrograde atrial activation during ventricular pacing were in the upper 1/3 of the triangle of Koch, including the presence of a His bundle potential (0.1 mV) at the successful ablation region.
2. Midseptal (MS) if the earliest ventricular activation during anterograde conduction or earliest retrograde atrial activation conduction during ventricular pacing were in the middle third of the triangle of Koch.
3. Posteroseptal (PS) if the earliest ventricular activation during anterograde conduction or retrograde atrial activation during ventricular pacing were located near or in the CS ostium or inside the proximal CS (right-PS). If the AP was located on the left side of the septum opposite the right-PS location, it was labeled as left-PS AP.
Ablations conducted through the CS and middle cardiac vein were categorized under a separate heading as “epicardial ablations.”
If the AP was considered to be left-sided, the patent foramen ovale was initially explored; otherwise, an anterograde approach was employed, typically through transeptal puncture under fluoroscopy utilizing a transseptal long sheath and Brokenbrough needle.
Catheter selection, technique, energy source, and ablation settings varied based on each case, resource availability, and expert preference. The Freezor Xtra™ catheter (8 FR, Medtronic Inc., Minneapolis, MN, USA) with 6-mm and 8-mm tips were used for the cryoablation procedures. When using a 6-mm tip catheter, cryomapping was conducted at –30°C at the previously marked location. Cryomapping was stopped if no effect was observed within 30–45 seconds. When using an 8-mm tip catheter, short cryoablation test applications lasting 30 seconds were performed and were terminated when no effect was seen. If the patient had manifest atrial pre-excitation, cryomapping was carried out during sinus rhythm to monitor for loss of delta wave, during orthodromic tachycardia to terminate it, or during ventricular pacing to establish retrograde AP block. For concealed APs, cryomapping was conducted either during orthodromic tachycardia to terminate it or during ventricular pacing to establish retrograde AP block. Ablation continued at -70°C to -80°C for 240-360 seconds once the AP block was achieved. Finally, insurance lesions were applied to achieve the freeze-thaw-freeze effect.
Conventional RF energy (7 FR RF Marinr™ Multi-curve Steerable Catheter; Medtronic, Minneapolis, MN, USA) was primarily preferred and delivered using an IBI generator (St. Jude Medical) in a temperature-controlled mode at 40-50 Watts (W) with a temperature cut-off of 50–60 degrees Celsius (°C). Irrigated-tip RF catheters (7 FR 4-mm tip Cool Flex™ and 8 FR 4-mm tip Flex Ability™ Catheters; St. Jude Medical, Inc., St. Paul, MN, USA) were utilized with the same generator in temperature-controlled mode, starting with 25 W and increasing to 30-35 W, at 85–90 Ω and a temperature range of 30–35 °C. Power was titrated from 15 W to 20-25 W while delivering energy into the coronary sinus. The duration of the energy lesion was limited to 60 seconds, typically employing two consolidation lesions. Irrigated radiofrequency ablation (RFA) was preferred for patients weighing more than 30 kg when standard RF catheter procedures were unsuccessful or the desired wattage could not be achieved.
The AV node conduction was closely monitored during mapping and ablation. Ablation was stopped immediately if any AV conduction delay was observed, and an accelerated junctional rhythm was noted during RFA. Acute success was defined as the elimination of both antegrade and retrograde AP conduction, along with the absence of other arrhythmia substrates at the end of the 30-minute waiting period.
2.3. Follow-Up
All patients were routinely monitored for 24 hours after the procedure. A 12-lead ECG and echocardiography were performed before discharge. Another 12-lead ECG was obtained 2 weeks, 3 months, and 6 months after the ablation at our outpatient department or by the referring physician. Aspirin was continued for 6 weeks following left-sided procedures.
Recurrence is defined as the reappearance of anterograde AP conduction or SVT) as documented by ECG, 24-hour Holter monitoring, or through an event recorder. Palpitations alone are not considered a recurrence of arrhythmia. Long-term success is defined as the absence of any recurrence of manifest AP conduction or documented SVT during the follow-up period.
2.4. Statistical Analysis
The data were analyzed using version 21.0 of the Statistical Package for the Social Sciences. Descriptive features were expressed as percentages and mean ± standard deviation or as medians, depending on the distribution of the data as determined by the Kolmogorov–Smirnov test.
3. Results
3.1. Patient Characteristics
During the study period, 291 children underwent 336 EPS and 332 ablation procedures. Ten patients (3.5%) had previously received EPS at other centers. The mean age and weight of the patients were 11.8 ± 4.9 years and 48.8 ± 27.3 kg, respectively. Congenital heart disease was present in 21 patients. The youngest patient included in the study was a 4-month-old (5 kg) infant diagnosed with ’tachycardia-induced dilated cardiomyopathy’ that was resistant to multiple antiarrhythmic drugs. Two hundred twenty-five cases (73%) were diagnosed with WPW syndrome (140 with SVT, 71 with asymptomatic WPW, and 1 with pre-excited atrial fibrillation), while 79 cases (27%) were diagnosed with SVT. The demographic and clinical characteristics of the patients are summarized in Table 1.
3.2. Initial procedure
We identified 298 AP connections in the 291 patients. Seven (2.4%) patients had multiple APs, including three with Ebstein anomaly. The prevailing anatomic AP location was PS (n = 159; 54%), followed by AS (n = 86; 30%) and MS (n = 46; 16%).
Of those diagnosed with WPW, 61 (28%) had high-risk AP based on procedural features, with APERP, SPERRI, and SPPCL ≤ 250 ms; 77 (34.5%) had borderline risk since their APERP, SPERRI, and SPPCL measurements ranged from 251 to 300 ms; 82 (36.5%) patients were classified as low risk according to their APERP, SPERRI, and SPPCL measurements ≥ 300 ms; and 5 (1%) cases were classified as unknown (Table 2).
After the EPS, all patients except 3 underwent ablation procedures. In 70 (24%) cases, mapping was performed by stimulation SVT, in 116 (40%) cases by delta mapping, in 71 (25%) cases by both SVT stimulation and delta mapping, and in 31 (11%) cases by V-pacing mapping. Five (2%) AP connections showed “Mahaim-like AP” properties, which resulted in the prolongation of AH, shortening of HV, and negativity of VH intervals.
Cryoablation was used in 190 patients (66%), RFA in 36 patients (12.5%), and both RFA and cryoablation in 62 patients (21.5%). Irrigated RFA catheters were employed in 10 patients (3.4%). Cryoablation was conducted using a 6 mm-tipped catheter for 188 patients, an 8 mm-tipped catheter for 62 patients, and both types of catheters for 2 patients. The average number of complete cryoablation lesions was 6.2 ± 3.2.
The acute success rate of overall initial procedures was 89.6%. A transient successful effect of ablation was observed during the procedure, with immediate AP conduction returning in 7 patients. The acute success rate for cryoablation was 86.6%, showing the highest efficacy in MS and the lowest in PS locations (AS: 89.1%, MS: 91.1%, PS: 80.7%). The acute success rate for RFA was 94.1%. Thirty-two patients (11.1%) underwent epicardial ablations, with an acute success rate of 53.1%.
The overall recurrence rate was 11.3%, with the highest at the right-PS location (16.4%). Thirty-three patients presented with recurrences; 20 (61%) had WPW on baseline ECG, while 13 (39%) presented with documented SVT. The overall recurrence rate of cryoablation is 12.1%, with the highest at the PS location (18.9%).
In our electrophysiology practice, fluoroscopy is only utilized when a transseptal approach is required or in rare cases to confirm catheter position. Fluoroscopy was used for 39 patients (13.5%), with a mean fluoroscopy time of 5.2±3.7 minutes (range: 0.3-18.3). A transseptal puncture was performed in 22 cases (7.6%) to identify the optimal site in the left PS area. The mean procedure duration was 154±54 minutes (range: 54-340).
3.3. Redo procedure
During a mean follow-up of 88.5±33.0 months, 45 out of 291 patients underwent repeat procedures due to initial failure or recurrences. The second procedure was conducted an average of 19.2 months after the initial ablation, with an average of 1.2 procedures per patient.
The acute success rate of redo procedures was 95.3%. During these redo procedures, an irrigated RFA was preferred in 20 (45%) cases, all of which were PS locations (19 right-PS, 1 left-PS). Only 3 (1%) patients underwent ≥ 2 procedures for the initial substrate that recurred multiple times. Consequently, the long-term success rate reached 99% when considering the repeat procedures. A comparison of initial and redo procedures based on pathway locations and ablation outcomes is summarized in Table 3.
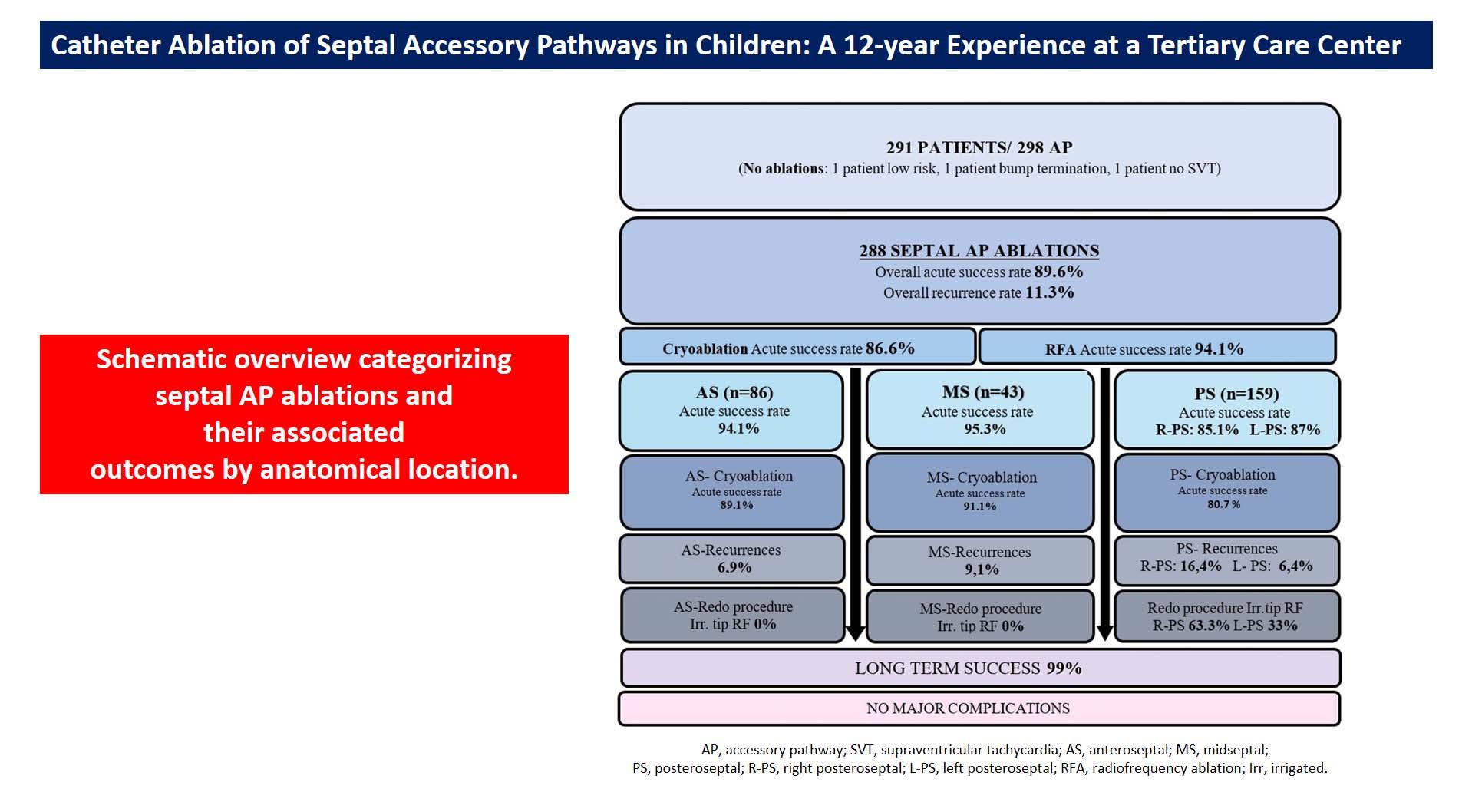
A schematic overview of the study categorizing septal AP ablations and their associated outcomes by anatomical location was presented in Figure 1.
3.4. Complications
Transient complete AV block occurred during energy delivery, and complete recovery was observed after tissue warming. At long-term follow-up, no permanent PR interval prolongation was observed, and we did not observe any other major complications, such as pericardial effusion and thrombotic events. None of the patients developed clinical or ECG signs of new-onset ischemia.
4. Discussion
The present study supports excellent contemporary pediatric data showing that the long-term high success rate of septal AP ablation, > 97%, can be achieved safely. We observed a moderate recurrence rate and a high long-term success rate, achieved with an average of 1.2 procedures per patient. Manifest APs and right-PS APs presented with the highest recurrence rate in the long term. RFA for the treatment of septal AP has higher overall acute and long-term efficacy rates than cryo energy. Cryoablation of PS APs showed the lowest acute and long-term efficacy rates compared to other septal APs. Furthermore, the other main finding of the present study was that irrigated-tip catheters are effective and safe for right-PS APs resistant to conventional RFA or for ones who presented with recurrences.
Cryoablation has emerged as a safe alternative to RFA for various arrhythmogenic substrates, particularly in the septal region among young patients with reduced dimensions of Koch’s triangle and overall tissue thickness [2]. The significance of precise mapping and catheter stability is paramount, yet a notable drawback is the stiffness of the catheter, complicating manipulation in small hearts [15]. Studies involving pediatric and adult populations have reported similar acute success rates for cryoablation and RFA, albeit with higher recurrence rates for cryoablation. Bar-Cohen et al. reported an acute success rate of 78% and a recurrence rate of 45% over an average follow-up period of 207 days. The risk of recurrence was noted to be particularly elevated in MS locations. The low success and high recurrence rates were attributed to the use of a 4 mm–tip cryocatheter in 89% of cases [7]. We previously reported the acute success rate of cryoablation for eliminating AS APs was 95.8%, with a short-term recurrence rate of 8.7% [16]. Bastani et al. observed a similar acute success rate but with a higher recurrence rate of 27% during an average follow-up of 33 months [5].
The first meta-analysis of 4,244 pediatric cohort articles comparing the efficacy and safety of cryoablation versus RFA for septal substrates reported similar acute procedural success rates for cryoablation and RFA (86% and 89%, respectively) [17]. However, it was noted that efficacy was highly dependent on the AP) location. The acute procedural success rate of cryoablation was highest for parahissian APs and lowest for posteroseptal (PS) APs. The recurrence rate for cryoablation was 18.1%, while it was 9.9% for RFA. Despite their similar acute efficacy rates, the meta-analysis demonstrates the superiority of RFA over cryoablation regarding long-term efficacy outcomes. When analyzing results according to AP location, cryoablation’s long-term outcomes for parahissian APs are comparable to those achieved by RFA, but its long-term efficacy at other septal locations was significantly lower. We reported an acute success rate of 93% for cryoablation and a recurrence rate of 12.5% for septal APs during mid-term follow-up from our center [18]. In our study, the overall success rate of initial procedures was 89.6%, and the recurrence rate was 11.3% in an extended pediatric case series with longer follow-up. Both RFA and cryoablation demonstrated excellent acute outcomes. The procedure’s success was highly dependent on the AP location, with the highest efficacy observed in midseptal (MS) locations and the lowest in PS locations.
The PS region of the heart is likely the most complex area for catheter ablation and is associated with a higher recurrence rate. A common reason for unsuccessful ablation attempts with the standard endocardial approach is the epicardial localization of the APs, which may necessitate intervention within the CS [19,20]. Recent studies suggest that the possibility of a CS diverticulum should be considered in cases of failed ablation attempts in the CS [15,20,21]. A previously published study involving 51 patients with a PS pathway found that 31% had a CS diverticulum [22]. Furthermore, a CS diverticulum was reported in 40% of patients undergoing CS ablations [19]. Some studies routinely recommend coronary vein angiography to detect coronary vein anomalies during PS ablations to enhance acute success [23]. In the study by Collins et al., cryoablation in the CS was successful in 71% of cases [21]. Due to the low acute success rates and high recurrence rates associated with cryoenergy, data indicated that RFA was predominantly used in adult studies with better outcomes [21,22]. Raja J. Selvaraj et al. collected data on adults who underwent ablation of PS APs with manifest preexcitation, comparing cases by dividing them into two groups based on the presence or absence of diverticulum [22]. RF energy was used for ablation in all cases. The acute procedural success rate was 88% in the diverticulum group and 97% in the non-diverticulum group. Our findings align with those of previous studies, showing that epicardial ablations had the highest number of unsuccessful applications. Since routine venography was not performed prior to CS ablations, the possibility of a coronary diverticulum may have been overlooked, potentially contributing to procedural failure. Coronary artery injury represents the most significant concern associated with intra-CS ablation with RF energy [15]. In a comprehensive study involving 68 ablation procedures in 62 patients, Alazard et al. conducted coronary angiography in 29 cases before and after the procedure [24]. In 12 cases, the ablation area was found to be in close proximity to the coronary artery, with a distance of less than 5 mm. In these cases, coronary damage was observed in 3 patients, with two cases involving an irrigated RF catheter and one case involving a non-irrigated RF catheter. In contrast, no coronary artery injury was reported in patients with a true safety margin. Although we did not perform coronary artery angiography in any patients before the procedure, all patients were closely monitored for electrocardiographic ST changes for ischemia throughout the procedure. None of the patients developed clinical or ECG signs of new onset ischemia.
In addition to the epicardial location in the PS area, the causes of recurrence were likely multiple, including insufficient lesion depth and inadequate energy delivery. Over the years, studies have indicated that irrigated RF energy is more effective on deep myocardial or epicardial substrates than on superficial endocardial structures [25,26]. Kamali et al. reported that their high success rate for CS ablations is linked to the use of irrigated RFA. In the study by Yamane et al., irrigated RFA (often used after conventional RFA) was associated with improved procedural success in right-PS APs [27]. In our study, the overall acute success rate for right-PS APs was 85.1%. Furthermore, right-PS APs exhibited the highest long-term recurrence rate (16.4%). Cryoablation demonstrated the lowest acute efficacy rate for the PS AP location. Consequently, we primarily utilized irrigated RFA in 60.6% of PS redo procedures. Given the numerous heat-related complications, including perforation, coronary damage, and the risk of venous stenosis in CS, we administered irrigated RF energy in a temperature-controlled mode ranging from 15-25 W within the CS and 25-35 W in the PS area. We attribute the low complication rate to these measures. Despite technological improvements, extensive RFA experience, and cautious RF applications, the iatrogenic incidence of undesired AV block during septal ablations is still non-negligible. No case of persistent AV block was reported using cryoablation, whereas RFA accounts for between 2 and 10 % [4,17,28]. Knowledge of these risks may influence both the patient’s and the electrophysiologists’ decisions. For instance, in a wide pediatric case series by Mandapati et al. (127 patients with 145 septal APs), RF ablation could not be performed [28].Due to the high risk of AV block, the electrophysiology study had to be stopped in 17 % of patients with anteroseptal APs and 15 % of patients with midseptal APs. Similarly, Ergul et al. reported that RFA was not performed in 29% of their patients who underwent previous EPSs at other centers due to the high risk of AV block [16]. So, despite the concerns regarding a greater recurrence rate, cryo energy has been recommended for AS and MS locations due to AV block risk reported for RFA [4,5,6,7,8,28]. In our study, only cryoablation was preferred in 94.1% of AS and 76% of MS APs. There were no instances of permanent damage to normal conduction in our series. Besides monitoring AV node conduction closely during mapping and ablation, we emphasize confirmation of underlying intact AV node conduction with differential atrial pacing maneuvres before and during the ablation. Using long sheaths, a superior approach via the jugular vein in selected patients, and performing the ablation during apnea may also increase catheter stability and help limit the risk of AV node injury.
Previous studies have reported that Ebstein’s anomaly poses a risk for failed ablation and recurrence, with difficulties being related to the high prevalence of multiple pathways and the lack of catheter stability caused by the displacement of the tricuspid valve [15,29]. Walsh et al. found similar results, noting that Ebstein malformation does not predict procedural failure or recurrence [30]. In our study, we did not observe procedural failure or recurrence in patients diagnosed with Ebstein’s anomaly. However, we believe that the limited number of patients in our study is insufficient to draw such a conclusion.
We have achieved an excellent long-term success rate within our patient group. It can be argued that reversible tissue injury represents a relative weakness of cryoablation concerning recurrence risk. However, this aspect may also be a major strength of the technology when ablating near-normal conduction tissues. In our opinion, utilizing a larger catheter tip size and a greater number of cryo-energy applications could significantly affect the overall long-term success rate of cryoablation. This is because the freeze-thaw–freeze technique has been reported to result in more effective lesion formation. Particularly with the use of RFA energy, the potential benefit of consolidated lesions must be weighed against the risk of AV nodal conduction and coronary artery injury. In such cases, it may be appropriate to limit consolidation time and accept a reasonable risk of recurrence. Additionally, employing a 3D electroanatomic mapping system aids in targeting locations and helps place the insurance lesions at precise anatomical locations. Furthermore, redo procedures may be enhanced by incorporating steerable long sheaths, the implantation of irrigated RF catheter technologies, and utilizing angiograms to better understand the anatomy. These strategies have the potential to improve long-term outcomes.
5. Study Limitations
This study represents a retrospective review of ablation procedures. Coronary sinus injection was not performed prior to CS ablations, which may be linked to the low acute success rates of ‘epicardial’ ablations. While we investigated the failure and recurrence rates, the underlying factors leading to procedural failures or recurrences were beyond the scope of the study study.
6. Conclusions
Despite impressive acute success rates, recurrences remain higher in septal AP ablations compared to other locations. Therefore, repeated procedures may be necessary to achieve definitive long-term success. An irrigated-tip RFA may help target deep myocardial or epicardial substrates for epicardial PS pathways. The results of this study indicate that comparable acute and long-term success rates can be achieved with cryoablation compared to RF ablation, along with the significant added benefit of increased safety with cryoablation in this patient group.
Author Contributions
Methodology, O.T. and C.A.; software, O.T., C.A and V.T.; investigation, O.T. and C.A.; data curation, O.T., C.A and V.T.; writing—original draft, O.T.; writing—review and editing, O.T., C.A and V.T.; supervision, C.A. and V.T.; project administration, O.T., C.A and V.T. All authors have read and agreed to the published version of the manuscript.
Funding
This study was conducted without financial support from any specific funding source.
Institutional Review Board Statement
This study was conducted following the Declaration of Helsinki, and the Antalya Training and Research Hospital Ethics Committee approved the protocol (approval code date and code: …………..).
Informed Consent Statement
In accordance with national legislation and institutional requirements, written informed consent from the participants’ legal guardians or next of kin was not necessary for participation in this study. Patient consent was waived due to the retrospective status of this study.
Data Availability Statement
Data are not publicly accessible due to patient privacy considerations; however, they can be obtained from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
APs: Accessory pathways
WPW: Wolff-Parkinson-White syndrome
RFA: Radiofrequency ablation
References
- Haghjoo, M.; Kharazi, A.; Fazelifar, A.F.; Alizadeh, A.; Emkanjoo, Z.; Sadr-Ameli, M.A. Electrocardiographic and electrophysiologic characteristics of anteroseptal, midseptal, and posteroseptal accessory pathways. Hear. Rhythm. 2007, 4, 1411–1419. [Google Scholar] [CrossRef]
- Schneider, H.E.; Kriebel, T.; Gravenhorst, V.D.; Paul, T. Incidence of coronary artery injury immediately after catheter ablation for supraventricular tachycardias in infants and children. Hear. Rhythm. 2009, 6, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Katritsis, DG.; Boriani, G.; Cosio, FG.; Hindricks, G.; Ja ̈ıs, P.; Josephson, ME. European Heart Rhythm Association (EHRA) consensus document on the management of supraventricular arrhythmias, endorsed by Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), and Sociedad Latinoamericana de Estimulacio ́n Cardiaca y Electrofisiologia (SOLAECE). Europace. 2017, 19, 465–511. [Google Scholar] [PubMed]
- Schaffer, M.S.; Silka, M.J.; Ross, B.A.; Kugler, J.D. Inadvertent Atrioventricular Block During Radiofrequency Catheter Ablation. Results of the Pediatric Radiofrequency Ablation Registry. Pediatric Electrophysiology Society. Circulation 1996, 94, 3214–3220. [Google Scholar] [CrossRef]
- Bastani, H.; Insulander, P.; Schwieler, J.; Tabrizi, F.; Braunschweig, F.; Kennebäck, G.; Drca, N.; Jensen-Urstad, M. Cryoablation of superoparaseptal and septal accessory pathways: a single centre experience. Eur. 2010, 12, 972–977. [Google Scholar] [CrossRef]
- Gaita, F.; Riccardi, R.; Hocini, M.; Haissaguerre, M.; Giustetto, C.; Jais, P.; Grossi, S.; Caruzzo, E.; Bianchi, F.; Richiardi, E. Safety and Efficacy of Cryoablation of Accessory Pathways Adjacent to the Normal Conduction System. J. Cardiovasc. Electrophysiol. 2003, 14, 825–829. [Google Scholar] [CrossRef]
- Bar-Cohen, Y.; Cecchin, F.; Alexander, M.E.; Berul, C.I.; Triedman, J.K.; Walsh, E.P. Cryoablation for accessory pathways located near normal conduction tissues or within the coronary venous system in children and young adults. Hear. Rhythm. 2006, 3, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Tuzcu, V. Cryoablation of Accessory Pathways in Children. Pacing Clin. Electrophysiol. 2007, 30, 1129–1135. [Google Scholar] [CrossRef]
- Liberman, L.; Spar, DS.; Nash, MC.; Silver, ES. Cryoablation of anteroseptal accessory pathways with a His bundle electrogram on the ablation catheter. Indian Pacing Electrophysiol J. 2014, 6, 284–290. [Google Scholar] [CrossRef]
- Saul, J.P.; Kanter, R.J.; Abrams, D.; Asirvatham, S.; Bar-Cohen, Y.; Blaufox, A.D.; Cannon, B.; Clark, J.; Dick, M.; Freter, A.; et al. PACES/HRS expert consensus statement on the use of catheter ablation in children and patients with congenital heart disease. Hear. Rhythm. 2016, 13, e251–e289. [Google Scholar] [CrossRef]
- Consensus Statement from the Cardiac Nomenclature Study Group of Arrhythmias of the European Society of Cardiology, and the Task Force on Cardiac Nomenclature from the North American Society of Pacing and Electrophysiology on Living Anatomy of the Atrioventricular Junction. J Cardiovasc Electrophysiol. 2000, 11, 1297–1297.
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomström-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.-P.; et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur. Hear. J. 2019, 41, 655–720. [Google Scholar] [CrossRef]
- Pediatric and Congenital Electrophysiology Society (PACES). ; Heart Rhythm Society (HRS).; American College of Cardiology Foundation (ACCF).; American Heart Association (AHA).; American Academy of Pediatrics (AAP).; Canadian Heart Rhythm Society (CHRS).; Cohen MI.; Triedman JK.; Cannon BC.; Davis AM.; et al. PACES/HRS expert consensus statement on the management of the asymptomatic young patient with a Wolf–Parkinson–White (WPW, ventricular preexcitation) electrocardiographic pattern: developed in partnership between the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Endorsed by the governing bodies of PACES, HRS, the American College of Cardiology Foundation (ACCF), the American Heart Association (AHA), the American Academy of Pediatrics (AAP), and the Canadian Heart Rhythm Society (CHRS). Heart Rhythm. 2012, 9, 1006–1024.
- Etheridge, SP.; Escudero, CA.; Blaufox, AD.; Law, IH.; DechertCrooks, BE.; Stephenson, EA.; Dubin, AM.; Ceresnak, SR.; Motonaga, KS.; Skinner, JR.; et al. Life threatening event risk in children with Wolf–Parkinson–White Syndrome: a multicenter international study. JACC Clin Electrophysiol. 2018, 4, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Corcia, M.C.G.; Stuart, G.; Walsh, M.; Radulescu, C.; Spera, F.; Tijskens, M.; Heidbuchel, H.; Sarkozy, A. Redo accessory pathway ablation in the pediatric population. J. Interv. Card. Electrophysiol. 2021, 63, 639–649. [Google Scholar] [CrossRef]
- Ergul, Y.; Tola, H.T.; Kiplapinar, N.; Akdeniz, C.; Saygi, M.; Tuzcu, V. Cryoablation of Anteroseptal Accessory Pathways in Children With Limited Fluoroscopy Exposure. Pediatr. Cardiol. 2012, 34, 802–808. [Google Scholar] [CrossRef]
- Bravo, L.; Atienza, F.; Eidelman, G.; Ávila, P.; Pelliza, M.; Castellanos, E.; Loughlin, G.; Datino, T.; Torrecilla, EG.; Almendral, J.; et al. Safety and efficacy of cryoablation vs. radiofrequency ablation of septal accessory pathways: systematic review of the literature and meta-analyses. Europace. 2018, 20, 1334–1342. [Google Scholar] [PubMed]
- Karadeniz, C.; Akdeniz, C.; Turan, O.; Tuzcu, V. Cryoablation of Septal Accessory Pathways in Children: Midterm Results. Pacing Clin. Electrophysiol. 2014, 37, 1095–1099. [Google Scholar] [CrossRef]
- Kamali, H.; Kafali, H.C.; Caran, B.; SULU, A.; Ergul, Y. Coronary sinus ablations in pediatric patients with supraventricular arrhythmias. J. Interv. Card. Electrophysiol. 2023, 66, 2153–2164. [Google Scholar] [CrossRef]
- Drago, F.; Tamborrino, PP.; Pazzano, V.; Di Mambro, C.; Silvetti, MS. 3D transvenous radiofrequency ablation of manifest epicardial posterior-septal accessory pathways in children: Can technology innovations improve the outcome? Cardiol Young. 2022, 32, 1229–1234. [Google Scholar] [CrossRef]
- Collins, K.K.; Rhee, E.K.; Kirsh, J.A.; Cannon, B.C.; Fish, F.A.; Dubin, A.M.; VAN Hare, G.F. Cryoablation of Accessory Pathways in the Coronary Sinus in Young Patients: A Multicenter Study from the Pediatric and Congenital Electrophysiology Society's Working Group on Cryoablation. J. Cardiovasc. Electrophysiol. 2007, 18, 592–597. [Google Scholar] [CrossRef]
- Selvaraj, R.J.; Sarin, K.; Singh, V.R.; Satheesh, S.; Pillai, A.A.; Kumar, M.; Balachander, J. Radiofrequency ablation of posteroseptal accessory pathways associated with coronary sinus diverticula. J. Interv. Card. Electrophysiol. 2016, 47, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Raatikainen, M.P.; Pedersen, A.K. Catheter ablation of a difficult accessory pathway guided by coronary sinus venography and 3D electroanatomical mapping. Eur. 2010, 12, 1200–1201. [Google Scholar] [CrossRef] [PubMed]
- Alazard, M.; Lacotte, J.; Horvilleur, J.; Ait Said, M.; Salerno, F.; Manenti, V.; Piechaud, JF.; Garot, J.; Bonnet, D.; Maltret, A. Preventing the risk of coronary injury in posteroseptal accessory pathway ablation in children: different strategies and advantages of fluoroscopy integrated 3D-mapping system (CARTO-UNIVUTM). J Interv Card Electrophysiol. 2018, 52, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Telishevska, M.; Faelchle, J.; Buiatti, A.; Busch, S.; Reents, T.; Bourier, F.; Semmler, V.; Kaess, B.; Horndasch, M.; Kornmayer, M.; et al. Irrigated-tip catheters for radiofrequency ablation of right-sided accessory pathways in adolescents. Pacing Clin. Electrophysiol. 2017, 40, 1167–1172. [Google Scholar] [CrossRef]
- Gulletta, S.; Tsiachris, D.; Radinovic, A.; Bisceglia, C.; Mazzone, P.; Trevisi, N.; Paglino, G.; Bellini, B.; Sala, S.; DELLA Bella, P. Safety and Efficacy of Open Irrigated-Tip Catheter Ablation of Wolff-Parkinson-White Syndrome in Children and Adolescents. Pacing Clin. Electrophysiol. 2013, 36, 486–490. [Google Scholar] [CrossRef]
- Yamane, T.; Jaïs, P.; Shah, D.C.; Hocini, M.; Peng, J.T.; Deisenhofer, I.; Clémenty, J.; Haïssaguerre, M. Efficacy and Safety of an Irrigated-Tip Catheter for the Ablation of Accessory Pathways Resistant to Conventional Radiofrequency Ablation. Circulation 2000, 102, 2565–2568. [Google Scholar] [CrossRef]
- Mandapati, R.; Berul, CI.; Triedman, JK.; Alexander, ME.; Walsh, EP. Radiofrequency catheter ablation of septal accessory pathways in the pediatric age group. Am J Cardiol. 2003, 92, 947–950. [Google Scholar] [CrossRef]
- Iturralde, P.; Guevara-Valdivia, M.; Rodríguez-Chávez, L.; Medeiros, A.; Colin, L. Radiofrequency ablation of multiple accessory pathways. Eur. 2002, 4, 273–280. [Google Scholar] [CrossRef]
- Walsh, M.A.; Gonzalez, C.M.; Uzun, O.J.; McMahon, C.J.; Sadagopan, S.N.; Yue, A.M.; Seller, N.; Hares, D.L.; Bhole, V.; Till, J.; et al. Outcomes From Pediatric Ablation: A Review of 20 Years of National Data. 2021; 7, 1358–1365. [Google Scholar] [CrossRef]
Figure 1.
Schematic overview categorizing septal AP ablations and their associated outcomes by anatomical location. AP, accessory pathway; SVT, supraventricular tachycardia; AS, anteroseptal; MS, midseptal; PS, posteroseptal; R-PS, right posteroseptal; L-PS, left posteroseptal; RFA, radiofrequency ablation; Irr, irrigated.
Figure 1.
Schematic overview categorizing septal AP ablations and their associated outcomes by anatomical location. AP, accessory pathway; SVT, supraventricular tachycardia; AS, anteroseptal; MS, midseptal; PS, posteroseptal; R-PS, right posteroseptal; L-PS, left posteroseptal; RFA, radiofrequency ablation; Irr, irrigated.
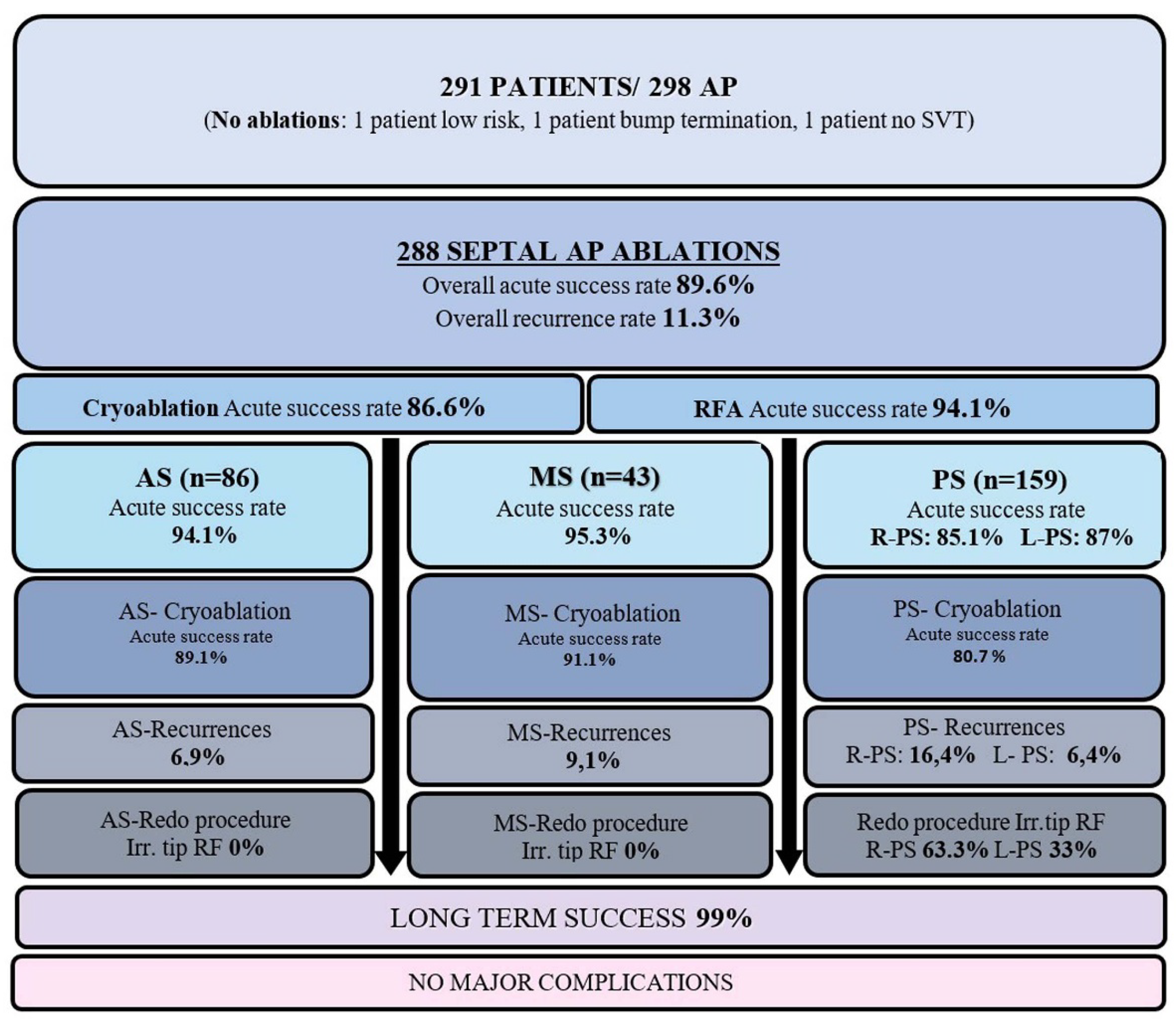

Table 1.
Demographic and clinical characteristics of 291patients.
| Characteristics | |
| Age (years) | 11.8 ± 4.9 |
| Gender (M/F) | 171/120 |
| Weight (kg) | 48.8± 27.3 |
|
Echocardiogram findings VSD Ebstein’s anomaly TOF D-TGA CAVSD Dextrcardia/Tricuspit atresia/DOLV/PB Bicuspit Aorta /Aortic insufficiency HCM DCM |
2 7 2 1 1 1 4 2 1 |
|
Endications of procedure (ECG findings) Asymptomatic WPW WPW-SVT Pre-excited Atrial Fibrillation SVT |
71 (24.5%) 140 (48.1%) 1 (0.3%) 79 (27.1%) |
| Prior EPS (at another center) | 10 (3.4%) |
| Follow-up time (months) | 88.5±33.0 |
F=Female; M=Male; VSD=Ventricular septal defect; TOF=Tetralogy of Fallot; D-TGA=D-Transposition of the Great Arteries; CAVSD=Complete atrioventricular septal defect; PB=Pulmonary Banding; HCM=Hypertrophic cardiomyopathy; DCM=Dilated cardiomyopathy; WPW= Wolf Parkinson White syndrome; SVT= Supraventricular tachycardia; ECG= Electrocardiogram.
Table 2.
Initial procedure characteristics of 291patients.
| n (%) | |
| Multiple AP* | 7 (2.4%) |
|
AP characteristics (n) Manifest AP (WPW) Concealed AP Permanent junctional reciprocating tachycardia |
298 225 (75.5%) 71 (23.8%) 2 (0.67%) |
|
Risk classification of AP APERP, SPERRI, and SPPCL ≤ 250 msn APERP, SPERRI, and SPPCL = 251–300 msn APERP, SPERRI, and SPPCL ≥ 300 msn Unknown |
225 61 (28%) 77 (34.5%) 82 (36.5%) 5 (1%) |
| APERP | 294.4 ± 5.3 |
| Adenosine responsive | 90 (40%) |
|
Septal AP locations Anteroseptal Midseptal Posteroseptal Right Left |
291 86 (29.5%) 46 (15.8%) 159 128 (43.9%) 31 (10.6%) |
| Epicardial ablation | 32 (11.1%) |
| Second arrhythmia substrate (AVNRT) | 22 (7.5%) |
|
Use of fluoroscopy (n) Transseptal puncture Other reasons |
39 (13.4%) 22 17 |
| Total fluoroscopy time (min) | 5.2±3.7 (0.3-18.3) |
| Procedure time (min) | 154±54 (54-340) |
* 3 left lateral, 1 left posterior, 2 right posterior, 1 right lateral location. AP=Accessory pathway; WPW=Wolf Parkinson White syndrome; APERP=Effective refractory period of the accessory pathway; SPERRI=Shortest pre-excitatory RR interval; SPPCL=Shortest paced cycle length with preexcitation during rapid atrial pacing; AVNRT= Atrioventricular nodal reentrant tachycardia.
Table 3.
AP location and ablation outcomes.
| Septal APs | ||||
| Anteroseptal | Midseptal | Posteroseptal | ||
| (n) | (n) | (n) | ||
| INITIAL PROCEDURES | Right-PS | Right-PS | ||
| EPS (n=291) | 86 | 46 | 128 | 31 |
| Ablations (n=288) | 86 | 43 | 128 | 31 |
| Ablation source (%) | ||||
| Cryo (66%) | 81 | 35 | 68 | 6 |
| RF (10,4%) | 0 | 2 | 10 | 18 |
| RF + cryo (20,1%) | 5 | 5 | 43 | 5 |
| Irrigated tip RF+ cryo (1.5%) | 0 | 1 | 3 | 0 |
| Irrigated tip RF (1.4%) | 0 | 0 | 4 | 0 |
| RF+ Irrigated tip RF (0.7%) | 0 | 0 | 0 | 2 |
| Transient complete AV block (4.8%) | 8 | 3 | 3 | 0 |
| Acute success rate (89.6%) | 81 (94.1%) | 41 (95.3%) | 109 (85.1%) | 27 (87.0%) |
| Recurrence rate (11.3%) | 6 (6.9%) | 4 (9.1%) | 21 (16.4%) | 2 (6.4%) |
|
REDO PROCEDURES (Initial procedure failure+ recurrences |
||||
| EPS (n=45) | 5 | 6 | 31 | 3 |
| Ablations (n=44) | 5 | 6 | 30 | 3 |
| Ablation source | ||||
| Cryo (29.5%) | 5 | 3 | 5 | 0 |
| RF (20.9%) | 0 | 2 | 5 | 2 |
| RF + cryo (4.6%) | 0 | 1 | 1 | 0 |
| Irrigated RF (44.1%) | 0 | 0 | 18 | 1 |
| RF+ Irrigated RF (2.3%) | 0 | 0 | 1 | 0 |
| Transient complete AV block (4.6%) | 2 | 0 | 0 | 0 |
| Acute success rate (95.3%) | 5 (100%) | 5 (83.3%) | 28 (93.3%) | 3 (100%) |
| Long term success rate (99%) | 100% | 97.6% | 98.4 % | 100% |
AP=Accessory pathway; EPS=Electrophysiological study; Cryo=Cryoablation; RF=Radiofrequency; AV=Atrioventricular block.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



