Submitted:
17 February 2025
Posted:
18 February 2025
You are already at the latest version
Abstract
Background: A remarkable increase in metabolic comorbidities occur in people living with HIV infection (PLWH). Supervised physical activity provides significant health benefits. Ginkgo biloba (GKB) extract has been reported to have a wide range of metabolic advantages. This study aimed to examine the effects of an exercise training (ET) program and a GKB extract on PLWH. Methods: This was a randomized placebo-controlled double-blind study. Twenty-eight PLWH were assigned to receive a placebo (n=10), GKB extract (n=10), or statins (n=8). All patients underwent a supervised ET program 3-5 times per week. Anthropometric measurements, functional capacity, and metabolic parameters were assessed in all participants at baseline and after 12 weeks of follow-up. Results: After the 12-week intervention, body fat decreased significantly by 2-3% in all groups relative to their baseline values (p<0.05). Total cholesterol and LDL-c were significantly decreased in the ET+statin group (p= 0.04, and p= 0.007, respectively) compared to baseline values, while HbA1c and the HOMA-IR index were significantly decreased in the ET+GKB group (p= 0.03 and p= 0.02, respectively) compared to baseline values, and a significant increase in CD4+ T cell mean was observed in the ET+placebo group (p=0.005) compared to baseline values. A significant increase in cardiorespiratory capacity (VO2 max) from their baseline values was observed in all groups (p<0.001) after 12-weeks of intervention from their baseline values. Conclusions: Body fat and cardiorespiratory fitness significantly improved after a 12-week supervised ET program. GKB extract significantly decreased insulin resistance. Future studies with larger sample sizes are required.
Keywords:
Physical activity
; Exercise training
; HIV infection
; Ginkgo biloba
; Statins
1. Introduction
An increase in the life expectancy of people living with HIV (PLWH) due to antiretroviral therapy (ART) has led to an increase in the burden of non-communicable diseases in this population[1]. PLWH have a high prevalence of obesity-related comorbidities, including dyslipidemia, type 2 diabetes mellitus (T2DM), hypertension, and chronic kidney disease[2]. The risk of cardiovascular disease (CVD) is 2-fold higher in PLWH,[3] and non-AIDS-related mortality rates are largely attributable to CVD[4].
Weight gain with contemporary ART based on integrase strand transfer inhibitors (INSTI)-containing regimens and tenofovir alafenamide (TAF) has been well documented [5,6,7]. The proportion of metabolically unhealthy individuals is higher in HIV-infected people with excessive weight and central obesity [8].
Studies have shown that physical activity (PA) has multiple health benefits for PLWH, including cardiovascular health[9], functional capacity[10], improvements in metabolic parameters[11], body muscle strength[12], body composition, [13] and quality of life (QoL)[14]. However, it has been reported that PA is lower in HIV-infected than in most other populations with chronic diseases, and more than half of PLWH do not meet the physical activity recommendations of the World Health Organization (WHO) of at least 150 minutes of moderate-intensity physical activity per week[15].
Cardiometabolic disease management strategies, including the use of medicinal herbs, have been used worldwide. Ginkgo biloba (GKB), an herb used in traditional Chinese medicine for thousands of years, has high medicinal value because it contains flavonoids, treptene lactones, and phenolic compounds[16]. GKB has various properties, including antioxidants, free radical scavenging, membrane-stabilizing, anti-inflammatory, anti-platelet activating factors, antihypertensive, vasodilatory, cardioprotective, neuroprotective, anti-apoptotic, and anticancer activities[16].
It is a well-known plant that is used to treat atherosclerosis, ischemic heart disease, dementia, cerebrovascular insufficiency, hypertension, and peripheral arterial occlusive disease[17,18,19]. Experimental and clinical studies have reported metabolic benefits in hypertriglyceridemia and hypoglycemic properties; therefore, GKB supplementation has been used to treat dyslipidemia and to prevent or treat T2DM[20,21,22].
Considering the increased prevalence of metabolic abnormalities in PLWH, we investigated the effect of an exercise training (ET) program alone or in combination with supplementation of GKB or statins in this population.
2. Materials and Methods
2.1. Design and Approval of the Study
This was a single-center, randomized, double-blind, placebo-controlled, parallel group study, with a three-arm group, conducted in Guadalajara, Jalisco, Mexico, in accordance with the ethical principles of the World Medical Association for Medical Research involving human subjects. This study was approved by the Ethics Committee of the Hospital Civil de Guadalajara (no.165/21) and was registered at ClinicalTrials.gov (identifier NCT06403787). The purpose of the study was explained to the participants and written informed consent was obtained before screening and data collection.
The eligibility criteria for the intervention groups were as follows: HIV-infected men aged 18-55 years on ART with coformulated bictegravir, emtricitabine, and tenofovir alafenamide, with at least six months of undetectable HIV viral load, CD4+ T cell count >200 cells/µL, and mixed dyslipidemia with two or more abnormal findings: total cholesterol ≥200 mg/dL, LDL-c ≥100 mg/dL, HDL-c ≤40 mg/dL, and triglycerides ≥150 mg/dL. The exclusion criteria were active hepatitis B and C infection, heavy alcohol use (≥15 drinks per week), known hypersensitivity to Ginkgo biloba extract or statins, and use of any dietary supplement within 30 days of study enrollment.
2.2. Randomization and blinding
After eligibility was confirmed, the patients were randomized into three groups (allocation ratio 1:1:1) using computer-generated random numbers to receive GKB extract 120 mg QD, atorvastatin 20 mg QD, or placebo (figure 1).
2.3. Procedures
All subjects participated in a supervised aerobic ET program 3-5 times per week for 12 weeks. Exercise intensity gradually increased; in the first 4 weeks, the intensity was 50-60% heart rate maximum (HRmax), and in the next 8 weeks, it increased to 60-80%. The duration of the exercise was 50 min per session; each exercise session included a 5-minute warm-up and 5 minutes cool-down period with stretching exercises. The sessions were conducted in a gym close to the center and were supervised by an exercise researcher.
2.4. Measurements
At the baseline visit and after 12 weeks, functional capacity, including VO2max (middle step test), strength (back-leg and hand-held dynamometers), flexibility (Sit and Reach test), and balance (single-leg stance balance test), in addition to anthropometric measurements were evaluated in all participants, who were given a diary to record medication adherence and report adverse events, and received dietary counseling. All patients attended visits every 4 weeks to the center to evaluate adherence to the ET program, intake of the study medication, reporting of adverse events, changes in functional capacity through the previously mentioned physical tests and anthropometric measurements, and completion of the IPAQ short-version questionnaire.
Laboratory tests to assess the metabolic profile were performed in a fasting state at the baseline visit and week 12, including hematology, glucose, creatinine, urea, BUN, total cholesterol, LDL-c, HDL-c, VLDL-c, triglycerides, total, direct, and indirect bilirubin, total protein, albumin, AST, ALT, GGT, alkaline phosphatase, insulin, and HbA1c. The Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) was calculated according to Matthews et al.[23], a value >2.5 was used as a cutoff for insulin resistance;
2.5. Statistical Analysis
The sample size for this pilot study considered recommendations when there was no information from previous research to base sample calculations[24]. The Shapiro-Wilk test was used to analyze the normality distribution of the quantitative variables. Non-normally distributed data were analyzed using nonparametric statistical tests. Quantitative variables are expressed as mean ± standard deviation (SD) or median (interquartile range); qualitative variables are expressed as frequency (n) and percentage (%). One-way ANOVA or Kruskal-Wallis test was used to compare quantitative variables between the three study groups. Friedman’s test was used to compare final and initial intragroup values . Data was analyzed using SPSS version 20. Statistical significance was set at p <0.05.
3. Results
Twenty-eight HIV-infected patients were included in this study. All the patients underwent supervised ET. Ten patients received placebo (ET + Placebo), 10 received GKB extract (ET + GKB), and 8 patients received statin (ET + Statin). When comparing the baseline demographic variables between the study groups, significantly higher levels of ALT, urea, and BUN were found in the ET + Statin group than in the ET + GKB group (p<0.05). No other significant differences were observed between groups (Table 1).
No significant differences were observed in the anthropometric variables after 12- week intervention between the three groups. The effect on metabolic variables after 12- week intervention showed a significant decrease in total cholesterol in the group receiving statins compared to that in the other two groups (p <0.05) (Table 2).
Body fat decreased significantly by 2-3% at the end of the 12-week intervention in all three groups relative to their baseline values (p<0.05) (figure 2a). Waist circumference (WC) also decreased significantly in participants receiving statins compared with baseline values (p= 0.009).
Total cholesterol and LDL-c were significantly decreased in the ET + statin group at the end of the study (p= 0.04 and p= 0.007, respectively) compared to baseline values (figure 2b), while HbA1c (figure 2c) and the HOMA index (figure 2d) were significantly decreased in the ET + GKB group (p= 0.03 and p= 0.02, respectively) compared to baseline values, and a significant increase in CD4+ T cell mean was observed in the ET + Placebo group (p=0.005) compared to baseline values.
A significant increase in cardiorespiratory capacity (VO2 max) from their baseline values was observed in all three groups (p<0.001) after 12-weeks of intervention from their baseline values, in addition to a significant increase in back strength in the ET + GKB group (p= 0.02) and flexibility in the ET + statin group (P=0.02) (Table 3).
4. Discussion
The prevalence of chronic comorbidities in PLWH is high[25], and a strategy that has demonstrated health benefits in this population is PA[13]. There is evidence that PA reduces the risk of chronic diseases including obesity, T2DM, osteoporosis, breast and colon cancer and coronary artery disease in the general population[26]. Studies on supervised and unsupervised PA have shown greater benefits when the activity is supervised[27], and supervised PA has been reported to improve functional capacity [28] and adherence in PLWH[29]. We found a significant reduction in total body fat with supervised aerobic ET in all groups, which is in accordance with other studies that have reported improvements in body fat and body composition in PLWH with supervised aerobic PA[30,31]. Resistance exercise and combined aerobic and resistance exercise have also demonstrated benefits in terms of body fat, body composition, muscle strength, cardiorespiratory fitness, and quality of life in PLWH[28,32,33,34].
PA has also shown multiple metabolic benefits including improvements in insulin resistance, blood lipid levels, and hepatic fat content, regardless of weight loss[35]. A reduction in the risk of diabetes with significant improvements in glucose and insulin, both fasting and postprandial, HOMA-IR, weight, systolic blood pressure, and triglycerides was found in a 6-month intervention study with diet and physical activity in PLWH and impaired fasting glucose[36]. Similarly, advanced glycation products (proteins or lipids that become glycated as a result of exposure to reduced sugars) are implicated in the risk of the development of cardiovascular disease, diabetes, and other chronic diseases, and triglycerides were significantly decreased after a supervised training program of combined exercise (aerobic, resistance, and flexibility) for three months in physically inactive HIV-infected subjects[11]. In our study, we did not find a decrease in HOMA-IR or HbA1c in the ET+P group compared to the ET+S group; however, in the ET+GKB group, there was a significant improvement in both parameters.
A significant increase in VO2 peak was found by Mutimura et al. in a 6-month study of supervised PA in PLWH[30], which is in line with our findings of a significant increase in VO2 max observed in the three groups, indicating an improvement in cardiorespiratory fitness through the 12-week ET program. However, one study in older HIV-infected men found that only high-intensity aerobic exercise and not moderate-intensity aerobic exercise for 16 weeks was associated with a significant improvement in cardiorespiratory fitness (VO2 peak)[37].
Several studies in HIV − and HIV+ subjects have demonstrated that exercise has anti-inflammatory effects by reducing inflammatory biomarkers, including IL-1β, IL-6-IL-8, TNFα, and improving immune function[32,38,39]. Nevertheless, a study of PA in PLWH found no differences in the markers of immune activation (CD38 and HLA-DR) or inflammation (IL-6 and TNF-α), although exercise was self-prescribed[40]. There are contradictory results regarding the improvement in immune function associated with physical activity in PLWH. Smith et al. found no significant changes in CD4+ T cell counts in an RCT after 12 weeks of aerobic exercise in PLWH, [31] whereas Brito-Neto et al. found that a 12-week resistance training program resulted in a significant increase (15.7%) in CD4+ T cell counts[33]. A significant increase in the number of CD4+ T cells was observed in the ET + P group.
The prevalence of T2DM among PLWH is up to four times higher than that among the general population in some regions of the world[41]. Several risk factors have been identified for the development of T2DM in older PLWH, including duration of HIV infection, lower CD4+ T cell nadir, long duration of HIV infection, use of older-generation antiretroviral therapy, high BMI, and arterial hypertension[42].
GKB exerts antidiabetic effects by increasing insulin expression and sensitivity. GKB extract increases pancreatic β-cell function [43]and improves insulin sensitivity by enhancing IRS-2 transcription[44], as IRS-2 is a crucial element in insulin signaling, and studies have found that a deficiency of IRS-2 causes insulin resistance[45]. We found a significant decrease in insulin resistance (HOMA-IR) and HbA1c levels in our study of non-diabetic PLWH; therefore, its usefulness as a dietary supplement for the prevention of diabetes should be considered. Aziz et al. found a significant decrease in HbA1c, fasting serum glucose, BMI, WC, and VAI in T2DM subjects ineffectively treated with metformin, to whom GKB extract supplementation was added for six months.[46] The effects on BMI, WC, and VAI have been associated with an increase in lipolysis induced by the GKB extract[47].
A pilot study of subjects with metabolic syndrome (MS) found a significant decrease in hs-CRP and HOMA-IR, as well as in other inflammation and oxidative stress biomarkers and nanoplaque formation, with the administration of GKB extract over 2 months. The HOMA-IR score and nanoplaque formation were significantly correlated in this study[48]. HOMA-IR predicts incident symptomatic CVD independent of classic risk factors and several blood biomarkers; therefore, insulin resistance should be an important target not only for reducing or treating T2DM, but also for reducing cardiovascular risk[49]. HOMA-IR has been correlated with increased CVD/total mortality in both the diabetic and non-diabetic populations[50,51]. Furthermore, in the MESA study, HOMA-IR was found to predict the incidence and progression of coronary artery calcification, although not independently of MetS status[52].
Experimental studies with GKB extract have observed other metabolic benefits, including reduction in body adiposity in diet-induced rats, restoration of obesity-induced insulin signaling impairment,[53] inhibition of adipogenesis, regulation of lipid metabolism, body weight reduction in mice,[54] and a decrease in adipocyte volume from obese rats to dimensions equivalent to adipocytes from non-obese rats, suggesting a potential anti-obesogenic effect of GKB[55]. Moreover, the GKB extract exerts several lipid-lowering effects, including decreased cholesterol absorption, inactivation of HMG-CoA, and improvement of essential polyunsaturated fatty acids[56]. The favorable effects of GKB on lipids have been observed in both experimental and clinical studies[57,58]. We did not find any relevant changes in the lipid parameters of our patients in the GKB group, probably because of the short study duration. However, the statin-treated group showed significant changes in total cholesterol and low-density lipoprotein cholesterol levels. These results agree with those of a study carried out by Zanetti et al., who found that ET, statin use, and the combination of both decreased total cholesterol, LDL-c, TG, CRP, IL-1-β, and carotid intima-media thickness compared with no intervention in PLWH. Furthermore, the combination of ET + statins showed a significant decrease in total cholesterol, TG, LDL-C, inflammatory markers (IL-1 β, IL-6, IL-8), and carotid intima-media thickness and a significant increase in HDL-c compared to the individual use of statins and ET[59]. Our study has limitations, including the small sample size, it was carried out in a single center and a single country, and only males were enrolled; therefore, the results cannot be generalized to other regions or to females. Analysis of inflammatory biomarkers would have strengthened the results of this study.
5. Conclusions
HIV infection is now a treatable chronic disease, and it is a concern that about half of PLWH are physically inactive. Our study demonstrated that supervised physical activity improves body fat and cardiorespiratory capacity. This effective non-pharmacological intervention should be encouraged in PLWH to engage them in physical activity. In contrast, GKB extract is an inexpensive supplement with effects on insulin resistance in PLWH and could be used in the prevention and add-on treatment of T2DM. Further large-scale studies are required to confirm these findings.
Author Contributions
Conceptualization, R.S-R., J.M-M. and F.A-L; methodology, E.J-U., J.L-T. and C.L-R.; software, N.TC.; validation, E.M-L., R.S-R. and, F.A-L.; formal analysis, NT-C; investigation, R.S-R., J.M-M. and F.A-L.; resources, R.S-R. and R.S-A.; data curation, F.A-L., R.S-R. and J.M-M.; writing—original draft preparation, J.M-M., F.A-L., and N.T-C.; writing - review and editing, R.S-R., F.A-L., E.M-L. and N.T-C.; visualization, NT-C, JM-M, FA-L, EM-L; supervision, E.M-L., E.J-U., J.L-T. and C.L-R.; project administration, R.S-R., J.M-M. and FA-L; funding acquisition, R.S-R;.
Funding
This study was funded by a grant from the Universidad de Guadalajara (PIN 2021-II).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Hospital Civil de Guadalajara (protocol code (no.165/21, date of approval 06/Dec/2021).” for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All relevant data are within the paper and its supporting Information files
Acknowledgments
We thank the staff of the HIV Unit of the Civil Hospital of Guadalajara for their invaluable contributions to patient enrollment.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Marcus, J.L.; Leyden, W.A.; Alexeeff, S.E.; Anderson, A.N.; Hechter, R.C.; Hu, H.; Lam, J.O.; Towner, W.J.; Yuan, Q.; Horberg, M.A.; et al. Comparison of Overall and Comorbidity-Free Life Expectancy Between Insured Adults With and Without HIV Infection, 2000-2016. JAMA Netw Open 2020, 3, e207954. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Westfall, A.O.; Chamot, E.; Willig, A.L.; Mugavero, M.J.; Ritchie, C.; Burkholder, G.A.; Crane, H.M.; Raper, J.L.; Saag, M.S.; et al. T: Patterns in HIV-Infected Patients, 2012.
- Shah, A.S.V.; Stelzle, D.; Lee, K.K.; Beck, E.J.; Alam, S.; Clifford, S.; Longenecker, C.T.; Strachan, F.; Bagchi, S.; Whiteley, W.; et al. Global Burden of Atherosclerotic Cardiovascular Disease in People Living With HIV. Circulation 2018, 138, 1100–1112. [Google Scholar] [CrossRef] [PubMed]
- Farahani, M.; Mulinder, H.; Farahani, A.; Marlink, R. Prevalence and Distribution of Non-AIDS Causes of Death among HIV-Infected Individuals Receiving Antiretroviral Therapy: A Systematic Review and Meta-Analysis. Int J STD AIDS 2017, 28, 636–650. [Google Scholar] [CrossRef] [PubMed]
- Sax, P.E.; Erlandson, K.M.; Lake, J.E.; McComsey, G.A.; Orkin, C.; Esser, S.; Brown, T.T.; Rockstroh, J.K.; Wei, X.; Carter, C.C.; et al. Weight Gain Following Initiation of Antiretroviral Therapy: Risk Factors in Randomized Comparative Clinical Trials. Clinical Infectious Diseases 2020, 71, 1379–1389. [Google Scholar] [CrossRef]
- Lake, J.E.; Trevillyan, J. Impact of Integrase Inhibitors and Tenofovir Alafenamide on Weight Gain in People with HIV. Curr Opin HIV AIDS 2021, 16, 148–151. [Google Scholar] [CrossRef]
- Mallon, P.W.; Brunet, L.; Hsu, R.K.; Fusco, J.S.; Mounzer, K.C.; Prajapati, G.; Beyer, A.P.; Wohlfeiler, M.B.; Fusco, G.P. Weight Gain before and after Switch from TDF to TAF in a U.S. Cohort Study. J Int AIDS Soc 2021, 24. [Google Scholar] [CrossRef]
- Neves, J.S.; Guerreiro, V.; Carvalho, D.; Serrão, R.; Sarmento, A.; Freitas, P. Metabolically Healthy or Metabolically Unhealthy Obese HIV-Infected Patients: Mostly a Matter of Age? Front Endocrinol (Lausanne) 2018, 9, 1–18. [Google Scholar] [CrossRef]
- Ozemek, C.; Erlandson, K.M.; Jankowski, C.M. Physical Activity and Exercise to Improve Cardiovascular Health for Adults Living with HIV. Prog Cardiovasc Dis 2020, 63, 178–183. [Google Scholar] [CrossRef]
- Voigt, N.; Cho, H.; Schnall, R. Supervised Physical Activity and Improved Functional Capacity among Adults Living with HIV: A Systematic Review. Journal of the Association of Nurses in AIDS Care 2018, 29, 667–680. [Google Scholar] [CrossRef]
- Rodrigues, K.L.; Borges, J.P.; Lopes, G. de O.; Pereira, E.N.G. da S.; Mediano, M.F.F.; Farinatti, P.; Tibiriça, E.; Daliry, A. Influence of Physical Exercise on Advanced Glycation End Products Levels in Patients Living With the Human Immunodeficiency Virus. Front Physiol 2018, 9. [Google Scholar] [CrossRef]
- Pérez Chaparro, C.G.A.; Zech, P.; Schuch, F.; Wolfarth, B.; Rapp, M.; Heiβel, A. Effects of Aerobic and Resistance Exercise Alone or Combined on Strength and Hormone Outcomes for People Living with HIV. A Meta-Analysis. PLoS One 2018, 13, e0203384. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.K.; Tynan, A.-M.; Nixon, S.A.; Glazier, R.H. Effectiveness of Aerobic Exercise for Adults Living with HIV: Systematic Review and Meta-Analysis Using the Cochrane Collaboration Protocol. BMC Infect Dis 2016, 16, 182. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.; Naclerio, F.; Karsten, B.; Vera, J.H. Physical Activity and Quality of Life in People Living with HIV. AIDS Care 2019, 31, 589–598. [Google Scholar] [CrossRef]
- Vancampfort, D.; Mugisha, J.; De Hert, M.; Probst, M.; Firth, J.; Gorczynski, P.; Stubbs, B. Global Physical Activity Levels among People Living with HIV: A Systematic Review and Meta-Analysis. Disabil Rehabil 2018, 40, 388–397. [Google Scholar] [CrossRef]
- Biernacka, P.; Adamska, I.; Felisiak, K. The Potential of Ginkgo Biloba as a Source of Biologically Active Compounds—A Review of the Recent Literature and Patents. Molecules 2023, 28, 3993. [Google Scholar] [CrossRef]
- Rodríguez, M.; Ringstad, L.; Schäfer, P.; Just, S.; Hofer, H.W.; Malmsten, M.; Siegel, G. Reduction of Atherosclerotic Nanoplaque Formation and Size by Ginkgo Biloba (EGb 761) in Cardiovascular High-Risk Patients. Atherosclerosis 2007, 192, 438–444. [Google Scholar] [CrossRef]
- Zhou, W.; Chai, H.; Lin, P.H.; Lumsden, A.B.; Yao, Q.; Chen, C. Clinical Use and Molecular Mechanisms of Action of Extract of Ginkgo Biloba Leaves in Cardiovascular Diseases. Cardiovasc Drug Rev 2004, 22, 309–319. [Google Scholar] [CrossRef]
- Mahady, G.B. Ginkgo Biloba for the Prevention and Treatment of Cardiovascular Disease: A Review of the Literature. J Cardiovasc Nurs 2002, 16, 21–32. [Google Scholar] [CrossRef]
- Eisvand, F.; Razavi, B.M.; Hosseinzadeh, H. The Effects of Ginkgo Biloba on Metabolic Syndrome: A Review. Phytotherapy Research 2020, 34, 1798–1811. [Google Scholar] [CrossRef]
- Li, L.; Yang, L.; Yang, F.; Zhao, X.; Xue, S.; Gong, F. Ginkgo Biloba Extract 50 (GBE50) Ameliorates Insulin Resistance, Hepatic Steatosis and Liver Injury in High Fat Diet-Fed Mice. J Inflamm Res 2021, Volume 14, 1959–1971. [Google Scholar] [CrossRef]
- Aziz, T.; Hussain, S.; Mahwi, T.; Ahmed, Z.A.; Rahman, H.; Rasedee, A. The Efficacy and Safety of <em>Ginkgo Biloba</Em> Extract as an Adjuvant in Type 2 Diabetes Mellitus Patients Ineffectively Managed with Metformin: A Double-Blind, Randomized, Placebo-Controlled Trial. Drug Des Devel Ther 2018, Volume 12, 735–742. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and ?-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Julious, S.A. Sample Size of 12 per Group Rule of Thumb for a Pilot Study. Pharm Stat 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Farahat, F.M.; Alghamdi, Y.S.; Farahat, A.F.; Alqurashi, A.A.; Alburayk, A.K.; Alabbasi, A.A.; Alsaedi, A.A.; Alshamrani, M.M. The Prevalence of Comorbidities among Adult People Diagnosed with HIV Infection in a Tertiary Care Hospital in Western Saudi Arabia. J Infect Public Health 2020, 13, 1699–1704. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.D.; Buchner, D.; Piña, I.L.; Balady, G.J.; Williams, M.A.; Marcus, B.H.; Berra, K.; Blair, S.N.; Costa, F.; Franklin, B.; et al. Exercise and Physical Activity in the Prevention and Treatment of Atherosclerotic Cardiovascular Disease. Circulation 2003, 107, 3109–3116. [Google Scholar] [CrossRef]
- Rossomanno, C.I.; Herrick, J.E.; Kirk, S.M.; Kirk, E.P. A 6-Month Supervised Employer-Based Minimal Exercise Program for Police Officers Improves Fitness. J Strength Cond Res 2012, 26, 2338–2344. [Google Scholar] [CrossRef]
- Voigt, N.; Cho, H.; Schnall, R. Supervised Physical Activity and Improved Functional Capacity among Adults Living with HIV: A Systematic Review. Journal of the Association of Nurses in AIDS Care 2018, 29, 667–680. [Google Scholar] [CrossRef]
- Vancampfort, D.; Mugisha, J.; Richards, J.; De Hert, M.; Lazzarotto, A.R.; Schuch, F.B.; Probst, M.; Stubbs, B. Dropout from Physical Activity Interventions in People Living with HIV: A Systematic Review and Meta-Analysis. AIDS Care 2017, 29, 636–643. [Google Scholar] [CrossRef]
- Mutimura, E.; Crowther, N.J.; Cade, T.W.; Yarasheski, K.E.; Stewart, A. Exercise Training Reduces Central Adiposity and Improves Metabolic Indices in HAART-Treated HIV-Positive Subjects in Rwanda: A Randomized Controlled Trial. AIDS Res Hum Retroviruses 2008, 24, 15–23. [Google Scholar] [CrossRef]
- Smith, B.A.; Neidig, J.L.; Nickel, J.T.; Mitchell, G.L.; Para, M.F.; Fass, R.J. Aerobic Exercise: Effects on Parameters Related to Fatigue, Dyspnea, Weight and Body Composition in HIV-Infected Adults. AIDS 2001, 15, 693–701. [Google Scholar] [CrossRef]
- Zanetti, H.R.; da Cruz, L.G.; Lourenço, C.L.M.; Neves, F. de F.; Silva-Vergara, M.L.; Mendes, E.L. Non-linear Resistance Training Reduces Inflammatory Biomarkers in Persons Living with HIV: A Randomized Controlled Trial. Eur J Sport Sci 2016, 16, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Brito-Neto, J.G. de; Andrade, M.F. de; Almeida, V.D. de; Paiva, D.C.C.; Morais, N.M. de; Bezerra, C.M.; Fernandes, J.V.; Nascimento, E.G.C. do; Fonseca, I.A.T.; Fernandes, T.A.A. de M. Strength Training Improves Body Composition, Muscle Strength and Increases CD4+ T Lymphocyte Levels in People Living with HIV/AIDS. Infect Dis Rep 2019, 11, 7925. [Google Scholar] [CrossRef] [PubMed]
- Gomes Neto, M.; Conceição, C.S.; Carvalho, V.O.; Brites, C. Effects of Combined Aerobic and Resistance Exercise on Exercise Capacity, Muscle Strength and Quality of Life in HIV-Infected Patients: A Systematic Review and Meta-Analysis. PLoS One 2015, 10, e0138066. [Google Scholar] [CrossRef]
- Barrón-Cabrera, E.; Soria-Rodríguez, R.; Amador-Lara, F.; Martínez-López, E. Physical Activity Protocols in Non-Alcoholic Fatty Liver Disease Management: A Systematic Review of Randomized Clinical Trials and Animal Models. Healthcare 2023, 11, 1992. [Google Scholar] [CrossRef]
- Duncan, A.D.; Peters, B.S.; Rivas, C.; Goff, L.M. Reducing Risk of Type 2 Diabetes in <scp>HIV</Scp> : A Mixed-methods Investigation of the <scp>STOP</Scp> -Diabetes Diet and Physical Activity Intervention. Diabetic Medicine 2020, 37, 1705–1714. [Google Scholar] [CrossRef]
- Oursler, K.K.; Sorkin, J.D.; Ryan, A.S.; Katzel, L.I. A Pilot Randomized Aerobic Exercise Trial in Older HIV-Infected Men: Insights into Strategies for Successful Aging with HIV. PLoS One 2018, 13, e0198855. [Google Scholar] [CrossRef]
- Hernández-Lepe, M.A.; Ortiz-Ortiz, M.; Hernández-Ontiveros, D.A.; Mejía-Rangel, M.J. Inflammatory Profile of Older Adults in Response to Physical Activity and Diet Supplementation: A Systematic Review. Int J Environ Res Public Health 2023, 20, 4111. [Google Scholar] [CrossRef]
- Pérez Chaparro, C.G.A.; Zech, P.; Schuch, F.; Wolfarth, B.; Rapp, M.; Heiβel, A. Effects of Aerobic and Resistance Exercise Alone or Combined on Strength and Hormone Outcomes for People Living with HIV. A Meta-Analysis. PLoS One 2018, 13, e0203384. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Pinacchio, C.; Santinelli, L.; Adami, P.E.; Borrazzo, C.; Cavallari, E.N.; Vullo, A.; Innocenti, G. Pietro; Mezzaroma, I.; Mastroianni, C.M.; et al. Physical Activity and HIV: Effects on Fitness Status, Metabolism, Inflammation and Immune-Activation. AIDS Behav 2020, 24, 1042–1050. [Google Scholar] [CrossRef]
- Chenciner, L.; Barber, T.J. Non-Infective Complications for People Living with HIV. Medicine 2022, 50, 304–307. [Google Scholar] [CrossRef]
- Mhlanga, N.L.; Netangaheni, T.R. Risks of Type 2 Diabetes among Older People Living with HIV: A Scoping Review. South African Family Practice 2023, 65. [Google Scholar] [CrossRef] [PubMed]
- Kudolo, G.B. The Effect of 3-Month Ingestion of Ginkgo Biloba Extract (EGb 761) on Pancreatic Β-Cell Function in Response to Glucose Loading in Individuals with Non-Insulin-Dependent Diabetes Mellitus. The Journal of Clinical Pharmacology 2001, 41, 600–611. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Meng, Q.; Qian, T.; Yang, Z. Ginkgo Biloba Extract Enhances Glucose Tolerance in Hyperinsulinism-Induced Hepatic Cells. J Nat Med 2011, 65, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Kubota, N.; Tobe, K.; Terauchi, Y.; Eto, K.; Yamauchi, T.; Suzuki, R.; Tsubamoto, Y.; Komeda, K.; Nakano, R.; Miki, H.; et al. Disruption of Insulin Receptor Substrate 2 Causes Type 2 Diabetes Because of Liver Insulin Resistance and Lack of Compensatory Beta-Cell Hyperplasia. Diabetes 2000, 49, 1880–1889. [Google Scholar] [CrossRef]
- Aziz, T.; Hussain, S.; Mahwi, T.; Ahmed, Z.A.; Rahman, H.; Rasedee, A. The Efficacy and Safety of <em>Ginkgo Biloba</Em> Extract as an Adjuvant in Type 2 Diabetes Mellitus Patients Ineffectively Managed with Metformin: A Double-Blind, Randomized, Placebo-Controlled Trial. Drug Des Devel Ther 2018, Volume 12, 735–742. [Google Scholar] [CrossRef]
- Dell’Agli, M.; Bosisio, E. Biflavones of Ginkgo Biloba Stimulate Lipolysis in 3T3-L1 Adipocytes. Planta Med 2002, 68, 76–79. [Google Scholar] [CrossRef]
- Siegel, G.; Ermilov, E.; Knes, O.; Rodríguez, M. Combined Lowering of Low Grade Systemic Inflammation and Insulin Resistance in Metabolic Syndrome Patients Treated with Ginkgo Biloba. Atherosclerosis 2014, 237, 584–588. [Google Scholar] [CrossRef]
- Bonora, E.; Kiechl, S.; Willeit, J.; Oberhollenzer, F.; Egger, G.; Meigs, J.B.; Bonadonna, R.C.; Muggeo, M. Insulin Resistance as Estimated by Homeostasis Model Assessment Predicts Incident Symptomatic Cardiovascular Disease in Caucasian Subjects From the General Population. Diabetes Care 2007, 30, 318–324. [Google Scholar] [CrossRef]
- Zuliani, G.; Morieri, M.L.; Volpato, S.; Maggio, M.; Cherubini, A.; Francesconi, D.; Bandinelli, S.; Paolisso, G.; Guralnik, J.M.; Ferrucci, L. Insulin Resistance and Systemic Inflammation, but Not Metabolic Syndrome Phenotype, Predict 9 Years Mortality in Older Adults. Atherosclerosis 2014, 235, 538–545. [Google Scholar] [CrossRef]
- Ausk, K.J.; Boyko, E.J.; Ioannou, G.N. Insulin Resistance Predicts Mortality in Nondiabetic Individuals in the U.S. Diabetes Care 2010, 33, 1179–1185. [Google Scholar] [CrossRef]
- Blaha, M.J.; DeFilippis, A.P.; Rivera, J.J.; Budoff, M.J.; Blankstein, R.; Agatston, A.; Szklo, M.; Lakoski, S.G.; Bertoni, A.G.; Kronmal, R.A.; et al. The Relationship Between Insulin Resistance and Incidence and Progression of Coronary Artery Calcification. Diabetes Care 2011, 34, 749–751. [Google Scholar] [CrossRef] [PubMed]
- Banin, R.M.; Hirata, B.K.S.; Andrade, I.S.; Zemdegs, J.C.S.; Clemente, A.P.G.; Dornellas, A.P.S.; Boldarine, V.T.; Estadella, D.; Albuquerque, K.T.; Oyama, L.M.; et al. Beneficial Effects of Ginkgo Biloba Extract on Insulin Signaling Cascade, Dyslipidemia, and Body Adiposity of Diet-Induced Obese Rats. Brazilian Journal of Medical and Biological Research 2014, 47, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Hypocholesterolemic Effect of Ginkgo Biloba Seeds Extract from High Fat Diet Mice. Biomedical Science Letters 2017, 23, 138–143. [Google Scholar] [CrossRef]
- Hirata, B.K.S.; Cruz, M.M.; de Sá, R.D.C.C.; Farias, T.S.M.; Machado, M.M.F.; Bueno, A.A.; Alonso-Vale, M.I.C.; Telles, M.M. Potential Anti-Obesogenic Effects of Ginkgo Biloba Observed in Epididymal White Adipose Tissue of Obese Rats. Front Endocrinol (Lausanne) 2019, 10. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, G.; A, J.; Wu, D.; Zhu, L.; Ma, B.; Du, Y. Application of GC/MS-Based Metabonomic Profiling in Studying the Lipid-Regulating Effects of Ginkgo Biloba Extract on Diet-Induced Hyperlipidemia in Rats. Acta Pharmacol Sin 2009, 30, 1674–1687. [Google Scholar] [CrossRef]
- Jie, L.; Hai, H. Clinical Observation of Gingko Biloba Extract Injection in Treating Early Diabetic Nephropathy. Chin J Integr Med 2005, 11, 226–228. [Google Scholar] [CrossRef]
- Cheng, D.; Liang, B.; Li, Y. Antihyperglycemic Effect of Ginkgo Biloba Extract in Streptozotocin-Induced Diabetes in Rats. Biomed Res Int 2013, 2013, 1–7. [Google Scholar] [CrossRef]
- Zanetti, H.R.; Gonçalves, A.; Teixeira Paranhos Lopes, L.; Mendes, E.L.; Roever, L.; Silva-Vergara, M.L.; Neves, F.F.; Resende, E.S. Effects of Exercise Training and Statin Use in People Living with Human Immunodeficiency Virus with Dyslipidemia. Med Sci Sports Exerc 2020, 52, 16–24. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the participants in the study. ET, Exercise training; GKB, Ginkgo biloba.
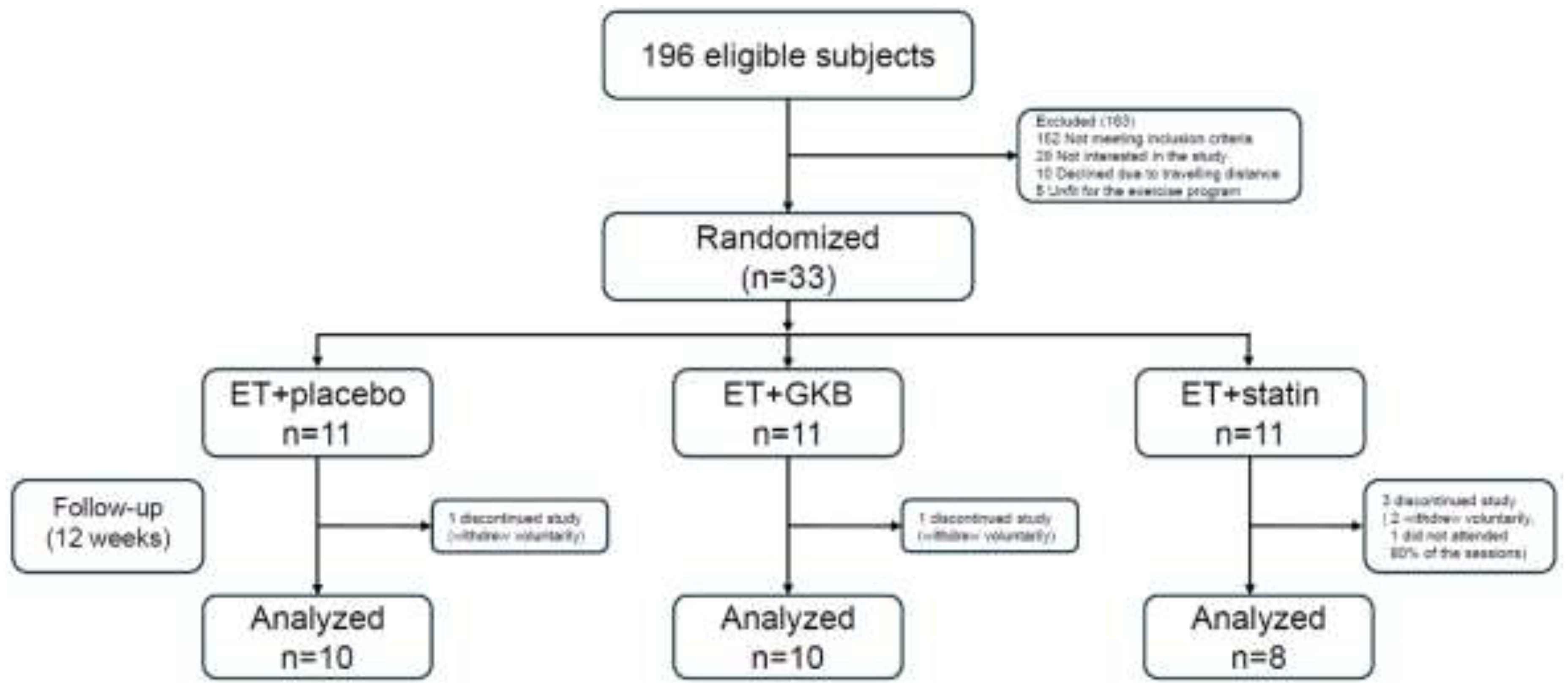
Figure 2.
Changes in body composition and metabolic parameters after 12 weeks of intervention. (a) Body fat. (b) LDL-c. (c) HbA1c (d) HOMA-IR.
Figure 2.
Changes in body composition and metabolic parameters after 12 weeks of intervention. (a) Body fat. (b) LDL-c. (c) HbA1c (d) HOMA-IR.
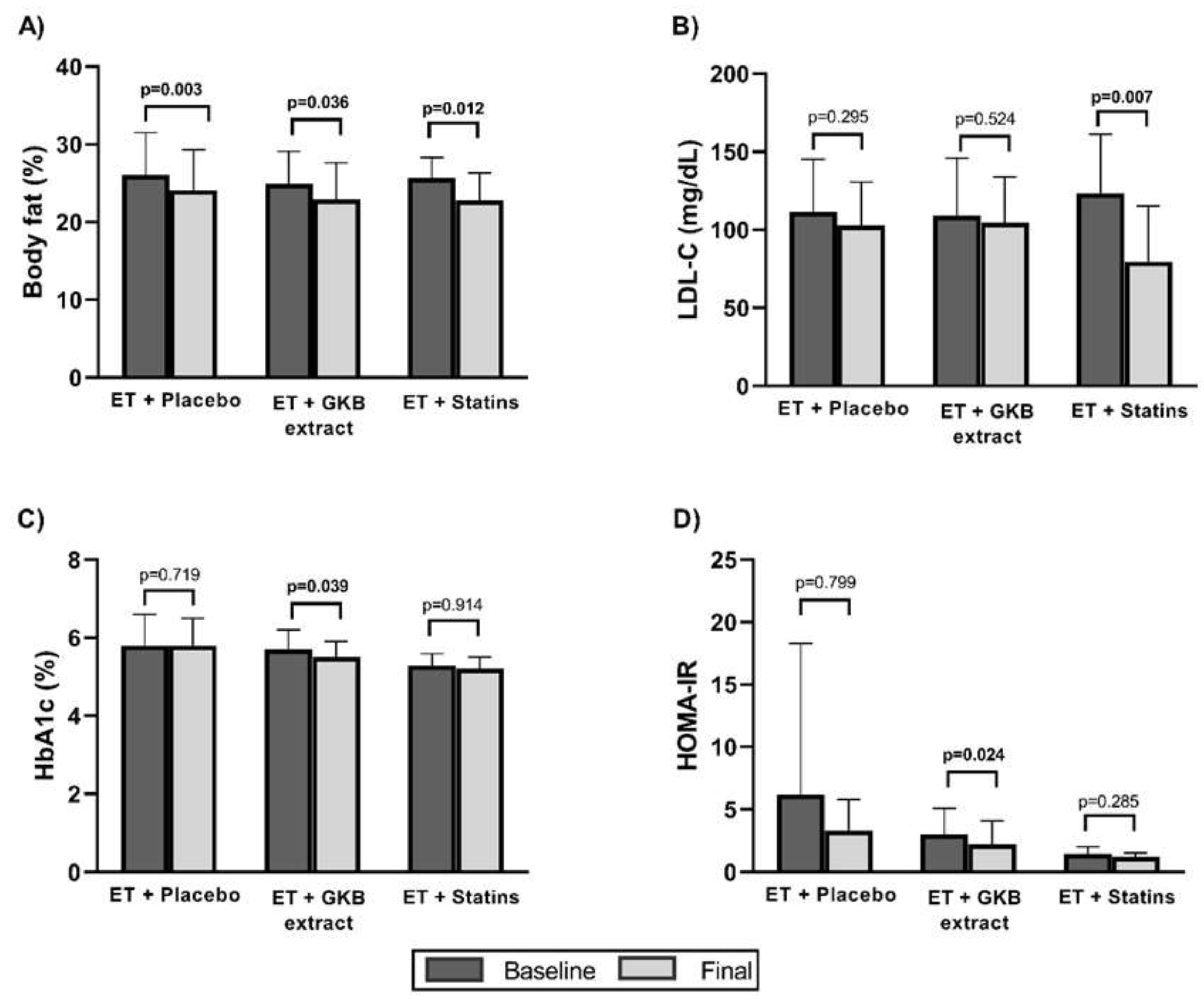

Table 1.
Basal characteristics of participants.
| Characteristics | ET + Placebo n=10 |
ET+ GKB n=10 |
ET+ Statin n=8 |
p value |
|---|---|---|---|---|
| Mean age, years (SD) | 41.8 ±11.0 | 41.8 ±7.0 | 40.5 ±10.5 | 0.949 |
| Weight (kg) | 80.7 ±13.3 | 75.9 ±12.4 | 76.2 ±12.5 | 0.277 |
| Waist circumference (cm) | 91.6 ±13.6 | 90.0 ±10.5 | 87.2 ±6.5 | 0.695 |
| Waist-to-hip ratio | 0.90 ±0.10 | 0.95 ±0.07 | 0.90 ±0.05 | 0.253 |
| Waist-to-height ratio | 0.53 ±0.08 | 0.53 ±0.08 | 0.52 ±0.04 | 0.906 |
| BMI (kg/m2) | 28.0 ±4.1 | 26.6 ±4.2 | 25.7 ±2.6 | 0.854 |
| Sum of 8 skinfolds (mm) | 118.8 ±47.7 | 127.6 ±40.8 | 129.6 ±43.9 | 0.855 |
| Body fat mass (%) | 26.0±5.5 | 24.9±4.2 | 25.7±2.6 | 0.854 |
| Lean body mass (%) | 39.0 ±6.4 | 40.3 ±4.9 | 40.2 ±3.4 | 0.827 |
| Bone mass (%) | 13.7 ±1.4 | 14.3 ±1.5 | 14.2 ±0.8 | 0.560 |
| Absolute CD4+ T Cell count/μl, mean | 534.3 ±310.4 | 694.2 ±310.1 | 570.6 ±154.6 | 0.171 |
| HIV-1 RNA (copies/mL), mean | 180.6 ±466.8 | 2,169.4±6,756.9 | 35.0 ±4.3 | 0.764 |
| Total, billirrubin (mg/dL) | 0.80 ±0.4 | 0.63 ±0.2 | 0.58 ±0.2 | 0.683 |
| Direct billirrubin (mg/dL) | 0.14 ±0.05 | 0.11 ±0.03 | 0.11 ±0.06 | 0.335 |
| Total, protein (g/dL) | 7.2 ±0.5 | 7.2 ±0.4 | 7.1 ±0.3 | 0.933 |
| Albumin (g/dL) | 4.2 ±0.1 | 4.2 ±0.2 | 4.3 ±0.2 | 0.518 |
| Globulin (g/dL) | 3.1 ±0.5 | 2.9 ±0.4 | 2.7 ±0.4 | 0.374 |
| Alanine aminotransferase (IU/L) | 31.8 ±11.2 | 36.8 ±55.0 | 18.7 ±5.4 | 0.024* |
| Aspartate aminotransferase (IU/L) | 22.0 ±5.9 | 30.1 ±29.0 | 17.2 ±4.5 | 0.061 |
| Gamma-glutamyl transpeptidase (IU/L) | 45.8 ±31.0 | 35.7 ±32.4 | 27.3 ±15.7 | 0.273 |
| Alkaline phosphatase (IU/L) | 79.7 ±21.4 | 73.6 ±14.8 | 69.2 ±19.5 | 0.533 |
| Lactate dehydrogenase (U/L) | 159.1 ±35.7 | 174.1 ±41.2 | 156.8 ±22.7 | 0.514 |
| Urea (mg/dL) | 34.0 ±10.9 | 28.3 ±7.7 | 41.2 ±11.2 | 0.039* |
| BUN (mg/dL) | 15.8 ±5.0 | 13.2 ±3.5 | 19.3 ±3.5 | 0.035* |
| Creatinine (mg/dL) | 0.91 ±0.12 | 0.096 ±0.12 | 1.04 ±0.19 | 0.213 |
| Prothrombin time | 10.8 ±0.9 | 11.0 ±0.4 | 10.7 ±0.6 | 0.824 |
| INR | 0.97 ±0.09 | 1.00 ±0.04 | 0.93 ±0.08 | 0.258 |
| Partial thromboplastin time | 32.4 ±2.5 | 33.6 ±4.5 | 31.4 ±2.7 | 0.487 |
| Fibrinogen (mg/dL) | 421.4 ±73.9 | 459.0 ±93.6 | 422.6 ±82.9 | 0.559 |
Abbreviations: ET, Exercise training; GKB, Ginkgo biloba; SD, Standard deviation; BMI, Body mass index; INR, International normalized ratio. A one-tailed analysis of variance (ANOVA) was used to compare groups and Bonferroni for post hoc comparisons. The Kruskal-Wallis test was used for nonnormally distributed variables. * p<0.05, comparing the ET + statin group vs the ET + GKB group.
Table 2.
Metabolic changes between study groups after 12-week intervention.
| Characteristics | ET + Placebo n=10 |
ET+ GKB n=10 |
ET+ Statin n=8 |
p value |
|---|---|---|---|---|
| Total cholesterol (mg/dL) | -11.5 ±33.2 | -12.3 ±20.9 | -53.7 ±63.9 | 0.044* |
| HDL cholesterol (mg/dL) | 0.5 ±9.1 | 2.1 ±3.5 | 1.8 ±7.9 | 0.882 |
| LDL cholesterol (mg/dL) | -8.9 ±25.3 | -4.3 ±20.5 | -44.0 ±32.5 | 0.426 |
| Triglycerides (mg/dL) | -9.5 ±93.9 | -27.0 ±90.1 | -0.8 ±141.5 | 0.522 |
| Glucose (mg/dL) | -5.9 ±22.2 | -2.4 ±11.1 | -2.6 ±19.6 | 0.687 |
| Insulin (µU/mL) | -4.4 ±20.5 | -3.0 ±2.7 | -0.9 ±2.2 | 0.107 |
| Glycated hemoglobin A1c (%) | -0.0 ±0.2 | -0.1 ±0.2 | 0.0 ±0.2 | 0.340 |
| HOMA-IR† | -2.9 ±10.0 | -0.7 ±0.7 | -0.2 ±0.5 | 0.119 |
| Triglycerides/HDL-c ratio | 0.1 ±2.6 | -1.4 ±3.0 | -0.6 ±3.4 | 0.903 |
Abbreviations: ET, Exercise training; GKB, Ginkgo biloba; HOMA-IR, Homeostatic Model Assessment of Insulin Resistance. One-tailed ANOVA test was used to compare between groups and Bonferroni for post hoc comparisons. The Wilcoxon test was used for non-normally distributed variables (†). * p<0.05 comparing ET + statin group vs ET + GKB group.
Table 3.
Changes in functional capacity pre and post 12-week intervention.
| Variable | ET+ Placebo n=10 |
ET+ GKB n=10 |
ET+ Statin n=8 |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Basal | Final | p vale | Basal | Final | p value | Basal | Final | p value | |
| VO2Máx† | 47.9 ±5.3 | 59.9 ±8.9 | 0.001** | 46.5 ±10.1 | 55.0 ±7.4 | 0.002** | 45.0 ±4.2 | 58.9 ±7.0 | 0.000*** |
| Grip strength in non-dominant hand (Kg) | 31.2 ±5.4 | 33.3 ±9.0 | 0.333† | 61.9 ±90.1 | 33.4 ±4.9 | 0.674† | 34.2 ±8.6 | 346 ±6.4 | 0.838 |
| Grip strength in dominant hand (Kg) | 33.7 ±8.6 | 33.3 ±11.9 | 0.849 | 34.4 ±4.1 | 35.6 ±6.1 | 0.380 | 35.6 ±6.1 | 37.8 ±6.1 | 0.297 |
| Back strength (Kg) | 36.5 ±20.7 | 42.8 ±18.1 | 0.272 | 32.6 ±11.4 | 40.0 ±12.9 | 0.025* | 39.3 ±18.1 | 39.2 ±15.0 | 0.978 |
| Lower limb strength (Kg) | 37.7 ±13.6 | 42.8 ±16.0 | 0.434 | 35.4 ±14.3 | 40.0 ±14.7 | 0.161 | 36.5 ±18.2 | 39.3 ±14.3 | 0.635 |
| Flexibility (cm) | 24.3 ±10.4 | 24.5 ±10.1 | 0.908 | 16.1 ±7.4 | 17.5 ±8.3 | 0.608 | 19.3 ±7.8 | 25.0 ±7.5 | 0.027* |
| Balance | 6.2 ±5.1 | 3.3 ±3.1 | 0.053 | 2.3 ±3.3 | 1.5 ±2.5 | 0.461† | 5.6 ±5.7 | 4.7 ±5.5 | 0.570 |
Abbreviations: VO2 max, maximum volume of oxygen; data are shown as mean ± standard deviation (SD). A one-tailed analysis of variance (ANOVA) was used to compare groups and Bonferroni for post hoc comparisons. The Wilcoxon test was used for non-normally distributed variables (†). * p < 0.05, ** p < 0.01, *** p < 0.001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



