Submitted:
18 February 2025
Posted:
18 February 2025
You are already at the latest version
Abstract
Coronary microvascular disease (CMVD) is not an uncommon complication after acute myocardial infarction (AMI), independent of prompt revascularization. It is a serious yet underdiagnosed disease that has a major impact on patient’s outcomes. Even when the infarct-related artery is successfully revascularized, a significant per-centage of patients still have compromised microvascular circulation, which is linked to higher cardiovascular mortality and hospitalization for heart failure. The well-known invasive methods, such as the index of microvascular resistance (IMR), and the coronary flow reserve (CFR) have been considered as gold standards. Howev-er, they are constrained by their hazards and complexity. Non-invasive techniques, such as the echocardiography doppler for CFR assessment, the positron emission to-mography (PET) and cardiac magnetic resonance imaging (CMR) and some other techniques provide alternatives, but their accessibility, the cost and their implementa-tion during the peri-AMI period raise obstacles for their wide use. This review high-lights both invasive and non-invasive modalities as it examines the diagnostic meth-ods and prognostic significance of CMVD in patients who have had an AMI. Enhanc-ing long-term results in this high-risk population requires an understanding of and commitment to CMVD.
Keywords:
Coronary Microvascular Disease (CMVD)
; Acute Myocardial Infarction (AMI)
; Microvascular Obstruction (MVO)
; Index of Microcirculatory Resistance (IMR)
; Percutaneous Coronary Intervention (PCI)
; Coronary Flow Reserve (CFR)
; Major Adverse Cardiovascular Events (MACE)
1. Introduction
Acute myocardial infarction (AMI), either ST-segment elevation myocardial infarction (STEMI) or non-ST elevation myocardial infarction (NSTEMI) is one of the major causes of mortality and morbidity worldwide. The coronary vasculature is usually divided into macrovascular and microvascular circulation. The latter constitutes the 90-95% of the whole coronary vasculature, but it is usually not seen in both invasive and non-invasive coronary angiography[1]. The prompt restoration of the epicardial coronary blood flow constitutes the standard of care of AMI therapy. After a successful revascularization of the infarct-related artery (IRA) with percutaneous coronary intervention (PCI) (primary or not), there is, in a significant proportion of patients, evidence of impaired microvascular circulation, termed as coronary microvascular disease (CMVD)[2]. Several mechanisms have been proposed: acute microvascular obstruction, intramyocardial haemorrhage (IMH), microvascular dysfunction potentially reversible, but none of them is fully elucidated,. CMVD reflects impaired myocardial reperfusion and is of clinical relevance.
The diagnosis of CMVD is of paramount importance, and there are invasive and non-invasive modalities. However, the accuracy of currently available diagnostic methods constitutes an inherent drawback of them. The thermodilution-based index of microvascular resistance (IMR) has been recommended as the gold standard among the invasive methods[3]. Additional methods using intra-vascular pressure wires have been proposed to calculate coronary flow reserve (CFR) or fractional flow reserve (FFR). Their invasive nature with associated risks and their timely application are important limitations. On the other hand, non-invasive strategies like echocardiography doppler-based CFR, cardiac Positron Emission Tomography (PET) and cardiac magnetic resonance (CMR) imaging have been alternatively suggested to overcome invasive methods’ limitations[4]. Significant disadvantages of the non-invasive modalities have limited their wider application, while none is the gold-standard method.
Post-AMI CMVD has been strongly associated with mortality and hospitalization for heart failure,[5,6]. A recent meta-analysis of retrospective studies demonstrated that severe CMVD assessed during PCI in patients with STEMI was associated with major adverse cardiovascular events (MACEs)[7]. The present review has focused on patients experiencing an AMI and its aim is to evaluate the methods for CMVD diagnosis and analyse their parallel prognostic value.
2. Search Methods
We searched the MEDLINE (via Ovid SP), EMBASE (via Ovid SP), and the Cochrane Library from 1990 through December 2024, using a predefined search strategy. For identifying any additional published and ongoing studies, we searched the Science Citation Index and checked the references of original research studies, previous systematic reviews or meta-analyses, literature reviews with related subjects. The following search terms, in titles and abstracts, including Medical Subject Headings (MeSH) were used: coronary microvascular disease, coronary microvascular dysfunction, coronary flow reserve (CFR), coronary flow velocity reserve (CFVR), (acute myocardial infarction (AMI), ST-elevation myocardial infarction (STEMI), non ST-elevation myocardial infarction (NSTEMI), acute coronary syndrome (ACS), myocardial infarction with non-obstructed coronary arteries (MINOCA), major adverse cardiac events (MACEs), death, cardiovascular death, cardiac death, myocardial infarction, hospital admission, and/or coronary revascularization.
3. Potential Mechanism of CMVD After AMI
Coronary microvascular dysfunction (CMVD) after AMI represents the failure to restore adequate blood flow within the coronary microcirculation in regions previously affected by ischemia, even after successful reperfusion of the epicardial arteries. CMVD involves vessels smaller than 0.5 mm in diameter, which constitute approximately 70% of the coronary artery network, playing a vital role in maintaining myocardial perfusion[8]. The clinical significance of CMVD becomes particularly evident in post-AMI patients, where impaired microvascular function exacerbates ischemic damage, despite patent epicardial coronary arteries[9]. Mechanistically, CMVD arises from a complex interplay of ischemic damage per se, ischemia-reperfusion injury and endothelial dysfunction, inflammatory cascades and distal embolization in the context of patient-specific risk factors[10]. Each of these mechanisms uniquely contributes to microvascular dysfunction of even microvascular obstruction (MVO) with impact on clinical outcomes.
3.1. Ischemia, Ischemia-Reperfusion Injury and Endothelial Dysfunction
Ischemia-induced microvascular injury serves as the foundation. Prolonged ischemia during AMI initiates a cascade of cellular and extracellular disturbances that culminate in cardiomyocyte necrosis and apoptosis[11]. The depletion of ATP impairs ion pump function and leads to intracellular calcium overload, acidosis, and reactive oxygen species (ROS) production[12]. Presumably, these changes result in myocardial cell swelling and interstitial oedema, mechanically compressing the microvascular network[3]. Additionally, the accumulation of metabolic byproducts, such as lactate and degraded nucleotide phosphates, creates an osmotic gradient further exacerbating cellular swelling and microvascular blood flow obstruction[13]. In parallel, reperfusion per se precipitates microvascular injury. Restoration of myocardial oxygen supply leads to a surge in ROS, which compromises cellular viability[14]. Furthermore, ROS trigger pathways such as ferroptosis and necroptosis, which release damage-associated molecular patterns (DAMPs) and amplify inflammation[15]. This self-propagating cycle of oxidative stress and inflammation worsens MVO.
The endothelium, which plays a pivotal role in regulating vascular tone and haemostasis, undergoes significant functional impairment in post-AMI[16]. It is affected by reduced nitric oxide (NO) bioavailability, heightened oxidative stress, and upregulated inflammation. Endothelial cell damage during reperfusion, induces IMH and interstitial oedema, further impairing myocardial perfusion[17]. The infiltration of neutrophils and platelet-leukocyte aggregation stimulate the release of vasoconstrictors[14]. Together with microvascular injury, a persistent endothelial dysfunction increases infarct size, hinder myocardial recovery, and promote adverse ventricular remodeling[18].
3.2. Inflammation
Inflammation represents a pathogenic response in CMVD. Following myocardial injury, releasing cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) recruit immune cells to clear necrotic debris,[19,20]. Moreover, the release of DAMPs during regulated cell death, such as necroptosis and pyroptosis, amplifies systemic inflammation[6]. As a result, an excessive or prolonged inflammation damages the microvasculature through endothelial apoptosis, increased permeability, and the deposition of extracellular matrix proteins, leading to the aforementioned adverse effects on microvascular dysfunction. In turn, the development of fibrosis reduced capillary density and impairs myocardial perfusion.
3.3. Percutaneous Coronary Intervention and Distal Embolization
PCI itself can contribute to CMVD,[5,21]. While restoring blood flow in the infarct-related epicardial coronary artery, manipulation during PCI, such as crossing wires, balloon pumping and stent implantation can induce myocardial injury and the no-reflow phenomenon[12]. Mechanisms such as distal embolization, endothelial blebbing, myocardial swelling, and IMH, alongside the formation of platelet-leukocyte plugs, further contribute to coronary MVO[8]. Among them. distal embolization during PCI poses a central role in CMVD[22]. The mechanical disruption of atherosclerotic plaques can release thrombotic and plaque debris into the coronary microcirculation, causing occlusion at the capillary level[23]. These microemboli not only block perfusion but also trigger localized inflammation and microinfarction[24]. The extent of myocardial damage correlates with the size of the emboli and the degree of MVO[17]. Furthermore, inflammatory processes in adjacent viable myocardium impair contractility and propagate CMVD, contributing to adverse outcomes such as arrhythmogenesis[18].
3.4. Patient’s-Specific Factors
Individual susceptibility and preexisting risk factors further influence the development of CMVD. Genetic predispositions significantly influence microvascular response, with polymorphisms in genes like VEGFA and CDKN2B-AS1 linked to an increased risk of MVO[25]. Additionally, sex-specific allelic variants in MYH15, NT5E, and VEGFA have been shown to differentially affect CMVD risk in men[26]. Hyperglycaemia worsens MVO risk by promoting leukocyte plugging, platelet hyperactivity, and impair endothelial vasodilation and exacerbate microvascular plugging[27]. Dyslipidaemia further impairs endothelial function, reduces NO bioavailability, and increases oxidative stress[28]. Hypertension may deteriorate endothelial function, coronary vasodilation and structural remodelling of microvessels[20]. Additionally, advanced age independently predisposes individuals to CMVD, reflecting cumulative declines in vascular function[18]. Finally, ischemic preconditioning, notably through pre-infarction angina, provides a protective mechanism by reducing cardiomyocyte death and MVO via adaptive responses to ischemic stress. However, its benefits may be diminished by preexisting risk factors[29].
4. Diagnostic Methods
Several invasive methods have been used in the cardiac catheterization laboratory for accurate diagnosis of post-AMI CMVD. These methods can be broadly divided into, angiography-based techniques, pressure-wire-based methods (either with thermodilution or doppler techniques), and novel angiography-derived markers using computational flow dynamics [30].
| Method (cut-off value) | Physiology | Prognostic value | Comments (pros & Cons) |
| Invasive methods | |||
| TIMI flow (≤2) | Qualitative index of blood flow of the epicardial coronary arteries | Correlation with increased in-hospital mortality | Pros: cost-free, simple technique, without hyperemic provocation Cons: may not capture the adequacy of myocardial perfusion, low accuracy and sensitivity, interobserver and intra-observer variability |
| MBG (≤1) | Qualitative index of myocardial perfusion, grading the intensity of contrast within the myocardium | larger infarct sizes, adverse ventricular remodelling, worse post-MI outcomes, increased hospitalisation for HF | Pros: cost-free, simple technique Cons: low accuracy, limited sensitivity, interobserver and intra-observer variability |
| CTFC (unknown) | microvascular resistance during hyperaemia | Independent association with in-hospital mortality | Cons: low accuracy, limited sensitivity, interobserver and intra-observer variability |
| IMR (>25, also 23 and 40 are proposed as cut-offs) | measurement of pressure and temperature in the coronary vessels | Association with adverse clinical events, independent predictor of MACE in 4 years | Pros: can be used as a stratification tool, has the largest body of evidence, objective measurement Cons: required hyperaemia, variability |
| CFR (<2) | Ratio: maximal coronary blood flow during hyperaemia / resting blood flow; using pressure-temperature sensor guidewire | Association with higher in-hospital mortality | Pros: Cons: cannot distinguish impairment between macro- and microcirculation, not independent predictor in STEMI, limited utility, requires hyperaemia, high variability, special equipment |
| CFR (<2.1) | Ratio: maximal coronary blood flow during hyperaemia / resting blood flow; using Doppler method | Association with increased cardiac mortality | Cons: cannot distinguish impairment between macro- and microcirculation, influenced by systemic hemodynamic changes |
| RRR (≤1.5, also 1.7 and 2.62 are proposed as cut-offs) | Functional reserve of the coronary microvasculature | In combination with IMR association with MVO, myocardial haemorrhage, infarct size and clinical outcomes | Pros: useful in identifying reduced microvascular responsiveness post-MI Cons: required hyperaemia |
| CFC (<2.8) | Combination of absolute flow measurements and CFR | Improves risk stratification following reperfusion, association with increased MACE | Pros: overcomes the limitations of CFR Cons: requires advanced imaging and technical expertise |
| HMR (≥3) |
Ratio: hyperaemic mean distal pressure /Doppler-derived hyperaemic average peak velocity | Prediction of adverse clinical outcomes | Pros: specific to microvasculature, independent of systemic factors Cons: required precise measurements and pharmacological hyperaemia, technically challenging |
| Non-invasive methods | |||
| CFR (<2) | Ratio: maximal coronary blood flow during hyperaemia / resting blood flow; using Doppler method | Reduced survival | Pros: easily accessible with echocardiography Cons: cannot distinguish microvascular from macrovascular obstruction, discrepancy between CFR und FFR |
| MCE | Myocardial contrast signal is calculated, which reflects the blood flow | Prognostic data not yet available | Cons: operator dependency, uncertain reproducibility, low sensitivity, reimbursement issues |
| CMR: MVO (≥2.6), MPI, MRPI | Direct visualization of myocardial perfusion and MVO, | MVO≥2.6: strong predictor of MACE, death, HF hospitalization | Pros: safe, significant with invasive-derived measurements Cons: Claustrophobia, high cost |
| PET: CFR (<2.6, also 2.0 is proposed as cut-off) | Detection no reflow phenomenon | increased long-term cardiovascular events und mortality | Pros: quantitative assessment, high sensitivity Cons: reduced availability, cost |
4.1. Angiography-Based Techniques
Invasive coronary angiography (ICA) alone, has limited sensitivity in detecting microvascular dysfunction. Thrombolysis in Myocardial Infarction (TIMI) Flow and Myocardial Blush Grade (MBG) are complementary angiographic, qualitative techniques used to assess coronary and myocardial perfusion after revascularization. TIMI Flow evaluates blood flow in the epicardial coronary arteries, but it may fail to capture the adequacy of microvascular perfusion, even when epicardial flow is restored to normal (TIMI flow grade 3)[31]. MBG assesses myocardial perfusion by grading the intensity and washout of contrast within the myocardium, with MBG: 0–1 indicating minimal or absent perfusion and MBG: 2–3 reflecting adequate perfusion. Of note, angiographic no-reflow defined as reduced myocardial perfusion (TIMI flow ≤2 or MBG 0–1) despite successful epicardial coronary artery reopening, is closely related to CMVD and MVO [32,33].
Corrected TIMI frame count (CTFC) is another angiography-based technique to assess post-AMI CMVD measured by microvascular resistance during hyperaemia [34]. However, all these angiography-based qualitative indices for CMVD diagnosis are significantly constrained by low accuracy and sensitivity, and high interobserver and intra-observer variability [35].
Pressure-Wire-Based Techniques
Index of Microcirculatory Resistance (IMR)
The use of thermodilution techniques can measure directly coronary blood flow and microvascular resistance. These techniques precisely quantify microvascular dysfunction using physiology rules and help stratify patients’ risk post-AMI. Among them, the IMR quantifies microvascular resistance using hyperaemic pressure and thermodilution techniques and it is the most widely used method [36]. A guide catheter is inserted through the coronary orifice, and then the pressure and temperature are measured by an extending guide wire. After maximal hyperaemia induced by adenosine or papaverine, the index is calculated using distal pressure and mean transit time of 3 boluses of room temperature saline injected in the IRA [37]. IMR can be calculated using the formula IMR = Pa × Tmn × ([Pd − Pw]/[Pa − Pw]), where Pa = mean proximal coronary pressure, Tmn = mean hyperaemic transit time, and Pd = mean distal coronary pressure. An IMR value above 25 is suggestive of CMVD, when epicardial artery is patent.
Coronary Flow Reserve (CFR)
It evaluates the ratio of maximal coronary blood flow during hyperaemia to resting flow [32]. It can be measured invasively using either a pressure-temperature sensor-tipped guidewire or a doppler catheter assessing blood flow velocity and resistance. Transthoracic Doppler echocardiography, PET, or stress CMR may provide alternative, non-invasive measurements of CFR [38]. Thermodilution-based CFR uses a pressure-temperature sensor guidewire, requiring at least three saline injections to measure the mean transit time (Tmn) at rest and during hyperaemia. CFR is calculated as Tmn(rest)/Tmn (hyperaemia), with a cut-off value of <2.0 indicating impaired microvascular function. Notably, invasive methods like thermodilution or Doppler flow velocity are recommended by ESC and AHA/ACC guidelines (IIa) for patients with persistent symptoms and normal or moderately stenosed coronary arteries [39,40]. Carrick et al. (2016), failed to demonstrate the added value of CFR in STEMI patients where combined IMR and CFR assessment did not outperform IMR alone in risk stratification [41]. CFR’s utility is limited due to increased resting flow in STEMI and its inability to isolate microvascular status from residual epicardial stenosis [42].
Resistive Reserve Ratio (RRR)
It assesses the functional reserve of the coronary microvasculature by comparing resistance at baseline versus during hyperaemia. It is calculated as the ratio of basal microvascular resistance to hyperaemic microvascular resistance. In acute STEMI, IMR and RRR, has been associated with MVO, IMH, infarct size, and clinical outcomes [43]. A low RRR indicates impaired vasodilatory capacity of the microcirculation, signifying microvascular dysfunction [44]. This method is particularly useful in identifying reduced microvascular responsiveness to primary PCI (PPCI) in AMI patients [45].
Microvascular Resistance Reserve (MRR)
The lack of established normal reference values, coupled with considerable variability between patients [46] has led to the recently described MRR, evaluating the capacity of the microvasculature to reduce resistance during hyperaemia compared to baseline, independently of epicardial resistance and autoregulation. It is calculated as the ratio of basal microvascular resistance to hyperaemic resistance (MRR = (CFR/FFR) x (Pa resting/Pa hyperaemia) [46]. A reduced MRR post-AMI reflects impaired functional reserve and the inability of the microcirculation to address increased demand [47]. More studies are needed to establish the cut-off values as well the prognostic relevance of MMR in post-AMI patients.
Invasive Doppler-Based Methods
They are widely used for CMVD by measuring coronary blood flow velocity and resistance [48]. These techniques provide real-time, dynamic assessments of microvascular function, but are limited by operator dependency and technical challenges. The key doppler-based indices include CFR, coronary flow capacity (CFC) and hyperaemic microvascular resistance (HMR). CFR evaluates the ratio of hyperaemic to resting flow velocity using Doppler method, reflecting microvascular reserve [49]. This method has significant disadvantages: a) insights into both epicardial and microvascular function, b) influenced by systemic hemodynamic changes, c) lower prognostic value compared to hyperaemic microvascular resistance in STEMI patients [50]. CFC combines maximum coronary flow measurements with CFR to assess the coronary circulation’s capacity. Therefore, it overcomes the limitations of the CFR but requires advanced imaging and technical expertise [51]. Of note, assessment of non-culprit vessel CFC in the setting of STEMI have shown to improve risk stratification following reperfusion of the IRA [52]. HMR is measured using a guidewire equipped with a distal pressure sensor and Doppler crystal. It calculates the ratio of hyperaemic mean distal pressure to Doppler-derived hyperaemic average peak velocity (APV). HMR can be specific to the microvasculature and independent of systemic factors but requires precise Doppler flow measurements and pharmacological hyperaemia. HMR can identify CMVD in STEMI patients and predict adverse clinical outcomes [50]. Also, HMR measured after PCI predicts microvascular injury and impaired myocardial blood flow, with a threshold of 2.5 mmHg/cm/s demonstrating high sensitivity for high-risk patients. HMR provides immediate results after revascularization and may be a better predictor of adverse clinical outcomes compared to CFR. However, its measurement is technically challenging, with higher failure rates due to the need for high-quality doppler signals, requiring further research to establish standardized cut-offs and enhance its prognostic utility.
Despite the high specificity of invasive techniques, their utility is often balanced against practical limitations such as cost, time, technical complexity, and patient’s risk. Invasive wire-based and sensor-based methods involves the induction of steady-state hyperaemia prolonging the procedure and further instrumentation of the IRA. Furthermore, they require an operator expertise limiting their widespread use. On the other hand, wire-based method directly quantifies the continuous absolute coronary flow (Q) and remains unaffected by systemic hemodynamic variations, ensuring high specificity [46]. Reduced absolute coronary flow indicate MVO or microvascular dysfunction, even when the epicardial arteries appear unobstructed in post-AMI patients [53]. Using Ohm’s law as the ratio of distal pressure to coronary flow, the continuous thermodilution technique may allow to calculate coronary microvascular resistance (Rμ) and identify STEMI patients with significant microvascular dysfunction after PPCI [54]. The lack of specific therapy of CMVD make them reserved for research settings, since their contribution to patient’s management is limited [55].
Angiography-derived computational flow dynamics.
More recently, evolution in invasive techniques has been proposed for the assessment of coronary microcirculation. Without traditional wire-based techniques, these simple methods mainly use the quantitative flow ratio (QFR) [56]. The angiography-derived IMR (IMRangio), uses computational fluid dynamics applied to the 3-dimensional reconstruction of the coronary artery derived from angiographic views during adenosine-induced steady-state hyperaemia. The procedure is faster, though it depends heavily on high-quality angiographic imaging and computational accuracy [57]. Similarly, the non-hyperaemic IMRangio (NH-IMRangio) avoids the use of pharmacologic hyperaemia, reducing patient discomfort with a good diagnostic accuracy in STEMI, but may not fully capture dynamic microvascular responses under stress [57]. Lastly, the computational protocol [40] has minimal procedural burden, but its clinical validation in certain scenarios remains limited to ensure reliability and facilitate their widespread adoption. [58]
4.2. Non-Invasive Methods
Stress Echocardiography (SE)
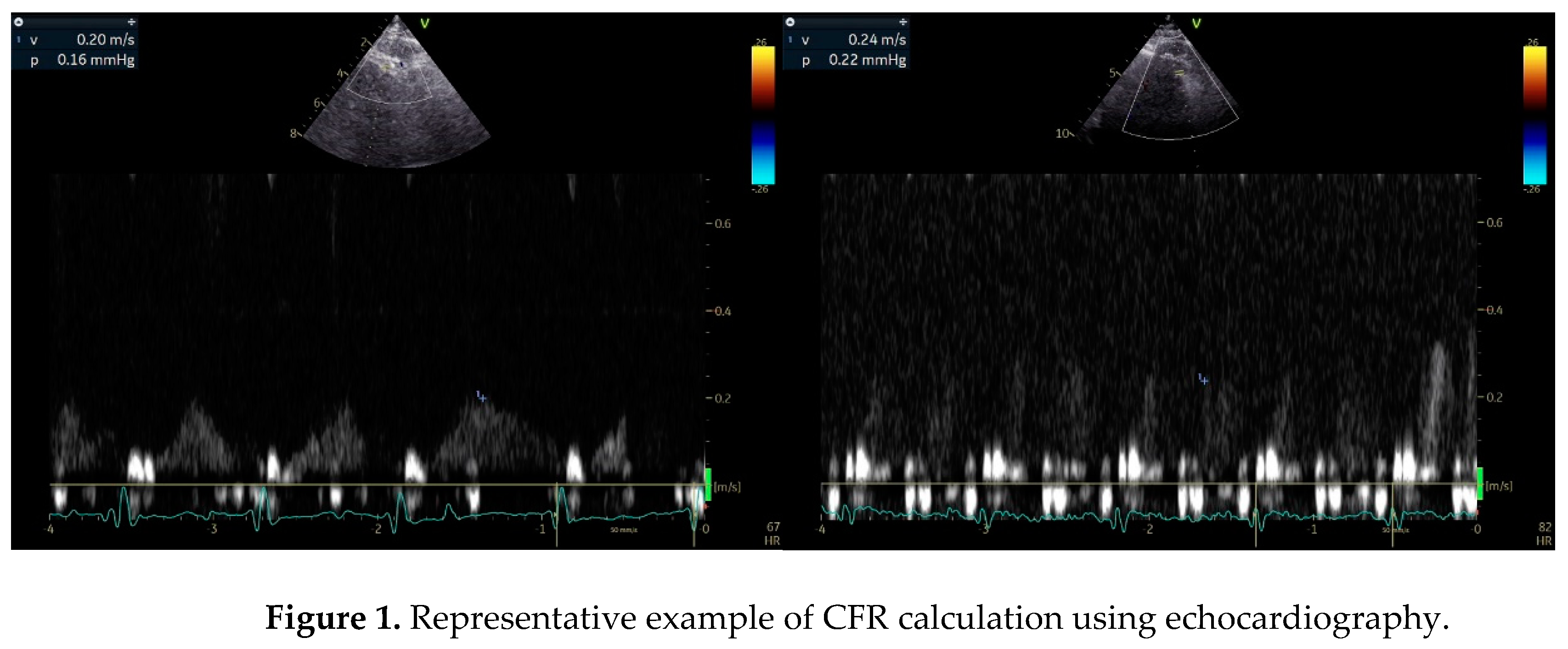
It remains a first-line technique for the diagnosis of significant CAD affecting epicardial coronary arteries. Wall motion abnormalities are usually not detected in patients with CMVD undergoing SE with dobutamine or exercise as stressors. Some operators have reported isolated hypokinesia of the apical segment of the interventricular septum, but this has not been established. Using the Doppler method and a modified apical view (between 2 and 3 chamber), the CFR can be measured during SE as an index of either absolute coronary flow in the left anterior descending artery (LAD) or microvascular circulation patency[59] (Figure 1). CFR is calculated as the ratio of baseline to hyperaemic coronary flow velocity, measured by pulsed wave Doppler during diastole, with vasodilators like dipyridamole or adenosine inducing hyperaemia[60,61]. This is a widely used and easily accessible technique, which unfortunately cannot distinguish macrovascular from microvascular dysfunction. In patients with MINOCA only after the exclusion of LAD significant stenosis, a low CFR (<2) indicates the impaired ability of vasculature to dilate adequately and meet metabolic demands during hyperemia[44,59,62]. However, CFR is not directly associated with fractional flow reserve (FFR) due to its dependence on microvascular resistance[63]. This discrepancy explains why CFR and FFR are often discordant in approximately 30% of patients with intermediate coronary artery stenoses. Despite this, CFR complements FFR findings, offering additional insights into coronary microvascular physiology, especially when assessing the interplay between epicardial stenosis and microvascular function[63]. A prospective study including 40 patients with INOCA found that dynamic CMVD was frequently provoked by hyperventilation, with a reduction in coronary flow velocity observed in 52% of cases, while adenosine-mediated vasodilation remained preserved, excluding significant structural CMVD. The test combining hyperventilation with exercise proved to be a more effective ischemia inducer than hyperventilation alone, highlighting its potential utility in noninvasive CMVD assessment[64]. In daily clinical practice, the timing of applying SE just after an AMI remains to be set.
Myocardial Perfusion in Stress Echocardiography
It is a bedside technique that assesses microvascular perfusion using echo contrast agents. It can effectively detect MVO and “no-reflow” areas after AMI[65]. During myocardial contrast echocardiography (MCE) a high mechanical index impulse is applied to destruct all microbubbles of the contrast agent. Myocardial contrast signal intensity is directly proportional to blood volume. In ischemic regions, a relative delayed myocardial replenishment will cause a reduction in the contrast signal. However, its adoption is hindered by operator dependency, reproducibility, moderate spatial resolution, safety concerns, and reimbursement issues[66]. In a meta-analysis including 13 studies evaluating the diagnostic accuracy of quantitative MCE for detecting coronary artery disease (CAD), it was demonstrated that parameters reflecting CMVD, such microbubble velocity and myocardial blood flow, were significantly reduced in patients with CAD, highlighting the utility of MCE for assessing microvascular dysfunction in patients with CAD[67].
Figure 1.
Representative example of CFR calculation using echocardiography.
CMR Imaging
It offers the capability to evaluate both global and per artery-related CFR with the use of pharmacological vasodilators like adenosine[68]. It is a safe, non-invasive method for evaluation of myocardial perfusion and/or MVO. CMR enables direct visualization and quantification of MVO, reflecting myocardial damage due to CMVD, using first-pass perfusion (FPP) and LGE techniques[69]. Dobutamine stress CMR is usually performed using a 1.5 T system with cine imaging and myocardial tagging during rest and incremental dobutamine infusion, followed by a bolus injection of gadolinium-DTPA at peak-dose dobutamine to acquire FPP images[70]. Wall motion and perfusion images are then visually analysed by an experienced radiologist and cardiologist to identify myocardial ischemia based on perfusion deficits in at least two segments of consecutive short-axis slices[70]. CMR-derived indices of myocardial perfusion like microcirculatory perfusion index (MPI), and perfusion resistance index (MPRI) may be associated with invasive measurements of CMVD and hold prognostic significance in clinical outcomes[62]. Additionally, by utilizing gadolinium-based contrast agents, CMR enables both visual and semi-quantitative evaluation of myocardial perfusion reserve (MPR), identifying areas of impaired blood flow suggestive of CMVD. Novel techniques like contrast-free T1 mapping show potential in providing further diagnostic insights into CMVD without reliance on gadolinium[71].
Single-photon emission computed tomography (SPECT) and cardiac PET/CT are nuclear imaging techniques capable of detecting the no-reflow phenomenon in patients with MVO[72]. PET, with its ability to measure absolute myocardial blood flow and flow reserve, provides a non-invasive, quantitative assessment of myocardial perfusion by calculating CFR before and after administration of vasodilators including adenosine[73]. However, PET scan remains underutilized mainly due to limited availability of PET scanners and cyclotrons and higher cost[72]. A study by Mayala involving 28 patients demonstrated that PET/CT identified reduced CFR (<2.6) in 89% of patients with normal coronary angiography findings, confirming the presence of CMVD and highlighting its high sensitivity[73], especially in the post-MI setting.PET offers several advantages, including accurate quantification of myocardial blood flow and perfusion, and outperforms other modalities like SPECT by reducing false-positive results. It excels in quantifying coronary physiology and detecting CMVD, even in non-culprit coronary arteries, where reduced CFR has been shown to predict long-term adverse cardiovascular events[74].
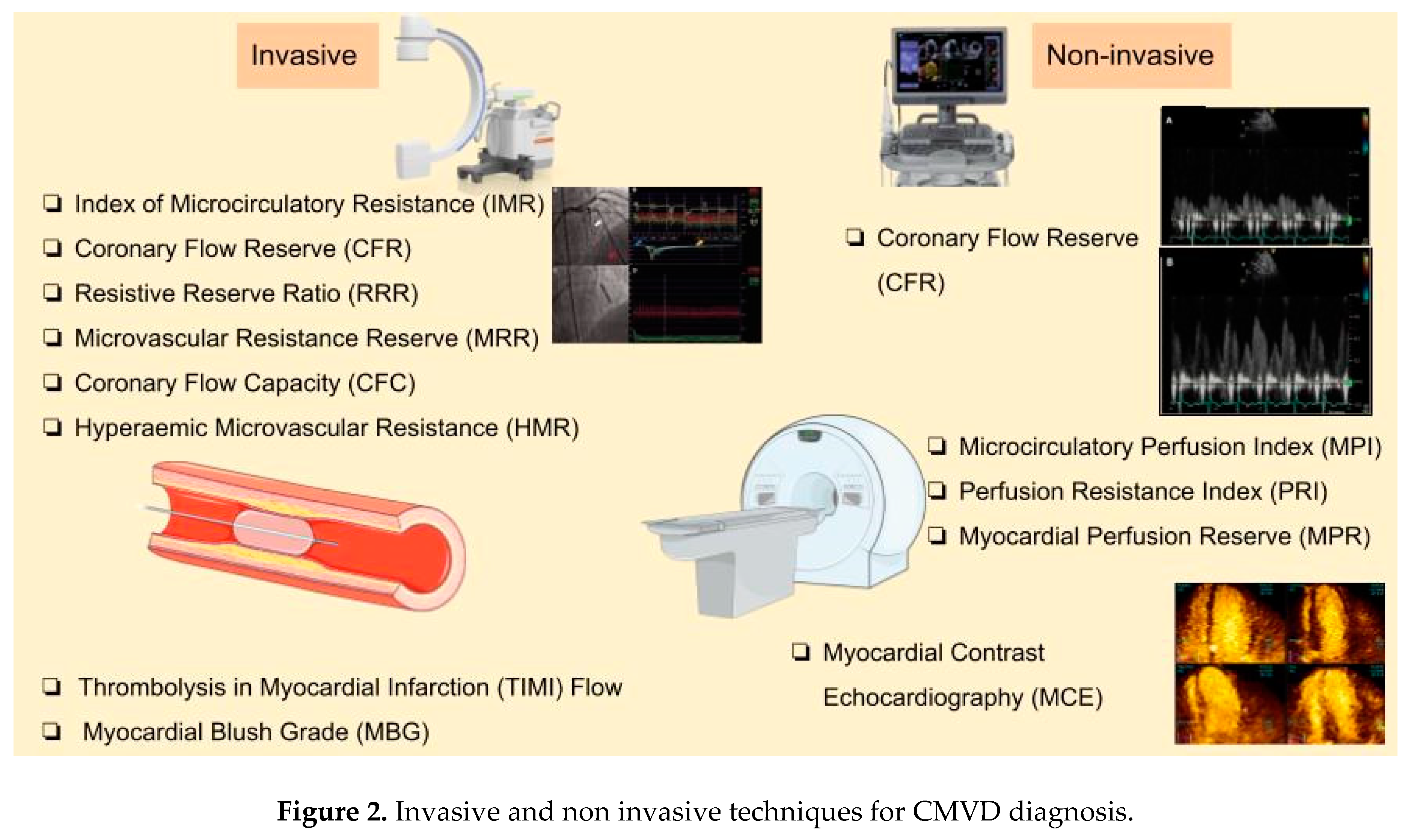
Figure 2.
Invasive and non invasive techniques for CMVD diagnosis.
5. Prognostic Value of CMVD
CMVD in post-AMI is linked to both poor prognosis and an impaired quality of life due to high morbidity, highlighting the clinical importance of accurate identification and diagnosis[75]. Over time, some of the diagnostic indices already mentioned in previous sections, not only provide valuable prognostic insights but may also serve as a guide for therapeutic interventions to ameliorate the long-term outcomes of post-AMI patients[76,77].
Myocardial contrast echocardiography (MCE): Delayed or absent myocardial uptake at first pass of contrast agent indicates areas of no-reflow and MVO. However, its widespread use is limited by the uncertain reproducibility, low sensitivity, and reimbursement challenges in some countries[65,78].
CMR imaging: Several indices of CMR have been analyzed for their potential prognostic value Symons et al. demonstrated that the early detection of CMR-based MVO is a strong independent predictor of MACE in patients after re-perfused STEMI. As already mentioned, MVO extent ≥2.6% of the left ventricle was the strongest independent predictor of death and heart failure hospitalization up to six years after STEMI[79]. Although MVO may occupy only a small portion of the total infarct area (around 1%–5% of the left ventricular mass in pooled studies), its extent correlates with the total infarct size and future events[80]. Notably, the diagnosis of MVO improves long-term risk stratification in patients with re-perfused STEMI[81]. The MVO assessment by CMR derives from both structural imaging and functional data. It may be implicated by subtle abnormalities in CFR and relates to poor prognosis during follow-up after AMI[74,82]. A small study enrolling 30 patients after AMI showed that FPP combined with delayed enhancement in CMR (DE-CMR) effectively evaluated myocardial viability, and MVO which in turn were associated to ventricular remodeling and patients’ outcomes[83]. The same modality accurately identified IMH, associated with impaired ventricular function and infarct size at 1-month post-AMI, which apparently determined clinical outcomes during recovery[84].
Cardiac PET studies: The dysregulated post-infarction inflammation and remodeling is associated with adverse outcomes in post-AMI patients[85]. A low CFR (<2) calculated in PET scan has been associated with higher cardiac mortality risk[86]. PET-derived CFR may assist to predict long-term cardiovascular outcomes,. A previous clinical study of 49 STEMI patients undergoing PET scan to assess 18F-FDG uptake demonstrated that abnormal responses to sympathetic stimulation linked to adverse functional outcomes like LVEF, LV end-systolic and end-diastolic volume despite PPCI[87].
Myocardial blush grade (MBG): This is a qualitive index of microcirculatory damage. Recent meta-analysis showed a relationship of low MBG with larger infarct size, adverse ventricular remodeling, and worse outcomes in post-AMI patients[88]. MBG 0–1 has been associated with increased mortality at 16-month follow-up in patients with AMI[9,89]. Kaya et al. demonstrated that MBG grade 3 serves as a significant marker for survival, superior to TIMI flow grades in post-AMI follow-up period[90]. A meta-analysis of eight observational studies, encompassing 8,044 patients with an overall low risk of bias, revealed that MBG grade: 0 or 1, indicative of poor or absent myocardial perfusion, carries a negative prognostic value for mortality (OR: 2.68; 95% CI [2.22–3.23]) and MACE (OR: 1.20; 95% CI [1.01–1.41]) in STEMI patients. Conversely, MBG grade 2 and 3, reflecting moderate and normal myocardial perfusion, respectively, were associated with improved survival outcomes (logHR: 0.47 (95% CI [0.43–0.52]) and log HR: 0.20 (95% CI [0.18–0.23], respectively)[88,7,91]. Despite the low sensitivity of MBG, it could be prognostic marker for STEMI patients with CMVD.
IMR: Up to now IMR remains the gold standard invasive technique for CMVD diagnosis. Growing body of data supports its prognostic value. In particular, it has been associated with MVO and adverse clinical events. In addition to diagnosis, IMR has been used to predict the recovery of left ventricular function after elective PCI[92]. Interestingly, patients with STEMI and an IMR >40 appeared with higher incidence of mortality and heart failure, and exhibited an 11.9-fold higher likelihood of having an infarct size greater than 25% of the myocardial mass at 6-month follow-up. That was further confirmed in another study of STEMI patients undergoing PPCI where the increased IMR due to MVO was independently associated with larger infarct size and poorer long-term clinical outcomes [HR: 4.2 (95% CI: 1.4–12.5); p = 0.009]. In contrast, when IMR remained preserved, even in the presence of MVO, significant regression of infarct size was achieved over time. Moreover, high IMR demonstrated a modest but significantly negative correlation with LVEF at 3 months (p = 0.004) and at 1 year (p < 0.0001), which is of clinical relevance. Maznyczka et al. recently demonstrated that in patients with STEMI presented within six hours from symptom onset, both Resistive Reserve Ratio (RRR) and IMR were associated with the extent of MVO, myocardial hemorrhage, infarct size, and clinical outcomes. [43]
The superiority of RRR (cut off: <2.62) over CFR (cut off: <2.5) has been proposed in patients with angina and non-obstructed coronary arteries, but further research is warranted[93]. On the other hand, the MRR offers a theoretical advantage by enabling more reliable inter-patient comparisons. However, it is a relatively novel index and available data are limited requiring validation. In a large cohort of 446 AMI patients undergoing PPCI, the low MRR cutoff for predicting the primary endpoint was set at (≤1.25). During a median follow-up of 3.1 years (Q1–Q3: 1.5–6.1 years), the composite outcome of all-cause mortality or heart failure hospitalization occurred in 27.3% vs 5.9% of patients with low MRR value than those with higher (>1.25) (HR: 4.16; 95% CI: 2.31–7.50; p < 0.001)[94]. The independent prognostic value of MRR measured just after PPCI was also recently mentioned by Tsai TY et al. 2024[47].
Hyperemic microvascular resistance (HMR): In a cohort of 176 STEMI patients treated with successful PPCI, HMR was a strong predictor of both adverse clinical outcomes (death and heart failure hospitalization) and microvascular injury during a follow-up of 3.2 years (median value)[95]. This observation indicates that an increased HMR distal to a coronary stenosis reflects important pathophysiological alterations in the distal microvasculature in the setting of obstructive coronary artery disease. HMR may therefore be a useful tool to quantify the functional status of the myocardial microvasculature in clinical practice.[96]
IMRangio: It has demonstrated good accuracy in predicting CMVD in the IRA of STEMI patients when compared with IMR and MVO[57]. In NSTEMI patients undergoing PCI, those with IMRangio >25 exhibited a significantly higher incidence of MACEs (cardiac death, readmission for heart failure, myocardial reinfarction, and target vessel revascularization) compared to those with IMRangio ≤25 (32.52% vs 9.37%; p<0.001). Moreover, post-PCI IMRangio >25 was identified as an independent predictor of MACEs (HR: 4.230; 95% CI: 3.151–5.679; p<0.001). The addition of IMRangio to a predictive model using exclusively conventional risk factors improved the discriminatory ability[97].
Coronary flow reserve (CFR): It reflects the functional status of both the epicardial and microvascular segment[61]. Despite its limited capability to assess coronary microcirculation in the presence of residual epicardial stenosis, an abnormal CFR has still been linked to a significantly higher incidence of MACEs in patients with acute coronary syndromes (HR: 3.76; 95% CI: 2.35–6.00)[98]. Two recent meta-analyses, comprising of 19 and 11 studies respectively, demonstrated that low CFR in patients with myocardial ischemia but with non-obstructive CAD—evaluated through either non-invasive techniques (SE, positron emission tomography (PET), or invasive methods—was significantly associated with an increased risk of death and MACE[99,100]. Moreover, CFR measured with either non-invasive or invasive methods was significantly associated with final infarct size and reduced LVEF in STEMI patients undergoing angiographically successful PPCI[101]. The early measurement of CFR by TDE can assess the degree of successful reperfusion in AMI and can predict LV functional recovery, myocardial viability and the final infarct size [102].
6. Discussion and Future Perspectives
Conclusively, a number of modalities have been proposed to enhance the diagnostic accuracy of CMVD in post-MI individuals. Since the presence of CMVD is associated with an increased risk of mortality and MACE even after a successful revascularization in individuals with AMI, invasive and non-invasive techniques have been developed. However, until now their implementation in daily practice is limited. The calculation of CFR through invasive methods like thermodilution or Doppler flow velocity are already recommended by ESC and AHA/ACC guidelines (IIa) for patients with persistent symptoms and normal or moderately stenosed coronary arteries in patients with chronic CAD or episodes of chest pain[40]. Furthermore, the measurement of IMR during catheterization could be a possible way, so that all participants with AMI would be evaluated for the presence of CMVD. This technique offers high specificity, modest sensitivity, it is time consuming and requiring hyperaemia provocation during acute phase for CMVD detection.
Stress doppler echocardiography offers an easy tool for measuring CFR, but it cannot distinguish microvascular from macrovascular obstruction. The presence of residual epicardial stenosis can interfere with the precision of the measurements. Moreover, it is important to decide the timing of performing the test, since shortly after the AMI (up to 6 weeks) a maximum stress test is contraindicated. During the early post-infarction period, the identification of CMVD with CMR could be useful for individuals with high probability, but negative results of invasive techniques. CMR constitutes an independent predictor of long-term morbidity. Lastly, PET could be reserved for patients with high probability of CMVD, because of its role in prediction of myocardial healing.
It is essential that all available indices should be validated through large prospective cohort studies and head-to-head comparisons. There are numerous medications that seem to be effective regarding the reduction of CMVD[30]. This includes the administration of aspirin, unfractionated heparin, potent P2Y12 inhibitors or nicorandil. During the PCI, medications such as adenosine, calcium channel blockers, glycoprotein IIb/IIIa inhibitors, low dose thrombolytics can also be administered. Also important is the post-PCI administration of high dose statins, unfractionated heparin, glycoprotein IIb/IIIa inhibitors and/or nicorandil. It is evident that the improvement of survival and morbidity for AMI patients is largely influenced by the combination of various medications simultaneously targeting multiple pathophysiological pathways.
Author Contributions
Conceptualization, N.P.E.K. and S.S.; methodology, E.K. and D.K.; validation, N.P.E.K. and AM.; formal analysis, N.V.; investigation, E.K., D.K., A.M.. and S.S..; resources, N.V..; data curation, NK.; writing—original draft preparation, E.K., D.K., T.P. and P.K.; writing—review and editing, N.P.E.K., A.M., E.K., D.K., N.V.,S.S.; supervision, N.P.E.K.; project administration, N.P.E.K.; funding acquisition, N.P.E.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the UNIVERSITY OF CYPRUS (Decision number 6950/2022).
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 18F-FDG | Fluorodeoxyglucose F-18 |
| AHA/ACC | American Heart Association/American College of Cardiology |
| ACS | Acute Coronary Syndrome |
| AMI | Acute Myocardial Infarction |
| ATP | Adenosine Triphosphate |
| CAD | Coronary Artery Disease |
| CDKN2B-AS1 | Cyclin-Dependent Kinase Inhibitor 2B Antisense RNA 1 |
| CFC | Coronary Flow Capacity |
| CFR | Coronary Flow Reserve |
| CFVR | Coronary Flow Velocity Reserve |
| CI | Confidence Interval |
| CMVD | Coronary Microvascular Disease |
| CMR | Cardiac Magnetic Resonance |
| CTFC | Corrected TIMI Frame Count |
| DAMPs | Damage-Associated Molecular Patterns |
| DE-CMR | Delayed Enhancement Cardiac Magnetic Resonance |
| ESC | European Society of Cardiology |
| FFR | Fractional Flow Reserve |
| FPP | First-Pass Perfusion |
| HF | Heart Failure |
| HMR | Hyperemic Microvascular Resistance |
| HR | Hazard Ratio |
| IL-6 | Interleukin-6 |
| IMH | Intramyocardial Haemorrhage |
| IMR | Index of Microcirculatory Resistance |
| IMRangio | Angiography-Derived Index of Microcirculatory Resistance |
| INOCA | Ischemia with Non-Obstructive Coronary Arteries |
| IRA | Infarct-Related Artery |
| LAD | Left Anterior Descending Artery |
| LGE | Late Gadolinium Enhancement |
| LV | Left Ventricular |
| LVEF | Left Ventricular Ejection Fraction |
| MACE | Major Adverse Cardiovascular Events |
| MBG | Myocardial Blush Grade |
| MCE | Myocardial Contrast Echocardiography |
| MINOCA | Myocardial Infarction with Non-Obstructed Coronary Arteries |
| MPI | Microcirculatory Perfusion Index |
| MPRI | Myocardial Perfusion Reserve Index |
| MRR | Microvascular Resistance Reserve |
| MVO | Microvascular Obstruction |
| MYH15 | Myosin Heavy Chain 15 |
| NH-IMRangio | Non-Hyperemic Angiography-Derived Index of Microcirculatory Resistance |
| NO | Nitric Oxide |
| NT5E | 5′-Nucleotidase Ecto |
| OR | Odds Ratio |
| PCI | Percutaneous Coronary Intervention |
| PET | Positron Emission Tomography |
| PPCI | Primary Percutaneous Coronary Intervention |
| QFR | Quantitative Flow Ratio |
| ROS | Reactive Oxygen Species |
| RRR | Resistive Reserve Ratio |
| SE | Stress Echocardiography |
| SPECT | Single-Photon Emission Computed Tomography |
| STEMI | ST-segment Elevation Myocardial Infarction |
| STR | ST-segment Resolution |
| TDE | Transthoracic Doppler Echocardiography |
| TIMI | Thrombolysis in Myocardial Infarction |
| TNF-α | Tumor Necrosis Factor-alpha |
| VEGFA | Vascular Endothelial Growth Factor A |
References
- Pries, A.R.; Badimon, L.; Bugiardini, R.; Camici, P.G.; Dorobantu, M.; Duncker, D.J.; Escaned, J.; Koller, A.; Piek, J.J.; De Wit, C. Coronary Vascular Regulation, Remodelling, and Collateralization: Mechanisms and Clinical Implications on Behalf of the Working Group on Coronary Pathophysiology and Microcirculation. Eur Heart J 2015, 36, 3134–3146. [CrossRef]
- Robbers, L.F.H.J.; Eerenberg, E.S.; Teunissen, P.F.A.; Jansen, M.F.; Hollander, M.R.; Horrevoets, A.J.G.; Knaapen, P.; Nijveldt, R.; Heymans, M.W.; Levi, M.M.; et al. Magnetic Resonance Imaging-Defined Areas of Microvascular Obstruction after Acute Myocardial Infarction Represent Microvascular Destruction and Haemorrhage. European Heart Journal 2013, 34, 2346–2353. [CrossRef]
- Choi, K.H.; Dai, N.; Li, Y.; Kim, J.; Shin, D.; Lee, S.H.; Joh, H.S.; Kim, H.K.; Jeon, K.-H.; Ha, S.J.; et al. Functional Coronary Angiography–Derived Index of Microcirculatory Resistance in Patients With ST-Segment Elevation Myocardial Infarction. JACC: Cardiovascular Interventions 2021, 14, 1670–1684. [CrossRef]
- Kunadian, V.; Chieffo, A.; Camici, P.G.; Berry, C.; Escaned, J.; Maas, A.H.E.M.; Prescott, E.; Karam, N.; Appelman, Y.; Fraccaro, C.; et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. European Heart Journal 2020, 41, 3504–3520. [CrossRef]
- Saad, M.; Stiermaier, T.; Fuernau, G.; Pöss, J.; De Waha-Thiele, S.; Desch, S.; Thiele, H.; Eitel, I. Impact of Direct Stenting on Myocardial Injury Assessed by Cardiac Magnetic Resonance Imaging and Prognosis in ST-Elevation Myocardial Infarction. International Journal of Cardiology 2019, 283, 88–92. [CrossRef]
- El Aidi, H.; Adams, A.; Moons, K.G.M.; Den Ruijter, H.M.; Mali, W.P.Th.M.; Doevendans, P.A.; Nagel, E.; Schalla, S.; Bots, M.L.; Leiner, T. Cardiac Magnetic Resonance Imaging Findings and the Risk of Cardiovascular Events in Patients With Recent Myocardial Infarction or Suspected or Known Coronary Artery Disease. Journal of the American College of Cardiology 2014, 63, 1031–1045. [CrossRef]
- Canu, M.; Khouri, C.; Marliere, S.; Vautrin, E.; Piliero, N.; Ormezzano, O.; Bertrand, B.; Bouvaist, H.; Riou, L.; Djaileb, L.; et al. Prognostic Significance of Severe Coronary Microvascular Dysfunction Post-PCI in Patients with STEMI: A Systematic Review and Meta-Analysis. PLoS ONE 2022, 17, e0268330. [CrossRef]
- Beltrame, J.F.; Crea, F.; Camici, P. Advances in Coronary Microvascular Dysfunction. Heart, Lung and Circulation 2009, 18, 19–27. [CrossRef]
- Niccoli, G.; Scalone, G.; Lerman, A.; Crea, F. Coronary Microvascular Obstruction in Acute Myocardial Infarction. Eur Heart J 2016, 37, 1024–1033. [CrossRef]
- Galli, M.; Niccoli, G.; De Maria, G.; Brugaletta, S.; Montone, R.A.; Vergallo, R.; Benenati, S.; Magnani, G.; D’Amario, D.; Porto, I.; et al. Coronary Microvascular Obstruction and Dysfunction in Patients with Acute Myocardial Infarction. Nat Rev Cardiol 2024, 21, 283–298. [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). Journal of the American College of Cardiology 2018, 72, 2231–2264. [CrossRef]
- Heusch, G. Myocardial Ischaemia–Reperfusion Injury and Cardioprotection in Perspective. Nat Rev Cardiol 2020, 17, 773–789. [CrossRef]
- Zhao, B.-H.; Ruze, A.; Zhao, L.; Li, Q.-L.; Tang, J.; Xiefukaiti, N.; Gai, M.-T.; Deng, A.-X.; Shan, X.-F.; Gao, X.-M. The Role and Mechanisms of Microvascular Damage in the Ischemic Myocardium. Cell. Mol. Life Sci. 2023, 80, 341. [CrossRef]
- Heusch, G. Treatment of Myocardial Ischemia/Reperfusion Injury by Ischemic and Pharmacological Postconditioning. In Comprehensive Physiology; Terjung, R., Ed.; Wiley, 2015; pp. 1123–1145 ISBN 978-0-470-65071-4.
- Maslov, L.N.; Popov, S.V.; Naryzhnaya, N.V.; Mukhomedzyanov, A.V.; Kurbatov, B.K.; Derkachev, I.A.; Boshchenko, A.A.; Khaliulin, I.; Prasad, N.R.; Singh, N.; et al. The Regulation of Necroptosis and Perspectives for the Development of New Drugs Preventing Ischemic/Reperfusion of Cardiac Injury. Apoptosis 2022, 27, 697–719. [CrossRef]
- Doherty, D.J.; Sykes, R.; Mangion, K.; Berry, C. Predictors of Microvascular Reperfusion After Myocardial Infarction. Curr Cardiol Rep 2021, 23, 21. [CrossRef]
- Reffelmann, T.; Kloner, R.A. The No-Reflow Phenomenon: A Basic Mechanism of Myocardial Ischemia and Reperfusion. Basic Res Cardiol 2006, 101, 359–372. [CrossRef]
- Konijnenberg, L.S.F.; Damman, P.; Duncker, D.J.; Kloner, R.A.; Nijveldt, R.; Van Geuns, R.-J.M.; Berry, C.; Riksen, N.P.; Escaned, J.; Van Royen, N. Pathophysiology and Diagnosis of Coronary Microvascular Dysfunction in ST-Elevation Myocardial Infarction. Cardiovascular Research 2020, 116, 787–805. [CrossRef]
- Dörge, H.; Schulz, R.; Belosjorow, S.; Post, H.; Van De Sand, A.; Konietzka, I.; Frede, S.; Hartung, T.; Vinten-Johansen, J.; Youker, K.A.; et al. Coronary Microembolization: The Role of TNF- α in Contractile Dysfunction. Journal of Molecular and Cellular Cardiology 2002, 34, 51–62. [CrossRef]
- Yuan, Y.; Li, B.; Peng, W.; Xu, Z. Protective Effect of Glycyrrhizin on Coronary Microembolization-induced Myocardial Dysfunction in Rats. Pharmacology Res & Perspec 2021, 9, e00714. [CrossRef]
- Loubeyre, C.; Morice, M.-C.; Lefèvre, T.; Piéchaud, J.-F.; Louvard, Y.; Dumas, P. A Randomized Comparison of Direct Stenting with Conventional Stent Implantation in Selected Patients with Acute Myocardial Infarction. Journal of the American College of Cardiology 2002, 39, 15–21. [CrossRef]
- Selvanayagam, J.B.; Cheng, A.S.H.; Jerosch-Herold, M.; Rahimi, K.; Porto, I.; Van Gaal, W.; Channon, K.M.; Neubauer, S.; Banning, A.P. Effect of Distal Embolization on Myocardial Perfusion Reserve After Percutaneous Coronary Intervention: A Quantitative Magnetic Resonance Perfusion Study. Circulation 2007, 116, 1458–1464. [CrossRef]
- Kleinbongard, P.; Heusch, G. A Fresh Look at Coronary Microembolization. Nat Rev Cardiol 2022, 19, 265–280. [CrossRef]
- Wu, K.C. CMR of Microvascular Obstruction and Hemorrhage in Myocardial Infarction. Journal of Cardiovascular Magnetic Resonance 2012, 14, 72. [CrossRef]
- Heusch, G.; Gersh, B.J. The Pathophysiology of Acute Myocardial Infarction and Strategies of Protection beyond Reperfusion: A Continual Challenge. Eur Heart J 2016, ehw224. [CrossRef]
- Yoshino, S.; Cilluffo, R.; Best, P.J.M.; Atkinson, E.J.; Aoki, T.; Cunningham, J.M.; De Andrade, M.; Choi, B.-J.; Lerman, L.O.; Lerman, A. Single Nucleotide Polymorphisms Associated with Abnormal Coronary Microvascular Function. Coronary Artery Disease 2014, 25, 281–289. [CrossRef]
- Iwakura, K.; Ito, H.; Ikushima, M.; Kawano, S.; Okamura, A.; Asano, K.; Kuroda, T.; Tanaka, K.; Masuyama, T.; Hori, M.; et al. Association between Hyperglycemia and the No-Reflow Phenomenon Inpatients with Acute Myocardial Infarction. Journal of the American College of Cardiology 2003, 41, 1–7. [CrossRef]
- Dąbrowska, E.; Narkiewicz, K. Hypertension and Dyslipidemia: The Two Partners in Endothelium-Related Crime. Curr Atheroscler Rep 2023, 25, 605–612. [CrossRef]
- Ferdinandy, P.; Andreadou, I.; Baxter, G.F.; Bøtker, H.E.; Davidson, S.M.; Dobrev, D.; Gersh, B.J.; Heusch, G.; Lecour, S.; Ruiz-Meana, M.; et al. Interaction of Cardiovascular Nonmodifiable Risk Factors, Comorbidities and Comedications With Ischemia/Reperfusion Injury and Cardioprotection by Pharmacological Treatments and Ischemic Conditioning. Pharmacological Reviews 2023, 75, 159–216. [CrossRef]
- Scarsini, R.; Portolan, L.; Della Mora, F.; Marin, F.; Mainardi, A.; Ruzzarin, A.; Levine, M.B.; Banning, A.P.; Ribichini, F.; Garcia Garcia, H.M.; et al. Angiography-Derived and Sensor-Wire Methods to Assess Coronary Microvascular Dysfunction in Patients With Acute Myocardial Infarction. JACC: Cardiovascular Imaging 2023, 16, 965–981. [CrossRef]
- The TIMI Study Group* The Thrombolysis in Myocardial Infarction (TIMI) Trial: Phase I Findings. N Engl J Med 1985, 312, 932–936. [CrossRef]
- Jaffe, R.; Charron, T.; Puley, G.; Dick, A.; Strauss, B.H. Microvascular Obstruction and the No-Reflow Phenomenon After Percutaneous Coronary Intervention. Circulation 2008, 117, 3152–3156. [CrossRef]
- Marra, M.P.; Corbetti, F.; Cacciavillani, L.; Tarantini, G.; Ramondo, A.B.; Napodano, M.; Basso, C.; Lacognata, C.; Marzari, A.; Maddalena, F.; et al. Relationship between Myocardial Blush Grades, Staining, and Severe Microvascular Damage after Primary Percutaneous Coronary Intervention. American Heart Journal 2010, 159, 1124–1132. [CrossRef]
- Ohara, Y. Relation between the TIMI Frame Count and the Degree of Microvascular Injury after Primary Coronary Angioplasty in Patients with Acute Anterior Myocardial Infarction. Heart 2005, 91, 64–67. [CrossRef]
- Kest, M.; Ágoston, A.; Szabó, G.T.; Kiss, A.; Üveges, Á.; Czuriga, D.; Komócsi, A.; Hizoh, I.; Kőszegi, Z. Angiography-Based Coronary Microvascular Assessment with and without Intracoronary Pressure Measurements: A Systematic Review. Clin Res Cardiol 2024, 113, 1609–1621. [CrossRef]
- Fearon, W.F.; Balsam, L.B.; Farouque, H.M.O.; Robbins, R.C.; Fitzgerald, P.J.; Yock, P.G.; Yeung, A.C. Novel Index for Invasively Assessing the Coronary Microcirculation. Circulation 2003, 107, 3129–3132. [CrossRef]
- Ng, M.K.C.; Yeung, A.C.; Fearon, W.F. Invasive Assessment of the Coronary Microcirculation: Superior Reproducibility and Less Hemodynamic Dependence of Index of Microcirculatory Resistance Compared With Coronary Flow Reserve. Circulation 2006, 113, 2054–2061. [CrossRef]
- Okura, H.; Fuyuki, H.; Kubo, T.; Iwata, K.; Taguchi, H.; Toda, I.; Yoshikawa, J. Noninvasive Diagnosis of Ischemic and Nonischemic Cardiomyopathy Using Coronary Flow Velocity Measurements of the Left Anterior Descending Coronary Artery by Transthoracic Doppler Echocardiography. Journal of the American Society of Echocardiography 2006, 19, 552–558. [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Chronic Coronary Syndromes. European Heart Journal 2020, 41, 407–477. [CrossRef]
- Gulati, M.; Levy, P.D.; Mukherjee, D.; Amsterdam, E.; Bhatt, D.L.; Birtcher, K.K.; Blankstein, R.; Boyd, J.; Bullock-Palmer, R.P.; Conejo, T.; et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 144. [CrossRef]
- Carrick, D.; Haig, C.; Ahmed, N.; Carberry, J.; Yue May, V.T.; McEntegart, M.; Petrie, M.C.; Eteiba, H.; Lindsay, M.; Hood, S.; et al. Comparative Prognostic Utility of Indexes of Microvascular Function Alone or in Combination in Patients With an Acute ST-Segment–Elevation Myocardial Infarction. Circulation 2016, 134, 1833–1847. [CrossRef]
- De Waard, G.A.; Hollander, M.R.; Teunissen, P.F.A.; Jansen, M.F.; Eerenberg, E.S.; Beek, A.M.; Marques, K.M.; Van De Ven, P.M.; Garrelds, I.M.; Danser, A.H.J.; et al. Changes in Coronary Blood Flow After Acute Myocardial Infarction. JACC: Cardiovascular Interventions 2016, 9, 602–613. [CrossRef]
- Maznyczka, A.M.; Oldroyd, K.G.; Greenwood, J.P.; McCartney, P.J.; Cotton, J.; Lindsay, M.; McEntegart, M.; Rocchiccioli, J.P.; Good, R.; Robertson, K.; et al. Comparative Significance of Invasive Measures of Microvascular Injury in Acute Myocardial Infarction. Circ: Cardiovascular Interventions 2020, 13, e008505. [CrossRef]
- Toya, T.; Ahmad, A.; Corban, M.T.; Ӧzcan, I.; Sara, J.D.; Sebaali, F.; Escaned, J.; Lerman, L.O.; Lerman, A. Risk Stratification of Patients With NonObstructive Coronary Artery Disease Using Resistive Reserve Ratio. JAHA 2021, 10, e020464. [CrossRef]
- Scarsini, R.; De Maria, G.L.; Borlotti, A.; Kotronias, R.A.; Langrish, J.P.; Lucking, A.J.; Choudhury, R.P.; Ferreira, V.M.; Ribichini, F.; Channon, K.M.; et al. Incremental Value of Coronary Microcirculation Resistive Reserve Ratio in Predicting the Extent of Myocardial Infarction in Patients with STEMI. Insights from the Oxford Acute Myocardial Infarction (OxAMI) Study. Cardiovascular Revascularization Medicine 2019, 20, 1148–1155. [CrossRef]
- Gallinoro, E.; Candreva, A.; Colaiori, I.; Kodeboina, M.; Fournier, S.; Nelis, O.; Di Gioia, G.; Sonck, J.; Van ’T Veer, M.; Pijls, N.H.J.; et al. Thermodilution-Derived Volumetric Resting Coronary Blood Flow Measurement in Humans. EuroIntervention 2021, 17, e672–e679. [CrossRef]
- Tsai, T.-Y.; Aldujeli, A.; Haq, A.; Knokneris, A.; Briedis, K.; Hughes, D.; Unikas, R.; Renkens, M.; Revaiah, P.C.; Tobe, A.; et al. The Impact of Microvascular Resistance Reserve on the Outcome of Patients With STEMI. JACC: Cardiovascular Interventions 2024, 17, 1214–1227. [CrossRef]
- Doucette, J.W.; Corl, P.D.; Payne, H.M.; Flynn, A.E.; Goto, M.; Nassi, M.; Segal, J. Validation of a Doppler Guide Wire for Intravascular Measurement of Coronary Artery Flow Velocity. Circulation 1992, 85, 1899–1911. [CrossRef]
- Van De Hoef, T.P.; Bax, M.; Meuwissen, M.; Damman, P.; Delewi, R.; De Winter, R.J.; Koch, K.T.; Schotborgh, C.; Henriques, J.P.S.; Tijssen, J.G.P.; et al. Impact of Coronary Microvascular Function on Long-Term Cardiac Mortality in Patients With Acute ST-Segment–Elevation Myocardial Infarction. Circ: Cardiovascular Interventions 2013, 6, 207–215. [CrossRef]
- De Waard, G.A.; Fahrni, G.; De Wit, D.; Kitabata, H.; Williams, R.; Patel, N.; Teunissen, P.F.; Van De Ven, P.M.; Umman, S.; Knaapen, P.; et al. Hyperaemic Microvascular Resistance Predicts Clinical Outcome and Microvascular Injury after Myocardial Infarction. Heart 2018, 104, 127–134. [CrossRef]
- Van De Hoef, T.P.; Echavarría-Pinto, M.; Van Lavieren, M.A.; Meuwissen, M.; Serruys, P.W.J.C.; Tijssen, J.G.P.; Pocock, S.J.; Escaned, J.; Piek, J.J. Diagnostic and Prognostic Implications of Coronary Flow Capacity. JACC: Cardiovascular Interventions 2015, 8, 1670–1680. [CrossRef]
- Van Lavieren, M.A.; Stegehuis, V.E.; Bax, M.; Echavarría-Pinto, M.; Wijntjens, G.W.M.; De Winter, R.J.; Koch, K.T.; Henriques, J.P.; Escaned, J.; Meuwissen, M.; et al. Time Course of Coronary Flow Capacity Impairment in ST-Segment Elevation Myocardial Infarction. European Heart Journal. Acute Cardiovascular Care 2021, 10, 516–522. [CrossRef]
- Wijnbergen, I.; Van ’T Veer, M.; Lammers, J.; Ubachs, J.; Pijls, N.H.J. Absolute Coronary Blood Flow Measurement and Microvascular Resistance in ST-Elevation Myocardial Infarction in the Acute and Subacute Phase. Cardiovascular Revascularization Medicine 2016, 17, 81–87. [CrossRef]
- Konstantinou, K.; Karamasis, G.V.; Davies, J.R.; Alsanjari, O.; Tang, K.H.; Gamma, R.A.; Kelly, P.R.; Pijls, N.H.J.; Keeble, T.R.; Clesham, G.J. Absolute Microvascular Resistance by Continuous Thermodilution Predicts Microvascular Dysfunction after ST-Elevation Myocardial Infarction. International Journal of Cardiology 2020, 319, 7–13. [CrossRef]
- Kogame, N.; Ono, M.; Kawashima, H.; Tomaniak, M.; Hara, H.; Leipsic, J.; Andreini, D.; Collet, C.; Patel, M.R.; Tu, S.; et al. The Impact of Coronary Physiology on Contemporary Clinical Decision Making. JACC: Cardiovascular Interventions 2020, 13, 1617–1638. [CrossRef]
- Tu, S.; Westra, J.; Yang, J.; Von Birgelen, C.; Ferrara, A.; Pellicano, M.; Nef, H.; Tebaldi, M.; Murasato, Y.; Lansky, A.; et al. Diagnostic Accuracy of Fast Computational Approaches to Derive Fractional Flow Reserve From Diagnostic Coronary Angiography. JACC: Cardiovascular Interventions 2016, 9, 2024–2035. [CrossRef]
- Oxford Acute Myocardial Infarction (OXAMI) Study Investigators; De Maria, G.L.; Scarsini, R.; Shanmuganathan, M.; Kotronias, R.A.; Terentes-Printzios, D.; Borlotti, A.; Langrish, J.P.; Lucking, A.J.; Choudhury, R.P.; et al. Angiography-Derived Index of Microcirculatory Resistance as a Novel, Pressure-Wire-Free Tool to Assess Coronary Microcirculation in ST Elevation Myocardial Infarction. Int J Cardiovasc Imaging 2020, 36, 1395–1406. [CrossRef]
- Fernández-Peregrina, E.; Garcia-Garcia, H.M.; Sans-Rosello, J.; Sanz-Sanchez, J.; Kotronias, R.; Scarsini, R.; Echavarria-Pinto, M.; Tebaldi, M.; De Maria, G.L. Angiography-derived versus Invasively-determined Index of Microcirculatory Resistance in the Assessment of Coronary Microcirculation: A Systematic Review and Meta-analysis. Cathet Cardio Intervent 2022, 99, 2018–2025. [CrossRef]
- Parwani, P.; Kang, N.; Safaeipour, M.; Mamas, M.A.; Wei, J.; Gulati, M.; Naidu, S.S.; Merz, N.B. Contemporary Diagnosis and Management of Patients with MINOCA. Curr Cardiol Rep 2023, 25, 561–570. [CrossRef]
- Abreu, J.S.D.; Rocha, E.A.; Machado, I.S.; Parahyba, I.O.; Rocha, T.B.; Paes, F.J.V.N.; Diogenes, T.C.P.; Abreu, M.E.B.D.; Farias, A.G.L.P.; Carneiro, M.M.; et al. Prognostic Value of Coronary Flow Reserve Obtained on Dobutamine Stress Echocardiography and Its Correlation with Target Heart Rate. Arquivos Brasileiros de Cardiologia 2017. [CrossRef]
- Simova, I.; National Cardiology Hospital, Sofia, Bulgaria Coronary Flow Velocity Reserve Assessment with Transthoracic Doppler Echocardiography. European Cardiology Review 2015, 10, 12. [CrossRef]
- Almeida, A.G. MINOCA and INOCA: Role in Heart Failure. Curr Heart Fail Rep 2023, 20, 139–150. [CrossRef]
- Garcia, D.; Harbaoui, B.; Van De Hoef, T.P.; Meuwissen, M.; Nijjer, S.S.; Echavarria-Pinto, M.; Davies, J.E.; Piek, J.J.; Lantelme, P. Relationship between FFR, CFR and Coronary Microvascular Resistance – Practical Implications for FFR-Guided Percutaneous Coronary Intervention. PLoS ONE 2019, 14, e0208612. [CrossRef]
- Dikic, A.D.; Dedic, S.; Jovanovic, I.; Boskovic, N.; Giga, V.; Nedeljkovic, I.; Tesic, M.; Aleksandric, S.; Cortigiani, L.; Ciampi, Q.; et al. Noninvasive Evaluation of Dynamic Microvascular Dysfunction in Ischemia and No Obstructive Coronary Artery Disease Patients with Suspected Vasospasm. Journal of Cardiovascular Medicine 2023. [CrossRef]
- Dwivedi, G.; Janardhanan, R.; Hayat, S.A.; Lim, T.K.; Greaves, K.; Senior, R. Relationship between Myocardial Perfusion with Myocardial Contrast Echocardiography and Function Early after Acute Myocardial Infarction for the Prediction of Late Recovery of Function. International Journal of Cardiology 2010, 140, 169–174. [CrossRef]
- Galiuto, L.; Garramone, B.; Scarà, A.; Rebuzzi, A.G.; Crea, F.; La Torre, G.; Funaro, S.; Madonna, M.; Fedele, F.; Agati, L. The Extent of Microvascular Damage During Myocardial Contrast Echocardiography Is Superior to Other Known Indexes of Post-Infarct Reperfusion in Predicting Left Ventricular Remodeling. Journal of the American College of Cardiology 2008, 51, 552–559. [CrossRef]
- Abdelmoneim, S.S.; Dhoble, A.; Bernier, M.; Erwin, P.J.; Korosoglou, G.; Senior, R.; Moir, S.; Kowatsch, I.; Xian-Hong, S.; Muro, T.; et al. Quantitative Myocardial Contrast Echocardiography during Pharmacological Stress for Diagnosis of Coronary Artery Disease: A Systematic Review and Meta-Analysis of Diagnostic Accuracy Studies. European Heart Journal - Cardiovascular Imaging 2009, 10, 813–825. [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation. Journal of the American College of Cardiology 2018, 72, 3158–3176. [CrossRef]
- Herling De Oliveira, L.L.; Correia, V.M.; Nicz, P.F.G.; Soares, P.R.; Scudeler, T.L. MINOCA: One Size Fits All? Probably Not—A Review of Etiology, Investigation, and Treatment. JCM 2022, 11, 5497. [CrossRef]
- Lubbers, D.D.; Janssen, C.H.C.; Kuijpers, D.; Van Dijkman, P.R.M.; Overbosch, J.; Willems, T.P.; Oudkerk, M. The Additional Value of First Pass Myocardial Perfusion Imaging during Peak Dose of Dobutamine Stress Cardiac MRI for the Detection of Myocardial Ischemia. Int J Cardiovasc Imaging 2008, 24, 69–76. [CrossRef]
- Tonet, E.; Pompei, G.; Faragasso, E.; Cossu, A.; Pavasini, R.; Passarini, G.; Tebaldi, M.; Campo, G. Coronary Microvascular Dysfunction: PET, CMR and CT Assessment. JCM 2021, 10, 1848. [CrossRef]
- Adjedj, J.; Picard, F.; Durand-Viel, G.; Sigal-Cinqualbre, A.; Daou, D.; Diebold, B.; Varenne, O. Coronary Microcirculation in Acute Myocardial Ischaemia: From Non-Invasive to Invasive Absolute Flow Assessment. Archives of Cardiovascular Diseases 2018, 111, 306–315. [CrossRef]
- Mayala, H.A.; Yan, W.; Jing, H.; Shuang-ye, L.; Gui-wen, Y.; Chun-xia, Q.; Ya, W.; Xiao-li, L.; Zhao-hui, W. Clinical Characteristics and Biomarkers of Coronary Microvascular Dysfunction and Obstructive Coronary Artery Disease. J Int Med Res 2019, 47, 6149–6159. [CrossRef]
- Flores, C.H.; Díez-Delhoyo, F.; Sanz-Ruiz, R.; Vázquez-Álvarez, M.E.; Tamargo Delpon, M.; Soriano Triguero, J.; Elízaga Corrales, J.; Fernández-Avilés, F.; Gutiérrez Ibañes, E. Microvascular Dysfunction of the Non-Culprit Circulation Predicts Poor Prognosis in Patients with ST-Segment Elevation Myocardial Infarction. IJC Heart & Vasculature 2022, 39, 100997. [CrossRef]
- Taqueti, V.R.; Solomon, S.D.; Shah, A.M.; Desai, A.S.; Groarke, J.D.; Osborne, M.T.; Hainer, J.; Bibbo, C.F.; Dorbala, S.; Blankstein, R.; et al. Coronary Microvascular Dysfunction and Future Risk of Heart Failure with Preserved Ejection Fraction. European Heart Journal 2018, 39, 840–849. [CrossRef]
- Henriques, J.P.S.; Zijlstra, F.; Van ‘T Hof, A.W.J.; De Boer, M.-J.; Dambrink, J.-H.E.; Gosselink, M.; Hoorntje, J.C.A.; Suryapranata, H. Angiographic Assessment of Reperfusion in Acute Myocardial Infarction by Myocardial Blush Grade. Circulation 2003, 107, 2115–2119. [CrossRef]
- Taqueti, V.R.; Shaw, L.J.; Cook, N.R.; Murthy, V.L.; Shah, N.R.; Foster, C.R.; Hainer, J.; Blankstein, R.; Dorbala, S.; Di Carli, M.F. Excess Cardiovascular Risk in Women Relative to Men Referred for Coronary Angiography Is Associated With Severely Impaired Coronary Flow Reserve, Not Obstructive Disease. Circulation 2017, 135, 566–577. [CrossRef]
- Ćorović, A.; Nus, M.; Mallat, Z.; Rudd, J.H.F.; Tarkin, J.M. PET Imaging of Post-Infarct Myocardial Inflammation. Curr Cardiol Rep 2021, 23, 99. [CrossRef]
- De Waha, S.; Patel, M.R.; Granger, C.B.; Ohman, E.M.; Maehara, A.; Eitel, I.; Ben-Yehuda, O.; Jenkins, P.; Thiele, H.; Stone, G.W. Relationship between Microvascular Obstruction and Adverse Events Following Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction: An Individual Patient Data Pooled Analysis from Seven Randomized Trials. European Heart Journal 2017, 38, 3502–3510. [CrossRef]
- Hamirani, Y.S.; Wong, A.; Kramer, C.M.; Salerno, M. Effect of Microvascular Obstruction and Intramyocardial Hemorrhage by CMR on LV Remodeling and Outcomes After Myocardial Infarction. JACC: Cardiovascular Imaging 2014, 7, 940–952. [CrossRef]
- Symons, R.; Pontone, G.; Schwitter, J.; Francone, M.; Iglesias, J.F.; Barison, A.; Zalewski, J.; De Luca, L.; Degrauwe, S.; Claus, P.; et al. Long-Term Incremental Prognostic Value of Cardiovascular Magnetic Resonance After ST-Segment Elevation Myocardial Infarction. JACC: Cardiovascular Imaging 2018, 11, 813–825. [CrossRef]
- Atkins, T.; Freidoonimehr, N.; Beltrame, J.; Zeitz, C.; Arjomandi, M. The Impact of the Microvascular Resistance on the Measures of Stenosis Severity. Journal of Biomechanics 2024, 176, 112353. [CrossRef]
- Sun, W.; Sun, L.; Yang, F.; Zhao, X.; Cai, R.; Yuan, W. Evaluation of Myocardial Viability in Myocardial Infarction Patients by Magnetic Resonance Perfusion and Delayed Enhancement Imaging. Herz 2019, 44, 735–742. [CrossRef]
- Demirkiran, A.; Robbers, L.F.H.J.; Van Der Hoeven, N.W.; Everaars, H.; Hopman, L.H.G.A.; Janssens, G.N.; Berkhof, H.J.; Lemkes, J.S.; Van De Bovenkamp, A.A.; Van Leeuwen, M.A.H.; et al. The Dynamic Relationship Between Invasive Microvascular Function and Microvascular Injury Indicators, and Their Association With Left Ventricular Function and Infarct Size at 1-Month After Reperfused ST-Segment–Elevation Myocardial Infarction. Circ: Cardiovascular Interventions 2022, 15, 892–902. [CrossRef]
- Westman, P.C.; Lipinski, M.J.; Luger, D.; Waksman, R.; Bonow, R.O.; Wu, E.; Epstein, S.E. Inflammation as a Driver of Adverse Left Ventricular Remodeling After Acute Myocardial Infarction. Journal of the American College of Cardiology 2016, 67, 2050–2060. [CrossRef]
- Dorbala, S.; Di Carli, M.F. Cardiac PET Perfusion: Prognosis, Risk Stratification, and Clinical Management. Seminars in Nuclear Medicine 2014, 44, 344–357. [CrossRef]
- Rischpler, C.; Dirschinger, R.J.; Nekolla, S.G.; Kossmann, H.; Nicolosi, S.; Hanus, F.; Van Marwick, S.; Kunze, K.P.; Meinicke, A.; Götze, K.; et al. Prospective Evaluation of18 F-Fluorodeoxyglucose Uptake in Postischemic Myocardium by Simultaneous Positron Emission Tomography/Magnetic Resonance Imaging as a Prognostic Marker of Functional Outcome. Circ: Cardiovascular Imaging 2016, 9. [CrossRef]
- Vera Cruz, P.; Palmes, P.; Bacalangco, N. Prognostic Value of Myocardial Blush Grade in ST-Elevation MI: A Systematic Review and Meta-Analysis. Interv Cardiol 2022, 17, e10. [CrossRef]
- Li, Y.; Yu, J.; Wang, Y. Mechanism of Coronary Microcirculation Obstruction after Acute Myocardial Infarction and Cardioprotective Strategies. Rev. Cardiovasc. Med. 2024, 25, 367. [CrossRef]
- M.G. Kaya; F. Arslan; A. Abaci; G. van der Heijden; T. Timurkaynak; A. Cengel Myocardial Blush Grade: A Predictor for Major Adverse Cardiac Events after Primary PTCA with Stent Implantation for Acute Myocardial Infarction. Acta Cardiologica 2007, 445–451. [CrossRef]
- Wang, D.; Li, X.; Feng, W.; Zhou, H.; Peng, W.; Wang, X. Diagnostic and Prognostic Value of Angiography-Derived Index of Microvascular Resistance: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2024, 11, 1360648. [CrossRef]
- Geng, Y.; Wu, X.; Liu, H.; Zheng, D.; Xia, L. Index of Microcirculatory Resistance: State-of-the-Art and Potential Applications in Computational Simulation of Coronary Artery Disease. J. Zhejiang Univ. Sci. B 2022, 23, 123–140. [CrossRef]
- Mahmoudi Hamidabad, N.; Kanaji, Y.; Ozcan, I.; Sara, J.D.S.; Ahmad, A.; Lerman, L.O.; Lerman, A. Prognostic Implications of Resistive Reserve Ratio in Patients With Nonobstructive Coronary Artery Disease With Myocardial Bridging. JAHA 2024, 13, e035000. [CrossRef]
- Eerdekens, R.; El Farissi, M.; De Maria, G.L.; Van Royen, N.; Van ‘T Veer, M.; Van Leeuwen, M.A.H.; Hoole, S.P.; Marin, F.; Carrick, D.; Tonino, P.A.L.; et al. Prognostic Value of Microvascular Resistance Reserve After Percutaneous Coronary Intervention in Patients With Myocardial Infarction. Journal of the American College of Cardiology 2024, 83, 2066–2076. [CrossRef]
- Milasinovic, D.; Nedeljkovic, O.; Maksimovic, R.; Sobic-Saranovic, D.; Dukic, D.; Zobenica, V.; Jelic, D.; Zivkovic, M.; Dedovic, V.; Stankovic, S.; et al. Coronary Microcirculation: The Next Frontier in the Management of STEMI. JCM 2023, 12, 1602. [CrossRef]
- Nolte, F.; Hoef, T.P. van de; Meuwissen, M.; Voskuil, M.; Chamuleau, S.; Henriques, J.P.S.; Verberne, H.J.; Eck-Smit, B.L.F. van; Koch, K.; Winter, R. de; et al. Increased Hyperaemic Coronary Microvascular Resistance Adds to the Presence of Myocardial Ischaemia Available online: https://eurointervention.pcronline.com/article/increased-hyperaemic-coronary-microvascular-resistance-adds-to-the-presence-of-myocardial-ischaemia (accessed on 1 February 2025).
- Zhang, Y.; Pu, J.; Niu, T.; Fang, J.; Chen, D.; Yidilisi, A.; Zheng, Y.; Lu, J.; Hu, Y.; Koo, B.-K.; et al. Prognostic Value of Coronary Angiography–Derived Index of Microcirculatory Resistance in Non–ST-Segment Elevation Myocardial Infarction Patients. JACC: Cardiovascular Interventions 2024, 17, 1874–1886. [CrossRef]
- Rinaldi, R.; Salzillo, C.; Caffè, A.; Montone, R.A. Invasive Functional Coronary Assessment in Myocardial Ischemia with Non-Obstructive Coronary Arteries: From Pathophysiological Mechanisms to Clinical Implications. Rev. Cardiovasc. Med. 2022, 23, 371. [CrossRef]
- Gdowski, M.A.; Murthy, V.L.; Doering, M.; Monroy-Gonzalez, A.G.; Slart, R.; Brown, D.L. Association of Isolated Coronary Microvascular Dysfunction With Mortality and Major Adverse Cardiac Events: A Systematic Review and Meta-Analysis of Aggregate Data. JAHA 2020, 9, e014954. [CrossRef]
- Jensen, S.M.; Prescott, E.I.B.; Abdulla, J. The Prognostic Value of Coronary Flow Reserve in Patients with Non-Obstructive Coronary Artery Disease and Microvascular Dysfunction: A Systematic Review and Meta-Analysis with Focus on Imaging Modality and Sex Difference. Int J Cardiovasc Imaging 2023, 39, 2545–2556. [CrossRef]
- Montisci, R.; Marchetti, M.F.; Ruscazio, M.; Biddau, M.; Secchi, S.; Zedda, N.; Casula, R.; Tuveri, F.; Kerkhof, P.L.; Meloni, L.; et al. Non-Invasive Coronary Flow Velocity Reserve Assessment Predicts Adverse Outcome in Women with Unstable Angina without Obstructive Coronary Artery Stenosis. Journal of Public Health Research 2023, 12, 22799036231181716. [CrossRef]
- Sadauskiene, E.; Zakarkaite, D.; Ryliskyte, L.; Celutkiene, J.; Rudys, A.; Aidietiene, S.; Laucevicius, A. Non-Invasive Evaluation of Myocardial Reperfusion by Transthoracic Doppler Echocardiography and Single-Photon Emission Computed Tomography in Patients with Anterior Acute Myocardial Infarction. Cardiovasc Ultrasound 2011, 9, 16. [CrossRef]
- Schröder, R. Prognostic Impact of Early ST-Segment Resolution in Acute ST-Elevation Myocardial Infarction. Circulation 2004, 110. [CrossRef]
- Nijveldt, R.; Van Der Vleuten, P.A.; Hirsch, A.; Beek, A.M.; Tio, R.A.; Tijssen, J.G.P.; Piek, J.J.; Van Rossum, A.C.; Zijlstra, F. Early Electrocardiographic Findings and MR Imaging-Verified Microvascular Injury and Myocardial Infarct Size. JACC: Cardiovascular Imaging 2009, 2, 1187–1194. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



