Submitted:
17 February 2025
Posted:
18 February 2025
You are already at the latest version
Abstract
Background/Objectives: Three-dimensional (3D) printing is transforming dentistry by enabling precise and personalized treatments in prosthodontics, orthodontics, and en-dodontics. However, challenges such as high costs, material limitations, and post-processing requirements hinder its broader adoption. This review evaluates the clinical applications, benefits, and limitations of 3D printing in these disciplines. Methods: A narrative review was conducted using literature from PubMed, Google Scholar, and Scopus, covering studies from January 2006 to November 2024. Key top-ics included applications, material properties, and technological challenges in pros-thodontics, orthodontics, and endodontics. Results: In prosthodontics, 3D printing fa-cilitates the fabrication of crowns, bridges, and dentures with high accuracy, though material strength and stability remain challenges. Orthodontics benefits from 3D-printed aligners and diagnostic models, improving patient comfort and treatment precision, but issues with material durability persist. In endodontics, 3D-printed sur-gical guides and training models enhance procedural accuracy and educational out-comes. Across disciplines, 3D printing reduces production time and enhances custom-ization but incurs high costs and requires significant post-processing. Conclusions: 3D printing has revolutionized dental care by improving precision, efficiency, and patient satisfaction. However, material and cost-related barriers limit its widespread clinical use. Ongoing research and technological advancements are essential to address these challenges, improve material properties, and reduce costs, paving the way for broader applications and better patient outcomes in personalized dental care.
Keywords:
three-dimensional printing
; 3D printing
; dental prosthodontics
; 3D-printed aligners
; 3D-printed guide
1. Introduction
Recent advancements in 3D printing technology within the dentistry filed have catalyzed transformative innovations across a wide range of treatment methodologies [1]. In particular, the integration of 3D printing in prosthodontics, orthodontics, and endodontics has significantly enhanced the precision and efficiency of treatments [2,3,4]. 3D printing offers clinically numerous advantages, including increased patient satisfaction and reduced production time [5]. Consequently, there is an increasing necessity for more comprehensive analysis in research on the clinical applications of 3D printing technology.
3D printing technology is emerging as an innovative approach that provides customized solutions in the field of dentistry [6]. Traditional dental treatments have limitations in offering patient-specific, optimized care due to various constraints [7]. However, the advancement of digital technology alongside 3D printing opens possibilities to overcome these limitations.
Traditional methods often involve extended production times for prosthetics or orthodontic appliances, which may result in prolonged discomfort for patients [1]. Patients may need multiple visits to complete the desired treatment, further compounding their discomfort. Additionally, prosthetics produced manually by technicians tend to increase overall treatment costs due to labor and production expenses, potentially limiting accessibility for some patients [2]. 3D printing technology enables personalized treatment by generating precisely designed prosthetics or orthodontic devices tailored to the patient’s tooth and periodontal tissue [6]. This contributes to maximizing treatment outcomes. Through 3D printing, digital scan-based modeling and manufacturing are achieved, minimizing human error and significantly reducing production time [5]. Such precision can directly enhance patient safety and treatment effectiveness.
Various 3D-printable materials play a crucial role in enhancing the durability and biocompatibility of dental appliances [8,9,10]. For instance, prosthetics made with recent innovations in biocompatible metals or high-performance polymers have been effectively developed, contributing to improved treatment outcomes by minimizing contaminants.
3D printing has the potential to simplify and automate production processes, reducing labor and material costs, which can greatly enhance the efficiency of dental practice operations [11]. Cost reduction in treatments directly affecting patients is a crucial factor in improving dental treatment accessibility.
Despite these advantages, 3D printing technology faces several challenges, such as the cost of technical equipment, maintenance expenses, and surface finishing techniques [12]. Firstly, the initial purchase cost of 3D printers is considerably high [13,14]. Moreover, maintenance and material costs add to the expense. This makes it challenging for privately owned dental practices to adopt this technology. Secondly, the quality of printed products varies significantly depending on the materials used and the printing technology [15,16]. Although it allows for design, incorrect settings or substandard materials may lead to unsatisfactory results. Furthermore, additional surface finishing steps are often required to improve the quality of the final product [17]. Printed products frequently require post-processing, including surface finishing, minor adjustments, and sterilization, which add time and effort to the process. Nevertheless, continuous research and technological development should aim to overcome the limitations of 3D printing and enhance personalized treatments. Such research benefits both dentists and patients. This research related to these challenges is essential for the advancement and dissemination of 3D printing technology, providing an important foundation for its broader application in clinical settings.
3D printing has rapidly transformed dental practice by offering precise and personalized solutions in prosthodontics, orthodontics, and endodontics. However, existing research often focuses on isolated applications or narrow subfields, leaving a fragmented understanding of the broader landscape. Traditional systematic reviews, while valuable, typically address specific research questions or outcomes and may overlook emerging trends, diverse applications, or interdisciplinary challenges. In contrast, a scoping review provides a flexible and broad approach, making it possible to gather and organize information from various areas of research. This method helps to map out what is currently known, identify gaps where more research is needed, and point to key areas for future studies. By offering a clear and comprehensive picture, this scoping review aims to support both clinical applications and future investigations, giving a better understanding of how 3D printing is being used and evolving in modern dentistry.
The objective of this scoping review is to explore and map the breadth of evidence regarding the clinical applications, advantages, and challenges of 3D printing in dentistry. By synthesizing findings across prosthodontics, orthodontics, and endodontics, this review aims to provide an overview of current advancements, identify gaps in existing knowledge, and highlight opportunities for future research.
2. Materials and Methods
2.1. Protocol and Search Strategy
This scoping review was conducted following the PRISMA for scoping review guidelines to ensure methodological rigor and transparency. A review protocol was developed prior to the initiation of the study but was not formally registered in an external database. Should the journal or reviewers require access to the protocol, it can be provided upon request. This narrative review examines how 3D printing technology is utilized across the fields of dental prosthodontics, orthodontics, and endodontics. By analyzing recent literature, this study aims to evaluate clinical applications, advantages, material properties, and technical challenges. The study methodology includes identifying relevant research, defining inclusion and exclusion criteria, selecting studies, extracting relevant data, and summarizing the results. The literature search was conducted using major databases such as PubMed, Google Scholar, and Scopus, employing relevant MeSH terms and keywords. The search period covered publications from January 2006 to November 2024. The final search was conducted on November 15, 2024. Common search keywords included "3D printing" or “three-dimensional printing” and “dentistry” or “dental” and “prosthodontics” or “orthodontics” or “endodontics”
For the field of dental prosthodontics, search keywords were defined as follows: "Prosthodontics," “3d-printed fixed prosthesis,” “Prosthesis,” " "Denture," "Removable Dental Prostheses," "Removable Denture," “3d-printed dentures,” "Complete Denture," "Dental implants," and "Crowns and bridges."
For orthodontics, the keywords included: "Orthodontics," "Dental aligners," "braces," "Clear aligners," “3d-printed dental aligner,” “3d-printed clear aligner,” “mouthguard,” “3d-printed indirect bonding tray,” “3d-printed orthodontic model,” “3d-printed surgical splint,” "Digital orthodontics," and "Orthodontic treatment."
For the field of endodontics, search keywords included: "Endodontics," "clinical endodontic applications," “3d-printed guide,” "endodontic surgical guide," "guided endodontic surgery," “3d-guided endodontic surgery,” "guided endodontic access," and "guided endodontic autotransplantation." “3d-printed root canal model,” “3d-printed model,”
2.2. Literature Selection and Eligibiltiy Criteria
The literature selection process involved reviewing titles and abstracts to identify studies evaluating the use of 3D printing in dental clinical procedures, encompassing fields such as prosthodontics, orthodontics, and endodontics. For articles meeting the inclusion criteria, a thorough full-text review was conducted. Data extraction was performed independently by two reviewers (MK, JW). In cases of disagreement, the reviewers engaged in discussion to reach a consensus. When necessary, a corresponding reviewer [18] was consulted to make the final decision. The quality of the chosen articles was assessed based on qualitative evaluation criteria, and comparisons were made regarding each study’s design, applied technology, and validity of results.
2.2.1. Inclusion Criteria
This narrative review included original research studies, systematic reviews, and meta-analyses published in peer-reviewed journals between 2006 and 2024. Only studies focusing on the technique, applications, materials (e.g., polymers, ceramics, biocompatible metals), or limitations of 3D printing in dentistry were considered.
2.2.2. Exclusion Criteria
Articles not primarily centered on 3D printing or lacking sufficient methodological detail were excluded. Studies were excluded if they were narrative reviews, not peer-reviewed, lacked sufficient methodological detail, were not published in English, or focused on non-dental applications of 3D printing. Additionally, studies published before 2006 or containing duplicate data were excluded to ensure relevance and quality
2.3. Data Analysis
The data analysis for this narrative review was conducted through a comprehensive examination of the selected literature. The process involved the following steps:
- Categorization: The selected studies were categorized into three main dental specialties: prosthodontics, orthodontics, and endodontics. This classification allowed for a structured analysis of 3D printing applications in each field.
- Thematic Analysis: Within each specialty, key themes were identified, including: Clinical applications of 3D printing, Advantages and limitations of 3D printing techniques, Comparison with traditional methods, Material properties and their impact on outcomes
- Comparative Assessment: Where available, comparative data between 3D printing and other manufacturing methods (e.g., milling, traditional casting) were analyzed. This included: Accuracy and precision of fabricated products, Mechanical properties of materials used, Time efficiency in production, Cost-effectiveness
- Technological Evaluation: The analysis included an assessment of different 3D printing technologies used in dentistry, such as Stereolithography (SLA) and Digital Light Processing (DLP), focusing on their specific advantages and limitations in dental applications.
- Clinical Relevance: The clinical significance of findings from various studies was evaluated, particularly in terms of the applicability and effectiveness of 3D-printed dental products in real-world clinical settings.
- Quality Assessment: The quality of evidence presented in each study was assessed, considering factors such as study design, sample size, and methodological rigor
- Synthesis of Findings: The analyzed data were synthesized to form comprehensive conclusions about the current state and future potential of 3D printing in dentistry, highlighting both its promising aspects and areas needing further research and development.
This multi-faceted analysis approach enabled a thorough examination of the current landscape of 3D printing in dentistry, providing insights into its clinical applications, technological advancements, and future prospects across different dental specialties
3. Results and Discussion
3.1. Study Selection
The review process diagram is shown in Figure 1. 3D printing technology is utilized across various specialties in the dental field, with dental milling technology also playing a prominent role alongside 3D printing [19]. Dental milling technique, a popular technique, employs CAD/CAM systems and is widely adopted in clinical dental practices. Numerous previous studies have compared the accuracy and strength of 3D printing and milling technologies [20,21,22]. The foundational principle of 3D printing involves additive manufacturing, where materials are layered sequentially to form the desired shape, allowing the use of diverse materials such as plastics, metals, and ceramics [23]. In contrast, milling operates on a subtractive manufacturing basis, in which solid blocks of material are carved into the desired shape using cutting tools, typically utilizing harder materials like metals and ceramics [24]. The advantages of 3D printing include the ability to easily produce complex structures and reduce material waste by manufacturing only the necessary portions [25]. However, limitations include longer production times compared to milling for large-scale manufacturing and potentially lower strength [26]. Milling technology, on the other hand, offers high precision and superior strength, making it highly durable. Its disadvantages include material waste from the subtractive process and challenges in creating intricate internal structures [27]. In dental applications, 3D printing and milling technologies play complementary roles, and selecting the appropriate technology based on the treatment objective is essential.
Notable 3D printing techniques in dentistry include Stereolithography (SLA) and Digital Light Processing (DLP) [28]. The SLA technique operates by using a laser to selectively cure liquid polymer resin, building the model layer by layer. Following printing, a post-curing process using UV light is required [8]. While SLA offers the advantage of high resolution, it also has the drawback of requiring additional post-processing, which can extend production time. In contrast, DLP cures each layer simultaneously with projected light, enabling the entire layer to be cured at once [29]. While DLP has a limited build volume, posing challenges for larger parts, it offers faster print times than SLA, making it suitable for mass production. In the dental field, SLA is preferred for tasks that require detailed, high-resolution work.
3.2. 3D Printing Techniques in Prosthetic Dentistry
The methods of using 3D printers in each dentistry field are presented in Table 1. In prosthetic dentistry, 3D printing technology is currently employed for a range of applications, including the fabrication of prostheses (e.g., zirconia crowns, Co-Cr copings, and bridge crowns), surgical guides for dental implants, and complete and partial dentures [2,30,31].
Study comparing traditional casting methods with 3D printing techniques (No information about 3d printing type) for prosthesis fabrication indicate that, for maxillary molar crowns, crowns produced via casting achieved the smallest marginal gaps [30]. However, several studies report no significant differences between 3D printing (SLA and DLP type) and milling in terms of accuracy, with both methods providing clinically acceptable results [31,32,33,34,35,36]. When fabricating fixed prostheses, metal copings produced by 3D printing (DLP type, SLM type; Selective Laser Melting, polyjet type) exhibited better marginal fit than those produced by milling [37,38,39].
While there is limited clinical research evaluating the effectiveness of 3D-printed metal-ceramic crowns (SLM type), one study reported that the crown retention force were not yet satisfactory for clinical application [40]. Nonetheless, with further technological advancements, clinical use of 3D-printed metal-ceramic crowns may become feasible because better internal and marginal fit.
Selective Laser Melting (SLM) and Stereolithography (SLA) are two distinct 3D printing technologies with significant differences in their mechanisms, materials, and applications. SLM, primarily used for metal fabrication, employs a high-power laser to selectively melt and fuse metal powder particles, building the object layer by layer [41,42]. This technique is particularly suitable for creating complex metal structures in dentistry, such as metal coping and metal framework. In contrast, SLA utilizes a laser to cure and solidify liquid photopolymer resin, producing highly detailed plastic parts [43]. SLA is widely used in dentistry for creating diagnostic models, surgical guides, and some temporary prosthetics due to its high resolution and smooth surface finish. While SLM offers the advantage of producing functional metal parts with high strength, it typically requires post-processing and can be more time-consuming [41]. SLA, on the other hand, provides faster printing speeds for smaller objects and requires post-curing but is limited to photopolymer materials. The choice between these technologies in dental applications depends on the specific requirements of the final product, such as material properties, precision, and intended use.
In denture and denture base production, achieving precise fit between the denture base and underlying mucosal tissue is crucial for successful retention. Comparative studies on the surface adaptation of dentures fabricated via 3D printing (SLA, DLP and polyjet type) versus traditional manual methods reported no significant difference [44,45]. However, 3D-printed dentures (SLA type) showed a decrease in dimensional stability over time and in color stability, with milling yielding superior results in this regard [46,47,48]. Although deformation of 3D-printed dentures over time has been observed, the clinical significance of these changes has yet to be evaluated. In terms of mechanical properties, the strength of 3D-printed denture materials (DLP type) remains lower than that of materials fabricated through milling or traditional methods, primarily due to weaker interlayer bonding and strength variation based on build orientation [49,50,51].
Despite the growing adoption of 3D printing in prosthodontics, significant advancements are required in four key areas before it can fully replace milling machines: material properties, surface quality, speed and cost efficiency, and workflow standardization.
Firstly, 3D printing materials currently lag behind milling materials in strength, durability, and biocompatibility required for dental applications. Further research is needed to develop new high-performance photocurable resins and composite materials that can match or exceed the properties of milled prosthetics.
Secondly, 3D printing must achieve the precision and smooth surface finish comparable to milling. The technology needs to provide clinically acceptable surface quality without requiring additional polishing or coating processes, thereby reducing post-processing steps.
Thirdly, reproducibility is crucial. There is a need to develop processes that ensure consistent results under identical conditions. This includes seamless integration between CAD software and 3D printing technology through standardization.
Addressing these challenges will be essential for 3D printing to become a viable alternative to milling in prosthodontics. Future research should focus on enhancing material properties, improving surface quality, increasing speed and cost-effectiveness, and standardizing workflows to fully realize the potential of 3D printing in dental applications.
In conclusion, while 3D printing technology achieves clinically acceptable levels of accuracy, it currently exhibits lower mechanical strength and stability compared to milling and traditional methods, highlighting areas for future improvement.
3.3. 3D Printing in Orthodontic Dentistry
3D printing technology has ushered in significant innovations within orthodontic dentistry, playing a crucial role in generating precise digital dental models and enabling the development of custom orthodontic appliances and treatment plans. Applications of 3D printing in orthodontics include customized clear aligners, dental aligner molds, 3d-printed orthodontic models, mouth guards, 3D-printed indirect bonding trays, retainers, and 3D-printed surgical splints [52,53,54].
The popularity of 3D-printed aligners among both clinicians and patients is primarily due to their aesthetic aspect and functionality [55]. When fabricated with transparent resins, they demonstrate high biocompatibility, minimal deformation, and long-term stability. Traditional metal brackets tend to irritate the oral mucosa, often causing abrasions; in contrast, 3D-printed aligners provide a smoother experience, significantly reducing discomfort for patients [56]. This meticulous production approach has been favorably assessed for its enhanced adaptability and wearability [56]. Generally, the process involves scanning the patient’s teeth, designing the aligner using CAD software, and fabricating it via high-resolution 3D printing techniques such as SLA and DLP. Two studies have noted that certain materials may develop minor fractures or undergo physical property changes during use. [57,58] A study comparing the accuracy of clear aligners produced with different 3D printing technologies found that models fabricated using SLA printing exhibited significantly lower trueness errors than those created with DLP printers [59]. Another study also indicates that SLA technology yields more precise clear aligners compared to DLP and LCD technologies, with the color-coded map showing that trueness errors primarily affect the occlusal and proximal surfaces of teeth [60]. Recent studies also explore advanced polymer and composite materials for these devices, aiming to refine the elastic properties of aligners in response to tooth movement [61]. Resin-based 3D-printed aligners, when appropriately cured, have been reported to achieve high accuracy, potentially offering greater mechanical strength and elasticity than traditional thermoplastic-based thermoformed clear aligners while also reducing production time [55] . Compared to traditional aligner fabrication, 3D printing streamlines the entire design, production, and inspection workflow through digitalization, significantly reducing overall production time. Some studies have reported that 3D-printed aligners improve productivity by 40-60% over traditional manufacturing methods [56]. It is anticipated that further advancements in material science and printing technologies will be essential to resolve these issues. Furthermore, comprehensive long-term clinical studies involving larger patient populations are necessary to substantiate the efficacy and clinical viability of 3D-printed orthodontic devices.
The utilization of 3D printing in orthodontics has enabled the production of highly precise and customized aligners. The use of 3D printing extends beyond the production of orthodontic aligners; it is also employed in the fabrication of molds suitable for aligner manufacturing. Several prominent companies dominate this field by integrating advanced 3D printing technologies into their manufacturing processes. First, Align Technology (San Jose, California, USA), the creator of Invisalign, is a global leader in the orthodontic aligner market [62]. The company employs SLA and DLP technologies to produce molds for aligners [63,64]. These molds are subsequently used to thermoform aligners made from thermoplastic polyurethane (TPU) [63]. Second, ClearCorrect (Basel, Switzerland), owned by Straumann Group, employs SLA-based 3D printers for creating detailed and precise aligner molds [65,66]. Their aligners are designed to compete with Invisalign, offering a similar level of customization and quality. ClearCorrect emphasizes affordability and flexibility for both patients and providers.
Diagnostic models for initiating orthodontic treatments and retention devices post-treatment are also fabricated using 3D printing [67]. While traditional models tend to be bulky, difficult to store, and challenging to replicate, 3D-printed cast models allow the creation of optimal tooth movement using software simulations [68]. Studies comparing traditional cast stone models with 3D-printed cast models have demonstrated that, regardless of whether the printed model is solid or hollow, the precision of the 3D printed models is inherently influenced by the printing technology employed [69]. Specifically, CLIP (Continuous Liquid Interface Production) printers showed notably lower deviations from traditional cast models than DLP printers. The CLIP and DLP technologies are both photopolymerization-based 3D printing methods, yet they exhibit significant differences in their operational principles and outcomes [69,70]. CLIP technology employs a continuous printing process, utilizing an oxygen-permeable window to create a "dead zone" between the light source and the resin. This allows for uninterrupted part growth without discrete layering [70]. In contrast, DLP operates on a layer-by-layer basis, necessitating a peel step between each layer, which can significantly impact printing speed. While CLIP technology offers significant advantages over DLP in terms of printing speed and surface quality, it currently faces limitations in build volume and remains dependent on underlying DLP principles. This dichotomy presents both opportunities and challenges for the advancement of additive manufacturing technologies. Another study demonstrated that DLP printing achieved clinically acceptable accuracy in measuring tooth dimensions such as mesiodistal crown width and crown height, potentially making 3D-printed models a viable alternative to traditional models [71]. However, comparisons between conventional casts and models fabricated with PolyJet and DLP printing indicated that traditional casts exhibited lower dimensional changes over time, suggesting that while 3D-printed models showed the smallest initial change, they had slightly lower accuracy and reproducibility [52].
Orthodontic brackets and indirect bonding trays are also being produced with 3D printing, although studies on bracket applications in patient use are limited [53]. The production of indirect bonding trays through 3D printing offers increased precision by creating trays that conform closely to the tooth structures, allowing for more accurate bracket placement, improving patient comfort, and reducing procedure time for clinicians. Another study reported on the reproducibility of digital indirect bonding using 3D models and 3D-printed transfer trays [72]. The results showed no statistically significant differences in bracket positions, except for minor mesial-distal discrepancies. This study concluded that the digital indirect bonding technique using 3D-printed transfer trays demonstrates high reproducibility in bracket positioning, regardless of the orthodontist's experience level.
In orthodontics, the durability and biomechanical properties of 3D-printed aligners remain underexplored, particularly in long-term clinical scenarios. While 3D printing offers precise and customizable solutions, research on material degradation and its impact on treatment outcomes is limited. Additionally, the workflow for digital orthodontic applications lacks standardization, with few studies comparing the accuracy and efficiency of SLA and DLP technologies. Furthermore, existing research is predominantly laboratory-based, necessitating large-scale clinical trials to validate the effectiveness of 3D-printed aligners across diverse patient populations.
The introduction of 3D printing into orthodontics has facilitated customized design, cost savings, and productivity improvements, resulting in high satisfaction among both patients and clinicians. Nevertheless, further studies are needed to evaluate the durability and long-term efficacy of 3D-printed materials to strengthen clear aligners as a sturdy and effective orthodontic solution.

Table 2.
Summary of 3D printer types, research objectives, evaluation criteria, and application in orthodontics dentistry.
Table 2.
Summary of 3D printer types, research objectives, evaluation criteria, and application in orthodontics dentistry.
| Dentistry field | 3d printer type | Objective | Evaluation criteria |
Advantages | Disadvantages |
|---|---|---|---|---|---|
| Orthodontics | SLA | Fabrication of clear aligners | Aesthetics, patient comfort |
High precision for clear aligners, Biocompatible materials |
Post-processing required |
| DLP | Fabrication of diagnostic models | Reproducibility, accuracy |
Faster production of aligners,Minimal deformation | Limited size for larger appliances |
SLA= Stereolithography, DLP = Digital Light Processing.
3.3. Endodontic Application of 3D Printing in Dentistry
The integration of 3D printing technology into endodontics has significantly advanced diagnostic accuracy, treatment planning, education, and research. Currently, most studies utilizing endodontic surgical guides are limited to case reports. A prominent application is in the fabrication of endodontic surgical guide for procedures such as apicoectomy, where 3D-printed guides assist in precisely positioning surgical instruments, enabling the clinician to accurately access and remove periapical lesions [5]. Studies have shown that utilizing these guides increases precision in locating canal entrances and establishing access pathways, significantly reducing procedural errors compared to non-guided surgeries, regardless of the clinician’s experience level [73,74]. For challenging cases, such as calcified or complex, curved canals, 3D-printed guides have demonstrated improved accessibility and higher success rates compared to conventional hand instrumentation [75,76]. The use of these guides allows for safer procedures by minimizing unnecessary removal of tooth structure while searching for canal entrances, thus preserving tooth integrity [75,77,78]. Guided surgical endodontics employs 3D printed surgical guides designed using integrated CBCT and optical scan data to enhance precision in complex cases[79,80]. The technique utilizes guide sleeves to accurately identify osteotomy sites and control the depth and angle of access, with depth-calibrated instruments maintaining parallelism to limit osteotomy size [18]. This approach not only improves accuracy in determining osteotomy sites and root resection levels but also serves as a valuable tool for skill development in educational settings, representing a significant advancement in surgical endodontic procedures. Multiple studies indicate that 3D-guided endodontic surgery improve lesion removal accuracy and ensure a reliable canal seal, thereby reducing recurrence rates and enhancing long-term treatment outcomes [77,81,82,83]. Furthermore, patient satisfaction has been reported to increase with the use of surgical guides due to shorter procedural times and reduced discomfort [5].
While surgical guides are commonly used, non-surgical guides are also being utilized in 3D printing and can be applied for guided endodontic access, particularly in cases involving calcified canals. These guides allow clinicians to follow pre-planned drilling paths, reducing errors, preserving tooth structure, and improving the efficiency and success rates of complex procedures [73]. An ex-vivo study found that guided endodontic access cavity preparation using 3D-printed templates achieved high accuracy, with mean deviations below 0.7 mm [84]. A study on non-surgical guided endodontics in mandibular anterior teeth demonstrated high accuracy, with mean deviation 0.2 mm at the bur tip and angular deviation less than 2° [81]. The technique proved to be efficient and operator-independent, with an average treatment time of 10 minutes per tooth, suggesting its effectiveness for preparing access cavities in teeth with narrow roots.
The utilization of 3D printing to create endodontic models has proven to be a valuable tool for training and research in endodontic treatment. These models replicate complex root canal anatomies, allowing for hands-on practice in a controlled and safe environment [85]. This application enhances procedural skills and promotes a deeper understanding of endodontic techniques [86]. A study utilizing commercially available 3D-printed mandibular molar replicas compared the performance of two contemporary rotary instrumentation systems in a pre-clinical student course setting [87]. Numerous studies have highlighted the utility of 3D-printed root canal models as effective platforms for simulating and practicing procedures prior to performing actual root canal treatments in clinical settings [88,89,90]. By practicing with the model, practitioners can familiarize themselves with the specific shape and location of the root canal, allowing them to refine their choice of instruments and approach. This preparatory step has been shown to reduce the likelihood of unforeseen complications arising during the actual procedure [91]. . One study found that clinicians who practiced with these models achieved higher success rates and shorter procedure times in real cases [77,92]. Another study reported that 3D-printed root canal models serve as an essential educational tool for students and novice dental practitioners [93]. Practicing with 3D-printed models of diverse root canal anatomies enables students to deepen their understanding of complex canal structures and enhances their confidence in performing clinical procedures [94]. A study utilizing 3D-printed models of a lower first molar demonstrated high effectiveness for endodontic training, with 85% of students considering the models effective tools, significant improvements in confidence (75% after vs. 38% before), and enhanced understanding of access cavity shape (70%) and root canal anatomy visualization (83%) [94]. Furthermore, 3D-printed root canal models serve as valuable research tools for evaluating and testing the efficacy of novel instruments and materials used in endodontic treatment. These models can also be employed as visual aids during patient consultations, providing a tangible representation of the endodontic procedure and the necessity of each step. This approach enhances patient understanding and fosters greater trust and confidence in their treatment.
Table 3.
Summary of 3D printer types, research objectives, evaluation criteria, and application in endodontic dentistry.
Table 3.
Summary of 3D printer types, research objectives, evaluation criteria, and application in endodontic dentistry.
| Dentistry field | 3d printer type | Objective | Evaluation criteria |
Advantages | Disadvantages |
|---|---|---|---|---|---|
| Endodontics | SLA | Fabrication of surgical guides and anatomical models | Accuracy surgical planning support, training effectiveness |
High accuracy for surgical guides | Longer production time |
| DLP | Fabrication of endodontic training for root canals models |
Similarity to actual clinical environment |
Faster production of root canal models | Limited build volume for larger models |
|
| PolyJet | Fabrication of complex surgical guides | Accuracy, safety | Multi-material printing capability,High precision for complex anatomical models |
Higher material costs,Post-processing required |
SLA= Stereolithography, DLP = Digital Light Processing.
In the field of endodontics in dentistry, efforts are being made to utilize 3D printing technology for autotransplantation to enhance procedural accuracy and clinical outcomes [95,96,97]. The integration of 3D printing, particularly computer-aided rapid prototyping (CARP), has significantly improved the predictability and outcomes of autotransplantation by addressing challenges such as prolonged extra-oral time and periodontal ligament (PDL) damage. By enabling the preoperative preparation of recipient sites with 3D-printed replicas of donor teeth, CARP minimizes trauma and enhances surgical precision. Studies have demonstrated success rates of 80–91%, with reduced extra-oral times to under one minute in some cases [98,99,100,101]. Innovations such as CAD-designed prototypes and 3D-printed surgical guides further optimize procedures by ensuring accurate tooth positioning and preserving critical structures like the apical papilla [102]. These advancements highlight the transformative role of 3D printing in making autotransplantation a reliable and efficient treatment option.
In endodontics, guided techniques using 3D-printed templates have shown promise, but large-scale studies assessing their safety and efficacy are scarce. Another significant research gap lies in the potential advancements of 3D printing for surgical endodontic treatments, which require further exploration in future studies. First, the development of ultra-miniaturized surgical guides designed specifically to avoid obstructing the surgical field could enhance the precision of procedures while maintaining optimal visibility for clinicians. These guides would be particularly beneficial in complex apicoectomy cases or when access to posterior regions is limited. Second, designing 3D-printed, specialized tools such as spoon-shaped instruments or custom drill tips tailored to the unique anatomy of root apexes could facilitate less invasive treatment. These tools would minimize unnecessary removal of surrounding tissues, reducing post-operative complications and improving patient recovery. Lastly, the integration of 3D printing with nanotechnology presents an exciting avenue for innovation. Customizable microstructures could be developed to repair compromised root canal walls or enable drug delivery continuously. Such advancements would not only reinforce structural integrity but also promote long-term healing and prevent reinfection. These areas of research represent promising directions for leveraging 3D printing to achieve more efficient, minimally invasive, and patient-centered endodontic care.
Table 4.
Characteristics of the included 3d printing studies.
| Application | Author (Year) | Study design |
Printer technology |
Objective of study |
|---|---|---|---|---|
| Fabrication of protheses | Huang, Zhuoli et al. (2015) [34] | In vitro | SLM | To compare the marginal and internal fit of single crowns fabrication |
| Chang, Hao-Sheng et al. (2019) [30] | In vitro | No information |
To evaluate the marginal gaps of dental restorations | |
| Khaledi, Amir-Alireza et al. (2020) [37] | In vitro | SLA and Polyjet | To evaluate the marginal fit of metal copings fabrication | |
| Addugala, Hemavardhini et al. (2022) [38] | In vitro | DLP | To compare the marginal discrepancy and internal adaptation of copings fabrication | |
| Ali Majeed, Zainab et el. (2023) [39] | In vitro | SLM | To evaluate the trueness and fitness of Co-Cr crown copings fabrication | |
| Kim, Dong-Yeon et al. (2018) [41] | In vitro | SLM | To evaluate the marginal and internal gaps of Co-Cr alloy copings fabrication | |
| Qian, B et al. (2015) [42] | In vitro | SLM | To investigate the microstructure of SLM specimens and its effect on mechanical properties | |
| Goguta, Luciana et al. (2021) [40] | In vitro | SLM | To ascertain the retention forces for telescopic crowns fabricated with SLM and SLS | |
| Complete denture | Herpel, Christopher et al. (2021) [20] | In vitro | SLA and DLP |
To compare the accuracy of 3D-printed and milled complete dentures. |
| Kalberer, Nicole et al. (2019) [45] | In vivo | Prototype machine | To compare the differences in trueness of complete dentures. | |
| Gad, Marwa A et al. (2024) [46] | In vitro | SLA | To assess and contrast the color stability and dimensional accuracy of denture base resins before and after aging | |
| Helal, Mohamed Ahmed et al. (2023) [47] | In vitro | DLP | To compare the dimensional changes of complete denture | |
| Prpić, Vladimir et al. (2020) [49] | In vitro | DLP | To evaluate the mechanical properties of denture base materials | |
| Freitas, Rodrigo Falcão Carvalho Porto de et al. (2023) [50] | In vitro | DLP | To investigate the surface roughness and contact angle, anti-biofilm formation, and mechanical properties of denture base resins | |
| Zeidan, Ahmed Abd El-Latif et al. (2023) [51] | In vitro | DLP | To compare the flexural strength of the denture base resin | |
| Dental cast model | Jeong, Yoo-Geum et al. (2018) [48] | In vitro | SLA | To evaluate the accuracy of models for dental prosthesis production |
| Park, Mid-Eum et al. (2018) [52] | In vitro | Polyjet | to compare the accuracy and reproducibility of dental casts production | |
| Grassia, Vincenzo et al. (2023) [60] | In vitro | SLA and DLP | To assess the trueness and precision of orthodontic models | |
| Ellakany, Passent et al. (2022) [68] | In vitro | SLA | To compare the accuracy of dental casts | |
| Rungrojwittayakul, Oraphan et al. (2020) [69] | In vitro | CLIP and DLP | To evaluate the accuracy of 3D printed models production | |
| Brown, Gregory B et al. (2018) [71] | In vitro | DLP and Polyjet | To assess the accuracy of 2 types of 3D printing techniques. | |
| Indirect bonding tray | Bachour, Petra C et al. (2022) [53] | In vivo | DLP | To evaluate the transfer accuracy of indirect bonding trays |
| Duarte, Maria Eduarda Assad et al. (2020) [72] | In vitro | Polyjet | To evaluate the reproducibility of digital tray transfer fit on digital indirect bonding | |
| Clear dental aligners |
Jindal, Prashant et al. (2019) [55] | In vitro | SLA | To compare compressive mechanical properties and geometric inaccuracies of dental aligners |
| Venezia, Pietro et al. (2022) [59] | In vitro | SLA and DLP | To evaluate the accuracy of the production of clear aligners | |
| Willi, Andreas et al. (2023) [61] | In vitro | DLP | To quantitatively assess the degree of conversion and water-leaching compounds | |
| Šimunović, Luka et al. (2024) [65] | In vitro | SLA | To evaluate the aligners’ response to common staining agents in color and chemical stability. | |
| Pasaoglu Bozkurt, Aylin et al. (2025) [66] | In vitrp | SLA | to compare and evaluate time-dependent biofilm formation and microbial adhesion of clear aligner | |
| Surgical and non-surgical guide | Sarkarat, Farzin et al. (2023) [54] | In vivo | Polyjet | To investigate the accuracy of surgical splints for practical use |
| van der Meer, Wicher J et al. (2016) [73] | In vivo | Polyjet | To describe the application of 3D digital mapping technology for navigation of obliterated canal systems | |
| Ackerman, Shira et al. (2019) [74] | In vivo | SLA | To evaluate the accuracy of CBCT-designed surgical guides | |
| Connert, T et al. (2018) [75] | In vivo | Polyjet | To present a novel treatment for root canal localization | |
| Lara-Mendes, Sônia T de O et al. (2018) [76] | In vivo | Polyjet | to describe a guided technique for accessing root canals | |
| Connert, Thomas et al. (2019) [77] | In vitro | Polyjet | To compare endodontic access cavities in teeth with calcified root canals | |
| Loureiro, Marco Antônio Z et al. (2021) [78] | In vivo | DLP | To discuss the impact of new technologies on treating a complex case | |
| Lee, Seung-Jong et al. (2006) [79] | In vivo | Prototype machine | To demonstrate the anatomy of 3 distal roots of a right mandibular first molar | |
| Byun, Chanhee et al. (2015) [80] | In vivo | Polyjet | To present a case of successful root canal treatment | |
| Connert, Thomas et al. (2017) [81] | In vitro | Polyjet | To assess the accuracy of guided endodontics in mandibular anterior teeth | |
| Pinsky, Harold M et al. (2007) [82] | In vitro | No information | To introduce periapical surgical guidance computer-aided manufacturing surgical guides | |
| Buchgreitz, J et al. (2016) [84] | Ex vivo | No information | To evaluate the accuracy of a preparation for teeth with pulp canal obliteration | |
| Kfir, A et al. (2013) [85] | In vivo | Polyjet | To report on the use of a 3D plastic model for the diagnosis and treatment of densinvaginatus | |
| Hawkins, T K et al. (2020) [92] | In vitro | Polyjet | To compare surgical time, bevel angle and site volumetric profiles of osteotomy and resection area of endodontic microsurgery | |
| Clinical Training | Marending, M et al. (2016) [87] | In vitro | No information | To assess contemporary rotary instrumenting systems in a pre-clinical student course setting. |
| Tonini, Riccardo, et al. (2021) [89] | In vivo | No information | To evaluate the applicability of a novel print and try technique in the presence of aberrant endodontic anatomies | |
| Kamburoğlu, Kıvanç, et al. (2023) [90] | In vitro | SLA | To evaluate the accuracy of guides prepared using CBCT images on 3D-printed teeth for root canal treatment | |
| Llaquet Pujol, Marc et al. (2021) [91] | In vivo | SLA | To describe the endodontic management of pulp canal obliteration by guided endodontics using both a virtually designed 3D guide | |
| Kröger, E et al. (2017) [93] | In vitro | Polyjet | To introduce workflow to create 3D printed simulation models based on real patient situations for hands-on practice. | |
| Pouhaër, Matéo et al. (2022) [94] | In vitro | SLA | To show the design phases of different dental models of a lower first molar, showing root canal anatomy and the ideal access cavity. | |
| Autotrans-plantation | Kamio, Takashi et al. (2019) [95] | In vivo | Fused filament fabrication |
To describe 3D morphological evaluation, preoperative treatment planning, and surgical simulation |
| Lee, Seung-Jong, et al. (2001) [96] | In vivo | Prototype machine | To minimize extra-oral time and achieve optimal contact in autotransplantation | |
| Lee, Seung-Jong, et al. (2012) [97] | In vivo | Prototype machine | To reduce extra-oral time and secure optimal contact in autogenous tooth transplantation | |
| Honda, M et al. [99] | In vivo | SLA | To simplify the surgical technique in autotransplantation | |
| Keightley, Alexander J et al. (2010) [100] | In vivo | Binder jetting (powder-based type) |
To develop and apply a surgical template for autotransplantation | |
| Park, Young-Seok et al. (2012) [101] | In vivo | Prototype machine | To develop autotransplantation with simultaneous sinus floor elevation and implant installation | |
| Strbac, Georg D et al. (2016) [102] | In vivo | Polyjet | To introduce a method for autotransplantation of teeth |
4. Conclusions
This scoping review highlights the transformative potential of 3D printing in dentistry, particularly in prosthodontics, orthodontics, and endodontics. The findings reveal significant advancements in precision, customization, and efficiency, demonstrating how 3D printing has revolutionized the production of dental prostheses, aligners, and surgical guides. However, key challenges remain, including material durability, cost-effectiveness, and standardization of workflows.
In prosthodontics, while 3D printing offers enhanced accuracy for crowns, bridges, and dentures, the long-term clinical performance of these restorations remains underexplored. Future studies must address critical challenges including material performance, surface quality, and long-term clinical reliability. Investigating the development of advanced photocurable resins, improving precision, and understanding the biomechanical properties of 3D-printed prosthetics will be essential. By systematically exploring these areas and potentially developing hybrid approaches that combine traditional techniques with emerging 3D printing technologies, researchers can optimize the clinical application and cost-efficiency of digital dental restoration methods.
In orthodontics, although 3D-printed aligners and diagnostic models have improved treatment precision and patient comfort, material properties such as durability and wear resistance require further refinement. Large-scale, multi-center clinical trials are essential to validate the long-term efficacy of 3D-printed orthodontic solutions and assess their impact on diverse patient populations. Research into standardizing digital workflows and streamlining the integration of 3D printing with existing orthodontic protocols is also necessary.
In endodontics, 3D-printed surgical guides and educational models have enhanced procedural accuracy and training outcomes. However, the integration of advanced imaging technologies, such as CBCT, with customized 3D-printed tools for complex cases requires further development. Future research should also focus on designing minimally invasive tools and biocompatible materials that can improve the success rates of challenging treatments such as root canal navigation and apical surgery.
By mapping current knowledge and identifying these research gaps, this scoping review provides a roadmap for future studies aimed at overcoming the limitations of 3D printing in dentistry. Addressing these challenges will expand its clinical applications, improve patient outcomes, and ensure that 3D printing becomes a more accessible, cost-effective, and reliable tool in modern dental care.
Author Contributions
Conceptualization, M.-K.J. and H.-M.K.; methodology, H.-M.K. and M.-K.J.; software, H.-M.K.; validation, J.-W.K.; formal analysis, J.-W.K.; investigation, M.-K.J.; data curation, H.-M.K. and Y.-M.L.; writing—original draft preparation, M.-K.J. and J.-W.K.; writing—review and editing, H.-M.K. All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Haidar, Z.S. Digital dentistry: past, present, and future. Digital Medicine and Healthcare Technology 2023. [Google Scholar] [CrossRef]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: a narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef] [PubMed]
- Harikrishnan, S.; Subramanian, A.K. 3D printing in orthodontics: A narrative review. Journal of International Oral Health 2023, 15, 15–27. [Google Scholar]
- Shah, P.; Chong, B. 3D imaging, 3D printing and 3D virtual planning in endodontics. Clinical oral investigations 2018, 22, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Strbac, G.D.; Schnappauf, A.; Giannis, K.; Moritz, A.; Ulm, C. Guided Modern Endodontic Surgery: A Novel Approach for Guided Osteotomy and Root Resection. J Endod 2017, 43, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Tsoukala, E.; Lyros, I.; Tsolakis, A.I.; Maroulakos, M.P.; Tsolakis, I.A. Direct 3D-Printed Orthodontic Retainers. A Systematic Review. Children (Basel) 2023, 10. [Google Scholar] [CrossRef]
- Alyami, M.H. The Applications of 3D-Printing Technology in Prosthodontics: A Review of the Current Literature. Cureus 2024, 16, e68501. [Google Scholar] [CrossRef]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dental materials 2016, 32, 54–64. [Google Scholar] [CrossRef]
- Tahayeri, A.; Morgan, M.; Fugolin, A.P.; Bompolaki, D.; Athirasala, A.; Pfeifer, C.S.; Ferracane, J.L.; Bertassoni, L.E. 3D printed versus conventionally cured provisional crown and bridge dental materials. Dental materials 2018, 34, 192–200. [Google Scholar] [CrossRef]
- Park, S.-M.; Park, J.-M.; Kim, S.-K.; Heo, S.-J.; Koak, J.-Y. Flexural strength of 3D-printing resin materials for provisional fixed dental prostheses. Materials 2020, 13, 3970. [Google Scholar] [CrossRef]
- Vitali, J.; Cheng, M.; Wagels, M. Utility and cost–effectiveness of 3D-printed materials for clinical use. Journal of 3D printing in medicine 2019, 3, 209–218. [Google Scholar] [CrossRef]
- Lin, L.; Fang, Y.; Liao, Y.; Chen, G.; Gao, C.; Zhu, P. 3D printing and digital processing techniques in dentistry: a review of literature. Advanced Engineering Materials 2019, 21, 1801013. [Google Scholar] [CrossRef]
- Koch, G.K.; Gharib, H.; Liao, P.; Liu, H. Guided access cavity preparation using cost-effective 3D printers. Journal of endodontics 2022, 48, 909–913. [Google Scholar] [CrossRef]
- Kessler, A.; Hickel, R.; Reymus, M. 3D printing in dentistry—State of the art. Operative dentistry 2020, 45, 30–40. [Google Scholar] [CrossRef]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dent Mater 2016, 32, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Lee, J.-H.; Lee, K.-B. Comparison of intaglio surface trueness of interim dental crowns fabricated with SLA 3D printing, DLP 3D printing, and milling technologies. In Proceedings of the Healthcare; 2021; p. 983. [Google Scholar]
- Steinmassl, O.; Dumfahrt, H.; Grunert, I.; Steinmassl, P.A. Influence of CAD/CAM fabrication on denture surface properties. Journal of oral rehabilitation 2018, 45, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kratchman, S. Modern endodontic surgery concepts and practice: a review. J Endod 2006, 32, 601–623. [Google Scholar] [CrossRef]
- Jeong, Y.-G.; Lee, W.-S.; Lee, K.-B. Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method. The journal of advanced prosthodontics 2018, 10, 245–251. [Google Scholar] [CrossRef]
- Herpel, C.; Tasaka, A.; Higuchi, S.; Finke, D.; Kühle, R.; Odaka, K.; Rues, S.; Lux, C.J.; Yamashita, S.; Rammelsberg, P. Accuracy of 3D printing compared with milling—A multi-center analysis of try-in dentures. Journal of Dentistry 2021, 110, 103681. [Google Scholar] [CrossRef]
- Mukai, S.; Mukai, E.; Santos-Junior, J.A.; Shibli, J.A.; Faveri, M.; Giro, G. Assessment of the reproducibility and precision of milling and 3D printing surgical guides. BMC Oral Health 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Valenti, C.; Federici, M.I.; Masciotti, F.; Marinucci, L.; Xhimitiku, I.; Cianetti, S.; Pagano, S. Mechanical properties of 3D printed prosthetic materials compared with milled and conventional processing: A systematic review and meta-analysis of in vitro studies. The Journal of Prosthetic Dentistry 2024, 132, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Yousef, H.; Harris, B.T.; Elathamna, E.N.; Morton, D.; Lin, W.-S. Effect of additive manufacturing process and storage condition on the dimensional accuracy and stability of 3D-printed dental casts. The Journal of Prosthetic Dentistry 2022, 128, 1041–1046. [Google Scholar] [CrossRef]
- Kim, C.-M.; Jeon, J.-H.; Kim, J.-H.; Kim, H.-Y.; Kim, W.-C. Three-dimensional evaluation of the reproducibility of presintered zirconia single copings fabricated with the subtractive method. The Journal of prosthetic dentistry 2016, 116, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.-S.; Jiang, H.B. A review of 3D printing in dentistry: Technologies, affecting factors, and applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef] [PubMed]
- Dawood, A.; Marti, B.M.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. British dental journal 2015, 219, 521–529. [Google Scholar] [CrossRef]
- Barazanchi, A.; Li, K.C.; Al-Amleh, B.; Lyons, K.; Waddell, J.N. Additive technology: update on current materials and applications in dentistry. Journal of Prosthodontics 2017, 26, 156–163. [Google Scholar] [CrossRef]
- Tsolakis, I.A.; Papaioannou, W.; Papadopoulou, E.; Dalampira, M.; Tsolakis, A.I. Comparison in terms of accuracy between DLP and LCD printing technology for dental model printing. Dentistry journal 2022, 10, 181. [Google Scholar] [CrossRef]
- Quan, H.; Zhang, T.; Xu, H.; Luo, S.; Nie, J.; Zhu, X. Photo-curing 3D printing technique and its challenges. Bioactive materials 2020, 5, 110–115. [Google Scholar] [CrossRef]
- Chang, H.S.; Peng, Y.T.; Hung, W.L.; Hsu, M.L. Evaluation of marginal adaptation of Co-Cr-Mo metal crowns fabricated by traditional method and computer-aided technologies. J Dent Sci 2019, 14, 288–294. [Google Scholar] [CrossRef]
- Lövgren, N.; Roxner, R.; Klemendz, S.; Larsson, C. Effect of production method on surface roughness, marginal and internal fit, and retention of cobalt-chromium single crowns. J Prosthet Dent 2017, 118, 95–101. [Google Scholar] [CrossRef]
- V, H.; Ali, S.A.M.; N, J.; Ifthikar, M.; Senthil, S.; Basak, D.; Huda, F.; Priyanka. Evaluation of internal and marginal fit of two metal ceramic system - in vitro study. J Clin Diagn Res 2014, 8, Zc53–56. [Google Scholar] [CrossRef] [PubMed]
- Sundar, M.K.; Chikmagalur, S.B.; Pasha, F. Marginal fit and microleakage of cast and metal laser sintered copings--an in vitro study. J Prosthodont Res 2014, 58, 252–258. [Google Scholar] [CrossRef]
- Huang, Z.; Zhang, L.; Zhu, J.; Zhao, Y.; Zhang, X. Clinical Marginal and Internal Fit of Crowns Fabricated Using Different CAD/CAM Technologies. J Prosthodont 2015, 24, 291–295. [Google Scholar] [CrossRef]
- Ates, S.M.; Yesil Duymus, Z. Influence of Tooth Preparation Design on Fitting Accuracy of CAD-CAM Based Restorations. J Esthet Restor Dent 2016, 28, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Dahl, B.E.; Rønold, H.J.; Dahl, J.E. Internal fit of single crowns produced by CAD-CAM and lost-wax metal casting technique assessed by the triple-scan protocol. J Prosthet Dent 2017, 117, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Khaledi, A.A.; Farzin, M.; Akhlaghian, M.; Pardis, S.; Mir, N. Evaluation of the marginal fit of metal copings fabricated by using 3 different CAD-CAM techniques: Milling, stereolithography, and 3D wax printer. J Prosthet Dent 2020, 124, 81–86. [Google Scholar] [CrossRef]
- Addugala, H.; Venugopal, V.N.; Rengasamy, S.; Yadalam, P.K.; Albar, N.H.; Alamoudi, A.; Bahammam, S.A.; Zidane, B.; Bahammam, H.A.; Bhandi, S.; et al. Marginal and Internal Gap of Metal Copings Fabricated Using Three Types of Resin Patterns with Subtractive and Additive Technology: An In Vitro Comparison. Materials (Basel) 2022, 15. [Google Scholar] [CrossRef]
- Ali Majeed, Z.; Hasan Jasim, H. Digital Evaluation of Trueness and Fitting Accuracy of Co-Cr Crown Copings Fabricated by Different Manufacturing Technologies. Cureus 2023, 15, e39819. [Google Scholar] [CrossRef]
- Goguta, L.; Lungeanu, D.; Negru, R.; Birdeanu, M.; Jivanescu, A.; Sinescu, C. Selective Laser Sintering versus Selective Laser Melting and Computer Aided Design - Computer Aided Manufacturing in Double Crowns Retention. J Prosthodont Res 2021, 65, 371–378. [Google Scholar] [CrossRef]
- Kim, D.Y.; Kim, J.H.; Kim, H.Y.; Kim, W.C. Comparison and evaluation of marginal and internal gaps in cobalt-chromium alloy copings fabricated using subtractive and additive manufacturing. J Prosthodont Res 2018, 62, 56–64. [Google Scholar] [CrossRef]
- Qian, B.; Saeidi, K.; Kvetková, L.; Lofaj, F.; Xiao, C.; Shen, Z. Defects-tolerant Co-Cr-Mo dental alloys prepared by selective laser melting. Dent Mater 2015, 31, 1435–1444. [Google Scholar] [CrossRef]
- Saini, R.S.; Gurumurthy, V.; Quadri, S.A.; Bavabeedu, S.S.; Abdelaziz, K.M.; Okshah, A.; Alshadidi, A.A.F.; Yessayan, L.; Mosaddad, S.A.; Heboyan, A. The flexural strength of 3D-printed provisional restorations fabricated with different resins: a systematic review and meta-analysis. BMC Oral Health 2024, 24, 66. [Google Scholar] [CrossRef] [PubMed]
- Herpel, C.; Tasaka, A.; Higuchi, S.; Finke, D.; Kühle, R.; Odaka, K.; Rues, S.; Lux, C.J.; Yamashita, S.; Rammelsberg, P.; et al. Accuracy of 3D printing compared with milling - A multi-center analysis of try-in dentures. J Dent 2021, 110, 103681. [Google Scholar] [CrossRef]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Müller, F.; Srinivasan, M. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J Prosthet Dent 2019, 121, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Gad, M.A.; Abdelhamid, A.M.; ElSamahy, M.; Abolgheit, S.; Hanno, K.I. Effect of aging on dimensional accuracy and color stability of CAD-CAM milled and 3D-printed denture base resins: a comparative in-vitro study. BMC Oral Health 2024, 24, 1124. [Google Scholar] [CrossRef]
- Helal, M.A.; Abdelrahim, R.A.; Zeidan, A.A.E. Comparison of Dimensional Changes Between CAD-CAM Milled Complete Denture Bases and 3D Printed Complete Denture Bases: An In Vitro Study. J Prosthodont 2023, 32, 11–19. [Google Scholar] [CrossRef]
- Jeong, Y.G.; Lee, W.S.; Lee, K.B. Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method. J Adv Prosthodont 2018, 10, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Prpić, V.; Schauperl, Z.; Ćatić, A.; Dulčić, N.; Čimić, S. Comparison of Mechanical Properties of 3D-Printed, CAD/CAM, and Conventional Denture Base Materials. J Prosthodont 2020, 29, 524–528. [Google Scholar] [CrossRef]
- Freitas, R.; Duarte, S.; Feitosa, S.; Dutra, V.; Lin, W.S.; Panariello, B.H.D.; Carreiro, A. Physical, Mechanical, and Anti-Biofilm Formation Properties of CAD-CAM Milled or 3D Printed Denture Base Resins: In Vitro Analysis. J Prosthodont 2023, 32, 38–44. [Google Scholar] [CrossRef]
- Zeidan, A.A.E.; Sherif, A.F.; Baraka, Y.; Abualsaud, R.; Abdelrahim, R.A.; Gad, M.M.; Helal, M.A. Evaluation of the Effect of Different Construction Techniques of CAD-CAM Milled, 3D-Printed, and Polyamide Denture Base Resins on Flexural Strength: An In Vitro Comparative Study. J Prosthodont 2023, 32, 77–82. [Google Scholar] [CrossRef]
- Park, M.E.; Shin, S.Y. Three-dimensional comparative study on the accuracy and reproducibility of dental casts fabricated by 3D printers. J Prosthet Dent 2018, 119, e861–e861. [Google Scholar] [CrossRef] [PubMed]
- Bachour, P.C.; Klabunde, R.; Grünheid, T. Transfer accuracy of 3D-printed trays for indirect bonding of orthodontic brackets: a clinical study. The Angle Orthodontist 2022, 92, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Sarkarat, F.; Tofighi, O.; Jamilian, A.; Fateh, A.; Abbaszadeh, F. Are Virtually Designed 3D Printed Surgical Splints Accurate Enough for Maxillary Reposition as an Intermediate Orthognathic Surgical Guide. Journal of Maxillofacial and Oral Surgery 2023, 22, 861–872. [Google Scholar] [CrossRef]
- Jindal, P.; Juneja, M.; Siena, F.L.; Bajaj, D.; Breedon, P. Mechanical and geometric properties of thermoformed and 3D printed clear dental aligners. American Journal of Orthodontics and Dentofacial Orthopedics 2019, 156, 694–701. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D printing of clear orthodontic aligners: current state and future possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef]
- Upadhyay, M.; Arqub, S.A. Biomechanics of clear aligners: hidden truths & first principles. J World Fed Orthod 2022, 11, 12–21. [Google Scholar] [CrossRef]
- Maspero, C.; Tartaglia, G.M. 3D Printing of Clear Orthodontic Aligners: Where We Are and Where We Are Going. Materials (Basel) 2020, 13. [Google Scholar] [CrossRef] [PubMed]
- Venezia, P.; Ronsivalle, V.; Rustico, L.; Barbato, E.; Leonardi, R.; Lo Giudice, A. Accuracy of orthodontic models prototyped for clear aligners therapy: A 3D imaging analysis comparing different market segments 3D printing protocols. J Dent 2022, 124, 104212. [Google Scholar] [CrossRef]
- Grassia, V.; Ronsivalle, V.; Isola, G.; Nucci, L.; Leonardi, R.; Lo Giudice, A. Accuracy (trueness and precision) of 3D printed orthodontic models finalized to clear aligners production, testing crowded and spaced dentition. BMC Oral Health 2023, 23, 352. [Google Scholar] [CrossRef]
- Willi, A.; Patcas, R.; Zervou, S.-K.; Panayi, N.; Schätzle, M.; Eliades, G.; Hiskia, A.; Eliades, T. Leaching from a 3D-printed aligner resin. European Journal of Orthodontics 2023, 45, 244–249. [Google Scholar] [CrossRef]
- Tamer, İ.; Öztaş, E.; Marşan, G. Orthodontic Treatment with Clear Aligners and The Scientific Reality Behind Their Marketing: A Literature Review. Turk J Orthod 2019, 32, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Narongdej, P.; Hassanpour, M.; Alterman, N.; Rawlins-Buchanan, F.; Barjasteh, E. Advancements in Clear Aligner Fabrication: A Comprehensive Review of Direct-3D Printing Technologies. Polymers (Basel) 2024, 16. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials (Basel) 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Šimunović, L.; Čekalović Agović, S.; Marić, A.J.; Bačić, I.; Klarić, E.; Uribe, F.; Meštrović, S. Color and Chemical Stability of 3D-Printed and Thermoformed Polyurethane-Based Aligners. Polymers (Basel) 2024, 16. [Google Scholar] [CrossRef]
- Pasaoglu Bozkurt, A.; Demirci, M.; Erdogan, P.; Kayalar, E. Comparison of microbial adhesion and biofilm formation on different orthodontic aligners. Am J Orthod Dentofacial Orthop 2025, 167, 47–62. [Google Scholar] [CrossRef]
- Tsoukala, E.; Lyros, I.; Tsolakis, A.I.; Maroulakos, M.P.; Tsolakis, I.A. Direct 3d-printed orthodontic retainers. a systematic review. Children 2023, 10, 676. [Google Scholar] [CrossRef]
- Ellakany, P.; Al-Harbi, F.; El Tantawi, M.; Mohsen, C. Evaluation of the accuracy of digital and 3D-printed casts compared with conventional stone casts. The Journal of Prosthetic Dentistry 2022, 127, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Rungrojwittayakul, O.; Kan, J.Y.; Shiozaki, K.; Swamidass, R.S.; Goodacre, B.J.; Goodacre, C.J.; Lozada, J.L. Accuracy of 3D Printed Models Created by Two Technologies of Printers with Different Designs of Model Base. J Prosthodont 2020, 29, 124–128. [Google Scholar] [CrossRef]
- Dawood, A.; Marti Marti, B.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. Br Dent J 2015, 219, 521–529. [Google Scholar] [CrossRef]
- Brown, G.B.; Currier, G.F.; Kadioglu, O.; Kierl, J.P. Accuracy of 3-dimensional printed dental models reconstructed from digital intraoral impressions. Am J Orthod Dentofacial Orthop 2018, 154, 733–739. [Google Scholar] [CrossRef]
- Duarte, M.E.A.; Gribel, B.F.; Spitz, A.; Artese, F.; Miguel, J.A.M. Reproducibility of digital indirect bonding technique using three-dimensional (3D) models and 3D-printed transfer trays. Angle Orthod 2020, 90, 92–99. [Google Scholar] [CrossRef]
- van der Meer, W.J.; Vissink, A.; Ng, Y.L.; Gulabivala, K. 3D Computer aided treatment planning in endodontics. J Dent 2016, 45, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, S.; Aguilera, F.C.; Buie, J.M.; Glickman, G.N.; Umorin, M.; Wang, Q.; Jalali, P. Accuracy of 3-dimensional-printed Endodontic Surgical Guide: A Human Cadaver Study. J Endod 2019, 45, 615–618. [Google Scholar] [CrossRef] [PubMed]
- Connert, T.; Zehnder, M.S.; Amato, M.; Weiger, R.; Kühl, S.; Krastl, G. Microguided Endodontics: a method to achieve minimally invasive access cavity preparation and root canal location in mandibular incisors using a novel computer-guided technique. Int Endod J 2018, 51, 247–255. [Google Scholar] [CrossRef]
- Lara-Mendes, S.T.O.; Barbosa, C.F.M.; Santa-Rosa, C.C.; Machado, V.C. Guided Endodontic Access in Maxillary Molars Using Cone-beam Computed Tomography and Computer-aided Design/Computer-aided Manufacturing System: A Case Report. J Endod 2018, 44, 875–879. [Google Scholar] [CrossRef] [PubMed]
- Connert, T.; Krug, R.; Eggmann, F.; Emsermann, I.; ElAyouti, A.; Weiger, R.; Kühl, S.; Krastl, G. Guided Endodontics versus Conventional Access Cavity Preparation: A Comparative Study on Substance Loss Using 3-dimensional-printed Teeth. J Endod 2019, 45, 327–331. [Google Scholar] [CrossRef]
- Loureiro, M.A.Z.; Silva, J.A.; Chaves, G.S.; Capeletti, L.R.; Estrela, C.; Decurcio, D.A. Guided endodontics: The impact of new technologies on complex case solution. Aust Endod J 2021, 47, 664–671. [Google Scholar] [CrossRef]
- Lee, S.J.; Jang, K.H.; Spangberg, L.S.; Kim, E.; Jung, I.Y.; Lee, C.Y.; Kum, K.Y. Three-dimensional visualization of a mandibular first molar with three distal roots using computer-aided rapid prototyping. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006, 101, 668–674. [Google Scholar] [CrossRef]
- Byun, C.; Kim, C.; Cho, S.; Baek, S.H.; Kim, G.; Kim, S.G.; Kim, S.Y. Endodontic Treatment of an Anomalous Anterior Tooth with the Aid of a 3-dimensional Printed Physical Tooth Model. J Endod 2015, 41, 961–965. [Google Scholar] [CrossRef]
- Connert, T.; Zehnder, M.S.; Weiger, R.; Kühl, S.; Krastl, G. Microguided Endodontics: Accuracy of a Miniaturized Technique for Apically Extended Access Cavity Preparation in Anterior Teeth. J Endod 2017, 43, 787–790. [Google Scholar] [CrossRef]
- Pinsky, H.M.; Champleboux, G.; Sarment, D.P. Periapical surgery using CAD/CAM guidance: preclinical results. J Endod 2007, 33, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Rabié, C.; Torres, A.; Lambrechts, P.; Jacobs, R. Clinical applications, accuracy and limitations of guided endodontics: a systematic review. Int Endod J 2020, 53, 214–231. [Google Scholar] [CrossRef] [PubMed]
- Buchgreitz, J.; Buchgreitz, M.; Mortensen, D.; Bjørndal, L. Guided access cavity preparation using cone-beam computed tomography and optical surface scans - an ex vivo study. Int Endod J 2016, 49, 790–795. [Google Scholar] [CrossRef]
- Kfir, A.; Telishevsky-Strauss, Y.; Leitner, A.; Metzger, Z. The diagnosis and conservative treatment of a complex type 3 dens invaginatus using cone beam computed tomography (CBCT) and 3D plastic models. Int Endod J 2013, 46, 275–288. [Google Scholar] [CrossRef]
- Anderson, J.; Wealleans, J.; Ray, J. Endodontic applications of 3D printing. Int Endod J 2018, 51, 1005–1018. [Google Scholar] [CrossRef]
- Marending, M.; Biel, P.; Attin, T.; Zehnder, M. Comparison of two contemporary rotary systems in a pre-clinical student course setting. Int Endod J 2016, 49, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Peters, O.; Scott, R.; Arias, A.; Lim, E.; Paque, F.; Almassi, S.; Hejlawy, S. Evaluation of Dental Students' Skills Acquisition in Endodontics Using a 3D Printed Tooth Model. European endodontic journal 2021, 6, 290–294. [Google Scholar] [CrossRef]
- Tonini, R.; Xhajanka, E.; Giovarruscio, M.; Foschi, F.; Boschi, G.; Atav-Ates, A.; Cicconetti, A.; Seracchiani, M.; Gambarini, G.; Testarelli, L. Print and try technique: 3D-printing of teeth with complex anatomy a novel endodontic approach. Applied Sciences 2021, 11, 1511. [Google Scholar] [CrossRef]
- Kamburoğlu, K.; Sönmez, G.; Koç, C.; Yılmaz, F.; Tunç, O.; Isayev, A. Access Cavity Preparation and Localization of Root Canals Using Guides in 3D-Printed Teeth with Calcified Root Canals: An In Vitro CBCT Study. Diagnostics 2023, 13, 2215. [Google Scholar] [CrossRef]
- Llaquet Pujol, M.; Vidal, C.; Mercadé, M.; Muñoz, M.; Ortolani-Seltenerich, S. Guided Endodontics for Managing Severely Calcified Canals. J Endod 2021, 47, 315–321. [Google Scholar] [CrossRef]
- Hawkins, T.K.; Wealleans, J.A.; Pratt, A.M.; Ray, J.J. Targeted endodontic microsurgery and endodontic microsurgery: a surgical simulation comparison. Int Endod J 2020, 53, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Kröger, E.; Dekiff, M.; Dirksen, D. 3D printed simulation models based on real patient situations for hands-on practice. Eur J Dent Educ 2017, 21, e119–e125. [Google Scholar] [CrossRef] [PubMed]
- Pouhaër, M.; Picart, G.; Baya, D.; Michelutti, P.; Dautel, A.; Pérard, M.; Le Clerc, J. Design of 3D-printed macro-models for undergraduates' preclinical practice of endodontic access cavities. Eur J Dent Educ 2022, 26, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Kamio, T.; Kato, H. Autotransplantation of Impacted Third Molar Using 3D Printing Technology: A Case Report. Bull Tokyo Dent Coll 2019, 60, 193–199. [Google Scholar] [CrossRef]
- Lee, S.J.; Jung, I.Y.; Lee, C.Y.; Choi, S.Y.; Kum, K.Y. Clinical application of computer-aided rapid prototyping for tooth transplantation. Dent Traumatol 2001, 17, 114–119. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, E. Minimizing the extra-oral time in autogeneous tooth transplantation: use of computer-aided rapid prototyping (CARP) as a duplicate model tooth. Restor Dent Endod 2012, 37, 136–141. [Google Scholar] [CrossRef]
- Verweij, J.P.; Jongkees, F.A.; Anssari Moin, D.; Wismeijer, D.; van Merkesteyn, J.P.R. Autotransplantation of teeth using computer-aided rapid prototyping of a three-dimensional replica of the donor tooth: a systematic literature review. Int J Oral Maxillofac Surg 2017, 46, 1466–1474. [Google Scholar] [CrossRef]
- Honda, M.; Uehara, H.; Uehara, T.; Honda, K.; Kawashima, S.; Honda, K.; Yonehara, Y. Use of a replica graft tooth for evaluation before autotransplantation of a tooth. A CAD/CAM model produced using dental-cone-beam computed tomography. Int J Oral Maxillofac Surg 2010, 39, 1016–1019. [Google Scholar] [CrossRef]
- Keightley, A.J.; Cross, D.L.; McKerlie, R.A.; Brocklebank, L. Autotransplantation of an immature premolar, with the aid of cone beam CT and computer-aided prototyping: a case report. Dent Traumatol 2010, 26, 195–199. [Google Scholar] [CrossRef]
- Park, Y.S.; Baek, S.H.; Lee, W.C.; Kum, K.Y.; Shon, W.J. Autotransplantation with simultaneous sinus floor elevation. J Endod 2012, 38, 121–124. [Google Scholar] [CrossRef]
- Strbac, G.D.; Schnappauf, A.; Giannis, K.; Bertl, M.H.; Moritz, A.; Ulm, C. Guided Autotransplantation of Teeth: A Novel Method Using Virtually Planned 3-dimensional Templates. J Endod 2016, 42, 1844–1850. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of data filtration process.
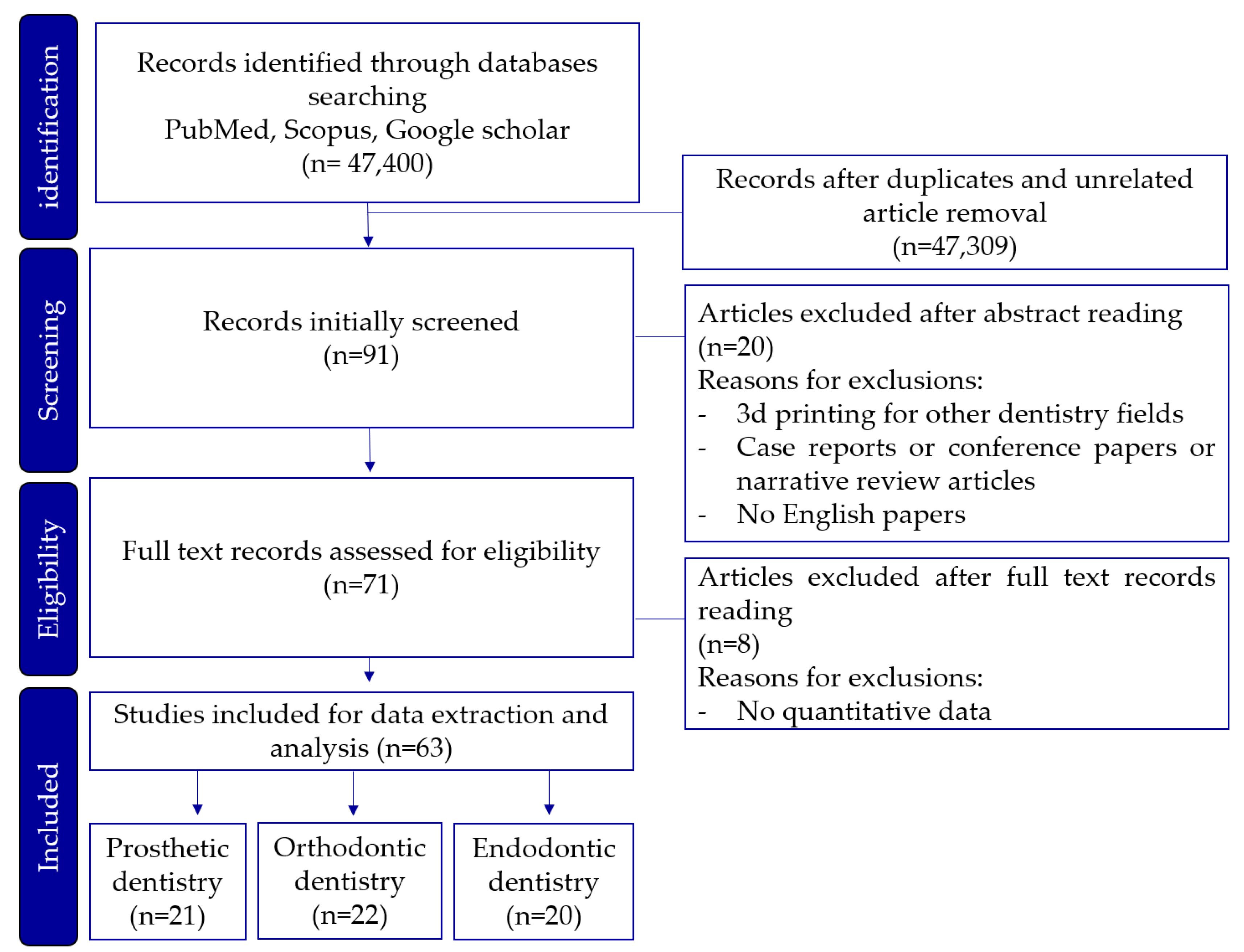
Table 1.
Summary of 3D printer types, research objectives, evaluation criteria, and application in prosthodontics dentistry.
Table 1.
Summary of 3D printer types, research objectives, evaluation criteria, and application in prosthodontics dentistry.
| Dentistry field | 3d printer type | Objective | Evaluation criteria |
Advantages | Disadvantages |
|---|---|---|---|---|---|
| Prosthodontics | SLA | Fabrication of prosthetics | Accuracy, resolution, post-processing needs |
High resolution,Suitable for detailed work |
Requires post- curing,Longer production time |
| DLP | Mass production of prosthetics | Production speed, build volume | Faster print times,Cost-effective for large-scale production | Limited build volume | |
| Milling | Final crown fabrication | Accuracy, durability |
Superior strength and durability,High precision |
Material waste,Difficulty in creating intricate internal structures |
|
| PolyJet | Fabrication of metal coping | Accuracy, resolution, safety |
Multi-material printing High precision for coping | Higher material costs, Low durabilityPost-processing required |
SLA= Stereolithography, DLP = Digital Light Processing.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



