
Submitted:
14 February 2025
Posted:
14 February 2025
You are already at the latest version
Abstract
Male infertility can be the result of many factors, including pathologies in the motility and formation of sperm as well as obstructions in the genitourinary system. Oriental medicine, use of multiple components to address various targets and enhance therapeutic effectiveness, has been used to treat male infertility for thousands of years. Given the complex pathological mechanisms of aspermatogenesis, this multi-target approach in oriental medicine is believed to positively impact the prevention of male infertility. Efforts have been made to evaluate the pharmacological properties of many herbs; however, the testicular immune responses and mechanisms of these oriental medicines remain unclear from a modern scientific perspective. Some studies reviewed here have reported the damage to and recovery of spermatogenesis in infertility, and the available research evaluating the efficacy of oriental medicines in the treatment of aspermatogenesis and briefly summarize the available rodent and human data on facilitating immunological differences in male infertility. These findings augment the current understanding of the immune molecular of oriental medicine as a treatment solution for male infertility.
Keywords:
infertility
; oriental medicine
; molecular immune suppress
; spermatogenesis
1. Introduction
Infertility is a global health issue affecting up to 15% of couples, with male fertility contributing to at least 50% of cases [1,2,3]. Male infertility arises from various factors, including anatomical and genetic defects, testicular injury and disease, sperm disorders, hormonal imbalances, aging, and environmental and lifestyle influences [4,5,6]. A wide range of factors influences sperm production, including varicocele, idiopathic causes, obstructive issues, cryptorchidism, immunological factors, ejaculatory problems, testicular insufficiency, as well as medicinal, radioactive, and endocrinological influences. These factors can contribute to male infertility [7]. Modern medicine emphasizes identifying the primary causes and utilizing various hormones in treatment [8]. The main approaches include general treatment such as lifestyle change, endocrine therapy (gonadotropin-releasing hormone (GnRH) agonists, gonadotropins, anti-estrogens, and aromatase inhibitors), anti-infective therapy, antioxidant therapy, antibiotics, corticosteroids, vitamins, minerals (such as zinc) and amino acids (such as arginine), surgical intervention, and assisted reproductive technology (ART) [9,10]. Gene therapy is still in the research phase and has not yet been implemented in clinical practice [11]. Although ART has significantly improved conception rates among infertility patients, it has not fundamentally enhanced sperm quality. Infertility is not an isolated condition, but arises from multiple diseases and factors [12,13]. On the other hands, oriental medicine has been used to treat male infertility for thousands of years. A key characteristic of oriental medicine is the use of multiple components to address various targets and enhance therapeutic effectiveness. Given the complex pathological mechanisms of aspermatogenesis, this multi-target approach in oriental medicine is believed to positively impact the prevention of male infertility [14].
Immunology of reproduction has a long story and robust literature. Although the mechanisms of immune privilege in male reproductive organs are well studied, a deeper understanding of the underlying immune responses and mechanisms of male infertility is essential for advancing treatment. The most recognized immunological privilege mechanism in the testis is the blood–testis barrier (BTB), which is formed by the junctions of adjacent Sertoli cells. This barrier restricts access to germ cell antigens for interstitial immune cells and protects against antibody attacks from the interstitium [15]. Immunological privileges outside the BTB involve the secretion of immunosuppressive factors primarily by macrophages, Sertoli cells, peritubular cells, and Leydig cells [16,17] (see Table 1).
Herbal formulas play a significant role in traditional medical treatments, with individual herbs classified into broad therapeutic categories based on their principal effects. The treatment of spermatogenesis with various oriental medicines differs from modern medicine [18]. In recent years, efforts have been made to evaluate the pharmacological properties of many herbs; however, the testicular immune responses and mechanisms of these oriental medicines remain unclear from a modern scientific perspective. This review aimed to describe some etiologies induced male infertility associated with several immune factors and to examine studies evaluating the use of traditional herbal formulas rather than individual herbal medicines in treating this condition. Our findings enhance the current understanding of the potential of oriental medicine as a treatment option for male infertility.
2. Types and causes of infertility
Spermatogenesis is a complex process involving the production of normal mature spermatozoa in the testis. The established causes of male infertility range from pre-testicular to testicular to post-testicular. The pretesticular causes include hypogonadotropic hypogonadism, chronic alcoholism, cigarette smoking, drugs and substance abuse. The testicular causes include congenital anomalies, cryptorchidism, orchitis, testicular tumors, testicular torsion/detorsion, varicocele, radiotherapy and chemotherapy. The post-testicular causes include obstruction or absence of the vas deferens or ejaculatory duct, hypospadias and erectile dysfunction [4,5,6]. This review aims to summarize some infertility types with insufficient treatment effects in western medicine and will discuss oriental medicines employed to combat these conditions.
Around 30%–40% of infertile men fall into the category of idiopathic oligoasthenozoospermia (IOA), characterized by a low sperm count (16 × 106 spermatozoa per milliliter of semen) and poor sperm quality (<30% of spermatozoa exhibiting progressive motility) [19,20]. Common causes of IOA include endocrine factors, reproductive tract infections, chromosomal abnormalities, cryptorchidism, varicocele, systemic diseases, and various genetic, metabolic, and immune dysfunctions. IOA is not an independent condition; rather, it results from a combination of multiple diseases and factors [12,13]. Although various factors contribute to the pathogenesis of IOA, the underlying mechanisms remain unclear. Consequently, Western medicine faces certain limitations: its clinical efficacy is often suboptimal, and finding a cure for IOA has long been a significant challenge in the medical field. Modern medical treatments for IOA include general treatment, endocrine therapy (such as GnRH agonists, gonadotropins, antiestrogens, and aromatase inhibitors), antioxidant therapy, antibiotics, corticosteroids, vitamins (e.g., vitamin E), minerals (such as zinc), amino acids (such as arginine), anti-infective therapy, surgical interventions, and ART [9,10]. However, these strategies are often associated with poor outcomes. Therefore, there is an urgent need to investigate the molecular mechanisms underlying IOA and identify effective treatments for IOA-related infertility.
There is growing evidence that oxidative stress in seminal fluid is a key factor in poor semen quality, including in IOA [21]. Oxidative stress, characterized by an imbalance between reactive oxygen species (ROS) and antioxidant levels, is the primary cause of infertility in men. Testis contains high levels of polyunsaturated fatty acids, making them an ideal substrate for ROS generation. Elevated ROS levels can lead to infertility through mechanisms such as lipid peroxidation, DNA damage, enzyme inactivation, and protein oxidation in spermatozoa. These processes compromise sperm functionality and reduce sperm motility and viability [22]. Studies indicate that 30–80% of infertile men exhibit elevated ROS levels, which can damage DNA as well as the proteins and lipids of sperm [23]. This damage can interfere with the capacitation processes necessary for successful fertilization [24,25]. The body’s antioxidant systems—comprising enzymatic factors such as superoxide dismutase, catalase, and glutathione peroxidase, along with non-enzymatic factors such as low-molecular-weight compounds (e.g., glutathione, N-acetylcysteine, vitamins E, A, and C, coenzyme Q10, carnitines, myo-inositol, and lycopene) and essential nutrients (selenium, zinc, and copper)—play a critical role in protecting against oxidative stress. A deficiency in any of these antioxidants can reduce the antioxidant capacity of plasma [26]. Furthermore, in our daily lives, genital heat stress—such as sitting in a hot bath or car for an extended period—is associated with significantly higher scrotal temperatures. This condition is a major factor contributing to the impairment of male reproductive health, resulting in the downregulation of spermatogenesis and declines in semen volume, sperm motility, and sperm morphology [21]. It has been demonstrated that body weight, testicular weight, sperm count, and sperm motility were significantly reduced in male mice subjected to heat stress in a 43°C water bath for 10 min twice per day, six days per week, over a period of five weeks [27,28]. Germ cell death and decreased sperm motility resulting from heat stress appear to be caused by oxidative stress and apoptosis. These processes involve ROS, the tumor suppressor protein p53, nitric oxide synthase (NOS), and translocation of the pro-apoptotic factor Bax. [29,30]. Many urologists prescribe oral antioxidants to address infertility because they enhance seminal plasma clearance and lower ROS levels in the semen [31].
Varicocele, another common cause of IOA, characterized by the enlargement of the pampiniform venous plexus within the spermatic cord, is generally acknowledged as the most common but curable cause of male infertility. Varicocele can affect spermatogenesis in many ways e.g., increased testicular temperature, increased intratesticular pressure, hypoxia due to attenuation of blood flow, reflux of toxic metabolites from the adrenal glands and hormonal profile abnormalities [32]. Varicocele also has been associated with increased oxidative stress, especially in the gonads [33]. The incidence of varicocele is approximately 15%, affecting more than 40% of men in infertile couples [34,35,36]. The precise mechanism by which varicocele leads to infertility remains unclear. However, factors such as the testicular immune response, including the production of anti-sperm antibodies (ASA), activation of inflammatory pathways (increase in the pro-inflammatory cytokines such as interleukin (IL)-1 and tumor necrosis factor (TNF)-alpha in the seminal plasma, testicular tissue, and even peripheral blood), and disruption of the BTB (abnormal permeability of proteins, such as claudin-11), may contribute to the development of varicocele-related infertility [37] (see Table 1). Currently, there are no effective medications for most varicoceles, and the primary treatment approach is surgery. However, some patients may still struggle to regain their natural fertility after surgery. Medications are often considered the first-line option for patients with low spermatogenesis and varicocele who do not undergo surgical treatment, although their endocrine effects are debated. Selective estrogen receptor modulators (SERMs), such as clomiphene and tamoxifen, are commonly used as empirical treatments for male infertility. These medications function by blocking estrogen receptor (ER) activity, which promotes luteinizing hormone (LH) production and stimulates sperm production. Although the use of SERMs may have positive effects on pregnancy outcomes, their overall efficacy remains uncertain [38]. In clinical practice, antioxidants, such as kallikrein, L-carnitine, anthocyanin, silymarin, chrysin, selenium, and resveratrol, are also used in the treatment of varicocele. However, current studies do not provide sufficient evidence to support the use of these substances for treating varicocele [39]. Therefore, the development of safe medical treatments for varicocele with fewer side effects is still in demand.
On the other hand, the risk of anti-cancer treatment induced oligoasthenozoospermia and azoospermia increases with the development of chemotherapy and radiotherapy that significantly improved survival rates in children with cancer. More than 70% of patients survive childhood cancer; however, these treatments may cause irreversible impairment of reproductive function. Infertility affects 30% of long-term survivors of childhood acute myelogenous leukemia (AML), leaving them unable to father children, even with the use of assisted reproductive techniques [40,41]. The testis is more sensitive to anti-cancer drugs and radiation than the ovary, and both anti-cancer agents and radiation therapy are often used in combination with hematopoietic cell transplantation pretreatment methods, further increasing the risk of testicular injury. Cytotoxic agents, including alkylating agents such as cyclophosphamide (CP), ifosfamide, and chlorambucil, as well as procarbazine, cisplatin, and vinblastine, can cause long-lasting or permanent damage to germ cells, resulting in oligozoospermia or azoospermia. In fact, azoospermia is permanent in 90% of men treated with cyclophosphamide at doses greater than 7.5 g/m2 [42]. Germ cells are also susceptible to fractionation by radiotherapy, with doses exceeding 1.2 Gy leading to permanent azoospermia [43]. Following treatment with total body irradiation (9.9 or 13.2 Gy) and cyclophosphamide for bone marrow transplantation, azoospermia was observed in 85% of adult male patients [44]. Testicular toxicity is one of the main side effects of CP, with oxidative stress damage being the primary cause of testicular spermatogenesis disorders induced by this agent [45]. Studies have confirmed that oxidative stress can lead to abnormal expression of tight junctions, the key components of the BTB, and related proteins by activating the p38 MAPK pathway [46,47]. It is well known that occludin and ZO-1 play crucial roles in maintaining the normal function of tight junctions. Fibrous actin (F-actin), a polymer of actin filaments, is associated with ZO-1 and is essential for the integrity of tight junction network structures. Li et al. [48] demonstrated that CP could reduce the expression of occludin, ZO-1, and F-actin, while increasing the expression of p38, significantly inducing BTB damage in rats (see Table 1). Although advancements in molecular biology, such as the assessment of sperm mRNAs, microRNAs, histone modifications, and DNA methylation, have been made, there is a lack of innovative approaches that could enhance the evaluation of sperm health following anti-cancer therapy. Currently, the only established option is cryopreservation of sperm prior to treatment. Sperm cryobanking allows patients to preserve sperm before undergoing gonadotoxic therapies, facilitating future assisted reproduction techniques, such as the in vitro fertilization or intracytoplasmic sperm injection [40]. Although post-pubertal males can cryopreserve their own sperm, there are currently no options available to prevent infertility in pre-pubertal boys undergoing chemotherapy and/or radiotherapy. Hormonal protection of germ cells using GnRH agonists has shown success in rodent models [49] but has not been effective in humans [50]. Over the past decade, fertility preservation has emerged as an area of increasing awareness among researchers, clinicians, and patients, particularly in light of improved survival rates following cancer treatment [51]. However, there is limited information regarding therapies for anticancer-induced male infertility. Although some attempts at medical treatment for male factor infertility have been reported, adequately controlled studies of potential therapeutic agents often fail to demonstrate significant improvements in fertility.
3. Pharmacological Effects and Immune Mechanisms Of Oriental Medicines
Oriental medicine posits that sperm production and maturation are closely linked to Kidney deficiency, viewing Kidney as a congenital foundation that stores essence and governs growth, development, and reproduction. Robust Kidney qi (Stagnation of circulation of vital energy) enhances sperm motility, whereas a decline in sperm motility is associated with Kidney hypofunction. Insufficient Kidney- Yang impairs Kidney-Yin’s ability to generate essence and qi, leading to reduced sperm count, decreased sperm motility, and infertility. Several studies have identified the active components of herbal medicines that nourish the Kidney, support blood circulation in the reproductive system, and regulate testosterone secretion [52]. They have been shown to significantly improve sperm motility in animal studies [53]. It has also been shown to have positive effects in enhancing sperm parameters in infertile men [54].
3.1. Varicocele
In oriental medicine, varicocele cryptozoospermia is considered to be linked to the deficiency syndrome of “qi-stagnation”, “blood-stasis” (coagulation of blood), and Kidney-Yang [55]. Tonification of the Kidney is the fundamental theory underlying the treatment of varicocele and male infertility in oriental medicine.
Jiawei Runjing Decoction (JWRJD) by adding two traditional Chinese medicines [Homo Sapiens and Eupolyphaga seu Steleophaga] (see Table 2) into Runjing Decoction, could be more powerful to promote blood circulation and clear collaterals, nourish Kidney-Yang and other functions to improve the proliferation of mouse germ cells, and increase the number of sperms [56,57]. Liu et al. [57] applied JWRJD to 58 cryptozoospermic patients with varicocele who were observed for 3 months and found that JWRJD may promote spermatogenesis in cryptozoospermic patients with varicocele closely related to the sex hormone mechanism and improve the testicular microenvironment, especially for patients >35-year-old and having grade III varicocele. Although they demonstrated an increase in testicular volume, decreased follicle-stimulating hormone (FSH), decreased testicular vein width, and increased seminal plasma zinc levels after treatment with JWRJD, they did not investigate testicular immune response in the pathogenesis of varicocele-mediated infertility.
Another Chinese research group [58] investigated the mechanism of action of Taohong Siwu Decoction (THSWD) (see Table 2), which are believed to remove blood stasis, clear collaterals, and nourish the blood, effectively alleviating symptoms such as testicular swelling, perineal swelling and pain, and bulging of testicular tendons in varicocele-associated male infertility. Using network pharmacology and molecular docking, they demonstrated that THSWD regulates varicocele-associated male infertility through multiple compounds and targets. Their findings indicate that the mechanism is closely linked to the inflammatory response, ROS damage, and blood vessel function. This study identified that THSWD may exert its therapeutic effects through the HIF-1, PI3K-Akt, and Relaxin signaling pathways. This study provides scientific evidence for subsequent experimental research and rational clinical administration of THSWD for the treatment of varicocele-associated male infertility.
In an experimental varicocele model study, Peng et al. [59] orally administered Zishen Yutai Pill (ZYP), which contains 15 traditional Chinese medicines (see Table 2). Their results demonstrated that ZYP significantly improved sperm motility reduced the sperm DNA fragmentation index and alleviated testicular tissue damage caused by experimental varicocele in rats. Furthermore, the mRNA and protein expression levels of nucleotide-binding oligomerization domain-like receptor family pyrin (NLRP) inflammasome components, specifically NLRP3, ASC, and caspase-1, were significantly downregulated in rats treated with ZYP. The serum level of IL-1β was also significantly reduced in ZYP-treated rats, suggesting that ZYP may act as an NLRP3 inhibitor, suppressing the IL-1β-dependent inflammatory response in the testicles of varicocele-affected rats. These data are similar with and support the previous study showed that the involved in the activation of potential inflammatory pathways, such as the NLRP3 pathway in varicocele induced infertility [37]. This animal study is noteworthy for its exploration of the immune and inflammatory factors associated with varicocele-related cryptozoospermia (see Table 1).
3.2. Oxidant Stress
Herbal therapy is increasingly being considered as a preventive measure against infertility, as these natural antioxidants can help mitigate the harmful effects of oxidative stress [60]. MOTILIPERM (MTP), a formulation made from a mixture of three medicinal plants (see Table 2), was developed to treat male infertility in South Korea. [61]. Karna et al. investigated the mechanisms underlying the effects of MTP on testicular dysfunction induced by immobilization stress in rats. They demonstrated that MTP could reduce oxidative stress by significantly increasing testicular superoxide dismutase (SOD) levels and decreasing malondialdehyde (MDA) and ROS/RNS levels. Additionally, they measured markers of testicular apoptosis and observed downregulation of cleaved caspase-3 and B-cell lymphoma 2 (Bcl-2)-associated X protein (Bax) levels, alongside increased levels of pro-caspase-3 and Bcl-2, as well as upregulated germ cell proliferation in the testes (see Table 1). This research group also demonstrated that MTP could restore testicular function by decreasing ROS-induced endoplasmic reticulum stress and germ cell apoptosis while upregulating testosterone synthesis in a varicocele-induced rat model [62] (see Table 1).
Qilin Pills (QLPs), a classic traditional Chinese medicine formula, contain 15 types of herbal medicines (see Table 2). Clinical trials have shown that QLPs effectively improve semen quality. Zhang et al. [63] demonstrated that QLPs have a therapeutic effect in a rat model of oligoasthenozoospermia by restored levels of FSH and LH, along with reduced levels of oxidative stress products (see Table 1).
Kyung-Ok-Ko (KOK) (see Table 2), also known as Qiong-yu-gao in China, is a well-known traditional medicinal formula in both Korean and Chinese medicine and has long been used to invigorate essential qi [64]. Some studies have demonstrated that KOK treatment significantly restores the morphological appearance of seminiferous tubules and epithelium. Additionally, a significant increase in sperm count and motility was observed in mice following heat exposure. [65]. KOK was also found to inhibit the expression of IL-1β, a proinflammatory cytokine, thus showing anti-inflammatory properties [66], and inhibit TNF-α secretion by inhibiting IL-1 secretion and has anti-inflammatory activity [67] (see Table 1). The above research indicates
that KOK improves heat-induced male infertility through its antioxidant, anti-inflammatory, anti-apoptotic, and protective effects on spermatogenesis.
3.3. IOA
In oriental medicine, IOA should be treated by regulating both Kidney-Yin and -Yang. The Wuzi Yanzong pill (WZYZP) (see Table 2) is one of the most commonly prescribed Chinese herbal formulas for treating male infertility. Originating from the renowned traditional Chinese medicine prescriptions of the Tang Dynasty, these ingredients have been widely used for an extended period to improve semen quality and address infertility. Some clinical studies [68,69,70] have indicated that the WZYZP exerts therapeutic effects in patients with IOA by significantly increasing sperm concentration, improving sperm motility, and decreasing the sperm DNA fragmentation index. Additionally, both in vivo and in vitro studies have demonstrated that WZYZP treatment can enhance germ cell proliferation, inhibit apoptosis, restore serum hormone levels, reduce oxidative stress-induced damage, promote spermatogenesis, and improve sperm cell quality in IOA model rats [71]. More importantly, these studies demonstrated that the WZYZP also suppressed TGF-β expression and activated the PI3K/AKT/mTOR signaling pathway, thereby promoting germ cell proliferation and inhibiting germ cell apoptosis [71]. (see Table 1). It is well established that mitochondria play a crucial role in sperm motility and fertilization, primarily through glycolysis and oxidative phosphorylation, which provide the energy necessary for sperm motility [72]. Mitochondrial membrane potential (MMP), directly linked to sperm motility, serves as an indicator of mitochondrial energy status [73]. Studies have also reported correlations between impaired mitochondrial function, reduced sperm motility, and decreased reproductive ability [74]. Lower MMP levels can lead to decreased sperm motility owing to reduced ATP production [75]. Shen et al. [70] found that the WZYZP restored spermatogenic functions in IOA rats, including increased sperm density, motility, viability, MMP levels, and testicular histopathology.
Several clinical trials have confirmed the efficacy of Yishentongluo decoction (YSTL) (see Table 2), as a complementary therapy for IOA. YSTL has been shown to be an effective prescription for treating male infertility associated with Kidney deficiency and blood stasis. Some studies have reported that the components of Cuscuta chinensis, Epimedium brevicornu, and Rehmannia glutinosa can reduce ROS, improve sperm motility, and significantly increase pregnancy rates [76]. Other active ingredients in herbal medicines contained in YSTL also provide a well-balanced supply of minerals, antioxidants, and nutrients [77,78]. Zhang et al. [79] provided initial evidence for the potential mechanisms by which YSTL improves sperm motility were explored based on the assessment of MMP in spermatozoa (see Table 1).
3.4. Anti-Cancer Treatment
Li et al. [79] investigated whether Qiangjing tablets (QJT) (see Table 2) could contribute to the recovery from BTB dysfunction in CP-treated rats. Their results showed that the expression levels of the aforementioned indicators returned to normal after treatment with QJT, highlighting the role of QJT in regulating the expression of key proteins in the BTB and p38 MAPK pathways, thereby mitigating CP-induced BTB dysfunction.
Sheng Jing Decoction (SJD), a traditional Chinese medicine (see Table 2), is primarily used to treat male infertility [80]. Yan et al. investigated the role of SJD in treating male infertility in ICR mice with CP-induced oligozoospermia [81]. Their data showed that SJD treatment increased the expression of the Sertoli cell marker GATA4 and germ cell marker TRA98 in CP-induced asthenozoospermic mice. In addition, sperm concentration and vitality were significantly enhanced following SJD treatment. Furthermore, this study demonstrated that SJD plays a crucial role in sustaining mitochondrial function and sperm motility by restoring MMP levels and preserving sperm plasma membrane integrity, both of which are impaired by CP induction (see Table 1).
A Korean research group investigated the therapeutic effects of MYOMI formulations on CP-induced male infertility in a mouse model. They demonstrated that treatment with MYOMI formulations reduced CP-induced apoptosis of germ cells, as indicated by the expression levels of Bax, Bcl-2, and caspase-3, as well as oxidative stress markers, including ROS and MDA (see Table 1). Among the formulations, MYOMI-7, a Korean herbal medicine (see Table 2), showed superior results in recovering CP-induced damage to the testes and improving fertility [82].
In pediatric patients treated with busulfan (BSF; Myleran, 1,4-butanediol dime thanesulfonate), an alkylating agent used for bone marrow transplantation [83], the recovery of spermatogenesis is a slow and progressive process [84,85,86,87]. Given that BSF induces death and depletion of spermatogonia [88,89,90], it has been widely utilized to prepare testicular recipients for spermatogonia stem cells transplantation [86,91,92]. The expression of proliferation-related genes was significantly decreased by BSF treatment while apoptotic genes (Fas, FasL, Caspase3, and Caspase8) were significantly increased. Furthermore, BSF-induced spermatogenic cell damage upregulated Toll-like receptors (TLR) 2 and TLR4 expressions in Sertoli cells and facilitated macrophage infiltration into the testes (see Figure 1). Despite considerable efforts to improve spermatogenesis following BSF disruption, there is currently no effective treatment for this condition. In Japan, traditional herbal medicines have been approved for clinical use by the National Health Insurance Program and are used to treat male infertility. One such herbal medicine, Goshajinkigan (TJ107), composed of 10 herbal ingredients (see Table 2), has been widely used in Japan and China to treat conditions such as meralgia, lower back pain, numbness, and neuropathy, particularly in elderly patients. Recently, we demonstrated that TJ107 was able to completely recover the injured seminiferous epithelium by normalizing macrophage migration and reducing the expression of TLR 2 and 4, and to promote recovery from severe aspermatogenesis following BSF treatment in mice [93,94] (see Table 1 and Figure 1). This suggests that TJ107 has a therapeutic effect on BSF-induced aspermatogenesis [93,94] (see Figure 1).
Importantly, our examination further demonstrated that impaired reproductive function induced by cancer treatment, including chemotherapy and radiotherapy, is associated with various pathophysiological conditions [17]. In particular, examination detected that antigerm cell antibody production and inter-Sertoli tight junction barrier disruption was induced by 6Gy of total body irradiation. The breakdown of the BTB tight junction due to irradiation may cause repeated leakage of germ cell autoantigens within the BTB, leading to a continuous supply of autoantigens for immune stimulation. This process results in the production of ASA and prolongs testicular inflammation [17]. Supplementation with TJ107 restored disrupted inter-Sertoli tight junctions by normalizing the expression of claudin-11, occludin, and ZO-1, while also reducing serum anti-sperm antibody levels [95] (see Table 1 and Figure 1). Our studies demonstrated that impaired reproductive function induced by cancer treatments including chemotherapy and radiotherapy related with the different immune-pathophysiological conditions can be cured by TJ107. We will examine the effects of the other traditional Japanese medicine such as Hachimijiogan and Hochuekkito on oncologic aspermatogenesis and evaluate the efficacy of polyherbal formulation for improving fertility after cancer treatment in the next experiments.
4. Cons Related to the Oriental Medicines Treatment
Oriental medicine has a long history. The history of medical development shows that oriental medicine, or traditional medicine, was born through medical practice during the times when science and technology were immature and underdeveloped. So oriental medicine is primarily applied as a clinical treatment, and its chemical and pharmacological foundations are not well understood in most cases. Although above research mentioned in this review provide some preliminary insights into the pharmacological basis and molecular immune mechanisms of oriental medicines for treating male infertility, further experimental analysis and research are required to validate these findings.
5. Conclusions
Oriental medicine has gained attention and is increasingly being utilized as a complementary therapy in infertility. The limited information regarding the underlying immune response and understanding the mechanisms of male infertility is essential for advancing treatment. From the above limited reported data, further experimental research on oriental medicines may verify various abnormalities in immune-related cells or active molecules with infertility and molecular immune mechanisms underlying these findings. Empirical oriental medicine treatment, which is prescribed based on the experience of clinicians, is expected to create an academic foundation for oriental medicine treatment for male infertility, and collaboration between modern medicine and traditional medicine should be fostered, to promote the advancement of knowledge and patient care.
Abbreviations: acute myelogenous leukemia: AML; anti-sperm antibodies: ASA; B-cell lymphoma 2: Bcl-2; Bcl-2 associated X protein: Bax; busulfan: BSF; blood–testis barrier: BTB; cyclophosphamide: CP; estrogen receptor: ER; Fibrous actin: F-actin; Fas ligand: Fas-L; follicle-stimulating hormone: FSH; gonadotropin-releasing hormone: GnRH; intracytoplasmic sperm injection: ICSI; interferon-γ: IFN-γ; interleukin: IL; luteinizing hormone: LH; idiopathic oligoasthenozoospermia: IOA; macrophage chemotactic protein: MCP; malondialdehyde: MDA; mitochondrial membrane potential: MMP; nucleotide-binding oligomerization domain-like receptor family pyrin: NLRP; nitric oxide synthase: NOS; reactive nitrogen species: RNS; reactive oxygen species: ROS; Selective estrogen receptor modulators: SERMs; superoxide dismutase: SOD; transforming growth factor β: TGF-β;tool-like receptor: TLR; tumor necrosis factor α: TNF-α.
Author Contributions
Ning Qu was responsible for the conceptualization, methodology, and overall execution of the research presented in this manuscript. Additionally, Ning Qu wrote and revised the manuscript, ensuring the accuracy and integrity of the work. She also prepared the figures and tables and coordinated the submission process.
Funding
This work was supported by Grants-in-Aid for General Science Research (C: 19K07876 and C:23K06875) from the Ministry of Education, Science, Sports, and Culture of Japan.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Gosha-jinki-gan extracts were manufactured by Tsumura and Co. (Tokyo, Japan). The author wishs to acknowledge the Department of Anatomy and the Department of Immunoregulation, Institute of Medical Science, Tokyo Medical University, and the Department of Anatomy and the Support Center for Medical Research and Education, Tokai University. The author would like to thank Editage (www.editage.jp) for English language editing.
Conflicts of Interest
The funders had no role in the study design; collection, analyses, or interpretation of data; writing of the manuscript; or decision to publish the results.
References
- Collins, J.A. Male infertility: the interpretation of the diagnostic assessment. In The Year Book of Infertility, Mishell, D.R., Paulsen, C.A., Lobo, R.A., Eds.; Year Book Medical Publishers Inc.: Chicago, 1989; Vol. 1989; p. 45.
- Rowe, P.J. WHO Manual for the Standardized Investigation, Diagnosis and Management of the Infertile Male, Cambridge Uni Varsity Press; Cambridge, UK, 2000.
- Barratt, C.L.; Björndahl, L.; De Jonge, C.J.; Lamb, D.J.; Osorio Martini, F.; McLachlan, R.; Oates, R.D.; van der Poel, S.; St John, B.; Sigman, M.; et al. The diagnosis of male infertility: an analysis of the evidence to support the development of global WHO guidance-challenges and future research opportunities. Human Reproduction Update 2017, 23, 660–680. [Google Scholar] [CrossRef]
- Dohle, G.R.; Halley, D.J.J.; Van Hemel, J.O.; van den Ouwel, A.M.; Pieters, M.H.; Weber, R.F.; Govaerts, L.C. Genetic risk factors in infertile men with severe oligozoospermia and azoospermia. Hum Reprod 2002, 17, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Kidd, S.A.; Eskenazi, B.; Wyrobek, A.J. Effects of male age on semen quality and fertility: a review of the literature. Fertil Steril 2001, 75, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Oliva, A.; Spira, A.; Multigner, L. Contribution of environmental factors to the risk of male infertility. Hum Reprod 2001, 16, 1768–1776. [Google Scholar] [CrossRef] [PubMed]
- Machen, G.L.; Sandlow, J.I. Causes of male infertility. Male Infertil Springer 2020, 3–14. [Google Scholar]
- Jo, J.; Kang, M.J. Successful Treatment of Oligoasthenozoospermia Using Traditional Korean Medicine Resulting in Spontaneous Preg Nancy: Two Case Reports; Vol. 12; Explore Publications, 2016; pp. 136–138.
- Tournaye, H. Male factor infertility and ART. Asian J Androl 2012, 14, 103–108. [Google Scholar] [CrossRef]
- Rhoton-Vlasak, A. Drury KC. ART and its impact on male infertility management. Male Infertility; Springer: New York, 2012.
- Smith, R.P.; Lipshultz, L.I.; Kovac, J.R. Stem cells, gene therapy, and advanced medical management hold promise in the treatment of male infertility. Asian J Androl 2016, 18, 364. [Google Scholar] [CrossRef]
- Zheng, L.I.; Wu, C.G.; Jun, S.X.; et al. A controlled randomized trial of the use of combined L-carnitine and acetyl-L-carnitine treatment in men with oligoasthenozoospermia. J Androl 2005, 11, 761–764. [Google Scholar]
- Schwarzstein, L.; Aparicio, N.J.; Schally, A.V. D-Tryptophan-6-luteinizing hormone-releasing hormone in the treatment of normogonadotropic oligoasthenozoospermia. Int J Androl 2010, 5, 171–178. [Google Scholar] [CrossRef]
- Jiang, D.; Coscione, A.; Li, L.; Zeng, B.-Y. Effect of Chinese herbal medicine on male infertility. Int Rev Neurobiol 2017, 135, 297–311. [Google Scholar] [CrossRef]
- Head, J.R.; Billingham, R.E. Immune privilege in the testis. II. Evaluation of potential local factors. Transplantation 1982, 40, 269–295. [Google Scholar] [CrossRef] [PubMed]
- Bhushan, S.; Meinhardt, A. The macrophages in testis function. J. Reprod. Immunol. 2017, 119, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Qu, N.; Itoh, M.; Sakabe, K. Effects of chemotherapy and radiotherapy on spermatogenesis: the role of testicular immunology. Int J Mol Sci 2019, 20, E957. [Google Scholar] [CrossRef]
- Miner, S.A.; Robins, S.; Zhu, Y.J.; Keeren, K.; Gu, V.; Read, S.C.; Zelkowitz, P. Evidence for the use of complementary and alternative medicines during fertility treatment: a scoping review. BMC Complement. Altern. Med. 2018, 18, 158. [Google Scholar] [CrossRef]
- Amory, J.K.; Ostrowski, K.A.; Gannon, J.R.; Berkseth, K.; Stevison, F.; Isoherranen, N.; Muller, C.H.; Walsh, T. Isotretinoin administration improves sperm production in men with infertility from oligoasthenozoospermia: a pilot study. Andrology 2017, 5, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- WorldHealthOrganization. WHOLaboratoryManualfortheExaminationandProcessingofHumanSemen; WorldHealthOrganization: Geneva, Switzerland, 2021; Volume 6, pp. 1–276. [Google Scholar]
- Jung, A.; Schuppe, H.C. Influence of genital heat stress on semen quality in humans. Andrologia 2007, 39, 203–215. [Google Scholar] [CrossRef]
- Castleton, P.E.; Deluao, J.C.; Sharkey, D.J.; McPherson, N.O. Measuring reactive oxygen species in Semen for Male Preconception Care: A Scientist Perspective. Antioxidants (Basel) 2022, 11, 264. [Google Scholar] [CrossRef]
- O’Flaherty, C. Reactive oxygen species and male fertility. Antioxidants (Basel) 2020, 9, 287. [Google Scholar] [CrossRef]
- Alahmar, A.T. Role of oxidative stress in male infertility: an updated review. J Hum Reprod Sci 2019, 12, 4–18. [Google Scholar] [CrossRef]
- Agarwal, A.; Parekh, N.; Panner Selvam, M.K.; Henkel, R.; Shah, R.; Homa, S.T.; Ramasamy, R.; Ko, E.; Tremellen, K.; Esteves, S.; et al. Male oxidative stress infertility (MOSI): proposed terminology and clinical practice guidelines for management of idiopathic male infertility. World J Mens Health 2019, 37, 296–312. [Google Scholar] [CrossRef]
- Walczak-Jedrzejowska, R.; Wolski, J.K.; Slowikowska-Hilczer, J. The role of oxidative stress and antioxidants in male fertility. Cent Eur J Urol 2013, 66, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Mieusset, R.; Bujan, L. Testicular heating and its possible contributions to male infertility: a review. Int J Androl 1995, 18, 169–184. [Google Scholar] [CrossRef]
- Ren, L.; Medan, M.S.; Ozu, M.; Li, C.; Watanabe, G.; Taya, K. Effects of experimental cryptorchidism on sperm motility and testicular endocrinology in adult male rats. J Reprod Dev 2006, 52, 219–228. [Google Scholar] [CrossRef]
- Setchell, B.P. The effects of heat on the testes of mammals. Anim Reprod 2006, 3, 81–91. [Google Scholar]
- Mahfouz, R.Z.; du Plessis, S.S.; Aziz, N.; Sharma, R.; Sabanegh, E.; Agarwal, A. Sperm viability, apoptosis, and intracellular reactive oxygen species levels in human spermatozoa before and after induction of oxidative stress. Fertil Steril 2010, 93, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Esteves, S.C.; Agarwal, A. Novel concepts in male infertility. Int Braz J Urol 2011, 37, 5–15. [Google Scholar] [CrossRef]
- Wright, E.J.; Young, G.P.; Goldstein, M. Reduction in testicular temperature after varicocelectomy in infertile men. Urology 1997, 50, 257–259. [Google Scholar] [CrossRef]
- Allamaneni, S.S.; Naughton, C.K.; Sharma, R.K.; Thomas, A.J., Jr.; Agarwal, A. Increased seminal reactive oxygen species levels in patients with varicoceles correlate with varicocele grade but not with testis size. Fertil Steril. 2004, 82, 1684–1686. [Google Scholar] [CrossRef]
- Will, M.A.; Swain, J.; Fode, M.; Sonksen, J.; Christman, G.M.; Ohl, D. The great debate: varicocele treatment and impact on fertility. Fertil Steril 2011, 95, 841–852. [Google Scholar] [CrossRef]
- Romeo, C.; Santoro, G. Varicocele Infertil Why Prev? J Endocrinol Invest. 2009, 32, 559.e561. [Google Scholar] [CrossRef]
- Dubin, L.; Amelar, R.D. Varicocelectomy as therapy in male infertility: a study of 504 cases. Fertil Steril 1975, 26, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Su, Y.; Xu, J.; Hu, Z.; Zhao, K.; Liu, C.; Zhang, H. Varicocele-mediated male infertility: from the perspective of testicular immunity and inflammation. Front Immunol 2021, 12, 729539. [Google Scholar] [CrossRef] [PubMed]
- Vandekerckhove, P.; Lilford, R.; Vail, A.; Hughes, E. Clomiphene or tamoxifen for idiopathic oligo/asthenospermia. Cochrane Database Syst Rev 2000, 1996, CD000151. [Google Scholar] [CrossRef]
- Razi, M.; Tavalaee, M.; Sarrafzadeh-Rezaei, F.; Moazamian, A.; Gharagozloo, P.; Drevet, J.R.; Nasr-Eshafani, M.-H. Varicocoele and oxidative stress: new perspectives from animal and human studies. Andrology 2021, 9, 546–558. [Google Scholar] [CrossRef]
- Leung, W.; Hudson, M.M.; Strickland, D.K.; Phipps, S.; Srivastava, D.K.; Ribeiro, R.C.; Rubnitz, J.E.; Sandlund, J.T.; Kun, L.E.; Bowman, L.C.; et al. Late effects of treatment in survivors of childhood acute myeloid leukemia. J Clin Oncol 2000, 18, 3273–3279. [Google Scholar] [CrossRef]
- Thomson, A.B.; Campbell, A.J.; Irvine, D.C.; Anderson, R.A.; Kelnar, C.J.H.; Wallace, W.H.B. Semen quality and spermatozoal DNA integrity in survivors of childhood cancer: a case-control study. Lancet 2002, 360, 361–367. [Google Scholar] [CrossRef]
- Meistrich, M.L.; Wilson, G.; Brown, B.W.; da Cunha, M.F.; Lipshultz, L.I. Impact of cyclophosphamide on long-term reduction in sperm count in men treated with combination chemotherapy for Ewing and soft tissue sarcomas. Cancer 1992, 70, 2703–2712. [Google Scholar] [CrossRef] [PubMed]
- Speiser, B.; Rubin, P.; Casarett, G. Aspermia following lower truncal irradiation in Hodgkin’s disease. Cancer 1973, 32, 692–698. [Google Scholar] [CrossRef]
- Anserini, P.; Chiodi, S.; Spinelli, S.; Costa, M.; Conte, N.; Copello, F.; Bacigalupo, A. Semen analysis following allogeneic bone marrow transplantation. Additional data for evidence-based counselling. Bone Marrow Transplant 2002, 30, 447–451. [Google Scholar] [CrossRef]
- Ghobadi, E.; Moloudizargari, M.; Asghari, M.H.; Abdollahi, M. The mechanisms of cyclophosphamide-induced testicular toxicity and the protective agents. Expert Opin Drug Met. 2017, 13, 525–536. [Google Scholar] [CrossRef]
- Dietze, R.; Shihan, M.; Stammler, A.; Konrad, L.; Scheiner-Bobis, G. Cardiotonic steroid ouabain stimulates expression of blood-testis barrier proteins claudin-1 and −11 and formation of tight junctions in Sertoli cells. Mol Cell Endocrinol 2015, 405, 1–13. [Google Scholar] [CrossRef]
- Urriola-Muñoz, P.; Lagos-Cabré, R.; Moreno, R.D. A mechanism of male germ cell apoptosis induced by bisphenol-A and nonylphenol involving ADAM17 and p38 MAPK activation. PLOS ONE 2014, 9, e113793. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; You, Y.; Zhang, P.; Huang, X.; Dong, L.; Yang, F.; Yu, X.; Chang, D. Qiangjing tablets repair blood-testis barrier dysfunction in rats via regulating oxidative stress and p38 MAPK pathway. BMC Complement Med Ther 2022, 22, 133. [Google Scholar] [CrossRef]
- Ward, J.A.; Robinson, J.; Furr, B.J.; Shalet, S.M.; Morris, I.D. Protection of spermatogenesis in rats from the cytotoxic procarbazine by the depot formulation of Zoladex, a gonadotropin-releasing hormone agonist. Cancer Res 1990, 50, 568–574. [Google Scholar]
- Johnson, D.H.; Linde, R.; Hainsworth, J.D.; Vale, W.; Rivier, J.; Stein, R.; Flexner, J.; Van Welch, R.; Greco, F.A. Effect of a luteinizing hormone releasing hormone agonist given during combination chemotherapy on posttherapy fertility in male patients with lymphoma: preliminary observations. Blood 1985, 65, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Brinster, R.L.; Zimmermann, J.W. Spermatogenesis following male germ-cell transplantation. Proc Natl Acad Sci U S A 1994, 91, 11298–11302. [Google Scholar] [CrossRef] [PubMed]
- Tempest, H.G.; Homa, S.T.; Routledge, E.J.; Garner, A.; Zhai, X.P.; Griffin, D.K. Plants used in Chinese medicine for the treatment of male infertility possess antioxidant and anti-oestrogenic activity. Syst Biol Reprod Med 2008, 54, 185–195. [Google Scholar] [CrossRef]
- Yun, S.J.; Bae, G.S.; Park, J.H.; Song, T.H.; Choi, A.; Ryu, B.Y.; Pang, M.G.; Kim, E.J.; Yoon, M.; Chang, M.B. Antioxidant effects of cultured wild ginseng root extracts on the male reproductive function of boars and guinea pigs. Anim Reprod Sci 2016, 170, 51–60. [Google Scholar] [CrossRef]
- Park, H.J.; Choe, S.; Park, N.C. Effects of Korean red ginseng on semen parameters in male infertility patients: A randomized, placebo-controlled, double-blind clinical study. Chin J Integr Med 2016, 22, 490–495. [Google Scholar] [CrossRef]
- Hu, M.; Zhang, Y.; Ma, H.; Ng, E.H.Y.; Wu, X.K. Eastern medicine approaches to male infertility. Semin Reprod Med 2013, 31, 301–310. [Google Scholar] [CrossRef]
- Yang, K.; Li, S.G.; Zhang, T.Y.; Dong, P.P.; Zeng, Q.Q. Runjing Extract Promotes Spermatogenesis in Rats with Ornidazole-Induced Oligoasthenoteratozoospermia through Extracellular Signal-Regulated Kinase Signalling, and Regulating Vimentin Expression. J. Tradit. Chin. Med. 2021, 41, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Huang, Z.; Zheng, H.; Zhu, Z.; Yang, H.; Liu, X.; Pang, T.; He, L.; Lin, H.; Hu, L.; et al. Jiawei Runjing decoction improves spermatogenesis of cryptozoospermia with varicocele by regulating the testicular microenvironment: two-center prospective cohort study. Front Pharmacol 2022, 13, 945949. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Lan, X.; Chen, X.; Wu, Q.; Yang, Y.; Wang, Y. Researching the molecular mechanisms of Taohong Siwu Decoction in the treatment of varicocele-associated male infertility using network pharmacology and molecular docking: a review. Medicine 2023, 102, e34476. [Google Scholar] [CrossRef]
- Peng, M.; Wang, W.; Zhu, W.; Bai, Y.; Ning, N.; Huang, Q.; Pang, X.; Zhou, J.; Zhang, H.; Zhao, K. Zishen Yutai Pill improves sperm quality and reduces testicular inflammation in experimental varicocele rats. Heliyon 2023, 9, e17161. [Google Scholar] [CrossRef]
- SenGupta, P.; Agarwal, A.; Pogrebetskaya, M.; Roychoudhury, S.; Durairajanayagam, D.; Henkel, R. Role of Withania somnifera (Ashwagandha) in the management of male infertility. Reprod Biomed Online 2018, 36, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Karna, K.K.; Soni, K.K.; You, J.H.; Choi, N.Y.; Kim, H.K.; Kim, C.Y.; Lee, S.W.; Shin, Y.S.; Park, J.K. MOTILIPERM ameliorates immobilization stress-induced testicular dysfunction via inhibition of oxidative stress and modulation of the Nrf2/HO-1 pathway in SD rats. Int J Mol Sci 2020, 21, 4750. [Google Scholar] [CrossRef]
- Soni, K.K.; Zhang, L.T.; Choi, B.R.; Karna, K.K.; You, J.H.; Shin, Y.S.; Lee, S.W.; Kim, C.Y.; Zhao, C.; Chae, H.J.; et al. Protective effect of motiliperm in varicocele-induced oxidative injury in rat testis by activating phosphorylated inositol requiring kinase 1alpha (p-IRE1alpha) and phosphorylated c-Jun N-terminal kinase (p-JNK) pathways. Pharm Biol 2018, 56, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Fu, L.; An, Q.; Hu, W.; Liu, J.; Tang, X.; Ding, Y.; Lu, W.; Liang, X.; Shang, X.; et al. Effects of Qilin pills on spermatogenesis, reproductive hormones, oxidative stress, and the TSSK2 gene in a rat model of oligoasthenospermia. BMC Complement Med Ther 2020, 20, 42. [Google Scholar] [CrossRef]
- Kim, M.D. The literature study on the efficacy and manufacturing process of gyeongoggo. J Orient Med Clas Sics 2011, 24, 51–64. [Google Scholar]
- Hwang, D.-S.; Kim, H.G.; Park, S.; Hong, N.D.; Ryu, J.H.; Oh, M.S. Effect of a traditional herbal prescription, Kyung-ok-Ko, on male mouse spermatogenic ability after heat-induced damage. Evid Based Complement Alternat Med 2015, 2015, 950829. [Google Scholar] [CrossRef]
- Cai, M.; Shin, B.Y.; Kim, D.H.; Kim, J.M.; Park, S.J.; Park, C.S.; Won, D.H.; Hong, N.D.; Kang, D.H.; Yutaka, Y.; et al. Neuroprotective effects of a traditional herbal prescription on transient cerebral global ischemia in gerbils. J Ethnopharmacol 2011, 138, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.M.; An, C.S.; Jung, K.Y.; Choo, Y.K.; Park, J.K.; Nam, S.Y. Rehmannia glutinosa inhibits tumour necrosis factor-α and interleukin-1 secretion from mouse astrocytes. Pharmacol Res 1999, 40, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.P.; Shi, X.; Kong, G.W.S.; Wang, C.C.; Wu, J.C.Y.; Lin, Z.X.; Li, T.C.; Chan, D.Y.L. The therapeutic effects of a traditional Chinese medicine formula Wuzi Yanzong Pill for the treatment of oligoasthenozoospermia: a meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med 2018, 2018, 2968025. [Google Scholar] [CrossRef]
- Li, Y.; Xue, Y.; Bao, B.; Wang, J.; Dai, H.; Gong, X.; Zheng, W.; Li, Y.; Zhang, B. Effectiveness comparison of a Chinese dicitraditionalmene formula Wuzi Yanzong Pill and its analogous prescriptions for the treatment of oligoasthenozoospermia: A systematic review and meta-analysis protocol. Medicine 2019, 98, e15594. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Zhang, Z.; Tong, K.; Wang, C.; Wang, S.; Zhao, P.; Gu, M.; Hu, J.; Tang, Y.; Liu, Z. Mechanism of action of Wuzi Yanzong pill in the treatment of oligoasthenozoospermia in rats determined via serum metabolomics. J Trad Chin Med Sci 2024, 11, 180–190. [Google Scholar] [CrossRef]
- Chen, W.Q.; Wang, B.; Ding, C.F.; Wan, L.Y.; Hu, H.M.; Lv, B.D.; Ma, J.X. In vivo and in vitro protective effects of the Wuzi Yanzong pill against experimental spermatogenesis disorder by promoting germ cell proliferation and suppressing apoptosis. J Ethnopharmacol 2021, 280, 114443. [Google Scholar] [CrossRef]
- Condorelli, R.A.; Barbagallo, F.; Calogero, A.E.; Cannarella, R.; Crafa, A.; La Vignera, S. D-Chiro-inositol improves sperm mitochondrial membrane potential: in vitro evidence. J Clin Med 2020, 9, 1373. [Google Scholar] [CrossRef]
- Agnihotri, S.K.; Agrawal, A.K.; Hakim, B.A.; Vishwakarma, A.L.; Narender, T.; Sachan, R.; Sachdev, M. Mitochondrial membrane potential (MMP) regulates sperm motility. In Vitro Cell Dev Biol Anim 2016, 52, 953–960. [Google Scholar] [CrossRef]
- Paoli, D.; Gallo, M.; Rizzo, F.; Baldi, E.; Francavilla, S.; Lenzi, A.; Lombardo, F.; Gandini, L. Mitochondrial membrane potential profile and its correlation with increasing sperm motility. Fertil Steril 2011, 95, 2315–2319. [Google Scholar] [CrossRef]
- Alamo, A.; De Luca, C.; Mongioì, L.M.; Barbagallo, F.; Cannarella, R.; La Vignera, S.; Calogero, A.E.; Condorelli, R.A. Mitochondrial membrane potential predicts 4-hour sperm motility. Biomedicines 2020, 8, 196. [Google Scholar] [CrossRef]
- Wang, S.C.; Wang, S.C.; Li, C.J.; Lin, C.H.; Huang, H.L.; Tsai, L.M.; Chang, C.H. The therapeutic effects of traditional Chinese medicine for poor semen quality in infertile males. J Clin Med 2018, 7, 239. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Sun, Z.X.; Zhao, S.P.; Zhang, X.H.; Chen, J.S.; Wang, R.; Men, B. Yishen Tongluo Recipe combined with minimally invasive surgery for the treatment of varicocele-associated asthenospermia. Zhonghua Nan Ke Xue 2020, 26, 341–345. [Google Scholar]
- Idänpään-Heikkilä, J.E. Ethical principles for the guidance of physicians in medical research–the Declaration of Helsinki. Bull World Health Organ 2001, 79, 279. [Google Scholar] [PubMed]
- Zhang, Q.; Fan, L.; Li, F.; Sun, Z.; Zhang, C.; Chen, R. Yishentongluo decoction in treatment of idiopathic asthenozoospermia infertility: study protocol for a randomized controlled trial. Medicine 2020, 99, e22662. [Google Scholar] [CrossRef]
- Yan, G.; Tian, F.; Liu, P.; et al. Sheng Jing decoction as a traditional Chinese medicine prescription can promote spermatogenesis and increase sperm motility (Research Square), 2021. Available online: https://www.researchsquare.com/article/rs-167175/v1.
- Yan, G.; Tian, F.; Liu, P.; Sun, J.; Mao, J.; Han, W.; Mo, R.; Guo, S.; Yu, Q.Yu.S. Sheng Jing Decoction can promote spermatogenesis and increase sperm motility of the oligozoospermia mouse model. Evid Based Complement Alternat Med 2021, 2021, 3686494. [Google Scholar] [CrossRef]
- Park, A.; Yang, Y.; Jo, J.; Yoon, S.R. Modified MYOMI-14 Korean herbal formulations have protective effects against cyclophosphamide-induced male infertility in mice. Andrologia 2021, 53, e14025. [Google Scholar] [CrossRef]
- Kadam, P.; Van Saen, D.; Goossens, E. Can mesenchymal stem cells improve spermatogonial stem cell transplantation efficiency? Andrology 2017, 5, 2–9. [Google Scholar] [CrossRef]
- Wilhelmsson, M.; Vatanen, A.; Borgström, B.; Gustafsson, B.; Taskinen, M.; Saarinen-Pihkala, U.M.; Winiarski, J.; Jahnukainen, K. Adult testicular volume predicts spermatogenetic recovery after allogeneic HSCT in childhood and adolescence. Pediatr Blood Cancer 2014, 61, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Sanderson, B.J.; Shield, A.J.; Sanderson, B.J.S. Mutagenic damage to mammalian cells by therapeutic alkylating agents. Mutat Res 1996, 355, 41–57. [Google Scholar] [CrossRef]
- Grigg, A.P.; McLachlan, R.; Zaja, J.; Szer, J. Reproductive status in long-term bone marrow transplant survivors receiving busulfan-cyclophosphamide (120 mg/kg). Bone Marrow Transplant 2000, 26, 1089–1095. [Google Scholar] [CrossRef]
- Pfitzer, C.; Orawa, H.; Balcerek, M.; Langer, T.; Dirksen, U.; Keslova, P.; Zubarovskaya, N.; Schuster, F.R.; Jarisch, A.; Strauss, G.; Borgmann-Staudt, A.; et al. Dynamics of fertility impairment and recovery after allogeneic haematopoietic stem cell transplantation in childhood and adolescence: results from a longitudinal study. J Cancer Res Clin Oncol 2015, 141, 135–142. [Google Scholar] [CrossRef]
- Bucci, L.R.; Meistrich, M.L. Effects of busulfan on murine spermatogenesis: cytotoxicity, sterility, sperm abnormalities, and dominant lethal mutations. Mutat Res 1987, 176, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Ok, D.W.; Kwon, D.N.; Il Chung, J.I.; Kim, H.C.; Yeo, S.M.; Kim, T.; Seo, H.G.; Kim, J.H. Murine male germ cell apoptosis induced by busulfan treatment correlates with loss of c-kit-expression in a Fas/FASL- and p53-independent manner. FEBS Lett 2004, 575, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Vasiliausha, S.R.; Beltrame, F.L.; de Santi, F.; Cerri, P.S.; Caneguim, B.H.; Sasso-Cerri, E. Seminiferous epithelium damage after short period of busulphan treatment in adult rats and vitamin B12 efficacy in the recovery of spermatogonial germ cells. Int J Exp Pathol 2016, 97, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Zohni, K.; Zhang, X.; Tan, S.L.; Chan, P.; Nagano, M.C. The efficiency of male fertility restoration is dependent on the recovery kinetics of spermatogonial stem cells after cytotoxic treatment with busulfan in mice. Hum Reprod 2012, 27, 44–53. [Google Scholar] [CrossRef]
- Qin, Y.; Liu, L.; He, Y.; Ma, W.; Zhu, H.; Liang, M.; Hao, H.; Qin, T.; Zhao, X.; Wang, D. Testicular injection of busulfan for recipient preparation in transplantation of spermatogonial stem cells in mice. Reprod Fertil Dev 2016, 28, 1916–1925. [Google Scholar] [CrossRef]
- Qu, N.; Kuramasu, M.; Hirayanagi, Y.; Nagahori, K.; Hayashi, S.; Ogawa, Y.; Terayama, H.; Suyama, K.; Naito, M.; Sakabe, K.; et al. Gosha-Jinki-Gan recovers spermatogenesis in mice with busulfan-induced aspermatogenesis. Int J Mol Sci 2018, 19, E2606. [Google Scholar] [CrossRef]
- Qu, N.; Nagahori, K.; Kuramasu, M.; Ogawa, Y.; Suyama, K.; Hayashi, S.; Sakabe, K.; Itoh, M. Effect of Gosha-Jinki-Gan on levels of specific mRNA transcripts in mouse testes after busulfan treatment. Biomedicines 2020, 8, 432. [Google Scholar] [CrossRef]
- Takahashi, K.; Nagahori, K.; Qu, N.; Kuramasu, M.; Hirayanagi, Y.; Hayashi, S.; Ogawa, Y.; Hatayama, N.; Terayama, H.; Suyama, K.; et al. The effectiveness of traditional Japanese medicine Goshajinkigan in irradiation-induced aspermatogenesis in mice. BMC Complement Altern Med 2019, 19, 362. [Google Scholar] [CrossRef]
Figure 1.
Different immune mechanisms of Goshajinkigan in infertility after anti-cancer treatment. ↑ indicates an increase and ↓ indicates a decrease. Abbreviations: Goshajinkigan: TJ107; macrophage chemotactic protein: MCP; Toll-like receptors: TLR.
Figure 1.
Different immune mechanisms of Goshajinkigan in infertility after anti-cancer treatment. ↑ indicates an increase and ↓ indicates a decrease. Abbreviations: Goshajinkigan: TJ107; macrophage chemotactic protein: MCP; Toll-like receptors: TLR.
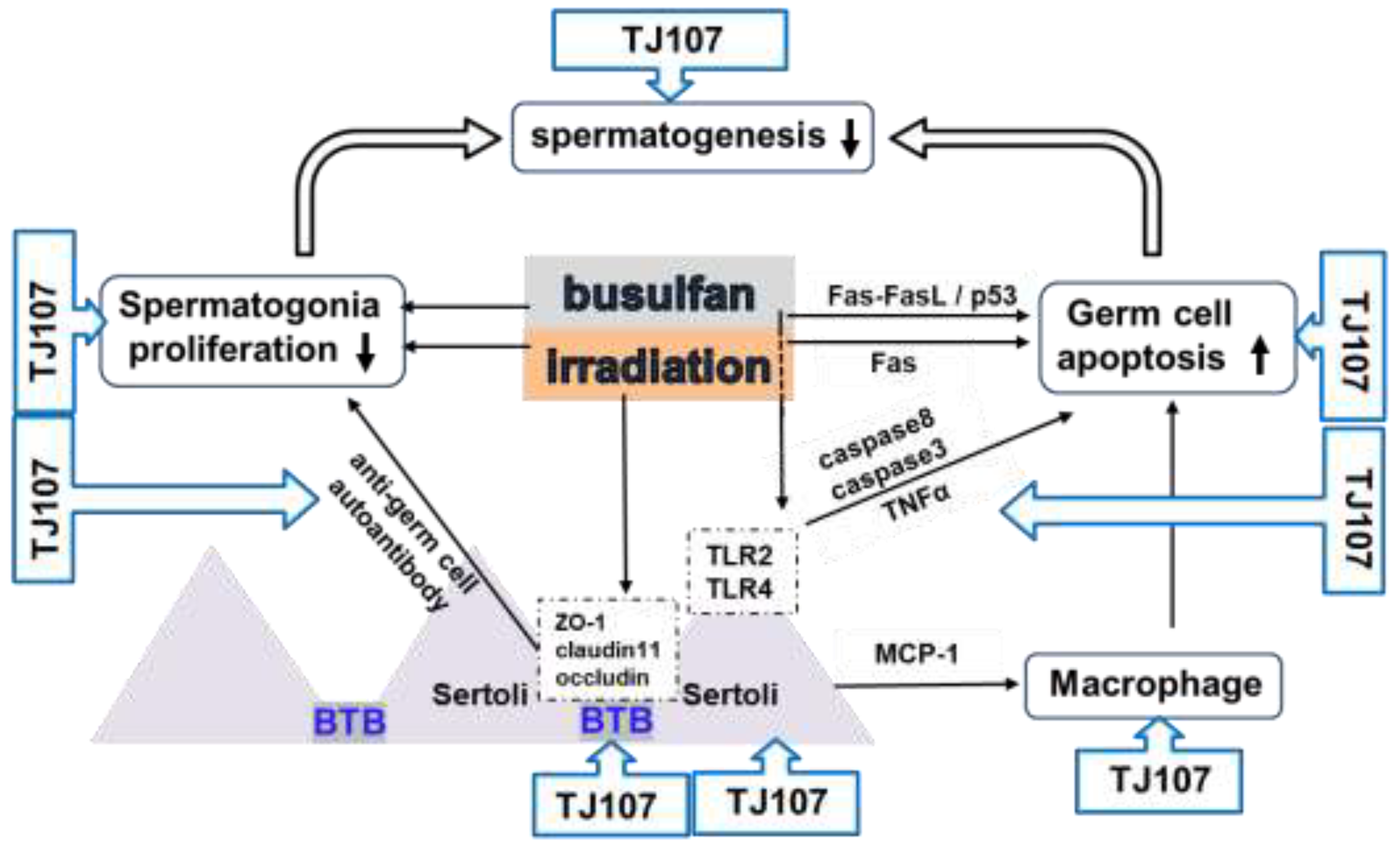

Table 1.
Immune factors in the normal and infertile testes.
|
Immuno- suppressive Factors in Normal Testis |
Anti-cancer treatment |
Varicocele |
Oxidant stress |
IOA | |
| germ | TGF-β | ↑37 | ↑22 | ↑70 | |
| cells | Fas-L | ↑82,93,94 | ↑or (-)37 | ↑70 | |
| IFN-γ | ↑37 | ||||
| TNF-α | ↑82,93,94 | ↑37 | ↑22,61 | ||
| Fas ↑ Bax ↑82 | Fas ↑37 | caspase3 ↑61 | PI3K/AKT/mTOR↓70 | ||
| Caspase3,8 ↑82,93,95 | Caspase1 ↑59 | Bax ↑ p53↑29,30,62 | ROS↑75 | ||
| p53-ROS↑82 | SOD↑29 | ||||
| Sertoli | activin | ||||
| cells | inhibin | ||||
| IL-6 | ↑37 | ↑67 | |||
| Fas-L | ↑93,94 | ↑70 | |||
| TNF-α | ↑82,93,94 | ↑37 | ↑67 | ||
| MCP-1↑93,94 | claudin-11↓37 | ||||
| TLR2,4↑93,94 | |||||
| Occludin↓48,95 | |||||
| ZO-1↓48,95 | |||||
| F-actin↓48 | |||||
| Leydig | testosterone | ↓48 | ↓37,38 | ↓62 | ↓20 |
| cells | portein s | ||||
| Fas-L | |||||
| IL-10 | ↑37 | ||||
| TGF-β | ↑37 | ||||
| Bcl-2↑82 | |||||
| Testicular | IL-10 | ↑37 | ↑70 | ||
| macro- | IFN-γ | ↑37 | |||
| phages | IL-6 | ↑37 | ↑29,30 | ||
| TNF-α | ↑93,94 | ↑37 | ↑67 | ||
| macrophage infiltration ↑93,94 |
IL-1β ↑37, 59 | IL-1β↑67 | |||
| Others | FSH, LH↓51 | ASA↑37 | ROS/NOS↑22, 29,30,60-63 | MMP ↓69,72,74,78 | |
| MMP ↓81 | ROS↑33,58 | FSH, LH↓63 | |||
| ROS, MDA↑51,82 | FSH ↑57 | ||||
| ASA↑17,95 | NLRP3↑37, 59 |
↑ indicates an increase and ↓ indicates a decrease. Abbreviations: anti-sperm antibodies: ASA; B-cell lymphoma 2: Bcl-2; Bcl-2 associated X protein: Bax; Fas ligand: Fas-L; follicle-stimulating hormone: FSH; interferon-γ: IFN-γ; interleukin: IL; luteinizing hormone: LH; macrophage chemotactic protein: MCP; malondialdehyde: MDA; mitochondrial membrane potential: MMP; nucleotide-binding oligomerization domain-like receptor family pyrin: NLRP; nitric oxide synthase: NOS; reactive oxygen species: ROS; superoxide dismutase: SOD; transforming growth factor β: TGF-β;tool-like receptor: TLR; tumor necrosis factor α: TNF-α.
Table 2.
The list of oriental medicines affects male immune-reproductive system.
| Oriental medicine | Compounds | |
|
Anti-cancer treatment |
Goshajinkigan (TJ107) 93-95 Japanese herbal medicines |
Rehmanniae radix, Achyranthis radix, Corni fructus, Dioscoreae rhizome, Plantaginis semen, Alismatis rhizome, Hoelen, Moutan cortex, Cinnamomi cortex, processed Aconite tuber |
|
MYOMI- 7 82 Korean herbal medicines |
Cuscuta chinensis, Lycium chinense, Epimedium koreanum, Rubus coreanus, Morinda officinalis, Cynomorium songaricum, Cistanche deserticola | |
|
Qiangjing tablets (QJT) 47 Chinese herbal medicines |
Ginseng radix et rhizoma, Angelica sinensis radix, Rehmanniae radix praeparata, Corni fructus, Lycii fructus, Schisandrae chinensis fructus, Cuscutae semen, Plantaginis semen, Epimedii folium, Common curculigo orchioides, Herba leonuri | |
|
Sheng Jing Decoction (SJD) 48,81 Chinese herbal medicines |
Rehmannia glutinosa, Astragalus membranaceus, Pseudostellaria heterophylla, Dipsacus acaulis, Lycium arenicolum, Astragalus complanatus, Gleditsia sinensis | |
| Varicocele |
Jiawei Runjing Decoction (JWRJD) 57 Chinese herbal medicines |
Cuscuta chinensis, Dioscorea polystachya, Polygonatum sibiricum, Epimedium brevicornu, Lycium barbarum, Eleutherococcus senticosus, Rhodiola crenulata, Cyathula officinalis, Citrus × aurantium, Hirudo, Homo sapiens, Eupolyphaga seu Steleophaga. |
|
Taohong Siwu Decoction (THSWD) 58 Chinese herbal medicines |
Persicae semen, Carthami flos, Rehmanniae radix praeparata, Paeoniae radix alba, Chuanxiong rhizoma, Angelicae sinensis radix | |
|
Zishen Yutai Pill (ZYP) 59 Chinese herbal medicines |
Cuscutae semen, Ginseng radix et rhizoma, Dipsaci radix, Taxilli herba, Eucommiae cortex, Morindae officinalis radix, Cervi cornu degelatinatum, Codonopsis radix, Atractylodis macrocephalae rhizoma, Asini corii colla, Lycii fructus, Rehmanniae radix praeparata, Polygoni multiflori radix praeparata, Artemisiae argyi, Amomi fructus | |
|
Oxidant and Heat stress |
Kyung-Ok-Ko (KOK) 64-67 Korean herbal medicines |
Rehmannia glutinosa var. purpurea, Panax ginseng, Poria cocos, Lycium chinense, Aquilaria agallocha, honey |
|
MOTILIPERM (MTP) 61 Korean herbal medicines |
Rubiaceae root, Convol vulaceae seed, Liliaceae outer scales | |
|
Qilin pills (QLPs) 63 Chinese herbal medicines |
Polygonum multijiorum, Herba Ecliptae, Eclipta prostrata, Epimedium brevicornu, Cuscuta chinensis, Cynomorium songaricum, Codonopsis pilosula, Curcuma aromatica, Lycium chinense, Rubus idaeus, Dioscorea oppositifolia, Salvia miltiorrhiza, Astragalus membranaceus, Paeonia lactiflora, Citrus reticulata, Morus alba | |
| IOA |
Wuzi Yanzong pill (WZYZP) 54,68-70 Chinese herbal medicines |
Cuscutae chinensis semen, Lycii fructus, Rubi fructus, Schizandrae fructus, Plantaginis semen |
|
Yishentongluo decoction (YSTL) 75-78 Chinese herbal medicines |
Cuscuta chinensis, Epimedium brevicornu, Rehmannia glutinosa, Astragalus propinquus, Salvia miltiorrhiza, Cyathula officinalis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



