Submitted:
13 February 2025
Posted:
14 February 2025
Read the latest preprint version here
Abstract
Peripherally inserted central catheters (PICCs) play a crucial role in providing long-term intravenous therapy for patients requiring extended vascular access. With multiple PICC types available, understanding their cost-effectiveness is essential for healthcare decisions that balance clinical benefits with economic considerations. This study assesses the economic and clinical outcomes of chlorhexidine-coated PICCs (Type A) versus standard PICCs (Type B), aiming to guide best practices in vascular access by addressing the gap in comprehensive cost-effectiveness comparisons. Using a decision-analytic model, costs and quality-adjusted life years (QALYs) between the two types were compared. Primary data from five Chinese university-affiliated medical centers were gathered from 2020 to 2023, with a Delphi panel validating the model inputs. The analysis revealed that while Type A PICCs offer lower initial placement costs, they incur higher complication rates compared to Type B PICCs, which influences long-term cost-effectiveness. After adjusting for complication rates and QALYs, Type B PICCs emerged as more cost-effective over a one-year period, with an incremental cost-effectiveness ratio (ICER) of ¥-40,043.78 ($5,905.90, average exchange rate ¥678.03=$100) per QALY gained. Although Type B PICCs have higher initial costs, their lower complication rates make them a more valuable option for long-term vascular access, offering better overall cost-efficiency.
Keywords:
PICC
; cost-effectiveness
; quality-adjusted life year (QALY)
; incremental cost-effectiveness ratio (ICER)
; healthcare economics
Peripherally inserted central catheters (PICCs) are widely used for long-term intravenous therapy, such as chemotherapy or antibiotics. Different types of PICCs are available, and understanding their cost-effectiveness is important for making the best healthcare decisions.
1. Introduction
Central line-associated bloodstream infection (CLABSI) is a leading concern for central venous catheters (CVCs). Peripherally inserted central catheters (PICCs) compared to CVC, the benefit was the lower infection rate and ease of care, which have become indispensable in modern healthcare for oncology and other long-term venous infusion patients [1,2]. Two distinct types have garnered attention for their potential to minimize adverse events associated with catheter use: Type A, the chlorhexidine-coated PICC, and Type B, the standard PICC.
The advent of chlorhexidine coatings represents a significant stride in CLABSI control within healthcare settings [3,4]. The existing randomized controlled studies compared trials discussed antimicrobial-impregnated CVC versus standard CVC and the result showed that reduced CLABSI risk of chlorhexidine/silver sulfadiazine coated CVC was RR 0.73; 95% CI [0.57–0.94][5]. The existing published randomized controlled trials about PICCs were not too many: one compared the miconazole and rifampicin-impregnated PICC with the standard PICC, and the result was no significant difference; the other compared the chlorhexidine PICC with the standard PICC, the result was no significant on development of a CLABSI (P = .61) or VTE (P > .99) [6,7].
To date, one open-label and randomized clinical trial has been conducted on the clinical comparison in the Hematology departments of Chinese Class 3A hospital facilities from Oct 2020 to Jun 2023, with a 90-day follow-up. The clinical outcome has on the published process; the final report has been submitted to China National Medical Products Administration (NMPA) to support local commercialization.
Scientific journals rarely publish studies on the economic sustainability of two distinct types of peripherally inserted central catheters (PICCs). On understanding the economic implications associated with their use in long-term intravenous therapy, the stages of patient severity are difficult to generalize the unique costs of nursing and complication treatment. We will use second-hand data to do the Cost-Effectiveness Analysis (CEA) to evaluate the new catheter by objectifying the consequences of the accompanying complications. This work uses social insight to analyze the economic implications of Type A over Type B catheters.
2. Materials and Methods
2.1. Study Design and Population
The cost-effectiveness analysis was based on data from a study conducted in the hematology departments of Chinese Class 3A hospitals from September 2020 to May 2023. The study included 227 adult hematology patients who required either a bone marrow transplant or chemotherapy and had an expected survival period of more than 90 days (Figure 1). Due to the study catheter body is blue, and the control catheter is white, so the study is open-label. The randomization program was controlled the 3rd party independent CRO, and randomization sequences were computer-generated by an independent statistician in random blocks of four and stratified by site. The study group, which used chlorhexidine-coated PICCs (Type A), enrolled 114 patients, while the control group, which used standard PICCs (Type B), enrolled 113 patients.
Devices placed in individuals under the age of 18 years who need to accept infusion therapy, those in which insertion failure occurred (Failure to insert catheter more than 2 times), those in which the distal tip could not be properly positioned to start infusion therapy, and those in place the catheter at the same arm least than 365 days were excluded from the study.
All patients signed informed consent forms agreeing to participate in the study, allowing their treatment data to be used for research, and understanding their rights during the research period. The study followed the principles of the Declaration of Helsinki and Good Clinical Practice (GCP) and was approved by the hospital’s ethics committee.
2.2. Therapeutic Intervention
Trial participants were randomly allocated to the following devices: the standard PICC (ArrowTM PICC: Teleflex Inc.), or the chlorhexidine-coated PICC (Arrowg+ard Blue Advance™ PICC), single or double lumen, 4 Fr to 5.5 Fr, length 40 cm to 55 cm catheter. 114 randomly accepted the Type A catheter (the chlorhexidine-coated PICCs) compared with standard PICCs, and 113 patients underwent the Type B catheter.
Considering the same conditions for central access, the PICC insertion nurses are all certified by the Chinese Nurse Society and have completed more than 50 cases of experience per year, to keep the insertion technology stable and high quality. The catheter insertion and maintenance procedures are all following the same standard. All procedures adopted the CLABSI prevention programs, which were the CDC’s recommended bundle strategies; the main components include the maximum sterilized barrier, the chlorhexidine-based antiseptic skin preparation, hand hygiene, and related training[8,9,10,11,12]. The observation time was 90 days, with 6 times follow-ups to maintain the catheter’s function. If the patients want to volunteer to remove the catheter earlier than 90 days because of the therapy gap, the data would be included when the catheter indwelling period was longer than 30 days. The follow-up frequency was once per week in the 1st month, once per 2 weeks in the 2nd month, and once per 4 weeks in the 3rd month. The standard procedures of follow-ups included insertion point care, the ultrasound assessment of central venous catheter-related thrombosis, and catheter function check (Figure 2).
2.3. Evaluation of endpoints
The main outcomes of effectiveness were the 1st puncture success and the Bloodstream infection. The Central Line-Associated Bloodstream Infections (CLABSI) rate is determined based on the laboratory-confirmed bloodstream infection criteria during PICC indwelling time, excluding Mucosal Barrier Injury Laboratory-Confirmed Bloodstream Infection (MBI-LCBI) [12,14,15]. The rate of unknown fever origin among patients is recorded based on patient-reported symptoms and clinical assessments, which could not meet CLABSI criteria and do not think about disease-leading symptoms. We consider the study to be of interest; the clinical endpoints included CLABSI and unknown fever rates. Other local catheter-related complications were also recorded within 90 days. Quality-adjusted life Years (QALYs) were not observed in the clinical trial, referred to in the other reported articles, and the direct costs related to PICC insertion and maintenance came from the trial data [16,17,18,19,20].
2.4. Cost Evaluation Measures
The public-hospital perspective of the analysis reflects the costs in Chinese public hospitals covered by the Urban and Rural Residents Basic Medical Insurance (URRBMI). For both groups, we calculated the following: The price of standard PICC and estimated price of study PICC (¥/Piece), the average costs of insertion and maintenance once for one patient (¥/Time), the average costs for CLABSI diagnosis and treatment for one patient (¥/Time), the average duration of hospitalization per therapy stage (Day). In the costs of both groups, we did not include the costs for the original disease and other costs unrelated to the catheter. The ultrasound equipment for the study was provided by the study sponsor; the long-term and rental costs of the equipment were not included in the calculation.
2.5. Currency Rate and Conversion
Costs were calculated on the real value from 2019 to 2023. All costs are presented in RMB; the official currency conversion average rate of the China Central Bank from 2020 Jan to 2023 Dec is 1 RMB = 0.1475 US dollar.
2.6. Cost-Effectiveness Analysis
2.7. Statistical Analysis
We processed data using Stata/SE 15.1 and TreeAge Pro Healthcare (version 2023 R1.2), a software package tailored for health outcomes research, provided by TreeAge Software, Inc. To process the obtained data, continuous variables were presented as mean and SD, and categorical variables were expressed as absolute and relative frequencies. Data for expenditure calculation of complication treatments were collected by the micro-costing method alongside standard patient care through the study [23,24,25]. The mean expenditure of daily care in each scenario was used to estimate the average cost of each procedure associated with central vascular access. The study product has no selling price in China market, the expenditure was estimated through comparison with the existing products.
The two groups were compared using Pearson’s chi-square test for categorical variables, and the independent sample t-test (two-tailed, significance level P<0.05) for continuous variables [26].
3. Results
In our analysis, 227 patients signed the informed consent, and 4 patients withdrew from the study because of their engagement in another study. A total of 224 patients (136 male and 88 female) with hematology disease needed to accept PICC catheters aged 18-83 years (mean age 42.34 (±13.70) ) underwent 90-day catheter follow-up according to the scheduled protocol. Baseline data on all patients included in the study are shown in Table 1.
3.1. Comparison of Primary Endpoints in Two Groups
113 patients (Type A) accepted chlorhexidine-coated PICCs, and 111 (Type B) accepted standard PICCs. We analyzed 220 patients with CLABSI, unknown fever, and local complications. 8 patients met the criteria of BSI, but 3 of 8 patients met the criteria of CLABSI, and the other 5 were diagnosed as MBI-LCBI. 36 patients had CLABSI-related symptoms, but the lab exam results could not meet all items, and other infection sources were excluded. 3 CLABSI cases all happened in the control group, but the statistic had no significance between two groups (P=0.076). 17 (15.18%) unknown fevers were in the study group, compared to the control group (N=20, 19.05%, P=0.449), the incidence rate was higher than the study group. In the study group, 1 patient needed to go through the 2nd time puncture, and 3 patients in the control group accepted the 2nd time puncture, but it was not statistically significant (P=0.304). Regarding the local complications’ performance, the study group was also better than the control group, but the difference was of no significance. This study includes the cost-effectiveness analysis part, so the unplanned withdrawal catheter rate was summarized. (Table 2)
3.2. Cost Analysis
The price of the standard PICC, nursing expense per patient, and the lab test items were identified by Beijing Municipal Price Bureau in Class 3A hospital. For comparison, the price of the standard PICC was ¥2100 in 2020. To complete the decision tree model, we set the estimated price of AGBA PICC was ¥2300.
The regular care and insertion costs of PICC are all covered by China’s basic medical insurance for urban and rural residents. The additional costs over the regular care were related to the catheter-related complications. The direct costs of PICC are characterized in Table 3. This is a calculation of per case costs, from which the costs per insertion and maintenance in 2020 were calculated. The CLABSI diagnosis needed at least 2 doses of central catheter blood cultures per lumen and 2 doses of peripheral blood cultures. The average diagnosis of CLABSI needed ¥1332.77 per time, and the average treatment per patient per time of CLABSI in this study was ¥87147.08 per patient per time, which included parenteral antibiotics, catheter removal, and other empiric therapies. The CLABSI is the most feared complication, the attributed mortality of CLABSI to be 2.27–2.75%.
3.3. Decision Tree Model
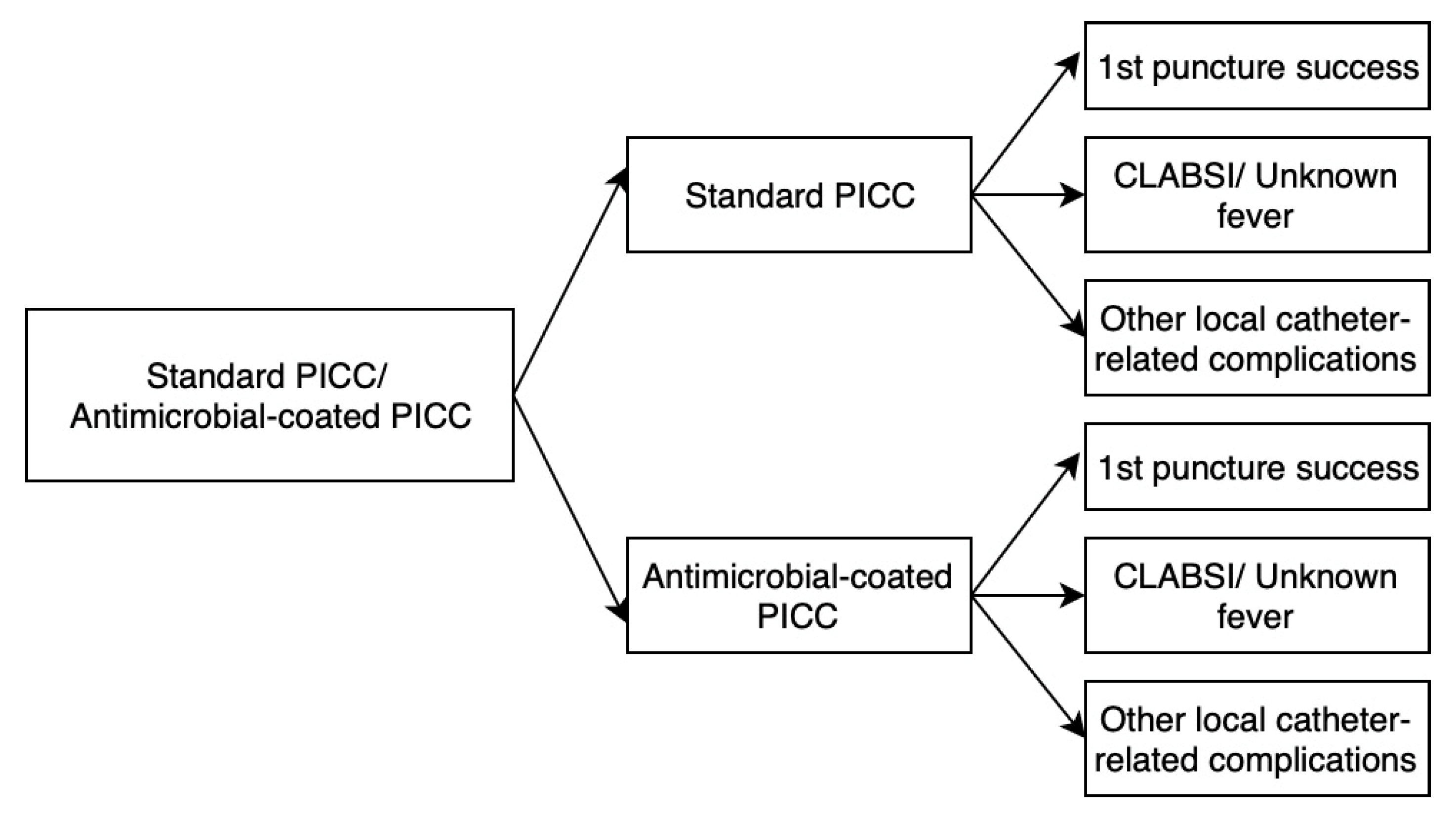
The decision tree for economic analysis to present the trajectory of 2 types PICCs from placement until the end of infusion therapy, demonstrating the likelihood of failure to catheter related complications. In Figure 3, we present the decision tree model for the potential complication of the standard PICC and AGBA-coated PICC, the result is that AGBA-coated is a more advanced device on the catheter-related complication’s expense control; rather we expect a significant difference on clinical points.
3.4. Cost-Effectiveness Analysis
CEA (Cost-Effectiveness Analysis) measures the cost per unit of effect[22,28,29,30]. Since the costs of type B (AGBA-coated PICC) are lower than those of type A, we evaluated the ICER effects.
ICER=C1-C2/E1-E2 is defined as the ratio of the difference in the costs of 2 types of PICCs and the difference in clinical effects, where C1 and C2 are the costs of the entire in-patient and out-patient process for the catheter-related indwelling period, E1 and E2 document the clinical effectiveness of the primary clinical outcomes.
In this case, the PICC catheter could not improve the treatment outcome, but it impacts the complication incidence rate so that we will divide the difference costs of all complications. The result was calculated the difference of 1st puncture success rate, CLABSI, and other local catheter-related complications.
ICER=Ctype B − Ctype A/Etype B -Etype A
The result is then interpreted as the cost per patient with a catheter per QALY on the complication incidence. In general, the lower ICER could incur the higher value.
We found that the average cost of 1 QALY improvement in the AGBA group per patient is ¥62,817.79. The average cost of 1 QALY improvement in the standard group per patient is ¥102,861.57. According to the calculated ICER for AGBA, compared to the standard PICC, results in average cost decrease of ¥40043.78 per patient (Table 4).
Due to the AGBA-coated PICC does not launch in China market, we estimated higher price for the new technology. The result showed it has the lower expense on 90 days’ catheter indwelling period compared to the standard PICC. The unknown fever would take empiric therapies, although it could diagnose to be CLABSI, but the related diagnosis and treatments costs are almost same in both groups. The unknown fever might need higher cost compared to diagnosed CLABSI, because of the repeated lab examinations to figure out the infection source, in standard group, the cost of unknown fever was ¥444,819.29 and CLABSI was ¥444,404.50; in AGBA-coated PICC group, the cost of unknown fever was ¥314,742.50 and CLABSI was ¥314,204.50. Thus, AGBA-coated PICC appears to be a more cost-effective alternative on acute-care and home-care solution for oncology patient.
Figure 3.
Model structure. The PICC is an invasive procedure; a good device needs to be inserted easily, and there is a low complication rate. CLABSI, unknown fever, and other local catheter-related complications are all evaluated during the catheter indwelling period.
Figure 3.
Model structure. The PICC is an invasive procedure; a good device needs to be inserted easily, and there is a low complication rate. CLABSI, unknown fever, and other local catheter-related complications are all evaluated during the catheter indwelling period.
4. Results
Despite the improvement in care quality of PICC and CVC over the past almost twenty years, many studies have proved effective procedures and devices that could control CLABSI to a very low level. However, empiric therapies of unknown fever in real clinical practice related to catheters are still existing [31,32]. Therefore, researchers continuously search for and develop advanced devices to reduce the infection rate to improve healthcare quality.
A general perspective of long-term indwelling catheters is their low complication, high comfort, and easy care focused on safety and long-lasting performance [33,34,35]. The implanted port is popular in Western countries, but the specific and expensive needles are not reimbursed in China, and the practice is more invasive, so the utility is low [36,37,38].
The aim of this study was to analyze the cost-effectiveness of two types PICCs from the social perspective on the objectification of the catheter, which is easy to use, and lower complication rate compared to the standard catheter.
According to the works of the same coated center venous catheter, chlorhexidine has a positive effect on reducing CLABSI and microorganism colonization in acute-care facilities. 23 trials reported that comparing the standard catheter and chlorhexidine/silver sulfadiazine-coated catheters had a lower CRBSI incidence rate (RR 0.70, 95% CI 0.53–0.91, p = 0.008). Regarding catheter colonization performance, chlorhexidine/silver sulfadiazine-coated catheters also presented a positive result. However, the 2 types of peripherally inserted central catheters related RCT study is rare.
This study has several strengths, including extensive data collection, a rigorous decision-analytic model, and validation by a Delphi panel. However, there are limitations:
- Observation time and sample size. The clinical outcomes in this RCT had no significant difference, but it had clinical value. The observation time might need longer, and sample size should be bigger, this risk has been discussed on the clinical study protocol. The further study on CLABSI might suit to surveillance study, to observe the longer time and all population. However, the RCT is not an economic and efficacy solution.
- QALY adoption. In this evaluation, QALY was adopt from other hematology related patient quality life changing study of pre- and post- treatment. This data has described the general life quality changing around the treatment on this disease, it has the relationship with the catheter, but the catheter has no significant impact on the QALY, except death event related to the catheter infection. The catheter complication must lead the patient life qualities’ change, while previous research provides a general perspective, the catheter’s impact on QALYs may require further study with direct data collection or more effective indices to describe its effectiveness.
- Economic Evaluation Methods. Along with the people’s life quality pursuing, the more treatment and medical products work on life quality’s improvement. Almost procedures do not change the pathway of disease and just postpone the progress of disease. The current economic evaluation methods may not fully capture the value of treatments and medical products that primarily improve quality of life rather than altering disease pathways. Innovative theories and tools are needed to address the suitable value of such interventions scientifically.
4.1. Implications for Practice and Policy
With more and more new technology, clinicians should weigh the long-term benefits and higher initial costs. On AGBA-coated PICCs showed a better performance on complications control and trusted safety. Policymakers should consider incorporating cost-effective PICCs into standard healthcare practices and coverage policies to optimize patient satisfaction and resource utilization.
4.2. Future Research Directions
PICC catheters are common infusion devices used in many healthcare facilities. Future research should focus on multi-center trials to validate these findings across diverse healthcare settings. Additionally, studies should examine the long-term satisfaction associated with new treatment adoption to provide more comprehensive insights into their effectiveness and value.
5. Conclusions
In conclusion, this study suggests that coated PICC might have no significant statistical difference in CLABSI reduction. However, the coated PICC provides a solid outcome on cost-effectiveness analysis. The findings suggest that, on social respective, the coated PICC for high-risk patients is economically justified. Here is a rare study and guideline mentioning coated PICC and a recommendation for further study. While this study passed the COVID-19 pandemic period, its result was also analyzed in the specific economic context. The present study recommends policymakers boom the new devices’ evaluation method, for the non-treatment device, the treatment effect could be complications. The low complications also could save healthcare expenses and resources, at the same time improve the quality of care.
Author Contributions
The study was conceptualized and executed by JX, who designed the model, collected necessary data, and conducted the analysis. RC, HZ and HCC served as clinical and economic expert panel members. HF took the lead in drafting the manuscript, and the final version received input, approval, and contributions from all team members. All authors have collectively agreed to investigate and resolve any such questions and document the resolution in the literature.
Funding
This research received no external funding. It was conducted as part of a PhD thesis supported by Teleflex Medical Device Corp. (Ethical Code: 2019PHC005-001).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is provided within the manuscript or supplementary information files.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Caris, M.G.; de Jonge, N.A.; Punt, H.J.; Salet, D.M.; de Jong, V.M.T.; Lissenberg-Witte, B.I.; Zweegman, S.; Vandenbroucke-Grauls, C.M.J.E.; van Agtmael, M.A.; Janssen, J.J.W.M. Indwelling time of peripherally inserted central catheters and incidence of bloodstream infections in haematology patients: a cohort study. Antimicrob. Resist. Infect. Control. 2022, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, Y.; Zhu, N.; Li, Y.; Fu, J.; Liu, J. Comparison of peripherally inserted central catheters (PICCs) versus totally implantable venous-access ports in pediatric oncology patients, a single center study. Sci. Rep. 2022, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Novikov, A.; Lam, M.Y.; A Mermel, L.; Casey, A.L.; Elliott, T.S.; Nightingale, P. Impact of catheter antimicrobial coating on species-specific risk of catheter colonization: a meta-analysis. Antimicrob Resist Infect Control 2012, 1, 40–40. [Google Scholar] [CrossRef] [PubMed]
- Chong, H.Y.; Lai, N.M.; Apisarnthanarak, A.; Chaiyakunapruk, N. Comparative Efficacy of Antimicrobial Central Venous Catheters in Reducing Catheter-Related Bloodstream Infections in Adults: Abridged Cochrane Systematic Review and Network Meta-Analysis. Clin. Infect. Dis. 2017, 64, S131–S140. [Google Scholar] [CrossRef]
- Jaeger, K.; Zenz, S.; Jüttner, B.; Ruschulte, H.; Kuse, E.; Heine, J.; Piepenbrock, S.; Ganser, A.; Karthaus, M. Reduction of catheter-related infections in neutropenic patients: a prospective controlled randomized trial using a chlorhexidine and silver sulfadiazine-impregnated central venous catheter. Ann. Hematol. 2004, 84, 258–262. [Google Scholar] [CrossRef]
- R. Gilbert et al., “Antimicrobial-impregnated central venous catheters for prevention of neonatal bloodstream infection (PREVAIL) : an open-label, parallel-group, pragmatic, randomised controlled trial,” Lancet Child Adolesc Health, vol. 3, no. 6, pp. 381–390, Jun. 2019. [CrossRef]
- Storey, S.; Brown, J.; Foley, A.; Newkirk, E.; Powers, J.; Barger, J.; Paige, K. A comparative evaluation of antimicrobial coated versus nonantimicrobial coated peripherally inserted central catheters on associated outcomes: A randomized controlled trial. Am. J. Infect. Control. 2016, 44, 636–641. [Google Scholar] [CrossRef]
- Ardura, M.I.D.; Bibart, M.J.M.; Mayer, L.C.B.; Guinipero, T.; Stanek, J.; Olshefski, R.S.; Auletta, J.J. Impact of a Best Practice Prevention Bundle on Central Line-associated Bloodstream Infection (CLABSI) Rates and Outcomes in Pediatric Hematology, Oncology, and Hematopoietic Cell Transplantation Patients in Inpatient and Ambulatory Settings. J. Pediatr. Hematol. 2020, 43, e64–e72. [Google Scholar] [CrossRef]
- Marschall, J.; Mermel, L.A.; Fakih, M.; Hadaway, L.; Kallen, A.; O’grady, N.P.; Pettis, A.M.; Rupp, M.E.; Sandora, T.; Maragakis, L.L.; et al. Strategies to Prevent Central Line–Associated Bloodstream Infections in Acute Care Hospitals: 2014 Update. Infect. Control. Hosp. Epidemiology 2014, 35, 753–771. [Google Scholar] [CrossRef]
- Böll, B.; Schalk, E.; Buchheidt, D.; Hasenkamp, J.; Kiehl, M.; Kiderlen, T.R.; Kochanek, M.; Koldehoff, M.; Kostrewa, P.; Claßen, A.Y.; et al. Central venous catheter–related infections in hematology and oncology: 2020 updated guidelines on diagnosis, management, and prevention by the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO). Ann. Hematol. 2020, 100, 239–259. [Google Scholar] [CrossRef]
- Lee, K.H.; Cho, N.H.; Jeong, S.J.; Na Kim, M.; Han, S.H.; Song, Y.G. Effect of Central Line Bundle Compliance on Central Line-Associated Bloodstream Infections. Yonsei Med J. 2018, 59, 376–382. [Google Scholar] [CrossRef]
- N. P. O et al., “Guidelines for the Prevention of Intravascular Catheter-Related Infections (2011). Available online: https://www.cdc.gov/infectioncontrol/guidelines/bsi/c-i-dressings/index.html (accessed on 24 December 2022).
- 2021 Infusion Therapy Standards of Practice Updates. J. Infus. Nurs. 2021, 44, 189–190. [CrossRef] [PubMed]
- Kato, Y.; Hagihara, M.; Kurumiya, A.; Takahashi, T.; Sakata, M.; Shibata, Y.; Kato, H.; Shiota, A.; Watanabe, H.; Asai, N.; et al. Impact of mucosal barrier injury laboratory-confirmed bloodstream infection (MBI-LCBI) on central line-associated bloodstream infections (CLABSIs) in department of hematology at single university hospital in Japan. J. Infect. Chemother. 2018, 24, 31–35. [Google Scholar] [CrossRef] [PubMed]
- CDC, Ncezid, and DHQP, “Bloodstream Infection Event (Central Line-Associated Bloodstream Infection and Non-central Line Associated Bloodstream Infection).
- Xie, F.; Zhou, T.; Humphries, B.; Neumann, P.J. Do Quality-Adjusted Life Years Discriminate Against the Elderly? An Empirical Analysis of Published Cost-Effectiveness Analyses. Value Heal. 2024, 27, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.D.; Do, L.A.; Synnott, P.G.; Lavelle, T.A.; Prosser, L.A.; Wong, J.B.; Neumann, P.J. Developing Criteria for Health Economic Quality Evaluation Tool. Value Heal. 2023, 26, 1225–1234. [Google Scholar] [CrossRef]
- Guliyeva, A. Measuring quality of life: A system of indicators. Econ. Politi- Stud. 2021, 10, 476–491. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Anderson, K.L. The Quality of Life Scale (QOLS): Reliability, Validity, and Utilization. Heal. Qual. Life Outcomes 2003, 1, 1–60. [Google Scholar] [CrossRef]
- Wang, K.; Zhou, Y.; Huang, N.; Lu, Z.; Zhang, X. Peripherally inserted central catheter versus totally implanted venous port for delivering medium- to long-term chemotherapy: A cost-effectiveness analysis based on propensity score matching. J. Vasc. Access 2021, 23, 365–374. [Google Scholar] [CrossRef]
- Bloemen, A.; Daniels, A.; Janssen, R.; Samyn, M.; Elshof, J.-W. ECG Guided Tip Positioning Technique for Peripherally Inserted Central Catheters in a teaching Hospital: Feasibility and Cost-effectiveness Analysis in a Prospective Cohort Study. Eur. J. Vasc. Endovasc. Surg. 2019, 58, e531. [Google Scholar] [CrossRef]
- Comas, M.; Domingo, L.; Jansana, A.M.; Lafuente, E.M.; Civit, A.M.; García-Pérez, L.; de la Vega, C.M.L.; Cots, F.; Sala, M.; Castells, X. Cost-effectiveness Analysis of Peripherally Inserted Central Catheters Versus Central Venous Catheters for in-Hospital Parenteral Nutrition. J. Patient Saf. 2022, 18, e1109–e1115. [Google Scholar] [CrossRef]
- Gupta, N.; Verma, R.; Dhiman, R.K.; Rajsekhar, K.; Prinja, S. Cost-Effectiveness Analysis and Decision Modelling: A Tutorial for Clinicians. J. Clin. Exp. Hepatol. 2019, 10, 177–184. [Google Scholar] [CrossRef]
- K. Kuntz et al., “Overview of Decision Models Used in Research,” 2013. Available: https://www.ncbi.nlm.nih.gov/books/NBK127474/. (accessed on 18 June 2023).
- Briggs, A. “StAtistical Issues in Economic Evaluations,” Encyclopedia of Health Economics; 2014; pp. 352–361. [CrossRef]
- Neumann, P.J.; Kim, D.D.; Trikalinos, T.A.; Sculpher, M.J.; Salomon, J.A.; Prosser, L.A.; Owens, D.K.; Meltzer, D.O.; Kuntz, K.M.; Krahn, M.; et al. Future Directions for Cost-effectiveness Analyses in Health and Medicine. Med Decis. Mak. 2018, 38, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Wang, H.; Niu, M.; Zhu, X.; Cai, J.; Wang, X. Health-related quality of life before and after hematopoietic stem cell transplant: evidence from a survey in Suzhou, China. Hematology 2018, 23, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Choong, S.H.C.; Poon, M.M.; Soh, T.G.; Lieow, J.; Tan, L.K.; Koh, L.P.; Chng, W.-J.; Lee, Y.M.; Lee, J.S.X.; Ramos, D.G.; et al. Use of Peripherally Inserted Central Catheter (PICC) for the Infusion of Peripheral Blood Stem Cell Products Is Safe and Effective. Blood 2020, 136, 41–42. [Google Scholar] [CrossRef]
- Godino, C.; Scotti, A.; Marengo, A.; Battini, I.; Brambilla, P.; Stucchi, S.; Slavich, M.; Salerno, A.; Fragasso, G.; Margonato, A. Effectiveness and ost-efficacy of iuretics ome dministration via eripherally nserted entral enous atheter in atients with nd- tage eart ailure. Int. J. Cardiol. 2022, 365, 69–77. [Google Scholar] [CrossRef]
- Health economic evaluation: Important principles and methodology. Available: https://onlinelibrary.wiley.com/doi/epdf/10.1002/lary.23943?saml_referrer. (accessed on 8 January 2023).
- Buetti, N.; Marschall, J.; Drees, M.; Fakih, M.G.; Hadaway, L.; Maragakis, L.L.; Monsees, E.; Novosad, S.; O’grady, N.P.; Rupp, M.E.; et al. Strategies to prevent central line-associated bloodstream infections in acute-care hospitals: 2022 Update. Infect. Control. Hosp. Epidemiology 2022, 43, 553–569. [Google Scholar] [CrossRef]
- Wang, H.; Tong, H.; Liu, H.; Wang, Y.; Wang, R.; Gao, H.; Yu, P.; Lv, Y.; Chen, S.; Wang, G.; et al. Effectiveness of antimicrobial-coated central venous catheters for preventing catheter-related blood-stream infections with the implementation of bundles: a systematic review and network meta-analysis. Ann. Intensiv. Care 2018, 8, 1–12. [Google Scholar] [CrossRef]
- Hanna, H.; Benjamin, R.; Chatzinikolaou, I.; Alakech, B.; Richardson, D.; Mansfield, P.; Dvorak, T.; Munsell, M.F.; Darouiche, R.; Kantarjian, H.; et al. Long-Term Silicone Central Venous Catheters Impregnated With Minocycline and Rifampin Decrease Rates of Catheter-Related Bloodstream Infection in Cancer Patients: A Prospective Randomized Clinical Trial. J. Clin. Oncol. 2004, 22, 3163–3171. [Google Scholar] [CrossRef]
- Lai, N.M.; Chaiyakunapruk, N.; O'Riordan, E.; Pau, W.S.C.; Saint, S. Catheter impregnation, coating or bonding for reducing central venous catheter-related infections in adults. Cochrane Database Syst. Rev. 2016, 2018, CD007878. [Google Scholar] [CrossRef]
- Safdar, N.; Maki, D.G. Risk of Catheter-Related Bloodstream Infection With Peripherally Inserted Central Venous Catheters Used in Hospitalized Patients. Chest 2005, 128, 489–495. [Google Scholar] [CrossRef]
- A Leech, A.; Kim, D.D.; Cohen, J.T.; Neumann, P.J. Are low and middle-income countries prioritising high-value healthcare interventions? BMJ Glob. Heal. 2020, 5, e001850. [Google Scholar] [CrossRef]
- Butt, T.; Liu, G.G.; Kim, D.D.; Neumann, P.J. Taking stock of cost-effectiveness analysis of healthcare in China. BMJ Glob. Heal. 2019, 4, e001418. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Xiao, K.; Zhu, H.; Luo, L. The impacts of public hospital comprehensive reform policies on hospital medicine cost, revenues and healthcare expenditures 2014–2019: An analysis of 103 tertiary public hospitals in China. Front. Heal. Serv. 2023, 3, 1079370. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of participants enrollment and randomization.
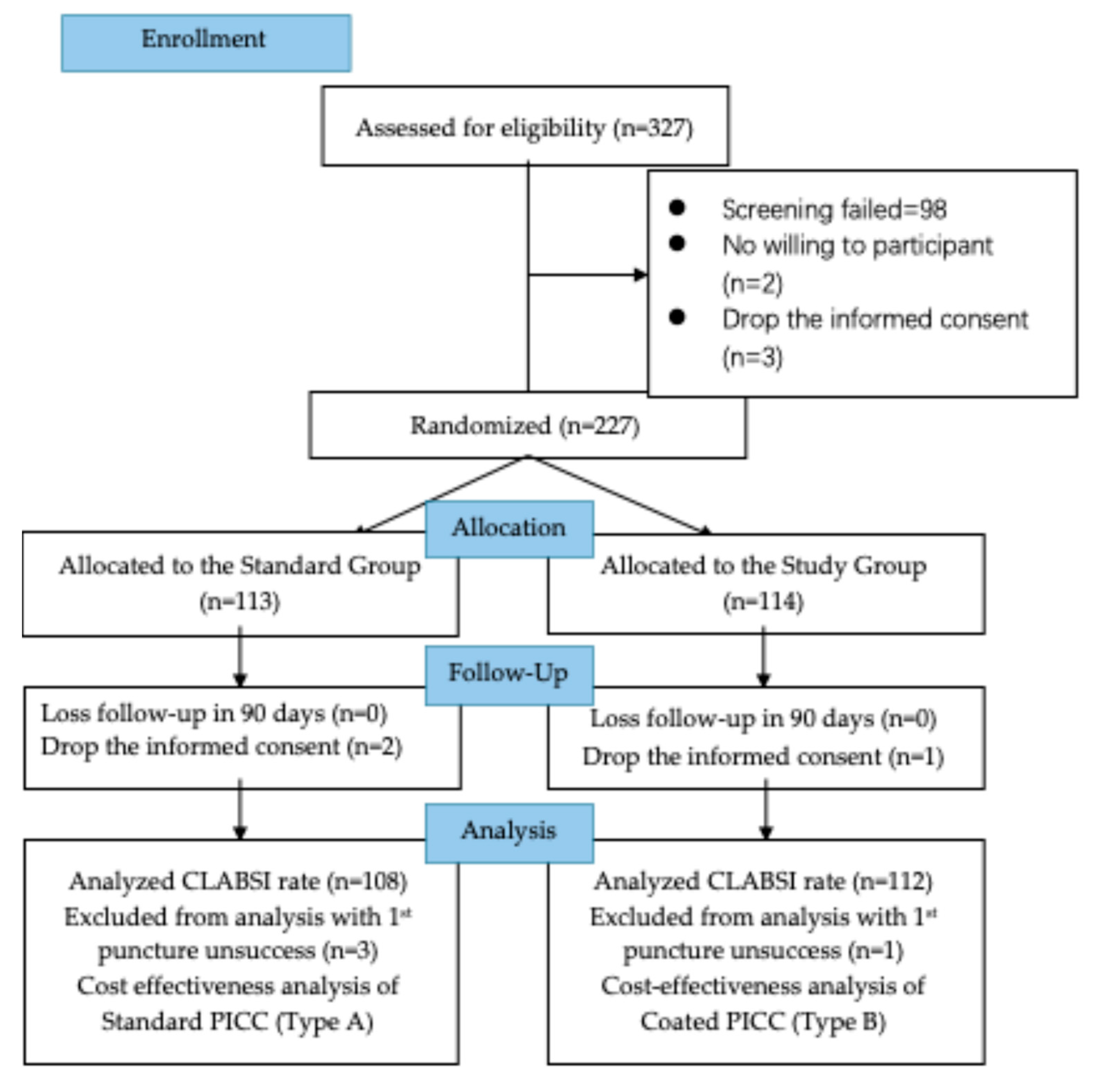
Figure 2.
The standard procedures of catheter care follow the American INS recommendation: (a) Insertion point care; (b) Ultrasound assessment of vein/catheter-related thrombosis. Check the insertion point to the axilla; the study nurse will check the ultrasonic echo of the outer wall of the catheter; (c) Catheter function check. Follow INS standard recommendation, use the Saline-Administration-Saline-Heparin (SASH) principle [13].
Figure 2.
The standard procedures of catheter care follow the American INS recommendation: (a) Insertion point care; (b) Ultrasound assessment of vein/catheter-related thrombosis. Check the insertion point to the axilla; the study nurse will check the ultrasonic echo of the outer wall of the catheter; (c) Catheter function check. Follow INS standard recommendation, use the Saline-Administration-Saline-Heparin (SASH) principle [13].
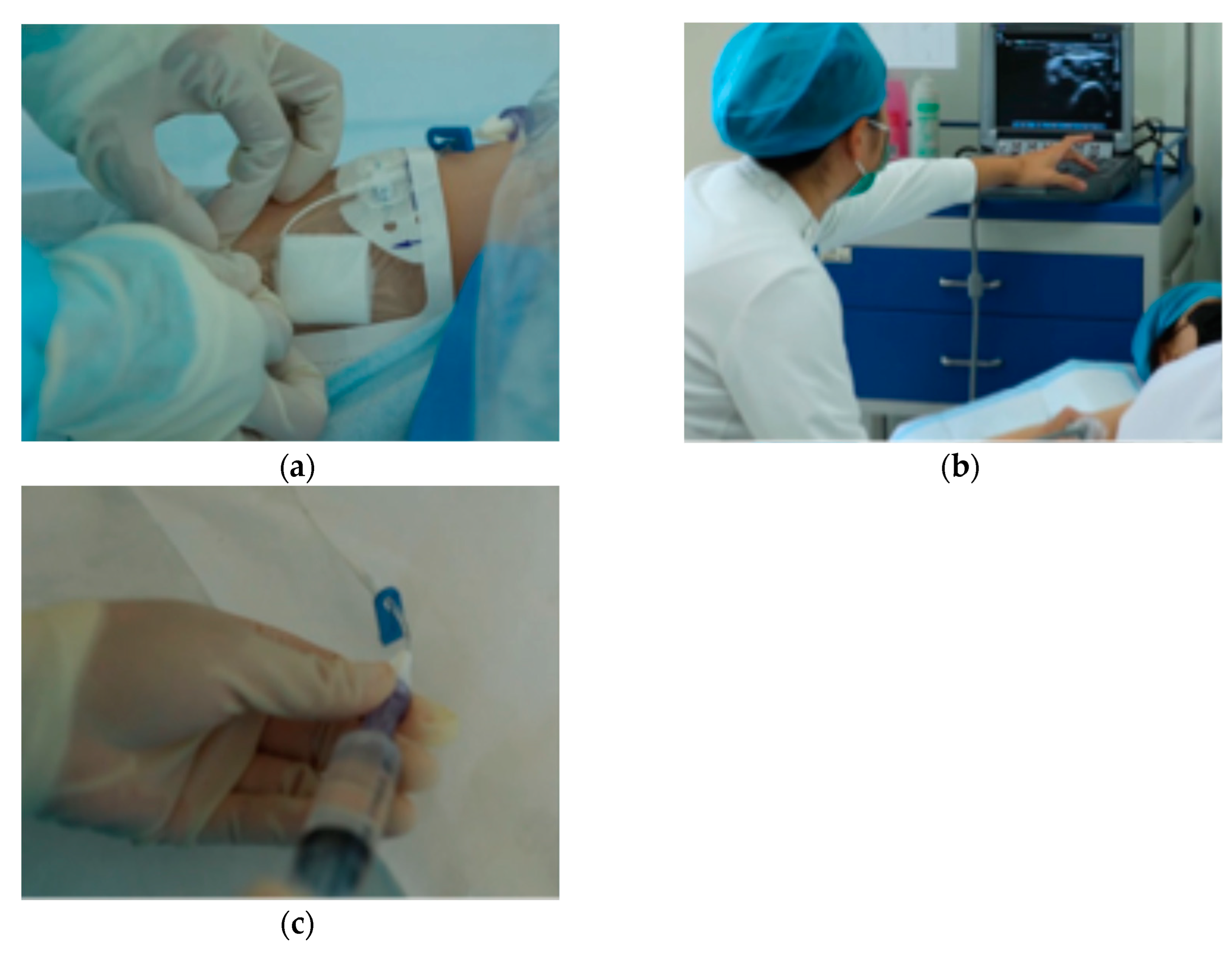

Table 1.
Patient Clinical Variables for Two PICCs Group.
| Observation Item | Study (n=113) n (%) |
Control (n=111) n (%) |
Total (N=224) n (%) |
P-Value* | |
|---|---|---|---|---|---|
| Gender | 0.513 | ||||
| Male | 71 (62.83%) | 65 (58.56%) | 136 (60.71%) | ||
| Female | 42 (37.17%) | 46 (41.44%) | 88 (39.29%) | ||
| Puncture | arm | 0.605 | |||
| Left arm | 42 (37.17%) | 45 (40.54%) | 87 (38.84%) | ||
| Right arm | 71 (62.83%) | 66 (59.46%) | 137 (61.16%) | ||
| Catheter size | 0.834 | ||||
| 4.0-4.5 French | 55 (48.67%) | 52 (47.27%) | 107 (47.98%) | ||
| 5.0-5,0 French | 58 (51.33%) | 58 (52.73%) | 116 (52.02%) | ||
| Catheter lumen | 0.894 | ||||
| Single lumen | 56 (49.56%) | 56 (50.45%) | 112 (50.00%) | ||
| Double lumen | 57 (50.44%) | 55 (49.55%) | 112 (50.00%) | ||
| Age† | 41.36 (±12.98) | 43.34 (±14.38) | 42.34 (±13.70) | 0.280 | |
| BMI† | 22.97 (±3.21) | 24.03 (±3.40) | 23.50 (±3.34) | 0.020 | |
| APTT† | 31.13 (±3.77) | 30.58 (±3.41) | 30.86 (±3.60) | 0.251 | |
| INR† | 1.05 (±0.10) | 1.06 (±0.13) | 1.06 (±0.11) | 0.852 | |
| Indwell Period (Days) † | 62.81 (±27.98) | 69.04 (±26.65) | 65.89 (±27.44) | 0.089 | |
Antimicrobial coated PICCs (Type A) is study group, Standard PICCs (Type B) is control group. *Pearson’s chi-square test for heterogeneity. † Value are presented as mean and ± SD compared by t-test. P-level of statistical significance, significant at P<0.05.
Table 2.
The clinical outcomes between the two groups.
| Clinical Outcomes | Study Group (n=112) n (%) | Control Group (n=108) n (%) | Total (n=220) n (%) |
P-Value* | |
|---|---|---|---|---|---|
| CLABSI | 0.076 | ||||
| Non-CLABSI | 112 (100.00%) | 105 (97.22%) | 217 (98.65%) | ||
| CLABSI | 0 (0.00%) | 3 (2.65%) | 3 (1.32%) | ||
| Unknown Fever | 0.449 | ||||
| No | 95 (84.82%) | 85 (80.95%) | 180 (82.95%) | ||
| Yes | 17 (15.18%) | 20 (19.05%) | 32 (17.05%) | ||
| The 1st puncture success | 0.304 | ||||
| 1st puncture success | 112 (99.12%) | 108 (97.30%) | 220 (98.05%) | ||
| No 1st puncture success | 1 (0.88%) | 3 (2.70%) | 4 (1.95%) | ||
| Other local complications | 0.449 | ||||
| Non complications | 95 (84.82%) | 85 (80.95%) | 180 (82.95%) | ||
| Catheter-related complications | 17 (15.18%) | 20 (19.05%) | 37 (17.05%) | ||
| Catheter withdraw types | 0.411 | ||||
| Withdraw as planned | 71 (69.61%) | 77 (74.76%) | 148 (72.20%) | ||
| Withdraw with complication | 31 (30.39%) | 26 (25.24%) | 57 (27.80%) | ||
Table 3.
The variables in decision trees.
| Model Input | Base-Case Value | Source | |
|---|---|---|---|
| Cost | |||
| Price of Standard PICC (¥/piece) | 2100.00 | Industry data | |
| Estimated Price of AGBA PICC (¥/piece) | 2300.00 | Industry data | |
| Catheter maintenance (¥/per patient) | 2100.11 | Study data | |
| Catheter insertion/replacement (¥/per patient) | 364.25 | Study data | |
| CLABSI Diagnosis (¥/per time) | 1332.77 | Study data | |
| CLABSI Treatment (¥/per time) | 87147.08 | Study data | |
| Hospitalization per day in Beijing Class 3A hospital (¥/per bed per day) | 200.00 | Supplementary Materials | |
| QALY of pre-treatment | 0.65 | Liang Y, Wang H, et al., 2018 [27] | |
| QALY of treatment | 0.90 | Liang Y, Wang H, et al., 2018 [27] | |
| Length of stay, day | |||
| Patient with CLABSI | 20.6 | Study data | |
| Patient without CLABSI | 11.2 | Study data | |
Table 4.
Cost-effectiveness analysis of AGBA-coated PICC compared to standard PICC.
| Clinical Outcomes | Study Group (n=112) | Control Group (n=108) | P-Value | ||||
|---|---|---|---|---|---|---|---|
| Costs | Effectiveness | Probability | Costs | Effectiveness | Probability | ||
| Total expense | 62,817.79 | 0.90 | 100.00% | 102,861.57 | 0.89 | 100.00% | <0.05 |
| 1st time puncture unsuccess | 17,328.50 | 0.65 | 0.98% | 18,928.50 | 0.65 | 2.91% | |
| CLABSI | 314,204.50 | 0.90 | 0.00% | 444,404.50 | 0.9 | 2.91% | |
| Unknown fever | 314,742.50 | 0.90 | 16.67% | 444,819.29 | 0.9 | 18.45% | |
| Other local catheter-related complications | 30,964.25 | 0.90 | 13.72% | 14,374.87 | 0.9 | 2.91% | |
| Complications free | 8,664.25 | 0.90 | 68.63% | 9,464.25 | 0.9 | 72.81% | |
| ICER (AGBA Coated PICC vs. Standard PICC) | -40043.78 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



