Submitted:
05 February 2025
Posted:
05 February 2025
You are already at the latest version
Abstract
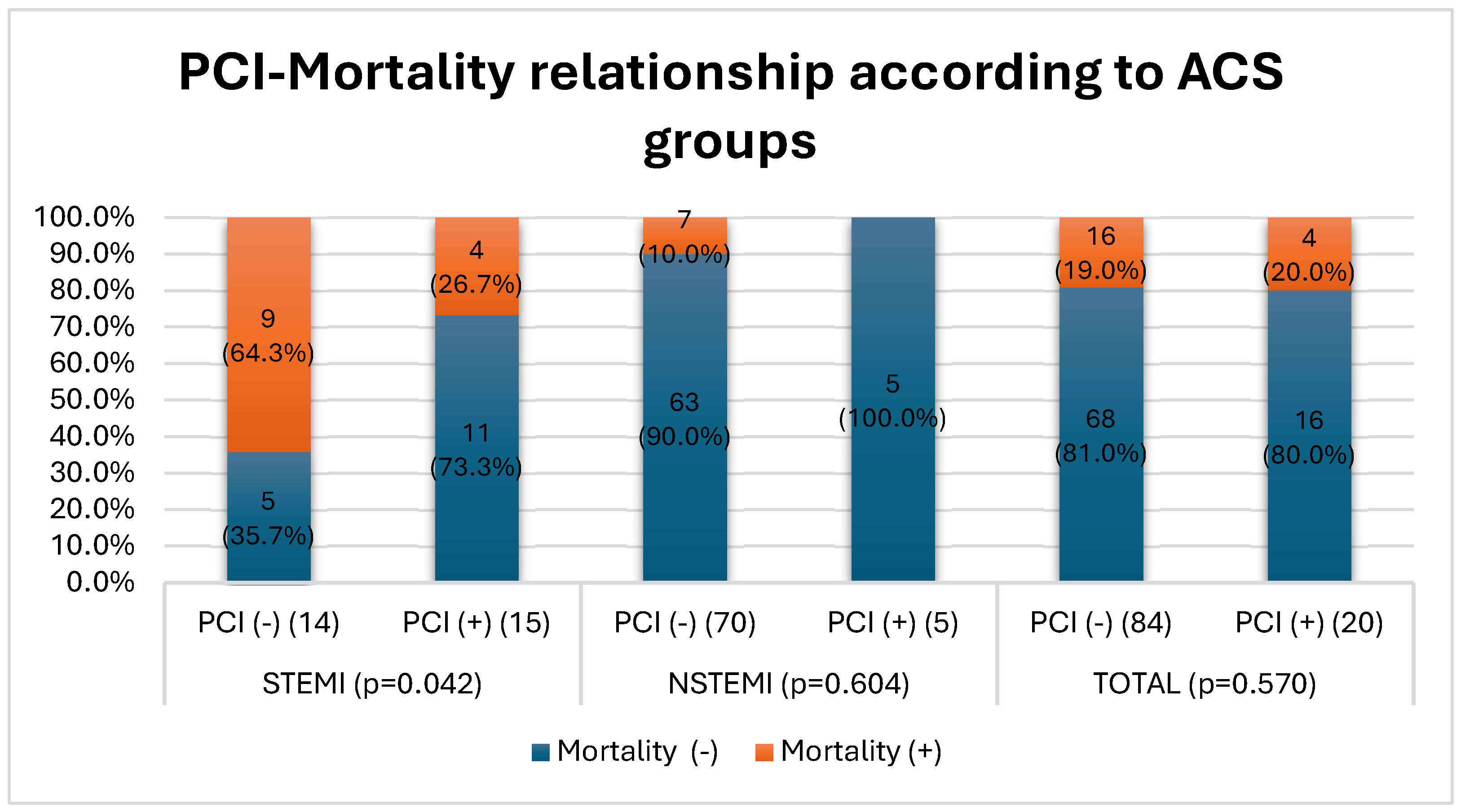
Objective: With the growing number of individuals over the age of 90 (nonagenarians), understanding the risk factors and clinical outcomes associated with acute coronary syndrome (ACS) in this population has become increasingly important. This study aims to compare demographic, biochemical, and clinical parameters between nonagenarian ACS patients and a control group of healthy individuals within the same age bracket as well as to analyze differences within the ACS group according to myocardial infarction type and evaluate the impact of percutaneous coronary intervention (PCI) on in-hospital mortality. Methods: This retrospective case-control study included 104 patients aged 90-100 years diagnosed with ACS for the first time between January 2022 and January 2024. The patients were categorized into ST-elevation myocardial infarction (STEMI) and non-ST-elevation myocardial infarction (NSTEMI) groups based on their electrocardiographic findings. The control group consisted of 113 healthy individuals in the same age range who had no history of coronary artery disease. Data on traditional risk factors, including lipid profiles and family history, were analyzed using logistic regression models. Additionally, differences in clinical outcomes, including length of hospital stay and mortality rates, were evaluated based on the application of PCI. Results: The ACS group exhibited significantly higher glucose, white blood cell count, and total cholesterol levels, along with lower hemoglobin and mean corpuscular volume, compared to the control group (p<0.05). While no significant difference was found in low-density lipoprotein (LDL) levels, high-density lipoprotein (HDL) levels were significantly lower in ACS patients (p<0.001). Family history played a more substantial role in the STEMI group compared to the NSTEMI group (p=0.049). Additionally, STEMI patients were more likely to undergo invasive procedures, which were associated with reduced in-hospital mortality (p=0.042). In contrast, no significant difference in mortality was observed in the NSTEMI group based on PCI status. Conclusion: This study highlights the distinct risk profiles of elderly ACS patients, emphasizing the critical role of low HDL levels and family history, particularly in STEMI cases. Furthermore, PCI was shown to reduce in-hospital mortality rates in STEMI patients, suggesting that invasive treatment approaches may be beneficial even in this vulnerable population. Personalized and multidisciplinary management strategies are essential for this vulnerable population. Further prospective research is needed to validate these findings and guide clinical decision-making for nonagenarians.
Keywords:
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. Risk Factors for ACS Development
4.2. Differences According to ACS Groups
4.3. Invasive Treatment and Mortality Reduction
4.4. Limitations and Significance of the Study
5. Conclusions
References
- Population Division, Department of Economic and Social Affairs. World Population Prospects 2024, Online Edition. United Nations; 2024.
- Leucker TM, Gerstenblith G, editors. Cardiovascular Disease in the Elderly. Cham: Springer International Publishing; 2023. [CrossRef]
- Mostaza JM, Lahoz C, Salinero-Fort MA, Cardenas J. Cardiovascular disease in nonagenarians: Prevalence and utilization of preventive therapies. Eur J Prev Cardiolog 2019;26:356–64. [CrossRef]
- Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, et al. Heart Disease and Stroke Statistics—2023 Update: A Report From the American Heart Association. Circulation 2023;147. [CrossRef]
- Rich MW. Epidemiology, Clinical Features, and Prognosis of Acute Myocardial Infarction in the Elderly. American J Geri Cardiology 2006;15:7–13. [CrossRef]
- Forman DE, Maurer MS, Boyd C, Brindis R, Salive ME, Horne FM, et al. Multimorbidity in older adults with cardiovascular disease. Journal of the American College of Cardiology 2018;71:2149–61.
- Couture EL, Farand P, Nguyen M, Allard C, Wells GA, Mansour S, et al. Impact of an invasive strategy in the elderly hospitalized with acute coronary syndrome with emphasis on the nonagenarians. Cathet Cardio Intervent 2018;92. [CrossRef]
- Shah P, Najafi AH, Panza JA, Cooper HA. Outcomes and Quality of Life in Patients ≥85 Years of Age With ST-Elevation Myocardial Infarction. The American Journal of Cardiology 2009;103:170–4. [CrossRef]
- Cepas-Guillén PL, Echarte-Morales J, Caldentey G, Gómez EM, Flores-Umanzor E, Borrego-Rodriguez J, et al. Outcomes of Nonagenarians With Acute Coronary Syndrome. Journal of the American Medical Directors Association 2022;23:81-86.e4. [CrossRef]
- Goel K, Gupta T, Gulati R, Bell MR, Kolte D, Khera S, et al. Temporal Trends and Outcomes of Percutaneous Coronary Interventions in Nonagenarians. JACC: Cardiovascular Interventions 2018;11:1872–82. [CrossRef]
- Jokhadar M. Review of the treatment of acute coronary syndrome in elderly patients. CIA 2009:435. [CrossRef]
- Zimmerman FH, Cameron A, Fisher LD, Grace N. Myocardial infarction in young adults: Angiographic characterization, risk factors and prognosis (coronary artery surgery study registry). Journal of the American College of Cardiology 1995;26:654–61. [CrossRef]
- Ferrucci L, Fabbri E. Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nature Reviews Cardiology 2018;15:505–22.
- Liberale L, Montecucco F, Tardif J-C, Libby P, Camici GG. Inflamm-ageing: the role of inflammation in age-dependent cardiovascular disease. European Heart Journal 2020;41:2974–82.
- García-Blas S, Cordero A, Diez-Villanueva P, Martinez-Avial M, Ayesta A, Ariza-Solé A, et al. Acute Coronary Syndrome in the Older Patient. JCM 2021;10:4132. [CrossRef]
- Kannel WB. Factors of Risk in the Development of Coronary Heart Disease—Six-Year Follow-up Experience: The Framingham Study. Ann Intern Med 1961;55:33. [CrossRef]
- Kannel WB. Coronary heart disease risk factors in the elderly. The American Journal of Geriatric Cardiology 2002;11:101–7.
- Wenger NK. Dyslipidemia as a risk factor at elderly age. Am J Geriatr Cardiol 2004;13:4–9.
- Krumholz HM, Seeman TE, Merrill SS, de Leon CFM, Vaccarino V, Silverman DI, et al. Lack of association between cholesterol and coronary heart disease mortality and morbidity and all-cause mortality in persons older than 70 years. Jama 1994;272:1335–40.
- Madhavan MV, Gersh BJ, Alexander KP, Granger CB, Stone GW. Coronary artery disease in patients≥ 80 years of age. Journal of the American College of Cardiology 2018;71:2015–40.
- Liu X-M, Ma C-S, Liu X-H, Du X, Kang J-P, Zhang Y, et al. Relationship between red blood cell distribution width and intermediate-term mortality in elderly patients after percutaneous coronary intervention n.d.
- Xanthopoulos A, Tryposkiadis K, Dimos A, Bourazana A, Zagouras A, Iakovis N, et al. Red blood cell distribution width in elderly hospitalized patients with cardiovascular disease. WJC 2021;13:503–13. [CrossRef]
- Weijenberg MP, Feskens EJM, Kromhout D. White Blood Cell Count and the Risk of Coronary Heart Disease and All-Cause Mortality in Elderly Men. ATVB 1996;16:499–503. [CrossRef]
- Yayan J. Association of traditional risk factors with coronary artery disease in nonagenarians: the primary role of hypertension. Clinical Interventions in Aging 2014:2003–12.
- Di Stefano R, Di Bello V, Barsotti MC, Grigoratos C, Armani C, Dell’Omodarme M, et al. Inflammatory markers and cardiac function in acute coronary syndrome: Difference in ST-segment elevation myocardial infarction (STEMI) and in non-STEMI models. Biomedicine & Pharmacotherapy 2009;63:773–80. [CrossRef]
- Sugiyama T, Hasegawa K, Kobayashi Y, Takahashi O, Fukui T, Tsugawa Y. Differential Time Trends of Outcomes and Costs of Care for Acute Myocardial Infarction Hospitalizations by ST Elevation and Type of Intervention in the United States, 2001–2011. JAHA 2015;4:e001445. [CrossRef]
- Sheldon M, Blankenship JC. STEMI in nonagenarians: Never too old. Cathet Cardio Intervent 2022;100:17–8. [CrossRef]
- From AM, Rihal CS, Lennon RJ, Holmes DR, Prasad A. Temporal Trends and Improved Outcomes of Percutaneous Coronary Revascularization in Nonagenarians. JACC: Cardiovascular Interventions 2008;1:692–8. [CrossRef]
- Sawant AC, Josey K, Plomondon ME, Maddox TM, Bhardwaj A, Singh V, et al. Temporal Trends, Complications, and Predictors of Outcomes Among Nonagenarians Undergoing Percutaneous Coronary Intervention. JACC: Cardiovascular Interventions 2017;10:1295–303. [CrossRef]
- Tokarek T, Siudak Z, Dziewierz A, Rakowski T, Krycińska R, Siwiec A, et al. Clinical outcomes in nonagenarians undergoing a percutaneous coronary intervention: data from the ORPKI Polish National Registry 2014–2016. Coronary Artery Disease 2018;29:573–8. [CrossRef]
- Antonsen L, Jensen LO, Terkelsen CJ, Tilsted H, Junker A, Maeng M, et al. Outcomes after primary percutaneous coronary intervention in octogenarians and nonagenarians with ST-segment elevation myocardial infarction: From the Western Denmark heart registry. Cathet Cardio Intervent 2013;81:912–9. [CrossRef]
- Oh S, Jeong MH, Cho KH, Kim MC, Sim DS, Hong YJ, et al. Outcomes of Nonagenarians with Acute Myocardial Infarction with or without Coronary Intervention. JCM 2022;11:1593. [CrossRef]
- Lee KH, Ahn Y, Kim SS, Rhew SH, Jeong YW, Jang SY, et al. Characteristics, In-Hospital and Long-Term Clinical Outcomes of Nonagenarian Compared with Octogenarian Acute Myocardial Infarction Patients. J Korean Med Sci 2014;29:527. [CrossRef]
- Wu Y-J, Hou CJ-Y, Chou Y-S, Tsai C-H. Percutaneous coronary intervention in nonagenarians. Acta Cardiologica Sinica 2004;20:73–82.
- Sahin M, Ocal L, Kalkan AK, Kilicgedik A, Kalkan ME, Teymen B, et al. In-Hospital and long term results of primary angioplasty and medical therapy in nonagenarian patients with acute myocardial infarction. J Cardiovasc Thorac Res 2017;9:147–51. [CrossRef]

| CONTROL | ACS | p | |
| n | 113 (52.3) | 104 (47.7) | |
| Age | 91±7 2.2 | 91.3±1.8 | 0.302 |
| Male | 40 (35.4) | 38 (36.5) | 0.861 |
| BMI | 26.6±3.3 | 26.9±4.8 | 0.896 |
| Smoking | 35 (31.0) | 38 (36.9) | 0.358 |
| HT | 91 (80.5) | 72 (%69.9) | 0.070 |
| DM | 27 (23.9) | 25 (24.0) | 0.980 |
| Family history | 51 (45.1) | 33 (32.0) | 0.049 |
| Biochemical Parameters | |||
| Hgb(g/dL) | 12.4±1.4 | 11.8±1.8 | 0.008 |
| MCV (fL) | 89.6±6.9 | 87.4±6.8 | 0.009 |
| RDW (%) | 15.1±1.9 | 15.6±2.0 | 0.020 |
| WBC (103/µL) | 7.2±1.7 | 10.1±3.7 | <0.001 |
| PLT (103/µL) | 229.2±77.9 | 232.5±82.4 | 0.902 |
| MPV (fL) | 9.4±1.9 | 8.7±1.5 | 0.021 |
| glucose (mg/dL) | 111.3±32.0 | 152.9±71.7 | <0.001 |
| HbA1c (%) | 6.23±0.9 | 6.29±1.01 | 0.910 |
| Creatinine (mg/dL) | 1.09±0.3 | 1.16±0.52 | 0.517 |
| Lipid Profiles | |||
| TC (mg/dL) | 197.9±44.1 | 179.6±42.7 | 0.003 |
| LDL (mg/dL) | 119.7 ±36.9 | 115.0±36.2 | 0.272 |
| TG (mg/dL) | 114.6±47.7 | 123.4±47.7 | 0.612 |
| HDL (mg/dL) | 55.5±15.9 | 38.6±12.1 | <0.001 |
| AIP | 0.299±0.24 | 0.485±0.264 | <0.001 |
| NSTEMI | STEMI | p | |
| n | 75 (72.1) | 29 (27.9) | |
| Age | 91.3±2.1 | 90.8±1.40 | 0.442 |
| Male | 24 (32) | 14 (48.3) | 0.122 |
| BMI | 27.1±5.6 | 27.4±3.1 | 0.865 |
| Smoking | 26 (35.1) | 12 (41.4) | 0.555 |
| HT | 55 (74.3) | 17 (58.6) | 0.118 |
| DM | 21 (28.0) | 4 (13.8) | 0.128 |
| Family history | 15 (20.3) | 18 (62.1) | <0.001 |
| Biochemical Parameters | |||
| Hgb | 11.9±1.8 | 11.2±1.8 | 0.142 |
| MCV (fL) | 86.6±6.7 | 87.7±8.3 | 0.893 |
| RDW (%) | 15.4±1.8 | 16.1±2.8 | 0.324 |
| WBC (103/µL) | 9.78±3.70 | 11.48±4.20 | 0.030 |
| PLT (103/µL) | 233.5±90.3 | 231.2±59.1 | 0.798 |
| MPV (fL) | 8.93±1.60 | 8.31±1.03 | 0.721 |
| Glucose (mg/dL) | 152.5±73.9 | 145.4±67.5 | 0.364 |
| HbA1c (%) | 6.40±0.99 | 6.15±1.14 | 0.422 |
| Creatinine (mg/dL) | 1.12±0.52 | 1.18±0.48 | 0.522 |
| Lipid Profiles | |||
| TC (mg/dL) | 177.4±38.7 | 187.3±54.9 | 0.461 |
| LDL (mg/dL) | 112.2±33.4 | 124.9±44.4 | 0.167 |
| TG (mg/dL) | 127.7±70.7 | 108.0±41.9 | 0.285 |
| HDL (mg/dL) | 39.1±12.5 | 36.9±10.9 | 0.426 |
| AIP | 0.486±0.284 | 0.460±0.182 | 0.627 |
| CAG | 8 (10.7) | 19 (65.5) | <0.001 |
| PCI | 5 (6.7) | 15 (51.7) | <0.001 |
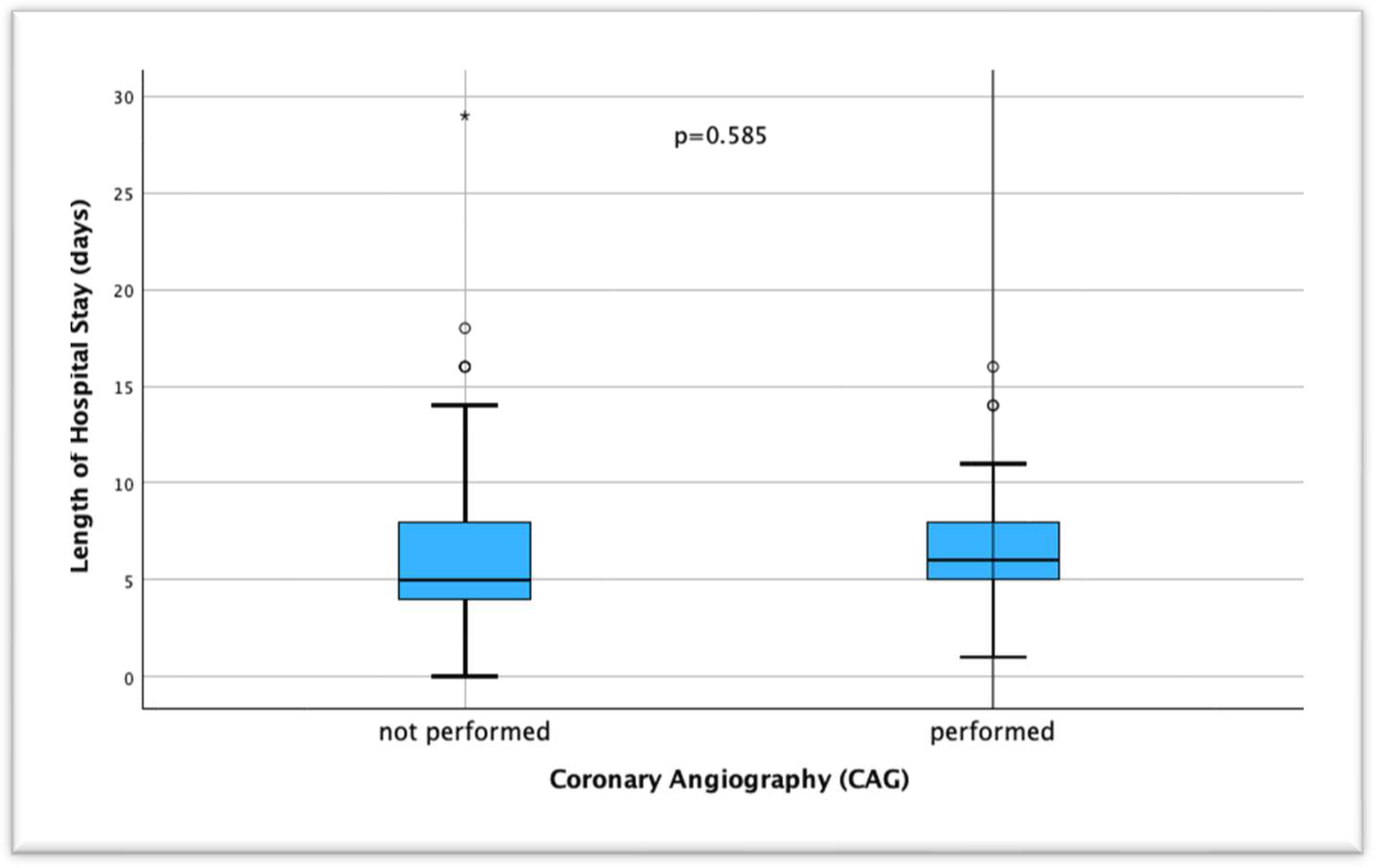
| Length of hospital stay (days) | 5.7±4.3 | 6.6±4.1 | 0.781 |
| Mortality | 7 (9.3) | 13 (44.8) | <0.001 |
| ACS | ||
| 95% CI | p | |
| Sex | 0.905 (0.482-1.699) | 0.755 |
| Family history | 0.492 (0.264-0.917) | 0.026 |
| Smoking | 1.868 (0.955-3.655) | 0.068 |
| HT | 0.525 (0.268-1.027) | 0.060 |
| DM | 1.038 (0.533-2.024) | 0.912 |
| Dyslipidemia | 1.953 (1.034-3.692) | 0.039 |
| Obesity | 1.777 (0.856-3.687) | 0.123 |
| Crude OR | Adjusted OR | ||
|
Model 0 OR (95% CI) p value |
Model 1 OR (95% CI) p value |
Model 2 OR (95% CI) p value |
|
| High LDL | 0.544 (0.287-1.033) 0.063 |
0.528 (0.277-1.009) 0.053 |
0.440 (0.222-0.872) 0.019 |
| High TG | 1.054 (0.460-2.416) 0.901 |
0.980 (0.416-2.307) 0.962 |
1.047 (0.424-2.585) 0.921 |
| Low HDL | 5.534 (2.615-11.713) <0.001 |
5.619 (2.648-11.921) <0.001 |
5.554 (2.536-12.160) <0.001 |
| High AIP | 0.933 (0.406-2.142) 0.869 |
0.955 (0.415-2.202) 0.915 |
1.061 (0.439-2.564) 0.895 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



