Submitted:
03 February 2025
Posted:
04 February 2025
You are already at the latest version
Abstract
Vitamin D (VD) is a fat-soluble steroid hormone with crucial physiological functions beyond calcium and bone metabolism. In recent years, the role of VD in women’s reproductive health has garnered significant attention. It has been implicated in ovarian function, follicular development, endometrial receptivity, and the regulation of steroid hormone production. VD deficiency has been associated with a range of reproductive health disorders, including Polycystic Ovarian Syndrome (PCOS), endometriosis, and infertility. Studies indicate that up to 40-50% of healthy pregnant women exhibit deficient serum VD levels, which may be linked to adverse pregnancy outcomes and impaired fertility. VD plays a key role in regulating ovarian function, promoting proper follicular development, and modulating the immune response in reproductive tissues. Its deficiency has been linked to insulin resistance, hormonal imbalances, and inflammatory processes, all of which contribute to the pathophysiology of reproductive disorders. This review synthesizes current research on VD's therapeutic potential in managing these disorders and enhancing fertility outcomes, emphasizing the importance of maintaining adequate VD levels for optimal reproductive health. Understanding the reference values for VD in reproductive medicine is essential for optimizing fertility treatments and improving clinical outcomes in women with reproductive health disorders.
Keywords:
Vitamin D
; Reproductive Health
; Fertility
; Infertility
; Endometriosis
; Polycystic Ovarian Syndrome
1. Introduction
VD is a fat-soluble substance essential for overall health, extending beyond its well-known role in bone metabolism to influence various physiological processes. The biologically active form, calcitriol (1,25(OH)2D3), exerts its effects through both genomic and non-genomic mechanisms [1]. Genomically, VD binds to the cytoplasmic vitamin D receptor (VDR), while non-genomic actions occur via interactions with membrane-bound VDR. These receptors are distributed throughout the human body, including reproductive tissues in both males and females [2,3].
In the male reproductive system, VDR is expressed in Sertoli and Leydig cells, germ cells, developing spermatozoa, and mature sperm. In females, VDR is present in the uterus, ovaries, and reproductive tract, as well as in the placenta during pregnancy [4]. Given its widespread distribution, VD plays a pivotal role in reproductive health by regulating processes such as ovarian steroidogenesis, folliculogenesis, spermatogenesis, and acrosome reaction. Moreover, VD levels have been correlated with sperm quality and ovarian reserve, underscoring its relevance in fertility [5].
Deficiencies in VD have been implicated in reproductive disorders, including polycystic ovarian syndrome (PCOS), endometriosis, and infertility. Observational studies suggest that inadequate VD levels may negatively impact reproductive function by influencing hormonal balance, follicular development, and implantation processes [6]. Additionally, VD plays a role in conception and placental development, emphasizing its significance in sustaining reproductive health.
VD plays a multifaceted role in fertility, with studies indicating that adequate levels are associated with improved ovarian reserve and enhanced outcomes in assisted reproductive technologies like in vitro fertilization (IVF) [7]. Conversely, VD deficiency has been linked to reduced anti-Müllerian hormone (AMH) levels, a key marker of ovarian reserve, and decreased fertility potential [8]. In PCOS, a prevalent endocrine disorder marked by hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology, 67–85% of affected women exhibit serum 25-hydroxy VD levels below 20 ng/mL, correlating with insulin resistance, menstrual irregularities, hyperandrogenism, and heightened cardiovascular risk factors [9,10]. VD supplementation has demonstrated potential in mitigating these manifestations by improving menstrual regularity, enhancing folliculogenesis, and lowering serum testosterone levels, making it a promising adjunctive therapy in PCOS management. Regarding endometriosis, a chronic condition characterized by the ectopic growth of endometrial-like tissue, VD’s role remains complex. Some studies suggest that VD modulates immune responses and inflammation, potentially influencing disease progression, while others find no significant effect of VD supplementation on symptoms [11,12].
Given the accumulating evidence linking VD to reproductive function and pathology, this review aims to critically evaluate the molecular and endocrine mechanisms underlying VD’s influence on fertility, endometriosis, and PCOS. By synthesizing recent findings, this analysis seeks to elucidate VD’s potential as a therapeutic target for improving reproductive health and fertility outcomes.
2. Vitamin D Structure and Metabolism
VD is a fat-soluble steroid hormone with diverse physiological roles. Among its functions, VD acts as an immunomodulator and anti-proliferative mediator while also playing a pivotal role in maintaining calcium, magnesium, and phosphate homeostasis [13]. Recent studies report that up to 40-50% of healthy pregnant women exhibit deficient serum VD levels (≤20 ng/ml), despite concentrations below 30 ng/ml now being recognized as inadequate [14]. VD deficiency is associated with a range of adverse outcomes during pregnancy, including congenital abnormalities, and is a notable risk marker for complications. Furthermore, inadequate VD levels have been linked to fertility challenges and reduced success rates in IVF [13,14].
The primary source of VD synthesis is cutaneous production, accounting for approximately 90% of total VD through ultraviolet (UV) light exposure, while dietary intake contributes the remaining 10% [15]. Foods with high VD concentrations include fatty fish, beef liver, cheese, egg yolks, and fortified milk [16]. Lesser amounts of VD are found in mushrooms, cereals, chicken, beef, and various vegetables. The recommended daily intake is 600 IU for individuals under 70 years old and 800 IU for those over 70 [17].
VD is a steroid hormone with two primary forms: vitamin D2 (D2) and vitamin D3 (D3). D3 is synthesized in the skin from 7-dehydrocholesterol (7-DHC) upon ultraviolet B (UVB) exposure, while D2 is derived from ergosterol in plants and fungi, typically obtained through dietary sources [18,19]. Both forms of VD circulate in the bloodstream bound to the vitamin D-binding protein (DBP) and undergo sequential hydroxylation in the liver and kidneys.
In the liver, D2 and D3 are hydroxylated by 25-hydroxylase to form 25-hydroxyvitamin D (25-OH-VD or calcifediol), the major circulating form with a half-life of approximately 14 days [20]. Calcifediol is subsequently hydroxylated by 1-alpha-hydroxylase in the kidneys, producing the biologically active metabolite, 1,25-dihydroxyvitamin D (1,25-OH-2D or calcitriol). This active form plays a crucial role in calcium and phosphate homeostasis and regulates cellular processes integral to reproductive health [20,21]. Notably, 1-alpha-hydroxylase is also expressed in extra-renal tissues, including the ovaries, brain, mammary glands, prostate, and colon, allowing localized synthesis of active VD [22,23].
Calcitriol exerts its physiological effects by binding to the vitamin D receptor (VDR) in target tissues, such as the uterus and ovaries, to modulate gene expression and cellular functions. Its actions are essential for reproductive health, influencing calcium absorption, steroidogenesis, and immune modulation. These functions are particularly relevant in fertility and endometriosis, where VD impacts ovarian function, implantation, and inflammation [24].
The degradation of VD metabolites occurs through two primary pathways: the C24 oxidation and the C23 lactone pathways. These pathways, mediated by CYP24A1 (24-hydroxylase), convert calcifediol and calcitriol into their inactive forms, such as calcitroic acid, which are excreted in bile and feces. Tight regulation of these metabolic processes ensures a balance of calcitriol levels, preventing toxicity and maintaining calcium homeostasis, which is particularly crucial during pregnancy and in conditions such as endometriosis [20,21].
The hormonal form of VD, 1,25(OH)2D, exhibits paracrine and autocrine functions across a range of tissues, including the skin, immune system, parathyroid gland, intestinal epithelium, hypothalamic-pituitary axis, prostate, and breast. These biological actions are mediated by the VDR, which is widely distributed in cells, including those within the reproductive system [19].The interaction of the hypothalamic-pituitary axis with VDR underscores a potential regulatory role in reproductive physiology. This axis coordinates reproductive function through hormonal signaling pathways, with the hypothalamus releasing hormones that stimulate the pituitary gland to secrete reproductive hormones targeting the gonads [25].
VDR expression is notably prevalent in the female reproductive system, including the ovaries, uterus, placenta, and endometrium. Within ovarian follicles, VDR facilitates the physiological actions of 1,25(OH)2D3, underscoring its critical involvement in gonadal function [19,25]. These findings highlight the direct implications of VD in fertility and broader aspects of reproductive health, establishing its significance in gynecological endocrinology and metabolism.
Figure 1.
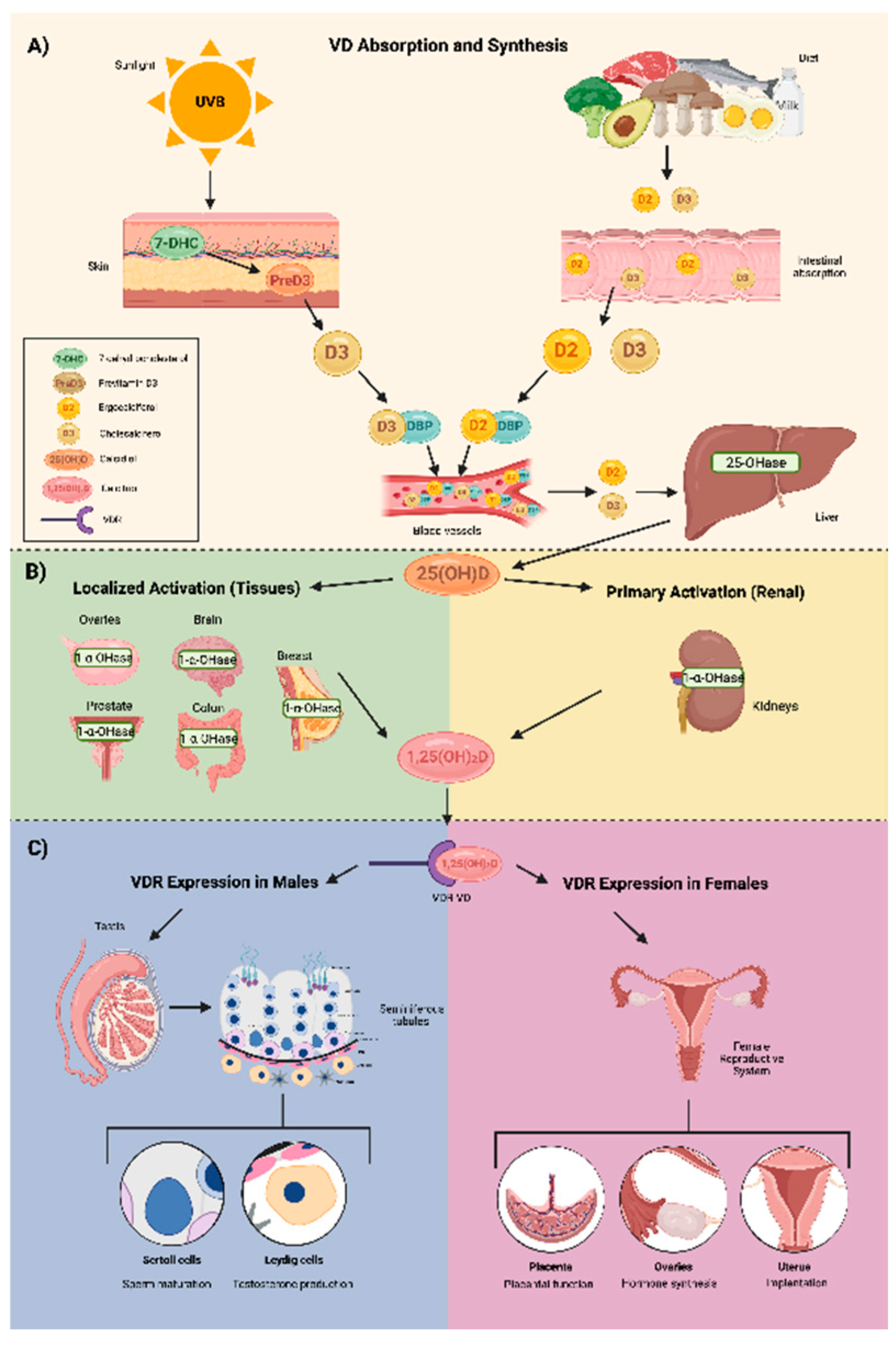
This figure illustrates the role of VD in synthesis, activation, and reproductive health. A) VD absorption and synthesis: VD is obtained from UVB exposure and dietary sources, leading to the formation of cholecalciferol (D3) and ergocalciferol (D2), which undergo hydroxylation in the liver and kidneys to become the active form, calcitriol (1,25(OH)₂D). B) Activation: Calcitriol is synthesized in the kidneys and locally in various tissues, including the ovaries, prostate, brain, colon, and breast, through 1-α hydroxylase activity. C) VDR expression in reproductive health: In males, VDR is present in Sertoli and Leydig cells, influencing sperm maturation and testosterone production. In females, VDR plays a role in placental function, ovarian hormone synthesis, and uterine implantation, processes that are often disrupted in endometriosis and PCOS, contributing to infertility.
Figure 1.
This figure illustrates the role of VD in synthesis, activation, and reproductive health. A) VD absorption and synthesis: VD is obtained from UVB exposure and dietary sources, leading to the formation of cholecalciferol (D3) and ergocalciferol (D2), which undergo hydroxylation in the liver and kidneys to become the active form, calcitriol (1,25(OH)₂D). B) Activation: Calcitriol is synthesized in the kidneys and locally in various tissues, including the ovaries, prostate, brain, colon, and breast, through 1-α hydroxylase activity. C) VDR expression in reproductive health: In males, VDR is present in Sertoli and Leydig cells, influencing sperm maturation and testosterone production. In females, VDR plays a role in placental function, ovarian hormone synthesis, and uterine implantation, processes that are often disrupted in endometriosis and PCOS, contributing to infertility.
3. Vitamin D Deficiency
VD deficiency is a global health concern, with prevalence rates varying by geographic region, age, and other socio-demographic factors. In particular, it is a widespread issue in both developed and developing countries, with significant implications for women's reproductive health. Elevated body mass index (BMI) and specific ethnicities, particularly Asian and African-American populations, have been identified as significant risk factors for VD deficiency, with Asian individuals at particularly high risk [18]. A comprehensive epidemiological study conducted across Mexico, Chile, and Brazil revealed that the Mexican population exhibited the highest prevalence of VD deficiency, with 67% of postmenopausal women affected [17]. In particular, individuals with obesity have lower bioavailability of VD due to its sequestration in adipose tissue, which leads to suboptimal circulating levels [21]. These findings are concerning as VD is essential not only for skeletal health but also for optimal reproductive function [26]. The broad epidemiological data indicate that anyone, regardless of their health status or demographic characteristics, may be vulnerable to VD deficiency, making it an important public health concern globally [20,27].
4. Correlation Between Vitamin D with Ovarian Reserve, Steroidogenesis, and Follicular Development
VD exhibits anti-inflammatory and immunomodulatory effects, it has shown to contribute to immune regulation by suppressing pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin-1 (IL-1), and IL-6, while enhancing the expression of anti-inflammatory cytokines [28,29]. A significant correlation between VD levels and follicular development has been observed, suggesting that VD is essential for proper ovarian function and fertility [30].
In particular, research by Safaei et al (2020), demonstrated that VD affects the expression of crucial genes involved in follicular development and steroidogenesis in human granulosa cells. The study reported that the presence of VD in granulosa cell cultures increased the mRNA expression of AMH and the follicle-stimulating hormone (FSH) receptor gene, both of which play pivotal roles in follicular maturation and selection [31,32]. Moreover, the presence of the VDR in ovarian tissues has been confirmed, and stimulating granulosa cells with calcitriol resulted in increased production of important reproductive hormones such as progesterone, estradiol, and estrone [33,34]. These findings collectively suggest that VD has a critical role in regulating follicular development and steroid hormone production.
Additionally, a correlation has been observed between VD concentrations in serum and follicular fluid, indicating that VD may be crucial for follicular maturity and development [30]. A meta-analysis conducted by McLaughlin et al. (2021), concluded that higher circulating VD levels in women undergoing IVF are associated with increased rates of live births. This emphasizes the role of adequate VD concentrations in supporting reproductive success during assisted reproduction treatments [35,36].
Recent studies have also explored the influence of VD levels on the expression of transcription factors critical for reproductive health. The HOXA10 and HOXA11 genes, which play key roles in the development of reproductive tissues, are expressed in the endometrial stromal cells of adult women [37]. These transcription factors are essential for the success of embryo implantation and fertility, as they facilitate continuous tissue proliferation and differentiation [38]. Research by Ozkan et al (2019), revealed that adequate VD levels are associated with higher expression of HOXA10 mRNA, particularly during the luteal phase of the menstrual cycle, which is crucial for implantation and endometrial receptivity [39]. In contrast, women with VD deficiency or insufficiency exhibit reduced expression of HOXA10, potentially impairing reproductive outcomes [40].
Further supporting these findings, Ozkan et al (2019), conducted a prospective cohort study that showed women with higher VD levels in follicular fluid were significantly more likely to achieve successful implantation and pregnancy, with gestational sacs detected on ultrasonography, whether intrauterine or ectopic [40]. Similarly, a retrospective study by Rudick et al (2020), found that VD insufficiency was linked to lower clinical pregnancy rates in women undergoing assisted reproductive treatments, further emphasizing the importance of maintaining optimal VD levels for reproductive success [37].
5. Vitamin D Receptor on Reproductive-Associated Tissues
VD plays a significant role in fertility, with its importance emphasized by the widespread distribution of the VDR in both central and peripheral reproductive tissues in males and females [23]. VDRs have been detected in various reproductive organs and cells, including the hypothalamus, pituitary gland, ovaries, granulosa cells, endometrium, placenta, decidua, testicles, and spermatogenesis cells [41,42]. The human placenta expresses CYP27B1, which encodes the enzyme 1-alpha hydroxylase responsible for converting VD into its active form, calcitriol. This suggests that the placenta can synthesize active VD, which is critical for regulating pregnancy outcomes, immune responses, and placental development [43]. In the pituitary gland, it plays a role in regulating the secretion of hormones involved in ovulation and menstrual cycle control. The presence of VDR in the endometrium suggests that VD may regulate uterine lining preparation for implantation. The endometrium expresses the CYP27B1 gene, which encodes 1-α-hydroxylase, the enzyme responsible for locally converting 25(OH)D3 into its active form, 1,25(OH)2D3 [43,44]. The first study to demonstrate the presence of VDR in human endometrial tissue was conducted in 2004 by Vienonen et al, who investigated the expression pattern of nuclear receptors and co-factors in the endometrium using real-time PCR. Notable differences in expression levels were reported among individuals based on age, but no difference in receptor expression was found between the proliferative and secretory phases of the menstrual cycle [45]. Subsequently, Bergadà and Cols in 2014 demonstrated that there are indeed differences in VDR expression according to the menstrual cycle, reporting a decrease in total VDR expression in the proliferative endometrium, contrasting with an increase in VDR protein expression during the secretory phase [46]. A systematic review by Cermisoni et al. (2018), confirmed that VDR is expressed in the ovaries, endometrium, and myometrium, highlighting VD’s involvement in fertility and reproductive health [47]. These findings suggest that VD may play a role in endometrial remodeling and preparation for embryo implantation, particularly during the secretory phase.
In male reproductive organs, including the testis, epididymis, and prostate, VDR plays an important role specifically in testicular somatic and germ cells [43]. These are capable of synthesizing and breaking down Testicular somatic and germ cells appear capable of synthesizing and breaking down VD independently of systemic metabolism. Furthermore, VDR expression in the testes indicates that VD may exert autocrine and paracrine effects, potentially contributing to testicular function regulation and influencing male fertility independently of systemic metabolism [48].
These findings collectively underscore the essential role of VD and its receptor in regulating multiple aspects of reproductive function, ranging from steroidogenesis in the ovaries to endometrial receptivity and immune regulation during pregnancy.
6. Vitamin D and Fertility
Low serum levels of VD may adversely affect female fertility by influencing ovarian function, implantation, and embryo development. In a study conducted by Pal et al. (2018), it was found that women with VD deficiency exhibited a significantly lower ovarian reserve and an increased risk of anovulation, both of which are critical factors influencing fertility outcomes [24].
Infertility, as defined by the International Glossary on Infertility and Fertility Care, refers to the inability to achieve a clinical pregnancy after 12 months of regular, unprotected intercourse or due to an impairment in reproductive capacity [49]. While the International Society of Endocrinology provides general guidelines for serum VD concentrations, considering levels over 30 ng/mL as optimal, those between 21-29 ng/mL as insufficient, and below 20 ng/mL as deficient, there are currently no precise criteria to define VD deficiency in the context of infertility [50,51]. A prospective cohort study by Jukic et al. (2019) demonstrated that fertility outcomes improve with higher VD levels, with each 10 ng/mL increase in 25-OH-VD correlating to a 10% higher fertilization rate. Women with 25-OH-VD levels below 20 ng/mL experienced a 45% reduction in fertilization rates compared to those with levels between 30-40 ng/mL, emphasizing the importance of maintaining optimal VD levels for improved fertility outcomes [52].
Additionally, VD’s role in regulating immune function and reducing inflammation has been implicated in its effect on the uterine environment, particularly in terms of implantation and pregnancy maintenance [53]. VD influences the expression of several genes that are important for embryo development and implantation success, emphasizing its potential as a modulator of reproductive outcomes [54].
In females, VD levels are correlated with AMH levels, a marker of ovarian reserve and function [55]. AMH levels, which fluctuate seasonally, are notably lower in winter compared to summer, with a reduction of up to 18% during the colder months [56]. In males, VD also has a significant impact on testosterone levels, which is age-dependent. In adolescents, no significant relationship between VD and testosterone is observed. However, in older men, higher VD levels are positively correlated with increased testosterone production [57]. VD has also shown to influence spermatogenesis and sperm motility in the male reproductive system through its interaction with the CYP24A enzyme and the cAMP/PKA signaling pathways [58]. Studies have shown that maternal VD levels affect sperm selection during the fertilization process, facilitating key processes such as capacitation, hyperactivation, and acrosomal reaction, which are necessary for successful fertilization [41,56]. However, the exact mechanisms through which it exerts these effects remain inadequately understood, highlighting gaps in current research.
A study by Bacanakgil et al. (2022) revealed that higher serum concentrations of 25-hydroxyvitamin D (25-OH-VD) in women undergoing IVF were associated with better embryo quality and higher clinical pregnancy rates. [30] VD also influences telomere length and telomerase activity, which has been linked to a reduction in chromosomal abnormalities, thereby optimizing IVF outcomes. [30]
The SUNDRO study, which aimed to assess whether VD supplementation could improve IVF outcomes, found no significant difference between the VD supplementation group and the placebo group. Both groups achieved clinical pregnancies, with a slightly higher success rate in the placebo group (40% vs. 37%) [60]. However, the confidence intervals for the VD supplementation group were broader, suggesting that VD supplementation did not significantly improve clinical pregnancy rates in this cohort [61].
VD supplementation has been shown to enhance endometrial receptivity by modulating inflammatory markers and improving immune responses [54]. Although these findings are promising, the optimal dosage and duration of VD supplementation in infertile women remain areas of active research, as the therapeutic response may vary depending on individual characteristics such as baseline VD levels and comorbidities [62]. Table 1 emphasizes the most important studies regarding infertility and VD.
7. Vitamin D and PCOS
In women with PCOS, VD supplementation has been linked to improved insulin sensitivity and hormonal regulation, further supporting its use as a therapeutic strategy [70]. PCOS is a heterogeneous disease of unclear etiology and one of the most frequent endocrine disorders in females of reproductive age. Its prevalence ranges from 6–13%, depending on the diagnostic criteria [71]. The American College of Obstetrics and Gynecology (ACOG) defines PCOS as a disorder characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovaries [72]. The Rotterdam criteria, one of the most widely used diagnostic tools, it evaluates oligo- and/or anovulation, clinical or biochemical signs of hyperandrogenism (such as acne and hirsutism), and polycystic ovaries on transvaginal ultrasound when having 20 or more cysts or a volume of 10mL in any ovary [73].
Functional ovarian hyperandrogenism has been identified as the essential feature of PCOS, with genetic and environmental factors also playing a role. Patients with PCOS often present with abnormal ovarian androgenic function, resulting in elevated levels of insulin resistance, obesity, or luteinizing hormone (LH). Ovarian hyperandrogenism, combined with insulin-resistant hyperinsulinism, is considered the most significant factor in PCOS pathophysiology, followed by increased LH levels and obesity [74].
VD supplementation has shown promise in experimental models and clinical studies. VD has been found to decrease androgen levels and endometrial thickness in experimental PCOS rat models [75]. A randomized controlled trial demonstrated that ovulation in women with PCOS was directly related to VD levels, with higher VD levels increasing the probability of ovulation from 68% in cases with levels below 20 ng/mL to 78% in cases with levels above 30 ng/mL [76].
Low VD levels have been correlated with follicular arrest in women with PCOS. A study involving 60 women with PCOS found that a combination of VD, calcium, and metformin increased the number of dominant follicles [77,78]. Regarding insulin resistance in PCOS, low VD levels have been linked to metabolic syndrome, exacerbating its symptoms [79]. In a randomized, double-blind, placebo-controlled trial, Maktabi et al (2017), found that a VD supplementation of 50,000 IU decreased fasting plasma glucose (p = 0.02), reduced insulin levels (p = 0.004), and increased insulin sensitivity (p = 0.007) [80]. However, a more recent study found that VD supplementation reduced plasma glucose during an oral glucose tolerance test but had no other significant metabolic effects [81].
Hormones and endocrine markers have also been studied in relation to PCOS and VD. Davis et al. (2018), found that PCOS cases with androgen excess were more prevalent in VD-deficient patients (p = 0.06) [82]. Another randomized controlled trial found a significant treatment effect on the LH/FSH ratio (p = 0.022) but no significant effects on FSH and AMH levels in women with PCOS [83]. Table 2 demonstrates the most important studies regarding PCOS and VD.
8. Vitamin D and Endometriosis
Endometriosis is a chronic inflammatory disease dependent on estrogen, characterized by the presence of endometrium-like tissue in extrauterine locations (columnar epithelium and stroma), affecting 10% of women in reproductive age [94]. This ectopic tissue can be located in pelvic organs such as the bladder, ovaries, fallopian tubes, intestines, and abdominal wall. However, its presence has also been reported in extra-pelvic organs, such as the central nervous system (CNS), pleura and pericardium [95,96]. Endometriosis is accompanied by clinical manifestations such as chronic pelvic pain, dysmenorrhea, dyspareunia, bladder or intestinal dysfunction, and infertility [97].
The prevalence of endometriosis varies significantly depending on the population and diagnostic methods used. Globally, it affects 5-15% of women in reproductive age, with a peak incidence between 25-45 years. However, it is also observed in adolescents and less commonly, in postmenopausal women (2-5%) [96]. Prevalence estimates range from 2-11% in asymptomatic women, 5-50% in infertile women, and 5-21% in those hospitalized for pelvic pain [96,98]. In the U.S., incidence rates are highest in women aged 25-34 years, reaching up to 380.6 cases per 100,000 person-years [98,99]. In Mexico, insufficient emphasis has been placed on this pathology, making it challenging to obtain reliable epidemiological data. However, it is estimated that 34.5% of infertility cases are associated with endometriosis. Moreover, a higher prevalence has been observed in reproductive-age patients with Müllerian malformations [100].
Given its association with anti-inflammatory, immunomodulatory, and antiproliferative processes, VD has been emphasized as a potential supplement for the treatment and symptomatic improvement of endometriosis, as it may enhance cellular apoptosis and reduce inflammation [51,101]. The VDR is expressed in the healthy human endometrium and myometrium, as well as in patients with endometriosis, specifically in peritoneal endometriotic lesions. Moreover, immune cells have been shown to be present within endometrial lesions [102]. Additionally, a study by Delbandi et al. analyzed serum levels of 25(OH)D in Iranian women, including 56 healthy participants and 54 patients with endometriosis. The study found that patients with serum 25(OH)D levels below 20 ng/mL had a 2.7-fold higher risk of developing endometriosis compared to women with higher 25(OH)D levels [103,104].
Nodler et al. conducted a randomized trial involving 69 adolescent women aged 12-25 years, who were divided into three groups: 20 received fish oil supplements, 22 received a placebo, and 27 received VD supplementation. Among the three groups, the most significant improvement over a six-month period was observed in patients supplemented with VD, as reflected in the Visual Analog Scale (VAS) for pain. Initially, participants had an average VAS score of 7.0, which decreased to an average of 5.5 in the final month of the study [101].
Zheng et al. performed a systematic review and meta-analysis on the use of antioxidants such as VD, vitamin E (VE), and vitamin C (VC) to evaluate their effectiveness in reducing pelvic pain in patients with endometriosis. Their findings indicated that VD significantly reduces dysmenorrhea over a 12-month period when administered at a dose of 50,000 IU weekly or biweekly. However, VD did not show a significant improvement in dyspareunia compared to the placebo group [105]. Table 3 highlights the findings regarding VD and endometriosis.
9. Discussion
VD deficiency among women of reproductive age constitutes a significant public health concern, driven by factors such as inadequate dietary intake, limited sun exposure, and lifestyle changes. National supplementation programs, such as Denmark’s margarine fortification initiative, demonstrated reproductive benefits, including improved live birth rates in women diagnosed with infertility. These findings underscore the value of population-level interventions to address VD deficiency as a cost-effective strategy for enhancing reproductive outcomes [50,79].
A randomized controlled trial by Pal et al. (2016), demonstrated that higher VD levels were associated with a significant increase in ovulation rates among women with PCOS. This study, while providing valuable evidence, has limitations, including a relatively small sample size and a focus on a narrow patient group, which may limit the generalizability of its findings. Additionally, it did not establish an optimal dose of VD supplementation for maximal reproductive benefit. In contrast, a larger study by Maktabi et al. (2017), also found improvements in insulin sensitivity and metabolic markers in PCOS patients following VD supplementation, reinforcing the potential of VD in managing the metabolic aspects of PCOS [80]. However, the absence of consistent effects on other reproductive outcomes, such as follicular development and ovulation, suggests that VD’s impact may be more significant for managing metabolic dysregulation than for directly influencing fertility. This variability between studies underscores the need for more tailored research to identify which aspects of PCOS are most responsive to VD supplementation.
On the other hand, studies involving VD supplementation in women with endometriosis have yielded more inconsistent results. While some studies have reported a reduction in endometriotic lesion size and improved pain management with VD supplementation [102], others have failed to demonstrate significant clinical benefits [113]. These discrepancies may be attributed to differences in study methodologies, such as varying VD dosages, treatment durations, and patient populations. Moreover, the underlying pathophysiology of endometriosis is complex, and the mechanisms through which VD could influence disease progression are not fully understood. While VD’s potential anti-inflammatory properties and its role in immune modulation provide a plausible mechanism, further investigations are needed to establish definitive clinical guidelines for VD use in managing endometriosis.
Current research on VD’s role in reproductive health, while promising, is hindered by several limitations. One of the most significant challenges is the variability in VD supplementation protocols across studies. For instance, different studies have employed varying doses of VD (ranging from 1000 IU to 50,000 IU daily), without a consensus on the optimal dose for improving fertility outcomes [62]. Additionally, the duration of supplementation varies widely, with some studies using short-term regimens (e.g., 8-12 weeks) and others extending over several months. This inconsistency makes it difficult to draw definitive conclusions about the efficacy of VD supplementation in improving reproductive health outcomes [115].
Moreover, many studies have small sample sizes and lack long-term follow-up, limiting the robustness of their findings. Larger, multicenter trials are needed to confirm these findings and to establish the long-term effects of VD supplementation on fertility, especially in women with reproductive disorders such as PCOS and endometriosis.
Another challenge is the lack of standardized VD deficiency thresholds and treatment protocols. Studies often define VD deficiency differently, and the lack of universally accepted guidelines for VD levels in fertility and reproductive disorders complicates the interpretation and comparison of results. For example, while some studies use a threshold of 20 ng/mL for VD deficiency, others set it at 30 ng/mL, which may influence the observed outcomes [50,51]. These discrepancies highlight the need for future research to standardize VD deficiency criteria and supplementation regimens to ensure consistency across clinical studies.
Despite these limitations, the evidence suggests that VD supplementation could hold significant promise as a therapeutic strategy for improving fertility outcomes in women with PCOS, endometriosis, and other reproductive health disorders.
10. Conclusion
VD deficiency is a major public health challenge for women of reproductive age due to its implications for fertility. Scientific literature suggests that VD supplementation can enhance fertility outcomes, particularly in conditions such as endometriosis and PCOS. The primary benefit of VD supplementation appears to be its role in metabolic regulation, which in turn influences reproductive function. Additionally, some studies have demonstrated positive effects on metabolic markers and ovulation in both endometriosis and PCOS. However, the absence of standardized criteria for diagnosing VD deficiency and the lack of consensus on optimal supplementation regimens considering dosage, treatment duration, and individual patient needs remain significant limitations. Despite these challenges, VD supplementation emerges as a promising therapeutic strategy for improving reproductive health, particularly in individuals with documented deficiencies.
References
- Huhtakangas JA, Olivera CJ, Bishop JE, Zanello LP, Norman AW. The vitamin D receptor is present in caveolae-enriched plasma membranes and binds 1α, 25 (OH) 2-vitamin D3 in vivo and in vitro. Mol Endocrinol. 2004;18:2660–71.
- Kahlon Simon-Collins M, Nylander E, Segars J, Singh BBK. A systematic review of vitamin D and endometriosis: role in pathophysiology, diagnosis, treatment, and prevention. F&S Rev. 2022;4:1–14.
- Khurana, M., et al. (2021). Vitamin D and female reproductive health: A review of molecular mechanisms and clinical implications. Reproductive Health Journal, 18(1), 123-134. [CrossRef]
- Bouillon R. Vitamin D: from photosynthesis, metabolism, and action to clinical applications, endocrinology: adult and pediatric: vitamin D, 7th ed. Philadephia, PA: Elsevier, 2015:1018–37.10.1016/B978-0-323-18907-1.00059-7.
- Christakos S, Seth T, Wei R, Veldurthy V, Sun C, Kim KI, Kim KY, Tariq U, Dhawan P. Vitamin D and health: beyond bone. MD Advis 2014;7:28–32.
- John, N., et al. (2022). Role of vitamin D in reproductive health: Implications for infertility and pregnancy. Journal of Clinical Endocrinology & Metabolism, 107(9), 2301-2310. [CrossRef]
- Karimzadeh, M., et al. (2023). Vitamin D supplementation in assisted reproduction: Outcomes in IVF and ICSI cycles. Fertility and Sterility, 120(4), 718-725. [CrossRef]
- Sadeghi, N., et al. (2021). Association between vitamin D deficiency and reduced ovarian reserve: Implications for fertility. Fertility and Sterility, 115(5), 1092-1099. [CrossRef]
- Mohan A, Haider R, Fakhor H, Hina F, Kumar V, Jawed A, et al. Vitamin D and polycystic ovary syndrome (PCOS): a review. Ann Med Surg (Lond). 2023; 85(7):3506-3511. [CrossRef]
- Thomson RL, Spedding S, Buckley JD. Vitamin D in the aetiology and management of polycystic ovary syndrome. Clin Endocrinol (Oxf). 2012 Sep;77(3):343-50. [CrossRef] [PubMed]
- Gonzalez, M., et al. (2022). Vitamin D as a potential therapeutic approach in endometriosis: A systematic review. Journal of Reproductive Immunology, 154, 103462. [CrossRef]
- Martinez, E., et al. (2020). The effect of vitamin D supplementation on endometriosis symptoms: A randomized trial. Journal of Obstetrics and Gynecology, 42(1), 11-18. [CrossRef]
- Lagana, A.S., Vitale, S.G., Ban Frangež, H., Vrtačnik-Bokal, E., D’Anna, R. (2017). Vitamin D in human reproduction: the more, the better? An evidence-based critical appraisal. European Review for Medical and Pharmacological Sciences, 21(18), 4243–4251.
- Pilz, S., Zittermann, A., Obeid, R., Hahn, A., Pludowski, P., Trummer, C., et al. (2018). The role of vitamin D in fertility and during pregnancy and lactation: A review of clinical data. International Journal of Environmental Research and Public Health, 15(10), 2241. [CrossRef]
- Chang, S.W., Lee, H.C. (2019). Vitamin D and health - The missing vitamin in humans. Pediatrics and Neonatology, 60(3), 237-244. [CrossRef]
- Fantini, C., Corinaldesi, C., Lenzi, A., Migliaccio, S., Crescioli, C. (2023). Vitamin D as a shield against aging. International Journal of Molecular Sciences, 24(5), 4546. [CrossRef]
- Martínez-Zavala, N., López-Sánchez, G.N., Vergara-Lopez, A., Chávez-Tapia, N.C., Uribe, M., Nuño-Lámbarri, N. (2020). Vitamin D deficiency in Mexicans has a high prevalence: A cross-sectional analysis of patients from the Centro Médico Nacional 20 de noviembre. Archives of Osteoporosis, 15(1), 88. [CrossRef]
- Płudowski, P., Kos-Kudła, B., Walczak, M., Fal, A., Zozulińska-Ziółkiewicz, D., Sieroszewski, P., et al. (2023). Guidelines for preventing and treating vitamin D deficiency: A 2023 update in Poland. Nutrients, 15(3), 695. [CrossRef]
- Irani, M., Merhi, Z. (2014). Role of vitamin D in ovarian physiology and its implication in reproduction: A systematic review. Fertility and Sterility, 102(2), 460-468.e3. [CrossRef]
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007 Jul 19;357(3):266-81. [CrossRef]
- Wortsman J, et al. "Decreased bioavailability of vitamin D in obesity." American Journal of Clinical Nutrition. 2000.
- Silva, I.C.J., Lazzaretti-Castro, M. (2022). Vitamin D metabolism and extraskeletal outcomes: An update. Archives of Endocrinology and Metabolism, 66(5), 748-755. [CrossRef]
- Várbíró, S., Takács, I., Tűű, L., Nas, K., Sziva, R.E., Hetthéssy, J.R., et al. (2022). Effects of Vitamin D on fertility, pregnancy, and polycystic ovary syndrome - A review. Nutrients, 14(8), 1649. [CrossRef]
- Pál É, Hadjadj L, Fontányi Z, Monori-Kiss A, Mezei Z, Lippai N, Magyar A, Heinzlmann A, Karvaly G, Monos E, Nádasy G, Benyó Z, Várbíró S. Vitamin D deficiency causes inward hypertrophic remodeling and alters vascular reactivity of rat cerebral arterioles. PLoS One. 2018 Feb 6;13(2):e0192480. [CrossRef] [PubMed] [PubMed Central]
- Nandi, A., Sinha, N., Ong, E., Sonmez, H., Poretsky, L. (2016). Is there a role for vitamin D in human reproduction? Hormones Molecular Biology and Clinical Investigations, 25(1), 15-28. [CrossRef] [PubMed]
- Trujillo J, et al. "Prevalence of vitamin D deficiency in postmenopausal women in Mexico, Chile, and Brazil." Journal of Endocrinology and Metabolism. 2018.
- Thacher TD, et al. "Vitamin D deficiency and insufficiency in women of reproductive age in Mexico." Journal of Clinical Endocrinology & Metabolism. 2017.
- Soto JR, Anthias C, Madrigal A, Snowden JA. Insights Into the Role of Vitamin D as a Biomarker in Stem Cell Transplantation. Front Immunol. 2020;11:500910.
- Sassi F, Tamone C, D'Amelio P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients. 2018;10(11):1656. [CrossRef]
- Bacanakgil BH, İlhan G, Ohanoğlu K. Effects of vitamin D supplementation on ovarian reserve markers in infertile women with diminished ovarian reserve. Medicine (Baltimore). 2022 Feb 11;101(6):e28796. [CrossRef] [PubMed] [PubMed Central]
- Moridi I, Chen A, Tal O, Tal R. The Association between Vitamin D and Anti-Müllerian Hormone: A Systematic Review and Meta-Analysis. Nutrients. 2020;12(6):1567. Published 2020 May 28. [CrossRef]
- Safaei Z, Bakhshalizadeh SH, Nasr Esfahani MH, Akbari Sene A, Najafzadeh V, Soleimani M, et al. Effect of Vitamin D3 on Mitochondrial Biogenesis in Granulosa Cells Derived from Polycystic Ovary Syndrome. Int J Fertil Steril. 2020;14(2):143-149. [CrossRef]
- Ling Y, Xu F, Xia X, Dai D, Xiong A, Sun R, Qiu L, Xie Z. Vitamin D supplementation reduces the risk of fall in the vitamin D deficient elderly: An updated meta-analysis. Clin Nutr. 2021 Nov;40(11):5531-5537. [CrossRef] [PubMed]
- Wang, H., et al. "Vitamin D and female fertility: A systematic review." Journal of Steroid Biochemistry and Molecular Biology. 2018.
- Ozkan S, Jindal S, Greenseid K, Shu J, Zeitlian G, Hickmon C, Pal L. Replete vitamin D stores predict reproductive success following in vitro fertilization. Fertil Steril. 2010 Sep;94(4):1314-1319. [CrossRef]
- McLaughlin, J. M., et al. "Impact of vitamin D status on live birth rates in women undergoing IVF: A meta-analysis." Journal of Assisted Reproduction and Genetics. 2021.
- Rudick, B. M., et al. "Vitamin D deficiency and assisted reproductive outcomes: A retrospective study." Fertility and Sterility. 2020.
- Ekanayake DL, Małopolska MM, Schwarz T, Tuz R, Bartlewski PM. The roles and expression of HOXA/Hoxa10 gene: A prospective marker of mammalian female fertility? Reprod Biol. 2022 Jun;22(2):100647. [CrossRef] [PubMed]
- Shilpasree AS, Kulkarni VB, Shetty P, Bargale A, Goni M, Oli A, et al. Induction of Endometrial HOXA 10 Gene Expression by Vitamin D and its Possible Influence on Reproductive Outcome of PCOS Patients Undergoing Ovulation Induction Procedure. Indian J Endocrinol Metab. 2022;26(3):252-258. [CrossRef]
- Ozkan, S., et al. "Vitamin D levels in follicular fluid and pregnancy outcomes following IVF." Reproductive Biology and Endocrinology. 2019.
- Bischof, P., et al. "Vitamin D and reproductive health: The role of VDR in male and female fertility." Journal of Endocrinology. 2020.
- Bollen, S.E., Bass, J.J., Fujita, S., Wilkinson, D., Hewison, M., Atherton, P.J. (2022). The vitamin D/vitamin D receptor (VDR) axis in muscle atrophy and sarcopenia. Cell Signal, 96, 110355. [CrossRef]
- Blomberg Jensen M, et al. "Vitamin D receptor and vitamin D metabolizing enzymes are expressed in the human male reproductive tract." Human Reproduction. 2010.
- Becker S, Cordes T, Diesing D, Diedrich K, Friedrich M. Expression of 25 hydroxyvitamin D3-1α-hydroxylase in human endometrial tissue. J Steroid Biochem Mol Biol. 2007;103:771–5.
- Vienonen, A., Miettinen, S., Bläuer, M., Martikainen, P.M., Tomás, E., Heinonen, P.K., et al. (2004). Expression of nuclear receptors and cofactors in human endometrium and myometrium. Journal of the Society for Gynecological Investigation, 11(2), 104–112. [CrossRef]
- Bergadà, L., Pallares, J., Maria Vittoria, A., Cardus, A., Santacana, M., Valls, J., et al. (2014). Role of local bioactivation of vitamin D by CYP27B1 in human endometrial tissue. Fertility and Sterility, 101(4), 1014-1020. [CrossRef]
- Cermisoni GC, Alteri A, Corti L, Rabellotti E, Papaleo E, Viganò P, Sanchez AM. Vitamin D and Endometrium: A Systematic Review of a Neglected Area of Research. Int J Mol Sci. 2018 Aug 8;19(8):2320. [CrossRef] [PubMed] [PubMed Central]
- Cito G, Cocci A, Micelli E, Gabutti A, Russo GI, Coccia ME, Franco G, Serni S, Carini M, Natali A. Vitamin D and Male Fertility: An Updated Review. World J Mens Health. 2020 Apr;38(2):164-177. [CrossRef]
- Zegers-Hochschild F, Adamson GD, Dyer S, Racowsky C, de Mouzon J, Sokol R, et al. The International Glossary on Infertility and Fertility Care, 2017. Hum Reprod. 2017;32(9):1786-1801. [CrossRef]
- Holick, M.F., Binkley, N.C., Bischoff-Ferrari, H.A., Gordon, C.M., Hanley, D.A., Heaney, R.P., et al. (2011). Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology & Metabolism, 96(7), 1911–1930. [CrossRef]
- Farhangnia P, Noormohammadi M, Delbandi AA. Vitamin D and reproductive disorders: a comprehensive review with a focus on endometriosis. Reprod Health. 2024 May 2;21(1):61. [CrossRef] [PubMed] [PubMed Central]
- Jukic AMZ, Baird DD, Weinberg CR, Wilcox AJ, McConnaughey DR, Steiner AZ. Pre-conception 25-hydroxyvitamin D (25(OH)D) and fecundability. Hum Reprod. 2019;34(11):2163–72. [CrossRef]
- Zhang S, Lin H, Kong S, et al. Physiological and molecular determinants of embryo implantation. Mol Aspects Med. 2013;34(5):939-980. [CrossRef]
- Baldini GM, Russo M, Proietti S, Forte G, Baldini D, Trojano G. Supplementation with vitamin D improves the embryo quality in in vitro fertilization (IVF) programs, independently of the patients' basal vitamin D status [published correction appears in Arch Gynecol Obstet.2024 Jun;309(6):2963. doi: 10.1007/s00404-024-07540-z]. Arch Gynecol Obstet. 2024;309(6):2881‐2890. [CrossRef]
- Moolhuijsen LME, Visser JA. Anti-Müllerian Hormone and Ovarian Reserve: Update on Assessing Ovarian Function. J Clin Endocrinol Metab. 2020;105(11):3361–73. [CrossRef]
- Karami, S., et al. "Seasonal fluctuations of vitamin D and ovarian function: Implications for fertility." Journal of Clinical Endocrinology and Metabolism. 2021.
- Javed Z, Papageorgiou M, Deshmukh H, Kilpatrick ES, Mann V, Corless L, Abouda G, Rigby AS, Atkin SL, Sathyapalan T. A Randomized, Controlled Trial of Vitamin D Supplementation on Cardiovascular Risk Factors, Hormones, and Liver Markers in Women with Polycystic Ovary Syndrome. Nutrients. 2019 Jan 17;11(1):188. [CrossRef]
- Calagna G, Catinella V, Polito S, Schiattarella A, De Franciscis P, D’Antonio F, et al. Vitamin D and Male Reproduction: Updated Evidence Based on Literature Review. Nutrients. 2022;14(16):3278.
- Bischof, P., et al. "Vitamin D and reproductive health: The role of VDR in male and female fertility." Journal of Endocrinology. 2020.
- Somigliana, E., Panina-Bordignon, P., Murone, S., Di Lucia, P., Vercellini, P., & Vigano, P. (2007). Vitamin D reserve is higher in women with endometriosis. Human reproduction (Oxford, England), 22(8), 2273–2278. [CrossRef]
- Urbina, A., et al. "Effect of vitamin D supplementation on IVF success rates: A randomized controlled trial." Reproductive Biology and Endocrinology. 2020.
- Meng X, Zhang J, Wan Q, et al. Influence of Vitamin D supplementation on reproductive outcomes of infertile patients: a systematic review and meta-analysis. Reprod Biol Endocrinol. 2023;21(1):17. Published 2023 Feb 3. [CrossRef]
- Zhou X, Wu X, Luo X, Shao J, Guo D, Deng B, Wu Z. Effect of Vitamin D Supplementation on In Vitro Fertilization Outcomes: A Trial Sequential Meta-Analysis of 5 Randomized Controlled Trials. Front Endocrinol (Lausanne). 2022 Mar 17;13:852428. [CrossRef] [PubMed] [PubMed Central]
- Moridi I, Chen A, Tal O, Tal R. The Association between Vitamin D and Anti-Müllerian Hormone: A Systematic Review and Meta-Analysis. Nutrients. 2020;12(6):1567. Published 2020 May 28. [CrossRef]
- Moradkhani A, Azami M, Assadi S, Ghaderi M, Azarnezhad A, Moradi Y. Association of vitamin D receptor genetic polymorphisms with the risk of infertility: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2024 May 30;24(1):398. [CrossRef] [PubMed] [PubMed Central]
- Chu J, Gallos I, Tobias A, Tan B, Eapen A, Coomarasamy A. Vitamin D and assisted reproductive treatment outcome: a systematic review and meta-analysis. Hum Reprod. 2018 Jan 1;33(1):65-80. [CrossRef] [PubMed]
- Lv SS, Wang JY, Wang XQ, Wang Y, Xu Y. Serum vitamin D status and in vitro fertilization outcomes: a systematic review and meta-analysis. Arch Gynecol Obstet. 2016 Jun;293(6):1339-45. [CrossRef] [PubMed]
- Karimi E, Arab A, Rafiee M, Amani R. A systematic review and meta-analysis of the association between vitamin D and ovarian reserve. Sci Rep. 2021 Aug 6;11(1):16005. [CrossRef] [PubMed] [PubMed Central]
- Cozzolino M, Busnelli A, Pellegrini L, Riviello E, Vitagliano A. How vitamin D level influences in vitro fertilization outcomes: results of a systematic review and meta-analysis. Fertil Steril. 2020 Nov;114(5):1014-1025. [CrossRef] [PubMed]
- Gupta, K., Thakur, R., Sharma, P., Kamra, P, Khetarpal, P. Polycystic Ovarian Syndrome (PCOS) and its association with VDR gene variants Cdx2 (rs11568820) and ApaI (rs7975232): Systematic review, meta-analysis and in silico analysis,Human Gene,Volume 40,2024,201293, ISSN 2773-0441, https://. [CrossRef]
- Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2016;31(12):2841-2855. [CrossRef]
- American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 194: Polycystic Ovary Syndrome [published correction appears in Obstet Gynecol. 2020 Sep;136(3):638. doi: 10.1097/AOG.0000000000004069. Obstet Gynecol. 2018;131(6):e157-e171. [CrossRef]
- Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril. 2018;110(3):364-379. [CrossRef]
- Rosenfield RL, Ehrmann DA. The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited. Endocr Rev. 2016;37(5):467-520. [CrossRef]
- Kuyucu Y, Çelik LS, Kendirlinan Ö, Tap Ö, Mete UÖ. Investigation of the uterine structural changes in the experimental model with polycystic ovary syndrome and effects of vitamin D treatment: An ultrastructural and immunohistochemical study. Reproductive Biology. 2018 Mar;18(1):53-59. DOI: 10.1016/j.repbio.2018.01.002. [PubMed]
- Pal L, Zhang H, Williams J, Santoro NF, Diamond MP, Schlaff WD, Coutifaris C, Carson SA, Steinkampf MP, Carr BR, McGovern PG, Cataldo NA, Gosman GG, Nestler JE, Myers E, Legro RS; Reproductive Medicine Network. Vitamin D Status Relates to Reproductive Outcome in Women With Polycystic Ovary Syndrome: Secondary Analysis of a Multicenter Randomized Controlled Trial. J Clin Endocrinol Metab. 2016 Aug;101(8):3027-35. [CrossRef] [PubMed] [PubMed Central]
- Thomson RL, Spedding S, Buckley JD. Vitamin D in the aetiology and management of polycystic ovary syndrome. Clin Endocrinol (Oxf). 2012;77(3):343-350. [CrossRef]
- Anagnostis P, Karras S, Goulis DG. Vitamin D in human reproduction: a narrative review. Int J Clin Pract. 2013;67(3):225-235. [CrossRef]
- Morgante G, Darino I, Spanò A, Luisi S, Luddi A, Piomboni P, Governini L, De Leo V. PCOS Physiopathology and Vitamin D Deficiency: Biological Insights and Perspectives for Treatment. J Clin Med. 2022 Aug 2;11(15):4509. [CrossRef] [PubMed] [PubMed Central]
- Maktabi M, Chamani M, Asemi Z. The Effects of Vitamin D Supplementation on Metabolic Status of Patients with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Horm Metab Res. 2017;49(7):493-498. [CrossRef]
- Trummer C, Schwetz V, Kollmann M, et al. Effects of vitamin D supplementation on metabolic and endocrine parameters in PCOS: a randomized-controlled trial. Eur J Nutr. 2019;58(5):2019-2028. [CrossRef]
- Davis EM, Peck JD, Hansen KR, Neas BR, Craig LB. Associations between vitamin D levels and polycystic ovary syndrome phenotypes. Minerva Endocrinol. 2019;44(2):176-184. [CrossRef]
- Lerchbaum E, Theiler-Schwetz V, Kollmann M, et al. Effects of Vitamin D Supplementation on Surrogate Markers of Fertility in PCOS Women: A Randomized Controlled Trial. Nutrients. 2021;13(2):547. Published 2021 Feb 7. [CrossRef]
- 84. TABLA.
- Trummer C, Schwetz V, Kollmann M, Wölfler M, Münzker J, Pieber TR, Pilz S, Heijboer AC, Obermayer-Pietsch B, Lerchbaum E. Effects of vitamin D supplementation on metabolic and endocrine parameters in PCOS: a randomized-controlled trial. Eur J Nutr. 2019 Aug;58(5):2019-2028. [CrossRef]
- Ostadmohammadi V, Jamilian M, Bahmani F, Asemi Z. Vitamin D and probiotic co-supplementation affects mental health, hormonal, inflammatory and oxidative stress parameters in women with polycystic ovary syndrome. J Ovarian Res. 2019 Jan 21;12(1):5. [CrossRef]
- Lerchbaum E, Theiler-Schwetz V, Kollmann M, Wölfler M, Pilz S, Obermayer-Pietsch B, Trummer C. Effects of Vitamin D Supplementation on Surrogate Markers of Fertility in PCOS Women: A Randomized Controlled Trial. Nutrients. 2021 Feb 7;13(2):547. [CrossRef]
- Dastorani M, Aghadavod E, Mirhosseini N, Foroozanfard F, Zadeh Modarres S, Amiri Siavashani M, Asemi Z. The effects of vitamin D supplementation on metabolic profiles and gene expression of insulin and lipid metabolism in infertile polycystic ovary syndrome candidates for in vitro fertilization. Reprod Biol Endocrinol. 2018 Oct 4;16(1):94. [CrossRef]
- Javed Z, Papageorgiou M, Deshmukh H, Kilpatrick ES, Mann V, Corless L, Abouda G, Rigby AS, Atkin SL, Sathyapalan T. A Randomized, Controlled Trial of Vitamin D Supplementation on Cardiovascular Risk Factors, Hormones, and Liver Markers in Women with Polycystic Ovary Syndrome. Nutrients. 2019 Jan 17;11(1):188. [CrossRef]
- Azhar A, Alam SM, Rehman R. Vitamin D and Lipid Profiles in Infertile PCOS and Non-PCOS Females. J Coll Physicians Surg Pak. 2024 Jul;34(7):767-770. [CrossRef]
- Irani M, Seifer DB, Grazi RV, Julka N, Bhatt D, Kalgi B, Irani S, Tal O, Lambert-Messerlian G, Tal R. Vitamin D Supplementation Decreases TGF-β1 Bioavailability in PCOS: A Randomized Placebo-Controlled Trial. J Clin Endocrinol Metab. 2015 Nov;100(11):4307-14. [CrossRef]
- Wen X, Wang L, Li F, Yu X. Effects of vitamin D supplementation on metabolic parameters in women with polycystic ovary syndrome: a randomized controlled trial. J Ovarian Res. 2024 Jul 16;17(1):147. [CrossRef]
- Krul-Poel YHM, Koenders PP, Steegers-Theunissen RP, Ten Boekel E, Wee MMT, Louwers Y, Lips P, Laven JSE, Simsek S. Vitamin D and metabolic disturbances in polycystic ovary syndrome (PCOS): A cross-sectional study. PLoS One. 2018 Dec 4;13(12):e0204748. [CrossRef]
- Edi R, Cheng T. Endometriosis: Evaluation and Treatment. Am Fam Physician. 2022 Oct;106(4):397-404. [PubMed]
- Cousins FL, McKinnon BD, Mortlock S, Fitzgerald HC, Zhang C, Montgomery GW, Gargett CE. New concepts on the etiology of endometriosis. J Obstet Gynaecol Res. 2023 Apr;49(4):1090-1105. [CrossRef]
- Cano-Herrera, G.; Salmun Nehmad, S.; Ruiz de Chávez Gascón, J.; Méndez Vionet, A.; van Tienhoven, X.A.; Osorio Martínez, M.F.; Muleiro Alvarez, M.; Vasco Rivero, M.X.; López Torres, M.F.; Barroso Valverde, M.J.; et al. Endometriosis: A Comprehensive Analysis of the Pathophysiology, Treatment, and Nutritional Aspects, and Its Repercussions on the Quality of Life of Patients. Biomedicines 2024, 12, 1476. [CrossRef]
- Giudice LC, Oskotsky TT, Falako S, Opoku-Anane J, Sirota M. Endometriosis in the era of precision medicine and impact on sexual and reproductive health across the lifespan and in diverse populations. FASEB J. 2023 Sep;37(9):e23130. [CrossRef]
- Shafrir, A.L.; Farland, L.V.; Shah, D.K.; Harris, H.R.; Kvaskoff, M.; Zondervan, K.; Missmer, S.A. Risk for and consequences of endometriosis: A critical epidemiologic review. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 51, 1–15.
- Smolarz, B.; Szyłło, K.; Romanowicz, H. Endometriosis: Epidemiology, Classification, Pathogenesis, Treatment and Genetics (Review of Literature). Int. J. Mol. Sci. 2021, 22, 10554. [CrossRef]
- Ocampo Hernández Dulce María, Gallardo Valencia Luis Ernesto, Guzmán-Valdivia Gómez Gilberto. Evaluación de la calidad de vida en pacientes con endometriosis mediante una escala original. Acta méd. Grupo Ángeles. 2023 Dez [citado 2025 Jan 29] ; 21( 4 ): 349-355. Disponible en: http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S1870-72032023000400349&lng=pt. Epub 21-Out-2024. [CrossRef]
- Nodler JL, DiVasta AD, Vitonis AF, Karevicius S, Malsch M, Sarda V, Fadayomi A, Harris HR, Missmer SA. Supplementation with vitamin D or ω-3 fatty acids in adolescent girls and young women with endometriosis (SAGE): a double-blind, randomized, placebo-controlled trial. Am J Clin Nutr. 2020 Jul 1;112(1):229-236. [CrossRef] [PubMed] [PubMed Central]
- Kalaitzopoulos DR, Samartzis N, Daniilidis A, Leeners B, Makieva S, Nirgianakis K, Dedes I, Metzler JM, Imesch P, Lempesis IG. Effects of vitamin D supplementation in endometriosis: a systematic review. Reprod Biol Endocrinol. 2022 Dec 28;20(1):176. [CrossRef] [PubMed] [PubMed Central]
- Delbandi AA, Torab M, Abdollahi E, Khodaverdi S, Rokhgireh S, Moradi Z, Heidari S, Mohammadi T. Vitamin D deficiency as a risk factor for endometriosis in Iranian women. J Reprod Immunol. 2021 Feb;143:103266. [CrossRef] [PubMed]
- Jennings BS, Hewison M. Vitamin D and Endometriosis: Is There a Mechanistic Link? Cell Biochem Funct. 2025 Jan;43(1):e70037. [CrossRef] [PubMed] [PubMed Central]
- Zheng SH, Chen XX, Chen Y, Wu ZC, Chen XQ, Li XL. Antioxidant vitamins supplementation reduce endometriosis related pelvic pain in humans: a systematic review and meta-analysis. Reprod Biol Endocrinol. 2023 Aug 29;21(1):79. [CrossRef] [PubMed] [PubMed Central]
- Hartwell, D., Rødbro, P., Jensen, S. B., Thomsen, K., & Christiansen, C. (1990). Vitamin D metabolites--relation to age, menopause and endometriosis. Scandinavian journal of clinical and laboratory investigation, 50(2), 115–121. [CrossRef]
- Somigliana, E., Panina-Bordignon, P., Murone, S., Di Lucia, P., Vercellini, P., & Vigano, P. (2007). Vitamin D reserve is higher in women with endometriosis. Human reproduction (Oxford, England), 22(8), 2273–2278. [CrossRef]
- Miyashita, M., Koga, K., Izumi, G., Sue, F., Makabe, T., Taguchi, A., Nagai, M., Urata, Y., Takamura, M., Harada, M., Hirata, T., Hirota, Y., Wada-Hiraike, O., Fujii, T., & Osuga, Y. (2016). Effects of 1,25-Dihydroxy Vitamin D3 on Endometriosis. The Journal of clinical endocrinology and metabolism, 101(6), 2371–2379. [CrossRef]
- Bellerba, F., Muzio, V., Gnagnarella, P., Facciotti, F., Chiocca, S., Bossi, P., Cortinovis, D., Chiaradonna, F., Serrano, D., Raimondi, S., Zerbato, B., Palorini, R., Canova, S., Gaeta, A., & Gandini, S. (2021). The Association between Vitamin D and Gut Microbiota: A Systematic Review of Human Studies. Nutrients, 13(10), 3378. [CrossRef]
- Jennings, B. S., & Hewison, M. (2025). Vitamin D and Endometriosis: Is There a Mechanistic Link?. Cell biochemistry and function, 43(1), e70037. [CrossRef]
- Shrateh, O. N., Siam, H. A., Ashhab, Y. S., Sweity, R. R., & Naasan, M. (2024). The impact of vitamin D treatment on pregnancy rate among endometriosis patients: A Systematic Review and Meta-Analysis. Annals Of Medicine And Surgery, 86(7), 4098-4111. [CrossRef]
- Mun MJ, Kim TH, Hwang JY, Jang WC. Vitamin D receptor gene polymorphisms and the risk for female reproductive cancers: A meta-analysis. Maturitas. 2015 1 Jun;81(2):256-265. DOI: 10.1016/j.maturitas.2015.03.010. [PubMed]
- Xie, B., Liao, M., Huang, Y., Hang, F., Ma, N., Hu, Q., Wang, J., Jin, Y., & Qin, A. (2024). Association between vitamin D and endometriosis among American women: National Health and Nutrition Examination Survey. PloS one, 19(1), e0296190. [CrossRef]
- Kalaitzopoulos, D. R., Lempesis, I. G., Athanasaki, F., Schizas, D., Samartzis, E. P., Kolibianakis, E. M., & Goulis, D. G. (2020). Association between vitamin D and endometriosis: a systematic review. Hormones (Athens, Greece), 19(2), 109–121. [CrossRef]
- Espinola MSB, Bilotta G, Aragona C. Positive effect of a new supplementation of vitamin D3 with myo-inositol, folic acid and melatonin on IVF outcomes: a prospective randomized and controlled pilot study. Gynecol Endocrinol. 2020;37:1–4. [CrossRef]

| STUDY | COUNTRY | VIT D (n) | TYPE OF STUDY | CONCLUSIONS |
|---|---|---|---|---|
| Zhou X et al, 2022. [63] | Switzerland | n=5 | Meta-Analysis. | VD may positively influence early pregnancy outcomes in women undergoing IVF, particularly for those with VD deficiency. |
| Moridi I et al, 2020. [64] | United States | n=5 | Systematic Review and Meta-Analysis. | Vitamin D is a safe, affordable supplement with growing evidence supporting its benefits in improving pregnancy rates, live births in assisted reproduction, reducing pregnancy loss, and minimizing pregnancy complications. |
| Moradkhani et al, 2024. [65] | Iran | n=4 | Systematic Review and Meta-Analysis. | Taql polymorphisms of the VDR gene are associated with susceptibility to infertility in women. But the protective polymorphisms for infertility are Fokl and Apal in women. |
| Chu et al, 2018. [66] | United Kingdom | n=11 | Systematic Review and Meta-Analysis. | Women with sufficient levels of VD are more likely to achieve positive results in assisted reproductive treatments compared to women with VD deficiency. |
| Lv SS et al, 2016. [67] | China | n=5 | Systematic Review and Meta-Analysis. | Women with adequate levels of VD are more likely to give birth to a live child after undergoing in vitro fertilization. |
| Karimi E et al, 2021. [68] | Iran | n=38 | Systematic Review and Meta-Analysis. | No direct relationship was found between overall VD levels with ovarian reserve in women. However, further studies are required to understand the fundamental role of VD in ovarian reserve. |
| Cozzolino et al, 2020. [69] | Spain | n=14 | Systematic Review and Meta-Analysis. | VD levels do not significantly affect IVF outcomes in terms of the number of pregnancies.As well as the number of live births. |
| Meng et al, 2023. | China | RCT n=9 | Systematic Review and Meta-Analysis. | VD supplementation increases the probability of pregnancy in infertile women, mainly in patients with low VD levels, but further clinical studies are recommended. |
| STUDY | COUNTRY | VIT D (N) | TYPE OF STUDY | CONCLUSIONS |
|---|---|---|---|---|
| Trummer et al, 2018. [81] | Austria. | N = 123 | Randomized controlled trial | VD supplementation resulted in a reduction in plasma glucose after 60 minutes during the OGTT. Aside from this, it had no significant effect on metabolic and endocrine parameters in PCOS. |
| Ostadmohammadi et al, 2019. [86] | Iran. | N = 60 | Randomize, double-blinded, placebo-controlled clinical trial | Supplementation of VD and probiotics, when compared to placebo, significantly improved depression, anxiety, stress, general health, and overall well-being in women with PCOS. It also contributed to a decrease in total testosterone, hirsutism, inflammation, and oxidative stress. Furthermore, there was a notable increase in total antioxidant capacity and glutathione levels. |
| Lerchbaum et al, 2021. [83] | Austria. | N = 180 | Double-blind randomized controlled trial | VD treatment in women with PCOS significantly affected FSH and the LH/FSH ratio after 24 weeks, but did not impact AMH levels. No significant effects were observed in non-PCOS women. |
| Dastorani et al, 2018. [88] | Iran. | N = 40 | Randomize, double-blinded, placebo-controlled trial | VD supplementation significantly reduced serum AMH, insulin levels, and insulin resistance (HOMA-IR), while increasing insulin sensitivity (QUICKI) compared to the placebo. Additionally, it led to a significant decrease in total cholesterol and LDL cholesterol levels. |
| Javed et al, 2019. [57] | United Kingdom. | N = 44 | Randomized, double-blind, placebo-controlled study | This study shows that VD supplementation has beneficial effects on liver injury and fibrosis markers (ALT levels), along with modest improvements in insulin resistance (HOMA-IR) in overweight and obese, VD-deficient women with PCOS. However, no significant changes were seen in other cardiovascular risk factors or hormones. |
| Azhar et al, 2024. [90] | Pakistan. | N = 180 | Comparative descriptive study. | Women with PCOS had lower VD levels. Both women with PCOS and VD deficiency exhibited lower HDL levels and higher total cholesterol, LDL, VLDL, and triglyceride levels compared to women without PCOS or those with sufficient or insufficient VD levels. |
| Irani et al, 2015. [91] | United States. | N = 93 | Randomized Placebo-Controlled Trial. | VD supplementation in women with PCOS increased VD levels and led to shorter menstrual cycles, reduced hirsutism (Ferriman-Gallwey score), lower triglycerides, and a decreased TGF-β1 to sENG ratio, highlighting VD's potential role in improving lipid metabolism and inflammation in PCOS. |
| Wen et al, 2024. [92] | China | N = 60 | Randomized controlled trial. | VD supplementation increased serum 25(OH)D levels. After 12 weeks, women in the VD group had lower BMI, WHR, insulin, HOMA-IR, triglycerides, total cholesterol, and LDL-C compared to the control group in women with obesity or insulin resistance. |
| Krul et al, 2018. [93] | Netherlands | N = 1088 | Cross-sectional comparison study. | VD deficiency in PCOS may contribute to metabolic issues, especially insulin resistance and lipid abnormalities. Women with PCOS had lower VD levels, which were associated with higher insulin resistance (HOMA-IR) and poorer lipid profiles, including reduced HDL-cholesterol and apolipoprotein A1. |
| STUDY | COUNTRY | VIT D (N) | TYPE OF STUDY | CONCLUSIONS |
|---|---|---|---|---|
| Hartwell D et al., (1990) [106]. | Denmark | N = 345 | Observational Cross-Sectional Study | This study analyzed vitamin D metabolite levels in women with and without endometriosis, across different age groups and menopausal status. It found that vitamin D levels fluctuate with age and menopause but did not establish a clear link between vitamin D and endometriosis severity. |
| Somigliana E et al (2007) [60] | England | N= 140 | Observational Case-Control Study | This study measured vitamin D reserves in women with endometriosis and found that, paradoxically, women with the condition had higher levels of vitamin D compared to controls. The findings suggest that increased vitamin D levels may be a compensatory response rather than a protective factor. |
| Miyashita M et al (2016) [108] | Japan | N= 35 | Experimental In Vitro Study | This study investigated the effects of the active form of vitamin D (1,25-dihydroxy vitamin D3) on endometrial cells. It found that vitamin D3 inhibited the proliferation of endometrial stromal cells and reduced inflammatory markers, suggesting a potential therapeutic role for vitamin D in managing endometriosis. |
| Bellerba et al (2021) [109] | Italy | N= 25 analysis reviewed | Systematic review | This systematic review the authors explore the link between vitamin D and gut microbiota, indicating that vitamin D significantly influences the gut's microbial makeup and diversity. They found that higher vitamin D levels correlate with a richer microbiota, potentially increasing beneficial bacteria while decreasing harmful ones. The review points out that vitamin D deficiency may contribute to dysbiosis,.However, initial findings suggest that vitamin D may impact the immune system and cellular processes related to endometriosis. |
| Jennings et. al., (2025) [110] | USA | 12 studies reviewed | Systematic review | This study explores potential biological mechanisms linking vitamin D deficiency to endometriosis. It highlights the role of vitamin D in regulating inflammatory and immune responses, which may influence lesion development. |
| Zheng et al (2023) [105] | China | 13 RCTs involving 589 patients | Randomized Controlled Trial | A randomized controlled trial showed that supplementation with antioxidant vitamins, including vitamin D, significantly reduced dysmenorrhea, dyspareunia, and chronic pelvic pain in women with endometriosis. It also improved the overall quality of life. |
| Shrateh et al (2024) [111] | Israel | N=3 | Systematic Review and Meta analysis | The beneficial effects of VD supplementation on endometriosis-related symptoms may indirectly support better pregnancy outcomes and improved fertility. |
| Mun et al (2015) [112] | Ireland | N= 123 | Meta analysis | This meta-analysis found that certain vitamin D receptor gene polymorphisms are associated with an increased risk of endometriosis, suggesting a genetic component to the disease's susceptibility. |
| Farhangnia et al (2024) [51] | Iran | N=180 | Comprehensive Review | This review examined the role of vitamin D in normal reproductive function and disorders, with a focus on endometriosis. Cellular and molecular studies suggest that vitamin D can inhibit key processes involved in endometriosis, such as cell proliferation, invasion,angiogenesis, and inflammation. Animal studies support these findings, showing that vitamin D treatment reduces endometriotic lesions in rats. However, human studies have yielded inconsistent results regarding the relationship between vitamin D levels and the risk or severity of endometriosis. |
| Kalaitzopoulos et al (2022) [102] | Greece | N = 12 | Systematic review | This review amalgamates results of available studies where supplementation of Vitamin D has a role as a treatment in endometriosis. |
| Xie. et al, 2024 [113] | Germany | N = 257 | Observational Cross-Sectional Study | A cross-sectional study found that higher serum 25(OH)D concentrations were associated with a decreased incidence of endometriosis women with endometriosis. These results lend credence to the possible advantages of maintaining sufficient vitamin D levels to prevent endometriosis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



