Submitted:
28 January 2025
Posted:
29 January 2025
You are already at the latest version
Abstract
Cancer is the second leading cause of death worldwide after cardiovascular disease, claiming not only a staggering number of lives but also causing considerable health and economic devastation globally, particularly in less-developed countries. Additionally, therapeutic interventions are further impeded by patient-to-patient differences in responses to anti-cancer drugs. Therefore, personalized medicines approach is crucial for this specific patient group including use of molecular and genetic screens to find appropriate stratification of patients that respond (and those that will not) to treatment regimen. But the information on which risk stratification method can be used to hone in on those cancer types and patients that will be likely responders to a specific anti-cancer agent remains elusive for most cancers. Novel developments in 3D bioprinting technology have been widely applied to recreate relevant bioengineered tumor organotypic structures, capable of mimicking the human tissue and microenvironment or adequate drug response in high throughput screening settings. Experiences are autogenously printed in the form of 3D bioengineered tissue using a computer-aided design concept where multiple layers each include different cell types and compatible biomaterials to build up specific configurations. Patient-derived cancer and stromal cells together with genetic material, extracellular matrix proteins and growth factors are used to create bioprinted cancer models which provide a possible platform for the screening of new personalized therapies in advance. To encourage the growth of cells and biological material in those personalized tumor models/implants both natural as well synthetic biopolymers have been used. These models may help in a physiologically relevant cell–cell and cell–matrix interactions with 3D heterogeneity resembling real tumors.
Keywords:
Keywords: 3D bioprinting
; tumor model
; tumor microenvironment
; personalized medicine
Introduction
Globally, cancer has emerged as the predominant cause of mortality, accounting for nearly one-sixth of all deaths in 2020. The urgency to elucidate cancer's developmental mechanisms to discover more efficacious treatments is underscored by this mortality rate. The genesis and evolution of cancer are intricately linked to the heterogeneity of cancer cells and their dynamic interplay with the surrounding microenvironment. The conventional 2D culture model, characterized by a homogenous cell type and equalized nutrient and growth factor distribution, fails to capture the complexity of cellular interactions and intratumoral diversity. Consequently, data derived from 2D models diverge significantly from in vivo conditions [1,2]. Although in vivo tumor models utilizing experimental animals are prevalent, disparities in genetics and species result in data that may not accurately mirror human tumorigenesis and progression. Additionally, these models are encumbered by ethical considerations and necessitate extensive cultivation periods, rendering them both time-intensive and laborious [3]. To reconcile the discrepancies between 2D cultures and animal models, 3D culture models have been innovated [1]. The advent of 3D printing technology has facilitated its application within the biomedical domain. These models adeptly emulate the in vivo microenvironment and biomimetic human tissue architecture, thereby enabling the exploration of cancer initiation and progression mechanisms. Furthermore, they hold potential for clinical utility in precise surgical navigation, among other applications [4,5,6]. This review accentuates the pivotal role of 3D cancer models in reconstructing the tumor microenvironment and their prospective clinical implementations, while also acknowledging the existing challenges.
2. Technical Methods of 3D Printing
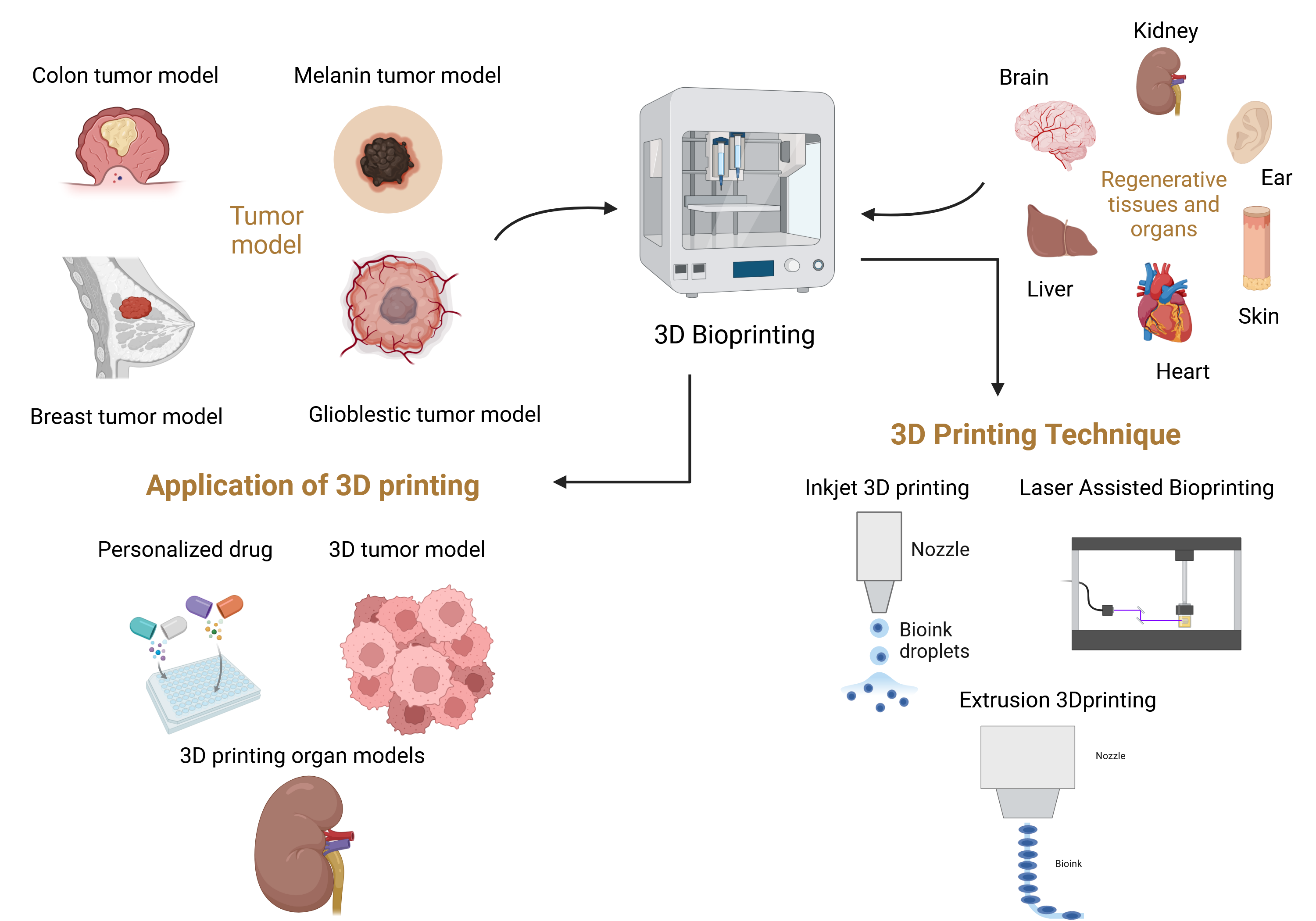
Bioprinting technology mainly magnetizes laser printing, inkjet printing and extrusion [7]. The combination of cells and biomaterials are used to form what we want print in layer by layer based on the CAD model of tissues and organs. It will differ from the traditional composite manufacturing way of “ells and scaffolds”, providing accurate spatial positioning for the cells. Multiplexed 3D printing of cells: multiple types of living cells or biological materials can be printed simultaneously (e.g., muscle and endothelial cell) [8] and create functional vascularized tissue (Figure 1).
2.1. Inkjet Bioprinting
Inkjet bioprinting technology has become matured since the beginning of twentieth century. It is the earliest application of biological printing technology. It is a non-contact technology further classified into ink (cells or biological material) 3D printing, which fabricates organs on the basis of computerized digital model of tissues and organ [9,10].
In thermal inkjet printing technology, heating element is commonly used to vaporize the droplets. The element is utilized to swiftly heat the surrounding area of ink, causing the ink in the pressure cavity will be vaporized into bubbles [11]. The gasification pressure causes bioink to leak from the extrusion nozzle as surface tension of a droplet is overcome, after that when voltage stops being applied the cooling phase occurs quite rapidly and within which time all boils back into space. Voltage could be applied and released many times, squeezing the droplets continuously. This type of droplet is mostly used to spray piezoelectric materials in piezoelectric inkjet printing technology. When voltage is applied to both ends of the piezoelectric element, the piezoelectric material deflects and squeezes out droplet near nozzle. The piezoelectric element will return to its original shape when the voltage is released [12]. This method enables the continuous extrusion of droplets by repeatedly applying and releasing voltage. Cui et al.[13], inkjet printing technology could be used to regenerate articular cartilage of human body demonstrated promising ability for guiding tissues to efficiently recover. A system controlled the process parameters such as cell concentration, volume and precision of droplet, nozzle diameter and average diameter for printing cells as well biological materials [14]. A multi-nozzles inkjet printing platform for the fabrication of composite structures has been developed by Weiss et al [15,16]. Different growth factors (fibrinogen, thrombin) with cells were printed into cell skull defect of the mice in situ. They demonstrated the in-situ printability but were not practical to use due to its complexity.
In comparison, inkjet printing technology shines for its long history and relative maturity, with the main advantages include: (1) color print that multiple nozzles can be incorporated in synchronization attended by cell/growth factor/biomaterials co-printing as well, hence allowing building heterogeneous tissues/organs [17]; and (2) inkjet printing is non-contact approach for biofabrication. The nozzles and the culture medium are also kept separately to minimize possible cross contamination during printing [18]. It can be printed on solid, hydrogels, and liquid interfaces There is no additional requirement for printing graphic smoothness, which provides a convenience to the in situ print; (3) Inkjet printing high speed and efficiency high production of organs such as liver lead assays related problems for long term can be solved due time consuming biological activity decline and suitable from large auto parts processing.(4) The droplet volume is diminutive, comparable to that of a single body cell, hence enabling precise manipulation at the cellular level. [19]. Although there are significant research breakthroughs with inkjet printing technology, nonetheless there are certain limitations: (1) the insignificant nozzle diameter increases the likelihood of cell precipitation and accumulation, hence restricting the printing density (<5×106 cells/ml) [20]; (2) During the heat-induced printing procedure, the nozzle is heated to an elevated temperature, which can be detrimental to cells, while the presence of shear stress concurrently diminishes cellular activity. (3) The amalgamation of droplets is challenging, as the morphology of the droplets cannot be precisely regulated. The structural integrity of printed materials is a challenge that must be addressed in inkjet printing.
2.2. Extrusion Bioprinting
The extrusion deposition technique secures the print head on a three-axis electronically regulated moving platform. The printing material is extruded from the print head with applied pressure, while the activation and deactivation of the print head are regulated by an on-off valve. The printing material comprises suspended cells combined with extracellular matrix-mimicking substances, like agar and hydrogels. Upon the extrusion of the printing material onto the base plate, it undergoes crosslinking to create a superposition, so facilitating the formation of a 3D cellular structure [21]. A comparable technique employs a multi-jet extrusion method, which constructs layer by layer by alternating between a layer of heat-sensitive material and a layer of cells, then regulating the temperature to destroy the heat-sensitive material and retain just the cells, thereby creating a three-dimensional cellular structure. The extrusion deposition technique must satisfy the following criteria [22]: (i) The printed material should retain its shape as much as feasible after deposition and undergo in situ cross-linking; (ii) The material and printing technique must exert no or minimal influence on the cellular state; (iii) The degrading properties of the scaffolds post-molding must be regulated. Extrusion-based 3D printing techniques are among the most prevalent manufacturing methods utilized in tissue engineering applications [23]. The purpose of extrusion additives is to substitute the ink with a liquid or molten substance that is dispensed through the nozzle, forming a line that solidifies on the stencil. The nozzle adheres to a pre-established trajectory defined by the computer model to fabricate the three-dimensional product incrementally as the material is extruded. The ink is pulled into a heated die, melted in the nozzle, and extruded into various shapes. These materials, typically polymers, can generate filaments exhibiting a solid-to-melt transformation. This method is distinguished by a minimal threshold for scientific processes and a brief duration necessary for platform construction. The precision and viability of printing primarily rely on the printing substance [24]. On the one hand, the deformation of the printing material during extrusion and descent constrains the final molding reliability, resulting in a printing precision on the order of hundreds of microns. On the other hand, the nozzles employed in this technology are prone to obstruction, hence diminishing processing efficiency. The present investigation emphasizes on a balance between the biocompatibility and printability of printed materials. Jasim Ahmed et al. examined a prospective application of improved formulations in 3D bioprinting. The bioink mixture was transformed into a semi-solid viscous substance via twin-screw casting method. The extruded material was subsequently utilized to produce 3D printable bioinks in the presence of sodium alginate polymer [25]. This technology offers advantages over conventional methods by enabling the production of reproducible, customizable, and functional structures, including the 3D printing of circular thin alginate films, thereby facilitating the regeneration of various tissues.
2.3. Light-Assisted Printing
Laser-assisted 3D bioprinting is a bioprinting approach that utilizes laser energy for the artificial development of tissues. The system has three essential types of machinery: (i) a pulsed laser source, (ii) a target for printing biological material, and (iii) a substrate to collect the printed material. This domain of bioengineering technology integrates laser science with biological engineering, aiming to fabricate living tissues and organs using bioink droplets or cells. 3D bioprinting is a swiftly evolving domain garnering significant attention from multiple scientific disciplines. Laser-assisted 3D bioprinting provides an alternative to traditional non-contact methods, including inkjet printing and nozzle-based bioprinting techniques. Laser-assisted 3D bioprinting employs lasers, offering numerous advantages such as high processing precision, non-contact fabrication, simplicity, and cost-effectiveness [26,27].
Laser-assisted 3D bioprinting offers significant advantages in the fabrication of cancer models due to its high precision and ability to construct complex microscale structures. Techniques such as Direct Laser Writing (DLW) and Laser-Induced Forward Transfer (LIFT) allow for the creation of models that closely mimic the intricate tumor microenvironment. For instance, these techniques enable the printing of bioinks containing cancer cells, extracellular matrix components, and growth factors, facilitating the study of cancer progression and drug responses. Moreover, laser bioprinting can accommodate bioresorbable and biocompatible materials, such as fibrinogen and collagen, making it a valuable tool for producing physiologically relevant cancer models [28,29,30].
By employing laser-induced vapor bubbles or direct photopolymerization, these methods achieve high spatial resolution (up to 100 nm in DLW), crucial for replicating the tumor's cellular heterogeneity. Furthermore, laser-assisted techniques enable the integration of pre-formed cell spheroids, allowing for rapid construction of three-dimensional tumor structures. This capability is particularly important in studying the interaction between cancer cells and the tumor microenvironment, as well as in screening therapeutic interventions [28,29,31].
2.3.1. Direct Laser Writing (DLW):
Direct Laser Writing (DLW) is a laser-assisted bioprinting technique that uses focused laser beams to achieve photopolymerization in photosensitive bioinks. This method offers exceptional resolution (up to 100 nm), making it particularly suitable for replicating the intricate features of the tumor microenvironment. Bioresorbable materials such as gelatin methacrylate (GelMA) and collagen have been successfully employed in DLW to create scaffolds that support cell adhesion, proliferation, and differentiation, critical for cancer research applications [32,33].
Advantages:
- High Precision: DLW enables the construction of microvascular networks, crucial for mimicking tumor angiogenesis.
- Customizability: The technique allows the incorporation of multiple bioinks, including cancer cell-laden hydrogels, extracellular matrix proteins, and growth factors, to create physiologically relevant models.
- Flexibility: It supports the integration of pre-formed cancer cell spheroids, allowing for rapid assembly of complex tumor structures.
Challenges:
- Material Limitations: The need for photosensitive bioinks restricts the range of compatible materials.
- Throughput: The high resolution of DLW comes at the cost of slower fabrication times, making it less suitable for large-scale models.
- Cost: The equipment and processing requirements for DLW are more expensive than alternative bioprinting methods, such as extrusion printing.
DLW's precision and adaptability make it a valuable tool for studying the dynamics of cancer cell invasion, tumor-stroma interactions, and therapeutic responses. However, its scalability and material limitations necessitate further advancements to fully realize its potential in cancer model development.
2.3.2. Laser-Induced Forward Transfer (LIFT)
Laser-induced forward transfer (LIFT) is a non-contact bioprinting technique that uses a pulsed laser to transfer biological materials, such as living cells, bioinks, or cell spheroids, from a donor substrate to a receiving substrate. This method involves applying a thin layer of bioink or cell-laden hydrogel to a transparent donor substrate, followed by the focused application of a laser pulse. The laser energy generates a localized pressure wave or vapor bubble beneath the material, propelling a droplet or cell-laden jet onto the receiving substrate [34,35].
Advantages:
- Cell Viability: LIFT has been shown to maintain high cell viability due to its non-contact nature and precise energy control.
- Resolution: The technique allows for the deposition of droplets with diameters as small as a few microns, enabling the creation of fine structures and intricate tissue architectures.
- Compatibility: LIFT can accommodate various bioinks, including those containing fragile living cells, making it ideal for cancer models requiring physiological accuracy.
Challenges:
- Thermal Effects: While the energy used in LIFT is finely tuned, excessive laser intensity can generate heat, potentially compromising cell viability.
- Material Transfer Limitations: The uniformity and reproducibility of material transfer depend on the bioink's viscosity and the laser's energy settings.
This method has been widely employed in cancer research for creating tumor models that replicate the cellular heterogeneity of tumors and their microenvironments. LIFT enables the printing of pre-formed cancer cell spheroids, expediting the development of 3D tumor constructs for drug screening and therapeutic testing [34,36,37,38,39].
The print speed value of 100–1600 mm/s represents the horizontal travel speed of the print head in laser-assisted bioprinting processes. This metric is important in comparing bioprinting techniques, as higher speeds can enhance throughput but may compromise resolution and precision. For example, in Laser-Induced Forward Transfer (LIFT), faster print speeds are suitable for high-throughput applications like large-scale tissue models, whereas slower speeds may be preferred for intricate, high-resolution constructs such as microvascular networks. This value provides insight into the method's balance between speed, precision, and its suitability for specific applications, such as fabricating cancer models with precise spatial cell arrangements.
2.3.3. Laser-Induced Side Transfer (LIST)
Laser-Induced Side Transfer (LIST), a new and modified type of laser-assisted bioprinting, supports lateral transfer of bioink, contrasting LIFT that is based on the vertical material ejection. In LIST, a consistent lateral displacement of liquid bioink or particles is created with a laser pulse on a donor substrate. Introduction of such a lateral arrangement provides greater precision and control over the flow and deposition of materials, which makes LIST especially valuable in generating complex tissue architecture and tailorable extensions [40,41,42].
Unlike classical vertical approaches, the LIST uses a modified bioink that enables imaging prior to transfer and avoids direct light interaction. It will enable a different set of edits and optimizations to be performed that will not be transferable directly from LIFT. This technique has produced high lateral and depth resolution by means of galvanometric scanning head, allowing fine steering of the laser beam. Hence, LIST is ideal for high-resolution bioprinting devices, such as the manufacture of 3D tissue scaffolds and multicellular structures [43,44].
The system is versatile and works with a range of bioinks, including hydrogels and particulate-based solutions, which when endow energy upon laser-induced particle energy absorbance can turn from solid to fluid state. Bioink composition, laser wavelength, and energy parameters are among several factors affecting the quality and resolution of printed structures. Nanosecond lasers in the UV range and femtosecond lasers in the visible range are generally applied for LIST. The type of laser chosen will depend on the desired resolution and material and its properties. Micromachining with UV nanosecond lasers, which offers accurate delivery of energy, is capable of enabling material transfer over large distances. On the other hand, femtosecond lasers in the visible spectrum can be focused on the order of ~0.5 microns laterally, making these systems better suited for microscale applications [45,46].
Sure, LIST's transfer speed outperforms other non-continuous printing techniques, and this makes LIST particularly suitable for the high-throughput production of micron-sized structures. For instance, while preserving their integrity and resolution, LIST can print constructs over 60 mm in 30 seconds. Thus, biocompatible and high-precision tissue models will be produced by LIST, of which the increasing use of hydrogels and cells as bioinks is a recent priority. These advances have special implications in cancer studies, as LIST can be used to construct complex models of tumor microenvironments that more closely represent native-tissue cell–cell interactions [47,48].
2.3.4. Laser-Induced Bubble Printing (LIBP)
Laser-Induced Bubble Printing (LIBP) is a novel bioprinting method that utilizes pulsed laser energy to generate vapor bubbles that can be leveraged to eject bioinks and cell-laden hydrogels. This process utilizes the creation of microbubbles in the bioink layer that can be controlled, producing localized pressure that forces the material into the receiving substrate. In particular, its ability to reach high spatial resolution together with fine level of droplet size and placement control makes LIBP an attractive technology for complex tissue architectures fabrication [49,50].
The LIBP method exhibits a versatility in that it can interface with a variety of bioinks (hydrogels, living cells, synthetic biomaterials), which makes it useful for a wide range of biomedical applications. LIBP has also been used in tissue-engineering to create 3D scaffolds with spatially defined cell populations. Using the technique, it is also possible to quickly transfer pre-formed cell spheroids or cellular aggregates, paving the way for physiologically relevant tumor microenvironments for cancer studies. The controlled placement of bioinks using LIBP allows generating reproducible and scalable models [51].
Advantages:
· Easy-coating mechanism: Due to the high deposition rate, LIBP can achieve excellent morphology from just a few seconds' exposure time compared to the other laser-assisted post-processing methods.
· Surface Structures: With precise control over the size and location of vapor bubbles, materials can be accurately patterned.
· Cost Efficiency: Reducing material waste, especially with costly bioinks or cell-laden hydrogels.
Challenges:
· Thermal Effects: The energy of the laser required to form bubbles might induce heat that could impact viability of the cells. Laser parameter tuning is done carefully to eliminate the thermal damage.
· Bubble Dynamics: Unrestricted growth of bubbles can impact flow uniformity or destabilize transferred materials, imposing difficulties for intricate structures [47,52,53,54,55].
The configuration of laser-assisted bioprinting is a nozzle-free system that integrates a near-infrared pulsed laser with a focusing mechanism utilizing a scanning mirror, which directs the laser beam onto the biological material [56]. According to the CAD modeling, laser pulses are concentrated on the target area to produce a high-pressure vapor pocket, resulting in the creation of a cell-laden droplet that descends into the receiving substrate. This technique inhibits cell obstruction and preserves cell viability. Its enhanced high throughput capacity and reproducibility enable the generation of 3D-printed pre-cancerous and cancer models. Hakobyan et al. [57] created replicable 3D arrays of cellular spheroids comprising acinar and ductal exocrine pancreatic cells using laser-assisted bioprinting, which can serve as a 3D model for investigating the early phases of pancreatic ductal adenocarcinoma development. Laser-assisted bioprinting (LAB) was employed to create corneal tissue analogs utilizing human embryonic stem cell (hESC)-derived limbal epithelial stem cells, lamellar corneal stroma with interspersed acellular bio-ink layers, and layers containing human adipose tissue-derived stem cells (ADSCs). Post-printing, the 3D constructions demonstrated favorable vitality for adipose stem cells, and the epithelial cells were arranged comparable to native corneal stroma, exhibiting migratory potential. The research demonstrated the successful development of multilayer 3D bioprinted tissues that replicate corneal tissue [58]. Another research has shown that LAB facilitates the printing and organization of nano-hydroxyapatite and human osteoprogenitors while maintaining viability and proliferation for up to 15 days. Additionally, it was proposed as an essential approach for two-dimensional cell patterning and is vital to the production of three-dimensional composite materials [59]. Tissue engineering is essential in the management of chronic skin disorders and burn injuries. An investigation employed the LAB technique to create fully cellularized skin, effectively utilizing various cell types in three-dimensional spatial configurations. Fibroblasts, keratinocytes, and Matriderm® were employed to create skin substitutes, which were subsequently evaluated in vivo using nude mice. The data indicated that cells had experienced differentiation and proliferation, resulting in tissue creation, and notably, small blood veins developed towards the printed tissue from the wound bed and margins [60]. In an additional investigation, ADSCs were structured into a 3D grid pattern with LAB, and it was determined that cell proliferation and differentiation were unaffected post-printing. The expression of adipogenic markers indicated that the cell lineages resemble three-dimensional grafts comparable to real adipose tissue [61]. An investigation has created injectable micro-scaffolds from electrospun material utilizing LAB, capable of producing ten thousand micro-scaffolds rapidly with a high injectability rate. Furthermore, the cells were seeded into micro-scaffolds, revealing that these structures function as cell carriers and provide a more comprehensive investigation of minimally invasive cell therapies [62]. Even though the technology to this type of treatment is still in its early development stages, it has some promising potential and would also help alleviate existing organ-replacement transplantation shortages. The Table 1 highlights their unique advantages and drawbacks summarizes key bioprinting methods, focusing on their bioink compatibility, resolution, material deposition rates, and applications. The inclusion of metrics such as 'Resolution' and 'Material Deposition Rate' provides a clearer understanding of each technique's capabilities and limitations in creating high-precision cancer models and other biomedical constructs. Table 2 highlights their unique advantages and drawbacks.
3. Opportunities Provided by 3D Bioprinted Cancer Models
3.1. Tumor Microenvironment Characteristics.
Tumors are defined by uncontrolled cell proliferation and are complex mini-organs comprising several cell types and matrix proteins, as illustrated in Figure 2. Particularly, certain tumors may consist of almost 50% of their mass of the tumor comprised of nonmalignant cells [86,87]. Malignant cells actively engage with both elements of the tumor microenvironment [88]. In numerous cases, the accompanying nonmalignant cells facilitate cancer development by the production of substances including cytokines and matrix remodeling enzymes. The lymphatic and immune system cells, blood vessels, pericytes, stromal cells, and adipocytes all contribute to the microenvironment, with their functions being consistent across many cancer types [89]. In the tumor microenvironment, populations of T cells, such as cytotoxic CD8+ memory T cells, may be located at the peripheries of infiltrating tumors and within the lymphatic drainage pathways of organs. Furthermore, CD8+ T lymphocytes that produce interleukin-2 and interferon gamma (IFN-γ) are also present and frequently contribute to the prognosis of the disease determination. Conversely, immunosuppressive T regulatory cells, such as CD4+ T cells that secrete TGF-β and IL-10, facilitate tumor development [90,91] B cells also appear at the margins of tumors and in lymphatic structures, although both tumor-suppressive and tumor-promoting populations have been identified [92,93]. Natural killer cells are known to infiltrate the tumor stroma and may exhibit altered functions as a result of their interactions with tumor cells. Tumor-associated macrophages are a primary infiltrate in the tumor microenvironment and primarily exhibit tumor- and metastasis-promoting behaviors through the secretion of elevated amounts of IL-10. Macrophages possess a diverse array of angiogenic substances, facilitate neoangiogenesis in tumors, and engage in reciprocal contact with the surroundings. Tumors exhibit increased hypoxia, facilitating the recruitment of tumor-associated macrophages. The roles of several immune system cells, including myeloid-derived suppressor cells, tumor-associated neutrophils, and dysfunctional dendritic cells, are being examined inside the tumor microenvironment [87,94]. The other significant cellular alteration in the tumor microenvironment is the transformation of surrounding fibroblasts into myofibroblasts, facilitated through paracrine signaling pathways. Myofibroblasts contribute to cancer progression by inducing organ fibrosis. CAFs release mitogenic fibroblast growth factor (FGF) and insulin-like growth factor 1 (IGF1), while the epithelial−mesenchymal transition (EMT) stimulates TGF-β production. These fibroblasts additionally produce enzymes that facilitate ECM remodeling. CAFs may be organized in a core-branching configuration or may ring the tumor mass, frequently influencing the capacity of pharmaceuticals to access targeted malignant cells [95,96]. Vascular endothelial cells are another crucial cell type associated with the tumor microenvironment. The tumor vasculature significantly contrasts with normal vasculature in both structure and function characterized by disordered bifurcations, diverse lumens, and heightened permeability. The leakiness induces abnormal interstitial pressure and exacerbates hypoxia, ultimately promoting metastasis. Pericytes are frequently detected in many tumor microenvironments, providing structural support to the vasculature [97]. The extracellular matrix (ECM), in conjunction with the cellular component, is crucial in determining cellular fates within the tumor microenvironment [98]. ECM engages in a dynamic interaction with the tumor cells to regulate the initiation and metastasis of malignancies. Modulation of cell−ECM adhesions is necessary for the cells to establish the microenvironment. The extracellular matrix serves as a storehouse for various growth factors. The spatiotemporal delivery of growth factors from three-dimensional matrices can be adjusted by matrix development. Growth factors are often generated by recombinant technology in bacteria or cells and necessitate rigorous standardization via techniques such as SDS-PAGE and ELISA examinations. From a physical perspective, tumor matrices exhibit increased extracellular matrix deposition by cancer-associated fibroblasts, leading to a greater elastic modulus than adjacent areas. Collagen and elastin fibers generate more rigid fibrils as a result of cross-linking facilitated by lysyl oxidase and transglutaminase. Matrix metalloproteinases, cysteine proteases, and cathepsins are the enzymes that facilitate the remodeling of the extracellular matrix in the tumor microenvironment. Furthermore, the extracellular matrix (ECM) comprises a variety of biomaterials exhibiting distinct mechanical and compositional characteristics that vary across different body's tissues [99]. The mechanical characteristics of the microenvironment significantly influence cancer cell migration through the activation of mechanotransduction pathways. The migration of tumor cells in dense or unstructured 3D matrices has been confirmed to be specifically correlated with cellular stiffness [100,101]. Similarly, U373-MG human glioma cells exhibited differential migration behavior when the matrix modulus was adjusted between 0.4 and 120 kPa [102]. Therefore, the aforementioned discussion underscores the necessity of employing suitable fabrication techniques to accurately represent the intricate structure and functionality of the tumor microenvironment.
3.1.1. Enhanced Tumor Microenvironment
The tumor microenvironment consists of fibroblasts, epithelial cells, stroma, blood vessels, immune cells, signaling chemicals from both tumor and normal cells, and extracellular matrix (ECM) [103]. Despite advancements in 3D co-culture and microfluidic technologies, numerous obstacles persist in the development of tumor microenvironments. Recently, 3D bioprinting has recognized as an innovative technique for constructing intricate tissue models with many biological applications, and we examined the function of 3D printing in the tumor microenvironment. A study shown that 3D glioma stem cells displayed improved capabilities to form spheroids, produce tubule-like structures, secrete VEGFA, and efficiently transform into endothelial cells. Furthermore, it was discovered that a 3D bioprinted hydrogel scaffold facilitates the requisite tumor microenvironment for glioma cells and glioma stem cells (GSCs) [104]. Acoustic droplet 3D printing operates without a nozzle, hence eliminating the risk of clogging. It enhances cell viability and elevates the quantity of cancer-associated fibroblasts within the tumor microenvironment, resulting in functional native tissue or pathological models [105]. A study on tumors and fibroblasts for generating a tumor microenvironment utilized a 3D-printed plastic microfluidic device, which facilitates heterotypic co-culturing and supports phenotypic analysis and molecular assays. The acquired data were confirmed through a mouse xenograft model, revealing that the 3D in vitro technique enhances the comprehension of carcinogenesis and the related tumor microenvironment [106]. A 3D bioprinted GelMA/PEGDA hybrid scaffold replicated the tumor microenvironment of human malignant melanoma cells and was deemed appropriate for the tumor cells' proliferation and differentiation; furthermore, the tumor cells exhibited accelerated growth and demonstrated drug-resistant capabilities [107]. Alginate and gelatin bioprintable hydrogel, in conjunction with BC cells and fibroblasts, were printed to create a three-dimensional model of a tumor microenvironment. This strategy increased cell survival and promoted the formation of tumor spheroids that interact with cancer-associated fibroblasts, offering an alternate paradigm to animal tumor models and 2D cultures for studying cancer biology [108]. In a different study, gastric tissue-specific bio-inks, cellulose nanoparticles, and gastric dECM were employed to develop a tissue-specific microenvironment. The research showed that the utilization of cellulose nanoparticles enhanced mechanical capabilities, thereby augmenting gastric cell aggressiveness, and it may serve as an appropriate model for elucidating gastric cancer biology [109]. The influence of synthetic β-tricalcium phosphate structures on the interaction between neuroblastoma tumor cells and stromal components was investigated, revealing that the tumor microenvironment was influenced by the stroma and supported the proliferation of neuroblastoma cells. Furthermore, cytokine and fibronectin synthesis were induced, and the data elucidate how the 3D microenvironment prompts tumor cells to adopt spheroid morphology, so enhancing the comprehension of metastatic neuroblastoma [110]. Another study utilized 3D printing technology to replicate the MCF-7 cell growth microenvironment with Cs/Gel composite scaffolds. The proposed scaffold demonstrates significant mechanical capability, improved biocompatibility, and an accurate platform for drug screening. The impact of Geniposide was evaluated in a 3D culture system, revealing that cell growth was suppressed while cell apoptosis increased, indicating the anticancer properties of Geniposide [111].
3.2. Personalized Medicine
Recent breakthroughs have contributed to the development of novel surgical instruments in cancer surgery. Nonetheless, achieving success with the requisite surgical techniques and perioperative management remains challenging. Recently, the application of 3D printing has facilitated surgical planning, minimized surgical duration, enhanced therapeutic outcomes, and underscored the significance of 3D printing in cancer surgeries [112]. A study including 61 patients with right hemicolon cancer who had laparoscopic surgery classified them into three groups: control (n = 22), 3D printing (n = 20), and 3D-image (n = 19), to assess the significance of 3D printing in surgical procedures. It has been claimed that 3D printing significantly decreased surgical duration, blood loss, and the quantity of lymph node dissections, making it potentially more beneficial for beginner surgeons [113]. Patients who have undergone malignant pelvic bone cancer surgery (n = 12) via a 3D-printed bone-cutting guide and reconstruction with a 3D-printed implant were analyzed using clinical information. Three-dimensional printed guidelines facilitated patient recovery by yielding negative pathological results and promoting expedited rehabilitation. Furthermore, it was discovered that, in contrast to the anatomical filling of bone deficiencies, 3D printed implants may be fabricated and utilized [114]. In a study, patients' CT data were gathered for 3D reconstruction and printing, resulting in the development of 3D models to elucidate the relationship between a tumor and the hepatic bile duct, artery, portal vein, and hepatic vein, facilitating surgical planning and simulated procedures. The data indicated that liver failure or patient mortality was not identified perioperatively, eventually suggesting that 3D printing enhances surgical safety and mitigates surgical risk [115]. 3D printing was utilized by ten out of twenty patients who were having endoscopic transsphenoidal surgery after being diagnosed with macroadenoma. The clinical findings indicated that patients utilizing 3D technology experienced shorter surgery durations, exhibited a lower incidence of complications, and ultimately benefited from an improved prognosis [116]. A separate study indicated that colorectal surgery might be enhanced by 3D printing technology, which improves patient education prior to stoma construction and aids in pre-operative surgical planning and the assessment of liver metastases to chemotherapy via 3D ultrasonography [117] Hong et al. [118] indicated that elucidating the thyroid gland, its anatomy, and surgical procedures poses significant challenges for doctors in their communication with patients. An investigation utilized a 3D-printed thyroid gland with cancer, derived from CT scans of patients, which demonstrated the intricate structure of veins, arteries, nerves, and adjacent organs surrounding the cancerous growth. Consequently, this technology assists clinicians in educating patients and enhances comprehension of the disease. A hybrid 3D model modeling laparoscopic choledochal surgery was produced utilizing a 3D Systems Project 660Pro with Visit PXL core powder. Nevertheless, the study indicated that additional refinement is required for this choledochal cyst excision simulation [119]. Three patients had their lung hilums 3D printed, and sixteen patients' pre-operative imaging was examined. The three-dimensional-printed hilum demonstrated superior accuracy compared to 3D-reconstructed CT, indicating that 3D printing is essential for thoracic surgical planning and offers greater advantages than traditional imaging techniques [120]. A research study investigated the efficacy of radioactive 125I seed (RIS) implantation, guided by CT and utilizing non-coplanar template 3D printing, in 66 patients with locally recurrent rectal cancer. The findings indicate that this method is a highly effective treatment strategy for patients post-surgery or external beam radiotherapy [121]. A randomized clinical experiment was performed to enhance patient understanding of informed consent for the utilization of individualized 3D-printed models in Stage I lung cancer surgery. According to assessments of patient knowledge, benefits, drawbacks, alternative therapies, and satisfaction, it was noted that personalized 3D printing may be applicable for patients suspected of having stage I lung cancer [122]. Utilizing CT image source data for 3D printing is considered highly advantageous, as data obtained from CT machines cannot be printed without prior processing. A cost-efficient 3D printed skull was created, incorporating the nasal cavity's shape at different stages of pituitary cancer, which can be utilized for surgical preparation of the endonasal trans-sphenoidal pituitary approach. Moreover, neurosurgeons and medical students can practice surgical techniques on various tumor stages [123]. A study was performed on lung cancer patients, categorizing them into several categories based on 3D chest CT reconstruction, 3D printing, and enhanced chest CT scans for 3D reconstruction. According to operation duration, bleeding loss, and post-operative problems, it has been discovered that comparative 3D printing techniques assist in accurately locating nodules and enhance surgical safety [124]. A 3D-printed model featuring a skull base, cerebral arteries, and a tumor/aneurysm was designed for a study, during which 49 simulated surgeries were executed under a microscope, followed by an actual surgical procedure after acquiring expertise. The authors proposed that 3D-printed craniocerebral models adequately imitate surgical settings and assist in surgical planning, experience, and validation during actual procedures [125]. Figure 3 illustrates the categorization of medical bioprinting's applications.
3.3. Drug Discovery and Screening
The development of cancer treatments is a formidable challenge, with just 5% of drugs successfully reaching the market [126] and an estimated cost of roughly 800 million USD [127]. This might be due to the inability of 2D cultures and animal models to replicate the in vivo tumor microenvironment, in contrast to 3D-printed cancer models [128], which also exhibit increased treatment resistance [129]. In recent years, there has been an increase in study utilizing 3D printing technology for pharmaceutical development. Chen et al. created an innovative 3D-printed microfluidic device that can amalgamate several cancer therapeutics, potentially enhancing the efficacy of cancer treatment [130]. The aforementioned microfluidic chip demonstrates enhanced scalability, precision, and compactness, mostly due to the 3D printing capabilities to produce intricate and flexible designs [130]. Zhao et al. have developed a 3D-printed model for anticancer drug screening utilizing gelatin, alginate, and fibrinogen as the matrix [131]. This study utilized hepatocyte and/or adipose-derived stem cells (ADSC) to assess drug screening in 2D and 3D-printed models [131]. Multiple stains and three distinct medicines, namely 5-FU, astragalus polysaccharide (AP), and matrine, were employed in three groups with varying quantities [131]. Gelatin in different concentrations, both high and low, has been alternated within the matrix [131]. The investigation conducted by Zhao et al. indicates that the 3D model exhibits a stronger intercellular connection as cells migrate to the extracellular matrix, resembling the in vivo tumor microenvironment [131]. A low concentration of gelatin enhances cell–cell interactions in the 3D-printed model [131]. The concentration of anticancer drugs significantly influences cell survival and drug resistance; for example, 5-FU is more effective at low concentrations in reducing cell survival, whereas high concentrations result in a rebound effect. Additionally, the co-culture of hepatocytes and ADSCs demonstrates the highest level of drug resistance [131]. In comparison with 2D cell culture, a model developed using 3D printing technology is more likely to facilitate high-throughput, scalable, and dependable drug screening [131].
4. Challenges Facing 3D Bioprinted Cancer Models
4.1. Technical Challenges in 3D Bioprinting
Numerous technological challenges are linked to the application of 3D bioprinting for the creation of cancer models. 3D biofabrication technologies have consistently advanced to enhance microresolution printing. Exceptional anatomical detail is achieved using photolithographic manufacture employing laser scanning or digital light processing, alongside two-photon polymerization, microfluidic chip-mediated techniques, and ionizing radiation [132]. Besides the quality of high-definition printing, the presence of numerous live biological cells poses an additional challenge. Following printing, it is crucial that the cells retain their functionality and vasculogenic properties throughout time. Vascular bioprinting poses a challenge in vascular perfusion. 3D bioprinting of materials facilitates luxury-level cancer cell behavior at the microscale. Organ or tissue systems comprise populations of capital goods at varying densities. Cellular aggregates must be vascularized in a 3D bioprint to provide robust blood and oxygen circulation. The application of 3D printing technology in intricate, multicellular systems, including organoids or pregnancy cultures, is crucial [133]. Moreover, bioprinting entails intrinsic variability, necessitating the establishment of operational frameworks and methodologies that ensure consistent variables. Troubleshooting room temperature presents several opportunities for bioreactor variation. Reproducibility is seldom addressed; nonetheless, a qualitative and functional bioprinting model, particularly one designed for scale-up, necessitates the use of polymers that are both robust and reproducible. To instill confidence in professionals regarding the authorization of new medication development processes or findings, it is essential to establish standardized technologies and methodologies. Advancement necessitates a thorough comprehension of the discourse and recommendations regarding the execution of bioprinting. The computational challenges are propelling cancer model technology towards more effective techniques. [134]
4.2. Reproducibility in 3D Bioprinted Cancer Models
Reproducibility is fundamental to scientific inquiry. The capacity to provide consistent data across several biological investigations signifies the potential reliability of their results. A major difficulty confronting 3D bioprinted cancer models currently is their low repeatability. Establishing a reliable model that yields same outcomes upon rejuvenation can be challenging. Consequently, investigations into diverse technical challenges pertinent to this research domain must incorporate this aspect and replicate the disease process or model to yield statistically accurate results. Overcoming this challenge necessitates the development of dependable and adaptable bioprinting methods. Biological materials have intrinsic variability; nevertheless, by selecting an appropriate combination of cells, hydrogels, and bioinks, one can effectively mitigate or manage this variability to an acceptable degree. [135] Variability may arise from various sources, including discrepancies in material properties, especially in printed gel configurations, which could stem from changes in crosslinking, environmental factors, or cellular viability. Variability can be minimized, if not entirely eradicated, from the printing process. The inherent unpredictability of the printing method and materials necessitates careful selection or design of printing parameters in the development of 3D bioprinted cancer models. It is essential to document and report the procedure with adequate detail to ensure its reproducibility. This will mitigate unpredictability resulting from technical discrepancies in print configuration. Adhering to a standard operating procedure enables the regulation of these bioinks, facilitating reproducibility among various bioinks as a measure of quality control. Moreover, the printing technology must effectively handle ergonomic concerns to integrate with standard cell culture infrastructure. This necessitates the operator's perspective. The design of models within the realms of tissue engineering and materials science necessitates a perspective akin to a 'beauty contest': there is no definitive 'winner', yet as long as there is a consensus on the criteria for success, collective advancement is achievable. In constructing a 3D bioengineered cancer model, it is imperative to clearly define our objectives. We can proceed to devise optimal methods for creating a replicable model. Consequently, the inquiry need to be, 'The reproducibility of what?' The veracity of this response will propel the discipline forward. Researchers must reach consensus on the protocols for model development, so augmenting the practical use of the discipline. Certain domains of 3D cell culture are expected to gain more from enhanced inter- and intra-laboratory reliability than others. Entities that directly influence disease control are likely to derive the greatest advantage, although this has to be determined. The previously identified application areas provide insight into the current priorities in the field. Consolidating a standardized document will enhance reproducibility for individuals unfamiliar with biological work and facilitate the usage of 3D printing in their scientific endeavors. This will significantly strengthen the utility of 3D printing and bioprinting techniques within the broader domain of cell culture. The enhanced reliability among groups will facilitate the unequivocal clinical translation of research. Partnerships between printing firms and research institutions may yield potential alternatives; however, it is regrettably improbable that this will occur in the foreseeable future. [136]
4.3. Standardization of Protocols
Despite significant advancements in the development of complex biological models, an attrition rate of over 90% persists between preclinical and clinical trials. A significant obstacle to advancement is the absence of standardized techniques for the development of 3D bioprinted cancer models. The various protocols employed for materials, printer configurations, or post-processing techniques in the fabrication of 3D cellular structures can significantly influence the uniformity and ultimate biological outcomes of these models. Consequently, there is a need for more comprehensive and reproducible methodologies for model creation to ensure uniform and consistent outcomes from both independent laboratories and multi-entry studies. Standardization and the establishment of industry-wide standards for materials and techniques could enhance efficiency, facilitate cancer modeling, replace animal trials, and yield disease-relevant and physiologically meaningful outcomes [137,138,139]. 3D bioprinted cancer models are becoming acknowledged for their significant differences in characteristics and results relative to 2D cultures, especially in drug reactivity testing. The fabrication processes used to create these bioengineered models may provide challenges for their transition from fundamental research to practical use. Diverse workgroups and researchers may leverage their distinct knowledge, with certain techniques trademarked and hence inaccessible to the community. Consequently, study results may vary significantly between laboratories, rendering comparisons challenging and models impossible to employ effectively. Establishing a consistent [137,138,139] methodology for printers, software, and materials will enable researchers to swiftly transition from a recognized platform to assess their alterations, hence enhancing productivity and efficiency [140,141].
4.4. Bioink Limitations
Despite considerable advancements in the development of bioinks, obstacles and limits persist in the fabrication of optimal hydrogel-based bioinks for cancer simulation. Currently, hydrogel-based bioinks are inadequate for accurately mimicking the tumor microenvironment (TME) in vitro due to trade-offs in bioprinter compatibility, biocompatibility, slow gelation dynamics, shear thinning properties, and suboptimal printing resolution, hindering the effective preclinical development of cancer therapies. TMEs are intricate and dynamic, consisting of numerous components that are organized geographically and temporally, which collectively influence tumor growth, invasion, and metastasis. Nevertheless, hydrogel bioinks remain significantly inadequate in replicating natural tumor microenvironments. The hydrogels employed for bioprinting cancer models must exhibit specific characteristics. Structural stability and print resolution of bioinks are critical considerations in the design of bioinks for cancer model printing. The matrices must possess an extended gelation time to facilitate the 3D–2D migration of multi-cancer cell populations post-printing, while simultaneously achieving shear thinning to enhance cell handling and rapid gelation after printing, thereby preserving the printed shape for subsequent cell phenotypic performance analysis. Thus, it is crucial to combine excellent printability with the preservation of the intended shape. The trade-off in bioink development presents a limitation for the advantageous properties of hydrogels in bioprinting. Moreover, for multi-material printing requiring the development of bioinks compatible with bioprinters, multiple printability assessment methodologies should be taken into account in bioink innovation [142,143,144].
4.4.1. Biocompatibility Issues
Bioinks utilized in 3D bioprinting must be compatible with cells and facilitate an environment conducive to cell growth, proliferation, and differentiation. Certain applications may necessitate support functions such as conduction or medication release. Various applications necessitate distinct specifications for the composition, structure, and characteristics of bioinks. Researchers have performed comprehensive studies, and typically, there are bioinks tailored for certain applications. Biological tissues typically comprise a multitude of diverse cells and their corresponding extracellular matrix. These bioinks are utilized to create 3D structures via 3D printing technology, emulating the natural tissue of the human body. The biological bioink typically comprises cells and the extracellular matrix. The classification of cell types is based on the distribution of cell composition within the tissue or organ designated for repair. At present, stem cells are the preferred option. The optimal biological bioink serves as an effective carrier for cells, offers an appropriate environment for cellular proliferation, and closely mimics the natural tissues of the human body [145,146,147]. Nevertheless, the specifications for bioink frequently conflict in practical usage. To ensure that the printed cells preserve their biological activity and reproduction rate, the extracellular matrix network within the bioink must exhibit excellent biocompatibility. To ensure the bioink remains continuous during 3D printing and is capable of producing intricate structures of varying shapes, its physical qualities must be exceptional. Simultaneously accomplishing both is a significant challenge. Consequently, mechanical stability, the presence of a chemical crosslinking agent, and certain synergistic effects, along with the interaction between the cell and the 3D printing system, as well as the adjustment of bioink parameters throughout the 3D printing process, frequently result in diminished biocompatibility. In recent years, researchers have attained specific outcomes in artificially synthesized materials inside the sector; yet, these materials require enhancement when juxtaposed with biological natural materials. Artificial materials frequently exhibit inferior biocompatibility compared to natural materials. In comparison to biodegradability, synthetic materials are significantly inferior. Biological tissues excel in both domains [148,149,150].
4.4.2. Mechanical Properties
Bioinks for bioprinting must have adequate rheological and mechanical qualities to guarantee proper gelation throughout the printing process. Furthermore, the printed biocomposite must maintain high shape accuracy and resolution to accurately replicate intricate biological interactions. This encompasses the dimensions and hierarchical arrangement of cells and their extracellular matrix, particularly the rigidity of the supportive structures created. Bioinks exhibiting plastic and elastic deformation properties suitable for cellular structures, while preserving dimensional stability, are essential in this context. In cancer cell biology research, cells must be printed within a soft matrix that accurately replicates the tissue-level mechanics of the underlying tumor environment. Mechanical qualities are crucial for cellular preservation, encompassing adhesion, survival, migration, and participation in specialized tasks [151,152]. Tumor tissue exhibits different degrees of stiffness, with the periphery becoming rigid while the middle region softens in in vitro two-dimensional monolayer cultures or conventional three-dimensional bulk investigations, rendering specific interactions incomparable. To preserve the whole range of cellular behaviors, including survival, motility, and responses to chemokines implicated in malignancy, it is essential to sustain a soft tissue-like microenvironment for cancer cells. It is crucial to acknowledge that certain tumor cell types tend to selectively infiltrate stiffer surroundings akin to the rigid fibrotic milieu of a primary or metastatic tumor. The development of hydrogels tailored to mimic differences in tissue-level mechanics is essential for the printed cancer model. Furthermore, the physiological environment must be engineered to replicate in vivo conditions, ensuring adequate breathability, sufficient transparency, and the capacity to facilitate oxygen and nutrient circulation, as well as efficient waste elimination [153,154].
5. Current Advances and Emerging Solutions
5.1. AI Optimization in Bioprinting
The advancement of bioprinting has enabled the fabrication of intricate three-dimensional synthetic cellular architectures. Nonetheless, numerous research obstacles persist in bioprinting. Contemporary 3D printing technologies facilitate the design of bioprinted objects at the micrometer scale, whereby the fundamental functional unit is the cell. Biomimicry serves as a significant emphasis and a powerful impetus for the bioprinting sector. A substantial segment of human tissue is vascularized, prompting the development of diverse bioprinting techniques aimed at constructing microvascular networks using hydrogel, cells, and extracellular matrix ink. Consequently, the fabrication of biomimetic organized tissues is a primary objective for numerous researchers. In bioprinting, the integration of heterogeneous characteristics, including cell-laden components with diverse extracellular matrices and vasculature, has garnered attention due to their distinctive properties and tissue functionality in reaction to bioactive chemicals [155,156,157]. Integrating various modules or pieces for the production of bioprinted complex structures at the cellular scale has emerged as a significant problem to achieve these needs. The swift advancement of bioprinting technologies has led to significant progress and accomplishments in hybrid biointegrations. Moreover, optimization is integrated into bioprinting, and this combination has already proven its capacity to enhance the quality and functionality of bioprinted living constructions. This model expedited printing and enhanced the morphological quality of printed brain tissue models. Nonetheless, the advancement of sophisticated network systems for the fabrication of intricate functional bioprinted biostructures at the cellular level remains largely nascent. We propose a vision in which the integration of bioprinting, biointegration, and assisted mammalian research accelerates the development of functional, complex biomimetic tissue constructs at cellular scales, potentially enhancing our understanding of the developmental biology of living tissues [158,159,160].
5.2. Hybrid Techniques in Bioprinting
Using a standard bioprinter based on a macroscopic 3D bioprinting technology in conjunction with a microfluidic device, hybrid bioprinting enables highly precise spatial assembly of cells and gel growth factors. The scaffolds' biofabricated heterotypic tissue zones, nutritional upkeep, and metabolite waste elimination can all be supported by an embedded microfluidic network. The benefits of both bioprinting methods are combined in hybrid bioprinting. Combining bioprinting and microfluidic technologies, microfluidic bioprinting enables drug screening, miniature tissue models, and the highly accurate dispensing of biochemical components. For drug screening, organ reproduction, and single-cell resolution analysis in regenerative medicine, 3D tissues, organoids, and functional cell–matrix interactions can also be bioprinted in situ. Successfully filling delayed gelation hydrogels or being severely impacted by shear stress and obstruction are issues in three-dimensional bioprinting systems [161]. It is possible to alter the pH of the helping hydrogel and generate the ionized amino gel for the bone-like structure without raising the temperature by adding the proper mineral acid. Sodium alginate, carrageenan, and pre-made mussel-inspired micro silica are combined to create a possible precursor ink for direct extrusion bioprinting. Channel-cable, multi-level, multi-material, and gradient material assembly are features of hybrid-scale 3D bioprinting scaffolds. By carefully regulating the cell placement at the micro-scale resolution and printing gel scaffold structures, modern 3D bioprinters are able to print many cell kinds immersed in their remarkable hydrogel in multi-layer patterns. The gel network can maintain cell growth to accomplish a multi-level assembly and adapt to the 3D cell culture landscape in vivo after undergoing bio-maturation in the incubator. The printing format results are mostly restricted to the production of inorganic ceramics, but the system can process colloidal inks and pastes and offers spatial diversity in the body design and granularity. The printing of several components at the microscale while creating realistic chemical and physical microenvironments in three dimensions remains a considerable problem, despite the development of numerous bioprinting methods. With the ability to print live cells, biodegradable biomaterials, and cell-matrix-stimulus multi-components at high-resolution scales in living subjects, in situ bioprinting can be regarded as a novel tissue engineering technique that produces intricate, biocompatible, and tissue-mimetic three-dimensional forms. This multi-stage technique can produce UV-started gels, such as those with high humidity and biocompatibility, as well as thermally initiated gels with cross-linking agents and chemically catalytic curable gels. Cells made of thermopolymerizable materials can form in situ, multi-layered, three-dimensional tissue nanostructures in a variety of sizes by encasing growth factors and support structures in multilayers. Thus, by integrating microfluidic principles that may create a wide variety of shapes, the aforesaid item improves the ability to include cells [162,163,164,165].
5.3. Microfluidics in Bioprinting
Microfluidics pertains to systems that manage small volumes of liquids, possess a high surface area for confined flow, and exhibit flow characteristics predominantly defined by laminar flow. Diverse bioprinting matrices and cell types have been employed in microfluidics, with numerous innovative approaches and foundational studies documented. One facet of study is the production of biomaterials for microfluidics bioprinters, with the objective of producing high-resolution, rapid-response, and stimuli-responsive substrates. A singular example can illustrate the research methodology in biomaterials development. Viscoelastic droplets have been employed to illustrate gas sensing on a flexible polymer substrate, and the outcomes of UV irradiation exposure confirm that the viscoelastic droplet remains entirely intact without degradation [166,167]. Continuous attempts are underway to develop novel bio-ink compositions to enhance cell viability. A novel polymer is developed to offer distinct attributes, including enhanced resolution, superior mechanical strength, and great transparency. In certain microfluidic methodologies, matrices have been developed to enhance cell spreading and optimize cell-matrix interactions by regulating cellular alignment and other characteristics. Cells can exert pressures to elongate their hanging nuclei. Numerous cellular processes are intimately linked to cell spreading; hence, elongated cells can facilitate biosensing of their environment. The stretching behavior of preosteoblasts is demonstrated in their findings [168,169].
5.4. Advanced Formulations of Bioink
Bioinks can be formulated using several polymers, ceramics, and non-matriomorphic substances. Polymer-based bioinks are extensively utilized owing to their straightforward composition, manipulation, and market accessibility. These are frequently hydrogels originating from natural polymers, including gelatin, collagen, hyaluronic acid, alginate, fibrin, or photoinsensitive synthetic polymers such as polyethylene glycol, poly(lactic-co-glycolic acid), or polyacrylate. Ceramic-based bioinks, consisting of hydrogels infused with inorganic nanoparticles, frequently incorporating hydroxyapatite, exhibit potential for application in bone models. Non-matriomorphic bioinks consist of cells encapsulated in carrier droplets, which are printed in conjunction with biocompatible inks that facilitate cell seeding, proliferation, self-assembly, and colonization. While polymer-based bioinks are frequently advantageous for cellular proliferation, their synthetic composition presents a disadvantage by compromising the interaction between the hydrogel and cells, obstructing cell motility, constraining biological responses, and perhaps influencing the intended cellular phenotype [170,171]. Notably, synthetic polymers typically inadequately replicate natural extracellular matrix compared to naturally generated hydrogels, rendering them less favorable for cellular functions. To address these limitations, extensive research has focused on creating innovative biomaterials, resulting in the development of numerous advanced bioinks. These can be tailored in various domains, including physical, chemical, and biological characteristics, as well as functionality, utilizing advanced assisting technologies such as micropatterning, cross-linking, coprinting, or electrospinning, and/or to directly integrate biologically functional molecules before or after printing. Furthermore, prevascularization studies have propelled the creation of composite bioinks, which consist of tissue-specific cell-laden hydrogels and sodium alginate pericellular capsules containing releasing factors. Benefits have been observed from the improved vascular supply of transplanted 3D-bioprinted tissues. As a result, recent advancements in bioinks have shown diverse stimuli-responsive characteristics, customized structural designs, and distinctive biofunctionality, providing promise for tissue organ regeneration [172,173,174].
6. Future Prospects and Implications for Cancer Research
Despite the significant potential of 3D bioprinting in the efficient and economical production of intricate in vitro tumors, numerous hurdles persist in advancing this technology within personalized oncology. Currently, existing 3D bioprinting techniques are unable to accurately replicate the intricate architecture of the numerous tissues within the human body. Moreover, the availability of biomaterials for 3D bioprinting is restricted, frequently lacking the ability to accurately replicate the characteristics of genuine tissue. To effectively integrate additional natural biomaterials into the bioprinting process, collaboration among chemists, materials engineers, and other professionals is essential. Moreover, technical obstacles pertaining to printing resolution and speed must be surmounted. Regulatory agencies are encountering difficulties in converting tumor models for personalized or precision medicine, which threatens the timely integration of bioprinted items into clinical practice, similar to the challenges faced with animal models and other reduced models. Biofabrication is inherently a multidisciplinary field, as is the advancement and enhancement of novel technologies for customized oncology. Interdisciplinary collaboration is essential to overcome existing restrictions and advance 3D bioprinting in oncology. Collaboration across multidisciplinary research teams can enhance the consistency and predictive validity of 3D bioprinted tumor models. Engineers and chemists are urged to integrate various biofabrication techniques to substantially improve the tumor model and ultimately establish a novel paradigm in cancer treatment. Indeed, distinct limitations emerge, particularly regarding cellular compartmentalization and the imperative to use microfluidics inside integrative body-on-chip investigations. Moreover, 3D bioprinting techniques involving post-printing or post-differentiation stages that necessitate additional tissue maturation are exceptionally efficient, as they provide enhanced regulation of the intricate arrangement of various cell layers or vascular structures. An instance of the latter technology is the integration of photoreactive extrusion-based bioprinting. Significant advancements pertain to the incorporation of artificial intelligence to enhance the precise deposition of cells and distinctive microphysiological bioprinted systems [157,175,176,177].
7. Conclusions
3D printing technology, in its advanced application within oncological research, facilitates not merely the replication of tumors’ three-dimensional spatial configuration but also the emulation of the tumor microenvironment, thereby revealing cancer’s intrinsic attributes. This dual capability significantly enhances the exploration of cancer’s etiology and progression, fosters the translation of fundamental research into clinical application, and addresses pragmatic clinical challenges. Clinically, 3D printing has demonstrated its utility in precision and personalized medicine. Despite the rapid evolution of 3D printing technology, current constraints in printing apparatuses and the spectrum of printable bioinks preclude its routine clinical deployment. Thus, it is imperative to persist in refining printing techniques, discovering novel biomaterials, broadening printers’ biocompatibility with diverse biomaterials, and enhancing resolution. Concurrently, efforts must focus on augmenting cell viability and density, curtailing printing durations, expanding the dimensions of printed tissues, and diminishing costs.
Acknowledgments
This work was supported by project: Study on the effect of novel nitric oxide responsive nano sustained-released particles on osteoarthritis Foundation: National Natural Science Foundation of China (NSFC) No. 81860386.
Conflicts of Interest
The author declares no conflict of interest.
References
- Kang Y, Datta P, Shanmughapriya S, et al. (2020) 3D Bioprinting of Tumor Models for Cancer Research. ACS Appl Bio Mater. 3(9):5552-5573. [CrossRef]
- Colombo E ,Cattaneo M G (2021) Multicellular 3D Models to Study Tumour-Stroma Interactions. Int J Mol Sci. 22(4). [CrossRef]
- Zimmer J, Castriconi R ,Scaglione S (2021) Editorial: Recent 3D Tumor Models for Testing Immune-Mediated Therapies. Front Immunol. 12:798493. [CrossRef]
- Zhou Y ( 2016) Understanding the cancer/tumor biology from 2D to 3D. J Thorac Dis. 8(11):E1484-E1486. [CrossRef]
- Ren Y, Yang X, Ma Z, et al.(2021) Developments and Opportunities for 3D Bioprinted Organoids. Int J Bioprint. 7(3):364. [CrossRef]
- Stone L (2014) Kidney cancer: A model for the masses--3D printing of kidney tumours. Nat Rev Urol. 11(8): 428. [CrossRef]
- Zhang XY, Zhang YD (2015) Tissue engineering applications of three-dimensional bioprinting. Cell Biochem Biophys. 72(3):777–782. [CrossRef]
- Melchels FPW, Domingos MAN, Klein TJ et al (2012) Additive manufacturing of tissues and organs. Prog Polym Sci. 37(8):1079–1104. [CrossRef]
- Boland T, Xu T, Damon B, Cui X (2006) Application of inkjet printing to tissue engineering. Biotechnol J 1(9):910–917. [CrossRef]
- Calvert P (2007) Printing cells. Science. 318(5848):208–209. [CrossRef]
- Cui X, Booland T, D’Lima DD, Lotz MK (2012) Thermal inkjet printing in tissue engineering and regenerative medicine. Recent Patents Drug Deliv Formul. 6(2):149–155. [CrossRef]
- Sumerel J, Lewis J, Doraiswamy A, Deravi LF, Sewell SL, Gerdon AE, Wright DW, Narayan RJ (2006) Piezoelectric ink jet processing of materials for medical and biological applications. Biotechnol J. 1(9):976–987. [CrossRef]
- Cui XF, Breitenkamp K, Finn MG et al (2012) Direct human cartilage repair using three-dimensional bioprinting technology. Tissue Eng Part A. 18(11–12):1304–1312. [CrossRef]
- Cui XF, Boland T (2009) Human microvasculature fabrication using thermal inkjet printing technology. Biomaterials. 30(31):6221–6227. [CrossRef]
- Weiss LE, Amon CH, Finger S et al (2005) Bayesian computeraided experimental design of heterogeneous scaffolds for tissue engineering. Comput Aided Des. 37(11):1127–1139. [CrossRef]
- Campbell PG, Weiss LE (2007) Tissue engineering with the aid of inkjet printers. Expert Opin Biol Therapy. 7(8):1123–1127.
- Saunders RE, Derby B (2014) Inkjet printing biomaterials for tissue engineering: bioprinting. Int Mater Rev. 59(8):430–448.
- Setti L, Fraleoni-Morgera A, Ballarin B et al (2005) An amperometric glucose biosensor prototype fabricated by thermal inkjet printing. Biosens Bioelectron. 20(10):2019–2026. [CrossRef]
- Chen FM, Lin LY, Zhang J et al (2016) Single-cell analysis using drop-on-demand inkjet printing and probe electrospray ionization mass spectrometry. Anal Chem. 88(8):4354–4360. [CrossRef]
- Ozbolat IT, Yu Y (2013) Bioprinting toward organ fabrication: challenges and future trends. IEEE Trans Biomed Eng. 60(3):691–699. [CrossRef]
- Kim H, Lee S (2020) Printability and physical properties of iron slag powder composites using material extrusion-based 3D printing. Journal of Iron and Steel Research International. 28 (1): 111–121. [CrossRef]
- Asif M (2018) A new photopolymer extrusion 5-axis 3D printer. Addit. Manuf. 23: 355–361. [CrossRef]
- Liu Q, Zhai W (2022) Hierarchical porous Ceramics with Distinctive microstructures by Emulsion-based direct ink writing. ACS Appl. Mater. Interfaces. 14 (28):32196–32205. [CrossRef]
- Qiu J (2021) Constructing customized Multimodal Phantoms through 3D printing: a Preliminary evaluation. Frontiers in Physics. 9. [CrossRef]
- Atakok G, Kam M, Koc HB (2022) Tensile, three-point bending and impact strength of 3D printed parts using PLA and recycled PLA filaments: a statistical investigation. J. Mater. Res. Technol. 18:1542–1554. [CrossRef]
- Chang J, Sun X ( 2023) Laser-induced forward transfer based laser bioprinting in biomedical applications. Frontiers in Bioengineering and Biotechnology. 11: 01-11. [CrossRef]
- Al Javed MO, Bin Rashid A ( 2024) Laser-assisted micromachining techniques: an overview of principles, processes, and applications. Advances in Materials and Processing Technologies. 1-44. [CrossRef]
- Garg A, Yang F, Ozdoganlar OB, LeDuc PR (2024) Physics of microscale freeform 3D printing of ice. Proceedings of the National Academy of Sciences. 121: p.e2322330121. [CrossRef]
- Tay RY, Song Y, Yao DR, Gao W (2023) Direct-ink-writing 3D-printed bioelectronics. Materials Today. 71: 135-151. [CrossRef]
- Mojdeh M, Hamid R, Fatemeh Y, Abbas R, Francesco B (2024) Advancements in tissue and organ 3D bioprinting: Current techniques, applications, and future perspectives. Materials & Design. 240:112853. [CrossRef]
- Yongcong F, Yuzhi G, Tiankun L, Runze X, Shuangshuang M, Xingwu M, Ting Zh, Liliang O, Zhuo X, Wei S (2022) Advances in 3D Bioprinting. Chinese Journal of Mechanical Engineering: Additive Manufacturing Frontiers 1:100011.
- Young OM, Xu X, Sarker S, Sochol R D (2024) Direct laser writing-enabled 3D printing strategies for microfluidic applications. Lab on a Chip. 24: 2371-2396. [CrossRef]
- Garciamendez-Mijares CE, Aguilar FJ, Hernandez P, Kuang X, Gonzalez M, Ortiz V, Riesgo RA, Ruiz DSR, Rivera VAM, Rodriguez JC, Mestre FL (2024) Design considerations for digital light processing bioprinters. Applied physics reviews. 11:031314. [CrossRef]
- Das A, Ghosh A, Chattopadhyaya S, Ding CF (2024) A review on critical challenges in additive manufacturing via laser-induced forward transfer. Optics & Laser Technology. 168:109893. [CrossRef]
- Marcos F, Pere S (2020) Laser-Induced Forward Transfer: A Method for Printing Functional Inks. Crystals. 10:651. [CrossRef]
- Mierke CT (2024) Bioprinting of Cells, Organoids and Organs-on-a-Chip Together with Hydrogels Improves Structural and Mechanical Cues. Cells. 13:1638. [CrossRef]
- Chang J, Sun X (2023) Laser-induced forward transfer based laser bioprinting in biomedical applications. Front. Bioeng. Biotechnol. 11:1255782. [CrossRef]
- Molpeceres C, Ramos-Medina R, Marquez A (2023) Laser transfer for circulating tumor cell isolation in liquid biopsy. Int J Bioprint, 9: 720. [CrossRef]
- Gabriella NH, Yuchao F, Bertrand V, Antonio I, Andreas D, Claire P, Aude C, Frank P L, Fabien G, Ioannis p (2024) Laser-assisted bioprinting of targeted cartilaginous spheroids for high density bottom-up tissue engineering. Biofabrication. 16:045029. [CrossRef]
- Yang Z (2023) Laser-Induced Forward Transfer of Functional Microdevices.
- Piqué, A, Charipar KM (2021) Laser-induced forward transfer applications in micro-engineering. Handbook of Laser Micro-and Nano-Engineering. [CrossRef]
- Xing F, Xu J, Yu P, Zhou Y, Zhe M, Luo R, Liu M, Xiang Z, Duan X, Ritz U (2023) Recent advances in biofabrication strategies based on bioprinting for vascularized tissue repair and regeneration. Materials & Design. 229:111885. [CrossRef]
- Ventura RD (2021) An overview of laser-assisted bioprinting (LAB) in tissue engineering applications. Medical Lasers; Engineering, Basic Research, and Clinical Application. 10:76-81. [CrossRef]
- Suamte L, Tirkey A, Barman J, Babu PJ (2023) Various manufacturing methods and ideal properties of scaffolds for tissue engineering applications. Smart Materials in Manufacturing. [CrossRef]
- Manshina AA, Tumkin II, Khairullina EM, Mizoshiri M, Ostendorf A, Kulinich SA, Makarov S, Kuchmizhak AA, Gurevich EL (2024) The second laser revolution in chemistry: Emerging laser technologies for precise fabrication of multifunctional nanomaterials and nanostructures. Advanced Functional Materials. 34:2405457. [CrossRef]
- Sota K, Mondal S, Ando K, Uchimoto Y, Nakajima T (2024) Nanosecond laser texturing of Ni electrodes as a high-speed and cost-effective technique for efficient hydrogen evolution reaction. International Journal of Hydrogen Energy. 93: 1218-1226. [CrossRef]
- all GN, Fan Y, Viellerobe B, Iazzolino A, Dimopoulos A, Poiron C, Clapies A, Luyten FP, Guillemot F, Papantoniou I (2024) Laser-assisted bioprinting of targeted cartilaginous spheroids for high density bottom-up tissue engineering. Biofabrication. 16:045029. [CrossRef]
- Erfanian M, Mohammadi A, Orimi HE, Zapata-Farfan J, Saade J, Meunier M, Larrivée B, Boutopoulos C( 2024) Drop-on-demand bioprinting: A redesigned laser-induced side transfer approach with continuous capillary perfusion. International Journal of Bioprinting. 10: 2832.
- Mareev E, Minaev N, Zhigarkov V, Yusupov V (2021) Evolution of Shock-Induced Pressure in Laser Bioprinting. Photonics. 8:374. [CrossRef]
- Qu J, Dou C, Xu B, Li J, Rao Z, Tsin A ( 2021) Printing quality improvement for laser-induced forward transfer bioprinting: Numerical modeling and experimental validation. Physics of Fluids. 33:071906. [CrossRef]
- Wan Z, Liu Z, Zhang Q, Zhang Q, Gu M (2024) aser Technology for Perovskite: Fabrication and Applications. Advanced Materials Technologies. 9: 2302033. [CrossRef]
- Ng W L, Shkolnikov V( 2024) Jetting-based bioprinting: process, dispense physics, and applications. Bio-Design and Manufacturing. 7:771–799. [CrossRef]
- Gundu S, Varshney N, Sahi AK, Mahto SK (2022) Recent developments of biomaterial scaffolds and regenerative approaches for craniomaxillofacial bone tissue engineering. Journal of Polymer Research. 29:73. [CrossRef]
- Aadil KR, Bhange K, Kumar N, Mishra G (2024)Keratin nanofibers in tissue engineering: bridging nature and innovation. Biotechnology for Sustainable Materials. 1: 1-21. [CrossRef]
- Cheng F, Song D, Li H, Ravi SK, Tan SC ( 2025) Recent Progress in Biomedical Scaffold Fabricated via Electrospinning: Design, Fabrication and Tissue Engineering Application. Advanced Functional Materials. 35:2406950. [CrossRef]
- Gruene M, Deiwick A, Koch L, Schlie S (2011) Unger, C.; Hofmann, N.; Bernemann, I.; Glasmacher, B.; Chichkov, B. Laser Printing of Stem Cells for Biofabrication of Scaffold-Free Autologous Grafts. Tissue Eng. Part C Methods.17:79–87. [CrossRef]
- Hakobyan D, Médina C, Dusserre N, Stachowicz ML, Handschin C, Fricain JC, Guillermet-Guibert J, Oliveira H (2020) Laser-assisted 3D bioprinting of exocrine pancreas spheroid models for cancer initiation study. Biofabrication. 12:035001. [CrossRef]
- Sorkio A, Koch L, Koivusalo L, Deiwick A, Miettinen S, Chichkov B, Skottman H (2018) Human stem cell based corneal tissue mimicking structures using laser-assisted 3D bioprinting and functional bioinks. Biomaterials. 171:57–71. [CrossRef]
- Catros S, Fricain JC, Guillotin B, Pippenger B, Bareille R, Remy M, Lebraud E, Desbat B, Amédée J, Guillemot F (2011) Laserassisted bioprinting for creating on-demand patterns of human osteoprogenitor cells and nano-hydroxyapatite. Biofabrication. 3:025001. [CrossRef]
- Michael S, Sorg H, Peck CT, Koch L, Deiwick A, Chichkov B (2013) Vogt, P.M.; Reimers, K. Tissue Engineered Skin Substitutes Created by Laser-Assisted Bioprinting Form Skin-Like Structures in the Dorsal Skin Fold Chamber in Mice. PLoS ONE. 8:e57741. [CrossRef]
- Gruene M, Pflaum M, Deiwick A, Koch L, Schlie S, Unger C, Wilhelmi M, Haverich A, Chichkov B (2011) Adipogenic differentiation of laser-printed 3D tissue grafts consisting of human adipose-derived stem cells. Biofabrication. 3:015005. [CrossRef]
- Nakielski P, Rinoldi C, Pruchniewski M, Pawłowska S, Gazi´ nska M, Strojny B, Rybak D, Jezierska-Wo´zniak K, Urbanek O, Denis P (2021) Laser-Assisted Fabrication of Injectable Nanofibrous Cell Carriers. Small. 18:2104971. [CrossRef]
- Guillotin B, Souquet A, Catros S et al (2010) Laser assisted bioprinting of engineered tissuewith high cell density andmicroscale organization. Biomaterials. 31(28):7250–7256. [CrossRef]
- Koch L, Deiwick A, Schlie S et al (2012) Skin tissue generation by laser cell printing. Biotechnol Bioeng. 109(7):1855–1863. [CrossRef]
- Ali M, Pages E, Ducom A et al (2014) Controlling laser-induced jet formation for bioprinting mesenchymal stem cells with high viability and high resolution. Biofabrication. 6(4):045001. [CrossRef]
- NahmiasY, Schwartz RE,VerfaillieCMet al (2005) Laser-guided direct writing for three-dimensional tissue engineering. Biotechnol Bioeng. 92(2):129–136. [CrossRef]
- Odde DJ, Renn MJ (1999) Laser-guided direct writing for applications in biotechnology. Trends Biotechnol. 17(10):385–389. [CrossRef]
- Wang ZJ, Abdulla R, Parker B et al (2015) A simple and highresolution stereolithography-based 3D bioprinting system using visible light crosslinkable bioinks. Biofabrication. 7(4):045009. [CrossRef]
- Lee W, Debasitis JC, Lee VK et al (2009) Multi-layered culture of human skin fibroblasts and keratinocytes through threedimensional freeform fabrication. Biomaterials 30(8):1587–1595. [CrossRef]
- MinD,LeeW, Bae I-H,Lee TR,Croce P,Yoo S-S (2017) Bioprinting of biomimetic skin containing melanocytes. Exp Dermatol.1–7. [CrossRef]
- Kim BS, Lee JS, Gao G et al (2017) Direct 3D cell-printing of human skin with functional transwell system. Biofabrication. 9(2):025034. [CrossRef]
- Xu F, Celli J, Rizvi I et al (2011) A three-dimensional in vitro ovarian cancer coculture model using a high-throughput cell patterning platform. Biotechnol J. 6(2):204–212. [CrossRef]
- Faulkner-JonesA, FyfeC,CornelissenDJ et al (2015) Bioprinting of human pluripotent stem cells and their directed differentiation into hepatocyte-like cells for the generation of mini-livers in 3D. Biofabrication. 7(4):044102. [CrossRef]
- Ávila HM, Schwarz S, Rotter N, Gatenholma P (2016) 3D bioprinting of human chondrocyte-laden nanocellulose hydrogels for patient-specific auricular cartilage regeneration. Bioprinting. 1–2:22–35. [CrossRef]
- Lee JS, Hong JM, Jung JW et al (2014) 3D printing of composite tissue with complex shape applied to ear regeneration. Biofabrication. 6(2):1–12. [CrossRef]
- Muller M, Ozturk E, Arlov O et al (2017) Alginate sulfatenanocellulose bioinks for cartilage bioprinting applications. Ann Biomed Eng. 45(1):210–223. [CrossRef]
- 34. Huang S, Yao B, Xie JF et al (2016) 3D bioprinted extracellular matrix mimics facilitate directed differentiation of epithelial progenitors for sweat gland regeneration. Acta Biomater. 32:170–177. [CrossRef]
- GaoQ, LiuZ,Lin Z, Qiu J,LiuY, LiuA,WangY,XiangM, Chen B, Fu J, He Y (2017) 3D bioprinting of vessel-like structures with multilevel fluidic channels. ACS Biomater Sci Eng. 3(3):399–408. [CrossRef]
- Ozbolat IT,ChenH,YuY(2014) Development of ’Multi-arm Bioprinter’ for hybrid biofabrication of tissue engineering constructs. Robot Comput Integr Manuf. 30(3):295–304. [CrossRef]
- Zhang B, Gao L, Gu L, Yang H, Luo Y, Ma L (2017) Highresolution 3D bioprinting system for fabricating cell-laden hydrogel scaffolds with high cellular activities. Procedia Cirp. 65:219–224. [CrossRef]
- Khalil S, Nam J, Sun W (2005) Multi-nozzle deposition for construction of 3D biopolymer tissue scaffolds. Rapid Prototyp J. 11(1):9–17. [CrossRef]
- Kang HW, Lee SJ, Ko IK et al (2016) A 3D bioprinting system to produce human-scale tissue constructs with structural integrity. Nat Biotechnol. 34(3):312–319. [CrossRef]
- Dilip K C, Rui LR, Subhas CK, Awanish K, Chinmaya M (2024) Nanomaterials-Based Hybrid Bioink Platforms in Advancing 3D Bioprinting Technologies for Regenerative Medicine. ACS Biomater. Sci. Eng. 10(7):4145–4174. [CrossRef]
- Hao W, Wang Z, Dimitra L, Haoyi Y, Darius G, Hongtao W, Cheng-Feng P, Parvathi Nair Suseela N, Yujie K, Tomohiro M, John You En Ch, Qifeng R, Maria F, Mangirdas M, Saulius J, Min G, Joel K W Y (2023) Two-Photon Polymerization Lithography for Optics and Photonics: Fundamentals, Materials, Technologies, and Applications. ADVANCED FUNCTIONAL MATERILAS.33:2214211. [CrossRef]
- Hyunmin Ch, Won-Sup L, Won Seok Ch (2024) Three-dimensional photopolymerization additive manufacturing technology based on two-photon polymerization. JMST Advances. 6:371-377. [CrossRef]
- Balkwill FR, Capasso M, Hagemann T (2012) The Tumor Microenvironment at a Glance. J. Cell Sci. 125 (23):5591−5596. [CrossRef]
- Kerkar SP, Restifo NP (2012) Cellular Constituents of Immune Escape within the Tumor Microenvironment. Cancer Res. 72(13):3125−3130. [CrossRef]
- Baghban R, Roshangar L, Jahanban-Esfahlan R, Seidi K, Ebrahimi-Kalan A, Jaymand M, Kolahian S, Javaheri T, Zare P (2020)Tumor Microenvironment Complexity and Therapeutic Implications at a Glance. Cell Commun. Signaling.18 (1): 1−19. [CrossRef]
- Jin Y, Ai J, Shi J (2015) Lung Microenvironment Promotes the Metastasis of Human Hepatocellular Carcinoma Cells to the Lungs. Int. J. Clin. Exp. Med.8 (6): 9911−9917.
- Iwahori K (2020) Cytotoxic CD8+ Lymphocytes in the Tumor Microenvironment. Adv. Exp. Med. Biol.1224: 53−62. [CrossRef]
- Maimela NR, Liu S, Zhang Y (2019) Fates of CD8+ T Cells in Tumor Microenvironment. Comput. Struct. Biotechnol. J.17:1−13. [CrossRef]
- Sharonov GV, Serebrovskaya EO, Yuzhakova DV, Britanova OV, Chudakov DM (2020) B Cells, Plasma Cells and Antibody Repertoires in the Tumour Microenvironment. Nat. Rev. Immunol. 20 (5): 294−307. [CrossRef]
- Wang S, Liu W, Ly D, Xu H, Qu L, Zhang L (2019) Tumor-Infiltrating B Cells: Their Role and Application in Anti-Tumor Immunity in Lung Cancer. Cell. Mol. Immunol. 16 (1): 6−18. [CrossRef]
- Larsen SK, Gao Y, Basse PH (2014) NK Cells in the Tumor Microenvironment. Crit. Rev. Oncog. 19 (1-2): 91−105.
- Liao Z, Tan ZW, Zhu P, Tan NS (2019) Cancer-Associated Fibroblasts in Tumor Microenvironment − Accomplices in Tumor Malignancy. Cell. Immunol. 343:103729. [CrossRef]
- Monteran L, Erez N (2019) The Dark Side of Fibroblasts: Cancer- Associated Fibroblasts as Mediators of Immunosuppression in the Tumor Microenvironment. Front. Immunol.10:1−15. [CrossRef]
- Chouaib S, Kieda C, Benlalam H, Noman MZ, Mami-Chouaib F, Rüegg C (2010) Endothelial Cells as Key Determinants of the Tumor Microenvironment: Interaction with Tumor Cells, Extracellular Matrix and Immune Killer Cells. Crit. Rev. Immunol. 30(6):529−545.
- Walker C, Mojares E, Del Río Hernández A (2018) Role of Extracellular Matrix in Development and Cancer Progression. Int. J. Mol. Sci.19 (10):3028. [CrossRef]
- Padhi A, Nain AS (2020) ECM in Differentiation: A Review of Matrix Structure, Composition and Mechanical Properties. Ann. Biomed. Eng. 48 (3):1071−1089. [CrossRef]
- Mierke CT (2019) The Matrix Environmental and Cell Mechanical Properties Regulate Cell Migration and Contribute to the Invasive Phenotype of Cancer Cells. Rep. Prog. Phys. 82 (6): 064602. [CrossRef]
- Fischer T, Wilharm N, Hayn A, Mierke CT (2017) Matrix and Cellular Mechanical Properties Are the Driving Factors for Facilitating Human Cancer Cell Motility into 3D Engineered Matrices. Converg. Sci. Phys. Oncol. 3 (4): 044003. [CrossRef]
- Pathak A, Kumar S (2012) Independent Regulation of Tumor Cell Migration by Matrix Stiffness and Confinement. Proc. Natl. Acad. Sci. U. S. A.109 (26) :10334−10339. [CrossRef]
- Whiteside TL (2008) The tumor microenvironment and its role in promoting tumor growth. Oncogene. 27:5904–5912. [CrossRef]
- Wang X, Li X, Ding J, Long X, Zhang H, Zhang X, Jiang X, Xu T (2021) 3D bioprinted glioma microenvironment for glioma vascularization. J. Biomed. Mater. Res. Part A.109: 915–925. [CrossRef]
- Chen K, Jiang E, Wei X, Xia Y, Wu Z, Gong Z, Shang Z, Guo S (2021) The acoustic droplet printing of functional tumor microenvironments. Lab Chip. 21:1604–1612.
- Liu Y, Liu Y, Zheng X, Zhao L, Zhang X (2020) Recapitulating and Deciphering Tumor Microenvironment by Using 3D Printed Plastic Brick–Like Microfluidic Cell Patterning. Adv. Health Mater.9:e1901713. [CrossRef]
- Duan J, Cao Y, Shen Z, Cheng Y, Ma Z, Wang L, Zhang Y, An Y, Sang S(2022) 3D Bioprinted GelMA/PEGDA Hybrid Scaffold for Establishing an In Vitro Model of Melanoma. J. Microbiol. Biotechnol. 32:531–540. [CrossRef]
- Jiang T, Munguia-Lopez J, Flores-Torres S, Grant J, Vijayakumar S, De Leon-Rodriguez A, Kinsella, JM (2018) Bioprintable Alginate/Gelatin Hydrogel 3D In Vitro Model Systems Induce Cell Spheroid Formation. J. Vis. Exp.137:e57826. [CrossRef]
- Kim J, Jang J, Cho DW (2021) Controlling Cancer Cell Behavior by Improving the Stiffness of Gastric Tissue-Decellularized ECM Bioink With Cellulose Nanoparticles. Front. Bioeng. Biotechnol. 9: 605819. [CrossRef]
- Aveic S, Janßen S, Nasehi R, Seidelmann M, Vogt M, Pantile M, Rütten S, Fischer H (2021) A 3D printed in vitro bone model for the assessment of molecular and cellular cues in metastatic neuroblastoma. Biomater. Sci. 9:1716–1727.
- Lv K, Zhu J, Zheng S, Jiao Z, Nie Y, Song F, Liu T, Song K (2021) Evaluation of inhibitory effects of geniposide on a tumor model of human breast cancer based on 3D printed Cs/Gel hybrid scaffold. Mater. Sci. Eng. C Mater. Biol. Appl. 119:111509. [CrossRef]
- Vanderburgh J, Sterling JA, Guelcher SA (2017) 3D Printing of Tissue Engineered Constructs for In Vitro Modeling of Disease Progression and Drug Screening. Ann. Biomed Eng. 45:164–179. [CrossRef]
- Chen Y, Bian L, Zhou H, Wu D, Xu J, Gu C, Fan X, Liu Z, Zou J, Xia J (2020) Usefulness of three-dimensional printing of superior mesenteric vessels in right hemicolon cancer surgery. Sci. Rep. 10:11660. [CrossRef]
- Park JW, Kang HG, Kim JH, Kim HS (2021) The application of 3D-printing technology in pelvic bone tumor surgery. J. Orthop. Sci. 26:276–283. [CrossRef]
- Zeng N, Yang J, Xiang N, Wen S, Zeng S, Qi S, Zhu W, Hu H, Fang C (2020) Application of 3D visualization and 3D printing in individualized precision surgery for Bismuth-Corlette type III and IV hilar cholangiocarcinoma. Nan Fang Yi Ke Da XueXue Bao. 40:1172–1177, (In Chinese).
- Huang X, Liu Z, Wang X, Li XD, Cheng K, Zhou Y, Jiang XB (2019) A small 3D printing model of macroadenomas for endoscopic endonasal surgery. Pituitary. 22: 46–53. [CrossRef]
- Emile SH, Wexner SD (2019) Systematic review of the applications of three-dimensional printing in colorectal surgery. Color. Dis. 21:261–269. [CrossRef]
- Hong D, Lee S, Kim T, Baek JH, Kim WW, Chung KW, Kim N, Sung TY (2020) Usefulness of a 3D-Printed Thyroid Cancer Phantom for Clinician to Patient Communication. World J. Surg. 44:788–794. [CrossRef]
- Burdall OC, Makin E, Davenport M, Ade-Ajayi N (2016) 3D printing to simulate laparoscopic choledochal surgery. J. Pediatric Surg. 51: 828–831. [CrossRef]
- Smelt JL, Suri T, Valencia O, Jahangiri M, Rhode K, Nair A, Bille A (2019) Operative Planning in Thoracic Surgery: A Pilot Study Comparing Imaging Techniques and Three-Dimensional Printing. Ann. Thorac. Surg. 107: 401–406. [CrossRef]
- Wang L, Wang H, Jiang Y, Ji Z, Guo F, Jiang P, Li X, Chen Y, Sun H, Fan J (2020) The efficacy and dosimetry analysis of CT-guided 125I seed implantation assisted with 3D-printing non-co-planar template in locally recurrent rectal cancer. Radiat. Oncol. 15:179. [CrossRef]
- Yoon SH, Park S, Kang CH, Park IK, Goo JM, Kim YT (2019) Personalized 3D-Printed Model for Informed Consent for Stage I Lung Cancer: A Randomized Pilot Trial. Semin. Thorac. Cardiovasc. Surg. 31:316–318. [CrossRef]
- Shen Z, Xie Y, Shang X, Xiong G, Chen S, Yao Y, Pan Z, Pan H, Dong X, Li Y (2020) The manufacturing procedure of 3D printed models for endoscopic endonasal transsphenoidal pituitary surgery. Technol. Health Care. 28:131–150.
- Chen Y, Zhang J, Chen Q, Li T, Chen K, Yu Q, Lin X (2020) Three-dimensional printing technology for localised thoracoscopic segmental resection for lung cancer: A quasi-randomised clinical trial. World J. Surg. Oncol. 18: 223. [CrossRef]
- Lan Q, Zhu Q, Xu L, Xu T (2020) Application of 3D-Printed Craniocerebral Model in Simulated Surgery for Complex Intracranial Lesions. World Neurosurg. 134:e761–e770. [CrossRef]
- Wang L, Cao T, Li X. Huang L (2016) Three-dimensional printing titanium ribs for complex reconstruction after extensive posterolateral chest wall resection in lung cancer. J. Thorac. Cardiovasc. Surg. 152: e5–e7.
- Valente KP, Khetani S, Kolahchi AR, Sanati-Nezhad A, Suleman A, Akbari M (2017) Microfluidic technologies for anticancer drug studies. Drug Discov. Today. 22:1654–1670. [CrossRef]
- Serrano DR, Terres MC, Lalatsa A (2018) Applications of 3D printing in cancer. J. 3D Print. Med. 2:115–127. [CrossRef]
- Marei I, Abu Samaan T, Al-Quradaghi MA, Farah AA, Mahmud SH, Ding H and Triggle CR (2022) 3D Tissue-Engineered Vascular Drug Screening Platforms: Promise and Considerations. Front. Cardiovasc. Med. 9:847554. [CrossRef]
- Chen X, Chen H, Wu D, Chen Q, Zhou Z, Zhang R, Peng X, Su YC, Sun D (2018) 3D printed microfluidic chip for multiple anticancer drug combinations. Sens. Actuators B Chem. 276: 507–516. [CrossRef]
- Zhao X, Du S, Chai LM, Xu Y, Liu L, Zhou X, Wang J, Zhang W, Liu CH, Wang X (2015) Anti-cancer drug screening based on a adipose-derived stem cell/hepatocyte 3D printing technique. J. Stem Cell Res. Ther. 5:273.
- J.Gonzalez-Barahona JM, Robles G (2023) Revisiting the reproducibility of empirical software engineering studies based on data retrieved from development repositories. Information and Software Technology. 164: 107318. [CrossRef]
- Moreau D, Wiebels K, Boettiger C (2023) Containers for computational reproducibility .Nature Reviews Methods Primers. 3:50. [CrossRef]
- Ding Y, DeSarbo WS, Hanssens DM, Jedidi K (2020) The past, present, and future of measurement and methods in marketing analysi. Marketing Letters. 31:175–186. [CrossRef]
- Dong Y, Zhou X, Ding Y, Luo Y, Zhao H (2024) Advances in tumor microenvironment: applications and challenges of 3D bioprinting," Biochemical and Biophysical. 730:150339. [CrossRef]
- Zeng Y, Hao D, Huete A, Dechant B, Berry J (2022) Optical vegetation indices for monitoring terrestrial ecosystems globally. Earth & Environment. 3:477–493. [CrossRef]
- Catacutan DB, Alexander J, Arnold A (2024) Machine learning in preclinical drug discovery. Nature Chemical. 20:960–973. [CrossRef]
- Ren F, Aliper A, Chen J, Zhao H, Rao S, Kuppe C (2024) A small-molecule TNIK inhibitor targets fibrosis in preclinical and clinical models. Nature. [CrossRef]
- Vergis N, Patel V, Bogdanowicz K (2024) IL-1 Signal Inhibition in Alcohol-Related Hepatitis: A Randomized, Double-Blind, Placebo-Controlled Trial of Canakinumab. Clinical. [CrossRef]
- Sztankovics D, Moldvai D, Petővári G, Gelencsér R, Krencz I, Raffay R, Dankó T, Sebestyén A (2023), 3D bioprinting and the revolution in experimental cancer model systems—A review of developing new models and experiences with in vitro 3D bioprinted breast cancer tissuemimetic structures. Pathol. Oncol. Res. 29:1610996. [CrossRef]
- Wang X, Yang X, Liu X, Shen Z, Li M, Cheng R, Zhao L (2024) 3D bioprinting of an in vitro hepatoma microenvironment model: establishment, evaluation, and anticancer drug testing. Acta Biomaterialia. 185: 173-189. [CrossRef]
- Gogoi D, Kumar M, Singh J (2024) A comprehensive review on hydrogel-based bio-ink development for tissue engineering scaffolds using 3D printing. Annals of 3D Printed Medicine. 15: 100159. [CrossRef]
- Bini F, D’Alessandro S, Agarwal T (2023) Biomimetic 3D bioprinting approaches to engineer the tumor microenvironment. Int J Bioprint. 9(6): 1022. [CrossRef]
- Himanshu T, Sandeep MS, Avanish SP, Shilpi Ch (2022) Hydrogel based 3D printing: Bio ink for tissue engineering. Journal of Molecular Liquids. 367:120390. [CrossRef]
- Guan X, Fei Z, Wang L, Ji G (2025) Engineered streaky pork by 3D co-printing and co-differentiation of muscle and fat cells. Food Hydrocolloids. 158:110578. [CrossRef]
- Pereira I, Lopez-Martinez MJ, Villasante A, Introna C, Tornero D, Canals JM and Samitier J (2023), Hyaluronic acid-based bioink improves the differentiation and network formation of neural progenitor cells. Front. Bioeng. Biotechnol. 11:1110547. [CrossRef]
- Rahman TT, Wood N, Akib YM, Qin H (2024) Experimental Study on Compatibility of Human Bronchial Epithelial Cells in Collagen–Alginate Bioink for 3D Printing. Bioengineering. 11(9): 862. [CrossRef]
- Wei Q, An Y, Zhao X, Li M, Zhang J (2024) Three-dimensional bioprinting of tissue-engineered skin: Biomaterials, fabrication techniques, challenging difficulties, and future directions: A review. International Journal of Biological. 266: 131281. [CrossRef]
- Wang J, Cui Z, Maniruzzaman M (2023) Bioprinting: a focus on improving bioink printability and cell performance based on different process parameters. International journal of pharmaceutics. 640:123020. [CrossRef]
- Zhang H, Wang Y, Zheng Z, Wei X, Chen L, Wu Y (2023) Strategies for improving the 3D printability of decellularized extracellular matrix bioink. Theranostics.13 (8):2562–2587. [CrossRef]
- Morenikeji A, Fabien B, Romain S, Noelia MS, Sylvie B, Ian S, Martial S (2024) Evaluation of the printability of agar and hydroxypropyl methylcellulose gels as gummy formulations: Insights from rheological properties. International Journal of Pharmaceutics. 654:123937. [CrossRef]
- Lee SC, Gillispie G, Prim P, Lee SJ (2020) Physical and chemical factors influencing the printability of hydrogel-based extrusion bioinks. Chemical reviews. 120(19):10834–10886. [CrossRef]
- Uroz M, Stoddard AE, Sutherland BP, Courbot O (2024) Differential stiffness between brain vasculature and parenchyma promotes metastatic infiltration through vessel co-option. Nature Cell. [CrossRef]
- Link R, Weißenbruch K, Tanaka M (2024) Cell shape and forces in elastic and structured environments: from single cells to organoids. Advanced Functional. 34: 2302145. [CrossRef]
- Mao H, Yang L, Zhu H, Wu L, Ji P, Yang J (2020) Recent advances and challenges in materials for 3D bioprinting. Progress in Natural, Elsevier. 30(5):618-634. [CrossRef]
- Murphy SV, De Coppi P, Atala A (2020) Opportunities and challenges of translational 3D bioprinting. Nature biomedical engineering. 4:370–380. [CrossRef]
- Levato R, Jungst T, Scheuring RG, Blunk T (2020) From shape to function: the next step in bioprinting. Advanced. 32(12):1906423. [CrossRef]
- Phung LX, Ta TQ, Pham VH, Nguyen MTH, Do T (2024) The development of a modular and open-source multi-head 3D bioprinter for fabricating complex structures. Bioprinting. 39:e00339. [CrossRef]
- Hwang DG, Choi H, Yong U, Kim D, Kang W (2024) Bioprinting-assisted Tissue Assembly for Structural and Functional Modulation of Engineered Heart Tissue Mimicking Left Ventricular Myocardial Fiber Orientation. Advanced. 36(34):2400364. [CrossRef]
- De Spirito M, Palmieri V, Perini G, Papi M (2024) Bridging the gap: integrating 3D bioprinting and microfluidics for advanced multi-organ models in biomedical research. Bioengineering.11 (7):664. [CrossRef]
- Rathnayaka M, Karunasinghe D, Gunasekara C (2024) Machine learning approaches to predict compressive strength of fly ash-based geopolymer concrete: A comprehensive review. Construction and Building Materials. 419:135519. [CrossRef]
- Ramesh S, Deep A, Tamayol A, Kamaraj A, Mahajan C (2024) Advancing 3D bioprinting through machine learning and artificial intelligence. Bioprinting 38:E00331. [CrossRef]
- Levato R, Dudaryeva O (2023) Light-based vat-polymerization bioprinting. Nature Reviews.47. [CrossRef]
- Makode S, Maurya S, Niknam SA (2024) Three dimensional (bio) printing of blood vessels: from vascularized tissues to functional arteries. 16(2):022005. [CrossRef]
- Bercea M (2023) Rheology as a tool for fine-tuning the properties of printable bioinspired gels. Molecules. 28(6):2766. [CrossRef]
- Niculescu AG, Chircov C, Bîrc˘a AC, Grumezescu AM (2021) Fabrication and Applications of Microfluidic Devices: A Review. Int. J. Mol. Sci. 22: 2011. [CrossRef]
- Ferreira M, Carvalho V, Ribeiro J, Lima RA, Teixeira S (2024) Advances in Microfluidic Systems and Numerical Modeling in Biomedical Applications: A Review. Micromachines. 15(7):873. [CrossRef]
- Taghizadeh M, Taghizadeh A, Yazdi MK, Zarrintaj P (2022) Chitosan-based inks for 3D printing and bioprinting. Green. 24: 62-101. [CrossRef]
- Fatimi A, Okoro OV, Podstawczyk D, Siminska-Stanny J (2022) Natural hydrogel-based bio-inks for 3D bioprinting in tissue engineering: a review. Gels.8(3):179. [CrossRef]
- Satchanska G, Davidova S, Petrov PD (2024) Ntural and Synthetic Polymers for Biomedical and Environmental Applications. Polymers. 16:1159. [CrossRef]
- Benwood C, Chrenek J, Kirsch RL, Masri NZ (2021) Natural biomaterials and their use as bioinks for printing tissues. Bioengineering. 8(2):27. [CrossRef]
- Sánchez DH, Comtois-Bona M, Muñoz M, Ruel M (2024) Manufacturing and validation of small-diameter vascular grafts: A mini review. Iscience. 27:109845. [CrossRef]
- Arulmozhivarman JC, Rajeshkumar L (2024) Synthetic fibers and their composites for biomedical applications. Synthetic and Mineral, Elsevier. 495-511. [CrossRef]
- Chakraborty J, Mu X, Pramanick A, Kaplan DL (2022) Recent advances in bioprinting using silk protein-based bioinks. Biomaterials. 287:121672. [CrossRef]
- Matai I, Kaur G, Seyedsalehi A, McClinton A (2020) Progress in 3D bioprinting technology for tissue/organ regenerative engineering. Biomaterials. 226:119536. [CrossRef]
- Mirshafiei M, Rashedi H, Yazdian F, Rahdar A (2024) Advancements in tissue and organ 3D bioprinting: Current techniques, applications, and future perspectives. Materials & Design. 240:112853. [CrossRef]
- Lee SJ, Jeong W, Atala A (2024) 3D Bioprinting for Engineered Tissue Constructs and Patient-Specific Models: Current Progress and Prospects in Clinical Applications. Advanced Materials. 2408032. [CrossRef]
Figure 1.
The figure illustrates key 3D bioprinting methods, including laser-assisted techniques (LIFT and LIBP), photopolymerization methods (TPP and DLP), and extrusion-based methods.
Figure 1.
The figure illustrates key 3D bioprinting methods, including laser-assisted techniques (LIFT and LIBP), photopolymerization methods (TPP and DLP), and extrusion-based methods.
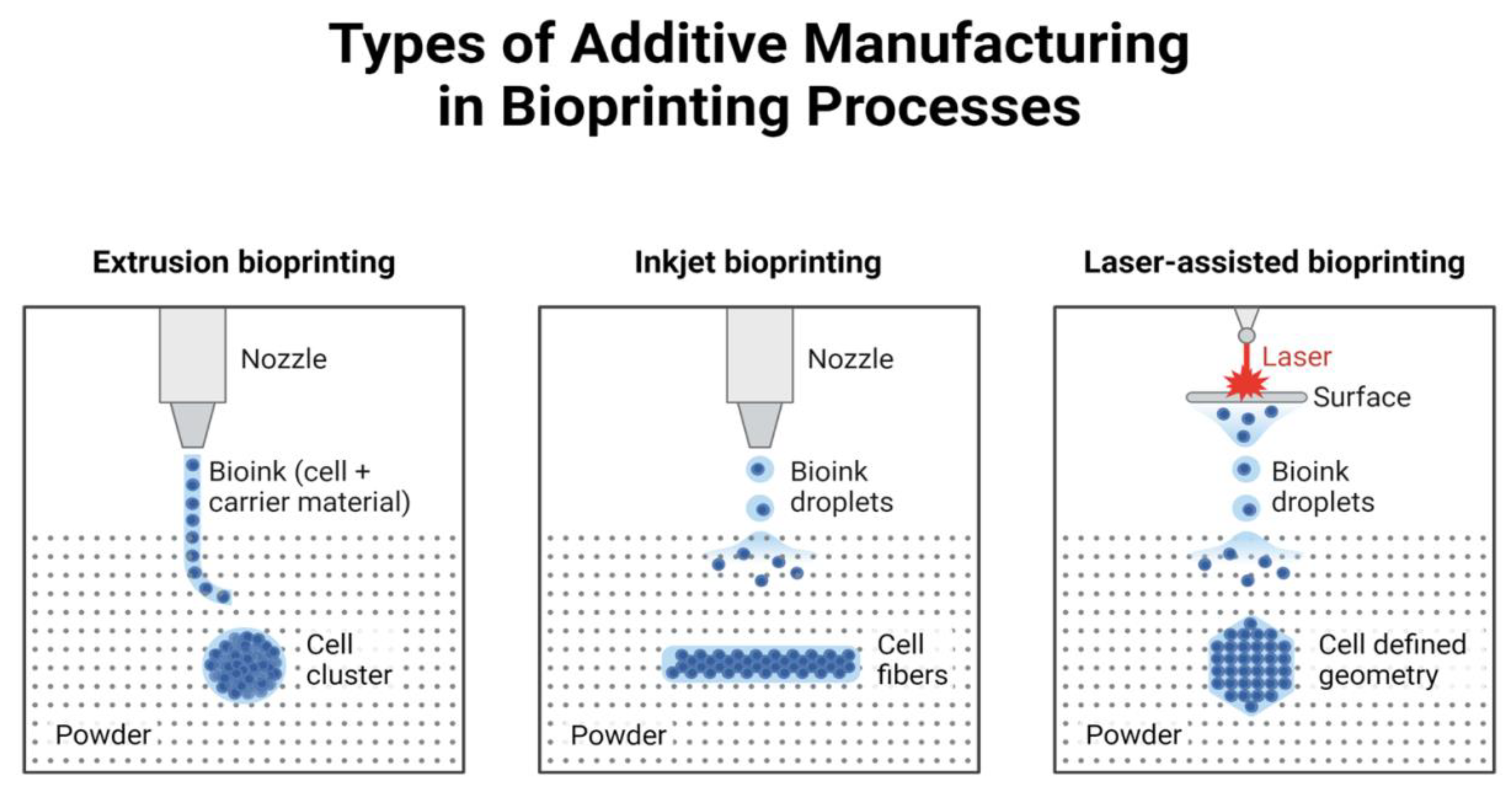
Figure 2.
Characteristics of the tumor microenvironment. Tumors are defined by the presence of cells undergoing uncontrolled proliferation and are complex mini-organs comprising many cell types and matrix components Created in https://BioRender.com.
Figure 2.
Characteristics of the tumor microenvironment. Tumors are defined by the presence of cells undergoing uncontrolled proliferation and are complex mini-organs comprising many cell types and matrix components Created in https://BioRender.com.
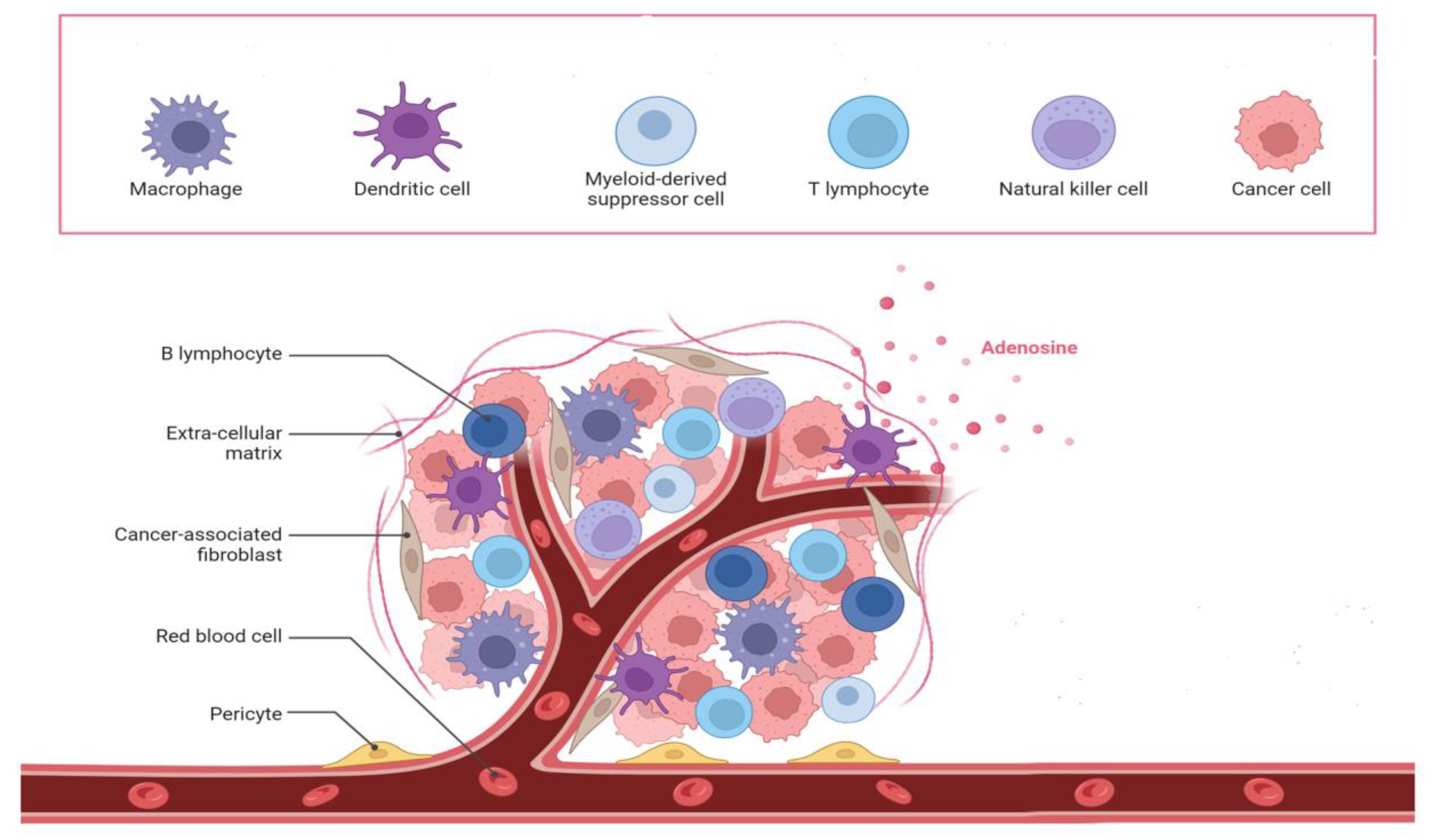
Figure 3.
Classification and application of medical biopriniting .


Table 1.
Characteristics of several bioprinting techniques.
| Print methods | Bioinks | Resolution | Material Deposition rate | Suitability | References |
|---|---|---|---|---|---|
|
Laser-assisted printing |
Fibrinogen, collagen, GelMA |
1–50μm | High | High-resolution skin, vessel, and tumor models. | [63,64,65,66,67,68] |
|
Inkjet printing |
Collagen, poly(ethylene glycol) dimethacrylate (PEGDMA), fibrinogen, alginate, GelMA |
50–500μm | Medium | Medium-resolution structures; drug testing. | [13,69,70,71,72,73] |
|
Extrusion printing |
Gelatin, polycaprolactone (PCL), polyethylene glycol (PEG), alginate, hyaluronic acid (HA), polyamide(PA), polydimethylsiloxane (PDMS) dECM, nanocellulose |
>50μm | Low | Large-scale tissue scaffolds. | [74,75,76,77,78,79,80,81,82,83] |
| Photopolymerization | Photosensitive Hydrogels | Sub-1 µm (TPP/DLP) | Medium to High | High-resolution, cell-laden tumor and organ-on-chip models. | [84,85] |
Table 2.
Comparison of commonly used 3D bioprinting techniques.
| Method | Advantages | Disadvantages | Latest Developments (2025) |
|---|---|---|---|
| Inkjet Printing | High efficiency; low cost; compatible with multi-material printing. | Limited viscosity of bioinks; potential cell damage from droplet ejection. | Advances in nozzle designs to reduce shear stress on cells. |
| Extrusion Printing | Affordable; wide range of bioink viscosities; high cell density deposition. | Low resolution; slower for complex structures; limited material types. | Multi-material extrusion allowing for gradient tissue constructs. |
| Laser-Assisted Printing | High precision; non-contact printing; adaptable for living cells. | Equipment cost; challenges with scalability; potential thermal effects. | LIFT techniques now employ hydrogel coatings instead of metal layers. |
| Photopolymerization (TPP/DLP) | Exceptional resolution (sub-micron); suitable for creating intricate structures. | Limited to photosensitive materials; potential phototoxicity. | Expanded use of biocompatible photoinitiators for living cell encapsulation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



