Submitted:
27 January 2025
Posted:
28 January 2025
You are already at the latest version
Abstract
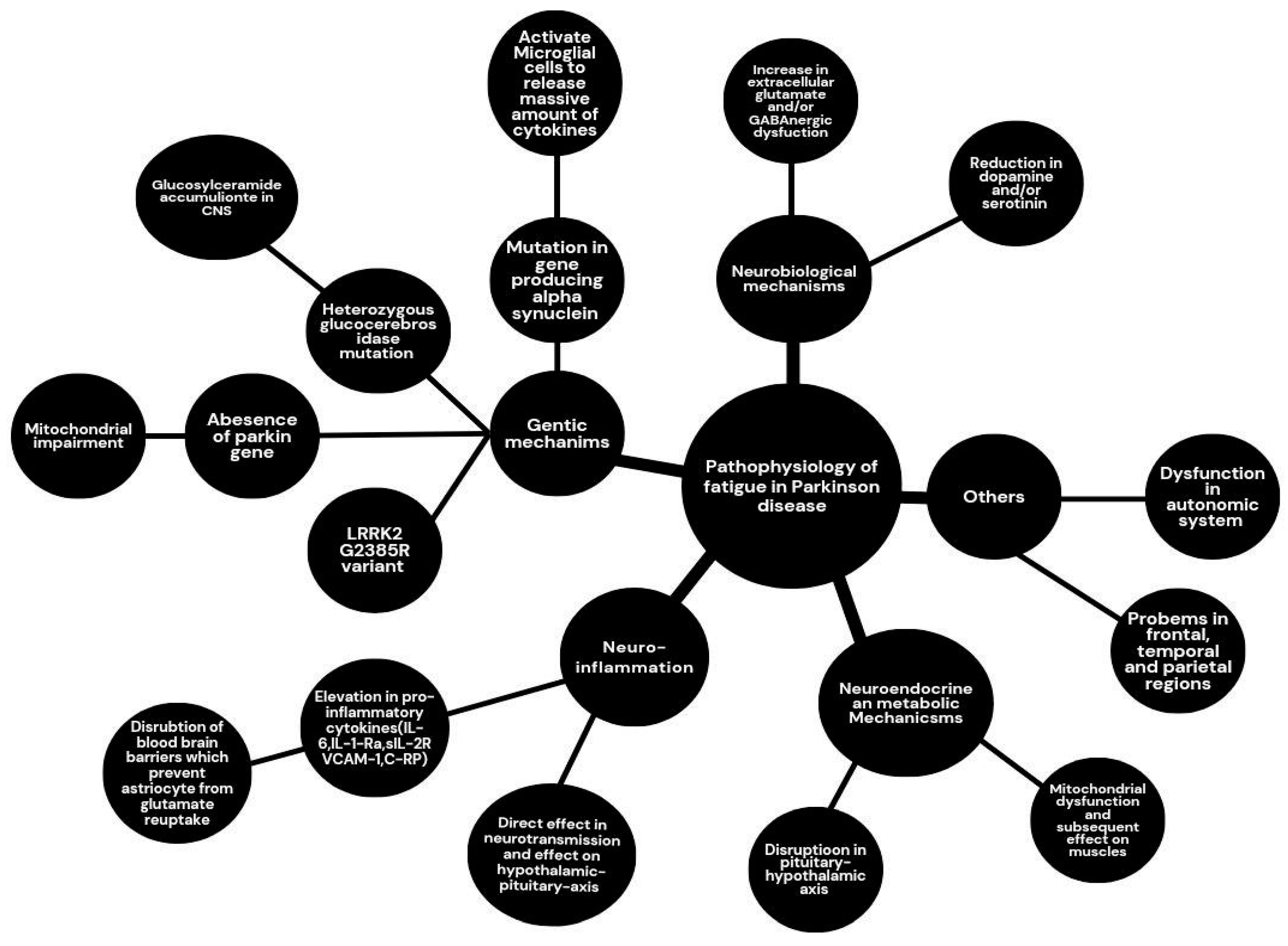
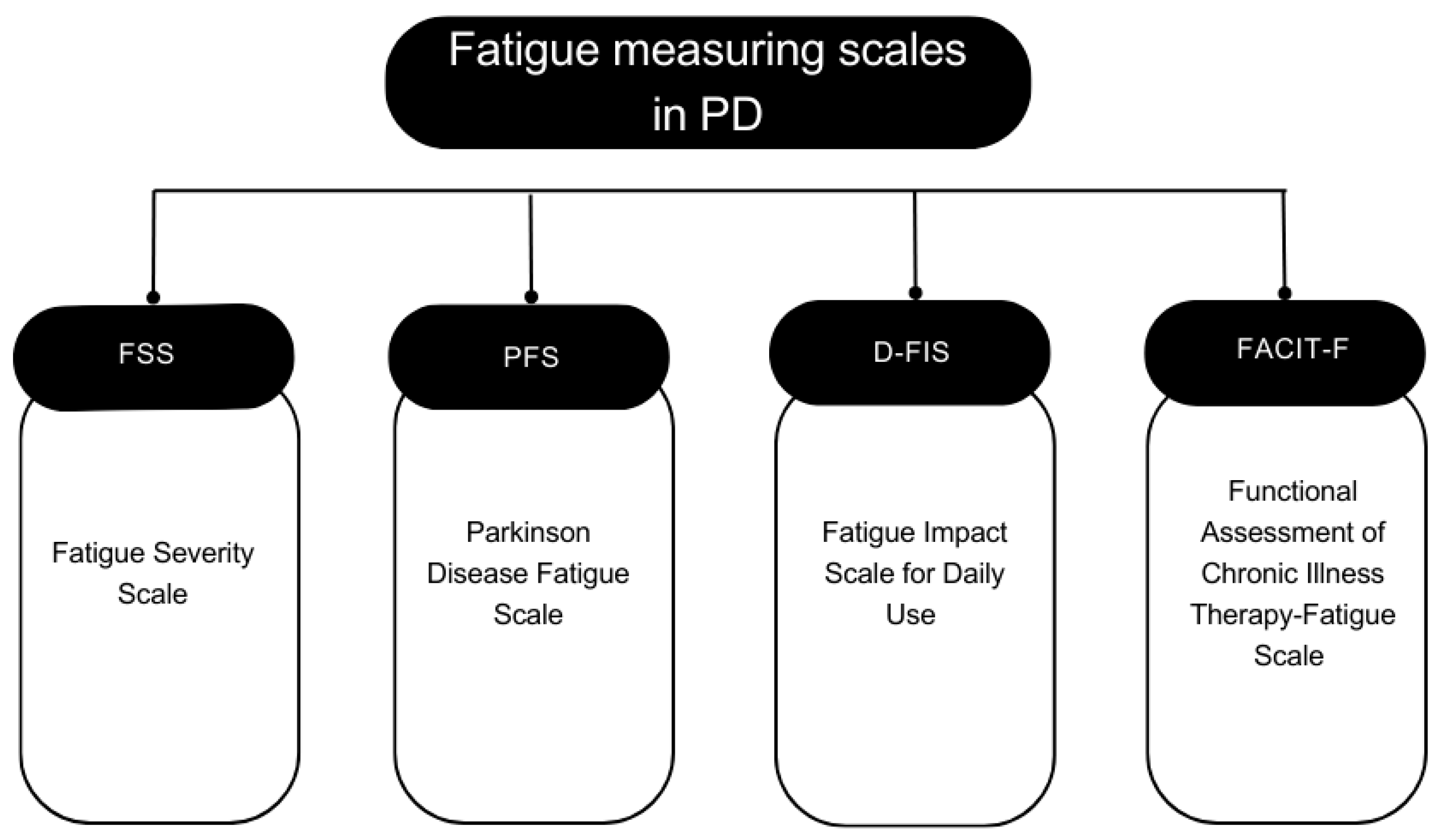
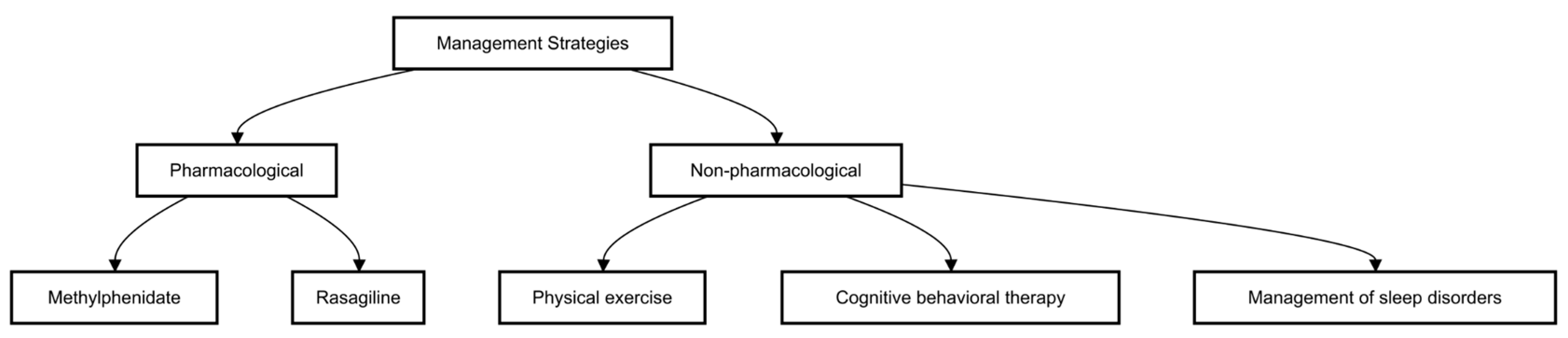
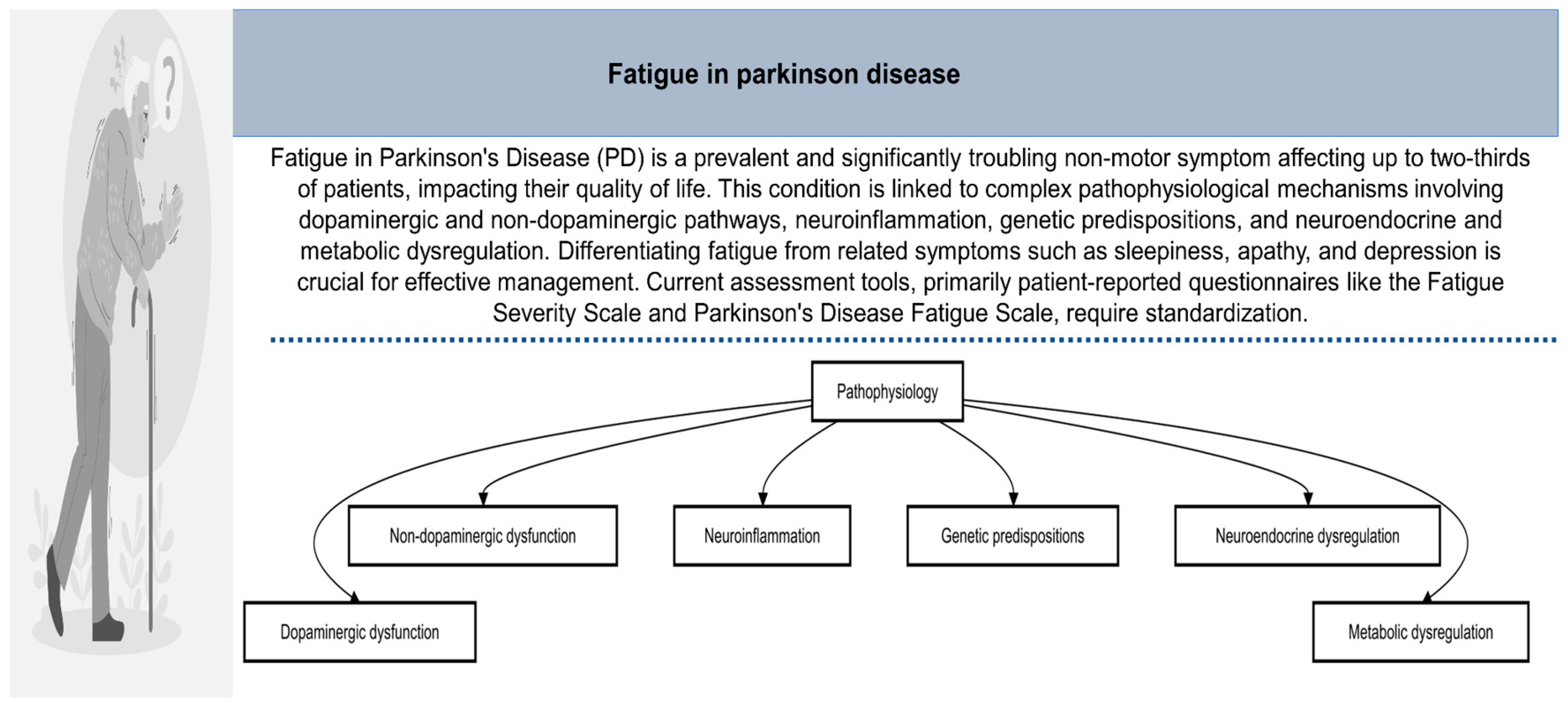
One of the most common and usually very incapacitating non-motor manifestations in PD, fatigue is both a symptom experienced by up to two-thirds of all patients and significantly troubling in relation to quality of life. This review will give a thorough overview of complex pathophysiology, prevalence, course, specific clinical presentation, methods of assessment, and current strategies in the management of fatigue in PD. Finally relating to dysfunction in dopaminergic and non-dopaminergic pathways, neuroinflammation, genetic predispositions, and neuroendocrine and metabolic dysregulation, the underlying mechanisms of fatigue in PD relate to the latter disorders. Generally, prevalence rates of fatigue in PD have been reported to be within the bracket of 36-60%, underlining the need for standardization of assessment tools and a universal definition. Fatigue in PD appear “feeling of abnormal and overwhelming tiredness and lack of energy that is distinct both qualitatively and quantitatively from normal tiredness, clinically many times pre-dating the manifestation of motor symptoms by years. The differentiation of fatigue from sleepiness, apathy, and depression is very important for PD symptoms and treatment. The present available assessment tools include mainly patient-reported questionnaires the Fatigue Severity Scale and Parkinson's Disease Fatigue Scale. The management include both pharmacological and non-pharmacological managements. Well, though drugs like methylphenidate and rasagiline hold promise, an equally important role is played by physical exercise, cognitive behavioral therapy, and the management of sleep disorders. Further research is needed to clarify the complex pathophysiology of fatigue in PD, with a view toward the identification of objective biomarkers, and the development of targeted and effective treatment strategies for relief of this common and burdensome symptom.
Keywords:
1. Introduction
2. Pathophysiology
2.1. Overview of Fatigue In Neurological Disorders
2.2. Neurobiological Mechanisms
2.2.1. Dopaminergic Pathways
2.2.2. Non-Dopaminergic Systems
2.3. Role Of Inflammation
2.4. Genetic Factors
2.5. Neuroendocrine And Metabolic Dysregulation
2.6. Other Mechanisms
3. Prevalence And Epidemiology
4. Clinical Manifestations
4.1. Assessment Of Fatigue In Parkinson's Disease
4.2. Factors Contributing To Fatigue In Parkinson’s Disease
4.3. Overlap Of Fatigue with Other Conditions
4.3.1. Sleep Disorders
4.3.2. Depressive Disorders
4.3.3. Cognitive Deficits
4.4. Deep Brain Stimulation And Parkinson’s Disease Fatigue
5. Management
5.1. Pharmacological Management
5.2. Non-Pharmacological Interventions
6. Specialist Recommendations And Future Studies
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACTH | Adrenocorticotropic Hormone |
| CBT | Cognitive Behavioral Therapy |
| CNS | Central Nervous System |
| CSF | Cerebrospinal Fluid |
| EDS | Excessive Daytime Sleepiness |
| FACIT-F | Functional Assessment of Chronic Illness Therapy-Fatigue Scale |
| FSS | Fatigue Severity Scale |
| HADS | Hospital Anxiety and Depression Scale |
| HRQoL | Health-Related Quality of Life |
| IL-1Ra | Interleukin 1 Receptor Antagonist |
| IL-6 | Interleukin 6 |
| LEDD | Levodopa Equivalent Daily Dose |
| MAO | Monoamine Oxidase |
| MoCA | Montreal Cognitive Assessment |
| NMSS | Non-Motor Symptoms Scale |
| PFS | Parkinson's Disease Fatigue Scale |
| PD | Parkinson's Disease |
| REM | Rapid Eye Movement |
| RBD | REM Sleep Behavior Disorder |
| SNpc | Substantia Nigra pars compacta |
| TLR4 | Toll-Like Receptor 4 |
| TNF-α | Tumor Necrosis Factor-alpha |
| VCAM-1 | Vascular Cell Adhesion Molecule 1 |
References
- Hindeya Gebreyesus, H.; Gebrehiwot Gebremichael, T. The Potential Role of Astrocytes in Parkinson’s Disease (PD). Med Sci (Basel) 2020, 8. [Google Scholar] [CrossRef]
- Garcia Ruiz, P.J.; Catalán, M.J.; Fernández Carril, J.M. Initial Motor Symptoms of Parkinson Disease. Neurologist 2011, 17, S18–20. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; Pollina, D.A. Mechanisms and Management of Fatigue in Progressive Neurological Disorders. Curr Opin Neurol 1996, 9, 456–460. [Google Scholar] [CrossRef]
- Sauerbier, A.; Jenner, P.; Todorova, A.; Chaudhuri, K.R. Non Motor Subtypes and Parkinson’s Disease. Parkinsonism Relat Disord 2016, 22 Suppl 1, S41–46. [Google Scholar] [CrossRef]
- Siciliano, M.; Trojano, L.; Santangelo, G.; De Micco, R.; Tedeschi, G.; Tessitore, A. Fatigue in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Mov Disord 2018, 33, 1712–1723. [Google Scholar] [CrossRef]
- Kluger, B.M.; Herlofson, K.; Chou, K.L.; Lou, J.-S.; Goetz, C.G.; Lang, A.E.; Weintraub, D.; Friedman, J. Parkinson’s Disease-Related Fatigue: A Case Definition and Recommendations for Clinical Research. Mov Disord 2016, 31, 625–631. [Google Scholar] [CrossRef]
- Prakash, K.M.; Nadkarni, N.V.; Lye, W.-K.; Yong, M.-H.; Tan, E.-K. The Impact of Non-Motor Symptoms on the Quality of Life of Parkinson’s Disease Patients: A Longitudinal Study. Eur J Neurol 2016, 23, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.H.; Friedman, H. Fatigue in Parkinson’s Disease: A Nine-Year Follow-Up. Mov Disord 2001, 16, 1120–1122. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.-Y.; Zhang, J.-R.; Shen, Y.; Mao, C.-J.; Shen, Y.-B.; Cao, Y.-L.; Gu, H.-Y.; Wang, F.; Liu, C.-F. Fatigue Correlates with Sleep Disturbances in Parkinson Disease. Chin Med J (Engl) 2020, 134, 668–674. [Google Scholar] [CrossRef]
- Metta, V.; Logishetty, K.; Martinez-Martin, P.; Gage, H.M.; Schartau, P.E.S.; Kaluarachchi, T.K.; Martin, A.; Odin, P.; Barone, P.; Stocchi, F.; et al. The Possible Clinical Predictors of Fatigue in Parkinson’s Disease: A Study of 135 Patients as Part of International Nonmotor Scale Validation Project. Parkinsons Dis 2011, 2011, 125271. [Google Scholar] [CrossRef]
- Siciliano, M.; Trojano, L.; De Micco, R.; De Mase, A.; Garramone, F.; Russo, A.; Tedeschi, G.; Tessitore, A. Motor, Behavioural, and Cognitive Correlates of Fatigue in Early, de Novo Parkinson Disease Patients. Parkinsonism Relat Disord 2017, 45, 63–68. [Google Scholar] [CrossRef]
- Lou, J.-S.; Kearns, G.; Benice, T.; Oken, B.; Sexton, G.; Nutt, J. Levodopa Improves Physical Fatigue in Parkinson’s Disease: A Double-Blind, Placebo-Controlled, Crossover Study. Mov Disord 2003, 18, 1108–1114. [Google Scholar] [CrossRef]
- Gołąb-Janowska, M.; Kotlęga, D.; Safranow, K.; Meller, A.; Budzianowska, A.; Honczarenko, K. Risk Factors of Fatigue in Idiopathic Parkinson’s Disease in a Polish Population. Parkinsons Dis 2016, 2016, 2835945. [Google Scholar] [CrossRef] [PubMed]
- Bruno, A.E.; Sethares, K.A. Fatigue in Parkinson Disease: An Integrative Review. J Neurosci Nurs 2015, 47, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Chou, K.L.; Gilman, S.; Bohnen, N.I. Association between Autonomic Dysfunction and Fatigue in Parkinson Disease. J Neurol Sci 2017, 377, 190–192. [Google Scholar] [CrossRef] [PubMed]
- Kluger, B.M.; Krupp, L.B.; Enoka, R.M. Fatigue and Fatigability in Neurologic Illnesses: Proposal for a Unified Taxonomy. Neurology 2013, 80, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Finsterer, J.; Mahjoub, S.Z. Fatigue in Healthy and Diseased Individuals. Am J Hosp Palliat Care 2014, 31, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, A.; Behan, P.O. Fatigue and Basal Ganglia. J Neurol Sci 2000, 179, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Lou, J.S.; Kearns, G.; Oken, B.; Sexton, G.; Nutt, J. Exacerbated Physical Fatigue and Mental Fatigue in Parkinson’s Disease. Mov Disord 2001, 16, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.H.; Beck, J.C.; Chou, K.L.; Clark, G.; Fagundes, C.P.; Goetz, C.G.; Herlofson, K.; Kluger, B.; Krupp, L.B.; Lang, A.E.; et al. Fatigue in Parkinson’s Disease: Report from a Mutidisciplinary Symposium. NPJ Parkinsons Dis 2016, 2, 15025. [Google Scholar] [CrossRef] [PubMed]
- Havlikova, E.; Rosenberger, J.; Nagyova, I.; Middel, B.; Dubayova, T.; Gdovinova, Z.; W Groothoff, J.; P van Dijk, J. Clinical and Psychosocial Factors Associated with Fatigue in Patients with Parkinson’s Disease. Parkinsonism Relat Disord 2008, 14, 187–192. [Google Scholar] [CrossRef]
- Skorvanek, M.; Nagyova, I.; Rosenberger, J.; Krokavcova, M.; Ghorbani Saeedian, R.; Groothoff, J.W.; Gdovinova, Z.; van Dijk, J.P. Clinical Determinants of Primary and Secondary Fatigue in Patients with Parkinson’s Disease. J Neurol 2013, 260, 1554–1561. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Wang, W.-S.; Lewis, S.J.G.; Wu, S.-L. Fighting Against the Clock: Circadian Disruption and Parkinson’s Disease. J Mov Disord 2024, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Antonini, A.; Barone, P.; Marconi, R.; Morgante, L.; Zappulla, S.; Pontieri, F.E.; Ramat, S.; Ceravolo, M.G.; Meco, G.; Cicarelli, G.; et al. The Progression of Non-Motor Symptoms in Parkinson’s Disease and Their Contribution to Motor Disability and Quality of Life. J Neurol 2012, 259, 2621–2631. [Google Scholar] [CrossRef] [PubMed]
- Diaconu, S.; Monescu, V.; Filip, R.; Marian, L.; Kakucs, C.; Murasan, I.; Chaudhuri, K.R.; Jianu, D.C.; Falup-Pecurariu, C.; Opritoiu, B. The Impact of Fatigue on Sleep and Other Non-Motor Symptoms in Parkinson’s Disease. Brain Sci 2024, 14. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.-Y.; Sun, L.; Liu, Z.; Huang, X.-Y.; Zuo, L.-J.; Cao, C.-J.; Zhang, W.; Wang, X.-M. Sleep Disorders in Parkinson’s Disease: Clinical Features, Iron Metabolism and Related Mechanism. PLoS One 2013, 8, e82924. [Google Scholar] [CrossRef]
- Maestri, M.; Romigi, A.; Schirru, A.; Fabbrini, M.; Gori, S.; Bonuccelli, U.; Bonanni, E. Excessive Daytime Sleepiness and Fatigue in Neurological Disorders. Sleep Breath 2020, 24, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Vallone, D.; Picetti, R.; Borrelli, E. Structure and Function of Dopamine Receptors. Neuroscience & biobehavioral reviews 2000, 24, 125–132. [Google Scholar]
- Rascol, O.; Fitzer-Attas, C.J.; Hauser, R.; Jankovic, J.; Lang, A.; Langston, J.W.; Melamed, E.; Poewe, W.; Stocchi, F.; Tolosa, E.; et al. A Double-Blind, Delayed-Start Trial of Rasagiline in Parkinson’s Disease (the ADAGIO Study): Prespecified and Post-Hoc Analyses of the Need for Additional Therapies, Changes in UPDRS Scores, and Non-Motor Outcomes. Lancet Neurol 2011, 10, 415–423. [Google Scholar] [CrossRef]
- Stocchi, F. Benefits of Treatment with Rasagiline for Fatigue Symptoms in Patients with Early Parkinson’s Disease. Eur J Neurol 2014, 21, 357–360. [Google Scholar] [CrossRef]
- Mendonça, D.A.; Menezes, K.; Jog, M.S. Methylphenidate Improves Fatigue Scores in Parkinson Disease: A Randomized Controlled Trial. Mov Disord 2007, 22, 2070–2076. [Google Scholar] [CrossRef] [PubMed]
- Hwang, W.J.; Lin, T.S. Evaluation of Fatigue in Parkinson’s Disease Patients with Stimulated Single Fiber Electromyography. Acta Neurol Scand 2001, 104, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Oved, D.; Ziv, I.; Treves, T.A.; Paleacu, D.; Melamed, E.; Djaldetti, R. Effect of Dopamine Agonists on Fatigue and Somnolence in Parkinson’s Disease. Mov Disord 2006, 21, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Folkerts, A.-K.; Nielsen, J.; Gollan, R.; Lansu, A.; Solfronk, D.; Monsef, I.; Ernst, M.; Skoetz, N.; Zeuner, K.E.; Kalbe, E. Physical Exercise as a Potential Treatment for Fatigue in Parkinson’s Disease? A Systematic Review and Meta-Analysis of Pharmacological and Non-Pharmacological Interventions. J Parkinsons Dis 2023, 13, 659–679. [Google Scholar] [CrossRef] [PubMed]
- Pardini, M.; Bonzano, L.; Mancardi, G.L.; Roccatagliata, L. Frontal Networks Play a Role in Fatigue Perception in Multiple Sclerosis. Behav Neurosci 2010, 124, 329–336. [Google Scholar] [CrossRef]
- Tang, W.K.; Chen, Y.K.; Mok, V.; Chu, W.C.W.; Ungvari, G.S.; Ahuja, A.T.; Wong, K.S. Acute Basal Ganglia Infarcts in Poststroke Fatigue: An MRI Study. J Neurol 2010, 257, 178–182. [Google Scholar] [CrossRef]
- Abe, K.; Takanashi, M.; Yanagihara, T. Fatigue in Patients with Parkinson’s Disease. Behav Neurol 2000, 12, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Meeusen, R.; Watson, P.; Hasegawa, H.; Roelands, B.; Piacentini, M.F. Central Fatigue: The Serotonin Hypothesis and Beyond. Sports Med 2006, 36, 881–909. [Google Scholar] [CrossRef] [PubMed]
- Hornung, J.-P. The Human Raphe Nuclei and the Serotonergic System. J Chem Neuroanat 2003, 26, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Pavese, N.; Metta, V.; Bose, S.K.; Chaudhuri, K.R.; Brooks, D.J. Fatigue in Parkinson’s Disease Is Linked to Striatal and Limbic Serotonergic Dysfunction. Brain 2010, 133, 3434–3443. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Ouchi, Y.; Onoe, H.; Yoshikawa, E.; Tsukada, H.; Takahashi, H.; Iwase, M.; Yamaguti, K.; Kuratsune, H.; Watanabe, Y. Reduction of Serotonin Transporters of Patients with Chronic Fatigue Syndrome. Neuroreport 2004, 15, 2571–2574. [Google Scholar] [CrossRef]
- Pauletti, C.; Mannarelli, D.; Locuratolo, N.; Maffucci, A.; Currà, A.; Marinelli, L.; Fattapposta, F. Serotonergic Central Tone in Parkinson’s Disease with Fatigue: Evidence from the Loudness Dependence of Auditory Evoked Potentials (LDAEP). Neurosci Lett 2021, 764, 136242. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Lang, A.E.; Munhoz, R.P.; Charland, K.; Pelletier, A.; Moscovich, M.; Filla, L.; Zanatta, D.; Rios Romenets, S.; Altman, R.; et al. Caffeine for Treatment of Parkinson Disease: A Randomized Controlled Trial. Neurology 2012, 79, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Pagonabarraga, J.; Tinazzi, M.; Caccia, C.; Jost, W.H. The Role of Glutamatergic Neurotransmission in the Motor and Non-Motor Symptoms in Parkinson’s Disease: Clinical Cases and a Review of the Literature. J Clin Neurosci 2021, 90, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Versace, V.; Sebastianelli, L.; Ferrazzoli, D.; Romanello, R.; Ortelli, P.; Saltuari, L.; D’Acunto, A.; Porrazzini, F.; Ajello, V.; Oliviero, A.; et al. Intracortical GABAergic Dysfunction in Patients with Fatigue and Dysexecutive Syndrome after COVID-19. Clin Neurophysiol 2021, 132, 1138–1143. [Google Scholar] [CrossRef]
- Sanjari Moghaddam, H.; Valitabar, Z.; Ashraf-Ganjouei, A.; Mojtahed Zadeh, M.; Ghazi Sherbaf, F.; Aarabi, M.H. Cerebrospinal Fluid C-Reactive Protein in Parkinson’s Disease: Associations with Motor and Non-Motor Symptoms. Neuromolecular Med 2018, 20, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Katarina, V.; Gordana, T.; Svetlana, M.D.; Milica, B. Oxidative Stress and Neuroinflammation Should Be Both Considered in the Occurrence of Fatigue and Depression in Multiple Sclerosis. Acta Neurol Belg 2020, 120, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Prell, T.; Witte, O.W.; Grosskreutz, J. Biomarkers for Dementia, Fatigue, and Depression in Parkinson’s Disease. Front Neurol 2019, 10, 195. [Google Scholar] [CrossRef]
- Lindqvist, D.; Hall, S.; Surova, Y.; Nielsen, H.M.; Janelidze, S.; Brundin, L.; Hansson, O. Cerebrospinal Fluid Inflammatory Markers in Parkinson’s Disease--Associations with Depression, Fatigue, and Cognitive Impairment. Brain Behav Immun 2013, 33, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.R.; Santos, L.V.D.; Santos, R.M.S.; Campos, A.L.F.; Pimenta, A.L.; de Oliveira, M.S.; Bacheti, G.G.; Rocha, N.P.; Teixeira, A.L.; Christo, P.P.; et al. IL-6 Serum Levels Are Elevated in Parkinson’s Disease Patients with Fatigue Compared to Patients without Fatigue. J Neurol Sci 2016, 370, 153–156. [Google Scholar] [CrossRef]
- Wang, L.; Yi, H.; Liang, X.; Xu, F.; Li, T.; Yang, X.; Wei, M.; Ou, Z.; Tong, Q. Plasma TNF-α and Phosphorylated α-Syn Are Associated with Fatigue in Patients with Parkinson’s Disease. J Neuroimmunol 2023, 385, 578222. [Google Scholar] [CrossRef]
- Tansey, M.G.; McCoy, M.K.; Frank-Cannon, T.C. Neuroinflammatory Mechanisms in Parkinson’s Disease: Potential Environmental Triggers, Pathways, and Targets for Early Therapeutic Intervention. Exp Neurol 2007, 208, 1–25. [Google Scholar] [CrossRef]
- Wang, H.; Liu, Y.; Zhao, J.; Guo, X.; Hu, M.; Chen, Y. Possible Inflammatory Mechanisms and Predictors of Parkinson’s Disease Patients with Fatigue (Brief Review). Clin Neurol Neurosurg 2021, 208, 106844. [Google Scholar] [CrossRef] [PubMed]
- McNeill, A.; Duran, R.; Hughes, D.A.; Mehta, A.; Schapira, A.H.V. A Clinical and Family History Study of Parkinson’s Disease in Heterozygous Glucocerebrosidase Mutation Carriers. J Neurol Neurosurg Psychiatry 2012, 83, 853–854. [Google Scholar] [CrossRef]
- Grabowski, G.A.; Zimran, A.; Ida, H. Gaucher Disease Types 1 and 3: Phenotypic Characterization of Large Populations from the ICGG Gaucher Registry. Am J Hematol 2015, 90 Suppl 1, S12–18. [Google Scholar] [CrossRef]
- Kim, J.-M.; Lee, J.-Y.; Kim, H.J.; Kim, J.S.; Shin, E.-S.; Cho, J.-H.; Park, S.S.; Jeon, B.S. The LRRK2 G2385R Variant Is a Risk Factor for Sporadic Parkinson’s Disease in the Korean Population. Parkinsonism Relat Disord 2010, 16, 85–88. [Google Scholar] [CrossRef]
- Fu, R.; Cui, S.-S.; Du, J.-J.; He, Y.-C.; Gao, C.; Huang, P.; Qian, Y.-W.; Luo, X.-G.; Chen, S.-D. Fatigue Correlates with LRRK2 G2385R Variant in Chinese Parkinson’s Disease Patients. Parkinsonism Relat Disord 2017, 44, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Wang, H.; Yuan, Y.; Fan, S.; Li, L.; Jiang, C.; Mao, C.; Shi, C.; Xu, Y. Peripheral Synucleinopathy in Parkinson Disease with LRRK2 G2385R Variants. Ann Clin Transl Neurol 2021, 8, 592–602. [Google Scholar] [CrossRef] [PubMed]
- van der Merwe, C.; Loos, B.; Swart, C.; Kinnear, C.; Henning, F.; van der Merwe, L.; Pillay, K.; Muller, N.; Zaharie, D.; Engelbrecht, L.; et al. Mitochondrial Impairment Observed in Fibroblasts from South African Parkinson’s Disease Patients with Parkin Mutations. Biochem Biophys Res Commun 2014, 447, 334–340. [Google Scholar] [CrossRef]
- Ross, O.A.; Braithwaite, A.T.; Skipper, L.M.; Kachergus, J.; Hulihan, M.M.; Middleton, F.A.; Nishioka, K.; Fuchs, J.; Gasser, T.; Maraganore, D.M.; et al. Genomic Investigation of Alpha-Synuclein Multiplication and Parkinsonism. Ann Neurol 2008, 63, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Forloni, G. Alpha Synuclein: Neurodegeneration and Inflammation. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Zuo, L.J.; Yu, S.Y.; Wang, F.; Hu, Y.; Piao, Y.S.; Du, Y.; Lian, T.H.; Wang, R.D.; Yu, Q.J.; Wang, Y.J.; et al. Parkinson’s Disease with Fatigue: Clinical Characteristics and Potential Mechanisms Relevant to α-Synuclein Oligomer. J Clin Neurol 2016, 12, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, A.; Behan, P.O. Fatigue in Neurological Disorders. Lancet 2004, 363, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, M.; Kümpfel, T.; Flachenecker, P.; Uhr, M.; Trenkwalder, C.; Holsboer, F.; Weber, F. Fatigue and Regulation of the Hypothalamo-Pituitary-Adrenal Axis in Multiple Sclerosis. Arch Neurol 2005, 62, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, S.; Boegershausen, N.; Meyer, S.; Ivan, D.; Schepelmann, K.; Kann, P.H. Hypothalamic-Pituitary Insufficiency Following Infectious Diseases of the Central Nervous System. Eur J Endocrinol 2008, 158, 3–9. [Google Scholar] [CrossRef]
- Kenangil, G.; Orken, D.N.; Ur, E.; Forta, H.; Celik, M. The Relation of Testosterone Levels with Fatigue and Apathy in Parkinson’s Disease. Clin Neurol Neurosurg 2009, 111, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Stevens-Lapsley, J.; Kluger, B.M.; Schenkman, M. Quadriceps Muscle Weakness, Activation Deficits, and Fatigue with Parkinson Disease. Neurorehabil Neural Repair 2012, 26, 533–541. [Google Scholar] [CrossRef]
- Khalil, I.; Sayad, R.; Kedwany, A.M.; Sayed, H.H.; Caprara, A.L.F.; Rissardo, J.P. Cardiovascular Dysautonomia and Cognitive Impairment in Parkinson’s Disease (Review). Med Int (Lond) 2024, 4, 70. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Shawky, O.A.; Kamel, N.F.; Rothwell, J.C.; Ahmed, M.A.; Hamdy, A. Dopamine Release after Repetitive Transcranial Magnetic Stimulation of Motor Cortex in Parkinson’s Disease Patients. Egypt J Neurol Psychiat Neurosurg 2007, 44, 323–331. [Google Scholar]
- Pitton Rissardo, J.; Fornari Caprara, A.L. Cardiac 123I-Metaiodobenzylguanidine (MIBG) Scintigraphy in Parkinson’s Disease: A Comprehensive Review. Brain Sci 2023, 13. [Google Scholar] [CrossRef]
- Souza, B.R.A.; Nóbrega, K.C.C.; Silva, B.E. de A. da; Gonçalves, R.A.; Martins, T.S.; Santos, G.F.; Frazão, A.H.; Roque, A.C.; Nascimento, I.A.P. da S.; Piemonte, M.E.P. The Impact of Motor, Non-Motor, and Social Aspects on the Sexual Health of Men Living with Parkinson’s Disease. J Parkinsons Dis 2024, 14, 565–574. [Google Scholar] [CrossRef]
- Minibajeva, O.; Zeltiņa, E.; Karelis, G.; Kurjāne, N.; Ķēniņa, V. Clinical Symptoms Influencing Parkinson’s Patients’ Quality of Life in Latvia: A Single-Center Cohort Study. Medicina (Kaunas) 2023, 59. [Google Scholar] [CrossRef]
- Zhou, X.; Xiang, Y.; Song, T.; Zhao, Y.; Pan, H.; Xu, Q.; Chen, Y.; Sun, Q.; Wu, X.; Yan, X.; et al. Characteristics of Fatigue in Parkinson’s Disease: A Longitudinal Cohort Study. Front Aging Neurosci 2023, 15, 1133705. [Google Scholar] [CrossRef]
- Nassif, D.V.; Pereira, J.S. Fatigue in Brazilian Patients with Parkinson’s Disease. Dement Neuropsychol 2022, 16, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Güler, S.; Caylan, A.; Turan, F.N.; Dağdeviren, N. Prevalence and Clinical Features of Idiopathic Parkinson’s Disease in Western Turkey. Noro Psikiyatr Ars 2022, 59, 98–104. [Google Scholar] [CrossRef]
- Ineichen, C.; Baumann-Vogel, H. Deconstructing Apathy in Parkinson’s Disease: Challenges in Isolating Core Components of Apathy From Depression, Anxiety, and Fatigue. Front Neurol 2021, 12, 720921. [Google Scholar] [CrossRef] [PubMed]
- Siciliano, M.; Trojano, L.; De Micco, R.; Giordano, A.; Russo, A.; Tedeschi, G.; Chiorri, C.; Tessitore, A. Predictors of Fatigue Severity in Early, de Novo Parkinson Disease Patients: A 1-Year Longitudinal Study. Parkinsonism Relat Disord 2020, 79, 3–8. [Google Scholar] [CrossRef]
- Fu, R.; Luo, X.-G.; Ren, Y.; He, Z.-Y.; Lv, H. Clinical Characteristics of Fatigued Parkinson’s Patients and the Response to Dopaminergic Treatment. Transl Neurodegener 2016, 5, 9. [Google Scholar] [CrossRef]
- Mukadam, N.; Kinger, S.B.; Neargarder, S.; Salazar, R.D.; McDowell, C.P.; Wall, J.; Kaplan, R.I.; Cronin-Golomb, A. Changes in Subjective Cognitive and Social Functioning in Parkinson’s Disease from Before to During the COVID-19 Pandemic. Healthcare (Basel) 2025, 13. [Google Scholar] [CrossRef]
- Brown, R.G.; Dittner, A.; Findley, L.; Wessely, S.C. The Parkinson Fatigue Scale. Parkinsonism Relat Disord 2005, 11, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Pont-Sunyer, C.; Hotter, A.; Gaig, C.; Seppi, K.; Compta, Y.; Katzenschlager, R.; Mas, N.; Hofeneder, D.; Brücke, T.; Bayés, A.; et al. The Onset of Nonmotor Symptoms in Parkinson’s Disease (the ONSET PD Study). Mov Disord 2015, 30, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Schrag, A.; Horsfall, L.; Walters, K.; Noyce, A.; Petersen, I. Prediagnostic Presentations of Parkinson’s Disease in Primary Care: A Case-Control Study. Lancet Neurol 2015, 14, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Müller, B.; Assmus, J.; Herlofson, K.; Larsen, J.P.; Tysnes, O.-B. Importance of Motor vs. Non-Motor Symptoms for Health-Related Quality of Life in Early Parkinson’s Disease. Parkinsonism Relat Disord 2013, 19, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Miwa, H.; Miwa, T. Fatigue in Patients with Parkinson’s Disease: Impact on Quality of Life. Intern Med 2011, 50, 1553–1558. [Google Scholar] [CrossRef]
- Friedman, J.H.; Abrantes, A.; Sweet, L.H. Fatigue in Parkinson’s Disease. Expert Opin Pharmacother 2011, 12, 1999–2007. [Google Scholar] [CrossRef] [PubMed]
- Luo, R.; Qi, Y.; He, J.; Zheng, X.; Ren, W.; Chang, Y. Analysis of Influencing Factors of Apathy in Patients with Parkinson’s Disease. Brain Sci 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Kluger, B.M. Fatigue in Parkinson’s Disease. Int Rev Neurobiol 2017, 133, 743–768. [Google Scholar] [CrossRef]
- Zesiewicz, T.A.; Patel-Larson, A.; Hauser, R.A.; Sullivan, K.L. Social Security Disability Insurance (SSDI) in Parkinson’s Disease. Disabil Rehabil 2007, 29, 1934–1936. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, G.D.; Rizvi, S.; Abrantes, A.M.; Crabtree, B.; Cahill, J.; Friedman, J.H. The Association between Fatigue and Apathy in Patients with Either Parkinson’s Disease or Multiple Sclerosis. Parkinsonism Relat Disord 2015, 21, 1093–1095. [Google Scholar] [CrossRef]
- Elbers, R.G.; van Wegen, E.E.; Verhoef, J.; Kwakkel, G. Impact of Fatigue on Health-Related Quality of Life in Patients with Parkinson’s Disease: A Prospective Study. Clin Rehabil 2014, 28, 300–311. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Guo, X.; Chen, K.; Chen, X.; Cao, B.; Wei, Q.; Huang, R.; Zhao, B.; Wu, Y.; Shang, H.-F. The Impact of Non-Motor Symptoms on the Health-Related Quality of Life of Parkinson’s Disease Patients from Southwest China. Parkinsonism Relat Disord 2014, 20, 149–152. [Google Scholar] [CrossRef]
- Dogan, V.B.; Koksal, A.; Dirican, A.; Baybas, S.; Dirican, A.; Dogan, G.B. Independent Effect of Fatigue on Health-Related Quality of Life in Patients with Idiopathic Parkinson’s Disease. Neurol Sci 2015, 36, 2221–2226. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.; Friedman, H. Fatigue in Parkinson’s Disease. Neurology 1993, 43, 2016–2018. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The Fatigue Severity Scale. Application to Patients with Multiple Sclerosis and Systemic Lupus Erythematosus. Arch Neurol 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.E.; Jandorf, L.; Krupp, L.B. The Measurement of Fatigue: A New Instrument. J Psychosom Res 1993, 37, 753–762. [Google Scholar] [CrossRef]
- Schiehser, D.M.; Ayers, C.R.; Liu, L.; Lessig, S.; Song, D.S.; Filoteo, J.V. Validation of the Modified Fatigue Impact Scale in Parkinson’s Disease. Parkinsonism Relat Disord 2013, 19, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martin, P.; Catalan, M.J.; Benito-Leon, J.; Moreno, A.O.; Zamarbide, I.; Cubo, E.; van Blercon, N.; Arillo, V.C.; Pondal, M.; Linazasoro, G.; et al. Impact of Fatigue in Parkinson’s Disease: The Fatigue Impact Scale for Daily Use (D-FIS). Qual Life Res 2006, 15, 597–606. [Google Scholar] [CrossRef]
- Hagell, P.; Höglund, A.; Reimer, J.; Eriksson, B.; Knutsson, I.; Widner, H.; Cella, D. Measuring Fatigue in Parkinson’s Disease: A Psychometric Study of Two Brief Generic Fatigue Questionnaires. J Pain Symptom Manage 2006, 32, 420–432. [Google Scholar] [CrossRef]
- Pitton Rissardo, J.; Fornari Caprara, A.L. Parkinson’s Disease Rating Scales: A Literature Review. Annals of Movement Disorders 2020, 3. [Google Scholar] [CrossRef]
- Huether, A.X.A.; Pottinger, T.; Lou, J.-S. Screening Cut-off Scores for Clinically Significant Fatigue in Early Parkinson’s Disease. Clin Park Relat Disord 2023, 9, 100228. [Google Scholar] [CrossRef] [PubMed]
- Niimi, Y.; Shima, S.; Mizutani, Y.; Ueda, A.; Ito, S.; Mutoh, T. Fatigue Evaluated Using the 16-Item Parkinson Fatigue Scale (PFS-16) Predicts Parkinson’s Disease Prognosis. Fujita Med J 2019, 5, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Chong, R.; Albor, L.; Wakade, C.; Morgan, J. The Dimensionality of Fatigue in Parkinson’s Disease. J Transl Med 2018, 16, 192. [Google Scholar] [CrossRef]
- Panigrahi, B.; Pillai, K.S.; Radhakrishnan, D.M.; Rajan, R.; Srivastava, A.K. Fatigue in Parkinson’s Disease—A Narrative Review. Annals of Movement Disorders 2024, 7, 157–171. [Google Scholar] [CrossRef]
- Sáez-Francàs, N.; Hernández-Vara, J.; Corominas Roso, M.; Alegre Martín, J.; Casas Brugué, M. The Association of Apathy with Central Fatigue Perception in Patients with Parkinson’s Disease. Behav Neurosci 2013, 127, 237–244. [Google Scholar] [CrossRef]
- Hagell, P.; Brundin, L. Towards an Understanding of Fatigue in Parkinson Disease. J Neurol Neurosurg Psychiatry 2009, 80, 489–492. [Google Scholar] [CrossRef]
- Spirgi, S.; Meyer, A.; Calabrese, P.; Gschwandtner, U.; Fuhr, P. Effects of Cognitive Performance and Affective Status on Fatigue in Parkinson’s Disease. Dement Geriatr Cogn Dis Extra 2019, 9, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Lin, I.; Edison, B.; Mantri, S.; Albert, S.; Daeschler, M.; Kopil, C.; Marras, C.; Chahine, L.M. Triggers and Alleviating Factors for Fatigue in Parkinson’s Disease. PLoS One 2021, 16, e0245285. [Google Scholar] [CrossRef]
- Okuma, Y.; Kamei, S.; Morita, A.; Yoshii, F.; Yamamoto, T.; Hashimoto, S.; Utsumi, H.; Hatano, T.; Hattori, N.; Matsumura, M.; et al. Fatigue in Japanese Patients with Parkinson’s Disease: A Study Using Parkinson Fatigue Scale. Mov Disord 2009, 24, 1977–1983. [Google Scholar] [CrossRef] [PubMed]
- Koh, M.R.E.; Chua, C.Y.; Ng, S.Y.-E.; Chia, N.S.-Y.; Saffari, S.E.; Chen, R.Y.-Y.; Choi, X.; Heng, D.L.; Neo, S.X.; Tay, K.Y.; et al. Poor Sleep Quality Is Associated with Fatigue and Depression in Early Parkinson’s Disease: A Longitudinal Study in the PALS Cohort. Front Neurol 2022, 13, 998103. [Google Scholar] [CrossRef]
- Junho, B.T.; Kummer, A.; Cardoso, F.E.; Teixeira, A.L.; Rocha, N.P. Sleep Quality Is Associated with the Severity of Clinical Symptoms in Parkinson’s Disease. Acta Neurol Belg 2018, 118, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Solla, P.; Cannas, A.; Mulas, C.S.; Perra, S.; Corona, A.; Bassareo, P.P.; Marrosu, F. Association between Fatigue and Other Motor and Non-Motor Symptoms in Parkinson’s Disease Patients. J Neurol 2014, 261, 382–391. [Google Scholar] [CrossRef]
- Kwon, K.-Y.; Joo, B.-E.; You, J.; Kim, R.O. Impact of Motor Features on Non-Motor Symptoms in Patients with de Novo Parkinson’s Disease: Cognition, Depression, Anxiety, Fatigue, and Dysautonomia. Geriatr Gerontol Int 2025. [Google Scholar] [CrossRef] [PubMed]
- Sáez-Francàs, N.; Hernández-Vara, J.; Corominas-Roso, M.; Alegre, J.; Jacas, C.; Casas, M. Relationship between Poor Decision-Making Process and Fatigue Perception in Parkinson’s Disease Patients. J Neurol Sci 2014, 337, 167–172. [Google Scholar] [CrossRef]
- Yu, H.-X.; Guo, M.-R.; Li, G.; Zhang, B. Association between Fatigue and Motor Progression in Parkinson’s Disease in Southern Chinese. Neurol Sci 2020, 41, 161–164. [Google Scholar] [CrossRef]
- Alves, G.; Wentzel-Larsen, T.; Larsen, J.P. Is Fatigue an Independent and Persistent Symptom in Patients with Parkinson Disease? Neurology 2004, 63, 1908–1911. [Google Scholar] [CrossRef] [PubMed]
- Terra, M.B.; Lopes, J.; Bueno, M.E.B.; Trinca, L.A.; Smaili, S.M. Association between Fatigue and MDS-UPDRS in Individuals with Parkinson’s Disease: Cross-Sectional Study. Neurol Sci 2024, 45, 4309–4321. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martin, P.; Falup Pecurariu, C.; Odin, P.; van Hilten, J.J.; Antonini, A.; Rojo-Abuin, J.M.; Borges, V.; Trenkwalder, C.; Aarsland, D.; Brooks, D.J.; et al. Gender-Related Differences in the Burden of Non-Motor Symptoms in Parkinson’s Disease. J Neurol 2012, 259, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Beiske, A.G.; Loge, J.H.; Hjermstad, M.J.; Svensson, E. Fatigue in Parkinson’s Disease: Prevalence and Associated Factors. Mov Disord 2010, 25, 2456–2460. [Google Scholar] [CrossRef] [PubMed]
- Lerdal, A.; Wahl, A.; Rustøen, T.; Hanestad, B.R.; Moum, T. Fatigue in the General Population: A Translation and Test of the Psychometric Properties of the Norwegian Version of the Fatigue Severity Scale. Scand J Public Health 2005, 33, 123–130. [Google Scholar] [CrossRef]
- Ongre, S.O.; Dalen, I.; Tysnes, O.-B.; Alves, G.; Herlofson, K. Progression of Fatigue in Parkinson’s Disease - a 9-Year Follow-Up. Eur J Neurol 2021, 28, 108–116. [Google Scholar] [CrossRef]
- Ou, R.; Hou, Y.; Liu, K.; Lin, J.; Jiang, Z.; Wei, Q.; Zhang, L.; Cao, B.; Zhao, B.; Song, W.; et al. Progression of Fatigue in Early Parkinson’s Disease: A 3-Year Prospective Cohort Study. Front Aging Neurosci 2021, 13, 701906. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, K.; Larsen, J.P.; Tandberg, E.; Jørgensen, K. Fatigue in Patients with Parkinson’s Disease. Mov Disord 1999, 14, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Valko, P.O.; Waldvogel, D.; Weller, M.; Bassetti, C.L.; Held, U.; Baumann, C.R. Fatigue and Excessive Daytime Sleepiness in Idiopathic Parkinson’s Disease Differently Correlate with Motor Symptoms, Depression and Dopaminergic Treatment. Eur J Neurol 2010, 17, 1428–1436. [Google Scholar] [CrossRef]
- Shulman, L.M.; Taback, R.L.; Bean, J.; Weiner, W.J. Comorbidity of the Nonmotor Symptoms of Parkinson’s Disease. Mov Disord 2001, 16, 507–510. [Google Scholar] [CrossRef]
- Ortelli, P.; Versace, V.; Saltuari, L.; Randi, A.; Stolz, J.; Dezi, S.; Maestri, R.; Buechner, S.; Giladi, N.; Oliviero, A.; et al. Looking Deeper: Does a Connection Exist between Fatigue and Attentional Deficits in Parkinson’s Disease? A Conceptual Framework. Front Neurol 2023, 14, 1212876. [Google Scholar] [CrossRef] [PubMed]
- Di Vico, I.A.; Cirillo, G.; Tessitore, A.; Siciliano, M.; Venturelli, M.; Falup-Pecurariu, C.; Tedeschi, G.; Morgante, F.; Tinazzi, M. Fatigue in Hypokinetic, Hyperkinetic, and Functional Movement Disorders. Parkinsonism Relat Disord 2021, 86, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Kluger, B.M.; Parra, V.; Jacobson, C.; Garvan, C.W.; Rodriguez, R.L.; Fernandez, H.H.; Fogel, A.; Skoblar, B.M.; Bowers, D.; Okun, M.S. The Prevalence of Fatigue Following Deep Brain Stimulation Surgery in Parkinson’s Disease and Association with Quality of Life. Parkinsons Dis 2012, 2012, 769506. [Google Scholar] [CrossRef]
- Rissardo, J.P.; Vora, N.M.; Tariq, I.; Mujtaba, A.; Caprara, A.L.F. Deep Brain Stimulation for the Management of Refractory Neurological Disorders: A Comprehensive Review. Medicina (Kaunas) 2023, 59, 1991. [Google Scholar] [CrossRef]
- Lazcano-Ocampo, C.; van Wamelen, D.; Samuel, M.; Silverdale, M.; Rizos, A.; Sauerbier, A.; Koch, J.; Podlewska, A.; Leta, V.; Dafsari, H.S.; et al. Evaluation of the Effect of Bilateral Subthalamic Nucleus Deep Brain Stimulation on Fatigue in Parkinson’s Disease as Measured by the Non-Motor Symptoms Scale. Br J Neurosurg 2024, 38, 712–715. [Google Scholar] [CrossRef]
- Honig, H.; Antonini, A.; Martinez-Martin, P.; Forgacs, I.; Faye, G.C.; Fox, T.; Fox, K.; Mancini, F.; Canesi, M.; Odin, P.; et al. Intrajejunal Levodopa Infusion in Parkinson’s Disease: A Pilot Multicenter Study of Effects on Nonmotor Symptoms and Quality of Life. Mov Disord 2009, 24, 1468–1474. [Google Scholar] [CrossRef]
- Rios Romenets, S.; Creti, L.; Fichten, C.; Bailes, S.; Libman, E.; Pelletier, A.; Postuma, R.B. Doxepin and Cognitive Behavioural Therapy for Insomnia in Patients with Parkinson’s Disease -- a Randomized Study. Parkinsonism Relat Disord 2013, 19, 670–675. [Google Scholar] [CrossRef]
- Kelly, N.A.; Ford, M.P.; Standaert, D.G.; Watts, R.L.; Bickel, C.S.; Moellering, D.R.; Tuggle, S.C.; Williams, J.Y.; Lieb, L.; Windham, S.T.; et al. Novel, High-Intensity Exercise Prescription Improves Muscle Mass, Mitochondrial Function, and Physical Capacity in Individuals with Parkinson’s Disease. J Appl Physiol (1985) 2014, 116, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Uc, E.Y.; Doerschug, K.C.; Magnotta, V.; Dawson, J.D.; Thomsen, T.R.; Kline, J.N.; Rizzo, M.; Newman, S.R.; Mehta, S.; Grabowski, T.J.; et al. Phase I/II Randomized Trial of Aerobic Exercise in Parkinson Disease in a Community Setting. Neurology 2014, 83, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Canning, C.G.; Allen, N.E.; Dean, C.M.; Goh, L.; Fung, V.S.C. Home-Based Treadmill Training for Individuals with Parkinson’s Disease: A Randomized Controlled Pilot Trial. Clin Rehabil 2012, 26, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, J.K.; Andrews, L.A.; Witcraft, S.M.; Powers, M.B.; Smits, J.A.J.; Hofmann, S.G. Cognitive Behavioral Therapy for Anxiety and Related Disorders: A Meta-Analysis of Randomized Placebo-Controlled Trials. Depress Anxiety 2018, 35, 502–514. [Google Scholar] [CrossRef]
- Luo, F.; Ye, M.; Lv, T.; Hu, B.; Chen, J.; Yan, J.; Wang, A.; Chen, F.; He, Z.; Ding, Z.; et al. Efficacy of Cognitive Behavioral Therapy on Mood Disorders, Sleep, Fatigue, and Quality of Life in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Front Psychiatry 2021, 12, 793804. [Google Scholar] [CrossRef] [PubMed]
- Knie, B.; Mitra, M.T.; Logishetty, K.; Chaudhuri, K.R. Excessive Daytime Sleepiness in Patients with Parkinson’s Disease. CNS Drugs 2011, 25, 203–212. [Google Scholar] [CrossRef]
- Wade, R.; Pachana, N.A.; Mellick, G.; Dissanayaka, N. Factors Related to Sleep Disturbances for Individuals with Parkinson’s Disease: A Regional Perspective. Int Psychogeriatr 2020, 32, 827–838. [Google Scholar] [CrossRef]
- Yan, M.; Fan, J.; Liu, X.; Li, Y.; Wang, Y.; Tan, W.; Chen, Y.; He, J.; Zhuang, L. Acupuncture and Sleep Quality Among Patients With Parkinson Disease: A Randomized Clinical Trial. JAMA Netw Open 2024, 7, e2417862. [Google Scholar] [CrossRef]
- Tan, W.; Pan, Z.; He, J.; Wu, T.; Wu, F.; Xu, Y.; Liu, L.; Yang, Z.; Li, C.; Hu, Y.; et al. Traditional Chinese Exercises for the Treatment of Neuropsychiatric Symptoms in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Complement Ther Med 2025, 103134. [Google Scholar] [CrossRef]
- Crichton, A.; Ignjatovic, V.; Babl, F.E.; Oakley, E.; Greenham, M.; Hearps, S.; Delzoppo, C.; Beauchamp, M.H.; Guerguerian, A.-M.; Boutis, K.; et al. Interleukin-8 Predicts Fatigue at 12 Months Post-Injury in Children with Traumatic Brain Injury. J Neurotrauma 2021, 38, 1151–1163. [Google Scholar] [CrossRef] [PubMed]
- Eidem, L.E.; Birkeland, E.; Austdal, M.; Bårdsen, K.; Lange, J.; Alves, G.; Berven, F.; Nilsen, M.M.; Herlofson, K.; Tysnes, O.-B.; et al. Fatigue in Parkinson’s Disease: A Proteomic Study of Cerebrospinal Fluid. Mov Disord 2024, 39, 749–751. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Luo, Y.; Qu, Y.; Wang, C.; Li, Z.; Zhou, J.; Xu, Z. Pharmacological and Behavioral Interventions for Fatigue in Parkinson’s Disease: A Meta-Analysis of Randomized Controlled Trials. J Geriatr Psychiatry Neurol 2023, 36, 487–495. [Google Scholar] [CrossRef]
- Coe, S.; Franssen, M.; Collett, J.; Boyle, D.; Meaney, A.; Chantry, R.; Esser, P.; Izadi, H.; Dawes, H. Physical Activity, Fatigue, and Sleep in People with Parkinson’s Disease: A Secondary per Protocol Analysis from an Intervention Trial. Parkinsons Dis 2018, 2018, 1517807. [Google Scholar] [CrossRef] [PubMed]
- Wasson, E.; Rosso, A.L.; Santanasto, A.J.; Rosano, C.; Butters, M.A.; Rejeski, W.J.; Boudreau, R.M.; Aizenstein, H.; Gmelin, T.; Glynn, N.W. Neural Correlates of Perceived Physical and Mental Fatigability in Older Adults: A Pilot Study. Exp Gerontol 2019, 115, 139–147. [Google Scholar] [CrossRef]

| Criteria | Description |
|---|---|
| A. Symptoms |
1. Symptoms may be induced by routine activities of daily living. 2. Symptoms may occur with little or no exertion. 3. Symptoms limit the type, intensity, or duration of activities performed by the patient. 4. Symptoms are not reliably relieved by rest or may require prolonged periods of rest. 5. Symptoms may be brought on by cognitive tasks or situations requiring sustained attention, including social interactions. 6. Patients avoid rigorous activities because of fear of experiencing worsening of symptoms. 7. Mild to moderate exertion may induce a worsening of symptoms lasting hours to days. 8. Symptoms have a predictable diurnal pattern regardless of activities performed (e.g., worsening in the afternoon). 9. Symptoms are unpredictable and may have a sudden onset. |
| B. Functional Impact | The patient experiences clinically significant distress or impairment in social, occupational, or other important areas of function as a result of fatigue. |
| C. Association with Parkinson’s Disease | There is evidence from the history and physical examination suggesting fatigue is a consequence of PD. |
| D. Exclusion of Other Causes | The symptoms are not primarily a consequence of comorbid psychiatric disorders (e.g., depression), sleep disorders (e.g., obstructive sleep apnea), or medical conditions (e.g., anemia, congestive heart failure). |
| Reference | Sample size | Age (mean) | Sex (Male) | Prevalence of fatigue | Comments |
|---|---|---|---|---|---|
| Siciliano et al. (2017) [11] | 81 consecutive de novo PD patients | 65.73 (SD: 8.26) | 52 | 15%(n=12) of patients reported distressing fatigue (defined as a PFS score ≥ 8) | 15% of patients with early, de novo PD reported distressing fatigue. |
| Friedman et al. (2001) [8] | 26 | NA | NA | At the initial assessment, 42% of the patients reported fatigue as one of their three most disabling symptoms. At the follow-up assessment, 50% of the patients reported fatigue as their most disabling symptom, and 62% reported it as one of their three most disabling symptoms. | Fatigue is a common and often disabling symptom, affecting a significant proportion of PD patients. |
| Diaconu et al. (2024) [25] | 131 PD patients and 131 age- and sex-matched healthy controls | NA | NA | In PD patients: 38.16% reported fatigue based on the Chalder fatigue scale. 46.54% reported fatigue based on the PFS. In healthy controls: 26.71% reported fatigue based on the Chalder fatigue scale. | Highlight the importance of recognizing and addressing fatigue in PD management. |
| Souza et al. (2024) [71] | 80 | 53.55 years (SD: 10.8) | 80 | Mean FSS score was 36.97 ± 16.45, indicating a moderate level of fatigue in the sample | The study focuses on men with PD, a population that is often understudied in terms of sexual health. |
| Minibajeva et al. (2023) [72] | 43 | 65.21 years (SD 8.9) | 20 | 95.3% | Non-motor symptoms, which are often overlooked but significantly impact the quality of life of PD patients |
| Zhou et al. (2023) [73] | 2100 | 60.47 years | 1048 | 36.8% | Routinely assess for fatigue in PD patients. Fatigue is associated with increased disease severity and progression. Clinicians should consider the potential impact of fatigue on quality of life when managing PD patients. |
| Nassif et al. (2022) [74] | 53 | Non-fatigued group: 64.75 years (SD: 7.23). Fatigued group: 65.71 years (SD: 8.72) | Non-fatigued group: 68.75%. Fatigued group: 66.67%. | 39.62% | High prevalence of fatigue (39.62%) in PD patients, which is consistent with other studies. The study found that fatigue was associated with worse quality of life, which is an important finding. |
| Güler et al. (2022) [75] | 9887 (118 with IPD (idiopathic PD)) | 78.6 years | 58.4% of the PD patients were male | 46.8% | In this study, all the numbers are for the 188 patients with IPD |
| Ineichen et al. (2021) [76] | 337 | 69.3 | 38.3% | Significant fatigue (FSS total score ≥ 4): 40.3%. Severe fatigue (FSS total score ≥ 5): 17.8% | |
| Siciliano et al. (2020) [77] | 55 | 64.7 | NA | At baseline: 22% using the Parkinson Fatigue Scale (PFS) cut-off. At 1-year follow-up: 38% using the PFS cut-off. | Fatigue affected 22% of the population at baseline, and increasing over time to 38% at 1-year follow-up. |
| Siciliano et al. (2018) [5] | 7427 | NA | NA | 50% | Systematic review and meta-analysis |
| Fu et al. (2016) [78] | 222 | NA | NA | 59.46% | Fatigue is influenced by multiple factors beyond motor symptoms. While dopaminergic treatment can be beneficial for some patients, addressing sleep disturbances and depression may be crucial for effectively managing fatigue in PD. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



