
Submitted:
24 January 2025
Posted:
27 January 2025
You are already at the latest version
Abstract
Introduction: Spigelian hernia (SH) is an aponeurotic defect, either acquired or congenital, in Spiegel's semilunar line. SH is exceptional in pediatric patients. Methods: A comprehensive non-systematic review of the previous literature was conducted. Eligible studies were identified by searching the primary existing medical bibliography databases. Median and interquartile range or mean and standard deviation were used to describe quantitative variables and proportions for categorical variables. The Kruskal-Wallis, Mann-Whitney U, and Fisher's exact tests were used to compare group variables. The Spearman, Pearson and Cramér´s V correlation analyses were used to assess the degree of correlation between the study variables. A p-value <0.05 (two tails) was considered statistically significant. Results: Eighty-two publications reporting 123 patients were included. Of these, 105 were male (85.4%). The age range was from 0 to 21 years. Forty-seven patients (38.2%) had a left-sided SH, and 13 (10.6%) had a bilateral SH. Forty-five cases (36.6%) were classified as traumatic, the majority attributable to bicycle-related injuries. Forty-one patients (33.3%) presented with a SH associated with undescended testis (UDT). A peak incidence around 7-9 years was identified for traumatic SH, and a concentration of cases before one year of age for SH associated with UDT. Fifteen patients (12.2%) were reported to have hernia incarceration/strangulation (I/S). These patients were significantly younger than those without I/S (p=0.02), but no gender differences were seen (p=0.63). In 95 patients (77.2%), surgical correction of the defect was reported. Fourteen were approached laparoscopically, with a 35.7% conversion rate. Eight (6.5%) were managed conservatively. Overall, the reported evolution has been favorable. Conclusions: HS is an uncommon condition in pediatric populations, predominantly affecting males. It can present congenitally, with a significant association with ipsilateral UDT, or it can be acquired, typically related to bicycle trauma involving the SL. The risk of incarceration is relatively high, particularly during early childhood. Most reported cases have been treated surgically, with favorable outcomes. Evidence regarding conservative management is limited.
Keywords:
Spigelian hernia
; handlebar hernia
; traumatic abdominal wall hernia
; cryptorchidism
; Spigelian-Cryptorchidism Syndrome
; congenital
Introduction
Abdominal wall hernias are one of the most common pediatric surgical pathologies worldwide. However, the incidence of the different types of hernia are highly variable. While inguinal and umbilical hernias are frequent, other types, such as femoral or Spigelian hernias (SH), are highly infrequent [1].
Anatomy and Embryology of Semilunaris Line (Spigelian Line)
During embryonic development, the primitive mesoderm formed during gastrulation differentiates into the splanchnic mesoderm (which develops into the peritoneum) and the somatic mesoderm (which contributes to the formation of the abdominal wall). Between the fourth and tenth weeks of gestation, myocytes migrate bilaterally from the paravertebral regions to form the muscular and aponeurotic layers of the anterior abdominal wall, completing their fusion and establishing the linea alba by approximately week ten. In the following weeks, these layers gain strength, and the superficial fascia undergoes complete differentiation [6–8]. This process is often associated with congenital points of weakness, such as the linea alba (where epigastric hernias occur) or the umbilicus (where umbilical hernias develop).
The linea semilunaris or Spigelian line (SL) was first described by Adriaan Van Den Spiegel (1578-1625) as the region of the anterior abdominal wall formed by the transition from muscle to aponeurosis of the transversus abdominis muscle of the abdomen. It is a structure located on the lateral margin of the anterior rectus abdominis muscle. It extends from the inferior edge of the costal cartilage (approximately at the ninth rib) to the pubic tubercle, following a curved and descending path along the anterior abdominal wall. It is considered a point of fascial weakness [1–3]. Although SL partially overlaps within the lateral margin of the anterior rectus abdominis muscle, recent studies suggest that the anatomic boundaries of these two structures are different [8].
SL is an infrequent but well-described site where hernias can occur. Hernias that occur along the SL are referred to as SH [4]. These hernias are usually located deep to the external oblique muscle. They are referred to as interparietal hernias (abdominal hernias in which the hernial sac is situated between the layers of the abdominal wall, specifically between the fascias or muscles, rather than completely protruding through them). About pediatric SH, two variants have been described: congenital SH and acquired SH. Figure 1 presents an schematic diagram of the two subtypes of Spigelian hernia (SH) described in the pediatric population (congenital and acquired) and their distinguishing characteristics. The aim of this integrative review is to analyze the existing literature on this condition in the pediatric population to better characterize it in terms of epidemiology, diagnosis, treatment, and prognosis.
Methods
An integrative non-systematic review of the previous literature was conducted. Eligible studies were identified by searching the primary existing medical bibliography databases (PubMed, Web of Science, Scopus, and OVID). Search terms and keywords were: “(Spiegel OR Spigelian OR semilunar OR semilunaris) AND (hernia) AND (cryptorchidism OR undescended testis OR) AND (pediatric OR children OR infant). Supplementary File 1 shows inclusion and exclusion criteria. JAM and MRJ selected articles using the COVIDENCE ® tool. The search results were imported into the platform, and both authors screened the articles separately. Disagreements were resolved by consensus.
Regarding descriptive statistics, median and interquartile range or the mean and standard deviation were used for quantitative variables and proportions for categorical variables. The Kolmogorov-Smirnov test was applied to assess the normality of quantitative variables. Mann-Whitney U, Kruskal-Wallis, and Fisher's exact tests were used to compare sociodemographic and clinical variables between groups. Pearson, Spearman, and Cramér's V correlation analyses were performed to assess the degree of correlation between the study variables. A p-value of <0.05 (two-tailed) was considered statistically significant. All statistical analyses were conducted using STATA 18.0 (StataCorp LLC). Graphical plots were generated using Python (version 3.9). The visualizations were created with the Seaborn library (version 0.11.2) for histograms and kernel density estimates and Matplotlib (version 3.4.3) for plotting. Kernel density plots were generated using default bandwidth parameters, which were adjusted to ensure smoothness in the density curves. Supplementary file 2 includes a database with the main variables analyzed.
Results
Main Characteristics of the Included Studies. Sociodemographic Features of the Patients.
The literature review, covering the PubMed/Medline, Web of Science, Scopus, and OVID databases, identified 82 indexed publications by 79 authors [9–90]. Table 1 summarizes all the published cases of congenital Spigelian hernia (SH) described in the pediatric population to date.
The distribution of publications by country was as follows: USA (n=23), India (n=10), Italy (n=6), Turkey (n=5), Spain (n=4), United Kingdom (n=4), Australia (n=4), Greece (n=3), Israel (n=3), Japan (n=3), New Zealand (n=2), and Saudi Arabia (n=2). Algeria, Ireland, Norway, Germany, Puerto Rico, Canada, Ghana, and Tunisia each contributed one publication. The geographic origin of five publications could not be determined. A total of 123 patients were reported. Of these, 105 were male (85.4%) and 18 were female (14.6%). The age range was from 0 days to 21 years (mean = 5.21, standard deviation = 5.34). Forty-six patients were one year or younger.
Characteristics of the Spigelian Hernia
Forty-seven patients (38.2%) had a left-sided SH, 56 (45.5%) had a right-sided SH, and 13 (10.6%) had a bilateral SH. In seven cases (5.7%) laterality was not explicitly reported. Concerning SH measurements, 55 cases reported numerical values, of which 15 provided two independent values in centimeters (major and minor axes), and 40 provided a single value in centimeters (corresponding to the major axis). A significant heterogeneity was identified in the methodology used to determine the measurements. Some authors utilized radiological or intraoperative measurements of the fascial defect (ring), while others, such as Fraser et al., measured the diameter of the cutaneous bulge [40]. Some authors, such as Vaos et al., Inan et al., and Upasani et al., provided both characterizations, noting a substantially larger size of the cutaneous protrusions compared to the actual size of the fascial defect [44,56,65].On the other hand, some authors, such as Bilici et al. and Okumuş et al. [87], provided a range of measurements for the defect [60,87]. For the statistical analysis of these patients, the central value of the range was used as the imputed value.
For cases reported as a single measurement, the mean (standard deviation) was 3.21 (2.23) cm. For cases reported with two measurements, the values were converted to surface area (cm²), resulting in a mean (standard deviation) of 19.41 (24.37) cm². No statistically significant differences were found in the size of fascial defects between patients with undescended testis (UDT) and those without UDT (p=0.96), nor between patients with traumatic etiology and those without traumatic etiology (p=0.45). No differences in fascial size were observed based on age (Spearman, p=0.93) or sex (p=0.68). Similarly, no statistically significant differences were found concerning laterality (Kruskal Wallis, p=0.65).
Spigelian Hernia Etiology and associations.
Regarding etiology, 45 out of 123 cases (36.6%) were classified as acquired or traumatic. Specifically, 2 cases (1.6%) were caused by unspecified local trauma, 32 cases (26%) by bicycle (n=31) or motorcycle (n=1) handlebar trauma, 2 cases (1.6%) by bicycle falls, 1 case (0.8%) by an ATV accident, 2 cases (1.6%) by BMX accidents, 1 case (0.8%) by a nail puncture, 1 case (0.8%) by cow goring, 2 cases (1.6%) by road or automobile accidents, and 3 cases (2.4%) related to surgical procedures (1 case of Bochdalek hernia associated with intense parietal traction during surgical correction, 1 case of bilateral inguinal herniorrhaphy with hernia detected in the immediate postoperative period, and 1 case of a surgically treated lower mediastinal neuroblastoma). The remaining cases were either congenital or had no attributable etiology described. No statistically significant differences were found between patients with traumatic and non-traumatic SH based on gender (p=0.57).
Forty-one patients (33.3%) presented with a SH associated with UDT. Concerning laterality, 16 (39%) UDT were left-sided, 15 (36.6%) right-sided, and 10 (24.4%) bilateral. Fisher's exact test confirmed a statistically significant association between the side of SH and the side of UDT (p<0.0001). When a Cramér's V analysis was performed between the side of SH and the side of UDT, a very strong association was found (0.83).
Regarding age and the etiology of SH, the mean age of patients with traumatic SH was 9.2 (4) years, while for patients with non-traumatic SH, it was 2.9 (4.6) years (p<0.0001). Similarly, patients with SH and associated UDT had a mean age of 0.7 (1.1) years, compared to a mean age of 7.5 (5.2) years for patients without UDT (p<0.0001).
Histograms and kernel density plots (Figure 2) were used to visually represent both etiologies, highlighting a peak incidence of traumatic SH around 7–9 years and a concentration of SH cases associated with UDT occurring predominantly before one year of age. In this case, the presence of UDT was used as a reference for congenital SH in both epidemiological and analytical terms, although a perfect equivalence can´t be assumed.
Lastly, Table 1 details the associated malformations of patients diagnosed with HS.
Complications Associated with Spigelian Hernia
Fifteen out of 123 patients (12.2%) were reported to have some hernia incarceration or strangulation. These 15 patients were significantly younger than the group of patients without hernia incarceration: 2.7 (4.3) years vs. 5.6 (5.4) years (p=0.02), but no gender differences were seen (p=0.63). Additionally, no differences were found in the hernia incarceration rate between the UDT group and the non-UDT group (p=0.37) nor between the traumatic and non-traumatic SH groups (p=0.25). Seven visceral injuries (5.6%) were described, all of them in patients with traumatic SH and attributable to the injury mechanism that caused the SH (p=0.001).
Spigelian Hernia Diagnosis
Regarding the most commonly used imaging modalities for the diagnosis of SH, plain abdominal X-rays were reported in 10 patients (8.1%), with most cases corresponding to traumatic or incarcerated/strangulated SH. In 32 patients (26%), ultrasound scan (US) was reported as the imaging modality used, and in 20 patients (16.3%), computed tomography (CT) was reported, with the vast majority being trauma cases. Several authors reported using two or more imaging modalities.
Spigelian Hernia Treatment
In 95 patients (77.2%), surgical correction of the defect was reported, and in at least 15 of them (15.8%), it was performed urgently. The treatment provided was not detailed in 9 studies (9.6%). Of the surgically treated patients, 14 (14.7%) were approached laparoscopically. Of these, 8 (57.1%) were repaired entirely laparoscopically, 1 (7.1%) was laparoscopically explored but not repaired, and 5 (35.7%) required conversion to open surgery.
In most cases, primary repair of the defect was performed. Few authors reported the use of mesh for the repair of pediatric SH. Singal et al. [55] reported using a VYPRO™ mesh and Fascetti-Leon et al. reported using a Vicryl™ mesh [51].
Eight patients (6.5%) were managed conservatively. Of these, 3 (2.4%) had a complete spontaneous resolution, 3 (2.4%) had a partial resolution (these 3 cases were traumatic SH with a limited follow-up period), 1 (0.8%) patient died, and 1 (0.8%) had no reported follow-up.
Table 1 provides specific details for each case regarding the surgical approach, findings, and the available follow-up period.
Outcomes. Complications Associated with Spigelian Hernia corrective surgery
Ninety-five patients (77.2%) were reported as having a favorable outcome, with a highly variable follow-up period. Sixteen (13%) had no data on their follow-up and outcome. One of the patients (0.8%) died due to SH strangulation. Concerning post-surgical complications, one patient (0.8%) experienced persistent postoperative pain, 1 (0.8%) had abdominal wall laxity, and 3 patients with SH associated with UDT (2.4%) developed a scrotal abscess. Two of them developed testicular atrophy secondary to the process.
Discussion
The reported cases demonstrate a broad geographical distribution and no consistent pattern was identified. We found a clear predominance of this pathology in males (85.4%) and a slight predominance of right-sided HS over left-sided HS (45.5% vs. 38.2%), with a relatively high proportion of bilateral HS cases (10.6%). A significant variability has been identified in the way fascial defects are characterized, making it challenging to extrapolate information on this aspect.
Trauma-related HS accounts for 37.2% of reported cases in the literature. This type predominantly occurs in the age range of 7 to 9 years, with no sex predominance. Trauma-related HS has been associated with various injury mechanisms, with a clear predominance of activities involving bicycles, motorcycles, and BMX bikes. The most common mechanisms are sudden deceleration and blunt impact of the handlebar on the SL. In these cases, visceral injuries of various kinds have been documented. Therefore, in the presence of trauma with associated SH (or handlebar trauma), one must assume a high-energy injury mechanism and conduct a thorough and exhaustive screening for underlying injuries that could compromise life and whose diagnostic delay may be associated with morbidity and mortality. It is also relevant to mention that several cases have been reported as 'handlebar hernia' in a nonspecific manner. In our literature review, we were able to categorize some of these as SH (based on anatomical description or CT images), but others corresponded to anatomical areas of the abdominal wall different from SL. For this reason, we consider it essential that future authors report the anatomy of the lesions accurately and in detail, as there may be diagnostic, therapeutic, and prognostic variations between SH and other parietal lesions.
On the other hand, SH associated with UDT represents 32.2% of pediatric SH reported cases. In most instances, this is assumed to be a congenital hernia, with a strong correlation between the side of the UDT and the hernia. It is striking the high number of patients with associated anterior wall defects, ranging from non-formed inguinal canals to hernias. For example, Silberstein et al. [32] reported an absence of inguinal canal formation with associated muscle atrophy. Ostlie et al. [35], Raveenthiram [43], Bilici et al. [60] and Parihar et al. [63] reported similar findings, and Al-Salem et al. [37], Ostlie et al. [35], Bilici et al. [60] and Parihar et al. [63] reported an absence of Gubernaculum testis formation [35]. More recent authors, such as Gonuguntla et al. [85] reported similar findings. In general, when muscular alterations have been reported, they have been described in relation to the internal oblique and transversus abdominis muscles and have been described as hypoplastic, thinned out, or even absent (Komura et al., Singal et al., Inan et al.) [29,55,56]. Komura et al. reported in 1994 [29] the histology of the muscles adjacent to the affected area in HS, demonstrating atrophy with fat infiltration and interstitial fibrosis. In this context, it may be necessary to differentiate between congenital and acquired HS in terms of the likelihood of spontaneous resolution with conservative management (which might be more likely in cases of traumatic HS). A more comprehensive characterization of the defect in future cases could influence the choice of the best therapeutic approach, reserving conservative management for minor asymptomatic non-congenital fascial defects. Nevertheless, the evidence in this regard is limited. Lastly, it is relevant to consider that some authors have proposed that UDT and SH may constitute a pathological spectrum encompassed under the term “Spigelian-Cryptorchidism Syndrome”. It has also been suggested that this could be a variant of Prune-Belly syndrome, although we have not found a consistent pattern of visceral, cardiac, genitourinary, or musculoskeletal malformations in the reported patients.
Regarding complications, a relatively high percentage of patients (12.2%) experienced hernia incarceration or strangulation, with this complication predominantly occurring in younger patients. This percentage, significantly higher than other hernia-related conditions such as umbilical or epigastric hernias, should be considered when recommending prompt correction of the defect, especially during early childhood.
Diagnosing this condition has traditionally been considered challenging due to the limited clinical expression of the defect (secondary to its intraparietal location). Given that pediatric patients have a thinner anterior abdominal wall due to less muscular development and a reduced adipose layer, these hernias are potentially easier to identify clinically. However, familiarity with the anatomy of the abdominal wall and a high index of suspicion are essential for an accurate diagnosis. Several cases of misdiagnosis and diagnostic confusion with other pediatric abdominal wall defects, such as inguinal hernia, have been reported [45].
Concerning radiology tests, this review highlights the use of different imaging modalities for this condition, with a predominance of plain abdominal X-rays and CT scans in urgent or trauma scenarios and an increasing use of ultrasound in elective settings, particularly in recent years. It is important to emphasize that SH is an uncommon diagnosis in the pediatric population, and radiological studies should be performed in a targeted manner by expert radiologists to avoid diagnostic errors.
The most widely accepted and utilized treatment approach in the existing literature is open surgery. Laparoscopy has been employed in selective cases, although it is associated with a relatively high conversion rate. Conservative management is scarcely documented for this condition but has proven effective in some patients. From a perspective of biological plausibility and surgical safety, we believe that conservative management should be limited to small fascial defects in healthy patients with a traumatic etiology, who are asymptomatic and show no herniated contents on imaging studies. Likewise, we consider that these patients require close clinical and ultrasound follow-up.
Concerning the use of mesh, although the evidence is limited, given the favorable healing profile of the pediatric population and the excellent outcomes reported in cases with primary repair, the routine use of mesh for the surgical correction of this condition is not justified.
Regarding the surgical prognosis of UDT specifically in this context, the majority of authors have reported the successful performance of primary orchidopexy in a single stage. We attribute this to the fact that the hernial sac allows for progressive elongation of the spermatic vessels and the vas deferens, in contrast to purely intra-abdominal testes. Concerning medium and long term results, most published cases report a favorable outcome, but with a variable follow-up period. However, in many cases, follow-up is limited or not reported at all. Once again, it is essential to address this aspect to better understand this condition in prognostic terms.
This review has significant strengths, such as the comprehensive analysis of the existing literature and its statistical approach, with findings relevant to understanding the disease. However, it also has notable limitations, including the low number of reported cases of the condition, the lack of data or incomplete reports for some patients, the use of inferential statistics, and the inability to perform meta-analytical models.
In conclusion, HS is an uncommon condition in pediatric populations, predominantly affecting males. It can present congenitally, with a significant association with ipsilateral UDT, or it can be acquired, typically related to bicycle trauma involving the SL. The risk of incarceration is relatively high, particularly during early childhood. Most reported cases have been treated surgically, with favorable outcomes. Evidence regarding conservative management is limited.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Conflicts of interest
The authors declare that they have no conflict of interest.
Financial statement/funding
This work received no specific grant from public, commercial, or not-for-profit funding agencies; none of the authors have external funding to declare.
Contributor declaration page (CRediT statement)
Dr. Javier Arredondo Montero conceptualized and designed the study, collected and analyzed the data, drafted the initial manuscript, and revised the manuscript. Dr. María Rico-Jiménez collected the data and revised the manuscript.
Original work
All manuscript authors declare this is an original contribution that has not been previously published.
Data availability
The dataset used to carry out this study is attached as Supplementary File 2.
Informed consent
N/A.
Ethical Approval
This study is a review of the literature in which neither human nor animal patients participated. Therefore, no ethics committee assessment was sought.
References
- Skandalakis, P.N.; Zoras, O.; Skandalakis, J.E.; Mirilas, P. Spigelian hernia: Surgical anatomy, embryology, and repair technique. Am Surg. 2006, 72, 42–8. [Google Scholar] [CrossRef] [PubMed]
- Huttinger, R.; Sugumar, K.; Baltazar-Ford, K.S. Spigelian Hernia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 2024. [Google Scholar] [PubMed]
- Hanzalova, I.; Schäfer, M.; Demartines, N.; Clerc, D. Spigelian hernia: Current approaches to surgical treatment-a review. Hernia 2022, 26, 1427–1433. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jones, B.C.; Hutson, J.M. The syndrome of Spigelian hernia and cryptorchidism: A review of paediatric literature. J Pediatr Surg. 2015, 50, 325–30. [Google Scholar] [CrossRef] [PubMed]
- Larsen, W.J. Human Embryology; Elsevier, 2014. [Google Scholar]
- Sadler, T.W. Langman’s Medical Embryology; Wolters Kluwer, 2020. [Google Scholar]
- Moore, K.L.; Persaud, T.V.N.; Torchia, M.G. Before We Are Born: Essentials of Embryology and Birth Defects; Elsevier, 2020. [Google Scholar]
- Vierstraete, M.; Pereira Rodriguez, J.A.; Renard, Y.; Muysoms, F. EIT Ambivium, Linea Semilunaris, and Fulcrum Abdominalis. J Abdom Wall Surg. 2023, 2, 12217. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Scopinaro, A.J. Hernia in Spigel’s semilunar line in a newborn. Semana Med 1935, 1, 284. [Google Scholar]
- Hurwitt, E.S.; Borow, M. Bilateral Spigelian hernias in childhood. Surgery 1955, 37, 963–8. [Google Scholar] [PubMed]
- LANDRYRM Traumatic hernia. Am J Surg. 1956, 91, 301–2. [CrossRef] [PubMed]
- Isaacson, N.H. Spigelian Hernia. Report of four cases. Med Ann Dist Columbia 1956, 58, 23–26. [Google Scholar]
- Wilson, T.H., Jr. Traumatic hernia of the abdominal wall. Am J Surg. 1959, 97, 340–1. [Google Scholar] [CrossRef] [PubMed]
- Roberts, G.R. TRAUMATIC ABDOMINAL WALL RUPTURE. Br J Surg. 1964, 51, 153–4. [Google Scholar] [CrossRef] [PubMed]
- Bertelsen, S. The surgical treatment of spigelian hernia. Surg Gynecol Obstet. 1966, 122, 567–72. [Google Scholar] [PubMed]
- Hurlbut, H.J.; Moseley, T. Spigelian hernia in a child. South Med J. 1967, 60, 602. [Google Scholar] [CrossRef] [PubMed]
- Graivier, L.; Alfieri, A.L. Bilateral Spigelian hernias in infancy. Am J Surg. 1970, 120, 817–9. [Google Scholar] [CrossRef] [PubMed]
- Graivier, L.; Bernstein, D.; RuBane, C.F. Lateral ventral (spigelian) hernias in infants and children. Surgery 1978, 83, 288–90. [Google Scholar] [PubMed]
- Graivier, L.; Bronsther, B.; Feins, N.R.; Mestel, A.L. Pediatric lateral ventral (spigelian) hernias. South Med J. 1988, 81, 325–6. [Google Scholar] [CrossRef] [PubMed]
- Herbert, R.J.; Turner, F.W. Traumatic Abdominal Wall hernia in a 7-year-old child. J Pediatr Surg 1977, 12, 609–610. [Google Scholar]
- Constantino, L.; Contestabile, D.; Rocua, E. Strangulated spigelian hernia in a child. Riv Chir Pediatr 1974, 16, 236–238. [Google Scholar]
- Atiemo, E.A.; Goswami, G. Traumatic ventral hernia. J Trauma. 1974, 14, 181–2. [Google Scholar] [CrossRef] [PubMed]
- Houlihan, T.J. A review of Spigelian hernias. Am J Surg. 1976, 131, 734–5. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, P.A.; Seltzer, M.H. Pediatric Spigelian hernia: A case report. J Pediatr Surg. 1977, 12, 609–10. [Google Scholar] [CrossRef] [PubMed]
- Bar-Maor, J.A.; Sweed, Y. Spigelian hernia in children, two cases of unusual etiology. Pediatr Surg Int 1989, 4, 357–359. [Google Scholar] [CrossRef]
- Mitchiner, J.C. Handlebar hernia: Diagnosis by abdominal computed tomography. Ann Emerg Med. 1990, 19, 812–3. [Google Scholar] [CrossRef] [PubMed]
- Damschen, D.D.; Landercasper, J.; Cogbill, T.H.; Stolee, R.T. Acute traumatic abdominal hernia: Case reports. J Trauma. 1994, 36, 273–6. [Google Scholar] [CrossRef] [PubMed]
- Kubalak, G. Handlebar hernia: Case report and review of the literature. J Trauma. 1994, 36, 438–9. [Google Scholar] [CrossRef] [PubMed]
- Komura, J.; Yano, H.; Uchida, M.; Shima, I. Pediatric spigelian hernia: Reports of three cases. Surg Today. 1994, 24, 1081–4. [Google Scholar] [CrossRef] [PubMed]
- Pul, N.; Pul, M. Spigelian hernia in children--report of two cases and review of the literature. Yonsei Med J. 1994, 35, 101–4. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.E. Spigelian hernia in childhood. Pediatr Surg Int 1994, 9, 170–171. [Google Scholar] [CrossRef]
- Silberstein, P.A.; Kern, I.B.; Shi, E.C. Congenital spigelian hernia with cryptorchidism. J Pediatr Surg. 1996, 31, 1208–10. [Google Scholar] [CrossRef] [PubMed]
- Iuchtman, M.; Kessel, B.; Kirshon, M. Trauma-related acute spigelian hernia in a child. Pediatr Emerg Care. 1997, 13, 404–5. [Google Scholar] [CrossRef] [PubMed]
- Perez, V.M.; McDonald, A.D.; Ghani, A.; Bleacher, J.H. Handlebar hernia: A rare traumatic abdominal wall hernia. J Trauma. 1998, 44, 568. [Google Scholar] [CrossRef] [PubMed]
- Ostlie, D.J.; Zerella, J.T. Undescended testicle associated with spigelian hernia. J Pediatr Surg. 1998, 33, 1426–8. [Google Scholar] [CrossRef] [PubMed]
- Kubota, A.; Shono, J.; Yonekura, T.; Hoki, M.; Asano, S.; Hirooka, S.; Kosumi, T.; Kato, M.; Oyanagi, H. Handlebar hernia: Case report and review of pediatric cases. Pediatr Surg Int. 1999, 15, 411–2. [Google Scholar] [CrossRef] [PubMed]
- Al-Salem, A.H. Congenital spigelian hernia and cryptorchidism: Cause or coincidence? Pediatr Surg Int. 2000, 16, 433–6. [Google Scholar] [CrossRef] [PubMed]
- White, J.J. Concomitant Spigelian and inguinal hernias in a neonate. J Pediatr Surg. 2002, 37, 659–60. [Google Scholar] [CrossRef] [PubMed]
- Losanoff, J.E.; Richman, B.W.; Jones, J.W. Spigelian hernia in a child: Case report and review of the literature. Hernia 2002, 6, 191–3. [Google Scholar] [CrossRef] [PubMed]
- Fraser, N.; Milligan, S.; Arthur, R.J.; Crabbe, D.C. Handlebar hernia masquerading as an inguinal haematoma. Hernia 2002, 6, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Levy, G.; Nagar, H.; Blachar, A.; Ben-Sira, L.; Kessler, A. Pre-operative sonographic diagnosis of incarcerated neonatal Spigelian hernia containing the testis. Pediatr Radiol. 2003, 33, 407–9. [Google Scholar] [CrossRef] [PubMed]
- Goliath, J.; Mittal, V.; McDonough, J. Traumatic handlebar hernia: A rare abdominal wall hernia. J Pediatr Surg. 2004, 39, e20–2. [Google Scholar] [CrossRef] [PubMed]
- Raveenthiran, V. Congenital Spigelian hernia with cryptorchidism: Probably a new syndrome. Hernia 2005, 9, 378–80. [Google Scholar] [CrossRef] [PubMed]
- Vaos, G.; Gardikis, S.; Zavras, N. Strangulated low Spigelian hernia in children: Report of two cases. Pediatr Surg Int. 2005, 21, 736–8. [Google Scholar] [CrossRef] [PubMed]
- Torres de Aguirre, A.; Cabello Laureano, R.; García Valles, C.; Garrido Morales, M.; García Merino, F.; Martínez Caro, A. Hernia de Spiegel: A propósito de 2 casos asociados a criptorquidia [Spigelian hernia: Two cases associated to cryptorchidism]. Cir Pediatr. 2005, 18, 99–100. [Google Scholar] [PubMed]
- Durham, M.M.; Ricketts, R.R. Congenital spigelian hernias and cryptorchidism. J Pediatr Surg. 2006, 41, 1814–7. [Google Scholar] [CrossRef] [PubMed]
- O'Sullivan, O.; Bannon, C.; Clyne, O.; Flood, H. Hypospadias associated undescended testis in a Spigelian hernia. Ir J Med Sci. 2006, 175, 77–8. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.R. Ravi; Singal, Arbinder Kumar1,. Undescended testis in spigelian hernia. Journal of Indian Association of Pediatric Surgeons 2007, 12, 233–234. [Google Scholar] [CrossRef]
- Aksu, B.; Temizöz, O.; Inan, M.; Gençhellaç, H.; Başaran, U.N. Bilateral spigelian hernia concomitant with multiple skeletal anomalies and fibular aplasia in a child. Eur J Pediatr Surg. 2008, 18, 205–8. [Google Scholar] [CrossRef] [PubMed]
- Litton, K.; Izzidien, A.Y.; Hussien, O.; Vali, A. Conservative management of a traumatic abdominal wall hernia after a bicycle handlebar injury (case report and literature review). J Pediatr Surg. 2008, 43, e31–2. [Google Scholar] [CrossRef] [PubMed]
- Fascetti-Leon, F.; Gobbi, D.; Gamba, P.; Cecchetto, G. Neonatal bilateral spigelian hernia associated with undescended testes and scalp aplasia cutis. Eur J Pediatr Surg. 2010, 20, 123–5. [Google Scholar] [CrossRef] [PubMed]
- Christianakis, E.; Paschalidis, N.; Filippou, G. Low Spigelian hernia in a 6-year-old boy presenting as an incarcerated inguinal hernia: A case report. J Med Case Reports 2009, 3, 34. [Google Scholar] [CrossRef]
- Rushfeldt, C.; Oltmanns, G.; Vonen, B. Spigelian-cryptorchidism syndrome: A case report and discussion of the basic elements in a possibly new congenital syndrome. Pediatr Surg Int. 2010, 26, 939–42. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vega, Y.; Zequeira, J.; Delgado, A.; Lugo-Vicente, H. Spigelian hernia in children: Case report and literature review. Bol Asoc Med P R. 2010, 102, 62–4. [Google Scholar] [PubMed]
- Singal, A.K.; Ravikumar, V.R.; Kadam, V.; Jain, V. Undescended testis in Spigelian hernia--a report of 2 cases and review of the literature. Eur J Pediatr Surg. 2011, 21, 194–6. [Google Scholar] [CrossRef] [PubMed]
- Inan, M.; Basaran, U.N.; Aksu, B.; Dortdogan, Z.; Dereli, M. Congenital Spigelian hernia associated with undescended testis. World J Pediatr. 2012, 8, 185–7. [Google Scholar] [CrossRef] [PubMed]
- Lopez, R.; King, S.; Maoate, K.; Beasley, S. Trauma may cause Spigelian herniae in children. ANZ J Surg. 2010, 80, 663. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Wood, J.; Bevan, C.; Cheng, W.; Wilson, G. Traumatic abdominal wall hernia--a case report and literature review. J Pediatr Surg. 2011, 46, 1642–5. [Google Scholar] [CrossRef] [PubMed]
- Lopez, R.; King, S.; Maoate, K.; Beasley, S. Laparoscopic repair of paediatric traumatic Spigelian hernia avoids the need for mesh. ANZ J Surg. 2011, 81, 396–7. [Google Scholar] [CrossRef] [PubMed]
- Bilici, S.; Güneş, M.; Göksu, M.; Melek, M.; Pirinçci, N. Undescended testis accompanying congenital Spigelian hernia: Is it a reason, a result, or a new syndrome? Eur J Pediatr Surg. 2012, 22, 157–61. [Google Scholar] [CrossRef] [PubMed]
- Rathore, A.; Simpson, B.J.; Diefenbach, K.A. Traumatic abdominal wall hernias: An emerging trend in handlebar injuries. J Pediatr Surg. 2012, 47, 1410–3. [Google Scholar] [CrossRef] [PubMed]
- Decker, S.; Engelmann, C.; Krettek, C.; Müller, C.W. Traumatic abdominal wall hernia after blunt abdominal trauma caused by a handlebar in children: A well-visualized case report. Surgery 2012, 151, 899–900. [Google Scholar] [CrossRef] [PubMed]
- Parihar, D.; Kadian, Y.S.; Raikwar, P.; Rattan, K.N. Congenital spigelian hernia and cryptorchidism: Another case of new syndrome. APSP J Case Rep. 2013, 4, 41. [Google Scholar] [PubMed] [PubMed Central]
- Thakur, S.K.; Gupta, S.; Goel, S. Traumatic spigelian hernia due to handlebar injury in a child: A case report and review of literature. Indian J Surg. 2013, 75, 404–6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Upasani, A.; Bouhadiba, N. Paediatric abdominal wall hernia following handlebar injury: Should we diagnose more and operate less? BMJ Case Rep. 2013, 2013, bcr2012008501. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Balsara, Z.R.; Martin, A.E.; Wiener, J.S.; Routh, J.C.; Ross, S.S. Congenital spigelian hernia and ipsilateral cryptorchidism: Raising awareness among urologists. Urology 2014, 83, 457–9. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, C.; Strambi, S.; Pucci, V.; Liserre, J.; Spinelli, G.; Palombo, C. Spigelian hernia in a 14-year-old girl: A case report and review of the literature. European J Pediatr Surg Rep. 2014, 2, 58–62. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Talutis, S.D.; Muensterer, O.J.; Pandya, S.; McBride, W.; Stringel, G. Laparoscopic-assisted management of traumatic abdominal wall hernias in children: Case series and a review of the literature. J Pediatr Surg. 2015, 50, 456–61. [Google Scholar] [CrossRef] [PubMed]
- Pederiva, F.; Guida, E.; Maschio, M.; Rigamonti, W.; Gregori, M.; Codrich, D. Handlebar injury in children: The hidden danger. Surgery 2016, 159, 1477. [Google Scholar] [CrossRef] [PubMed]
- Montalvo Ávalos, C.; Álvarez Muñoz, V.; Fernández García, L.; López López, A.J.; Oviedo Gutiérrez, M.; Lara Cárdenas, C. Atypical hernia defects in childhood. Rev Pediatr Aten Primaria. 2015, 17, 139–43. [Google Scholar] [CrossRef]
- Volpe, A.; Virgone, C.; Gamba, P. Successful conservative management of handlebar hernia in children. Pediatr Int. 2017, 59, 105–106. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.; Fasano, G.; Cohen, I.T. Pediatric Spigelian hernia: A case report and review of the literature. Journal of Pediatric Surgery Case Reports 2017. [Google Scholar] [CrossRef]
- Kamal, N.R.; Shubhangi, S. Spigelian Hernia in 2-Year-Old Male Child: A Rare Case Report. JOJ Case Stud. 2017, 3, 555612. [Google Scholar] [CrossRef]
- Rinaldi, V.E.; Bertozzi, M.; Magrini, E.; Riccioni, S.; Di Cara, G.; Appignani, A. Traumatic Abdominal Wall Hernia in Children by Handlebar Injury: When to Suspect, Scan, and Call the Surgeon. Pediatr Emerg Care. 2020, 36, e534–e537. [Google Scholar] [CrossRef] [PubMed]
- Sinopidis, X.; Panagidis, A.; Alexopoulos, V.; Karatza, A.; Georgiou, G. Congenital Spigelian Hernia Combined with Bilateral Inguinal Hernias. Balkan Med J. 2018, 35, 402–403. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sengar, M.; Mohta, A.; Neogi, S.; Gupta, A.; Viswanathan, V. Spigelian hernia in children: Low versus classical. J Pediatr Surg. 2018, 53, 2346–2348. [Google Scholar] [CrossRef] [PubMed]
- So, H.F.; Nabi, H. Handlebar hernia - A rare complication from blunt trauma. Int J Surg Case Rep. 2018, 49, 118–120. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vega-Mata, N.; Vázquez-Estevez, J.J.; Montalvo-Ávalos, C.; Raposo-Rodríguez, L. Laparoscopic Spigelian hernia repair in childhood. Literature review [Abordaje laparoscópico de una hernia de Spiegel en edad pediátrica. Revisión de la literatura]. Cir Cir. 2019, 87, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, S.S.; Kothari, P.R.; Gupta, A.R.; Dikshit, V.B.; Patil, P.; Kekre, G.A.; Deshpande, A.; Kulkarni, A.A.; Hukeri, A. Total laparoscopic repair of Spigelian hernia with undescended testis. J Minim Access Surg. 2019, 15, 265–267. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nagara, S.; Fukaya, S.; Muramatsu, Y.; Kaname, T.; Tanaka, T. A case report of rare ZC4H2-associated disorders associated with three large hernias. Pediatr Int. 2020, 62, 985–986. [Google Scholar] [CrossRef] [PubMed]
- Taha, A.; Algethami, N.E.; AlQurashi, R.; Alnemari, A.K. Outcome of Orchidopexy in Spigelian Hernia-Undescended Testis Syndrome. Cureus 2021, 13, e13714. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- García Sánchez, P.; Bote Gascón, P.; González Bertolín, I.; Bueno Barriocanal, M.; López López, R.; de Ceano-Vivas la Calle, M. Handlebar Hernia: An Uncommon Traumatic Abdominal Hernia. Pediatr Emerg Care. 2021, 37, e879–e881. [Google Scholar] [CrossRef] [PubMed]
- Sinacer, S.; Semari, B.Z.; Khemari, S.; Kharchi, A.; Haif, A.; Soualili, Z. Congenital Spigelian hernia in a neonate associated with several anomalies: A case report. J Neonatal Surg 2021, 10, 38. [Google Scholar] [CrossRef]
- Thamri, F.; Houidi, S.; Zouaoui, A. Traumatic Spigelian hernia in a child. J Pediatr Surg Case Rep. 2021, 75, 102099. [Google Scholar] [CrossRef]
- Gonuguntla, A.; Thotan, S.P.; Pai, N.; Kumar, V.; Prabhu, S.P. Congenital Spigelian Hernia With Ipsilateral Ectopic Testis. Ochsner J. 2022, 22, 277–280. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kropilak, A.D.; Sawaya, D.E. Traumatic Spigelian Hernia in a Pediatric Patient Following a Bicycle Injury. Am Surg. 2022, 88, 1933–1935. [Google Scholar] [CrossRef] [PubMed]
- Okumuş, M.; Zerbaliyev, E.; Akdağ, A. Congenital spigelian hernia and ipsilateral undescended testis: An ongoing etiological debate – A case report. Int J Abdom Wall Hernia Surg 2022, 5, 209–11. [Google Scholar] [CrossRef]
- Kangabam, B. Traumatic Spigelian Hernia Following Blunt Abdominal Trauma. Cureus 2023, 15, e35564. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Farina, R.; Pennisi, M.; Desiderio, C.; Valerio Foti, P.; D'Urso, M.; Inì, C.; Motta, C.; Galioto, S.; Garofalo, A.; Clemenza, M.; Ilardi, A.; Lavalle, S.; Basile, A. Spigelian-cryptorchidism syndrome: Lesson based on a case report. Radiol Case Rep. 2024, 19, 3372–3375. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ablatt, S.; Escobar, M.A., Jr. Spigelian hernia and cryptorchidism syndrome: Open spigelian hernia repair and laparoscopic one-stage orchiopexy for ectopic testis. BMJ Case Rep. 2025, 18, e261858. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Graphic representation of the two main subtypes of Spiegel's hernia in the pediatric age group. Left: Acquired (traumatic) Spiegel's hernia. Right: Spiegel's hernia in the context of Spigelian-Cryptorchidism Syndrome. Created in BioRender. Arredondo montero, J. (2025) https://BioRender.com/a53g564.
Figure 1.
Graphic representation of the two main subtypes of Spiegel's hernia in the pediatric age group. Left: Acquired (traumatic) Spiegel's hernia. Right: Spiegel's hernia in the context of Spigelian-Cryptorchidism Syndrome. Created in BioRender. Arredondo montero, J. (2025) https://BioRender.com/a53g564.
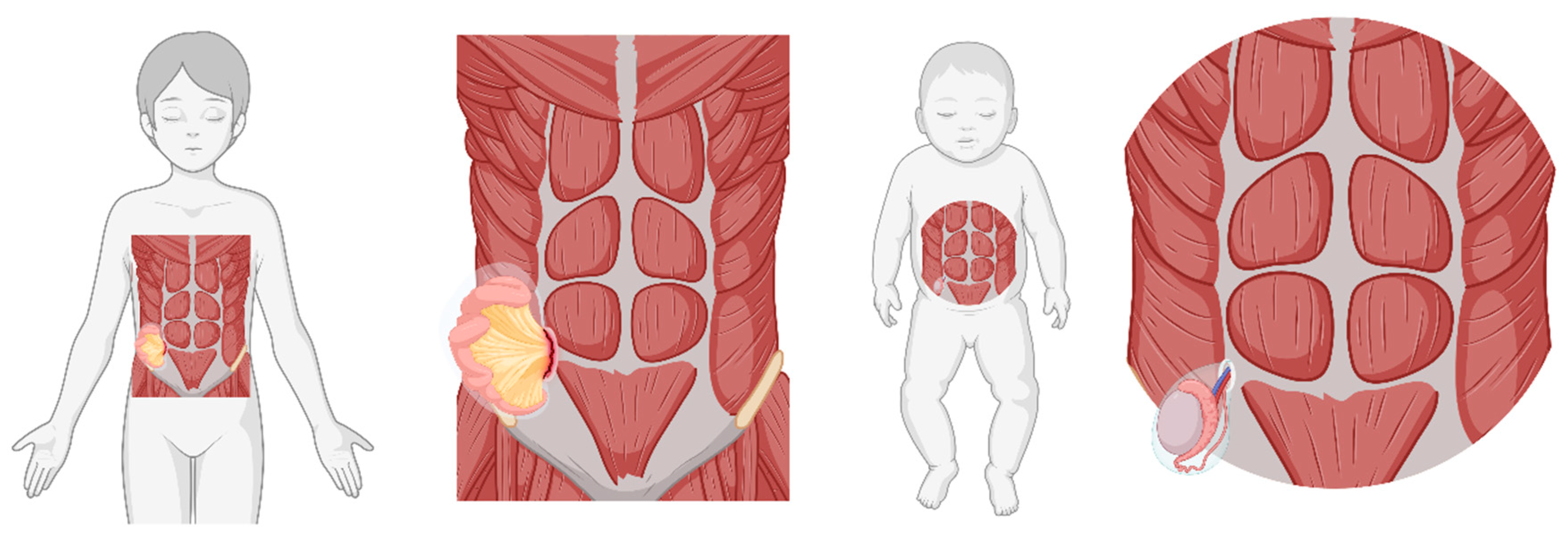
Figure 2.
Histogram and kernel density plots showing the age distribution of SH associated with UDT (top) and trauma-related SH (bottom).
Figure 2.
Histogram and kernel density plots showing the age distribution of SH associated with UDT (top) and trauma-related SH (bottom).
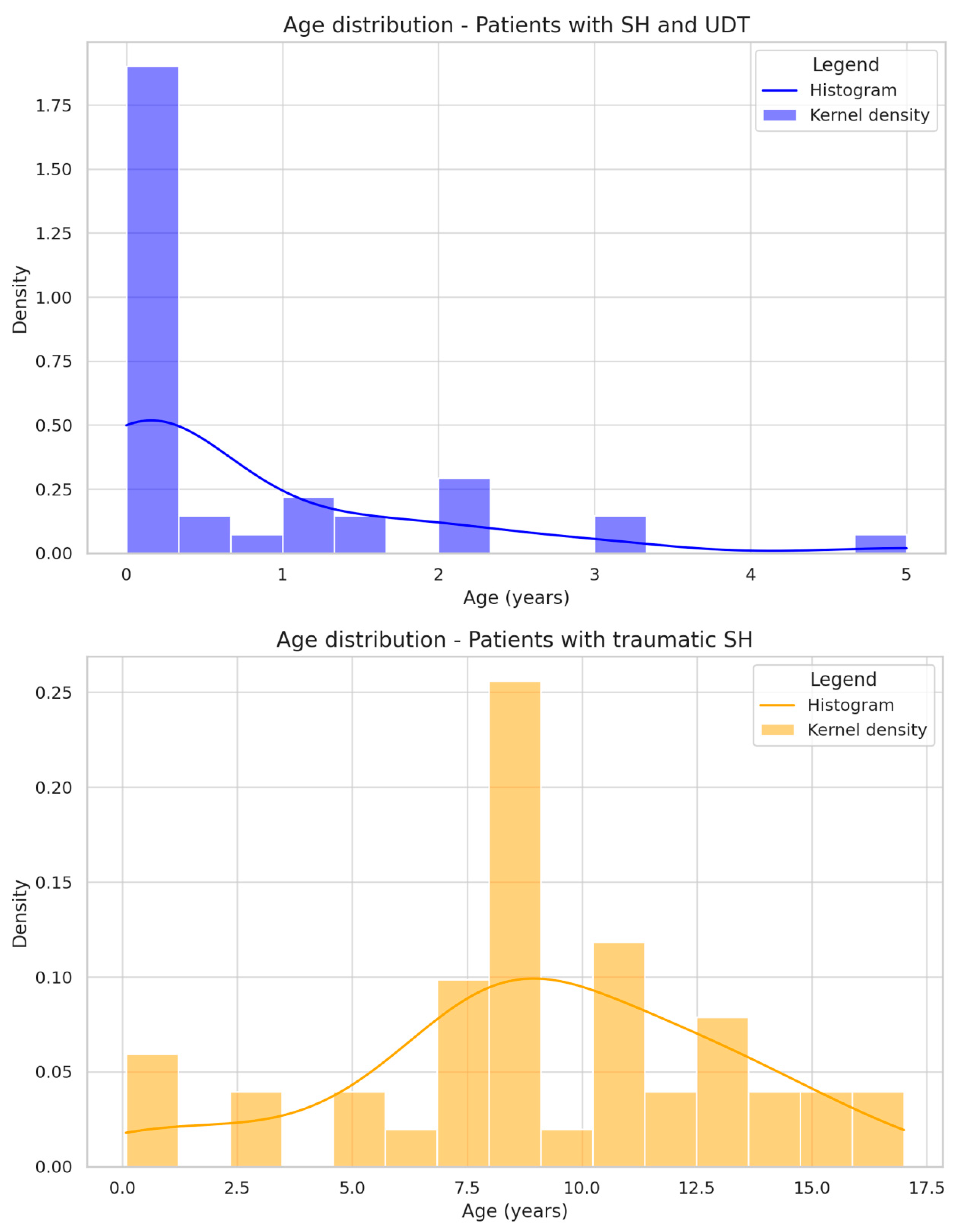

Table 1.
Previously reported cases of pediatric spigelian hernia in the medical literature.
| Author | Country | Patient´s age | Patient´s Sex | Laterality | Associated malformations/anomalies | Complications associated with SP | Relevant background |
Defect size | Radiological studies | Treatment | Surgical approach/findings | Surgical outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Scopinaro et al. (1935) [9] | - | 6-days-old | Male | - | - | Strangulation | - | - | - | - | - | Death |
| Hurwitt et al. (1955) [10] | - | 8y | Male | Bilateral | - | - | - | Right side: 2,6 cm | - | - | - | - |
| Landry et al. (1956) [11] | - | 14y | Male | Left | - | - | Previous local trauma | 4cm | - | - | - | - |
| Isaacson et al. (1956) [12]* | USA | 3y | Male | Right | - | - | Nail puncture | - | - | - | - | - |
| Wilson et al. (1959) [13] | USA | 2.5y | Male | Left | - | - | Previous local trauma (automobile) | - | Plain abdominal x-ray: traumatic hernia of the abdominal wall | Surgical | ESR 6 days after the accident Hernial sac containing omentum and transverse colon. Repair: Interrupted silk suture |
- |
| Roberts et al. (1964) [14]***** | UK | 9y | Male | Left | - | - | Previous local trauma (bicycle handlebar) | 7x3 cm | - | Surgical | Repair: Interrupted catgut suture | Favorable (6m follow-up) |
| Bertelsen S (1966) [15]* | - | 9y | Male | Right | - | - | - | 2x2 cm | - | - | - | Favorable |
| Hurlbut et al. (1967) [16] | USA | 8y | Male | Right | - | - | Previous local trauma | 3x5 cm | Plain abdominal X-ray: gas-filled small bowel loops compatible with incarcerated hernia | Surgical | ESR | Favorable |
| Graivier et al. (1967-1988) [17-19]. | USA | 1) 10m 2) 6m 3) 6m 4) 9m 5) 15y 6)17y 7)15m 8)4y 9)10d |
1) Male 2) Male 3) Male 4) Male 5) Female 6) Female 7) Female 8) Female 9) Female |
1) Bilateral 2) Right 3) Right 4) Left 5) Right 6) Bilateral 7) Bilateral 8) Left 9) Left |
1) Umbilical Hernia and bilateral indirect Inguinal hernias |
- | - | 1) 2x5 cm (left) 1x3 cm (right) |
- | Surgical | Patients 1-8: ESR Patient 9: loss of follow-up previous to surgery Hernial sacs: resected or reduced Repair: Interrupted silk suture |
Favorable. No recurrences (follow-up up to 19y) |
| Herbert et al. (1973) [20] | Canada | 7y | Male | Left | - | - | Previous local trauma (bicycle handlebar) | 4cm | Plain Abdominal X-ray: acute gastric dilatation | Surgical | ESR 3 weeks after the accident. SH Repair: Interrupted 2-0 polyglycolic acid suture. | Favorable |
| Constantino et al. (1974) [21] | - | 8y | Male | Left | - | Strangulation | - | - | - | - | - | Favorable |
| Atiemo et al. (1974) [22]***** | Ghana | 6y | Male | Left | Splenic enlargement (physical examination) | - | Previous local trauma (cow goring) | - | - | Surgical | ESR 6 days after the accident. Full abdominal wall hernia. Primary repair. | Favorable |
| Houlihan et al. (1976) [23] | USA | 21y | Male | Bilateral | - | - | - | - | - | - | ESR | Favorable |
| Jarvis et al. (1977) [24] | USA | 13y | Female | Left | - | - | - | 3 cm | - | Surgical | SH. Peritoneal sac present. | - |
| Bar-Maor et al. (1989) [25] | Israel | 1) 5y 2) 3m |
1) Female 2) Male |
1) Right 2) Left |
2) Left Bochdalek hernia | - | 1) Abdominal blunt trauma (road accident) 2) Previous abdominal surgery with forceful stretching of the abdominal wall (Bochdalek hernia) |
1) 4 cm 2) 1 cm |
- | 1) Conservative (spontaneous resolution) 2) Surgical |
ESR. SH | Favorable |
| Mitchiner et al. (1990) [26]***** | USA | 7y | Male | Left | - | Incarceration | Previous local trauma (bicycle handlebar) | 6 cm | CT (oral and intravenous contrast media): rent in the anterior abdominal wall with a loop of small bowel exteriorized in the subcutaneous tissue | Surgical (Urgent) |
3 feet of viable small bowel found in the subcutaneous tissue protruding through a large fascial defect. Reduction and primary repair. |
Favorable (4 months follow-up) |
| Damschen et al. (1994) [27]***** | USA | 5y | Male | Right | - | - | Previous local trauma (bicycle handlebar) | - | - | Surgical | Urgent surgery: SH. Small bowel herniating through the muscle layers. Repair: Interrupted polyglycolic acid suture. | Lost to follow-up (unknown) |
| Kubalak G (1994) [28]***** | USA | 8y | Male | Right | - | - | Previous local trauma (bicycle handlebar) | 6 cm | - | - | - | Favorable (2y follow-up) |
| Komura et al. (1994) [29] | Japan | 1) 6m 2) 8m 3) 3y |
1) Female 2) Female 3) Male |
1) Right 2) Right 3) Left |
1) Ipsilateral mediastinal neuroblastoma (10-12th IC spaces) - Incidental diagnosis of tumor during ultrasound examination of the SH. 2) Ipsilateral mediastinal neuroblastoma (9-10th IC spaces) |
- | 2) Previous tumor extirpation (1 week before) | 1) 5x3 cm 2) 4cm 3) 7cm |
3) US: hernial orifice 4x3 cm. Thin muscular layer in the area (3 mm). MRI: fatty infiltration of internal oblique/transverse muscles | 1) Surgical 2) Conservative 3) Surgical |
1) SH. Peritoneal sac present. Primary repair (mattress 3-0 silk sutures)** 3) SH. Primary repair (mattress 2-0 silk sutures)** |
1) Favorable (5y follow-up) 2) Favorable (spontaneous resolution) *** 3) Favorable (2m follow-up) |
| Pul et al. (1994) [30] | Turkey | 1) 18m 2) 2,5m |
1) Male 2) Male |
1) Right 2) Right |
1) Right UDT 2) Right indirect inguinal hernia |
- | - | 1) 7x7 cm 2) 4x4 cm |
1) Surgical | 1) SH. Small ring defect (1x1cm). Peritoneal sac present and excised. Primary repair. 2) SH. Small ring defect (2 cm). Peritoneal sac present and excised. Primary repair. |
1) Favorable 2) Favorable |
|
| Wright JE. (1994) [31] | Australia | 1) 19m 2) 5y 3) 7y |
1) Male 2) Male 3) Male |
1) Right 2) Right 3) Left |
- | - | - | - | - | 3) Surgical | 3) SH. Peritoneal sac present (not excised). Two-layer repair | 3) Favorable (8y follow-up) |
| Silberstein et al. (1996) [32] | Australia | 1) Newborn 2) Newborn |
1) Male 2) Male |
1) Left 2) Right |
1) Contralateral generalized abdominal musculature weakness. Left UDT. 2) Right UDT. |
- | - | 2) 3 cm | - | 1) Surgical (10w of age) 2) Surgical (4.5m of age) |
1) SH. Peritoneal sac present containing left testis (small in size, without testicular-epididymal dissociation). Absence of inguinal canal. Primary repair and orchidopexy. 2) HS. The internal oblique and transversalis muscles were poorly developed. Peritoneal sac present containing right testis. Absence of inguinal canal. Primary repair and orchidopexy. |
- |
| Iuchtman et al. (1997) [33] | Israel | 7y | Male | - | - | - | Previous local trauma (bicycle) | - | US: normal | Surgical | Urgent surgery: SH. Peritoneal protrusion (intact peritoneum). Primary repair without mesh. | Favorable |
| Pérez et al. (1998) [34]***** | USA | 11y | Male | Left | - | - | Previous local trauma (bicycle handlebar) | - | - | Surgical | Urgent surgery: SH. Peritoneal tearing. Repair in layers. | Favorable |
| Ostlie et al. (1998) [35] | USA | Newborn | Male | Right | 1) Right UDT. The right testis was palpable on the hernial sac. | - | - | 1.5 cm | - | Surgical | SH. Thinning of the layers. Absence of inguinal canal. Peritoneal sac containing the right testis. Primary repair (absorbable sutures) and orchidopexy. | - |
| Kubota et al. (1999) [36]***** | Japan | 9y | Male | Right | - | - | Previous local trauma (bicycle handlebar) | 4 cm | CT: rent in the abdominal wall through which intestinal loops protruded into the subcutaneous space. |
Surgical | SH. Peritoneal rupture. Primary repair | Favorable |
| Al-Salem et al. (2000) [37] | Saudi Arabia | 1) 3m 2) Newborn |
1) Male 2) Male |
1) Left 2) Left |
1) Left UDT. 2) Micrognathia, cleft palate, malformed ears, right clubfoot, malformed left lower limb, left UDT. Left testis palpable on the hernial sac. (Insulin-dependent diabetic mother). |
- | - | 1) 5 cm | 1) US: normal | 1) Surgical | 1) SH. Peritoneal sac present containing left testis (small in size, without testicular-epididymal dissociation) and sigmoid colon. Primary repair and orchidopexy. | 1) Favorable (2.5y follow-up) 2) Died before surgery (sepsis, not related to SH) |
| White J (2002) [38] | USA | 1m | Female | Right | Bilateral inguinal hernia. | Incarceration/small bowel obstruction. | SH appeared in the immediate postoperative period after bilateral inguinal hernia repair. | 1.5 cm (ring) | Plain abdominal X-ray: Partial small bowel obstruction US: bowel in the mass, under the skin |
Surgical | SH. Reduction of the small bowel, primary repair. | Favorable |
| Losanoff et al. (2002) [39] | USA | 12y | Male | Right | - | Omentum incarceration mimicking acute appendicitis. | . | 1.5 cm | Plain chest and abdominal X-rays: Normal | Surgical (urgent) | Normal appendix. SH with incarcerated and infarcted omentum. Resection, primary repair | Favorable (6m follow-up) |
| Fraser et al. (2002) [40]***** | UK | 11y | Male | Right | - | Inguinal hematoma | Previous local trauma (bicycle handlebar) | 12x8 cm (bulge) | US: disruption of the muscle layers of the abdominal wall with bowel and free fluid lateral to the rectus muscle. Plain abdominal X-ray (lateral): A collection of gas was visible in the anterior abdominal |
Surgical | Traumatic hernia involving all layers of the lower abdominal wall above the inguinal canal. Primary repair (absorbable suture). | Favorable |
| Levy et al. (2003) [41] | Israel | 1) 1m 2) 5w |
1) Male 2) Male |
1) Bilateral 2) Left |
1) Bilateral UDT. 2) Left UDT. |
1) Incarceration | - | 2) 5 cm | 1) US (Right side): HS containing Incarcerated bowel loops and the undescended right testis US (Left side): small SH containing the undescended left testis 2) US: left SH containing bowel loops and the undescended left testis |
1) Right side: Surgical (urgent) Left side: Surgical (deferred, with 10m) 2) Surgical (deferred, with 2m) |
1) Right side: SH. Small bowel reduction, primary repair, right orchidopexy Left side: SH primary repair, left orchidopexy 2) SH. Peritoneal sac present containing small bowel and left testis. Reduction, primary repair, and orchidopexy |
Favorable |
| Goliath et al. (2004) [42] ***** | USA | 11y | Male | Right | - | - | Previous local trauma (bicycle handlebar) | - | CT: Intestinal loops protruding through a defect in the abdominal wall into the subcutaneous space. |
Surgical | Defect throughout his entire abdominal wall, including the fascia, muscular layers, and peritoneum, with bowel protruding into the subcutaneous space, leaving his skin and intraabdominal organs completely intact. Primary repair |
Favorable |
| Raveenthiran V (2005) [43] | India | Newborn (2d) | Male | Right | Imperforate anus. Bilateral UDT. Hypoplastic scrotum. Left inguinal hernia (noted with 1m of life), umbilical hernia (noted with 2m of life) | - | - | 5x5cm | US: bowel loops in the intermuscular plane at the site of the SH | Surgical (deferred, with 13m) | SH. Peritoneal sac present containing right testis. Absence of inguinal canal. | Favorable |
| Vaos et al. (2005) [44] | Greece | 1) 20m 2) 8m |
1) Male 2) Male |
1) Left 2) Right |
- | 1) Strangulation 2) Strangulation |
- | 1) 2.5 cm (bulge), 2 cm (ring) 2) 2 cm (bulge), 1 cm (ring) |
1) Plain abdominal X-ray: several gas-fluid levels in the small bowel | 1) Surgical (urgent) 2) Surgical (urgent) |
1) SH. Peritoneal sac present containing incarcerated viable small bowel loops and infarcted omentum. Omentectomy, reduction, primary repair. 2) SH. Peritoneal sac present containing incarcerated viable small bowel loops. Reduction, primary repair. |
1) Favorable (12m follow-up) 2) Favorable (6m follow-up) |
| Torres de Aguirre (2005) [45] | Spain | 1) Newborn 2) Infant (5w) |
1) Male 2) Male |
1) Right 2) Bilateral |
1) Right UDT. 2) Bilateral UDT. |
1) Incarceration 2) Right incarceration |
- | - | 1) US and Plain abdominal x-ray: incarcerated right inguinal hernia | 1) Surgical (urgent) 2) Surgical (urgent) |
1) SH. Peritoneal sac present containing incarcerated small bowel and right testis. Reduction, primary repair, and orchidopexy 2) Bilateral SH. Right: Peritoneal sac present containing incarcerated viable small bowel loops. Reduction, primary repair. Left: peritoneal sac present containing a hypoplastic left testis with epididymal-testicular dissociation. Orchiectomy and primary repair. |
Favorable |
| Durham et al. (2006) [46] | USA | 1) 8m 2) 13m 3) 14m**** 4) 2m**** |
1) Male 2) Male 3) Male 4) Male |
1) Left 2) Bilateral 3) Bilateral 4) Right |
1) Left UDT 2) Bilateral UDT 3) Bilateral UDT 4) Bilateral UDT |
- | - | - | - | Surgical | 1) SH. Peritoneal sac present containing left testis. Orchidopexy and primary repair 2) bilateral SH. Staged repair: right side with 13m and left with 16m. Peritoneal sac present containing testes. Orchidopexy and primary repair (absorbable sutures, 8-ply SIS mesh on right side) 3) bilateral SH. Repair. Testicles found in their ipsilateral SH sac. Orchidopexy and primary repair 4) With 13m: Right intraabdominal testis: orchidopexy. Right SH: primary repair. With 16m: left inguinal orchidopexy. |
1) Complication: scrotal abscess. Loss of follow-up 2) Favorable (laxity on the right side where the SIS patch was used) 3) Favorable (45m follow-up) 4) Favorable (12m follow-up) |
| O´Sullivan et al. (2006) [47] | Ireland | 4m | Male | Left | Left UDT. Hypospadias. | - | - | - | - | Surgical | SH. Peritoneal sac present containing left testis. Orchidopexy, primary repair. | - |
| Kumar et al. (2007) [48] | India | 3y | Male | Right | Right UDT. | - | - | 7 cm (neck of peritoneal sac) | - | Surgical | SH. Peritoneal sac present containing right testis. Orchidopexy, primary repair (VYPRO mesh) | Favorable |
| Aksu et al. (2007) [49] | Turkey | 4y | Female | Bilateral | Consanguineous parents. Multiple skeletal anomalies. | - | - | 6.5 cm (bulges), 3x2 cm (right ring) 2x1 cm (left ring) |
- | Surgical | Bilateral SH. Internal oblique and transverse abdominus missing. Peritoneal sac present containing small bowel loops. Reduction, primary repair (3/0 Vicryl sutures). | Favorable (8m follow-up) |
| Litton et al. (2008) [50]***** | UK | 13y | Male | Right | - | - | Previous local trauma (bicycle handlebar) | CT: herniation of bowels. No intraabdominal injury | Conservative (spontaneous resolution) | - | Favorable (4m follow-up) | |
| Fascetti-Leon et al. (2009) [51] | Italy | Newborn | Male | Bilateral | Bilateral UDT. Scalp aplasia cutis. Hypertelorism, delayed growth, small head circumference, hypoplasia of the nasal alae, dentition anomalies | - | - | - | US: bilateral SH. Bilateral UDT | Surgical | Bilateral SH. Peritoneal sac present containing testes. Orchidopexy and primary repair (VICRYLTM mesh) | Favorable (12m follow-up) |
| Christianakis et al. (2009) [52] | Greece | 6y | Male | Left | - | Inguinoscrotal pain | - | 1.5 cm (ring) | - | Surgical | SH. Peritoneal sac present. Primary repair (non-absorbable sutures) | Favorable (8y follow-up) |
| Rushfeldt et al. (2010) [53] | Norway | Newborn | Male | Right | Right UDT | Incarceration | - | - | US: SH with hernial sac between the obliquus externus and the obliquus internus (7mm hernia opening) containing right testis and a loop of small bowel. | Surgical (urgent) | SH. Peritoneal sac present containing incarcerated viable small bowel loops and right testis Reduction, orchidopexy, primary repair. | Favorable |
| Vega et al. (2010) [54] | Puerto Rico | 9y | Male | Left | - | - | - | - | - | Surgical | SH. Primary repair. | - |
| Singal et al. (2011) [55] | India | 1) 3y 2) 3m |
1) Male 2) Male |
1) Right 2) Left |
1) Right UDT 2) Left UDT. Glanular hypospadias |
- | - | 1) 7 cm (ring/neck) | - | Surgical | 1) SH. Thinned out internal oblique. Peritoneal sac present containing right testis. Orchidopexy and primary repair (VYPRO mesh) 2) SH. Peritoneal sac present containing left testis. No inguinal canal nor gubernaculum present. Orchidopexy and primary repair |
1) Favorable (4y follow-up) 2) Favorable (1y follow-up) |
| Inan et al. (2011) [56] | Turkey | Newborn (26d) | Male | Right | Right UDT | - | - | 3 cm (bulge), 2 cm (ring) | US: fascial plane defect through the linea semilunaris with herniation of bowel loops between the internal and external oblique muscles. Absence of testis in right scrotum. No inguinal canal nor spermatic cord. |
Surgical | SH. Thinning of layers. Peritoneal sac present containing right testis. Orchidopexy and primary repair. | Complication: scrotal abscess (postoperative day 8) and atrophy of the testis |
| Lopez et al. (2011) [57,58] | New Zealand | 14y | Male | Left | - | - | Previous local trauma (bicycle handlebar) | - | CT: herniation of fat and vessels through a defect in the abdominal wall musculature consistent with a diagnosis of SH |
Surgical | SH. Laparoscopic repair | - |
| Yan et al. (2011) [59] ***** | Australia | 8y | Male | Right | - | - | Previous local trauma (BMX handlebar) | - | CT: TAWH | Surgical (urgent) | TAWH. Primary repair | Favorable (1m follow-up) |
| Bilici et al. (2012) [60] | Turkey | 1) 6m 2) 1y 3) 2y 4) 5y |
1) Male 2) Male 3) Male 4) Male |
2 patients: left 2 patients: right |
4 patients: Ipsilateral UDT | 4 patients: abdominal distension | - | 1.5 to 2.5 cm | - | Surgical | SH. Peritoneal sac present containing ipsilateral testis (all cases). Absence of inguinal canal Orchidopexy and primary repair | Favorable (6m follow-up) |
| Rathore et al. (2012) [61] ***** | USA | Five patients (9-15y) 1) 15y 2) 15y 3) 13y 4) 9y 5) 11y |
All male | - | - | Three patients with associated visceral injury: 1,4) cecal wall hematoma, 2) duodenal hematoma, pancreatic contusion | Previous local trauma (bicycle handlebar) in all patients | - | CT (patient no.5): compatible with an SH | Surgical | - | 2) pancreatic pseudocyst. 1) persistent pain. Three cases evolved favorably. |
| Decker et al. (2012) [62] ***** | Germany | 13y | Male | Right | - | Abdominal wall hematoma | Previous local trauma (bicycle handlebar) | - | CT: 18.39 mm gap in the fascia of the abdominal rectus muscle and the internal and external oblique muscles with two intestinal loops | Surgical | SH. Primary repair. | Favorable |
| Parihar et al. (2013) [63] | India | 3m | Male | Right | Right UDT | - | - | - | US: testis in the layers of the abdominal wall, along with small bowel loops, echoes. | Surgical | SH. Peritoneal sac present containing ipsilateral testis. Absence of inguinal canal. Orchidopexy and primary repair | Favorable |
| Thakur et al. (2013) [64] | India | 9y | Male | Right | - | - | Previous local trauma (bicycle handlebar) 5 weeks before | 6x4 cm (bulge), 4x4 cm (ring) |
US: 4x4 cm defect along the right semilunar line with small bowel loops | Surgical | SH. Peritoneal sac present (opened). Primary repair (non-absorbable sutures) | Favorable (18m follow-up) |
| Upasani et al. (2013) [65] ***** | UK | 12y | Male | Left (upper) | - | - | Previous local trauma (BMX handlebar) | 10x10 cm (bulge),2cm (ring) | US: abdominal wall hematoma. CT: 2 cm fascial defect with fat herniating through the defect | Conservative (partial resolution) | - | Favorable (6m follow-up) |
| Balsara et al. (2014) [66] | USA | Newborn (2w) | Male | Left | Left UDT | - | - | - | US: normal-sized left testicle within the SH in the left lower quadrant with loops of bowel. | Surgical | Exploratory laparoscopy: vas deferens and spermatic vessels entering the hernia sac. Left testis confirmed to lie within the sac itself. Open correction: SH. Hernial sac present containing left testis. Orchidopexy and primary repair. | Favorable (7m follow-up) |
| Spinelli et al. (2014) [67] | Italy | 14y | Female | Right | - | One-year history of recurrent abdominal pain. | - | 1.5 cm | US: fascial defect in right hemiabdomen | Surgical | SH. Hernia lipoma. Peritoneal sac present containing greater omentum. Reduction and primary repair. | Favorable |
| Talutis et al. (2014) [68] | USA | 1) 9y 2) 7y 3) 11y 4) 7y |
1) Male 2) Male 3) Male 4) Female |
1) Left 2) Right 3) Left 4) Right |
- | 1) Contusion to the mid-jejunum. 2) Mesenteric defect in the ileocecal region 4) Ileal perforation |
1,3,4) Previous local trauma (bicycle handlebar) 2) ATV collision |
1) 4x3 cm | 1) CT: 4x3 cm fascial defect (SH) with a contusion to the mid-jejunum. 4) CT: Handlebar sign. Evidence of RLQ abdominal wall defect with herniation |
1-3) Surgical | 1,3,4) Laparoscopic. Conversion to open surgery. 2) Open surgery |
1-4) Favorable |
| Pederiva et al. (2015) [69] ***** | Italy | 9y | Male | Left | - | Ileal perforation (not diagnosed at CT) | Previous local trauma (bicycle handlebar) | - | CT: abdominal wall hematoma. Defect through rectus sheath between left rectus abdominis and internal and external oblique. Intraabdominal fat herniated through the defect. | Surgical | Laparotomy. Intestinal resection. Primary repair (absorbable sutures). | Favorable |
| Montalvo et al. (2015) [70] | Spain | 1m | Female | Left | Left UDT | - | - | - | US (NR) | - | SH. Laparoscopic approach: Peritoneal sac present containing left testis. Orchidopexy. NO primary repair | Favorable (unknown follow-up) |
| Volpe et al. (2016) [71] ***** | Italy | 1) 8y 2) 9y |
1) Male 2) Male |
1) Right 2) Right |
- | - | 1) Previous local trauma (bicycle handlebar) 2) Previous local trauma (bicycle handlebar) |
1) 1.5 cm 2) 1 cm |
1) US: 1.5 cm hernia between the rectus and the internal oblique with herniation of the omentum 2) US: 1 cm defect with bowel herniation |
1) Conservative 2) Conservative |
- | 1) Favorable (last control: 3mm defect) (12m follow-up 2) Favorable (last control: 3 mm defect) (2m follow-up |
| Shea et al. (2017) [72] | USA | 16y | Male | Left | - | - | Previous local trauma (bicycle handlebar) | 1x1cm | CT: SH in the anterior left lower abdominal wall. | Surgical | SH. No peritoneal sac. Primary repair (absorbable sutures) | Favorable |
| Kamal et al. (2017) [73] | India | 2y | Male | Right | Patchy frontal hair loss, left eye deviation, bilateral UDT. | - | - | - | US: defect in the anterior abdominal wall lateral to the rectus muscle with herniation of preperitoneal fat. Absence of both testes in the scrotal sac. CT: SH with small bowel herniation. Both testes on the inguinal region | Surgical | SH. Peritoneal sac present. Primary repair One month later, bilateral orchidopexy. |
Favorable |
| Rinaldi et al. (2017) [74] ***** | Italy | 1) 12y 2) 13y |
1) Male 2) Male |
1) Left 2) Right |
- | - | 1) Previous local trauma (bicycle fall) 2) Previous local trauma (bicycle fall) |
1) 5 cm | 1) US: no peritoneal lesions; CT: defect in left anterior abdominal wall between lateral margin of the left rectus and medial margin of ipsilateral oblique muscles. 2) US: right rectus hemorrhage, free liquid in the right lower quadrant. CT: defect of the right anterior abdominal wall, with a slight separation between the right rectus and the oblique muscules. |
1) Surgical (urgent) 2) Surgical (urgent) |
1) SH. Omentum identified under the skin. Primary repair (absorbable sutures). 2) Exploratory laparoscopy. Peritoneal repair (partial report) |
1) Favorable 2) Favorable |
| Sinopidis et al. (2018) [75] | Greece | Newborn | Male | Left | Bilateral inguinal hernias | - | - | - | US: preperitoneal fat protruding through a defect of the transversalis fascia | Surgical | 2-month-old: bilateral inguinal hernia repair 5-month-old: SH. Preperitoneal fat adhered to the tip of the hernial sac. Primary repair. |
Favorable (18m follow-up) |
| Sengar et al. (2018) [76] | India | 1) 12y 2) 4y 3) 4y 4) 2.5y 5) 2.3y 6) 2y 7) 1.6y 8) 1m 9) 1m 10) 6d |
1) Female 2) Female 3) Male 4) Male 5) Male 6) Male 7) Male 8) Female 9) Male 10) Male |
1) Bilateral 2) Right 3) Left 4) Bilateral 5) Right 6) Right 7) Right 8) Left 9) Right 10) Left |
5) Right UDT 6) Right UDT 7) Right UDT 9) Umbilical hernia, lumbar hernia 10) Hypospadias |
- | - | - | - | Surgical | 3) SH containing small bowel 5,6,7,10) SH containing testis. All testes were normal without epidydimal-testicular dissociation. In all cases orchidopexy was performed. 2 cases could be brought down up to a high scrotal level only All cases: primary repair. |
Favorable (2m-8y follow-up) |
| Fai-So et al. (2018) [77] ***** | Australia | 10y | Male | Left | - | Incarcerated sigmoid colon | Previous local trauma (bicycle handlebar) | - | CT: SH with a loop of sigmoid colon | Surgical (urgent) | Exploratory laparoscopy. Primary repair (laparoscopic). Absorbable sutures. | Favorable (5w follow-up) |
| Vega-Mata et al. (2019) [78] | Spain | 13y | Male | Right | - | Obesity (BMI 32.5) | - | - | US: 7mm SH with fat herniation | Surgical | SH. Peritoneal sac containing omentum. Primary repair (laparoscopic). Non-absorbable sutures. | Favorable (1y follow-up) |
| Deshmukh et al. (2019) [79] | India | 11m | Male | Left | Left UDT | - | - | - | - | Surgical | SH. Laparoscopic repair: Peritoneal sac present containing left testis. Orchidopexy and primary repair | - |
| Nagara et al. (2020) [80] | Japan | Newborn | Male | Left | Right-sided inguinal hernia. Left UDT. ZC4H2 associated disorders: Congenital contractures of upper and lower extremities, hypokinesia, paraesophageal hiatal hernia |
Small bowel incarceration | - | - | CT: left SH with incarcerated small bowel. Right-sided inguinal hernia. | Conservative | - | Death (SH incarceration, sepsis) |
| Taha et al. (2021) [81] | Saudi-Arabia | 50d | Male | Right | Right UDT | Incarceration | - | - | Plain abdominal X-ray: distended bowel loops, gasless lower abdomen, and right lower quadrant lucency. US: small amount of intraperitoneal free fluid and a loop of bowel herniated through the abdominal wall, defect; the defect was (10 mm) in diameter. |
Surgical (urgent) | SH. Peritoneal sac present containing fluid, small bowel loops, and the right testis. Reduction, orchidopexy, primary repair | Complication: scrotal infection (conservative management). Testicular atrophy (2y follow-up) |
| García-Sanchez et al. (2021) [82] ***** | Spain | 11y | Female | Right | - | - | Previous local trauma (bicycle handlebar) | 2.4x1.8 cm | US: 2.4x1.8 cm defect between rectus abdominis and oblique/transversus with omentum and small bowel loops inside | Surgical | - | Favorable (1w follow-up) |
| Sinacer et al. (2021) [83] | Algeria | Newborn | Male | Right | Right inguinal hernia (incarcerated), bilateral UDT, polydactyly (right hand), anal stenosis (type 1 diabetic mother) | - | - | 1.5 cm | - | Surgical | SH. Peritoneal sac present containing small bowel loops and the left testis. Reduction, orchidopexy, primary repair (non-absorbable sutures) | - |
| Tahmri et al. (2021) [84] | Tunisia | 9y | Male | Right | - | - | Previous local trauma (bicycle handlebar) | 2 cm | US: right rectus abdominis hematoma. Diastasis between the lateral edge of the rectus abdominis and the ipsilateral oblique and transverse muscles resulting in a 14 mm hernia sac containing omentum | Surgical | SH. Peritoneal sac present. Primary repair (absorbable sutures) | Favorable |
| Gonuguntlaet al. (2022) [85] | India | 3m | Male | Left | Left UDT | - | - | - | US: 2 abdominal wall defects. 1) in the left iliac fossa (1.6 cm) 2) posterosuperior to the the first defect in the posterior abdominal wall lateral to the kidney (1.3 × 0.6 cm). Left testis not visible. |
Surgical | SH. Laparoscopic repair. Absence of inguinal canal and gubernaculum.Orchidopexy and primary repair | Favorable (1y follow-up) |
| Kropilak et al. (2022) [86] | USA | 8y | Male | Left | - | - | Previous local trauma (bicycle handlebar) | - | CT: traumatic SH in the left lower quadrant with incarceration of loops of small bowel and associated stranding of surrounding tissues. | Surgical (urgent) | Diagnostic laparoscopy. Laparotomy conversion. SH. Small bowel mesenteric injury with a devitalized jejunum. Intestinal resection and anastomosis. Primary repair (absorbable suture) | |
| Okumus et al. (2022) [87] | Turkey | Newborn | Male | Right | Right UDT | - | - | 2-3 cm | Plain abdominal X-ray: intestinal loops under the skin, US: Ventral hernia | Surgical | SH. Peritoneal sac present containing the right testis. Orchidopexy, primary repair. | Favorable (6m follow-up) |
| Kangabam et al. (2023) [88] | India | 17y | Male | Right | - | - | Previous local trauma (motorcycle handlebar) | 1 cm | US: 1x1 cm defect in right Spigelian aponeurosis with herniating bowel loops CT: confirmation of findings |
Conservative (patient´s choice) | - | - |
| Farina et al. (2024) [89] | Italy | 4m | Male | Left****** | Left UDT | Large Bowel Incarceration | - | US: 5,8 mm hernia breach containing a sac with colon loop, adipose tissue, fluid collection and a testicle. | Surgical (urgent) | Herniopexy and testicle repositioning in the scrotal sac | Favorable | |
| Ablatt et al. (2025) [90] | USA | 2w | Male | Left | Left UDT, bilateral inguinal hernia, umbilical hernia | - | - | US: left inguinal hernia containing fluid and nonobstructive bowel. SH not diagnosed. | Surgical (urgent) | Open umbilical hernia repair, laparoscopic left orchiopexy, open SH repair, open left inguinal hernia repair, open right inguinal hernia repair | Favorable (6w follow-up) |
SH: Spigelian Hernia; US: ultrasound; NR: not reported; y: years; m: months; d: days; w: weeks; USA: United States of America; UK: United Kingdom; cm: centimeters; ESR: elective surgical repair; In some cases, there was duplication or redundancy of patients between publications: CT: computer tomography; US: ultrasound; IC: intercostal; UDT: undescended testis; TAWH: Traumatic abdominal wall hernia; BMI: Body mass index. *The original article could not be found, and the data reported correspond to other previous reviews; **: the histological study showed muscle atrophy with fatty infiltration; ***: authors suspect that it was an incisional hernia (postoperative hernia); ****: Siblings; *****: reported unspecifically as a handlebar hernia or traumatic abdominal wall hernia (TAWH) but radiologically and clinically compatible with an SH, ******: The authors report inconsistent data in the manuscript, sometimes referring to left-sided laterality and other times to right-sided laterality. However, the overall interpretation of the case suggests that it involves left-sided laterality. The authors were contacted to resolve this matter.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



