Submitted:
27 January 2025
Posted:
28 January 2025
You are already at the latest version
Abstract
It is well established by research that large-scale and indiscriminate prescribing, dispensing and use of antimicrobials drive antimicrobial resistance (AMR) endangering the health and well-being of people, animals, and the environment. In the context of low- and middle-income countries (LMICs), the prescribing of antimicrobials is often not based on biomedical rationality but involves alternative logic driven by social, cultural, and institutional factors. This paper seeks to develop a “biosocial” perspective, reflecting a unified perspective that treats the biomedical and social conditions as two sides of the same coin. This integrated perspective helps develop synergistic insights on both the nature of prescriptions and why they occur. This analysis is based on an empirical investigation of prescription slips that patients carry to buy drugs from the pharmacy following an outpatient department encounter with the clinician. Data collection involves mixed methods, including the quantitative analysis of the antimicrobials prescribed and a qualitative analysis of the underlying reasons for these prescriptions, as described by doctors, pharmacists, and patients. Data analysis involved triangulating quantitative and qualitative data, to develop a “biosocial” perspective, which can provide implications for the development of antimicrobial stewardship policies, particularly relevant for health institutions in low- and middle-income countries.
Keywords:
1. Introduction
3. Material and Methods
3.1. The Research Context
3.2. Research Design
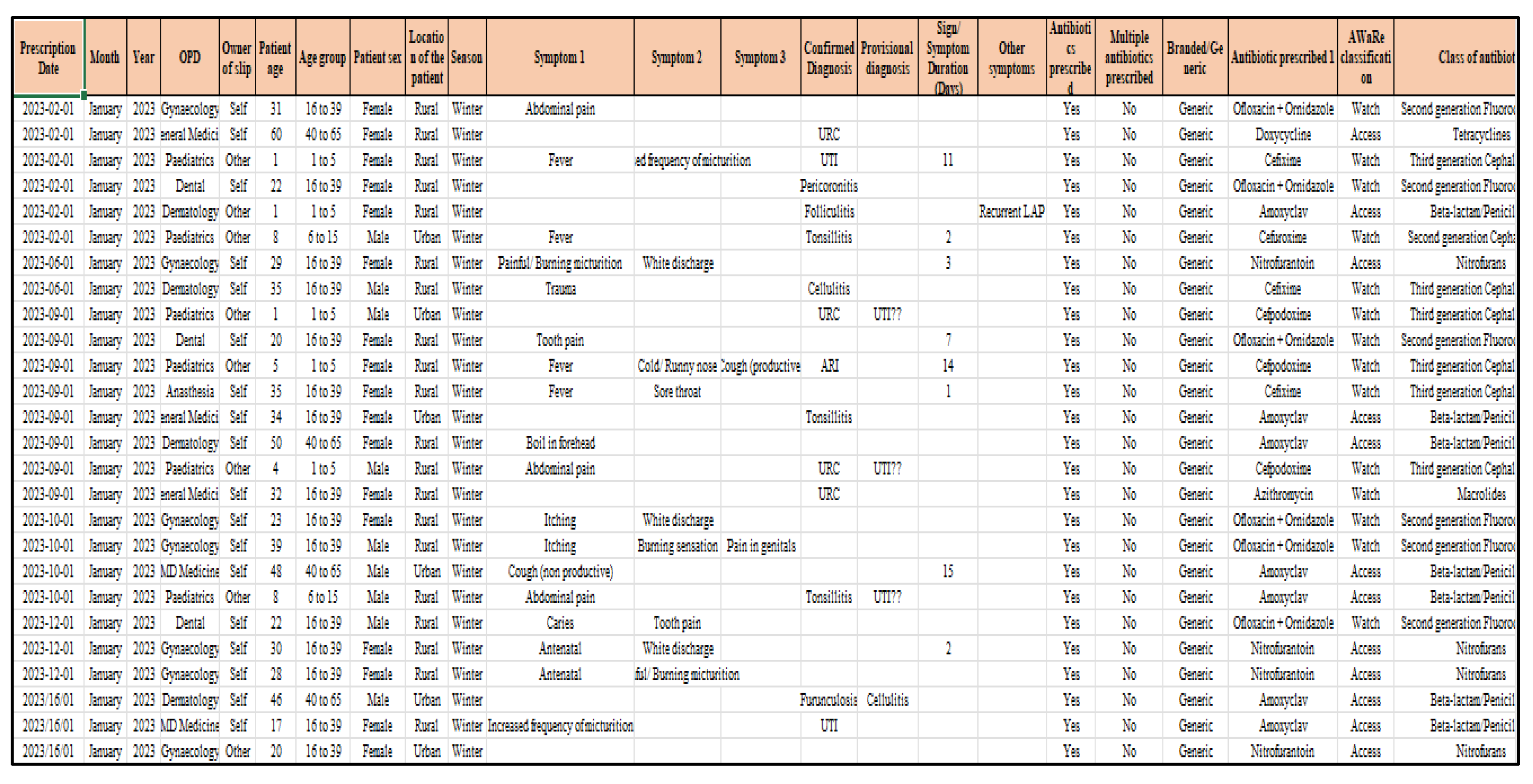
3.3. Quantitative Study of Prescription Patterns
3.4. Qualitative Study to Understand the “Why” of Prescriptions
3.5. Data Analysis
4. Results
4.1. Summary Statistics
4.2. Evaluation Of Antibiotic Prescription Patterns
4.3. Source of Prescriptions
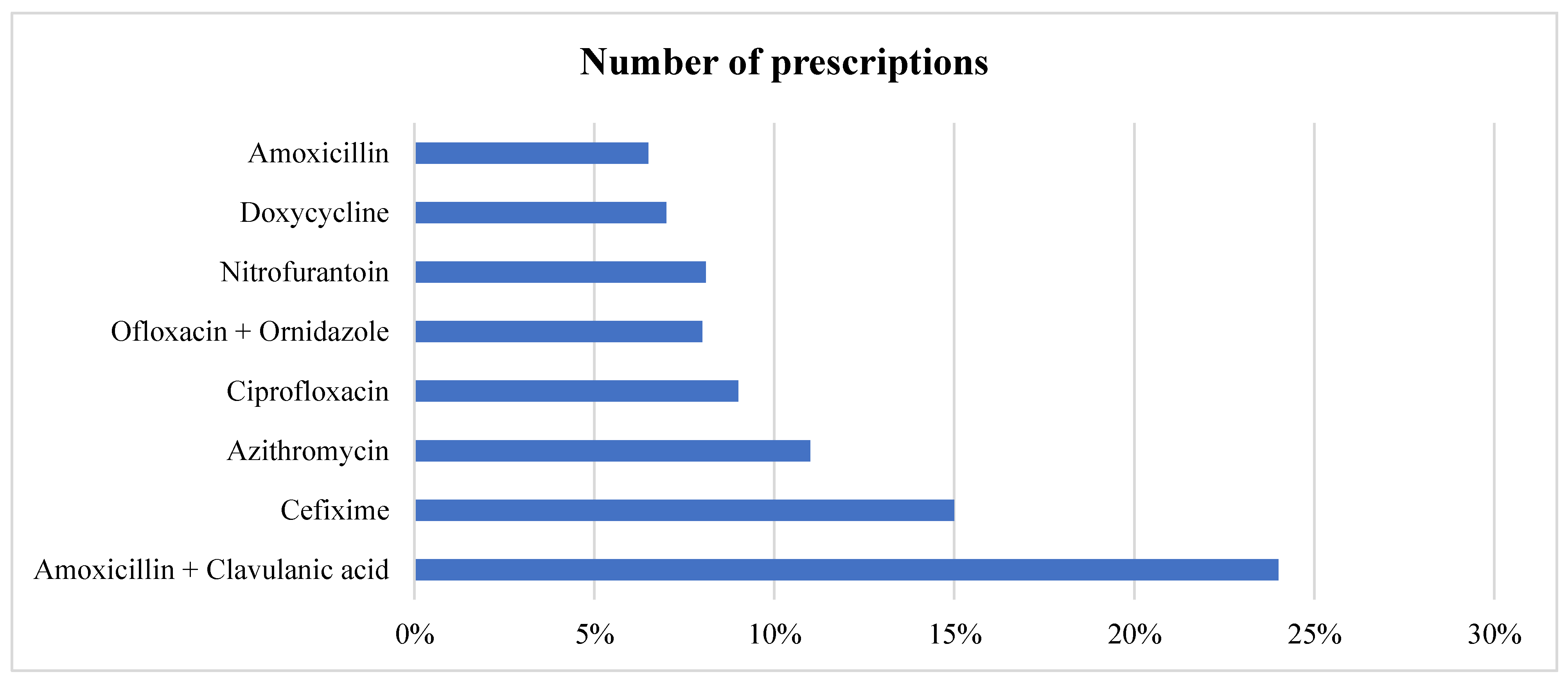
4.4. Most Prescribed Antimicrobials for Symptomatic Treatment

| S No. | Diagnosis/ Sign/ Symptom | Broad categorization | Top antimicrobials prescribed for it | Class of antimicrobial | Broad and Narrow spectrum |
|---|---|---|---|---|---|
| 1. |
Caries |
Dental condition |
Ofloxacin+ornidazole | 2nd generation Fluoroquinolones |
Broad spectrum |
| Amoxicillin | Aminopenicillins | Broad spectrum | |||
| Amoxicillin- Metronidazole | Aminopenicillins + 2nd generation Fluoroquinolones | Broad + Narrow spectrum | |||
| 2. | ARI | Respiratory condition | Amoxicillin + clavulanic acid | Aminopenicillins + Beta- lactamase | Broad spectrum |
| Cefixime | 3rd generation Cephalosporins | Broad spectrum | |||
| Azithromycin | Macrolides | Broad spectrum | |||
| 3. |
UTI |
Urogenital condition |
Cefixime |
3rd generation Cephalosporins | Broad spectrum |
| Nitrofurantoin |
Nitrofuran | Broad spectrum | |||
| Amoxicillin + clavulanic acid | Aminopenicillins + beta lactamase inhibitor | Broad spectrum | |||
| 4. |
Tonsillitis |
Otolaryngological condition |
Amoxicillin + clavulanic acid | Aminopenicillins + beta lactamase inhibitor | Broad spectrum |
| Azithromycin | 1st generation Macrolides | Broad spectrum | |||
| Cefixime | 3rd generation Cephalosporins | Broad spectrum | |||
| 5. | Acne / Acne vulgaris | Respiratory condition | Azithromycin | 1st generation Macrolides | Broad spectrum |
| Doxycycline | 1st generation Tetracycline | Broad spectrum | |||
| 6. |
Cellulitis |
Skin condition |
Amoxicillin + clavulanic acid | Aminopenicillins + beta- lactamase inhibitor | Broad spectrum |
| Cefixime | 3rd generation Cephalosporins | Broad spectrum | |||
| 7. |
Fever |
Respiratory condition |
Azithromycin | 1st generation Macrolides | Broad spectrum |
| Cefixime | 3rd generation Cephalosporins | Broad spectrum | |||
| Doxycycline | 1st generation Tetracyclines | Broad spectrum | |||
| 8. |
Diarrhea |
Gastroenteritis |
Ciprofloxacin | 2nd generation Fluoroquinolones | Broad spectrum |
| Ofloxacin + ornidazole | 2nd generation Fluoroquinolones | Broad spectrum |
4.5. WHO AWaRe Classification
4.6. Incomplete Prescriptions
5. Discussion
5.1. Qualitative Data Analysis
Theme 1: Poor Understanding Amongst Patients of What Are “Antimicrobials”
Theme 2: Limited Knowledge and Awareness of Antimicrobial Prescription Among Patients
Theme 3: Pharmacists as a Repository of Administrative Information
Theme 4: Doctors Justify Their Prescriptions on Medical Grounds
Theme 5: Limited Compliance of Prescriptions to National Guidelines
5.2. Phase 3 Analysis
5.3. Biosocial Themes
Theme 1: Minimizing Biomedical Risks of Infections Through Broad-Spectrum Antimicrobials
Theme 2: Hospital Drugs Perceived to Be of Insufficient Quality for Treating Children
Theme 3: Invisibility of Infections Promotes the “Doctor Knows All” Attitude
Theme 4: Time Pressures of Doctors’ Limits Counseling of Patients
Theme 5: Follow-Up Visits by Patients Depend on Their State of Health and Social Advice, Often at the Cost of Defying Doctors’ Advice
Theme 6: Symptoms Guiding Prescription of Antimicrobials
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alqarni, M.A.; Alshammari, N.A.; Aljohani, A.A.; Alenezi, B.H.; Alsubhi, I.M.; Al-Harbi, H.R.; Alamri, K.A.; Algthami, N.D.; Alhosayni, S.A.; Alsukhayri, O.M.; et al. The Role Of Community Pharmacists In Educating Patients About Drug Interactions And Medication Safety. 2023, 10, 276–281. [Google Scholar] [CrossRef]
- Avent, M.L.; Cosgrove, S.E.; Price-Haywood, E.G.; van Driel, M.L. Antimicrobial stewardship in the primary care setting: from dream to reality? BMC Fam. Pr. 2020, 21, 1–9. [Google Scholar] [CrossRef]
- Beyene, K.A.; Sheridan, J.; Aspden, T. Prescription Medication Sharing: A Systematic Review of the Literature. Am. J. Public Heal. 2014, 104, e15–e26. [Google Scholar] [CrossRef]
- Hindi, A.M.K.; Schafheutle, E.I.; Jacobs, S. Patient and public perspectives of community pharmacies in the United Kingdom: A systematic review. Heal. Expect. 2017, 21, 409–428. [Google Scholar] [CrossRef] [PubMed]
- Cars, O.; Mölstad, S.; Melander, A. Variation in antibiotic use in the European Union. Lancet 2001, 357, 1851–1853. [Google Scholar] [CrossRef] [PubMed]
- Charani, E. BSAC Vanguard Series: Why culture matters to tackle antibiotic resistance. J. Antimicrob. Chemother. 2022, 77, 1506–1507. [Google Scholar] [CrossRef] [PubMed]
- Mesafint, E.; Wondwosen, Y.; Dagnaw, G.G.; Gessese, A.T.; Molla, A.B.; Dessalegn, B.; Dejene, H. Study on knowledge, attitudes and behavioral practices of antimicrobial usage and resistance in animals and humans in Bahir Dar City, Northwest Ethiopia. BMC Public Heal. 2024, 24, 1–14. [Google Scholar] [CrossRef]
- Deschepper, R.; Grigoryan, L.; Lundborg, C.S.; Hofstede, G.; Cohen, J.; Van Der Kelen, G.; Deliens, L.; Haaijer-Ruskamp, F.M. Are cultural dimensions relevant for explaining cross-national differences in antibiotic use in Europe? BMC Heal. Serv. Res. 2008, 8, 123–123. [Google Scholar] [CrossRef] [PubMed]
- Foo, K.M.; Sundram, M.; Legido-Quigley, H. Facilitators and barriers of managing patients with multiple chronic conditions in the community: a qualitative study. BMC Public Heal. 2020, 20, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.G.; Adithan, C.; Harish, B.; Roy, G.; Malini, A.; Sujatha, S. Antimicrobial resistance in India: A review. J. Nat. Sci. Biol. Med. 2013, 4, 286–91. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Y.H.T.; van Doorn, R.; Van Nuil, J.I.; Lewycka, S. Dilemmas of care: Healthcare seeking behaviours and antibiotic use among women in rural communities in Nam Dinh Province, Vietnam. Soc. Sci. Med. 2024, 363, 117483. [Google Scholar] [CrossRef] [PubMed]
- Jaam, M.; Naseralallah, L.M.; Hussain, T.A.; Pawluk, S.A. Pharmacist-led educational interventions provided to healthcare providers to reduce medication errors: A systematic review and meta-analysis. PLOS ONE 2021, 16, e0253588. [Google Scholar] [CrossRef] [PubMed]
- Abdu-Aguye, S.N.; Labaran, K.S.; Danjuma, N.M.; Mohammed, S. An exploratory study of outpatient medication knowledge and satisfaction with medication counselling at selected hospital pharmacies in Northwestern Nigeria. PLOS ONE 2022, 17, e0266723. [Google Scholar] [CrossRef]
- Jonas, O.B. , Irwin, A., Berthe, F.C.J., Le Gall, F.G., Marquez, P. V., 2017. Drug-Resistant Infections: A Threat to Our Economic Future. World Bank Rep.
- Kaur, A.; Bhagat, R.; Kaur, N.; Shafiq, N.; Gautam, V.; Malhotra, S.; Suri, V.; Bhalla, A. A study of antibiotic prescription pattern in patients referred to tertiary care center in Northern India. Ther. Adv. Infect. Dis. 2018, 5, 63–68. [Google Scholar] [CrossRef]
- Knesebeck, O.v.D.; Koens, S.; Marx, G.; Scherer, M. Perceptions of time constraints among primary care physicians in Germany. BMC Fam. Pr. 2019, 20, 1–5. [Google Scholar] [CrossRef]
- Kotwani, A.; Joshi, J.; Lamkang, A.S. Over-the-Counter Sale of Antibiotics in India: A Qualitative Study of Providers’ Perspectives across Two States. Antibiotics 2021, 10, 1123. [Google Scholar] [CrossRef] [PubMed]
- Koya, S.F.; Ganesh, S.; Selvaraj, S.; Wirtz, V.J.; Galea, S.; Rockers, P.C. Consumption of systemic antibiotics in India in 2019. Lancet Reg. Heal. - Southeast Asia 2022, 4, 100025. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Shanshan, Y.; Lwin, M.O. Are threat perceptions associated with patient adherence to antibiotics? Insights from a survey regarding antibiotics and antimicrobial resistance among the Singapore public. BMC Public Heal. 2023, 23, 1–8. [Google Scholar] [CrossRef]
- Lim, J.M.; Singh, S.R.; Duong, M.C.; Legido-Quigley, H.; Hsu, L.Y.; Tam, C.C. Impact of national interventions to promote responsible antibiotic use: a systematic review. J. Antimicrob. Chemother. 2019, 75, 14–29. [Google Scholar] [CrossRef]
- Liu, C.; Liu, C.; Wang, D.; Deng, Z.; Tang, Y.; Zhang, X. Determinants of antibiotic prescribing behaviors of primary care physicians in Hubei of China: a structural equation model based on the theory of planned behavior. Antimicrob. Resist. Infect. Control. 2019, 8, 1–8. [Google Scholar] [CrossRef]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Machado-Duque, M.E.; García, D.A.; Emura-Velez, M.H.; Gaviria-Mendoza, A.; Giraldo-Giraldo, C.; Machado-Alba, J.E. Antibiotic Prescriptions for Respiratory Tract Viral Infections in the Colombian Population. Antibiotics 2021, 10, 864. [Google Scholar] [CrossRef] [PubMed]
- Marlière, G.L.L.; Ferraz, M.B.; dos Santos, J.Q. Antibiotic consumption patterns and drug leftovers in 6000 Brazilian households. Adv. Ther. 2000, 17, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Minssen, T.; Outterson, K.; Van Katwyk, S.R.; Batista, P.H.D.; Chandler, C.I.R.; Ciabuschi, F.; Harbarth, S.; Kesselheim, A.S.; Laxminarayan, R.; Liddell, K.; et al. Social, cultural and economic aspects of antimicrobial resistance. Bull. World Heal. Organ. 2020, 98, 823–823A. [Google Scholar] [CrossRef]
- Mukherjee, A.; Surial, R.; Sahay, S.; Thakral, Y.; Gondara, A. Social and cultural determinants of antibiotics prescriptions: analysis from a public community health centre in North India. Front. Pharmacol. 2024, 15, 1277628. [Google Scholar] [CrossRef]
- Muteeb, G. , Rehman, T., Shahwan, M., Aatif, M., 2023. Origin of Antibiotics and Antibiotic Resistance, and Their Impacts on Drug Development : A Narrative Review 1–54.
- Norlin, C.; Fleming-Dutra, K.; Mapp, J.; Monti, J.; Shaw, A.; Bartoces, M.; Barger, K.; Emmer, S.; Dolins, J.C. A Learning Collaborative to Improve Antibiotic Prescribing in Primary Care Pediatric Practices. Clin. Pediatr. 2021, 60, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Otaigbe, I.I.; Elikwu, C.J. Drivers of inappropriate antibiotic use in low- and middle-income countries. JAC-Antimicrobial Resist. 2023, 5, dlad062. [Google Scholar] [CrossRef] [PubMed]
- E Ryan, R.; Santesso, N.; Lowe, D.; Hill, S.; Grimshaw, J.M.; Prictor, M.; Kaufman, C.; Cowie, G.; Taylor, M. Interventions to improve safe and effective medicines use by consumers: an overview of systematic reviews. Cochrane Database Syst. Rev. 2014, 2022, CD007768. [Google Scholar] [CrossRef]
- Salam, A.; Al-Amin, Y.; Salam, M.T.; Pawar, J.S.; Akhter, N.; Rabaan, A.A.; Alqumber, M.A.A. Antimicrobial Resistance: A Growing Serious Threat for Global Public Health. Healthcare 2023, 11, 1946. [Google Scholar] [CrossRef]
- Saleh, N.; Awada, S.; Awwad, R.; Jibai, S.; Arfoul, C.; Zaiter, L.; Dib, W.; Salameh, P. Evaluation of antibiotic prescription in the Lebanese community: a pilot study. Infect. Ecol. Epidemiology 2015, 5, 27094. [Google Scholar] [CrossRef]
- Seeberg, J. An Epidemic of Drug Resistance: Tuberculosis in the Twenty-First Century. Pathogens 2023, 12, 652. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Payal, N.; Devi, L.S.; Gautam, D.; Khandait, M.; Hazarika, K.; Sardar, M. Study on Prescription Audit from a Rural Tertiary Care Hospital in North India. J. Pure Appl. Microbiol. 2021, 15, 1931–1939. [Google Scholar] [CrossRef]
- Shetty, Y.; Kamat, S.; Tripathi, R.; Parmar, U.; Jhaj, R.; Banerjee, A.; Balakrishnan, S.; Trivedi, N.; Chauhan, J.; Chugh, P.K.; et al. Evaluation of prescriptions from tertiary care hospitals across India for deviations from treatment guidelines & their potential consequences. Indian J. Med Res. 2024, 159, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Loh, M.; Mills, D. Prescription audit. Br. Dent. J. 2021, 230, 189–189. [Google Scholar] [CrossRef] [PubMed]
- Sulis, G.; Adam, P.; Nafade, V.; Gore, G.; Daniels, B.; Daftary, A.; Das, J.; Gandra, S.; Pai, M. Antibiotic prescription practices in primary care in low- and middle-income countries: A systematic review and meta-analysis. PLOS Med. 2020, 17, e1003139. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.T.; Ferreira, M.; Roque, F.; Falcão, A.; Ramalheira, E.; Figueiras, A.; Herdeiro, M.T. Physicians’ attitudes and knowledge concerning antibiotic prescription and resistance: questionnaire development and reliability. BMC Infect. Dis. 2015, 16, 1–8. [Google Scholar] [CrossRef]
- Velazquez-Meza, M.E.; Galarde-López, M.; Carrillo-Quiróz, B.; Alpuche-Aranda, C.M. Antimicrobial resistance: One Health approach. Veter- World 2022, 15, 743–749. [Google Scholar] [CrossRef]
- Worlds, B. n.d. No Title.
- Wozniak, T.M.; Cuningham, W.; Ledingham, K.; McCulloch, K. Contribution of socio-economic factors in the spread of antimicrobial resistant infections in Australian primary healthcare clinics. J. Glob. Antimicrob. Resist. 2022, 30, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Yau, J.W.; Thor, S.M.; Tsai, D.; Speare, T.; Rissel, C. Antimicrobial stewardship in rural and remote primary health care: a narrative review. Antimicrob. Resist. Infect. Control. 2021, 10, 1–33. [Google Scholar] [CrossRef]
| S.No. | ICMR Guidelines | NCDC Guidelines |
|---|---|---|
| 1. | Make a clinical diagnosis before starting treatment. | Send the patient to follow up on standard investigations to make the correct diagnosis |
| 2. | Limiting empirical treatment of antimicrobial therapy. | Antimicrobials should be started only after sending culture if facilities are available. |
| 3. | Knowing your bug before starting antimicrobial treatment. | Assessing the factors affecting the activity of antimicrobials. |
| 4 | Choosing appropriate antimicrobials for treatment and modifying them depending on culture-sensitive reports | Review antimicrobial therapy and it should be escalated or de-escalated accordingly after receipt of culture report. |
| Parameter | N (%) |
|---|---|
| Total prescription slips | 1175 |
| Total prescriptions with antimicrobials | 1151 (98%) |
| Total prescriptions with provisional diagnosis | 24 (2%) |
| Total Antimicrobial prescriptions included in EDL | 1134 (98.5%) |
| Prescriptions based on generic names | 1050 (91%) |
| Prescriptions with multiple antimicrobials | 135 (12%) |
| Average number of drugs in a slip | 2.5 |
| Demographic parameter | Characteristic N (%) |
|---|---|
| Gender | Male 525 (43%) Female 651 (57%) |
|
Age group (in years) |
1-5 years: 180 (15.6% 6-15 years: 164 (1,4%) 16-39 years: 386 (34% 40-65 years: 325 (24%) Above 65: 96 (8.4% |
| Patient location | Rural: 549 (67%) Urban: 266 (33%) |
| Name of antimicrobials | Number of prescriptions | Class of antimicrobials | Spectrum | AWaRe category |
|---|---|---|---|---|
| Amoxicillin + Clavulanic acid | 275 (24%) | Aminopenicillins + Clavulanic acid | Broad |
Access |
| Cefixime | 170 (15%) | 3rd generation Cephalosporins | Broad | Watch category |
| Azithromycin | 131 (11%) | Macrolides | Broad | Access category |
| Ciprofloxacin | 100 (9%) | 2nd generation Fluoroquinolones | Broad | Watch category |
|
Ofloxacin+ Ornidazole |
90 (8%) | Aminopenicillins | Broad | Watch category |
| Nitrofurantoin | 89 (8.1%) | Nitrofurans | Narrow | Access category |
| Doxycycline | 86 (7%) | Tetracycline | Broad | Access category |
| Amoxicillin | 75 (6.5%) | Aminopenicillins | Narrow | Access category |
|
S.No. |
Conditions mentioned by doctors requiring antimicrobial prescriptions | Antimicrobials prescribed by Medical Doctors (with MBBS) | Antimicrobials that doctors (with higher MD degrees) think need to be prescribed | Antimicrobials that were mostly prescribed as seen in the data |
|---|---|---|---|---|
| 1. | RTI | Azithromycin or Amoxicillin or Doxycycline | Amoxicillin | Amoxicillin + clavulanic acid |
| 2. |
UTI |
Nitrofurantoin | Nitrofurantoin | Syrup Cefixime (in case of children) Nitrofurantoin |
| 3. | Tonsillitis | Azithromycin | --- | Amoxicillin + clavulanic acid |
| 4. | Skin Cellulitis | Doxycycline or Amoxicillin + clavulanic acid | Amoxicillin + clavulanic acid | Amoxicillin + clavulanic acid |
| 5. | Pneumonia | Amoxicillin or Doxycycline or Azithromycin | Amoxicillin + clavulanic acid or Cefixime | Amoxicillin + clavulanic acid |
| 6. | Fever | Azithromycin or Doxycycline | Doxycycline | Azithromycin |
| ICMR guideline | NCDC guidelines | Levels of compliance based on data |
|---|---|---|
| Make a clinical diagnosis before starting any treatment. | Send the patient for follow-up on standard investigation for correct diagnosis | The clinical diagnosis (presumptive or confirmatory) was made in 52% of the slips and the rest 48% were given antimicrobial treatment based on signs and symptoms. |
| Limiting empirical treatment of antimicrobial therapy. | Antimicrobials should be started only after sending the appropriate culture if facilities are available. | From the 681 slips analyzed, 93 were sent for urine and 25 for pus culture. All patients advised for pus culture were started with empirical treatment of Amoxicillin + clavulanic acid. Out of 93 patient slips advised with urine culture, 77 were prescribed empirical treatment with Nitrofurantoin (for adults) or Cefixime (for children). Only in 16 cases, the doctor waits for the AST report. |
| Knowing your bug before starting antimicrobial treatment. | Assessing the factors affecting the activity of antimicrobials. | ASTs are rarely conducted before empirical therapy |
| Choosing appropriate antimicrobials for the treatment and modifying treatment based on AST results. | A review of antimicrobial therapy must be done and escalated or de-escalated based on the culture report. | There were only 11 such cases (out of 93 patient slips for urine culture) where the AST report led to the escalation or de-escalation of the therapy. |
| Main themes | Biomedical perspective | Social perspective of clinicians | Social perspective of patients | Social perspective of pharmacists | Interpretation of the biosocial |
|---|---|---|---|---|---|
| Antimicrobial prescription | Most prescribed drugs: Amoxiclav, Cefixime, Azithromycin | What the doctors say: Amoxicillin, Doxycycline, Azithromycin |
Limited idea about the content of the prescription | Most dispensed drug Amoxiclav for almost all ailments | Minimizing risks through initiating treatment with broad-spectrum antimicrobials |
| Order for AST culturing tests | Only 9% were advised | They say they order AST before prescribing | Limited idea about the need for AST | ASTs are mostly done only in case of recurrence of illness | ASTs not advised because of the invisibility of infection and that the “doctor knows” |
| Compliance with the Essential Drug list | 98% of the prescriptions were from EDL | Doctors have adequate guidelines | No information on what the EDL is | The list is well followed in this facility as there are sufficient medicines in the health setting | The EDL includes 14 antimicrobials, which is sufficient for most cases, except for children |
| Generic drugs | 91% of prescriptions are based on generic names | Doctors prescribe branded drugs only when not available in hospital pharmacy | Their priority is to only get free drugs | Only stock branded drugs | Prescriptions based primarily on access to drugs |
| Counseling of patients | Limited counseling done by doctors for lack of time | They say they counsel | Receive drug administration information from pharmacists | The doctors should do it, but don’t, forcing them to provide information | Social interactions between doctors (pediatrics and dermatology) promoted a limited degree of counseling |
| Follow up treatment | 30% of the patients completed their course after follow-up | Patients complete the course and report back | Course taken until they felt better and very few reported back to the doctor | Only chronic patients report back as they need to get their monthly stock of medicines | Doctor’s advice on follow-up is generally ignored |
| Symptoms guiding prescription of antimicrobials | The most common symptoms are fever, abdominal pain, burning micturition, tooth extraction | URTI. UTI, Abscess, or when there is a visible infection | Patients with a prior history of using antimicrobials demand more, most have no idea what antimicrobials are | Tonsillitis, respiratory conditions, bronchitis, not viral | Antimicrobials are prescribed to deal with changing patterns of infections |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



