Submitted:
22 January 2025
Posted:
22 January 2025
You are already at the latest version
Abstract
Background: Radial sensory nerve (RSN) injuries occur during common surgical procedures or injuries to the wrist and often result in the formation of painful neuromas. Management strategies of primary repair or secondary reconstruction are limited by poor patient satisfaction. We present a targeted muscle reinnervation (TMR) technique, its clinical outcomes, and a novel classification system for the treatment of recalcitrant RSN neuromas with transfer of the RSN to the anterior interosseous nerve (AIN). Methods: Cadaveric specimens were used to devise a classification system for transfer. RSN to AIN transfer was performed after simulated injury at three levels: proximal, at, and distal to the bifurcation. Transfer was performed in five patients with symptomatic recalcitrant RSN neuromas. Clinical and patient-reported outcomes were prospectively collected for one year. Results: A cadaveric classification system was devised to guide nerve transfer. Five patients underwent RSN to AINN transfer for symptomatic recalcitrant RSN neuromas. The mean visual analog scale (VAS) pain score significantly improved by 6±2 points. The mean Quick Disabilities of Arm, Shoulder, & Hand (DASH) scores significantly improved by 37±11 points. The wrist flexion/extension arc significantly improved by 30±14 °, and the radial/ulnar deviation arc significantly improved by 10±3 degrees. Conclusions: Our classification system can guide intraoperative decision-making for RSN to AIN transfer based on the zone of RSN injury. RSN to AIN transfer resulted in significant improvement in QuickDASH and VAS Pain scores that exceeded the established thresholds for substantial clinical benefit.
Keywords:
Introduction
Materials and Methods
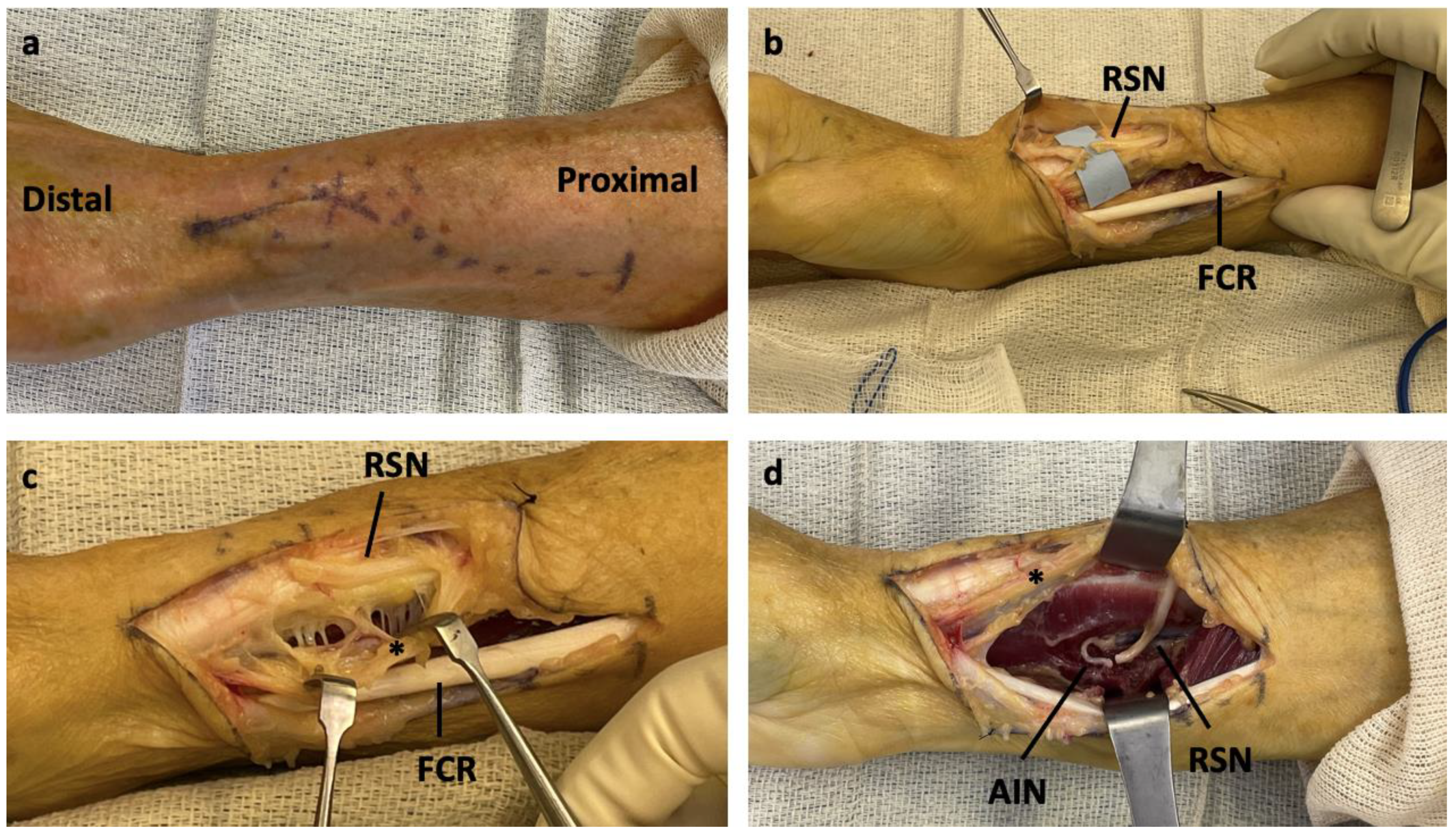
Surgical Technique
Clinical Outcomes
Patient Characteristics
Patient 1 -Zone 1 Injury
Patient 2 -Zone 2 Injury
Patient 3 -Zone 2 Injury
Patient 4 -Zone 3 Injury
Patient 5 -Zone 3 Injury
Results
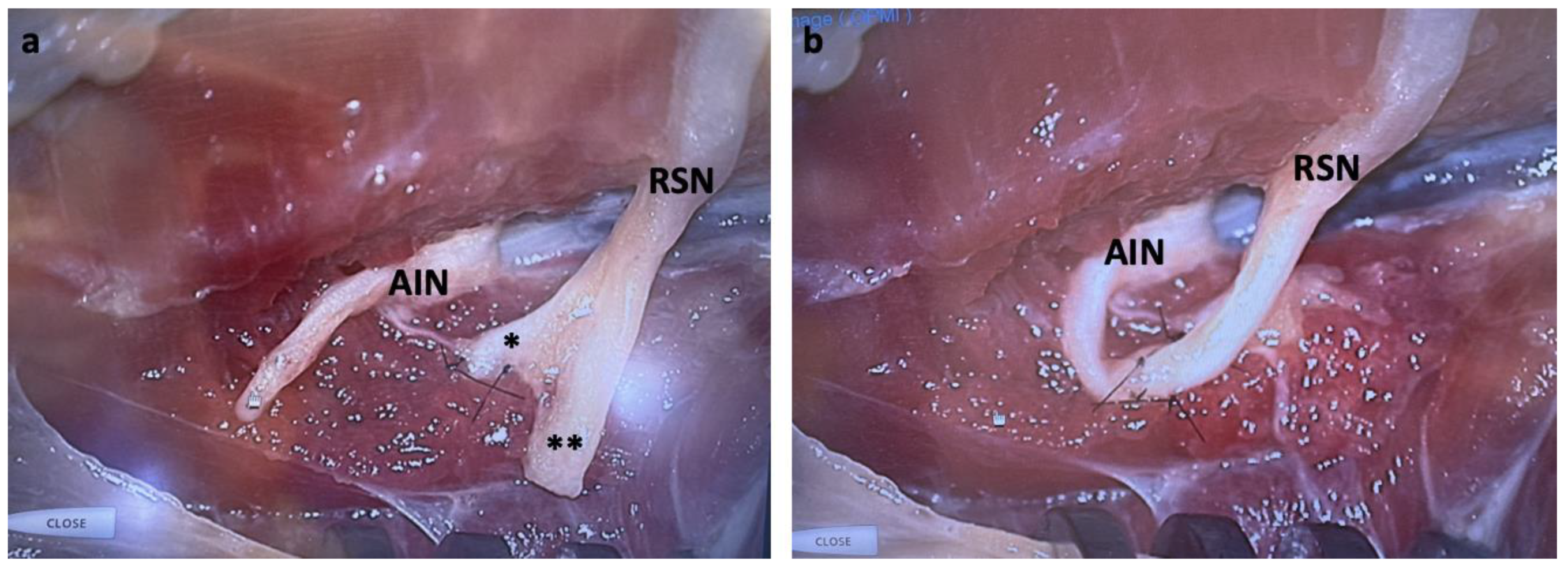
Surgical Technique
Clinical Outcomes
Discussion
Financial Disclosure Statement
References
- Watson, J.; Gonzalez, M.; Romero, A.; Kerns, J. Neuromas of the hand and upper extremity. J Hand Surg Am 2010, 35, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Eberlin, K.R.; Ducic, I. Surgical Algorithm for Neuroma Management: A Changing Treatment Paradigm. Plast Reconstr Surg Glob Open 2018, 6, e1952. [Google Scholar] [CrossRef]
- Bowen, J.B.; Wee, C.E.; Kalik, J.; Valerio, I.L. Targeted Muscle Reinnervation to Improve Pain, Prosthetic Tolerance, and Bioprosthetic Outcomes in the Amputee. Adv Wound Care (New Rochelle) 2017, 6, 261–267. [Google Scholar] [CrossRef]
- Souza, J.M.; Cheesborough, J.E.; Ko, J.H.; Cho, M.S.; Kuiken, T.A.; Dumanian, G.A. Targeted muscle reinnervation: a novel approach to postamputation neuroma pain. Clin Orthop Relat Res 2014, 472, 2984–2990. [Google Scholar] [CrossRef]
- Gottlieb, R.W.; Westenberg, R.F.; Chen, N.C.; Coert, J.H.; Eberlin, K.R. Long-Term Outcomes after Surgical Treatment of Radial Sensory Nerve Neuromas: Patient-Reported Outcomes and Rate of Secondary Surgery. Plast Reconstr Surg 2021, 147, 101–111. [Google Scholar] [CrossRef]
- Al-Qattan, M.M. Prevention and treatment of painful neuromas of the superficial radial nerve by the end-to-side nerve repair concept: an experimental study and preliminary clinical experience. Microsurgery 2000, 20, 99–104. [Google Scholar] [CrossRef]
- Aszmann, O.C.; Korak, K.J.; Rab, M.; Grunbeck, M.; Lassmann, H.; Frey, M. Neuroma prevention by end-to-side neurorraphy: an experimental study in rats. J Hand Surg Am 2003, 28, 1022–1028. [Google Scholar] [CrossRef]
- Konofaos, P.; Bassilios Habre, S.; Wallace, R.D. End-to-Side Nerve Repair: Current Concepts and Future Perspectives. Ann Plast Surg 2018, 81, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Grome, L.J.; Agrawal, N.A.; Wang, E.; Netscher, D.T. Targeted Muscle Reinnervation for Symptomatic Neuromas Utilizing the Terminal Anterior Interosseous Nerve. Plast Reconstr Surg Glob Open 2020, 8, e2979. [Google Scholar] [CrossRef] [PubMed]
- Langeveld, M.; Bruin, L.L.; Hundepool, C.A.; Power, D.; Duraku, L.S.; Zuidam, J.M. Anatomy of the Superficial Radial Nerve and Its Target Nerves for Targeted Muscle Reinnervation: An Anatomical Cadaver Study. Plast Reconstr Surg 2024, 153, 95e–100e. [Google Scholar] [CrossRef] [PubMed]
- Muneer, M. TMR for Peripheral Sensory Nerve Neuroma around the Wrist Utilizing the Distal Anterior Interosseous Nerve. Plast Reconstr Surg Glob Open 2024, 12, e5531. [Google Scholar] [CrossRef] [PubMed]
- Pierrie, S.N.; Gaston, R.G.; Loeffler, B.J. Targeted Muscle Reinnervation for Prosthesis Optimization and Neuroma Management in the Setting of Transradial Amputation. J Hand Surg Am 2019, 44, 525–e521. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, M.; Rose, A.; King, W.; Engelman, K.; Bednarz, B. Anterior Interosseous Nerve to Ulnar Nerve Transfer: A Systematic Review. JPRAS Open 2022, 32, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Stokvis, A.; Coert, J.H.; van Neck, J.W. Insufficient pain relief after surgical neuroma treatment: Prognostic factors and central sensitisation. J Plast Reconstr Aesthet Surg 2010, 63, 1538–1543. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, J.C.; Zhang, Y.; Qiu, Y.; Yoo, M.; Stephens, A.R.; Zeidan, M.; Kazmers, N.H. Establishing the Substantial Clinical Benefit in a Non-Shoulder Hand and Upper Extremity Population for the QuickDASH and PROMIS Upper Extremity and Physical Function Computer Adaptive Tests. J Hand Surg Am 2022, 47, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Randall, D.J.; Zhang, Y.; Li, H.; Hubbard, J.C.; Kazmers, N.H. Establishing the Minimal Clinically Important Difference and Substantial Clinical Benefit for the Pain Visual Analog Scale in a Postoperative Hand Surgery Population. J Hand Surg Am 2022, 47, 645–653. [Google Scholar] [CrossRef] [PubMed]
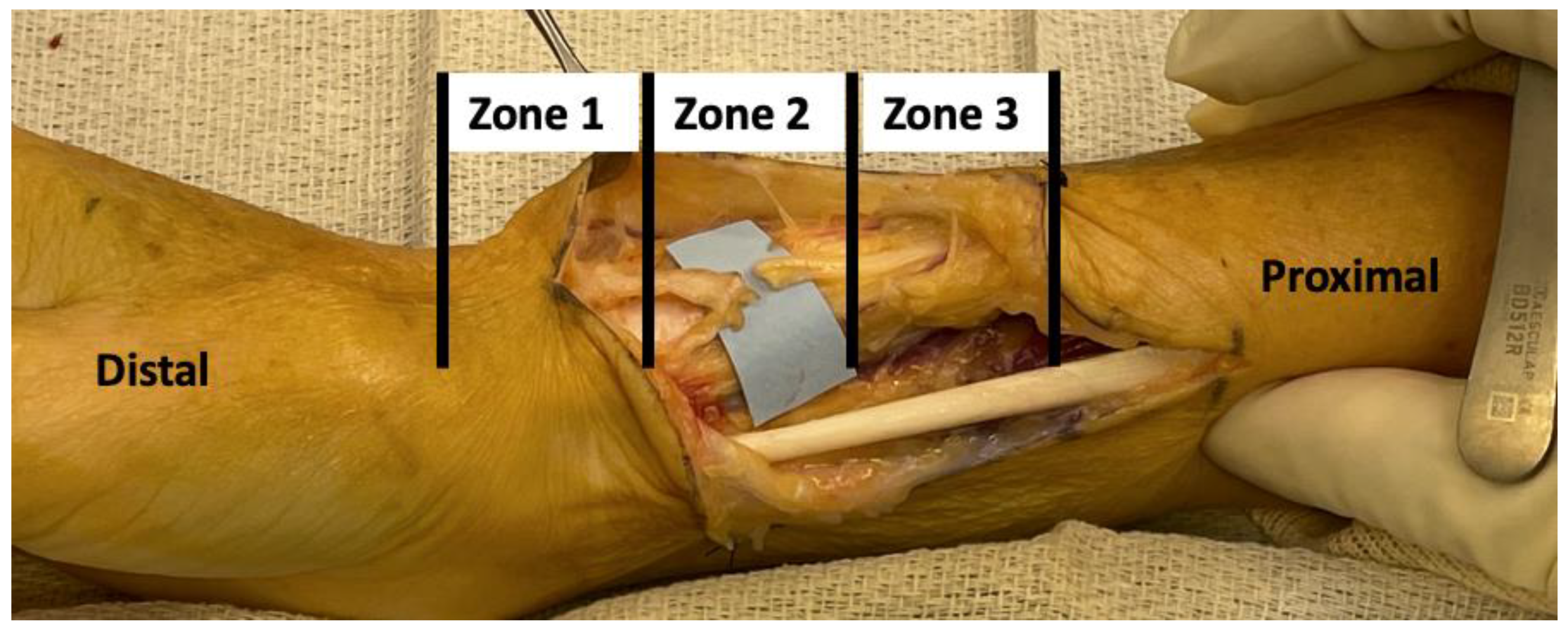

| Location | Transfer | |
|---|---|---|
| Zone 1 |
|
Radial or Ulnar RSN to Distal AIN after PQ innervation Radial or Ulnar RSN burial in PQ |
| Zone 2 |
|
Radial or Ulnar RSN to AIN at midpoint of PQ Radial or Ulnar RSN burial in PQ |
| Zone 3 |
|
|
| RSN, radial sensory nerve; AIN, anterior interosseous nerve; PQ, pronator quadratus | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



